
Submitted:
20 October 2025
Posted:
21 October 2025
You are already at the latest version
Abstract
Background: This study aimed to (a) determine how frequently chiropractors are using postural assessment when treating patients with back or neck pain, (b) determine the rationale for the use of postural assessment by chiropractors, (c) examine the assess-ment methods employed, (d) explore which specific aspects of posture are assessed and (e) determine the types of back and neck conditions being treated. Methods: An 11-item online questionnaire was developed. A link to this survey was distributed using Sur-veyMonkey to the entire membership of the Royal College of Chiropractors. Results: There were 272 respondents to the survey. Of the respondents, 79% ‘almost always’ used postural assessment when treating patients with back or neck pain. Respondents reported using postural assessment to help determine whether a patient was making progress (61.8%), provide an outcome measure (57.1%) and help inform the diagnosis (89.2%) and treatment plan (81.8%); almost all respondents (98.1%) reported carrying out a postural assessment visually, with no aids. Most respondents reported assessing their patient posteriorly, anteriorly and from both left and right sides, observing 44 specific anatomical items. The conditions treated included sacroiliac pain (96.7%), stiff neck (95.6%), non-specific low-back pain (92.6%), lumbar disc herniation (91.5%), cer-vical arthritis (89.7%), lumbar strain (87.1%), lumbar arthritis (86.4%), thoracic pain (86.4%), neck strain (84.9%) and whiplash (79.8%). Conclusions: The findings suggest that the unaided visual assessment of posture using a large range of anatomical points is used by UK chiropractors for the purposes of aiding diagnosis and treatment of patients with back and neck pathologies.
Keywords:
postural assessment
; chiropractors
; practicing
1. Introduction
The assessment of posture is a common skill set within chiropractic care [1] and is considered to be an appropriate method of clinical examination [2]. Instructional texts intended for use by manual therapists describe the traditional method of using unaided visual assessment of posture [3,4,5,6], but due to a paucity in the literature regarding many aspects of chiropractic care [7] the frequency of postural assessment used by chiropractors, the reasons as well as the methods, is largely unknown.
Postural assessment aligns with the biomechanical model of dysfunction that has historically defined the profession [8], but there is scant information in the literature about the frequency with which this form of assessment is used by chiropractors or other manual therapists. Studies by Enwemeka et al. (1986) [9], Fedorak et al. (2003) [10], Silva, Punt and Johnson (2009) [11] and Silva et al. (2009) [12] indicate that postural assessment is often or routinely used by physiotherapists and there is some indication that this is the case within the profession of chiropractic [13,14]. For example, in an early survey of 120 physiotherapists in New York, New Jersey and Puerto Rico, 72% (n = 33) of respondents said they ‘frequently’ used postural correction when treating patients with neck pain [9]. In another study [10] the 28 clinicians who were recruited—six chiropractors, seven physical therapists, six physiatrists, four rheumatologists and five orthopaedic surgeons—all reported assessing spinal posture ‘regularly’. Although Silva et al. (2009) [12] was unable to find any empirical evidence on the procedures for posture assessment used in practice by physiotherapists, in a focus group study of 21 physiotherapists practicing in Portugal, one question asked, ‘do you assess head posture for patients with neck pain in your clinical practice?’ to which all 21 physiotherapists reported they ‘routinely’ assessed head posture for patients with neck pain. Similar findings were revealed in surveys of chiropractors. In a survey in which 80 Belgian chiropractors returned questionnaires, 72 of them reported ‘often to always’ using visual posture analysis during practice [13]. Further, in a survey of chiropractors in the Canadian province of Saskatchewan, of the 62 respondents, 79% ‘always’ documented their visual observation of posture [14].
Unfortunately, a drawback to all of these studies [9,10,13,14] is that the terms ‘often’, ‘regularly’, ‘routinely’ and ‘often to always’ were not quantified, making it difficult to quantify the frequency of use of postural assessment by either physiotherapists or chiropractors. However, in a survey of Canadian chiropractors the terms for the frequency of use of postural assessment were quantified. Of the 500 respondents, 34.4% said they used postural assessment ‘always’ (76-100% of the time), 28.2% said they ‘usually’ used it (51-75% of the time) and 18.6% said they ‘often’ used it (26-50% of the time) [15]. Prior to the survey reported here it was unknown with what frequency chiropractors in the UK are using postural assessment. It is possible, however, that the frequency with which chiropractors and other manual therapists perform postural assessment has increased in recent years as a result of public information websites and articles in the press promoting a link between posture and pain. The consequence of such information may induce people to wonder whether they have poor posture, whether their posture might be the cause of their symptoms, and they may come to expect an assessment of their posture when seeking treatment. For example, the ‘Bone and Joint Decade’ is a global alliance of over one thousand patient, professional and scientific organisations with a mandate to develop evidence-based strategies aimed at preventing and treating musculoskeletal health. Their patient education pages state that ‘neck pain may be due to… poor posture’ [16] and that ‘overuse of the musculoskeletal system, including poor posture and position, can often contribute to osteoarthritis and back pain’ [16]. The WHO advised that inadequate posture is a risk factor for musculoskeletal conditions [17] and the International Organization for standardization warn that sustained inadequate working postures may result in pain, fatigue and disorders of the muscular system [18]. Information about common postural mistakes and how to correct these is available on the NHS website [19]. Newspaper articles warning against ‘text neck’ and ‘hunchback’ [20,21] may lead people to feel fearful that their posture might adversely affect their health. It is therefore possible that chiropractors are using postural assessment frequently not only because it aligns with the biomechanical model of dysfunction inherent to their profession, but because patients have come to expect it.
An assessment of posture is carried out to determine whether a patient’s symptoms are posture-related and could be the rationale for the use of postural assessment by chiropractors. Assessment of the static posture of athletes is also thought to be important because poor posture may be detrimental to movement efficiency [22]. However, there are few studies in which the rationale for the use of postural assessment by chiropractors is examined. The 72 respondents in the study by Ailliet, Rubinstein, and de Vet (2010) [13] and 71.5% (n = 339) of survey respondents in the study by Puhl, Reinhart and Injeyan (2015) [15] report using posture analysis as a diagnostic procedure. In a survey of 2448 UK chiropractors, which looked into preventative and promotional care offered to patients, there were 509 respondents [23]. Of these respondents, 97.1% (n = 494) reported that they considered it reasonable to discuss improvement in posture with their patients, 96.3% (n = 490) gave advice about poor posture, and 80.4% (n = 409) set goals and re-evaluated progress with regards to poor posture.
The method of postural assessment used by chiropractors and other manual therapists is largely unknown. Although small in scale, a selection of studies indicates that postural assessment by physiotherapists and chiropractors is performed visually, without the aid of measurement devices. Ninety-three percent (n = 26) of the respondents in the previously mentioned study by Fedorak et al. (2003) [10] stated that visual postural assessment was the tool they used most frequently to assess spinal posture and in a postal survey of members of the Portuguese physiotherapists Association, Silva, Punt and Johnson (2009) [11] reported that 100% (n = 275) of respondents used ‘observation’ when assessing neck pain patients. In a study to determine the clinical acceptance of a low-cost portable system for postural assessment, Van Schaik, Bettany-Saltikov and Warren (2002) [24] surveyed 49 physiotherapists based in Teesside in the north-east of England and reported that visual, unaided postural assessment was used by 84% (n = 41) of the physiotherapists. Of the small number of chiropractors (n = 62) who responded to Hinton’s survey, 79% (n = 48) reported using visual assessment of posture [14] and this was the method of assessment reported by 72% of therapists (n = 80) in the study by Ailliet, Rubinstein, and de Vet (2010) [13].
