Submitted:
13 November 2025
Posted:
14 November 2025
You are already at the latest version
Abstract
Chronic allograft dysfunction (CLAD) is the main cause of graft loss after lung transplantation (LTR). Within the immunological factors involved in CLAD development, the antibody-mediated rejection (ABMR) has the most impact. However, ABMR diagnosis is difficult due to the limited sensitivity of histopathological, immunhistochemical, and immunological criteria currently used. Growing evidence is demonstrating the impact of molecular mismatch in ABMR; here, we ought to assess the potential role of molecular mismatch in CLAD development. A total of 457 LTR were recruited for the study, with HLA type from donors and recipients to assess molecular mismatch, and with a minimum follow-up of 180 days. The combination of molecular mismatch in class-II (HLA-EMMA and HLA-Matchmaker algorithms) with EMMA DR score >12 and antibody verified eplet mismatch in DRB1345 (AbV DRB1345) > 3 predicts CLAD development independently of ex-smoker, prolonged period of hospitalization (>33 days), acute cellular rejection (ACR), and ABMR. The HR of the prediction model for molecular mismatch in class-II was 1.52 (1.01-2.56, p=0.045). This observation could point to a potential role of poor molecular mismatch in class-II to fill the gap of underdiagnosis of ABMR, previous to CLAD development. Prospective studies should be addressed to confirm the utility of molecular mismatch in the identification of patients at risk of CLAD development.
Keywords:
molecular mismatch
; immunological risk
; CLAD
; prediction
; lung transplant
; ABMR
; ACR
1. Introduction
Chronic Lung Allograft Dysfunction (CLAD) is the main cause of graft loss after lung transplantation, directly impacting both patient and graft survival [1]. Immunological and non-immunological factors are involved in CLAD development, but other factors remain to be elucidated [2].
Within the immunological factors, the antibody-mediated rejection (ABMR) is well characterized. However, ABMR diagnosis in lung transplantation remains elusive. The last Banff Lung report criteria classification points to a multidimensional approach for ABMR diagnosis, where all immunological, histopathological, and immunohistochemical criteria should be fulfilled [3]. There are patients with suspicion of ABMR without donor-specific anti-HLA antibodies (DSA), together with low sensitivity of histopathological and immunohistochemical findings, which make ABMR diagnosis a real challenge [3,4].
Here, we focus on the immunological factors. The classical way to assess immunological compatibility is based on human leukocyte antigen (HLA) match, where the most ABDR HLA mismatch, the worst long-term graft survival in solid organ transplantation, in the kidney [5], liver [6] and heart [7] including lung transplantation [8].
New molecular biology methods in HLA typing have enabled the development of novel approaches to assess donor-recipient compatibility, such as molecular mismatch, based on different algorithms that could better define the immunological risk of donor-recipient pairs. In fact, there is increasing evidence supporting that high molecular mismatch increases the risk of de novo anti-HLA antibodies, using a single algorithm as HLA-Matchmaker [9], PIRCHE [10] or combined algorithms [11,12]. Moreover, the combination of algorithms improved the prediction of ABMR in pediatric cardiac allografts [13].
We aim to study the potential role of MM algorithms in CLAD prediction after lung transplantation.
2. Results
2.1. CLAD Development in Lung Transplantation
A total of 592 lung transplant recipients (LTR) were performed in our institution from 2010 to 2024. Ninety-five LTR without HLA type data from donor or recipient were discarded. In addition, 40 of 497 remaining LTR had a follow-up less than 6 months. Finally, a total of 457 lung transplant recipients (LTR) were included in the analysis. The main parameters studied are summarized in Table 1.
The median of censored follow-up was 4.7 years, and the proportion of female lung transplants was 39.4%. One hundred and sixty out of 457 (35%) patients developed CLAD. The difference in the demographic, immunological, and clinical variables between groups of LTR developing CLAD or not is summarized in Supplementary Table 1 and Table 2.

Table 2.
Frequency comparison and Kaplan Meier analysis of parameters included in the study: Recipients, donors, lung transplants, clinical and immunological parameters.
Table 2.
Frequency comparison and Kaplan Meier analysis of parameters included in the study: Recipients, donors, lung transplants, clinical and immunological parameters.
| Parameter | No-CLAD group Frequency (total valid cases) |
CLAD group Frequency (total valid cases) |
Chi-square (p-value) | Kaplan-Meier Log-rank test (p-value) |
|
|---|---|---|---|---|---|
| Recipient | Recipient sex (% female) | 43.43 (297) | 31.88 (160) | 0.0208 | 0.0082 |
| Recipient age bin | 26.60 (297) | 21.88 (160) | 0.3173 | 0.4561 | |
| Recipient smoker (never) | 24.24 (297) | 21.02 (157) | 0.5107 | 0.0198 | |
| Tobacco consumption bin | 22.52 (222) | 21.01 (119) | 0.8535 | 0.9966 | |
| Hypertension (yes) | 21.55 (297) | 17.09 (158) | 0.3128 | 0.7294 | |
| Diabetes (yes) | 7.74 (297) | 11.39 (158) | 0.2619 | 0.9251 | |
| Dyslipidemia (yes) | 36.70 (297) | 24.36 (156) | 0.0105 | 0.7057 | |
| Size bin | 21.01 (276) | 25.00 (120) | 0.4561 | 0.2142 | |
| Weight bin | 24.19 (277) | 26.67 (120) | 0.6906 | 0.7257 | |
| BMI bin | 23.55 (276) | 27.50 (120) | 0.4776 | 0.5464 | |
| LAS score bin | 25.10 (255) | 25.00 (92) | 1.0000 | 0.9220 | |
| Donor | Donor sex (% female) | 50.51 (297) | 44.38 (160) | 0.2490 | 0.1152 |
| Hypertension (yes) | 33.68 (285) | 31.79 (151) | 0.7691 | 0.8568 | |
| Diabetes (yes) | 10.47 (277) | 3.62 (138) | 0.0274 | 0.1229 | |
| Donor smoker (yes) | 32.06 (287) | 39.47 (152) | 0.1474 | 0.4799 | |
| Donor age bin | 26.94 (297) | 17.50 (160) | 0.0316 | 0.2675 | |
| Donor size bin | 17.69 (294) | 19.62 (158) | 0.7049 | 0.2864 | |
| Donor weight bin | 24.91 (293) | 20.13 (159) | 0.3008 | 0.5310 | |
| Immunological | Anti-HLA class-I antibodies pre transplant (yes) | 9.02 (255) | 4.26 (94) | 0.2106 | 0.3894 |
| Anti-HLA class-II antibodies pre transplant (yes) | 5.10 (255) | 4.26 (94) | 0.9648 | 0.7539 | |
| Anti-MICA antibodies pre transplant (yes) | 1.01 (255) | 0.63 (94) | 1.0000 | 0.9468 | |
| Antibody verified eplet mismatch All bin | 20.20 (297) | 25.00 (160) | 0.2870 | 0.4267 | |
| Antibody verified eplet mismatch ABC bin | 20.20 (297) | 23.75 (160) | 0.4460 | 0.1478 | |
| Antibody verified eplet mismatch DQDR bin | 20.88 (297) | 27.50 (160) | 0.1377 | 0.7146 | |
| Antibody verified eplet mismatch DQA1DQB1 bin | 18.86 (297) | 23.13 (160) | 0.3372 | 0.8879 | |
| Antibody verified eplet mismatch DRB1345 bin | 20.88 (297) | 25.00 (160) | 0.3722 | 0.0864 | |
