
Submitted:
23 October 2025
Posted:
24 October 2025
You are already at the latest version
Abstract
Background/Objectives: Glutathione (GSH) and its precursor cysteine (Cys) plays an important role in the neuronal injury process in stroke. We evaluate the association of cysteine and glutathione forms in blood plasma with the severity and disability of acute hemorrhagic stroke. Methods: A total of 64 patients (39-59 years old) with intracerebral (n=12) or subarachnoid hemorrhage (n=52) were examined. The patients' conditions were estimated using the National Institutes of Health Stroke Scale (NIHSS) and the modified Rankin Scale (mRS). Results: The median levels of plasma cystine (CysS) and reduced glutathione (rGSH) were 51.1 and 1.04 µM, respectively. Patients with high levels (≥50 μM) of CysS had a significantly higher frequency of mild or moderate neurological impairment (NIHSS≤10) than patients with levels of CysS<50 µM (OR=7.73, CI95% 2.19-27.28). Also, patients with high levels (≥1.9 μM) of rGSH had a significantly higher frequency of mild disability (mRS≤2) compared to patients with rGSH<1.9 µM (OR=12.35, CI95% 3.43-44.5). Conclusions: CysS and rGSH levels are associated with a reduced risk of high neurological deficit and disability, respectively, in the acute period of hemorrhagic stroke. These indicators could be used to evaluate neurologic impairment severity of stroke patient. Further research is needed to determine potential of circulating free thiols as biomarkers and to evaluate the usefulness of GSH-targeting therapy in acute hemorrhagic stroke.
Keywords:
cysteine
; disability
; glutathione
; hemorrhage stroke
; neurological deficit
1. Introduction
Hemorrhagic stroke (HS) is a non-traumatic intracranial hemorrhage occurring in the space between the pia mater and arachnoid mater (subarachnoid hemorrhage, SAH) or in the brain tissue itself (intracerebral hemorrhage, ICH). According to various data, HS accounts for 15 to ~ 40% of all strokes and has an incidence of 10–30/100,000 [1,2,3]. HS is characterized by a higher incidence of complications associated with cerebral edema and hydrocephalus, mortality and disability than ischemic stroke, as well as a higher risk of relapse.
Numerous studies have demonstrated that oxidative damage is a critical pathological mechanism involved in brain injury, and the diagnostic role of oxidative stress (OS) markers has been actively studied [4,5]. Low molecular weight aminothiols (cysteine, Cys; homocysteine, Hcy; glutathione, GSH) are present in blood plasma in oxidized (to disulfides) and native forms, the dynamic equilibrium of which is ensured by oxidation reactions, disulfide exchange, and their transmembrane transfer from/into cells. Aminothiols play an active role in both protective and damaging mechanisms that are directly related to oxidative damage. Thus, Hcy, an intermediate product of methionine metabolism, is actively studied as a pathogenetic factor and a marker of HS risk and outcome [6,7,8,9].
Much less clinical research has been conducted to identify the association of other aminothiols, GSH and Cys, with HS, although they play an even more important role in the pathogenesis of neuronal injury. GSH is the main cytoplasmic component of the cell defense system against OS and it could provide mechanisms of adaptation to OS during stroke. This is the fundamental difference between GSH and other low-molecular markers of OS, which are by-products of reactions involving reactive oxygen species (malonic dialdehyde, 4-OH-nonenal, 8-isoprostane, 8-hydroxydeoxyguanosine, 8-hydroxyguanine, etc.). The disturbance of the GSH redox balance plays an important role in key mechanisms of HS (apoptosis, ferroptosis and pyroptosis) [5,10]. Under ischemic conditions, a decrease in the GSH content or its redox status in the brain is observed [11,12], and maintaining its level makes it possible to attenuate the negative effects of ischemia observed in experimental models [13,14]. GSH synthesis is critically dependent on the extracellular level of Cys as the rate-limiting substrate [15]. The level of Cys consumption was inversely associated with the risk of HS [16].
Thus, the above arguments suggest that Cys and GSH may be of interest as potential markers of severity or prognosis of HS. Typically, only total aminothiols are measured in clinical studies. However, these metabolites are present in the blood in various forms (bound and free), and have different activities. Of particular interest here may be the free forms, such as cystine (CysS) and reduced GSH (rGSH). CysS is the most bioavailable form of Cys for brain cells [17]. Experimental and clinical studies have shown that rGSH levels are most susceptible to decreases in acute cerebral ischemia [18,19]. However, to our knowledge, no targeted clinical studies on the diagnostic role of these aminothiols in HS have been published yet. Therefore, the aim of the present study was to search for an association of free forms of Cys in blood plasma, namely its reduced form (rCys) and CysS and the reduced form of GSH in blood plasma (rGSH) and whole blood (bGSH), as well as its disulfide in whole blood (GSSG), with severity and disability in the acute period of HS.
2. Materials and Methods
2.1. Patients
This study was conducted from November 2023 to May 2024 in accordance with the ethical principles of the Declaration of Helsinki of the World Medical Association (1964 and 2004) and the written voluntary informed consent of all patients. The study protocol was developed in accordance with CONSORT 2010 recommendations and was approved by the ethics committee of the Moscow Regional Research Clinical Institute (protocol No. 7 from 13 July 2023). In February–March 2025, an oral survey of patients was conducted in order to determine the state of their vital functions, the occurrence of a recurrent stroke or the death of the patient.
The study included 64 patients (aged 39-59) with HS who were admitted in the first 10–72 h after the development of neurological disorders. Patients were admitted to the neurology department of Moscow Regional Research Clinical Institute and selectively included in the cohort. The subtype of stroke was determined according to the TOAST (Trial of ORG 10172 in Acute Stroke Treatment) classification criteria. Information on hypertension, type 2 diabetes mellitus and heart disease (i.e. coronary heart disease, myocardial infarction, valvular disease and atrial fibrillation) was based on the medical history and clinical data.
The criteria for the non-inclusion of patients in the study include an inability of the patient to undergo a CT/MRI procedure; the presence of neuroimaging signs (brain tumor, arteriovenous malformation, brain abscess, edema of the infarct zone) leading to dislocation of brain structures (malignant course of cerebral infarction); repeated ischemic or hemorrhagic stroke; traumatic brain injury lasting 6 months; a history of surgical intervention on the brain or spinal cord; epilepsy; and severe cognitive impairment in the anamnesis.
Criteria for excluding patients from the study were a positive blood test for HIV, syphilis, hepatitis B and/or C, detected at the start of the study; the appearance of any diseases or conditions during the study that worsened the patient's prognosis, or made it impossible for the patient to continue participating in the clinical trial; violation of the study protocol, such as erroneous inclusion of a patient who does not meet the inclusion and/or non-inclusion criteria; taking drugs for prohibited therapy; other protocol violations that, in the opinion of the investigator, were significant; and a patient's refusal to participate in the study.
The severity of the neurological disorders was rated on the National Institutes of Health Stroke Scale (NIHSS), and the degree of disability and functional independence on the modified Ranking Scale, mRS [20,21].
All patients underwent magnetic resonance imaging of the brain using Magnetom Verio (Siemens) and Magnetom Symphony (Siemens) devices with magnetic induction values of 3 and 1.5 T, respectively. MRI angiography was performed in a 3D-TOF mode to detect intracranial artery pathology. Intracerebral hematoma was identified as a round area with a high-intensity signal in T2, T2-FLAIR, and hypointense in T2*. Confirmation of subarachnoid hemorrhage was performed by lumbar puncture. CT was used to determine the intensity and extent of subarachnoid hemorrhage [22].
2.2. Laboratory Studies
Patients’ venous blood was collected in 3 mL K3EDTA tubes (Lab-Vac, Heze, China) at admission. A volume of 0.35 mL 0.5 M citrate Na (pH 4.3) was added to blood immediately. After mixing, the samples were cooled at 4◦C for 3–4 h. The plasma (1 mL) was obtained via blood centrifugation at 350 g for 10 min at room temperature. After collecting the blood plasma, a mixture (1 ml) containing 0.5 M Na citrate (pH 4.3) and phosphate-buffered saline in a ratio of 1:9 was added to the remainder of the sample. The content of free forms of aminothiols in blood plasma (rGSH, rCys and CysS), as well as native and oxidized GSH in the blood (bGSH, GSSG), was determined by capillary electrophoresis with 200 nm ultraviolet detection (CE-UV), as described in [23] and [24], respectively. A capillary electrophoresis system, Capel-205 (Lumex, Russia), was used with an unbound silica capillary of 50 μm i.d. and 42 cm total (35 cm effective) length.
Briefly, plasma samples (200 μL) were mixed with 20 mM N-ethylmaleimide (200 μL) and filtered at 12 000 g for 10 min using Amicon Ultra-0.5 mL 3 K cartridges (Millipore) for free aminothiols determination. Filtrates (200 μL) were mixed with internal standard (5 mM glycyl-asparagine, 10 μL) and water (10 μL) case of prior analysis. A plug of 50 mM triethanolamine with 7.5% polyethyleneglycole-600 was injected (900 mbar•s) before the sample in capillary filled with 0.115 M Na phosphate with 7.5% (v/v) polyethyleneglycole-600 (pH 2.3). The sample was injected for 1200 mbar•s. Phosphoric acid (0.1 M) with 7.5% polyethyleneglycole-600 was injected (125 mbar•s) after the sample. A positive polarity (25 kV) was applied for CE for 11 min.
