
Submitted:
21 October 2025
Posted:
22 October 2025
You are already at the latest version
Abstract
Epigallocatechin gallate (EGCG), the principal constituent of catechins, has garnered considerable attention owing to its diverse health benefits. As a natural antioxidant and anti-inflammatory agent, EGCG has been shown in numerous studies to exert pronounced cardioprotective effects. Cardiovascular health is essential for human survival, yet it remains threatened by injuries associated with metabolic disorders, myocardial infarction, ischemia–reperfusion, and even general anesthesia. The development of a safe and effective cardioprotective agent would be of considerable value in diverse clinical settings. EGCG not only protects the coronary arteries but also attenuates adverse cardiac remodeling, prevents cardiomyocyte death, and enhances cardiac function, effects that have been consistently demonstrated in multiple animal models. Although clinical studies have confirmed the beneficial effects of EGCG on metabolic disorders, endothelial dysfunction, and cardiac hypertrophy, the sample sizes of these investigations remain relatively small. Moreover, numerous potential cardioprotective effects of EGCG under diverse clinical conditions remain to be systematically investigated. Further studies evaluating diverse dosing regimens of EGCG across various clinical contexts are required to establish its safety and efficacy and to facilitate its translation into clinical practice.
Keywords:
epigallocatechin gallate
; metabolic disorders
; coronary artery disease
; adverse cardiac remodeling
; myocardial infarction
; myocardial ischemia-reperfusion injury
; cardiomyocyte injury
; cardiac function
1. Introduction
Cardiac health is fundamental to overall human well-being, yet it is increasingly challenged by a variety of factors. Metabolic disorders, such as obesity, metabolic syndrome (MS), and type 2 diabetes mellitus (T2DM), have emerged as major health threats in the modern world [1]. Abnormalities in multiple metabolic components caused by these diseases impose persistent stress on the cardiovascular system, ultimately leading to coronary artery disease (CAD) and adverse cardiac remodeling [2]. Myocardial infarction (MI), the most severe clinical manifestation of CAD, affects approximately 3.8% of the global population under 60 years of age and up to 9.5% of those over 60 [3]. Another pressing issue associated with the rising incidence of MI is the lack of effective pharmacological interventions to prevent or treat myocardial ischemia–reperfusion injury (MIRI) during reperfusion therapy. In addition, with the widespread adoption of medical technology, the number of anesthesia cases has been rapidly increasing, rising annually by approximately 10% in China between 2015 and 2017 [4]. Consequently, the incidence of myocardial injury after non-cardiac surgery (MINS) is also expected to rise. MINS, defined as an elevation in cardiac troponin (cTn) concentrations within 30 days postoperatively, is a frequent complication associated with increased postoperative mortality. Because most cases are asymptomatic, MINS is often overlooked [5].
Given the multiple threats to cardiac health, developing cardioprotective agents holds considerable clinical significance. Natural compounds, compared with synthetic substances, may be more suitable as therapeutic agents and play a pivotal role in drug development [6]. Tea has demonstrated a wide range of health benefits [7], for its rich content of polyphenolic compounds. Catechins are the main polyphenolic compounds in green tea (GT) and the unique polyphenolic compounds in other types of tea are mostly derived from their oxidation and fermentation processes [8]. EGCG, which represents 50–80% of the total catechins in GT, exhibits the strongest antioxidant capacity owing to its abundant hydroxyl groups [9]. As a natural anti-inflammatory and antioxidant substance, EGCG improves glucose and lipid metabolism [10], exerts preventive and therapeutic effects in CAD [11] and diabetic cardiomyopathy (DCM) [2]. Furthermore, EGCG demonstrates substantial potential in MI, MIRI [12], restrictive cardiomyopathy (RCM) [13], and heart failure (HF) [14], underscoring its broad cardioprotective effects. To bridge the gap between preclinical research and clinical application, we conducted this review. We summarize the cardioprotective effects of EGCG from four perspectives: coronary artery protection, inhibition of adverse cardiac remodeling, prevention of cardiomyocyte injury, and preservation of cardiac function. We also discuss its potential adverse reactions and future research directions, emphasized the significant impact of rational dosing regimens on outcomes, and provided specific experimental suggestions aiming to provide a foundation for the clinical translation of EGCG as a cardioprotective agent.
2. Cardioprotective Effects
2.1. Coronary Artery Protection
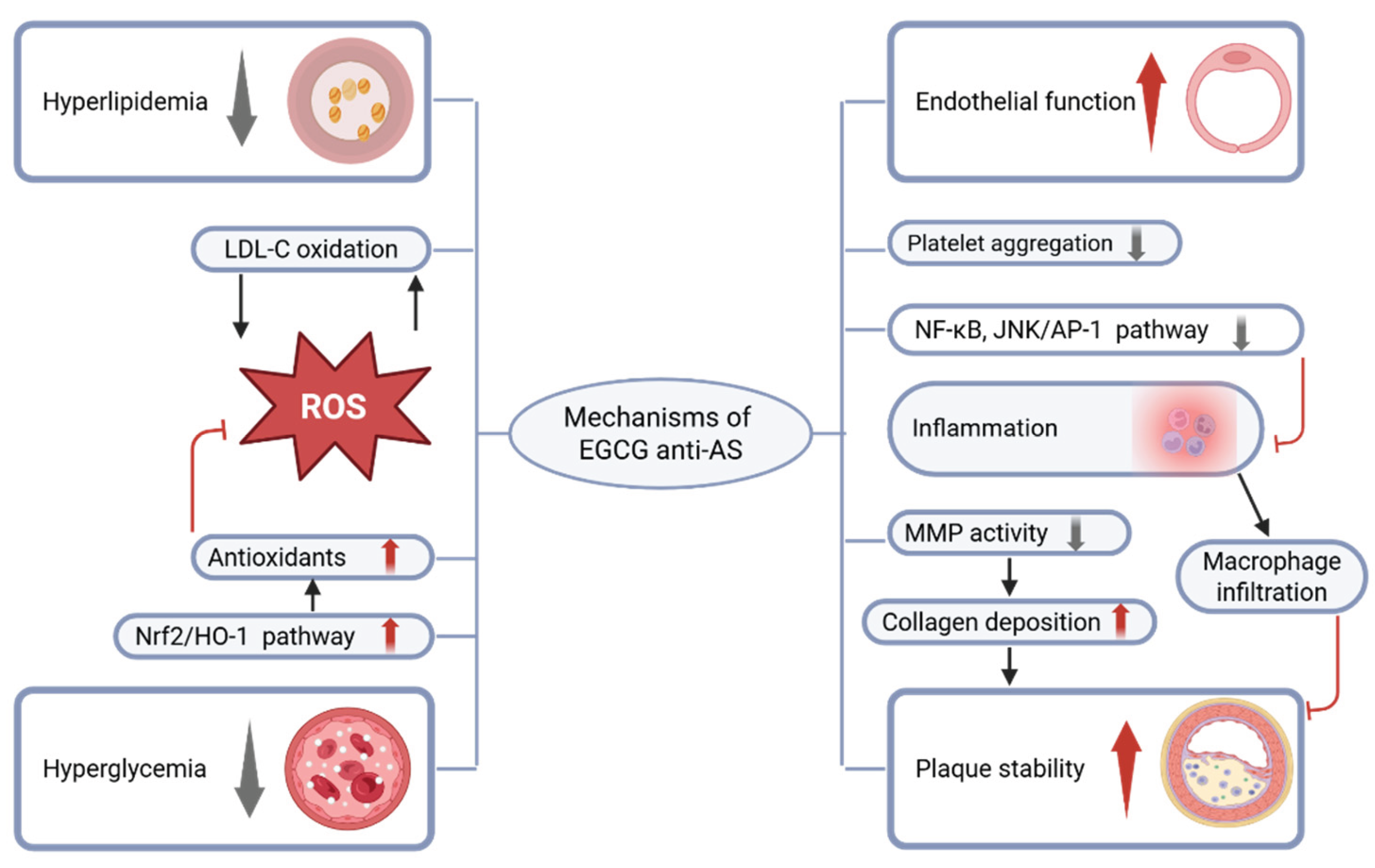
Atherosclerosis (AS) is a chronic inflammatory vascular disorder primarily induced by hyperlipidemia, hyperglycemia, smoking, and other risk factors. The primary pathological mechanism involves endothelial dysfunction and vascular wall injury induced by harmful stimuli, which promote lipid deposition and plaque formation, ultimately leading to CAD [15]. Chronic inflammation is critically involved in the initiation and progression of numerous diseases [16]. MS is also recognized as an inflammatory disorder [17]. EGCG, with potent antioxidant and anti-inflammatory activities, may play an essential role in protecting against MS [10]. The Nrf2/HO-1 signaling pathway, a major regulator of intracellular defense against oxidative stress, is regarded as an ideal target for alleviating endothelial cell injury [18]. EGCG not only attenuates oxidative stress via activation of the Nrf2/HO-1 pathway but also suppresses inflammatory responses in AS [19], thereby conferring endothelial protection. EGCG also exhibits anti-platelet aggregation effects, which are beneficial for preventing thrombosis. Matrix metalloproteinases (MMPs), key enzymes involved in extracellular matrix remodeling, are critical determinants of plaque stability. Numerous studies have indicated that polyphenols enhance plaque stability by suppressing MMP gene expression and enzymatic activity [20,21]. The main anti-AS mechanisms of EGCG are illustrated in Figure 1.
Figure 1.
EGCG improves metabolic disorders and reduces the damaging effects of hyperlipidemia and hyperglycemia on blood vessels. At the same time, as a natural antioxidant, EGCG activates the Nrf2/HO-1 pathway, increases the levels of both enzymatic and non-enzymatic antioxidants in the body, inhibits the oxidation of low-density lipoprotein cholesterol (LDL-C) and the mutual promotion between ROS, reduces oxidative stress, and improves endothelial dysfunction. At the same time, it reduces inflammatory responses and inhibits macrophage infiltration in plaques by suppressing signaling pathways such as NF-kB and JNK/AP-1. In addition, EGCG inhibits the activity of matrix metalloproteinases (MMPs), increases collagen fiber content in plaques, inhibits platelet aggregation, thereby enhancing plaque stability.
Figure 1.
EGCG improves metabolic disorders and reduces the damaging effects of hyperlipidemia and hyperglycemia on blood vessels. At the same time, as a natural antioxidant, EGCG activates the Nrf2/HO-1 pathway, increases the levels of both enzymatic and non-enzymatic antioxidants in the body, inhibits the oxidation of low-density lipoprotein cholesterol (LDL-C) and the mutual promotion between ROS, reduces oxidative stress, and improves endothelial dysfunction. At the same time, it reduces inflammatory responses and inhibits macrophage infiltration in plaques by suppressing signaling pathways such as NF-kB and JNK/AP-1. In addition, EGCG inhibits the activity of matrix metalloproteinases (MMPs), increases collagen fiber content in plaques, inhibits platelet aggregation, thereby enhancing plaque stability.
2.1.1. Improve Metabolic Disorders
Clinical studies have demonstrated that long-term oral administration of EGCG exerts therapeutic effects on lipid abnormality (LA) associated with obesity [22,23,24] and smoking [25]. A clinical trial demonstrated that oral EGCG also has the effect of lowering blood pressure in obese patients [26]. Although another clinical trial reported no lipid-lowering effect of oral EGCG at 400 mg twice daily in obese patients [27] while noting a reduction in blood pressure, a systematic review demonstrated that daily oral intake of 107–856 mg of EGCG for 4–14 weeks significantly reduced serum low-density lipoprotein cholesterol (LDL-C) levels [28]. In patients with T2DM, a meta-analysis revealed that supplementation with green tea extract (GTE) for more than 8 weeks at doses exceeding 800 mg/day significantly reduced serum triglyceride (TG) concentrations [29]. Two clinical trials in T2DM patients with LA or obesity reported that daily oral administration of 1500 mg GTE (≈865 mg EGCG) for 16 weeks did not significantly improve insulin resistance or LA compared with placebo. However, both studies observed modest improvements in insulin resistance after 16 weeks of GTE treatment compared with baseline [30,31]. This outcome may be attributed to the bidirectional exacerbation between T2DM and LA, which resulted in more severe conditions in the study population [32], rendering the EGCG dosage and treatment duration insufficient. Extending EGCG administration to two months resulted in observable improvements in LA among T2DM patients [33]. In contrast, administration of EGCG in gestational diabetes mellitus (GDM), a condition less severe than T2DM, improved maternal glycemic indicators and reduced neonatal complications [34]. Although the anti-diabetic effects of EGCG have been validated in numerous preclinical studies [35,36,37], they remain inconclusive in humans. Across observational studies, the association between tea consumption and T2DM incidence has been inconsistent. Overall, drinking tea appears to confer some protection against T2DM, but the evidence remains inconclusive and may be confounded by lifestyle and dietary factors [38]. Habitual tea consumption provides only modest doses of EGCG, which are insufficient to override the influence of broader lifestyle and dietary factors. Although current clinical trials have not demonstrated significant anti-diabetic efficacy of EGCG, they have reported improvements in LA among T2DM patients, reductions in blood pressure [33], and amelioration of arterial stiffness [39], all of which are beneficial for CAD. The clinical trial findings regarding the coronary protective effects of EGCG and its inhibition of adverse cardiac remodeling are summarized in Table 1.

Table 1.
