
Submitted:
20 October 2025
Posted:
24 October 2025
You are already at the latest version
Abstract
Nanotechnology has transformed all fields of medicine for years, and the most modern patient care in medicine is now closely tied to the use of nanotechnology and nanomaterials, with dentistry being no exception. Since biomaterials interact with tissues through their surface activities after implantation, the properties of their reactivity are critical in controlling biological response in bone regeneration and repair. New bone-like nanostructures of calcium phosphate have been developed to repair and replace damaged or brittle bone. Chronic apical periodontitis is an inflammation of the dental and periapical tissues produced by a variety of bacteria that generate an immune-inflammatory response in the microorganism. Untreated teeth may need to be removed or undergo periapical surgery to be saved. For that reason, it is desired to build biomimetic nanostructured engineering scaffolds that provide structural support for early cell attachment while developing novel materials. Recently, attention has been drawn to bone-like biomaterials, which have the potential to replace bone as a natural functional nanostructure in certain applications. The proposed workflow includes: (1) material preparation; (2) material characteristics; (3) clinical follow-up design; (4) clinical protocol; (5) clinical outcome. The clinical use of hydroxyapatite/hyaluronan biomimetic nano-hybrid material for reconstruction of periapical bone defects in the treatment of teeth with chronic apical periodontitis is presented in this paper.
Keywords:
biomimetic
; chronic apical periodontitis
; hydroxyapatite
; hybrid hydroxyapatite
; hyaluronan
1. Introduction
Chronic apical periodontitis (CAP) is clinically defined by alterations in the surrounding bone structure and periodontal ligament, and changes in the cementum and dentine, among other things [1,2]. When it comes to CAP, the anatomically separated physiological narrowing is either missing or greatly enlarged in a large proportion of instances. It has been discovered that there is intra- and extraforaminal resorption in the apical zone, as a result of chronic inflammation. A clinical finding that is more uncommon is inflammatory internal root resorption with CAP, which may occur because of trauma to the tooth [3].
The contemporary principles of preparation techniques and knowledge of the root canal morphology are all essential so that appropriate chemo-mechanical cleaning and disinfection of the entire root canal system are achieved. Nowadays, dental practice is related to the continuous improvement of clinical techniques and materials. But the problems related to the treatment process have not yet been eliminated. Finally, endodontic failures are strongly linked to the correct diagnosis. Endodontic treatment procedures in some teeth are still a challenge in clinical practice. One of the main principles of endodontic science is the preparation and conditioning of the dentin walls and three-dimensional root canal filling after that, with a focus on filling the apical third of the root. Obturation becomes a more predictable stage when the walls of the root canal form a physiological narrowing apically, suggesting the preparation of an apical stop that facilitates the proper application of the chosen filling method [4,5,6]. Consequently, it is desirable to design innovative materials and construct biomimetic nanostructured engineering scaffolds that give structural support for early cell attachment while also producing biomimetic nanostructured engineering scaffolds [7,8]. Clinical studies have shown that the observance of aseptic preparation of the endodontic space and the availability of a distance from the apical pulp tissue stimulate the natural healing process. If an appropriate sealer is chosen, the healing occurs with the formation of cement-like tissue [3,9]. There is a resorption lesion on the root tip in many cases with periapical bone lesions. This resorption process is very difficult to diagnose. During a time of clinical intervention, the clinician must assess and measure the width of the apical foramen and establish the absence of apical narrowing. If the resorption of the apical part of the tooth has been diagnosed, the clinician has to condition the dentin and seal it with a precise technique and materials [10,11,12,13].
A variety of materials and methods that partly mimic natural ones have been introduced in medicine, particularly dentistry, in the past few decades. “Biomimicry" or "Biomimetics" describes the technique of taking inspiration from nature for artificial design. Biomimicry (from the Greek bios, which means "life," and mimesis, which means "to copy") examines nature's most successful achievements and then replicates them to introduce additional materials [14,15].
The materials that possess biomimetic characteristics and are nanostructured provide promising results in today’s dentistry. In addition, the nanostructured materials offered a more suitable architecture for normal cell attachment, osteoblast development, and osteoblast function. Dental ceramics and orthopaedical ceramics are two branches of biomaterials that offer a range of materials for use in biomedical applications such as dentistry and orthopaedics [16]. Nanostructured surfaces and materials are a new trend in Dental medicine [17,18]. Significant potential solutions to problems in medicine and dentistry are provided by new biomaterials with controlled nano-features and engineering techniques such as coating, modelling, functionalization and molecular nanoscale grafting.
This study aims to present a preparation protocol of hydroxyapatite/hyaluronan (HA/HyA) biomimetic nano-hybrid material, a description of the material characteristics and clinical application of nano-hybrid material in contemporary endodontic treatment.
2. Materials and Methods
2.1. Material Preparation Protocol
Under controlled temperature and pH = 10.5–11 conditions, biphasic calcium phosphate was prepared by sintering a precursor precipitate sample obtained by the chemical wet precipitation method in a typical process by double decomposition of 1M calcium nitrate solution (prepared from Ca(NO3)2x4H2O) in de-ionized water and di-ammonium hydrogen phosphate (prepared with (NH4)2HP04, 0.6 M) in stoichiometric. But there are some inherent disadvantages to this method, including difficulty in maintaining pH values greater than 9, difficulty in avoiding the formation of Ca-deficient HA, which during the sintering process forms tertiary calcium phosphate, and difficulty in controlling the pH value greater than pH = 9. An agate planetary ball mill (‘pulverisette Fritsch) running in a programmed manner with agate balls (10 mm diameter) was used to dry mill the sintered material after it had been sintered. The standard mass of the sample was 30g, and the mill speed was 600 rev/min. After 40 hours of milling, nano-crystalline HA (nHA) was formed, which was then utilized to create nano-hybrids from HyANa solution in various ratios of HA/HyA-Na.
Powder XRD was used to determine the phase content and crystallite sizes of nanohybrid samples made from 40-hour milled HA and HyA in a 3:1 ratio. The samples were treated to a second wet milling for 2 and 5 hours and then characterized for phase content and crystallite sizes. A 10% concentration of hyaluronan (designated as L) was combined with nHA milled material (designated as S) in a variety of empirically selected ratios ranging from 0.2 to 3.3 S/L. As dense pastes, samples were made from the acquired combined ingredients and placed in rubber moulds with diameters of 10 mm and heights of 5 mm, where they were left to dry in the open air for 24 hours at room temperature. The Vicar Needle technique was used to determine the start and ultimate setting times of the nanohybrid material that was created in the rubber moulds and then dried (ASTM C191-9 1993)[19].
