
Submitted:
01 November 2025
Posted:
04 November 2025
You are already at the latest version
Abstract
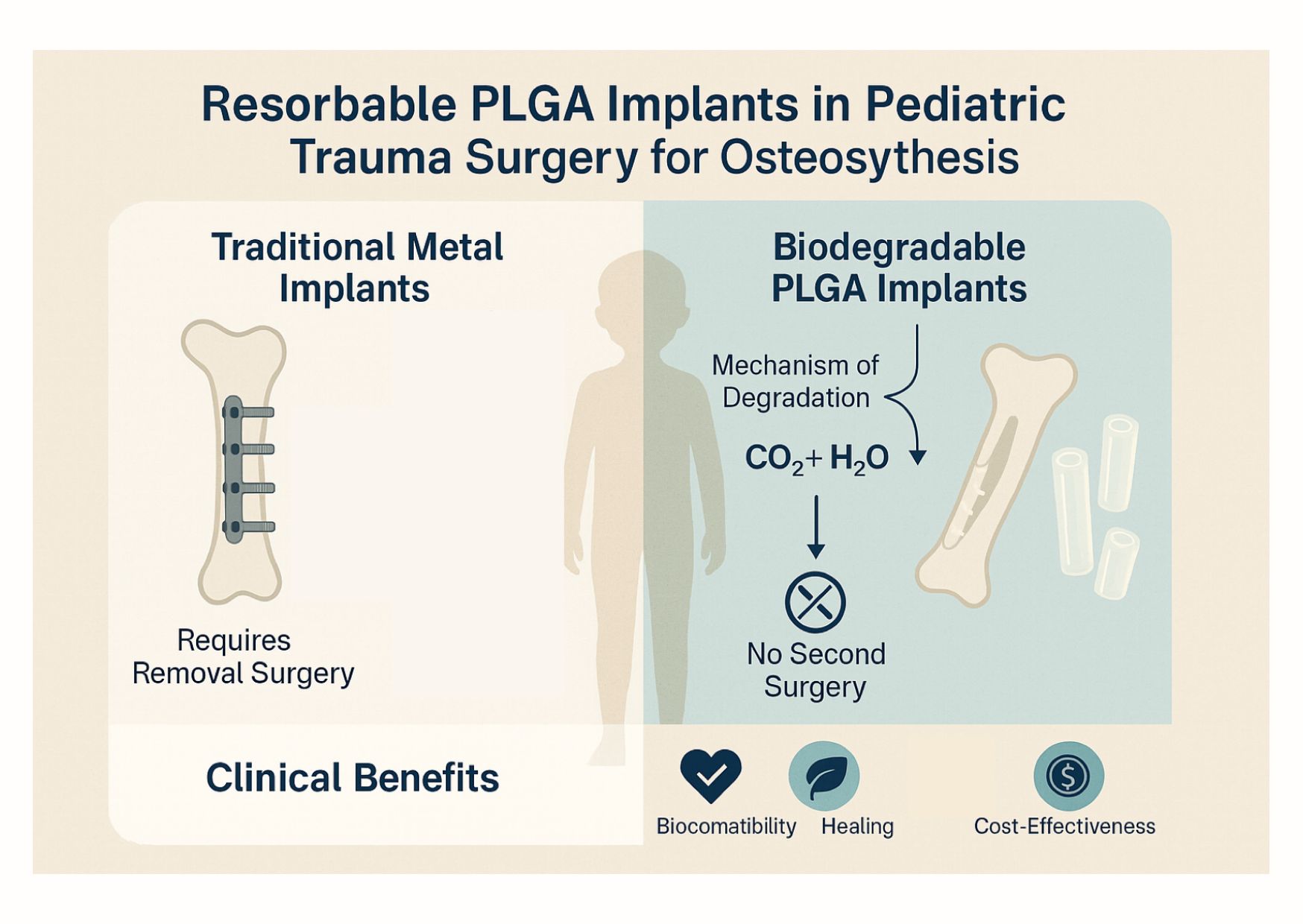
A promising alternative to traditional metal hardware in pediatric surgical care has been on the rise. Avoiding the need for hardware removal is particularly beneficial in children, who would otherwise face a second surgery with attendant risks. This brief review discusses the use of biodegradable implants, with a focus on poly(lactic-co-glycolic acid) (PLGA) devices, for fracture fixation in the growing skeleton, as well as outlines the challenges of managing pediatric fractures with traditional fixation and how bioabsorbable implants address some of these issues. The mechanism of PLGA implant degradation is summarised, highlighting how controlled hydrolysis allows implants to provide support during healing and then safely resorb. Clinical applications are reviewed through recent studies and case examples, including forearm, distal radius, ankle, and elbow fractures, which demonstrate effective healing and outcomes comparable to metal hardware. The benefits and limitations of presently used resorbable instruments are also discussed, together with future directions in research and material innovation, including newer biodegradable polymers and alloys.