| PIRCHE II score bin | 26.60 (297) | 21.25 (160) | 0.2498 | 0.1915 | |
| PIRCHE II HLA-A bin | 24.58 (297) | 22.50 (160) | 0.7021 | 0.9443 | |
| PIRCHE II HLA-B bin | 26.26 (297) | 21.25 (160) | 0.2827 | 0.1881 | |
| PIRCHE II HLA-C bin | 23.91 (297) | 26.25 (160) | 0.6596 | 0.5086 | |
| PIRCHE II HLA-DQA1 bin | 24.58 (297) | 25.63 (160) | 0.8941 | 0.4268 | |
| PIRCHE II HLA-DQB1 bin | 26.26 (297) | 22.50 (160) | 0.4393 | 0.2650 | |
| PIRCHE II HLA-DRB1 bin | 24.58 (297) | 24.38 (160) | 1.0000 | 0.6668 | |
| EMMA score HLA-All bin | 22.90 (297) | 26.88 (160) | 0.4055 | 0.3461 | |
| EMMA score HLA-ABC bin | 25.59 (297) | 23.75 (160) | 0.7489 | 0.9439 | |
| EMMA score HLA-A bin | 22.90 (297) | 24.38 (160) | 0.8100 | 0.2867 | |
| EMMA score HLA-B bin | 23.91 (297) | 21.25 (160) | 0.5981 | 0.5953 | |
| EMMA score HLA-C bin | 20.54 (297) | 20.00 (160) | 0.9883 | 0.7256 | |
| EMMA score HLA-DQABDR bin | 22.22 (297) | 26.88 (160) | 0.3182 | 0.4498 | |
| EMMA score HLA-DQA1 bin | 14.48 (297) | 21.88 (160) | 0.0609 | 0.0936 | |
| EMMA score HLA-DQB1 bin | 22.90 (297) | 21.88 (160) | 0.8952 | 0.6383 | |
| EMMA score HLA-DR bin | 20.20 (297) | 25.63 (160) | 0.2245 | 0.0391 | |
| Lung transplant | Donation (DBD) | 74.07 (297) | 81.25 (160) | 0.1069 | 0.7096 |
| Type of transplant (Unipulmonar) | 14.48 (297) | 31.25 (160) | <0.0001 | <0.0001 | |
| Indication (Elective) | 98.32 (297) | 95.00 (160) | 0.0820 | 0.1855 | |
| CMV pairing (High risk) | 14.74 (285) | 10.00 (150) | 0.2142 | 0.4139 | |
| Donor pO2 (mmHg) | 23.84 (281) | 25.48 (157) | 0.7904 | 0.3530 | |
| ECMO during surgery (yes) | 11.49 (296) | 9.49 (158) | 0.6220 | 0.2436 | |
| Ischemic time first bin | 23.57 (297) | 27.22 (158) | 0.4574 | 0.1018 | |
| Ischemic time second bin | 22.92 (253) | 26.36 (110) | 0.5676 | 0.4334 | |
| Surgery time bin | 25.30 (253) | 24.73 (93) | 1 | 0.1341 | |
| Transfusion (yes) | 30.20 (255) | 37.23 (94) | 0.2626 | 0.9374 | |
| Number of packed RBC bin | 22.08 (77) | 17.14 (35) | 0.7286 | 0.3023 | |
| Surgical reintervention (yes) | 6.40 (297) | 9.43 (159) | 0.3225 | 0.0835 | |
| Clinical | Induction (yes) | 90.64 (267) | 71.70 (106) | <0.0001 | 0.0327 |
| Calcineurin inhibitor (tacrolimus) | 97.25 (255) | 91.49 (94) | 0.0395 | 0.0197 | |
| Antimetabolite (mycophenolate) | 99.61 (255) | 100.00 (94) | 1 | 0.5640 | |
| Tracheostomy (yes) | 4.31 (255) | 6.38 (94) | 0.6056 | 0.2502 | |
| Hospitalization bin | 20.27 (296) | 29.94 (157) | 0.0286 | 0.0245 | |
| Intubation bin | 18.15 (248) | 23.08 (91) | 0.3890 | 0.4635 | |
| Primary graft dysfunction (yes) | 27.95 (297) | 26.25 (160) | 0.7810 | 0.9693 | |
| Primary graft dysfunction grade 3 (yes) | 14.29 (126) | 14.29 (133) | 1 | 0.3167 | |
| Acute cellular rejection (yes) | 41.08 (297) | 66.88 (160) | <0.0001 | 0.0002 | |
| Antibody mediated rejection (yes) | 3.37 (297) | 17.50 (160) | <0.0001 | <0.0001 | |
* BMI: body mass index; IQR interquartile range; DBD: Donation after Brain Death; RBC: Red Blood Cells; SD: standard deviation. All quantitative parameters were binned (bin) as described in section 4.5.3. p values <0.05 (bold) and <0.01 (italic).
Patients who developed CLAD were significantly younger, had higher body weight at listing, lower donor pO2, and experienced longer hospitalization times after transplantation. With increased frequency of single transplant, acute cellular rejection (ACR), antibody-mediated rejection (ABMR), and decreased frequency of recipient dyslipidemia, donor diabetes, induction treatment, less tacrolimus as calcineurin inhibitor treatment, and a low rate of females. Of note, since 2016, all lung transplant recipients have received basiliximab induction, and cyclosporine has no longer been used as a calcineurin inhibitor treatment. The last single-lung transplant was performed in 2019. For these reasons, the last variables were no longer selected for further analysis of CLAD prediction models.
2.2. Immunological Variables Associated with CLAD-Free Survival
Within the immunological variables, only a high EMMA-DQA score was significantly increased in the CLAD development group, median [interquartile range (IQR)] of 8 [0-16] vs 10 [0-18] in LTR without and with CLAD development, p=0.04. The results of the remaining molecular mismatch variables are summarized in Supplementary Table 1. To perform survival analysis, all molecular mismatch variables were transformed into binary based on 75 percentile [14], and combined each molecular mismatch algorithm as described in the Materials and Methods section to focus on the higher value of each variable with the risk of CLAD development, and the Kaplan Meier test was performed. The results of the log-rank test, area under the curve, sensitivity, and specificity are described in Supp Table 2. Within the new variables, calculated only molecular mismatch in DR (combination of HLA-Matchmaker and HLA-EMMA) was significantly associated with shorter time to CLAD development in our cohort, p=0.0055. The combination of antibody-verified eplet mismatch in DRB1345 (AbV DRB1345) > 3 and EMMA DR score >12 was associated with CLAD, with very low sensitivity (19.4%) but high specificity (87.5%). This variable (identified as MM-DR2 was further used as a high immunological parameter.
2.3. Prediction Model for CLAD
The next step was to assess the time free of CLAD survival using all demographic, clinical, and immunological parameters in a univariate Cox regression analysis. The results of each parameter are summarized in Supp Table 3. To perform a multivariate regression model to predict CLAD development, the significant parameters in the univariate Cox analysis were selected (recipient sex, never smoker, EMMA score DR bin, Snow score HLA-C bin, days of hospitalization bin, ACR, ABMR, and high immunological risk variable DR2), and parameters previously described [15,16] as being involved in CLAD were also included (recipient and donor age, donor smoker, donor pO2, ischemic time of the first lung, type of donation, higher risk of CMV pairing and Grade 3 of primary graft dysfunction).
In order to test the robustness of variable selection for the Cox model and to address collinearity among variables, we conducted a penalized Cox model using Lasso selection, and a further stepwise selection based on the Akaike Information Criterion (AIC) approach was performed. The proportional hazards assumption was tested to evaluate a constant effect over time. The final variables included in the model were: ACR, ABMR, high immunological risk variable DR2, Recipient never smoker, and hospitalization bin. The DR2 variable was independently associated with CLAD development of humoral and cellular rejection, recipient smoker, and days at Hospital post transplant_bin (>33 days), with a hazard ratio (HR) of 1.499 (p=0.05) (Table 3). The hazard ratio and p-values of the variables included in the model are depicted in Figure 1.
Table 3.