2.2. Material Characteristics
EDTA complex-metrically titration and potentiometrically were used to measure the concentration of calcium in the sintered material. At pH = 10, a Cu ion-selective electrode and a Cu/AgCl reference electrode were used to measure the concentration of calcium in the material. In order to measure the concentration of P-PO4 3– spectrophotometrically, we used NOVA 60 equipment with Merck and Spectroquant® kits. For the scanning electron microscopy (SEM) study, nano-metric materials were mixed with water, put on specimen stubs, dried, and then coated with conductive material (Au) to be viewed in the SEM JEOL JSM-5510 at an accelerating voltage of 10 kV and an electron beam current of 2–20 nA to see the texture of nano-metric agglomerations after dry milling for 40 hours. They were put in deionized water and sonicated for 15 minutes. Then, they were placed on formvar-coated M grids and examined in a JEOL JEM-2100 TEM at 200kV. Ten minutes after grinding them in an agate mortar, they were suspended in de-ionized water and sonicated for 15 minutes. It took 20 minutes for the supernatant to set up. The supernatant was then collected and re-dropped on formvar-coated grids and TEM JEOL JEM-2100 at 200 kV to see [19].
2.3. Retrospective Clinical Follow-Up Design
This study included the patients referred to our clinical practice for endodontic treatment with periapical bone lesions with Periapical index - PAI3 to PAI5. This clinical follow-up was done in accordance with the Declaration of Helsinki. Informed consent was obtained from the patients who met the inclusion criteria and were willing to participate in the study after being briefed on the aim of the study and its method. The main inclusion criteria were that patients had no severe systemic diseases, had to be followed up for a ten-year period, and the tooth had to be mobile. No retained apical narrowing/constriction - the dimensions of the apical foramen were larger than #0.50 ISO. At the beginning of this study, 18 patients were considered for inclusion, but only 12 patients (12 endodontically treated teeth) fulfilled the strict control examination (n =12). The mean age of the participants was 39.3 ± 9.1 years (n = 12), with individual ages ranging from 25 to 57 years. This distribution indicates that the study group encompassed both younger and older adults, thereby providing a representative age variation for the investigated clinical condition. Control radiographs were taken immediately after filling and periodically at the third and sixth months, and at the first, fourth, and tenth years.
2.4. Clinical Protocol
The endodontic treatments of the teeth were performed under a dental operating microscope Zeiss Opmi Pico (Zeiss, Oberkochen, Germany). The root canals were prepared using ProTaper Universal instruments (Dentsply Sirona, Charlotte, North Carolina, USA), calibrated with hand K-files (Dentsply Sirona, Charlotte, North Carolina, USA) and classic endodontic irrigating protocol – 5.25% NaOCl, 17% EDTA and distilled water. The endodontic space was ozonated for maximum decontamination - Ozonytron (MIO Int. Ozonytron GmbH, Germany). Ozone was applied for 40 sec. – 40 μg/ml for a volume of 1–3 cc three times during the endodontic treatment process. At the final preparation stage of the endodontic space of the tooth with a periapical bone lesion, a hybrid HA/HyA biomimetic nano-hybrid material was applied, and after that, the root canal was obturated with bioceramic sealer TotalFill (FKG Dentaire SA, La Chaux-de-Fonds, Switzerland) and gutta-percha. It is known that hyaluronic acid and synthetic calcium phosphate have osteoconductive and biodegradable qualities, and this was shown in the clinical case that we have reported [20].
The development of inorganic nano-sized crystalline hydroxyapatite (nHA) is now the focus of major studies due to the crystallite size, active surface, and possible biological activity of nano-sized crystalline hydroxyapatite (nHA) [21,22,23]. Moreover, nHA particles will provide an increased ratio of high surface area to volume, and their ultra-fine structure, similar to biological apatite, can suitably affect their biological activity in biomedical applications. Recently, HA at the nanoscale has begun to play an increasingly important role in a variety of biological applications [24,25]. Generally, the focus is based on nHA as filler in combination with biodegradable natural or synthetic polymers. It was demonstrated that a HyA matrix is a promising biomimetic material [26,27]. According to these investigations, HyA-containing scaffold materials are effective in bone resorption and regeneration. In the medical community, HyA is commonly referred to as hyaluronan or hyaluronate (Na salts of hyaluronic acid) [28,29], which is a linear glycosaminoglycan polysaccharide composed of repeated disaccharide units of negatively charged high–molecular–weight linear polymer, with repeated units of N-acetyl glucosamine and glucuronic acid, and in water, they form three dimensional (3D) network [30,31].
2.5. Follow-Up and Outcome
It was found in general that the repair of the periapical lesions depends on the achievement of maximum apical and coronal sealing. For clinical purposes, it is important to stress that:
- The result of healing was evaluated using an X-ray examination as well as the periapical index scoring method developed by Ørstavik, which ranged from an initial PAI4 to PAI1 [32].
- The follow-up process demonstrates good clinical and radiographic healing possibilities.
- The use of hybrid HA/HyA biomimetic nano-hybrid material in the treatment of chronic apical lesions as an attempt to improve a regenerative healing process and to create conditions for exact canal obturation.
The orthograde treatment of severe periapical lesions in combination with apical resorption can heal with good bone regeneration after adequate decontamination and the creation of a biomimetic apical stop. The orthograde application of promising nanosized biphasic calcium phosphate materials stimulates the mechanisms of complete bone regeneration, as well as in cases with critical-size apical bone defects.
2.6. Statistical Analysis
The results from this study were analyzed using descriptive statistical analysis, the Friedman test, and post-hoc Wilcoxon signed-rank tests with Holm correction. The analysis was performed using SPSS Statistics version 28 (IBM Corp., Armonk, NY, USA).
3. Results
Following the 40-hour milling process, the morphological characterization of the obtained nHA material revealed a continuous decrease in particle sizes until a certain lower size limit was reached, at which point many defects in the crystal lattice are accumulated and the phase of TCP is almost completely transformed into an amorphous phase, as previously demonstrated [33]. The aggregates are randomly formed, with some of them connecting with one another to create considerably bigger and porous agglomerates when they come into contact. It is likely that these agglomerates are secondary assemblies that have developed because of the preparation process for SEM analysis (Figure 1 and Figure 2).
The sonication procedure used for the TEM sample preparation allows for substantially excluding the secondary aggregation and observing the actual microstructure of the milled material. This case is well illustrated in Figure 3, where two steady aggregates with sizes 300×500 and 200×300 nm are shown.
The healing process of monitored cases showed satisfactory periapical bone regeneration. In general, the repair of the periapical lesions depends on the achievement of maximum apical and coronal sealing. The appropriate characteristics of materials used for apical sealing and periapical bone stimulations are of particular importance. For clinical point, it is important to stress that the result of healing was evaluated using an X-ray examination as well as the periapical index scoring method introduced by Ørstavik, which ranged from an initial score PAI3 to PAI5 to postoperative index PAI4 to PAI1 [32]. The results are presented in Table 1. The cases with preoperative PAI5 were n=7 (58.3%), PAI4 - n=2 (16.6%) and PAI3 - n=3 (25%), respectively. The follow-up process shows that six cases (50%) healed from PAI5 to PAI1 by the fourth year. Two of these cases remained at PAI1 until the tenth year, and three healed to a normal radiographic periapical structure. One of these cases (n=1; 8.3%) exhibits symptoms of relapse and return to PAI2 at the tenth year (N3). In the greater percentage of cases (n=11; 91.6%), the healing process in the periapical area is satisfactory, and on radiographic observation, the restoration of the destroyed bone structure with normal characteristics is presented (N4). This case is presented in Figure 4A-H.