Posture may be assessed from the front, back or side views, and different elements of posture such as the relationship between different body parts—may be given specific consideration. Whilst little is known about the specific method of postural assessment used by chiropractors, it seems reasonable to assume that they are using the method taught to them during their undergraduate training. It is not known how postural assessment is taught to UK chiropractors as this is generally left to individual training establishments to define, although the General Chiropractic Council state that chiropractors are taught to assess posture visually without the use of measurement devices [25]. Harrison et al. (2000) [26] state that all chiropractic, osteopathic, physical therapy and medical colleges teach a plumb line analysis, concluding, ‘we find it paramount to measure the patient’s structure on the outside (posture) and use radiography for the segmental alignments on the inside (spine)’. The General Survey and Postural Analysis document [27] from the AECC University College (formerly the Anglo European College of Chiropractic) which is used when teaching undergraduate chiropractic students describes the traditional method of assessing posture, that is, visually, observing the patient from the front, back and side views and documenting observations using a body chart. The AECC University College training document also reveals use of the subjective nomenclature familiar to manual therapists (such as ‘round shoulders’, ‘elevation of shoulders’ and ‘forward-drawn head’) which permeates the literature relating to postural assessment. Despite the unaided visual assessment of posture lacking validity [28] or reliability [10], it seems probable that chiropractors use this method of posture assessment as has been the tradition amongst the professions of physiotherapy and osteopathy. In summary, as the frequency, rationale and methods of postural assessment used by UK chiropractors is largely unknown, more understanding in this area could help to inform a more evidence-based approach to practice. To the authors’ knowledge this is the first survey to ask in detail about the frequency and specific methods of postural assessment used by chiropractors in the UK.
2. Materials and Methods
2.1. Participants
The entire membership of the Royal College of Chiropractors (RCC) was invited to take part (N = 1206). The rationale for selecting RCC members was that they have a large number of members who could easily be accessed.
2.2. Measures and Instrumentation
Questionnaire Development and Pre-Testing
A new 11-question multiple-choice, cross-sectional on-line survey was developed. Following a pilot study of the questionnaire by clinicians and the supervisory team (n = 10), minor changes were made. Therefore, to the answer options for Question One, percentages were awarded matching those used by Puhl, Reinhart and Injeyan (2015). The answer options were quantified as follows: ‘almost always’ (76-100% of the time); ‘frequently’ (51-75% of the time); ‘some of the time’ (26-50% of the time); ‘rarely’ (1-25% of the time). It was hoped that by providing percentages to quantify the frequency of use of postural assessment this would clarify what was meant by ‘almost always’, ‘frequently, ‘some of the time’ and ‘rarely’ and make it easier for chiropractors to answer that question. The second reason for adding these percentages was that it would make it possible to compare the results with those of Puhl, Reinhart and Injeyan. The web survey design included a series of short, set pages rather than scrolling pages, questions were made mandatory and a skip function was implemented, as advocated by Peytchev et al. (2006). Specifically, questions were mandatory with the exception of those that were not relevant to the participant who was automatically ‘skipped’ to the next mandatory question. For example, if a participant answered that they ‘never’ use postural assessment, all questions were automatically ‘skipped’ until the remaining two, asking the participant whether they wanted to say anything else about postural assessment; they were then asked to select their profession. The rationale for these changes was twofold: Peytchev et al. (2006) found set pages to be quicker to complete than scrolling pages and that the use of automated skip logic was important for removing errors of both omission and commission. An error of commission is a mistake that consists of doing something wrong (Cambridge University Press, 2019). In the survey of chiropractors, an example of an error of commission would be accidentally selecting that posture is observed from the front view, when it is not. An error of omission is not doing something that should have been done (Cambridge University Press, 2019). For example, in the survey of chiropractors, not selecting that posture is observed from the front view, when it is.
Questionnaire
Postural assessment items listed in the survey were constructed using the limited literature available, the AECC University College training document (Newell, 2016a), two texts on postural assessment aimed at manual therapists (Kendall, Kendall and Boynton, 1952) and the clinical experience of the author. This survey focused on the chiropractic assessment of a patient during their first appointment, as opposed to assessment as part of ongoing treatment. Questions asked about the frequency (objective 1) and rationale (objective 2) for the use of postural assessment, methods of use (objective 3), which specific aspects of posture were assessed (objective 4) and the sorts of pathology chiropractors routinely came across in practice (objective 5). One question was open-ended and asked whether the participant wished to add any further comments. The final question asked the participant to select the professional category (chiropractor, osteopath, physiotherapist, sports therapist, other) with which they identified, as the survey was later intended for use with other manual therapists. Questions 2, 3, 4, 6, 7, 8, 9 and 10 of the survey contained free-text boxes, but there were no free-text options for questions 1, 5 and 11 (Table 1).
Data Collection Procedure
A participant’s information sheet was created and ethical approval sought from the AECC University College in February 2016. The AECC University College responded that the survey fell beneath their criteria for risk, and ethical approval was granted. During April and May 2016, a link to the survey was disseminated via Survey Monkey to 1206 members of the Royal College of Chiropractors (1151 based in the UK and 55 based overseas).
2.3. Data Analysis
For questions which generated numerical data, descriptive analysis of responses to each answer were converted to percentages. In particular, descriptive analysis was performed for questions relating to the frequency of use of postural assessment, rationale for use of postural assessment, method used to assess posture, specific postural assessment indices observed, and back and neck pathologies encountered.
For free-text questions, content analysis was used: a coding framework was developed to determine whether any themes emerged from written responses. In order to ensure consistency of coding by raters, a Manual for Raters was created. This manual consisted of a set of coding rules as advocated by Zhang and Wildemuth (2009). Repetition of words or phrases is one of the easiest methods to identify themes (Ryan and Bernard, 2003) and this method was used to develop themes. The author and another manual therapist cut and sorted the free-text, identifying important expressions, and arranged these in thematic piles. For each question, emergent themes were each assigned an alphabetic code. In the example of question 2, there were three themes labelled A, B and C. Coding of free-text responses was then performed by two independent reviewers. That is, each reviewer assigned responses to questions to one or more of the codes. Discrepancies were resolved by a third reviewer.
3. Results
3.1. Quantitative Analysis
There were 272 respondents to the survey, constituting a response rate of 22%.
3.1.1. The Frequency of Use of Postural Assessment
Almost 80% of chiropractic respondents reported almost always (76%-100% of the time) using postural assessment with a new patient who attends for back or neck pain (Figure 1).
3.1.2. Rationale for the Use of Postural Assessment
Of the 259 respondents who said they used postural assessment ‘always,’ ‘frequently’ or ‘some of the time’, over half (61.8%) said they used postural assessment because it helped determine whether a patient was making progress and that it provided an outcome measure (57.1%), with the majority stating that it helped inform the diagnosis (89.2%) and treatment plan (81.8%) (Figure 2).
3.1.3. Method of Assessing Posture
Of the 259 respondents who said they used postural assessment ‘always,’ ‘frequently’ or ‘some of the time’, almost all (98.1%) reported carrying out a postural assessment visually, with no aids. Most respondents reported observing their patient posteriorly (n = 249, 96.1%), anteriorly (n = 207, 79.9%), left lateral only (n = 33, 12.7%), right lateral only (n = 40, 15.4%), and from both left and right sides (n = 186, 71.8%) (Figure 3).
