
Submitted:
17 November 2025
Posted:
18 November 2025
You are already at the latest version
Abstract
Sarcopenia is a progressive condition in older adults characterized by reduced muscle mass, strength, and function, increasing the risk of disability and mortality. Resistance training is the primary intervention, and creatine supplementation may enhance its ef-fects. This meta-analysis assessed the impact of creatine, alone or combined with re-sistance training, on muscle mass and strength in elderly individuals with sarcopenia. A systematic search was conducted in PubMed, Scopus, and Web of Science following PRISMA 2020 guidelines, identifying 14 eligible studies. Two primary outcomes were an-alyzed: lean mass gain and strength improvement measured by leg press. Creatine com-bined with resistance training significantly increased lean mass (p = 0.0034; I² = 0%), in-dicating consistent benefits, while no significant improvement was observed in leg press strength (MD = −0.66; p = 0.83; I² = 21%). Reported adverse effects were minimal and mainly gastrointestinal. These findings suggest creatine supplementation effectively im-proves muscle mass but does not enhance leg press performance, which may not ade-quately reflect functional recovery. Future research should incorporate comprehensive functional assessments, including balance and mobility tests, to better evaluate the clini-cal impact of creatine in sarcopenia.
Keywords:
sarcopenia
; creatine supplementation
; resistance training
; elderly
; muscle mass
; muscle strength
; meta-analysis
; functional assessment
; lean mass
; leg press
1. Introduction
Sarcopenia is a progressive and generalized muscle disorder characterized by a decline in muscle mass, strength, and function, associated with increased risks of falls, disability, hospitalization, and mortality [1]. The prevalence of sarcopenia varies depending on the population and diagnostic criteria used, but it can exceed 60% in individuals with chronic conditions [2]. Major risk factors include physical inactivity, malnutrition, type 2 diabetes, smoking, and sleep disturbances. The consequences of sarcopenia extend beyond the muscular domain, negatively impacting metabolic, cognitive, and bone health [2].
Initially defined solely by the loss of muscle mass, its definition was revised in 2019 by the European Working Group on Sarcopenia in Older People (EWGSOP2). According to the EWGSOP2 group, diagnosis is based on three main criteria: muscle strength, muscle mass, and physical performance [3].
It is estimated that sarcopenia affects between 10% and 16% of the global elderly population, with higher rates in patients with specific medical conditions [4]. For example, among patients with unresectable esophageal cancer, the prevalence of sarcopenia is estimated to be as high as 66% [5], while among diabetic patients it is around 27.6% in men and 18.6% in women [6].
Sarcopenia is influenced by several risk factors, many of which are related to lifestyle and pre-existing chronic conditions. Malnutrition is a major key factor, as an inadequate diet (particularly one lacking in protein and essential nutrients) compromises the body’s ability to maintain and repair muscle tissue [7].
Sarcopenia has significant consequences for health and well-being, both in older adults and in patients with chronic medical conditions. One of the main consequences is the increased risk of falls and fractures [8]. Another significant consequence is functional decline, since loss of muscle strength and mobility reduces older adults’ ability to perform daily activities, increasing dependence on others [9]. Furthermore, sarcopenia is associated with a higher risk of prolonged hospitalization and postoperative complications, especially in patients undergoing oncology or orthopedic surgery [10].
Among the intervention strategies, resistance training (RT) has emerged as the main cornerstone of intervention [11]. Moreover, creatine supplementation has shown promising effects in enhancing muscle strength when combined with RT, more than RT alone does [12].
Creatine is a nitrogenous organic compound derived from amino acids, naturally present in the human body. It plays a crucial role in energy metabolism, particularly in muscles and the brain, where it helps store and release energy rapidly. Creatine is synthesized primarily in the liver, kidneys, and pancreas from the amino acids arginine, glycine, and methionine. It exists in two main forms: a free form, known as creatine, and a phosphorylated form, called phosphocreatine. The latter is particularly relevant in muscle energy production, as it is involved in the rapid regeneration of adenosine triphosphate (ATP), the primary “energy currency” of cells [13]. Creatine is primarily concentrated in skeletal muscle tissue, where approximately 95% of the body’s reserves are found in the form of free creatine and phosphocreatine [13].
In recent decades, creatine has become one of the most studied and used supplements in the world of fitness and sports. Commercial supplements, usually in the form of creatine monohydrate, are used to enhance physical performance, particularly in activities requiring explosive strength and sprinting. Numerous scientific studies have shown that creatine supplementation can significantly increase strength, power, and muscle mass [14]. Creatine supplementation has been shown to significantly increase phosphocreatine stores within muscles, allowing for a greater capacity to regenerate ATP during intense exercise. Creatine supplementation has been shown to increase muscle phosphocreatine levels by up to 20-40% compared to baseline values, thus improving performance in short, repetitive activities [15].
Thus, we carried out a metanalysis to investigate the effectiveness of creatine in treating sarcopenia in older adults, when combined with exercise. The objective is to understand whether this typical sports product could have clinical applications, particularly in improving muscle mass and strength in sarcopenia.
2. Materials and Methods
2.1. Search and Selection of Papers
We carried out a systematic review and meta-analysis on the effects of creatine supplementation—alone or in combination with exercise—on sarcopenia and frailty in older adults, following the PRISMA 2020 guidelines [16].
