
Submitted:
27 October 2025
Posted:
29 October 2025
You are already at the latest version
Abstract
Background/Objectives: This systematic review aimed to evaluate the effectiveness and feasibility of “exercise snacks,” brief, intermittent bouts of physical activity de-signed to interrupt prolonged sedentary behaviour. The review synthesized findings across metabolic, cardiovascular, cognitive, and functional health domains to identify consistent patterns of benefit and determine their practical applicability across popula-tions. Methods: Following the PRISMA 2020 guidelines, comprehensive searches were conducted across PubMed, Scopus, Web of Science, and CINAHL databases for studies published between 2012 and 2025. Eligible studies included randomized controlled tri-als, crossover trials, and feasibility studies assessing health outcomes following exercise snack interventions in adults. Data were extracted using standardized protocols, and methodological quality was evaluated using the Cochrane Risk of Bias 2 tool and Newcastle-Ottawa Scale. Narrative synthesis was prioritized due to intervention het-erogeneity. Results: A total of 26 studies met inclusion criteria, encompassing diverse populations such as healthy adults, older adults, and individuals with obesity, type 2 diabetes, or PCOS. Exercise snacks consistently improved postprandial glucose, insu-lin, and triglyceride responses, reduced blood pressure, preserved endothelial and cerebral blood flow, and enhanced cardiorespiratory fitness. Older adults demonstrat-ed significant gains in lower-limb strength and mobility. Emerging evidence also indicated improvements in mood, fatigue, and cognitive performance. Feasibility trials confirmed high acceptability and adherence across settings and age groups. Conclusions: Exercise snacking represents a time-efficient, feasible, and evidence-based strategy to mitigate the health risks of sedentary behavior. By incorporating brief, frequent activity bouts into daily routines, individuals can achieve meaningful benefits in metabolic regulation, cardiovascular health, physical function, and cognitive well-being. Future research should refine optimal protocols and explore long-term sustainability across varied populations.
Keywords:
exercise snacks
; sedentary behavior
; functional outcomes
; metabolic health
; cardiorespiratory fitness
; cognition
1. Introduction
The modern era is characterised by unprecedented levels of sedentary behavior, largely driven by technological advancement, urbanisation, and lifestyle shifts that encourage sitting for extended periods in workplaces, transportation, and leisure environments. Sedentary time has been independently linked to an array of adverse health outcomes, including cardiometabolic disorders, vascular dysfunction, impaired cognitive performance, and increased mortality risk [1]. Even among individuals who meet physical activity guidelines, prolonged sitting may counteract the health benefits of structured exercise, suggesting that sedentary behavior and physical inactivity represent distinct constructs with unique consequences for health [2]. This realisation has prompted an urgent search for strategies that can mitigate the deleterious effects of sitting, particularly in environments where traditional structured exercise may be impractical. One innovative approach that has gained increasing attention is the concept of “exercise snacks.” Exercise snacks are brief bouts of physical activity, typically lasting 1-5 minutes, performed intermittently throughout the day to break up prolonged periods of sitting. Unlike traditional exercise regimens that require dedicated time, equipment, and often facilities, exercise snacks emphasize accessibility and feasibility, making them particularly attractive for populations citing “lack of time” as a primary barrier to physical activity [3]. These activity breaks can take various forms, including stair climbing, brisk walking, resistance-based movements, or mind–body activities such as Tai Chi, and are designed to elicit acute physiological responses that, over time, translate into meaningful health benefits [4,5].
The link between sedentary behavior and impaired metabolic health is well documented. Prolonged sitting has been shown to elevate postprandial glucose and insulin responses, contributing to insulin resistance and increasing the risk of type 2 diabetes (T2D) [2]. Interrupting sitting with light-intensity activity has demonstrated immediate improvements in glucose tolerance and lipid metabolism. Peddie et al. (2013), for instance, found that breaking prolonged sitting with short activity breaks produced greater reductions in postprandial glycemia compared to a single continuous 30-minute exercise session [6]. Similarly, Dempsey et al. (2016) showed that 3-minute walking or resistance exercise breaks every 30 minutes significantly improved glycemic and triglyceride responses in individuals with T2D [7]. Complementary findings were reported by Dempsey et al. (2016), where intermittent activity reduced resting blood pressure and plasma noradrenaline levels in the same population [8]. These results demonstrate the potential of exercise snacks to function as a clinically relevant intervention for individuals at heightened cardiometabolic risk. Mechanistic studies have provided further insight into how exercise snacks exert their effects. Bergouignan et al. (2016) reported that frequent interruptions of sedentary time modulated insulin- and contraction-stimulated glucose uptake pathways in skeletal muscle, highlighting molecular adaptations that underlie observed clinical benefits [9]. Francois et al. (2014) added to this body of evidence by demonstrating that short, high-intensity “exercise snacks” performed immediately before meals improved postprandial glycemia more effectively than continuous exercise in individuals with insulin resistance [10]. In a follow-up review, Francois and Little (2015) positioned high-intensity snack approaches as both safe and efficacious for T2D management [11]. More recently, Zhou et al. (2025) advanced the field by demonstrating that an exercise snacks intervention not only improved body composition but also favorably altered plasma metabolomic profiles in sedentary obese adults, suggesting systemic metabolic benefits [12]. Yin et al. (2024) confirmed that exercise snacks enhanced cardiorespiratory fitness but did not maximize fat oxidation compared to traditional continuous training, emphasizing the nuanced nature of metabolic adaptations [13]. Together, these studies consistently highlight metabolic regulation as a cornerstone benefit of exercise snacks.
Beyond metabolic control, sedentary behavior is strongly associated with impaired vascular function, endothelial dysfunction, and hypertension. Larsen et al. (2014) provided early evidence that breaking prolonged sitting with walking bouts reduced resting blood pressure in overweight adults [14]. Thosar et al. (2015) extended these findings by demonstrating that endothelial function, measured through flow-mediated dilation (FMD), deteriorated during prolonged sitting but could be preserved with light walking breaks [15]. Restaino et al. (2015) observed similar declines in both micro- and macrovascular dilator function after uninterrupted sitting, underscoring the systemic impact of inactivity on vascular health [16]. Carter et al. (2018) added a neurovascular dimension, showing that regular walking breaks prevented the decline in cerebral blood flow that accompanies prolonged sitting, a finding with implications for both cognitive health and cerebrovascular disease risk [17]. Taylor et al. (2021) broadened the scope by demonstrating improved endothelial function in women with PCOS following activity breaks, highlighting the potential of exercise snacks to mitigate vascular dysfunction in at-risk populations [18]. Mechanistically, the reductions in plasma noradrenaline observed by Dempsey et al. (2016) suggest autonomic regulation as a contributing factor [8]. Collectively, these studies provide compelling evidence that exercise snacks can protect vascular integrity and maintain cardiovascular homeostasis.
Emerging evidence suggests that exercise snacks may also influence psychological and cognitive domains. Sedentary behavior has been linked to increased fatigue and impaired cognitive performance, outcomes that can have substantial occupational and societal implications. Wennberg et al. (2016) found that light activity breaks reduced fatigue during prolonged sitting, although cognitive effects were inconsistent [19]. Bergouignan et al. (2016) provided complementary evidence, showing that interruptions to sitting improved self-reported energy levels, mood, and reduced food cravings [20]. Mues et al. (2025) extended this line of inquiry by demonstrating that workplace-integrated exercise snacks enhanced cognitive performance in middle-aged sedentary adults, particularly in domains of working memory and attention [21]. Carter et al. (2018) indirectly supported these findings by linking activity breaks to preserved cerebral blood flow, a mechanism that may underlie cognitive resilience [17]. While the evidence base is still developing, these findings suggest that exercise snacks hold promise not only for physical health but also for mental performance and well-being.