The graphic representation clearly shows a progressive decrease in the PAI index over time, with the values already stabilizing at a very low level after the 4th year - PAI1 to PAI0 (Figure 5).
The statistical analysis by the Friedman test demonstrated a highly significant difference in PAI scores across the four observation periods (χ² = 33.34, p < 0.001).
Following the global analysis, post-hoc Wilcoxon signed-rank tests were conducted to evaluate pairwise differences in PAI scores across the observation periods (Preop (Preoperative), 1st year, 4th year, and 10th year). The comparisons of interest included Preop versus 1st year, Preop versus 4th year, Preop versus 10th year, 1st year versus 4th year, and 1st year versus 10th year. The Holm procedure was applied to control for type I error arising from multiple testing.
The results demonstrated statistically significant reductions in PAI scores between Preop and all subsequent time points. Specifically, the Preoperative versus 1st-year comparison revealed a marked improvement (W = 0.0, adjusted p = 0.0138), indicating substantial healing within the first year postoperatively. Even more pronounced differences were observed for Baseline versus 4th year and Preop versus 10th year, both yielding highly significant outcomes (W = 0.0, adjusted p = 0.0029). These findings support the interpretation that periapical healing progresses steadily over time and that the clinical improvements established in the first year are further consolidated over the longer term. Comparisons between consecutive postoperative intervals also confirmed ongoing, statistically significant improvements. The 1st-year versus 4th-year analysis showed a significant reduction in PAI (W = 0.0, adjusted p = 0.0083), highlighting continued periapical repair during the medium-term follow-up. Similarly, the 1st year versus 10th year comparison produced strong evidence of long-term benefit (W = 0.0, adjusted p = 0.0029). Interestingly, no cases demonstrated a worsening of periapical status over time, further supporting the durability of the clinical outcomes. Taken together, these findings indicate that the intervention was associated with progressive and sustained periapical healing. Initial improvements were evident as early as the first postoperative year, with further statistically significant gains documented at both 4 and 10 years. The consistent pattern across all comparisons underscores the robustness and long-term predictability of the treatment effect. The detailed results of the post-hoc Wilcoxon signed-rank analyses, including W-statistics and Holm-adjusted p-values for each pairwise comparison, are presented in Table 2.
For clarity, both the Raw p-values obtained from the Wilcoxon signed-rank tests and the Holm-adjusted p-values are presented. While the raw values indicate strong statistical significance, the adjusted values provide a more conservative estimate that still supports the robustness of the observed differences across time points. In addition to significance testing, effect sizes were calculated to provide an estimate of the magnitude of change. The Friedman test yielded a Kendall’s W of 0.923, indicating a very strong association across the four time points and underscoring the consistency of the observed trend in periapical healing. Pairwise Wilcoxon signed-rank tests demonstrated large effect sizes for all comparisons (r ≈ 0.88), further confirming the robustness of the improvements over time. These results suggest that the reductions in PAI scores were not only statistically significant but also clinically meaningful, with a consistently strong treatment effect observed between baseline and each follow-up period as well as between successive follow-ups. The combination of high Kendall’s W and large Wilcoxon effect sizes reinforces the interpretation that periapical healing followed a pronounced and durable trajectory of improvement (Table 2).
4. Discussion
The present findings underscore the critical role of predictable apical and coronal sealing in the long-term management of periapical lesions. Across the monitored cases, healing dynamics confirm that when optimal sealing and biologically compatible materials are utilized, periapical bone regeneration can be achieved in a predictable and clinically significant manner. The majority of cases initially scored as PAI5 (58.3%) exhibited substantial radiographic improvement, with half progressing to PAI1 by the fourth year. The relapse observed in one case at the ten-year mark emphasizes the importance of long-term follow-up. Statistical analyses corroborate the clinical observations, providing quantitative evidence of sustained periapical healing. The Friedman test revealed a highly significant overall reduction in PAI scores across time (χ²(3) = 33.21, p < 0.001), with Kendall’s W = 0.92 indicating an exceptionally strong level of concordance among repeated measures. Post-hoc Wilcoxon signed-rank tests confirmed that each pairwise comparison between baseline and follow-up points, as well as between successive follow-ups, was statistically significant after Holm correction. Effect sizes were consistently large (r ≈ 0.88), underlining the robustness and clinical relevance of the improvements. Radiographic evidence of bone regeneration, exemplified in Figure 4, documents the transition from severe periapical pathology to restitutio ad integrum. These findings align with recent literature. Sabeti et al. reported that long-term periapical healing rates remain high provided coronal leakage is prevented, emphasizing that apical and coronal seals are critical determinants of treatment outcome [34]. Similarly, Almufleh L. demonstrated that biomaterials with bioactive and osteoconductive properties contribute to accelerated bone regeneration and more predictable periapical healing, particularly over extended follow-up periods [35]. Although the study included both younger and older adults, the small sample size of 12 cases limits the generalizability of the findings. Individual variability underscores the importance of considering patient-specific factors, including age, lesion size, and initial periapical status. These preliminary results emphasize the importance of larger-scale studies to confirm observed trends and refine treatment protocols. The hybrid HA/HyA biomimetic nano-hybrid material underwent chemical, morphological, and structural examination [33]. High-energy milling increased the binding capability of the nanomaterial, producing nano-hydroxyapatite with a crystallite size of approximately 30 nm, with TEM revealing aggregation of nHA crystallites. A hybrid material consisting of nHA and 1% hyaluronan, which was further milled, was used to treat bone defects with critical dimensions, producing positive clinical outcomes [33]. Calcium hydroxide remains effective for treating external resorption due to its high Ca²⁺ concentration and alkaline pH [36,37]. Seltzer and Bender emphasize the importance of available Ca²⁺ for activating adenosine triphosphatase, inducing remineralization of dental tissues [38]. The complexity of bone is reflected in technical challenges in bone scaffolding. Organic-inorganic hybrid systems aim to provide signals within a conductive apatite layer to encourage cell adhesion, proliferation, and differentiation into bone tissue [39]. Dual-functioning peptides that adhere to the apatite layer and promote cell adhesion via recognition sequences can enhance osteogenesis. Tissue engineering, combining life sciences and engineering, develops biological substitutes to restore, maintain, or improve tissue function [40,41]. These technologies hold significant potential for treating tissue or organ loss and genetic or metabolic disorders [42]. Operative technique selection depends on biological and mechanical parameters, with individualization of each case. Challenges include root canal transportation, cleavage in the apical third, via falsa, steps, and perforations, often complicated by existing radicular pins, old fillings, or broken canal instruments [38,43,44]. Apical transportation affects root canal curvature by 0.01–0.15 mm, increasing the difficulty in sealing and the risk of leakage. Healing prognosis after endodontic treatment is closely related to the degree of resorption, the extent of the apical lesion, and the possibility of biological sealing. Healing in chronic apical periodontitis results from decontamination and three-dimensional obturation with biomimetic materials, particularly in cases lacking physiological apical narrowing [4,45,46,47].
Farhana F. et al. concluded that future dentistry would involve biomimetic materials capable of replacing lost dentine, cementum, and even pulp tissue [48]. Ongoing developments in biomaterials and regenerative techniques may enhance long-term predictability and clinical outcomes in periapical healing. The combination of apical lesions and internal root resorption remains a clinical challenge [45], but tissue engineering and biomimetic materials offer promising avenues for complete biological restoration.