Multivariate Cox model for CLAD development prediction.
| Parameter | Variable | Univariate | Multivariate (Lasso+AIC) (n=215) |
Multivariate Final Model (n=457) |
||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HR | 95CI | p-value | HR | 95CI | p-value | HR | 95CI | p-value | ||||||||||||||||||
| Recipient | Recipient sex (male) | 1.56 | 1.12-2.18 | 0.0087 | ||||||||||||||||||||||
| Recipient smoker (never) | 0.63 | 0.43-0.93 | 0.0209 | 0.59 | 0.37-0.93 | 0.0225 | 0.58 | 0.39-0.86 | 0.0072 | |||||||||||||||||
| Donor | Donor sex (male) | 1.28 | 0.94-1.76 | 0.1163 | ||||||||||||||||||||||
| Donor age_bin | 0.79 | 0.53-120 | 0.2690 | |||||||||||||||||||||||
| Donor smoker | 1.13 | 0.81-1.56 | 0.4798 | |||||||||||||||||||||||
| Immunological | EMMA score HLA-DR_bin | 1.45 | 1.02-2.07 | 0.0403 | ||||||||||||||||||||||
| MM-DR2 | 1.74 | 1.17-2.57 | 0.0061 | 1.62 | 1.02-2.58 | 0.0426 | 1.50 | 1.01-2.26 | 0.0452 | |||||||||||||||||
| Lung transplant | Donation (DBD) | 1.08 | 0.72-1.62 | 0.7091 | ||||||||||||||||||||||
| CMV pairing (High risk) | 0.80 | 0.47-1.37 | 0.4147 | |||||||||||||||||||||||
| Donor pO2_bin | 1.19 | 0.83-1.70 | 0.3532 | |||||||||||||||||||||||
| Ischemic time first_bin | 1.34 | 0.94-1.90 | 0.1027 | |||||||||||||||||||||||
| Clinical | Hospitalization days_bin | 1.48 | 1.05-2.08 | 0.0254 | 1.42 | 0.94-2.15 | 0.0983 | 1.55 | 1.09-2.20 | 0.0141 | ||||||||||||||||
| PGD 3 (yes) | 1.28 | 0.79-2.09 | 0.3186 | |||||||||||||||||||||||
| ACR | 1.86 | 1.34-2.58 | <0.0001 | 1.69 | 1.10-2.60 | 0.0173 | 1.51 | 1.07-2.13 | 0.0180 | |||||||||||||||||
| ABMR | 3.84 | 2.54-5.80 | <0.0001 | 2.70 | 1.48-4.93 | 0.0013 | 2.91 | 1.88-4.51 | <0.0001 | |||||||||||||||||
* ABMR antibody antibody‐mediated rejection, ACI: Akaike Information Criteria, ACR: acute cellular rejection,
DBD: Donation after Brain Death, PGD: primary graft dysfunction.
2.4. Dynamic Model for CLAD Prediction
In order to evaluate the dynamic impact of the CLAD prediction model, which incorporates five variables at different stages of lung transplantation, we analyzed the sequential effect of each risk factor, from baseline through the occurrence of humoral rejection, on the risk of developing CLAD. We further assessed the cumulative risk of CLAD associated with each additional parameter relative to the optimal scenario. The mean CLAD-free survival decreased to 3,714 days among smokers. For smokers with high immunological risk, mean CLAD-free survival decreased to 2,761 days. If these lung transplant recipients also remained hospitalized for over 33 days post-transplant, CLAD-free survival declined further to 1,966 days; with the onset of ACR, this dropped to 1,461 days, and with confirmed ABMR, the mean CLAD-free survival was 928 days. The comparative risks under each scenario are illustrated in Figure 2.
3. Discussion
CLAD development is the main clinical event affecting lung allograft survival. However, its multifactorial nature makes its approach very complicated. One of the main factors is the development of DSA and ABMR. However, the diagnosis of ABMR in lung transplantation is currently a challenge due to the lack of immunohistochemical and immunopathological markers. Furthermore, in suspected humoral rejection after lung transplantation, anti-HLA antibodies are often not detected in the circulation. It has been proposed that these DSA may infiltrate lung tissue [17]. In fact, recently, the detection of graft DSA has demonstrated better sensitivity for ABMR diagnosis than peripheral DSA [17]. Furthermore, the development of non-HLA antibodies has also been implicated in the humoral component of CLAD in a multicentre study [18]. In our lung transplant cohort, the non-HLA antibodies were also associated with ABMR[19].
The main reason eliciting an alloimmune response is the antigen HLA mismatch between donor and recipient, as demonstrated several decades ago. The greater the HLA mismatch, the lower the graft survival in solid organ transplantation [20,21]. However, this observation was not confirmed in the collaborative transplant study in LTR, where the well-matched HLA pairs did not show superior graft survival in the early stages after lung transplantation, probably motivated by the impact of infections and surgical issues [8]. Some studies confirm that a greater number of HLA disparities is related to the development of CLAD [22]. It would be necessary to have tools to minimize the risk of developing CLAD in LTRs to increase graft and patient survival. These studies have been conducted using HLA typing tools that determine disparity at the antigenic level. However, improvements in molecular biology techniques have allowed for studying HLA typing at the allelic level, facilitating the identification of disparities between donor and recipient through molecular disparities, which has been proposed as a new tool to define immunological risk between donor and recipient. However, the lack of large multicenter studies is delaying the implementation of these methods in the workflow of histocompatibility laboratories. Greater molecular disparity measured by class II eplet load has been shown to be useful in identifying patients at risk for developing de novo DSA in renal [23,24] and lung transplantation [25]. The risk epitope mismatch in DQA1*05 has been previously identified as a major cause of the development of de novo anti-HLA antibodies in cardiothoracic transplantation [26]. We did not include this analysis in our study; however, given the evidence presented, it will be a factor to consider in future CLAD predictive models.
A large multicentre cohort in kidney transplantation confirmed the utility of molecular mismatch in class-II, which was independently associated with ABMR [27]. In some studies, it has been observed that the combination of different molecular mismatch algorithms in class-II increased the predictive capacity of ABMR [25].
The majority of the studies on molecular mismatch were focused on de novo anti-HLA antibody or ABMR, but not on chronic rejection. Here, we ought to study the combined molecular mismatch algorithm and assess the ability to predict the risk of CLAD development. Despite the limitation of a single-centre study, we studied a large cohort of LTR where the main clinical factors involved in CLAD, as humoral rejection and ACR [28], are confirmed in this study.
Although several variables classically associated with CLAD (such as CMV mismatch [29], donor age [30], or prolonged ischemic time [31] were not significant in our cohort, this may be related to sample size, centre-specific practices (ie. different CMV prophylaxis) [32], or collinearity with other included parameters.
On the contrary, recipient dyslipidemia or diabetic donor frequency was decreased in our cohort of CLAD. Although these findings may appear counterintuitive within this clinical context, we observed that patients who subsequently developed CLAD had a higher body weight at the time of inclusion on the transplant waiting list. Post-transplant weight gain has been previously associated with distinct CLAD phenotypes [33]. In this study, CLAD development was analyzed regardless of restrictive or bronchiolitis obliterans syndrome phenotypes.
In our cohort, we observe the impact of molecular mismatch in class-II as an independent factor for CLAD development adjusted by the smoking history of the patients, prolonged inpatient after transplantation, ACR, and ABMR. This observation points to a potential usefulness of immunological risk assessment for predicting chronic rejection at early stages. These findings suggest that incorporating molecular mismatch assessment, particularly in class II loci, could improve donor–recipient risk stratification and guide individualized post-transplant monitoring strategies. However, the model obtained in this study takes parameters along the lung transplantation, so the cumulative risk for the patient increases over time, remaining the presence of ABMR the most important factor in CLAD development. The fact that molecular mismatch in DR class-II predicts CLAD independently of ABMR could be explained in terms that the current criteria for ABMR diagnosis have low sensitivity. Thus, the disparity in class II could fill the gap in underdiagnosed ABMR. Future multicentre prospective studies integrating molecular mismatch algorithms with non-HLA antibody detection and dynamic clinical models will be essential to refine CLAD risk prediction.
4. Materials and Methods
4.1. Study Design
All consecutive lung transplant recipients were followed in the Pneumology Department at Marqués de Valdecilla Hospital since 2010. All the patients signed informed consent, and the study was approved by the Regional Committee with the Code number (2022.202). This retrospective observational study consisted of a total of 497 LTR with donor HLA typing studies. To assess the CLAD involvement and to avoid bias, we selected those LTR with a follow-up more than 180 days after lung transplantation. A total of 457 LTR were finally selected for the study.
4.2. Clinical Data
The clinical data were gathered by clinicians at the Pneumology Department prospectively. The details of clinical data are described in 4.5.1, including demographic data from both donor and recipients, transplant, and finally, the immunological parameters were collected by the histocompatibility laboratory staff.
