
Submitted:
17 May 2025
Posted:
19 May 2025
You are already at the latest version
Abstract
The case-fatality rate of severe leptospirosis can exceed 50%. This retrospective cohort study examined 111 individuals with laboratory-confirmed leptospirosis admitted to Cairns Hospital, a referral hospital in tropical Australia, between January 2015 and June 2024. We examined the patients’ demographic, clinical, laboratory and imaging findings at presentation and correlated them with disease course. Severe disease was defined as the presence of pulmonary haemorrhage or a requirement for intensive care unit (ICU) admission. The patients’ median (interquartile range) age was 38 (24-55) years; 85/111 (77%) were transferred from another health facility. Only 13/111 (12%) had any comorbidities. There were 63/111 (57%) with severe disease, including 56/111 (50%) requiring ICU admission. Overall, 56/111 (50%) required vasopressor support, 18/111 (16%) required renal replacement therapy, 14/111 (13%) required mechanical ventilation and 2/111 (2%) required extracorporeal membrane oxygenation. Older age – but not comorbidity – was associated with the presence of severe disease. Hypotension, respiratory involvement, renal involvement and myocardial injury – but not liver involvement – frequently heralded a requirement for ICU care. Every patient in the cohort survived to hospital discharge. Leptospirosis can cause multi-organ failure in otherwise well young people in tropical Australia; however, outcomes are usually excellent in the country’s well-resourced health system.
Keywords:
leptospirosis
; clinical management
; critical care
; tropical medicine
; zoonotic infection
; tropical Australia
Introduction
Leptospirosis is a life-threatening zoonotic infection caused by pathogenic spirochaetes of the genus Leptospira [1]. The highest incidence of leptospirosis is in low- and middle-income countries in tropical and subtropical regions [2]. In 2015, it was estimated that there were over 1 million annual cases of leptospirosis worldwide with ~60000 deaths and the loss of 2.9 million disability-adjusted life years [1,2,3]. With urban expansion and, potentially, the impact of anthropogenic climate change, the global incidence of leptospirosis is expected to rise [4,5].
Mammals are the primary reservoir for Leptospira organisms which can survive for many months in urine-contaminated soil and fresh water [1]. Humans become infected by direct contact with infected animals or after exposure to contaminated water or soil, through a breach in the skin or penetration of mucous membranes or the conjunctiva [1]. Infection commonly occurs after occupational or recreational exposure [6,7,8]. The incidence is highest during warmer months and periods of heavy rain which favour the organism’s survival in the environment [9,10].
The clinical presentation of leptospirosis can range from mild, non-specific symptoms that include fever, headache and myalgia, to life-threatening manifestations that include shock, pulmonary haemorrhage, acute kidney injury and multiorgan failure that requires intensive care unit (ICU) admission [1,11]. The case fatality rate of severe leptospirosis can exceed 50% but reported rates vary enormously and are likely to be explained, predominantly, by geographical variation in access to advanced supportive care [1,12,13,14,15,16].
Far North Queensland (FNQ) in tropical Australia has the highest incidence of leptospirosis in the country [17]. In approximately 85% of local cases there is a history of potential occupational or recreational exposure to the pathogen, with almost 90% of the cases occurring in districts where there is high-intensity banana and cattle farming [18]. FNQ’s largest hospital – Cairns Hospital – has the region’s only ICU. About 11% of laboratory-confirmed adult cases in FNQ require admission to the Cairns Hospital ICU; the case fatality rate of patients requiring ICU admission at Cairns Hospital between 1998 and 2018 was 4% [11]. This high survival rate can be explained by local familiarity with the disease, a well-resourced retrieval network and access to advanced multimodal critical care support in Australia’s universal health system [11,19]. Since that study was completed there have been further enhancements in local critical care services which include the establishment of a statewide extracorporeal membrane oxygenation (ECMO) retrieval service, the employment of more ICU specialists and the expansion of high dependency unit services at Cairns Hospital.
This study was performed to describe the contemporary clinical phenotype of laboratory-confirmed leptospirosis in the FNQ region of tropical Australia. The study also examined the epidemiological, clinical and laboratory characteristics of the patients who developed life-threatening disease. We hypothesised that the recent local expansion of critical care capacity would have translated into better patient outcomes, justifying the health service’s investment in these services.
Methods
This retrospective study was performed at Cairns Hospital, the 771-bed referral hospital for the FNQ region. The hospital serves a population of 290,000 people who live across an area of 380,000 km2 in Northeast tropical Australia. The FNQ region contains two health districts: the Cairns and Hinterland Hospital and Health Service (CHHHS) which serves the administrative hub of Cairns and the surrounding region; the Torres and Cape Hospital and Health Service (TCHHS) serves the almost exclusively remote population residing in the Cape York Peninsula and the Torres Strait Islands (Figure 1). Only individuals who were admitted to Cairns Hospital between 1st January 2015 and 30th June 2024 with a laboratory confirmed diagnosis of leptospirosis were eligible for this study. The study period was chosen as it coincided with the local introduction of an electronic medical record (EMR) system.
Potential study participants were identified by interrogating the Queensland public health system’s electronic laboratory database (AUSLAB). Participants were said to have laboratory confirmed leptospirosis if they satisfied one or more of the following four criteria: (1) isolation of pathogenic Leptospira species from blood culture; (2) a single Leptospira microscopic agglutination titre ≥ 400 supported by a positive enzyme-linked immunosorbent assay IgM result; (3) a fourfold or greater rise in Leptospira microscopic agglutination titre between acute and convalescent phase sera obtained at least two weeks apart or (4) detection of Leptospira in blood by polymerase chain reaction (PCR).
The patients’ EMR was reviewed to collect demographic data and to identify any comorbidities (Supplementary Table 1). Individuals living in the TCHHS were said to have a remote residence and these individuals, and the individuals living in the CHHHS, but outside the city of Cairns, were said to have a rural residence. The patients’ symptoms and clinical signs that were documented at their presentation to Cairns Hospital were also recorded. The patients’ SPiRO score, a marker of disease severity, was calculated as defined previously [18]. Laboratory data were collected from AUSLAB; these data included the values at presentation (either at the regional referring hospital or Cairns Hospital) and the highest or, where relevant, lowest values during the patient’s hospitalisation at Cairns Hospital. A patient was defined as having acute kidney injury at presentation if their estimated glomerular filtration rate was <60ml/min/m2; they were said to have acute liver injury at presentation if they had a serum alanine transferase greater than five times the upper limit of normal (≥150 IU/mL) or a total serum bilirubin greater than three times the upper limit of normal (≥ 60 µmol/L). Oliguria was recorded as present if it was documented in the medical record. All diagnostic testing for leptospirosis – including PCR, serology, and culture – was sought and the results were recorded. Specialist radiologist and cardiologist reporting of any imaging was also collated.
The patients’ treatment and their clinical course was also reviewed. There was a particular focus on the antibiotics that were prescribed, the time to antibiotic therapy and its duration. If patients developed pulmonary haemorrhage, required ICU admission, required vasopressor support, required intubation and mechanical ventilation, required renal replacement therapy (RRT) or required transfer to another facility for ECMO, this was recorded. Pulmonary haemorrhage was said to be present if there was documented frank haemoptysis or if frank blood was present on tracheal aspirate. Individuals were said to have severe leptospirosis if they were admitted to the ICU, or they had pulmonary haemorrhage. The patients’ in-hospital and 90-day mortality was recorded. The patients’ length of stay in hospital and, if relevant, the ICU was also documented.
Statistical Analysis
Data were de-identified, entered into an electronic database (Microsoft Excel) and analysed with statistical software (Stata version 18). Groups were analysed using the Wilcoxon rank-sum test, the chi-squared test, Fisher’s exact test or logistic regression, where appropriate. Trends over time were analysed using Spearman’s test for correlation. If individuals were missing data, they were not included in analyses which evaluated those variables.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki and approved by the Far North Queensland Human Research Ethics Committee (HREC/EX/2024/QCH/108994) on the 2 August 2024. As the retrospective data were deidentified and presented in an aggregated manner, the Committee waived the requirement for informed consent.
Results
There were 111 individuals who satisfied inclusion criteria for the study, 94/111 (85%) were male and 86/111 (77%) were transferred to Cairns Hospital from another health facility. Most individuals (67/111, 60%) presented during the local December-April wet season (Supplementary Figure 1). In 81/111 (73%) there was a potential occupational or environmental exposure preceding the presentation. The number of cases admitted to Cairns Hospital increased between 2015 and 2023, the first and last completed calendar years in the study period (rs=0.75, p=0.02) (Figure 2).
Disease Severity and Clinical Course
All 111 individuals survived to hospital discharge, and all were alive 90 days after their presentation. The median (interquartile range (IQR)) duration of hospitalisation was 5 (3-8) days. There were 56/111 (50%) who required admission to ICU; the median (IQR) length of their stay in ICU was 3 (2-5) days. There were 4/111 (4%) who were transferred from Cairns Hospital to another centre for escalation of care (including ECMO) or, as Cairns Hospital does not have a paediatric ICU, because of their age.
Age, Comorbidity and Correlation with Subsequent Clinical Course
The median (IQR) age of the cohort was 38 (24-55) years; there were only 6 children in the cohort and only one of these children was aged less than 10 years (Table 1). Severe disease was more common in older patients, but 40/63 (63%) of patients with severe disease were under the age of 50. There were 13/111 (12%) who had a documented comorbidity, but there was no association between the presence of comorbidity and severe disease, and 53/63 (84%) with severe disease had no comorbidity. The median (IQR) duration of symptoms in patients with severe disease was 5 (3-6) days compared to 4 (2-5) days in individuals without severe disease (p=0.07).
