
Submitted:
24 October 2025
Posted:
29 October 2025
You are already at the latest version
Abstract
Background/Objectives: Allergen immunotherapy (AIT) with chemically modified allergoids represents a promising approach for the treatment of allergic rhinoconjunctivitis. This post-hoc analysis investigated the clinical efficacy of a mannan-conjugated birch pollen allergoid (T502) by comparing outcomes in patients who received placebo in one pollen season and active treatment in the following year. Methods: Data were derived from four randomized clinical trials (EudraCT Numbers. 2018-002522-23, 2020-004126-32, 2021-002252-36, 2022-004082-20) conducted over four consecutive years. Two independent patient groups were analyzed, each receiving placebo in the first year and subcutaneous T502 (10,000 mTU/mL) in the subsequent year. Daily symptom score (dSS), daily medication score (dMS), and combined symptom and medication score (CSMS) were assessed during the birch pollen season each April. Results: In the first comparison between 2020 and the early start in January 2021, treatment with T502 led to a 43.79% reduction in dSS (p = 0.000), a 71.43% reduction in dMS (p = 0.001), and a 42.1% reduction in CSMS (p = 0.001), all statistically significant. In the second comparison between 2022 and a late start in March 2023, the reduction in dMS was 74.47% (p = 0.001), whereas reductions in dSS (1.47%, p = 0.898) and CSMS (20.3%, p = 0.057) were not statistically significant. Conclusions: Subcutaneous immunotherapy (SCIT) with T502 significantly reduces allergic symptoms and medication use, particularly when all injections are completed before the onset of the birch pollen season in April. These findings highlight both the clinical value of T502 and the importance of optimized treatment timing.
Keywords:
birch pollen allergy
; AIT
; mannan-conjugated birch pollen allergoid
; SCIT
; combined symptom and medication score
; CSMS
1. Introduction
Birch pollen (Betula) allergy is the most widespread tree pollen allergy in regions such as Northern and Central Europe [1,2] and also important in China [3]. Sensitization to birch pollen affects approximately 8% to 16% of the European population, with regional differences in prevalence [2]. Recent studies indicate a rising prevalence of allergic rhinitis, especially in regions where it was previously less widespread [4]. The development of allergic rhinitis is likely the result of multiple factors, including genetic predisposition [5,6].
Allergic rhinitis (AR) is primarily triggered by an immunoglobulin E (IgE)-mediated hypersensitivity reaction following allergen exposure [7]. The condition was first defined in 1929 by its three cardinal symptoms: sneezing, nasal congestion, and mucus secretion [8]. Beyond the physical symptoms, AR can significantly affect social life, academic performance, and work productivity [9,10].
Effective management is therefore essential—not only to alleviate symptoms but also to address associated or complicating respiratory conditions such as asthma, sinusitis, and sleep apnea [11]. In addition to pollen avoidance, which is not always possible, anti-allergic medications are commonly used to alleviate allergy symptoms [12]. However, they require continuous use for as long as symptoms persist—often lifelong [13]. Unlike symptomatic therapies, AIT remains the only disease-modifying approach for allergic respiratory conditions [14,15,16].
One challenge of AIT is poor patient adherence [17], as the treatment requires numerous injections over 3-5 months and continuation of administration for at least three years is advised [18]. A study by Scadding et al. (2017) examined a two-year course of either subcutaneous or sublingual grass pollen immunotherapy but found no sustained long-term benefit [19]. Supporting the benefit of a treatment duration of at least three years, a study by Durham et al. showed that three to four years of grass pollen immunotherapy led to long-term clinical remission and sustained immunologic changes, with symptom and medication scores remaining low even after discontinuation [20].
Side effects can occur with the initial doses, often leading to early discontinuation [21]. These limitations highlight the urgent need for safer and more effective AIT to improve patient compliance and therapeutic outcomes [22].
To optimize the efficacy of AIT and shorten treatment duration, allergens modified with glutaraldehyde or formaldehyde, known as allergoids, have been developed [23]. This modification improves immunogenicity properties by reacting with primary amino groups in the polypeptide chain of the allergen to form high molecular weight cross-linked polymers. This inactivates the conformational IgE epitopes while preserving the linear T-cell epitopes [21,24]. This structure allows the administration of high doses during a short accumulation phase [21,25]. The efficacy of allergoids has been further enhanced by combining them with adjuvants such as mannan, a polymannose backbone derived from yeast, a natural ingredient of bread and beer, to which subjects are exposed to everyday life [25,26]. An adjuvant is a molecule that amplifies the immune response through physical or chemical interaction with antigens [21,27]. In this context, allergoids are conjugated to non-oxidized mannan—typically using glutaraldehyde as a cross-linker—which enables targeted delivery to dendritic cells via C-type lectin receptors. This targeted approach aims to increase the bioavailability of the administered dose [22].
T502 is a mannan-conjugated birch pollen allergoid consisting of a glutaraldehyde-polymerized birch pollen extract coupled to mannan from Saccharomyces cerevisiae. In the first human trial (T502-SIT-020) all tested doses were found to be safe, however, 10,000 mTU, the highest dose tested (mannan therapeutic units)/mL demonstrated the highest efficacy and was therefore selected for subsequent studies [28].
This study analyzes four studies on AIT with T502. The focus is on patients who received placebo in one year and active therapy in the next. Symptom improvement and medication use are assessed. Notably, the former study administered AIT partly during the birch pollen season, allowing – in addition – the comparison with only pre-seasonal treatments in the earlier studies. This might enable conclusions on the optimal timing of therapy.
2. Materials and Methods
2.1. T502-SIT-020 Study (EudraCT Number: 2018-002522-23) [28].
Conducted in 2020, this phase II, randomized, double-blind, placebo-controlled dose-finding study evaluated the safety and efficacy of pre-seasonal subcutaneous immunotherapy with mannan-conjugated birch pollen allergoids (T502) in patients with birch pollen-induced allergic rhinoconjunctivitis (ARC).
Patients received one of three T502 concentrations (1,000 (n=62) / 3,000 (n=62)/ 10,000 (n=61) mTU/mL) or placebo (n=61). Symptoms and medication use during the pollen season were analyzed.
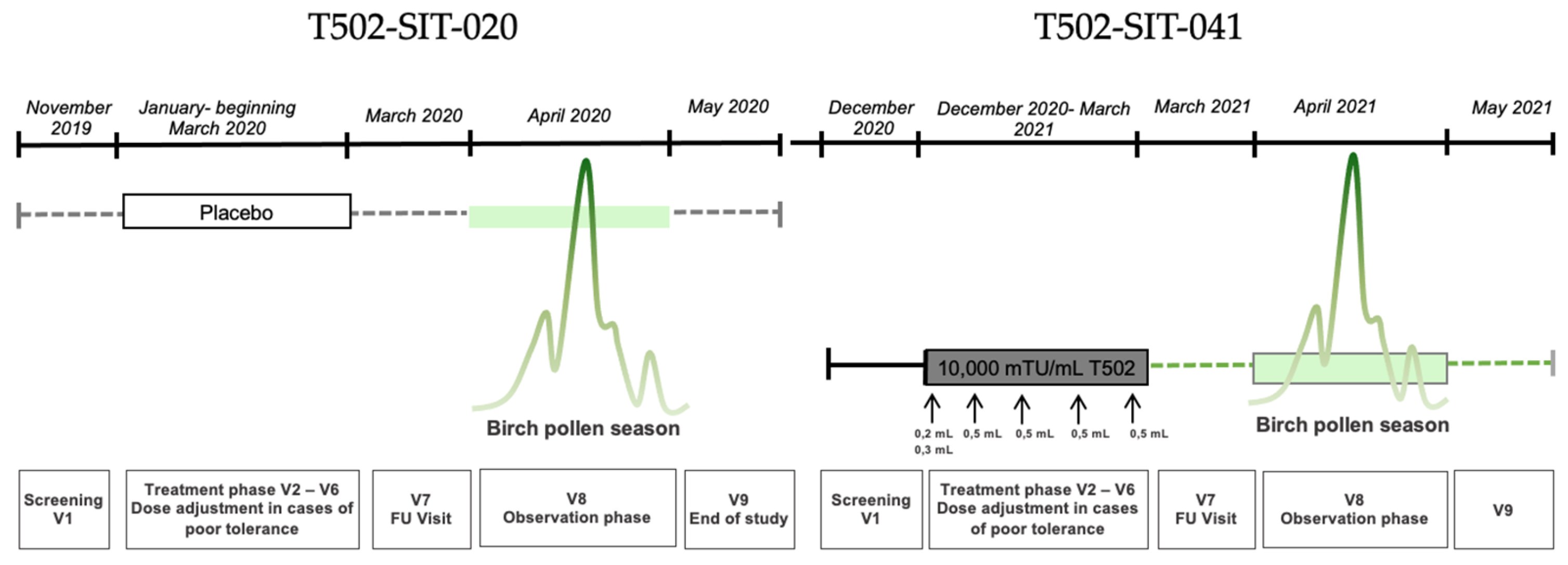
The study included nine visits: one screening, five pre-seasonal treatment visits, one follow-up, and two visits during and after the peak pollen season. Subcutaneous injections were administered at intervals of 7 to 30 days between visits V2 and V6, prior to the pollen season. Each dose consisted of 0.5 mL, divided into two injections during the first visit: 0.2 mL in one arm and 0.3 mL in the other after a 30-minute interval. In total, 246 patients were randomized into one placebo group and three active treatment groups with different T502 concentrations.
