
Submitted:
17 October 2025
Posted:
20 October 2025
You are already at the latest version
Abstract
Background:
Acute limb ischemia (ALI) is a vascular emergency where timely revascularization is crucial for limb salvage and survival. While open surgical revascularization (OSR) has been the traditional standard, catheter-directed thrombolysis (CDT) has emerged as a minimally invasive alternative. Comparative real-world evidence in early-stage ALI (Rutherford I–IIa) remains limited.
Methods:
We conducted a retrospective single-center cohort study including 36 patients with ALI treated between 2019 and 2023 (OSR: n=24; CDT: n=12). Demographics, comorbidities, procedural details, and outcomes were analyzed. The primary endpoint was a composite of in-hospital mortality, primary patency, and secondary patency. Secondary endpoints included amputation, cerebrovascular events, renal function, and hospital stay. Effect sizes with 95% confidence intervals were reported alongside p-values to address type II error risk.
Results:
Baseline characteristics were comparable between groups. Both OSR and CDT significantly improved ankle-brachial index (0.64 ± 0.43 to 0.93 ± 0.33, p< 0.001) and postoperative arterial patency. At 12 months, primary patency was 66.7% (OSR) vs. 50.0% (CDT), and secondary patency was 79.2% vs. 75.0% (p>0.05). Major amputation (12.5% vs. 16.7%) and mortality (8.3% vs. 16.7%) rates did not differ significantly. Hospital stay was longer after OSR (7.29 ± 4.58 vs. 6.08 ± 8.75 days, p=0.038). Fibrinogen levels decreased significantly during CDT, but no major bleeding events occurred.
Conclusion:
Both OSR and CDT provide effective revascularization in early ALI, with comparable limb salvage and survival outcomes. CDT offers a minimally invasive alternative with acceptable safety when accompanied by careful monitoring, whereas OSR remains a reliable option with immediate reperfusion. Larger multicenter studies are needed to refine patient selection and optimize treatment algorithms.
Keywords:
Acute Limb Ischemia
; Catheter-Directed Thrombolysis
; Surgical Revascularization
; Limb Salvage
Introduction
Acute limb ischemia (ALI) is a vascular emergency characterized by a sudden reduction in limb perfusion that, if untreated, may rapidly progress to limb loss and life-threatening complications [1]. The severity of ischemia is commonly classified using the Rutherford system [2]. Patients with Rutherford class I–IIa ischemia represent an early and potentially reversible stage, where timely intervention can restore perfusion before irreversible neuromuscular damage occurs. This subgroup is clinically important because outcomes are more favorable when revascularization is achieved promptly, and treatment choice in these patients may determine long-term limb salvage and functional recovery [3,4].
Traditionally, open surgical revascularization (OSR) with thromboembolectomy has been the standard approach, offering immediate flow restoration [5]. However, it carries important drawbacks: surgical trauma, anesthesia-related risk, and reduced effectiveness in distal or atherosclerotic disease [6]. More recently, catheter-directed thrombolysis (CDT) has emerged as a minimally invasive alternative, allowing gradual clot dissolution and preservation of distal branches [7]. Long-term clinical data have also shown favorable outcomes with endovascular therapy, including improved survival compared to open surgery in selected patients [8]. Yet, CDT entails longer treatment duration, risk of hemorrhage, and potential contrast-related renal complications [9,10].
Despite increasing adoption of CDT, the optimal strategy for ALI management remains unresolved [11]. Prior studies report conflicting findings on long-term outcomes, limb salvage, and complication rates [12,13]. Moreover, there is no consensus on thrombolytic dosing protocols, anticoagulation regimens, or post-procedural surveillance, leading to wide practice variations across centers [14]. This uncertainty underscores a critical knowledge gap, highlighting the need to determine how the clinical outcomes of OSR and CDT compare when these treatments are applied in routine practice, particularly in early Rutherford stages (I–IIa). Addressing this question is essential to guide treatment selection and inform standardization efforts.
Therefore, in this study we retrospectively compared OSR and CDT in patients with ALI, focusing on efficacy, safety, and key prognostic parameters—including renal function, thrombolytic dosage, and arterial patency. By clarifying these real-world outcomes, we aim to contribute evidence toward individualized decision-making in ALI management, particularly given the current lack of standardized protocols and the heterogeneous outcome reporting in previous studies, as highlighted by Veenstra et al [15].
Methods
This study was designed as a retrospective, single-center cohort analysis, focusing on 36 patients diagnosed with ALI who underwent either OSR (n=24) or CDT (n=12) between January 1, 2019, and December 31, 2023. Patient data were obtained from electronic medical records and institutional databases. All procedures included in the analysis were performed by board-certified cardiovascular surgeons with extensive experience in the management of ALI.
Patient Selection and Inclusion Criteria:
Eligible patients were those aged 18 years and older who were diagnosed with ALI based on clinical examination and imaging findings (e.g., Doppler ultrasound, computed tomography angiography), and subsequently underwent either OSR or CDT as a primary intervention. Exclusion criteria included patients with chronic limb ischemia, incomplete medical records, prior major lower limb amputation, or those who received hybrid or purely endovascular treatments not involving thrombolysis (Figure 1).
Treatment allocation was not randomized but was determined by the cardiovascular surgeon based on ischemia severity, comorbidities, anatomical factors, and contraindications to thrombolysis. As such, physician judgment inherently introduced a potential source of selection bias. To mitigate this, baseline demographics and comorbidities were compared between groups to ensure clinical comparability.
Intervention Details
CDT Protocol
CDT was performed by intra-arterial administration of thrombolytic agents (e.g., alteplase) through percutaneously inserted catheters under fluoroscopic guidance. The infusion was typically initiated at a rate of 0.5–1.0 mg/h, with subsequent dose and duration adjustments made at the discretion of the physician, based on individual patient characteristics, angiographic findings, and bleeding risk. Plasma fibrinogen levels were systematically monitored before initiation and following completion of therapy to guide dosage modifications and ensure procedural safety.
Anticoagulation
During CDT, all patients received concomitant low-dose unfractionated heparin infusion (typically 500–1,000 IU/h) through the sheath to maintain catheter patency and reduce peri-procedural thrombosis risk. Activated clotting time was not routinely measured, but infusion rates were adjusted if bleeding tendency was suspected [16].
After completion of CDT or OSR, all patients were transitioned to systemic anticoagulation (either low-molecular-weight heparin-LMWH or intravenous unfractionated heparin, followed by oral anticoagulation where indicated, such as atrial fibrillation) [12,17]. While the general principle of peri- and post-procedural anticoagulation was standardized, exact drug choice and duration were tailored according to comorbidities, bleeding risk, and prior antithrombotic therapy.
OSR Anticoagulation & Adjunctive Therapies
OSR consisted of standard thromboembolectomy performed under general or regional anesthesia. Systemic intravenous unfractionated heparin (3,000–5,000 IU bolus) was administered intraoperatively after vascular control was obtained, in line with routine surgical practice, to minimize thrombus propagation. Adjunctive maneuvers, such as intraoperative flushing with heparinized saline, were also employed at the discretion of the operating surgeon [18].