Diagnosis of Leptospirosis
PCR was performed on blood in 99/111 (89%) and was positive 89/99 (90%). Whole blood culture was performed in 48/111 (43%) and was positive in 30/48 (63%). Acute serology testing was performed in 104/111 (94%) and was positive in 45/104 (43%). Convalescent serology was collected in 51/111 (47%). This was frequently to define the infecting serovar, but in 12/51 (24%) it established the diagnosis of leptospirosis. It was possible to determine the serovar in 59 individuals; the most common were Zanoni (21/59, 36%) and Australis (12/59, 21%) (supplementary table 2). A greater proportion of individuals with confirmed infection with the Zanoni serovar had severe disease than individuals infected with a confirmed infection with other serovars, but in this modestly sized cohort the difference failed to reach statistical significance (table 1). In 71/111 (64%) leptospirosis was in the admitting clinician’s differential diagnosis.
Clinical Signs and Symptoms at Presentation and Correlation with Subsequent Clinical Course
The most common symptoms on presentation were subjective fevers, myalgia, headache and nausea and vomiting (Table 2). It was notable that only 10/26 (38%) individuals presenting directly to Cairns Hospital were febrile (temperature ≥ 38°C) and that a temperature ≥ 38°C had been documented previously in only 51/85 (60%) individuals who were transferred to Cairns Hospital from another facility. Conjunctival suffusion was documented at presentation in only 23/111 (21%). Patients with subjective dyspnoea at presentation were more likely to develop severe disease. Patients with hypotension, tachycardia, oliguria, tachypnoea and a requirement for oxygen supplementation on their initial assessment at Cairns Hospital were also more likely to develop severe disease. The only physical examination finding that was associated with severe disease was abnormal chest auscultation. The 3-point SPiRO score calculated on admission to Cairns Hospital was associated with subsequent development of severe disease; severe disease developed in 10/32 (31%) with a score of 0, 16/36 (44%) with a score of 1, 21/26 (81%) with a score of 2 and 16/17 (94%) with a score of 3, p<0.0001 (Figure 4).
Laboratory Values on Admission and Correlation with Subsequent Clinical Course
The laboratory values on admission, evolution during the patients’ hospitalisation and the association with severe disease are presented in Table 3 and Table 4. Acute kidney injury was present in 49/111 (44%) at presentation. Patients presenting with acute kidney injury were more likely to develop severe disease than patients without acute kidney injury (33/49 (67%) versus 30/62 (48%), OR (95% CI): 2.20 (1.01-4.79), p=0.047). Acute liver injury was documented in only 23/111 (21%) at presentation and patients presenting with acute liver injury were no more likely to develop severe disease than patients without acute liver injury (12/23 (52%) versus 51/88 (58%), OR (95% CI): 0.79 (0.32-1.99), p=0.62). There were 25/111 (23%) with an elevated troponin I at presentation; patients presenting with an elevated troponin I were more likely to develop severe disease than patients without an elevated troponin I (23/25 (92%) versus 40/86 (47%); OR (95% CI): 13.23 (2.93-59.61), p<0.0001). There were 105/111 (95%) with urine microscopy available; 28/105 (27%) had significant haematuria (greater than 50 red blood cells x 106/L) and 58/105 (55%) had significant pyuria (greater than 50 white blood cells x 106/L), but neither haematuria nor pyuria had any association with the development of severe disease.
Chest Imaging Findings on Presentation and During Admission
There were 109/111 (98%) individuals who had chest imaging at presentation; it was abnormal in 37/109 (34%). Individuals with abnormal chest imaging at presentation were more likely to develop severe disease during their hospitalisation than those with normal chest imaging (27/37 (73%) versus 36/72 (50%), OR (95% CI): 2.70 (1.14-6.38), p=0.02). There were 71/109 who had further chest imaging during their hospitalisation; including 45 patients who had normal or no imaging at presentation; in 26/45 (58%) there were abnormalities on this chest imaging. The changes on chest imaging were frequently multilobar and alveolar; patients with multilobar and alveolar changes on chest imaging were more likely to have severe disease (Table 5).
Echocardiography
Echocardiography was performed in 25/111 (23%); it was abnormal in 12; 7/12 (58%) had impaired left ventricular function, 2/12 had impaired right ventricular function and 3 had a pericardial effusion.
Antibiotic Therapy
Antibiotic therapy was prescribed to 109/111 (98%); two children (aged 7 and 11 respectively) were admitted to the general ward with fever and observed without antibiotic therapy. By the time leptospirosis was confirmed their symptoms had abated and so no antibiotics were commenced. The median (IQR) time from the onset of symptoms to the receipt of antibiotic therapy in the other 109 individuals was 4 (3-5) days. Patients with severe disease had a longer duration of symptoms prior to receiving antibiotics than those that did not (5 (3-6) days versus 4 (2-5) days, p=0.02).
The patients received a range of antibiotics, for a variety of durations, but doxycycline (83/109 (76%)) and ceftriaxone (75/109 (69%)) were prescribed most commonly. Broad spectrum antibiotics (meropenem and piperacillin/tazobactam) were prescribed to 42/109 (39%) for at least some time. Patients admitted to ICU were more likely to receive broad spectrum antibiotics than those managed outside the ICU (odds ratio (OR) (95% confidence interval (CI)): 9.08 (3.61-22.82), p<0.001). It was possible to determine the duration of antibiotic therapy in 106/109 (97%) individuals who received antibiotics; the median (IQR) duration of antibiotic therapy was 7 (7-10) days. There was only 1 documented Jarisch-Herxheimer reaction.
ICU Care
Of the patients admitted to ICU, 38/56 (68%) required vasopressor support, 14/56 (25%) required intubation and mechanical ventilation and 13/56 (23%) required RRT. Vasopressor support was initially with noradrenaline. In patients requiring mechanical ventilation, lung protective ventilation strategies were employed. In patients requiring RRT, conventional indications for dialysis were employed. There were 2 patients who required ECMO; both these patients also required vasopressor support and RRT. There were 6 individuals admitted to ICU who did not require vasopressor support, RRT or intubation and mechanical ventilation, but who had critical illness which necessitated close monitoring. Pulmonary haemorrhage was present in 19/56 (34%) who were admitted to ICU and an additional 7 individuals who were not admitted to ICU. There were an additional 4 individuals who required vasopressor support and another 3 individuals who required RRT who were managed without being admitted to the ICU (Figure 3). No patients received plasmapheresis.
Other Management
The patients, in general, received cautious fluid resuscitation. Patients with hypoxia had early use of high flow oxygen via nasal prongs. A conservative transfusion strategy was employed (trigger for blood transfusion haemoglobin < 70g/L, trigger for platelet transfusion major bleeding with platelet count < 50 x 109/L). Patients did not receive corticosteroid therapy routinely, although some patients received corticosteroids as part of their critical care management, particularly those requiring vasopressor support to maintain their blood pressure. Deep venous thrombosis prophylaxis was pharmacological, although it was generally avoided when the platelet count was < 100 x 109/L when mechanical prophylaxis was preferred. Patients admitted to ICU routinely received proton pump inhibitors for stress ulcer prophylaxis and early enteral nutritional support when indicated.
Discussion
Every patient admitted to our referral hospital with laboratory-confirmed leptospirosis survived their hospital admission and were alive 90 days later. This is despite the fact that over half of the cohort required ICU admission for supportive care which included vasopressors, mechanical ventilation, RRT and ECMO. This compares favourably with series from other parts of the world where the case-fatality rate of severe leptospirosis, in one series, exceeded 50% [1,12,20]. It is also important to highlight that more than three-quarters of the cohort were transferred from another health facility, which in some cases was over 800 kilometres away. The encouraging outcomes seen in this cohort again highlight the success of the hub and spoke model in remote, tropical Australia [19].
The explanation for this excellent survival rate is likely to be multifactorial, but it is notable that all but two of the cohort (both children without severe disease) received antibiotic therapy. There is still uncertainty about the benefit of antibiotic therapy in cases of leptospirosis [1,21]. A systematic review in 2024 suggested a shorter time to defervesce, but no effect on mortality or length of hospital stay [22]. A 2024 Cochrane review also emphasised the uncertainty about the ability of antibiotics to reduce mortality or morbidity in individuals with leptospirosis [23]. However both of these reviews highlighted the paucity of quality studies to examine the issue. While antibiotic therapy was only one element in a suite of interventions for the patients in our cohort, those receiving antibiotics earlier in their disease were less likely to develop severe disease.
There are few downsides to antibiotic therapy in critically ill patients with leptospirosis which remains sensitive to antibiotics used in empirical regimes such as penicillins, cephalosporins and macrolides [1,24]. Although the Jarisch Herxheimer reaction is seen locally it can usually be managed easily with simple supportive care [25]. It is also important to highlight that there are often delays in the laboratory confirmation of the diagnosis of leptospirosis and that it is frequently difficult to distinguish leptospirosis from other locally endemic pathogen such as rickettsial disease and Q fever that can also cause life threatening disease [26,27,28]. The early prescription of antibiotic has been linked to better outcomes in patients with both rickettsial infections and Q fever and is also a key tenet of recommendations for managing the critically ill patient with other infections [29,30,31]. Until data emerge to confirm that the harms of antibiotic therapy outweigh its benefits, we would argue that pragmatic clinicians, particularly those in remote or resource-limited settings, should continue to prescribe antibiotic therapy for their patients with possible leptospirosis.
The patients were also able to receive sophisticated multimodal ICU care including early vasopressor support, mechanical ventilation, RRT and, in two cases, ECMO. No patient received plasmapheresis [32]. Patients did not receive corticosteroids routinely, although many received these agents as part of their critical care, particularly in the setting of hypotension unresponsive to fluid resuscitation [33]. Although there are some data to support the use of corticosteroid therapy in individuals with leptospirosis, particularly in those with pulmonary involvement, the well-recognised side effects of corticosteroid therapy including neuromuscular weakness, hyperglycaemia and immunosuppression argue against their routine prescription in leptospirosis until definitive supportive data become available [34,35,36]. Early recognition of the high-risk patients at referral sites and enhanced acute care, enabled by a greater awareness of sepsis, the electronic promulgation of clinical guidelines and an effective aeromedical retrieval network in Australia’s well-resourced universal health system are also likely to have contributed to the cohort’s excellent outcomes [37,38,39].
