
Submitted:
15 October 2025
Posted:
17 October 2025
You are already at the latest version
Abstract
Background/Purpose: Reproductive health and fertility outcomes are essential but often overlooked aspects of occupational well-being. Organizational dysfunction, demanding workloads, and limited workplace accommodations may negatively affect fertility, while supportive policies and inclusive cultures can mitigate risks. This review aimed to map current evidence on these relationships and their economic consequences.
Methodology/Approach: A scoping review was conducted using PCC (Population–Concept–Context) framework. Systematic searches across multiple databases identified 28 eligible studies, including quantitative, qualitative, and mixed-method designs, spanning different sectors and international contexts.
Findings: Four main domains emerged: shift work and circadian disruption, organiza-tional stress and burnout, workplace flexibility and accommodations, and fertility-related policies and organizational support. Hazardous working conditions, long hours, and psychosocial stressors were consistently associated with impaired fertility, reduced fe-cundability, and pregnancy complications. Conversely, flexible scheduling, fertility bene-fits, and supportive organizational cultures were linked to improved well-being, retention, and productivity.
Originality/Value: This review integrates evidence across occupational health, organiza-tional psychology, and labor economics, offering a comprehensive overview of workplace influences on reproductive health. It highlights gaps in equity and representa-tion—particularly for men, LGBTQ+ employees, and workers in precarious jobs—and calls for longitudinal, interdisciplinary, and intervention-based studies to inform effective workplace policies.
Keywords:
reproductive health
; workplace accommodations
; organizational dysfunction
; fertility outcomes
; occupational well-being
1. Introduction
Although the intersection of occupational conditions and reproductive health has received growing attention in the last two decades, the literature remains fragmented across disciplines, and limited effort has been made to systematically assess the dual impact of organizational dysfunction on both individual health and organizational-level economic outcomes.
Research suggests that various occupational and organizational factors can negatively impact employees’ reproductive health and fertility outcomes. Exposure to harmful substances such as organic solvents, heavy metals, and pesticides has been linked to impaired fertility in both men and women (Baranski, 1993; Kumar, 2004). Additionally, physical stressors like shift work, prolonged standing, and heavy lifting have been associated with increased risks of spontaneous abortion and preterm birth (Gold & Tomich, 1994). Women exposed to such harmful conditions face heightened risks of pregnancy complications and childbirth disorders (Babanov et al., 2019), while organizational practices in the fertility treatment sector may inadvertently reinforce masculine norms, particularly surrounding male infertility (Cervi & Knights, 2022).
While previous research has explored individual occupational hazards or workplace accommodations in isolation, a comprehensive synthesis connecting these factors to both reproductive health trajectories and organizational productivity remains lacking. Moreover, economic outcomes, though frequently mentioned, are rarely analyzed systematically or given equal analytical weight alongside health-related consequences.
Although findings are occasionally inconsistent, there is sufficient evidence to support the implementation of protections for pregnant workers against well-documented occupational hazards (Figa-Talamanca, 2006). However, some scholars argue that occupational exposures may play a limited role compared to other contributing factors such as increasing maternal age (Winker & Rüdiger, 2005). Even so, research continues to emphasize the importance of addressing these risks.
Workplace conditions extend beyond physical hazards. Flexibility bias, for example, is associated with a range of negative health outcomes, including depression and sleep disturbances (Cech & O’Connor, 2017). Many chemicals used in workplaces have not been adequately tested for their reproductive effects, exposing workers to unknown risks (Rim, 2017). The lack of family-responsive policies, particularly in smaller and non-unionized firms, has been linked to increased job-family stress (GLASS & FUJIMOTO, 1995). To mitigate these risks, experts recommend enhanced protective measures, improved policy design, and continued research into occupational reproductive hazards (Cox et al., 2000; GIACOLA, 1992; Sonika, 2020; Virgillito et al., 2025).
Inadequate organizational support for fertility and reproductive health also has significant economic and productivity consequences for employers. Infertility treatments often involve high out-of-pocket expenses, sometimes resulting in catastrophic health expenditures for employees (Dyer & Patel, 2012). Conversely, organizations offering fertility-related benefits have reported improved employee retention, recruitment, and morale (Isaacs, 2008). Nearly 30% of employees facing fertility challenges report decreased productivity, with LGBTQ+ individuals disproportionately affected (Steyn et al., 2024). Endometriosis alone results in an average annual cost of €9579 per affected woman, with €6298 attributable to productivity losses (Simoens et al., 2012). The economic burden of infertility is comparable to that of other chronic diseases (Simoens et al., 2012), and male reproductive disorders linked to endocrine-disrupting chemical exposure are estimated to cost nearly €15 billion annually within the EU (Hauser et al., 2015).
Positive organizational practices, on the other hand, can support employee well-being and fertility outcomes. Access to childcare leave has been associated with increased first-birth intentions, while multiple family-supportive workplace benefits correlate with higher intentions for second births (Kim & Parish, 2020). Fertility-friendly policies, such as flexible scheduling and leave for medical appointments, can improve the physical and emotional health of employees navigating fertility challenges (Steyn et al., 2022, 2024). Paid maternity leave has also been linked to improved retention of health insurance coverage postpartum (Jou et al., 2016), and fertility-related quality of life is influenced by job demands, co-worker support, and access to time off (Maeda et al., 2022). However, many workplaces still lack adequate fertility support, particularly for LGBTQ+ and BAME employees (Steyn et al., 2024). Comprehensive fertility benefits may represent not only a matter of health equity but also a competitive advantage in talent recruitment and retention (De Oliveira Trigo et al., 2023; Steyn et al., 2024).
Finally, the role of stigma and organizational culture must not be overlooked. Perceived stigma around fertility issues is associated with lower rates of disclosure, diminished social support, and heightened psychological distress (Slade et al., 2007). Employees often fear discrimination or career repercussions, leading them to withhold information about fertility or mental health needs (Toth & Dewa, 2014; van den Akker et al., 2017). In contrast, supportive organizational cultures that encourage disclosure are linked to improved well-being and job performance (Lyubykh et al., 2025). Policies that facilitate open communication and provide emotional support can reduce fertility-related distress (Payne et al., 2018). Nevertheless, many employees still struggle to balance work responsibilities with fertility treatments, leading to reduced productivity and hindered career progression (Steyn et al., 2022, 2024). Disclosure decisions remain complex and are shaped by privacy concerns, stigma, and the need for workplace accommodations (Nachtigall et al., 1997; van den Akker et al., 2017).
As workforce demographics shift and fertility challenges become more prevalent, especially among professionals in high-demand roles, the need to address reproductive health as a dimension of occupational well-being has become increasingly urgent. This includes understanding not only health-related outcomes but also organizational costs, such as productivity losses, turnover, and presenteeism.
Given the complex interplay between organizational dynamics, reproductive health, and economic performance, a comprehensive review of the existing literature is essential to understand the extent and mechanisms of these relationships. This scoping review aims to synthesize empirical findings and theoretical contributions from multidisciplinary perspectives, including occupational health, organizational behavior, gender studies, and health economics. By examining both the detrimental effects of organizational dysfunction and the potential benefits of supportive workplace policies, the review seeks to identify critical knowledge gaps and inform evidence-based strategies for improving employee well-being and organizational outcomes.
2. Materials and Methods
This scoping review was conducted in accordance with the methodological framework proposed by Arksey and O’Malley (Arksey & O’Malley, 2005), further refined by Levac et al. (Levac et al., 2010) and the Joanna Briggs Institute (Peters et al., 2021). The reporting of results follows the PRISMA Extension for Scoping Reviews (PRISMA-ScR) guidelines (Tricco et al., 2018).