Postoperatively, patients were continued on systemic anticoagulation (LMWH or intravenous unfractionated heparin) with transition to oral anticoagulants or dual antiplatelet therapy, depending on comorbidities, underlying atrial fibrillation, or atherosclerotic burden.
Outcome Measures
The primary outcome of the study was a composite endpoint consisting of:
- In-hospital mortality,
- Primary patency, defined as uninterrupted patency of the treated vessel without need for further intervention, and
- Secondary patency, defined as patency restored after a reintervention following an initial occlusion.
Secondary outcomes included:
- Major amputation rates (above the ankle),
- Incidence of cerebrovascular events (e.g., stroke or transient ischemic attack) during hospitalization, and
- Length of hospital stay, measured in days from admission to discharge.
Statistical Analysis
Descriptive statistics were represented as mean (standard deviation), median (minimum–maximum), and frequency (%) for continuous and categorical variables, respectively. The normality assumption was evaluated using the Shapiro–Wilk test, boxplots, histograms, and Q–Q plots. Independent groups were compared with the independent samples t-test or the Mann–Whitney U test, depending on parametric assumptions. Associations among categorical variables were assessed with the chi-square test or Fisher’s exact test. Longitudinal changes were analyzed using repeated measures ANOVA with one fixed factor, and binary changes over time were evaluated with McNemar’s test.
Given the small sample size and the risk of type II error, effect sizes were reported alongside p-values. For continuous outcomes, we present mean differences with 95% confidence intervals (Welch method) and Cohen’s d where appropriate. For binary outcomes, group proportions are reported with Wilson 95% CIs, risk differences with Newcombe 95% CIs, and risk ratios with log (Katz) 95% CIs. Effect sizes for nonparametric tests are given as r, and categorical associations as Phi (φ). Statistical significance was set at p ≤ 0.05, but estimates with 95% CIs are emphasized to aid interpretation. All analyses were conducted using SPSS version 23 (IBM SPSS, 2015).
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Ankara University 2025000665-1 on 22/08/2025.
Results
A total of 36 patients were included in the study, of whom 24 (66.7%) underwent OSR and 12 (33.3%) received CDT. The mean age of the entire cohort was 62.56 ± 13.39 years, with a range of 32 to 100 years. Most patients were male (75%), while 25% (n=9) were female. Demographical data are shown in Table 1.
Preoperative and Postoperative Clinical Parameters
The mean preoperative ankle-brachial index (ABI) was 0.64 ± 0.43, which improved significantly to 0.93 ± 0.33, postoperatively (p < 0.001). Similarly, preoperative creatinine level was 1.12 ± 1.02 mg/dL, and increased slightly in postoperative period but it was not significant (1.22 ± 0.94 mg/dL, p = 0.103). The mean duration of hospitalization was 6.89 ± 6.18 days (median: 5 days, range: 1–32 days).
Comorbidities and Baseline Characteristics
The most prevalent comorbid conditions were hyperlipidemia (58.33%), diabetes mellitus (55.56%), hypertension (52.78%), smoking history (66.67%), and atrial fibrillation (41.67%). Other common comorbidities included atherosclerotic heart disease (38.89%), heart failure (22.22%), kidney disease (22.22%), and prior vascular interventions (47.22%).
Patency and Outcomes
Preoperatively, the popliteal artery was patent in only 13.89% of patients whereas anterior tibial artery in 8.33%, and posterior tibial artery in 22.22%. These rates demonstrated a significant postoprative improvement to 94.44%, 66.67%, and 80.56%, respectively (all p < 0.001).
Primary patency at 6 and 12 months was observed in 69.4% and 61.1% of patients, respectively. Secondary patency rates were higher, with 83.3% at 6 months and 77.8% at 12 months. The overall amputation rate was 13.9%, mortality rate was 11.1%, and one patient (2.8%) experienced a procedure-related cerebrovascular event. According to Rutherford classification, 22.2% of patients presented with Class I ischemia, while 77.8% had Class IIa ischemia (Figure 2). No patients with Rutherford class IIb or III ischemia were included in the present cohort.
Comparison Between OSR and CDT Groups
There were no statistically significant differences between the OSR and CDT groups in terms of age (60.21 ± 11.76 vs 67.25 ± 15.66 years, p = 0.139), preoperative ABI (0.63 ± 0.45 vs 0.66 ± 0.39, p = 0.540), or preoperative creatinine (1.19 ± 1.24 vs 0.99 ± 0.16 mg/dL, p = 0.120). Hospital stay was longer in the OSR group (7.29 ± 4.58 vs 6.08 ± 8.75 days, p = 0.038). The mean difference with 95% CI is illustrated in Figure 3.
Comorbidity profiles were similar, with no significant differences in hypertension, diabetes mellitus, atrial fibrillation, or smoking. Likewise, procedural outcomes did not differ significantly: amputation (12.5% OSR vs 16.7% CDT, p = 1.000), mortality (8.3% OSR vs 16.7% CDT, p = 0.588), and cerebrovascular events (0% OSR vs 8.3% CDT, p = 0.333). Effect sizes with 95% confidence intervals for binary outcomes are summarized in Figure 4.
However, given the unequal group sizes (24 vs 12) and the overall small cohort, these comparisons are underpowered. The absence of statistical significance should therefore be interpreted cautiously, as clinically meaningful differences may not have been detectable. To address type II error risk, effect sizes with 95% confidence intervals (CIs) are reported. The mean difference in hospital stay was +1.21 days (95% CI −3.43 to +5.85). At 12 months, primary patency was 66.7% vs 50.0% (risk difference +0.17; 95% CI −0.13 to +0.42; risk ratio 1.33; 95% CI 0.69–2.59), and secondary patency 79.2% vs 75.0% (risk difference +0.04; 95% CI −0.24 to +0.32; risk ratio 1.06; 95% CI 0.72–1.57). For major amputation and in-hospital mortality, 95% CIs were wide and included clinically relevant effects, again underscoring limited power. At 12 months, primary patency was 66.7% vs 50.0% and secondary patency 79.2% vs 75.0% for OSR and CDT, respectively. Figure 5 illustrates the Kaplan–Meier survival curve comparing cumulative survival rates between the two groups during the 12-month follow-up period log-rank p =0.653).
Thrombolytic Infusion
In the CDT cohort, the duration of thrombolytic infusion and the total administered dose of alteplase demonstrated considerable variability. The median infusion duration was 24 hours (range: 15–32 hours), while the median total dose was 19.5 mg (range: 12–28 mg). Most patients received infusion periods of 15 to 24 hours, with total doses generally aligned with the treatment duration, reflecting standardized yet patient-tailored dosing strategies. Figure 6 presents individual patient data, showing that although infusion times tended to cluster within the 24-hour range, total doses exhibited greater variability, likely due to adjustments for body weight, clinical response, and bleeding risk. These findings underscore the individualized nature of CDT protocols in real-world practice and highlight the importance of flexible dosing regimens tailored to patient characteristics.