Figure 1.
Study design for a patient with placebo in the T502-SIT-020 study in 2020 with nine visits and treatment afterwards in the T502-SIT-041 study in 2021 with nine visits.
Figure 1.
Study design for a patient with placebo in the T502-SIT-020 study in 2020 with nine visits and treatment afterwards in the T502-SIT-041 study in 2021 with nine visits.
V1-V9.
2.2. T502-SIT-041 Study (EudraCT Number: 2020-004126-32)
This open-label phase II follow-up study, conducted in 2021-2024, included patients from the previous T502-SIT-020 study. For this study presented here, only the first year of treatment (2021) of patients having received placebo was analyzed. All participants received the recommended dose of 10,000 mTU/mL T502, regardless of their prior group assignment.
Nine visits were scheduled in the first year of the study: one screening, five pre-seasonal treatment visits, one follow-up, and two visits during and after the peak pollen season. During pre-seasonal treatment, patients received five subcutaneous injections of 10,000 mTU/mL T502 at two-week intervals (±6 days). At the first visit, the 0.5 mL dose was split into two injections; at subsequent visits, it was administered as a single injection. Between December 2020 and May 2021, a total of 154 patients from the T502-SIT-020 study were treated with T502 in this open-label trial.
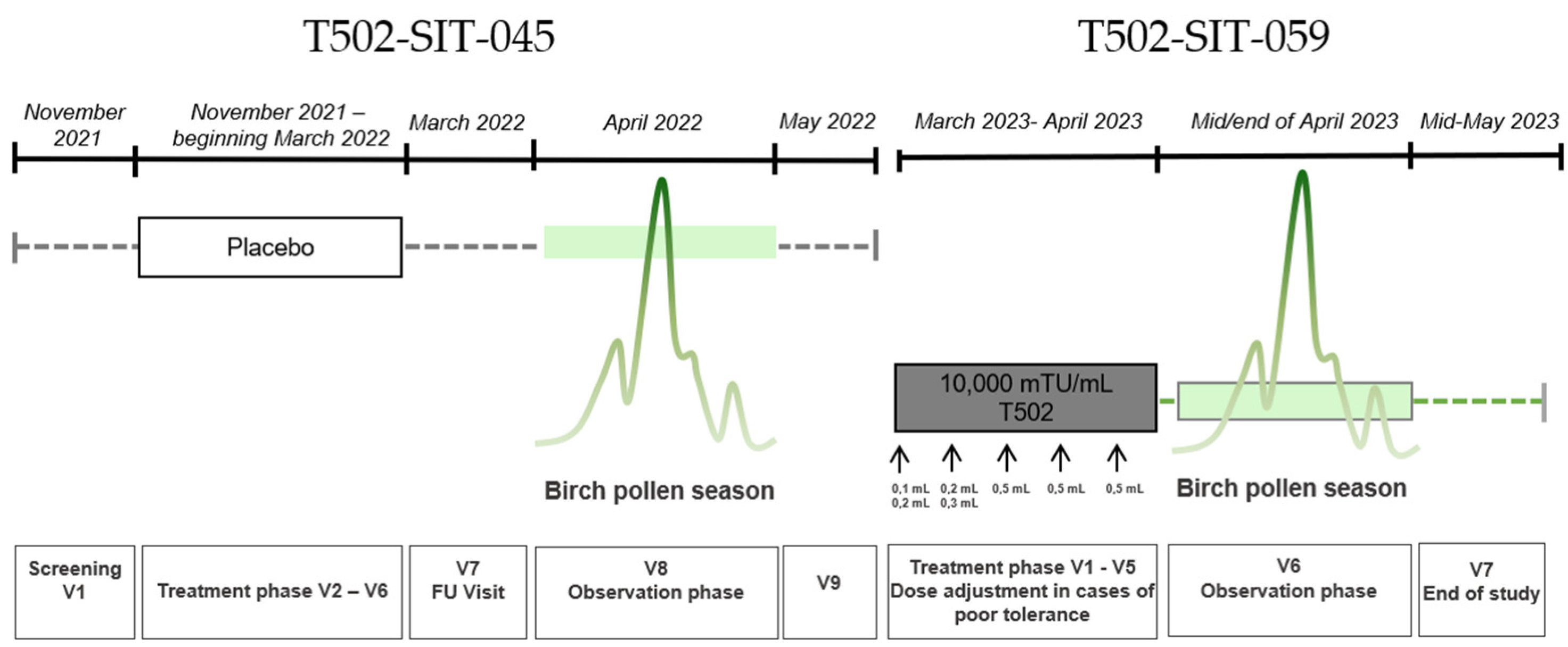
Figure 2.
Study design for a patient with placebo in the T502-SIT-045 study in 2022 with nine visits V1-V9 and treatment afterwards in the T502-SIT-059 study in 2023 with seven visits.
Figure 2.
Study design for a patient with placebo in the T502-SIT-045 study in 2022 with nine visits V1-V9 and treatment afterwards in the T502-SIT-059 study in 2023 with seven visits.
2.3. T502-SIT-045-Study (EudraCT-Number: 2021-002252-36)
The T502-SIT-045 study (2022) was a prospective, randomized, double-blind, placebo-controlled, multicenter phase III trial evaluating the efficacy of subcutaneous T502 (10,000 mTU/mL) in patients with birch pollen-induced ARC. A total of 298 patients were randomized to receive either T502 (n=199) or placebo (n=99) prior to the birch pollen season. Treatment was administered as follows: 1st treatment visit: 0.1 + 0.2 mL, 2nd treatment visit: 0.2 + 0.3 mL, all other treatment visits: 0.5 mL across five preseasonal visits with split dosing at the first two visits based on prior study protocols. For this study presented here, only the placebo patients were analyzed. Symptoms and medication use were assessed during the peak birch pollen season.
2.4. T502-SIT-059-Study (EudraCT-Number: 2022-004082-20)
The T502-SIT-059 study (2023) was an open-label phase III follow-up trial in patients previously treated in the T502-SIT-045 study. All participants received subcutaneous T502 (10,000 mTU/mL) to evaluate its continued clinical efficacy. A total of seven visits were conducted, five treatment visits and two during and after the birch pollen season respectively. Treatment was administered as follows: 1st treatment visit: 0.1 + 0.2 mL, 2nd treatment visit: 0.2 + 0.3 mL, all other treatment visits: 0.5 mL across five visits with split dosing during the first two visits. Symptoms and medication use during the 2023 birch pollen season were compared to individual results from the 2022 season. The study aimed to provide all patients with active treatment and assess year-over-year improvements in allergic symptom control.
2.5. Endpoints
During the birch pollen season, patients in the T502-SIT-020 and T502-SIT-041 studies recorded their dSS and dMS using the mobile app CSMS+. For the T502-SIT-045 and T502-SIT-059 studies, the CSMS+ app was used.