As in prior studies leptospirosis was diagnosed more commonly in young men: 85% of the cohort was male and almost 70% were younger than 50 years of age, which is no doubt explained by the greater likelihood of occupational and recreational exposure to the pathogen in these populations [1,2]. It was, however, notable that there was only one child under the age of 10 in the cohort and she recovered without antibiotic therapy. A lower incidence of leptospirosis in children – and less severe disease – has been noted in other geographic locations [40,41]. Other zoonotic infections in the region – including rickettsial diseases and Q fever – are also less common and typically cause less severe disease [27,42]. These findings may assist local clinicians in determining the likelihood of these diagnoses while the results of definitive laboratory testing are awaited. Older age was associated with severe disease in this cohort and has been associated with mortality in other studies [2,20,43]. However, more than half of the patients in the cohort with severe disease were younger than 50 years of age without comorbidity, emphasising that leptospirosis can cause life-threatening disease in otherwise well individuals.
Leptospirosis was in the initial differential diagnosis of almost two-thirds of the cohort; however, it was notable that some of the “classic” findings of leptospirosis were not apparent. It was notable that at presentation conjunctival suffusion was documented in only 20%, a prior fever had been documented in only 63% and only 7% had a bilirubin > 50µmol/L. This latter point is important, because anicteric leptospirosis is described in the literature as a typically mild condition [1,20]. Over half of the patients with a bilirubin < 50µmol/L at presentation were subsequently admitted to ICU. Indeed, there was no association between acute liver injury and severe disease in this cohort. The clinical phenotype of leptospirosis cases can vary in different geographical regions and is likely to be explained, at least partially, by differences in the locally prevalent serovars [44,45]. Jaundice is more likely to seen in patients infected with the Icterohemorrhagiae serogroup, a serogroup that is rare in FNQ, where instead serovar Zanoni (Pyrogenes serogroup) and Australis (Australis serogroup) are the most commonly seen (supplementary table 2) [46].
Instead, individuals with hypotension, respiratory involvement (dyspnoea, tachypnoea, abnormal auscultation, hypoxia), acute kidney injury (oliguria, elevated creatinine) and evidence of myocardial injury (elevated cardiac biomarkers) were more likely to develop severe disease, findings that replicate prior studies in the region and other parts of the world [15,16,18,20,47,48,49]. Earlier identification of patients at risk of severe disease enables the escalation of care which fortunately, in Australia’s well-resourced health system includes ready access to advanced ICU support which can support patients who develop these complications while they recover. There were also no deaths in series from a tertiary-care university-affiliated hospital in metropolitan France where 5/34 patients required ICU care [50].
Globally, unfortunately, most cases of leptospirosis occur in socioeconomically disadvantaged individuals living in resource-constrained settings, where access to mechanical ventilation, RRT and, especially, ECMO are often limited [1], The early identification and treatment of individuals at risk of deterioration is therefore essential. The three-point SPiRO score, which identifies high-risk individuals using the three clinical variables of hypotension (SBP < 100mmHg), oliguria and abnormal findings on chest auscultation correlated with disease severity in this cohort. However, the score was devised to identify the patients presenting with symptoms who most urgently require escalation of care and as this study only included patients who were in a referral centre (with 76% already transferred from another facility). There were fewer individuals with a SPiRO score of 0 reducing the negative predictive value of the score in this cohort. Other severity prediction scores also include hypotension, acute kidney injury and evidence of respiratory involvement and the addition of demographic factors, other clinical signs and laboratory indices further increase their ability to identify the high-risk patient [48,49]. However, these disease-specific scores were derived from cohorts of patients with confirmed leptospirosis and the diagnosis is frequently delayed even in well-resourced settings. The study demonstrates the utility of thorough bedside clinical assessment, basic laboratory tests and simple imaging in identifying high-risk patients, an approach which is equally applicable in other conditions that may resemble leptospirosis – and who also are likely to require an escalation of care – in endemic regions [51,52,53,54].
The study again highlights the value of PCR in the prompt diagnosis of leptospirosis [55]. PCR had a sensitivity of almost 90% in our cohort compared with a sensitivity of 43% for serology when these tests were collected early in the patient’s hospitalisation. Serological methods also have a lower specificity in a region where leptospirosis is endemic. Serological tests will also have variability in sensitivity and specificity across countries or regions due to differences in the locally prevalent serovars [1]. However, even in Australia’s well-resourced system, access to those PCR results was often delayed because testing was performed by the statewide reference laboratory, which is 1,390 kilometres away. The development of local PCR diagnostic capacity is a current focus of Cairns Hospital’s laboratory.
Although this study was able to examine the demographic, clinical, laboratory and radiological findings of patients with confirmed leptospirosis in some detail, it has several limitations. The study’s retrospective nature precluded the collection of comprehensive data in all cases. Investigations and clinical assessment were not standardised, and the patients’ symptoms and signs had to be actively sought and then documented in the medical record. The vital signs that were recorded and the clinical findings that were documented were based on the initial assessment in Cairns Hospital, not the findings at the patient’s initial presentation to the health system. The incidence of the Jarisch-Herxheimer reaction is likely to be underestimated as most individuals received their first dose of antibiotics prior to their admission at Cairns Hospital. The referral hospital setting of this study will tend to underestimate the local incidence of the disease while tending to tend to overestimate the local frequency of severe disease. The cohort was heterogeneous, including both adults and children, and had a variety of clinical manifestations; there are significant differences in the assessment and management of a child with a non-localising fever for investigation and an older adult with multiorgan failure, although this highlights the protean manifestations of the leptospirosis [1]. There is significant geographical variation in the prevalence of different serovars of leptospirosis which exerts an influence on the clinical presentation of the cases, limiting the applicability of our findings to other regions [44]. The patients were managed in Australia’s well-resourced universal health system and may therefore be less generalisable to resource-limited settings, where most cases of leptospirosis are seen. However, a high index of suspicion for leptospirosis in the appropriate clinical context, thorough clinical assessment, cautious fluid resuscitation and early referral of high-risk patients to centres where sophisticated critical care support is available are almost certainly likely to be equally relevant in these locations.
Although we understand how the pathogen infects humans the fact that the number of cases of leptospirosis admitted to this referral centre increased during the study period emphasises the challenges of preventing this life-threatening infection. There is currently no safe and effective universal vaccine to prevent leptospirosis in humans and no conclusive evidence that chemoprophylaxis is effective [1,56]. Although every patient in this cohort survived their hospitalisation, they received a suite of interventions, and it is uncertain which of these therapies provided the greatest benefit. There are major gaps in the understanding of the pathophysiology of leptospirosis and while host, pathogen and health system factors all contribute to the disease course and outcomes, their relative contributions are incompletely defined [1,45,57,58,59]. From a therapeutic perspective, the incremental value of antibiotic therapy and corticosteroids (in the critically ill patient) has not been established [1]. Future prospective studies must address these issues. We are currently examining, in detail, the presentation and management of the patients in his cohort with cardiac involvement, respiratory involvement and a requirement for ICU admission in an effort to define these clinical phenotypes in more detail and the therapeutic strategies that were associated with their positive outcomes.
Conclusions
In tropical FNQ, the region of Australia with the highest incidence of leptospirosis in the country, life-threatening disease occurred in young people without comorbidity. Individuals presenting with hypotension, acute kidney injury, evidence of respiratory involvement and evidence of myocardial injury at presentation were at greatest risk of requiring ICU support. Outcomes were excellent in Australia’s well-resourced healthcare system where individuals are able to access prompt, sophisticated, multimodal critical care support. The challenge now is to translate these strategies into the resource-limited settings which are disproportionately affected by leptospirosis, but which have less research, diagnostic, and therapeutic capacity to improve outcomes in their local populations [60,61].
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, H.S, S.S and J.H.; Methodology, H.S and J.H.; Formal analysis, J.H.; Investigation, H.S., P.R. T.K and J.H.; Data curation, H.S., P.R, T.K., S.S and J.H ;Writing—original draft, H.S. and J.H.; Writing review & editing, H.S., P.R, T.K., L.P, S.S and J.H.; Supervision, S.S and J.H. All authors have read and agreed to the published version of the manuscript.
Funding
The authors declare that they have received no specific financial support.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Far North Queensland Human Research Ethics Committee (HREC/EX/2024/QCH/108994) on the 2 August 2024.
Informed Consent Statement
As the retrospective data were de-identified and presented in an aggregated manner, the committee waived the requirement for informed consent.
Data Availability Statement
Data cannot be shared publicly because of the Queensland Public Health Act 2005. Data are available from the Far North Queensland Human Research Ethics Committee (contact via email FNQ_HREC@health.qld.gov.au) for researchers who meet the criteria for access to confidential data.
Acknowledgments
The authors would like to thank the many health care workers who were involved in the care of the patients.