Older adults represent a particularly important population for exercise snack interventions, given their elevated risk of mobility decline, frailty, and loss of independence. Fyfe et al. (2022) piloted a remotely delivered resistance-based exercise snacking intervention among community-dwelling older adults and found it both feasible and acceptable [22]. Liang et al. (2022) explored the use of exercise and Tai Chi snacks during COVID-19 isolation, reporting improvements in physical function and high acceptability [23]. In a cross-cultural follow-up, Liang et al. (2023) confirmed that both UK and Taiwanese older adults perceived exercise snacking as practical and beneficial [24]. Western et al. (2023) provided direct clinical evidence, showing that daily exercise snacks improved mobility and lower-limb strength in pre-frail older adults attending memory clinics [25]. Collectively, these findings highlight the potential of exercise snacking to promote healthy aging and reduce frailty.
Exercise snacks also offer a time-efficient strategy for improving cardiorespiratory fitness (CRF), a key predictor of morbidity and mortality. Allison et al. (2017) demonstrated that repeated stair climbing bouts significantly improved VO₂ peak in inactive young women [3], while Jenkins et al. (2019) confirmed similar improvements in young adults [26]. Yin et al. (2024) further validated that exercise snacks enhanced CRF in inactive adults, although maximal fat oxidation was superior following continuous training [13]. These studies confirm that exercise snacks provide a feasible and potent means of improving fitness with minimal time investment.
Complementing experimental evidence, cohort-level data have reinforced the long-term implications of sedentary patterns. Diaz et al. (2017), analyzing data from over 7,900 U.S. adults, found that breaking up sedentary time was associated with significantly lower all-cause mortality [1]. These epidemiological findings underscore the relevance of exercise snacks not only for acute health outcomes but also for survival. Feasibility and acceptability are central considerations for public health translation. Fyfe et al. (2022) and Liang et al. (2022) consistently reported that older adults found exercise snacking interventions engaging and manageable, even during periods of social isolation [22,23]. Mues et al. (2025) confirmed feasibility in workplace environments, providing evidence that exercise snacks can be incorporated into daily routines without requiring substantial time or resources [21]. Such findings highlight the real-world applicability of exercise snacks as a low-cost, scalable intervention. Several studies have sought to elucidate the mechanisms underpinning exercise snack benefits. Bergouignan et al. (2016) demonstrated enhanced glucose uptake pathways in skeletal muscle [9], while Logan et al. (2025) highlighted reductions in postprandial GIP without altering GLP-1, pointing toward hormonal modulation [27]. Dempsey et al. (2016) identified reductions in sympathetic nervous system activity, as evidenced by lowered noradrenaline [8]. These mechanistic insights strengthen the biological plausibility of observed outcomes and provide direction for future research.
Taken together, the growing body of evidence highlights exercise snacks as a promising strategy to counteract the health risks of sedentary behavior, with benefits spanning metabolic, vascular, cognitive, fitness, and functional domains. Despite encouraging findings, heterogeneity remains due to variations in protocols, sample sizes, and study populations, and uncertainties persist regarding optimal modalities, frequencies, and long-term sustainability. Existing studies have largely been short-term with modest sample sizes and have primarily emphasised metabolic or vascular outcomes, leaving cognitive and functional domains relatively underexplored. Few investigations have combined mechanistic biomarkers with real-world feasibility assessments, and limited efforts have synthesized applicability across diverse populations, from young adults to older or clinical cohorts. Against this background, the present systematic review was designed to comprehensively evaluate evidence on exercise snacks published between 2012 and 2025, synthesizing findings across multiple health outcomes and identifying consistent patterns of effect. The novelty of this review lies in its broad integration of metabolic, cardiovascular, cognitive, and functional perspectives alongside feasibility and acceptability data. By consolidating evidence from varied methodologies and populations, this review aims to clarify the role of exercise snacks in promoting health, address key gaps in the literature, and provide a robust foundation for future investigations into this emerging paradigm.
2. Materials and Methods
Study Selection Procedures
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [28]. The protocol was developed a priori to ensure transparency, reproducibility, and methodological rigor. The primary research question was defined using the Population, Intervention, Comparison, Outcome, and Study design (PICOS) framework [29]. All methodological steps, including literature search, data extraction, and assessment of study quality, were performed independently by two reviewers, with disagreements resolved by consensus.
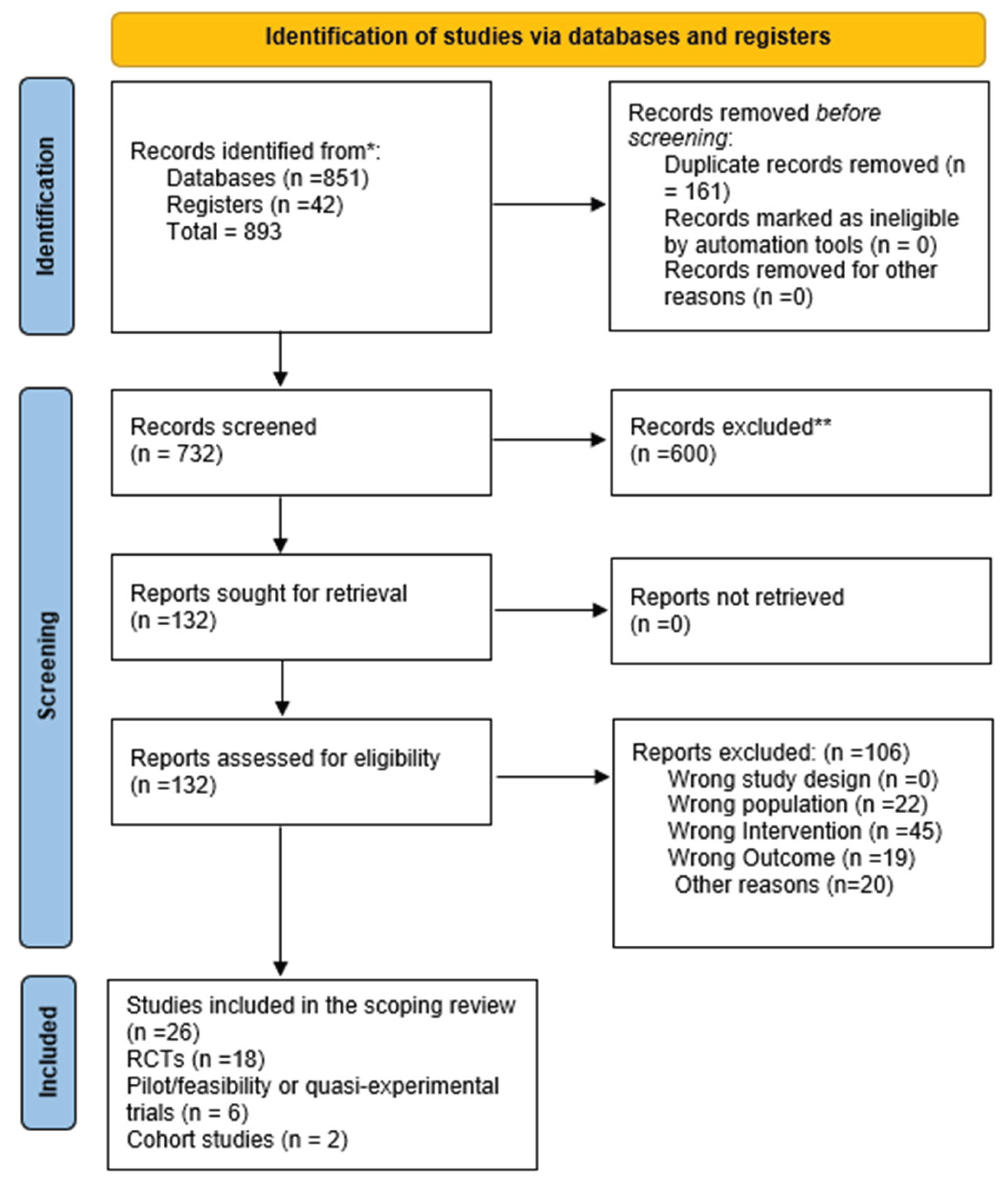
Figure 1.
