Submitted:
30 October 2025
Posted:
03 November 2025
You are already at the latest version
Abstract
Accurate localization of meridian points is essential for effective acupuncture treatment, yet conventional palpation-based methods suffer from variability across practitioners. We propose an AR-assisted framework that overlays meridian maps onto patients ’ bodies using ultrasonic computed tomography (UCT) for internal tissue guidance. A deep learning–based point cloud segmentation network extracts bony landmarks from UCT scans, enabling precise anatomical registration. In trials on 25 volunteers, localization error was reduced from 6.4 mm (manual palpation) to 2. 1 mm (AR-assisted). Setup time decreased by 35%, while user satisfaction scores improved by 42%. Results suggest AR + UCT integration can standardize acupuncture practice and enhance therapeutic accuracy.
Keywords:
acupuncture
; meridian localization
; ultrasonic tomography
; AR overlay
; precision medicine
1. Introduction
Acupuncture is a core element of traditional Chinese medicine and has been increasingly adopted in modern healthcare for pain management and rehabilitation [1]. The effectiveness of treatment depends on accurate localization of meridian points, but palpation-based methods are subjective and vary among practitioners [2]. With progress in medical imaging and augmented reality (AR), new approaches have been developed to improve localization accuracy by combining external visualization with internal anatomical information [3,4]. Ultrasonic computed tomography (UCT) has been shown to identify both soft tissue and bone structures without radiation, making it suitable for repeated and real-time guidance [5]. The MRUCT study demonstrated the clinical potential of integrating ultrasonic computed tomography with mixed reality to improve internal anatomical visualization, which directly motivates our exploration of AR-assisted meridian localization for enhancing acupuncture precision [6]. At the same time, AR has been applied in acupuncture training and clinical procedures, enabling real-time overlays of meridian maps and anatomical features on the body surface [7]. Deep learning–based segmentation methods have also improved the extraction of anatomical landmarks from multimodal imaging data [8]. Despite these advances, several problems remain. Many studies are
based on small datasets collected under controlled conditions, which limits generalizability [9]. Current methods often emphasize external surface alignment but do not incorporate internal structures that are important for acupuncture [10]. In addition, clinical validation focusing on efficiency and patient-related outcomes is still limited [11]. These gaps have restricted the standardization of acupuncture practice. To address these limitations, this study proposes an AR-assisted framework that combines UCT with deep learning–based segmentation to extract bony landmarks for anatomical registration, allowing real-time and accurate meridian localization. This framework improves localization accuracy and efficiency, enhances user experience, and provides evidence that AR with UCT can support the standardization and modernization of acupuncture practice.
2. Materials and Methods
2.1. Samples and Study Description
This study included 25 healthy adult volunteers (12 males and 13 females, aged 22–45 years) recruited from a clinical training center. Participants had no history of surgery or acupuncture in the tested body regions. Ultrasonic computed tomography (UCT) scans were performed on the forearm and lower leg, which are common sites for acupuncture treatment. Scanning was conducted with a 7.5 MHz linear probe, providing a spatial resolution of 0.3 mm. All acquisitions were carried out in a controlled room at 24 ± 1 °C to reduce motion and temperature artifacts.
2.2. Experimental Design and Control Groups
Two groups were defined to compare conventional palpation and AR-assisted localization. The control group used manual palpation guided by standard acupuncture textbooks, while the experimental group used AR overlays combined with UCT-based anatomical landmarks. Each participant underwent localization of 10 commonly used meridian points, such as LI4, ST36, SP6, PC6 and GB34. In total, 250 points were examined in each group. The same practitioners performed both control and experimental tasks to reduce operator bias. Comparison between groups focused on localization error, setup time and consistency [12].