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
- Rajapakse, S.; Fernando, N.; Dreyfus, A.; Smith, C.; Rodrigo, C. Leptospirosis. Nature Reviews Disease Primers 2025, 11, 32. [CrossRef]
- Costa, F.; Hagan, J.E.; Calcagno, J.; Kane, M.; Torgerson, P.; Martinez-Silveira, M.S.; Stein, C.; Abela-Ridder, B.; Ko, A.I. Global Morbidity and Mortality of Leptospirosis: A Systematic Review. PLoS Negl Trop Dis 2015, 9, e0003898. [CrossRef]
- Torgerson, P.R.; Hagan, J.E.; Costa, F.; Calcagno, J.; Kane, M.; Martinez-Silveira, M.S.; Goris, M.G.; Stein, C.; Ko, A.I.; Abela-Ridder, B. Global Burden of Leptospirosis: Estimated in Terms of Disability Adjusted Life Years. PLoS Negl Trop Dis 2015, 9, e0004122. [CrossRef]
- Lau, C.L.; Smythe, L.D.; Craig, S.B.; Weinstein, P. Climate change, flooding, urbanisation and leptospirosis: fuelling the fire? Trans R Soc Trop Med Hyg 2010, 104, 631-638. [CrossRef]
- Obels, I.; Mughini-Gras, L.; Maas, M.; Brandwagt, D.; van den Berge, N.; Notermans, D.W.; Franz, E.; van Elzakker, E.; Pijnacker, R. Increased incidence of human leptospirosis and the effect of temperature and precipitation, the Netherlands, 2005 to 2023. Euro Surveill 2025, 30. [CrossRef]
- Dreesman, J.; Toikkanen, S.; Runge, M.; Hamschmidt, L.; Lusse, B.; Freise, J.F.; Ehlers, J.; Nockler, K.; Knorr, C.; Keller, B.; et al. Investigation and response to a large outbreak of leptospirosis in field workers in Lower Saxony, Germany. Zoonoses Public Health 2023, 70, 315-326. [CrossRef]
- Pages, F.; Larrieu, S.; Simoes, J.; Lenabat, P.; Kurtkowiak, B.; Guernier, V.; Le Minter, G.; Lagadec, E.; Gomard, Y.; Michault, A.; et al. Investigation of a leptospirosis outbreak in triathlon participants, Reunion Island, 2013. Epidemiol Infect 2016, 144, 661-669. [CrossRef]
- Baharom, M.; Ahmad, N.; Hod, R.; Ja'afar, M.H.; Arsad, F.S.; Tangang, F.; Ismail, R.; Mohamed, N.; Mohd Radi, M.F.; Osman, Y. Environmental and Occupational Factors Associated with Leptospirosis: A Systematic Review. Heliyon 2024, 10, e23473. [CrossRef]
- Fairhead, L.J.; Smith, S.; Sim, B.Z.; Stewart, A.G.A.; Stewart, J.D.; Binotto, E.; Law, M.; Hanson, J. The seasonality of infections in tropical Far North Queensland, Australia: A 21-year retrospective evaluation of the seasonal patterns of six endemic pathogens. PLOS Glob Public Health 2022, 2, e0000506. [CrossRef]
- Casanovas-Massana, A.; Pedra, G.G.; Wunder, E.A., Jr.; Diggle, P.J.; Begon, M.; Ko, A.I. Quantification of Leptospira interrogans Survival in Soil and Water Microcosms. Appl Environ Microbiol 2018, 84. [CrossRef]
- Smith, S.; Liu, Y.H.; Carter, A.; Kennedy, B.J.; Dermedgoglou, A.; Poulgrain, S.S.; Paavola, M.P.; Minto, T.L.; Luc, M.; Hanson, J. Severe leptospirosis in tropical Australia: Optimising intensive care unit management to reduce mortality. PLoS Negl Trop Dis 2019, 13, e0007929. [CrossRef]
- Chawla, V.; Trivedi, T.H.; Yeolekar, M.E. Epidemic of leptospirosis: an ICU experience. J Assoc Physicians India 2004, 52, 619-622.
- Smith, S.; Hanson, J. Improving the mortality of severe leptospirosis. Intensive Care Medicine 2020, 46, 827-828. [CrossRef]
- Miailhe, A.F.; Mercier, E.; Maamar, A.; Lacherade, J.C.; Le Thuaut, A.; Gaultier, A.; Asfar, P.; Argaud, L.; Ausseur, A.; Ben Salah, A.; et al. Severe leptospirosis in non-tropical areas: a nationwide, multicentre, retrospective study in French ICUs. Intensive Care Med 2019, 45, 1763-1773. [CrossRef]
- Fonseka, C.L.; Dahanayake, N.J.; Mihiran, D.J.D.; Wijesinghe, K.M.; Liyanage, L.N.; Wickramasuriya, H.S.; Wijayaratne, G.B.; Sanjaya, K.; Bodinayake, C.K. Pulmonary haemorrhage as a frequent cause of death among patients with severe complicated Leptospirosis in Southern Sri Lanka. PLoS Negl Trop Dis 2023, 17, e0011352. [CrossRef]
- Pongpan, S.; Thanatrakolsri, P.; Vittaporn, S.; Khamnuan, P.; Daraswang, P. Prognostic Factors for Leptospirosis Infection Severity. Trop Med Infect Dis 2023, 8. [CrossRef]
- Lau, C.; Smythe, L.; Weinstein, P. Leptospirosis: an emerging disease in travellers. Travel Med Infect Dis 2010, 8, 33-39. [CrossRef]
- Smith, S.; Kennedy, B.J.; Dermedgoglou, A.; Poulgrain, S.S.; Paavola, M.P.; Minto, T.L.; Luc, M.; Liu, Y.H.; Hanson, J. A simple score to predict severe leptospirosis. PLoS Negl Trop Dis 2019, 13, e0007205. [CrossRef]
- Salaveria, K.; Smith, S.; Liu, Y.H.; Bagshaw, R.; Ott, M.; Stewart, A.; Law, M.; Carter, A.; Hanson, J. The Applicability of Commonly Used Severity of Illness Scores to Tropical Infections in Australia. Am J Trop Med Hyg 2021, 106, 257-267. [CrossRef]
- Taylor, A.J.; Paris, D.H.; Newton, P.N. A Systematic Review of the Mortality from Untreated Leptospirosis. PLoS Negl Trop Dis 2015, 9, e0003866. [CrossRef]
- Guzman Perez, M.; Blanch Sancho, J.J.; Segura Luque, J.C.; Mateos Rodriguez, F.; Martinez Alfaro, E.; Solis Garcia Del Pozo, J. Current Evidence on the Antimicrobial Treatment and Chemoprophylaxis of Human Leptospirosis: A Meta-Analysis. Pathogens 2021, 10. [CrossRef]
- Ji, Z.; Jian, M.; Su, X.; Pan, Y.; Duan, Y.; Ma, W.; Zhong, L.; Yang, J.; Song, J.; Wu, X.; et al. Efficacy and safety of antibiotics for treatment of leptospirosis: a systematic review and network meta-analysis. Syst Rev 2024, 13, 108. [CrossRef]
- Win, T.Z.; Han, S.M.; Edwards, T.; Maung, H.T.; Brett-Major, D.M.; Smith, C.; Lee, N. Antibiotics for treatment of leptospirosis. Cochrane Database Syst Rev 2024, 3, CD014960. [CrossRef]
- Trott, D.J.; Abraham, S.; Adler, B. Antimicrobial Resistance in Leptospira, Brucella, and Other Rarely Investigated Veterinary and Zoonotic Pathogens. Microbiol Spectr 2018, 6. [CrossRef]
- Guerrier, G.; Lefevre, P.; Chouvin, C.; D'Ortenzio, E. Jarisch-Herxheimer Reaction Among Patients with Leptospirosis: Incidence and Risk Factors. Am J Trop Med Hyg 2017, 96, 791-794. [CrossRef]
- Bagshaw, R.J.; Stewart, A.G.A.; Smith, S.; Carter, A.W.; Hanson, J. The Characteristics and Clinical Course of Patients with Scrub Typhus and Queensland Tick Typhus Infection Requiring Intensive Care Unit Admission: A 23-year Case Series from Queensland, Tropical Australia. Am J Trop Med Hyg 2020, 103, 2472-2477. [CrossRef]
- Price, C.; Smith, S.; Stewart, J.; Hanson, J. Acute Q Fever Patients Requiring Intensive Care Unit Support in Tropical Australia, 2015-2023. Emerg Infect Dis 2025, 31, 332-335. [CrossRef]
- Susilawati, T.N.; McBride, W.J. Undiagnosed undifferentiated fever in Far North Queensland, Australia: a retrospective study. Int J Infect Dis 2014, 27, 59-64. [CrossRef]
- Dijkstra, F.; Riphagen-Dalhuisen, J.; Wijers, N.; Hak, E.; Van der Sande, M.A.; Morroy, G.; Schneeberger, P.M.; Schimmer, B.; Notermans, D.W.; Van der Hoek, W. Antibiotic therapy for acute Q fever in The Netherlands in 2007 and 2008 and its relation to hospitalization. Epidemiol Infect 2011, 139, 1332-1341. [CrossRef]
- Gavey, R.; Stewart, A.G.A.; Bagshaw, R.; Smith, S.; Vincent, S.; Hanson, J. Respiratory manifestations of rickettsial disease in tropical Australia; Clinical course and implications for patient management. Acta Trop 2025, 266, 107631. [CrossRef]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; McIntyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med 2021, 47, 1181-1247. [CrossRef]
- Fonseka, C.L.; Lekamwasam, S. Role of Plasmapheresis and Extracorporeal Membrane Oxygenation in the Treatment of Leptospirosis Complicated with Pulmonary Hemorrhages. J Trop Med 2018, 2018, 4520185. [CrossRef]
- Rygård, S.L.; Butler, E.; Granholm, A.; Møller, M.H.; Cohen, J.; Finfer, S.; Perner, A.; Myburgh, J.; Venkatesh, B.; Delaney, A. Low-dose corticosteroids for adult patients with septic shock: a systematic review with meta-analysis and trial sequential analysis. Intensive Care Med 2018, 44, 1003-1016. [CrossRef]
- Rodrigo, C.; Lakshitha de Silva, N.; Goonaratne, R.; Samarasekara, K.; Wijesinghe, I.; Parththipan, B.; Rajapakse, S. High dose corticosteroids in severe leptospirosis: a systematic review. Trans R Soc Trop Med Hyg 2014, 108, 743-750. [CrossRef]
- Shenoy, V.V.; Nagar, V.S.; Chowdhury, A.A.; Bhalgat, P.S.; Juvale, N.I. Pulmonary leptospirosis: an excellent response to bolus methylprednisolone. Postgrad Med J 2006, 82, 602-606. [CrossRef]
- Pitre, T.; Drover, K.; Chaudhuri, D.; Zeraaktkar, D.; Menon, K.; Gershengorn, H.B.; Jayaprakash, N.; Spencer-Segal, J.L.; Pastores, S.M.; Nei, A.M.; et al. Corticosteroids in Sepsis and Septic Shock: A Systematic Review, Pairwise, and Dose-Response Meta-Analysis. Crit Care Explor 2024, 6, e1000. [CrossRef]
- National Sepsis Program. Available online: https://www.safetyandquality.gov.au/our-work/national-sepsis-program (accessed on 21 March ).