Keywords:
PLGA
; fracture
; osteosynthesis
; biodegradable
; absorbable
; poly-l-lactic-co-glycolic-acid
1. Introduction
Pediatric fractures are common injuries, yet managing them poses unique challenges due to the growing skeleton [1,2]. While many simple childhood fractures heal with casting alone, more complex fracture patterns will commonly require internal fixation [2]. Traditional implants made of stainless steel or titanium reliably stabilise fractures [3]. Still, in children, these permanent implants are to be removed after healing to prevent interference with bone maturation and to avoid long-term complications. The mandated double operation carries risks of infection, complications of anaesthesia, and damage to tissues. It also adds psychological and economic burdens by exposing children and families to additional hospital visits and procedures [4]. Among other concerns, mainly these drove the interest in biodegradable implants, which can fix and hold fractures during healing and safely dissolve, obviating the need for removal [5,6]. Over the past few decades, advances in materials science have yielded bioresorbable polymers and alloys suitable for orthopaedic use in both children and adults [7,8,9]. In this review, we focus on the clinical applications of biodegradable implants – particularly PLGA-based devices – in pediatric trauma, and we discuss their benefits, limitations, and prospects in improving fracture management for young patients. Children’s bones differ from adults’ in structure and healing capacity. Pediatric long bones have growth plates (physes) and a thick periosteum, allowing many fractures to remodel with time [10,11]. However, particular injuries – open fractures, multi-fragmentary breaks, accompanying soft tissue damage, or fractures affecting the articular surfaces – require surgical stabilisation to ensure accurate alignment and function [12,13,14]. Traditional metal implants are associated with reliable and durable support over the healing period and a limited presence of foreign body reactions. Generally, Kirschner wires (K-wires), flexible intramedullary (IM) rods, and mini-plates are used. Despite their effectiveness, metal implants are designed to be temporary; removal is necessary to mitigate risks associated with growth disturbance or implant migration. Hardware traversing through or near a growth plate can cause growth arrest. Protruding or retained implants may irritate surrounding soft tissues, cause foreign body reactions, or lead to stress shielding and refractures. Moreover, the presence of a stiff metal implant can potentially alter bone remodelling during growth. As mentioned, a removal procedure entails a repeat anaesthesia and surgical dissection, which carries a risk of infection, nerve injury, and scarring. Particularly in small children, anaesthesia exposure itself is not without concern. From a health system perspective, scheduled implant removals increase the overall cost and workload in trauma care. Consequently, there has been a long-standing motivation to develop fixation methods that render hardware removal obsolete while still ensuring a reliable fixation.
Polylactic acid (PLA), polyglycolic acid (PGA) and their synthetic copolymers are the most widely adopted bioresorbable appliances [7,15]. Poly(lactic-co-glycolic acid) (PLGA), a copolymer of lactic and glycolic acids, is a second-generation bioresorbable material with enhanced mechanical properties and highly predictable degradation kinetics [7]. These polymer-based implants break down over time through hydrolysis and secondary enzymatic reactions, breaking ester bonds [16]. In a moist environment, water infiltrates the implant, triggering chemical degradation [17]. Ultimately, the polymer is metabolised via the citric acid cycle into carbon dioxide and water [17]. These innocuous end-products exit the body through normal respiratory and renal pathways; however, this hydrolysis may cause a localised drop in pH as acidic byproducts are released [17]. Modern implant designs and polymers aim to minimise any inflammatory response from this process. The feature that makes PLGA implants so desirable in a clinical setting is their tunable resorption rate. By altering the molecular composition of PLGA, the degradation rate can be tailored for optimal absorption [7,17]. In simple terms, the ratio of the two monomers determines how quickly the implant loses mass and mechanical strength over time. A higher glycolide content speeds up degradation, while a greater proportion of lactide, particularly the L-isomer, extends the implant’s lifespan [7,17]. By fine-tuning these ratios, manufacturers can ensure the implant maintains sufficient strength throughout the healing process. In practice, PLGA constructs with an 85L:15G composition are reported to be mostly absorbed in about 12–16 months, with substantial loss of mechanical strength occurring around the time the bone consolidation is expected [17,18,19]. This timeframe aligns well with the typical healing time for pediatric fractures, which is often a few months for most bones. By two years post-injury, many PLGA devices have largely dissolved, leaving behind only remodelled bone with no foreign material [20]. Mechanical performance of the implants could be a concern, since polymers are not as strong or stiff as metal. Even though it is a tough polymer, it possesses a lower bending modulus and tensile strength compared to stainless steel or titanium [21,22]. In practice, current resorbable implants such as PLGA pins and screws are made in sizes suitable for small bones and are intended for fractures where extreme forces are not expected before healing. Their ability to maintain fixation stability for the necessary duration has been supported by clinical studies, as discussed in the literature. During degradation, these implants typically lose strength gradually, which is ideal: the bone progressively takes on more load as it heals, while the implant material slowly vanishes. In essence, biodegradable implants aim to provide adequate strength and simultaneous remodelling within the bone during healing.
2. Clinical Applications and Case Examples:
- Forearm Fractures: One of the most common fracture sites in the pediatric population. Elastic stable intramedullary nailing (ESIN) with metal rods is a standard treatment for unstable diaphyseal forearm fractures. However, nowadays, instead of metal rods, bioabsorbable IM-nails made of PLGA are an alternative solution. In a 2024 cohort study of 38 children, all patients achieved bone union with stable alignment [23]. At one-year follow-up, the children showed nearly full recovery of their range of motion (ROM); minor reductions in forearm rotation and elbow flexion were not clinically significant. Complications such as refractures or irritation were not reported. The efficacy of the minimally invasive approach was reflected by excellent scar assessment scores. Another study, composed of 161 patients, emphasised the significance of surgical technique in order to evade complications [24]. In the literature, several other papers can be found that confirm that RIN is a safe and effective method for internal fixation of the forearm fractures, which produces results that are comparable to traditional metal implants [19,25,26,27].