Primary graft dysfunction (PGD) was defined and graded according to the criteria of the International Society for Heart and Lung Transplantation (ISHLT) [34]. Acute cellular rejection after transplantation was defined and graded according to the ISHLT Working Formulation [35]. CLAD diagnosis and phenotyping were performed using ISHLT criteria [36]. Finally, the ISHLT consensus was used for the diagnosis of antibody-mediated rejection [37].
4.3. HLA Typing
The HLA typing results from donors and recipients were available at the serological level or with a 2-digit resolution for Class-I (A, B, C loci) and Class-II (DRB1 and DQB1 loci). The HLA typing was performed using Luminex technology with sequence-specific oligonucleotide probes from both vendors (One Lambda, Inc, Canoga Park, CA, USA) and Werfen, LifeCodes). The National Marrow Donor Program (NMDP) haplotype reference database (https://haplostats.org/haplostats) was used to infer a second field (4-digit) resolution HLA typing. The most likely high-resolution HLA genotypes are listed among ambiguous typing results according to the highest haplotype frequency in Caucasians.
4.4. Molecular Mismatch Algorithms
4.4.1. Eplet Mismatch
The eplet mismatch scores were calculated from second field resolution HLA typing. The HLA-Matchmaker tool (HLA-ABCEpletMatching v4.0 and DRDQDPEpletMatching Program v3.1 from (http://www.epitopes.net/downloads.html) was used; the number of antibody-verified (AbV) eplets was considered for HLA eplet mismatch scores.
4.4.2. HLA-EMMA Mismatch
The solvent amino acid (SAA) mismatch between donor and recipient was assessed by HLA-EMMA software (https://hla-emma.com) [38]. The SAA mismatch in each locus was gathered from the software report.
4.4.3. PIRCHE-II Scores
The PIRCHE-II algorithm predicts mismatched HLA-derived peptides that can be presented by class-II molecules from recipients, which is related to the indirect CD4+ T cell alloreactivity. We record both the total HLA-locus specific mismatched peptides (sum of HLA-A, -B, -C, DRB1, -DQB1 derived peptide count) and the locus-specific mismatched peptides (HLA-A, -B, -C, -DR and –DQ) presented by recipient HLA-DRB1 molecules (https://www.pirche.com).
4.5. Statistical Analysis
4.5.1. List of Variables and Description, and Calculation
Recipient parameters:
1. Recipient´s sex: dichotomous variable (male or female)
2. Recipient´s age: numeric variable (years)
3. Recipient smoker (history of smoking at inclusion): dichotomous variable (never or Yes)
4. Tobacco consumption: numeric variable (cigarette packs/year)
5. Hypertension: dichotomous variable (yes or no)
6. Diabetes: dichotomous (yes or no)
7. Dyslipidaemia: dichotomous (yes or no)
8. Recipient´s size: numeric variable (meters)
9. Recipient´s weight: numeric variable (kilograms)
10. Recipient´s body mass index (BMI): numeric variable (kg/m2)
11. Lung allocation score: numeric variable
Donor parameters:
12. Donor´s sex dichotomous variable (male or female)
13. Donor´s age: numeric variable (years)
14. Donor smoker: dichotomous variable (yes or no)
15. Hypertension: dichotomous variable (yes or no)
16. Diabetes: dichotomous (yes or no)
17. Donor´s size: numeric variable (meters)
18. Donor´s weight: numeric variable (kilograms)
Immunological parameters:
19. Anti-HLA class-I antibodies pre-transplant: dichotomous (yes or no)
20. Anti-HLA class-II antibodies pre-transplant: dichotomous (yes or no)
21. Anti-MICA antibodies pre-transplant: dichotomous (yes or no)
22. Antibody verified eplet mismatch All: numeric variable (eplet mismatched)
23. Antibody verified eplet mismatch ABC: numeric variable (eplet mismatched)
24. Antibody verified eplet mismatch DQDR: numeric variable (eplet mismatched)
25. Antibody verified eplet mismatch DQA1DQB1: numeric variable (eplet mismatched)
26. Antibody verified eplet mismatch DRB1345: numeric variable (eplet mismatched)
27. PIRCHE II score: numeric variable (no unit)
28. PIRCHE II HLA-A: numeric variable (no unit)
29. PIRCHE II HLA-B: numeric variable (no unit)
30. PIRCHE II HLA-C: numeric variable (no unit)
31. PIRCHE II HLA-DQA1: numeric variable (no unit)
32. PIRCHE II HLA-DQB1: numeric variable (no unit)
33. PIRCHE II HLA-DRB1: numeric variable (no unit)
34. EMMA score All: numeric variable (solvent amino acids mismatched)
35. EMMA score HLA-ABC: numeric variable (solvent amino acids mismatched)
36. EMMA score HLA-A: numeric variable (solvent amino acids mismatched)
37. EMMA score HLA-B: numeric variable (solvent amino acids mismatched)
38. EMMA score HLA-C: numeric variable (solvent amino acids mismatched)
39. EMMA score HLA-DQABDR: numeric variable (solvent amino acids mismatched)
40. EMMA score HLA-DQA1: numeric variable (solvent amino acids mismatched)
41. EMMA score HLA-DQB1: numeric variable (solvent amino acids mismatched)
42. EMMA score HLA-DR: numeric variable (solvent amino acids mismatched)
Lung transplant parameters
43. Donation type was categorized as DBD vs non-heart-beating donors)
44. Type of transplant: dichotomous variable (Unipulmonar or Bipulmonar)
45. Indication: dichotomous variable (Elective or Urgent)
46. CMV pairing: dichotomous variable (high risk or another pairing)
47. Donor pO2: numeric variable (mmHg)
48. ECMO during surgery: dichotomous variable (yes or no)
49. Ischemic time first: numeric variable (minutes)
50. Ischemic time second: numeric variable (minutes)
51. Surgery time: numeric variable (minutes)
52. Transfusions: dichotomous variable (yes or no)
53. Number of packet RBC: numeric variable (units)
54. Surgical reintervention: dichotomous variable (yes or no)
Clinical parameters
55. Induction: dichotomous variable (yes or no)
56. Calcineurin inhibitor: dichotomous variable (tacrolimus vs cyclosporine)
57. Anti-metabolite: dichotomous variable (MMF vs Aza)
58. Tracheostomy: dichotomous variable (yes or no)
59. Hospitalization: numeric variable (days)
60. Intubation: numeric variable (days)
61. Primary graft dysfunction: dichotomous variable (yes or no)
62. Primary graft dysfunction grade 3: dichotomous variable (yes or no)
63. Acute cellular rejection: dichotomous variable (yes or no)
64. Antibody-mediated rejection: dichotomous variable (yes or no)
65. Chronic allograft dysfunction: dichotomous variable (yes or no)
4.5.2. Calculation of New Immunological Parameters
To focus on the importance of high immunological risk in the CLAD development, we calculated new immunological variables using the 75th percentile (p75) as cut-off for each molecular mismatch algorithm to convert to a dichotomous variable. Furthermore, to perform combinations of molecular mismatch algorithms, firstly, the combination of 2 molecular mismatch algorithms (HLA-EMMA and HLA-Matchmaker) was performed, when the 2 parameters were over p75 in both algorithms, immunological high risk was assigned, and the other combinations were defined as low risk. Further combination with PIRCHE molecular mismatch was performed using the same approach.
4.5.3. Survival Analysis
Time to CLAD development was calculated from the transplant date in all LTR. In order to perform survival analysis, all numeric variables were binned into dichotomous using the 75th percentile as a cut-off to perform Kaplan Meier analysis, the log rank test p-value, area under the curve, sensitivity, and specificity for each parameter were calculated (Supp Table 2).
4.5.4. Cox Regression Approach
Survival analysis was performed using a Cox proportional hazards regression model to identify risk factors associated with the development of CLAD after lung transplantation. Variables included in the modelling process were selected based on clinical relevance and statistical significance (p < 0.05) in the univariate analyses (Suppl Table 3).
Variable selection for the multivariable Cox model followed a two-step strategy. First, the Least Absolute Shrinkage and Selection Operator (LASSO) penalization technique was applied using 10-fold cross-validation to identify a parsimonious set of predictive covariates and prevent model overfitting. Second, stepwise selection based on the Akaike Information Criterion (stepwise AIC, bi-directional) was conducted among variables shortlisted by LASSO to further optimize model fit and interpretability.