2.1. Objectives and Research Questions
The primary objective of this scoping review is to map the existing literature on the impact of organizational dysfunction and inadequate workplace accommodations on fertility outcomes and reproductive health, and to explore the associated economic and productivity costs for businesses. The review specifically addresses the following research questions:
- How does organizational dysfunction affect employees’ fertility outcomes and reproductive health?
- What organizational factors most significantly hinder reproductive health in the workplace?
- What are the economic and productivity costs associated with insufficient support for fertility?
- Which workplace accommodations and policies have been shown to improve fertility-related outcomes?
- How do stigma and organizational culture influence employees’ willingness to disclose or seek support?
2.2. Eligibility Criteria
To ensure methodological transparency and to clearly define the scope of the review, inclusion and exclusion criteria were structured using the PCC (Population–Concept–Context) framework, as recommended by the Joanna Briggs Institute for scoping reviews (Peters et al., 2021; Pollock et al., 2022). This approach enabled the systematic identification of relevant literature across multiple disciplines, including occupational medicine, organizational psychology, public health, and labor economics (see Table 1).
This framework guided the formulation of clear inclusion and exclusion parameters, ensuring the review remained focused while capturing a broad range of relevant studies across disciplines.
2.3. Search Strategy
A comprehensive and systematic search strategy was developed to identify relevant peer-reviewed and grey literature across multiple disciplines, including occupational health, organizational behavior, public health, and labor economics. The search aimed to capture studies examining the intersection of workplace conditions, organizational dysfunction, and reproductive health.
Electronic searches were conducted in the following databases: PubMed, Scopus, Web of Science, PsycINFO, and CINAHL. Additionally, Google Scholar was used to screen grey literature and academic reports. The search covered publications from January 1990 to June 2025, in line with the increased scholarly interest in reproductive health and workplace equity during this period. Only studies published in English were included.
The search strategy combined both controlled vocabulary terms (e.g., MeSH) and free-text keywords, adapted for each database. Boolean operators (AND, OR) and truncation symbols were employed to enhance the sensitivity and specificity of the results. A full list of search terms and strategies for each database is available in Supplementary Table S1.
2.4. Study Selection
Following the completion of the search process, all retrieved references were imported into Rayyan software (rayyan, 2024), where duplicate entries were identified and removed.
The study selection proceeded in two sequential phases:
- Title and Abstract Screening: Two reviewers independently screened all titles and abstracts to determine initial relevance according to the inclusion and exclusion criteria outlined in the PCC framework (see Table 1). Studies that did not meet the basic eligibility requirements were excluded at this stage.
- Full-Text Review: Full texts of potentially eligible studies were retrieved and assessed for inclusion. Discrepancies between reviewers were resolved through discussion.
A PRISMA-ScR flow diagram was used to document the study selection process, including the number of records identified, screened, excluded, and included at each stage. Reasons for exclusion during the full-text review were recorded to ensure transparency.
The final selection included studies that directly addressed the relationship between organizational dysfunction, workplace accommodations, and reproductive health outcomes.
3. Results
A comprehensive search across several electronic databases initially yielded 461 records. The PRISMA flowchart (Figure 1) details the process of selecting relevant publications at each step of the review. After eliminating 267 duplicate entries and other 6 ineligible paper, 188 records advanced to the screening phase. During this stage, 140 records were excluded based on their failure to meet the established inclusion criteria. This left 48 articles to be further assessed for eligibility. In the final phase, 28 studies were included in the quali/quantitative synthesis.
3.1. Characteristics of Included Studies
The 28 included studies (Table 2) employed a variety of methodological designs, including quantitative surveys, retrospective and prospective cohort studies, qualitative interviews, and mixed-methods approaches. Sample sizes ranged from small qualitative cohorts (e.g., 12–30 participants) to large-scale surveys involving thousands of respondents.
The populations examined were predominantly working women of reproductive age, with a strong focus on healthcare professionals such as surgeons, physicians, nurses, and midwives. Several studies investigated women undergoing fertility treatments or those experiencing pregnancy and postpartum conditions, while others included general employed women across sectors. A limited number of contributions incorporated the perspectives of employers or mixed samples of workers and managers, offering insight into organizational approaches to reproductive health and workplace accommodations.
The workplace factors considered varied considerably across the studies. Some focused on hazardous or demanding working conditions, such as long hours, shift work, or exposure to chemicals. Others examined policies and benefits, including maternity leave, flexible work, fertility coverage, or breastfeeding support. A number of studies also investigated social and organizational aspects, including support from colleagues, managerial practices, and broader organizational culture.
The outcomes reported were equally diverse, encompassing fertility and reproductive health outcomes (e.g., infertility, fecundability, miscarriage), pregnancy and postpartum experiences (e.g., complications, depression, health insurance retention), as well as work- and career-related consequences, such as absenteeism, productivity loss, burnout, and career progression.
Together, these characteristics highlight the breadth of approaches and contexts represented in the literature, while reflecting a shared focus on how workplace environments intersect with reproductive health and employment outcomes.
To facilitate comparison and synthesis across the included literature, the studies were grouped according to the primary workplace factors investigated. As shown in Table 3, four main domains were identified: (i) shift work and circadian disruption, (ii) organizational stress and burnout, (iii) workplace flexibility and accommodations, and (iv) fertility-related policies and organizational support.
The first cluster captures research on shift work, rotating schedules, and physically demanding tasks, often in healthcare and service occupations, which were consistently associated with disrupted reproductive cycles, reduced fecundability, and increased risks of miscarriage and infertility. The second group addresses organizational stress and burnout, highlighting how excessive workloads, high training demands, and psychosocial strain may adversely affect fertility treatment outcomes and amplify barriers to childbearing, particularly among female professionals.
A third body of evidence examines the role of workplace flexibility and accommodations, including reduced workload during pregnancy, access to sick leave, and organizational sensitivity to reproductive health needs. These studies emphasize how flexible arrangements can mitigate productivity loss, absenteeism, and emotional distress, while also supporting long-term career trajectories. Finally, the fourth domain covers fertility-related policies and organizational support mechanisms, such as maternity leave provisions, fertility benefits, and insurance coverage. Research in this area consistently points to positive associations with fertility intentions, employee retention, morale, and workplace well-being, while also exposing persistent gaps in accessibility for minority groups.
This thematic categorization offers a structured overview of how different organizational and workplace conditions intersect with reproductive health and fertility outcomes, providing a foundation for identifying both risk factors and protective organizational practices.
3.2. Synthesis of Research Questions
To ensure analytical coherence between the thematic domains and the conceptual aims of this review, the following section synthesizes key findings in direct relation to the guiding research questions.
- Impact of organizational dysfunction on fertility and reproductive health
Across multiple studies, organizational dysfunction—characterized by high work intensity, excessive time demands, lack of autonomy, insufficient supervisory support, and rigid scheduling—was consistently associated with adverse reproductive outcomes. These include diminished fecundability, menstrual irregularities, pregnancy complications, and reduced effectiveness of fertility treatments. Mechanistically, these associations appear mediated by chronic stress, endocrine disruption, and reduced access to timely care.
- Organizational barriers to reproductive well-being
The most salient organizational barriers identified were shift work (especially night shifts), exposure to occupational hazards, lack of reproductive leave, inflexible work arrangements, and limited employer-sponsored fertility coverage. These conditions were shown to impair reproductive health both directly—through physiological stressors—and indirectly—by delaying care-seeking or exacerbating psychosocial burdens.
- Economic and productivity consequences of inadequate support
Several studies reported measurable economic impacts associated with the absence of reproductive health accommodations, including reduced employee productivity, increased absenteeism, greater turnover intentions, and elevated health-related expenditures. These findings highlight the organizational costs incurred when reproductive health is insufficiently integrated into workplace policy frameworks.