We used the string “sarcopenia AND creatine” to search across PubMed, Web of Science, and Scopus. Studies were selected based on the following predefined inclusion and exclusion criteria.
Inclusion criteria:
- study population made of elderly or frail individuals
- interventions based on creatine supplementation (with or without exercise)
- presence of a control group
- quantitative outcomes related to muscle mass and/or muscle strength were considered.
Exclusion criteria:
- studies done on animals
- protocols not yet implemented
- studies lacking control groups
- studies lacking numerical quantification of outcomes
- studies already classified as meta-analyses
- studies whose research objective did not correspond to ours
- studies that presented confounding factors.
The systematic search was completed by August 2024.
After that date, an additional search was carried out by checking the reference lists of all selected articles.
2.2. Outcomes
Two primary outcomes were considered:
OUTCOME 1: increase in lean mass at the end of the treatment period compared to baseline. The change measured is expressed in kilograms.
OUTCOME 2: increase in weight moved during the leg press exercise. This parameter is useful for monitoring strength gains over time. The measured change is expressed in kilograms.
2.3. Statistical Analysis
Each study included in the meta-analysis reported mean values for the treatment and control groups, measured both before and after the intervention, along with standard deviations (or other measures standardized as standard deviations).
The effect size for each study was expressed as the mean difference (MD), derived by comparing the mean outcome values between the treatment and control groups.
To account for between-study variability, we weighted studies according to sample size and intervention duration.
A regression model was applied with MD as the dependent variable and group and treatment duration as independent variables, quantifying the influence of each covariate on the overall treatment effect.
Confidence intervals (CIs) were calculated around the overall MD to measure the precision of the pooled estimate, and significance tests were conducted to assess the statistical significance of the overall effect.
The I2 statistic was used to assess heterogeneity between studies.
For each study, data were extracted on mean values, standard deviations, sample sizes, and duration of interventions. The effect size was calculated as the mean difference (MD) between treatment and control groups. A regression model was applied, with MD as the dependent variable, and weighting based on sample size and intervention duration.
Heterogeneity among studies was evaluated using the I2 index, and results were visually represented through forest plots to illustrate the aggregated effects.
3. Results
3.1. Literature Selection
Figure 1 describes the search and selection of the papers to be included in the metanalysis:
The meta-analysis was therefore performed on 14 studies, which were each assigned an identification number (ID) (Table 1).
Table 2 summarizes the demographic data of patients included in the 14 interventional studies. Sample sizes varied widely across trials, ranging from fewer than 10 to approximately 50 participants per arm with a total of 510 patients. Six studies included exclusively male patients, while others reported mixed or unreported sex distributions. The mean age of participants, when available, was generally in the sixth to seventh decade of life, although in some studies age was reported only as a range or by a threshold. In a subset of papers, sex or age data were not available. Both intervention and control groups were generally well matched within study.
Table 3 reports the characteristics of the interventions across the included studies. The creatine dosage varied substantially between trials, ranging from a single week of supplementation with 0.3 g/kg/day to long. term regimens of up to 32 weeks. In most protocols, creatine was administered as a daily fixed dose (typically 5 g/day) or adjusted to body weight. Several studies implemented a loading phase followed by a lower maintenance dose. In some trials, additional supplements were provided, including maltodextrin, dextrose, sucrose, or sugar
Figure 2 displays the mean difference in lean. mass change (kg) between treatment and control from baseline to end of intervention. Most studies favoured the treatment group; two (IDs 13 and 14) showed statistically significant positive effects. Tests for heterogeneity indicated no residual variability (I2 = 0%; Q
The pooled random-effects estimate showed a significant benefit of treatment on lean mass (MD = 0.73 kg, 95% CI 0.29–1.17; p = 0.003).
Meta-regression indicated provided no evidence that longer duration of treatment modified the outcome (β = −0.08; p = 0.12).
Figure 3 presents the mean difference in strength change between treatment and control groups from baseline to the end of the intervention. Individual study results range from positive to negative effects, with most confidence intervals crossing the line of no effect. The pooled random. effects estimate indicated no significant overall difference between groups (MD = −0.66; 95% CI −7.63 to 6.31; p = 0.83). Between
Meta-regression provided no evidence that treatment duration influenced the effect size (β = 0.50; p = 0.32).
3.3. Safety
Of the 14 studies considered for the meta-analysis, adverse effects to treatment were reported in only two cases, although they were mild and of limited clinical urgency.
In study 8, three side effects were significantly more frequent in the creatine group than in the placebo group. Loose stools were an adverse effect reported during the loading phase (week 1) of supplementation, while increased muscle cramps and muscle tension or tightness were adverse side effects that began between the third and fifth weeks of creatine supplementation.
Regarding gastrointestinal problems, this result is most likely attributable to the chosen supplementation protocol. As previously noted, a loading phase in which the daily amount of creatine is above 20g exposes the risk of unpleasant GI events, such as diarrhea. To address this problem, it is recommended to take the recommended dose at four different times of the day. This should, in fact, limit GI distress.
In study 14, there were only two adverse events, and this also involved gastrointestinal distress.