A mixture of water (100 μl), acetonitrile containing 30 mM N-ethylmaleimide (300 μl), and 95% ethanol (300 μl) was added to 200 μl of blood for bGSH, GSSG determination. The mixture was centrifuged for 5 min at 15 000 g. Then, the supernatant (250 μl) was mixed with glycyl-asparagine (50 μl, 1 mM) and diethyl ester (270-μl). This mixture was stirred vigorously for 1 min and centrifuged for 2 min at 4000 g. The upper phase was discarded, and the lower phase was concentrated in vacuo (25 min at 45◦C), and 150 μl of water was added prior to analysis. A plug of 75 mM citric acid was injected (1000 mbar•s) before the sample in capillary filled with 75 mM citrate Na (pH 5.8) with 0.2 mM cetriltrimethylammonium bromide and 5 μM sodium dodecyl sulfate. The sample was injected over 1000 mbar•s. Tricitrate Na (75 mM) was injected (1000 mbar•s) after the sample. A negative polarity of −14 kV was applied for CE for 5.5 min.
LODs for rGSH, rCys, CysS, GSSG and bGSH were 0.5, 0.9, 1.6, 0.5 and 0.6 μM, correspondingly; inter-assay and intra-assay variability were within 2.0-4.5 and 2.6-5.0 %, correspondingly; and accuracy was 96.4-98.9 % for rGSH, rCys, CysS and 101.2-103.7 % for GSSG and bGSH. The total Hcy plasma level was determined by liquid chromatography, as described in [25].
Blood samples for the study of hemostasis parameters were obtained by venipuncture from the ulnar veins (~12 mL) using disposable vacuum systems containing 2.5% sodium citrate. To study the biochemical parameters, blood was taken into a test tube with a coagulation activator. Samples were processed no later than 30 min after venipuncture. An ACL TOP 700 hemostasis analyzer (IL Werfen, Barcelona, Spain), an AU 680 biochemical analyzer (Beckman Coulter, Brea, CA, USA), and a PENTRA 120 hematology analyzer (Horiba ABX, Montpellier, France) were used. The determination of IL-6 in plasma was carried out using test systems from Bender Medsystems GmbH (Vienna, Austria), according to the manufacturer’s instructions [26].
The atherogenicity coefficient was calculated using the formula (Total cholesterol - High-Density Lipoprotein Cholesterol) / Low-Density Lipoprotein Cholesterol [27]. In women under 40 years of age, the normal value of this indicator is less than 2.5, and at an older age, it is up to 3.5. In men before and after 40 years of age, the normal level of this indicator was less than 2.4 and 3.5, respectively.
2.3. Data Processing
Data collection and primary processing (identification and integration of the chromatographic peaks) were performed using MassLynx v4.1 (Waters, Milford, MA, USA) and Elforun software v. 4.2.5 (Lumex, St. Petersburg, Russia). Statistical data analysis was performed using SPSS Statistics v. 22 (IBM, Armonk, NY, USA). Quantitative indicators were expressed as medians (and 1st and 3rd quartiles). Optimal cut-off values for variables were determined by receiver operating characteristic (ROC) analysis. Logistic regression analysis was employed to evaluate the influence of variables on the NIHSS and mRS score. To separate severe and mild stroke, a cut-off NIHSS ≤ 10 was used, and to separate the cohort according to the functional state criterion, a cut-off mRS ≤ 2 was used. The comparison of binomial indicators (variable analysis) was carried out via the relative risk ratio (RR) and odds ratio (OR); p < 0.05 was considered to indicate a significant difference. The relationships between the studied parameters were analyzed and a comparison of patient subgroups was performed using rank analysis methods. Correlation analysis was performed using Spearman's rank correlation coefficient. When comparing variables between groups, the Mann–Whitney criterion was used. For all comparisons and tests, a two-sided critical significance level (p) was used. In the case of multiple comparisons, the Holm–Bonferroni method was used to correct p values.
3. Results
The demographic characteristics and laboratory data of patients are presented in Table 1. The median age of patients was 55 years, and the range 39–59 years. Only 12 (18.8%) patients had ICH; the rest had SAH. Most patients were men. The cohort had a high frequency of stroke risk factors, such as smoking, arterial hypertension, ischemic heart disease, atrial fibrillation and regular alcohol consumption. Interestingly, only 21.3% of patients had hyperhomocysteinemia (Hcy > 15 M). After correction for multiple comparisons, we found no significant differences in any of the above parameters between patients with ICH and SAH. CysS, GSSG and bGSH levels were reliably determined in almost all patients (95.3-98.4%), rCys was determined in 92.2% of samples, and the rGSH level was only determined in 90.6% of cases. Among all aminothiols, only rCys and Hcy (= -0.450, p = 0.0057) showed a reliable correlation with each other.
When dividing patients by the criterion of disability (Table 2), only rGSH demonstrated a reliable difference. Thus, patients with a minor degree of disability (mRS ≤ 2) were characterized by a significantly higher level of rGSH. Other aminothiol parameters did not have reliable differences. No significant differences were found between these subgroups in the distribution of HS subtypes, risk factors and comorbidities, except for a higher frequency of CAD in the subgroup of patients with mRs > 2 (65.1 vs. 28.6%, p=0.027; see Supplementary Materials, Table S1).
Having conducted the ROC analysis of the cohort of patients by the outcome criterion mRS ≤ 2, we identified the cut-off level of rGSH = 1.9 M (Figure 1A). In the group of patients with rGSH ≥ 1.9 M, a minor degree of disability was observed significantly less frequently than in patients with rGSH < 1.9 M (RR=4.15, p=0.00003). When dividing the cohort by the cutoff criterion of rGSH ≥ 1.9 M, Mann–Whitney analysis revealed that patients with high rGSH levels were characterized by a significantly higher frequency of mRS ≤ 2 compared to patients with low levels of rGSH (72.2 vs. 17.4%, p = 3∙10-5). Also, in the subgroup with high rGSH levels, the frequency of CAD was lower (27.8 vs. 63%, p=0.0495, Supplementary Materials, Table S2). Accordingly, the rGSH level in patients with CAD was lower (0.59 (0.11; 1.47) vs 1.52 (0.5; 2.96) μM, p=0.007). Therefore, in the group of patients with CAD, the rGSH level ≥ 1.9 μM was associated with the outcome mRS ≤ 2 (RR=7.0, p=0.0036; OR=13, CI 95% 1.5-111.8). But this association was also observed in the group of patients without CAD (RR=3.33, p=0.005; OR=8.0, CI95% 1.5-42.0).
When dividing patients by the severity of neurological deficit (Table 3), it was found that in patients with more severe HS (NIHSS > 10), the CysS level was lower than in patients with NIHSS ≤ 10. The other aminothiol indices also did not differ significantly. ROC analysis for the outcome criterion NIHSS ≤ 10 revealed a cut-off at CysS = 50 M (Figure 1B). In patients with mild neurological deficit, the frequency of CysS ≥50 M was significantly higher than in patients with severe neurological deficit (RR=1.82, p=0.00033). Also, comparing groups of patients with high (≥ 50 M) and low (<50 M) CysS levels, it was found that in the first group, the vast majority of patients had a mild stroke (NIHSS ≤ 10), while in the second group, this indicator was significantly lower (87.9 vs. 48.4%, p = 0.0057). No significant differences were found between these subgroups in the distribution of HS subtypes, risk factors and comorbidities when dividing the cohort into subgroups according to the above criteria (Supplementary Materials, Tables S3 and S4).
Additionally, a questionnaire was conducted on the patients' vital functions 9-14.5 months (mean 11.8 months) after the stroke. Only 54 of 64 (84.4%) patients had data obtained during the questionnaire. During this time, nine cases of death and two cases of recurrent stroke were identified. No significant association was found between aminothiol levels and stroke outcome.
4. Discussion
At present, it is known from clinical and experimental studies that HS is accompanied by an increase in the level of various OS-associated low molecular markers such as malondialdehyde, 4-OH-nonenal, isoprostaglandines and 7,8-dihydro-8-oxoguanine, and some of them have shown an association with hematoma volume, adverse outcome and mortality in HS [4]. Changes in the aminothiol system in HS and their diagnostic role have so far been studied fragmentarily and insufficiently. Our results, although they do not provide grounds for using rGSH and CysS as prognostic indicators, did reveal their rather close association with disability and neurological deficit in the acute period of stroke.
On average, the normal content of CysS and rCys in blood plasma is 30-60 and rCys 5-15 μM, respectively [23,28,29,30]. The total GSH content in plasma is 5.5-8 μM. The normal level of rGSH, according to various sources, is in the range of ~2.0-5.5 μM [23,28,29,30,31]. In whole blood, the level of reduced GSH is significantly higher (~ 1 mM), and GSSG is about ~2.5~5 μM [24]. It has previously been shown that decreased plasma total GSH levels may be a risk factor for CVD, including ICH [32]. A low total GSH level has also been found in the acute period in patients with ICH [33]. Reduced GSH is the most reactive fraction of GSH and may therefore be a more sensitive indicator in conditions associated with OS. However, a study found no significant differences in rGSH levels between ischemic stroke patients and controls, although total GSH levels were lower in the former group [29]. However, this study did not clearly indicate the time of blood collection from the onset of the disease, and therefore the results obtained cannot be unambiguously attributed to the acute period of stroke. According to our data, rGSH levels in acute HS have not yet been determined in clinical studies. Our data show that while the average Cys, rCys, bGSH and GSSG levels in patients with HS were close to previously published normal ranges, the rGSH level in most patients with acute HS was apparently significantly lower than normal [23].