5. Conclusions
The use of a biomimetic technique and material in the clinical protocol for the treatment of teeth with periapical lesions demonstrates that hydroxyapatite/hyaluronan biomimetic nano-hybrid material stimulates bone healing in chronic apical lesions. Statistical analysis confirmed a highly significant reduction in PAI scores over time (Friedman χ²(3) = 33.21, p < 0.001; r ≈ 0.88), supporting the predictability of periapical healing. This clinical case further emphasizes the importance of achieving good apical sealing, which is not possible with standard obturation methods. These findings indicate that biomimetic materials and techniques hold considerable potential for wider application in clinical dental practice.
Author Contributions
Conceptualization, A.G. and E.D.; methodology, E.D.; software, A.G.; validation, A.G. and E.D.; formal analysis, A.G.; investigation, A.G.; resources, A.G.; data curation, A.G.; writing—original draft preparation, A.G.; writing—review and editing, E.D.; visualization, A.G.; supervision, E.D.; project administration, A.G.; funding acquisition, A.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research was financially supported by the Medical University of Sofia and was approved by the Ethics Committee for Scientific Research at the Medical University of Sofia (ECSRMUS) through Grant Project D-39/16.09.2009.
Institutional Review Board Statement
In the university policy regarding grant agreements for projects at the Medical University of Sofia, there is no separate document from the grant agreement. Before the agreement with the university for funding the research project is concluded, the docu- Institutional Review Board (IRB) approval must be obtained. The university does not issue a separate document statement. The agreement itself certifies this. This study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee for Scientific Research at the Medical University of Sofia (ECSRMUS), approval number 39/16.09.2009.
Informed Consent Statement
Written informed consent was obtained from the patients for the treatment and to use the data and results for this investigation and to publish the results in this paper.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.
Acknowledgements
The authors gratefully acknowledge the Institute of General and Inorganic Chemistry, Bulgarian Academy of Sciences, Acad. G. Bontchev Str., Bl. 11, 1113 Sofia, Bulgaria and Institute of Mineralogy and Crystallography, Bulgarian Academy of Sciences, Acad. G. Bontchev Str., Bl. 107, 1113 Sofia, Bulgaria
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CAP | Chronic apical periodontitis |
| nHA | nano-crystalline hydroxyapatite |
| SEM | Scanning Electron Microscopy |
| PAI | Periapical index |
References
- Pihlstrom, B. L.; Michalowicz, B. S.; Johnson, N. W. Periodontal diseases. Lancet 2005, 366(9499), 1809–1820.
- Silva, N.; Abusleme, L.; Bravo, D.; et al. Host response mechanisms in periodontal diseases. J. Appl. Oral Sci. 2015, 23(3), 329–355. [CrossRef]
- Andreasen, J. O.; Andreasen, F. M. Textbook and Color Atlas of Traumatic Injuries to the Teeth, 3rd ed.; Munksgaard & Mosby: St. Louis, 1994; pp 370–372. [CrossRef]
- Leonardo, M.; Silva, A.; Leonardo, R.; et al. Histological evaluation of therapy using a calcium hydroxide dressing for teeth with incompletely formed apices and periapical lesions. J. Endod. 1993, 19, 348–352. . [CrossRef]
- Maroto, M.; Barbería, E.; Planells, P.; Vera, V. Treatment of non-vital immature incisor with mineral trioxide aggregate (MTA). Dent. Traumatol. 2003, 19(3), 165–169. [CrossRef]
- Webber, R. T. Apexogenesis versus apexification. Dent. Clin. North Am. 1984, 28, 669–697. [CrossRef]
- Tibbitt, M.; Anseth, K. Hydrogels as extracellular matrix mimics for 3D cell culture. Biotechnol. Bioeng. 2009, 103(4), 655–663. . [CrossRef]
- Tsiklin, I. L.; Shabunin, A. V.; Kolsanov, A. V.; Volova, L. T. In Vivo Bone Tissue Engineering Strategies: Advances and Prospects. Polymers (Basel) 2022, 14(15), 3222. [CrossRef]
- Bergenholtz, G.; Spangberg, L. Controversies in Endodontics. Crit. Rev. Oral Biol. Med. 2004, 15(2), 99–114. [CrossRef]
- Gusiyska, A. In vivo analysis of some key characteristics of the apical zone in teeth with chronic apical periodontitis. J. IMAB 2014, 20(5), 638–641. [CrossRef]
- Lyu, P.; Song, Y.; Bi, R.; et al. Protective Actions in Apical Periodontitis: The Regenerative Bioactivities Led by Mesenchymal Stem Cells. Biomolecules 2022, 12(12), 1737. [CrossRef]
- Muñoz-Soto, E.; Elmsmari, F.; Mahmoud, O.; González, J. A. Case Report: Apical periodontitis due to calculus-like deposit on the external surface of the root apex. Front. Oral Health 2025, 6, 1615050. [CrossRef]
- Gusiyska, A.; Dyulgerova, E. Calcium Phosphate Bioceramic as Apical Barrier Material in Complicated Endodontic Cases—A Case Report. Int. J. Sci. Res. 2015, 4(2), 2177–2181.
- Benyus, J. M. Biomimicry: Innovation Inspired by Nature; William Morrow: New York, 1997. .
- Vaiani, L.; Boccaccio, A.; Uva, A. E.; et al. Ceramic Materials for Biomedical Applications: An Overview on Properties and Fabrication Processes. J. Funct. Biomater. 2023, 14(3), 146. [CrossRef]
- Gusiyska, A.; Ilieva, R. Nanosize Biphasic Calcium Phosphate used for Treatment of Periapical Lesions. Int. J. Curr. Res. 2015, 7(1), 11564–11567.
- Nicolae, C.-L.; Pîrvulescu, D.-C.; Niculescu, A.-G.; et al. An Overview of Nanotechnology in Dental Medicine. J. Compos. Sci. 2024, 8, 352. [CrossRef]
- Zhai, P.; Peng, X.; Li, B.; et al. The application of hyaluronic acid in bone regeneration. Int. J. Biol. Macromol. 2020, 151, 1224–1239. [CrossRef]
- Ilieva, R.; Dyulgerova, E.;Petrov, O.;Tarassov. M.;Gusiyska, A.; Vasileva, R. Preparation of hydroxyapatite/hyaluronan biomimetic nanohybrid material for reconstruction of critical size bone defects. Bulgar. Chem. Commun. 2018, 50, 97–105.
- Suzuki, K.; Anada, T.; et al. Effect of addition of hyaluronic acids on the osteoconductivity and biodegradability of synthetic octacalcium phosphate. Acta Biomater. 2014, 10, 531–543. [CrossRef]
- Combes, C.; Rey, C. Adsorption of Proteins and Calcium Phosphate Materials Bioactivity. Biomaterials 2002, 23(13), 2817–2823. [CrossRef]
- Sun, Y.; Wang, Y.; Ji, C.; et al. The impact of hydroxyapatite crystal structures and protein interactions on bone's mechanical properties. Sci. Rep. 2024, 14(1), 9786. [CrossRef]
- Hench, L. Bioceramics: From Concept to Clinic. J. Am. Ceram. Soc. 1991, 74(7), 1487.