- Leptospirosis. Available online: https://www.tg.org.au (accessed on 11 May 2025).
- Franklin, R.C.; King, J.C.; Aitken, P.J.; Elcock, M.S.; Lawton, L.; Robertson, A.; Mazur, S.M.; Edwards, K.; Leggat, P.A. Aeromedical retrievals in Queensland: A five-year review. Emerg Med Australas 2021, 33, 34-44. [CrossRef]
- Klement-Frutos, E.; Tarantola, A.; Gourinat, A.C.; Floury, L.; Goarant, C. Age-specific epidemiology of human leptospirosis in New Caledonia, 2006-2016. PLoS One 2020, 15, e0242886. [CrossRef]
- Spichler, A.; Athanazio, D.A.; Vilaca, P.; Seguro, A.; Vinetz, J.; Leake, J.A. Comparative analysis of severe pediatric and adult leptospirosis in Sao Paulo, Brazil. Am J Trop Med Hyg 2012, 86, 306-308. [CrossRef]
- Stewart, A.G.A.; Smith, S.; Binotto, E.; Hanson, J. Clinical Features of Rickettsial Infection in Children in Tropical Australia-A Report of 15 Cases. J Trop Pediatr 2020, 66, 655-660. [CrossRef]
- Lopes, A.A.; Costa, E.; Costa, Y.A.; Sacramento, E.; de Oliveira Junior, A.R.; Lopes, M.B.; Lopes, G.B. Comparative study of the in-hospital case-fatality rate of leptospirosis between pediatric and adult patients of different age groups. Rev Inst Med Trop Sao Paulo 2004, 46, 19-24. [CrossRef]
- Levett, P.N. Leptospirosis. Clin Microbiol Rev 2001, 14, 296-326. [CrossRef]
- Evangelista, K.V.; Coburn, J. Leptospira as an emerging pathogen: a review of its biology, pathogenesis and host immune responses. Future Microbiol 2010, 5, 1413-1425. [CrossRef]
- Katz, A.R.; Ansdell, V.E.; Effler, P.V.; Middleton, C.R.; Sasaki, D.M. Assessment of the clinical presentation and treatment of 353 cases of laboratory-confirmed leptospirosis in Hawaii, 1974-1998. Clin Infect Dis 2001, 33, 1834-1841. [CrossRef]
- Rajapakse, S.; Rodrigo, C.; Haniffa, R. Developing a clinically relevant classification to predict mortality in severe leptospirosis. J Emerg Trauma Shock 2010, 3, 213-219. [CrossRef]
- Marotto, P.C.; Ko, A.I.; Murta-Nascimento, C.; Seguro, A.C.; Prado, R.R.; Barbosa, M.C.; Cleto, S.A.; Eluf-Neto, J. Early identification of leptospirosis-associated pulmonary hemorrhage syndrome by use of a validated prediction model. J Infect 2010, 60, 218-223. [CrossRef]
- Galdino, G.S.; de Sandes-Freitas, T.V.; de Andrade, L.G.M.; Adamian, C.M.C.; Meneses, G.C.; da Silva Junior, G.B.; de Francesco Daher, E. Development and validation of a simple machine learning tool to predict mortality in leptospirosis. Sci Rep 2023, 13, 4506. [CrossRef]
- Jaureguiberry, S.; Roussel, M.; Brinchault-Rabin, G.; Gacouin, A.; Le Meur, A.; Arvieux, C.; Michelet, C.; Tattevin, P. Clinical presentation of leptospirosis: a retrospective study of 34 patients admitted to a single institution in metropolitan France. Clin Microbiol Infect 2005, 11, 391-394. [CrossRef]
- Stewart, A.G.A.; Smith, S.; Binotto, E.; McBride, W.J.H.; Hanson, J. The epidemiology and clinical features of rickettsial diseases in North Queensland, Australia: Implications for patient identification and management. PLoS Negl Trop Dis 2019, 13, e0007583. [CrossRef]
- Mar Minn, M.; Aung, N.M.; Kyaw, Z.; Zaw, T.T.; Chann, P.N.; Khine, H.E.; McLoughlin, S.; Kelleher, A.D.; Tun, N.L.; Oo, T.Z.C.; et al. The comparative ability of commonly used disease severity scores to predict death or a requirement for ICU care in patients hospitalised with possible sepsis in Yangon, Myanmar. Int J Infect Dis 2021, 104, 543-550. [CrossRef]
- Hanson, J.; Lee, S.J.; Mohanty, S.; Faiz, M.A.; Anstey, N.M.; Price, R.N.; Charunwatthana, P.; Yunus, E.B.; Mishra, S.K.; Tjitra, E.; et al. Rapid clinical assessment to facilitate the triage of adults with falciparum malaria, a retrospective analysis. PLoS One 2014, 9, e87020. [CrossRef]
- Niriella, M.A.; Liyanage, I.K.; Udeshika, A.; Liyanapathirana, K.V.; A, P.D.S.; H, J.d.S. Identification of dengue patients with high risk of severe disease, using early clinical and laboratory features, in a resource-limited setting. Arch Virol 2020, 165, 2029-2035. [CrossRef]
- Sreevalsan, T.V.; Chandra, R. Relevance of Polymerase Chain Reaction in Early Diagnosis of Leptospirosis. Indian J Crit Care Med 2024, 28, 290-293. [CrossRef]
- Win, T.Z.; Perinpanathan, T.; Mukadi, P.; Smith, C.; Edwards, T.; Han, S.M.; Maung, H.T.; Brett-Major, D.M.; Lee, N. Antibiotic prophylaxis for leptospirosis. Cochrane Database Syst Rev 2024, 3, CD014959. [CrossRef]
- Lingappa, J.; Kuffner, T.; Tappero, J.; Whitworth, W.; Mize, A.; Kaiser, R.; McNicholl, J. HLA-DQ6 and ingestion of contaminated water: possible gene-environment interaction in an outbreak of Leptospirosis. Genes Immun 2004, 5, 197-202. [CrossRef]
- Agampodi, S.B.; Matthias, M.A.; Moreno, A.C.; Vinetz, J.M. Utility of quantitative polymerase chain reaction in leptospirosis diagnosis: association of level of leptospiremia and clinical manifestations in Sri Lanka. Clin Infect Dis 2012, 54, 1249-1255. [CrossRef]
- Hochedez, P.; Theodose, R.; Olive, C.; Bourhy, P.; Hurtrel, G.; Vignier, N.; Mehdaoui, H.; Valentino, R.; Martinez, R.; Delord, J.M.; et al. Factors Associated with Severe Leptospirosis, Martinique, 2010-2013. Emerg Infect Dis 2015, 21, 2221-2224. [CrossRef]
- Munoz-Zanzi, C.; Dreyfus, A.; Limothai, U.; Foley, W.; Srisawat, N.; Picardeau, M.; Haake, D.A. Leptospirosis-Improving Healthcare Outcomes for a Neglected Tropical Disease. Open Forum Infect Dis 2025, 12, ofaf035. [CrossRef]
- Tshokey, T.; Ko, A.I.; Currie, B.J.; Munoz-Zanzi, C.; Goarant, C.; Paris, D.H.; Dance, D.A.B.; Limmathurotsakul, D.; Birnie, E.; Bertherat, E.; et al. Leptospirosis, melioidosis, and rickettsioses in the vicious circle of neglect. PLoS Negl Trop Dis 2025, 19, e0012796. [CrossRef]
- Bird, K.; Bohanna, I.; McDonald, M.; Wapau, H.; Blanco, L.; Cullen, J.; McLucas, J.; Forbes, S.; Vievers, A.; Wason, A.; et al. A good life for people living with disability: the story from Far North Queensland. Disabil Rehabil 2024, 46, 1787-1795. [CrossRef]
Figure 1.
Map of Far North Queensland, Australia, showing catchment area for current study. Image adapted from Bird, K. et al. [62].
Figure 1.
Map of Far North Queensland, Australia, showing catchment area for current study. Image adapted from Bird, K. et al. [62].