- Distal Radius Fractures: Generally, injuries affecting the wrists are managed with percutaneous K-wire fixation. Modern alternatives include biodegradable pins and short IM-nails. In 2022, a multicenter retrospective study compared outcomes in children with severely displaced distal radius/forearm fractures treated with either standard K-wires or bioresorbable PLGA pins [28]. The findings were instructive: the group treated with biodegradable pins had significantly lower complication rates than those treated with buried or exposed K-wires. Specifically, the PLGA implants avoided typical K-wire problems such as pin track infections or irritation [28]. By six weeks to six months post-injury, all groups had similar alignment and functional outcomes, but the children with absorbable implants were spared the anxiety and discomfort of wire removal. After 1.5 years of follow-up, there were no growth disturbances observed in any patients, indicating that neither the biodegradable implants nor the K-wires affected the physes negatively [28]. [28]
- Ankle (Physeal) Fractures: Fractures of the distal tibia involving the growth plate (Salter-Harris fractures) are another scenario where implant choice is critical. Metal screws across a growth plate must be removed promptly to avoid growth arrest. In a retrospective study of 128 pediatric ankle fractures compared PLGA absorbable screws were compared to standard metallic screws for fixing physeal fractures (mainly Salter-Harris II, III, IV of the distal tibia) [29,30]. The study noted that the PLGA implants achieved comparable fracture stability and healing as metal screws, but without necessitating implant removal [30]. In the literature, similar results are reported through randomised controlled trials (RCTs) and systematic reviews [22,29,31,32,33]
- Elbow Fractures: Injuries of the lateral humeral condyles are the second most common elbow fractures in children, which often require operative solutions. Traditionally, management includes K-wires or screws, but as of late, biodegradable pins offer an alternate solution. The outcomes of biodegradable pins versus K-wires were examined by Li et al. and were found to be safe and effective, with no significant differences in union rates or functional scores [34]. The pins yielded satisfactory fracture stability and healing, comparable to the standard wires [35].
- Other Applications: IM-nails were used with success for the fixation of the clavicle [36]. Osteochondral fractures of the patella, as well as femoral condylar fractures, which affect the articular surfaces, were treated with resorbable nails, pins, and screws [37,38,39]. Implants have also been used in other pediatric orthopaedic scenarios, including fractures of the radial neck, tibial eminence avulsion fractures, osteotomies for deformity correction, and even spinal deformity surgery in experimental settings. [15,40,41,42]
4. Discussion
The foremost advantage of resorbable implants is their ability to obviate the need for an additional surgery for removal. This spares children from additional anaesthesia exposure, surgical pain, and psychological stress [43]. It also reduces the risk of complications that can occur during a removal procedure, such as infections, soft tissue damage, or nerve injuries. Avoiding the routine implant removal translates to decreased expenses and a more rapid return to everyday life [43]. The polymers used may invoke only a minimal inflammatory response as they degrade; as it is reported in the literature, they typically do not elicit significant adverse tissue reactions [20]. Any local acidity from degradation is usually buffered by the body without incident [21,44]. A systematic review reported that no implant-related toxicity or systemic effects were noted, underscoring their safety [45,46]. As the implant absorbs, it gradually transfers load back to the healing bone in a more natural manner. Progressive loading may stimulate bone remodelling and avoid stress-shielding effects that sometimes occur with stiff metal implants. Continuous remodelling will yield a well-healed bone without the risk of refracture that might occur immediately after rigid metal implants are removed. Additionally, it is particularly useful for percutaneous techniques, as pins avoid having external wires protruding from the skin, decreasing the chance of soft tissue reaction or skin infections, as well as improving comfort during the healing phase. Generally, these implants have lower initial strength and stiffness than metallic ones [21,47]. While PLGA implants are strong enough for many pediatric fractures, they are not yet suitable for very large load-bearing applications, for instance, femoral shaft fractures or children with increased BMI, where metal still excels [48]. There is a risk that a bioimplant could fail (bend, break, or lose fixation) if subjected to excessive stress or weight before the bone heals. Furthermore, the physical properties of polymer implants (like their flexibility) can make them tricky to handle during surgery. Additionally, as the implants are not visible on plain radioimaging, placement that requires video confirmation is often challenging and requires experience [20,49]. A large observational series with PLGA forearm nails recorded a small number of complications, such as implant breakage or migration, leading to issues like secondary displacement or refracture in a few patients [26,27]. Some of these were attributed to technical factors (choosing the incorrect size for the implant diameter, or inadvertent cortex perforation during insertion, rather than the material failing unpredictably. Nonetheless, these events highlight that meticulous surgical technique and proper implant selection are critical to avoid early failure. In the rest of the cases, refracture occurred due to repeat trauma to the affected limb, highlighting that the correct choice might include the use of metal implants, for example, in the case of highly active children or in the case of children with disabilities. Although generally biocompatible, the degradation of polymers can lead to localised tissue reactions [44]. The acidic byproducts of PLGA resorption may cause transient inflammation, fluid accumulation, or a mild foreign-body reaction in the surrounding tissue [17,24,44]. Historically, fast-degrading materials like PGA pins occasionally produced sterile abscesses or osteolytic areas as they broke down. Modern PLGA implants, with optimised composition, have largely mitigated these issues, but surgeons should be aware of the potential. Patients might experience some localised swelling or discomfort as the implant resorbs, usually self-limited [19]. In the rare event of a severe reaction, it might necessitate a minor intervention (e.g., draining a fluid collection) [24,44]. Fortunately, large-scale studies in recent years have reported no implant-related adverse reactions requiring medical treatment, indicating that significant complications from the degradation process are quite rare. Unfortunately, biodegradable implants are not as universally available as standard metal implants. The initial cost per unit is generally higher than a simple stainless-steel screw or K-wire [50,51]. However, the savings of eliminating a second surgery potentially amount to more. In some regions, a lack of familiarity or limited supply can be a barrier to use. Additional training might be required by surgeons and operating room staff to become familiar with equipment handling. While PLGA implants present clear benefits in avoiding removal surgery and reducing certain complications, they demand careful surgical technique and case selection to overcome their current limitations.