- Effective organizational accommodations and policy interventions
Workplace policies that demonstrated positive impacts included flexible scheduling, fertility-related insurance coverage, protected leave for medical appointments, and clear anti-discrimination protocols. Such measures were associated with improved treatment adherence, greater reproductive autonomy, higher employee morale, and enhanced retention—particularly among women undergoing fertility treatment or managing chronic reproductive conditions.
5. Role of stigma and organizational culture in disclosure and support-seeking
The presence of fertility-related stigma within organizational culture was a major determinant of employee silence, distress, and disengagement. Conversely, inclusive and supportive environments were found to promote disclosure, reduce emotional burden, and facilitate access to accommodations. Organizational climates that normalize reproductive health needs and implement confidential support systems appear critical to ensuring equitable outcomes.
Collectively, these synthesized insights clarify how structural and cultural dimensions of the workplace shape fertility-related health trajectories, informing potential interventions at both policy and practice levels.
4. Discussion
This scoping review mapped the evidence on how organizational dysfunction and workplace accommodations affect employees’ reproductive health, fertility outcomes, and associated economic consequences. Across the 28 included studies, four main domains emerged: shift work and circadian disruption, organizational stress and burnout, workplace flexibility and accommodations, and fertility-related policies and organizational support. The findings suggest that while hazardous working conditions and excessive workloads are consistently linked to adverse reproductive health outcomes, supportive organizational practices, including flexible scheduling, fertility-related benefits, and a culture that reduces stigma, can mitigate risks and promote both employee well-being and organizational productivity.
Several survey-based and cohort studies (Izadi et al., 2024; Mínguez-Alarcón et al., 2017; Moćkun-Pietrzak et al., 2022) consistently show that night duties, rotating schedules, and physically demanding tasks are associated with disrupted ovarian cycles, reduced ovarian reserve, and higher miscarriage risks, particularly among healthcare workers. These findings are supported by broader occupational health research, which links shift work to menstrual disturbances, increased risk of endometriosis, and subfecundity (Bisanti et al., 1996; Gamble et al., 2013; Stocker et al., 2014). Night shift work has also been associated with early spontaneous pregnancy loss (Fernandez et al., 2016; Zhu et al., 2003).
Mechanistically, circadian disruption appears to affect the hypothalamic–pituitary–gonadal axis, altering hormone secretion and impairing fertility (Mahoney, 2010; Mills & Kuohung, 2019; Sen & Sellix, 2016). Animal studies confirm that light exposure at night disrupts molecular and endocrine timekeeping in the female reproductive system (Yaw et al., 2020). Longitudinal evidence also suggests associations with earlier menopause onset (Stock & Schernhammer, 2019) and lower IVF success (Mínguez-Alarcón et al., 2017). Nevertheless, findings remain heterogeneous, partly due to methodological differences and contextual variation (Caetano et al., 2021; Chau et al., 2013). Further high-quality studies are needed to clarify causal mechanisms and inform targeted interventions.
Occupational stress emerged as a second major factor influencing reproductive health. Studies on physicians (Armijo et al., 2021; Győrffy et al., 2014) and fertility patients (Barzilai-Pesach et al., 2006) showed that high job strain, long working hours, and training demands negatively affect fertility, delaying childbearing and reducing treatment success. Stress activates the hypothalamic–pituitary–adrenal axis, suppressing reproductive hormone secretion and impairing pregnancy outcomes (Goel, 2025; Joseph & Whirledge, 2017). Empirical findings further suggest associations with reduced fertility intentions, increased treatment cycles, and poorer conception rates (Boivin & Schmidt, 2005; Dehkordi et al., 2025).
Emerging biomarkers, such as hair cortisol, provide promising tools to capture the impact of chronic stress (Santa-Cruz & Agudo, 2020), while mechanistic research points to pathways involving immune regulation and metabolic hormones like ghrelin (NEPOMNASCHY et al., 2007; Sominsky et al., 2017). Overall, psychosocial stress appears as consequential as physical hazards in shaping fertility outcomes, though most studies remain reliant on self-reported measures.
Flexibility and organizational support were strongly associated with improved reproductive outcomes and employee well-being. Studies among Japanese women undergoing fertility treatment (Maeda et al., 2022), female surgeons (Castillo-Angeles et al., 2022), and women with chronic reproductive conditions (Hvala & Hammarberg, 2025) demonstrated that access to workload reduction, sick leave, and partner support alleviates emotional distress, improves quality of life, and preserves work ability.
Qualitative studies (Fernandez-Pineda et al., 2025; Gilbert et al., 2023; Mirick & Wladkowski, 2022) further highlight the lived experiences of stigma, miscarriage, and disclosure dilemmas, showing that organizational culture critically mediates the effectiveness of accommodations. Broader literature confirms that flexible arrangements, when employee-driven, are associated with improved health and reduced absenteeism (Joyce et al., 2010; Shifrin & Michel, 2021), although in some contexts they may paradoxically increase work–family conflict (Higgins et al., 2014).
Productivity losses during fertility treatments are substantial: absences average 23 hours per treatment cycle, with direct costs exceeding €500 per woman (BOUWMANS et al., 2008). Without adequate support, employees report difficulties combining treatment with work, reduced productivity, and intentions to leave their jobs (Payne et al., 2018; Steyn et al., 2022). Conversely, supportive policies and digital health tools mitigate these losses and improve employee retention (Gifford & Zong, 2017; Henrich et al., 2025).
Several studies (Herweck et al., 2025; Jou et al., 2016; Kim & Parish, 2020; Silverberg et al., 2009; Steyn et al., 2022, 2024) highlight the role of institutional policies in shaping fertility and career trajectories. Employer-sponsored fertility benefits and maternity leave are linked to improved retention, morale, and fertility intentions. However, extended leaves can have ambivalent effects—enhancing short-term retention but sometimes limiting long-term career advancement (Brugiavini et al., 2013; Hideg et al., 2018; Stearns, 2016). Cultural attitudes and organizational climates further moderate these effects (Budig et al., 2012; Motaung et al., 2017).
Cross-national evidence suggests that family-friendly policies, including childcare leave and workplace daycare, foster higher fertility intentions (Choi et al., 2018; Kim & Parish, 2020), particularly in contexts supportive of maternal employment (Billingsley & Ferrarini, 2014; Castles, 2003; Mills & Kuohung, 2019). Yet, persistent inequities remain. Steyn et al. (2024) (Steyn et al., 2024) found that LGBTQ+ and minority employees face barriers to accessing fertility-related benefits, while De Oliveira Trigo et al. (2023) (De Oliveira Trigo et al., 2023) showed that fertility-friendly policies are also perceived by employers as enhancing organizational legitimacy.
Finally, stigma and disclosure play a critical role. Perceived stigma reduces disclosure of fertility struggles (Slade et al., 2007; Toth & Dewa, 2014), while supportive policies and inclusive organizational climates encourage openness, improve mental health, and reduce distress (Lyubykh et al., 2025; Webster et al., 2017). These findings underscore that the effectiveness of formal policies depends not only on legal frameworks but also on workplace culture.
This review presents several notable strengths. Methodologically, it adheres to the PRISMA-ScR guidelines and employs the PCC framework to ensure a transparent and replicable search strategy. The inclusion of diverse study designs, quantitative, qualitative, and mixed-methods, across multiple countries and professional sectors allows for a multidimensional synthesis of evidence. The thematic grouping of studies across four distinct domains enhances analytical clarity and supports the identification of organizational levers relevant to both reproductive outcomes and workplace functioning. Furthermore, the review integrates evidence from occupational health, organizational psychology, and labor economics, thereby contributing a multidisciplinary perspective that is often missing in existing literature.