3.1.4. Specific Postural Assessment Indices
When assessing a subject posteriorly, the 259 respondents who said they used postural assessment ‘always,’ ‘frequently’ or ‘some of the time’ reported observing a range of anatomical items including symmetry between left and right sides of the body (95.8%), scoliosis (91.1%), foot position (85.7%), iliac crests (88%), inferior angles of the scapulae (81%) plus 14 other points (Figure 4).
When assessing a subject anteriorly, these respondents reported observing general symmetry between left and right sides of the body (88%), feet (74.9%), knees (65.3), specific knee shape (genu varus/valgus) (64.5%), clavicles (61.8%) and 11 other points.
When assessing a subject from a lateral position, anatomical items observed include head position (98.1%), shape of the thoracic spine (91.5%), shape of the lumbar spine (90.7), shape of the cervical spine (90.0%), position of the pelvis (85.3%) and four other points.
3.1.5. Back and Neck Pathologies Encountered by Chiropractors
The 272 survey respondents reported treating a wide variety of back- and neck conditions including sacroiliac pain (96.7%), stiff neck (95.6%), non-specific low- back pain (92.6%), herniation of a vertebral disc in the lumbar spine (91.5%), arthritis of the cervical spine (89.7%), muscle strain of the lumbar spine (87.1%), arthritis in the lumbar spine (86.4%), thoracic pain (86.4%), muscle strain of the neck (84.9%), whiplash (79.8%) and nine other conditions (Figure 5).
3.2. Qualitative Analysis
Eight survey questions (question 2 – 4, 6-10) contained free-text options. Of these, 7 received free-text responses. Table 2 shows how many responses were obtained for each of the free-text questions and the percentage level of agreement between raters for the assignment of codes for each response. There were 229 free-text responses. The coding process was used to explore emerging themes from these responses. The codes assigned to each by independent raters using the Manual for Raters and the percentage level of agreement between raters for each response.
3.2.1. Rationale for the Use for Postural Assessment
Question 2 was,
As you answered ‘always’, ‘frequently’ or ‘some of the time’ to the previous question, please tick as many of the statements as you agree with. I use postural assessment because:
Responses to Question 2 fell predominantly into two themes: postural assessment was used because, first, it informs the clinician or was for their benefit.
“It alerts me to poor postural habits that need to be addressed and advised against” [Participant 132];
“it helps inform my rehabilitation protocols” [Participant 25]
And, second, it informs the patient or is for the benefit of the patient
“Patients understand it and think it is important” [Participant 148];
“It helps to educate the patient” [Participant 74].
Question 3 was,
As you answered ‘rarely’ or never’ to the previous question, please tick any of the following statements you agree with. I rarely or never carry out postural assessment because: I’m wondering if this was because it may have been seen as being repetitive?
3.2.2. Methods Used to Carry Out Postural Assessment
Question 4 was,
What methods do you use to carry out postural assessment?
Eight methods were identified for responses to this question, and each method was used as a theme to code the responses. The eight methods were an, ‘app’ (n = 2)
A ‘goniometer’ (n = 1), ‘a grid or chart’ (n = 1), ‘mirror’ (n = 2), ‘palpation’ (n = 2), ‘photograph’ (n = 1), ‘Spinal Analysis Machine’ (n = 4) and ‘x-ray’ (n = 3). One respondent commented that they did not use any technology to assess posture.
3.2.3. Positions Used for Postural Assessment
Question 6 was,
If you perform POSTERIOR postural assessment with back- and neck- pain patients, what are the things you observe?
Postural indices reported were wide-ranging and included those relating to the head (n = 11) and the relationship between one body part and another (n = 11). For example, ‘ear level’, and ‘lordosis/kyphosis relationship’ respectively.
Question 7 was,
If you perform ANTERIOR postural assessment with back- and neck- pain patients, what are the things you observe?
The postural indices reported were again wide-ranging and included indices relating to the lower limb (n = 6) such as ‘foot arch’ and ‘hip rotation’ and body shape or size (n = 4) such as ‘abdomen size’ and ‘abdominal contours’.
Question 8 was,
If you perform LATERAL postural assessment with back- and neck- pain patients, what are the things you observe?
Responses to this question included those relating to the position of the body and weight distribution (n = 6). For example, ‘balance of anterior/posterior weight’ and ‘whether the weight is being carried forward onto the toes’. All of the themes for responses to Questions 6, 7 and 8 are listed in the Manual for Raters.
3.2.4. Back- and Neck Pathologies Encountered in Clinical Practice
Question 9 was,
Thinking only about patients with back- or neck- pain, what sorts of pathologies do you come across commonly in your practice?
In response to Question 9, in addition to the pathologies listed, the participants stated that other pathologies in the free-text box available for this purpose and included conditions affecting the face, head and neck (dizziness, headaches, sinusitis), upper limb (brachial plexus problems, thoracic outlet syndrome), chest/ribs (costotransverse joint sprain), spine (dural tube problems, spinal stenosis), pelvis (perineal pain), lower limb (piriformis syndrome, sciatica) and conditions not specific to a part of the spine (cancer, neuralgia, tension).
3.2.5. Additional Comments
Question 10 was,
Is there anything else you would like to say about your use of postural assessment?
Responses to question 10 were wide-ranging and fell within four broad themes. The first theme was regarding the methods of postural assessment: below are a few of the statements that participants mentioned.
“How can you assess posture without xray? You can look visually at someone and their structure on xray can be very different to what you expect. You must understand spinal coupling mechanisms and 3D analysis if you wish to correct posture photographs like x-rays can project distortion especially if they are not taken correctly” [Participant 74];
“I combine it with dynamic assessment and gait” [Participant 238].
The second theme included comments made regarding specific aspects of posture that were reported to be observed during the assessment:
“I also look for torque, i.e., rotation in the horizontal plane, of the head, shoulder and pelvic girdles in relation to each other and to the position of the feet” [Participant 73].
The third theme comprised of comments that were made regarding the use and value of postural assessment (both positive and negative).
“It is an absolute must in practice for us and the patient.” [Participant 55] “I think it is way overrated.” [Participant 253]
Finally, the fourth theme comprised of comments about the rationale for postural assessment:
“Posture is adapted, neutral and, unique to the individual - to not assess posture is doing an unforgivable disservice to the patient and not fulfilling our remit of neuro-musculoskeletal consultants” [Participant 257];
4. Discussion
Key Findings
The results of this study demonstrated that the majority of respondents reported carrying out postural assessment almost all of the time on patients with neck- and back conditions, using visual assessment alone. This was conducted for the purposes of informing their diagnosis and treatment of patients with back- and neck pain. Over 50% of participants reported that they used it to provide a clinical outcome measure. Generally, chiropractors in this survey reported observing their patients from the posterior, anterior and lateral views in order to carry out the assessment, observing a large number of different indices. The most common indices of these were symmetry, spine shape and the position of the head and pelvis, as well as the position of the shoulders, knees and feet. The back- and neck presentations most commonly encountered were sacroiliac pain, stiff neck, non-specific low-back pain, herniation of a vertebral disc in the lumbar spine, arthritis of the cervical and lumbar spine, muscle strain of the lumbar spine or neck, thoracic pain and whiplash. It is not known whether the response rate of 22% for this survey falls within the norm for surveys of chiropractors.
The response rate of this study is similar to that of Fikar, Edlund and Newell (2015) (22%), but lower than those of Puhl, Reinhart and Injevan (2015) (68%) and of Alliet, Rubinstein and de Vet (2010). It seems that postal questionnaires — of which the latter two citations are examples — might generate higher response rates. Secondary analysis by Russell et al., (2004) of data from 46 published postal surveys of chiropractors ranged from 7% to 91.4% (mean 52.7%).