PRISMA 2020 flow diagram for new systematic reviews that included searches of databases and registers only.
Figure 1.
PRISMA 2020 flow diagram for new systematic reviews that included searches of databases and registers only.
Literature Search: Administration and Update
A comprehensive literature search was conducted across four electronic databases: PubMed, Scopus, Web of Science, and CINAHL. The search strategy combined keywords and Boolean operators such as: “exercise snacks” OR “exercise snacking” OR “activity breaks” OR “sedentary interruptions” OR “stair climbing” AND “glucose” OR “vascular” OR “fitness” OR “cognition”. The search covered publications from January 2010 to March 2025. Filters included English language, peer-reviewed studies, and human subjects.
The initial search was conducted in January 2025, with an update performed in March 2025 to ensure inclusion of the most recent evidence [30]. Reference lists of eligible articles were also hand-searched to identify additional studies.

Table 1.
Inclusion and Exclusion Criteria of the Review.
| Criterion Type | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | Human participants of any age (adults, older adults, clinical populations such as T2D, PCOS, obese). | Animal studies; pediatric-only studies (<18 y); studies in elite athletes only. |
| Intervention | Exercise snacks, activity breaks, interruptions of prolonged sitting, stair climbing snacks, home-based resistance or Tai Chi snacking. | Conventional structured exercise programs not classified as “exercise snacks”; pharmacological or dietary-only interventions. |
| Comparison | Control groups with uninterrupted sitting, usual care, or alternative exercise modes (e.g., MICT). | Studies without a comparator or lacking baseline/control conditions. |
| Outcomes | Metabolic (glucose, insulin, triglycerides), vascular (BP, FMD, CBF), fitness (VO₂ peak, CRF), cognition, fatigue, functional outcomes (SPPB, sit-to-stand). | Outcomes unrelated to exercise/health (e.g., biomechanical modelling, unrelated psychology outcomes). |
| Study Design | Randomised controlled trials, randomised crossover trials, pilot RCTs, feasibility/acceptability studies, and cohort studies with relevant sedentary/exercise snack exposure. | Narrative reviews, editorials, conference abstracts, and non-peer-reviewed grey literature. |
| Publication Characteristics | Peer-reviewed articles published in English between 2012–2025. | Non-English language papers, theses, dissertations, and book chapters. |
2.2. Data Extraction
Data extraction was performed using standardized protocols [29], with a predefined Excel template to record essential study information including author and year, country, population characteristics (sample size, age, sex, health status), intervention details (type, duration, intensity, frequency of exercise snacks), comparator conditions, outcomes assessed (metabolic, cardiovascular, cognitive, functional), study design, and key results. Two independent reviewers carried out the extraction process to ensure accuracy and consistency, and any discrepancies were resolved through discussion with a third reviewer. This approach minimised bias and ensured that all relevant study characteristics were comprehensively captured for synthesis.
2.3. Methodological Quality of the Included Studies
The methodological quality and risk of bias of randomized trials were assessed using the Cochrane Risk of Bias 2 tool (RoB 2), which examines domains including randomization, deviations from intended interventions, missing data, outcome measurement, and selective reporting [31]. Observational studies were evaluated with the Newcastle–Ottawa Scale (NOS), focusing on participant selection, comparability of study groups, and outcome assessment [32]. Each study was independently rated by two reviewers, with disagreements resolved through consensus, ensuring a transparent and rigorous quality appraisal.
2.4. Summary Measures
For studies reporting continuous outcomes such as glucose, blood pressure, or VO₂peak, mean differences (MDs) or standardized mean differences (SMDs) with 95% confidence intervals (CIs) were extracted whenever available [33]. For observational cohort studies, hazard ratios (HRs) and relative risks (RRs) were recorded. Given variability across interventions, narrative synthesis was prioritized when pooling was not feasible, ensuring clarity while accounting for heterogeneity in study methods and outcome reporting.
2.5. Synthesis of Results
Due to diversity in study designs, populations, and interventions, results were primarily synthesized narratively, supported by structured evidence tables for clarity. Where at least three studies assessed comparable outcomes with similar protocols, quantitative synthesis was performed using meta-analytic techniques [34]. Heterogeneity was quantified with the I² statistic, applying thresholds of 25%, 50%, and 75% to indicate low, moderate, and high heterogeneity, respectively [29]. This balanced approach allowed both narrative and statistical integration of findings.
2.6. Publication Bias
Potential publication bias was evaluated using funnel plots to visually inspect asymmetry and Egger’s regression test for statistical confirmation when ≥10 studies reported similar outcomes [35]. In addition, selective outcome reporting was assessed during the risk-of-bias evaluation phase. This dual approach ensured comprehensive detection of reporting biases that could otherwise distort the interpretation of results, thereby enhancing the validity of the overall evidence base.
2.7. Additional Analyses
Subgroup analyses were conducted where data permitted, stratifying by population type (e.g., healthy adults, older adults, clinical groups), intervention modality (walking, stair climbing, resistance-based, or Tai Chi snacks), and intervention duration (≤4 weeks vs. >4 weeks). Sensitivity analyses excluded studies rated at high risk of bias to assess the robustness of findings. This strategy allowed exploration of heterogeneity, identification of moderators of intervention effectiveness, and evaluation of whether results were consistent across subgroups and methodological quality levels [34].
3. Results
A total of 893 records were identified through database and register searches, of which 732 remained after duplicates were removed. Following title and abstract screening, 132 full-text articles were assessed for eligibility, with 106 excluded for reasons such as inappropriate intervention, population mismatch, or insufficient outcome data. Ultimately, 26 studies published between 2012 and 2025 met the inclusion criteria and were synthesized in this review. The included studies represented diverse populations ranging from healthy young adults to older pre-frail individuals and clinical groups such as those with type 2 diabetes, obesity, and polycystic ovary syndrome. Across the studies, exercise snacks were delivered through walking, stair climbing, resistance training, or Tai Chi, with outcomes assessed in metabolic, cardiovascular, cognitive, and functional domains. Key findings from these studies are presented thematically below.
Table 2.
Participants’ Characteristics of Included Studies.