The dSS used for all 4 studies included six symptoms: four nasal (rhinorrhea, sneezing, nasal itching, nasal congestion) and two ocular symptoms (ocular itching, watery eyes). Each symptom was rated daily using a 4-point ordinal scale:
0 = no symptoms
1 = mild symptoms (clearly present but minimal perception; easy to tolerate)
2 = moderate symptoms (clearly bothersome but tolerable)
3 = severe symptoms (difficult to tolerate; interferes with daily activities and/or sleep).
The six symptom scores were summed and divided by six to calculate the dSS, resulting in a score between 0 and 3.
The dMS reflected the highest level of medication used per day. Initially, for the T502-SIT-020 and T502-SIT-041 studies a stepwise approach was defined as follows:
0 = no medication
1 = use of antihistamine tablets
2 = use of nasal corticosteroids (with or without antihistamines)
3 = use of oral corticosteroids (with or without nasal corticosteroids and antihistamines).
The CSMS was calculated by adding dSS and dMS: CSMS = dSS (0–3) + dMS (0–3), resulting in a range from 0 to 6 [29].
In the T502-SIT-045 and T502-SIT-059 studies, an expanded additive version of the dMS was introduced for improved differentiation, given that the use of oral corticosteroids was reported in less than 1% of patients in the previous studies [30]:
0 = no medication
0.5 = antihistamine eye drops
1 = antihistamine tablets
1.5 = nasal corticosteroids.
2.6. Patient Groups
For this analysis, patient identification numbers of all individuals who received placebo treatment in 2020 (T502-SIT-020) or 2022 (T502-SIT-045) and subsequently participated in the follow-up studies (T502-SIT-041 and T502-SIT-059, respectively) the following year were compiled. The focus was on comparing their CSMS, dSS, and dMS for the month of April in each year.
The dSS and dMS were recorded daily via an electronic patient diary and used to calculate the CSMS. This yielded in 30 daily values per patient for each score during April. These were averaged to obtain one monthly value per patient for dSS, dMS, and CSMS. Each patient’s monthly value from the placebo year was then compared to their corresponding value in the following treatment year.
In total, 32 patients who received placebo in T502-SIT-020 and active treatment in T502-SIT-041 were identified, forming the T502-SIT-020- T502-SIT-041 comparison group. For the comparison, individual CSMS, dSS, and dMS values were analyzed. Similarly, 32 patients from the T502-SIT-045 placebo group who received AIT in T502-SIT-059 were included in the T502-SIT-045 – T502-SIT-059 comparison group. For this comparison, mean values for dSS and the additive dMS were used to calculate the CSMS, based on the additive scoring system introduced in 2022.
2.7. Statistical Analysis
Statistical analysis was performed using SPSS in version 30 (Armonk, New York USA). For the evaluation of continuous variables, the median, mean, minimum, maximum, standard deviation and quartiles were calculated. Two statistical tests were applied to assess significance, with the threshold for statistical significance set at α = 0.05.
In cases of normally distributed data, the mean was used as the central tendency measure, and statistical significance was determined using the t-test. For data that did not meet the assumption of normality, the median was used, and significance was assessed using the Wilcoxon signed-rank test.
3. Results
3.1. Patients
A total of 64 patients were analyzed in two groups of 32 patients each. This resulted in a group of 32 patients for the combination of T502-SIT-020 to T502-SIT-041 in the years 2020 and 2021 and a group of 32 participants for the second combination between T502-SIT-045 to T502-SIT-059 in the years 2022 and 2023.
3.2. Combined Symptom and Medication Score
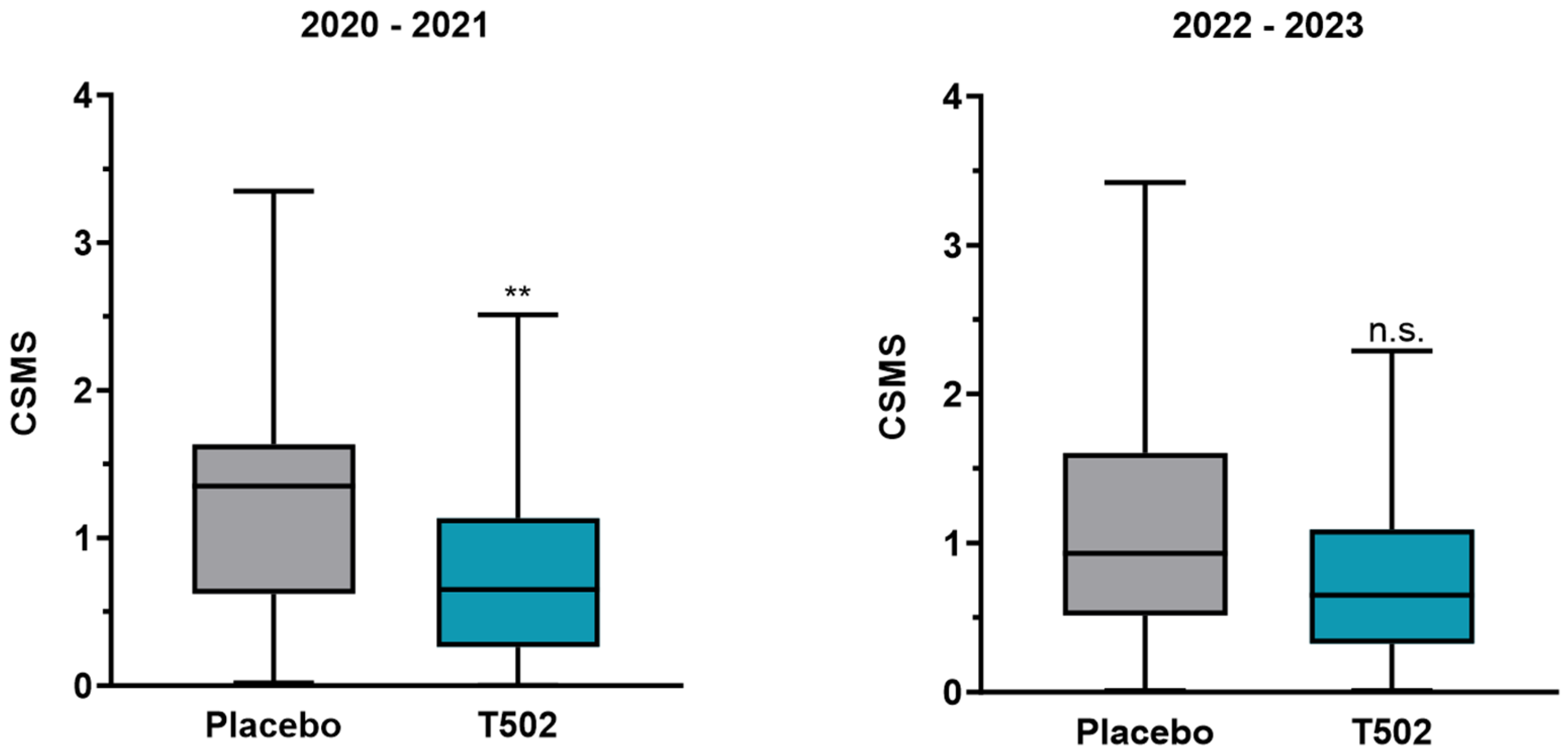
The CSMS showed a clear treatment effect in the comparison between T502-SIT-020 and T502-SIT-041, with the mean CSMS decreasing significantly by 42.1%, from 1.31 to 0.784 (t-test p = 0.001).
In the second comparison between T502-SIT-045 and T502-SIT-059, the mean CSMS decreased by 20.3%, from 0.95 to 0.7572 (Table S1), but this change did not reach statistical significance (t-test p = 0.057).
Figure 3.
The mean±SD CSMS development of: Left panel – patients with placebo in the T502-SIT-020 study in 2020 and treatment in the T502-SIT-041 study in 2021; Right panel – patients with placebo in the T502-SIT-045 study in 2022 and treatment in the T502-SIT-059 study in 2023. ** - p = 0.001, n.s. – non significant.
Figure 3.