Although the total level of serum GSH may increase in patients with stroke during the acute period, according to some studies [37,41], the total level of SH-groups and reduced aminothiols are subject to a significant decrease in blood plasma according to both experimental and clinical studies [11,22,40,42,43]. Therefore, it can be assumed that changes in circulating rGSH in acute ischemic and hemorrhagic strokes are unidirectional.
According to our data, the diagnostic and prognostic role of rGSH in HS has not yet been studied. Our study revealed that a smaller proportion of patients (28.1%) with HS had a plasma rGSH level of more than 1.9 μM, and in such patients, a minor degree of disability (mRS 0-2) at admission was significantly more common than in patients with an rGSH level of less than 1.9 μM (OR=12.35, see Figure 1A). Although mRS has traditionally been used as an outcome measure for stroke, mRS at admission also finds a place in patient characterization and as a prognostic marker [44,45,46,47]. Thus, rGSH here acts as a protective marker of patient vital activity in the acute period of HS.
The incidence of CAD was significantly higher in the group of patients with mRS > 2. rGSH levels were also somewhat lower in patients with CAD. This suggests the important role of GSH and its redox balance in the pathogenesis of arterial atherosclerosis. This result is generally consistent with a number of clinical observations that have shown that patients with CAD have lower levels of reduced GSH in the blood (erythrocytes) [25,48,49] and in serum [50]. Moreover, low plasma rGSH levels (as well as high CysS levels) are associated with the risk of future death in a high-risk population with CAD, which supports the use of these aminothiols as key biomarkers of OS [51]. At the same time, according to our data, rGSH was also associated with mRS in patients without a history of CAD, although it was less pronounced. Therefore, CAD appears to only partially contribute to the association of rGSH with mRS, and larger studies are needed to more confidently answer the question of whether rGSH is an independent marker.
The level of rGSH is determined by the balance of its synthesis, oxidation and hydrolysis. GSH and related enzymes participate in oxidative processes, and changes in the GSH system are complex and multi-faceted. On the one hand, in animal stroke models, an increase in GSH synthetase in the brain (which facilitates GSH synthesis) was revealed [34]. On the other hand, enzymes that use GSH, such as GSH peroxidase 4, may also be increased [35] or, conversely, decreased [10]. However, clinical data on its activity are ambiguous. Thus, the increased activity of this enzyme in the blood plasma of patients with SAH was detected in clinical observations [36,37], but its activity in the brain or at plasma level did not differ significantly between the HS and control groups in others [38,39]. Another reason for the decrease in plasma rGSH levels may be the intensification of its hydrolysis by -glutamyltranspeptidase. As was shown in the study [40], in patients with stroke, there is an increase in the activity of this enzyme at admission.
Another important finding of our study was the identification of a significantly higher frequency of mild or moderate neurological deficit (NIHSS ≤ 10) at admission in the group of patients with CysS levels ≥ 50 μM than in patients with lower CysS levels (OR = 7.73, see Figure 1B). This suggests that CysS may also be considered as a protective marker in the acute phase of HS. Although our study did not reveal an association of CysS with rGSH or bGSH, as noted above, the bioavailability of Cys plays a key role in GSH synthesis and in protecting the brain from OS [15]. The depletion of brain GSH by a reduced supply of dietary Cys may be important during brain ischemia [52]. On the other hand, there are various mechanisms by which Cys can exert a neurotoxic effect [53]. In particular, the role of cysteine in disrupting mitochondrial respiration by limiting intracellular iron availability through an oxidant-based mechanism has been noted [54,55].
Among the numerous mechanisms of action of Cys, its role in the synthesis of H2S by the enzyme cystathionine-β-synthase (CβS) attracts special attention; however, the results of both experimental and clinical studies have not allowed us to clearly judge whether it is protective or neurotoxic. On the one hand, some experimental studies have shown that endogenous production of H2S and CβS in the brain was significantly inhibited by SAH, while treatment with NaHS or Cys restored H2S production and the expression of CβS, and has protective effects (attenuate brain edema, neuronal cell death, improve neurological function and other) [56,57,58,59]. However, an increase in the activity of CβS was noted in other experimental studies of brain ischemia [60,61,62], the activation of CβS was associated with neuronal damage, and the inhibition of CβS had a protective role [61,63,64,65]. Finally, inhalation of H2S may cause a protective effect (anti-apoptotic and anti-inflammatory), accompanied by the inhibition of CβS [66].
Clinical trial data are also mixed. Thus, the level of CβS in Cerebrospinal fluid was closely associated with the inflammatory response and neurological deficits after SAH [63,67]. At the same time, data from a study of CβS polymorphism among patients with SAH showed that increased CβS activity may exert its neuroprotective effects and decrease the incidence of delayed cerebral ischemia [68,69].
Although the total concentration of Cys in plasma is ~120-320 μM [28,29,30,31], most of it is bound to proteins (mainly albumin) and does not penetrate the blood–brain barrier (BBB). The reduced form of Cys also practically does not penetrate into the brain from the bloodstream. The most accessible form of cysteine for the brain is CysS [70]. CysS is taken up by astrocytes and, to a lesser extent, neurons via the xc- transporter in exchange for glutamic acid in a 1:1 ratio [71,72]. A number of studies have also revealed a protective effect of enhancing xc− expression [73,74,75] and a negative effect of xc− inhibition [74] under hypoxic conditions.
However, the release of glutamate associated with CysS uptake is considered a serious factor in neuronal death due to the activation of N-methyl-D-aspartate (NMDA) receptors, since xc− provides transport for 60-80% of the entire extracellular glutamate pool [76]. In addition, excessive glutamate around the hematoma inhibits CysS uptake, leading to GSH depletion [10]. A number of studies have shown that xc- inhibition suppressed neuronal death under conditions of oxygen and glucose deprivation [77,78]. All this, in the first approximation, contradicts the fact that CysS can play a protective role, but, at the same time, cause an increase in the intracellular pool of Cys; not only was the expression of xc− inhibited, but an increase in the expression of the glutamate scavenger Glutamate transporter-1 (GLT-1) was also observed, which counteracted the increase in the extracellular pool of glutamate in the brain [70]. Thus, the comparison of the association of CysS levels with neurological deficit revealed in the present study with the known mechanisms of Cys action indicates the relevance of studying GSH as a metabolic target in the search for new approaches for the treatment of acute HS.
Thus, much attention is now being paid to the enzyme GSH peroxidase 4 (GPx4) as a target, since it plays a crucial role in regulating ferroptosis and stroke pathophysiology [10]. Maintaining the GSH level in cells is essential for GPx4 function. Although experimental models of HS have shown that there is a decrease in the amount of this enzyme in the affected area, and its inhibition causes negative effects [10], to our knowledge, clinical studies in this area have not yet been conducted.
In a number of clinical studies in neurodegenerative and cardiovascular diseases, the bioavailable form of Cys, N-acetylcysteine (NAC), has been shown to protect against OS and neuronal death [79,80]. However, to our knowledge, such clinical studies in HS have not yet been conducted. Of interest here is an experimental study [81] performed on the ICH model. The intraperitoneal administration of NAC produced therapeutic effects on neurological functions. It was found that, firstly, the inhibition of ICH-induced upregulation of 5-lipoxygenase was identified as a key event leading to the improved outcome. Secondly, NAC efficacy required increases in GSH level. In another study [82], it was found that the intraperitoneal administration of GSH significantly reduced mortality rate and infarct volume, and also caused an improvement in the neurological deficits score and impaired motor and sensory functions in a dose-dependent manner in a mouse model of ICH. The role of up-regulated protein expression of mitochondrial complex I as part of the protective effect of GSH was also revealed.
Reduced GSH, reacting with nitric oxide (NO) or S-nitrosohemoglobin, forms nitrosoglutathione (GSNO). NO is an extremely unstable and short-lived molecule but plays a very important role in the regulation of blood flow and cell inflammation [83]. GSNO has a significantly longer lifetime and gradually, spontaneously releases NO or participates in the S-nitrosylation of proteins. Thus, rGSH acts as a carrier of NO, and GSNO makes up a significant part of the circulating pool of NO. The results of a number of experimental studies show that the introduction of GSNO protects the brain against ischemia/reperfusion and traumatic injury (reduced brain infarctions, BBB leakage, edema, improved neurological and sensorimotor function) [84,85,86,87]. In the SAH model, it has also been previously established that GSNO administration can reverse acute vasoconstriction and prevent brain injury [88]. There have been no clinical studies on the therapeutic effects of GSNO in acute stroke, but several studies have demonstrated that GSNO is effective in reducing embolic signals in patients with symptomatic internal carotid artery stenosis undergoing carotid endarterectomy or stenting [89]. All this provides a basis for more in-depth studies of the role of GSNO in NO metabolism and the possibility of its use as a diagnostic marker or neuroprotective agent in stroke. However, its determination requires specific methods and routine blood collection methods are not suitable due to the fact that level of GSNO in plasma is extremely low (about 100 nM or less), [90]. According to our data, GSNO levels have not yet been determined in either experimental or clinical studies of stroke, and we cannot yet say whether this metabolite undergoes any changes and whether they are associated with the severity or prognosis of the disease. In the present study, it was shown that, firstly, rGSH levels are significantly lower than normal in patients with acute HS, and, secondly, patients with low (<1.9 μM) rGSH levels were characterized by a greater degree of impairment of vital functions. Since rGSH is a NO carrier, it is logical to assume that low rGSH limits the possibility of GSNO formation and thereby creates a deficit in the circulating NO pool. This makes it relevant to conduct detailed studies of the relationship between GSH and NO metabolism and studies on rGSH as a diagnostic marker of HS.