A summary of clinical trials on the cardioprotective effects of EGCG.
| Study population | Dose | Effect | References |
|---|---|---|---|
| 88 obese male patients aged 40-65 years |
400 mg of EGCG (po, bid) for 8 weeks |
DBP ↓ NS between groups: HOMA-IR index, OGTT TG, TC, HDL-C, LDL-C |
[27] |
| 56 obese patients with hypertension |
379 mg of GTE (po, qd) for 3 months |
SBP, DBP ↓ HOMA-IR index, FBG ↓ TNF-α, CRP ↓ T-AOC ↑ TC, TG, LDL-C ↓ HDL-C ↑ |
[22] |
| 102 women with central obesity |
856.8mg of EGCG (po, qd) for 12 weeks |
TC, LDL-C ↓ | [23] |
| 30 obese patients | 150mg of EGCG (po, bid) for 8 weeks |
Serum kisspeptin, TG ↓ | [24] |
| 30 obese patients | 150mg of EGCG (po, bid) for 8 weeks |
SBP, DBP, MAP ↓ | [26] |
| 68 T2DM patients with obesity |
1,500 mg of GTE (po, qd) for 16 weeks (Supplement to routine medication) |
NS between groups: HOMA-IR index, FBG, HbA1c Within GTE group: Compared to baseline HbA1c ↓ |
[30] |
| 77 T2DM patients with LA |
500 mg of GTE (po, tid) for 16 weeks (Supplement to routine medication) |
NS between groups: HOMA-IR index, FBG, HbA1c TG, TC, HDL-C, LDL-C Within GTE group: Compared to baseline GLP-1 ↑ HOMA-IR ↓ |
[31] |
| 326 pregnant women diagnosed with GDM during third trimester |
500 mg of EGCG (po, qd) until full term |
Maternal diabetic parameters ↑ Cases of neonatal complications ↓ |
[34] |
| 20 T2DM patients | 400 mg of GTE (po, qd) for 12 weeks |
Improved arterial stiffness | [39] |
| 50 T2DM patients | 300 mg of EGCG (po, bid) for 2 months (Supplement to routine medication) |
MAP, DBP ↓ TC, TG, AIP ↓ T-AOC ↑ |
[33] |
| 120 South Indian male smokers |
100 ml of GT (po, tid) for 1 year |
Improved LA | [25] |
| 52 patients with early AS |
30 ml olive oil with 280 mg of EGCG (po, qd) for 4 months (Supplement to routine medication) |
Endothelial function ↑ | [40] |
| 42 CAD patients | 150 mg of EGCG (po, bid) for 2 weeks (Supplement to routine medication) |
Endothelial function ↑ | [41] |
| 19 patients with ATTR-CM |
GT and/or GTE (Exposure factors) for 1 year (Supplement to routine medication) |
Left ventricular mass ↓ TC, LDL-C ↓ |
[42] |
| 25 male patients with wtATTR-CM |
600 mg of EGCG (po, qd) for 1 year (Supplement to routine medication) |
Left ventricular mass ↓ Extracellular volume fraction ↓ TC ↓ |
[13,43] |
2.1.2. Alleviate Endothelial Dysfunction
The vascular endothelium is pivotal in regulating vascular homeostasis, and preserving its vasodilatory, anti-inflammatory, antithrombotic, and antiproliferative functions is essential for mitigating cardiovascular risk. Notably, the endothelial protective effects of EGCG have been confirmed in clinical trials involving patients with early AS or CAD [40,41]. All preclinical studies investigating the coronary protective effects and the inhibition of adverse cardiac remodeling by EGCG are summarized in Table 2. In vivo animal studies demonstrated that EGCG activated the Nrf2/HO-1 pathway to attenuate oxidative stress, inhibited lipid peroxide formation, suppressed NF-κB signaling, and limited the release of inflammatory mediators, thereby conferring endothelial protection in high-fat diet–fed mice [44,45,46]. Furthermore, human primary T cells cultured in vitro and pretreated with EGCG exhibited marked reductions in AP-1 activity and inflammatory cytokine secretion upon stimulation [47]. Collectively, the potent antioxidant and anti-inflammatory properties of EGCG safeguard endothelial integrity, a mechanism critical for attenuating the progression of CAD.
Table 2.
A summary of preclinical studies on the protective effects of EGCG on atherosclerosis and adverse cardiac remodeling with different dosing regimens in various injury models.
Table 2.
A summary of preclinical studies on the protective effects of EGCG on atherosclerosis and adverse cardiac remodeling with different dosing regimens in various injury models.
| Injury Models | Dosage regimen | Results | References |
|---|---|---|---|
| Atherogenic diet for 45 days in male Wistar rats |
EGCG 100 mg/kg (ip, qd) for the last 14 days |
CRP, ESR ↓ | [44] |
| High-fat diet for 15 weeks P. gingivalis (iv, tiw) for 3 weeks in ApoE-deficient mice |
Drinking water with EGCG (0.2 g/L) for 7 weeks |
AS areas ↓ CRP, IL-8, MCP-1 ↓ HO-1 ↑ oxidized LDL-C ↓ |
[45] |
| High-fat diet for 30 days in Wistar rats |
EGCG 100 mg/kg (ip, qd) for 6/12 days |
TC, TG, LDL-C ↓ HDL-C ↑ Antioxidants ↑ Lipid peroxidation ↓ |
[46] |
| High-fat diet for 16 weeks in ApoE-deficient mice |
EGCG 10 mg/kg (ip, qd) for 16 weeks |
TNF-α, IL-6, MCP-1, INF-γ ↓ EMMPRIN, MMP-2, MMP-9 ↓ Plaque stability ↑ |
[48] |
| High-fat diet for 6 weeks in ApoE-deficient mice |
EGCG 10, 20, 40 mg/kg (po, qd) for 6 weeks |
TC, TG, LDL-C, ↓ HDL-C ↑ VEGFA, MMP-2 ↓ SOD, Nrf2/HO-1 pathway ↑ ROS ↓ |
[49] |
| T2DM in db/db mice |
Diet with EGCG (10 g/ kg) for 10 weeks |
FBG ↓ Plasma insulin ↑ Number of pancreatic islets ↑ |
[35] |
| NAM 100 mg/kg (ip) 20 min later STZ 55 mg/kg (ip) in male Wistar rats |
After induction of DM EGCG 2 mg/kg (po, qod) for 1 month |
HOMA-IR index, FBG, HbA1c ↓ TG, TC, LDL-C, VLDL-C ↓ HDL-C ↑ SOD, CAT, GSH ↑ ROS ↓ IL- 1β, IL-6, TNF-α, ICAM-1, VCAM-1 ↓ cTnT, CK-MB, LDH, AST ↓ Histopathological injury ↓ Apoptosis ↓ Fibrosis area ↓ |
[36] |
| STZ 65 mg/kg (ip) in male SD rats |
After induction of DM EGCG 10, 20, 40 mg/kg (po, qd) for 12 weeks |
FBG ↓ TG, TC, LDL-C ↓ HDL-C ↑ Fibrosis area, COL-I, COL-III ↓ |
[37] |
| Senium (24-26 months of age) in albino Wistar rats |
EGCG 200 mg/kg for 30 days |
Nrf2 ↑ ROS ↓ NF-κB ↓ TGFβ, TNFα ↓ Apoptosis ↓ COL ↓ |
[50] |
| AAC for 4 weeks in male SD rats |
EGCG 25, 50 mg/kg (po, qd) for 4 weeks |
NF-κB activation, CTGF ↓ Fibrosis area ↓ |
[51] |
| TAC for 4 weeks in male C57BL/6 mice |
EGCG 20, 40, 80 mg/kg (po, qd) for 4 weeks |
HW/BW, HW/TL, COL ↓ AKT/mTOR pathway ↓ |
[52] |
| COL (10 µg/mL) for 5 min with washed platelets from male SD rats |
Preincubated with 1, 5, 10, 30, 50 μM EGCG for 3 min |
Platelet aggregation ↓ | [53] |
| 100 nM Ang II for 24 h with CFs of adult rats |
Preincubated with 1, 10 μM EGCG for 1 h |
CFs proliferation ↓ NF-κB, CTGF ↓ COL-I, COL-III ↓ |
[51] |
| 10nM Ang II for 4h with CFs of adult rats |
At the same time EGCG 1, 10,100 μM for 4h |
JNK/AP-1 ↓ Endoglin ↓ CFs proliferation ↓ |
[54] |
| ADP 6.5 μM or COL 3.2μg/ml for 6 min with blood samples from people taking antiplatelet drugs |
EGCG 50, 100, 200 μM preincubated for 30 min |
Platelet aggregation ↓ | [55] |
| Human primary T cells incubated with P/I for 20 h |
EGCG 10, 20 μM preincubated for 4 h |
AP-1 binding activity ↓ IL-2, IL-4, INF-γ, TNF-α ↓ |
[47] |
| TGF-β2 10 ng/mL IL-1β 1 ng/mL for 24 h with HUVECs |
After injury EGCG 1, 5, 10 μM for 24h |
ROS ↓ NF-κB, SMAD pathways↓ RhoA ↓ Cell migration ↓ EndMT ↓ |
[56] |
| 10 mM β-GP and 3 mM CaCl2 with HASMCs |
EGCG 20, 30 μM | JunB ↓ Osteogenic differentiation ↓ Mineral deposition ↓ |
[57] |
2.1.3. Prevent Coronary Thrombosis
In vitro studies have demonstrated that EGCG suppresses platelet aggregation [53,55], thereby contributing to thrombosis prevention. Furthermore, as nearly 76% of fatal coronary thrombi are triggered by plaque rupture, maintaining plaque stability is of critical importance for patients with AS. In AS mouse models, EGCG exhibited anti-inflammatory, antioxidant, and lipid-lowering effects, and further suppressed MMP-2 and MMP-9 activity in plaque tissues, reduced macrophage infiltration, increased smooth muscle cell and collagen content, thickened the fibrous cap, and ultimately enhanced plaque stability [48,49].
2.2. Inhibition of Adverse Cardiac Remodeling
The reconstruction of the cardiac extracellular matrix requires a finely regulated balance. Moderate fibrotic repair preserves cardiac structural stability, whereas excessive collagen deposition impairs cardiac function. Adverse cardiac remodeling occurs in multiple pathologies, including post–MI [58], DCM, HF, RCM, hypertrophic cardiomyopathy (HCM). Consequently, inhibiting adverse cardiac remodeling represents a critical therapeutic strategy and objective.
2.2.1. Inhibit Collagen Deposition
In vitro studies have demonstrated that EGCG suppresses the proliferation of cardiac fibroblasts (CFs) and collagen (COL) deposition, potentially by downregulating the NF-κB pathway to decrease connective tissue growth factor (CTGF) expression [51], or by inhibiting the JNK/AP-1 pathway to attenuate endoglin expression [54]. Beyond its actions on CFs, EGCG also inhibits endothelial-to-mesenchymal transition (EndMT) and calcium deposition in vascular smooth muscle cells by suppressing NF-κB signaling and inactivating JunB [56,57]. In diabetic mouse models, EGCG improved glucose and lipid metabolism, reduced cardiomyocyte apoptosis, and decreased the extent of cardiac fibrosis [36,37]. Similarly, in vivo experiments in aging [50] and HF mouse models [51,52], also demonstrated reduced COL deposition following EGCG treatment.
2.2.2. Inhibit Amyloid Deposition
Transthyretin is the most common precursor protein of hereditary amyloidosis, and its cardiac deposition leads to RCM. In contrast to the hereditary form, no characteristic mutations in the transthyretin gene are detected in patients with wild-type transthyretin amyloid cardiomyopathy (wtATTR-CM), a condition predominantly affecting elderly individuals, and the underlying pathogenic mechanisms remain to be elucidated. In clinical trials, long-term oral administration of EGCG reduced left ventricular mass in patients with wtATTR-CM [13,42]. Imaging analyses further revealed that the reduction in left ventricular mass originated not from CMs but from the extracellular matrix [43]. These findings suggest that EGCG may exert therapeutic benefits in wtATTR-CM by modulating extracellular matrix remodeling rather than directly affecting CMs.
2.3. Prevention of Cardiomyocyte Injury
MI and MIRI expose CMs to severe oxidative stress and inflammatory responses [59], which consequently result in cardiomyocyte injury, mitochondrial damage, pro-apoptotic factor release, and apoptosis [60]. EGCG exerts potent antioxidant, anti-inflammatory, and anti-apoptotic effects [61], showing great potential for application in MI and MIRI. Beyond apoptosis, other forms of regulated cell death (RCD) also have increasingly attracted attention in the context of MI and MIRI [62,63]. Autophagy constitutes a crucial metabolic pathway that supports cell survival under conditions of nutrient deprivation, hypoxia, or oxidative stress. Excessive autophagy, however, aggravates cellular dysfunction and induces RCD [64]. Preclinical studies have demonstrated that MI and MIRI suppress PI3K/Akt signaling pathway [65] and induce excessive autophagy in CMs, thereby increasing RCD, whereas EGCG administration markedly reversed these pathological responses. A meta-analysis confirmed the cardioprotective effects of EGCG against MI and MIRI in small-animal models [12]. However, there are currently no clinical studies to validate the efficacy of EGCG in MI and MIRI, and all preclinical studies on its protective effects against cardiomyocyte injury in different diseases are summarized in Table 3.
Table 3.
A summary of preclinical studies on the protective effects of EGCG on cardiomyocyte injury with different dosing regimens in various injury models.
Table 3.
A summary of preclinical studies on the protective effects of EGCG on cardiomyocyte injury with different dosing regimens in various injury models.
| Injury Models | Dosage regimen | Results | References |
|---|---|---|---|
| CPB Bypass-time for 90 min Reperfusion for 2 h in domestic piglets (10–15 kg) |
Before CPB EGCG 10 mg/kg (iv) After CPB EGCG 10 mg/kg (iv) |
CK ↓ Nitrosative and oxidative stress ↓ Inflammation ↓ Apoptosis ↓ |
[66] |
| ISO 100 mg/kg (sc, qd) for 2 days in male Wistar rats |
After induction of MI EGCG 10, 20, 30 mg/kg (po, qd) for 21 days |
LDL-C, VLDL-C ↓ HDL-C ↑ AIP ↓ GSH, VC, VE, CER ↑ SOD, CAT ↑ MDA ↓ Mitochondrial damage ↓ Lysosomal enzymes ↓ CK, CK-MB, LDH, AST, ALT ↓ Histopathological injury ↓ |
[67,68,69,70,71,72] |
| ISO 100 mg/kg (sc, qd) for 2 days in male Wistar rats |
Before induction of MI EGCG 15 mg/kg (ip, qd) for 7days |
HW, HW/BW ↓ TC, TG, LDL-C ↓ HDL-C ↑ SOD, CAT ↑ MDA ↓ TNF-α ↓ CK-MB, LDH, ALT, ALP, cTnT ↓ DNA damage, Apoptosis ↓ |
[101] |
| LADO for 30 min Reperfusion for 2 h in male SD rats |
5 min before reperfusion EGCG 10 mg/kg (iv) |
PI3K/AKT pathway ↑ p38, JNK ↓ Infarct size ↓ |
[73] |
| LADO for 30 min Reperfusion for 2 h in male Wistar rats |
5 min before reperfusion EGCG 10 mg/kg (iv) |
PI3K/AKT pathway ↑ Plasma mtDNA, TNF--α, IL--6, IL--8 ↓ Incidence of ventricular arrhythmia ↓ Infarct size ↓ |
[74] |
| LADO for 30 min Reperfusion for 12 h in SD rats |
30 min before ischemia EGCG 10 mg/kg (iv) |
PI3K/AKT pathway ↑ miR-384 ↑ Beclin-1, Excessive autophagy ↓ cTnI ↓ Infarct size ↓ |
[75] |
| LADO for 45 min Reperfusion for 3 h in male C57BL/6 mice |
Before injury EGCG 250 mg/kg (po, qd) for 10 days |
LncRNA Gm4419 ↓ ERK1/2 ↓ Excessive autophagy ↓ Apoptosis ↓ Histopathological injury ↓ Infarct size ↓ |
[76] |
| H2O2 or HRI with MEFs or CMs of neonatal mice |
Before injury EGCG 20, 30, 40 μM for 1-3 h |
Self-cleavage of OMA1 ↓ Proteolysis of OPA1 ↓ Mitochondrial function ↑ Mitochondrial morphology ↑ Apoptosis ↓ |
[77] |
| miR30a knockdown cells Hypoxia for 24 h |
Exosomes from EGCG-Treated CMs |
miR30a ↑ Cell viability ↑ |
[78] |
| H2O2 100 μM for 24 h with CMs of neonatal mice |
EGCG (The dose is unknown) |
LncRNA Gm4419 ↓ ERK1/2 ↓ Excessive autophagy ↓ Apoptosis ↓ Cell viability ↑ LDH ↓ |
[76] |
| HL-1 cells Hypoxia for 18 h |
Before hypoxia EGCG 5, 25 μM for 8h |
GSH, GPX4 ↑ ROS ↓ miR-450b-5p ↑ ACSL4, Ferroptosis ↓ Cell viability ↓ |
[79] |
| H9c2 cells in 30 mM glucose Hypoxia for 2 h Reoxygenation for 4 h |
Before injury EGCG 20 μM for 24 h |
SIRT1 ↑ Mn-SOD ↑ MDA ↓ Apoptosis ↓ Cell viability ↑ LDH ↓ |
[80] |
| H9c2 cells Hypoxia for 6 h Reoxygenation for 12h |
Before injury EGCG 6.25, 25 μM for 4 h |
miR30a ↑ p53 ↓ Apoptosis ↓ CK-MB, LDH ↓ Cell viability ↑ ATP ↑ |
[78] |
| H9c2 cells Hypoxia for 6 h Reoxygenation for 12h |
Before injury EGCG 25 μM for 4 h |
PI3K/AKT pathway ↑ miR-384 ↑ Beclin-1, Excessive autophagy ↓ cTnI ↓ Cell viability ↑ |
[75] |
| H9c2 cells Hypoxia for 6 h Reoxygenation for 12h |
Before injury EGCG 8 mg/L for 24 h |
ROS ↓ ATG4C ↑ Excessive autophagy ↓ ATP ↑ Apoptosis ↓ Cell viability ↑ |
[81] |
| HL-1 cells Hypoxia for 2, 4, 8, 12 h Reoxygenation for 24h |
Before injury 5, 10, 20, 40, 80, 100 μM of EGCG for 3h |
LncRNA MEG3 ↓ TAF15 in cytoplasm ↓ AIM2 mRNA stability ↓ Pyroptosis ↓ Cell death rate ↓ Cell viability ↑ |
[82] |
| H9c2 cells Hypoxia for 3 h Reoxygenation for 2 h |
Before injury EGCG 10 μM for 48 h |
ROS, MDA ↓ 14–3-3η↑ Excessive autophagy ↓ Ferroptosis, Apoptosis ↓ Cell viability ↑ LDH ↓ |
[83] |
2.3.1. Alleviate Oxidative Stress and Inflammatory Responses
Although the global ischemic injury induced by hypothermic cardiac arrest during cardiopulmonary bypass (CPB) is less severe than that observed in MI or MIRI and typically does not result in irreversible cardiac dysfunction, CMs are nevertheless exposed to oxidative stress and inflammatory damage, leading to apoptosis and elevated plasma myocardial enzyme levels, a condition partially resembling MINS. In a large-animal model simulating CPB injury, supplementation of the cardioplegic solution with EGCG alleviated cardiomyocyte injury [66]. Subcutaneous injection of isoproterenol (ISO) to induce MI in mice resulted in LA, heightened oxidative stress and inflammation, and subsequent cardiomyocyte injury. EGCG administration, whether before or after MI induction, significantly improved LA, lowered the atherogenic index of plasma (AIP), and elevated antioxidant defenses—including enzymatic antioxidants such as superoxide dismutase (SOD) and catalase (CAT), as well as non-enzymatic antioxidants such as vitamin C, vitamin E, and ceruloplasmin—in mice. These effects collectively reduced reactive oxygen species (ROS) and malondialdehyde (MDA) levels, decreased tumor necrosis factor-α (TNF-α) expression, and ultimately alleviated cardiomyocyte injury [67,68,69,70,71,72,84].