The mean±SD CSMS development of: Left panel – patients with placebo in the T502-SIT-020 study in 2020 and treatment in the T502-SIT-041 study in 2021; Right panel – patients with placebo in the T502-SIT-045 study in 2022 and treatment in the T502-SIT-059 study in 2023. ** - p = 0.001, n.s. – non significant.
3.3. Daily Symptom Score
A significant reduction in dSS was observed in patients who received T502 in the year following placebo treatment in the T502-SIT-020 and T502-SIT-041 studies, with the median decreasing by 43.79% (Table S2) (p = 0.001).
In contrast, the comparison between the T502-SIT-045 and T502-SIT-059 studies showed no meaningful change, with a non-significant reduction of 1.47% in the mean dSS (t-test p = 0.898) (Figure 4).
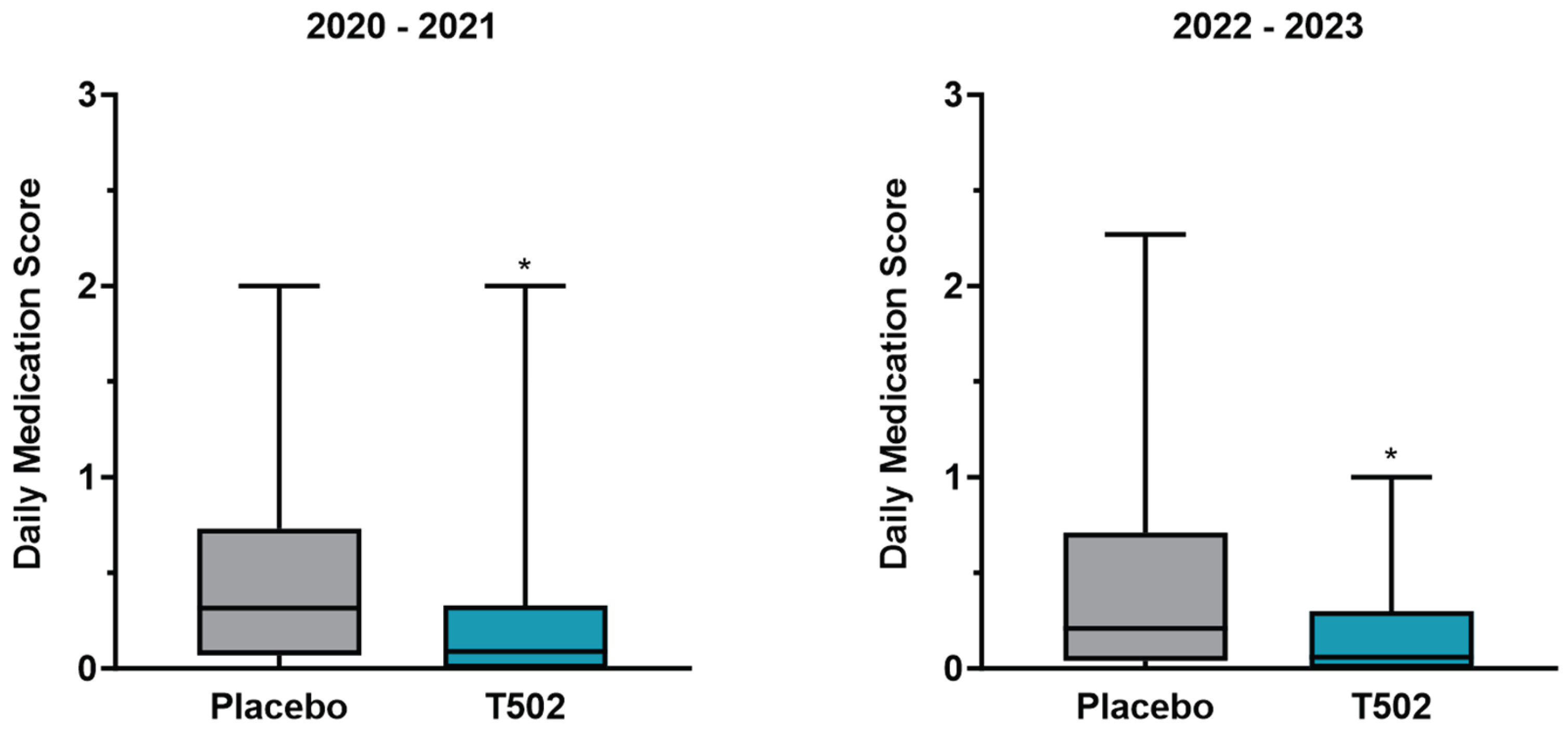
3.4. Daily Medication Score
The dMS showed a statistically significant reduction following treatment with T502 in both study comparisons (Table S3). In the comparison between T502-SIT-020 and T502-SIT-041, the median dMS was reduced by 71.43%, from 0.315 to 0.09 (Wilcoxon p = 0.001) (Figure 5). In the second comparison, between T502-SIT-045 and T502-SIT-059, treatment with T502 led to a 74.47% decrease in the median dMS, from 0.235 to 0.06 (Wilcoxon p = 0.001) (Table S4).
4. Discussion
According to the World Allergy Organization (WAO), an additional efficacy lower than that achieved with antihistamines is considered insufficient. Therefore, a minimum clinically relevant effect must demonstrate at least a 20% improvement over placebo [31].
Taken together with the reductions in dSS and dMS, the CSMS provides a comprehensive measure of treatment efficacy. In the present analysis, the first comparison (T502-SIT-020 to T502-SIT-041) demonstrated a pronounced CSMS reduction of 42.1%. In contrast, the second comparison (T502-SIT-045 to T502-SIT-059) showed a reduction of 20.3%, which did not reach statistical significance. This discrepancy appears to be primarily driven by differences in symptom scores, as medication use declined similarly in both groups. These results underscore the importance of treatment timing. Due to the late start of the T502-SIT-059 study with a treatment end during the birch pollen season, patient’s immune system had not enough time to develop tolerance. In T502-SIT-020 study it was shown that full effect was only seen in patients receiving their last injection before March, thus one month before the onset of the birch pollen season [28]. In a study by Pfaar et al. (2018), the primary endpoints after 3 to 6 months of sublingual immunotherapy (SLIT) treatment showed a significant and clinically relevant reduction in CSMS of 32% compared to placebo [16]. Similar results were reported in a 2013 study by Pfaar et al. on SCIT with a mixed depigmented-polymerised birch and grass pollen extract, where a 33.7% lower CSMS was observed in the second treatment year compared to placebo [32].
The dSS showed a statistically significant median reduction of 43.79% in the first comparison (T502-SIT-020 to T502-SIT-041). Gallego et al. also reported that AIT using depigmented, glutaraldehyde-modified allergens is highly effective in allergy treatment, demonstrating a 54% reduction in symptom scores compared to placebo [33]. A similarly high effect was observed in the present analysis. Whereas the observed mean improvement of 1.47% in the second comparison was minimal and not statistically significant. One possible explanation is the timing of treatment, as injections in the T502-SIT-059 study were partly administered during April, which may have prevented the AIT from developing its full effect in time before the start of the birch pollen season.
In contrast to the variability observed in symptom scores, the dMS showed a consistent and substantial reduction in both comparisons. A median decrease of 71.43% was observed in the first group, and an even greater median reduction of 74.47% in the second. These findings underline the therapeutic benefit of T502, particularly in reducing the need for medication across different treatment conditions.
In comparison, Biedermann et al. (2019) found a similar effect on SLIT for ARC caused by tree pollen: differences of 37% in the dSS and 49% in the dMS were reported between the treatment and placebo groups [12]. Consistently the symptom reduction between T502-SIT-020 and T502-SIT-041 reached 43.79%, thereby exceeding the effect observed by Biedermann et al.
4.1. Limitations
A methodological limitation is the use of different statistical measures: use of the median due to the non-normal distribution in one endpoint, while for the endpoints with normal distribution the mean value was used, which can be found in the comparison of the dSS (Table S4).
