
Submitted:
29 October 2025
Posted:
30 October 2025
You are already at the latest version
Abstract
Lung involvement in patients with leptospirosis is associated with a more complicated disease course. However, the demographic and clinical associations of lung involvement are incompletely defined, and its optimal management is uncertain. This retrospective study examined consecutive patients admitted to a referral hospital in tropical Australia, with laboratory-confirmed leptospirosis between January 2015, and June 2024. Lung involvement was defined as new lung parenchymal changes on chest imaging at any point during the patients’ hospitalisation. The demographics, clinical findings and clinical course of the patients with – and without – lung involvement were compared. The median (interquartile range (IQR)) age of the 109 patients was 39 (24-56) years; 93/109 (85%) were male. Lung involvement was present in 62/109 (57%), 55 (89%) of whom had no documented comorbidities. Patients with lung involvement re-ceived antibiotics later in their disease course than those without lung involvement (median (IQR): 5 (4-6) versus 3 (2-5) days of symptoms, p=0.001). Lung involvement was frequently just one component associated with multi-organ failure: patients with lung involvement were more likely to require inten-sive care unit admission than patients without lung involvement (41/62 (66%) versus 15/47 (32%), p< 0.001). Overall, 30/109 (28%) satisfied criteria for acute respiratory distress syndrome (ARDS) and 26/109 (24%) developed pulmonary haemorrhage. Patients with lung involvement received cautious fluid resuscitation, vasopressor support and prompt initiation of additional supportive care – including me-chanical ventilation, renal replacement therapy and extracorporeal membranous oxygenation – guided by the patients’ physiological parameters and clinical trajectory. All 109 patients in the cohort were alive 90 days after discharge. Life-threatening lung involvement can complicate leptospirosis in young and otherwise well individuals. However, in Australia’s well-resourced health system excellent outcomes can be achieved using a standard contemporary approach to the management of a patient with undif-ferentiated infection while a confirmed diagnosis of leptospirosis is awaited.
Keywords:
leptospirosis
; lung disease
; pulmonary haemorrhage
; clinical management
; critical care
; tropical medicine
; pathophysiology
1. Introduction
Leptospirosis is a potentially life-threatening zoonotic disease caused by pathogenic spirochetes of the genus Leptospira. In 2015, it was estimated that globally there were over one million human cases annually resulting in almost 59,000 deaths [1]. The case-fatality rate of patients with severe leptospirosis who are admitted to the intensive care unit (ICU) can exceed 50% [2]. Despite this, leptospirosis remains an under recognised disease and its pathophysiology and optimal management are still incompletely understood [3,4,5,6,7].
Symptomatic leptospirosis typically presents with fever, rigors, myalgia, nausea, vomiting and headache. In most individuals it is a mild illness, but approximately 10% of cases develop severe disease characterised by rapidly evolving multiorgan dysfunction with manifestations that can include hypotension, acute kidney injury (AKI), pulmonary haemorrhage and acute respiratory distress syndrome (ARDS) [5]. Lung involvement is often a harbinger of a more complicated disease course with death almost 10 times more common in patients with lung involvement in some series [8,9,10,11].
However, there is uncertainty about risk factors for lung involvement and how best to manage the patients who develop this complication. Although antibiotics are recommended in patients with symptomatic leptospirosis, the incremental value of antibiotic therapy above optimal supportive care is uncertain [5,12]. Conservative fluid management strategies are frequently employed in individuals with lung involvement although achieving an optimal fluid balance is challenging in individuals who are also often hypotensive and/or have AKI [13,14,15]. Some observational studies have suggested benefit of corticosteroid therapy in individuals with lung involvement, however evidence of benefit in randomised trials is lacking [16,17]. Plasma exchange, plasmapheresis and extracorporeal membrane oxygenation (ECMO) have been used by clinicians to treat severe leptospirosis, particularly when accompanied by pulmonary haemorrhage, however the benefits of these interventions have only been reported in small case series [5,18,19,20]. The role of inhaled or parenteral tranexamic acid for individuals with pulmonary haemorrhage is also incompletely defined [21].
Far North Queensland (FNQ), in tropical Australia, has the highest incidence of leptospirosis in the country [22,23]. Prompt access to sophisticated multidisciplinary care in the well-resourced Australian health system means that deaths from leptospirosis are very rare, even in patients with multi-organ failure requiring ICU care [14,24]. FNQ clinicians recognise that individuals with leptospirosis that is complicated by lung involvement are at greatest risk of death, but what are the characteristics of these patients and what is their optimal management? This study, performed in a high-volume centre where leptospirosis has a very low case-fatality rate, examined the demographic, clinical, laboratory and imaging findings of individuals with – and without – lung involvement. It was hoped that these data, might inform the management strategies of clinicians, less familiar with leptospirosis, who encounter individuals with this potentially life-threatening disease.
2. Materials and Methods
This retrospective cohort study was conducted at Cairns Hospital, the 770-bed referral hospital for the FNQ region. The hospital serves a population of approximately 290,000 who live across an area of approximately 380,000 km2 (Figure S1). FNQ has a hot, tropical climate; most local cases of leptospirosis occur in the December-April wet season when the average monthly rainfall can exceed 400 millimetres [25,26].
This is a substudy of a previously published report which examined all adults and children admitted to Cairns Hospital with a confirmed diagnosis of leptospirosis between January 1, 2015, and June 30, 2024 [24]. This study period was chosen as it coincided with the local introduction of an electronic medical record (EMR). Individuals were eligible for inclusion in the study if they satisfied the Australian definition of laboratory confirmed leptospirosis (Table S1) [27]. Culture of Leptospira from whole-blood, with subsequent serovar identification if isolated, polymerase chain reaction (PCR targeting outer membrane protein LipL32) testing and serology (Microscopic Agglutination Test; MAT) were performed at Australia’s Leptospirosis Reference Laboratory in Brisbane, 1390 km away from Cairns Hospital [28]. If individuals had no chest imaging performed during their hospitalisation they were not included in this study.
The patients’ EMRs were examined to collect demographic data and to identify any comorbidities (Table S2). The patients’ symptoms and clinical signs that were documented at their presentation to Cairns Hospital were also recorded. Laboratory data were collected from the Queensland statewide electronic database AUSLAB; these data included the values at presentation (either at the regional referring hospital or at Cairns Hospital) and the highest or, where relevant, lowest values during the patient’s hospitalisation. Specialist radiologist reporting of any imaging was also collated from the health system’s electronic database.
Individuals were said to have lung involvement if they had any new lung parenchymal changes on this chest imaging. Pulmonary haemorrhage was defined as present if there was documented frank haemoptysis or if frank blood was present on tracheal aspirate. ARDS was classified using the Berlin definition based on the partial pressure of arterial oxygen: fraction of inspired oxygen (PaO2/FiO2) ratio where this was available [29]. As many individuals did not have an arterial blood gas collected during their hospitalisation the pulse oximetry oxygen saturation: fraction of inspired oxygen ratio (SpO2/FiO2) was also calculated [30]. Oliguria was defined as a documented urine output of less than 0.5 mL/kg/hour.
The duration of symptoms prior to antibiotic therapy was noted. If patients developed pulmonary haemorrhage, required ICU admission, needed vasopressor support, required intubation and mechanical ventilation, needed renal replacement therapy (RRT) or required transfer to a quaternary centre for more specialised care, this was recorded. The administration of corticosteroids was documented, as was the agent that was chosen and the duration of this therapy. The total hospital length of stay and the length of stay in the ICU, where relevant, were recorded. All-cause 90-day mortality was documented.
Statistical Analysis
Data were de-identified and entered into a centralised electronic database (Microsoft Excel) and analysed using statistical software (Stata version 18). As many of the continuous variables had a non-parametric distribution they are presented as the median and interquartile range (IQR). Groups were analysed using the Wilcoxon rank-sum test, the chi-squared test, Fisher’s exact test or logistic regression, where appropriate. If individuals were missing data, they were not included in analyses which evaluated those variables.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki and approved by the Far North Queensland Human Research Ethics Committee (HREC/EX/2024/QCH/108994) on the 2 August 2024. As the retrospective data were de-identified and presented in an aggregated manner, the Committee waived the requirement for informed consent.
3. Results
There was a total of 111 individuals with laboratory-confirmed leptospirosis admitted to Cairns Hospital during the study period; two individuals had no chest imaging performed during their hospitalisation, leaving 109 individuals who were included in this analysis. Their median age was 39 (IQR: 24-56) years, and 93/109 (85%) were male. Most (65/109, 60%) presented during the wet season; 83/109 (76%) were transferred to Cairns Hospital from a smaller regional health facility for escalation of care.
Leptospirosis PCR was performed on blood in 98/109 (89%) patients and was positive (lipL32 target detected) in 88/98 (90%); whole-blood culture for leptospirosis was performed in 47/109 (44%) and was positive in 29/47 (62%). Overall, PCR of blood or whole-blood culture was positive in 92/101 (91%) who had either of these tests performed. Acute serology testing by MAT was performed in 102/109 (94%) and was reactive in 44/102 (43%). Convalescent serology was collected and tested by MAT in 50/109 (46%). Convalescent serology was frequently performed to infer the infecting serovar, but it established the diagnosis of leptospirosis in 11/50 (22%). It was possible to infer the serovar in 62 individuals; Leptospira interrogans serovar Zanoni (24/62, 39%) and L. interrogans serovar Australis were the most common (12/62, 19%) (Tables S3 and S4). Other elements of the presentation, diagnosis, care and clinical course of the cohort have been reported previously [24].