The final model was fit by maximizing the partial likelihood, and the proportional hazards assumption was rigorously assessed with Schoenfeld residual-based testing. Model outputs are expressed as hazard ratios (HRs) with their 95% confidence intervals (Table 3). Model performance was evaluated by measuring concordance, Wald statistics, and likelihood ratio tests.
The model was calculated with data from 215 patients. In order to increase the robustness of the prediction model, all the LTR data were assessed. The final multivariate Cox regression model was calculated with the variables selected by LASSO and using the method of inferring missing data in 6 LTR. In detail, multiple imputation was performed using the predictive mean matching method with five imputations (m=5) and a fixed random seed to ensure reproducibility. One imputed dataset was extracted and used for subsequent analysis.
The adjusted survival functions were estimated for different combinations of risk factors, enabling the visualization of CLAD-free survival probability as a function of key clinical profiles throughout the peri-transplant period.
4.5.5. Packages Used
R version 4.5.1,.
Packages:
library(survival 3.8-3), library(MASS v7.3-65), library (survminer v0.5.0), library (ggplot2 v3.5.2), library (dplyr v1.1.4), library (tidyr v1.3.1), library (writexl v1.5.4), library (gt v1.0.0), library (pROC v1.18.5), library (mice v.3.18.0).
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Comparison of Parameters included in the study: Recipients, donors, lung transplants, clinical and immunological parameters in Lung transplant recipients based on CLAD development; Table S2: Data of Area Under de Curve (AUC), sensitivity and specificity, and Kaplan Meier p-value of the parameters included in the study: Recipients, donors, lung transplants, clinical and immunological parameters; Table S3: Univariate Cox-regression model with the parameters included in the study: Recipients, donors, lung transplants, clinical and immunological parameters.
Author Contributions
Conceptualization, D.S.S. and V.M.M.C.; methodology, D.S.S., A.C.B.; software, D.S.S. and A.C.B.; formal analysis, D.S.S, V.M.M.C. and P.M.C.; investigation, D.S.S, A.C.B. and V.M.M.C.; resources, J.M.C., D.I.F., G.O.V., J.I.V., S.T.M., S.I.C.; data curation, D.S.S., P.M.C.; writing—original draft preparation, D.S.S.; writing—review and editing, A.C.B, V.M.M.C., P.M.C., and M.L.H; visualization, D.S.S. and A.C.B.; funding acquisition, J.M.C. and M.L.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by RICORS2040 (ISCIII RD21/0005/0010 and RD24/0004/0019, “Financiado por la Unión Europea—NextGeneration EU,” Mecanismo para la Recuperación y la Resiliencia [MRR]).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Cantabria Ethics and Research Committee (CEIm) under study code 2022.202.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data generated or analyzed in this study are included in this article. Further enquiries can be directed to the corresponding author.
Acknowledgments
The authors want to acknowledge Cinta Altadill and Miguel Mainer from the Werfen company for accessibility to PIRCHE platform.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Copeland, C.A.F.; Snyder, L.D.; Zaas, D.W.; Jackson Turbyfill, W.; Davis, W.A.; Palmer, S.M. Survival after Bronchiolitis Obliterans Syndrome among Bilateral Lung Transplant Recipients. Am J Respir Crit Care Med 2010, 182, 784–789. [CrossRef]
- Beeckmans, H.; Kerckhof, P.; Acet Öztürk, N.; Zajacova, A.; Van Slambrouck, J.; Bos, S.; Vermant, M.; Van Dieren, L.O.; Goeminne, T.; Vandervelde, C.; et al. Clinical Predictors for Restrictive Allograft Syndrome: A Nested Case-Control Study. American Journal of Transplantation 2025, 25, 1319–1338. [CrossRef]
- Roux, A.; Levine, D.J.; Zeevi, A.; Hachem, R.; Halloran, K.; Halloran, P.F.; Gibault, L.; Taupin, J.L.; Neil, D.A.H.; Loupy, A.; et al. Banff Lung Report: Current Knowledge and Future Research Perspectives for Diagnosis and Treatment of Pulmonary Antibody-Mediated Rejection (AMR). American Journal of Transplantation 2019, 19, 21–31. [CrossRef]
- Miyamoto, E.; Vosoughi, D.; Wang, J.; Al-Refaee, J.; Berra, G.; Daigneault, T.; Duong, A.; Joe, B.; Moshkelgosha, S.; Keshavjee, S.; et al. Local Intragraft Humoral Immune Responses in Chronic Lung Allograft Dysfunction. Journal of Heart and Lung Transplantation 2025, 44, 105–117. [CrossRef]
- Opelz, G. Strength of HLA-A, HLA-B, and HLA-DR Mismatches in Relation to Short- and Long-Term Kidney Graft Survival. Collaborative Transplant Study. Transpl Int 1992, 5 Suppl 1, 621–624. [CrossRef]
- Afzal Nikaein, L.B.L.J.M.F.L.R.G.T.G.M.J.S.G.K. HLA Compatibility and Liver Transplant Outcome: Improved Patient Survival by HLA and Cross-Matching. Transplantation 1994, 58, 786–792.
- Opelz, G.; Wujciak, T. The Influence of HLA Compatibility on Graft Survival after Heart Transplantation. The Collaborative Transplant Study. N Engl J Med 1994, 330, 816–819. [CrossRef]
- Opelz, G.; Süsal, C.; Ruhenstroth, A.; Döhler, B. Impact of HLA Compatibility on Lung Transplant Survival and Evidence for an HLA Restriction Phenomenon: A Collaborative Transplant Study Report. Transplantation 2010, 90, 912–917. [CrossRef]
- Duquesnoy, R.J.; Askar, M. HLAMatchmaker: A Molecularly Based Algorithm for Histocompatibility Determination. V. Eplet Matching for HLA-DR, HLA-DQ, and HLA-DP. Hum Immunol 2007, 68, 12–25. [CrossRef]
- Lachmann, N.; Niemann, M.; Reinke, P.; Budde, K.; Schmidt, D.; Halleck, F.; Pruß, A.; Schönemann, C.; Spierings, E.; Staeck, O. Donor–Recipient Matching Based on Predicted Indirectly Recognizable HLA Epitopes Independently Predicts the Incidence of De Novo Donor-Specific HLA Antibodies Following Renal Transplantation. American Journal of Transplantation 2017, 17, 3076–3086. [CrossRef]
- Ono, K.; Ide, K.; Tanaka, Y.; Ohira, M.; Tahara, H.; Tanimine, N.; Yamane, H.; Ohdan, H. Molecular Mismatch Predicts T Cell-Mediated Rejection and De Novo Donor-Specific Antibody Formation After Living Donor Liver Transplantation. Liver Transpl 2021, 27, 1592–1602. [CrossRef]
- Kleid, L.; Walter, J.; Vorstandlechner, M.; Schneider, C.P.; Michel, S.; Kneidinger, N.; Irlbeck, M.; Wichmann, C.; Möhnle, P.; Humpe, A.; et al. Predictive Value of Molecular Matching Tools for the Development of Donor Specific HLA-Antibodies in Patients Undergoing Lung Transplantation. HLA 2023, 102, 331–342. [CrossRef]
- Ellison, M.; Mangiola, M.; Marrari, M.; Bentlejewski, C.; Sadowski, J.; Zern, D.; Kramer, C.S.M.; Heidt, S.; Niemann, M.; Xu, Q.; et al. Immunologic Risk Stratification of Pediatric Heart Transplant Patients by Combining HLA-EMMA and PIRCHE-II. Front Immunol 2023, 14. [CrossRef]
- Lánczky, A.; Győrffy, B. Web-Based Survival Analysis Tool Tailored for Medical Research (KMplot): Development and Implementation. J Med Internet Res 2021, 23. [CrossRef]
- Flöthmann, K.; Davide de Manna, N.; Aburahma, K.; Kruszona, S.; Wand, P.; Bobylev, D.; Müller, C.; Carlens, J.; Schwerk, N.; Avsar, M.; et al. Impact of Donor Organ Quality on Recipient Outcomes in Lung Transplantation: 14-Year Single-Center Experience Using the Eurotransplant Lung Donor Score. JHLT Open 2024, 6, 100166. [CrossRef]
- Ghaidan, H.; Fakhro, M.; Lindstedt, S. Impact of Allograft Ischemic Time on Long-Term Survival in Lung Transplantation: A Swedish Monocentric Study. Scand Cardiovasc J 2020, 54, 322–329. [CrossRef]
- Hirschi, S.; Hell, G.; Levine, D.J.; Coiffard, B.; Severac, F.; Picard, C.; Bunel, V.; Le Pavec, J.; Essaidy, A.; Reynaud-Gaubert, M.; et al. Diagnostic Significance of Intragraft Donor–Specific Anti-HLA Antibodies in Pulmonary Antibody–Mediated Rejection. Journal of Heart and Lung Transplantation 2025. [CrossRef]
- Xu, Q.; Elrefaei, M.; Taupin, J.L.; Hitchman, K.M.K.; Hiho, S.; Gareau, A.J.; Iasella, C.J.; Marrari, M.; Belousova, N.; Bettinotti, M.; et al. Chronic Lung Allograft Dysfunction Is Associated with an Increased Number of Non-HLA Antibodies. Journal of Heart and Lung Transplantation 2024, 43, 663–672. [CrossRef]
- Comins-Boo, A.; Mora-Fernández, V.M.; Padrón-Aunceame, P.; Toriello-Suárez, M.; González-López, E.; Roa-Bautista, A.; Castro-Hernández, C.; Iturbe-Fernández, D.; Cifrián José, M.; López-Hoyos, M.; et al. Non-HLA Antibodies and the Risk of Antibody-Mediated Rejection without Donor-Specific Anti-HLA Antibodies After Lung Transplantation. Transplant Proc 2025, 57, 73–76. [CrossRef]
- Opelz, G.; Wujciak, T.; Döhler, B.; Scherer, S.; Mytilineos, J. HLA Compatibility and Organ Transplant Survival. Collaborative Transplant Study. Rev Immunogenet 1999.