Future Research and Outlook
The positive clinical experience to date with biodegradable implants sets the stage for broader adoption and further innovation [16]. Most studies so far report follow-up outcomes up to about 1–2 years after fracture fixation, which typically show successful healing and no early complications [7]. Nonetheless, it is suggested to examine long-term outcomes well into skeletal maturity. Additionally, more data on large patient cohorts will help identify any rare adverse events that might not surface in smaller studies. While retrospective studies have compared biodegradable implants with metal in various fractures, the field would benefit from prospective trials, including RCTs, to provide higher levels of evidence [7]. Comparing functional outcomes, complication rates, cost-effectiveness, and patient-reported outcomes (pain, satisfaction, cosmetic result) between bioabsorbable implants and standard care would highlight the benefits of modern implant types. The development of biodegradable metal implants, especially magnesium-based alloys, has also gained attention in recent years [52]. Magnesium (Mg) and Mg-based alloys can effectively dissolve in the body by way of corrosion, though with the advantage of metallic resilience [53]. Early clinical use of magnesium screws in children has shown good biocompatibility and fracture healing with complete implant resorption over time [45]. Bone healing was achieved in all patients with magnesium screws, with no implant-related adverse reactions and no need for removal, as reported by Baldini et al [5]. This favourable performance indicates that magnesium-based implants could address some constraints of polymer appliances. However, during the degradation of Mg-implants, hydrogen gas is released, which may form a pocket of gas around the implant, marked by a radiolucent area on X-ray. The gas produced during degradation could gradually be reabsorbed and poses no harm to surrounding tissues, according to some in the literature; however, there has been reports about adverse gas pocket formation. Continued development strives to design alloys and coatings that sufficiently regulate the rate of corrosion and further reduce or balance gas release. These strengthened implants could take on load-bearing applications that current polymers cannot, expanding the scope of resorbable fixation devices. Fibre-reinforced polymers (such as self-reinforced PLA) or bioactive ceramic particles that are osteogenetic during degradation are under evaluation [54,55]. Complications arising due to initial flexibility or sudden loss of mechanical integrity can be overcome by tailoring the microstructure of the polymers [16]. Drug-eluting bioimplants could further revolutionise orthopaedic care [56,57]. Implants which could release antibiotics or growth factors locally as they break down, thereby preventing infection or enhancing healing [57,58]. These multi-functional implants could be highly valuable in trauma cases with high infection risk (open fractures) or in scenarios with problematic healing [59]. Future directions are not only about the material but also implant design and how surgeons may utilise them. Computer-aided design and 3D printing are enabling patient-specific biodegradable implants, customised to the child’s anatomy and fracture pattern [15,60]. Researchers have begun exploring bioresorbable 3D-printed splints and plates that precisely fit complex shapes (acetabular fragments or small bones of the hand) [61,62]. To ensure safety and adequate selection of implant type, oversight is necessary with appropriate guidelines due to the expansion of use. Constant developments in bone and tissue engineering have led to safer, less invasive orthopaedic practices with fewer procedures required. In summary, biodegradable implants represent a noteworthy advancement in orthopaedic trauma care.
Limitations of this narrative review include the heterogeneity of the findings, with varied study designs, implant types, and follow-up durations, which makes plain comparison challenging. It does not include a systematic literature search or meta-analysis, so the selection of studies may be subject to bias. Moreover, long-term outcomes of biodegradable implants beyond several years are still limited in the literature, so the review cannot provide definitive conclusions on their effects well into skeletal maturity. Finally, because this review does not present new experimental or clinical data, its role is primarily to summarise current trends and applications rather than establish new evidence.
5. Conclusions
Biodegradable implants have introduced an important paradigm shift in the management of pediatric fractures. By providing stable fracture fixation that naturally vanishes after healing, these implants directly address the longstanding issue of routine hardware removal in children. Clinical experience over the last ten years – spanning forearm, wrist, ankle, and elbow injuries – demonstrates that modern bioresorbable devices (particularly PLGA-based implants) can achieve bone healing and functional outcomes equivalent to those of traditional metal hardware. At the same time, they confer unique benefits: children avoid additional surgeries, and the risk profile of treatment is improved with fewer implant-related complications. The safety record of these materials in growing patients has been reassuring, with high biocompatibility and minimal adverse reactions reported.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, H.N. and G.J.; methodology, G.J., and H.N.; software, H.N. and T.M.; validation, G.J., H.N..; formal analysis, H.N. and T.M.; investigation, G.J., T.M., and H.N.; resources, G.J., and H.N.; data curation, G.J.; writing—original draft preparation, H.N.; writing—review and editing, H.N. and T.M.; visualization, G.J., H.N., and T.M.; supervision, G.J.; project administration, H.N. and G.J.; funding acquisition, G.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
Not applicable. This study is a narrative review of previously published literature and did not involve new data collection or experiments with humans or animals.
Informed Consent Statement
Not applicable. The study is a review of previously published data and did not involve new research with human participants.