Fibrinogen Levels
Peri-procedural fibrinogen levels significantly decreased after intervention compared with baseline values (3.48 ± 1.33 g/L vs. 2.42 ± 1.36 g/L, p = 0.003), with a large effect size (r = 0.861). This reduction was more pronounced in patients undergoing CDT, reflecting the pharmacodynamic effect of thrombolysis. Despite the decline, no major bleeding events were observed, suggesting that close monitoring of fibrinogen remains important for procedural safety [19,20,21].
Longitudinal Analysis
Repeated measures ANOVA showed a significant improvement in ABI over time (F = 16.549, p < 0.001), but no significant interaction between treatment group and time (F = 0.053, p = 0.819), suggesting that both OSR and CDT led to comparable improvements in ABI. No significant differences were found over time or between groups for creatinine levels.
Arterial Segment Patency Comparison
Within-group analysis showed significant improvement in arterial patency (popliteal, anterior tibial, and posterior tibial arteries) from preoperative to postoperative assessments in both groups. However, between-group comparisons of postoperative patency rates did not reach statistical significance.
Discussion
In this retrospective single-center analysis comparing OSR and CDT in patients with early-stage ALI (Rutherford I–IIa), both modalities demonstrated comparable short and mid-term outcomes. Primary and secondary patency rates at 6 and 12 months did not differ significantly between groups, consistent with prior studies reporting similar limb salvage and survival outcomes in early ischemia [22,23]. This finding supports the role of CDT as a clinically valid alternative to OSR when applied in appropriately selected patients [24].
Our results align with previous randomized trials, meta-analyses, and large-scale registries that have compared CDT and OSR. Landmark trials such as STILE and TOPAS demonstrated similar limb salvage rates between modalities, albeit with higher bleeding risks in the CDT arm [22,25]. Meta-analyses, including those by Enezate et al. and Veenstra et al., confirmed that while OSR achieves immediate reperfusion, CDT avoids surgical trauma and is particularly advantageous in patients with higher operative risk [15,26]. More contemporary evidence from Yang et al. and Kolte et al. reported no differences in mortality, amputation, or long-term patency between endovascular and surgical approaches [13,23]. Systematic reviews and guideline recommendations also reinforce that both modalities remain valid, stage-dependent options in modern practice [12,26]. These findings, together with recent data from large national cohorts (e.g., Ozawa et al., Ugwumba et al.), are summarized in Table 2, which highlights the overall consistency of outcomes across diverse patient populations and practice settings [1,6].
Beyond limb-related endpoints, both treatment strategies significantly improved ABI, underscoring their efficacy in restoring perfusion during early ALI [27]. Importantly, renal function remained stable in our CDT cohort, despite theoretical concerns about contrast-induced nephropathy. In addition, we observed a significant postoperative reduction in fibrinogen levels, particularly among patients undergoing CDT. This decline is consistent with the pharmacological effects of thrombolytic therapy and highlights the importance of peri-procedural coagulation monitoring. While no major bleeding complications occurred in our cohort, systematic fibrinogen assessment may help optimize CDT safety, in line with current guideline recommendations [12,28]. This observation is consistent with contemporary evidence showing that CDT, when accompanied by adequate hydration and careful patient selection, is generally safe with respect to kidney function (9, 10, 14). Moreover, the ABI improvements observed in elderly patients treated with CDT highlight its feasibility in higher-risk populations, in line with reports that endovascular approaches can achieve meaningful hemodynamic gains across diverse age groups [1,4]. Collectively, these findings support CDT not only as an effective but also as a safe therapeutic option when peri-procedural protocols are optimized. Our experience, in line with prior reports, suggests that CDT can be performed with acceptable safety and efficacy, provided peri-procedural protocols are stringently optimized [7].
Length of hospitalization was modestly longer in the OSR cohort, reflecting the invasiveness of surgical intervention and associated perioperative management. Although the absolute difference in median stay was approximately one day in our series, even small reductions may have system-level implications in high-volume centers [29]. Contemporary comparative studies report shorter hospital stays with endovascular/CDT strategies relative to OSR, albeit with the need for close monitoring during thrombolysis [6,13]. From a broader perspective, shorter admissions can improve bed turnover and patient throughput; however, effects on cost are mixed—some datasets show higher index-hospitalization costs with endovascular approaches despite shorter length of stay, underscoring the need for formal cost-effectiveness analyses [9,13].
Limitations
This study is limited by its retrospective, non-randomized design and small sample size (n = 36), which reduce statistical power and introduce the risk of type II error. Treatment allocation was based on physician discretion, introducing potential selection bias, as patients at higher operative risk or with unfavorable anatomy were more likely directed toward CDT. Confidence intervals for outcomes remained wide, underscoring the need for cautious interpretation of apparent equivalence. Furthermore, functional outcomes, and quality-of-life measures were not systematically assessed. Future multicenter prospective studies with standardized CDT protocols, real-time coagulation monitoring, and cost-effectiveness analyses are warranted to optimize treatment algorithms and improve patient-centered care in ALI.
Conclusion
In this retrospective single-center study of patients with early-stage ALI (Rutherford I–IIa), CDT and OSR demonstrated comparable short- and mid-term outcomes in terms of primary and secondary patency, amputation, and mortality. Both modalities significantly improved ABI and arterial patency, with stable renal function observed across groups. Although OSR was associated with a slightly longer hospital stay, CDT required careful peri-procedural monitoring due to thrombolysis-related fibrinogen depletion. These findings support the use of both approaches as valid, stage-dependent treatment strategies in early ALI, with CDT representing a safe and effective minimally invasive alternative when applied in appropriately selected patients. This is further supported by the 10-year single-center series from Konstantinou et al., which demonstrated lower mortality and prolonged survival among patients undergoing endovascular therapy compared to those treated with open surgery [8]. Larger prospective studies are warranted to validate these findings and inform standardized treatment protocols.
References
- Ugwumba, L.; Mannan, F.; El-Sayed, T.; Saratzis, A.; Nandhra, S. A Systematic Review of Modern Endovascular Techniques Compared to Surgery for Acute Limb Ischaemia. Ann. Vasc. Surg. 2025, 119, 1–10. [CrossRef]
- Stoner, M.C.; Calligaro, K.D.; Chaer, R.A.; Dietzek, A.M.; Farber, A.; Guzman, R.J.; Hamdan, A.D.; Landry, G.J.; Yamaguchi, D.J. Reporting standards of the Society for Vascular Surgery for endovascular treatment of chronic lower extremity peripheral artery disease. J. Vasc. Surg. 2016, 64, e1–e21. [CrossRef]
- Obara H, Matsubara K, Kitagawa Y. Acute Limb Ischemia. Ann Vasc Dis. 2018;11(4):443-8.
- Olinic, D.-M.; Stanek, A.; Tătaru, D.-A.; Homorodean, C.; Olinic, M. Acute Limb Ischemia: An Update on Diagnosis and Management. J. Clin. Med. 2019, 8, 1215. [CrossRef]
- Choi, E.; Kwon, T.W. Endovascular Treatment versus Open Surgical Repair for Isolated Iliac Artery Aneurysms. Vasc. Spéc. Int. 2024, 40, 31. [CrossRef]
- Ozawa T, Yanishi K, Fujioka A, Seki T, Zen K, Matoba S. Editor’s Choice - Comparison of Clinical Outcomes in Patients with Acute Lower Limb Ischaemia Undergoing Endovascular Therapy and Open Surgical Revascularisation: A Large Scale Analysis in Japan. Eur J Vasc Endovasc Surg. 2024;68(6):748-56.