- Yacoub, R.; Nadkarni, G.N.; Cravedi, P.; He, J.C.; Delaney, V.B.; Kent, R.; Chauhan, K.N.; Coca, S.G.; Florman, S.S.; Heeger, P.S.; et al. Analysis of OPTN/UNOS Registry Suggests the Number of HLA Matches and Not Mismatches Is a Stronger Independent Predictor of Kidney Transplant Survival. Kidney Int 2018, 93, 482–490. [CrossRef]
- Yamada, Y.; Langner, T.; Inci, I.; Benden, C.; Schuurmans, M.; Weder, W.; Jungraithmayr, W. Impact of Human Leukocyte Antigen Mismatch on Lung Transplant Outcome. Interact Cardiovasc Thorac Surg 2018, 26, 859–864. [CrossRef]
- Wiebe, C.; Rush, D.N.; Nevins, T.E.; Birk, P.E.; Blydt-Hansen, T.; Gibson, I.W.; Goldberg, A.; Ho, J.; Karpinski, M.; Pochinco, D.; et al. Class II Eplet Mismatch Modulates Tacrolimus Trough Levels Required to Prevent Donor-Specific Antibody Development. J Am Soc Nephrol 2017, 28, 3353–3362. [CrossRef]
- Lee, H.; Min, J.W.; Kang, H.; Lee, H.; Eum, S.H.; Park, Y.; Yang, C.W.; Chung, B.H.; Oh, E.J. Combined Analysis of HLA Class II Eplet Mismatch and Tacrolimus Levels for the Prediction of De Novo Donor Specific Antibody Development in Kidney Transplant Recipients. Int J Mol Sci 2022, 23, 7357. [CrossRef]
- Kleid, L.; Walter, J.; Vorstandlechner, M.; Schneider, C.P.; Michel, S.; Kneidinger, N.; Irlbeck, M.; Wichmann, C.; Möhnle, P.; Humpe, A.; et al. Predictive Value of Molecular Matching Tools for the Development of Donor Specific HLA-Antibodies in Patients Undergoing Lung Transplantation. HLA 2023, 102, 331–342. [CrossRef]
- McCaughan, J.A.; Battle, R.K.; Singh, S.K.S.; Tikkanen, J.M.; Moayedi, Y.; Ross, H.J.; Singer, L.G.; Keshavjee, S.; Tinckam, K.J. Identification of Risk Epitope Mismatches Associated with de Novo Donor-Specific HLA Antibody Development in Cardiothoracic Transplantation. American Journal of Transplantation 2018, 18, 2924–2933. [CrossRef]
- Demir, Z.; Raynaud, M.; Divard, G.; Louis, K.; Truchot, A.; Niemann, M.; Ponsirenas, R.; Aubert, O.; Del Bello, A.; Hertig, A.; et al. Impact of HLA Evolutionary Divergence and Donor-Recipient Molecular Mismatches on Antibody-Mediated Rejection of Kidney Allografts. Nat Commun 2025, 16. [CrossRef]
- Parulekar, A.D.; Kao, C.C. Detection, Classification, and Management of Rejection after Lung Transplantation. J Thorac Dis 2019, 11, S1732–S1739. [CrossRef]
- Kawashima, M.; Ma, J.; Huszti, E.; Levy, L.; Berra, G.; Renaud-Picard, B.; Takahagi, A.; Ghany, R.; Sato, M.; Keshavjee, S.; et al. Association between Cytomegalovirus Viremia and Long-Term Outcomes in Lung Transplant Recipients. American Journal of Transplantation 2024, 24, 1057–1069. [CrossRef]
- Franz, M.; Aburahma, K.; Avsar, M.; Boethig, D.; Greer, M.; Alhadidi, H.; Sommer, W.; Tudorache, I.; Warnecke, G.; Haverich, A.; et al. Does Donor-Recipient Age Mismatch Have an Influence on Outcome after Lung Transplantation? A Single-Centre Experience. Eur J Cardiothorac Surg 2023, 63. [CrossRef]
- Pasupneti, S.; Nicolls, M.R. Airway Hypoxia in Lung Transplantation. Curr Opin Physiol 2019, 7, 21–26. [CrossRef]
- Banga, N.; Kanade, R.; Kappalayil, A.; Timofte, I.; Lawrence, A.; Bollineni, S.; Kaza, V.; Torres, F. Long-Term Outcomes Among Lung Transplant Recipients With High-Risk Cytomegalovirus Mismatch Managed With a Multimodality Regimen. Clin Transplant 2025, 39. [CrossRef]
- Beauchamp-Parent, C.; Jomphe, V.; Morisset, J.; Poirier, C.; Lands, L.C.; Nasir, B.S.; Ferraro, P.; Mailhot, G. Impact of Transplant Body Mass Index and Post-Transplant Weight Changes on the Development of Chronic Lung Allograft Dysfunction Phenotypes. Transplant Proc 2024, 56, 1420–1428. [CrossRef]
- Valentini, C.G.; Farina, F.; Pagano, L.; Teofili, L. Granulocyte Transfusions: A Critical Reappraisal. Biology of Blood and Marrow Transplantation 2017, 23, 2034–2041. [CrossRef]
- Stewart, S.; Fishbein, M.C.; Snell, G.I.; Berry, G.J.; Boehler, A.; Burke, M.M.; Glanville, A.; Gould, F.K.; Magro, C.; Marboe, C.C.; et al. Revision of the 1996 Working Formulation for the Standardization of Nomenclature in the Diagnosis of Lung Rejection. Journal of Heart and Lung Transplantation 2007, 26, 1229–1242. [CrossRef]
- Verleden, G.M.; Glanville, A.R.; Lease, E.D.; Fisher, A.J.; Calabrese, F.; Corris, P.A.; Ensor, C.R.; Gottlieb, J.; Hachem, R.R.; Lama, V.; et al. Chronic Lung Allograft Dysfunction: Definition, Diagnostic Criteria, and Approaches to Treatment―A Consensus Report from the Pulmonary Council of the ISHLT. Journal of Heart and Lung Transplantation 2019, 38, 493–503. [CrossRef]
- Levine, D.J.; Glanville, A.R.; Aboyoun, C.; Belperio, J.; Benden, C.; Berry, G.J.; Hachem, R.; Hayes, D.; Neil, D.; Reinsmoen, N.L.; et al. Antibody-Mediated Rejection of the Lung: A Consensus Report of the International Society for Heart and Lung Transplantation. Journal of Heart and Lung Transplantation 2016, 35, 397–406. [CrossRef]
- Kramer, C.S.M.; Koster, J.; Haasnoot, G.W.; Roelen, D.L.; Claas, F.H.J.; Heidt, S. HLA-EMMA: A User-Friendly Tool to Analyse HLA Class I and Class II Compatibility on the Amino Acid Level. HLA 2020, 96, 43–51. [CrossRef]
Figure 1.