Nonetheless, certain limitations must be acknowledged. The synthesis is constrained by the heterogeneity of the included studies in terms of design, population, and measurement tools, which limits direct comparability. Although economic consequences are addressed, they remain underdeveloped relative to the health-related dimensions, reflecting the limited availability of studies focusing explicitly on economic metrics. Most included studies relied on self-reported outcomes and cross-sectional designs, which hinders causal inference. Moreover, several populations, particularly men, LGBTQ+ employees, and precarious or informal workers, are underrepresented in the evidence base, restricting the generalizability of findings across workforce segments. These limitations underscore the need for future studies employing longitudinal designs, incorporating objective health and economic indicators, and focusing on underexplored worker groups.
5. Conclusions and Future Directions
This scoping review provides a comprehensive overview of how organizational dysfunction and workplace accommodations intersect with reproductive health, fertility outcomes, and associated economic consequences. The evidence highlights four central domains: shift work and circadian disruption, organizational stress and burnout, workplace flexibility and accommodations, and fertility-related policies and organizational support. Hazardous working conditions and psychosocial stressors consistently emerge as risk factors for impaired fertility and adverse pregnancy outcomes, while flexible arrangements, comprehensive fertility benefits, and stigma-free workplace cultures demonstrate potential to mitigate these risks and enhance both employee well-being and organizational performance.
From a practical perspective, the findings suggest that employers who implement family-supportive policies and targeted accommodations not only safeguard reproductive health but may also reduce absenteeism, improve retention, and strengthen talent attraction. At the same time, important gaps remain, particularly regarding equitable access to benefits across diverse groups, including LGBTQ+ and minority employees, as well as workers in precarious or low-wage sectors who are underrepresented in current research.
Future research should move beyond cross-sectional surveys and self-reported outcomes toward longitudinal, multi-country, and interventional studies capable of establishing causal links between workplace factors and reproductive outcomes. Integrating biological markers of stress and circadian disruption with organizational and economic analyses could help clarify mechanisms while quantifying productivity impacts. Moreover, comparative studies across cultural and institutional contexts are essential to understand how different policy environments mediate the relationship between work and reproductive health.
In light of global demographic shifts and increasing attention to workplace diversity and inclusion, fertility and reproductive health should be recognized as central dimensions of occupational well-being. Developing evidence-based workplace guidelines and embedding fertility support into broader health and safety frameworks will not only address employee needs but also strengthen organizational resilience in an evolving labor market.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: Search Strategy by Database.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Anderson, M., & Goldman, R. H. Occupational Reproductive Hazards for Female Surgeons in the Operating Room. AMA Surgery 2020, 155(3), 243. [CrossRef]
- Arksey, H., & O’Malley, L. (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8(1), 19–32. [CrossRef]
- Armijo, P. R., Flores, L., Huynh, L., Strong, S., Mukkamala, S., & Shillcutt, S. (2021). Fertility and Reproductive Health in Women Physicians. Journal of Women’s Health, 30(12), 1713–1719. [CrossRef]
- Babanov, S. A., Strizhakov, L. A., Agarkova, I. A., Tezikov, Y. V., & Lipatov, I. S. (2019). Workplace factors and reproductive health: Causation and occupational risks assessment. Gynecology, 21(4), 33–43. [CrossRef]
- Baranski, B. (1993). Effects of the workplace on fertility and related reproductive outcome s. Environmental Health Perspectives, 101(suppl 2), 81–90. [CrossRef]
- Barzilai-Pesach, V., Sheiner, E. K., Sheiner, E., Potashnik, G., & Shoham-Vardi, I. (2006). The Effect of Women???s Occupational Psychologic Stress on Outcome of Fertility Treatments. Journal of Occupational and Environmental Medicine, 48(1), 56–62. [CrossRef]
- Billingsley, S., & Ferrarini, T. (2014). Family Policy and Fertility Intentions in 21 European Countries. Journal of Marriage and Family, 76(2), 428–445. [CrossRef]
- Bisanti, L., Olsen, J., Basso, O., Thonneau, P., & Karmaus, W. (1996). Shift work and subfecundity: A European multicenter study. European St udy Group on Infertility and Subfecundity. Journal of Occupational and Environmental Medicine.
- Boivin, J., & Schmidt, L. (2005). Infertility-related stress in men and women predicts treatment outcome 1 year later. Fertility and Sterility, 83(6), 1745–1752. [CrossRef]
- BOUWMANS, C. A. M., LINTSEN, B. A. M. E., AL, M., VERHAAK, C. M., EIJKEMANS, R. J. C., HABBEMA, J. D. F., BRAAT, D. D. M., & HAKKAART-VAN ROIJEN, L. (2008). Absence from work and emotional stress in women undergoing IVF or ICSI: An analysis of IVF-related absence from work in women and the contri bution of general and emotional factors. Acta Obstetricia et Gynecologica Scandinavica, 87(11), 1169–1175. [CrossRef]
- Brugiavini, A., Pasini, G., & Trevisan, E. (2013). The direct impact of maternity benefits on leave taking: Evidence from complete fertility histories. Advances in Life Course Research, 18(1), 46–67. [CrossRef]
- Budig, M. J., Misra, J., & Boeckmann, I. (2012). The Motherhood Penalty in Cross-National Perspective: The Importance o f Work-Family Policies and Cultural Attitudes. Social Politics: International Studies in Gender, State & Society, 19(2), 163–193. [CrossRef]
- Caetano, G., Bozinovic, I., Dupont, C., Léger, D., Lévy, R., & Sermondade, N. (2021). Impact of sleep on female and male reproductive functions: A systemati c review. Fertility and Sterility, 115(3), 715–731. [CrossRef]
- Castillo-Angeles, M., Atkinson, R. B., Easter, S. R., Gosain, A., Hu, Y.-Y., Cooper, Z., Kim, E. S., Fromson, J. A., & Rangel, E. L. (2022). Postpartum Depression in Surgeons and Workplace Support for Obstetric and Neonatal Complication: Results of a National Study of US Surgeons. Journal of the American College of Surgeons, 234(6), 1051–1061. [CrossRef]
- Castles, F. G. (2003). The World Turned Upside Down: Below Replacement Fertility, Changing Preferences and Family-Friendly Public Policy in 21 OECD Countries. Journal of European Social Policy, 13(3), 209–227. [CrossRef]
- Cech, E. A., & O’Connor, L. T. (2017). ‘Like second-hand smoke’: The toxic effect of workplace flexibility bi as for workers’ health. Community, Work & Family, 20(5), 543–572. [CrossRef]
- Cervi, L., & Knights, D. (2022). Organizing male infertility: Masculinities and fertility treatment. Gender, Work & Organization, 29(4), 1113–1131. [CrossRef]
- Chau, Y. M., West, S., & Mapedzahama, V. (2013). Night Work and the Reproductive Health of Women: An Integrated Literature Review. Journal of Midwifery & Women’s Health, 59(2), 113–126. [CrossRef]
- Choi, S., Yellow Horse, A. J., & Yang, T.-C. (2018). Family policies and working women’s fertility intentions in South Kore a. Asian Population Studies, 14(3), 251–270. [CrossRef]
- Cox, S., Cox, T., & Pryce, J. (2000). Work-related reproductive health: A review. Work & Stress, 14(2), 171–180. [CrossRef]
- De Oliveira Trigo, B. R., De Oliveira Trigo, A., Folgado, J., & Lucas, C. (2023). P-576 The perspective of patients and company leaders regarding fertil ity support in the workplace in Portugal. Human Reproduction, 38(Supplement_1). [CrossRef]
- Dehkordi, S. M., Khoshakhlagh, A. H., Yazdanirad, S., Mohammadian-Hafshejani, A., & Rajabi-vardanjani, H. (2025). The effect of job stress on fertility, its intention, and infertility treatment among the workers: A systematic review. BMC Public Health, 25(1). [CrossRef]
- Dyer, S., & Patel, M. (2012). The economic impact of infertility on women in developing countries - a systematic review. Facts, views & vision in ObGyn.