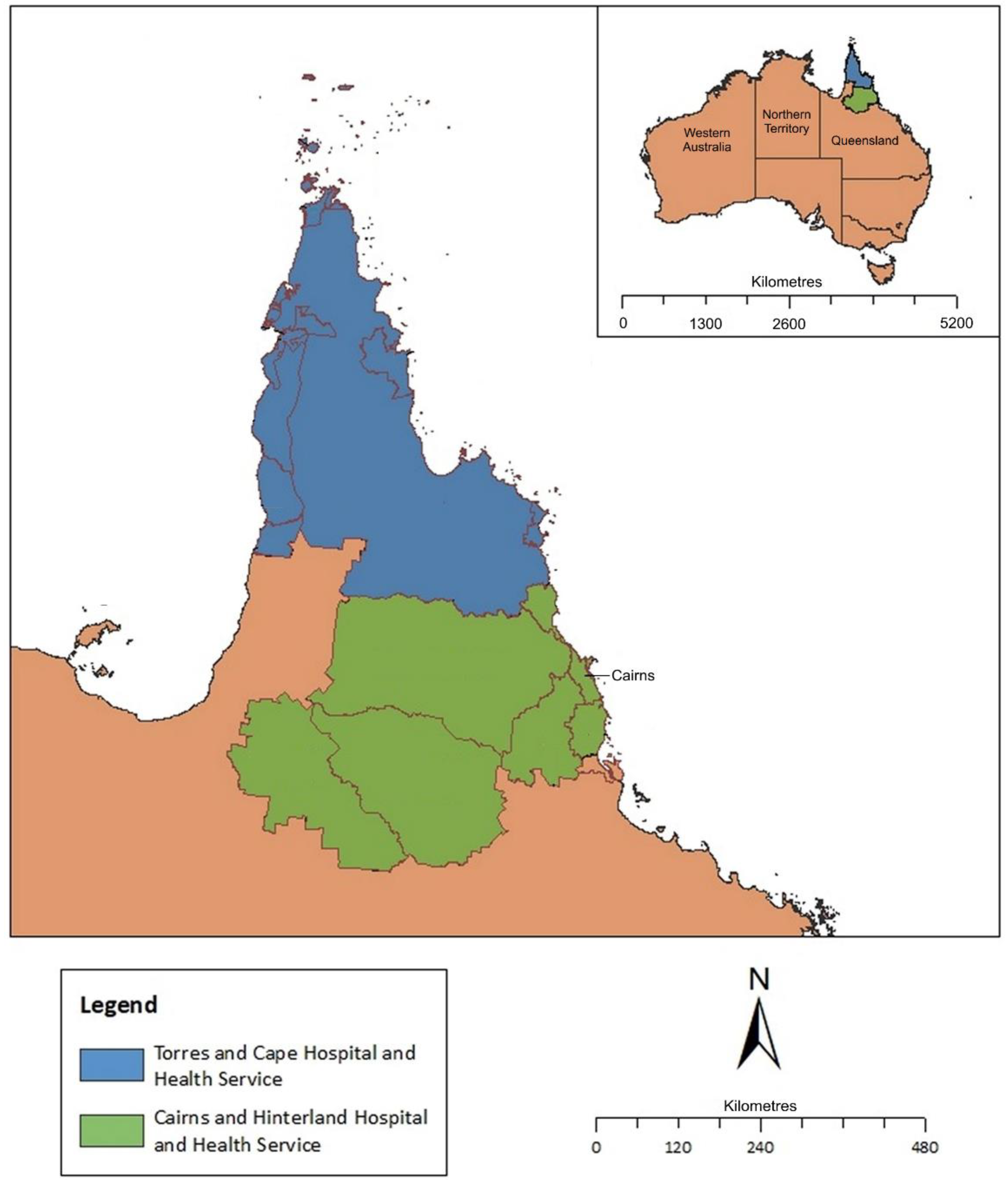
Figure 2.
Number of cases of laboratory confirmed leptospirosis admitted to Cairns Hospital January 2015 to June 2024. * Data collected only until June 2024.
Figure 2.
Number of cases of laboratory confirmed leptospirosis admitted to Cairns Hospital January 2015 to June 2024. * Data collected only until June 2024.
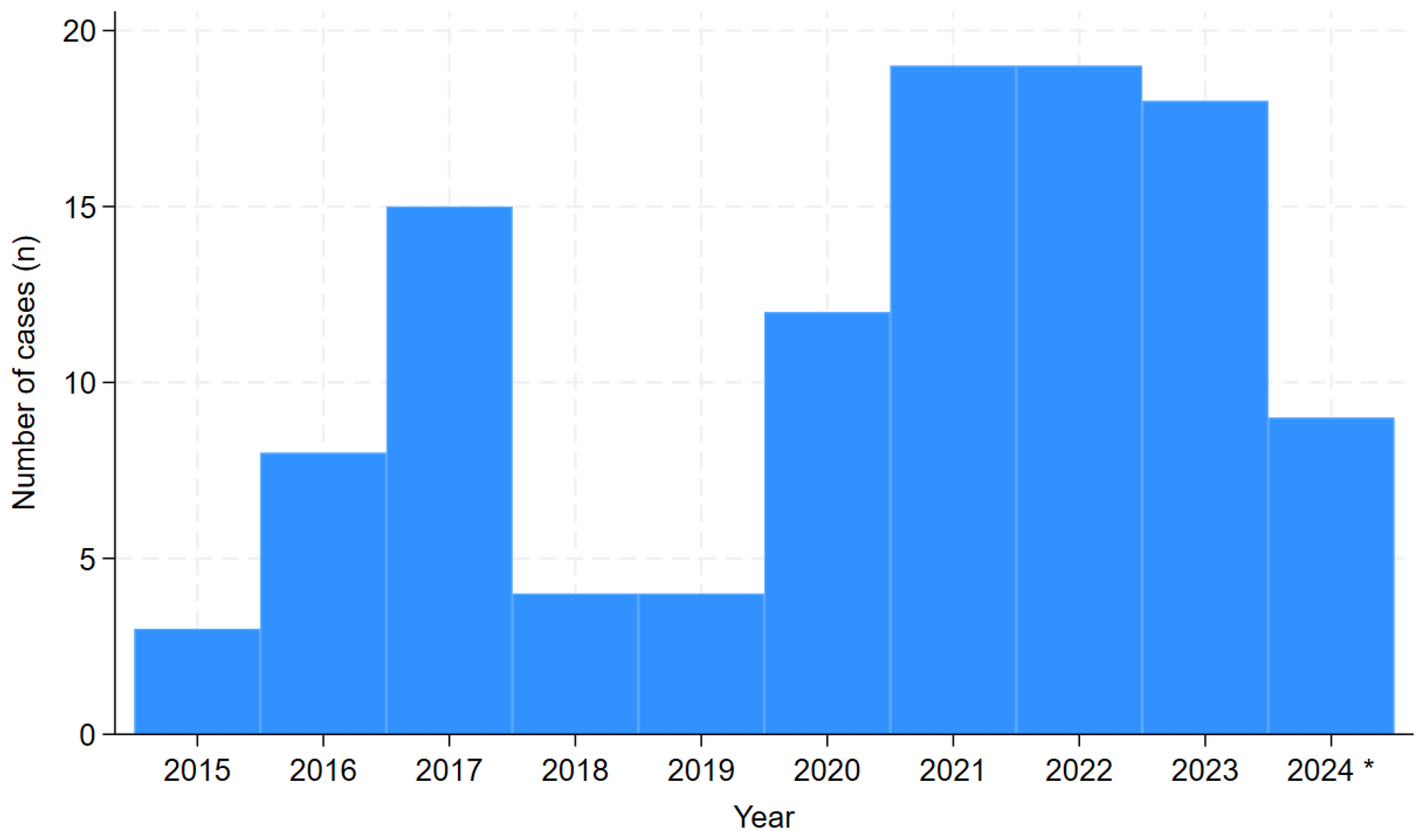
Figure 4.
Association between SPiRO score at presentation to Cairns Hospital and the development of severe disease in patients with laboratory confirmed leptospirosis admitted to Cairns Hospital January 2015 to June 2024.
Figure 4.
Association between SPiRO score at presentation to Cairns Hospital and the development of severe disease in patients with laboratory confirmed leptospirosis admitted to Cairns Hospital January 2015 to June 2024.
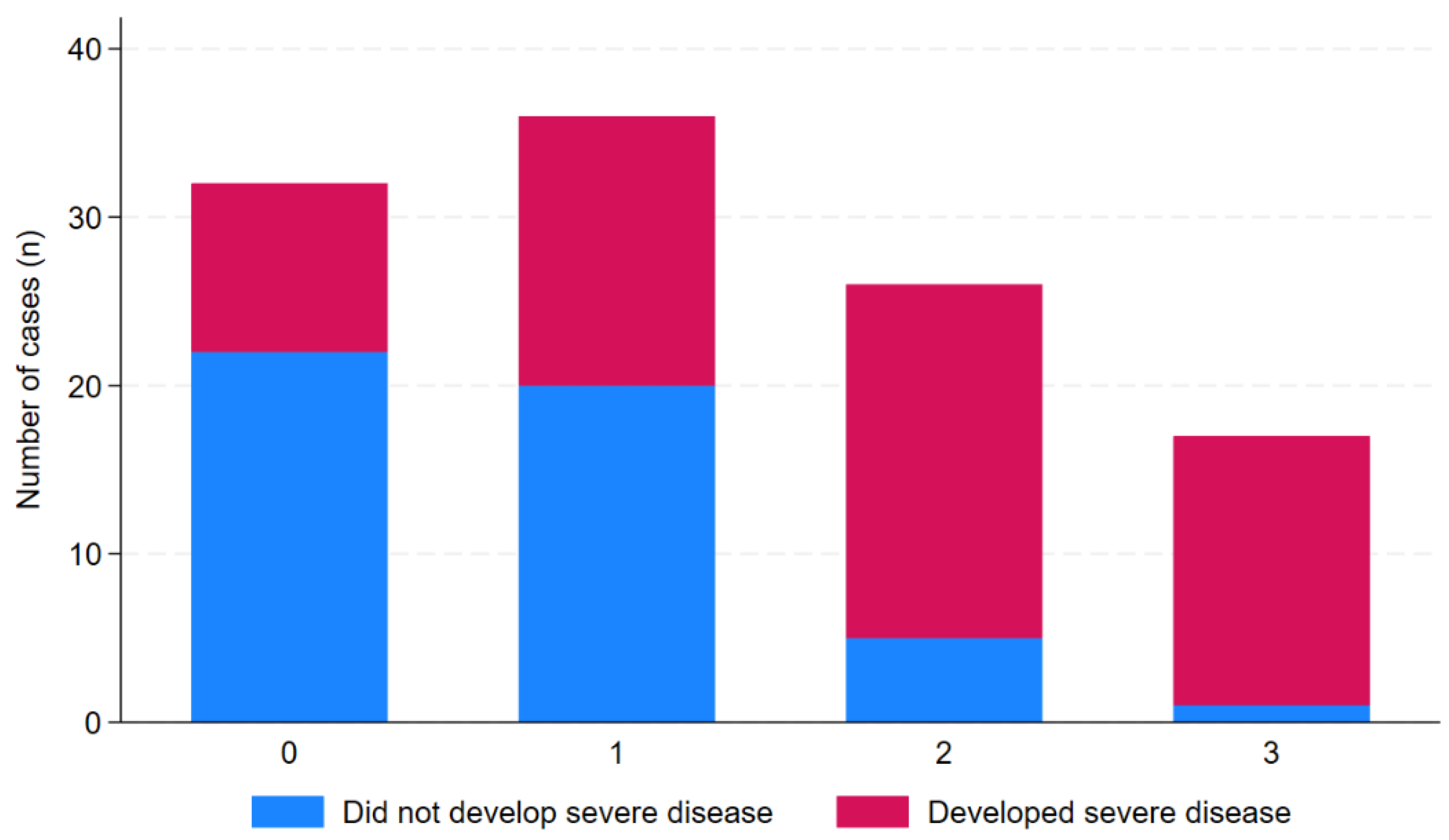
Figure 3.