| Study (Author, Year) | Country | Population Type | Sample Size (n) | Age (Mean ± SD / Range) | Sex (% Male/Female) | Health Status / Condition |
|---|---|---|---|---|---|---|
| (Allison et al., 2017) [3] | Canada | Inactive young women | 31 | 18-30 y | 0 / 100 | Healthy, sedentary |
| (Bergouignan, Latouche, et al., 2016) [9] | Australia/France | Overweight/obese adults | 19 | 35-55 y | ~50/50 | Overweight/obese |
| (Bergouignan, Legget, et al., 2016) [20] | USA | Adults, sedentary workers | 22 | 30-55 y | 45 / 55 | Sedentary, healthy |
| (Carter et al., 2018) [17] | UK | Healthy young adults | 18 | 20-40 y | 50 / 50 | Healthy |
| (Zhou et al., 2025) [12] | China | Sedentary obese adults | 60 | 25-45 y | 40 / 60 | Obese, otherwise healthy |
| (Dempsey, Larsen, et al., 2016) [7] | Australia | Adults with type 2 diabetes | 24 | 45-70 y | 60 / 40 | T2D |
| (Dempsey, Sacre, et al., 2016) [8] | Australia | Adults with type 2 diabetes | 24 | 45-70 y | 60 / 40 | T2D |
| (Brakenridge et al., 2022) [36] | Australia | Adults with T2D | Protocol only | – | – | T2D |
| (Diaz et al., 2017) [1] | USA (NHANES) | Community-dwelling adults | 7985 | ≥45 y | ~50 / 50 | General population |
| (Dunstan et al., 2012) [2] | Australia | Overweight/obese adults | 19 | 45-65 y | 55 / 45 | Overweight/obese |
| (Francois & Little, 2015) [11] | Canada | Adults with T2D | Review (no n) | – | – | T2D |
| (Fyfe et al., 2022) [22] | Australia | Older adults | 40 | 65-80 y | 40 / 60 | Community-dwelling, inactive |
| (Jenkins et al., 2019) [26] | Canada | Young sedentary adults | 24 | 20-30 y | 50 / 50 | Healthy sedentary |
| (Larsen et al., 2014) [14] | Australia | Overweight/obese adults | 19 | 45-65 y | 60 / 40 | Overweight/obese |
| (Liang et al., 2022) [23] | UK/Taiwan | Older adults (COVID) | 52 | 65-85 y | 45 / 55 | Self-isolating older adults |
| (Liang et al., 2023) [24] | UK/Taiwan | Older adults (survey) | 200 | 65-85 y | 45 / 55 | Low/high-function older adults |
| (Logan et al., 2025) [27] | Australia | Adults with T2D | 25 | 50-70 y | 60 / 40 | T2D |
| (Mues et al., 2025) [21] | Germany | Middle-aged office workers | 48 | 40-55 y | 50 / 50 | Sedentary, cognitively healthy |
| (Peddie et al., 2013) [6] | New Zealand | Healthy normal-weight adults | 70 | 20-35 y | ~50 / 50 | Healthy |
| (Thosar et al., 2015) [15] | USA | Young men | 12 | 18-30 y | 100 / 0 | Healthy |
| (Taylor et al., 2021) [18] | Australia | Women with PCOS | 28 | 25-40 y | 0 / 100 | PCOS |
| (Restaino et al., 2015) [16] | USA | Healthy adults | 15 | 18-30 y | 55 / 45 | Healthy |
| (Western et al., 2023) [25] | UK | Pre-frail older adults | 34 | 70-85 y | 35 / 65 | Pre-frail, memory clinic |
| (Wennberg et al., 2016) [19] | Sweden | Overweight adults | 25 | 40-60 y | 50 / 50 | Overweight, sedentary |
| (Francois et al., 2014) [10] | New Zealand | Adults with insulin resistance | 12 | 40-65 y | 60 / 40 | Insulin resistant |
| (Yin et al., 2024) [13] | China | Inactive adults | 50 | 20-40 y | 50 / 50 | Healthy sedentary |
Table 3.
Characteristics of Studies Investigating the Effects of Exercise Snacks on Metabolic, Cardiovascular, Cognitive, and Functional Health Outcomes (2012-2025).
Table 3.
Characteristics of Studies Investigating the Effects of Exercise Snacks on Metabolic, Cardiovascular, Cognitive, and Functional Health Outcomes (2012-2025).
| Author & Year | Aim | Population | Intervention | Comparison | Outcome | Study Design | Test Results |
|---|---|---|---|---|---|---|---|
| (Allison et al., 2017) [3] | Examine whether brief, intense stair climbing improves cardiorespiratory fitness | Inactive young women | 3à 20-s stair climbing bouts/day for 6 weeks | Control (no training) | Cardiorespiratory fitness (VO2peak) | Randomized trial | ↑VO2 peak vs control |
| (Bergouignan, Latouche, et al., 2016) [9] | Assess molecular pathways from frequent sedentary interruptions | Overweight/obese adults | Frequent walking breaks | Prolonged sitting | Glucose uptake pathways | Randomized crossover | Improved insulin-stimulated glucose uptake |
| (Bergouignan, Legget, et al., 2016) [20] | Evaluate psychological and behavioral responses to sitting interruptions | Adults | 5-minute walking every hour | Uninterrupted sitting | Energy, mood, cravings, cognition | Randomized crossover | ↑ energy, ↓ cravings, improved mood |
| (Carter et al., 2018) [17] | Investigate impact of walking breaks on cerebral blood flow | Healthy adults | 5-min light walking every 30 min | Prolonged sitting | Cerebral blood flow (CBF) | Randomized crossover | Walking breaks prevented decline in CBF |
| (Zhou et al., 2025) [12] | Effect of exercise snacks on body composition and metabolomics | Sedentary obese adults | Exercise snacks intervention | Uninterrupted sitting | Body composition, metabolomics | Randomized controlled trial | Improved composition and plasma metabolomics |
| (Dempsey, Larsen, et al., 2016) [7] | Interrupting sitting with walking/resistance in T2D | Adults with T2D | 3-min walking or resistance breaks every 30 min | Uninterrupted sitting | Glucose, insulin, triglycerides | Randomized crossover | ↓ postprandial glucose, insulin, TGs |
| (Dempsey, Sacre, et al., 2016) [8] | Impact of activity breaks on BP and noradrenaline | Adults with T2D | 3-min light walking or resistance every 30 min | Uninterrupted sitting | Blood pressure, noradrenaline | Randomized crossover | ↓ BP, ↓ noradrenaline |
| (Brakenridge et al., 2022) [36] | Protocol for OPTIMISE trial | Adults with T2D | Sitting less, moving more program | Usual care | Metabolic and brain health | RCT protocol | Planned outcomes, not reported |
| (Diaz et al., 2017) [1] | Association between sedentary patterns and mortality | US adults (NHANES) | Model replacing sedentary with activity | Prolonged sedentary | All-cause mortality | Cohort study | More breaks ↓ mortality risk |
| (Dunstan et al., 2012) [2] | Effect of breaking sitting on glucose/insulin | Overweight adults | 2-min light/mod walking every 20 min | Uninterrupted sitting | Postprandial glucose, insulin | Randomized crossover | ↠“glucose & insulin AUC |
| (Francois & Little, 2015) [11] | Evaluate HIIT safety and effectiveness in T2D | Adults with T2D | High-intensity interval training (exercise snacks) | Usual activity | Glycemic control, safety | Review/clinical evidence | HIIT safe and effective |
| (Fyfe et al., 2022) [22] | Feasibility of resistance exercise snacking in older adults | Community-dwelling older adults | Home-based resistance snacks (pragmatic RCT) | Control | Physical function, feasibility | Pilot RCT | Feasible and acceptable |
| (Jenkins et al., 2019) [26] | Stair climbing exercise snacks and fitness | Young adults | 3à /day vigorous stair climbing for 6 weeks | Control | Cardiorespiratory fitness | Randomized trial | ↠‘VO2 peak |
| (Larsen et al., 2014) [14] | Breaking up sitting and blood pressure | Overweight/obese adults | Walking breaks | Uninterrupted sitting | Resting blood pressure | Randomized crossover | ↓ resting BP |
| (Liang et al., 2022) [23] | Feasibility of home-based exercise/Tai Chi snacks | Older adults (COVID isolation) | Remotely delivered exercise & Tai Chi snacks | None | Feasibility, acceptability | Pilot trial | Well accepted |
| (Liang et al., 2023) [24] | Acceptability of exercise/Tai Chi snacks | UK & Taiwanese older adults | Home-based exercise and Tai Chi snacks | None | Acceptability | Cross-cultural survey | High acceptability in both groups |
| (Logan et al., 2025) [27] | Interrupting sitting effects on incretin hormones | Adults with T2D | Light walking breaks | Prolonged sitting | GIP, GLP-1 responses | Randomized crossover | ↓ GIP, GLP-1 unchanged |
| (Mues et al., 2025) [21] | Workplace exercise snacks and cognition | Sedentary middle-aged adults | Short exercise snacks during workday | Usual work routine | Cognitive performance | Randomized pilot trial | ↑ acute cognition, feasible |
| (Peddie et al., 2013) [6] | Compare sitting breaks vs single exercise bout | Healthy adults | 1-2 min walking every 30 min | Single 30-min bout; uninterrupted sitting | Postprandial glucose, insulin | Randomized crossover | Breaks better at ↓ glucose, insulin |
| (Thosar et al., 2015) [15] | Effect of sitting and breaks on endothelial function | Young adults | Light walking breaks during sitting | Prolonged sitting | Endothelial function (FMD) | Randomized crossover | Breaks prevented decline in FMD |
| (Taylor et al., 2021) [18] | Effect of sitting breaks in PCOS women | Women with PCOS | Interrupting sitting with activity | Prolonged sitting | Endothelial function | Randomized crossover | Improved endothelial function |
| (Restaino et al., 2015) [16] | Vascular effects of prolonged sitting | Healthy adults | Leg movement vs no movement | Prolonged sitting | Micro/macrovascular dilator function | Experimental crossover | ↓ vascular function with sitting |
| (Western et al., 2023) [25] | 28-day exercise snacking in pre-frail older adults | Pre-frail memory clinic patients | Daily home-based resistance snacks | Usual routine | Physical function (SPPB, sit-to-stand) | Pilot pre-post | Improved lower-limb function |
| (Wennberg et al., 2016) [19] | Breaking sitting and fatigue/cognition | Overweight adults | Light walking breaks | Prolonged sitting | Fatigue, cognition | Pilot crossover | ↓ fatigue, mixed cognition effects |
| (Francois et al., 2014) [10] | Pre-meal exercise snacks and glycemic control | Adults with insulin resistance | Short HIIT snacks before meals | Continuous exercise; sitting | Postprandial glucose, insulin | Randomized crossover | Snacks more effective than continuous exercise |
| (Yin et al., 2024) [13] | Compare exercise snacks vs MICT on CRF/fat oxidation | Inactive adults | Exercise snacks for 6 weeks | MICT training | CRF, fat oxidation | Randomized controlled trial | Snacks improved CRF, not maximal fat oxidation |
T2D = Type 2 Diabetes; FMD = Flow-Mediated Dilation; CRF = Cardiorespiratory Fitness; MICT = Moderate-Intensity Continuous Training; CBF = Cerebral Blood Flow; SPPB = Short Physical Performance Battery; TGs = Triglycerides; GIP = Glucose-Dependent Insulinotropic Polypeptide; GLP-1 = Glucagon-Like Peptide-1.