3.1. Lung Involvement
Overall, 62/109 (57%) had lung involvement; there was no difference in the demographic characteristics or the comorbidities of patients who had lung involvement and those who did not (Table 1). Notably, lung involvement was neither more common in individuals with chronic lung disease nor in those who were current smokers. Individuals with lung involvement had a longer duration of symptoms prior to the commencement of antibiotic therapy than individuals without lung involvement.
Among the 62 individuals with lung involvement, 27 (44%) had respiratory symptoms at presentation: 23 (37%) had a cough, 12 (19%) had haemoptysis and 11 (18%) complained of dyspnoea; 34/62 (54%) had abnormal chest auscultation at presentation (Table 2). On initial laboratory testing, individuals with lung involvement had greater renal impairment, a higher C-reactive protein and were more likely to have an abnormal troponin than individuals without lung involvement (Tables S5 and S6). Individuals with lung involvement usually had a positive blood PCR or positive blood cultures; this included all 41 individuals with lung involvement who required ICU admission. Individuals with lung involvement were more likely to have infection with L. interrogans serovar Zanoni than individuals without lung involvement (Table 1).
The acute parenchymal changes on chest imaging that defined lung involvement were present on initial imaging in 36/62 (58%) and were present on subsequent imaging in another 26 (Table 3). These changes were often multilobar and opacities were frequently alveolar. The presence of multilobar or alveolar changes were associated with a more complicated disease course (Table 3). Nodular parenchymal changes were often present in the most critically ill patients (Figure 1 and Figure 2).
Panels A-C. CXR imaging of an otherwise healthy 24-year-old female who presented with a 3-day history of fevers, but no respiratory symptoms and a normal chest x-ray (Panel A – day 1). She was commenced on ceftriaxone and azithromycin but remained febrile. A repeat CXR (Panel B – day 2) shows blunting of the left costophrenic angle without any focal parenchymal abnormality, but she developed dyspnoea and an oxygen requirement over the subsequent 48 hours. Panel C (day 5) demonstrates the associated widespread patchy alveolar changes. With supportive care, she avoided an ICU admission, made a full recovery and was discharged after a 7-day hospitalisation.
Panels D-F. CXR imaging of an otherwise healthy 37-year-old male reporting a four-day history of cough, fevers and general malaise. At presentation he had type I respiratory failure and required intubation in the Emergency Department before transfer to ICU. A CXR (Panel D – day 1) performed on arrival to Cairns Hospital revealed widespread bilateral patchy airspace consolidation. On day 2 of his admission, blood stained sputum was reported and a repeat CXR (Panel E) showed significant deterioration with diffuse airspace opacities consistent with pulmonary haemorrhage. Refractory hypoxia necessitated commencement of ECMO which he received for 20 days. Panel F, 26 days after his presentation, shows nearly complete resolution of the lung changes. He was discharged after a total of 8 weeks in hospital
CT chest images (A: axial and B: coronal) of an otherwise healthy 30-year-old male who presented with 4 days of generalised malaise, fevers and haematuria. On presentation he was haemodynamically stable and had no respiratory symptoms; however, within 8 hours he deteriorated requiring vasopressor support and supplemental oxygen. Images shortly after deterioration demonstrate diffuse alveolar opacities, ground glass opacities and centrilobular nodules. The patient was admitted to ICU where he required intubation and mechanical ventilation. He made a full recovery and was discharged after a 20-day hospitalisation.
CT chest images (C: axial and D: coronal) of an otherwise healthy 37-year-old male who presented with a 3-day history of cough, fevers and dyspnoea. He was tachypnoeic at presentation but had a clear chest on auscultation, normal oxygen saturation on room air by pulse oximetry and a normal chest x-ray. Within 3 hours of presentation the patient developed worsening respiratory distress and an oxygen requirement. At this time, the CT chest revealed extensive ground glass opacities with relative sparing of the lung bases, suggestive of diffuse pulmonary haemorrhage. He required an 8-day ICU admission for vasopressor support but did not require intubation. He made a full recovery and was discharged from hospital after an 11-day admission.
3.2. Pulmonary Haemorrhage
Pulmonary haemorrhage was diagnosed in 26/109 (24%). Individuals with pulmonary haemorrhage were more likely to be current smokers than individuals without pulmonary haemorrhage (14/26 (54%) versus 26/83 (31%), p=0.04). There were no other demographic or clinical associations with the development of pulmonary haemorrhage. In particular, there was no association with the development of pulmonary haemorrhage and the presence of underlying lung disease or the infecting serovar. The median (IQR) duration of symptoms prior to the initiation of antibiotic therapy in the individuals who developed pulmonary haemorrhage was 5 (4-6) days versus 4 (3-5) days in the individuals who did not develop pulmonary haemorrhage, but this difference did not reach statistical significance (p=0.10) (Table S7).
Among the 26 individuals with pulmonary haemorrhage, 16 (62%) had respiratory symptoms at presentation: 14 (54%) had a cough, 12 (46%) had haemoptysis and 8 (31%) complained of dyspnoea; 18 (69%) had abnormal chest auscultation at presentation. Individuals with pulmonary haemorrhage had lower SpO2/FiO2 ratios at presentation and were more likely to have oliguria and require vasopressor support than patients who did not have pulmonary haemorrhage. The other clinical and laboratory findings in the individuals who developed pulmonary haemorrhage are presented in Tables S8, S9 and S10. At presentation, individuals who developed pulmonary haemorrhage had greater renal impairment, a higher C-reactive protein and were more likely to have an abnormal troponin than individuals without lung involvement; 24/25 (96%) individuals with pulmonary haemorrhage who had PCR testing of blood were PCR positive and 7/15 (50%) who had blood cultures collected had a positive culture.
3.4. Clinical Course and Therapy
It was not possible to confirm the diagnosis of leptospirosis for several days and prior to this, patients tended to receive standard ward-based management guided by the patients’ physiological parameters. This care included antibiotic therapy, cautious crystalloid fluid therapy, and prompt initiation of additional supportive care – including vasopressors, RRT mechanical ventilation and ECMO – as necessary, using standard indications [31].
Individuals with lung involvement frequently had multi-organ dysfunction and were more likely to require ICU admission than individuals without lung involvement (41/62 (66%) versus 15/47 (32%), odds ratio (95% confidence interval): 4.17 (1.86-9.34), p<0.001) (Figure 3 and Table 4). Arterial blood gas analysis was performed in 41/62 (50%) individuals with lung involvement; the median (IQR) nadir PaO2/FiO2 ratio was 236 (151-303); 30/62 (48%) satisfied the Berlin criteria for ARDS: 12/30 (40%) had mild, 15/30 (50%) had moderate, and 3/30 (10%) had severe ARDS. Intubation and mechanical ventilation were necessary in 15/62 (24%); all 15 of these individuals had lung involvement. The demographic, clinical and laboratory indices in individuals requiring mechanical ventilation are presented in Tables S11, S12 and S13.
There were 10/62 (16%) who received vasopressor support, RRT and mechanical ventilation; 5/62 (8%) who received vasopressor support and mechanical ventilation; 3/62 (5%) who received vasopressor support and RRT; 23/62 (37%) who received only vasopressor support and 2/62 (3%) who received only RRT. There were 19/62 (31%) individuals with lung involvement who did not receive vasopressor support, RRT or mechanical ventilation.
Of the 109 patients, 107 (98%) received antibiotic therapy at some point in their hospitalisation. One patient (a patient with lung involvement) had a Jarisch-Herxheimer reaction, but this was managed successfully with simple supportive measures. A range of antibiotics were prescribed for a variety of durations, but doxycycline (81/109 (74%)) and ceftriaxone (74/109 (68%)) were the agents prescribed most commonly. The two individuals who did not receive antibiotics were children (aged 7 and 11 respectively) who had the diagnosis of leptospirosis confirmed after the resolution of symptoms; neither had lung involvement.
Corticosteroids were prescribed in 19/109 (17%) and were prescribed more often in individuals with lung involvement (16/62 (26%) versus 3/47 (6%), p=0.01). However, this corticosteroid therapy was usually intravenous hydrocortisone (typically at a dose of 50mg four times a day) in the setting of refractory hypotension in individuals requiring vasopressor support; all 19 patients who received steroids received vasopressor support. Two individuals received high dose pulse methylprednisolone for severe pneumonitis, while one patient received dexamethasone in the setting of concurrent severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. The median (IQR) duration of steroid therapy was 2 (1-4) days.
Two patients with refractory respiratory failure required evacuation to a quaternary centre to receive ECMO; 1 of these individuals also received intravenous tranexamic acid and nebulised adrenaline. Inhaled tranexamic acid was prescribed to 3 of the other 25 individuals with pulmonary haemorrhage. No patients received plasma exchange or plasmapheresis. All patients in the cohort were alive 90 days after presentation.
4. Discussion
The lungs are commonly affected in patients hospitalised with leptospirosis in tropical Australia, with radiological evidence of lung involvement identified in more than half of the patients in this cohort. This lung involvement is life-threatening: almost half of the patients with lung involvement satisfied criteria for ARDS and over 40% had pulmonary haemorrhage. Almost two-thirds of the patients with lung involvement required ICU admission, although importantly, lung involvement was commonly just one element of multi-organ dysfunction in these patients.