Regarding cramps and sensations of muscle tension, it’s difficult to assess them both because they were reported in a single case and because they aren’t adverse events typically associated with creatine use. It’s likely they’re related to the specific protocol followed in this study; based on what’s been said, it seems unlikely they can be considered typical of creatine supplementation.
We can therefore conclude that creatine intake, if performed according to the criteria indicated by the specific guidelines, does not pose a risk to the health of the subjects.
Gastrointestinal disorders may sometimes occur, which can be contained by a correct and – if necessary – more conservative supplementation protocol.
4. Discussion
As previously mentioned, two outcomes were taken into consideration: increase in lean mass and increase in strength expressed in the Leg Press exercise.
For the OUTCOME 1 there is an overall positive effect of the treatment and in most considered cases, creatine supplementation in combination with physical exercise had a positive influence on muscle mass gain.
In fact, the various intervention groups had an average and statistically significant increase in lean mass compared to the subjects in the control groups.
We can note how ‘STUDY 6’ has a very significant weight on the total studies (32.7%) and is the only one to have results that indicate the opposite of what is stated above.
It would therefore be very interesting to understand the reasons for this result or whether the dynamics of the trial itself, rather than other influencing factors, negatively affected the trial, the only one of the 14 to have had an opposite trend.
It was also highlighted that the duration of treatment, which was heterogeneous in the different studies, did not significantly influence the result, indicating that the treatment effect, at least in this model, was not duration dependent.
One limitation that may have influenced the different results obtained in the 14 studies is certainly the creatine supplementation protocol: in some cases, a loading phase was carried out followed by a maintenance phase, in others only the maintenance dose phase was administered, while in other studies the supplement was even taken only on training days (2 or 3 times a week).
The variability present in the protocols used certainly affected the speed of reaching (or not) the saturation of Phosphocreatine reserves, a fundamental factor in allowing the supplement to be effective.
The result of OUTCOME 1, however, appears to be aligned with the most recent guidelines regarding creatine supplementation, which indicate this supplement as useful in amplifying (directly or indirectly) the increase in muscle mass when combined with a resistance training program.
As regards OUTCOME 2, the treatment effect appears to be statistically NOT significant, thus indicating that, in terms of the increase in kg moved during the Leg Press exercise, creatine does not exert a useful effect on further increasing performance compared to the placebo.
While this finding doesn’t apply to all the studies considered, it’s still striking, as it contradicts common knowledge about this supplement. Creatine is used in sports specifically to increase strength and power performance, as it helps rapidly replenish phosphocreatine stores, which are involved in the rapid regeneration of adenosine triphosphate (ATP), the primary “energy currency” of cells.
The possible explanation lays in the fact that the relationship between leg press force and muscle weakness in frail sarcopenic elderly patients is complex, and leg press force alone is not a direct indicator of overall muscle weakness for several important reasons:
- The leg press is a single, isolated movement that primarily measures the force generated by the quadriceps and gluteal muscles. However, muscle weakness in sarcopenia is often generalized and affects multiple muscle groups, not just those involved in the leg press. Thus, a patient might perform relatively well on the leg press but still have significant weakness in other muscle groups that are critical for daily activities (e.g., hip flexors, ankle dorsiflexors, core muscles) [31]
- Functional weakness in sarcopenic elderly is best assessed by tasks that mimic daily activities (e.g., chair rise, walking speed, balance tests), not just by isolated muscle force. Leg press force does not capture balance, coordination, or endurance, all of which are crucial for Joint pain, arthritis, neurological disorders, and cardiovascular limitations can all affect leg press performance independently of muscle strength. For example, knee osteoarthritis may limit leg press force due to pain, not muscle weakness per se [32].
- Leg press machines may not be accessible or safe for all frail elderly patients, and results can be influenced by motivation, technique, and familiarity with the equipment. This can lead to underestimation or overestimation of true muscle strength For example, Wilson et al. found that older adults show greater variability in leg press results and less variability in technique, suggesting that rigidity in movement and lack of familiarity with the equipment may negatively impact muscle strength measurements [33].
Leg press force is just one piece of the puzzle, and it may not reflect the functional improvement. Future studies should adopt a more holistic approach to evaluating functional impairment in sarcopenic patients. This includes incorporating functional performance tests, balance assessments, and the examination of multiple muscle groups to more accurately quantify muscle weakness and its impact on daily living activities.
5. Conclusions
In conclusion, we can state that our research has led to two different outcomes.
While creatine supplementation in association with resistance training has indeed demonstrated a real potential benefit for OUTCOME 1, this is not valid and supported by OUTCOME 2, in which the intake has not demonstrated any additional beneficial effect.
Future research shall evaluate functional impact in sarcopenic patients using a more comprehensive assessment—including functional tests, balance, and evaluation of multiple muscle groups—is needed to accurately gauge muscle weakness and its impact on daily life.
That said, considering the results obtained and the limitations presented, we feel confident in stating that creatine supplementation combined with resistance training could still be a valid strategy for preventing, counteracting, and limiting muscle loss in elderly subjects at increased risk of frailty, pre-frailty, or sarcopenia. This strategy should always be monitored by a team of experts and in full compliance with the most recent guidelines on intake protocols and any contraindications.