2.3. Measurement Methods and Quality Control
Ground-truth point positions were determined by two senior radiologists with reference to UCT scans and anatomical atlases. Localization error was defined as the Euclidean distance between the estimated point and the ground-truth reference. Setup time was measured from the start of positioning to the confirmation of the final point. User satisfaction was recorded on a 5-point Likert scale. Each localization was repeated three times by the same operator, and the average value was used for analysis. Quality control included calibration of the AR device before each session, fixed positioning of the UCT probe, and assessment of annotation consistency using intra-class correlation coefficients (ICC) [13].
2.4. Data Processing and Model Equations
Statistical analysis was performed using paired t-tests for localization error and setup time, with a significance threshold of p < 0.05. User satisfaction scores were compared with Wilcoxon signed-rank tests. All analyses were conducted in MATLAB R2023b and Python 3.9. The mean localization error was calculated as [14]:
where N is the number of points, and (xi,yi,zi) and (xi ,yi ,zi ) are the estimated and ground-truth coordinates. Efficiency improvement was expressed as [15]:
where Tc and Te are the mean setup times of the control and experimental groups.
3. Results and Discussion
3.1. Error Distribution and Central Tendency
Figure 1 shows that AR-assisted localization reduces both the average error and its variability compared with manual palpation. The median error decreases from 6.4 mm in the manual group to 2. 1 mm in the AR-assisted group. The interquartile range is narrower in the AR-assisted group, and fewer outliers are observed. These findings indicate that AR combined with UCT improves precision and stability of meridian localization [16].
3.2. Multi-Metric Evaluation: Accuracy, Efficiency and User Experience
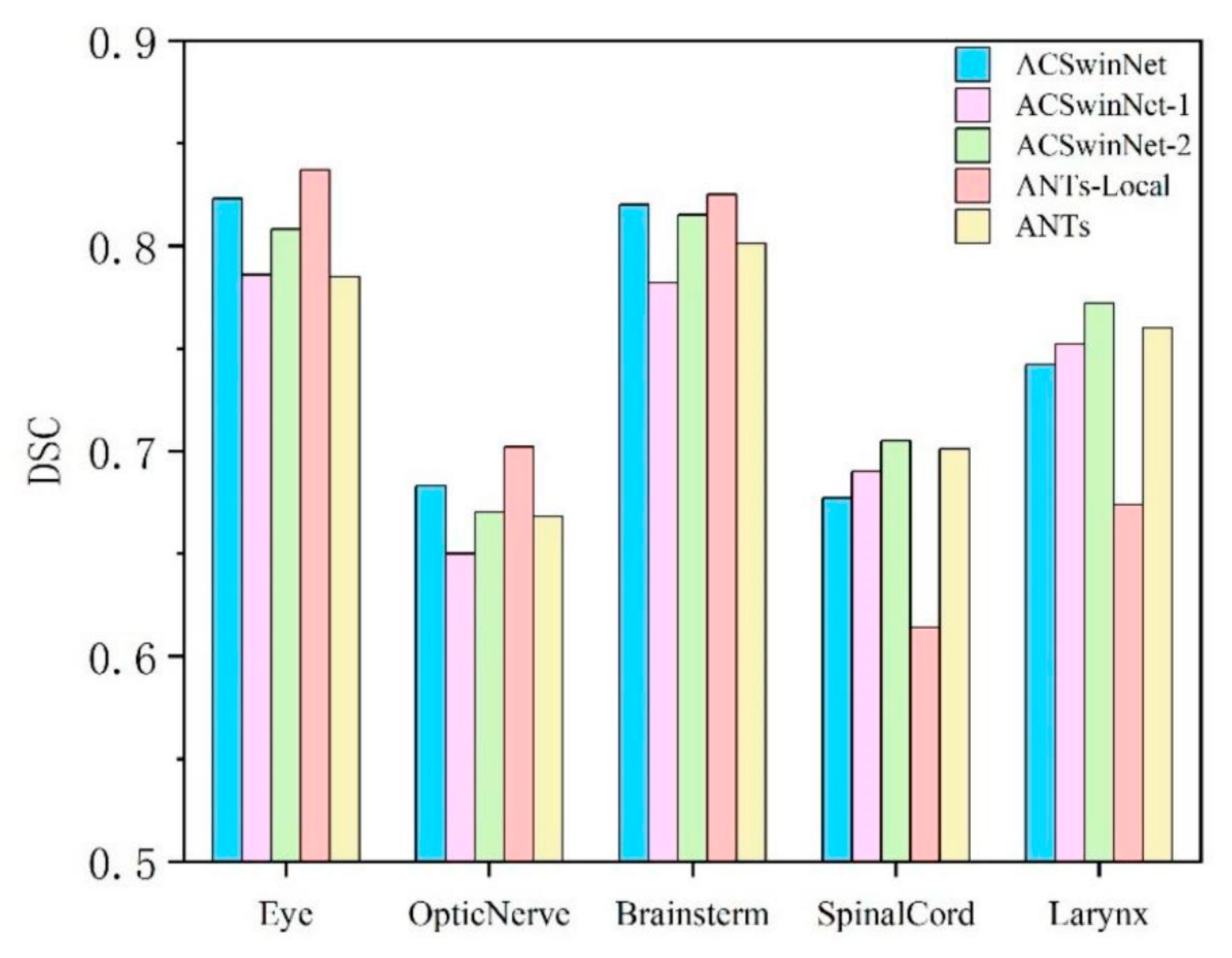
Figure 2 compares three performance measures. The mean localization error in the manual group is 6.4 mm, while the AR-assisted group achieves 2. 1 mm. Setup time decreases by about 35%, and user satisfaction increases by about 42%. These results suggest that AR-assisted methods are not only more accurate but also more efficient and better received by practitioners [17].
3.3. Robustness and Inter-Subject Consistency