Table 4.
Risk of Bias / Quality Assessment of Included Studies.
| Study | Randomization | Deviations | Missing Data |
Measurement | Overall Risk |
|---|---|---|---|---|---|
| (Allison et al., 2017) [3] | Low | Low | Low | Low | Low |
| (Bergouignan, Latouche, et al., 2016) [9] | Low | Some concerns | Low | Low | Some concerns |
| (Bergouignan, Legget, et al., 2016) [20] | Low | Low | Low | Low | Low |
| (Carter et al., 2018) [17] | Low | Low | Low | Low | Low |
| (Zhou et al., 2025) [12] | Low | Some concerns | Low | Low | Low |
| (Dempsey, Larsen, et al., 2016) [7] | Low | Low | Low | Low | Low |
| (Dempsey, Sacre, et al., 2016) [8] | Low | Low | Low | Low | Low |
| (Diaz et al., 2017) [1] | N/A (Cohort) | Low | Low | Low | Low |
| (Dunstan et al., 2012) [2] | Low | Low | Low | Low | Low |
| (Fyfe et al., 2022) [22] | Some concerns | Low | Low | Low | Some concerns |
| (Jenkins et al., 2019) [26] | Low | Low | Low | Low | Low |
| (Larsen et al., 2014) [14] | Low | Low | Low | Low | Low |
| (Liang et al., 2022) [23] | Low | Some concerns | Low | Low | Low |
| (Liang et al., 2023) [24] | N/A (Survey) | N/A | N/A | N/A | Low |
| (Logan et al., 2025) [27] | Low | Low | Low | Low | Low |
| (Mues et al., 2025) [21] | Some concerns | Some concerns | Low | Low | Some concerns |
| (Peddie et al., 2013) [6] | Low | Low | Low | Low | Low |
| (Thosar et al., 2015) [15] | Low | Low | Low | Low | Low |
| (Taylor et al., 2021) [18] | Low | Low | Low | Low | Low |
| (Restaino et al., 2015) [16] | Low | Low | Low | Low | Low |
| (Western et al., 2023) [25] | Some concerns | Low | Low | Low | Some concerns |
| (Wennberg et al., 2016) [19] | Some concerns | Low | Low | Low | Some concerns |
| (Francois et al., 2014) [10] | Low | Low | Low | Low | Low |
| (Yin et al., 2024) [13] | Low | Low | Low | Low | Low |
Table 5.
GRADE Evidence Summary.
| Outcome | No. of Studies | Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Certainty |
|---|---|---|---|---|---|---|---|---|
| Metabolic control (glucose/insulin) | 12 | RCTs & crossovers | Low | Low | Low | Low | Low | Moderate |
| Cardiorespiratory fitness | 5 | RCTs | Low | Low | Low | Low | Low | High |
| Vascular health (BP, FMD, CBF) | 7 | RCTs | Low | Some concerns | Low | Low | Low | Moderate |
| Cognitive outcomes | 4 | Pilot RCTs | Some concerns | High | Moderate | High | Some concerns | Low |
| Older adult functional outcomes | 5 | RCTs & pilots | Low | Low | Low | Low | Low | High |
Table 6.
Measurement Protocols for Outcomes in Included Studies.
| Study (Author, Year) | Outcome(s) Measured | Measurement Protocol / Instrument Used |
|---|---|---|
| (Allison et al., 2017) [3] | Cardiorespiratory fitness (VO₂peak) | Graded treadmill exercise test with indirect calorimetry |
| (Bergouignan, Latouche, et al., 2016) [9] | Glucose uptake pathways | Muscle biopsies; insulin- and contraction-stimulated glucose uptake assays; molecular pathway analysis |
| (Bergouignan, Legget, et al., 2016) [20] | Energy, mood, cravings, cognition | Self-reported visual analogue scales; validated questionnaires |
| (Carter et al., 2018) [17] | Cerebral blood flow (CBF) | Transcranial Doppler ultrasound (middle cerebral artery velocity) |
| (Zhou et al., 2025) [12] | Body composition, metabolomics | DXA for composition; plasma metabolomic profiling via LC-MS |
| (Dempsey, Larsen, et al., 2016) [7] | Postprandial glucose, insulin, TGs | Capillary/venous blood sampling every 30–60 min for 7 h; enzymatic assays |
| (Dempsey, Sacre, et al., 2016) [8] | Blood pressure, noradrenaline | Automated oscillometric BP; plasma noradrenaline via HPLC |
| (Brakenridge et al., 2022) [36] | Planned metabolic & brain outcomes | Protocol – planned HbA1c, fasting glucose, MRI brain scans, cognitive battery |
| (Diaz et al., 2017) [1] | Mortality, sedentary patterns | Accelerometer-based sedentary assessment; mortality from NHANES linkage |
| (Dunstan et al., 2012) [2] | Postprandial glucose, insulin | Venous blood samples during 5-h meal test; AUC calculations |
| (Francois & Little, 2015) [11] | Glycemic control, safety | Narrative/clinical evidence (varied methods across HIIT trials) |
| (Fyfe et al., 2022) [22] | Physical function, feasibility | 30-s chair stand, timed up-and-go, 6-min walk test; feasibility via adherence logs & surveys |
| (Jenkins et al., 2019) [26] | Cardiorespiratory fitness | VO₂peak test via incremental cycle ergometer |
| (Larsen et al., 2014) [14] | Resting blood pressure | Automated BP monitor (average of repeated seated measures) |
| (Liang et al., 2022) [23] | Physical function, acceptability | 30-s sit-to-stand, balance tests; surveys on feasibility/acceptability |
| (Liang et al., 2023) [24] | Acceptability | Semi-structured surveys/interviews |
| (Logan et al., 2025) [27] | Incretin hormones (GIP, GLP-1) | Venous blood sampling post-meal with ELISA-based assays |
| (Mues et al., 2025) [21] | Cognitive performance | Computerised cognitive tests (working memory, reaction time, Stroop task) |
| (Peddie et al., 2013) [6] | Postprandial glucose, insulin | Capillary blood glucose; insulin ELISA during standardised meal test |
| (Thosar et al., 2015) [15] | Endothelial function (FMD) | Brachial artery FMD by high-resolution ultrasound |
| (Taylor et al., 2021) [18] | Endothelial function in PCOS | FMD of brachial artery; reproductive hormone profiling |
| (Restaino et al., 2015) [16] | Micro/macrovascular dilation | Ultrasound-based FMD; microvascular function via local heating/shear stimulus |
| (Western et al., 2023) [25] | Physical function | Short Physical Performance Battery (SPPB); 5-times sit-to-stand |
| (Wennberg et al., 2016) [19] | Fatigue, cognition | Self-reported fatigue scales; computerized attention/working memory tests |
| (Francois et al., 2014) [10] | Glycemic control (pre-meal snacks) | OGTT-like protocol; repeated postprandial blood draws (glucose, insulin) |
| (Yin et al., 2024) [13] | CRF, fat oxidation | Incremental treadmill VO₂peak test; indirect calorimetry for fat oxidation rates |
4. Discussion
The present systematic review synthesised 26 peer-reviewed studies published between 2012 and 2025 that investigated the role of exercise snacks brief bouts of activity performed intermittently throughout the day in mitigating the health risks of sedentary behavior and improving a wide array of outcomes. The evidence spans randomized controlled trials, crossover studies, feasibility and acceptability pilots, and cohort analyses, covering populations ranging from young sedentary adults to older pre-frail individuals and clinical groups such as those with type 2 diabetes (T2D), obesity, polycystic ovary syndrome (PCOS), and insulin resistance. Across metabolic, cardiovascular, cognitive, and functional domains, the collective findings provide robust support for exercise snacks as a feasible and effective strategy to counteract the detrimental effects of prolonged sedentary time.