2.3.2. Alleviate Mitochondrial Dysfunction
Preserving mitochondrial structure and function not only ensures energy supply for cellular activities but also constitutes a fundamental mechanism for preventing the initiation of mitochondrial apoptosis and sustaining cell survival. Beyond the classical roles of Bcl-2 family proteins and the pro-apoptotic factor cytochrome c, EGCG mitigates mitochondrial injury and its downstream consequences through additional molecular pathways. In MI rat models, the activity of tricarboxylic acid cycle enzymes and mitochondrial respiratory chain marker enzymes in CMs was markedly reduced, whereas EGCG pretreatment significantly attenuated these alterations and preserved mitochondrial function [69]. Intravenous administration of EGCG (10 mg/kg) 5 minutes before reperfusion significantly reduced plasma levels of mitochondrial DNA (mtDNA) and inflammatory cytokines—including TNF-α, IL-6, and IL-8—in MIRI mice. Moreover, plasma mtDNA levels positively correlated with TNF-α, IL-6, and IL-8, suggesting that mtDNA may function as a pro-inflammatory mediator [74]. OPA1 is a key regulator of inner mitochondrial membrane fusion and cristae maintenance. OMA1, a metalloendopeptidase, initiates OPA1 proteolysis, and its short autolytic form exhibits hydrolytic activity. EGCG directly interacted with OMA1 and strongly inhibited its self-cleavage, thereby attenuating OPA1 proteolysis and suppressing mitochondrial apoptosis [77].
2.3.3. Activate the Protective PI3K/Akt Pathway
The PI3K/Akt signaling pathway serves as an intrinsic regulatory mechanism that promotes cell survival under harmful external stimuli, engaging multiple downstream targets and influencing diverse cellular functions. Multiple studies have demonstrated that the cardioprotective effects of EGCG in MI and MIRI are mediated through activation of this pathway, whereas pharmacological inhibition of PI3K/Akt signaling abolishes the protective effects of EGCG [73,74,75].
2.3.4. Inhibit Regulated Cell Death
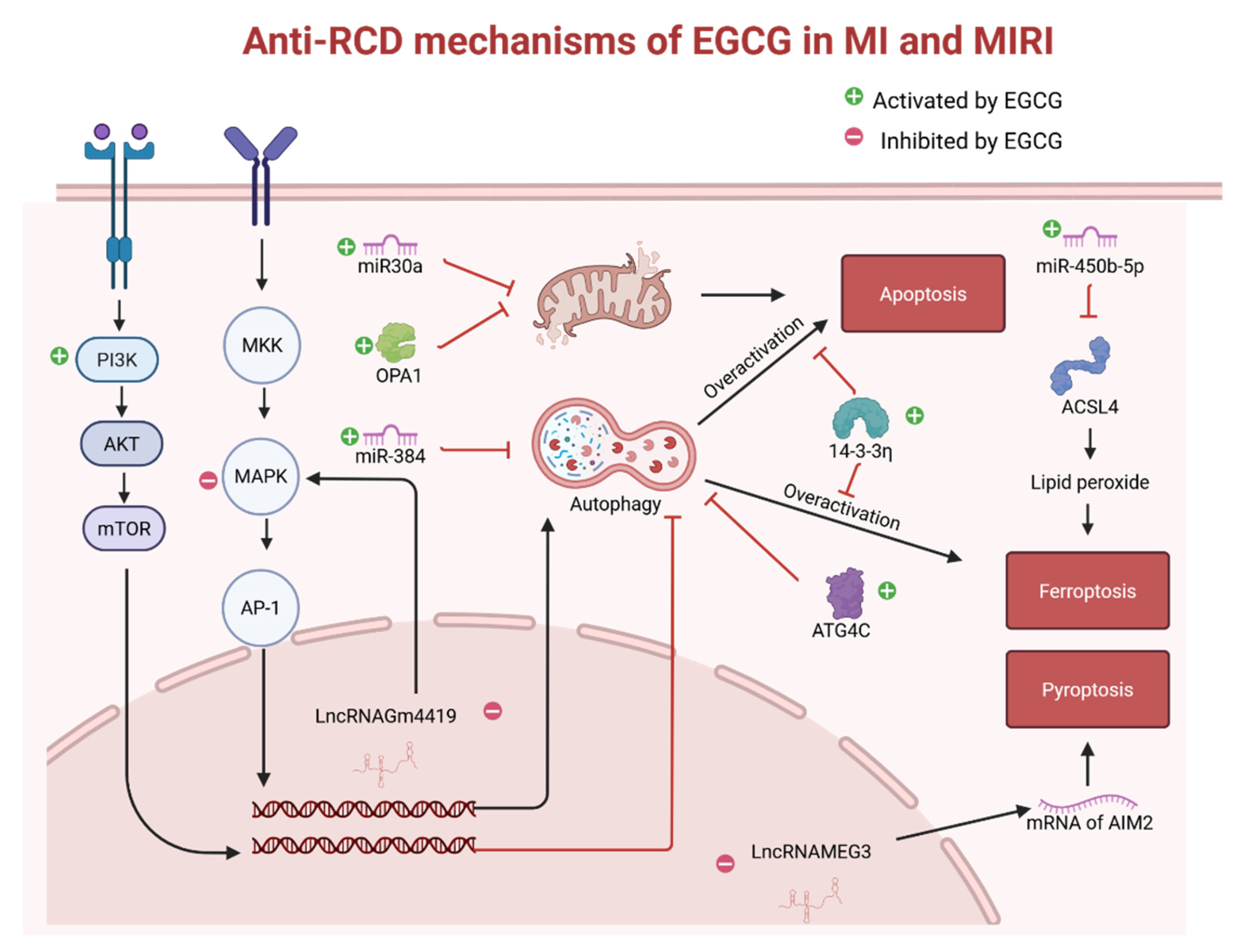
In addition to oxidative stress, inflammatory responses, and mitochondrial damage, MI and MIRI also induce excessive autophagy in CMs, leading to functional impairment and increased apoptosis. The inhibitory effects of EGCG on excessive autophagy and apoptosis have been confirmed in multiple studies [75,76,81]. MicroRNA-30a (miR-30a) inhibits apoptosis by regulating gene expression, and EGCG treatment in MI mice upregulated miR-30a expression in CMs. Notably, miR-30a can also be transferred to neighboring CMs via exosomes, thereby exerting protective effects [78]. In recent years, beyond apoptosis, which has been extensively characterized, other forms of RCD—including ferroptosis and pyroptosis—have been recognized as critical contributors to MI and MIRI. Studies have shown that EGCG inhibits ferroptosis in CMs by upregulating 14–3–3η protein [83] and miR-450b-5p [79] in mice, and suppresses pyroptosis by downregulating long non-coding RNA (LncRNA) MEG3, which reduces the stability of AIM2 mRNA [82]. Collectively, through multiple pathways, EGCG suppresses RCD in CMs and enhances their survival, and the main anti-RCD mechanisms of EGCG in MI and MIRI are illustrated in Figure 2.
Figure 2.
In MI and MIRI, cardiomyocytes often exhibit impaired PI3K signaling pathways and overactivation of MAPK pathways, leading to excessive autophagy and the induction of regulated cell death (RCD). EGCG mitigates this phenomenon through the mediation of miR-384, LncRNAGm4419, 14-3-3η protein, and ATG4C protein. In addition, EGCG increases the expression level of miR-30a, inhibits the hydrolysis of OPA1, and thereby suppresses mitochondrial apoptosis. EGCG reduces ACSL4 protein expression by increasing the expression level of miR-450b-5p, thereby inhibiting ferroptosis; and it reduces the stability of AIM2 mRNA by lowering the expression level of LncRNAMEG3, thereby inhibiting pyroptosis.
Figure 2.
In MI and MIRI, cardiomyocytes often exhibit impaired PI3K signaling pathways and overactivation of MAPK pathways, leading to excessive autophagy and the induction of regulated cell death (RCD). EGCG mitigates this phenomenon through the mediation of miR-384, LncRNAGm4419, 14-3-3η protein, and ATG4C protein. In addition, EGCG increases the expression level of miR-30a, inhibits the hydrolysis of OPA1, and thereby suppresses mitochondrial apoptosis. EGCG reduces ACSL4 protein expression by increasing the expression level of miR-450b-5p, thereby inhibiting ferroptosis; and it reduces the stability of AIM2 mRNA by lowering the expression level of LncRNAMEG3, thereby inhibiting pyroptosis.
2.4. Preservation of Cardiac Function
Cardiac function is regulated by multiple factors. The inhibitory effects of EGCG on adverse remodeling, its preservation of mitochondrial function, and its suppression of RCD in MI and MIRI collectively contribute to the attenuation of cardiac dysfunction. Beyond MI and MIRI, in vivo mouse studies have validated the protective effects of long-term oral EGCG on cardiac function in aging, manganese superoxide dismutase (Mn-SOD) deficient, and troponin mutation related RCM models [85,86,87]. Long-term oral administration of EGCG also enhanced tolerance to MIRI in T2DM mice [80], and spontaneously hypertensive rats (SHR) [88], thereby mitigating cardiac dysfunction. Furthermore, EGCG directly interacts with cTn, modulates thin-filament function, increases ATP content, and enhances calcium transients, thereby improving contractile function at the single-cell level. All preclinical studies on the cardioprotective effects of EGCG on cardiac function are summarized in Table 4.
Table 4.
A summary of preclinical studies on the protective effects of EGCG on cardiac function with different dosing regimens in various injury models.
Table 4.
A summary of preclinical studies on the protective effects of EGCG on cardiac function with different dosing regimens in various injury models.