However, although leptospirosis was considered in the initial differential diagnosis of approximately 60% of the patients with lung involvement, the diagnosis could only be confirmed several days into the admission. Prior to this, patients tended to receive standard sepsis management which included antibiotic therapy, cautious fluid resuscitation with crystalloid, vasopressors (with low-dose corticosteroids as necessary) to maintain blood pressure and prompt initiation of additional supportive care – including mechanical ventilation, RRT and ECMO – guided by the patients’ physiological parameters and clinical trajectory [31]. Fortunately, with access to care in Australia’s well-resourced health system, every patient in the cohort – including the 57% with confirmed lung involvement – was alive 90 days after presentation.
Over 95% of the patients with lung involvement had no history of chronic lung disease. Indeed, over 40% of the patients with lung involvement were aged younger than 40 and had no comorbidity, highlighting the pathogen’s ability to cause life-threatening disease in otherwise well young people. The minority of patients with lung involvement during their illness had respiratory symptoms at presentation, only 55% had an abnormal respiratory examination and only 58% had abnormal chest imaging, emphasising the importance of frequent clinical reassessment and a low threshold for repeat chest imaging in patients in whom leptospirosis is suspected, as clinical deterioration can be rapid [32].
The imaging findings in our cohort were similar to those identified in other series; multilobar and alveolar changes, in particular, were common and were associated with a more complicated disease course [33,34,35]. These radiological appearances would correlate with the histological findings of alveolar oedema and haemorrhage that are seen commonly in patients with fatal leptospirosis [36,37,38,39]. The precise pathophysiology of lung involvement in patients with leptospirosis remains incompletely understood, but human autopsy studies have demonstrated leptospiral antigen within endothelial cells of the interalveolar septa and attached to capillary endothelial cells, supporting the hypothesis that the organism exerts a locally destructive action on lung capillaries, leading to loss of vascular integrity and the alveolar oedema and haemorrhage which is seen in severe disease [32,37,38,40].
These clinicopathological correlation studies provide support for the management strategies employed in the patients with lung involvement in our cohort. Antibiotic therapy was prescribed to all but two individuals, both children without lung involvement. Some authors have expressed doubts about the incremental value of antibiotic therapy in patients with leptospirosis presenting later in their disease course and a Cochrane review – which emphasised that few quality studies have examined the issue – found little evidence to suggest benefit of antibiotic therapy in patients with the infection [5,12]. However, although patients with lung involvement in this cohort presented after a median of 5 days of symptoms, leptospiraemia was documented in 95% of those who had blood PCR performed or blood cultures collected (and in every patient with lung involvement who required ICU care). Indeed, the development of lung involvement was associated with delays in the administration of antibiotic therapy, echoing findings from other series and providing data to support the utility of antibiotic therapy in these patients [41,42].
In addition to the human autopsy studies demonstrating alveolar oedema – hypothesised to result from direct vascular injury – animal models of leptospirosis have documented decreased epithelial sodium channel (H-ENaC) protein expression and upregulation of the Na-K-2Cl cotransporter NKCC1 in the lungs which further impairs pulmonary fluid handling [36,37,38,43]. Although hypotension and AKI were common in the cohort, concerns about precipitating or exacerbating pulmonary oedema meant that fluid resuscitation was generally conservative in these patients, even before changes were apparent on chest imaging. Large fluid boluses were avoided in patients with hypotension or AKI who were instead managed using standard sepsis algorithms that included prompt vasopressor support to maintain a mean arterial pressure and, where necessary, RRT [31].
Pulmonary haemorrhage is the most common cause of death in patients with leptospirosis and even in ICUs with access to ECMO mortality can exceed 30% [19,38,39,44,45,46]. Pulmonary haemorrhage was identified in 26 individuals in our cohort and although this necessitated ECMO in two cases – and three others received tranexamic acid – the patients’ management was generally supportive and expectant, and outcomes were excellent. Although plasmapheresis is available locally, no patient had plasmapheresis or plasma exchange. There has been uncertainty about the contribution of disseminated intravascular coagulation (DIC) to the development of pulmonary haemorrhage, however while patients with pulmonary haemorrhage had a lower nadir platelet count than patients without pulmonary haemorrhage, their coagulation studies did not suggest the presence of DIC [47]. It was notable that pulmonary haemorrhage was more common in current cigarette smokers, echoing findings from a New Caledonian series [42]. The explanation for this possible association is uncertain although it is plausible that smoking could lead to damage to the alveolar basement membrane, increasing the risk of haemorrhage [48,49]. The fact that over a third of the cohort were current cigarette smokers – compared to a current rate of 8.3% in Australians aged 14 or older – may have contributed to the high incidence of pulmonary haemorrhage in our study [50].
Many authors have suggested that a dysregulated and intense immune response plays an important role in the pathogenesis of severe disease [5,51,52]. This is the basis for the high dose corticosteroid therapy that has been proposed by some authors, particularly for patients with lung involvement [53]. However, while infiltration of alveolar spaces by monocytes and neutrophils occurs, inflammatory infiltrates are generally not prominent [37,38,39,54]. Although almost 85% of the patients in our cohort with lung involvement received corticosteroids, this was usually modestly dosed hydrocortisone that was prescribed for less than 72 hours in the setting of hypotension requiring vasopressor support, rather than the high dose bolus methylprednisolone for three days (followed by oral corticosteroids for five-seven days) that has been used in some series [16,53]. The encouraging outcomes seen in our cohort suggest that higher dose corticosteroid therapy should not be considered as a routine intervention in patients with lung involvement, particularly given the risk of nosocomial infection, until definitive data from adequately powered randomised controlled trials is available to support this approach [55,56].
It is important to highlight that even in Australia’s well-resourced health system where there is access to a World Health Organization Collaborating Centre for Leptospirosis, the diagnosis of leptospirosis in our cohort was frequently not confirmed for 5-7 days, and in some cases it was a retrospective diagnosis [28]. The clinical and laboratory findings in patients with leptospirosis, while frequently suggestive, are often non-specific and it can be difficult to distinguish patients with leptospirosis from patients with other life-threatening infections and, indeed, non-communicable diseases [31,47,57,58,59]. Therefore, it is important not to institute specific interventions for the management of leptospirosis that fails to consider these other diagnoses or contains elements that may – either by omission or commission – increase the risk of deterioration. In this context the pragmatic clinician can be reassured that many elements of the care received by the patients with laboratory-confirmed leptospirosis in this cohort would be equally appropriate in patients with the other infectious diseases that may mimic it. These include early antibiotic therapy [31,60,61], a conservative approach to fluid resuscitation [62,63,64,65], cautious use of corticosteroids [66,67], and the early delivery of context dependent critical care support [31,68,69].
Although this study was able to examine the demographic, clinical, laboratory and radiological findings of patients with lung involvement complicating laboratory-confirmed leptospirosis in some detail, it has several limitations. The study’s retrospective nature meant that patients’ clinical assessment, investigations and management were not standardised. They occurred at different stages in the evolution of the disease and the reporting of comorbidities and clinical findings, relied on accurate documentation in the medical record. The study examined only patients managed in a referral hospital and therefore included patients with a more severe clinical phenotype, overestimating the incidence of severe disease. The definition of lung involvement, while pragmatic, is imperfect. Although we used the imaging reports of a specialist radiologist, a plain chest x-ray may not identify early parenchymal changes and lung imaging was performed only once in a third of the cohort, which will tend to underestimate the incidence of lung involvement [35]. The categorical definition of lung involvement lacked nuance; there is clearly a significant clinical difference between subtle, asymptomatic chest x-ray changes and multilobar alveolar changes causing respiratory failure. The definition of pulmonary haemorrhage was equally crude and required adequate documentation in the medical record. There is some geographical variation in the clinical presentation of leptospirosis which some clinicians might suggest limits the applicability of our observations to other settings [70,71,72]. Infection with serovars from the Icterohemorrhagiae serogroup has been reported to be associated with lung involvement and pulmonary haemorrhage [32,72,73,74]. However, it was notable that serovars from the Pyrogenes serogroup (Zanoni and Robinsoni) and Australis serogroup (Australis), the most common serovars in the region, were also the most commonly identified serovars in patients with lung involvement and pulmonary haemorrhage in this cohort. These data support the contention that there may be limited correlation between particular serovars and the severity and clinical manifestations of leptospirosis [51,75,76].
It is important to highlight that the patients in our cohort were managed in Australia’s well-resourced, universal health system which limits the generalisability of some of our recommendations, particularly to the resource-limited settings where, globally, most cases of leptospirosis are seen [1]. That said, we would argue that the clinical approach and management strategies which include prompt antibiotic therapy, conservative fluid resuscitation, efforts to exclude alternative diagnoses and the provision of additional supportive care – where this is available – are likely to be equally relevant in these locations [31,69]. Although we have presented the general approach to the management of patients with leptospirosis in the FNQ region, detailed quantitative data describing the different interventions (including precise volumes of fluid, ventilation strategies, blood product support and the indications for mechanical ventilation, RRT and ECMO) have not been presented. They will be the focus of a manuscript that is in preparation. Separate reports will also examine the manifestations of leptospirosis in other organ systems in patients in the FNQ region.