Author Contributions
AP carried out literature search and identified relevant data in each paper; IS supervised literature search and carried out statistical analysis; MB conceptualized the paper, supervised data search and analysis and wrote the draft paper; all authors contributed to the final paper and approved it. All authors have read and agreed to the published version of the manuscript. doi:
Funding
This work was supported by grants from the Italian Ministry of Health (Ricerca Corrente) and by the IRCCS Ospedale Policlinico San Martino (Genoa, Italy). doi:
Institutional Review Board Statement
Not applicable.
Data Availability Statement
Data supporting reported results can be found in the cited articles included in the meta-analysis. No new data were created.:
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Kirk, B.; Cawthon, P.M.; Arai, H.; Ávila-Funes, J.A.; Barazzoni, R.; Bhasin, S.; Binder, E.F.; Bruyere, O.; Cederholm, T.; Chen, L.-K.; et al. The Conceptual Definition of Sarcopenia: Delphi Consensus from the Global Leadership Initiative in Sarcopenia (GLIS). Age Ageing 2024, 53, afae052. [Google Scholar] [CrossRef]
- Yuan, S.; Larsson, S.C. Epidemiology of Sarcopenia: Prevalence, Risk Factors, and Consequences. Metabolism 2023, 144, 155533. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Beaudart, C.; Zaaria, M.; Pasleau, F.; Reginster, J.-Y.; Bruyère, O. Health Outcomes of Sarcopenia: A Systematic Review and Meta-Analysis. PLOS ONE 2017, 12, e0169548. [Google Scholar] [CrossRef] [PubMed]
- Schröder, W.; Bruns, C.J. [Sarcopenia as prognostic factor of overall survival in esophageal cancer patients]. Chirurgie (Heidelb) 2022, 93, 1192–1193. [Google Scholar] [CrossRef]
- Kim, T.N.; Park, M.S.; Yang, S.J.; Yoo, H.J.; Kang, H.J.; Song, W.; Seo, J.A.; Kim, S.G.; Kim, N.H.; Baik, S.H.; et al. Prevalence and Determinant Factors of Sarcopenia in Patients with Type 2 Diabetes: The Korean Sarcopenic Obesity Study (KSOS). Diabetes Care 2010, 33, 1497–1499. [Google Scholar] [CrossRef]
- Bang, M.-J.; Lee, S.; Lee, J.W.; Kim, W.; Sung, K.W.; Seo, J.-M. Sarcopenia with Decreased Total Psoas Muscle Area in Children with High-Risk Neuroblastoma. Asian J Surg 2024, 47, 2584–2588. [Google Scholar] [CrossRef]
- Di Monaco, M.; Vallero, F.; Di Monaco, R.; Tappero, R. Prevalence of Sarcopenia and Its Association with Osteoporosis in 313 Older Women Following a Hip Fracture. Arch Gerontol Geriatr 2011, 52, 71–74. [Google Scholar] [CrossRef]
- Landi, F.; Liperoti, R.; Fusco, D.; Mastropaolo, S.; Quattrociocchi, D.; Proia, A.; Tosato, M.; Bernabei, R.; Onder, G. Sarcopenia and Mortality among Older Nursing Home Residents. J Am Med Dir Assoc 2012, 13, 121–126. [Google Scholar] [CrossRef] [PubMed]
- COVIDSurg Collaborative; GlobalSurg Collaborative Effects of Pre-Operative Isolation on Postoperative Pulmonary Complications after Elective Surgery: An International Prospective Cohort Study. Anaesthesia 2021, 76, 1454–1464. [CrossRef]
- Peterson, M.D.; Rhea, M.R.; Sen, A.; Gordon, P.M. Resistance Exercise for Muscular Strength in Older Adults: A Meta-Analysis. Ageing Res Rev 2010, 9, 226–237. [Google Scholar] [CrossRef]
- Chrusch, M.J.; Chilibeck, P.D.; Chad, K.E.; Davison, K.S.; Burke, D.G. Creatine Supplementation Combined with Resistance Training in Older Men. Med Sci Sports Exerc 2001, 33, 2111–2117. [Google Scholar] [CrossRef] [PubMed]
- Wyss, M.; Kaddurah-Daouk, R. Creatine and Creatinine Metabolism. Physiol Rev 2000, 80, 1107–1213. [Google Scholar] [CrossRef] [PubMed]
- Buford, T.W.; Kreider, R.B.; Stout, J.R.; Greenwood, M.; Campbell, B.; Spano, M.; Ziegenfuss, T.; Lopez, H.; Landis, J.; Antonio, J. International Society of Sports Nutrition Position Stand: Creatine Supplementation and Exercise. J Int Soc Sports Nutr 2007, 4, 6. [Google Scholar] [CrossRef]