The CSMS has inherent limitations that concern both components of the score. The assessment of symptoms is influenced by individual differences in allergen exposure, variability in daily symptom burden, and the retrospective nature of symptom reporting [34]. Similarly, the evaluation of daily medication intake within the CSMS can be limited by insufficient differentiation of medication types and usage patterns. To address this, the second comparison in the present analysis applied the previously described additive CSMS approach, allowing for greater granularity in scoring. This may impact direct comparability between study groups. The use of such additive models has been recommended by Pfaar et al. [35] for future trials. Nonetheless, further research is needed to explore and validate additional clinical parameters to establish the most appropriate and reliable outcome measures for assessing AIT efficacy in clinical settings [36].
4.2. Covid-19
It is noteworthy that the use of face masks and the reduction in air pollution during COVID-19 lockdowns are considered potential factors in alleviating symptoms of AR [37,38]. Face masks not only reduce pathogen exposure but also limit inhalation of airborne allergens such as pollen (10–100 µm), which are key triggers of IgE-mediated allergic responses. Surgical masks can filter particles as small as 3 µm, while N95 masks provide even greater protection, retaining particles down to 0.04 µm [38]. A study by Mengi et al. [39] showed that face mask use significantly reduced nasal symptoms in pollen allergy sufferers, with a 36% decrease in moderate to severe complaints.
Since all four studies took place in April of different years, variations in mask usage or pandemic-related behavioral changes between years could have influenced dMS, dSS, or CSMS outcomes and may represent relevant confounding factors. It was also shown that the pandemic had an impact on AR treatment [40,41].
4.3. Conclusions for the Future
The analyses of this study allow for several conclusions, which may be of relevance for future research. The data suggest that symptom development is more sensitive to the timing of AIT, with delayed administration resulting in a less pronounced reduction in symptoms. In contrast, the reduction in medication use appears robust even when treatment begins later, with only minimal differences between the comparison groups, with only 3.04%. This indicates that a considerable clinical benefit—particularly in terms of reduced medication need—can still be achieved even with a delayed treatment start.
Nonetheless, the greatest improvement in CSMS appears to occur when there is sufficient time between the initiation of AIT and the onset of the pollen season. Further studies are required to determine the optimal timing of T502 administration. It should also be noted that external factors, such as behavioral changes during the COVID-19 pandemic, may have influenced the results and should be more thoroughly addressed in future investigations.
Overall, the results from both comparison groups demonstrate that treatment with T502 leads to improvements, reflected in a significant reduction of allergic symptoms in the first group and a reduced need for medication in both groups. This translates into a meaningful improvement in quality of life for patients during the pollen season [42] already after the first year of treatment and highlights T502 as a valuable therapeutic option for pollen allergy.
5. Conclusions
This study demonstrates the therapeutic potential of T502 AIT in birch pollen-induced ARC. While symptom scores proved more sensitive to treatment timing, medication scores showed robust improvement regardless of the injection schedule, underscoring the clinical benefit of T502 even with a delayed onset shortly before the start of the birch pollen season.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Descriptive statistics of the CSMS for the studies T502-SIT-020, T502-SIT-041, T502-SIT-045 and T502-SIT-059 with mean/median reduction from T502-SIT-020 to T502-SIT-041 or T502-SIT-045 to T502-SIT-059; Table S2: Descriptive statistics of the dSS for the studies T502-SIT-020, T502-SIT-041, T502-SIT-045 and T502-SIT-059 with mean/median reduction from T502-SIT-020 to T502-SIT-041 or T502-SIT-045 to T502-SIT-059; Table S3: Descriptive statistics of the dMS for the studies T502-SIT-020, T502-SIT-041, T502-SIT-045 and T502-SIT-059 with mean/median reduction from T502-SIT-020 to T502-SIT-041 or T502-SIT-045 to T502-SIT-059; Table S4: Significance tests with t-test for normally distributed data or Wilcoxon test for non-normally distributed data.
Author Contributions
Conceptualization, S.P., N.W., E.R., S.A., C.A., J.L.S., M.C.V., M.C., R.M. and O.P.; methodology, C.A., R.M. and O.P.; validation, R.M., H.S., S.A., A.R., S.P., J.L.S., M.C.V. and O.P.; formal analysis, C.A., H.S., M.C., N.W.; investigation, E.R.; resources, S.A., M.C.V. and J.L.S. data curation, H.S., N.W.; writing—original draft preparation, N.W., A.R., E.R. and R.M.; writing—review and editing, R.M., S.A., M.C., A.R., H.S., N.W., E.R., S.P., M.C.V., J.L.S. and O.P.; visualization, R.M., A.R. and N.W.; supervision, R.M., S.A., S.P., M.C.V., J.L.S., E.R. and N.W.; project administration, R.M., S.A., E.R., N.W. and S.P.; funding acquisition, R.M, S.A., M.C.V. and J.L.S. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. All authors have read and agreed to the published version of the manuscript.
Funding
These studies were funded by Inmunotek SL, Spain.
Institutional Review Board Statement
The studies were conducted in accordance with the Declaration of Helsinki, and it were carried out in accordance with the German Medicinal Products Act (Arzneimittelgesetz, AMG), Section 67, Subsection 6. For the T502-SIT-020 study, the independent ethics committee gave initial positive vote of the study on 09/NOV/2018, The study protocol was submitted in 2019 to the competent regulatory authority (Paul-Ehrlich-Institut) under the number 3695/01. Approval was given on 22/AUG/2019. For the T502-SIT-041 study, the independent ethics committee gave initial positive vote of the study on 01/DEC/2020. The study protocol was submitted in 2020 to the competent regulatory authority (Paul-Ehrlich-Institut) under the number 4244/01. Approval was given on 18/DEC/2020. For the T502-SIT-045 study, the independent ethics committee gave initial positive vote of the study on 27/SEP/2021. The study protocol was submitted in 2021 to the competent regulatory authority (Paul-Ehrlich-Institut) under the number 4564/01. Approval was given on 27/OCT/2021. For the T502-SIT-059 study, the independent ethics committee gave initial positive vote of the study on 21/FEB/2023. The study protocol was submitted in 2023 to the competent regulatory authority (Paul-Ehrlich-Institut) under the number 5190/01. Approval was given on 07/MAR/2023.
Informed Consent Statement
All patients gave written informed consent before study inclusion.
Data Availability Statement
Upon reasonable request, data will be available from the corresponding author.
Acknowledgments
The authors are grateful to participating trial sites and their patients.