5. Conclusions
Life-threatening lung involvement can complicate leptospirosis in young and otherwise well individuals. However, in Australia’s well-resourced health system excellent outcomes can be achieved using a standard contemporary approach to patient management while a confirmed diagnosis is awaited.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure: S1. Map of Far North Queensland, Australia, showing catchment area for the current study. Table: S1. Australian definition of laboratory confirmed leptospirosis. Table: S2. Definitions used for comorbidities in the cohort. Table: S3. Serovars in the Leptospira microscopic agglutination titre panel used at the Leptospirosis Reference Laboratory in Brisbane, Queensland. Table: S4. The patients in whom a serovar was identified and the association with lung involvement, pulmonary haemorrhage or a requirement of intubation and mechanical ventilation (Serovars listed in bold were culture positive). Table: S5. Haematological indices of individuals admitted to a referral hospital with leptospirosis in Far North Queensland, January 2015–June 2024, and the association of these factors with the development of lung involvement. Table: S6. Biochemical indices of individuals admitted to a referral hospital with leptospirosis in Far North Queensland, January 2015–June 2024, and the association of these factors with the development of lung involvement. Table: S7. The demographics and comorbidities of individuals admitted to a referral hospital with leptospirosis in Far North Queensland, January 2015–June 2024, and the association of these factors with the development of the development of pulmonary haemorrhage. Table: S8. The symptoms and signs at presentation of individuals admitted to a referral hospital with leptospirosis in Far North Queensland, January 2015–June 2024, and the association of these factors with the development of pulmonary haemorrhage. Table: S9. Haematological indices of individuals admitted to a referral hospital with leptospirosis in Far North Queensland, January 2015–June 2024, and the association of these factors with the development of pulmonary haemorrhage. Table: S10. Biochemical indices of individuals admitted to a referral hospital with leptospirosis in Far North Queensland, January 2015–June 2024, and the association of these factors with the development of pulmonary haemorrhage. Table: S11. The symptoms and signs at presentation of individuals admitted to a referral hospital with leptospirosis in Far North Queensland, January 2015–June 2024, and the association of these factors with the requirement for intubation and mechanical ventilation. Table: S12. Haematological indices of individuals admitted to a referral hospital with leptospirosis in Far North Queensland, January 2015–June 2024, and the association of these factors with the requirement for intubation and mechanical ventilation. Table: S13. Biochemical indices of individuals admitted to a referral hospital with leptospirosis in Far North Queensland, January 2015–June 2024, and the association of these factors with the requirement for intubation and mechanical ventilation.
Author Contributions
Methodology, A.S., S.S., H.S, and J.H.; Validation, J.H.; Formal analysis, A.S. and J.H.; Investigation, A.S., H.S. and J.H.; Data curation, A.S., H.S., M.S., P.R. and J.H; Writing —original draft, A.S. and J.H.; Writing — review & editing, A.S., S.S., M.S., A.B., S.V. and J.H.; Visualization, S.S. and J.H.; Supervision, S.S., S.V, and J.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Far North Queensland Human Research Ethics Committee (HREC/EX/2024/QCH/108994) on the 2 August 2024.
Informed Consent Statement
As the retrospective data were de-identified and presented in an aggregated manner, the Committee waived the requirement for informed consent.
Data Availability Statement
Data cannot be shared publicly because of the Queensland Public Health Act 2005. Data are available from the Far North Queensland Human Research Ethics Committee (contact via email: FNQ_HREC@health.qld.gov.au) for researchers who meet the criteria for access to confidential data.
Acknowledgments
The authors would like to thank all the clinicians and scientists involved in the care of the patients.
Conflicts of Interest
J.H is a member of the Editorial Board of Tropical Medicine and Infectious Diseases. The other authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AKI | Acute kidney injury |
| ARDS | Acute respiratory distress syndrome |
| DIC | Disseminated intravascular coagulation |
| ECMO | Extracorporeal membranous oxygenation |
| ICU | Intensive care unit |
| IQR | Interquartile range |
| RRT | Renal replacement therapy |
References
- Costa F, Hagan JE, Calcagno J, Kane M, Torgerson P, Martinez-Silveira MS, et al. Global Morbidity and Mortality of Leptospirosis: A Systematic Review. PLoS Negl Trop Dis. 2015;9(9):e0003898. [CrossRef]
- Chawla V, Trivedi TH, Yeolekar ME. Epidemic of leptospirosis: an ICU experience. J Assoc Physicians India. 2004;52:619-22.
- Muñoz-Zanzi C, Dreyfus A, Limothai U, Foley W, Srisawat N, Picardeau M, et al. Leptospirosis—Improving Healthcare Outcomes for a Neglected Tropical Disease. Open Forum Infectious Diseases. 2025;12(2). [CrossRef]
- Cagliero J, Villanueva S, Matsui M. Leptospirosis Pathophysiology: Into the Storm of Cytokines. Front Cell Infect Microbiol. 2018;8:204. [CrossRef]
- Rajapakse S, Fernando N, Dreyfus A, Smith C, Rodrigo C. Leptospirosis. Nat Rev Dis Primers. 2025;11(1):32. [CrossRef]
- Samrot AV, Sean TC, Bhavya KS, Sahithya CS, Chan-drasekaran S, Palanisamy R, et al. Leptospiral Infection, Pathogenesis and Its Diagnosis—A Review. Pathogens. 2021;10(2):145. [CrossRef]
- Evangelista KV, Coburn J. Leptospira as an emerging pathogen: a review of its biology, pathogenesis and host immune responses. Future Microbiol. 2010;5(9):1413-25. [CrossRef]
- Budiono E, Sumardi, Riyanto BS, Hisyam B, Hartopo AB. Pulmonary involvement predicts mortality in severe leptospirosis patients. Acta Med Indones. 2009;41(1):11-4.
- Spichler AS, Vilaça PJ, Athanazio DA, Albuquerque JO, Buzzar M, Castro B, et al. Predictors of lethality in severe leptospirosis in urban Brazil. Am J Trop Med Hyg. 2008;79(6):911-4.
- Rajapakse S, Rodrigo C, Haniffa R. Developing a clinically relevant classification to predict mortality in severe leptospirosis. J Emerg Trauma Shock. 2010;3(3):213-9. [CrossRef]
- So RAY, Danguilan RA, Chua E, Arakama MI, Ginete-Garcia JKB, Chavez JR. A Scoring Tool to Predict Pulmonary Complications in Severe Leptospirosis with Kidney Failure. Trop Med Infect Dis. 2022;7(1). [CrossRef]
- Win TZ, Han SM, Edwards T, Maung HT, Brett-Major DM, Smith C, et al. Antibiotics for treatment of leptospirosis. Cochrane Database Syst Rev. 2024;3(3):CD014960. [CrossRef]
- Wiedemann HP, Wheeler AP, Bernard GR, Thompson BT, Hayden D, deBoisblanc B, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med. 2006;354(24):2564-75. [CrossRef]
- Smith S, Liu YH, Carter A, Kennedy BJ, Dermedgoglou A, Poulgrain SS, et al. Severe leptospirosis in tropical Australia: Optimising intensive care unit management to reduce mortality. PLoS Negl Trop Dis. 2019;13(12):e0007929. [CrossRef]
- Karnik ND, Patankar AS. Leptospirosis in Intensive Care Unit. Indian J Crit Care Med. 2021;25(Suppl 2):S134-s7. [CrossRef]
- Kularatne SA, Budagoda BD, de Alwis VK, Wickramasinghe WM, Bandara JM, Pathirage LP, et al. High efficacy of bolus methylprednisolone in severe leptospirosis: a descriptive study in Sri Lanka. Postgrad Med J. 2011;87(1023):13-7. [CrossRef]
- Rodrigo C, Lakshitha de Silva N, Goonaratne R, Samarasekara K, Wijesinghe I, Parththipan B, et al. High dose corticosteroids in severe leptospirosis: a systematic review. Trans R Soc Trop Med Hyg. 2014;108(12):743-50. [CrossRef]
- Trivedi SV, Vasava AH, Bhatia LC, Patel TC, Patel NK, Patel NT. Plasma exchange with immunosuppression in pulmonary alveolar haemorrhage due to leptospirosis. Indian J Med Res. 2010;131:429-33.
- Fonseka CL, Dahanayake NJ, Mihiran DJD, Wijesinghe KM, Liyanage LN, Wickramasuriya HS, et al. Pulmonary haemorrhage as a frequent cause of death among patients with severe complicated Leptospirosis in Southern Sri Lanka. PLoS Negl Trop Dis. 2023;17(10):e0011352. [CrossRef]
- Milovanovic L, Singh G, Townsend D, Nagendran J, Sligl W. Extracorporeal Life Support for Severe Leptospirosis: Case Series and Narrative Review. J Assoc Med Microbiol Infect Dis Can. 2024;9(3):173-82. [CrossRef]
- Zhang P, Zheng J, Shan X, Zhou B. Advances in the study of nebulized tranexamic acid for pulmonary hemorrhage. Eur J Clin Pharmacol. 2025;81(2):237-46. [CrossRef]
- National Notifiable Disease Surveillance System Canberra: Australian Government. Department of Health Disability and Aging; 2025 [Available from: https://nindss.health.gov.au/pbi-dashboard/.