Data Availability Statement
All data supporting the findings of this study are contained within the article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| PLGA | poly(lactic-co-glycolic acid) |
| PGA | Polyglycolic Acid |
| PLA | Polylactic Acid |
| K-wire | Kirschner |
| ESIN | Elastic Stable Intramedullary Nailing |
| RIN | Resorbable Intramedullary Nailing |
| RCT | Randomised Controlled Trials |
| Mg | Magnesium |
References
- Ergun-Longmire, B.; Wajnrajch, M.P. Growth and Growth Disorders. In Endotext; Feingold, K.R., Ahmed, S.F., Anawalt, B., Blackman, M.R., Boyce, A., Chrousos, G., Corpas, E., de Herder, W.W., Dhatariya, K., Dungan, K., Hofland, J., Kalra, S., Kaltsas, G., Kapoor, N., Koch, C., Kopp, P., Korbonits, M., Kovacs, C.S., Kuohung, W., Laferrère, B., Levy, M., McGee, E.A., McLachlan, R., Muzumdar, R., Purnell, J., Rey, R., Sahay, R., Shah, A.S., Singer, F., Sperling, M.A., Stratakis, C.A., Trence, D.L., Wilson, D.P., Eds.; MDText.com, Inc.: South Dartmouth (MA), 2000.
- Kamel-ElSayed, S.A.; Nezwek, T.A.; Varacallo, M.A. Bone. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2025. [Google Scholar]
- Sananta, P.; Lesmana, A.; Alwy Sugiarto, M. Growth Plate Injury in Children: Review of Literature on PubMed. J. Public Health Res. 2022, 11, 22799036221104155. [Google Scholar] [CrossRef]
- Hedelin, H. Bioabsorbable Screws for Pelvic Osteotomies in Children.
- Baldini, M.; Coppa, V.; Falcioni, D.; Cusano, G.; Massetti, D.; Marinelli, M.; Gigante, A.P. Resorbable Magnesium Screws for Fixation of Medial Epicondyle Avulsion Fractures in Skeletally Immature Patients: A Comparison with Kirschner Wires. J. Child. Orthop. 2022, 16, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Gentile, P.; Chiono, V.; Carmagnola, I.; Hatton, P.V. An Overview of Poly(Lactic-Co-Glycolic) Acid (PLGA)-Based Biomaterials for Bone Tissue Engineering. Int. J. Mol. Sci. 2014, 15, 3640–3659. [Google Scholar] [CrossRef] [PubMed]
- Gentile, P.; Chiono, V.; Carmagnola, I.; Hatton, P.V. An Overview of Poly(Lactic-Co-Glycolic) Acid (PLGA)-Based Biomaterials for Bone Tissue Engineering. Int. J. Mol. Sci. 2014, 15, 3640–3659. [Google Scholar] [CrossRef]
- Sun, F.; Sun, X.; Wang, H.; Li, C.; Zhao, Y.; Tian, J.; Lin, Y. Application of 3D-Printed, PLGA-Based Scaffolds in Bone Tissue Engineering. Int. J. Mol. Sci. 2022, 23, 5831. [Google Scholar] [CrossRef]
- Yang, Y.; Chen, Z.; Hu, Y.; Tian, Y. Biomechanical Evaluation of Novel 3D-Printed Magnesium Alloy Scaffolds for Treating Proximal Humerus Fractures with Medial Column Instability. Injury 2025, 56. [Google Scholar] [CrossRef]
- Ağırdil, Y. The Growth Plate: A Physiologic Overview. EFORT Open Rev. 2020, 5, 498–507. [Google Scholar] [CrossRef]
- Burdan, F.; Szumiło, J.; Korobowicz, A.; Farooquee, R.; Patel, S.; Patel, A.; Dave, A.; Szumiło, M.; Solecki, M.; Klepacz, R.; et al. Morphology and Physiology of the Epiphyseal Growth Plate. Folia Histochem. Cytobiol. 2009, 47, 5–16. [Google Scholar] [CrossRef]
- Dl, H.; Np, H.; J, S.; P, M.; R, M.; B, H. AO Philosophy and Principles of Fracture Management-Its Evolution and Evaluation. J. Bone Joint Surg. Am. 2003, 85, 1156–1160. [Google Scholar]
- Hodgson, S. AO Principles of Fracture Management. Ann. R. Coll. Surg. Engl. 2009, 91, 448–449. [Google Scholar] [CrossRef]
- Singh, V.; Garg, V.; Parikh, S.N. Management of Physeal Fractures: A Review Article. Indian J. Orthop. 2021, 55, 525–538. [Google Scholar] [CrossRef]
- Banothu, D.; Kumar, P.; Ali, S.G.M.; Reddy, R.; Gobinath, R.; Dhanapalan, S. Design, Fabrication, and in Vitro Evaluation of a 3D Printed, Bio-Absorbable PLA Tibia Bone Implant with a Novel Lattice Structure. Biomed. Phys. Eng. Express 2025, 11. [Google Scholar] [CrossRef]
- Rocha, C.V.; Gonçalves, V.; da Silva, M.C.; Bañobre-López, M.; Gallo, J. PLGA-Based Composites for Various Biomedical Applications. Int. J. Mol. Sci. 2022, 23, 2034. [Google Scholar] [CrossRef] [PubMed]
- Landes, C.A.; Ballon, A.; Roth, C. In-Patient versus in Vitro Degradation of P(L/DL)LA and PLGA. J. Biomed. Mater. Res. B Appl. Biomater. 2006, 76, 403–411. [Google Scholar] [CrossRef]
- Whitepapers - Bioretec Ltd. Available online: https://bioretec.com/educational-materials/whitepapers?medical_professional=on&category=12 (accessed on 5 August 2023).