This study has a number of limitations, firstly due to the size of the cohort of patients, which did not allow us to study the influence of, for example, traditional stroke risk factors (diabetes mellitus, dyslipidemia, smoking), hyperhomocysteinemia, age, urine-forming function of the kidneys, etc., on the detected associations. Special attention should also be paid to CAD here. We also do not have information on the dynamics of changes in CysS and rGSH levels in acute HS and on the factors that may have a significant impact on it in the clinic, so we cannot conclude how optimal the time range for blood collection was. With age come changes in the aminothiol system, as well as an increase in the Hcy level and a decrease in the GSH level, which can affect the strength of the association of CysS and rGSH with the severity of HS, but our study did not include elderly people. Thus, additional and larger studies are required to clarify these issues.
5. Conclusions
CysS and rGSH are associated with a reduced risk of severe neurological deficit and serious impairment of patients' disability, respectively, in the acute period of HS. These indicators could be used to evaluate the neurologic impairment severity of stroke patients. On the other hand, it gives grounds to consider these patients as targets for metabolic therapy for HS. However, in both cases, this will require larger-scale studies of changes in aminothiols during the course of the disease, a search for factors that determine the relationship of these metabolites with the clinical characteristics of stroke, and investigations into various approaches aimed at intensifying GSH synthesis.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Comparative characteristics of patients by the degree of disability after HS; Table S2: Comparative characteristics of patients with low and high rGSH levels; Table S3: Comparative characteristics of patients by neurological deficit after HS; Table S4: Comparative characteristics of patients with low and high CysS levels.
Author Contributions
Conceptualization, A.V.I., M.Y.M., M.A.P., and A.A.K.; investigation, A.V.I. and P.A.P.; methodology, A.V.I., M.A.P., and M.P.K.; formal analysis, M.P.G., M.P.K., and V.V.A.; data collection and curation, R.A.M., P.A.P., and V.A.S.; resources, M.A.P. and E.V.S.; writing—original draft preparation, A.V.I., M.A.P., and M.Y.M.; writing—review and editing, A.V.I., M.Y.M., and M.P.G.; supervision, A.V.I. and M.A.P.; project administration, E.V.S. and A.A.K. All authors have read and agreed to the published version of this manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Moscow Regional Research Clinical Institute, Russia (protocol no. 7 from 13 July 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
The complete raw data are not publicly available due to local data protection laws, but de-identified data can be made available upon reasonable request from the corresponding author.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ADC | Apparent diffusion coefficient |
| aPTT | Activated partial thromboplastin time |
| BBB | Blood–brain barrier |
| bGSH | Blood glutathione (reduced) |
| CAD | Coronary artery disease |
| CE-UV | Capillary electrophoresis – ultraviolet detection |
| CT | Computer tomography |
| Cys | Cysteine |
| CysS | Cystine |
| CVD | Cardiovascular disease |
| CβS | Cystathionine beta-synthase |
| GLT-1 | Glutamate transporter-1 |
| GPx4 | GSH peroxidase 4 |
| GSH | Glutathione |
| GSNO | Nitrosoglutathione |
| GSSG | Glutathione disulfide (blood) |
| Hcy | Homocysteine |
| HDL-C | High-density lipoprotein cholesterol |
| HS | Hemorrhagic stroke |
| ICH | Intracerebral hemorrhage |
| IL-6 | Interleukin 6 |
| LDL-C | Low-density lipoprotein cholesterol |
| LOD | Limit of detection |
| MRI | Magnetic resonance imaging |
| mRS | Modified Rankin Scale |
| NAC | N-acetyl-L-cysteine |
| NIHSS | National Institutes of Health Stroke Scale |
| NMDA | N-methyl-D-aspartate |
| OR | Odds ratio |
| OS | Oxidative stress |
| rCys | Reduced cysteine |
| rGSH | Reduced glutathione (plasma) |
| ROC | Receiver operating characteristic |
| RR | Relative risk ratio |
| SAH | Subarachnoid hemorrhage |
| T1 | First tertile |
| T3 | Third tertile |
| TG | Triglycerides |
| tGSH | Total glutathione |
| tHcy | Total homocysteine |
| TOAST | Trial of ORG 10172 in Acute Stroke Treatment |
| WBCs | White blood cells |
| xc− | Cystine/glutamate transporter |
References
- GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef]
- Ananth, C.V. , Brandt, J.S., Keyes, K.M., Graham, H.L., Kostis, J.B., Kostis, W.J. Epidemiology and trends in stroke mortality in the USA, 1975-2019. Int. J. Epidemiol. 2023, 52, 858–866. [Google Scholar] [CrossRef] [PubMed]
- Montaño, A. , Hanley, D.F., Hemphill, J.C. 3rd. Hemorrhagic stroke. Handb. Clin. Neurol. 2021, 176, 229–248. [Google Scholar] [CrossRef] [PubMed]
- Yao, J. , Dai, X., Yv, X., Zheng, L., Zheng, J., Kuang, B., Teng, W., Yu, W., Li, M., Cao, H., Zou, W. The role of potential oxidative biomarkers in the prognosis of intracerebral hemorrhage and the exploration antioxidants as possible preventive and treatment options. Front. Mol. Biosci. 2025, 12, 1541230. [Google Scholar] [CrossRef]
- Ayer, R.E. , Zhang, J.H. Oxidative stress in subarachnoid haemorrhage: significance in acute brain injury and vasospasm. Acta Neurochir. Suppl. 2008, 104, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Wang, D. , Cao, Z., Li, Z., Gu, H., Zhou, Q., Zhao, X., Wang, Y. Homocysteine and Clinical Outcomes in Intracerebral Hemorrhage Patients: Results from the China Stroke Center Alliance. Neuropsychiatr. Dis. Treat. 2022, 18, 2837–2846. [Google Scholar] [CrossRef]
- Zhang, T. , Zhang, L., Nie, K., Yang, J., Lou, H., Wang, J., Huang, S., Gu, C., Yan, M., Zhan, R., Pan, J. Admission Homocysteine as a Potential Predictor for Delayed Cerebral Ischemia After Aneurysmal Subarachnoid Hemorrhage. Front. Surg. 2022, 8, 813607. [Google Scholar] [CrossRef]
- Dai, D. , Sun, Y., Liu, C., Xing, H., Wang, B., Qin, X., Liu, X., Li, A. Association of Glasgow Coma Scale with Total Homocysteine Levels in Patients with Hemorrhagic Stroke. Ann. Nutr. Metab. 2019, 75, 9–15. [Google Scholar] [CrossRef]
- Dhandapani, S. , Goudihalli, S., Mukherjee, K. K., Singh, H., Srinivasan, A., Danish, M., Mahalingam, S., Dhandapani, M., Gupta, S. K., Khandelwal, N., Mathuriya, S. N. Prospective study of the correlation between admission plasma homocysteine levels and neurological outcome following subarachnoid hemorrhage: a case for the reverse epidemiology paradox? Acta Neurochir. (Wien) 2015, 157, 399–407. [Google Scholar] [CrossRef]
- Wei, C. The role of glutathione peroxidase 4 in neuronal ferroptosis and its therapeutic potential in ischemic and hemorrhagic stroke. Brain Res. Bull. 2024, 217, 111065. [Google Scholar] [CrossRef]
- Ivanov, A.V. , Alexandrin, V.V., Paltsyn, A.A., Nikiforova, K A., Virus, E.D., Luzyanin, B.P., Maksimova, M.Y., Piradov, M.A., Kubatiev, A.A. Plasma low-molecular-weight thiol/disulphide homeostasis as an early indicator of global and focal cerebral ischaemia. Redox Rep. 2017, 22, 460–466. [Google Scholar] [CrossRef]