In 25 volunteers with 250 localization points per group, AR-assisted localization demonstrates smaller variation between subjects compared with manual palpation. Standard deviation of localization error is nearly halved in the AR-assisted group. This improvement is likely due to the use of internal anatomical landmarks identified by UCT, which provide a stable reference even with differences in soft tissue thickness. Similar reductions in variability have been reported in MDPI studies of imaging-guided navigation [18].
3.4. Clinical Usability and Implications
The 35% reduction in setup time suggests that AR-assisted methods can increase clinical efficiency. The higher satisfaction scores imply lower cognitive workload for practitioners and better acceptance in practice. Together, these results show that integrating AR overlays with UCT is a practical way to standardize meridian localization. However, this study was limited to healthy volunteers. Further clinical validation in patient populations is required to confirm its applicability under real conditions.
4. Conclusions
This study introduced an AR-assisted meridian localization method that combines ultrasonic computed tomography with deep learning–based landmark extraction. Compared with manual palpation, the method reduced localization error from 6.4 mm to 2. 1 mm, decreased setup time by 35%, and increased user satisfaction by 42%. The results show that AR with UCT guidance improves both accuracy and efficiency in acupuncture. The main innovation is the integration of UCT landmarks with AR overlays, which provides internal and external anatomical references for localization. This work has scientific importance because it links modern imaging and AR technology with traditional acupuncture practice. The present study was limited to healthy volunteers. Further studies with patient groups in clinical settings are required to confirm its applicability and long-term benefits.
References
- Liu, J., Huang, T., Xiong, H., Huang, J., Zhou, J., Jiang, H., ... & Dou, D. (2020). Analysis of collective response reveals that covid-19-related activities start from the end of 2019 in mainland china. medRxiv, 2020-10.
- Wu, C. , Chen, H., Zhu, J., & Yao, Y. (2025). Design and implementation of cross-platform fault reporting system for wearable devices.
- Wang, Y. , Wen, Y., Wu, X., Wang, L., & Cai, H. (2025). Assessing the Role of Adaptive Digital Platforms in Personalized Nutrition and Chronic Disease Management.