- Perhomaa, M.; Pokka, T.; Korhonen, L.; Kyrö, A.; Niinimäki, J.; Serlo, W.; Sinikumpu, J.-J. Randomized Controlled Trial of the Clinical Recovery and Biodegradation of Polylactide-Co-Glycolide Implants Used in the Intramedullary Nailing of Children’s Forearm Shaft Fractures with at Least Four Years of Follow-Up. J. Clin. Med. 2021, 10, 995. [Google Scholar] [CrossRef]
- Hedelin, H.; Hebelka, H.; Brisby, H.; Laine, T. MRI Evaluation of Resorbable Poly Lactic-Co-Glycolic Acid (PLGA) Screws Used in Pelvic Osteotomies in Children—a Retrospective Case Series. J. Orthop. Surg. 2020, 15, 329. [Google Scholar] [CrossRef]
- Félix Lanao, R.P.; Jonker, A.M.; Wolke, J.G.C.; Jansen, J.A.; van Hest, J.C.M.; Leeuwenburgh, S.C.G. Physicochemical Properties and Applications of Poly(Lactic-Co-Glycolic Acid) for Use in Bone Regeneration. Tissue Eng. Part B Rev. 2013, 19, 380–390. [Google Scholar] [CrossRef]
- Lee, J.S.; Curnutte, B.; Pan, K.; Liu, J.; Ebraheim, N.A. Biomechanical Comparison of Suture-Button, Bioabsorbable Screw, and Metal Screw for Ankle Syndesmotic Repair: A Meta-Analysis. Foot Ankle Surg. Off. J. Eur. Soc. Foot Ankle Surg. 2021, 27, 117–122. [Google Scholar] [CrossRef]
- Lőrincz, A.; Lengyel, Á.M.; Kedves, A.; Nudelman, H.; Józsa, G. Pediatric Diaphyseal Forearm Fracture Management with Biodegradable Poly-L-Lactide-Co-Glycolide (PLGA) Intramedullary Implants: A Longitudinal Study. J. Clin. Med. 2024, 13, 4036. [Google Scholar] [CrossRef] [PubMed]
- Perhomaa, M.; Pokka, T.; Korhonen, L.; Kyrö, A.; Niinimäki, J.; Serlo, W.; Sinikumpu, J.-J. Randomized Controlled Trial of the Clinical Recovery and Biodegradation of Polylactide-Co-Glycolide Implants Used in the Intramedullary Nailing of Children’s Forearm Shaft Fractures with at Least Four Years of Follow-Up. J. Clin. Med. 2021, 10, 995. [Google Scholar] [CrossRef] [PubMed]
- Eastwood, F.; Raheman, F.; Al-Dairy, G.; Popescu, M.; Henney, C.; Hunwick, L.; Buddhdev, P. Healing Smarter: A Systematic Review and Meta-Analysis of Bioresorbable Implants for Paediatric Forearm Fractures. J. Child. Orthop. 2025, 19, 422–431. [Google Scholar] [CrossRef] [PubMed]
- Roeder, C.; Alves, C.; Balslev-Clausen, A.; Canavese, F.; Gercek, E.; Kassai, T.; Klestil, T.; Klingenberg, L.; Lutz, N.; Varga, M.; et al. Pilot Study and Preliminary Results of Biodegradable Intramedullary Nailing of Forearm Fractures in Children. Child. Basel Switz. 2022, 9, 754. [Google Scholar] [CrossRef]
- Korhonen, L.; Perhomaa, M.; Kyrö, A.; Pokka, T.; Serlo, W.; Merikanto, J.; Sinikumpu, J.-J. Intramedullary Nailing of Forearm Shaft Fractures by Biodegradable Compared with Titanium Nails: Results of a Prospective Randomized Trial in Children with at Least Two Years of Follow-Up. Biomaterials 2018, 185, 383–392. [Google Scholar] [CrossRef]
- Varga, M.; Józsa, G.; Hanna, D.; Tóth, M.; Hajnal, B.; Krupa, Z.; Kassai, T. Bioresorbable Implants vs. Kirschner-Wires in the Treatment of Severely Displaced Distal Paediatric Radius and Forearm Fractures - a Retrospective Multicentre Study. BMC Musculoskelet. Disord. 2022, 23, 362. [Google Scholar] [CrossRef]
- Noh, J.H.; Roh, Y.H.; Yang, B.G.; Kim, S.W.; Lee, J.S.; Oh, M.K. Outcomes of Operative Treatment of Unstable Ankle Fractures: A Comparison of Metallic and Biodegradable Implants. J. Bone Joint Surg. Am. 2012, 94, e166. [Google Scholar] [CrossRef]
- Nudelman, H.; Lőrincz, A.; Lamberti, A.G.; Varga, M.; Kassai, T.; Józsa, G. Management of Pediatric Ankle Fractures: Comparison of Biodegradable PLGA Implants with Traditional Metal Screws. Front. Pediatr. 2024, 12, 1410750. [Google Scholar] [CrossRef] [PubMed]
- van der Eng, D.M.; Schep, N.W.L.; Schepers, T. Bioabsorbable Versus Metallic Screw Fixation for Tibiofibular Syndesmotic Ruptures: A Meta-Analysis. J. Foot Ankle Surg. Off. Publ. Am. Coll. Foot Ankle Surg. 2015, 54, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Rangdal, S.; Singh, D.; Joshi, N.; Soni, A.; Sament, R. Functional Outcome of Ankle Fracture Patients Treated with Biodegradable Implants. Foot Ankle Surg. Off. J. Eur. Soc. Foot Ankle Surg. 2012, 18, 153–156. [Google Scholar] [CrossRef]