Forest plot of parameters associated with CLAD development: final multivariate Cox analysis. Multivariable Cox result. The parameters included in the final multivariate model were selected using Lasso penalization and stepwise based on Akaike Information Criteria. The forest plot depicts hazard ratios (black squares) and 95% CI (horizontal black lines). The exact p-values are shown. (Total number of Lung transplant recipients 457, 160 with CLAD development).
Figure 1.
Forest plot of parameters associated with CLAD development: final multivariate Cox analysis. Multivariable Cox result. The parameters included in the final multivariate model were selected using Lasso penalization and stepwise based on Akaike Information Criteria. The forest plot depicts hazard ratios (black squares) and 95% CI (horizontal black lines). The exact p-values are shown. (Total number of Lung transplant recipients 457, 160 with CLAD development).
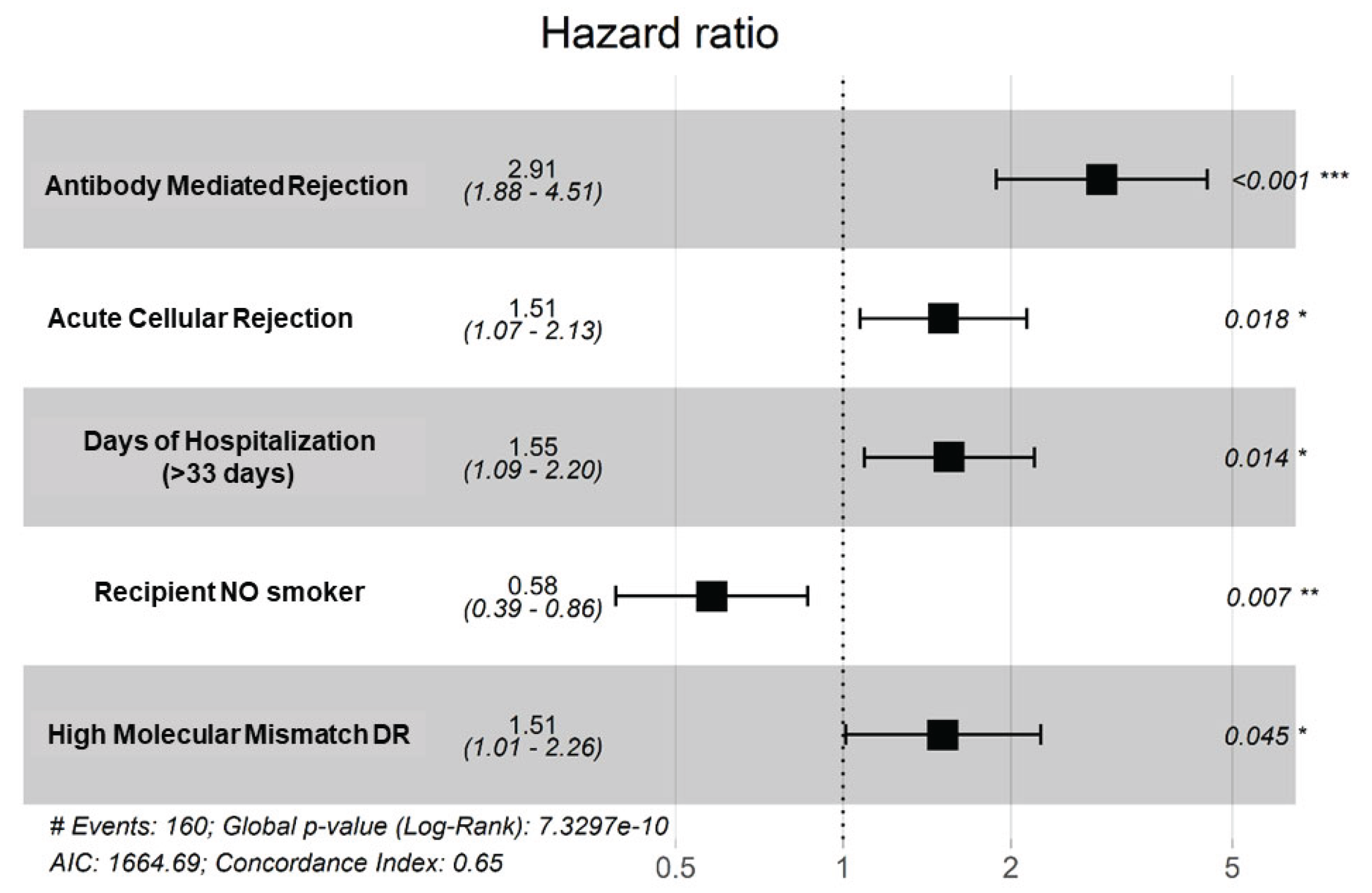
Figure 2.
Survival free of CLAD probability. Using the CLAD prediction model with the data of 457 lung transplant recipients, the mean CLAD-free survival decrease when adding each risk factor from inclusion in waiting list to ABMR diagnosis. Hosp (>33 days of hospitalization after lung transplantation), MMDR (class-II mismatch molecular in DR), ACR (acute cellular rejection), ABMR (antibody mediated rejection). .
Figure 2.
Survival free of CLAD probability. Using the CLAD prediction model with the data of 457 lung transplant recipients, the mean CLAD-free survival decrease when adding each risk factor from inclusion in waiting list to ABMR diagnosis. Hosp (>33 days of hospitalization after lung transplantation), MMDR (class-II mismatch molecular in DR), ACR (acute cellular rejection), ABMR (antibody mediated rejection). .
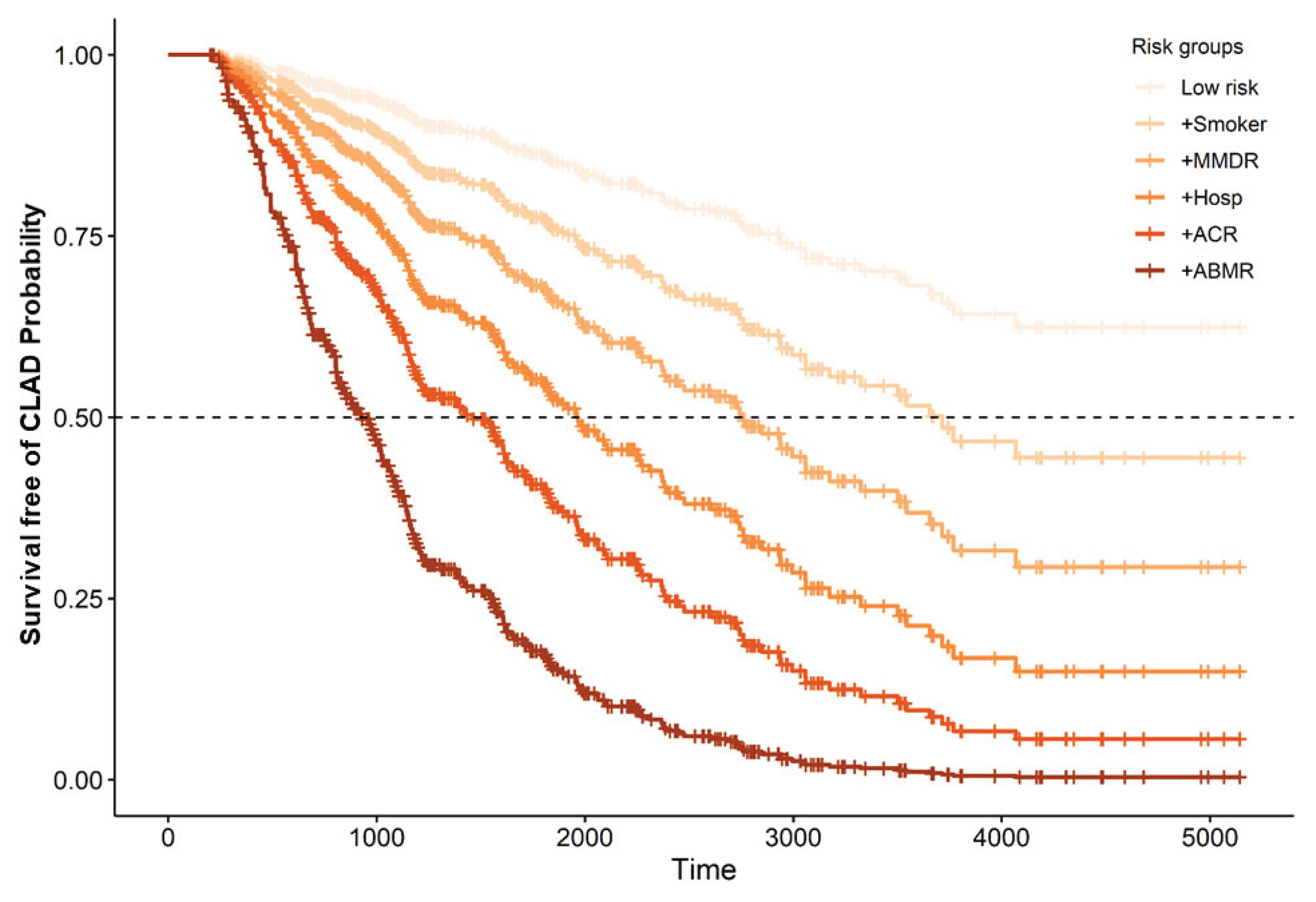
Table 1.