Quantitative and Qualitative Data
This study reported that 79% (n = 215) of respondents ‘almost always’ (76% – 100% of the time) used postural assessment when treating patients with back or neck pain. The only study found to quantify the frequency for the use of postural assessment by chiropractors is that by Puhl, Reinhart and Injeyan (2015). That study details that 29.9% (n = 146) of respondents ‘always’ (76% – 100% of the time) used postural assessment, 20.7% (n = 101) ‘usually’ (51% - 75%) used it. That is, 50.6% (n = 247) of chiropractors in Puhl, Reinhart and Injeyan’s study usually-always (75% - 100%) used postural assessment compared to the researcher’s study which found 79% of respondents almost always used it. The reason for the discrepancy between the frequency of use of postural assessment reported in the two studies is unknown. One reason may be any training variations between chiropractors working in different geographical regions: the researcher’s study surveyed UK chiropractors and Puhl, Reinhart and Injeyan surveyed Canadian chiropractors.
In the study by Alliet, Rubinstein and de Vet (2010) 72% (n = 80) of Belgian chiropractors reported ‘often to always’ using postural assessment and 97.1% of UK chiropractor respondents reported evaluating posture (Fikar, Edlund and Newell, 2015), but in both cases the description of frequency was not quantified, making comparisons difficult. In another study, 79% (n = 48) reported ‘always’ using visual assessment of posture with a new patient (Hinton, et al., 2010). Similarly, three studies in which the use of postural assessment by clinicians was embedded within the questions put to participants, failed to quantify the frequency of use. Enwemeka et al. (1986) surveyed 120 physiotherapists in New York, New Jersey and Puerto Rico and reported that 72% (n = 33) of respondents stated that they ‘often’ used postural correction when treating patients with neck pain. A focus group study carried out in Portugal and involving 21 physiotherapists used a variety of set questions, one of which was, ‘Do you assess head posture for patients with neck pain in your clinical practice?’ (p. 100) (Silva, Punt and Johnson, 2009). The authors stated that physiotherapists reported routinely assessing head posture for patients with neck pain. In the study of a mixed group of 28 clinicians (six chiropractors, seven physical therapists, six physiatrists, four rheumatologists and five orthopaedic surgeons), Fedorak et al. (2003) detailed that all participants reported regularly using visual spinal posture assessment, with 93% saying this was the tool they used most frequently to assess spinal posture.
This study identifies the rationale for the use of postural assessment by chiropractors, with almost 90% of respondents reporting that they used it to inform their diagnosis. Over 80% said that it helped inform their treatment and over 50% stated that it provided an outcome measure. This is consistent with the findings of Alliet, Rubinstein and de Vet (2010) who reported 72% (n = 80) of Belgian chiropractors used postural analysis as a diagnostic procedure. , 71.5% (n = 339) of English- speaking Canadian chiropractors used w it for this reason (Puhl, Reinhart and Injeyan, 2015) , with 80.4% (n = 409) of UK chiropractors setting goals and re- evaluating progress with regards to patient posture (Fikar, Edlund and Newell, 2015). Additionally, Puhl, Reinhart and Injeyan, (2015) reported that over 80% (n = 406) used ‘posture’ as a treatment method. This may be in the form of exercises to correct posture.
This study provides information about the methods used by chiropractors to carry out their assessment of posture, both generally and specifically. Generally, this study found that 98% of chiropractors reported performing the assessment of posture visually, unaided by devices. This is consistent with findings elsewhere for the use of postural assessment by chiropractors and physiotherapists where use of unaided visual assessment of posture was reported to be 84% (Van Schaik, Bettany-Saltikov and Warren, 2002, UK), 93% (Fedorak et al., 2003, Canada) and 100% (Silva, Punt and Johnson., 2009, Portugal). This current study also asked about the specifics of visual postural assessment and found that almost 100% of chiropractors reported assessing the posture of their patients from a posterior view, almost 80% used an anterior assessment and over 70% observed posture from both left and ride sides of their patient. Although no studies could be found that reported such specificity of use of postural assessment, Silva, Punt and Johnson (2009) noted that 86% of the 275 physiotherapists surveyed reported carrying out postural assessment with the patient standing.
This study also identified specific anatomical points that were routinely observed by chiropractors carrying out postural assessment. When assessing patients with back- or neck pain, the majority of respondents, reported observing symmetry between the left and right sides of the body, head position, shape of the spine, iliac crests and position of the pelvis. They also assessed for the presence of scoliosis, as well as foot position. Over 70% reported looking at the position of the shoulder and scapula and whether there was evidence of genu valgum or genu varum. No studies were found with which to contrast these findings.
This survey of UK Chiropractors revealed specific back- and neck pathologies UK chiropractors were treating, with over 90% treating patients with sacroiliac pain, stiff neck, lumbar disc herniations, non-specific low-back pain., over 85% of chiropractors treated arthritis in the cervical or lumbar spines, thoracic pain, and muscle strain in the lumbar region. A similar study by Ailliet, Rubinstein and de Vet (2010) reported that 85.5% of Belgian chiropractors treated patients whose primary complaint was low- back- and/or neck pain.
Limitations of the Study
Given the 78% non-response rate and the non-random nature of sampling potential participants, the results from this study may not be generalisable to the UK chiropractic profession as a whole. One reason that the response rate was low for this study could be that an advance warning of the survey was not provided, an approach believed to increase response rates (Fan and Yan, 2010). Another reason may be related to the large number of emails practitioners may receive, some of which may be ignored. Additionally, a high rate of non-responses creates an increased probability of statistical bias (Tomaskovic-Devey, Leiter and Thompson, 1994). However, Cook et al. (2007) argue that, in survey research, response representativeness is more important than response rate. The implications of this are that the study may need to be repeated. Unanswered questions: it is not known why the majority of respondents in this survey reported the use of visual postural assessment when this method is known to lack objectivity and therefore may be neither valid nor reliable. This may be because it has been used historically as part of the assessment process and, until recently, practical alternatives have been unavailable. Nor is it known why a large percentage of respondents used postural assessment to help inform their diagnosis and treatment when treating patients with back or neck pain, when the evidence to support a relationship between posture and pain is limited. In future research it would be useful to use, interviews and focus groups as a means to further investigate these questions.
5. Conclusions
In conclusion, the findings suggest that postural assessment is used by UK chiropractors for the purposes of aiding diagnosis and treatment, and that the method predominantly used is that of unaided visual assessment. Chiropractors also reported assessing their patients from the posterior, anterior and lateral viewpoints and observed a wide range of anatomical points. This information is used to inform both practitioners as well as their patients. A wide range of back- and neck pathologies were reported by these practitioners. The results from this cross-sectional study suggest that further exploration for the rationale for postural assessment is warranted. Further investigation is required to explore whether these findings match those of clinicians working in other fields of manual therapy such as physiotherapy and osteopathy. One of the reasons that chiropractors may be assessing posture visually could be because they lack an alternative method that is suitable for use in a clinic setting.
Author Contributions
Conceptualization, J.J., J.B-S., P.V.S., J.C., D.N.; methodology, J.J., J.B-S., P.V.S., D.N.; software, J.J., J.B-S., and D.N.; validation, J.J. formal analysis, J.J., J.B-S., P.V.S., J.C., D.N., and R.D.; resources, J.J. and D.N.; data curation, J.J., J.B-S., and R.D.; writing—original draft preparation, R.D. and J.B-S.; writing—review and editing, R.D. and J.B-S.; project administration, J.J. and R.D.; funding acquisition, J.J. and J.B-S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Teesside University and the Royal College of Chiropractors.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by AECC University College Ethics subcommittee (20 March 2016 for ethic approval).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the participants to publish this paper.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author (R.D.) upon reasonable request. These data, due to confidentiality and ethical considerations, are not publicly available.