- Morrison, H. Catheter-Directed Thrombolysis for Acute Limb Ischemia. Semin. Interv. Radiol. 2006, 23, 258–269. [CrossRef]
- Konstantinou, N.; Argyriou, A.; Dammer, F.; Bisdas, T.; Chlouverakis, G.; Torsello, G.; Tsilimparis, N.; Stavroulakis, K. Outcomes After Open Surgical, Hybrid, and Endovascular Revascularization for Acute Limb Ischemia. J. Endovasc. Ther. 2023, 32, 1499–1507. [CrossRef]
- Maheta, D.; Desai, D.; Agrawal, S.P.; Dani, A.; Frishman, W.H.; Aronow, W.S.M. Acute Limb Ischemia Management and Complications: From Catheter-Directed Thrombolysis to Long-Term Follow-up. Cardiol. Rev. 2024. [CrossRef]
- Butt, T.; Lehti, L.; Apelqvist, J.; Gottsäter, A.; Acosta, S. Contrast-Associated Acute Kidney Injury in Patients with and without Diabetes Mellitus Undergoing Computed Tomography Angiography and Local Thrombolysis for Acute Lower Limb Ischemia. Vasc. Endovasc. Surg. 2021, 56, 151–157. [CrossRef]
- Lind, B.; Morcos, O.; Ferral, H.; Chen, A.; Aquisto, T.; Lee, S.; Lee, C.J. Endovascular Strategies in the Management of Acute Limb Ischemia. Vasc. Spéc. Int. 2019, 35, 4–9. [CrossRef]
- Björck, M.; Earnshaw, J.J.; Acosta, S.; Gonçalves, F.B.; Cochennec, F.; Debus, E.S.; Hinchliffe, R.; Jongkind, V.; Koelemay, M.J.W.; Menyhei, G.; et al. Editor's Choice – European Society for Vascular Surgery (ESVS) 2020 Clinical Practice Guidelines on the Management of Acute Limb Ischaemia. Eur. J. Vasc. Endovasc. Surg. 2020, 59, 173–218. [CrossRef]
- Kolte D, Kennedy KF, Shishehbor MH, Mamdani ST, Stangenberg L, Hyder ON, et al. Endovascular Versus Surgical Revascularization for Acute Limb Ischemia: A Propensity-Score Matched Analysis. Circ Cardiovasc Interv. 2020;13(1):e008150.
- Gunes Y, Sincer I, Erdal E. Catheter-directed intra-arterial thrombolysis for lower extremity arterial occlusions. Anatol J Cardiol. 2019;22(2):54-9.
- Veenstra, E.B.; van der Laan, M.J.; Zeebregts, C.J.; de Heide, E.-J.; Kater, M.; Bokkers, R.P. A systematic review and meta-analysis of endovascular and surgical revascularization techniques in acute limb ischemia. J. Vasc. Surg. 2020, 71, 654–668.e3. [CrossRef]
- Hoebink, M.; Steunenberg, T.A.; Roosendaal, L.C.; Wiersema, A.M.; Hamer, H.M.; Yeung, K.K.; Jongkind, V. Ability of Activated Clotting Time Measurements to Monitor Unfractionated Heparin Activity During NonCardiac Arterial Procedures. Ann. Vasc. Surg. 2024, 110, 460–468. [CrossRef]
- Nair, A.; Maan, B.S.; El-Sayed, T. 460 Exploring Optimal Antithrombotic Strategies for Acute Limb Ischaemia: A Comprehensive Review. Br. J. Surg. 2024, 111. [CrossRef]
- Durran, A.C.; Watts, C. Current Trends in Heparin Use During Arterial Vascular Interventional Radiology. Cardiovasc. Interv. Radiol. 2012, 35, 1308–1314. [CrossRef]
- Sista, A.K. Fibrinogen Monitoring during Catheter-Directed Thrombolysis for Pulmonary Embolism: Can It Be Cleaved from Our Practice?. J. Vasc. Interv. Radiol. 2020, 31, 1290–1291. [CrossRef]
- Kaufman, C.; Kinney, T.; Quencer, K. Practice Trends of Fibrinogen Monitoring in Thrombolysis. J. Clin. Med. 2018, 7, 111. [CrossRef]
- Dorey, T.; Kong, D.; Lobo, W.; Hanlon, E.; Abramowitz, S.; Turcotte, J.; Jeyabalan, G. Plasma Fibrinogen Change as a Predictor of Major Bleeding During Catheter-Directed Thrombolysis. Ann. Vasc. Surg. 2023, 99, 262–271. [CrossRef]
- Ouriel, K.; Veith, F.J.; Sasahara, A.A. A Comparison of Recombinant Urokinase with Vascular Surgery as Initial Treatment for Acute Arterial Occlusion of the Legs. New Engl. J. Med. 1998, 338, 1105–1111. [CrossRef]
- Yang, P.-K.; Su, C.-C.; Hsu, C.-H. Clinical outcomes of surgical embolectomy versus catheter-directed thrombolysis for acute limb ischemia: a nationwide cohort study. J. Thromb. Thrombolysis 2021, 53, 517–522. [CrossRef]
- Pascoe, H.M.; Robertson, D. Catheter-directed thrombolysis for acute limb ischaemia: An audit. Australas. Med J. 2014, 7. [CrossRef]
- Results of a prospective randomized trial evaluating surgery versus thrombolysis for ischemia of the lower extremity. The STILE trial. Ann Surg. 1994;220(3):251-66; discussion 66-8.
- Enezate, T.H.; Omran, J.; Mahmud, E.; Patel, M.; Abu-Fadel, M.S.; White, C.J.; Al-Dadah, A.S. Endovascular versus surgical treatment for acute limb ischemia: a systematic review and meta-analysis of clinical trials. Cardiovasc. Diagn. Ther. 2017, 7, 264–271. [CrossRef]
- Jarosinski, M.C.; Li, K.; Andraska, E.A.; Reitz, K.M.; Liang, N.L.; Chaer, R.; Tzeng, E.; Sridharan, N.D. Comparison of open and endovascular therapy for infrainguinal acute limb ischemia in the era of percutaneous thrombectomy. J. Vasc. Surg. 2025, 82, 952–960.e3. [CrossRef]
- Doelare, S.A.; Oukrich, S.; Ergin, K.; Jongkind, V.; Wiersema, A.M.; Lely, R.J.; Ebben, H.P.; Yeung, K.K.; Hoksbergen, A.W. Major Bleeding During Thrombolytic Therapy for Acute Lower Limb Ischaemia: Value of Laboratory Tests for Clinical Decision Making, 17 Years of Experience. Eur. J. Vasc. Endovasc. Surg. 2022, 65, 398–404. [CrossRef]
- Decker, J.A.; Helmer, M.; Bette, S.; Schwarz, F.; Kroencke, T.J.; Scheurig-Muenkler, C. Comparison and Trends of Endovascular, Surgical and Hybrid Revascularizations and the Influence of Comorbidity in 1 Million Hospitalizations Due to Peripheral Artery Disease in Germany Between 2009 and 2018. Cardiovasc. Interv. Radiol. 2022, 45, 1472–1482. [CrossRef]
Figure 1.