- Todros, S.; Todesco, M.; Bagno, A. Biomaterials and Their Biomedical Applications: From Replacement to Regeneration. Processes 2021, 9(11), 1949. [CrossRef]
- Fang, C.; Lin, Y.; et al. Biomimetic Synthesis of Nanocrystalline Hydroxyapatite Composites: Therapeutic Potential and Effects on Bone Regeneration. Int. J. Mol. Sci. 2019, 20(23), 6002. [CrossRef]
- Tanaka, K.; Goto, T.; et al. Apatite-coated hyaluronan for bone regeneration. J. Dent. Res. 2011, 90(7), 906–911. [CrossRef]
- Bohner, M. Design of ceramic-based cements and putties for bone graft substitution. Eur. Cell Mater. 2010, 20(1), 1–12. [CrossRef]
- Laurent, T.; Frazer, J. Hyaluronan. FASEB J. 1992, 6(7), 2397–2404.
- Lorenzi, C.; Leggeri, A.; et al. Hyaluronic Acid in Bone Regeneration: Systematic Review and Meta-Analysis. Dent. J. 2024, 12(8), 263. [CrossRef]
- Valachová, K.; Hassan, M. E.; Šoltés, L. Hyaluronan: Sources, Structure, Features and Applications. Molecules 2024, 29(3), 739. [CrossRef]
- Simeonov, M.; Gusiyska, A.; et al. Novel hybrid chitosan/calcium phosphates microgels for remineralization of demineralized enamel – A model study. Eur. Polym. J. 2019, 119, 14–21.
- Ørstavik, D.; Kerekes, K.; Eriksen, H. The periapical index: a scoring system for radiographic assessment of apical periodontitis. Endod. Dent. Traumatol. 1986, 2, 20–34. [CrossRef]
- Ilieva, R.; Dyulgerova, E.; Petrov, O.; et al. Effects of high energy dry milling on biphase calcium phosphates. Adv. Appl. Ceram. 2013, 112(4), 219–226. [CrossRef]
- Sabeti, M.; Chung, Y. J.; Aghamohammadi, N.; et al. Outcome of Contemporary Nonsurgical Endodontic Retreatment: A Systematic Review of Randomized Controlled Trials and Cohort Studies. J. Endod. 2024, 50(4), 414–433. [CrossRef]
- Almufleh, L. S. The outcomes of nonsurgical root canal treatment and retreatment assessed by CBCT: a systematic review and meta-analysis. Saudi Dent. J. 2025, 37, 14. [CrossRef]
- Jiang, J.; Zuo, J.; Chen, S. H.; Holiday, L. S. Calcium hydroxide reduces lipopolysaccharide-stimulated osteoclast formation. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2003, 95(3), 348–354. [CrossRef]
- Thomas, R. P.; Moule, A. J.; Bryant, R. Root canal morphology of maxillary permanent first molar teeth at various ages. Int. J. Endod. 1993, 26(5), 257–267. [CrossRef]
- Bergenholtz, G. Biologische Grundlagen der Endodontie [Fundamental biologic considerations in endodontics]. Dtsch. Zahnarztl. Z. 1990, 45(4), 187–191.
- Segvich, S.; Biswas, S.; Becker, U.; Kohn, D. H. Identification of peptides with targeted adhesion to bone-like mineral via phage display and computational modeling. Cells Tissues Organs 2009, 189(14), 245–251. [CrossRef]
- Opalchenova, G.; Dyulgerova, E.; Petrov, O. Effect of calcium phosphate ceramics on gram-negative bacteria resistant to antibiotics. J. Biomed. Mater. Res. 1996, 32(3), 473–479.
- Kyaw, M. S.; Kamano, Y.; Yahata, Y.; et al. Endodontic Regeneration Therapy: Current Strategies and Tissue Engineering Solutions. Cells 2025, 14, 422. [CrossRef]
- Delpierre, A.; Savard, G.; Renaud, M.; Rochefort, G. Y. Tissue Engineering Strategies Applied in Bone Regeneration and Bone Repair. Bioengineering 2023, 10(6), 644. [CrossRef]
- Kulild, J. C.; Peters, D. D. Incidence and configuration of canal systems in the mesiobuccal root of maxillary first and second molars. J. Endod. 1990, 16(7), 311–317.
- Gorni, F. G.; Gagliani, M. M. The outcome of endodontic retreatment: a 2-year follow-up. J. Endod. 2004, 30(1), 1–4. [CrossRef]
- Gusiyska, A. Periapical resorptive processes in chronic apical periodontitis: an overview and discussion of the literature. J. IMAB 2014, 20(5), 601–605. [CrossRef]
- Kumar, N.; Maher, N.; Amin, F.; et al. Biomimetic Approaches in Clinical Endodontics. Biomimetics (Basel) 2022, 7(4), 229. [CrossRef]
- Gusiyska, A.; Gateva, N.; Kabaktchieva, R.; et al. Retrospective study of the healing processes of endodontically treated teeth characterized by osteolytic defects of the periapical area: four-year follow-up. Biotechnol. Biotechnol. Equip. 2017, 31(1), 187–192. [CrossRef]
- Farhana, F.; et al. Biomimetic materials: A realm in the field of restorative dentistry and endodontics: A review. Int. J. Appl. Dent. Sci. 2020, 6(1), 31–34.
Figure 1.
SEM images of nHA milled for 20 hours: (a) agglomerations and nanocrystals (magnification x 10 000); (b) rough foamy border on surfaces of particles (magnification x 30 000 ).
Figure 1.
SEM images of nHA milled for 20 hours: (a) agglomerations and nanocrystals (magnification x 10 000); (b) rough foamy border on surfaces of particles (magnification x 30 000 ).