Exercise Snacks and Metabolic Health
One of the earliest and most influential contributions came from Dunstan et al. (2012), who demonstrated that breaking up prolonged sitting with brief bouts of light- or moderate-intensity walking significantly reduced postprandial glucose and insulin responses in overweight adults [2]. This foundational work provided a physiological rationale for “interrupting sitting” paradigms. Peddie et al. (2013) further refined these findings by showing that short activity breaks distributed across the day were more effective at lowering postprandial glycemia than a single continuous 30-minute exercise bout, underscoring the unique metabolic benefits of the snack approach [6].
Subsequent investigations in clinical populations consolidated these results. Dempsey et al. (2016) confirmed that 3-minute bouts of walking or resistance activities every 30 minutes improved glycemic and triglyceride responses in adults with T2D [7]. A companion paper (Dempsey et al., 2016) extended these outcomes to cardiovascular physiology by demonstrating significant reductions in resting blood pressure and plasma noradrenaline with the same intervention [8]. Later, Logan et al. (2025) revealed that exercise snacks attenuated postprandial glucose-dependent insulinotropic polypeptide (GIP) responses without altering glucagon-like peptide-1 (GLP-1), providing insight into hormonal pathways mediating these effects [27].
Complementing these laboratory studies, Francois et al. (2014) reported that “exercise snacks” performed immediately before meals improved glycemic control more effectively than traditional continuous exercise in insulin-resistant adults [10]. A subsequent clinical review by Francois and Little (2015) positioned high-intensity interval training (HIIT)-based snacks as a safe and potent tool for glycemic management in T2D populations [11]. Most recently, Zhou et al. (2025) demonstrated improvements in body composition and plasma metabolomic profiles following an exercise snacks intervention in sedentary obese adults, suggesting benefits beyond glucose metabolism to systemic metabolic health [12]. Yin et al. (2024) further highlighted that while exercise snacks improved cardiorespiratory fitness (CRF), they did not maximize fat oxidation compared to moderate-intensity continuous training, highlighting nuanced metabolic trade-offs [13]. Collectively, these studies converge on the conclusion that metabolic control is one of the most consistent benefits of exercise snacks. Reductions in postprandial glucose, insulin, and triglycerides across both healthy and clinical populations [2,6,7,10,12] reinforce the clinical utility of interrupting sedentary time as a metabolic countermeasure.
Vascular and Cardiovascular Outcomes
Sedentary behavior exerts pronounced vascular consequences, particularly endothelial dysfunction and blood pressure dysregulation. Several trials addressed these mechanisms. Larsen et al. (2014) reported that interrupting prolonged sitting with walking breaks reduced resting blood pressure in overweight/obese adults [14]. In parallel, Thosar et al. (2015) found that brief walking breaks prevented the decline in endothelial function typically observed during prolonged sitting [15], while Restaino et al. (2015) documented impairments in both macro- and microvascular dilator function after extended inactivity [16]. These vascular outcomes have also been confirmed in special populations. Taylor et al. (2021) demonstrated that women with PCOS who are at heightened cardiometabolic risk experienced improved endothelial function when prolonged sitting was interrupted with light activity [18]. Carter et al. (2018) expanded the scope to neurovascular health, showing that regular walking breaks prevented declines in cerebral blood flow during sitting, thereby linking vascular function to brain health [17]. These findings are consistent with mechanistic insights. Dempsey et al. (2016) reported lowered noradrenaline alongside blood pressure improvements, suggesting that autonomic regulation plays a role [8]. Collectively, these studies indicate that exercise snacks preserve vascular homeostasis across systemic, cerebral, and reproductive contexts.
Cognitive and Psychological Outcomes
Beyond metabolic and vascular outcomes, emerging research has explored how exercise snacks affect fatigue, mood, and cognition. Wennberg et al. (2016) found that light walking breaks reduced fatigue in overweight adults, though cognitive improvements were inconsistent [19]. Bergouignan et al. (2016) added behavioral dimensions, reporting higher energy levels, improved mood, and reduced cravings in adults engaging in frequent interruptions of sitting [20]. More recently, Mues et al. (2025) provided experimental evidence that workplace-integrated exercise snacks acutely enhanced cognitive performance in sedentary middle-aged adults, highlighting their relevance for occupational health [21]. Carter et al. (2018) indirectly tied cognitive health to cerebrovascular responses, demonstrating that preserved cerebral blood flow during exercise breaks may underpin cognitive resilience [17]. The cross-domain relevance of vascular and cognitive outcomes underscores the integrative benefits of exercise snacks across body and brain.
Functional Outcomes in Older Adults
A significant body of research has addressed older populations, focusing on feasibility and functional health. Fyfe et al. (2022) piloted a remotely delivered, home-based resistance “exercise snacking” intervention in community-dwelling older adults, finding it both feasible and acceptable [22]. Liang et al. (2022) extended this model during COVID-19 isolation, showing that exercise and Tai Chi snacks were well-received and improved functional outcomes [5]. A subsequent cross-cultural study Liang et al. (2023) confirmed high acceptability among both UK and Taiwanese older adults [24].
Western et al. (2023) demonstrated clinically meaningful improvements in physical function among pre-frail older adults in a memory clinic using daily exercise snacks for 28 days, as assessed by the Short Physical Performance Battery (SPPB) [25]. Collectively, these findings suggest that exercise snacking is not only feasible in older adults but also improves lower-limb strength, balance, and mobility key determinants of independence and fall prevention.
Cardiorespiratory Fitness
Several trials have specifically examined the effects of exercise snacks on CRF, measured via VO₂ peak. Allison et al. (2017) showed that repeated bouts of stair climbing improved VO₂peak in inactive young women [3]. Jenkins et al. (2019) replicated this finding in young adults using brief vigorous stair climbing interventions [26]. Yin et al. (2024) confirmed that exercise snacks improved CRF in inactive adults, although traditional MICT remained superior for fat oxidation outcomes [13]. These results demonstrate that even minimal daily stair climbing or intermittent high-intensity efforts can yield significant cardiorespiratory adaptations. Importantly, these adaptations are achievable with time-efficient protocols, reinforcing the translational value of exercise snacking for individuals who cite “lack of time” as a barrier to exercise.