- Smith S, Kennedy BJ, Dermedgoglou A, Poulgrain SS, Paavola MP, Minto TL, et al. A simple score to predict severe leptospirosis. PLoS Negl Trop Dis. 2019;13(2):e0007205. [CrossRef]
- Stratton H, Rosengren P, Kinneally T, Prideaux L, Smith S, Hanson J. Presentation and Clinical Course of Leptospirosis in a Referral Hospital in Far North Queensland, Tropical Australia. Pathogens. 2025;14(7). [CrossRef]
- Fairhead LJ, Smith S, Sim BZ, Stewart AGA, Stewart JD, Binotto E, et al. The seasonality of infections in tropical Far North Queensland, Australia: A 21-year retrospective evaluation of the seasonal patterns of six endemic pathogens. PLOS Glob Public Health. 2022;2(5):e0000506. [CrossRef]
- Climate statistics for Australian locations. Summary statistics Cairns Aero.: Bureau of Meterology; 2025 [Available from: https://www.bom.gov.au/climate/averages/tables/cw_031011.shtml.
- Leptospirosis – Laboratory case definition Canberra: Public Health Laboratory Network; 2007 [Available from: https://www.health.gov.au/resources/publications/leptospirosis-laboratory-case-definition?language=en.
- Leptospirosis Reference Laboratory. Accreditations, certifications and terms of reference. Brisbane: Queensland Government; [Available from: https://www.health.qld.gov.au/public-health/forensic-and-scientific-services/testing-analysis/disease-investigation-and-analysis/leptospirosis-reference-laboratory/laboratory-accreditation-and-certification.
- Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, et al. Acute respiratory distress syndrome: the Berlin Definition. Jama. 2012;307(23):2526-33. [CrossRef]
- Rice TW, Wheeler AP, Bernard GR, Hayden DL, Schoenfeld DA, Ware LB. Comparison of the SpO2/FIO2 ratio and the PaO2/FIO2 ratio in patients with acute lung injury or ARDS. Chest. 2007;132(2):410-7. [CrossRef]
- Evans L, Rhodes A, Alhazzani W, Antonelli M, Coopersmith CM, French C, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181-247. [CrossRef]
- Silva JJ, Dalston MO, Carvalho JE, Setúbal S, Oliveira JM, Pereira MM. Clinicopathological and immunohistochemical features of the severe pulmonary form of leptospirosis. Rev Soc Bras Med Trop. 2002;35(4):395-9. [CrossRef]
- Matos ED, Costa E, Sacramento E, Caymmi AL, Neto CA, Barreto Lopes M, et al. Chest radiograph abnormalities in patients hospitalized with leptospirosis in the city of Salvador, Bahia, Brazil. Braz J Infect Dis. 2001;5(2):73-7. [CrossRef]
- Tanomkiat W, Poonsawat P. Pulmonary radiographic findings in 118 leptospirosis patients. Southeast Asian J Trop Med Public Health. 2005;36(5):1247-51.
- Marchiori E, Lourenço S, Setúbal S, Zanetti G, Gasparetto TD, Hochhegger B. Clinical and imaging manifestations of hemorrhagic pulmonary leptospirosis: a state-of-the-art review. Lung. 2011;189(1):1-9. [CrossRef]
- Dolhnikoff M, Mauad T, Bethlem EP, Carvalho CR. Pathology and pathophysiology of pulmonary manifestations in leptospirosis. Braz J Infect Dis. 2007;11(1):142-8. [CrossRef]
- Nicodemo AC, Duarte MI, Alves VA, Takakura CF, Santos RT, Nicodemo EL. Lung lesions in human leptospirosis: microscopic, immunohistochemical, and ultrastructural features related to thrombocytopenia. Am J Trop Med Hyg. 1997;56(2):181-7. [CrossRef]
- Arean VM. The pathologic anatomy and pathogenesis of fatal human leptospirosis (Weil's disease). Am J Pathol. 1962;40(4):393-423.
- Dolhnikoff M, Mauad T, Bethlem EP, Carvalho CR. Leptospiral pneumonias. Curr Opin Pulm Med. 2007;13(3):230-5. [CrossRef]
- Nicodemo AC, Duarte-Neto AN. Pathogenesis of Pulmonary Hemorrhagic Syndrome in Human Leptospirosis. Am J Trop Med Hyg. 2021;104(6):1970-2. [CrossRef]
- Thammakumpee K, Silpapojakul K, Borrirak B. Leptospirosis and its pulmonary complications. Respirology. 2005;10(5):656-9. [CrossRef]
- Tubiana S, Mikulski M, Becam J, Lacassin F, Lefèvre P, Gourinat AC, et al. Risk factors and predictors of severe leptospirosis in New Caledonia. PLoS Negl Trop Dis. 2013;7(1):e1991. [CrossRef]
- Andrade L, Rodrigues AC, Jr., Sanches TR, Souza RB, Seguro AC. Leptospirosis leads to dysregulation of sodium transporters in the kidney and lung. Am J Physiol Renal Physiol. 2007;292(2):F586-92. [CrossRef]
- Segura ER, Ganoza CA, Campos K, Ricaldi JN, Torres S, Silva H, et al. Clinical spectrum of pulmonary involvement in leptospirosis in a region of endemicity, with quantification of leptospiral burden. Clin Infect Dis. 2005;40(3):343-51. [CrossRef]
- Marotto PC, Nascimento CM, Eluf-Neto J, Marotto MS, Andrade L, Sztajnbok J, et al. Acute lung injury in leptospirosis: clinical and laboratory features, outcome, and factors associated with mortality. Clin Infect Dis. 1999;29(6):1561-3. [CrossRef]
- Gulati S, Gulati A. Pulmonary manifestations of leptospirosis. Lung India. 2012;29(4):347-53. [CrossRef]
- Haake DA, Levett PN. Leptospirosis in humans. Curr Top Microbiol Immunol. 2015;387:65-97. [CrossRef]
- Ioachimescu OC, Stoller JK. Diffuse alveolar hemorrhage: diagnosing it and finding the cause. Cleve Clin J Med. 2008;75(4):258, 60, 64-5 passim. [CrossRef]
- Donaghy M, Rees AJ. Cigarette smoking and lung haemorrhage in glomerulonephritis caused by autoantibodies to glomerular basement membrane. Lancet. 1983;2(8364):1390-3. [CrossRef]
- National Drug Strategy Household Survey 2022–2023. Canberra: Australian Institute of Health Welfare; 2025.
- Levett PN. Leptospirosis. Clin Microbiol Rev. 2001;14(2):296-326. [CrossRef]
- Abdulkader RC, Daher EF, Camargo ED, Spinosa C, da Silva MV. Leptospirosis severity may be associated with the intensity of humoral immune response. Rev Inst Med Trop Sao Paulo. 2002;44(2):79-83. [CrossRef]
- Shenoy VV, Nagar VS, Chowdhury AA, Bhalgat PS, Juvale NI. Pulmonary leptospirosis: an excellent response to bolus methylprednisolone. Postgrad Med J. 2006;82(971):602-6. [CrossRef]