Study consort diagram of patient selection and treatment allocation.
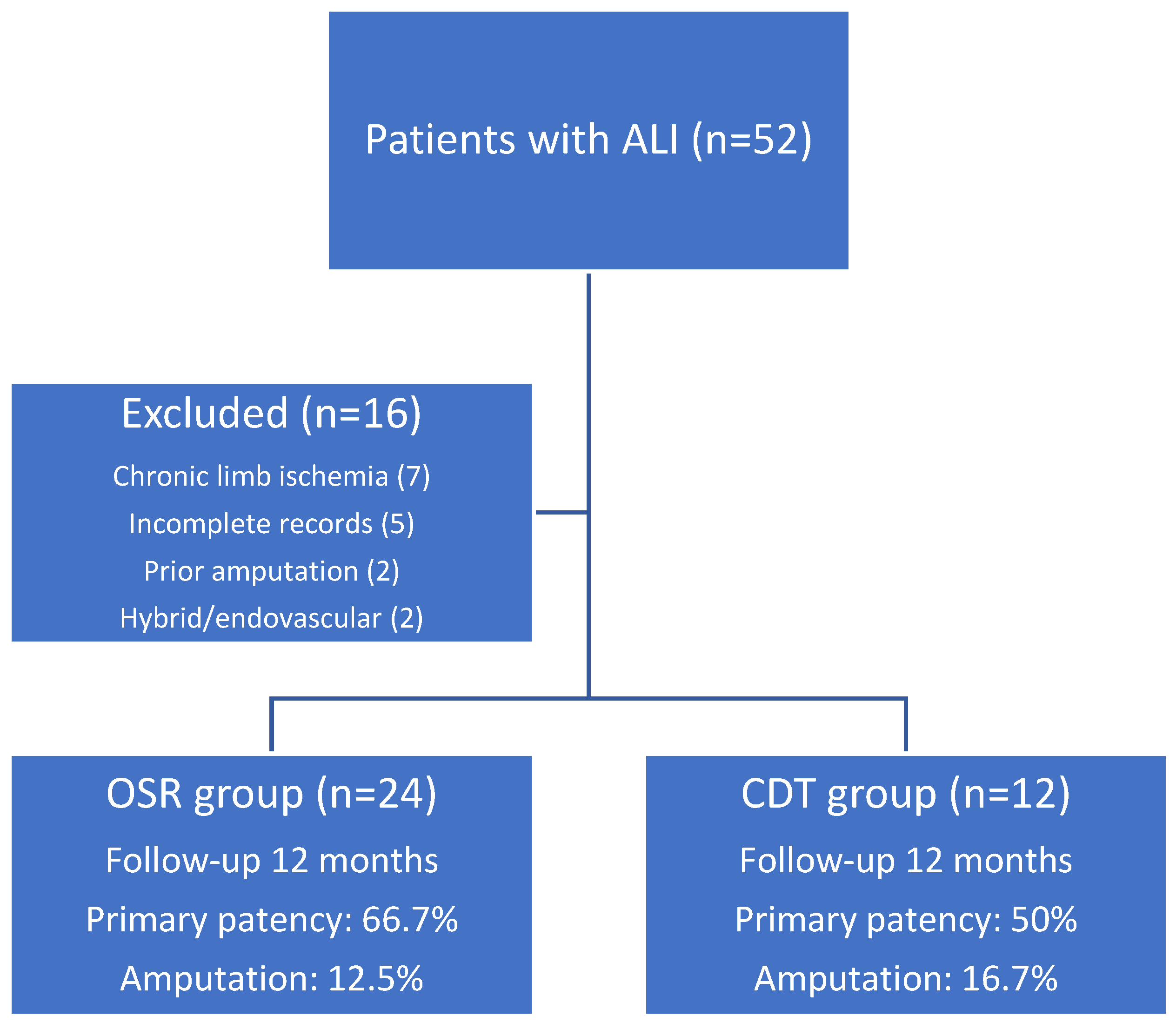
Figure 2.
Primary and secondary patency rates at 6 and 12 months following OSR and CDT.
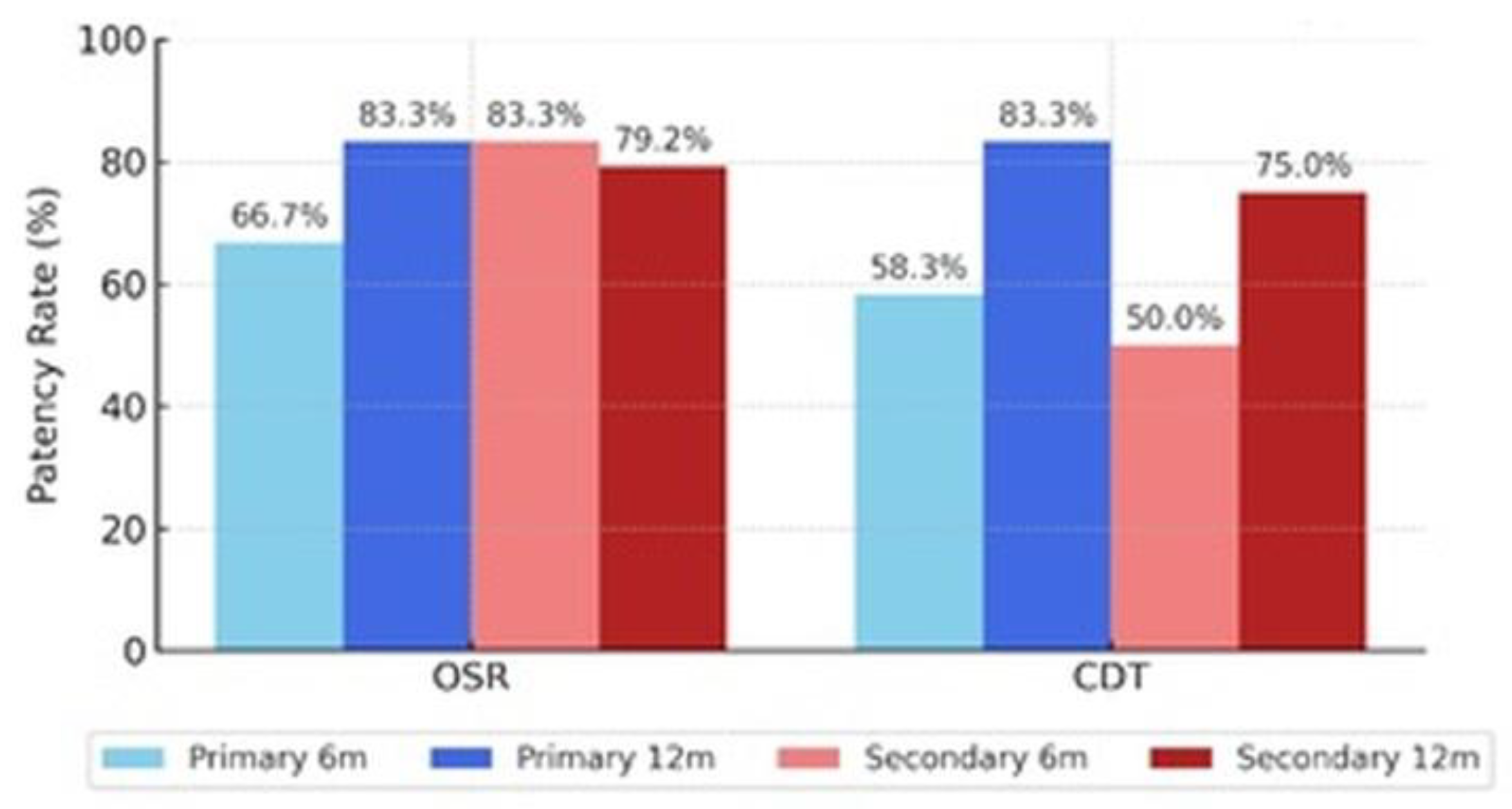
Figure 3.