Acknowledgments
I would like to thank Jacqui Rix from the AECC University College (formerly called the Anglo European College of Chiropractic) for providing feedback on the draft of the Survey of Chiropractors, along with physiotherapists Jaya Elango, Emma Clark-Eden, Janine Paul and James Morgan, plus osteopaths Jason Bianchi, Alan Rowe, and Richard Lewis. Thank you to the AECC University College for assisting in the dissemination of the Survey. I am grateful to the chiropractors who anonymously took part in this survey. Thank you to osteopath Jason Bianchi who acted as a second Coder when developing codes for the Survey’s qualitative responses.
Conflicts of Interest
The authors declare no conflicts of interest associated with the material presented in this paper. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- World Health Organization (2005) WHO Guidelines on basic training and safety in chiropractic. Geneva: World Health Organization. Available at: https://www.who.int/medicines/areas/traditional/Chiro-Guidelines.pdf (Accessed: 29 Jun 2016).
- General Chiropractic Council (2010b) Your first visit? Available at: https://www.gcc- uk.org/chiropractic-standards/seeing-a-chiropractor-for-the-first-time (Accessed: ). 1 July.
- Kendall, F.P.; McCreary, E.K.; Provance, P.G.; Rodgers, M.M.; Romani, W.A. Muscles: Testing and Function, with Posture and Pain, 5th ed.; LWW: Baltimore, MD, USA, 2005; ISBN 978-0-7817-4780-6. [Google Scholar]
- Johnson, J. (2012) Postural assessment. Champaign: Human Kinetics. Author 1, A.; Author 2, B. Book Title, 3rd ed.; Publisher: Publisher Location, Country, 2008; pp. 154–196. [Google Scholar]
- Magee, D. J. (2002) Orthopedic physical assessment. Philadelphia, US: Saunders.
- Page, P. , Frank, C.C. and Lardner, R. (2010) Assessment and treatment of muscle imbalance: the Janda approach. Champaign, US: Human Kinetics.
- Hartvigsen, J.; French, S. What is chiropractic? Chiropr. Man. Ther. 2017, 25, 30. [Google Scholar] [CrossRef]
- Lederman, E. The fall of the postural-structural-biomechanical model in manual and physical therapies: Exemplified by lower back pain. J. Bodyw. Mov. Ther. 2011, 15, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Enwemeka, C.S.; Bonet, I.M.; Ingle, J.A.; Prudhithumrong, S.; Ogbahon, F.E.; Gbenedio, N.A. Postural Correction in Persons with Neck Pain. I. A Survey of Neck Positions Recommended by Physical Therapists. J. Orthop. Sports Phys. Ther. 1986, 8, 235–239. [Google Scholar] [CrossRef]
- Fedorak, C.; Ashworth, N.; Marshall, J.; Paull, H. Reliability of the Visual Assessment of Cervical and Lumbar Lordosis: How Good Are We? Spine 2003, 28, 1857–1859. [Google Scholar] [CrossRef]
- Silva, A. , Punt D, Johnson M. (2009) ‘A postal survey gathering information about physiotherapists’ assessment of head posture for patients with chronic idiopathic neck pain’, European Journal of Pain. 13:S223.
- Silva, A.G.; Punt, T.D.; Sharples, P.; Vilas-Boas, J.P.; Johnson, M.I. Head Posture and Neck Pain of Chronic Nontraumatic Origin: A Comparison Between Patients and Pain-Free Persons. Arch. Phys. Med. Rehabilitation 2009, 90, 669–674. [Google Scholar] [CrossRef] [PubMed]
- Ailliet, L.; Rubinstein, S.M.; de Vet, H.C. Characteristics of Chiropractors and their Patients in Belgium. J. Manip. Physiol. Ther. 2010, 33, 618–625. [Google Scholar] [CrossRef] [PubMed]
- Hinton, P.M.; McLeod, R.; Broker, B.; Maclellan, C.E. Outcome measures and their everyday use in chiropractic practice. . 2010, 54, 118–31. [Google Scholar] [PubMed]
- A Puhl, A.; Reinhart, C.J.; Injeyan, H.S. Diagnostic and treatment methods used by chiropractors: A random sample survey of Canada's English-speaking provinces. . 2015, 59, 279–87. [Google Scholar] [PubMed]
- Bone and Joint Decade: Global Alliance for Musculoskeletal Health. (2017) The Neck. Available at: http://bjdonline.org/the-neck/. (Accessed: 20 Feb 2017).
- World Health Organization (2003) Preventing musculoskeletal disorders in the workplace. Switzerland: World Health organization. Available at: https://www.who.int/occupational_health/publications/en/oehmsd3.pdf. (Accessed: ). 14 August.
- International Organization for Standardization (2000) International Standard ISO 11226. Ergonomics – evaluation of static working postures. Available at: https://www.iso.org/standard/25573.html.
- NHS (2019) Common posture mistakes and fixes. Available at: http://www.nhs.uk/Livewell/Backpain/Pages/back-pain-and-common-posture- mistakes.aspx (Accessed: ). 2 July.
- Khaleeli, H. (2014) ‘Text neck: how smartphones are damaging our spines’ The Guardian.
- https://www.theguardian. 2014.
- cessed:10 Jan 2017).
- Snodgrass, S. (2016) ‘Is bad posture giving you a hunchback? Expert reveals how to prevent slumping at your desk from damaging your spine’, Daily Mail. 16 May. Available at: http://www.dailymail.co.uk/health/article-3592690/Is-bad-posture- giving-hunchback-Expert-reveals-prevent-slumping-desk-damaging-spine.html. (Accessed: 20 Feb 2020).
- Kritz, M.F.; Cronin, J. Static Posture Assessment Screen of Athletes: Benefits and Considerations. Strength Cond. J. 2008, 30, 18–27. [Google Scholar] [CrossRef]
- E Fikar, P.; A Edlund, K.; Newell, D. Current preventative and health promotional care offered to patients by chiropractors in the United Kingdom: a survey. Chiropr. Man. Ther. 2015, 23, 10–10. [Google Scholar] [CrossRef] [PubMed]
- Van Schaik, P.; Bettany-Saltikov, J.A.; Warren, J.G. Clinical acceptance of a low-cost portable system for postural assessment. Behav. Inf. Technol. 2002, 21, 47–57. [Google Scholar] [CrossRef]
- General Chiropractic Council (2010b) Your first visit? Available at: https://www.gcc- uk.org/chiropractic-standards/seeing-a-chiropractor-for-the-first-time (Accessed: ). 1 July.
- Harrison, D.E.; Harrison, D.D.; Troyanovich, S.J.; Harmon, S. A normal spinal position: It's time to accept the evidence. J. Manip. Physiol. Ther. 2000, 23, 623–644. [Google Scholar] [CrossRef] [PubMed]
- Newell, D.; Diment, E.; E Bolton, J. An Electronic Patient-Reported Outcome Measures System in UK Chiropractic Practices: A Feasibility Study of Routine Collection of Outcomes and Costs. J. Manip. Physiol. Ther. 2016, 39, 31–41. [Google Scholar] [CrossRef] [PubMed]
- DE Looze, M.P.; Toussaint, H.M.; Ensink, J.; Mangnus, C.; VAN DER Beek, A.J. The validity of visual observation to assess posture in a laboratory-simulated, manual material handling task. Ergonomics 1994, 37, 1335–1343. [Google Scholar] [CrossRef]
Figure 1.
Frequency of use of postural assessment.