- Fernandez, R., Marino, J., Varcoe, T., Davis, S., Moran, L., Rumbold, A., Brown, H., Whitrow, M., Davies, M., & Moore, V. (2016). Fixed or Rotating Night Shift Work Undertaken by Women: Implications for Fertility and Miscarriage. Seminars in Reproductive Medicine, 34(02), 074–082. [CrossRef]
- Fernandez-Pineda, M., Black, E. R., & Swift, A. (2025). Secondary Qualitative Analysis of the Effect of Work-Related Stress on Women Who Experienced Miscarriage During the COVID-19 Pandemic. Journal of Obstetric, Gynecologic, & Neonatal Nursing. [CrossRef]
- Figa-Talamanca, I. (2006). Occupational risk factors and reproductive health of women. Occupational Medicine, 56(8), 521–531. [CrossRef]
- Gamble, K. L., Resuehr, D., & Johnson, C. H. (2013). Shift Work and Circadian Dysregulation of Reproduction. Frontiers in Endocrinology, 4. [CrossRef]
- GIACOLA, G. P. (1992). Reproductive Hazards in the Workplace. Obstetrical & Gynecological Survey, 47(10), 679–687. [CrossRef]
- Gifford, B., & Zong, Y. (2017). On-the-Job Productivity Losses Among Employees With Health Problems. Journal of Occupational & Environmental Medicine, 59(9), 885–893. [CrossRef]
- Gilbert, S. L., Dimoff, J. K., Brady, J. M., Macleod, R., & McPhee, T. (2023). Pregnancy loss: A qualitative exploration of an experience stigmatized in the workplace. Journal of Vocational Behavior, 142, 103848. [CrossRef]
- GLASS, J., & FUJIMOTO, T. (1995). Employer Characteristics and the Provision of Family Responsive Polici es. Work and Occupations, 22(4), 380–411. [CrossRef]
- Goel, L. (2025). Understanding the Impact of Stress on Infertility: Biological Links an d Treatment Strategies. International Journal of Scientific and Research Publications, 15(1), 207–214. [CrossRef]
- Gold, E. B., & Tomich, E. (1994). Occupational hazards to fertility and pregnancy outcome. Occupational Medicine.
- Győrffy, Z., Dweik, D., & Girasek, E. (2014). Reproductive health and burn-out among female physicians: Nationwide, representative study from Hungary. BMC Women’s Health, 14(1). [CrossRef]
- Hauser, R., Skakkebaek, N. E., Hass, U., Toppari, J., Juul, A., Andersson, A. M., Kortenkamp, A., Heindel, J. J., & Trasande, L. (2015). Male Reproductive Disorders, Diseases, and Costs of Exposure to Endocr ine-Disrupting Chemicals in the European Union. The Journal of Clinical Endocrinology & Metabolism, 100(4), 1267–1277. [CrossRef]
- Henrich, N., Brinson, A., Karwa, S., & Jahnke, H. R. (2025). Use of a digital health benefit to maintain employees’ productivity wh ile trying to conceive. Social Science & Medicine, 382, 118329. [CrossRef]
- Herweck, A. M., Delawalla, M. LM., Reed, C., Carson, T. L., Ahuja, A., Chey, P., McNamara, M., Gupta, K., Bosch, A., Hipp, H. S., & Kawwass, J. F. (2025). Enhancing reproductive access: The influence of expanded employer fertility benefits at a single academic center from 2017 to 2021. American Journal of Obstetrics and Gynecology. [CrossRef]
- Hideg, I., Krstic, A., Trau, R. N. C., & Zarina, T. (2018). The unintended consequences of maternity leaves: How agency interventi ons mitigate the negative effects of longer legislated maternity leave s. Journal of Applied Psychology, 103(10), 1155–1164. [CrossRef]
- Higgins, C., Duxbury, L., & Julien, M. (2014). The relationship between work arrangements and work-family conflict. WORK: A Journal of Prevention, Assessment & Rehabilitation, 48(1), 69–81. [CrossRef]
- Hvala, T., & Hammarberg, K. (2025). The impact of reproductive health needs on women’s employment: A qualitative insight into managing endometriosis and work. BMC Women’s Health, 25(1). [CrossRef]
- Isaacs, J. C. (2008). Infertility coverage is good business. Fertility and Sterility, 89(5), 1049–1052. [CrossRef]
- Izadi, N., Aminian, O., Ghafourian, K., Aghdaee, A., & Samadanian, S. (2024). Reproductive outcomes among female health care workers. BMC Women’s Health, 24(1). [CrossRef]
- Joseph, D., & Whirledge, S. (2017). Stress and the HPA Axis: Balancing Homeostasis and Fertility. International Journal of Molecular Sciences, 18(10), 2224. [CrossRef]
- Jou, J., Kozhimannil, K. B., Blewett, L. A., McGovern, P. M., & Abraham, J. M. (2016). Workplace Accommodations for Pregnant Employees. Journal of Occupational & Environmental Medicine, 58(6), 561–566. [CrossRef]
- Joyce, K., Pabayo, R., Critchley, J. A., & Bambra, C. (2010). Flexible working conditions and their effects on employee health and w ellbeing. Cochrane Database of Systematic Reviews. [CrossRef]
- Kim, E. J., & Parish, S. L. (2020). Family-supportive workplace policies and benefits and fertility intent ions in South Korea. Community, Work & Family, 25(4), 464–491. [CrossRef]
- Kumar, S. (2004). Occupational Exposure Associated with Reproductive Dysfunction. Journal of Occupational Health, 46(1), 1–19. [CrossRef]
- Levac, D., Colquhoun, H., & O’Brien, K. K. (2010). Scoping studies: Advancing the methodology. Implementation Science, 5(1). [CrossRef]
- Lwin, T. M., Castillo-Angeles, M., Cunningham, C. E., Atkinson, R. B., Kim, E., Easter, S. R., Gosain, A., Hu, Y.-Y., & Rangel, E. L. (2024). The Impact of Low Workplace Support During Pregnancy on Surgeon Distress and Career Dissatisfaction. Annals of Surgery. [CrossRef]
- Lyubykh, Z., Turner, N., Weinhardt, J. M., Davis, J., & Dumaisnil, A. (2025). Facilitating Mental Health Disclosure and Better Work Outcomes: The Ro le of Organizational Support for Disclosing Mental Health Concerns. Human Resource Management. [CrossRef]