- Luks AM, Lakshminarayanan S, Hirschmann JV. Leptospirosis presenting as diffuse alveolar hemorrhage: case report and literature review. Chest. 2003;123(2):639-43. [CrossRef]
- Niwattayakul K, Kaewtasi S, Chueasuwanchai S, Hoontrakul S, Chareonwat S, Suttinont C, et al. An open randomized controlled trial of desmopressin and pulse dexamethasone as adjunct therapy in patients with pulmonary involvement associated with severe leptospirosis. Clin Microbiol Infect. 2010;16(8):1207-12. [CrossRef]
- Petakh P, Oksenych V, Kamyshnyi O. Corticosteroid Treatment for Leptospirosis: A Systematic Review and Meta-Analysis. J Clin Med. 2024;13(15). [CrossRef]
- Bagshaw RJ, Stewart AGA, Smith S, Carter AW, Hanson J. The Characteristics and Clinical Course of Patients with Scrub Typhus and Queensland Tick Typhus Infection Requiring Intensive Care Unit Admission: A 23-year Case Series from Queensland, Tropical Australia. Am J Trop Med Hyg. 2020;103(6):2472-7. [CrossRef]
- Price C, Smith S, Stewart J, Hanson J. Acute Q Fever Patients Requiring Intensive Care Unit Support in Tropical Australia, 2015-2023. Emerg Infect Dis. 2025;31(2):332-5. [CrossRef]
- Izurieta R, Galwankar S, Clem A. Leptospirosis: The "mysterious" mimic. J Emerg Trauma Shock. 2008;1(1):21-33. [CrossRef]
- Dijkstra F, Riphagen-Dalhuisen J, Wijers N, Hak E, Van der Sande MA, Morroy G, et al. Antibiotic therapy for acute Q fever in The Netherlands in 2007 and 2008 and its relation to hospitalization. Epidemiol Infect. 2011;139(9):1332-41. [CrossRef]
- Biggs HM, Behravesh CB, Bradley KK, Dahlgren FS, Drexler NA, Dumler JS, et al. Diagnosis and Management of Tickborne Rickettsial Diseases: Rocky Mountain Spotted Fever and Other Spotted Fever Group Rickettsioses, Ehrlichioses, and Anaplasmosis - United States. MMWR Recomm Rep. 2016;65(2):1-44. [CrossRef]
- Gavey R, Stewart AGA, Bagshaw R, Smith S, Vincent S, Hanson J. Respiratory manifestations of rickettsial disease in tropical Australia; Clinical course and implications for patient management. Acta Trop. 2025;266:107631. [CrossRef]
- Hanson JP, Lam SW, Mohanty S, Alam S, Pattnaik R, Mahanta KC, et al. Fluid resuscitation of adults with severe falciparum malaria: effects on Acid-base status, renal function, and extravascular lung water. Crit Care Med. 2013;41(4):972-81. [CrossRef]
- Casey JD, Semler MW, Rice TW. Fluid Management in Acute Respiratory Distress Syndrome. Semin Respir Crit Care Med. 2019;40(1):57-65. [CrossRef]
- Naorungroj T, Prajantasen U, Sanla-Ead T, Viarasilpa T, Tongyoo S. Restrictive fluid management with early de-escalation versus usual care in critically ill patients (reduce trial): a feasibility randomized controlled trial. Crit Care. 2025;29(1):405. [CrossRef]
- Warrell DA, Looareesuwan S, Warrell MJ, Kasemsarn P, Intaraprasert R, Bunnag D, et al. Dexamethasone proves deleterious in cerebral malaria. A double-blind trial in 100 comatose patients. N Engl J Med. 1982;306(6):313-9. [CrossRef]
- Nedel WL, Nora DG, Salluh JI, Lisboa T, Póvoa P. Corticosteroids for severe influenza pneumonia: A critical appraisal. World J Crit Care Med. 2016;5(1):89-95. [CrossRef]
- Losonczy LI, Papali A, Kivlehan S, Calvello Hynes EJ, Calderon G, Laytin A, et al. White Paper on Early Critical Care Services in Low Resource Settings. Ann Glob Health. 2021;87(1):105. [CrossRef]
- Schultz MJ, Dunser MW, Dondorp AM, Adhikari NK, Iyer S, Kwizera A, et al. Current challenges in the management of sepsis in ICUs in resource-poor settings and suggestions for the future. Intensive Care Med. 2017;43(5):612-24. [CrossRef]
- Katz AR, Ansdell VE, Effler PV, Middleton CR, Sasaki DM. Assessment of the clinical presentation and treatment of 353 cases of laboratory-confirmed leptospirosis in Hawaii, 1974-1998. Clin Infect Dis. 2001;33(11):1834-41. [CrossRef]
- Berman SJ, Tsai CC, Holmes K, Fresh JW, Watten RH. Sporadic anicteric leptospirosis in South Vietnam. A study in 150 patients. Ann Intern Med. 1973;79(2):167-73. [CrossRef]
- Trevejo RT, Rigau-Pérez JG, Ashford DA, McClure EM, Jarquín-González C, Amador JJ, et al. Epidemic leptospirosis associated with pulmonary hemorrhage-Nicaragua, 1995. J Infect Dis. 1998;178(5):1457-63. [CrossRef]
- Seijo A, Coto H, San Juan J, Videla J, Deodato B, Cernigoi B, et al. Lethal leptospiral pulmonary hemorrhage: an emerging disease in Buenos Aires, Argentina. Emerg Infect Dis. 2002;8(9):1004-5. [CrossRef]
- Vijayachari P, Sugunan AP, Sharma S, Roy S, Natarajaseenivasan K, Sehgal SC. Leptospirosis in the Andaman Islands, India. Trans R Soc Trop Med Hyg. 2008;102(2):117-22. [CrossRef]
- Vinetz JM. Leptospirosis. Curr Opin Infect Dis. 2001;14(5):527-38. [CrossRef]
- Smythe L, Dohnt M, Norris M, Symonds M, Scott J. Review of leptospirosis notifications in Queensland 1985 to 1996. Commun Dis Intell. 1997;21(2):17-20. [CrossRef]
Figure 1.
Illustrative chest x-ray (CXR) findings in individuals admitted to a referral hospital with leptospirosis in Far North Queensland, January 2015–June 2024, who had lung involvement.
Figure 1.
Illustrative chest x-ray (CXR) findings in individuals admitted to a referral hospital with leptospirosis in Far North Queensland, January 2015–June 2024, who had lung involvement.
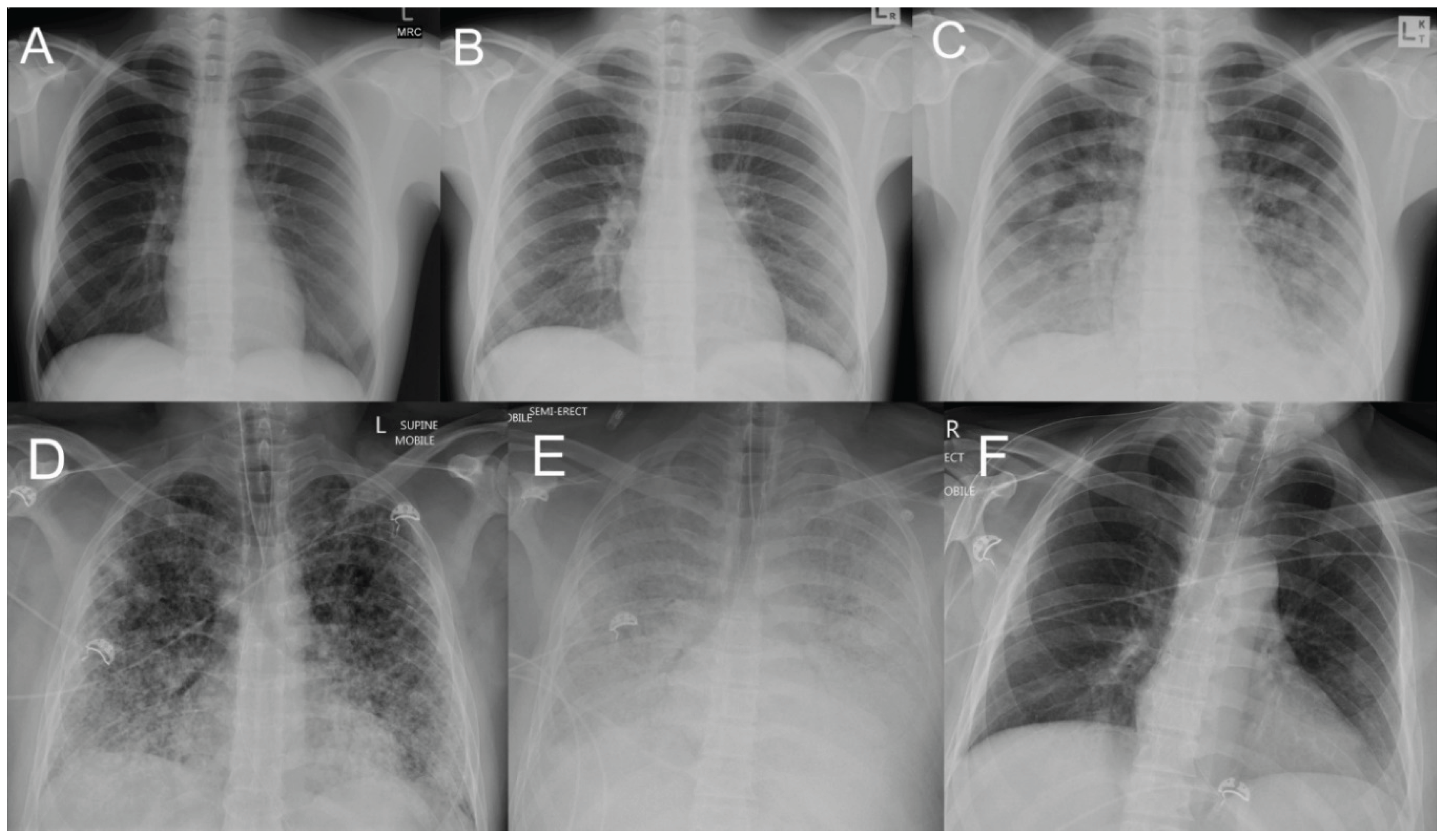
Figure 2.
Illustrative computed tomography (CT) findings in individuals admitted to a referral hospital with leptospirosis in Far North Queensland, January 2015–June 2024, who had lung involvement.
Figure 2.
Illustrative computed tomography (CT) findings in individuals admitted to a referral hospital with leptospirosis in Far North Queensland, January 2015–June 2024, who had lung involvement.