| Injury Models | Dosage regimen | Results | References |
|---|---|---|---|
| Healthy male Wistar rats | 0.12 mg of EGCG (po, qd) for 28 days |
Mitochondrial function ↑ ATP ↑ Cardiomyocyte mechanics ↑ Calcium transient ↑ |
[89] |
| Transgenic mice (cTnI-R193H) |
EGCG 50 mg/kg (ip, qd) for 3 months |
Diastolic function ↑ | [85] |
| Senium C57BL/6 mice (16-18 months old) |
At the age of 16 months EGCG 50 mg/kg (ip, qd) for 8 weeks |
Diastolic function ↑ HDAC1, HDAC3 ↓ cTnI ↑ |
[86] |
| Mn-SOD-deficient mice | At the age of 8 week EGCG 10, 100mg/L in drinking water for 8 weeks |
Survival rate ↑ Cardiac dilatation ↓ Cardiac contraction ↑ Oxidative stress, Free fatty acids ↓ Telomerase activity ↓ Telomere length ↑ |
[87] |
| High-fat diet for 4 weeks STZ 30 mg/kg (ip) for 2 doses in 1 week in male SD rats |
After induction of DM EGCG 40, 80 mg/ kg (po, qd) for 8 weeks |
FBG ↓ CK-MB, cTnI ↓ Histopathological injury ↓ Autophagy, MMP2, MMP9 ↑ Fibrosis area, COL-I, COL-III ↓ LVSP, ±dp/dt max ↑ LVEDP ↓ |
[90] |
| TAC for 4 weeks in C57BL/6 mice |
EGCG 10 mg/kg (ip, qd) for 4 weeks |
Histopathological injury ↓ BNP ↓ Oxidative stress ↓ Inflammation ↓ Apoptosis ↓ LVEDD, LVESD ↓ LVEF ↑ TGF-β1/smad3 pathway ↓ COL-I, COL-III ↓ |
[14] |
| TAC for 12 weeks in C57BL/6 mice |
After TAC EGCG 50 mg/kg (ip, qd) for 12 weeks |
Preventive effect on HF SERCA2a ↑ |
[91] |
| AAC for 4 weeks in rats |
After AAC EGCG (25, 50, 100 mg/kg/day) for 4 weeks |
GRK2 ↓ β1-AR ↑ HW/BW, Posterior wall thickness ↓ LVSP, ±dp/dt max ↑ LVEDP ↓ Histopathological injury ↓ |
[92] |
| TAC for 12 weeks in mice |
EGCG 50 mg/kg (ip, qd) for 12 weeks |
HDAC5 ↓ Cardiac enlargement ↓ Cardiac function ↑ |
[93] |
| AAC for 16 weeks in male SD rats |
8 weeks after AAC EGCG 100 mg/kg (ip, qd) for 8 weeks |
Cardiac function ↑ Myocardial hypertrophy, fibrosis ↓ Mitochondrial function ↑ |
[94] |
| LADO for 12h in male SD rats |
2h before induction of MI EGCG 10 mg/kg (iv) |
miR30a levels ↑ CK-MB, cTnI ↓ Histopathological injury ↓ Excessive autophagy ↓ Apoptosis ↓ LVEF, LVSP, ±dp/dt max ↑ LVEDP ↓ |
[78] |
| LADO for 18h in C57BL/6 mice |
30 min before induction of MI EGCG 5, 10, 20 mg/kg (iv) |
SOD ↑ MDA ↓ miR-450b-5p ↑ ACSL4, Ferroptosis ↓ LVEDD, LVESD ↓ LVEF, FS ↑ |
[79] |
| LADO for 4 weeks in C57BL/6 mice |
After induction of MI EGCG 50 mg/kg (po, qd) for 4 weeks |
CK-MB, LDH ↓ Histopathological injury ↓ LncRNA MEG3 ↓ Pyroptosis ↓ Cell death rate ↓ Infract size ↓ LVEF ↑ |
[82] |
| LADO for 14 days in adult Wistar rats |
After induction of MI EGCG 50 mg/kg (po, qd) for 14 days |
Endoglin ↓ HW/BW, Fibrosis area ↓ LVEDD, LVESD ↓ MAP, FS ↑ |
[54] |
| LADO for 4 weeks in C57BL/6 mice |
After induction of MI EGCG 50 mg/kg (po, qd) for 1 week |
1 week after MI: Snail (EndMT marker) ↓ MMP-2, MMP-9 ↓ COL-I, COL-III ↓ 4 weeks after MI: Apoptosis ↓ Infract size ↓ Fibrosis area ↓ Capillary density ↑ LVEF ↑ |
[56] |
| LADO for 30 min Reperfusion for 2 h in SD rats with DM |
Before injury EGCG 100 mg/kg (po, qd) for 2 weeks |
SIRT1 ↑ Mn-SOD ↑ MDA ↓ LDH ↓ Apoptosis ↓ Infarct size ↓ Fibrosis area ↓ LVSP, ±dp/dt max ↑ |
[80] |
| LADO for 30 min Reperfusion for 2 h In male SD rats |
10 min before reperfusion EGCG 10 mg/kg (iv) |
PI3K/AKT pathway ↑ Excessive autophagy ↓ CK-MB, LDH ↓ Nitric oxide ↑ Apoptosis ↓ Infarct size ↓ LVSP, ±dp/dt max ↑ LVEDP ↓ |
[95] |
| LADO for 30 min Reperfusion for 12 h in SD rats |
30 min before ischemia EGCG 10, 20 mg/kg (iv) |
miR30a ↑ p53 ↓ Apoptosis ↓ CK-MB, LDH ↓ Histopathological injury ↓ ATP ↑ LVEF, LVSP, ±dp/dt max ↑ LVEDP ↓ |
[96] |
| LADO for 60 min Reperfusion for 2 h in C57BL/6 mice |
Before injury EGCG 20 mg/kg (po, qd) for 6 weeks |
MDA ↓ Ferroptosis ↓ CK-MB, LDH ↓ Histopathological injury ↓ Infarct size ↓ LVEF ↑ |
[83] |
| LIHPS for hearts of male Wistar rats |
EGCG 1, 4 μM in perfusate |
LVSP, ±dp/dt max ↑ | [97] |
| LIHPS for hearts of Chinchilla rabbits Cardioplegia for 90 min Reperfusion for 1 h |
At the same time of cardioplegia EGCG 20 μM in cardioplegic solutions for 90 min |
Nitrosative and oxidative stress ↓ Apoptosis ↓ ATP ↑ LVSP ↑ |
[98] |
| LIHPS for hearts of male SHR Ischemia for 30 min Reperfusion for 2 h |
Before injury EGCG 200 mg/kg (po, qd) for 3 weeks |
Coronary flow ↑ Infarct size ↓ LVDP ↑ LVEDP ↓ |
[88] |
| LIHPS for hearts of guinea pigs Ischemia for 40 min Reperfusion for 40 min |
4 min before injury EGCG 30 μM in perfusate |
Mitochondrial Ca2+ elevation ↓ Apoptosis ↓ ATP ↑ LVEDP ↓ |
[99] |
| LIHPS for hearts of male Wistar rats Ischemia for 30 min Reperfusion for 2 h |
10 min before ischemia EGCG 1, 10 μM in perfusate for 40 min |
Infarct size ↓ LVDP, ±dp/dt max NS Mitochondrial KATP activity ↑ |
[100] |
| LIHPS for hearts of male Wistar rats Ischemia for 30 min Reperfusion for 2 h |
5 min before reperfusion EGCG 1, 10 μM in perfusate for 35 min |
Infarct size ↓ LVDP, ±dp/dt max ↑ |
[101] |
| LIHPS for hearts of male SD rats Ischemia for 20 min Reperfusion for 2 h |
10 min before injury EGCG 5 μM in perfusate for 130 min |
Mn-SOD, Cu/Zn-SOD ↑ Lipid peroxides ↓ Apoptosis ↓ Infarct size ↓ LVDP, ±dp/dt max ↑ LVEDP ↓ |
[102] |
| CMs of adult rats |
EGCG 2.5, 5 μM | Calcium transient ↑ FS ↑ |
[97] |
| CMs of C57BL/6 mice |
EGCG 10nM-100 μM | Calcium transient ↑ | [103] |
| Human cTn subunits with cTnT-Δ160E mutation |
EGCG 3 μM | Bind to the C-lobe of cTnC Binding of cTnI to cTnC ↑ Ca2+ sensitivity in myofilaments ↓ |
[104] |
| CMs of transgenic mice (cTnI-R193H) |
EGCG 5 μM | Ca2+ decay, Sarcomere relaxation ↑ | [85] |
| cTnT with mutations associated with HCM |
EGCG 100 μM | Restore the coupling between Ca2+ and cTnT |
[105] |
| Reconstituted TF with cTnC-G34S or cTnI-D127Y mutations |
EGCG 20 μM | Aggregation and elongation of TF ↑ Maximal myosin-S1-ATPase activity ↑ Ca2+ sensitivity in myofilaments ↓ |
[106] |
2.4.1. Better Cardiac Structure
Adverse cardiac remodeling results in myocardial fibrosis and reduced compliance. The inhibitory effects of EGCG on adverse cardiac remodeling have been discussed earlier, including clinical trials evaluating its ability to inhibit transthyretin deposition; however, improvement in cardiac function was not the primary endpoint. Numerous in vivo mouse studies have demonstrated that long-term EGCG treatment ameliorated myocardial fibrosis and improved cardiac function in models of T2DM [90], HF [14,91,92,93,94], and post-MI [54,56].
2.4.2. More Cardiomyocyte Survival
Increased cardiomyocyte survival supports cardiac function, and in vivo mouse studies demonstrated that emergency EGCG administration during MI and MIRI significantly reduced cardiomyocyte mortality and improved cardiac function [78,79,95,96]. In ex vivo experiments using the Langendorff isolated heart perfusion system (LIHPS) to maintain cardiac activity, supplementation of the perfusate with EGCG during the induction of MIRI [99,102] or CPB related injury [98] reduced cardiomyocyte apoptosis and mitigated cardiac dysfunction. Although one ex vivo MIRI study [100] reported no improvement in cardiac function, another study [101] employing the same methodology but altering the timing of EGCG administration demonstrated significant functional improvement. The negative findings of the former study may be attributable to suboptimal timing of administration, as EGCG was not delivered during the reperfusion period.
2.4.3. Better Cardiomyocyte Function
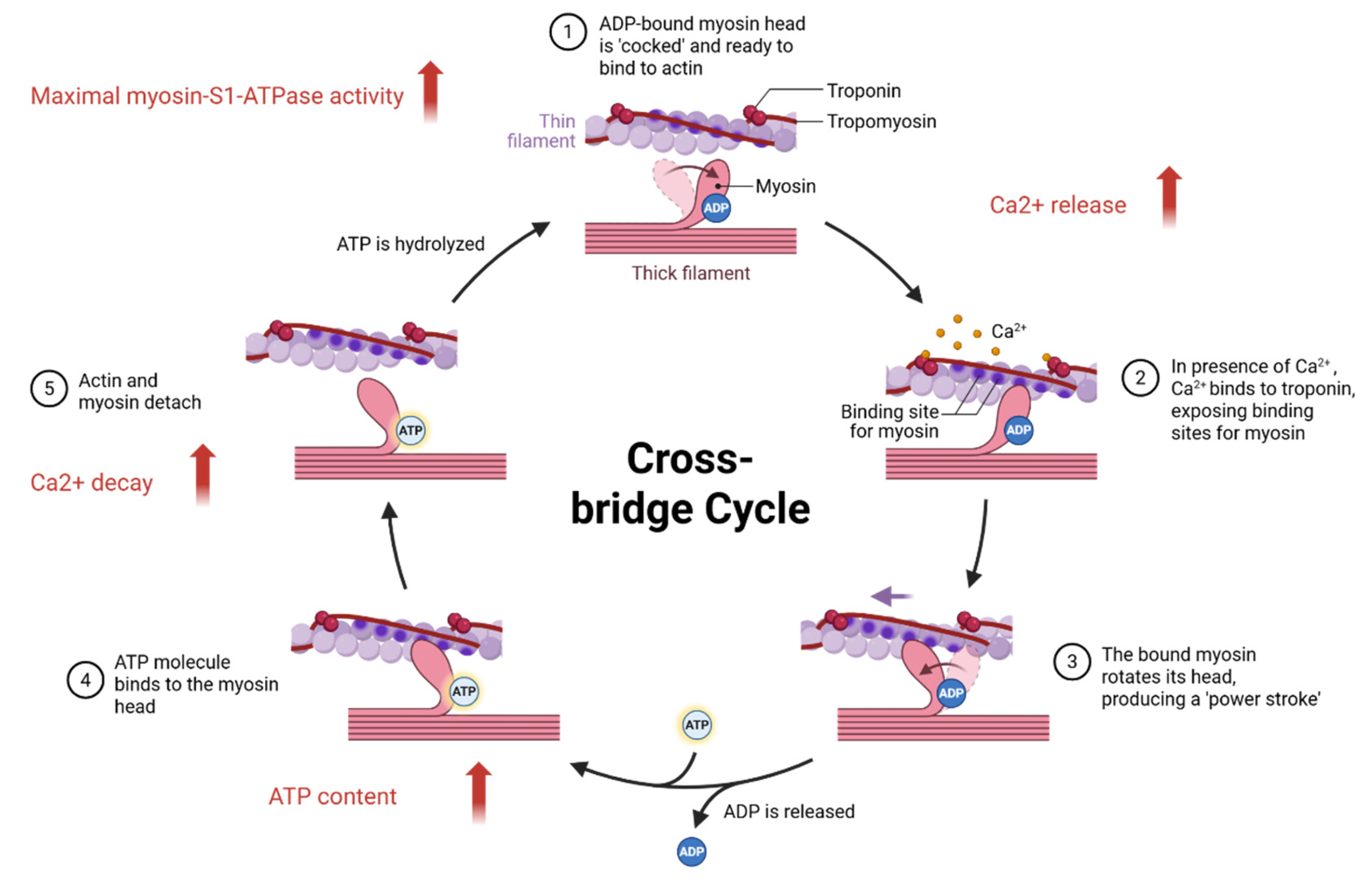
EGCG reduced mitochondrial injury in MI and MIRI mice and prevented downregulation of β1-adrenoceptors (β1-ARs) on cardiomyocyte membranes in HF mice [92], both of which favor enhanced cardiomyocyte contractile function. However, the effects of EGCG on β1-AR expression in cardiomyocyte membranes appear to be long-term, and whether it can elevate expression beyond baseline levels remains to be elucidated. The mechanisms underlying EGCG-mediated enhancement of cardiomyocyte contractile and diastolic function primarily involve regulation of mitochondrial activity, ion channel dynamics, and thin-filament function, with their mechanisms illustrated in Figure 3. Even in the absence of injurious stimuli, EGCG treatment increased mitochondrial activity in mouse CMs and improved cardiac function [89,97]. In vitro studies have demonstrated that EGCG augments calcium transient peaks in CMs [97,103], thereby enhancing cardiomyocyte contractility. In addition, EGCG directly interacts with cTn, suggesting therapeutic potential for patients with troponin mutations. EGCG modulates troponin calcium sensitivity, accelerates calcium dissociation from troponin, facilitates sarcomere relaxation [85,104,106], restores excitation–contraction coupling [105], and increases maximal myosin ATPase activity [106], thereby enhancing thin-filament contractile and diastolic function.
Figure 3.
EGCG increases calcium transients, enhancing the number of activated cross-bridges during excitation-contraction coupling, while also increasing ATP content to provide potential energy for more myosin, thereby improving cardiomyocyte contractile function. In addition, EGCG increases ATPase activity, accelerating the detachment of myosin and actin, reduces the increased calcium sensitivity caused by troponin mutations, and accelerates the detachment of troponin from calcium ions, thereby improving the diastolic function of cardiomyocytes.
Figure 3.
EGCG increases calcium transients, enhancing the number of activated cross-bridges during excitation-contraction coupling, while also increasing ATP content to provide potential energy for more myosin, thereby improving cardiomyocyte contractile function. In addition, EGCG increases ATPase activity, accelerating the detachment of myosin and actin, reduces the increased calcium sensitivity caused by troponin mutations, and accelerates the detachment of troponin from calcium ions, thereby improving the diastolic function of cardiomyocytes.
3. Adverse Reactions of Epigallocatechin Gallate
In preclinical toxicology studies, administration of EGCG at 50 mg/kg intravenously (iv, once daily) for 10 days or 2000 mg/kg orally (po, once daily) for 10 days did not induce genotoxicity in mice [107]. Similarly, oral EGCG at 500 mg/kg daily for 13 weeks did not cause dermal irritation in rats [108], and dietary supplementation with 1400, 4200, or 14,000 mg/kg EGCG during organogenesis was non-toxic to pregnant rats or their fetuses [109]. Oral EGCG reduces the bioavailability of iron [110], folic acid [111], and other drugs [112], by inhibiting their absorption. Moreover, although EGCG acts as an antioxidant, it exhibits pro-oxidative effects at higher doses [113,114]. In vitro, hepatocytes exhibited damage upon exposure to 200 μM EGCG. In vivo, a single intraperitoneal injection of 100 mg/kg EGCG elevated plasma ALT levels in mice, and doses of 150 mg/kg caused death within 22 hours [115]. Cai et al. reported that oral EGCG at 500 or 1000 mg/kg daily for 8 days induced mild cardiac fibrosis in mice [116]. Similarly, Rasheed et al. observed that intraperitoneal EGCG at 100 mg/kg daily for 4 days caused mild myocardial injury in diabetic mice [117]. In LIHPS experiments, low-dose EGCG (20 μM) enhanced cardiac contractility, whereas high-dose EGCG (50 μM) increased the incidence of arrhythmia and diastolic dysfunction [118]. Overall, animal studies indicate that adverse effects of EGCG occur only at relatively high doses, far exceeding those required for therapeutic efficacy.