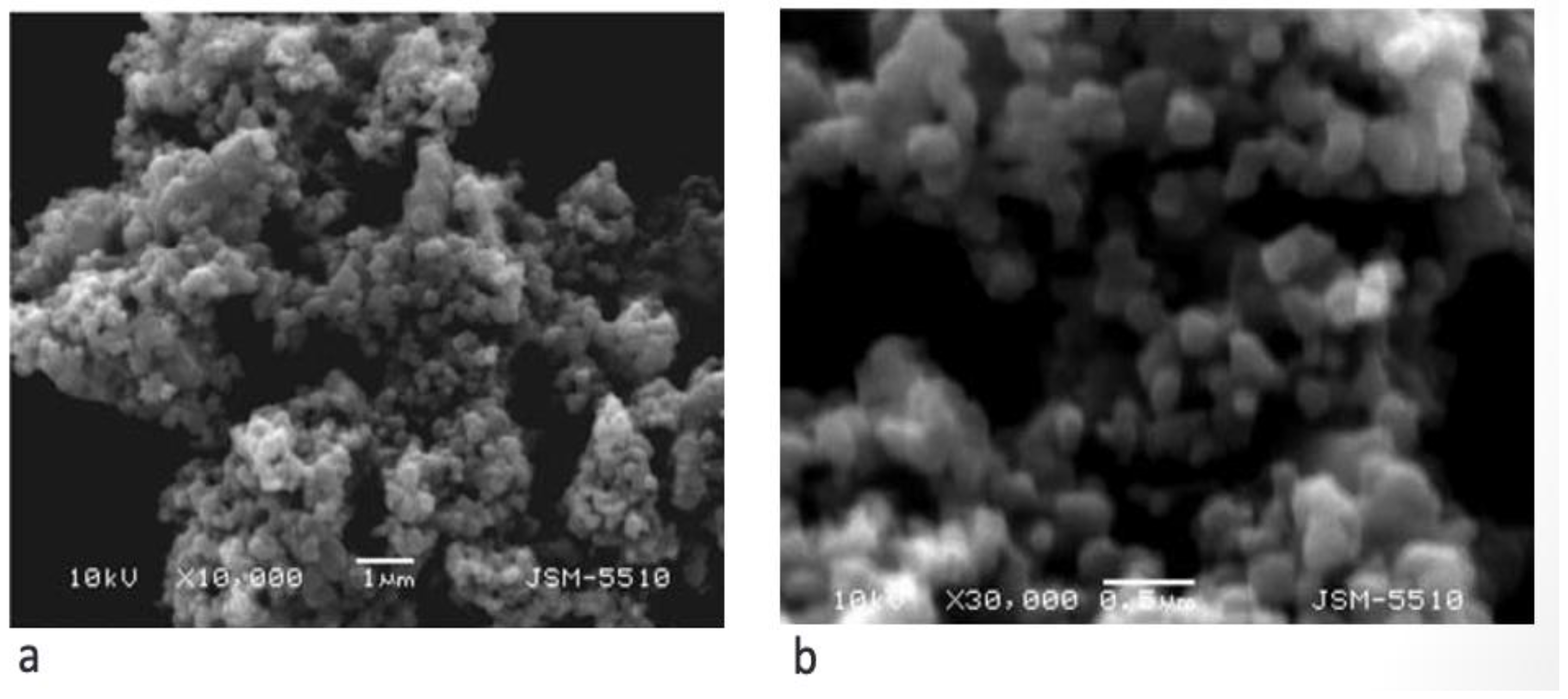
Figure 2.
SEM images of nHA milled for 40 hours: (a) and (b) particles agglomerations (magnification x 10 000 and x 30 000).
Figure 2.
SEM images of nHA milled for 40 hours: (a) and (b) particles agglomerations (magnification x 10 000 and x 30 000).
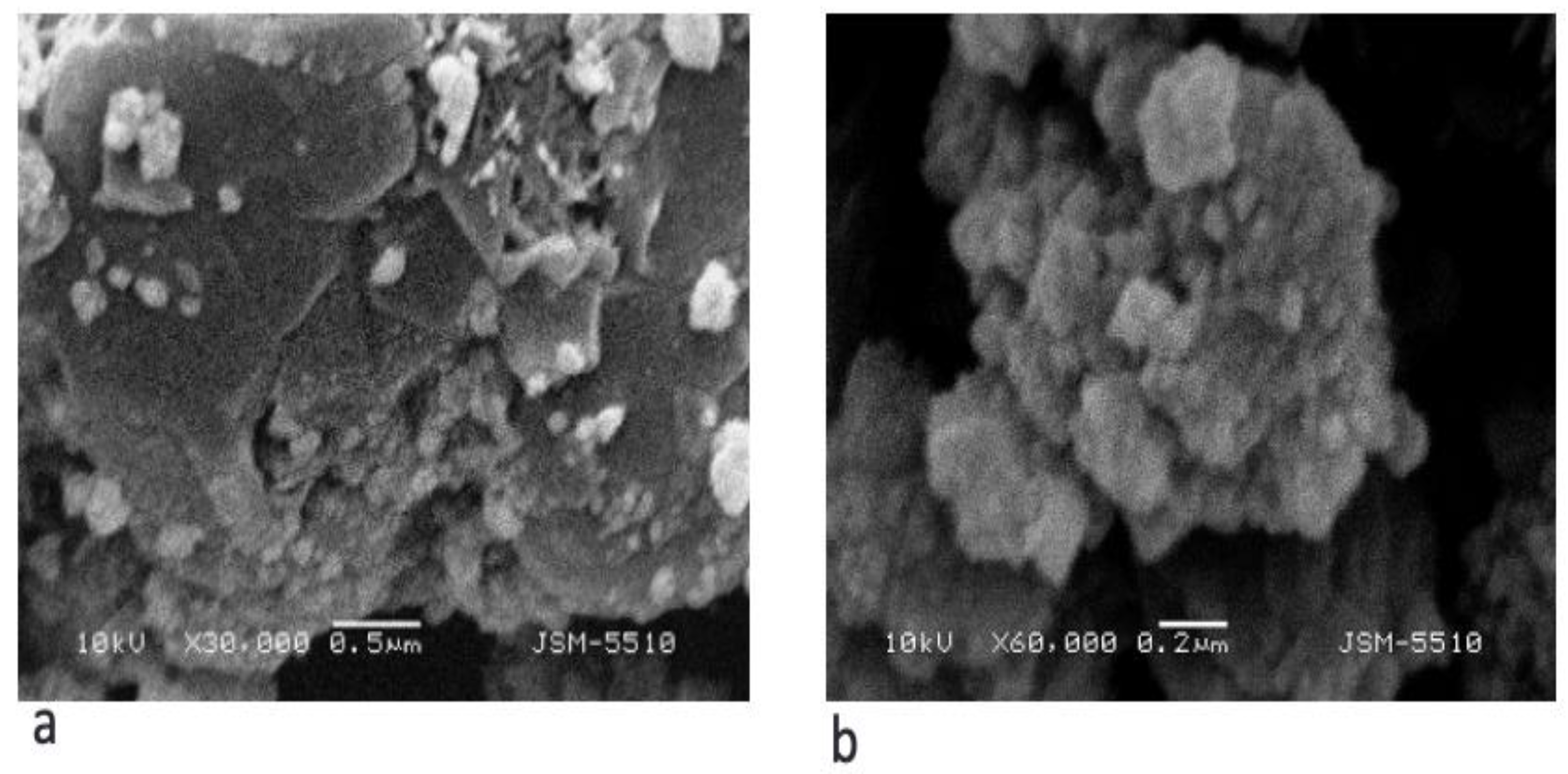
Figure 3.
Figure 3. TEM bright-field image of nHA aggregates (after 40 hours).