Mean difference in hospital stay (OSR – CDT) with 95% confidence interval.
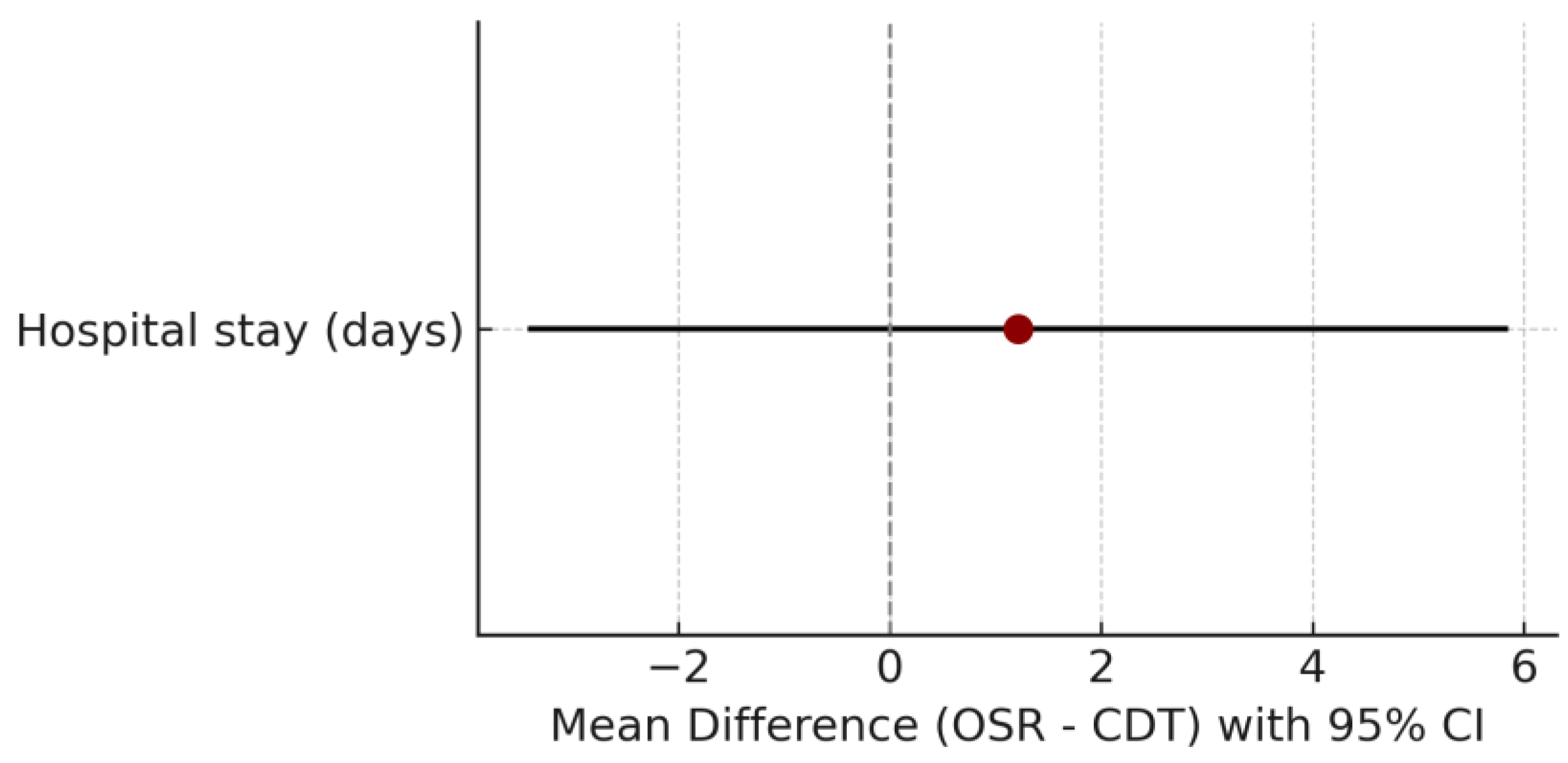
Figure 4.
Risk ratios with 95% confidence intervals for binary outcomes (primary and secondary patency at 12 months, amputation, mortality, cerebrovascular events).
Figure 4.
Risk ratios with 95% confidence intervals for binary outcomes (primary and secondary patency at 12 months, amputation, mortality, cerebrovascular events).