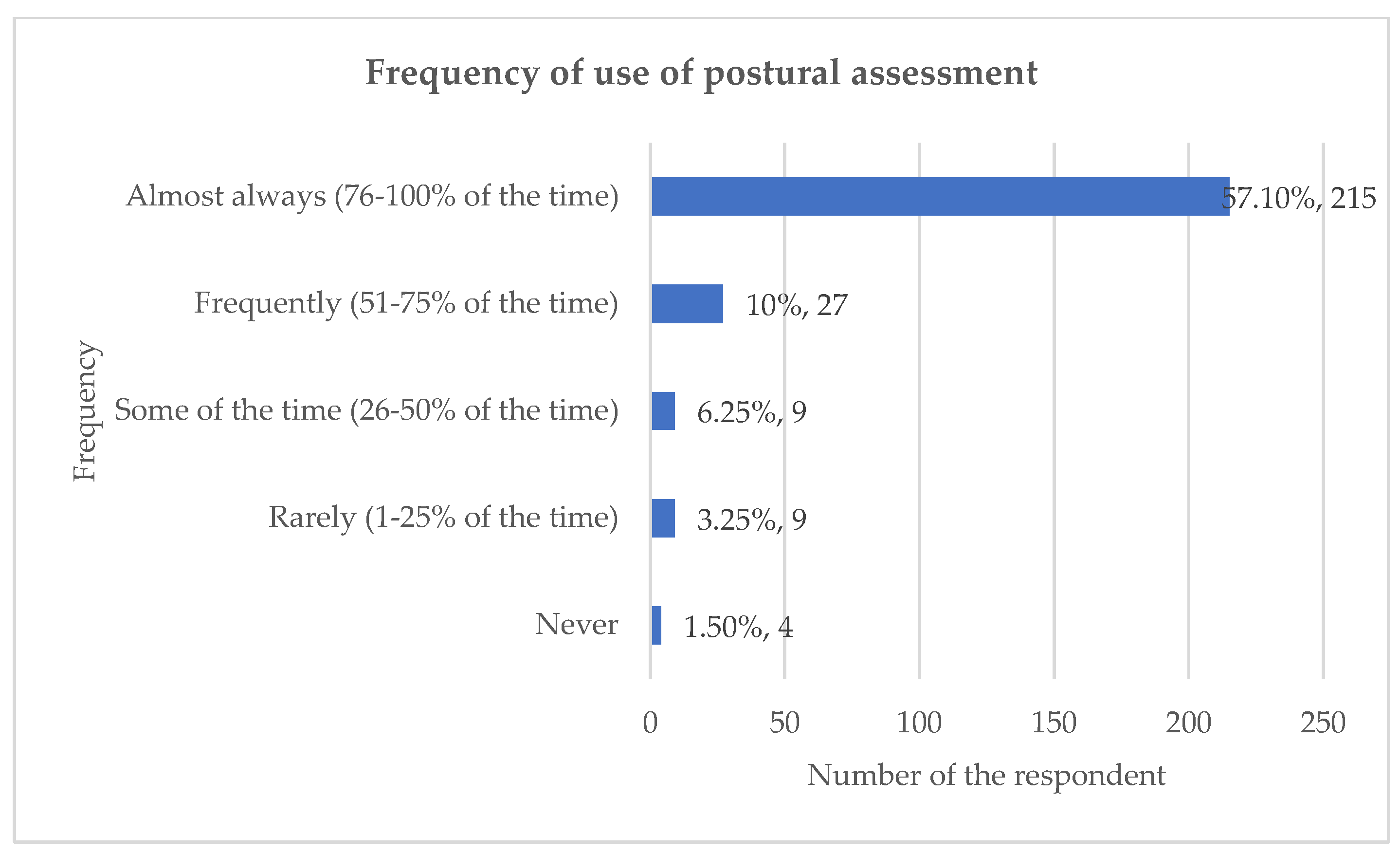
Figure 2.
Rationale for use postural assessment.

Figure 3.
Method of postural assessment.
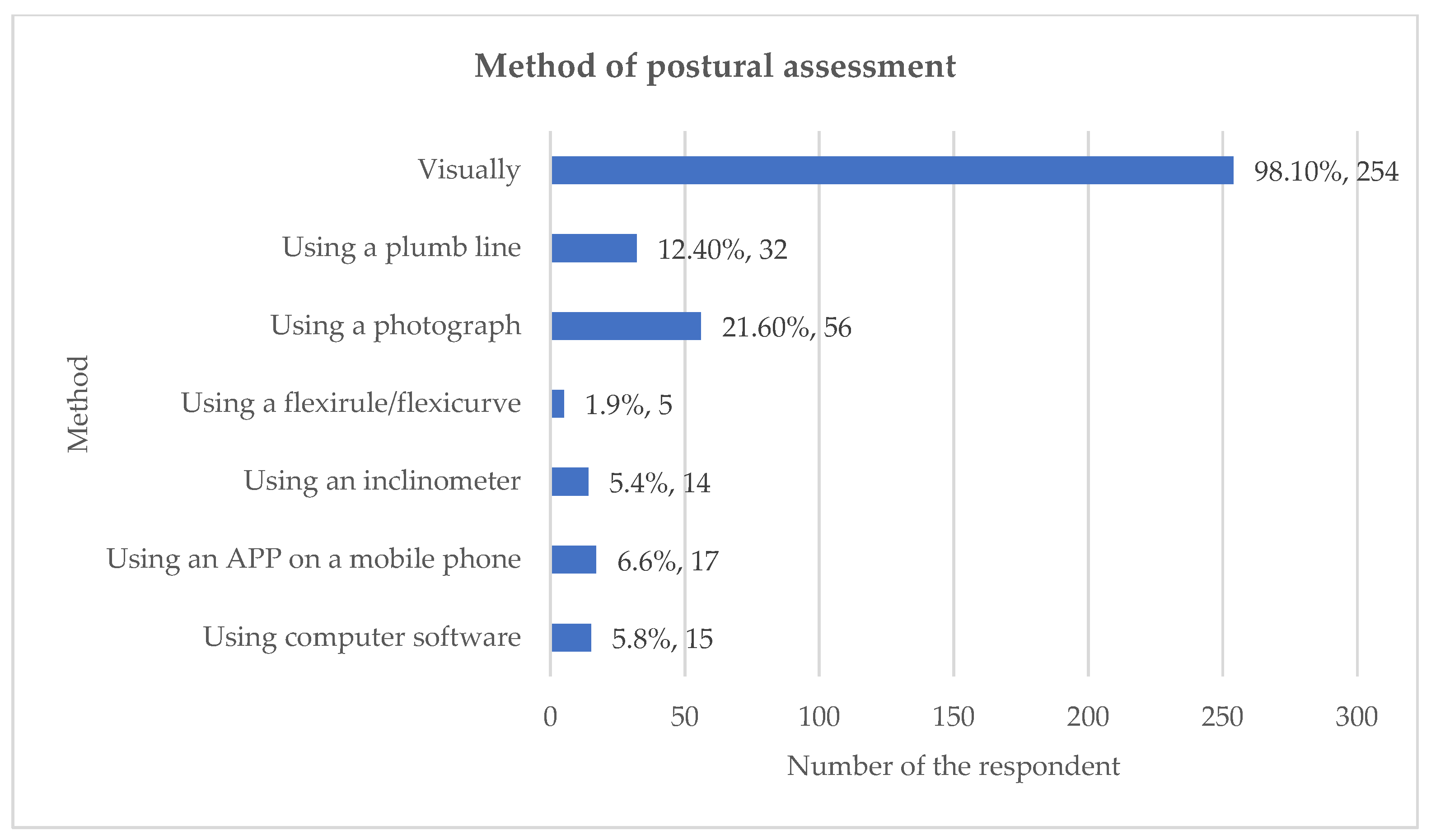
Figure 4.