Conflicts of Interest
S.P. is an employee of Inmunotek, J.L.S and M.C.V. are shareholders of Inmunotek. R.M. reports grants and personal fees from Inmunotek during the conduct of the trial; personal fees from ALK, grants from ASIT biotech, personal fees from Allergopharma, personal fees from Allergy Therapeutics, grants and personal fees from Bencard, grants from Leti, grants, personal fees and non-financial support from Lofarma, non-financial support from Roxall, grants and personal fees from Stallergenes, grants from Optima, personal fees from Friulchem, personal fees from Hexal, personal fees from Servier, personal fees from Klosterfrau, non-financial support from Atmos, personal fees from Bayer, non-financial support from Bionorica, personal fees from FAES, personal fees from GSK, personal fees from MSD, personal fees from Johnson&Johnson, personal fees from Meda, personal fees and non-financial support from Novartis, non-financial support from Otonomy, personal fees from Stada, personal fees from UCB, non-financial support from Ferrero, grants from Hulka, personal fees from Nuvo, grants and personal fees from Ursapharm, personal fees from Menarini, personal fees from Mundipharma, personal fees from Pohl-Boskamp, grants from Cassella-med GmbH & Co. KG, personal fees from Laboratoire de la Mer, personal fees from Sidroga, grants and personal fees from HAL BV, personal fees from Lek, personal fees from PRO-AdWise, personal fees from Angelini Pharma, grants and non-financial support from JGL, grants and personal fees from bitop, grants from Sanofi, personal fees from Menarini, outside the submitted work; MC declares honoraria for presentations from ALK-Abelló, Allergopharma, AstraZeneca, Bencard Allergie/ Allergy Therapeutics, GalaxoSmithKline, HAL Allergy, Leti Pharma, Novartis, Roxall, Sanofi-Aventis, Stallergenes outside the submitted work. Other non-financial interests: Member of German Society of Allergy (AeDA) and German Society of Oto-Rhino-Laryngology, Head and Neck Surgery DGHNO-KHC. Coordinating investigator of the present clinical trial; O.P. reports grants for his institution during the conduct of the trial from Inmunotek S.L., Spain, and he reports grants and/or personal fees and/or travel support from AEDA, Alfried Krupp Krankenhaus, ALK-Abelló, Allergopharma, Almirall, Altamira Therapeutics, ASIT Biotech, AstraZeneca, Bencard Allergie GmbH/Allergy Therapeutics, Blueprint, Breazy Health, Cliantha, Deutsche AllergieLiga e.V., Deutsche Forschungsgemeinschaft, Dustri-Verlag, ECM Expro&Conference Management GmBH, Forum für Medizinische Fortbildung, Georg-Thieme-Verlag, GSK, HAL Allergy Holding B.V./HAL Allergie GmbH, Inmunotek, Ingress Health, Institut für Disease Management, IQVIA Commercial, Japanese Society of Allergology, Königlich Dänisches Generalkonsulat, Laboratorios LETI/LETI Pharma, Lilly, Lofarma, Medizinische Hochschule Hannover, med update europe GmbH, Meinhardt Congress GmbH, Novartis, Paul-Ehrlich-Institut, Paul-Martini-Stiftung, PneumoLive, Pohl-Boskamp, Procter & Gamble, Red Maple Trials Inc., Regeneron, RG Aerztefortbildung, ROXALL Medizin, Sanofi Aventis, Sanofi Genzyme, Springer Publisher, Stallergenes Greer, streamedup! GmbH, Technical University Dresden, John Wiley & sons publishers, Wort & Bild Verlag, Verlag ME; all outside the submitted work, Oliver Pfaar is Vice President of the European Academy of Allergy and Clinical Immunology (EAACI), a member of EAACI Excom as well as a member of the external board of directors of the German Society of Allergy and Clinical Immunology (DGAKI); coordinator, main- or co-author of different position papers and guidelines in rhinology, allergology and allergen-immunotherapy; and he is Editor-in-Chief of Clinical Translational Allergy and Associate Editor of Allergy; SZ reports grants and personal fees from Inmunotek during the conduct of the trial; grants from Palas GmbH, grants and personal fees from Allergy Therapeutics GmbH, grants and personal fees from Böhringer Ingelheim, personal fees from Novartis GmbH, personal fees from Lofarma GmbH, personal fees from IMS HEALTH GmbH & Co. OHG, personal fees from GSK, personal fees from Stallergenes, personal fees from Engelhard Arzneimittel, personal fees from Sanofi-Pasteur, personal fees from AstraZeneca, personal fees from Erydel, outside the submitted work. N.W., E.R., A.R., C.A., H.S. and S.A. have nothing to disclose.
Abbreviations
| AIT | Allergen-specific immunotherapy |
| AR | Allergic Rhinitis |
| ARC | Allergic Rhinoconjunctivitis |
| COVID-19 | Coronavirus disease 2019 |
| CSMS | Combined symptom and medication score |
| dMS | Daily medication score |
| dSS | Daily symptom score |
| IgE | Immunoglobulin E |
| mTU | Mannan therapeutic units |
| p | (p-value) value for significance |
| SCIT | Subcutaneous Immunotherapy |
| SLIT | Sublingual immunotherapy |
| SPSS | Statistical Package for the Social Sciences |
| V | Visit |
| WAO | World Allergy Organisation |
References
- Novak, N.; Worm, M.; Staubach, P.; Jutel, M.; Sager, A.; Pfaar, O. Subcutaneous birch pollen allergen immunotherapy with a depigmented polymerized extract shows only sustained and long-term efficacy in a subgroup of monosensitized adults and adolescents with allergic rhinitis. Clin Transl Allergy 2022, 12, e12185. [Google Scholar] [CrossRef]
- Biedermann, T.; Winther, L.; Till, S.J.; Panzner, P.; Knulst, A.; Valovirta, E. Birch pollen allergy in Europe. Allergy 2019, 74, 1237–1248. [Google Scholar] [CrossRef]
- Ouyang, Y.; Yang, J.; Zhang, J.; Yan, Y.; Sun, S.; Wang, J.; Li, X.; Chen, R.; Zhang, L. Airborne pollen exposure and risk of hospital admission for allergic rhinitis in Beijing: A time-stratified case-crossover study. Clin Transl Allergy. 2024, 14, e12380. [Google Scholar] [CrossRef]
- Brożek, J.L.; Bousquet, J.; Agache, I.; Agarwal, A.; Bachert, C.; Bosnic-Anticevich, S.; Brignardello-Petersen, R.; Canonica, G.W.; Casale, T.; Chavannes, N.H.; et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines—2016 revision. Journal of Allergy and Clinical Immunology 2017, 140, 950–958. [Google Scholar]