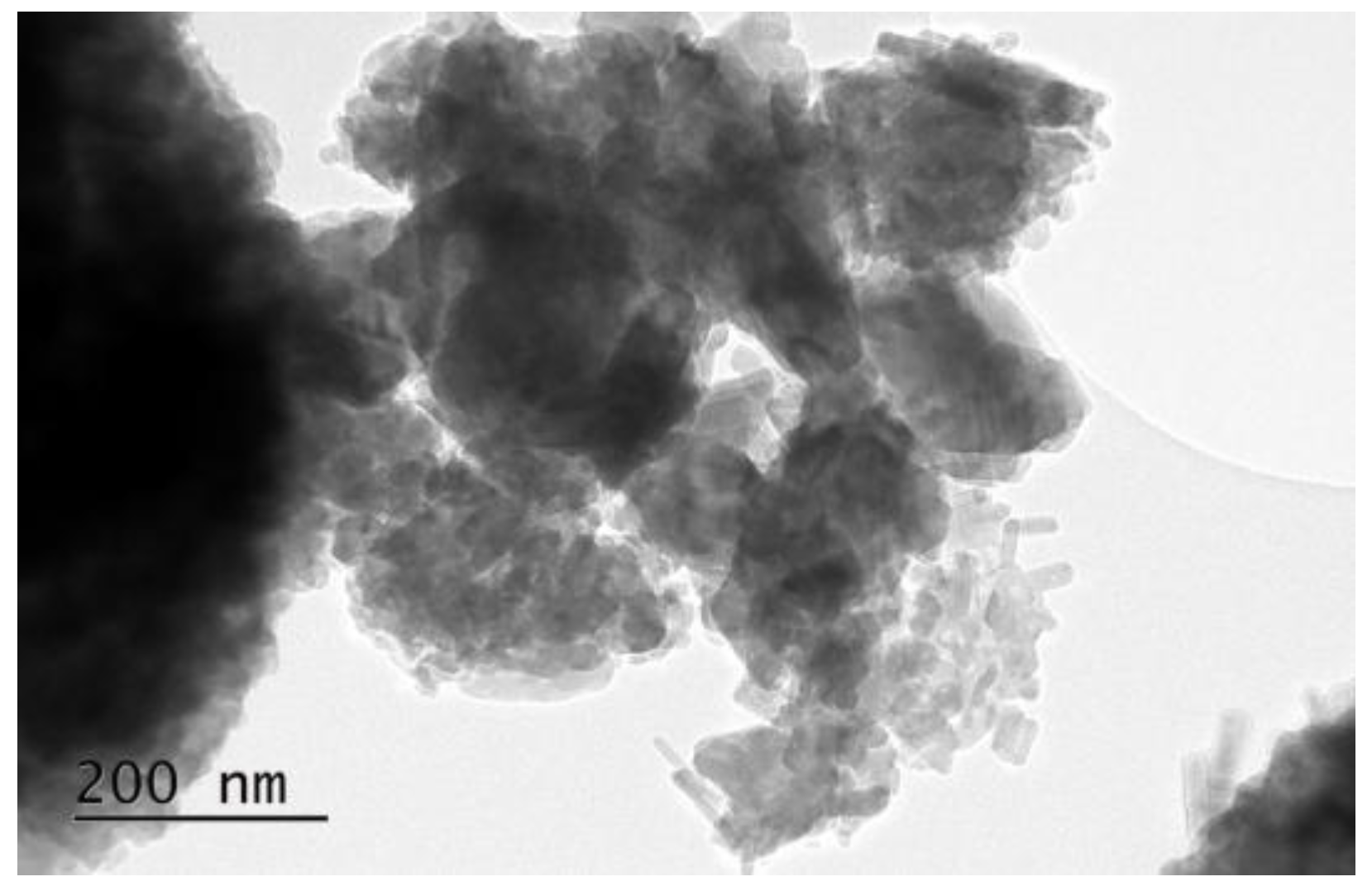
Figure 4.
A-H. Endodontic treatment of tooth #11 was seen on radiographs throughout the procedure: A/ The initial situation; B/ To verify the electrometrical working length measurement, a radiograph with a gutta-percha cone is taken; C/ Post-obturation radiograph; D/ Control radiograph - 3 months after definitive root canal obturation; E/ Control radiograph - 6 months after definitive root canal obturation; F/ Control radiograph - 12 months after definitive root canal obturation; G/ Control radiograph - 4 years after the treatment; H/ Control radiograph - 10 years after endodontic treatment.
Figure 4.
A-H. Endodontic treatment of tooth #11 was seen on radiographs throughout the procedure: A/ The initial situation; B/ To verify the electrometrical working length measurement, a radiograph with a gutta-percha cone is taken; C/ Post-obturation radiograph; D/ Control radiograph - 3 months after definitive root canal obturation; E/ Control radiograph - 6 months after definitive root canal obturation; F/ Control radiograph - 12 months after definitive root canal obturation; G/ Control radiograph - 4 years after the treatment; H/ Control radiograph - 10 years after endodontic treatment.
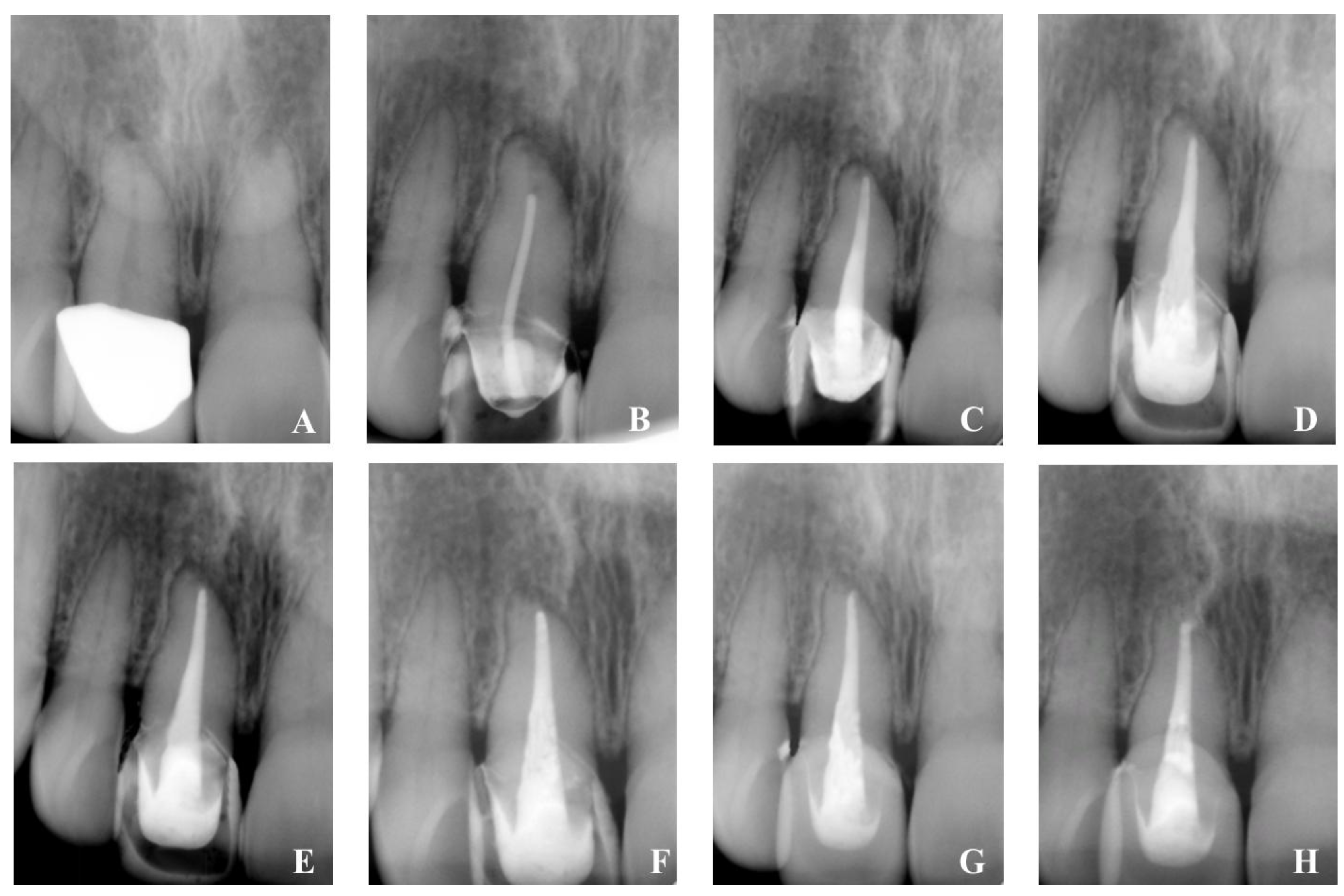
Figure 5.