- Higashi, Y. , Aratake, T., Shimizu, T., Shimizu, S., Saito, M. Protective Role of Glutathione in the Hippocampus after Brain Ischemia. Int. J. Mol. Sci. 2021, 22, 7765. [Google Scholar] [CrossRef]
- Lu, H. , Zhang, D.M., Chen, H.L., Lin, Y.X., Hang, C.H., Yin, H.X., Shi, J.X. N-acetylcysteine suppresses oxidative stress in experimental rats with subarachnoid hemorrhage. J. Clin. Neurosci. 2009, 16, 684–8. [Google Scholar] [CrossRef]
- Yabuki, Y. , Fukunaga, K. Oral administration of glutathione improves memory deficits following transient brain ischemia by reducing brain oxidative stress. Neuroscience 2013, 250, 394–407. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.C. Glutathione synthesis. Biochim. Biophys. Acta. 2013, 1830, 3143–3153. [Google Scholar] [CrossRef]
- Larsson, S.C. , Håkansson, N., Wolk, A. Dietary cysteine and other amino acids and stroke incidence in women. Stroke 2015, 46, 922–926. [Google Scholar] [CrossRef] [PubMed]
- Dringen, R. , Arend, C. Glutathione Metabolism of the Brain-The Role of Astrocytes. J. Neurochem. 2025, 169, e70073. [Google Scholar] [CrossRef]
- Maksimova, M.Y.; Ivanov, A.V.; Virus, E.D.; Nikiforova, K.A.; Ochtova, F.R.; Suanova, E.T.; Kruglova, M.P.; Piradov, M.A.; Kubatiev, A.A. Impact of glutathione on acute ischemic stroke severity and outcome: Possible role of aminothiols redox status. Redox Rep. Commun. Free Radic. Res. 2021, 26, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Ivanov, A.V. , Alexandrin, V.V., Paltsyn, A.A., Virus, E.D., Nikiforova, K.A., Bulgakova, P.O., Sviridkina, N.B., Svetlana Alexandrovna Apollonova, Kubatiev, A.A. Metoprolol and Nebivolol Prevent the Decline of the Redox Status of Low-Molecular-Weight Aminothiols in Blood Plasma of Rats During Acute Cerebral Ischemia. J. Cardiovasc. Pharmacol. 2018, 72, 195–203. [Google Scholar] [CrossRef]
- Brott, T.; Adams, H.P.; Olinger, C.P.; Marler, J.R.; Barsan, W.G.; Biller, J.; Spilker, J.; Holleran, R.; Eberle, R.; & Hertzberg, V. Measurements of acute cerebral infarction: A clinical examination scale. Stroke 1989, 20, 864–870. [Google Scholar] [CrossRef]
- Sulter, G.; Steen, C.; De Keyser, J. Use of the Barthel index and modified Rankin scale in acute stroke trials. Stroke 1999, 30, 1538–1541. [Google Scholar] [CrossRef]
- Maksimova, M.Y. , Ivanov, A.V., Virus, E.D., Alexandrin, V.V., Nikiforova, K.A., Bulgakova, P.O., Ochtova, F.R., Suanova, E.T., Piradov, M.A., Kubatiev, A.A. Disturbance of thiol/disulfide aminothiols homeostasis in patients with acute ischemic stroke stroke: Preliminary findings. Clin. Neurol. Neurosurg. 2019, 183, 105393. [Google Scholar] [CrossRef]
- Ivanov, A.V.; Popov, M.A.; Aleksandrin, V.; Pudova, P.A.; Galdobina, M.P.; Metelkin, A.A.; Kruglova, M.P.; Maslennikov, R.A.; Silina, E.V.; Stupin, V.A.; et al. Simultaneous determination of cysteine and other free aminothiols in blood plasma using capillary electrophoresis with pH-mediated stacking. Electrophoresis 2024, 45, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Ivanov, A.V. , Popov, M.A., Aleksandrin, V.V., Kozhevnikova, L.M., Moskovtsev, A.A., Kruglova, M.P., Vladimirovna, S.E., Aleksandrovich, S.V., Kubatiev, A.A. Determination of glutathione in blood via capillary electrophoresis with pH-mediated stacking. Electrophoresis 2022, 43, 1859–1870. [Google Scholar] [CrossRef]
- Ivanov, A.V.; Popov, M.A.; Metelkin, A.A.; Aleksandrin, V.V.; Agafonov, E.G.; Kruglova, M.P.; Silina, E.V.; Stupin, V.A.; Maslennikov, R.A.; Kubatiev, A.A. Influence of Coronary Artery Bypass Grafts on Blood Aminothiols in Patients with Coronary Artery Disease. Metabolites 2023, 13, 743. [Google Scholar] [CrossRef]
- Human IL-6. Platinum ELISA. In Product Information &Manual; BenderMedSystems GmbH Campus Vienna Biocenter 2: Vienna, Austria. 2012. Available online: http://www.ulab360.com/files/prod/manuals/201305/15/376695001.pdf (accessed on 10 March 2025).
- Kaneva, A.M. , Potolitsyna, N.N., Bojko, E.R. Range of values for lipid accumulation product (LAP) in healthy residents of the European north of Russia. Obesity and metabolism 2020, 17, 179–186. [Google Scholar] [CrossRef]
- Andersson, A. , Lindgren, A., Hultberg, B. Effect of thiol oxidation and thiol export from erythrocytes on determination of redox status of homocysteine and other thiols in plasma from healthy subjects and patients with cerebral infarction. Clin. Chem. 1995, 41, 361–366. [Google Scholar] [CrossRef]
- Williams, R.H. , Maggiore, J.A., Reynolds, R.D., Helgason, C.M. Novel approach for the determination of the redox status of homocysteine and other aminothiols in plasma from healthy subjects and patients with ischemic stroke. Clin. Chem. 2001, 47, 1031–1039. [Google Scholar] [CrossRef] [PubMed]
- Carru, C. , Deiana, L., Sotgia, S., Pes, G. M., Zinellu, A.Plasma thiols redox status by laser-induced fluorescence capillary electrophoresis. Electrophoresis 2004, 25, 882–889. [Google Scholar] [CrossRef]
- Katrusiak, A.E. , Paterson, P.G., Kamencic, H., Shoker, A., Lyon, A.W. Pre-column derivatization high-performance liquid chromatographic method for determination of cysteine, cysteinyl-glycine, homocysteine and glutathione in plasma and cell extracts. J. Chromatogr. B Biomed. Sci. Appl. 2001, 758, 207–212. [Google Scholar] [CrossRef]
- Shimizu, H. , Kiyohara, Y., Kato, I., Kitazono, T., Tanizaki, Y., Kubo, M., Ueno, H., Ibayashi, S., Fujishima, M., Iida, M. Relationship between plasma glutathione levels and cardiovascular disease in a defined population: the Hisayama study. Stroke 2004, 35, 2072–2077. [Google Scholar] [CrossRef]
- Akyol, M.E. , Demir, C., Görken, G. Investigation of Oxidative Stress Level and Antioxidant Enzyme Activities in Operated and Nonoperated Patients with Spontaneous Intracerebral Hematoma. J. Neurol. Surg. A Cent. Eur. Neurosurg. 2024, 85, 21–25. [Google Scholar] [CrossRef]
- Chang, M.L. , Klaidman, L.K., Adams, J.D. The effects of oxidative stress on in vivo brain GSH turnover in young and mature mice. Mol. Chem. Neuropathol. 1997, 30, 187–197. [Google Scholar] [CrossRef] [PubMed]
- Guégan, C. , Ceballos-Picot, I., Nicole, A., Kato, H., Onténiente, B., Sola, B. Recruitment of several neuroprotective pathways after permanent focal ischemia in mice. Exp. Neurol. 1998, 154, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Jarocka-Karpowicz, I. , Syta-Krzyżanowska, A., Kochanowicz, J., Mariak, Z.D. Clinical Prognosis for SAH Consistent with Redox Imbalance and Lipid Peroxidation. Molecules 2020, 25, 1921. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, C. , Winnefeld, K., Streck, S., Roskos, M., Haberl, R.L. Antioxidant status in acute stroke patients and patients at stroke risk. Eur. Neurol. 2004, 51, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Gaetani, P. , Pasqualin, A., Rodriguez y Baena, R., Borasio, E., Marzatico, F. Oxidative stress in the human brain after subarachnoid hemorrhage. J. Neurosurg. 1998, 89, 748–754. [Google Scholar] [CrossRef]
- Aygul, R. , Demircan, B., Erdem, F., Ulvi, H., Yildirim, A., Demirbas, F. Plasma values of oxidants and antioxidants in acute brain hemorrhage: role of free radicals in the development of brain injury. Biol. Trace Elem. Res. 2005, 108, 43–52. [Google Scholar] [CrossRef]