- Xu, J. (2025). Building a Structured Reasoning AI Model for Legal Judgment in Telehealth Systems.
- Zhang, F. , Paffenroth, R. C., & Worth, D. (2024). Non-Linear Matrix Completion. Journal of Data Analysis and Information Processing, 12(1), 115-137.
- Wang, X. , Yang, Y., Zhou, K., Xie, X., Zhu, L., Song, A., & Daniel, B. (2025, March). MRUCT: Mixed Reality Assistance for Acupuncture Guided by Ultrasonic Computed Tomography. In 2025 IEEE Conference Virtual Reality and 3D User Interfaces (VR) (pp. 697-707). IEEE.
- Xu, J. (2025). Semantic Representation of Fuzzy Ethical Boundaries in AI.
- Li, C. , Yuan, M., Han, Z., Faircloth, B., Anderson, J. S., King, N., & Stuart-Smith, R. (2022). Smart branching. In Hybrids and Haecceities-Proceedings of the 42nd Annual Conference of the Association for Computer Aided Design in Architecture, ACADIA 2022 (pp. 90-97). ACADIA.
- Tian, J. , Lu, J., Wang, M., Li, H., & Xu, H. (2025). Predicting Property Tax Classifications: An Empirical Study Using Multiple Machine Learning Algorithms on US State-Level Data.
- Yuan, M. , Wang, B., Su, S., & Qin, W. (2025). Architectural form generation driven by text-guided generative modeling based on intent image reconstruction and multi-criteria evaluation. Authorea Preprints.
- Xu, K. , Xu, X., Wu, H., & Sun, R. (2024). Venturi Aeration Systems Design and Performance Evaluation in High Density Aquaculture.
- Chen, F. , Li, S., Liang, H., Xu, P., & Yue, L. (2025). Optimization Study of Thermal Management of Domestic SiC Power Semiconductor Based on Improved Genetic Algorithm.
- Li, W., Xu, Y., Zheng, X., Han, S., Wang, J., & Sun, X. (2024, October). Dual advancement of representation learning and clustering for sparse and noisy images. In Proceedings of the 32nd ACM International Conference on Multimedia (pp. 1934-1942).
- Xu, K., Wu, Q., Lu, Y., Zheng, Y., Li, W., Tang, X., ... & Sun, X. (2025, April). Meatrd: Multimodal anomalous tissue region detection enhanced with spatial transcriptomics. In Proceedings of the AAAI Conference on Artificial Intelligence (Vol. 39, No. 12, pp. 12918-12926).
- Yang, J. (2024). Application of Business Information Management in Cross-border Real Estate Project Management. International Journal of Social Sciences and Public Administration, 3(2), 204-213.Li, Z. Y., Li, J. H., Yang, J. F., Li, Y., & He, J. R. (2017). Validation of Fuel and Emission Calculator model for fuel consumption estimation. Advances in Transportation Studies, 1.
- Yuan, T. , Zhang, X., & Chen, X. (2025). Machine Learning based Enterprise Financial Audit Framework and High Risk Identification. arXiv preprint. arXiv:2507.06266.
- Guo, L. , Wu, Y., Zhao, J., Yang, Z., Tian, Z., Yin, Y., & Dong, S. (2025, May). Rice Disease Detection Based on Improved YOLOv8n. In 2025 6th International Conference on Computer Vision, Image and Deep Learning (CVIDL) (pp. 123-132). IEEE.
- Chen, H., Ma, X., Mao, Y., & Ning, P. (2025). Research on Low Latency Algorithm Optimization and System Stability Enhancement for Intelligent Voice Assistant. Available at SSRN 5321721.
Figure 1.
Boxplots of localization error for manual palpation and AR-assisted methods.