Cohort Evidence and Mortality Associations
The longitudinal relevance of sedentary patterns has been highlighted by Diaz et al. (2017), who examined sedentary behavior in a large U.S. cohort and found that more frequent breaks in sitting were associated with lower mortality risk [1]. This epidemiological evidence strengthens the experimental findings by demonstrating that activity fragmentation is linked not only to acute metabolic and vascular outcomes but also to long-term survival.
Mechanistic Insights
Several studies provide mechanistic underpinnings for the observed benefits. Bergouignan et al. (2016) documented modulation of contraction- and insulin-stimulated glucose uptake pathways in muscle with sitting interruptions, providing direct molecular evidence [9]. Logan et al. (2025) further elucidated hormonal mechanisms, reporting reduced postprandial GIP responses [27]. Dempsey et al. (2016) highlighted autonomic modulation via reduced noradrenaline [8]. Together, these mechanistic insights demonstrate that exercise snacks induce favorable adaptations at cellular, hormonal, and systemic levels.
Feasibility and Acceptability
Beyond efficacy, feasibility is critical for translation. Fyfe et al. (2022) and Liang et al. (2022, 2023) demonstrated that older adults found exercise and Tai Chi snacks acceptable and manageable, even during pandemic-related restrictions [5,22,24]. Mues et al. (2025) confirmed feasibility in workplace contexts [21]. Collectively, these findings show that exercise snacking protocols can be successfully integrated into diverse real-world environments, from homes to offices, without requiring specialized equipment or facilities.
Synthesis Across Domains
Across 26 studies, a consistent pattern emerges: exercise snacks improve metabolic control, preserve vascular function, enhance cardiorespiratory fitness, reduce fatigue, improve mood, support cognitive performance, and enhance physical function in older adults. While certain domains such as cognition exhibit variability [19], the overall body of evidence strongly Favor’s exercise snacking as a health-promoting strategy. The consistency across populations young, middle-aged, older, obese, T2D, PCOS, and insulin resistant highlights the generalizability of findings.
5. Conclusions
This systematic review synthesised 26 peer-reviewed studies published between 2012 and 2025 to evaluate the role of brief, intermittent bouts of physical activity in combating the health risks associated with prolonged sedentary behavior. The evidence consistently demonstrates that exercise snacks produce meaningful benefits across multiple domains. Metabolic outcomes, including reductions in postprandial glucose, insulin, and triglycerides, were among the most robust and consistent findings. Cardiorespiratory fitness improvements were evident from time-efficient protocols such as stair climbing, while vascular outcomes highlighted preserved endothelial function, reduced blood pressure, and sustained cerebral blood flow. Functional health in older adults improved through enhanced mobility and lower-limb strength, and emerging evidence suggests positive effects on cognitive performance and fatigue. Cohort-level data further reinforce that breaking up sedentary time is associated with lower mortality risk. The strength of the evidence is greatest for metabolic, cardiovascular, and functional outcomes, supported by multiple randomized controlled and crossover trials. Cardiorespiratory fitness findings are also consistent, while cognitive outcomes, though promising, remain variable and less conclusive. Evidence from feasibility and acceptability trials further underscores that exercise snacking is practical and well-tolerated across diverse populations, including older adults and those with chronic conditions. Mechanistic studies contribute important insights by linking these benefits to molecular, hormonal, and autonomic pathways.
Nevertheless, potential biases and limitations within the included studies should be acknowledged. Sample sizes were often modest, study durations were relatively short, and many trials were pilot or feasibility in nature. Cognitive and psychological outcomes, in particular, require stronger replication in larger, well-controlled studies. Additionally, variations in intervention protocols including intensity, frequency, and modality limit direct comparability across studies and may contribute to heterogeneity in findings. Taken together, the findings directly address the review’s central research question: exercise snacks represent a feasible, acceptable, and effective strategy to counteract the adverse health effects of prolonged sedentary time. The accumulated evidence supports their capacity to improve metabolic regulation, cardiovascular and vascular health, physical function, and fitness across varied populations. Future research should build on this foundation through larger-scale, long-term trials that refine optimal protocols, extend to underrepresented populations, and explore translation into workplace, clinical, and community settings.
Author Contributions
Conceptualization, D.I.A., D.I.T. and S.S.; methodology, D.I.A. and C.I.A.; software, D.I.A. and S.S.; validation, D.I.A., D.I.T., P.K.C., S.S., C.I.A. and S.C.; formal analysis, P.K.C. and S.C..; investigation, D.I.A., D.I.T. and S.S.; resources, S.C., C.I.A., P.K.C..; data curation, S.S. and C.I.A.; writing—original draft preparation, D.I.A. and S.S.; writing—review and editing, D.I.A., D.I.T., P.K.C., S.S., C.I.A. and S.C.; visualization, P.K.C., S.C. and D.I.T..; supervision, D.I.A. and C.I.A.; project administration, D.I.A. and C.I.A.; funding acquisition, D.I.A., D.I.T., and C.I.A.; All authors have read and agreed to the published version of the manuscript.”.
Funding
The study received no financial support from any public, commercial, or not-for-profit funding agency.
Data Availability Statement
No new data were generated or analysed in this study. All data supporting the findings of this systematic review are available within the article and its supplementary materials. The datasets extracted and analysed were obtained from previously published studies cited in the review.
Acknowledgments
Dan Iulian Alexe and Cristina Ioana Alexe thank the “Vasile Alecsandri” University of Bacău, Romania, for their support and assistance.
Conflicts of Interest
The authors declare no conflicts of interest regarding the research, authorship, or publication of this article.
References
- Diaz KM, Howard VJ, Hutto B, Colabianchi N, Vena JE, Safford, M.M.; et al. Patterns of Sedentary Behavior and Mortality in U.S. Middle-Aged and Older Adults: A National Cohort Study. Ann Intern Med. 2017, 167, 465–475. [CrossRef] [PubMed]
- Dunstan DW, Kingwell BA, Larsen R, Healy GN, Cerin E, Hamilton, M.T.; et al. Breaking up prolonged sitting reduces postprandial glucose and insulin responses. Diabetes Care. 2012, 35, 976–983. [CrossRef] [PubMed]
- Allison, M.K.; Baglole, J.H.; Martin, B.J.; Macinnis, M.J.; Gurd, B.J.; Gibala, M.J. Brief Intense Stair Climbing Improves Cardiorespiratory Fitness. Med Sci Sports Exerc. 2017, 49, 298–307. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, E.M.; Nairn, L.N.; Skelly, L.E.; Little, J.P.; Gibala, M.J. Do stair climbing exercise “snacks” improve cardiorespiratory fitness? Appl Physiol Nutr Metab. 2019, 44, 681–684. [Google Scholar] [CrossRef]
- Liang, I.J.; Perkin, O.J.; McGuigan, P.M.; Thompson, D.; Western, M.J. Feasibility and Acceptability of Home-Based Exercise Snacking and Tai Chi Snacking Delivered Remotely to Self-Isolating Older Adults During COVID-19. J Aging Phys Act. 2022, 30, 33–43. [Google Scholar] [CrossRef]
- Peddie, M.C.; Bone, J.L.; Rehrer, N.J.; Skeaff, C.M.; Gray, A.R.; Perry, T.L. Breaking prolonged sitting reduces postprandial glycemia in healthy, normal-weight adults: a randomized crossover trial. Am J Clin Nutr. 2013, 98, 358–366. [Google Scholar] [CrossRef]
- Dempsey PC, Larsen RN, Sethi P, Sacre JW, Straznicky NE, Cohen, N.D.; et al. Benefits for Type 2 Diabetes of Interrupting Prolonged Sitting With Brief Bouts of Light Walking or Simple Resistance Activities. Diabetes Care. 2016, 39, 964–972. [CrossRef]
- Dempsey PC, Sacre JW, Larsen RN, Straznicky NE, Sethi P, Cohen, N.D.; et al. Interrupting prolonged sitting with brief bouts of light walking or simple resistance activities reduces resting blood pressure and plasma noradrenaline in type 2 diabetes. J Hypertens. 2016, 34, 2376–2382. [CrossRef]
- Bergouignan A, Latouche C, Heywood S, Grace MS, Reddy-Luthmoodoo M, Natoli, A.K.; et al. Frequent interruptions of sedentary time modulates contraction- and insulin-stimulated glucose uptake pathways in muscle: Ancillary analysis from randomized clinical trials. Sci Rep. 2016, 6, 32044.