- Manolescu, B. N. , Berteanu, M., Oprea, E., Chiriac, N., Dumitru, L., Vladoiu, S., Popa, O., Ianas, O. Dynamic of oxidative and nitrosative stress markers during the convalescent period of stroke patients undergoing rehabilitation. Ann. Clin. Biochem. 2011, 48, 338–343. [Google Scholar] [CrossRef]
- Ozkul, A. , Akyol, A., Yenisey, C., Arpaci, E., Kiylioglu, N., & Tataroglu, C. Oxidative stress in acute ischemic stroke. J. Clin. Neurosci. 2007, 14, 1062–1066. [Google Scholar] [CrossRef]
- Frassetto, S.S. , Schetinger, M.R., Webber, A., Sarkis, J.J., Netto, C.A. Ischemic preconditioning reduces peripheral oxidative damage associated with brain ischemia in rats. Braz. J. Med. Biol. Res. 1999, 32, 1295–1302. [Google Scholar] [CrossRef]
- Mizui, T. , Kinouchi, H., Chan, P.H. Depletion of brain glutathione by buthionine sulfoximine enhances cerebral ischemic injury in rats. Am. J. Physiol. 1992, 262, H313–H317. [Google Scholar] [CrossRef]
- Thilo, F.J. , Bilger, S., Halfens, R.J., Schols, J.M., Hahn, S. Involvement of the end user: exploration of older people's needs and preferences for a wearable fall detection device - a qualitative descriptive study. Patient Prefer Adherence. 2016, 11, 11–22. [Google Scholar] [CrossRef]
- Blum, F. , Hager, C., Taufik, H., Wiesmann, M., Hasan, D., Reich, A., Pinho, J., Nikoubashman, O. Seeing the good in the bad: actual clinical outcome of thrombectomy stroke patients with formally unfavorable outcome. Neuroradiology 2022, 64, 1429–1436. [Google Scholar] [CrossRef]
- Kwon, Y.D. , Yoon, S.S., Chang, H. Association of hospital arrival time with modified rankin scale at discharge in patients with acute cerebral infarction. Eur. Neurol. 2010, 64, 207–213. [Google Scholar] [CrossRef]
- Deng, P.P. , Wu, N., Chen, X.J., Chen, F.L., Xu, H.S., Bao, G.S. NIHSS-the Alberta Stroke Program Early CT Score mismatch in guiding thrombolysis in patients with acute ischemic stroke. J. Neurol. 2022, 269, 1515–1521. [Google Scholar] [CrossRef] [PubMed]
- Bastani, A. , Rajabi, S., Daliran, A., Saadat, H., Karimi-Busheri, F. Oxidant and antioxidant status in coronary artery disease. Biomed Rep. 2018, 9, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Musthafa, Q.A. , Abdul Shukor, M.F., Ismail, N.A.S., Mohd Ghazi, A., Mohd Ali, R., M Nor, I.F., Dimon, M.Z., Wan Ngah, W.Z. Oxidative status and reduced glutathione levels in premature coronary artery disease and coronary artery disease. Free Radic. Res. 2017, 51, 787–798. [Google Scholar] [CrossRef]
- Varadhan, S. , Venkatachalam R., Perumal S.M., Ayyamkulamkara S.S. Evaluation of Oxidative Stress Parameters and Antioxidant Status in Coronary Artery Disease Patients. Arch. Razi. Inst. 2022, 77, 853–859. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.S.; Ghasemzadeh, N.; Eapen, D.J.; Sher, S.; Arshad, S.; Ko, Y.A.; Veledar, E.; Samady, H.; Zafari, A.M.; Sperling, L.; et al. Novel Biomarker of Oxidative Stress Is Associated With Risk of Death in Patients With Coronary Artery Disease. Circulation 2016, 133, 361–369. [Google Scholar] [CrossRef]
- Paterson, P.G. Lyon, A.W., Kamencic, H., Andersen, L.B., Juurlink, B.H. Sulfur amino acid deficiency depresses brain glutathione concentration. Nutr. Neurosci. 2001, 4, 213–22. [Google Scholar] [CrossRef]
- Janáky, R.; Varga, V.; Hermann, A.; Saransaari, P.; Oja, S.S. Mechanisms of L-cysteine neurotoxicity. Neurochem. Res. 2000, 25, 1397–1405. [Google Scholar] [CrossRef]
- Hughes, C.E.; Coody, T.K.; Jeong, M.Y.; Berg, J.A.; Winge, D.R.; Hughes, A.L. Cysteine Toxicity Drives Age-Related Mitochondrial Decline by Altering Iron Homeostasis. Cell 2020, 180, 296–310. [Google Scholar] [CrossRef]
- Blagov, A.; Postnov, A.; Sukhorukov, V.; Popov, M.; Uzokov, J.; Orekhov, A. Significance of Mitochondrial Dysfunction in the Pathogenesis of Parkinson’s Disease. Front. Biosci. Landmark Ed. 2024, 29, 36. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Wang, L.; Hu, Q.; Liu, S.; Bai, X.; Xie, Y.; Zhang, T.; Bo, S.; Gao, X.; Wu, S.; et al. Neuroprotective Roles of l-Cysteine in Attenuating Early Brain Injury and Improving Synaptic Density via the CBS/H2S Pathway Following Subarachnoid Hemorrhage in Rats. Front. Neurol. 2017, 8, 176. [Google Scholar] [CrossRef]
- Cui, Y. , Duan, X., Li, H., Dang, B., Yin, J., Wang, Y., Gao, A., Yu, Z., Chen, G. Hydrogen Sulfide Ameliorates Early Brain Injury Following Subarachnoid Hemorrhage in Rats. Mol. Neurobiol. 2016, 53, 3646–3657. [Google Scholar] [CrossRef]
- Duan, H.Z. , Wu, C.W., Shen, S.L., Zhang, J.Y., Li, L. Neuroprotective Effects of Early Brain Injury after Subarachnoid Hemorrhage in Rats by Calcium Channel Mediating Hydrogen Sulfide. Cell. Mol. Neurobiol. 2021, 41, 1707–1714. [Google Scholar] [CrossRef]
- Cao, S. , Zhu, P., Yu, X., Chen, J., Li, J., Yan, F., Wang, L., Yu, J., Chen, G. Hydrogen sulfide attenuates brain edema in early brain injury after subarachnoid hemorrhage in rats: Possible involvement of MMP-9 induced blood-brain barrier disruption and AQP4 expression. Neurosci. Lett. 2016, 621, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.J.; Chai, C.; Lim, T.W.; Yamamoto, M.; Lo, E.H.; Lai, M.K.; Wong, P.T. Cystathionine β-synthase inhibition is a potential therapeutic approach to treatment of ischemic injury. ASN Neuro. 2015, 7, 1759091415578711. [Google Scholar] [CrossRef] [PubMed]
- Lechpammer, M. , Tran, Y.P., Wintermark, P., Martínez-Cerdeño, V., Krishnan, V. V., Ahmed, W., Berman, R. F., Jensen, F.E., Nudler, E., Zagzag, D. Upregulation of cystathionine β-synthase and p70S6K/S6 in neonatal hypoxic ischemic brain injury. Brain Pathol. 2017, 27, 449–458. [Google Scholar] [CrossRef]
- Omorou, M.; Liu, N.; Huang, Y.; Al-Ward, H.; Gao, M.; Mu, C.; Zhang, L.; Hui, X. Cystathionine beta-Synthase in hypoxia and ischemia/reperfusion: A current overview. Arch. Biochem. Biophys. 2022, 718, 109149. [Google Scholar] [CrossRef]
- Qu, K. , Chen, C.P., Halliwell, B., Moore, P.K., Wong, P.T. Hydrogen sulfide is a mediator of cerebral ischemic damage. Stroke 2006, 37, 889–893. [Google Scholar] [CrossRef]
- Wong, P.T.; Qu, K.; Chimon, G.N.; Seah, A.B.; Chang, H.M.; Wong, M.C.; Ng, Y.K.; Rumpel, H.; Halliwell, B.; Chen, C.P. High plasma cyst(e)ine level may indicate poor clinical outcome in patients with acute stroke: Possible involvement of hydrogen sulfide. J. Neuropathol. Exp. Neurol. 2006, 65, 109–115. [Google Scholar] [CrossRef]
- McCune, C.D.; Chan, S.J.; Beio, M.L.; Shen, W.; Chung, W.J.; Szczesniak, L.M.; Chai, C.; Koh, S.Q.; Wong, P.T.; Berkowitz, D.B. “Zipped Synthesis” by Cross-Metathesis Provides a Cystathionine β-Synthase Inhibitor that Attenuates Cellular H2S Levels and Reduces Neuronal Infarction in a Rat Ischemic Stroke Model. ACS Cent. Sci. 2016, 2, 242–252. [Google Scholar] [CrossRef]
- Scheid, S. , Goeller, M., Baar, W., Wollborn, J., Buerkle, H., Schlunck, G., Lagrèze, W., Goebel, U., Ulbrich, F. Hydrogen Sulfide Reduces Ischemia and Reperfusion Injury in Neuronal Cells in a Dose- and Time-Dependent Manner. Int. J. Mol. Sci. 2021, 22, 10099. [Google Scholar] [CrossRef]
- Han, M. , Liu, D., Qiu, J., Yuan, H., Hu, Q., Xue, H., Li, T., Ma, W., Zhang, Q., Li, G., Wang, Z. Evaluation of H2S-producing enzymes in cerebrospinal fluid and its relationship with interleukin-6 and neurologic deficits in subarachnoid hemorrhage. Biomed. Pharmacother. 2020, 123, 109722. [Google Scholar] [CrossRef] [PubMed]