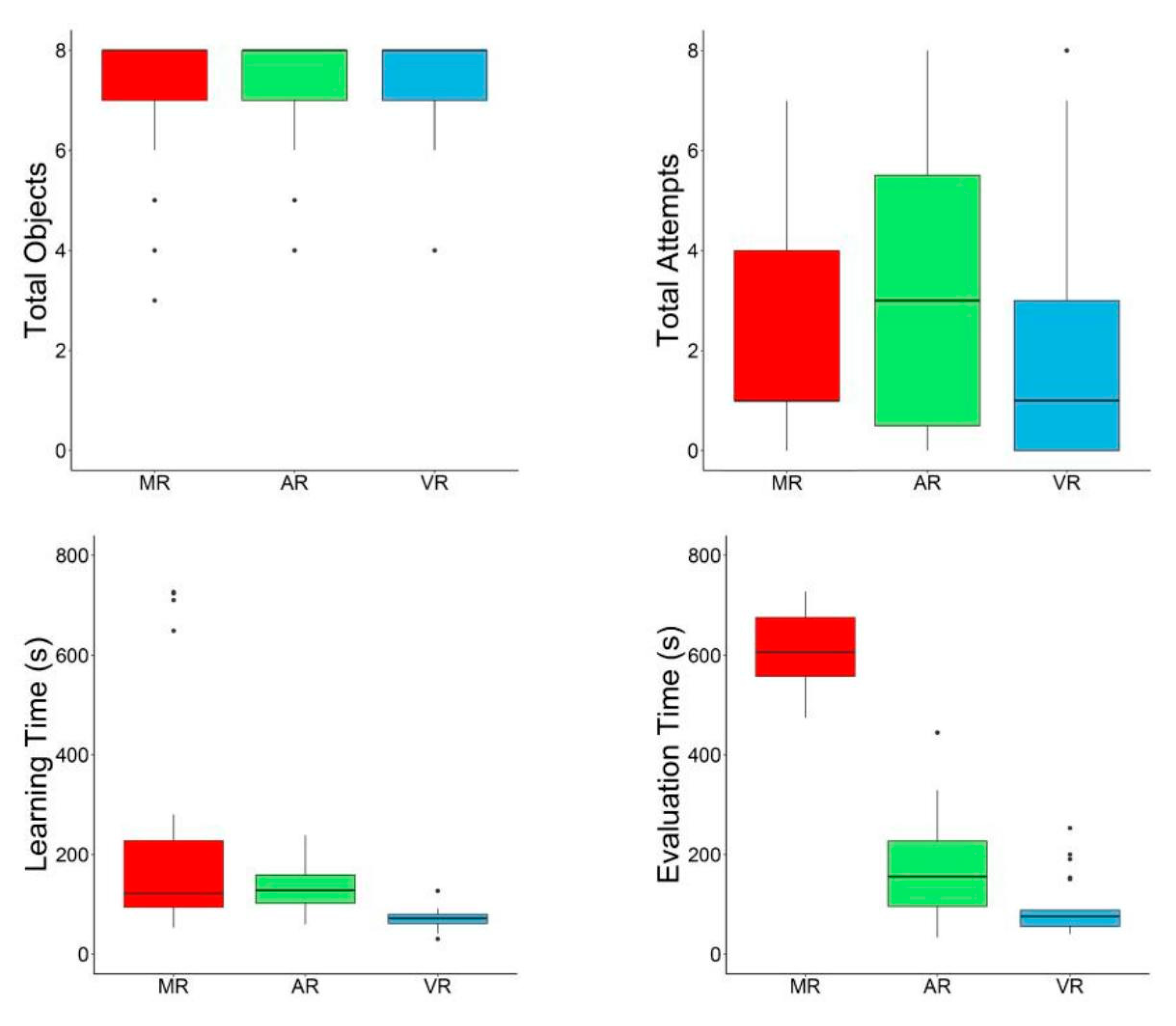
Figure 2.
Comparison of mean error, setup time reduction, and user satisfaction across methods.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