In clinical studies, the most frequently reported adverse effects are hepatotoxicity and gastrointestinal disturbances, particularly when consumed on an empty stomach [119,120]. A few case reports have suggested that EGCG may cause severe liver injury [121], however, given the very low incidence, current evidence is insufficient to establish a definitive causal relationship. In healthy volunteers, EGCG was shown to reduce folic acid bioavailability [122], although the doses and duration required to induce clinical folate deficiency remain unclear. A daily oral dose of 800 mg EGCG for 4 weeks was reported to be safe in healthy individuals [123]. According to the European Food Safety Authority, average daily intake of EGCG from GT ranges from 90 to 300 mg/day, reaching up to 866 mg/day in heavy tea drinkers [124]. Thus, EGCG intake through tea consumption is considered safe. Large-scale population studies have reported no association between tea consumption during pregnancy and adverse outcomes [125]. Subsequent clinical studies have shown that even higher oral doses of EGCG administered for 12 to 16 weeks (up to 865 mg/day) did not elicit significant adverse reactions, supporting its safety [23,30]. In a clinical trial, topical application of an EGCG spray (2574 μmol/L) three times daily for 2 weeks to treat severe radiotherapy-induced dermatitis revealed no EGCG-related adverse reactions [126].
Overall, the threshold doses of EGCG that induce serious adverse effects vary substantially depending on the administration route, treatment duration, and comorbidities of the subjects. The degree of oxidative stress also differs between healthy individuals and patients with T2DM, MI, or MIRI. In populations with high oxidative stress, doses considered therapeutic may correspond to high doses in healthy individuals, potentially exacerbating oxidative stress and inducing adverse effects. Current clinical research primarily focuses on oral administration, typically at relatively low doses, while the safety profile of higher doses and alternative administration routes requires further investigation. Collectively, the available evidence indicates that EGCG is generally safe at dietary and clinically tested doses, but careful dose selection and population-specific evaluation remain essential for its therapeutic application.
4. Conclusions and Future Perspectives
As a natural antioxidant and anti-inflammatory agent, long-term EGCG treatment improves glucose and lipid metabolism, prevents CAD progression, and alleviates adverse cardiac remodeling associated with T2DM, MI, HF, and related conditions. In acute injuries such as MI and MIRI, emergency EGCG administration reduces cardiomyocyte injury and suppresses RCD. The cardioprotective effects of EGCG have been validated in numerous cellular and small-animal studies. However, research in large-animal and comorbidity models remains limited, and clinical trials have primarily focused on metabolic outcomes, with few exploring EGCG in MI, MIRI, or CPB. Given its cardioprotective efficacy and favorable safety profile, further studies are warranted in large-animal models, comorbidity settings, and clinical trials assessing different EGCG dosages, administration routes, and timing strategies.
Particular attention should be paid to tailoring EGCG administration to disease-specific contexts. For instance, in the emergency management of MI and MIRI, intravenous administration is superior to oral delivery, as it circumvents the problem of low oral bioavailability, reduces the need for excessive oral dosing to achieve therapeutic concentrations, and minimizes the risk of adverse effects. By contrast, for chronic conditions such as T2DM, AS, and HF, oral administration is more practical, with dosing requirements—dependent on disease severity—differing substantially from those for intravenous therapy. In animal models, the safe oral dose may reach 500 mg/kg per day, whereas efficacy studies commonly employ ~50 mg/kg per day, equivalent to approximately 2500 mg/day in humans. Yet, the highest dose tested in current clinical trials does not exceed 1000 mg/day, and the safety and efficacy of higher oral doses remain to be clarified. For long-term oral administration, dividing the daily dose into three portions taken after meals is preferable, as this strategy reduces gastrointestinal irritation and minimizes fluctuations in plasma drug concentrations. Moreover, the timing of administration is critical. In MIRI, EGCG administration should precede reperfusion to counteract the surge of oxidative stress and inflammation during this phase.
Clinical investigations of EGCG can be extended to diverse clinical contexts. In designing dosing regimens, clinical applications should account for disease severity, the nature of injury (acute vs. chronic), and the practicality of administration. For example, to evaluate the preventive effect of EGCG on MINS, a relatively mild surgical complication, EGCG could be incorporated into the preoperative clear-liquid diet. To explore its therapeutic effect in MIRI, EGCG could be administered intravenously before or during reperfusion in patients with MI. For CPB, EGCG could be added to the cardioplegic solution to protect the arrested heart. In summary, dosing strategies for different administration routes must be carefully optimized, and the safety of these regimens should be rigorously monitored in human populations.
Moreover, EGCG could be applied as a coating for arterial stents in patients with AS [127], or incorporated into nanocomposite formulations with other therapeutic agents [128,129,130], offering further opportunities for drug-combination strategies. In addition to conducting more clinical studies, the combination of EGCG with other drugs through nanotechnology to design new multifunctional composite drugs is also an important research direction for future EGCG research.
Funding
This paper was not funded.
Acknowledgments
Figures were created with BioRender.com.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abbreviations
The following abbreviation are used in this manuscript:
| GT | Green tea |
| GTE | Green tea extract |
| EGCG | Epigallocatechin gallate |
| MS | Metabolic syndrome |
| T2DM | Type 2 diabetes mellitus |
| GDM | Gestational diabetes mellitus |
| DCM | Diabetic cardiomyopathy |
| ATTR-CM | Amyloidotic transthyretin cardiomyopathy |
| wtATTR-CM | wild-type transthyretin amyloid cardiomyopathy |
| AS | Atherosclerosis |
| CAD | Coronary artery disease |
| MI | Myocardial infarction |
| MIRI | Myocardial ischemia-reperfusion injury |
| MINS | Myocardial injury after non-cardiac surgery |
| RCM | Restrictive cardiomyopathy |
| HCM | Hypertrophic cardiomyopathy |
| HF | Heart failure |
| ApoE | Apolipoprotein E |
| SD | Sprague-Dawley |
| SHR | Spontaneously hypertensive rats |
| HUVECs | Human umbilical vein endothelial cells |
| HASMCs | Human aortic smooth muscle cells |
| MEFs | Mouse embryonic fibroblasts |
| CMs | Cardiomyocytes |
| CFs | Cardiac fibroblasts |
| TF | Thin filament |
| P. gingivalis | Porphyromonas gingivalis |
| NAM | Nicotinamide |
| STZ | Streptozotocin |
| ISO | Isoprenaline |
| AAC | Abdominal aortic constriction |
| TAC | Transverse aortic constriction |
| LADO | Left anterior descending artery occlusion |
| LMCAO | Left main coronary artery occlusion |
| LIHPS | Langendorff isolated heart perfusion system |
| CPB | Cardiopulmonary bypass |
| Ang II | Angiotensin II |
| P/I | Phorbol 12-myristate 13-acetate and ionomycin |
| β-GP | β-Glucopyranosyl phosphate |
| HRI | Hypoxia-reoxygenation injury |
| LA | Lipid abnormality |
| TC | Total cholesterol |
| TG | Triglyceride |
| LDL-C | Low-density lipoprotein cholesterol |
| VLDL-C | Very low-density lipoprotein cholesterol |
| HDL-C | High-density lipoprotein cholesterol |
| AIP | Atherogenic index of plasma |
| HOMA-IR | Homeostasis model assessment of insulin resistance |
| OGTT | Oral glucose tolerance test |
| FBG | Fasting blood glucose |
| HbA1C | Hemoglobin A1C |
| GLP-1 | Glucagon-like peptide 1 |
| ROS | Reactive oxygen species |
| SOD | Superoxide dismutase |
| Mn-SOD | Manganese superoxide dismutase |
| CAT | Catalase |
| GPX4 | Glutathione peroxidase 4 |
| GSH | Glutathione |
| VC | Vitamin C |
| VE | Vitamin E |
| CER | Ceruloplasmin |
| T-AOC | Total antioxidant capacity |
| MDA | Malondialdehyde |
| CRP | C-reactive protein |
| ESR | Erythrocyte sedimentation rate |
| MPO | Myeloperoxidase |
| MCP-1 | Monocyte chemoattractant protein-1 |
| VEGFA | Vascular endothelial growth factor |
| ICAM-1 | Intercellular adhesion molecule-1 |
| VCAM-1 | Vascular cell adhesion molecule-1 |
| CTGF | Connective tissue growth factor |
| EMMPRIN | Extracellular matrix metalloproteinase inducer |
| MMPs | Matrix metalloproteinases |
| EndMT | Endothelial-to-mesenchymal transition |
| COL | Collagen |
| HW | Heart weight |
| BW | Body weight |
| TL | Tibia length |
| SIRT1 | Silent information regulator 1 |
| mtDNA | Mitochondrial DNA |
| SERCA2a | Sarcoplasmic reticulum Ca-ATPase |
| β1-AR | β1-adrenoceptors |
| cTn | Cardiac troponin |
| cTnC | Cardiac troponin C |
| cTnT | Cardiac troponin T |
| cTnI | Cardiac troponin I |
| CK | Creatine kinase |
| CK-MB | Creatine kinase-MB |
| LDH | Lactate dehydrogenase |
| ALP | Alkaline phosphatase |
| AST | Aspartate aminotransferase |
| ALT | Alanine transaminase |
| RCD | Regulated cell death |
| CO | Cardiac output |
| SAP | Systolic arterial pressure |
| MAP | Mean arterial pressure |
| DAP | Diastolic arterial pressure |
| LVEF | Left ventricular ejection fraction |
| LVEDD | Left ventricular end-diastolic dimension |
| LVESD | Left ventricular end-systolic dimension |
| LVSP | Left ventricular systolic pressure |
| LVEDP | Left ventricular end-diastolic pressure |
| LVDP | Left ventricular developed pressure |
| ±dp/dt max | Maximal left ventricular pressure variation rate |
| FS | Fractional shortening |
| TXA2 | Thromboxane A2 |
| ATG4C | Autophagy related 4C |
| HDAC | Histone deacetylase |
| KATP | ATP-sensitive potassium channels |
| NS | Not Significant |
References
- Saklayen, M. G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef]
- Al Hroob, A. M.; Abukhalil, M. H.; Hussein, O. E.; Mahmoud, A. M. Pathophysiological Mechanisms of Diabetic Cardiomyopathy and the Therapeutic Potential of Epigallocatechin-3-Gallate. Biomed. Pharmacother. Biomedecine Pharmacother. 2019, 109, 2155–2172. [Google Scholar] [CrossRef]
- Salari, N.; Morddarvanjoghi, F.; Abdolmaleki, A.; Rasoulpoor, S.; Khaleghi, A. A.; Hezarkhani, L. A.; Shohaimi, S.; Mohammadi, M. The Global Prevalence of Myocardial Infarction: A Systematic Review and Meta-Analysis. BMC Cardiovasc. Disord. 2023, 23, 206. [Google Scholar] [CrossRef]
- Zhang, C.; Wang, S.; Li, H.; Su, F.; Huang, Y.; Mi, W.; Chinese Anaesthesiology Department Tracking Collaboration Group. Anaesthesiology in China: A Cross-Sectional Survey of the Current Status of Anaesthesiology Departments. Lancet Reg. Health West. Pac. 2021, 12, 100166. [Google Scholar] [CrossRef] [PubMed]
- Bello, C.; Rössler, J.; Shehata, P.; Smilowitz, N. R.; Ruetzler, K. Perioperative Strategies to Reduce Risk of Myocardial Injury after Non-Cardiac Surgery (MINS): A Narrative Review. J. Clin. Anesth. 2023, 87, 111106. [Google Scholar] [CrossRef] [PubMed]
- Atanasov, A. G.; Zotchev, S. B.; Dirsch, V. M.; International Natural Product Sciences Taskforce; Supuran, C. T. Natural Products in Drug Discovery: Advances and Opportunities. Nat. Rev. Drug Discov. 2021, 20, 200–216. [Google Scholar] [CrossRef]
- Brody, H. Tea. Nature 2019, 566, S1. [Google Scholar] [CrossRef]