- Hendrix, P. , Foreman, P.M., Harrigan, M.R., Fisher, W S., Vyas, N.A., Lipsky, R.H., Lin, M., Walters, B.C., Tubbs, R S., Shoja, M.M., Pittet, J.F., Mathru, M., Griessenauer, C.J. Association of cystathionine beta-synthase polymorphisms and aneurysmal subarachnoid hemorrhage. J. Neurosurg. 2018, 128, 1771–1777. [Google Scholar] [CrossRef] [PubMed]
- Grobelny, B.T. , Ducruet, A.F., DeRosa, P.A., Kotchetkov, I.S., Zacharia, B.E., Hickman, Z.L., Fernandez, L., Narula, R., Claassen, J., Lee, K., Badjatia, N., Mayer, S A., Connolly, E.S., Jr. Gain-of-function polymorphisms of cystathionine β-synthase and delayed cerebral ischemia following aneurysmal subarachnoid hemorrhage. J. Neurosurg. 2011, 115, 101–107. [Google Scholar] [CrossRef]
- Aoyama, K.; Nakaki, T. Impaired glutathione synthesis in neurodegeneration. Int. J. Mol. Sci. 2013, 14, 21021–21044. [Google Scholar] [CrossRef] [PubMed]
- Burdo, J.; Dargusch, R.; Schubert, D. Distribution of the cystine/glutamate antiporter system xc− in the brain, kidney, and duodenum. J. Histochem. Cytochem. 2006, 54, 549–557. [Google Scholar] [CrossRef]
- Massie, A.; Boillée, S.; Hewett, S.; Knackstedt, L.; Lewerenz, J. Main path and byways: Non-vesicular glutamate release by system xc− as an important modifier of glutamatergic neurotransmission. J. Neurochem. 2015, 135, 1062–1079. [Google Scholar] [CrossRef]
- He, Y.; Hewett, S.J. The Cystine/Glutamate Antiporter, System xc−, Contributes to Cortical Infarction After Moderate but Not Severe Focal Cerebral Ischemia in Mice. Front. Cell Neurosci. 2022, 16, 821036. [Google Scholar] [CrossRef]
- Lee, B.J.; Jun, H.O.; Kim, J.H.; Kim, J.H. Astrocytic cystine/glutamate antiporter is a key regulator of erythropoietin expression in the ischemic retina. FASEB J. 2019, 33, 6045–6054. [Google Scholar] [CrossRef]
- Liu, T.; Cui, Y.; Dong, S.; Kong, X.; Xu, X.; Wang, Y.; Wan, Q.; Wang, Q. Treadmill Training Reduces Cerebral Ischemia-Reperfusion Injury by Inhibiting Ferroptosis through Activation of SLC7A11/GPX4. Oxid. Med. Cell. Longev. 2022, 2022, 8693664. [Google Scholar] [CrossRef] [PubMed]
- Heit, B.S.; Chu, A.; McRay, A.; Richmond, J.E.; Heckman, C.J.; Larson, J. Interference with glutamate antiporter system xc− enables post-hypoxic long-term potentiation in hippocampus. Exp. Physiol. 2024, 109, 1572–1592. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.H.; Lin, Y.J.; Chen, W.L.; Huang, Y.C.; Chang, C.W.; Cheng, F.C.; Liu, R.S.; Shyu, W.C. HIF-1α triggers long-lasting glutamate excitotoxicity via system xc− in cerebral ischaemia-reperfusion. J. Pathol. 2017, 241, 337–349. [Google Scholar] [CrossRef]
- Soria, F.N.; Pérez-Samartín, A.; Martin, A.; Gona, K.B.; Llop, J.; Szczupak, B.; Chara, J.C.; Matute, C.; Domercq, M. Extrasynaptic glutamate release through cystine/glutamate antiporter contributes to ischemic damage. J. Clin. Investig. 2014, 124, 3645–3655. [Google Scholar] [CrossRef] [PubMed]
- Raghu, G. , Berk, M., Campochiaro, P.A., Jaeschke, H., Marenzi, G., Richeldi, L., Wen, F Q., Nicoletti, F., Calverley, P.M.A. The Multifaceted Therapeutic Role of N-Acetylcysteine (NAC) in Disorders Characterized by Oxidative Stress. Curr. Neuropharmacol. 2021, 19, 1202–1224. [Google Scholar] [CrossRef]
- Sabetghadam, M. , Mazdeh, M., Abolfathi, P., Mohammadi, Y., Mehrpooya, M. Evidence for a Beneficial Effect of Oral N-acetylcysteine on Functional Outcomes and Inflammatory Biomarkers in Patients with Acute Ischemic Stroke. Neuropsychiatr. Dis. Treat. 2020, 16, 1265–1278. [Google Scholar] [CrossRef]
- Karuppagounder, S.S. , Alin, L., Chen, Y., Brand, D., Bourassa, M.W., Dietrich, K., Wilkinson, C.M., Nadeau, C.A., Kumar, A., Perry, S., Pinto, J.T., Darley-Usmar, V., Sanchez, S., Milne, G.L., Pratico, D., Holman, T.R., Carmichael, S.T., Coppola, G., Colbourne, F., Ratan, R.R. N-acetylcysteine targets 5 lipoxygenase-derived, toxic lipids and can synergize with prostaglandin E2 to inhibit ferroptosis and improve outcomes following hemorrhagic stroke in mice. Ann. Neurol. 2018, 84, 854–872. [Google Scholar] [CrossRef]
- Diao, X. , Zhou, Z., Xiang, W., Jiang, Y., Tian, N., Tang, X., Chen, S., Wen, J., Chen, M., Liu, K., Li, Q., Liao, R. Glutathione alleviates acute intracerebral hemorrhage injury via reversing mitochondrial dysfunction. Brain Res. 2020, 1727, 146514. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.Q. , Mou, R.T., Feng, D.X., Wang, Z., Chen, G. The role of nitric oxide in stroke. Med. Gas. Res. 2017, 7, 194–203. [Google Scholar] [CrossRef]
- Khan, M. , Sakakima, H., Dhammu, T. S., Shunmugavel, A., Im, Y. B., Gilg, A. G., Singh, A. K., Singh, I. S-nitrosoglutathione reduces oxidative injury and promotes mechanisms of neurorepair following traumatic brain injury in rats. J. Neuroinflammation 2011, 8, 78. [Google Scholar] [CrossRef]
- Khan, M. , Dhammu, T.S., Sakakima, H., Shunmugavel, A., Gilg, A.G., Singh, A.K., Singh, I. The inhibitory effect of S-nitrosoglutathione on blood-brain barrier disruption and peroxynitrite formation in a rat model of experimental stroke. J. Neurochem. 2012, 123, 86–97. [Google Scholar] [CrossRef]
- Khan M, Dhammu TS, Matsuda F, et al. Blocking a vicious cycle nNOS/peroxynitrite/AMPK by S-nitrosoglutathione: implication for stroke therapy. BMC Neurosci. 2015, 16, 42. [Google Scholar] [CrossRef]
- Zaidi, S.K. , Ahmed, F., Alkhatabi, H., Hoda, M.N., Al-Qahtani, M. Nebulization of Low-Dose S-Nitrosoglutathione in Diabetic Stroke Enhances Benefits of Reperfusion and Prevents Post-Thrombolysis Hemorrhage. Biomolecules 2021, 11, 1587. [Google Scholar] [CrossRef]
- Sehba, F.A. , Ding, W.H., Chereshnev, I., Bederson, J.B. Effects of S-nitrosoglutathione on acute vasoconstriction and glutamate release after subarachnoid hemorrhage. Stroke 1999, 30, 1955–1961. [Google Scholar] [CrossRef] [PubMed]
- Liu, S. , Zheng, H., Yu, W., Ramakrishnan, V., Shah, S., Gonzalez, L.F., Singh, I., Graffagnino, C., Feng, W. Investigation of S-Nitrosoglutathione in stroke: A systematic review and meta-analysis of literature in pre-clinical and clinical research. Exp. Neurol. 2020, 328, 113262. [Google Scholar] [CrossRef] [PubMed]
- Bramanti, E. , Angeli, V., Mester, Z., Pompella, A., Paolicchi, A., D'Ulivo, A. Determination of S-nitrosoglutathione in plasma: comparison of two methods. Talanta 2010, 81, 1295–1299. [Google Scholar] [CrossRef]
Figure 1.
Association of disability with rGSH level (A) and neurological deficit with CysS level (B) in patients with acute HS. At the top are the ROC curves with the corresponding AUCs (and its CI95%). Below are the contingency tables corresponding to the splitting criteria, RR or OR values. AUC, area under curve; CysS, plasma cysteine; HS, hemorrhagic stroke; mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; OR, odds ratio; rGSH, plasma reduced glutathione; RR, relative ratio.
Figure 1.
Association of disability with rGSH level (A) and neurological deficit with CysS level (B) in patients with acute HS. At the top are the ROC curves with the corresponding AUCs (and its CI95%). Below are the contingency tables corresponding to the splitting criteria, RR or OR values. AUC, area under curve; CysS, plasma cysteine; HS, hemorrhagic stroke; mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; OR, odds ratio; rGSH, plasma reduced glutathione; RR, relative ratio.