Items observed with posterior postural assessment.
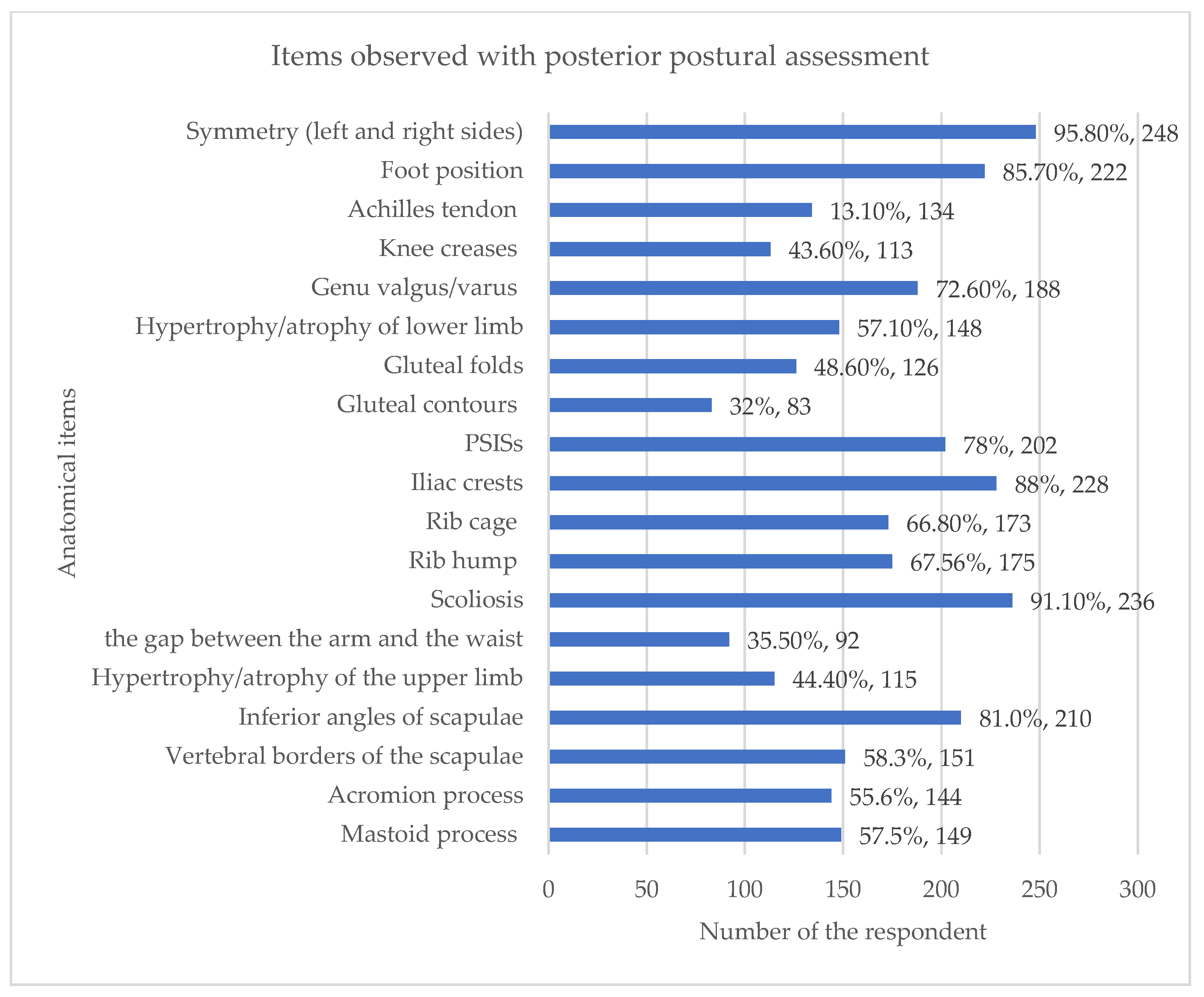
Figure 5.
Back-and neck pathologies commonly encountered.
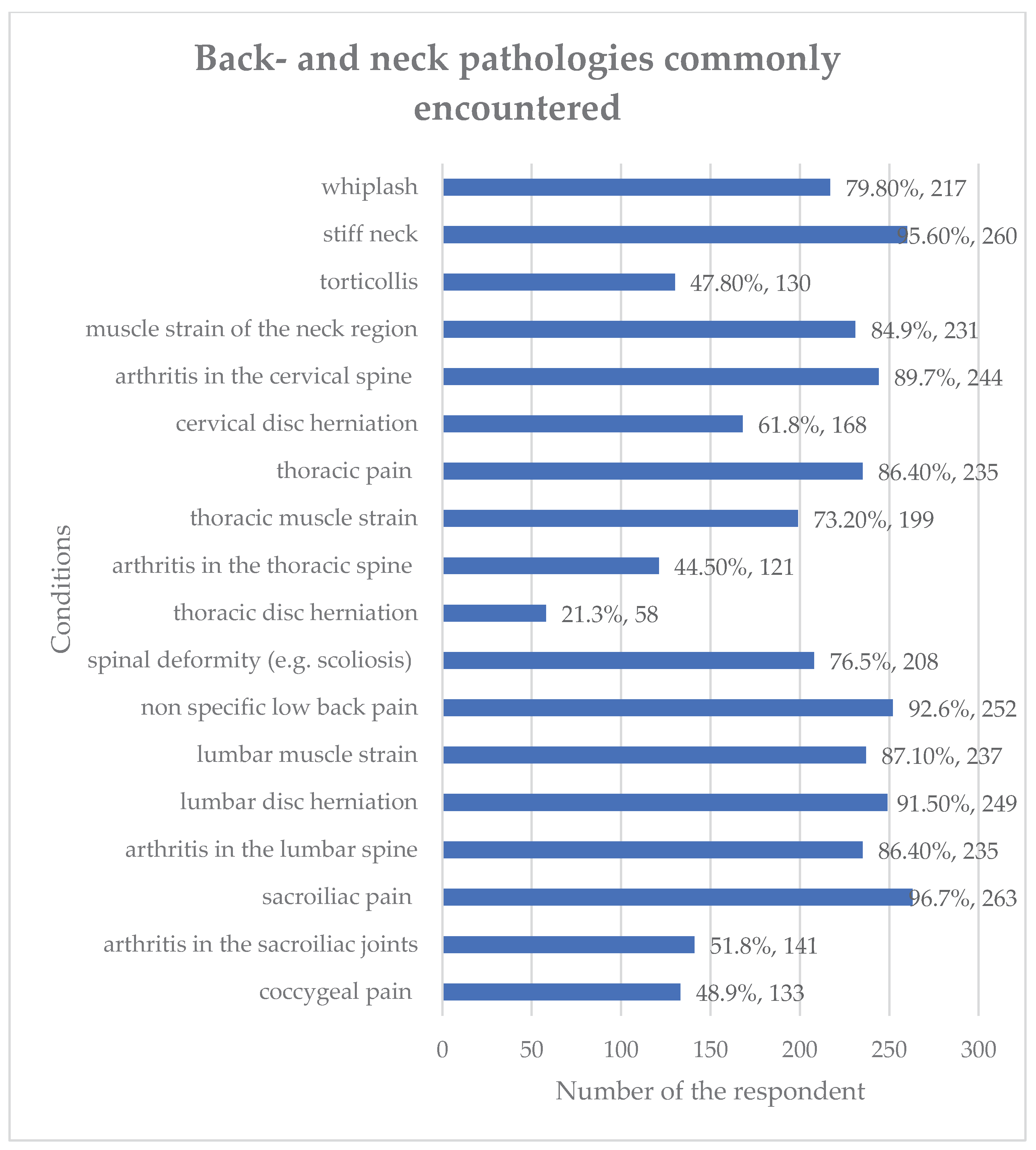

Table 1.