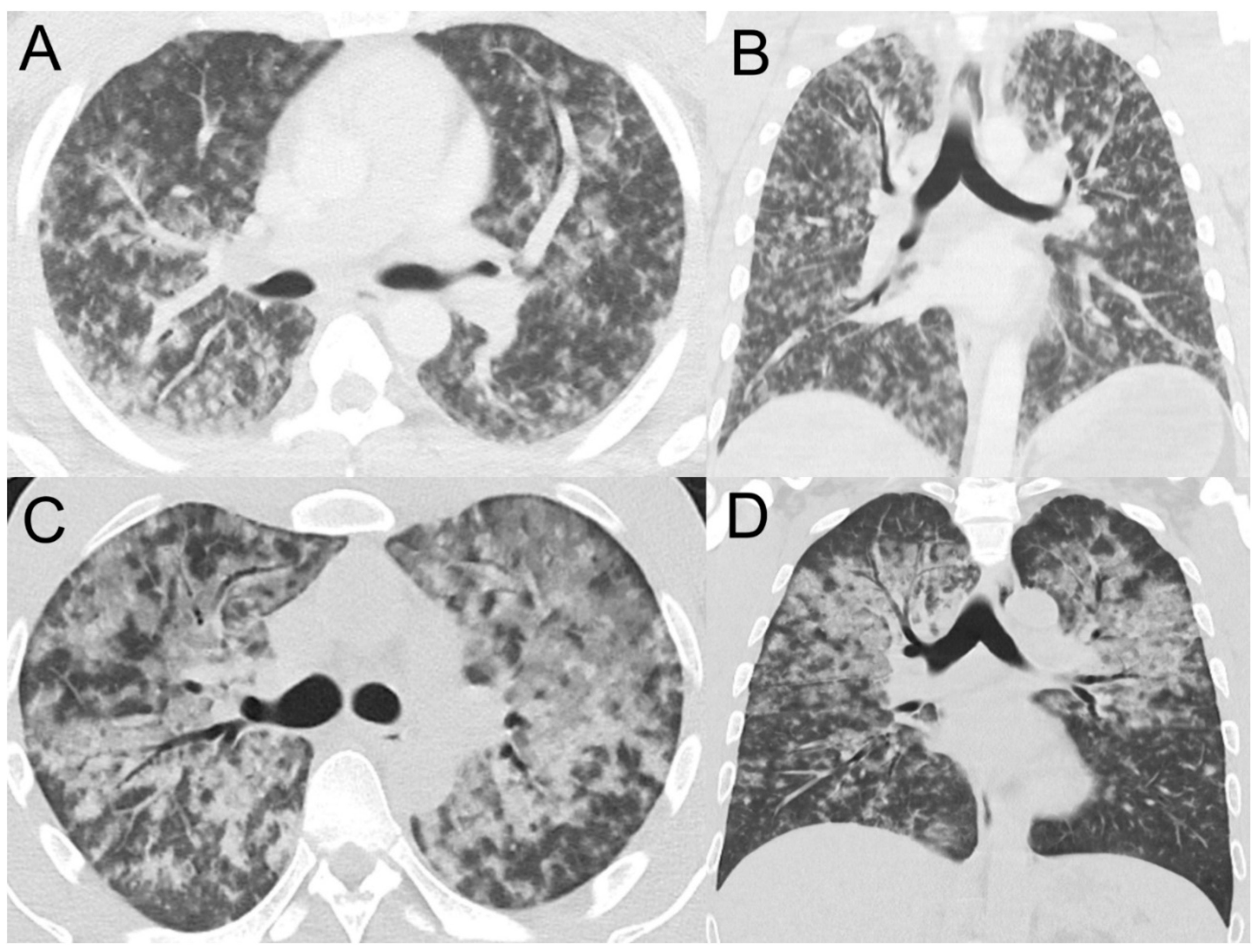
Figure 3.
Venn diagram demonstrating the supportive care provided to the patients with laboratory confirmed leptospirosis and lung involvement in a referral hospital in Far North Queensland, January 2015 to June 2024. RRT: renal replacement therapy.
Figure 3.
Venn diagram demonstrating the supportive care provided to the patients with laboratory confirmed leptospirosis and lung involvement in a referral hospital in Far North Queensland, January 2015 to June 2024. RRT: renal replacement therapy.
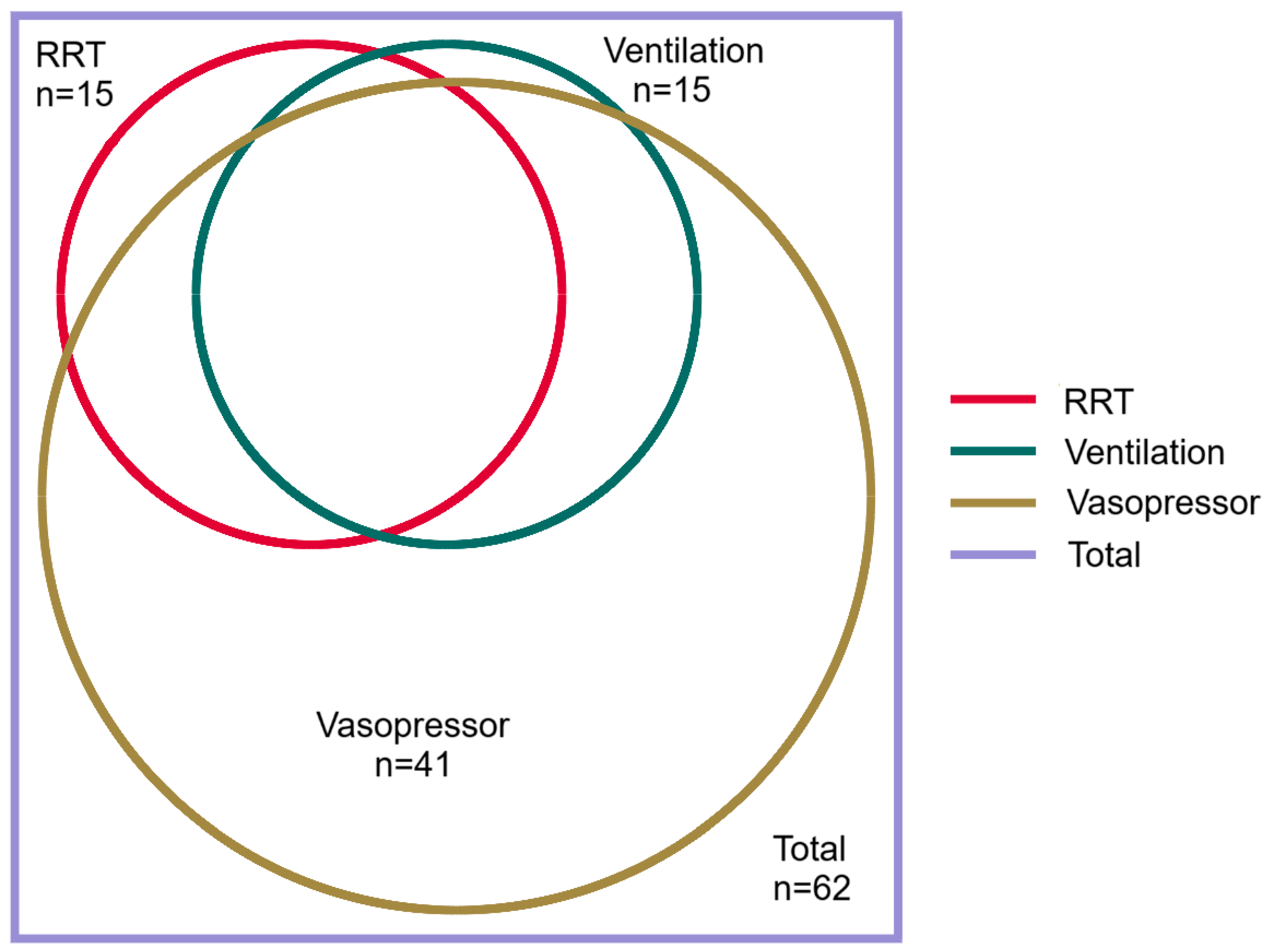

Table 1.
The demographics and comorbidities of individuals admitted to a referral hospital with leptospirosis in Far North Queensland, January 2015–June 2024, and the association of these factors with the development of lung involvement.
Table 1.
The demographics and comorbidities of individuals admitted to a referral hospital with leptospirosis in Far North Queensland, January 2015–June 2024, and the association of these factors with the development of lung involvement.
| Variable | All n=109 |
No lung involvement a n=47 |
Lung involvement a n=62 |
P |
|---|---|---|---|---|
| Age (years) | 38 (24-56) | 33 (21-53) | 42 (26-62) | 0.07 |
| Child (age <16 years) | 6 (6) | 3 (6) | 3 (5) | 1.0 |
| Male sex | 93 (85) | 39 (83) | 54 (87) | 0.55 |
| Rural or remote residence b | 87 (80) | 36 (77) | 51 (81) | 0.47 |
| Wet season presentation | 65 (60) | 28 (60) | 37 (60) | 0.99 |
| Leptospirosis in initial differential diagnosis | 70 (64) | 32 (68) | 38 (61) | 0.46 |
| Duration of symptoms prior to antibiotic therapy (days) | 4 (3-5) | 3 (2-5) | 5 (4-6) | 0.001 |
| Any comorbidity c | 13 (12) | 6 (13) | 7 (11) | 1.0 |
| Diabetes mellitus c | 2 (2) | 1 (2) | 1 (2) | 1.0 |
| Cardiac failure c | 3 (3) | 2 (4) | 1 (2) | 0.58 |
| Ischaemic heart disease c | 2 (2) | 1 (2) | 1 (2) | 1.0 |
| Chronic kidney disease c | 0 | 0 | 0 | - |
| Chronic lung disease c | 5 (5) | 2 (4) | 3 (5) | 1.0 |
| Liver disease c | 5 (5) | 3 (6) | 2 (3) | 0.65 |
| Malignancy c | 2 (2) | 0 | 2 (3) | 0.51 |
| Autoimmune disease c | 0 | - | - | - |
| Immunosuppressed c | 0 | - | - | - |
| Hazardous Alcohol use c | 29 (27) | 13 (28) | 16 (26) | 0.83 |
| Current smoker d | 40 (37) | 14 (30) | 26 (42) | 0.19 |
| PCR positive d | 88/98 (90) | 33/40 (83) | 55/58 (95) | 0.09 |
| Culture positive d | 30/47 (63) | 15/21 (71) | 14/26 (54) | 0.25 |
| Either PCR or culture positive d | 92/101 (91) | 35/41 (85) | 57/60 (95) | 0.15 |
| Serovar Zanoni d | 24/62 (39) | 7/29 (24) | 17/33 (52) | 0.04 |
| Serovar Australis d | 12/62 (19) | 5/29 (17) | 7/33 (21) | 1.0 |
Number (percentage) or median (interquartile range) presented. PCR: polymerase chain reaction. a Lung involvement defined as any new acute changes in lung parenchyma on chest imaging at any stage during the patient’s hospitalisation. b Residing outside the city of Cairns. c As defined in Table S2. d PCR was performed in 98, culture was performed in 47 and 62 had a serovar identified.