- Li, Z.-H.; Yu, A.-X.; Guo, X.-P.; Qi, B.-W.; Zhou, M.; Wang, W.-Y. Absorbable Implants versus Metal Implants for the Treatment of Ankle Fractures: A Meta-Analysis. Exp. Ther. Med. 2013, 5, 1531–1537. [Google Scholar] [CrossRef]
- Nazzal, E.M.; Mattar, L.T.; Newell, B.W.; Coutinho, D.V.; Kaufmann, R.A.; Baratz, M.E.; Debski, R.E. Do Intramedullary Screws Provide Adequate Fixation for Humeral and Ulnar Components in Total Elbow Arthroplasty? A Cadaveric Analysis. J. Hand Surg. 2025, 50, 239.e1–239.e8. [Google Scholar] [CrossRef]
- Helling, H.-J.; Prokop, A.; Schmid, H.U.; Nagel, M.; Lilienthal, J.; Rehm, K.E. Biodegradable Implants versus Standard Metal Fixation for Displaced Radial Head Fractures. A Prospective, Randomized, Multicenter Study. J. Shoulder Elbow Surg. 2006, 15, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Osborn, E.J.; Farnsworth, C.L.; Doan, J.D.; Edmonds, E.W. Bioabsorbable Plating in the Treatment of Pediatric Clavicle Fractures: A Biomechanical and Clinical Analysis. Clin. Biomech. Bristol Avon 2018, 55, 94–99. [Google Scholar] [CrossRef]
- Gkiokas, A.; Morassi, L.G.; Kohl, S.; Zampakides, C.; Megremis, P.; Evangelopoulos, D.S. Bioabsorbable Pins for Treatment of Osteochondral Fractures of the Knee after Acute Patella Dislocation in Children and Young Adolescents. Adv. Orthop. 2012, 2012, e249687. [Google Scholar] [CrossRef]
- Ren, G.-Z.; Zhang, Z.-L.; Han, P.-F.; Chen, T.-Y.; Li, P.-C.; Wei, X.-C. [Meta-analysis of clinical effects between non-metallic materials and metallic materials by internal fixation for patellar fracture]. Zhongguo Gu Shang China J. Orthop. Traumatol. 2018, 31, 927–932. [Google Scholar] [CrossRef]
- Camarda, L.; Morello, S.; Balistreri, F.; D’Arienzo, A.; D’Arienzo, M. Non-Metallic Implant for Patellar Fracture Fixation: A Systematic Review. Injury 2016, 47, 1613–1617. [Google Scholar] [CrossRef]
- Zeng, M.; Xie, K.; Cao, S.; Wen, J.; Wang, S.; Xiao, S. Midterm Comparative Result of Absorbable Screws and Metal Screws in Pediatric Medial Humeral Epicondyle Fracture. J. Orthop. Sci. 2025, 30, 824–829. [Google Scholar] [CrossRef]
- Kim, W.S.; Oh, M.J.; Park, M.S.; Sung, K.H. Comparison of Surgical Outcomes between Bioabsorbable and Metal Screw Fixation for Distal Tibial Physeal Fracture in Children and Adolescent. Int. Orthop. 2024, 48, 2681–2687. [Google Scholar] [CrossRef]
- Chen, T.; Wen, Y.; Zhu, D.; Feng, W.; Song, B.; Wang, Q. Comparison of Bioabsorbable Screw versus Metallic Screw Fixation for Tibial Tubercle Fractures in Adolescents: A Retrospective Cohort Study. BMC Musculoskelet. Disord. 2025, 26, 38. [Google Scholar] [CrossRef]
- Heye, P.; Matissek, C.; Seidl, C.; Varga, M.; Kassai, T.; Jozsa, G.; Krebs, T. Making Hardware Removal Unnecessary by Using Resorbable Implants for Osteosynthesis in Children. Children 2022, 9, 471. [Google Scholar] [CrossRef] [PubMed]
- Elmowafy, E.M.; Tiboni, M.; Soliman, M.E. Biocompatibility, Biodegradation and Biomedical Applications of Poly(Lactic Acid)/Poly(Lactic-Co-Glycolic Acid) Micro and Nanoparticles. J. Pharm. Investig. 2019, 49, 347–380. [Google Scholar] [CrossRef]
- Baldini, M.; Coppa, V.; Falcioni, D.; Senigagliesi, E.; Marinelli, M.; Gigante, A.P. Use of Resorbable Magnesium Screws in Children: Systematic Review of the Literature and Short-Term Follow-Up From Our Series. J. Child. Orthop. 2022, 16, 77–80. [Google Scholar] [CrossRef]
- Barber, F.A.; Spenciner, D.B.; Bhattacharyya, S.; Miller, L.E. Biocomposite Implants Composed of Poly(Lactide-Co-Glycolide)/β-Tricalcium Phosphate: Systematic Review of Imaging, Complication, and Performance Outcomes. Arthrosc. J. Arthrosc. Relat. Surg. Off. Publ. Arthrosc. Assoc. N. Am. Int. Arthrosc. Assoc. 2017, 33, 683–689. [Google Scholar] [CrossRef]