The 11-question asked in the questionnaire.
| Question |
| Q 1. Please tick ONE box to indicate how frequently you use postural assessment with a NEW patient who comes to you with back or neck pain. |
| Almost always (76-100% of the time) |
| Frequently (51-75% of the time) |
| Some of the time (26-50% of the time) |
| Rarely (1-25% of the time) |
| Never |
|
Q2. As you answered ‘always’, ‘frequently’ or ‘some of the time’ to the previous question, please tick as many of the statements you agree with. I use postural assessment because: |
| It provides an outcome measure |
| It helps inform my diagnosis |
| It helps inform my treatment |
| It helps me determine whether a patient is making progress or not |
| It is mandatory (employer requires it) |
| I was taught to use it during my training |
| Other (please specify)……………………………………………. |
|
Q3. As you answered ‘rarely or ‘never’ to the previous question, please tick any of the following statements you agree with. I rarely or never carry out postural assessments because: |
| I don’t have time |
| Postural assessment is not relevant to my diagnosis or treatment |
| I don’t believe it is accurate or objective |
| My patients don’t like it or it is not appropriate for them |
| I was not taught to use it |
| Other (please specify)……………………………………………. |
|
Q4. What methods do you use to carry out postural assessment? You may choose more than one option or tick as many as apply. |
| Visually |
| Using a plumb line |
| Using a photograph |
| Using a flexirule/flexicurve |
| Using an inclinometer |
| Using an APP on a mobile phone |
| Using computer software |
| Other (please specify)……………………………………………. |
| Q5. From which positions do you assess your subject?You may choose more than one option. |
| Both left and right sides |
| Right lateral only |
| Left lateral only |
| Posterior |
| Anterior Posterior |
|
Q6. If you perform POSTERIOR postural assessment with back- and neck pain patients, what are the things you observe? You may choose more than one option. |
| Symmetry between left and right sides of the body |
| Foot position |
| Achilles tendon |
| Knee creases |
| Genu valgus/varus |
| Hypertrophy/atrophy of lower limb muscles |
| Gluteal folds |
| Gluteal contours |
| PSISs |
| Iliac crests |
| Rib cage |
| Rib hump |
| Scoliosis |
| Size of the keyhole (gap between the upper limb and thorax) |
| Hypertrophy/atrophy of the upper limb |
| Inferior angles of scapulae |
| Vertebral borders of the scapulae (distance laterally from the spine) |
| Acromion process |
| Mastoid process |
| Other (please specify) ……………………………………………. |
|
Q7. If you perform ANTERIOR postural assessment with back- and neck pain patients, what are the things you observe? You may choose more than one option. |
| General symmetry between left and right sides of the body |
| Feet |
| Knees |
| Genu valgus/ varus |
| Hypertrophy/atrophy of lower limb muscles |
| Greater trochanters |
| ASISs |
| Iliac crests |
| Rib cage |
| Size of the “keyhole” (gap between the upper limb and thorax) |
| Hypertrophy/atrophy of upper limb muscles |
| Clavicles |
| Acromioclavicular joints |
| Muscles of the neck |
| Mastoid processes |
| Facial symmetry |
| Other (please specify) ……………………………………………. |
|
Q 8. If you perform a LATERAL postural assessment with back- and neck pain patients, what are the things you observe? You may choose more than one option. |
| Head position |
| Shape of cervical spine |
| Shape of thoracic spine |
| Shape of lumbar spine |
| Position of pelvis – anterior or posterior pelvic tilt |
| Shoulder position |
| Position of upper limb |
| Position of lower limb – e.g., genu recuravtum/genum flexum |
| Overall body shape |
| Other (please specify) ……………………………………………. |
| Q 9.Thinking only about patients with back or neck pain, which sorts of pathologies do you come across commonly in your practice? Please note, the following are only some of the possible pathologies you may commonly come across. (Please tick as many as apply and use the ‘other’ box to add others) |
| whiplash |
| stiff neck |
| torticollis |
| muscle strain of the neck region |
| arthritis in the cervical spine |
| herniation of an intervertebral disc in cervical spine |
| thoracic pain |
| muscle strain of the thoracic region |
| arthritis in the thoracic spine |
| herniation of an intervertebral disc in thoracic spine |
| spinal deformity (e.g., scoliosis) |
| non-specific low back pain |
| muscle strain of the lumbar spine |
| herniation of an intervertebral disc in lumbar spine |
| arthritis in the lumbar spine |
| sacroiliac pain |
| arthritis in the sacroiliac joints |
| coccygeal pain |
| Other (please specify) ……………………………………………. |
| Q10. Is there anything else you would like to say about your use of postural assessment? |
| please specify) ……………………………………………. |
| Q11. Finally, please select the answer that most closely represents your profession: |
| Chiropractor Osteopath Physiotherapist |
| Sports Therapist |
| Osteopath |
| Physiotherapist |
| Other (please specify) ……………………………………………. |
Table 2.
Number of responses to questions with a free-text option.
| Survey question | Number of free-text responses | Percentage (%) agreement |
| 1. No free-text option | NA | NA |
| 2.As you answered ‘always’, ‘frequently’ or ‘some of the time’ to the previous question, please tick as many of the statements you agree with. I use postural assessment because:R where are the statements they were responding to? | 28 | 21 had 100% agreement 2 had 50% agreement 5 had no agreement |
|
3.As you answered ‘rarely’ or ‘never’ to the previous question, please tick any of the following statements you agree with. I rarely or never carry out postural assessment because: |
0 | NA |
|
4.What methods do you use to carry out postural assessment? You may choose more than one option or tick as many as apply. |
17 | 16 had 100% agreement 1 had no agreement |
| 5.No free-text option | NA | NA |
|
6.If you perform POSTERIOR postural assessment with back and neck pain patients, what are the things you observe? You may choose more than one option. |
31 | 24 had 100% agreement 1 had 40% agreement 1 had 33% agreement 2 had 25% agreement 1 had 20% agreement 2 had zero agreement |
| 7.If you perform ANTERIOR postural assessment with back and neck pain patients, what are the things you observe? You may choose more than one option. | 28 | 26 had 100% agreement 1 had 75% agreement 1 had no agreement |
| 8.LATERAL postural assessment with back and neck pain patients, what are the things you observe? You may choose more than one option. | 18 | 6 had 100% agreement 6 had 50% agreement 1 had 33% agreement 1 had 20% agreement 4 had no agreement |
| 9.Thinking only about patients with back or neck pain, which sort of pathologies do you come across commonly in your practice? Please note, the following are only some of the possible pathologies you may commonly come across. (Please tick as many as apply and use the ‘other’ box to add others). | 41 | 26 had 100% agreement 1 had 83% agreement 1 had 66% agreement 1 had 62.5% agreement 6 had 50% agreement 2 had 33% agreement 3 had no agreement 1 response would not be rated |
| 10.Is there anything else you would like to say about your use of postural assessment? | 66 | 34 had 100% agreement 13 had 50% agreement 2 had 66% agreement 1 had 33% agreement 16 had no agreement |
| 11.No free-text option | NA | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