- Harris, R.C.; Söderlund, K.; Hultman, E. Elevation of Creatine in Resting and Exercised Muscle of Normal Subjects by Creatine Supplementation. Clin Sci (Lond) 1992, 83, 367–374. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Gualano; B.; Macedo; R, A.; Alves; R, C.; Roschel; H.; Benatti; B, F.; et al. Creatine Supplementation and Resistance Training in Vulnerable Older Women: A Randomized Double-Blind Placebo-Controlled Clinical Trial. Experimental Gerontology 2014. [CrossRef]
- Johannsmeyer; S.; Candow; G, D.; Brahms; M, C.; Michel; D.; Zello; A, G. Effect of Creatine Supplementation and Drop-Set Resistance Training in Untrained Aging Adults. Experimental Gerontology 2016. [CrossRef]
- Rawson; S, E. ; Wehnert; L, M.; Clarkson; M, P. Effects of 30 Days of Creatine Ingestion in Older Men. European Journal of Applied Physiology 1999. [Google Scholar] [CrossRef]
- Pinto, C.L.; Botelho, P.B.; Carneiro, J.A.; Mota, J.F. Impact of Creatine Supplementation in Combination with Resistance Training on Lean Mass in the Elderly. J Cachexia Sarcopenia Muscle 2016, 7, 413–421. [Google Scholar] [CrossRef]
- Candow, D.G.; Vogt, E.; Johannsmeyer, S.; Forbes, S.C.; Farthing, J.P. Strategic Creatine Supplementation and Resistance Training in Healthy Older Adults. Appl Physiol Nutr Metab 2015, 40, 689–694. [Google Scholar] [CrossRef]
- Roschel; H.; Hayashi; P, A.; Fernandes; L, A.; Jambassi-Filho; C, J.; Hevia-Larraín; V.; et al. Supplement-Based Nutritional Strategies to Tackle Frailty: A Multifactorial, Double-Blind, Randomized Placebo-Controlled Trial. Clinical Nutrition 2021. [CrossRef]
- Aguiar; F, A. ; Januário; B, R.S.; Junior, P.; R.; Gerage; M, A.; Pina; C, F.L.; et al. Long-Term Creatine Supplementation Improves Muscular Performance during Resistance Training in Older Women. European Journal of Applied Physiology 2013. [Google Scholar] [CrossRef]
- Chrusch, M.J.; Chilibeck, P.D.; Chad, K.E.; Davison, K.S.; Burke, D.G. Creatine Supplementation Combined with Resistance Training in Older Men. Med Sci Sports Exerc 2001, 33, 2111–2117. [Google Scholar] [CrossRef] [PubMed]
- Eliot, K.A.; Knehans, A.W.; Bemben, D.A.; Witten, M.S.; Carter, J.; Bemben, M.G. The Effects of Creatine and Whey Protein Supplementation on Body Composition in Men Aged 48 to 72 Years during Resistance Training. J Nutr Health Aging 2008, 12, 208–212. [Google Scholar] [CrossRef]
- Eijnde; O, B.; Leemputte, V.; M.; Goris; M.; Labarque; V.; Taes; Y.; et al. Effects of Creatine Supplementation and Exercise Training on Fitness in Men 55–75 Yr Old. Journal of Applied Physiology 2003. [CrossRef]
- Gotshalk; A, L. ; Kraemer; J, W.; Mendonca; G, M.A.; Vingren; L, J.; Kenny; M, A.; et al. Creatine Supplementation Improves Muscular Performance in Older Women. European Journal of Applied Physiology 2008. [Google Scholar] [CrossRef]
- Gotshalk; A, L.; Volek; S, J.; Staron; S, R.; Denegar; R, C.; Hagerman; C, F.; et al. Creatine Supplementation Improves Muscular Performance in Older Men. Medicine & Science in Sports & Exercise 2002. [CrossRef]
- Candow; G, D.; Little; P, J.; Chilibeck; D, P.; Abeysekara; S.; Zello; A, G.; et al. Low-Dose Creatine Combined with Protein during Resistance Training in Older Men. Medicine & Science in Sports & Exercise 2008. [CrossRef]
- Brose, A.; Parise, G.; Tarnopolsky, M.A. Creatine Supplementation Enhances Isometric Strength and Body Composition Improvements Following Strength Exercise Training in Older Adults. J Gerontol A Biol Sci Med Sci 2003, 58, B11–B19. [Google Scholar] [CrossRef] [PubMed]
- Seene, T.; Kaasik, P. Muscle Weakness in the Elderly: Role of Sarcopenia, Dynapenia, and Possibilities for Rehabilitation. Eur Rev Aging Phys Act 2012, 9, 109–117. [Google Scholar] [CrossRef]
- Taking Care of Elderly Patients with Muscle Weakness Available online:. Available online: https://www.care365.care/resources/taking-care-elderly-patients-muscle-weakness (accessed on 22 September 2025).
- Wilson, C.; Perkin, O.J.; McGuigan, M.P.; Stokes, K.A. The Effect of Age on Technique Variability and Outcome Variability during a Leg Press. PLOS ONE 2016, 11, e0163764. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Search and selection of the papers to be included in the metanalysis.