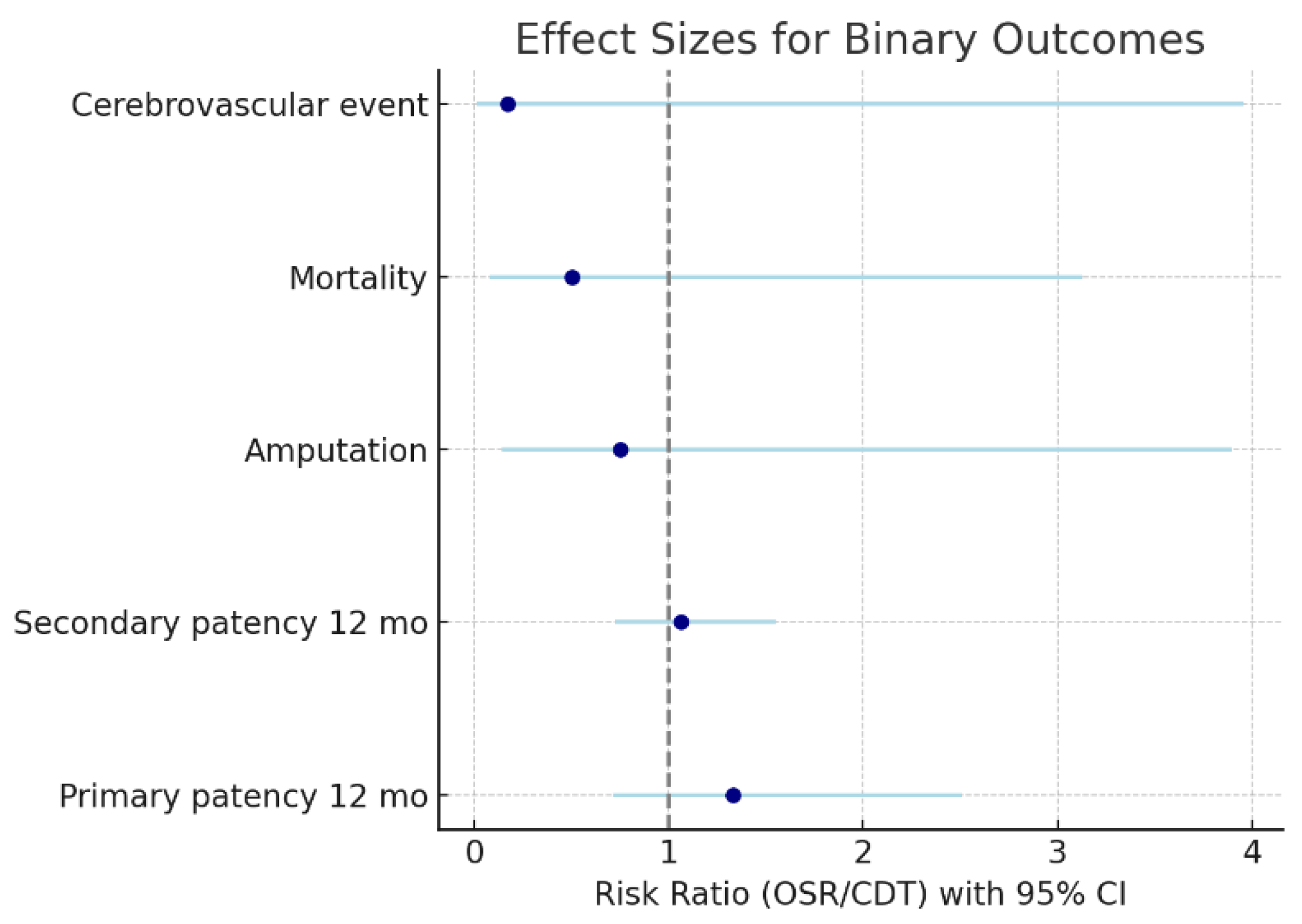
Figure 5.
Kaplan–Meier survival curve comparing cumulative survival rates between the OSR and CDT groups during the 12-month follow-up period.
Figure 5.
Kaplan–Meier survival curve comparing cumulative survival rates between the OSR and CDT groups during the 12-month follow-up period.
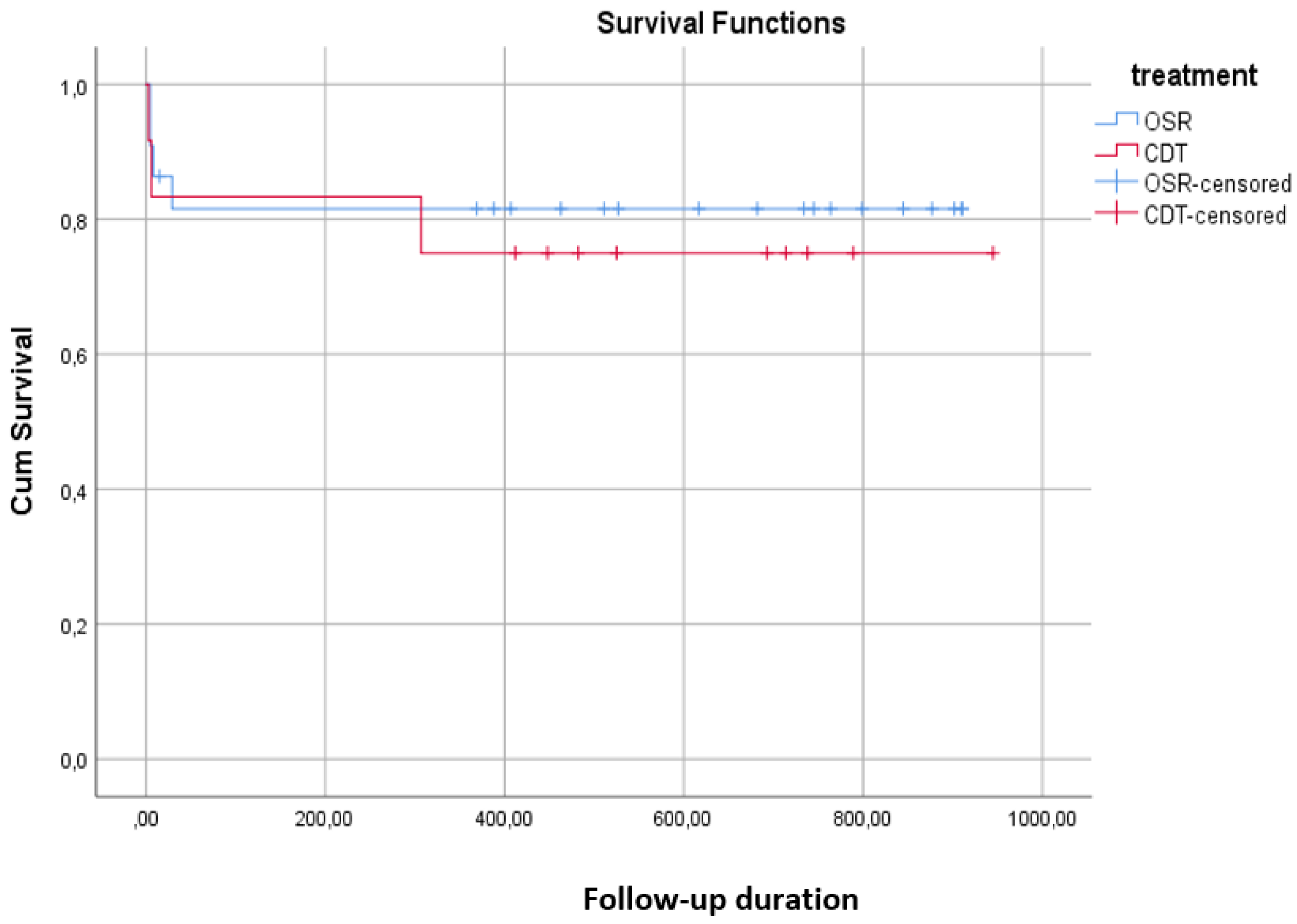
Figure 6.
Thrombolytic infusion duration and total dose administered per patient undergoing CDT.