- Abudureheman, B.; Yu, X.; Fang, D.; Zhang, H. Enzymatic Oxidation of Tea Catechins and Its Mechanism. Mol. Basel Switz. 2022, 27, 942. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.; Mukhtar, H. Tea Polyphenols in Promotion of Human Health. Nutrients 2018, 11, 39. [Google Scholar] [CrossRef]
- Ntamo, Y.; Jack, B.; Ziqubu, K.; Mazibuko-Mbeje, S. E.; Nkambule, B. B.; Nyambuya, T. M.; Mabhida, S. E.; Hanser, S.; Orlando, P.; Tiano, L.; Dludla, P. V. Epigallocatechin Gallate as a Nutraceutical to Potentially Target the Metabolic Syndrome: Novel Insights into Therapeutic Effects beyond Its Antioxidant and Anti-Inflammatory Properties. Crit. Rev. Food Sci. Nutr. 2024, 64, 87–109. [Google Scholar] [CrossRef]
- Wang, L.; Tang, C.; Pan, Q. Mechanisms Underlying the Anti-Atherosclerotic Effects of EGCG. Curr. Mol. Med. 2025. [Google Scholar] [CrossRef]
- Wei, X.-Y.; Zeng, Y.-F.; Guo, Q.-H.; Liu, J.-J.; Yin, N.; Liu, Y.; Zeng, W.-J. Cardioprotective Effect of Epigallocatechin Gallate in Myocardial Ischemia/Reperfusion Injury and Myocardial Infarction: A Meta-Analysis in Preclinical Animal Studies. Sci. Rep. 2023, 13, 14050. [Google Scholar] [CrossRef]
- aus dem Siepen, F.; Bauer, R.; Aurich, M.; Buss, S. J.; Steen, H.; Altland, K.; Katus, H. A.; Kristen, A. V. Green Tea Extract as a Treatment for Patients with Wild-Type Transthyretin Amyloidosis: An Observational Study. Drug Des. Devel. Ther. 2015, 9, 6319–6325. [Google Scholar] [CrossRef]
- Chen, K.; Chen, W.; Liu, S. L.; Wu, T. S.; Yu, K. F.; Qi, J.; Wang, Y.; Yao, H.; Huang, X. Y.; Han, Y.; Hou, P. Epigallocatechingallate Attenuates Myocardial Injury in a Mouse Model of Heart Failure through TGF--β1/Smad3 Signaling Pathway. Mol. Med. Rep. 2018, 17, 7652–7660. [Google Scholar] [CrossRef]
- Fan, J.; Watanabe, T. Atherosclerosis: Known and Unknown. Pathol. Int. 2022, 72, 151–160. [Google Scholar] [CrossRef]
- Wang, R.-X.; Zhou, M.; Ma, H.-L.; Qiao, Y.-B.; Li, Q.-S. The Role of Chronic Inflammation in Various Diseases and Anti-Inflammatory Therapies Containing Natural Products. ChemMedChem 2021, 16, 1576–1592. [Google Scholar] [CrossRef]
- Reddy, P.; Lent-Schochet, D.; Ramakrishnan, N.; McLaughlin, M.; Jialal, I. Metabolic Syndrome Is an Inflammatory Disorder: A Conspiracy between Adipose Tissue and Phagocytes. Clin. Chim. Acta Int. J. Clin. Chem. 2019, 496, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Liu, J.; Duan, H.; Li, R.; Peng, W.; Wu, C. Activation of Nrf2/HO-1 Signaling: An Important Molecular Mechanism of Herbal Medicine in the Treatment of Atherosclerosis via the Protection of Vascular Endothelial Cells from Oxidative Stress. J. Adv. Res. 2021, 34, 43–63. [Google Scholar] [CrossRef]
- Yamagata, K. Protective Effect of Epigallocatechin Gallate on Endothelial Disorders in Atherosclerosis. J. Cardiovasc. Pharmacol. 2020, 75, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J. L. Metalloproteinases in Atherosclerosis. Eur. J. Pharmacol. 2017, 816, 93–106. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Ohishi, T.; Tanabe, H.; Miyoshi, N.; Nakamura, Y. Anti-Inflammatory Effects of Dietary Polyphenols through Inhibitory Activity against Metalloproteinases. Mol. Basel Switz. 2023, 28, 5426. [Google Scholar] [CrossRef]
- Bogdanski, P.; Suliburska, J.; Szulinska, M.; Stepien, M.; Pupek-Musialik, D.; Jablecka, A. Green Tea Extract Reduces Blood Pressure, Inflammatory Biomarkers, and Oxidative Stress and Improves Parameters Associated with Insulin Resistance in Obese, Hypertensive Patients. Nutr. Res. N. Y. N 2012, 32, 421–427. [Google Scholar] [CrossRef]
- Chen, I.-J.; Liu, C.-Y.; Chiu, J.-P.; Hsu, C.-H. Therapeutic Effect of High-Dose Green Tea Extract on Weight Reduction: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Clin. Nutr. Edinb. Scotl. 2016, 35, 592–599. [Google Scholar] [CrossRef]
- Chatree, S.; Sitticharoon, C.; Maikaew, P.; Pongwattanapakin, K.; Keadkraichaiwat, I.; Churintaraphan, M.; Sripong, C.; Sririwichitchai, R.; Tapechum, S. Epigallocatechin Gallate Decreases Plasma Triglyceride, Blood Pressure, and Serum Kisspeptin in Obese Human Subjects. Exp. Biol. Med. Maywood NJ 2021, 246, 163–176. [Google Scholar] [CrossRef] [PubMed]
- Kanu, V. R.; Pulakuntla, S.; Kuruvalli, G.; Aramgam, S. L.; Marthadu, S. B.; Pannuru, P.; Hebbani, A. V.; Desai, P. P. D.; Badri, K. R.; Vaddi, D. R. Anti-Atherogenic Role of Green Tea (Camellia Sinensis) in South Indian Smokers. J. Ethnopharmacol. 2024, 332, 118298. [Google Scholar] [CrossRef]
- Wilasrusmee, K. T.; Sitticharoon, C.; Keadkraichaiwat, I.; Maikaew, P.; Pongwattanapakin, K.; Chatree, S.; Sririwichitchai, R.; Churintaraphan, M. Epigallocatechin Gallate Enhances Sympathetic Heart Rate Variability and Decreases Blood Pressure in Obese Subjects: A Randomized Control Trial. Sci. Rep. 2024, 14, 21628. [Google Scholar] [CrossRef]
- Brown, A. L.; Lane, J.; Coverly, J.; Stocks, J.; Jackson, S.; Stephen, A.; Bluck, L.; Coward, A.; Hendrickx, H. Effects of Dietary Supplementation with the Green Tea Polyphenol Epigallocatechin-3-Gallate on Insulin Resistance and Associated Metabolic Risk Factors: Randomized Controlled Trial. Br. J. Nutr. 2009, 101, 886–894. [Google Scholar] [CrossRef]
- Momose, Y.; Maeda-Yamamoto, M.; Nabetani, H. Systematic Review of Green Tea Epigallocatechin Gallate in Reducing Low-Density Lipoprotein Cholesterol Levels of Humans. Int. J. Food Sci. Nutr. 2016, 67, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Asbaghi, O.; Fouladvand, F.; Moradi, S.; Ashtary-Larky, D.; Choghakhori, R.; Abbasnezhad, A. Effect of Green Tea Extract on Lipid Profile in Patients with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.-H.; Liao, Y.-L.; Lin, S.-C.; Tsai, T.-H.; Huang, C.-J.; Chou, P. Does Supplementation with Green Tea Extract Improve Insulin Resistance in Obese Type 2 Diabetics? A Randomized, Double-Blind, and Placebo-Controlled Clinical Trial. Altern. Med. Rev. J. Clin. Ther. 2011, 16, 157–163. [Google Scholar]
- Liu, C.-Y.; Huang, C.-J.; Huang, L.-H.; Chen, I.-J.; Chiu, J.-P.; Hsu, C.-H. Effects of Green Tea Extract on Insulin Resistance and Glucagon-like Peptide 1 in Patients with Type 2 Diabetes and Lipid Abnormalities: A Randomized, Double-Blinded, and Placebo-Controlled Trial. PloS One 2014, 9, e91163. [Google Scholar] [CrossRef]
- Fryk, E.; Olausson, J.; Mossberg, K.; Strindberg, L.; Schmelz, M.; Brogren, H.; Gan, L.-M.; Piazza, S.; Provenzani, A.; Becattini, B.; Lind, L.; Solinas, G.; Jansson, P.-A. Hyperinsulinemia and Insulin Resistance in the Obese May Develop as Part of a Homeostatic Response to Elevated Free Fatty Acids: A Mechanistic Case-Control and a Population-Based Cohort Study. EBioMedicine 2021, 65, 103264. [Google Scholar] [CrossRef]
- Bazyar, H.; Hosseini, S. A.; Saradar, S.; Mombaini, D.; Allivand, M.; Labibzadeh, M.; Alipour, M. Effects of Epigallocatechin-3-Gallate of Camellia Sinensis Leaves on Blood Pressure, Lipid Profile, Atherogenic Index of Plasma and Some Inflammatory and Antioxidant Markers in Type 2 Diabetes Mellitus Patients: A Clinical Trial. J. Complement. Integr. Med. 2020, 18, 405–411. [Google Scholar] [CrossRef]
- Zhang, H.; Su, S.; Yu, X.; Li, Y. Dietary Epigallocatechin 3-Gallate Supplement Improves Maternal and Neonatal Treatment Outcome of Gestational Diabetes Mellitus: A Double-Blind Randomised Controlled Trial. J. Hum. Nutr. Diet. Off. J. Br. Diet. Assoc. 2017, 30, 753–758. [Google Scholar] [CrossRef]
- Ortsäter, H.; Grankvist, N.; Wolfram, S.; Kuehn, N.; Sjöholm, A. Diet Supplementation with Green Tea Extract Epigallocatechin Gallate Prevents Progression to Glucose Intolerance in Db/Db Mice. Nutr. Metab. 2012, 9, 11. [Google Scholar] [CrossRef]
- Othman, A. I.; El-Sawi, M. R.; El-Missiry, M. A.; Abukhalil, M. H. Epigallocatechin-3-Gallate Protects against Diabetic Cardiomyopathy through Modulating the Cardiometabolic Risk Factors, Oxidative Stress, Inflammation, Cell Death and Fibrosis in Streptozotocin-Nicotinamide-Induced Diabetic Rats. Biomed. Pharmacother. Biomedecine Pharmacother. 2017, 94, 362–373. [Google Scholar] [CrossRef] [PubMed]
- Gui, L.; Wang, F.; Hu, X.; Liu, X.; Yang, H.; Cai, Z.; Qi, M.; Dai, C. Epigallocatechin Gallate Protects Diabetes Mellitus Rats Complicated with Cardiomyopathy through TGF-Β1/JNK Signaling Pathway. Curr. Pharm. Des. 2022, 28, 2758–2770. [Google Scholar] [CrossRef] [PubMed]
- Martin, M. A.; Goya, L.; Ramos, S. Protective Effects of Tea, Red Wine and Cocoa in Diabetes. Evidences from Human Studies. Food Chem. Toxicol. Int. J. Publ. Br. Ind. Biol. Res. Assoc. 2017, 109 Pt 1, 302–314. [Google Scholar] [CrossRef]
- Quezada-Fernández, P.; Trujillo-Quiros, J.; Pascoe-González, S.; Trujillo-Rangel, W. A.; Cardona-Müller, D.; Ramos-Becerra, C. G.; Barocio-Pantoja, M.; Rodríguez-de la Cerda, M.; Nérida Sánchez-Rodríguez, E.; Cardona-Muñóz, E. G.; García-Benavides, L.; Grover-Páez, F. Effect of Green Tea Extract on Arterial Stiffness, Lipid Profile and sRAGE in Patients with Type 2 Diabetes Mellitus: A Randomised, Double-Blind, Placebo-Controlled Trial. Int. J. Food Sci. Nutr. 2019, 70, 977–985. [Google Scholar] [CrossRef] [PubMed]
- Widmer, R. J.; Freund, M. A.; Flammer, A. J.; Sexton, J.; Lennon, R.; Romani, A.; Mulinacci, N.; Vinceri, F. F.; Lerman, L. O.; Lerman, A. Beneficial Effects of Polyphenol-Rich Olive Oil in Patients with Early Atherosclerosis. Eur. J. Nutr. 2013, 52, 1223–1231. [Google Scholar] [CrossRef]
- Widlansky, M. E.; Hamburg, N. M.; Anter, E.; Holbrook, M.; Kahn, D. F.; Elliott, J. G.; Keaney, J. F.; Vita, J. A. Acute EGCG Supplementation Reverses Endothelial Dysfunction in Patients with Coronary Artery Disease. J. Am. Coll. Nutr. 2007, 26, 95–102. [Google Scholar] [CrossRef]
- Kristen, A. V.; Lehrke, S.; Buss, S.; Mereles, D.; Steen, H.; Ehlermann, P.; Hardt, S.; Giannitsis, E.; Schreiner, R.; Haberkorn, U.; Schnabel, P. A.; Linke, R. P.; Röcken, C.; Wanker, E. E.; Dengler, T. J.; Altland, K.; Katus, H. A. Green Tea Halts Progression of Cardiac Transthyretin Amyloidosis: An Observational Report. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2012, 101, 805–813. [Google Scholar] [CrossRef] [PubMed]
- aus dem Siepen, F.; Buss, S. J.; Andre, F.; Seitz, S.; Giannitsis, E.; Steen, H.; Katus, H. A.; Kristen, A. V. Extracellular Remodeling in Patients with Wild-Type Amyloidosis Consuming Epigallocatechin-3-Gallate: Preliminary Results of T1 Mapping by Cardiac Magnetic Resonance Imaging in a Small Single Center Study. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2015, 104, 640–647. [Google Scholar] [CrossRef]
- Ramesh, E.; Geraldine, P.; Thomas, P. A. Regulatory Effect of Epigallocatechin Gallate on the Expression of C-Reactive Protein and Other Inflammatory Markers in an Experimental Model of Atherosclerosis. Chem. Biol. Interact. 2010, 183, 125–132. [Google Scholar] [CrossRef]
- Cai, Y.; Kurita-Ochiai, T.; Hashizume, T.; Yamamoto, M. Green Tea Epigallocatechin-3-Gallate Attenuates Porphyromonas Gingivalis-Induced Atherosclerosis. Pathog. Dis. 2013, 67, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Pan, J.; Zhou, X. Amelioration of Lipid Profile and Level of Antioxidant Activities by Epigallocatechin-Gallate in a Rat Model of Atherogenesis. Heart Lung Circ. 2014, 23, 1194–1201. [Google Scholar] [CrossRef]
- Huang, S.-C.; Kao, Y.-H.; Shih, S.-F.; Tsai, M.-C.; Lin, C.-S.; Chen, L. W.; Chuang, Y.-P.; Tsui, P.-F.; Ho, L.-J.; Lai, J.-H.; Chen, S.-J. Epigallocatechin-3-Gallate Exhibits Immunomodulatory Effects in Human Primary T Cells. Biochem. Biophys. Res. Commun. 2021, 550, 70–76. [Google Scholar] [CrossRef]
- Wang, Q.; Zhang, J.; Li, Y.; Shi, H.; Wang, H.; Chen, B.; Wang, F.; Wang, Z.; Yang, Z.; Wang, L. Green Tea Polyphenol Epigallocatechin-3-Gallate Increases Atherosclerotic Plaque Stability in Apolipoprotein E-Deficient Mice Fed a High-Fat Diet. Kardiol. Pol. 2018, 76, 1263–1270. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Chu, Y.; Ren, H.; Pang, X. Antioxidation Function of EGCG by Activating Nrf2/HO-1 Pathway in Mice with Coronary Heart Disease. Contrast Media Mol. Imaging 2022, 2022, 8639139. [Google Scholar] [CrossRef] [PubMed]