- Maeda, E., Hiraike, O., Sugimori, H., Kinoshita, A., Hirao, M., Nomura, K., & Osuga, Y. (2022). Working conditions contribute to fertility-related quality of life: A cross-sectional study in Japan. Reproductive BioMedicine Online, 45(6), 1285–1295. [CrossRef]
- Mahoney, M. M. (2010). Shift Work, Jet Lag, and Female Reproduction. International Journal of Endocrinology, 2010, 1–9. [CrossRef]
- Metcalfe, A., Vekved, M., & Tough, S. (2011). P1-242 Impact of work place policies and educational attainment on women’s childbearing decisions in Canada. Journal of Epidemiology & Community Health, 65(Suppl 1), A133–A133. [CrossRef]
- Mills, J., & Kuohung, W. (2019). Impact of circadian rhythms on female reproduction and infertility tre atment success. Current Opinion in Endocrinology, Diabetes & Obesity, 26(6), 317–321. [CrossRef]
- Mínguez-Alarcón, L., Souter, I., Williams, P. L., Ford, J. B., Hauser, R., Chavarro, J. E., & Gaskins, A. J. (2017). Occupational factors and markers of ovarian reserve and response among women at a fertility centre. Occupational and Environmental Medicine, 74(6), 426–431. [CrossRef]
- Mirick, R. G., & Wladkowski, S. P. (2022). Infertility and Pregnancy Loss in Doctoral Education: Understanding Students’ Experiences. Affilia, 38(3), 503–524. [CrossRef]
- Moćkun-Pietrzak, J., Gaworska-Krzemińska, A., & Michalik, A. (2022). A Cross-Sectional, Exploratory Study on the Impact of Night Shift Work on Midwives’ Reproductive and Sexual Health. International Journal of Environmental Research and Public Health, 19(13), 8082. [CrossRef]
- Motaung, L. L., Bussin, M. H. R., & Joseph, R. M. (2017). Maternity and paternity leave and career progression of black African women in dual-career couples. SA Journal of Human Resource Management, 1(2). [CrossRef]
- Nachtigall, R. D., Tschann, J. M., Quiroga, S. S., Pitcher, L., & Becker, G. (1997). Stigma, disclosure, and family functioning among parents of children c onceived through donor insemination. Fertility and Sterility, 68(1), 83–89. [CrossRef]
- NEPOMNASCHY, P. A., SHEINER, E., MASTORAKOS, G., & ARCK, P. C. (2007). Stress, Immune Function, and Women’s Reproduction. Annals of the New York Academy of Sciences, 1113(1), 350–364. [CrossRef]
- Payne, N., Seenan, S., & van den Akker, O. (2018). Experiences and psychological distress of fertility treatment and empl oyment. Journal of Psychosomatic Obstetrics & Gynecology, 40(2), 156–165. [CrossRef]
- Peters, M. D. J., Marnie, C., Tricco, A. C., Pollock, D., Munn, Z., Alexander, L., McInerney, P., Godfrey, C. M., & Khalil, H. (2021). Updated methodological guidance for the conduct of scoping reviews. JBI Evidence Implementation, 19(1), 3–10. [CrossRef]
- Pollock, D., Peters, M. D. J., Khalil, H., McInerney, P., Alexander, L., Tricco, A. C., Evans, C., De Moraes, É. B., Godfrey, C. M., Pieper, D., Saran, A., Stern, C., & Munn, Z. (2022). Recommendations for the extraction, analysis, and presentation of results in scoping reviews. JBI Evidence Synthesis, 21(3), 520–532. [CrossRef]
- Ponzo, S., Wickham, A., Bamford, R., Radovic, T., Zhaunova, L., Peven, K., Klepchukova, A., & Payne, J. L. (2022). Menstrual cycle-associated symptoms and workplace productivity in US employees: A cross-sectional survey of users of the Flo mobile phone app. DIGITAL HEALTH, 8, 205520762211458. [CrossRef]
- Rangel, E. L., Castillo-Angeles, M., Hu, Y.-Y., Gosain, A., Easter, S. R., Cooper, Z., Atkinson, R. B., & Kim, E. S. (2022). Lack of Workplace Support for Obstetric Health Concerns is Associated With Major Pregnancy Complications. Annals of Surgery, 276(3), 491–499. [CrossRef]
- Rayyan. (2024, agosto 7). Available online: https://www.rayyan.ai/.
- Rim, K.-T. (2017). Reproductive Toxic Chemicals at Work and Efforts to Protect Workers’ H ealth: A Literature Review. Safety and Health at Work, 8(2), 143–150. [CrossRef]
- Sabbath, E. L., Willis, M. D., Wesselink, A. K., Wang, T. R., McKinnon, C. J., Hatch, E. E., & Wise, L. A. (2024). Association between job control and time to pregnancy in a preconception cohort. Fertility and Sterility, 121(3), 497–505. [CrossRef]
- Santa-Cruz, D. C., & Agudo, D. (2020). Impact of underlying stress in infertility. Current Opinion in Obstetrics & Gynecology, 32(3), 233–236. [CrossRef]
- Sen, A., & Sellix, M. T. (2016). The Circadian Timing System and Environmental Circadian Disruption: Fr om Follicles to Fertility. Endocrinology, 157(9), 3366–3373. [CrossRef]
- Shifrin, N. V., & Michel, J. S. (2021). Flexible work arrangements and employee health: A meta-analytic review. Work & Stress, 36(1), 60–85. [CrossRef]
- Shreffler, K. M. (2016). Contextual Understanding of Lower Fertility Among U.S. Women in Professional Occupations. Journal of Family Issues, 38(2), 204–224. [CrossRef]
- Silverberg, K., Meletiche, D., & Del Rosario, G. (2009). An employer’s experience with infertility coverage: A case study. Fertility and Sterility, 92(6), 2103–2105. [CrossRef]
- Simoens, S., Dunselman, G., Dirksen, C., Hummelshoj, L., Bokor, A., Brandes, I., Brodszky, V., Canis, M., Colombo, G. L., DeLeire, T., Falcone, T., Graham, B., Halis, G., Horne, A., Kanj, O., Kjer, J. J., Kristensen, J., Lebovic, D., Mueller, M., … D’Hooghe, T. (2012). The burden of endometriosis: Costs and quality of life of women with e ndometriosis and treated in referral centres. Human Reproduction, 27(5), 1292–1299. [CrossRef]