- Rosewich, M.; Lee, D.; Zielen, S. Pollinex Quattro: an innovative four injections immunotherapy in allergic rhinitis. Human vaccines & immunotherapeutics 2013, 9, 1523–1531. [Google Scholar]
- Meng, Y.; Wang, C.; Zhang, L. Recent developments and highlights in allergic rhinitis. Allergy 2019, 74, 2320–2328. [Google Scholar] [CrossRef]
- Wise, S.K.; Damask, C.; Roland, L.T.; Ebert, C.; Levy, J.M.; Lin, S.; Luong, A.; Rodriguez, K.; Sedaghat, A.R.; Toskala, E. International consensus statement on allergy and rhinology: Allergic rhinitis–2023. In Proceedings of the International forum of allergy & rhinology; 2023; pp. 293–859. [Google Scholar]
- Bousquet, J.; Khaltaev, N.; Cruz, A.A.; Denburg, J.; Fokkens, W.; Togias, A.; Zuberbier, T.; Baena-Cagnani, C.; Canonica, G.; Van Weel, C. Allergic rhinitis and its impact on asthma (ARIA) 2008. Allergy 2008, 63, 8–160. [Google Scholar] [CrossRef]
- Brożek, J.L.; Bousquet, J.; Baena-Cagnani, C.E.; Bonini, S.; Canonica, G.W.; Casale, T.B.; van Wijk, R.G.; Ohta, K.; Zuberbier, T.; Schünemann, H.J. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines: 2010 revision. Journal of Allergy and clinical immunology 2010, 126, 466–476. [Google Scholar] [CrossRef]
- Penagos, M.; Durham, S.R. Allergen Immunotherapy: Optimal Duration for Respiratory Allergy. Current Treatment Options in Allergy 2024, 1–12. [Google Scholar] [CrossRef]
- Wallace, D.V.; Dykewicz, M.S.; Bernstein, D.I.; Blessing-Moore, J.; Cox, L.; Khan, D.A.; Lang, D.M.; Nicklas, R.A.; Oppenheimer, J.; Portnoy, J.M. The diagnosis and management of rhinitis: an updated practice parameter. Journal of allergy and clinical immunology 2008, 122, S1–S84. [Google Scholar] [CrossRef]
- Biedermann, T.; Kuna, P.; Panzner, P.; Valovirta, E.; Andersson, M.; de Blay, F.; Thrane, D.; Jacobsen, S.H.; Stage, B.S.; Winther, L. The SQ tree SLIT-tablet is highly effective and well tolerated: results from a randomized, double-blind, placebo-controlled phase III trial. Journal of Allergy and Clinical Immunology 2019, 143, 1058–1066. e1056. [Google Scholar] [CrossRef]
- Gianni, M. Evolution of Immunotherapy Against Pollen Allergy. Curr Protein Pept Sci 2023, 24, 488–502. [Google Scholar] [CrossRef]
- Pfaar, O.; Sager, A.; Mosges, R.; Worm, M. A high-dose, depigmented polymerized birch pollen extract for subcutaneous allergen immunotherapy has a favourable efficacy/safety ratio. Clin Transl Allergy 2023, 13, e12315. [Google Scholar] [CrossRef]
- Roberts, G.; Pfaar, O.; Akdis, C.A.; Ansotegui, I.J.; Durham, S.R.; Gerth van Wijk, R.; Halken, S.; Larenas-Linnemann, D.; Pawankar, R.; Pitsios, C.; et al. EAACI Guidelines on Allergen Immunotherapy: Allergic rhinoconjunctivitis. Allergy 2018, 73, 765–798. [Google Scholar] [CrossRef]
- Pfaar, O.; Bachert, C.; Kuna, P.; Panzner, P.; Džupinová, M.; Klimek, L.; van Nimwegen, M.J.; Boot, J.D.; Yu, D.; Opstelten, D.J.E.; et al. Sublingual allergen immunotherapy with a liquid birch pollen product in patients with seasonal allergic rhinoconjunctivitis with or without asthma. J Allergy Clin Immunol 2019, 143, 970–977. [Google Scholar] [CrossRef]
- Vogelberg, C.; Brüggenjürgen, B.; Richter, H.; et al. House dust mite immunotherapy in Germany: real-world adherence to a subcutaneous allergoid and a sublingual tablet. Allergo J Int 2021, 30, 183–191. [Google Scholar] [CrossRef]
- Penagos, M.; Eifan, A.O.; Durham, S.R.; Scadding, G.W. Duration of Allergen Immunotherapy for Long-Term Efficacy in Allergic Rhinoconjunctivitis. Curr Treat Options Allergy 2018, 5, 275–290. [Google Scholar] [CrossRef]
- Scadding, G.W.; Calderon, M.A.; Shamji, M.H.; Eifan, A.O.; Penagos, M.; Dumitru, F.; Sever, M.L.; Bahnson, H.T.; Lawson, K.; Harris, K.M.; et al. Effect of 2 Years of Treatment With Sublingual Grass Pollen Immunotherapy on Nasal Response to Allergen Challenge at 3 Years Among Patients With Moderate to Severe Seasonal Allergic Rhinitis: The GRASS Randomized Clinical Trial. JAMA 2017, 317, 615–625. [Google Scholar] [CrossRef]
- Durham, S.R.; Walker, S.M.; Varga, E.-M.; Jacobson, M.R.; O’Brien, F.; Noble, W.; Till, S.J.; Hamid, Q.A.; Nouri-Aria, K.T. Long-term clinical efficacy of grass-pollen immunotherapy. New England Journal of Medicine 1999, 341, 468–475. [Google Scholar] [CrossRef]
- Pavón-Romero, G.F.; Parra-Vargas, M.I.; Ramírez-Jiménez, F.; Melgoza-Ruiz, E.; Serrano-Pérez, N.H.; Teran, L.M. Allergen Immunotherapy: Current and Future Trends. Cells 2022, 11. [Google Scholar] [CrossRef]
- Benito-Villalvilla, C.; Soria, I.; Subiza, J.L.; Palomares, O. Novel vaccines targeting dendritic cells by coupling allergoids to mannan. Allergo J Int 2018, 27, 256–262. [Google Scholar] [CrossRef]
- Pfaar, O.; Becker, S.; Calabria, C.; Hartenstein, D.; Jung, J.; Zimmer, J.; Ponda, P. Comparison of allergen immunotherapy practice patterns in inhalant allergies in the United States of America and Europe: Similarities and differences 2023. World Allergy Organization Journal 2023, 16, 100766. [Google Scholar] [CrossRef]
- Casanovas, M.; Gómez, M.; Carnés, J.; Fernández-Caldas, E. Skin tests with native, depigmented and glutaraldehyde polymerized allergen extracts. J Investig Allergol Clin Immunol 2005, 15, 30–36. [Google Scholar]
- Sirvent S, et al. J Allergy Clin Immunol. 2016 ;138(2):558-567.e11. Epub 2016 Apr 13. PMID: 27177779. [CrossRef] [PubMed]
- Manzano, A.I.; Javier Cañada, F.; Cases, B.; Sirvent, S.; Soria, I.; Palomares, O.; Fernández-Caldas, E.; Casanovas, M.; Jiménez-Barbero, J.; Subiza, J.L. Structural studies of novel glycoconjugates from polymerized allergens (allergoids) and mannans as allergy vaccines. Glycoconjugate Journal 2016, 33, 93–101. [Google Scholar] [CrossRef]
- Vinay, T.N.; Park, C.S.; Kim, H.Y.; Jung, S.J. Toxicity and dose determination of quillaja saponin, aluminum hydroxide and squalene in olive flounder (Paralichthys olivaceus). Vet Immunol Immunopathol 2014, 158, 73–85. [Google Scholar] [CrossRef]
- Mosges, R.; Zeyen, C.; Raskopf, E.; Acikel, C.; Sahin, H.; Allekotte, S.; Cuevas, M.; Shamji, M.H.; Subiza, J.L.; Casanovas, M. A randomized, double-blind, placebo-controlled trial with mannan-conjugated birch pollen allergoids. Allergy 2023. [CrossRef]