- Muhammed, I.; Sankar, S.; Govindaraj, S. Ameliorative Effect of Epigallocatechin Gallate on Cardiac Hypertrophy and Fibrosis in Aged Rats. J. Cardiovasc. Pharmacol. 2018, 71, 65–75. [Google Scholar] [CrossRef]
- Cai, Y.; Yu, S.-S.; Chen, T.-T.; Gao, S.; Geng, B.; Yu, Y.; Ye, J.-T.; Liu, P.-Q. EGCG Inhibits CTGF Expression via Blocking NF-κB Activation in Cardiac Fibroblast. Phytomedicine Int. J. Phytother. Phytopharm. 2013, 20, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Cui, Y.; Wang, Y.; Liu, G. Epigallocatechin Gallate (EGCG) Attenuates Myocardial Hypertrophy and Fibrosis Induced by Transverse Aortic Constriction via Inhibiting the Akt/mTOR Pathway. Pharm. Biol. 2021, 59, 1305–1313. [Google Scholar] [CrossRef]
- Ok, W.-J.; Cho, H.-J.; Kim, H.-H.; Lee, D.-H.; Kang, H.-Y.; Kwon, H.-W.; Rhee, M. H.; Kim, M.; Park, H.-J. Epigallocatechin-3-Gallate Has an Anti-Platelet Effect in a Cyclic AMP-Dependent Manner. J. Atheroscler. Thromb. 2012, 19, 337–348. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-M.; Chang, H.; Wang, B.-W.; Shyu, K.-G. Suppressive Effect of Epigallocatechin-3-O-Gallate on Endoglin Molecular Regulation in Myocardial Fibrosis in Vitro and in Vivo. J. Cell. Mol. Med. 2016, 20, 2045–2055. [Google Scholar] [CrossRef] [PubMed]
- Joo, H. J.; Park, J.-Y.; Hong, S. J.; Kim, K.-A.; Lee, S. H.; Cho, J.-Y.; Park, J. H.; Yu, C. W.; Lim, D.-S. Anti-Platelet Effects of Epigallocatechin-3-Gallate in Addition to the Concomitant Aspirin, Clopidogrel or Ticagrelor Treatment. Korean J. Intern. Med. 2018, 33, 522–531. [Google Scholar] [CrossRef]
- Kim, S.; Lee, H.; Moon, H.; Kim, R.; Kim, M.; Jeong, S.; Kim, H.; Kim, S. H.; Hwang, S. S.; Lee, M. Y.; Kim, J.; Song, B.-W.; Chang, W. Epigallocatechin-3-Gallate Attenuates Myocardial Dysfunction via Inhibition of Endothelial-to-Mesenchymal Transition. Antioxid. Basel Switz. 2023, 12. [Google Scholar] [CrossRef]
- Li, T.; Fang, F.; Yin, H.; Zhang, Z.; Wang, X.; Wang, E.; Yu, H.; Shen, Y.; Wang, G.; He, W.; Liu, X. Epigallocatechin-3-Gallate Inhibits Osteogenic Differentiation of Vascular Smooth Muscle Cells through the Transcription Factor JunB. Acta Biochim. Biophys. Sin. 2024, 57, 901–915. [Google Scholar] [CrossRef]
- Scalise, R. F. M.; De Sarro, R.; Caracciolo, A.; Lauro, R.; Squadrito, F.; Carerj, S.; Bitto, A.; Micari, A.; Bella, G. D.; Costa, F.; Irrera, N. Fibrosis after Myocardial Infarction: An Overview on Cellular Processes, Molecular Pathways, Clinical Evaluation and Prognostic Value. Med. Sci. Basel Switz. 2021, 9, 16. [Google Scholar] [CrossRef]
- Sánchez-Hernández, C. D.; Torres-Alarcón, L. A.; González-Cortés, A.; Peón, A. N. Ischemia/Reperfusion Injury: Pathophysiology, Current Clinical Management, and Potential Preventive Approaches. Mediators Inflamm. 2020, 2020, 8405370. [Google Scholar] [CrossRef]
- Su, X.; Zhou, M.; Li, Y.; An, N.; Yang, F.; Zhang, G.; Xu, L.; Chen, H.; Wu, H.; Xing, Y. Mitochondrial Damage in Myocardial Ischemia/Reperfusion Injury and Application of Natural Plant Products. Oxid. Med. Cell. Longev. 2022, 2022, 8726564. [Google Scholar] [CrossRef]
- Mokra, D.; Joskova, M.; Mokry, J. Therapeutic Effects of Green Tea Polyphenol (‒)-Epigallocatechin-3-Gallate (EGCG) in Relation to Molecular Pathways Controlling Inflammation, Oxidative Stress, and Apoptosis. Int. J. Mol. Sci. 2022, 24, 340. [Google Scholar] [CrossRef]
- Del Re, D. P.; Amgalan, D.; Linkermann, A.; Liu, Q.; Kitsis, R. N. Fundamental Mechanisms of Regulated Cell Death and Implications for Heart Disease. Physiol. Rev. 2019, 99, 1765–1817. [Google Scholar] [CrossRef]
- Zhao, W.-K.; Zhou, Y.; Xu, T.-T.; Wu, Q. Ferroptosis: Opportunities and Challenges in Myocardial Ischemia-Reperfusion Injury. Oxid. Med. Cell. Longev. 2021, 2021, 9929687. [Google Scholar] [CrossRef]
- Liu, S.; Yao, S.; Yang, H.; Liu, S.; Wang, Y. Autophagy: Regulator of Cell Death. Cell Death Dis. 2023, 14, 648. [Google Scholar] [CrossRef]
- Deng, R.-M.; Zhou, J. The Role of PI3K/AKT Signaling Pathway in Myocardial Ischemia-Reperfusion Injury. Int. Immunopharmacol. 2023, 123, 110714. [Google Scholar] [CrossRef] [PubMed]
- Salameh, A.; Dhein, S.; Mewes, M.; Sigusch, S.; Kiefer, P.; Vollroth, M.; Seeger, J.; Dähnert, I. Anti-Oxidative or Anti-Inflammatory Additives Reduce Ischemia/Reperfusions Injury in an Animal Model of Cardiopulmonary Bypass. Saudi J. Biol. Sci. 2020, 27, 18–29. [Google Scholar] [CrossRef]
- Devika, P. T.; Mainzen Prince, P. S. (-)-Epigallocatechin Gallate (EGCG) Prevents Isoprenaline-Induced Cardiac Marker Enzymes and Membrane-Bound ATPases. J. Pharm. Pharmacol. 2008, 60, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Devika, P. T.; Prince, P. S. M. Preventive Effect of (-)Epigallocatechin-Gallate (EGCG) on Lysosomal Enzymes in Heart and Subcellular Fractions in Isoproterenol-Induced Myocardial Infarcted Wistar Rats. Chem. Biol. Interact. 2008, 172, 245–252. [Google Scholar] [CrossRef]
- Devika, P. T.; Stanely Mainzen Prince, P. (-)Epigallocatechin-Gallate (EGCG) Prevents Mitochondrial Damage in Isoproterenol-Induced Cardiac Toxicity in Albino Wistar Rats: A Transmission Electron Microscopic and in Vitro Study. Pharmacol. Res. 2008, 57, 351–357. [Google Scholar] [CrossRef]
- Devika, P. T.; Stanely Mainzen Prince, P. (-)Epigallocatechingallate Protects the Mitochondria against the Deleterious Effects of Lipids, Calcium and Adenosine Triphosphate in Isoproterenol Induced Myocardial Infarcted Male Wistar Rats. J. Appl. Toxicol. JAT 2008, 28, 938–944. [Google Scholar] [CrossRef]
- Devika, P. T.; Stanely Mainzen Prince, P. Protective Effect of (-)-Epigallocatechin-Gallate (EGCG) on Lipid Peroxide Metabolism in Isoproterenol Induced Myocardial Infarction in Male Wistar Rats: A Histopathological Study. Biomed. Pharmacother. Biomedecine Pharmacother. 2008, 62, 701–708. [Google Scholar] [CrossRef]
- Devika, P. T.; Stanely Mainzen Prince, P. Preventive Effect of (-)Epigallocatechin Gallate on Lipids, Lipoproteins, and Enzymes of Lipid Metabolism in Isoproterenol-Induced Myocardial Infarction in Rats. J. Biochem. Mol. Toxicol. 2009, 23, 387–393. [Google Scholar] [CrossRef]
- Kim, S. J.; Li, M.; Jeong, C. W.; Bae, H. B.; Kwak, S. H.; Lee, S. H.; Lee, H. J.; Heo, B. H.; Yook, K. B.; Yoo, K. Y. Epigallocatechin-3-Gallate, a Green Tea Catechin, Protects the Heart against Regional Ischemia-Reperfusion Injuries through Activation of RISK Survival Pathways in Rats. Arch. Pharm. Res. 2014, 37, 1079–1085. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.-Y.; Zhang, H.-W.; Gu, J.; Xu, F.; Liang, H.-M.; Fan, K.-J.; Shen, J.-Y.; Xiao, Z.-H.; Zhang, E.-Y.; Hu, J. Mitochondrial DNA--induced Inflammatory Damage Contributes to Myocardial Ischemia Reperfusion Injury in Rats: Cardioprotective Role of Epigallocatechin. Mol. Med. Rep. 2017, 16, 7569–7576. [Google Scholar] [CrossRef]
- Zhang, C.; Liang, R.; Gan, X.; Yang, X.; Chen, L.; Jian, J. MicroRNA-384-5p/Beclin-1 As Potential Indicators For Epigallocatechin Gallate Against Cardiomyocytes Ischemia Reperfusion Injury By Inhibiting Autophagy Via PI3K/Akt Pathway. Drug Des. Devel. Ther. 2019, 13, 3607–3623. [Google Scholar] [CrossRef] [PubMed]
- Zeng, M.; Wei, X.; He, Y.-L.; Chen, J.-X.; Lin, W.-T.; Xu, W.-X. EGCG Protects against Myocardial I/RI by Regulating lncRNA Gm4419-Mediated Epigenetic Silencing of the DUSP5/ERK1/2 Axis. Toxicol. Appl. Pharmacol. 2021, 433, 115782. [Google Scholar] [CrossRef] [PubMed]
- Nan, J.; Nan, C.; Ye, J.; Qian, L.; Geng, Y.; Xing, D.; Rahman, M. S. U.; Huang, M. EGCG Protects Cardiomyocytes against Hypoxia-Reperfusion Injury through Inhibition of OMA1 Activation. J. Cell Sci. 2019, 132, jcs220871. [Google Scholar] [CrossRef]
- Zhang, C.; Gan, X.; Liang, R.; Jian, J. Exosomes Derived From Epigallocatechin Gallate-Treated Cardiomyocytes Attenuated Acute Myocardial Infarction by Modulating MicroRNA-30a. Front. Pharmacol. 2020, 11, 126. [Google Scholar] [CrossRef]
- Yu, Q.; Zhang, N.; Gan, X.; Chen, L.; Wang, R.; Liang, R.; Jian, J. EGCG Attenuated Acute Myocardial Infarction by Inhibiting Ferroptosis via miR-450b-5p/ACSL4 Axis. Phytomedicine Int. J. Phytother. Phytopharm. 2023, 119, 154999. [Google Scholar] [CrossRef]
- Wu, Y.; Xia, Z.-Y.; Zhao, B.; Leng, Y.; Dou, J.; Meng, Q.-T.; Lei, S.-Q.; Chen, Z.-Z.; Zhu, J. (-)-Epigallocatechin-3-Gallate Attenuates Myocardial Injury Induced by Ischemia/Reperfusion in Diabetic Rats and in H9c2 Cells under Hyperglycemic Conditions. Int. J. Mol. Med. 2017, 40, 389–399. [Google Scholar] [CrossRef]
- Liu, P.; Huang, J.; Mei, W.; Zeng, X.; Wang, C.; Wen, C.; Xu, J. Epigallocatechin-3-Gallate Protects Cardiomyocytes from Hypoxia-Reoxygenation Damage via Raising Autophagy Related 4C Expression. Bioengineered 2021, 12, 9496–9506. [Google Scholar] [CrossRef]
- Qin, C.; Wang, T.; Qian, N.; Liu, J.; Xi, R.; Zou, Q.; Liu, H.; Niu, X. Epigallocatechin Gallate Prevents Cardiomyocytes from Pyroptosis through lncRNA MEG3/TAF15/AIM2 Axis in Myocardial Infarction. Chin. Med. 2023, 18, 160. [Google Scholar] [CrossRef]
- Hu, T.; Hu, F.-J.; Huang, H.; Zhang, Z.-Y.; Qiao, Y.-M.; Huang, W.-X.; Wang, Y.-C.; Tang, X.-Y.; Lai, S.-Q. Epigallocatechin-3-Gallate Confers Protection against Myocardial Ischemia/Reperfusion Injury by Inhibiting Ferroptosis, Apoptosis, and Autophagy via Modulation of 14-3-3η. Biomed. Pharmacother. Biomedecine Pharmacother. 2024, 174, 116542. [Google Scholar] [CrossRef]
- Othman, A. I.; Elkomy, M. M.; El-Missiry, M. A.; Dardor, M. Epigallocatechin-3-Gallate Prevents Cardiac Apoptosis by Modulating the Intrinsic Apoptotic Pathway in Isoproterenol-Induced Myocardial Infarction. Eur. J. Pharmacol. 2017, 794, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Nan, C.; Chen, Y.; Tian, J.; Jean-Charles, P.-Y.; Getfield, C.; Wang, X.; Huang, X. Calcium Desensitizer Catechin Reverses Diastolic Dysfunction in Mice with Restrictive Cardiomyopathy. Arch. Biochem. Biophys. 2015, 573, 69–76. [Google Scholar] [CrossRef]
- Pan, B.; Quan, J.; Liu, L.; Xu, Z.; Zhu, J.; Huang, X.; Tian, J. Epigallocatechin Gallate Reverses cTnI-Low Expression-Induced Age-Related Heart Diastolic Dysfunction through Histone Acetylation Modification. J. Cell. Mol. Med. 2017, 21, 2481–2490. [Google Scholar] [CrossRef]
- Oyama, J.-I.; Shiraki, A.; Nishikido, T.; Maeda, T.; Komoda, H.; Shimizu, T.; Makino, N.; Node, K. EGCG, a Green Tea Catechin, Attenuates the Progression of Heart Failure Induced by the Heart/Muscle-Specific Deletion of MnSOD in Mice. J. Cardiol. 2017, 69, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Potenza, M. A.; Marasciulo, F. L.; Tarquinio, M.; Tiravanti, E.; Colantuono, G.; Federici, A.; Kim, J.-A.; Quon, M. J.; Montagnani, M. EGCG, a Green Tea Polyphenol, Improves Endothelial Function and Insulin Sensitivity, Reduces Blood Pressure, and Protects against Myocardial I/R Injury in SHR. Am. J. Physiol. Endocrinol. Metab. 2007, 292, E1378–1387. [Google Scholar] [CrossRef]
- Vilella, R.; Sgarbi, G.; Naponelli, V.; Savi, M.; Bocchi, L.; Liuzzi, F.; Righetti, R.; Quaini, F.; Frati, C.; Bettuzzi, S.; Solaini, G.; Stilli, D.; Rizzi, F.; Baracca, A. Effects of Standardized Green Tea Extract and Its Main Component, EGCG, on Mitochondrial Function and Contractile Performance of Healthy Rat Cardiomyocytes. Nutrients 2020, 12, 2949. [Google Scholar] [CrossRef] [PubMed]
- Jia, Q.; Yang, R.; Mehmood, S.; Li, Y. Epigallocatechin-3-Gallate Attenuates Myocardial Fibrosis in Diabetic Rats by Activating Autophagy. Exp. Biol. Med. Maywood NJ 2022, 247, 1591–1600. [Google Scholar] [CrossRef]