- Slade, P., O’Neill, C., Simpson, A. J., & Lashen, H. (2007). The relationship between perceived stigma, disclosure patterns, suppor t and distress in new attendees at an infertility clinic. Human Reproduction, 22(8), 2309–2317. [CrossRef]
- Sominsky, L., Hodgson, D. M., McLaughlin, E. A., Smith, R., Wall, H. M., & Spencer, S. J. (2017). Linking Stress and Infertility: A Novel Role for Ghrelin. Endocrine Reviews, 38(5), 432–467. [CrossRef]
- Sonika. (2020). Women Reproductive Health and Occupational Safety: A Literature Review. [CrossRef]
- Stanley, N. B., & Foti, T. R. (2020). HEALTH INSURANCE FOR INFERTILITY SERVICES: IT’S ABOUT WHERE YOU WORK, MORE THAN WHERE YOU LIVE. Fertility and Sterility, 114(3), e50. [CrossRef]
- Stearns, J. (2016). The Long-Run Effects of Wage Replacement and Job Protection: Evidence from Two Maternity Leave Reforms in Great Britain. SSRN Electronic Journal. [CrossRef]
- Steyn, F., Kearns, B., Pericleous-Smith, A., & Imogen, C. (2024). P-455 Exploring the impact of fertility care on the modern workforce: Key research findings. Human Reproduction, 39(Supplement_1). [CrossRef]
- Steyn, F., Sizer, A., & Pericleous-Smith, A. (2022). P-486 Fertility in the workplace: The emotional, physical and psycholo gical impact of infertility in the workplace. Human Reproduction, 37(Supplement_1). [CrossRef]
- Stock, D., & Schernhammer, E. (2019). Does night work affect age at which menopause occurs? Current Opinion in Endocrinology, Diabetes & Obesity, 26(6), 306–312. [CrossRef]
- Stocker, L. J., Macklon, N. S., Cheong, Y. C., & Bewley, S. J. (2014). Influence of Shift Work on Early Reproductive Outcomes. Obstetrics & Gynecology, 124(1), 99–110. [CrossRef]
- Toth, K. E., & Dewa, C. S. (2014). Employee Decision-Making About Disclosure of a Mental Disorder at Work. Journal of Occupational Rehabilitation, 24(4), 732–746. [CrossRef]
- Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., Levac, D., Moher, D., Peters, M. D. J., Horsley, T., Weeks, L., Hempel, S., Akl, E. A., Chang, C., McGowan, J., Stewart, L., Hartling, L., Aldcroft, A., Wilson, M. G., Garritty, C., … Straus, S. E. (2018). PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Annals of Internal Medicine, 169(7), 467–473. [CrossRef]
- van den Akker, O. B. A., Payne, N., & Lewis, S. (2017). Catch 22? Disclosing assisted conception treatment at work. International Journal of Workplace Health Management, 10(5), 364–375. [CrossRef]
- Virgillito, D., Catalfo, P., & Ledda, C. (2025). Wearables in Healthcare Organizations: Implications for Occupational Health, Organizational Performance, and Economic Outcomes. Healthcare, 13(18), 2289. [CrossRef]
- WAN, G., & CHUNG, F. (2011). Working conditions associated with ovarian cycle in a medical center nurses: A Taiwan study. Japan Journal of Nursing Science, 9(1), 112–118. [CrossRef]
- Wang, S., & Tan, J. (2024). Negotiating Work and Family Spheres: The Dyadic Effects of Flexible Work Arrangements on Fertility Among Dual-Earner Heterosexual Couples. Demography, 61(4), 1241–1265. [CrossRef]
- Webster, J. R., Adams, G. A., Maranto, C. L., Sawyer, K., & Thoroughgood, C. (2017). Workplace contextual supports for LGBT employees: A review, meta-analy sis, and agenda for future research. Human Resource Management, 57(1), 193–210. [CrossRef]
- Winker, R., & Rüdiger, H. W. (2005). Reproductive toxicology in occupational settings: An update. International Archives of Occupational and Environmental Health, 79(1), 1–10. [CrossRef]
- Yaw, A., McLane-Svoboda, A., & Hoffmann, H. (2020). Shiftwork and Light at Night Negatively Impact Molecular and Endocrine Timekeeping in the Female Reproductive Axis in Humans and Rodents. International Journal of Molecular Sciences, 22(1), 324. [CrossRef]
- Zhu, J. L., Hjollund, N. H., Boggild, H., & Olsen, J. (2003). Shift work and subfecundity: A causal link or an artefact? Occupational and Environmental Medicine, 60(9), e12–e12. [CrossRef]
Figure 1.
PRISMA-ScR flow diagram illustrating the identification, screening, eligibility, and inclusion of studies on endometriosis and work-related outcomes.
Figure 1.
PRISMA-ScR flow diagram illustrating the identification, screening, eligibility, and inclusion of studies on endometriosis and work-related outcomes.
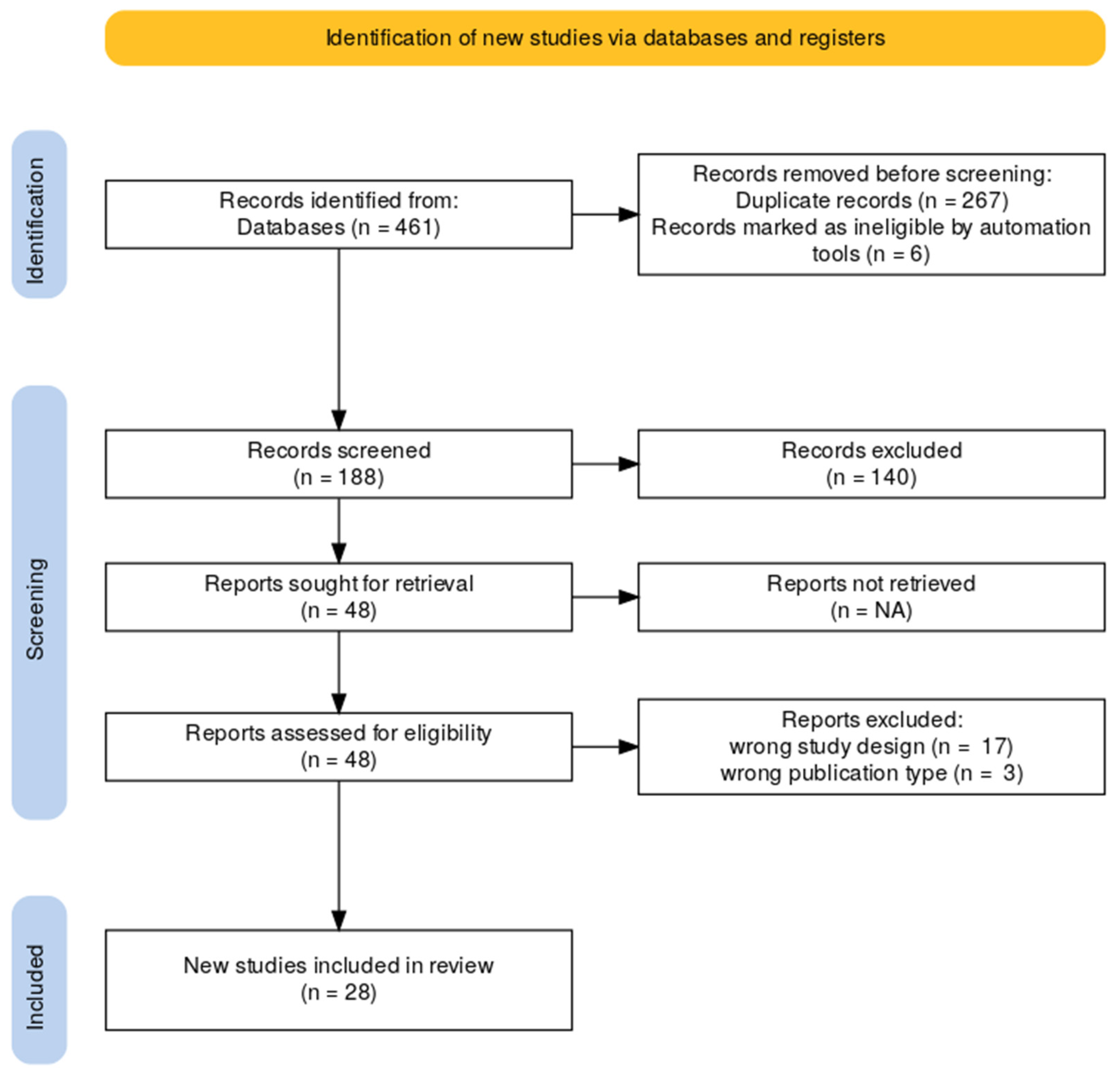

Table 1.
Eligibility Criteria Based on the PCC (Population–Concept–Context) Framework.
| Element | Description | Inclusion Criteria | Exclusion Criteria |
|---|---|---|---|
| Population | Adult female employees with endometriosis | Women aged ≥18 years with a clinically confirmed diagnosis of endometriosis, employed in any sector | Males, non-employed individuals, or women without confirmed diagnosis of endometriosis |
| Concept | Organizational factors affecting reproductive and work outcomes | Studies addressing workplace policies, organizational dysfunction, workplace accommodations, and their impact on fertility, absenteeism, or productivity | Studies not addressing organizational/workplace dimensions or outcomes related to fertility, absenteeism, or productivity |
| Context | Formal employment settings across sectors and regions | Studies conducted in formal workplace environments (any industry or geographical location) | Studies in informal work contexts, unpaid labor, or non-employment settings (e.g., homemaking, student populations) |
Table 2.
Characteristics of included studies examining workplace factors, reproductive health, and fertility-related outcomes.
Table 2.