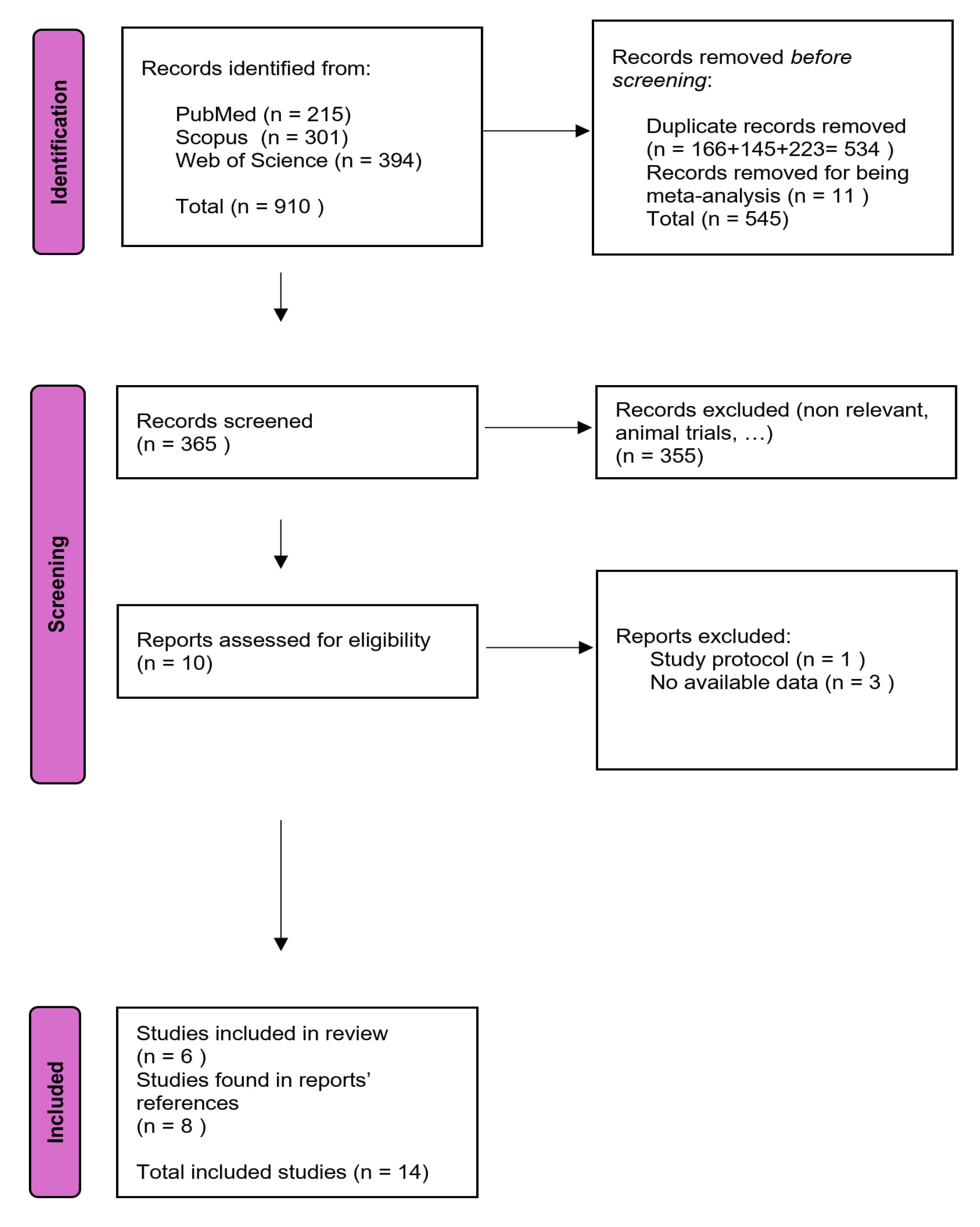
Figure 2.
Difference between groups in the change of lean mass.

Figure 3.
Difference between groups in the change of strength.
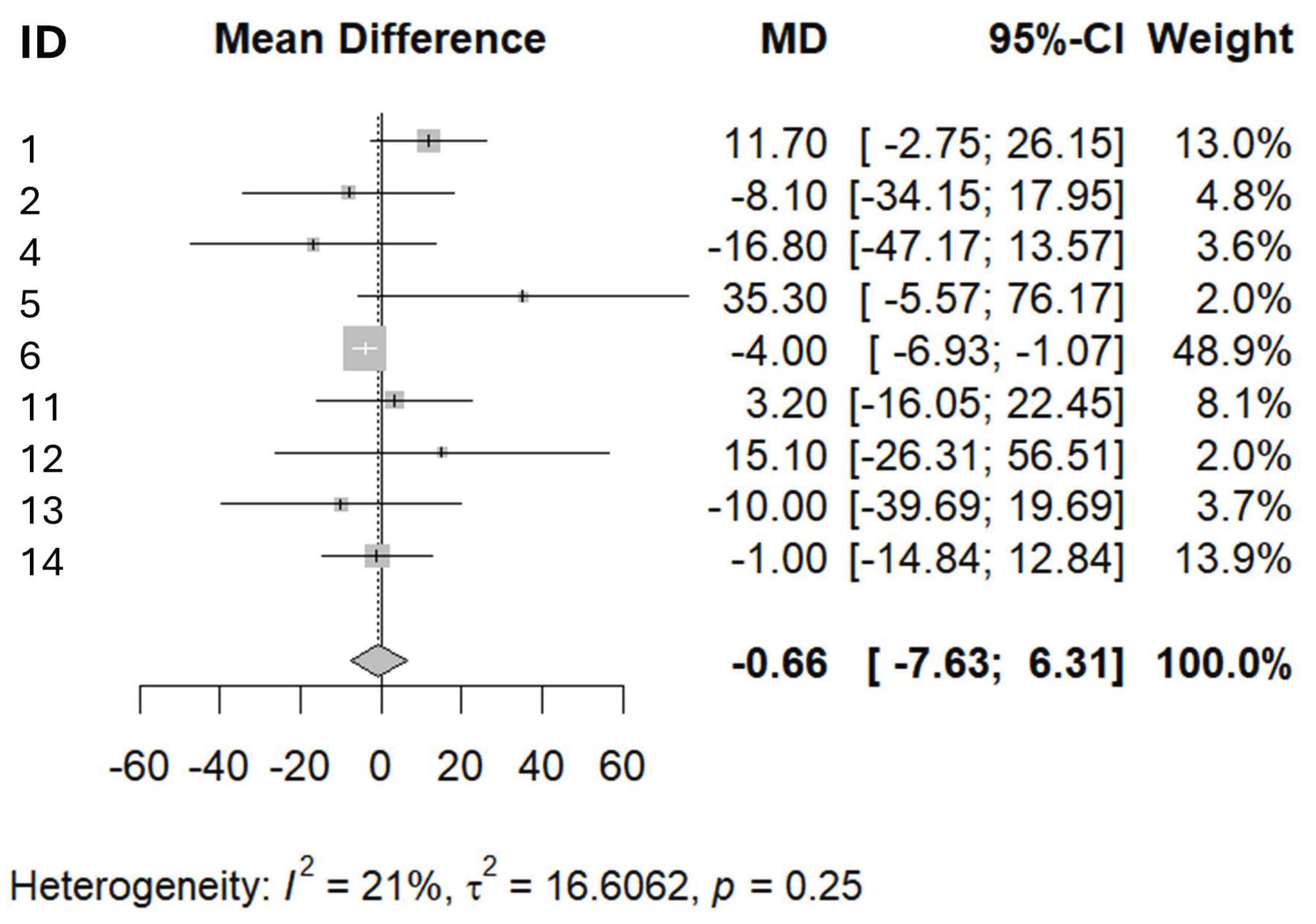

Table 1.
List of included studies.
| Number assigned to paper for data analysis | Number assigned to paper in the bibliography at the end of this paper | Paper (citation) |
|---|---|---|
| 1 | 17 | Gualano; B.; Macedo; R, A.; Alves; R, C.; Roschel; H.; Benatti; B, F.; et al. Creatine Supplementation and Resistance Training in Vulnerable Older Women: A Randomized Double-Blind Placebo-Controlled Clinical Trial. Experimental Gerontology 2014, |
| 2 | 18 | Johannsmeyer; S.; Candow; G, D.; Brahms; M, C.; Michel; D.; Zello; A, G. Effect of Creatine Supplementation and Drop-Set Resistance Training in Untrained Aging Adults. Experimental Gerontology 2016, doi:https://doi.org/10.1016/j.exger.2016.08.005. |
| 3 | 19 | Rawson; S, E.; Wehnert; L, M.; Clarkson; M, P. Effects of 30 Days of Creatine Ingestion in Older Men. European Journal of Applied Physiology 1999, doi:https://doi.org/10.1007/s004210050570. |
| 4 | 20 | Pinto, C.L.; Botelho, P.B.; Carneiro, J.A.; Mota, J.F. Impact of Creatine Supplementation in Combination with Resistance Training on Lean Mass in the Elderly. J Cachexia Sarcopenia Muscle 2016, 7, 413–421, doi:10.1002/jcsm.12094. |
| 5 | 21 | Candow, D.G.; Vogt, E.; Johannsmeyer, S.; Forbes, S.C.; Farthing, J.P. Strategic Creatine Supplementation and Resistance Training in Healthy Older Adults. Appl Physiol Nutr Metab 2015, 40, 689–694, doi:10.1139/apnm-2014-0498. |
| 6 | 22 | Roschel; H.; Hayashi; P, A.; Fernandes; L, A.; Jambassi-Filho; C, J.; Hevia-Larraín; V.; et al. Supplement-Based Nutritional Strategies to Tackle Frailty: A Multifactorial, Double-Blind, Randomized Placebo-Controlled Trial. Clinical Nutrition 2021, doi:https://doi.org/10.1016/j.clnu.2021.06.024. |