Venn diagram demonstrating the supportive care provided to the patients with laboratory confirmed leptospirosis admitted to Cairns Hospital January 2015 to June 2024. RRT: renal replacement therapy. There were 9 patients who received vasopressor support, RRT and mechanical ventilation; 6 patients who received vasopressor support and RRT; 5 patients who received vasopressor support and mechanical ventilation; 36 patients who received only vasopressor support and 3 patients who received only RRT.
Figure 3.
Venn diagram demonstrating the supportive care provided to the patients with laboratory confirmed leptospirosis admitted to Cairns Hospital January 2015 to June 2024. RRT: renal replacement therapy. There were 9 patients who received vasopressor support, RRT and mechanical ventilation; 6 patients who received vasopressor support and RRT; 5 patients who received vasopressor support and mechanical ventilation; 36 patients who received only vasopressor support and 3 patients who received only RRT.
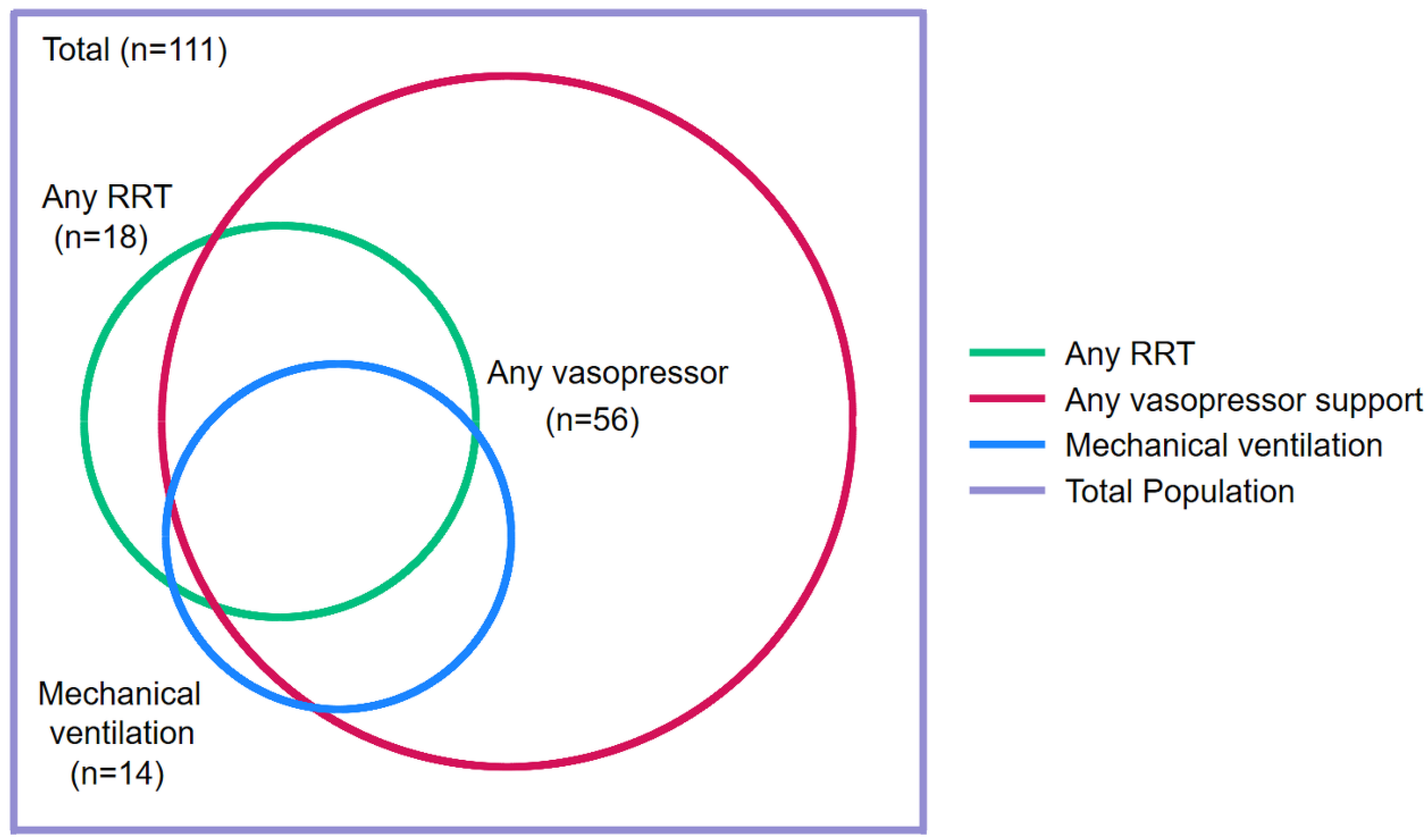

Table 1.
Demographics and comorbidities and association with severe leptospirosis.
| Variable | All n=111 | No severe disease n=48 | Severe disease n=63 | P |
| Age (years) | 38 (24-55) | 32 (19-48) | 41 (26-63) | 0.03 |
| Child (age <16 years) | 6 (5%) | 3 (6%) | 3 (5%) | 1.00 |
| Male sex | 94 (85%) | 38 (79%) | 56 (89%) | 0.19 |
| Remote residence a | 17 (15%) | 6 (12%) | 11 (18%) | 0.60 |
| Rural residence b | 89 (80%) | 36 (75%) | 53 (84%) | 0.23 |
| Wet season presentation c | 67 (60%) | 31 (63%) | 36 (58%) | 0.44 |
| Days of symptoms before presentation | 4 (2-5) | 4 (2-5) | 5 (3-6) | 0.07 |
| Any comorbidity d | 13 (12%) | 3 (6%) | 10 (16%) | 0.15 |
| Diabetes mellitus d | 2 (2%) | 1 (2%) | 1 (2%) | 1.0 |
| Cardiac failure d | 3 (3%) | 0 | 3 (5%) | 0.26 |
| Ischaemic heart disease d | 2 (2%) | 0 | 2 (3%) | 0.51 |
| Chronic kidney disease d | 0 | 0 | 0 | - |
| Lung disease d | 5 (5%) | 1 (2%) | 4 (6%) | 0.39 |
| Liver disease d | 5 (5%) | 1 (2%) | 4 (6%) | 0.39 |
| Malignancy d | 2 (2%) | 0 | 2 (3%) | 0.51 |
| Autoimmune disease d | 0 | 0 | 0 | - |
| Immunosuppressed d | 0 | 0 | 0 | - |
| Hazardous Alcohol use d | 29 (26%) | 12 (24%) | 17 (27%) | 0.81 |
| Smoker d | 41 (37%) | 14 (29%) | 27 (43%) | 0.14 |
| Serovar Zanoni | 21/59 (37%) | 7/30 (23%) | 14/29 (48%) | 0.06 |
| Serovar Australis | 12/59 (20%) | 6/40 (20%) | 6/29 (21%) | 0.72 |
a Residing in the Torres and Cape Hospital and Health Service (TCHHS) b Residing outside the city of Cairns c The local wet season runs from December to April inclusive d As defined in supplementary table 1.
Table 2.
Signs and symptoms and association with severe leptospirosis.
| Variable | Number with data | All n=111 | No severe disease n=48 | Severe disease n=63 | P |
| Subjective symptoms | |||||
| Headache | 111 | 80 (72%) | 40 (83%) | 40 (63%) | 0.02 |
| Fevers | 111 | 106 (96%) | 45 (94%) | 61 (97%) | 0.65 |
| Rigors | 111 | 40 (36%) | 18 (38%) | 22 (35%) | 0.78 |
| Confusion | 111 | 8 (7%) | 3 (6%) | 5 (8%) | 1.00 |
| Fatigue | 111 | 43 (39%) | 14 (29%) | 29 (47%) | 0.07 |
| Abdominal pain | 111 | 42 (38%) | 20 (41%) | 22 (35%) | 0.47 |
| Myalgia | 111 | 83 (75%) | 34 (71%) | 49 (79%) | 0.40 |
| Arthralgia | 111 | 48 (43%) | 17 (35%) | 31 (49%) | 0.15 |
| Diarrhoea | 111 | 41 (37%) | 14 (29%) | 27 (43%) | 0.14 |
| Nausea/vomiting | 111 | 74 (67%) | 35 (73%) | 39 (62%) | 0.14 |
| Chest pain | 111 | 9 (8%) | 4 (8%) | 5 (8%) | 1.00 |
| Dyspnoea | 111 | 16 (14%) | 2 (4%) | 14 (22%) | 0.01 |
| Cough | 111 | 33 (30%) | 11 (23%) | 22 (35%) | 0.17 |
| URTI symptoms | 111 | 15 (14%) | 6 (12%) | 9 (15%) | 1.00 |
| Haemoptysis | 111 | 12 (11%) | 0 | 12 (19%) | 0.001 |
| Abnormal bleeding or bruising | 111 | 11 (10%) | 3 (6%) | 8 (13%) | 0.34 |
| Objective examination findings | |||||
| Hepatomegaly | 111 | 11 (10%) | 4 (8%) | 7 (11%) | 0.75 |
| Splenomegaly | 111 | 0 | - | - | - |
| Lymphadenopathy | 111 | 6 (5%) | 1 (2%) | 5 (8%) | 0.23 |
| Conjunctival suffusion | 111 | 23 (21%) | 11 (23%) | 12 (19%) | 0.62 |
| Skin rash | 111 | 19 (17%) | 11 (23%) | 8 (13%) | 0.21 |
| Abnormal chest auscultation | 111 | 44 (40%) | 13 (27%) | 31 (49%) | 0.02 |
| Vital signs at presentation | |||||
| Oliguria a | 111 | 42 (38%) | 9 (19%) | 33 (52%) | <0.001 |
| Fever > 38.0° Celsius | 111 | 21 (38%) | 7 (15%) | 14 (22%) | 0.34 |
| Supplemental oxygen administered | 111 | 23 (21%) | 2 (4%) | 21 (33%) | <0.001 |
| Respiratory rate ≥ 22 beaths/minute | 111 | 44 (40%) | 14 (29%) | 30 (48%) | 0.049 |
| Heart rate ≥ 100 beats/minute | 111 | 54 (49%) | 17 (35%) | 37 (59%) | 0.02 |
| Systolic blood pressure <100 mmHg | 111 | 56 (50%) | 12 (25%) | 44 (70%) | <0.001 |
| Disease severity score | |||||
| SPiRO score b | 111 | 1 (0-2) | 1 (0-1) | 2 (1-3) | <0.001 |
URTI: upper respiratory tract infection a Documented oliguria in notes by the ICU or admitting team b Three-point SPiRO score (Systolic blood Pressure <100 mmHg, Respiratory auscultation abnormalities, Oliguria) each are awarded one point.