- Hedelin, H.; Larnert, P.; Antonsson, P.; Lagerstrand, K.; Brisby, H.; Hebelka, H.; Laine, T. Stability in Pelvic Triple Osteotomies in Children Using Resorbable PLGA Screws for Fixation. J. Pediatr. Orthop. 2021, 41, e787. [Google Scholar] [CrossRef]
- Taghipour, S.; Vakili-Tahami, F.; Chakherlou, T.N. Comparing the Performance of a Femoral Shaft Fracture Fixation Using Implants with Biodegradable and Non-Biodegradable Materials. Biomed. Phys. Eng. Express 2025, 11. [Google Scholar] [CrossRef]
- Gentile, P.; Chiono, V.; Carmagnola, I.; Hatton, P.V. An Overview of Poly(Lactic-Co-Glycolic) Acid (PLGA)-Based Biomaterials for Bone Tissue Engineering. Int. J. Mol. Sci. 2014, 15, 3640–3659. [Google Scholar] [CrossRef]
- Juutilainen, T.; Pätiälä, H.; Ruuskanen, M.; Rokkanen, P. Comparison of Costs in Ankle Fractures Treated with Absorbable or Metallic Fixation Devices. Arch. Orthop. Trauma Surg. 1997, 116, 204–208. [Google Scholar] [CrossRef]
- van Bakelen, N.B.; Vermeulen, K.M.; Buijs, G.J.; Jansma, J.; de Visscher, J.G. a. M.; Hoppenreijs, T.J.M.; Bergsma, J.E.; Stegenga, B.; Bos, R.R.M. Cost-Effectiveness of a Biodegradable Compared to a Titanium Fixation System in Maxillofacial Surgery: A Multicenter Randomized Controlled Trial. PloS One 2015, 10, e0130330. [Google Scholar] [CrossRef] [PubMed]
- Ahemad, D.A.Z.; Rattan, P.D.V.; Jolly, D.S.S.; Kalra, P.D.P.; Sharma, D.S. Biomechanical Comparison of Magnesium Bioresorbable and Titanium Lag Screws for Mandibular Symphysis Fracture Fixation: A Finite Element Analysis. J. Stomatol. Oral Maxillofac. Surg. 2025, 102383. [Google Scholar] [CrossRef] [PubMed]
- Takata, K.; Yugami, M.; Karata, S.; Karasugi, T.; Uehara, Y.; Masuda, T.; Nakamura, T.; Tokunaga, T.; Hisanaga, S.; Sugimoto, K.; et al. Plates Made from Magnesium Alloy with a Long Period Stacking Ordered Structure Promote Bone Formation in a Rabbit Fracture Model. Sci. Rep. 2025, 15, 12210. [Google Scholar] [CrossRef] [PubMed]
- Workie, A.B.; Shih, S.-J. A Study of Bioactive Glass-Ceramic’s Mechanical Properties, Apatite Formation, and Medical Applications. RSC Adv. 2022, 12, 23143–23152. [Google Scholar] [CrossRef]
- Brunello, G.; Elsayed, H.; Biasetto, L. Bioactive Glass and Silicate-Based Ceramic Coatings on Metallic Implants: Open Challenge or Outdated Topic? Mater. Basel Switz. 2019, 12, 2929. [Google Scholar] [CrossRef]
- Alshimaysawee, S.; Fadhel Obaid, R.; Al-Gazally, M.E.; Alexis Ramírez-Coronel, A.; Bathaei, M.S. Recent Advancements in Metallic Drug-Eluting Implants. Pharmaceutics 2023, 15, 223. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, P.; Srivastava, A.; Bhati, P.; Chaturvedi, M.; Patil, V.; Kunnoth, S.; Kumari, N.; Arya, V.; Pandya, M.; Agarwal, M.; et al. Enhanced Osseointegration of Drug Eluting Nanotubular Dental Implants: An in Vitro and in Vivo Study. Bioact. Mater. 2023, 28, 432–447. [Google Scholar] [CrossRef]
- Suhardi, V.J.; Bichara, D.A.; Kwok, S.; Freiberg, A.A.; Rubash, H.; Malchau, H.; Yun, S.H.; Muratoglu, O.K.; Oral, E. A Fully Functional Drug-Eluting Joint Implant. Nat. Biomed. Eng. 2017, 1, 0080. [Google Scholar] [CrossRef]
- Ballard, D.H.; Tappa, K.; Boyer, C.J.; Jammalamadaka, U.; Hemmanur, K.; Weisman, J.A.; Alexander, J.S.; Mills, D.K.; Woodard, P.K. Antibiotics in 3D-Printed Implants, Instruments and Materials: Benefits, Challenges and Future Directions. J. 3D Print. Med. 2019, 3, 83–93. [Google Scholar] [CrossRef]
- Li, Z.; Wang, Q.; Liu, G. A Review of 3D Printed Bone Implants. Micromachines 2022, 13, 528. [Google Scholar] [CrossRef]
- Nicum, A.; Hothi, H.; Henckel, J.; di Laura, A.; Schlueter-Brust, K.; Hart, A. Characterisation of 3D-Printed Acetabular Hip Implants. EFORT Open Rev. 2024, 9, 862–872. [Google Scholar] [CrossRef] [PubMed]
- Anil, U.; Terner, B.; Karim, M.A.; Ebied, A.; Polkowski, G.G.; Schwarzkopf, R. Total Hip Arthroplasty in Challenging Settings: Acetabular Fractures, Adolescents, Conversions, and Developmental Dysplasia of the Hip. J. Arthroplasty 2025, 40, S49–S58. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