| 7 | 23 | Aguiar; F, A.; Januário; B, R.S.; Junior, P.; R.; Gerage; M, A.; Pina; C, F.L.; et al. Long-Term Creatine Supplementation Improves Muscular Performance during Resistance Training in Older Women. European Journal of Applied Physiology 2013, doi:https://doi.org/10.1007/s00421-012-2514-6. |
| 8 | 24 | Chrusch, M.J.; Chilibeck, P.D.; Chad, K.E.; Davison, K.S.; Burke, D.G. Creatine Supplementation Combined with Resistance Training in Older Men. Med Sci Sports Exerc 2001, 33, 2111–2117, doi:10.1097/00005768-200112000-00021. |
| 9 | 25 | Eliot, K.A.; Knehans, A.W.; Bemben, D.A.; Witten, M.S.; Carter, J.; Bemben, M.G. The Effects of Creatine and Whey Protein Supplementation on Body Composition in Men Aged 48 to 72 Years during Resistance Training. J Nutr Health Aging 2008, 12, 208–212, doi:10.1007/BF02982622. |
| 10 | 26 | Eijnde; O, B.; Leemputte, V.; M.; Goris; M.; Labarque; V.; Taes; Y.; et al. Effects of Creatine Supplementation and Exercise Training on Fitness in Men 55–75 Yr Old. Journal of Applied Physiology 2003, doi:https://doi.org/10.1152/japplphysiol.00891.2002. |
| 11 | 27 | Gotshalk; A, L.; Kraemer; J, W.; Mendonca; G, M.A.; Vingren; L, J.; Kenny; M, A.; et al. Creatine Supplementation Improves Muscular Performance in Older Women. European Journal of Applied Physiology 2008, doi:https://doi.org/10.1007/s00421-007-0580-y. |
| 12 | 28 | Gotshalk; A, L.; Volek; S, J.; Staron; S, R.; Denegar; R, C.; Hagerman; C, F.; et al. Creatine Supplementation Improves Muscular Performance in Older Men. Medicine & Science in Sports & Exercise 2002, doi:https://doi.org/10.1097/00005768-200203000-00026. |
| 13 | 29 | Candow; G, D.; Little; P, J.; Chilibeck; D, P.; Abeysekara; S.; Zello; A, G.; et al. Low-Dose Creatine Combined with Protein during Resistance Training in Older Men. Medicine & Science in Sports & Exercise 2008, doi:https://doi.org/10.1249/MSS.0b013e318176b310. |
| 14 | 30 | Brose, A.; Parise, G.; Tarnopolsky, M.A. Creatine Supplementation Enhances Isometric Strength and Body Composition Improvements Following Strength Exercise Training in Older Adults. J Gerontol A Biol Sci Med Sci 2003, 58, B11–B19, doi:10.1093/gerona/58.1.B11 |
Table 2.