Table 3.
Haematology values on admission and peak or nadir during admission, with association with severe disease.
Table 3.
Haematology values on admission and peak or nadir during admission, with association with severe disease.
| Variable | Units | Number with data |
All n=111 |
No severe disease n=48 |
Severe disease n=63 |
P |
| Haemoglobin initial | g/dL | 111 | 134 (111-147) | 139 (129-150) | 131 (120-145) | 0.02 |
| Haemoglobin lowest | g/dL | 111 | 112 (98-123) | 122 (110-129) | 103 (86-119) | <0.0001 |
| White cell initial | x109/L | 111 | 9.3 (6.8-11.9) | 8.2 (6.3-11.0) | 9.8 (7.2-12.8) | 0.046 |
| White cell highest | x109/L | 111 | 12.8 (9.5-18.3) | 10.6 (8.1-13.3) | 15.9 (11.9-22.1) | <0.0001 |
| White cell lowest | x109/L | 111 | 5.7 (4.2-7.8) | 5.5 (4.2-6.9) | 6.1 (4.2-8.4) | 0.32 |
| Platelet initial | x109/L | 111 | 119 (72-165) | 146 (113-197) | 84 (47-141) | <0.0001 |
| Platelet count lowest | x109/L | 111 | 84 (33-121) | 115 (90-147) | 54 (24-90) | <0.0001 |
| Neutrophil initial | x109/L | 111 | 8.2 (5.5-10.6) | 6.7 (4.6-9.3) | 8.5 (6.3-11.7) | 0.02 |
| Neutrophil highest | x109/L | 111 | 10.7 (8.1-14.2) | 9.0 (6.1-11.8) | 12.8 (10.0-19.9) | <0.0001 |
| Neutrophil lowest | x109/L | 111 | 3.5 (2.7-5.6) | 3.4 (2.5-4.6) | 4.0 (2.8-6.1) | 0.10 |
| Lymphocyte initial | x109/L | 111 | 0.5 (0.3-0.7) | 0.6 (0.4-0.8) | 0.4 (0.3-0.6) | 0.005 |
| Lymphocyte lowest | x109/L | 111 | 0.3 (0.2-0.5) | 0.4 (0.3-0.6) | 0.3 (0.2-0.4) | 0.0001 |
| INR initial | - | 85 | 1.1 (1.1-1.3) | 1.1 (1.1-1.1) | 1.1 (1.1-1.3) | 0.02 |
| INR highest | - | 85 | 1.2 (1.1-1.3) | 1.1 (1.1-1.1) | 1.2 (1.1-1.4) | 0.0002 |
| APTT initial | seconds | 111 | 31 (29-34) | 31 (29-33) | 31 (28-34) | 0.52 |
| APTT highest | seconds | 111 | 32 (30-36) | 31 (29-33) | 33 (30-39) | 0.004 |
INR: international normalised ratio; APTT: activated partial thromboplastin time.
Table 4.
Biochemistry values on admission and peak or nadir during admission, with association with severe disease.
Table 4.
Biochemistry values on admission and peak or nadir during admission, with association with severe disease.
| Variable | Units | Number with data | All n=111 | No severe disease n=48 | Severe disease n=63 | P |
| Initial serum sodium | mmol/L | 111 | 133 (129-135) | 134 (130-137) | 132 (128-135) | 0.01 |
| Lowest serum sodium | mmol/L | 111 | 132 (129-135) | 133 (130-136) | 131 (126-134) | 0.001 |
| Initial serum potassium | mmol/L | 111 | 3.7 (3.4-4.0) | 3.7 (3.4-4.0) | 3.6 (3.4-4.0) | 0.55 |
| Lowest serum potassium | mmol/L | 111 | 4.4 (4.0-4.9) | 4.2 (3.8-4.7) | 4.6 (4.2-4.9) | 0.0003 |
| eGFR initial | mL/min/1.73 m2 | 99 | 64 (25-90) | 77 (27-90) | 54 (25-78) | 0.12 |
| eGFR lowest | mL/min/1.73 m2 | 99 | 38 (14-78) | 76 (18-90) | 25 (14-54) | 0.002 |
| Initial serum creatinine | µmol/L | 111 | 113 (88-205) | 100 (81-197) | 124 (93-232) | 0.04 |
| Highest serum creatinine | µmol/L | 111 | 179 (102-382) | 107 (85-337) | 211 (142-433) | 0.0008 |
| Initial serum bicarbonate | mmol/L | 111 | 23 (21-25) | 24 (22-26) | 23 (21-25) | 0.07 |
| Lowest serum bicarbonate | mmol/L | 111 | 20 (17-22) | 22 (19-23) | 19 (16-21) | 0.0001 |
| Initial serum bilirubin | µmol/L | 111 | 18 (12-28) | 16 (10-26) | 19 (13-29) | 0.19 |
| Highest serum bilirubin | µmol/L | 111 | 26 (19-48) | 20 (12-45) | 29 (21-50) | 0.004 |
| Initial serum ALT | IU/ml | 111 | 68 (27-115) | 68 (26-126) | 67 (27-110) | 0.91 |
| Highest serum ALT | IU/ml | 111 | 121 (68-208) | 131 (69-189) | 120 (68-220) | 0.66 |
| Initial serum AST | IU/ml | 111 | 63 (34-135) | 67 (32-113) | 59 (34-143) | 0.37 |
| Highest serum AST | IU/ml | 111 | 131 (74-210) | 102 (67-166) | 153 (80-287) | 0.02 |
| Initial serum GGT | IU/ml | 111 | 51 (22-120) | 52 (23-159) | 48 (22-103) | 0.66 |
| Highest serum GGT | IU/ml | 111 | 135 (70-235) | 142 (69-297) | 135 (70-217) | 0.57 |
| Initial serum SAP | IU/ml | 111 | 98 (67-171) | 113 (70-164) | 89 (64-174) | 0.49 |
| Highest serum SAP | IU/ml | 111 | 146 (109-208) | 143 (114-221) | 152 (91-208) | 0.88 |
| Initial serum LDH | IU/ml | 111 | 296 (236-359) | 295 (238-358) | 296 (234-386) | 0.66 |
| Highest serum LDH | IU/ml | 111 | 400 (327-534) | 359 (280-401) | 480 (377-690) | <0.0001 |
| Initial serum CK | IU/ml | 83 | 281 (104-1020) | 124 (73-438) | 486 (118-1160) | 0.01 |
| Highest serum CK | IU/ml | 83 | 350 (114-1020) | 124 (73-438) | 621 (124-1225) | 0.004 |
| Initial serum CRP | mg/L | 107 | 190 (138-287) | 156 (102-234) | 233 (165-323) | 0.002 |
| Highest serum CRP | mg/L | 107 | 227 (159-323) | 187 (137-238) | 258 (195-353) | 0.0002 |
| Initial serum lactate | mmol/L | 105 | 1.5 (1.1-2.3) | 1.3 (1.0-1.8) | 1.7 (1.2-2.4) | 0.02 |
| Highest serum lactate | mmol/L | 105 | 2.0 (1.4-2.7) | 1.5 (1.2-2.3) | 2.2 (1.8-3.6) | 0.0001 |
| Elevated initial serum troponin a | - | 111 | 25/111 (23%) | 2/48 (4%) | 23/63 (37%) | <0.0001 |
| Elevated serum troponin during hospitalisation a | - | 111 | 2/48 (4%) | 27/63 (43%) | <0.0001 |
ALT: alanine aminotransferase; AST: aspartate aminotransferase; GGT: gamma glutamyl transferase; SAP: serum alkaline phosphatase; LDH: lactate dehydrogenase; CK: creatinine kinase; CRP: C-reactive protein. a Troponin is expressed as a categorical variable as the Beckman Coulter assay for troponin I (normal reference range <0.040 µg/L) was replaced by the Siemens Atellica assay (reference range <20 ng/L normal for men; <10 normal for women) during the study period.
Table 5.
Imaging on admission and during admission associated with severe disease.
| Variable | Number with data | All n=111 | No severe disease n=48 | Severe disease n=63 | P |
| Abnormal initial chest imaging | 109 | 37/109 (34%) | 10/46 (22%) | 27 (43%) | 0.02 |
| Any abnormal chest imaging during hospitalisation | 109 | 63/109 (58%) | 17/46 (37%) | 46 (73%) | <0.001 |
| Multilobar involvement | 109 | 49/109 (45%) | 12/46 (26%) | 38 (60%) | <0.001 |
| Alveolar changes | 109 | 54/109 (49%) | 10/46 (22%) | 44 (70%) | <0.001 |
| Interstitial changes | 109 | 25/109 (23%) | 6/46 (13%) | 19 (30%) | 0.04 |
| Pleural effusion | 109 | 19/109 (17%) | 8/46 (17%) | 12 (19%) | 1.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