- Liu, L.; Zhao, W.; Liu, J.; Gan, Y.; Liu, L.; Tian, J. Epigallocatechin-3 Gallate Prevents Pressure Overload-Induced Heart Failure by up-Regulating SERCA2a via Histone Acetylation Modification in Mice. PloS One 2018, 13, e0205123. [Google Scholar] [CrossRef]
- Zhang, Q.; Hu, L.; Chen, L.; Li, H.; Wu, J.; Liu, W.; Zhang, M.; Yan, G. (-)-Epigallocatechin-3-Gallate, the Major Green Tea Catechin, Regulates the Desensitization of Β1 Adrenoceptor via GRK2 in Experimental Heart Failure. Inflammopharmacology 2018, 26, 1081–1091. [Google Scholar] [CrossRef]
- Han, X.; Peng, C.; Huang, L.; Luo, X.; Mao, Q.; Wu, S.; Zhang, H. EGCG Prevents Pressure Overload--induced Myocardial Remodeling by Downregulating Overexpression of HDAC5 in Mice. Int. J. Mol. Med. 2022, 49, 11. [Google Scholar] [CrossRef]
- Mou, Q.; Jia, Z.; Luo, M.; Liu, L.; Huang, X.; Quan, J.; Tian, J. Epigallocatechin-3-Gallate Exerts Cardioprotective Effects Related to Energy Metabolism in Pressure Overload-Induced Cardiac Dysfunction. Arch. Biochem. Biophys. 2022, 723, 109217. [Google Scholar] [CrossRef]
- Xuan, F.; Jian, J. Epigallocatechin Gallate Exerts Protective Effects against Myocardial Ischemia/Reperfusion Injury through the PI3K/Akt Pathway-Mediated Inhibition of Apoptosis and the Restoration of the Autophagic Flux. Int. J. Mol. Med. 2016, 38, 328–336. [Google Scholar] [CrossRef]
- Zhang, C.; Liao, P.; Liang, R.; Zheng, X.; Jian, J. Epigallocatechin Gallate Prevents Mitochondrial Impairment and Cell Apoptosis by Regulating miR-30a/P53 Axis. Phytomedicine Int. J. Phytother. Phytopharm. 2019, 61, 152845. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, M.; Hellige, N.; Rieder, P.; Kinkel, H.-T.; Trimpert, C.; Staudt, A.; Felix, S. B.; Baumann, G.; Stangl, K.; Stangl, V. Positive Inotropic Effects of Epigallocatechin-3-Gallate (EGCG) Involve Activation of Na+/H+ and Na+/Ca2+ Exchangers. Eur. J. Heart Fail. 2008, 10, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Salameh, A.; Schuster, R.; Dähnert, I.; Seeger, J.; Dhein, S. Epigallocatechin Gallate Reduces Ischemia/Reperfusion Injury in Isolated Perfused Rabbit Hearts. Int. J. Mol. Sci. 2018, 19, 628. [Google Scholar] [CrossRef] [PubMed]
- Hirai, M.; Hotta, Y.; Ishikawa, N.; Wakida, Y.; Fukuzawa, Y.; Isobe, F.; Nakano, A.; Chiba, T.; Kawamura, N. Protective Effects of EGCg or GCg, a Green Tea Catechin Epimer, against Postischemic Myocardial Dysfunction in Guinea-Pig Hearts. Life Sci. 2007, 80, 1020–1032. [Google Scholar] [CrossRef]
- Song, D.-K.; Jang, Y.; Kim, J. H.; Chun, K.-J.; Lee, D.; Xu, Z. Polyphenol (-)-Epigallocatechin Gallate during Ischemia Limits Infarct Size via Mitochondrial K(ATP) Channel Activation in Isolated Rat Hearts. J. Korean Med. Sci. 2010, 25, 380–386. [Google Scholar] [CrossRef]
- Kim, C. J.; Kim, J. M.; Lee, S. R.; Jang, Y. H.; Kim, J. H.; Chun, K. J. Polyphenol (-)-Epigallocatechin Gallate Targeting Myocardial Reperfusion Limits Infarct Size and Improves Cardiac Function. Korean J. Anesthesiol. 2010, 58, 169–175. [Google Scholar] [CrossRef]
- Piao, C. S.; Kim, D.-S.; Ha, K.-C.; Kim, H.-R.; Chae, H.-J.; Chae, S.-W. The Protective Effect of Epigallocatechin-3 Gallate on Ischemia/Reperfusion Injury in Isolated Rat Hearts: An Ex Vivo Approach. Korean J. Physiol. Pharmacol. Off. J. Korean Physiol. Soc. Korean Soc. Pharmacol. 2011, 15, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Feng, W.; Hwang, H. S.; Kryshtal, D. O.; Yang, T.; Padilla, I. T.; Tiwary, A. K.; Puschner, B.; Pessah, I. N.; Knollmann, B. C. Coordinated Regulation of Murine Cardiomyocyte Contractility by Nanomolar (-)-Epigallocatechin-3-Gallate, the Major Green Tea Catechin. Mol. Pharmacol. 2012, 82, 993–1000. [Google Scholar] [CrossRef] [PubMed]
- Tadano, N.; Du, C.-K.; Yumoto, F.; Morimoto, S.; Ohta, M.; Xie, M.-F.; Nagata, K.; Zhan, D.-Y.; Lu, Q.-W.; Miwa, Y.; Takahashi-Yanaga, F.; Tanokura, M.; Ohtsuki, I.; Sasaguri, T. Biological Actions of Green Tea Catechins on Cardiac Troponin C. Br. J. Pharmacol. 2010, 161, 1034–1043. [Google Scholar] [CrossRef]
- Messer, A. E.; Bayliss, C. R.; El-Mezgueldi, M.; Redwood, C. S.; Ward, D. G.; Leung, M.-C.; Papadaki, M.; Dos Remedios, C.; Marston, S. B. Mutations in Troponin T Associated with Hypertrophic Cardiomyopathy Increase Ca(2+)-Sensitivity and Suppress the Modulation of Ca(2+)-Sensitivity by Troponin I Phosphorylation. Arch. Biochem. Biophys. 2016, 601, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Hassoun, R.; Budde, H.; Mannherz, H. G.; Lódi, M.; Fujita-Becker, S.; Laser, K. T.; Gärtner, A.; Klingel, K.; Möhner, D.; Stehle, R.; Sultana, I.; Schaaf, T.; Majchrzak, M.; Krause, V.; Herrmann, C.; Nowaczyk, M. M.; Mügge, A.; Pfitzer, G.; Schröder, R. R.; Hamdani, N.; Milting, H.; Jaquet, K.; Cimiotti, D. De Novo Missense Mutations in TNNC1 and TNNI3 Causing Severe Infantile Cardiomyopathy Affect Myofilament Structure and Function and Are Modulated by Troponin Targeting Agents. Int. J. Mol. Sci. 2021, 22, 9625. [Google Scholar] [CrossRef]
- Isbrucker, R. A.; Bausch, J.; Edwards, J. A.; Wolz, E. Safety Studies on Epigallocatechin Gallate (EGCG) Preparations. Part 1: Genotoxicity. Food Chem. Toxicol. Int. J. Publ. Br. Ind. Biol. Res. Assoc. 2006, 44, 626–635. [Google Scholar] [CrossRef]
- Isbrucker, R. A.; Edwards, J. A.; Wolz, E.; Davidovich, A.; Bausch, J. Safety Studies on Epigallocatechin Gallate (EGCG) Preparations. Part 2: Dermal, Acute and Short-Term Toxicity Studies. Food Chem. Toxicol. Int. J. Publ. Br. Ind. Biol. Res. Assoc. 2006, 44, 636–650. [Google Scholar] [CrossRef] [PubMed]
- Isbrucker, R. A.; Edwards, J. A.; Wolz, E.; Davidovich, A.; Bausch, J. Safety Studies on Epigallocatechin Gallate (EGCG) Preparations. Part 3: Teratogenicity and Reproductive Toxicity Studies in Rats. Food Chem. Toxicol. Int. J. Publ. Br. Ind. Biol. Res. Assoc. 2006, 44, 651–661. [Google Scholar] [CrossRef]
- Kim, E.-Y.; Ham, S.-K.; Shigenaga, M. K.; Han, O. Bioactive Dietary Polyphenolic Compounds Reduce Nonheme Iron Transport across Human Intestinal Cell Monolayers. J. Nutr. 2008, 138, 1647–1651. [Google Scholar] [CrossRef]
- Duda-Chodak, A.; Tarko, T. Possible Side Effects of Polyphenols and Their Interactions with Medicines. Mol. Basel Switz. 2023, 28, 2536. [Google Scholar] [CrossRef]
- Kiss, T.; Timár, Z.; Szabó, A.; Lukács, A.; Velky, V.; Oszlánczi, G.; Horváth, E.; Takács, I.; Zupkó, I.; Csupor, D. Effect of Green Tea on the Gastrointestinal Absorption of Amoxicillin in Rats. BMC Pharmacol. Toxicol. 2019, 20, 54. [Google Scholar] [CrossRef] [PubMed]
- Yamanaka, N.; Oda, O.; Nagao, S. Green Tea Catechins Such as (-)-Epicatechin and (-)-Epigallocatechin Accelerate Cu2+-Induced Low Density Lipoprotein Oxidation in Propagation Phase. FEBS Lett. 1997, 401, (2–3). [Google Scholar] [CrossRef] [PubMed]
- Caro, A. A.; Davis, A.; Fobare, S.; Horan, N.; Ryan, C.; Schwab, C. Antioxidant and Pro-Oxidant Mechanisms of (+) Catechin in Microsomal CYP2E1-Dependent Oxidative Stress. Toxicol. In Vitro 2019, 54, 1–9. [Google Scholar] [CrossRef]
- Galati, G.; Lin, A.; Sultan, A. M.; O’Brien, P. J. Cellular and in Vivo Hepatotoxicity Caused by Green Tea Phenolic Acids and Catechins. Free Radic. Biol. Med. 2006, 40, 570–580. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; He, S.-Q.; Hong, H.-Q.; Cai, Y.-P.; Zhao, L.; Zhang, M. High Doses of (-)-Epigallocatechin-3-Gallate from Green Tea Induces Cardiac Fibrosis in Mice. Biotechnol. Lett. 2015, 37, 2371–2377. [Google Scholar] [CrossRef]
- Rasheed, N. O. A.; Ahmed, L. A.; Abdallah, D. M.; El-Sayeh, B. M. Paradoxical Cardiotoxicity of Intraperitoneally-Injected Epigallocatechin Gallate Preparation in Diabetic Mice. Sci. Rep. 2018, 8, 7880. [Google Scholar] [CrossRef]
- Bao, L.; Lu, F.; Chen, H.; Min, Q.; Chen, X.; Song, Y.; Zhao, B.; Bu, H.; Sun, H. High Concentration of Epigallocatechin-3-Gallate Increased the Incidences of Arrhythmia and Diastolic Dysfunction via Β2-Adrenoceptor. J. Food Sci. 2015, 80, T659–663. [Google Scholar] [CrossRef]
- Bedrood, Z.; Rameshrad, M.; Hosseinzadeh, H. Toxicological Effects of Camellia Sinensis (Green Tea): A Review. Phytother. Res. PTR 2018, 32, 1163–1180. [Google Scholar] [CrossRef]
- Hu, J.; Webster, D.; Cao, J.; Shao, A. The Safety of Green Tea and Green Tea Extract Consumption in Adults—Results of a Systematic Review. Regul. Toxicol. Pharmacol. RTP 2018, 95, 412–433. [Google Scholar] [CrossRef]
- Mazzanti, G.; Menniti-Ippolito, F.; Moro, P. A.; Cassetti, F.; Raschetti, R.; Santuccio, C.; Mastrangelo, S. Hepatotoxicity from Green Tea: A Review of the Literature and Two Unpublished Cases. Eur. J. Clin. Pharmacol. 2009, 65, 331–341. [Google Scholar] [CrossRef]
- Alemdaroglu, N. C.; Dietz, U.; Wolffram, S.; Spahn-Langguth, H.; Langguth, P. Influence of Green and Black Tea on Folic Acid Pharmacokinetics in Healthy Volunteers: Potential Risk of Diminished Folic Acid Bioavailability. Biopharm. Drug Dispos. 2008, 29, 335–348. [Google Scholar] [CrossRef]
- Chow, H.-H. S.; Cai, Y.; Hakim, I. A.; Crowell, J. A.; Shahi, F.; Brooks, C. A.; Dorr, R. T.; Hara, Y.; Alberts, D. S. Pharmacokinetics and Safety of Green Tea Polyphenols after Multiple-Dose Administration of Epigallocatechin Gallate and Polyphenon E in Healthy Individuals. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2003, 9, 3312–3319. [Google Scholar]
- EFSA Panel on Food Additives and Nutrient Sources added to Food (ANS); Younes, M.; Aggett, P.; Aguilar, F.; Crebelli, R.; Dusemund, B.; Filipič, M.; Frutos, M. J.; Galtier, P.; Gundert-Remy, U.; Kuhnle, G. G.; Lambré, C.; Leblanc, J.-C.; Lillegaard, I. T.; Moldeus, P.; Mortensen, A.; Oskarsson, A.; Stankovic, I.; Waalkens-Berendsen, I.; Woutersen, R. A.; Wright, M.; Di Domenico, A.; Fairweather-Tait, S.; McArdle, H. J.; Smeraldi, C.; Gott, D. Guidance on Safety Evaluation of Sources of Nutrients and Bioavailability of Nutrient from the Sources (Revision 1). EFSA J. Eur. Food Saf. Auth. 2021, 19, e06552. [Google Scholar] [CrossRef]
- Lu, J.-H.; He, J.-R.; Shen, S.-Y.; Wei, X.-L.; Chen, N.-N.; Yuan, M.-Y.; Qiu, L.; Li, W.-D.; Chen, Q.-Z.; Hu, C.-Y.; Xia, H.-M.; Bartington, S.; Cheng, K. K.; Lam, K. B. H.; Qiu, X.; Born in Guangzhou Cohort Study Group. Does Tea Consumption during Early Pregnancy Have an Adverse Effect on Birth Outcomes? Birth Berkeley Calif 2017, 44, 281–289. [Google Scholar] [CrossRef]
- Xie, J.; Jia, L.; Xie, P.; Yin, X.; Zhu, W.; Zhao, H.; Wang, X.; Meng, X.; Xing, L.; Zhao, H.; Li, X. Efficacy and Safety of Epigallocatechin-3-Gallate in Treatment Acute Severe Dermatitis in Patients with Cancer Receiving Radiotherapy: A Phase I Clinical Trial. Sci. Rep. 2023, 13, 13865. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhu, Q.; Chen, Z.; Wang, X.; Ma, B.; Wang, Y.; Xiao, Y.; Luo, R.; Zhang, W.; Wang, Y.; Fu, G. Self-Adaptive Covalent Coating for Vascular Stents: Coordinated Coagulation-Inflammation Regulation to Support Re-Endothelialization for Atherosclerosis Control. Biomaterials 2025, 325, 123600. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.; Jiang, C.; Song, J.; Bi, Y.; Chen, W.; Lu, C.; Chen, M.; Lv, L.; Yu, R.; Zou, J.; Zhao, Z.; Chen, X.; Ji, J. Microenvironment Responsive Nanoplatform for Targeted Removal of Cholesterol and Reshaping Inflammatory Microenvironment in Atherosclerotic Plaques. J. Control. Release Off. J. Control. Release Soc. 2025, 385, 114000. [Google Scholar] [CrossRef]
- Liu, T.; Hao, Y.; Zhang, Z.; Zhou, H.; Peng, S.; Zhang, D.; Li, K.; Chen, Y.; Chen, M. Advanced Cardiac Patches for the Treatment of Myocardial Infarction. Circulation 2024, 149, 2002–2020. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.; Wang, H.; Guo, L.; Cui, Y.; Zou, C.; Hu, J.; Zhang, H.; Yang, G.; Zhou, W. Multifunctional Nanomedicine for Targeted Atherosclerosis Therapy: Activating Plaque Clearance Cascade and Suppressing Inflammation. ACS Nano 2025, 19, 3339–3361. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