- Pfaar, O., Demoly, P., Gerth van Wijk, R., Bonini, S., Bousquet, J., Canonica, G.W., ... & Calderon, M.A. (2014). Recommendations for the standardization of clinical outcomes used in allergen immunotherapy trials for allergic rhinoconjunctivitis: an EAACI Position Paper. Allergy, 69, 854-867.
- Mösges, R.; Raskopf, E.; Klimek, L.; Pfaar, O.; Zielen, S.; Xenofontos, E.; Decker, L.; Neuhof, C.; Rybachuk, A.; Acikel, C. Short-course subcutaneous treatment with birch pollen allergoids greatly improves symptom and medication scores in birch allergy. Allergy 2024. [Google Scholar] [CrossRef]
- Canonica, G.; Baena-Cagnani, C.; Bousquet, J.; Bousquet, P.; Lockey, R.; Malling, H.J.; Passalacqua, G.; Potter, P.; Valovirta, E. Recommendations for standardization of clinical trials with Allergen Specific Immunotherapy for respiratory allergy. A statement of a World Allergy Organization (WAO) taskforce. Allergy 2007, 62, 317–324. [Google Scholar]
- Pfaar, O.; Biedermann, T.; Klimek, L.; Sager, A.; Robinson, D. Depigmented–polymerized mixed grass/birch pollen extract immunotherapy is effective in polysensitized patients. Allergy 2013, 68, 1306–1313. [Google Scholar] [CrossRef]
- Gallego, M.T.; Iraola, V.; Himly, M.; Robinson, D.S.; Badiola, C.; García-Robaina, J.C.; Briza, P.; Carnés, J. Depigmented and polymerised house dust mite allergoid: allergen content, induction of IgG4 and clinical response. Int Arch Allergy Immunol 2010, 153, 61–69. [Google Scholar] [CrossRef]
- Nguyen, N.T.; Raskopf, E.; Shah-Hosseini, K.; Zadoyan, G.; Mösges, R. A review of allergoid immunotherapy: is cat allergy a suitable target? Immunotherapy 2016, 8, 331–349. [Google Scholar] [CrossRef]
- Pfaar, O.; Agache, I.; de Blay, F.; Bonini, S.; Chaker, A.M.; Durham, S.R.; Gawlik, R.; Hellings, P.W.; Jutel, M.; Kleine-Tebbe, J.; et al. Perspectives in allergen immunotherapy: 2019 and beyond. Allergy 2019, 74 (Suppl. 108), 3–25. [Google Scholar] [CrossRef]
- Bousquet, J.; Sousa-Pinto, B.; Anto, J.M.; Bedbrook, A.; Czarlewski, W.; Ansotegui, I.J.; Bergmann, K.C.; Braido, F.; Brussino, L.; Cecchi, L.; Loureiro, C.C.; Cruz, A.A.; Devillier, P.; Fiocchi, A.; Gemicioglu, B.; Haahtela, T.; Ivancevich, J.C.; Klimek, L.; Kulus, M.; Kuna, P.; Kupczyk, M.; Kvedariene, V.; Larenas-Linnemann, D.E.; Louis, G.; Louis, R.; Makris, M.; Morais-Almeida, M.; Niedoszytko, M.; Ohta, K.; Ollert, M.; Papadopoulos, N.; Patella, V.; Pétré, B.; Pfaar, O.; Puggioni, F.; Quirce, S.; Regateiro, F.S.; Roche, N.; Rouadi, P.W.; Samolinski, B.; Sastre, J.; Schleich, F.; Scichilone, N.; Taborda-Barata, L.; Toppila-Salmi, S.; Valiulis, A.; Vardaloglu Koyuncu, I.; Ventura, M.T.; Yorgancioglu, A.; Fonseca, J.A.; Zuberbier, T. Concurrent validity, cut-offs and ability to change of patient-reported outcome measures for rhinitis and asthma in MASK-air®. Clin Transl Allergy. 2024, 14, e12390. [Google Scholar]
- Dayal, A.K.; Sinha, V. Trend of Allergic Rhinitis Post COVID-19 Pandemic: A Retrospective Observational Study. Indian J Otolaryngol Head Neck Surg 2022, 74, 50–52. [Google Scholar] [CrossRef]
- Dror, A.A.; Eisenbach, N.; Marshak, T.; Layous, E.; Zigron, A.; Shivatzki, S.; Morozov, N.G.; Taiber, S.; Alon, E.E.; Ronen, O.; et al. Reduction of allergic rhinitis symptoms with face mask usage during the COVID-19 pandemic. J Allergy Clin Immunol Pract 2020, 8, 3590–3593. [Google Scholar] [CrossRef]
- Mengi, E.; Kara, C.O.; Alptürk, U.; Topuz, B. The effect of face mask usage on the allergic rhinitis symptoms in patients with pollen allergy during the covid-19 pandemic. American journal of otolaryngology 2022, 43, 103206. [Google Scholar] [CrossRef]
- Akasaki, Y.; Inomata, T.; Iwagami, M.; Sung, J.; Nagino, K.; Adachi, T.; Morita, H.; Tamari, M.; Kainuma, K.; Kan-OK; Ogata, H.; Sakashita, M.; Futamura, M.; Kurashima, Y.; Nakajima, S.; Masaki, K.; Ogawa, Y.; Sato, S.; Miyagawa, A.; Midorikawa-Inomata, A.; Fujimoto, K.; Okumura, Y.; Fujio, K.; Huang, T.; Hirosawa, K.; Morooka, Y.; Murakami, A.; Nakao, S. The impact of COVID-19 on hay fever treatment in Japan: A retrospective cohort study based on the Japanese claims database. Clin Transl Allergy 2024, 14, e12394. [Google Scholar] [CrossRef]
- Korematsu, S.; Fujisawa, T.; Saito, N.; et al. Suppressed pediatric asthma hospitalizations during the COVID-19 pandemic in Japan, from a national survey. Clin Transl Allergy. 2024, 14, e12330. [Google Scholar] [CrossRef]
- Palathumpattu, B.; Pieper-Fürst, U.; Acikel, C.; Sahin, H.; Allekotte, S.; Singh, J.; Hess, M.; Sager, A.; Müller, T.; Mösges, R. Correlation of the combined symptom and medication score with quality of life, symptom severity and symptom control in allergic rhinoconjunctivitis. Clin Transl Allergy 2022, 12, e12191. [Google Scholar] [CrossRef]
Figure 4.
The mean±SD dSS development of: Left panel – patients with placebo in T502-SIT-020 study in 2020 and treatment in T502-SIT-041 study in 2021, Right panel –of patients with placebo in T502-SIT-045 study in 2022 and treatment in T502-SIT-059 study in 2023. ** - p = 0.001, n.s. – non significant
Figure 4.
The mean±SD dSS development of: Left panel – patients with placebo in T502-SIT-020 study in 2020 and treatment in T502-SIT-041 study in 2021, Right panel –of patients with placebo in T502-SIT-045 study in 2022 and treatment in T502-SIT-059 study in 2023. ** - p = 0.001, n.s. – non significant
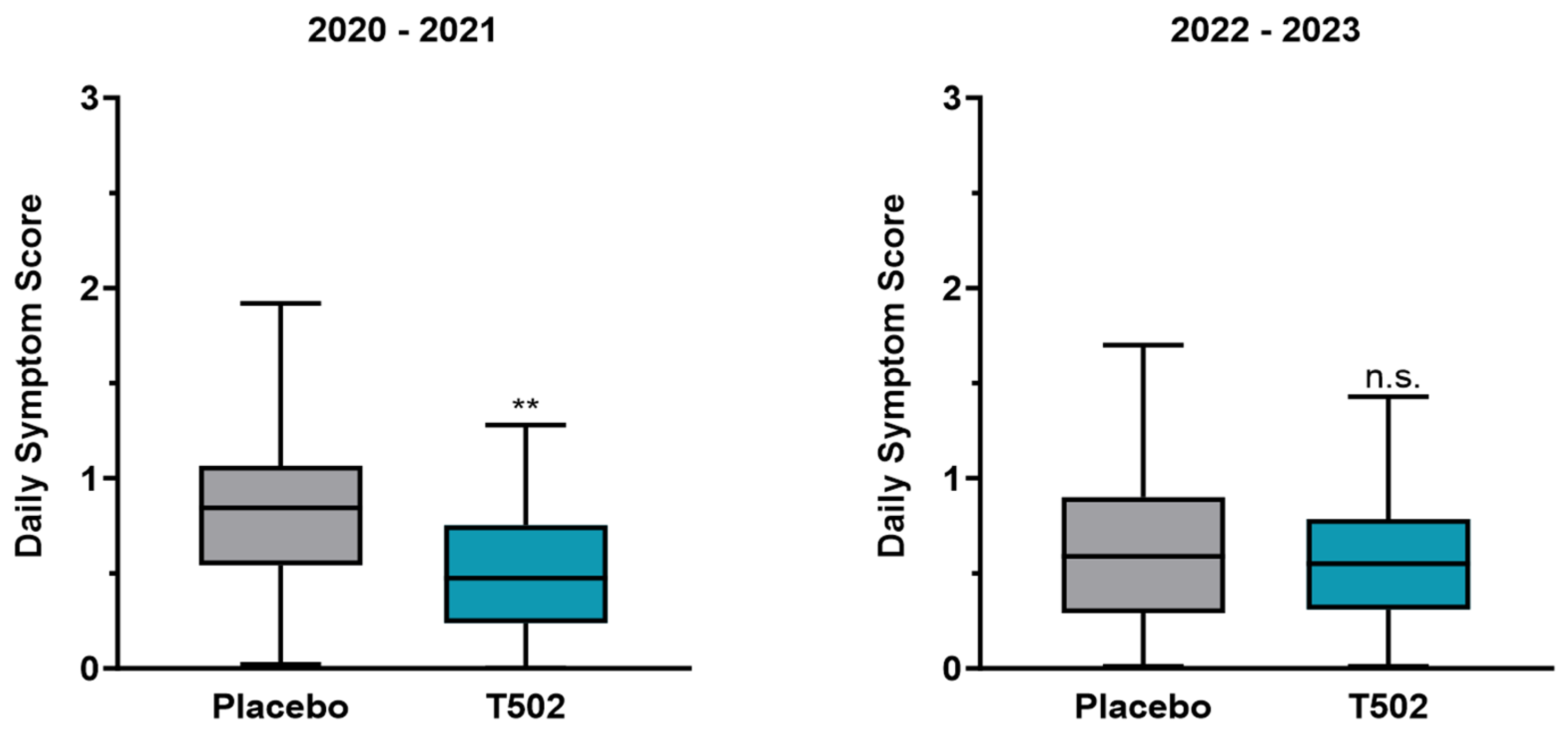
Figure 5.
The mean±SD dMS development of: Left panel – patients with placebo in T502-SIT-020 study in 2020 and treatment in T502-SIT-041 study in 2021, Right panel – of patients with placebo in T502-SIT-045 study in 2022 and treatment in T502-SIT-059 study in 2023. * - p = 0.001
Figure 5.
The mean±SD dMS development of: Left panel – patients with placebo in T502-SIT-020 study in 2020 and treatment in T502-SIT-041 study in 2021, Right panel – of patients with placebo in T502-SIT-045 study in 2022 and treatment in T502-SIT-059 study in 2023. * - p = 0.001
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