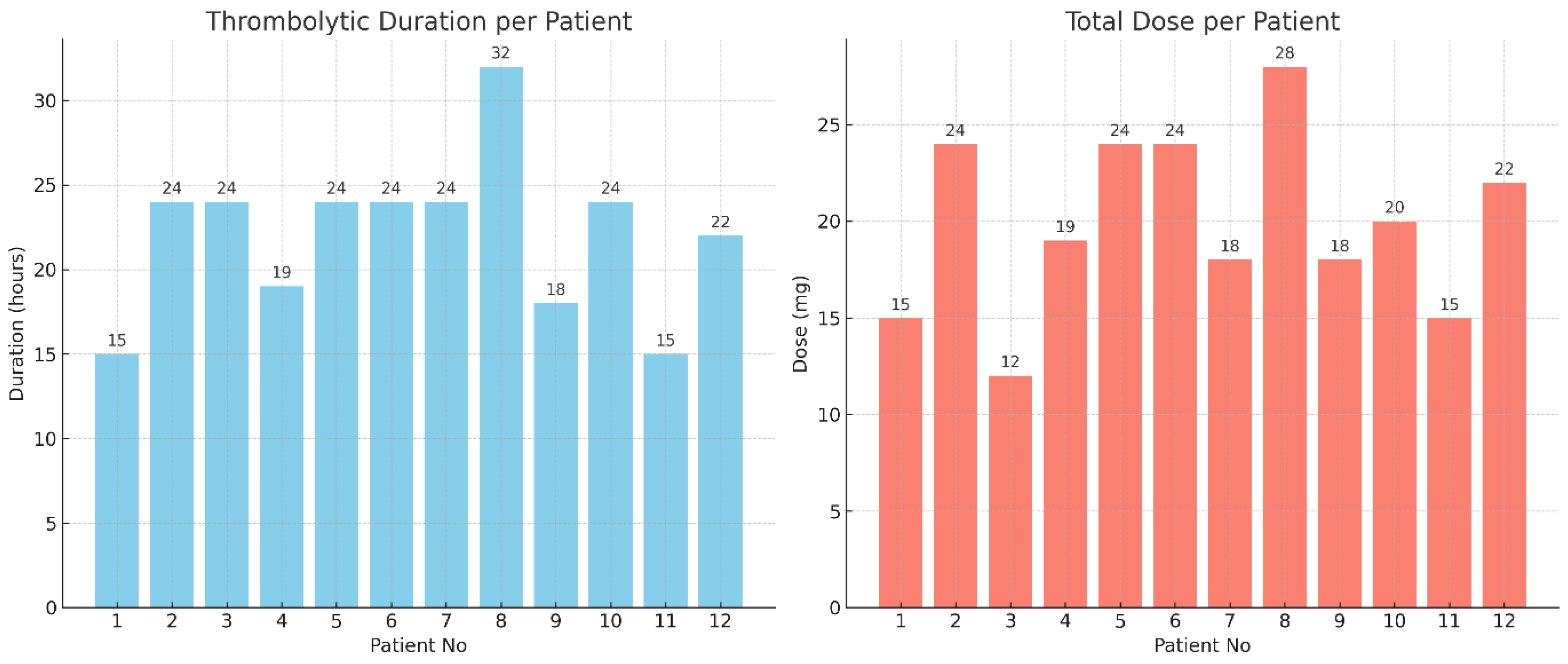

Table 1.
Baseline demographic and clinical characteristics of patients with ALI undergoing OSR or CDT. Data are presented as mean ± standard deviation, median (minimum–maximum), or n (%).
Table 1.
Baseline demographic and clinical characteristics of patients with ALI undergoing OSR or CDT. Data are presented as mean ± standard deviation, median (minimum–maximum), or n (%).
| Variable | OSR | CDT |
| Age | 60.21±11.76 61.00 (32.00 – 78.00) |
67.25±15.66 67.50 (50.00 – 100.00) |
| Gender, K | 7 (29.17) | 2 (16.67) |
| Hypertension | 13 (54.17) | 6 (50.00) |
| Diabetes Mellitus | 14 (58.33) | 6 (50.00) |
| Heart Failure | 5 (20.83) | 3 (25.00) |
| Coronary Artery Disease | 10 (41.67) | 4 (33.33) |
| Stroke | 4 (16.67) | 2 (16.67) |
| Atrial Fibrillation | 8 (33.33) | 7 (58.33) |
| Hyperlipidemia | 14 (58.33) | 7 (58.33) |
| COPD | 4 (16.67) | 2 (16.67) |
| Renal Disease | 4 (16.67) | 4 (33.33) |
| Smoking | 18 (75.00) | 6 (50.00) |
| Previous Vascular Intervention | 13 (54.17) | 4 (33.33) |
| Rutherford Class (I-IIa) | 20 (83.33) | 8 (66.67) |
Table 2.
Summary of landmark trials, meta-analyses, large cohort studies, guidelines, and the present study comparing CDT and OSR in ALI.
Table 2.
Summary of landmark trials, meta-analyses, large cohort studies, guidelines, and the present study comparing CDT and OSR in ALI.
| Study (Year) | Design / Setting | Population (ALI stage) | Interventions | Primary/Key Outcomes | Main Findings | Notes / Limitations |
| TOPAS (Ouriel et al., 1998, NEJM) | RCT, multicenter | Acute arterial occlusion (mixed) | CDT (urokinase) vs Surgery | Limb salvage, complications | Comparable limb salvage; higher bleeding with thrombolysis | Early protocols; outdated drugs/devices |
| STILE (Comerota et al., 1996, JVS) | Prospective randomized | Acute limb ischemia | CDT vs Operative therapy | Limb salvage, patency, bleeding | Similar limb salvage; increased bleeding in CDT | Older technology; limited generalizability |
| Enezate et al., 2017 (Cardiovasc Diagn Ther) | Meta-analysis | ALI (pooled) | Endovascular vs Surgery | Mortality, amputation, recurrent ischemia (1–12 mo) | No significant differences; trend toward lower short-term amputation with endovascular | Heterogeneity across included studies |
| Veenstra et al., 2020 (EJVES) | Systematic review & meta-analysis | ALI | CDT vs Surgery | Composite clinical endpoints | Comparable endpoints when appropriately selected | Supports individualized treatment selection |
| Yang et al., 2022 (J Thromb Thrombolysis) | Large cohort (Taiwan) | ALI | CDT vs Surgical thrombectomy | In-hospital mortality, amputation | No difference in mortality or amputation | Observational; potential selection bias |
| Kolte et al., 2020 (Circ Cardiovasc Interv) | Propensity-matched analysis | ALI | Endovascular vs Surgical | Limb salvage, mortality | Better in-hospital outcomes for endovascular therapy | Residual confounding possible |
| ESVS Guideline (Björck et al., 2020) | Guideline synthesis | ALI | — | Evidence-based recommendations | Both OSR and CDT valid depending on stage/anatomy | Emphasizes expertise & timely reperfusion |
| Ozawa et al., 2024 (EJVES, Japan) | Large-scale analysis | Acute lower-limb ischemia | Endovascular vs OSR | Clinical outcomes (national dataset) | Comparable results in modern practice | Administrative dataset; limited detail |
| Ugwumba et al., 2025 (Ann Vasc Surg) | Systematic review | Modern endovascular vs Surgery | Contemporary CDT vs OSR | Comparative effectiveness | No consistent superiority; selection matters | Highlights need for standardized protocols |
| Maheta et al., 2024 (Cardiol Rev) | Narrative review | ALI | Spectrum of CDT | Management/complications | Modern CDT feasible with careful monitoring | Bleeding/renal risks remain |
| This study (2019–2023) | Retrospective cohort (single-center) | Rutherford I–IIa (n=36; OSR 24 vs CDT 12) | OSR vs CDT (alteplase; heparin) | 6–12 mo patency, amputation, mortality, LOS | Comparable outcomes; OSR longer LOS; renal function stable | Small sample, non-randomized, no fibrinogen monitoring |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