Table 2.
Symptoms and signs of individuals admitted to a referral hospital with leptospirosis in Far North Queensland, January 2015–June 2024, and the association of these factors with the development of lung involvement.
Table 2.
Symptoms and signs of individuals admitted to a referral hospital with leptospirosis in Far North Queensland, January 2015–June 2024, and the association of these factors with the development of lung involvement.
| Variable | All n=109 |
No lung involvement a n=47 |
Lung involvement a n=62 |
P |
|---|---|---|---|---|
| Subjective symptoms | ||||
| Headache | 79 (72) | 36 (77) | 43 (69) | 0.40 |
| Fevers | 104 (95) | 46 (98) | 58 (94) | 0.39 |
| Rigors | 40 (37) | 16 (34) | 24 (39) | 0.62 |
| Confusion | 8 (7) | 2 (4) | 6 (10) | 0.46 |
| Fatigue | 43 (39) | 16 (34) | 27 (44) | 0.32 |
| Abdominal pain | 42 (39) | 19 (40) | 23 (37) | 0.72 |
| Myalgia | 82 (75) | 35 (74) | 47 (76) | 0.87 |
| Arthralgia | 46 (42) | 21 (45) | 25 (40) | 0.65 |
| Diarrhoea | 39 (36) | 13 (28) | 26 (42) | 0.12 |
| Nausea/vomiting | 73 (67) | 33 (70) | 40 (65) | 0.53 |
| Chest pain | 9 (8) | 3 (6) | 6 (10) | 0.73 |
| Dyspnoea | 16 (15) | 5 (11) | 11 (18) | 0.30 |
| Cough | 32 (29) | 9 (19) | 23 (37) | 0.04 |
| URTI symptoms | 15 (14) | 7 (15) | 8 (13) | 0.79 |
| Haemoptysis | 12 (11) | 0 | 12 (19) | 0.001 |
| Abnormal bleeding or bruising | 11 (10) | 4 (9) | 7 (11) | 0.75 |
| Objective examination findings | ||||
| Hepatomegaly | 11 (10) | 3 (6) | 8 (13) | 0.35 |
| Splenomegaly | 0 | 0 | 0 | - |
| Lymphadenopathy | 6 (6) | 1 (2) | 5 (8) | 0.23 |
| Conjunctival suffusion | 22 (20) | 9 (19) | 13 (21) | 1.0 |
| Skin rash | 19 (17) | 8 (17) | 11 (18) | 1.0 |
| Abnormal chest auscultation | 44 (40) | 10 (21) | 34 (55) | <0.001 |
| Vital signs at presentation | ||||
| Oliguria b | 42 (39) | 12 (26) | 30 (48) | 0.02 |
| Temperature ° Celsius | 37.1 (36.8-37.6) | 37.2 (36.8-37.8) | 37.1 (36.8-37.6) | 0.62 |
| Supplemental oxygen given | 23 (21) | 3 (6) | 20 (32) | 0.001 |
| SpO2/FiO2 | 462 (450-471) | 467 (457-471) | 462 (296-467) | 0.008 |
| Respiratory rate | 20 (18-24) | 20 (18-24) | 20 (18-25) | 0.54 |
| Heart rate | 99 (80-115) | 97 (78-107) | 104 (83-116) | 0.24 |
| Systolic blood pressure c | 111 (100-124) | 111 (99-124) | 111 (104-124) | 0.40 |
| Vasopressors administered | 42 (39) | 11 (23) | 31 (50) | 0.005 |
| Impaired consciousness | 6 (6) | 0 | 6 (10) | 0.04 |
| Disease severity score | ||||
| SPiRO score d | 1 (0-2) | 1 (0-1) | 2 (1-2) | 0.001 |
Number (percentage) or median (interquartile range) presented. URTI: upper respiratory tract infection. SpO2/FiO2: oxygen saturation: fraction of inspired oxygen ratio. a Lung involvement defined as any new acute changes in lung parenchyma on chest imaging at any stage during the patient’s hospitalisation. b Documented urine output of less than 0.5 mL/kg/hour. c In the patients in whom vasopressor therapy was not initiated. d Three-point SPiRO score (Systolic blood Pressure < 100 mmHg, Respiratory auscultation abnormalities, Oliguria), each is awarded one point [23].
Table 3.
Association between the findings on chest imaging and the subsequent clinical course of individuals admitted to a referral hospital with leptospirosis in Far North Queensland, January 2015–June 2024.
Table 3.
Association between the findings on chest imaging and the subsequent clinical course of individuals admitted to a referral hospital with leptospirosis in Far North Queensland, January 2015–June 2024.
| All n=109 n (%) |
ICU admission n=56 Odds ratio (95% CI) |
p | Pulmonary haemorrhage n=26 Odds ratio (95% CI) |
p | Mechanical ventilation n=15 Odds ratio (95% CI) |
p | |
|---|---|---|---|---|---|---|---|
| Multilobar changes | 50 (46) | 2.59 (1.19 - 5.54) | 0.02 | 26.31 (5.78 - 119.71) | <0.001 | 22.56 (2.84 - 178.92) | <0.001 |
| Alveolar changes | 54 (50) | 5.81 (2.55 - 13.27) | <0.001 | 21.20 (4.68 - 96.01) | <0.001 | 18.9 (2.39 - 149.71) | 0.005 |
| Only interstitial changes | 8 (7) | 0.29 (0.06 - 1.51) | 0.14 | 0.43 (0.05 - 3.79) | 0.45 | 0.89 (0.10 - 7.78) | 0.91 |
| No imaging changes | 47 (43) | 0.24 (0.11 - 0.54) | 0.001 | 0.03 (0.00 - 0.25) | 0.001 | - a | - a |
ICU: Intensive care unit. CI: confidence interval. a All 15 individuals requiring intubation and mechanical ventilation had lung involvement.
Table 4.
Comparison of the clinical course of individuals admitted to a referral hospital with leptospirosis in Far North Queensland, January 2015–June 2024, stratified by the presence of lung involvement, pulmonary haemorrhage or a requirement for mechanical ventilation.
Table 4.
Comparison of the clinical course of individuals admitted to a referral hospital with leptospirosis in Far North Queensland, January 2015–June 2024, stratified by the presence of lung involvement, pulmonary haemorrhage or a requirement for mechanical ventilation.
| All n=109 |
No lung involvement n=47 |
Lung involvement n=62 |
p | No pulmonary haemorrhage n=83 |
Pulmonary haemorrhage n=26 |
p | No mechanical ventilation n=94 |
Mechanical ventilation n=15 |
p | |
|---|---|---|---|---|---|---|---|---|---|---|
| Time to antibiotics (days) | 4 (3-5) | 3 (2-5) | 5 (4-6) | 0.001 | 4 (3-5) | 5 (4-6) | 0.10 | 4 (3-5) | 5 (4-6) | 0.12 |
| ICU admission | 56 (51) | 15 (32) | 41 (66) | <0.001 | 37 (45) | 19 (73) | 0.01 | 41 (44) | 15 (100) | <0.0001 |
| ICU length of stay (days) | 3 (2-5) | 1 (1-3) | 3 (2-6) | 0.002 | 2 (1-3) | 6 (3-11) | <0.0001 | 2 (1-3) | 9 (6-15) | <0.0001 |
| Received RRT | 18 (17) | 3 (6) | 15 (24) | 0.01 | 9 (11) | 9 (35) | 0.01 | 8 (9) | 10 (67) | <0.0001 |
| Received vasopressors | 56 (51) | 15 (32) | 41 (66) | <0.001 | 37 (45) | 19 (73) | 0.01 | 41 (44) | 15 (100) | <0.0001 |
| Steroids prescribed | 19 (17) | 3 (6) | 16 (26) | 0.01 | 8 (10) | 11 (42) | <0.0001 | 6 (6) | 13 (87) | <0.0001 |
| Received ECMO | 2 (2) | 0 | 2 (3) | 0.51 | 0 | 2 (8) | 0.06 | 0 | 2 (13) | 0.02 |
| Hospital length of stay (days) | 6 (3-8) | 4 (3-6) | 7 (5-11) | <0.001 | 5 (3-7) | 7 (6-14) | <0.0001 | 5 (3-7) | 18 (10-21) | <0.0001 |
| Died | 0 | 0 | 0 | - | 0 | 0 | - | 0 | 0 | - |
Number (percentage) or median (interquartile range) presented. ICU: Intensive care unit; RRT: renal replacement therapy; ECMO: extracorporeal membranous oxygenation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