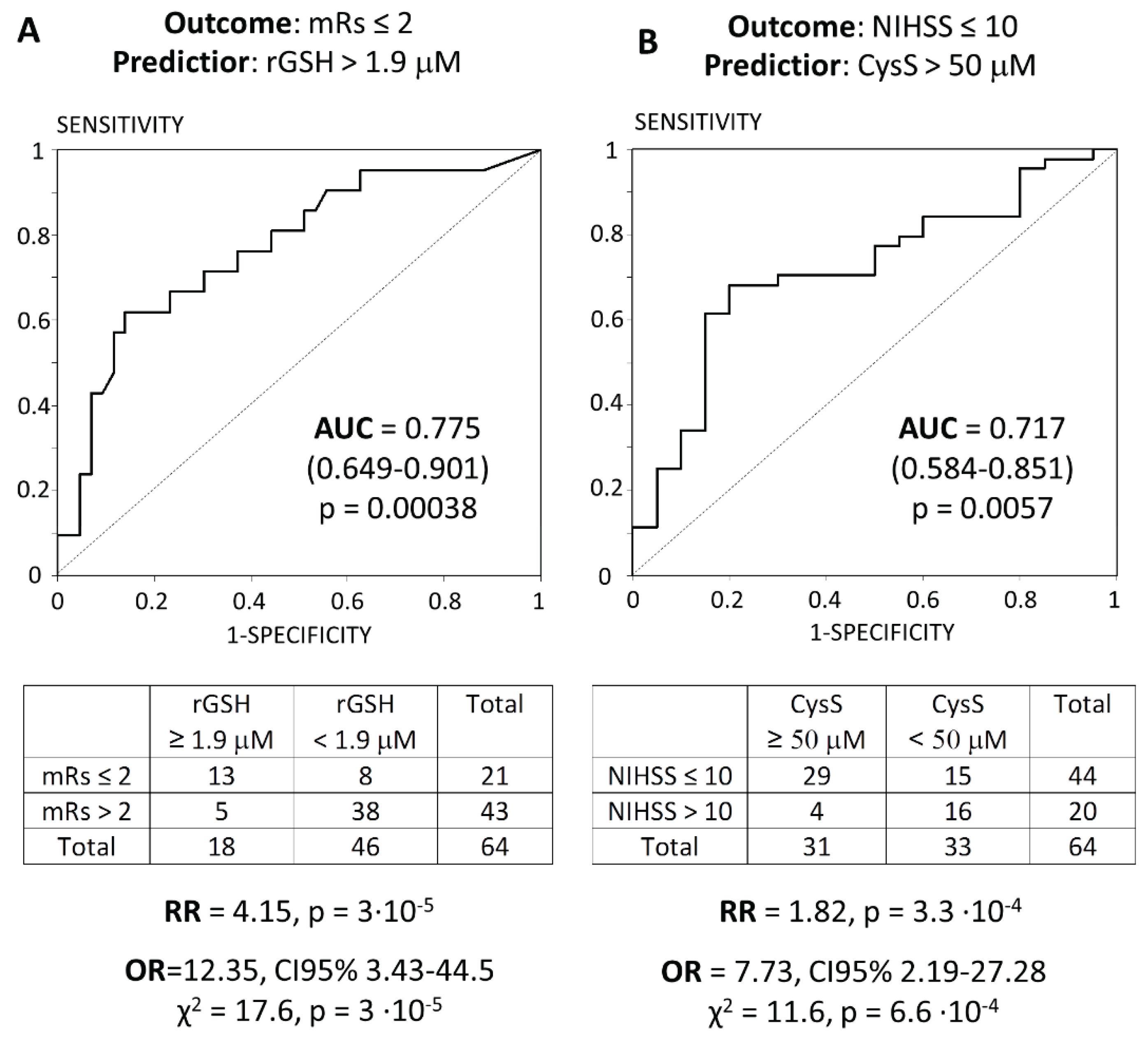

Table 1.
Characteristics of patients with HS.
| Characteristics | Whole cohort | ICH | SAH |
|---|---|---|---|
| Number of patients | 64 | 12 | 52 |
| Age, years | 55 (49; 58) | 50.5 (47; 55) | 55.5 (49.3; 58) |
| Man (%) | 51 (79.7) | 10 (83.3) | 41 (78.8) |
| NIHSS | 8.5 (7.0; 15.5) | 9.0 (6.25; 16) | 8.0 (7.0; 13.3) |
| mRS | 3 (2;3) | 3 (2; 3.75) | 3 (2; 3) |
| Risk factors | |||
| Hypertension, n (%) | 36 (56.3) | 6 (50) | 30 (57.7) |
| CAD, n (%) | 34 (53.1) | 9 (75) | 25 (48.1) |
| Atrial fibrillation, n (%) | 36 (56.3) | 6 (50) | 30 (57.7) |
| High atherogenic coefficient, n (%) | 35 (54.7) | 5 (41.7) | 29 (55.8) |
| Current cigarette smoking, n (%) | 57 (89.1) | 9 (75) | 48 (92.3) |
| Alcohol drinker, n (%) | 34 (53.1) | 8 (66.7) | 26 (50) |
| Hyperhomocysteinemia (Hcy > 15 μM), % | 20.3 | 25 | 19.2 |
| Laboratory findings | |||
| Total cholesterol, mM | 3.5 (1.5; 3.9) | 3.5 (1.7; 3.6) | 3.5 (1.5; 4.0) |
| TG, mM | 2.1 (1.7; 2.7) | 1.95 (1.1; 2.68) | 2.1 (1.85; 2.7) |
| HDL-C, mM | 1.2 (1.1; 1.4) | 1.35 (1.2; 1.7) | 1.2 (0.98; 1.3) |
| LDL-C, mM | 2.4 (2.1; 3.4) | 2.05 (1.9; 2.4) | 2.4 (2.2; 3.6) |
| Glucose, mM | 4.8 (4.7; 5.1) | 4.8 (4.8; 5.75) | 4.8 (4.7; 5.1) |
| aPTT, s | 33 (27; 35) | 32 (27; 36.5) | 33 (27; 35) |
| Fibrinogen, g/L | 3.9 (3.7; 3.9) | 3.9 (3.83; 3.9) | 3.8 (3.7; 3.9) |
| WBC,109/L | 7 (6; 8) | 7 (7; 9.5) | 7 (6; 8) |
| PLT,109/L | 278 (234; 311) | 278 (278; 300) | 278 (234; 311) |
| Ferritin, μg/L | 75 (45; 80) | 75 (39; 76.5) | 75 (45; 82.5) |
| Hcy, μM | 9.8 (7.5; 14.6) | 8.7 (6.2; 15.0) | 10.1 (7.8; 14.5) |
| Free plasma thiols | |||
| rCys, μM | 15.1 (7.4; 18.7) | 13.8 (8.1; 17.4) | 15.6 (6.3; 19.0) |
| CysS, μM | 51.1 (36.5; 63.1) | 57.3 (37.2; 66.8) | 50.2 (35.7; 62.1) |
| rGSH, μM | 1.04 (0.33; 2.00) | 0.79 (0.34; 1.96) | 1.09 (0.33; 2.04) |
| Blood GSH | |||
| bGSH, μM | 827 (689; 994) | 812 (739; 984) | 846 (678; 994) |
| GSSG, μM | 3.35 (2.12; 4.38) | 2.57 (2.18; 4.18) | 3.41 (2.03; 4.43) |
aPTT, activated partial thromboplastin time; bGSH, blood reduced glutathione; CAD, coronary artery disease; CysS, plasma cysteine; GSSG, blood oxidized glutathione; Hcy, plasma total homocysteine; HDL-C, high-density lipoprotein cholesterol; HS, hemorrhagic stroke; ICH, intracerebral haemorrhage; LDL-C, low-density lipoprotein cholesterol; mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; PLT, platelets; rCys, plasma reduced cysteine; rGSH, plasma reduced glutathione; SAH, subarachnoid hemorrhage; TG, triglycerides; WBC, white blood cells..
Table 2.
Comparative characteristics of patients by the degree of disability after stroke.
| Indicator | mRS ≤ 2 (N=21) | mRS > 2 (N=43) | pMann-U |
|---|---|---|---|
| Age, y | 55 (49; 58) | 55 (49; 57) | > .05 |
| Man (%) | 17 (81) | 34 (79.1) | > .05 |
| rGSH, μM | 2.06 (0.93; 3.24) | 0.61 (0.16; 1.34) | 0.0026 |
| GSSG, μM | 2.78 (2.24; 4.00) | 3.35 (1.79; 4.37) | > .05 |
| bGSH, μM | 804 (690; 936) | 839 (689; 1003) | > .05 |
| CysS, μM | 56.8 (45.7; 64.6) | 44.3 (32.5; 59.4) | > .05 |
| rCys, μM | 15.4 (8.6; 21.9) | 14.7 (7.4; 18.1) | > .05 |
bGSH, blood reduced glutathione; CysS, plasma cysteine; GSSG, blood oxidized glutathione; modified Rankin Scale; rCys, plasma reduced cysteine; rGSH, plasma reduced glutathione.
Table 3.
Comparative characteristics of patients by neurological deficit after stroke.
| Indicator | NIHSS ≤ 10 (N=44) | NIHSS > 10 (N=20) | pMann-U |
|---|---|---|---|
| Age, y | 55 (49; 57) | 55 (49.5; 58) | > .05 |
| Man (%) | 36 (81.8) | 15 (75) | > .05 |
| CysS, μM | 54.7 (41.3; 64.6) | 43.0 (32.6; 49.4) | .011 |
| rGSH, μM | 1.12 (0.32; 2.08) | 0.59 (0.33; 1.83) | > .05 |
| GSSG, μM | 3.36 (2.06; 4.26) | 3.28 (1.98; 4.53) | > .05 |
| bGSH, μM | 839 (701; 994) | 817 (611; 877) | > .05 |
| rCys, μM | 16.5 (7.8; 19.1) | 10.8 (5.9; 17.5) | > .05 |
bGSH, blood reduced glutathione; CAD, coronary artery disease; CysS, plasma cysteine; GSSG, blood oxidized glutathione; NIHSS, National Institutes of Health Stroke Scale; rCys, plasma reduced cysteine; rGSH, plasma reduced glutathione.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