Mean PAI values over time.
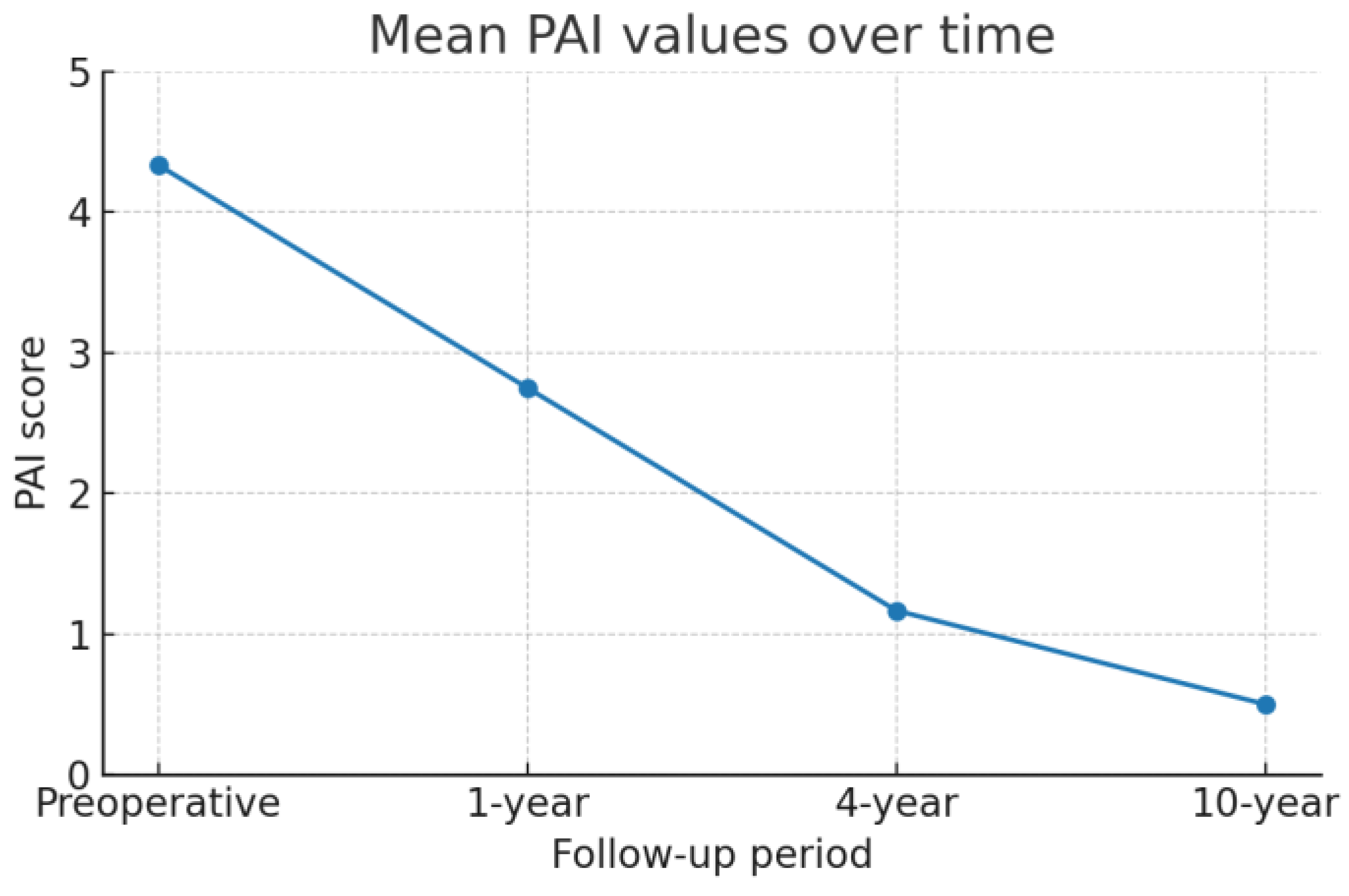

Table 1.
The results from assessment of the healing process of monitored cases (N1 - N12) through PAI score at first, fourth and tenth year, and from the apical foramen measurements in the stage of root canal preparation.
Table 1.
The results from assessment of the healing process of monitored cases (N1 - N12) through PAI score at first, fourth and tenth year, and from the apical foramen measurements in the stage of root canal preparation.
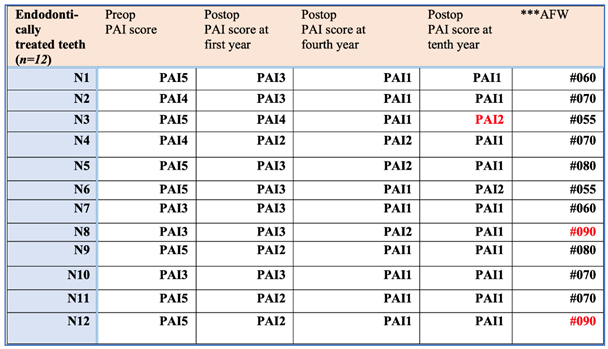
*n - number of clinical cases; **N - number of the clinical case; ***AFW - Apical Foramen Width.
Table 2.
Pairwise comparisons of PAI scores across time points using Wilcoxon signed-rank tests with Holm correction.
Table 2.
Pairwise comparisons of PAI scores across time points using Wilcoxon signed-rank tests with Holm correction.
| Comparison | W-statistic | Raw p-value |
Adjusted p-value (Holm) |
Effect size r |
|---|---|---|---|---|
| Preop. PAI score vs 1st year |
0.0 | 0.0069 | 0.0138 | 0.88 |
| Preop. PAI score vs 4th year |
0.0 | 0.0005 | 0.0029 | 0.88 |
| Preop. PAI score vs 10th year |
0.0 | 0.0005 | 0.0029 | 0.88 |
| 1st year PAI score vs 4th year |
0.0 | 0.0028 | 0.0083 | 0.88 |
| 1st year PAI score vs 10th year |
0.0 | 0.0005 | 0.0029 | 0.88 |
*Results of post-hoc Wilcoxon signed-rank tests with Holm correction for multiple comparisons. All pairwise comparisons demonstrated statistically significant differences at the 0.05 level.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