Description of the parameter included in the study: Recipients, donors, lung transplants, clinical and immunological parameters.
Table 1.
Description of the parameter included in the study: Recipients, donors, lung transplants, clinical and immunological parameters.
| Parameter | Total | Frequency (%) | Mean (SD) | Median (IQR) | |
|---|---|---|---|---|---|
| Recipient | Recipient sex (% female) | 457 | 180 (39.39) | ||
| Recipient age (years) | 457 | 56.8 (9.9) | 60.0 (53.9-63.5) | ||
| Recipient smoker (never) | 454 | 105 (23.13) | |||
| Tobacco consumption (cigarettes/day) |
341 | 37.2 (22.1) | 35 (20-50) | ||
| Hypertension (yes) | 455 | 91 (20.00) | |||
| Diabetes (yes) | 455 | 41 (9.01) | |||
| Dyslipidemia (yes) | 453 | 147 (32.45) | |||
| Size (meters) | 396 | 1.65 (0.09) | 1.66 (1.59-1.72) | ||
| Weight (kilograms) | 397 | 68.0 (12.7) | 68 (59-77) | ||
| BMI (kg/m2) | 396 | 24.76 (3.55) | 25.0 (22.2-27.7) | ||
| LAS score | 347 | 34.4 (3.56) | 33.3 (32.1-35.5) | ||
| Donor | Donor sex (% female) | 457 | 236 (51.64) | ||
| Donor age (years) | 457 | 52.3 (14.2) | 55 (44-63) | ||
| Donor smoker (yes) | 439 | 152 (34.62) | |||
| Hypertension (yes) | 436 | 144 (33.03) | |||
| Diabetes (yes) | 415 | 34 (8.19) | |||
| Donor size (meters) | 452 | 1.67 (1.16) | 1.69 (1.62-1.75) | ||
| Donor weight (kilograms) | 452 | 73.26 (13.33) | 75 (65-80) | ||
| Immunological | Anti-HLA class-I antibodies pre transplant (yes) | 349 | 27 (7.74) | ||
| Anti-HLA class-II antibodies pre transplant (yes) | 349 | 17 (4.87) | |||
| Anti-MICA antibodies pre transplant (yes) | 457 | 4 (0.88) | |||
| Antibody verified eplet mismatch All | 457 | 16.91 (6.33) | 16 (13-21) | ||
| Antibody verified eplet mismatch ABC | 457 | 8.70 (3.65) | 8 (6-11) | ||
| Antibody verified eplet mismatch DQDR | 457 | 8.21 (4.74) | 8 (5-11) | ||
| Antibody verified eplet mismatch DQA1DQB1 | 457 | 6.08 (3.98) | 5 (3-9) | ||
| Antibody verified eplet mismatch DRB1345 | 457 | 2.13 (1.86) | 2 (1-3) | ||
| PIRCHE II score | 457 | 274.2 (111.9) | 270 (195-343) | ||
| PIRCHE II HLA-A | 457 | 54.9 (38.9) | 49 (27-76) | ||
| PIRCHE II HLA-B | 457 | 46.8 (28.0) | 43 (26-64) | ||
| PIRCHE II HLA-C | 457 | 47.6 (33.8) | 41 (23-67) | ||
| PIRCHE II HLA-DQA1 | 457 | 47.3 (40.2) | 45 (0-74) | ||
| PIRCHE II HLA-DQB1 | 457 | 48.9 (32.9) | 46 (25-68) | ||
| PIRCHE II HLA-DRB1 | 457 | 33.1 (19.8) | 31 (19-44) | ||
| EMMA score HLA-All | 457 | 57.4 (22.1) | 55 (41-73) | ||
| EMMA score HLA-ABC | 457 | 27.9 (10.5) | 27 (21-34) | ||
| EMMA score HLA-A | 457 | 12.8 (7.2) | 12 (8-17) | ||
| EMMA score HLA-B | 457 | 8.27 (4.64) | 8 (5-11) | ||
| EMMA score HLA-C | 457 | 6.88 (4.14) | 7 (4-10) | ||
| EMMA score HLA-DQABDR | 457 | 29.4 (19.0) | 26 (14-43) | ||
| EMMA score HLA-DQA1 | 457 | 9.81 (8.58) | 8 (0-18) | ||
| EMMA score HLA-DQB1 | 457 | 11.2 (8.52) | 9 (4-18) | ||
| EMMA score HLA-DR | 457 | 8.43 (5.58) | 8 (4-12) | ||
| Lung transplant | Donation (DBD) | 457 | 350 (76.6) | ||
| Type of transplant (Unipulmonar) | 457 | 93 (20.4) | |||
| Indication (Elective) | 457 | 444 (97.2) | |||
| CMV pairing (High risk) | 435 | 57 (13.1) | |||
| Donor pO2 (mmHg) | 438 | 382.8 (153.1) | 422 (350-484) | ||
| ECMO during surgery (yes) | 454 | 49 (10.8) | |||
| Ischemic time first (minutes) | 455 | 298.9 (130.6) | 275 (235-323) | ||
| Ischemic time second (minutes) | 363 | 419 (155.3) | 388 (335-450) | ||
| Surgery time (minutes) | 346 | 291.6 (76.1) | 290 (240-330.8) | ||
| Transfusion (yes) | 349 | 112 (32.1) | |||
| Number of packet RBC (units) | 112 | 2.72 (2.44) | 2 (1-4) | ||
| Surgical reintervention (yes) | 456 | 34 (7.46) | |||
| Clinical | Induction (yes) | 373 | 318 (76.6) | ||
| Calcineurin inhibitor (tacrolimus) | 349 | 334 (95.7) | |||
| Antimetabolite (mycophenolate) | 349 | 348 (99.7) | |||
| Tracheostomy (yes) | 349 | 17 (4.87) | |||
| Hospitalization (days) | 453 | 31.2 (20.0) | 25 (21-33) | ||
| Intubation (days) | 339 | 2.28 (3.1) | 1 (1-2) | ||
| Primary graft dysfunction (yes) | 457 | 125 (27.4) | |||
| Primary graft dysfunction grade 3 (yes) | 259 | 37 (14.3) | |||
| Acute cellular rejection (yes) | 457 | 229 (50.1) | |||
| Antibody mediated rejection (yes) | 457 | 38 (8.32) | |||
| Chronic allograft dysfunction (yes) | 457 | 160 (35.0) |
* BMI: body mass index; IQR interquartile range; DBD: Donation after Brain Death; RBC: red blood cells; SD: standard deviation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