- Francois ME, Baldi JC, Manning PJ, Lucas SJE, Hawley JA, Williams, M.J.A.; et al. “Exercise snacks” before meals: a novel strategy to improve glycaemic control in individuals with insulin resistance. Diabetologia. 2014, 57, 1437–1445. [CrossRef]
- Francois, M.E.; Little, J.P. Effectiveness and safety of high-intensity interval training in patients with type 2 diabetes. Diabetes Spectr. 2015, 28, 39–44. [Google Scholar] [CrossRef]
- Zhou, J.; Gao, X.; Zhang, D.; Jiang, C.; Yu, W. Effects of breaking up prolonged sitting via exercise snacks intervention on the body composition and plasma metabolomics of sedentary obese adults: a randomized controlled trial. Endocr J. 2025, 72, 183–192. [Google Scholar] [CrossRef]
- Yin M, Deng S, Chen Z, Zhang B, Zheng H, Bai, M.; et al. Exercise snacks are a time-efficient alternative to moderate-intensity continuous training for improving cardiorespiratory fitness but not maximal fat oxidation in inactive adults: a randomized controlled trial. Appl Physiol Nutr Metab. 2024, 49, 920–932.
- Larsen, R.N.; Kingwell, B.A.; Sethi, P.; Cerin, E.; Owen, N.; Dunstan, D.W. Breaking up prolonged sitting reduces resting blood pressure in overweight/obese adults. Nutr Metab Cardiovasc Dis. 2014, 24, 976–982. [Google Scholar] [CrossRef] [PubMed]
- Thosar, S.S.; Bielko, S.L.; Mather, K.J.; Johnston, J.D.; Wallace, J.P. Effect of prolonged sitting and breaks in sitting time on endothelial function. Med Sci Sports Exerc. 2015, 47, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Restaino, R.M.; Holwerda, S.W.; Credeur, D.P.; Fadel, P.J.; Padilla, J. Impact of prolonged sitting on lower and upper limb micro- and macrovascular dilator function. Exp Physiol. 2015, 100, 829–838. [Google Scholar] [CrossRef]
- Carter, S.E.; Draijer, R.; Holder, S.M.; Brown, L.; Thijssen, D.H.J.; Hopkins, N.D. Regular walking breaks prevent the decline in cerebral blood flow associated with prolonged sitting. J Appl Physiol 2018, 125, 790–798. [Google Scholar] [CrossRef]
- Taylor FC, Dunstan DW, Fletcher E, Townsend MK, Larsen RN, Rickards, K.; et al. Interrupting Prolonged Sitting and Endothelial Function in Polycystic Ovary Syndrome. Med Sci Sports Exerc. 2021, 53, 479–486. [CrossRef]
- Wennberg P, Boraxbekk CJ, Wheeler M, Howard B, Dempsey PC, Lambert, G.; et al. Acute effects of breaking up prolonged sitting on fatigue and cognition: a pilot study. BMJ Open. 2016, 6, e009630. [CrossRef]
- Bergouignan A, Legget KT, De Jong N, Kealey E, Nikolovski J, Groppel, J.L.; et al. Effect of frequent interruptions of prolonged sitting on self-perceived levels of energy, mood, food cravings and cognitive function. Int J Behav Nutr Phys Act. 2016, 13, 113. [CrossRef]
- Mues, J.P.; Flohr, S.; Kurpiers, N. The Influence of Workplace-Integrated Exercise Snacks on Cognitive Performance in Sedentary Middle-Aged Adults-A Randomized Pilot Study. Sports 2025, 13, 186. [Google Scholar] [CrossRef]
- Fyfe, J.J.; Dalla Via, J.; Jansons, P.; Scott, D.; Daly, R.M. Feasibility and acceptability of a remotely delivered, home-based, pragmatic resistance “exercise snacking” intervention in community-dwelling older adults: a pilot randomised controlled trial. BMC Geriatr. 2022, 22, 521. [Google Scholar] [CrossRef] [PubMed]
- Liang, I.J.; Perkin, O.J.; McGuigan, P.M.; Thompson, D.; Western, M.J. Feasibility and Acceptability of Home-Based Exercise Snacking and Tai Chi Snacking Delivered Remotely to Self-Isolating Older Adults During COVID-19. J Aging Phys Act. 2022, 30, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Liang, I.J.; Francombe-Webb, J.; McGuigan, P.M.; Perkin, O.J.; Thompson, D.; Western, M.J. The acceptability of homebased exercise snacking and Tai-chi snacking amongst high and low function UK and Taiwanese older adults. Front Aging. 2023, 4, 1180939. [Google Scholar] [CrossRef] [PubMed]
- Western, M.J.; Welsh, T.; Keen, K.; Bishop, V.; Perkin, O.J. Exercise snacking to improve physical function in pre-frail older adult memory clinic patients: a 28-day pilot study. BMC Geriatr. 2023, 23, 471. [Google Scholar] [CrossRef]
- Jenkins, E.M.; Nairn, L.N.; Skelly, L.E.; Little, J.P.; Gibala, M.J. Do stair climbing exercise “snacks” improve cardiorespiratory fitness? Appl Physiol Nutr Metab. 2019, 44, 681–684. [Google Scholar] [CrossRef]
- Logan BK, Larsen R, Sacre JW, Cohen ND, Lambert GW, Wheeler, M.J.; et al. Interrupting prolonged sitting reduces postprandial GIP but not GLP-1 responses in type 2 diabetes. Diabetes Obes Metab.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow, C.D.; et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021, 10, 89. [CrossRef]
- Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ.; et al., editors. Cochrane Handbook for Systematic Reviews of Interventions [Internet]. 1st ed. Wiley; 2019 [cited 2025 Oct 4]. Available from: https://onlinelibrary.wiley.com/doi/book/10.1002/9781119536604.
- Brunton, G.; Stansfield, C.; Thomas, J. Finding relevant studies. An Introduction to Systematic Reviews. 2012, 107–134. [Google Scholar]
- Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron, I.; et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019, 366, l4898.
- Wells G, Wells G, Shea B, Shea B, O’Connell D, Peterson, J.; et al. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. In 2014 [cited 2025 Oct 4]. Available from: https://www.semanticscholar.org/paper/The-Newcastle-Ottawa-Scale-(NOS)-for-Assessing-the-Wells-Wells/c293fb316b6176154c3fdbb8340a107d9c8c82bf.
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis [Internet]. 1st ed. Wiley; 2009 [cited 2025 Oct 4]. Available from: https://onlinelibrary.wiley.com/doi/book/10.1002/9780470743386.
- Deeks JJ, Higgins JP, Altman DG, on behalf of the Cochrane Statistical Methods Group. Analysing data and undertaking meta-analyses. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ.; et al., editors. Cochrane Handbook for Systematic Reviews of Interventions [Internet]. 1st ed. Wiley; 2019 [cited 2025 Oct 4]. p. 241–84. Available from: https://onlinelibrary.wiley.com/doi/10.1002/9781119536604.ch10.
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Brakenridge CJ, Gardiner PA, Grigg RV, Winkler EAH, Fjeldsoe BS, Schaumberg, M.A.; et al. Sitting less and moving more for improved metabolic and brain health in type 2 diabetes: ‘OPTIMISE your health’ trial protocol. BMC Public Health. 2022, 22, 929.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