Demographic data of the patients included in the included papers.
| Paper number (assigned for data analysis) | Treatment group |
Control group | ||||
|---|---|---|---|---|---|---|
| ID | Total N | Males (N) | Age, years | Total N | Males (N) | Age, years |
| 1 | 30 | 0 | ~72 | 30 | 0 | ~72 |
| 2 | 14 | 7 | 58.0 ± 3.0 | 17 | 10 | 57.6 ± 5.0 |
| 3 | 10 | 10 | 60–82 | 10 | 10 | 60–82 |
| 4 | 13 | NA | 66.5 ± 4.5 | 14 | NA | 67.2 ± 5.1 |
| 5 | 27 | 14 | 50–71 | 12 | 3 | 50–71 |
| 6 | ~50 | 0 | 72 ± 6 | ~50 | 0 | 72 ± 6 |
| 7 | 9 | 0 | 64.9 ± 5.0 | 9 | 0 | 64.9 ± 5.0 |
| 8 | 16 | 16 | 70.4 ± 1.6 | 14 | 14 | 71.1 ± 1.8 |
| 9 | 21 | 21 | 48–72 | 10 | 10 | 48–72 |
| 10 | 23 | 23 | 55–75 | 23 | 23 | 55–75 |
| 11 | 15 | 0 | 63.3 ± 1.2 | 12 | 0 | 63.0 ± 1.1 |
| 12 | 10 | 10 | 59–72 | 8 | 8 | 59–72 |
| 13 | 23 | 23 | 59–77 | 12 | 12 | 59–77 |
| 14 | 14 | 8 | >65 | 14 | 7 | >65 |
| NA = not available | ||||||
Table 3.
Protocols of creatine administration and physical exercise.
| Paper number (assigned for data analysis) | Creatine dose (as per protocol) | Additional supplements | Duration, weeks | Physical exercise |
|---|---|---|---|---|
| 1 | 20 g/day for 5 days, then 5 g/day | 0.1 g/kg/day maltodextrin | 24 | 2x/week RT |
| 2 | 0.1 g/kg/day | 0.1g/kg/day of maltodextrin | 12 | RT |
| 3 | 5 g x 4/day x 10 days, then 4g/day x 20 days | 7 g dextrose x 4/day x 10 days, then 6.8g dextrose x 20 days | 4.3 | Not specified |
| 4 | 5 g/day | 100 g of lemon-flavoured maltodextrin (on training days only) | 12 | 3x/week RT |
| 5 | 0.1 g/kg occasional (2x15g/day) | Maltodextrin from corn starch (2x15g/day) | 32 | RT |
| 6 | 3g x2/day | either whey (15g x2/day) or placebo (corn starch) (15g x2/day) |
16 | RT |
| 7 | 5 g/day | CHO drink | 12 | 3x/week RT |
| 8 | 0.3 g/kg/day x 5days, 0.07g/kg/day thereafter | sucrose-flour mixture to mask the substance | 12 | 3x/week RT |
| 9 | Loading phase: 7g/day Maintenance phase: 5g/day (both only on training days) |
Some subjects received 35 g/day wheat proteins | 1+14 (loading+treatment phases) | 3x/week RT |
| 10 | 5g/ day | none | 24 (6 months) | 2-3 sessions/ week |
| 11 | 0.3 g/kg/day x 7 days |
none | 1 week supplementation protocol | familiarization tests, but the training program after that is not specified |
| 12 | 0.3 g/kg/day x 7days | none | 1 | 3x/week RT |
| 13 | 0.1 g·kg−1/day only on training days | Proteins, 0.1 g·kg−1/day only on training days | 10 | 3 days/week |
| 14 | 5g/day | 2g dextrose | 14 | 3x week RT |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