Characteristics of included studies examining workplace factors, reproductive health, and fertility-related outcomes.
| Study | Study design | Population | Workplace factors | Primary outcome |
|---|---|---|---|---|
| Anderson and Goldman, 2020 (Anderson & Goldman, 2020) | Quantitative (retrospective studies) | Female surgeons | Operating room hazards, working conditions | Infertility, pregnancy complications |
| Armijo et al., 2021 (Armijo et al., 2021) | Quantitative (survey) | 377 women physicians | Training demands, work hours, breastfeeding support | Childbearing trends, fertility issues, barriers |
| Barzilai-Pesach et al., 2006 (Barzilai-Pesach et al., 2006) | Quantitative (prospective cohort) | 75 working women (fertility problem) | Job stress, workload, satisfaction | Fertility treatment outcomes |
| Castillo-Angeles et al., 2022 (Castillo-Angeles et al., 2022) | Quantitative (survey) | 692 female surgeons with live birth | Workplace support for work reduction during pregnancy/neonatal complications | Postpartum depression, income loss |
| De Oliveira Trigo et al., 2023 (De Oliveira Trigo et al., 2023) | Mixed methods | 107 workers, 24 employers (Portugal) | Fertility-friendly policies, support | Career progression, anxiety, disclosure |
| Fernandez-Pineda et al., 2025 (Fernandez-Pineda et al., 2025) | Qualitative (interviews) | 13 women post-miscarriage | Work-related stress, accommodations, support | Emotional distress, work performance |
| Gilbert et al., 2023 (Gilbert et al., 2023) | Qualitative (interviews) | 29 working women | Pregnancy loss, workplace stigma, support | Work outcomes, wellbeing, return-to-work |
| Győrffy et al., 2014 (Győrffy et al., 2014) | Quantitative (survey) | 3,039 female physicians (Hungary) | Burnout, workload | Reproductive disorders, burnout |
| Herweck et al., 2025 (Herweck et al., 2025) | Quantitative (retrospective) | 1,586 patients at academic center | Expanded fertility benefits | Access, utilization, demographics |
| Hvala and Hammarberg, 2025 (Hvala & Hammarberg, 2025) | Qualitative (interviews) | 12 employed women with endometriosis, adenomyosis, or infertility | Reproductive health needs, workplace flexibility, sick leave | Impact on work ability, career progression, support needs |
| Izadi et al., 2024 (Izadi et al., 2024) | Quantitative (cross-sectional) | 733 female healthcare workers (Iran) | Chemical, ergonomic, shift work | Reproductive outcomes, breastfeeding |
| Jou et al., 2016 (Jou et al., 2016) | Quantitative (survey) | 700 US women (postpartum) | Paid/unpaid maternity leave | Health insurance coverage, turnover |
| Kim and Parish, 2020 (Kim & Parish, 2020) | Quantitative (survey) | 3,405 Korean working women | Family-supportive policies, benefits | Fertility intentions (by parity) |
| Lwin et al., 2024 (Lwin et al., 2024) | Quantitative (survey) | 557 US surgeons | Workplace support during pregnancy | Burnout, career satisfaction |
| Maeda et al., 2022 (Maeda et al., 2022) | Quantitative (cross-sectional survey) | 721 Japanese women (25-44, employed, fertility care) | Job stress, working hours, time off, partner support | Fertility-related quality of life |
| Metcalfe et al., 2011 (Metcalfe et al., 2011) | Quantitative (survey) | 836 Canadian women (postpartum) | Parental leave, workplace support | Timing of first pregnancy |
| Mínguez-Alarcón et al., 2017 (Mínguez-Alarcón et al., 2017) | Quantitative (prospective cohort, survey) | 473/313 women at fertility center | Physically demanding work, shift work | Ovarian reserve, oocyte yield |
| Mirick and Wladkowski, 2022 (Mirick & Wladkowski, 2022) | Qualitative (interviews) | 328 women doctoral students | Infertility, pregnancy loss, institutional support | Productivity, support needs |
| Moćkun-Pietrzak et al., 2022 (Moćkun-Pietrzak et al., 2022) | Quantitative (survey) | 520 midwives (Poland) | Shift work, night shifts | Infertility, miscarriage, sexual health |
| Payne et al., 2019 (Payne et al., 2018) | Quantitative (online survey) | 563 UK employees (fertility treatment) | Work-treatment conflict, policy | Absence, career impact, distress |
| Ponzo et al., 2022 (Ponzo et al., 2022) | Quantitative (survey) | 1,867 US employees (Flo app users) | Menstrual symptoms, workplace support | Productivity, absenteeism |
| Rangel et al., 2022 (Rangel et al., 2022) | Quantitative (survey) | 671 US surgeons (likely female) | Workplace support for clinical work reduction during pregnancy | Major pregnancy complications, workplace support |
| Sabbath et al., 2023 (Sabbath et al., 2024) | Quantitative (cohort) | 3,110 women (21-45, US/Canada) | Job control, independence, decision-making | Fecundability (time to pregnancy) |
| Shreffler, 2017 (Shreffler, 2016) | Quantitative (survey) | 1,800 US women (employed) | Professional job characteristics | Fertility intentions, behaviors |
| Silverberg et al., 2009 (Silverberg et al., 2009) | Mixed methods (case study, survey) | Employees of Southwest Airlines, 605 employers | Infertility coverage, managed care | Resource use, morale, retention |
| Stanley and Foti, 2020 (Stanley & Foti, 2020) | Qualitative (interviews) | 66 individuals, 8 experts | Employer insurance, state mandates | Access to infertility services |
| Steyn et al., 2022 (Steyn et al., 2022) | Quantitative (survey) | 1,557 UK employees | Fertility journey, workplace support | Wellbeing, job satisfaction, absence |
| Steyn et al., 2024 (Steyn et al., 2024) | Quantitative (survey) | 1,031 UK employees | Fertility support, workplace policies | Fertility challenges, productivity, retention |
| Wan and Chung, 2012 (WAN & CHUNG, 2011) | Quantitative (survey) | 200 nurses (Taiwan) | Shift work, unit type | Ovarian cycle pattern |
| Wang and Tan, 2024 (Wang & Tan, 2024) | Quantitative (longitudinal) | Dual-earner UK couples | Flexible work arrangements | Fertility (first birth probability) |
Table 3.
Grouping of included studies by workplace factors affecting reproductive health and fertility outcomes.
Table 3.
Grouping of included studies by workplace factors affecting reproductive health and fertility outcomes.
| Thematic Domain |
Studies | Key Workplace Factors | Reported Outcomes |
|---|---|---|---|
| Shift Work and Circadian Disruption | (Izadi et al., 2024; Mínguez-Alarcón et al., 2017; Moćkun-Pietrzak et al., 2022; WAN & CHUNG, 2011) | Night shifts, rotating schedules, chemical and ergonomic exposures, physically demanding work | Infertility, miscarriage, reduced ovarian reserve, disrupted ovarian cycles, adverse reproductive outcomes |
| Organizational Stress and Burnout | (Armijo et al., 2021; Barzilai-Pesach et al., 2006; Győrffy et al., 2014) | Job stress, heavy workload, training demands, burnout, lack of breastfeeding support | Reproductive disorders, negative fertility treatment outcomes, barriers to childbearing, burnout |
| Workplace Flexibility and Accommodations | (Castillo-Angeles et al., 2022; Fernandez-Pineda et al., 2025; Gilbert et al., 2023; Hvala & Hammarberg, 2025; Maeda et al., 2022; Mirick & Wladkowski, 2022; Ponzo et al., 2022) | Working hours, workload reduction during pregnancy, sick leave, accommodations for reproductive health, workplace stigma | Fertility-related quality of life, postpartum depression, emotional distress, absenteeism, productivity loss, career impact |
| Fertility-Related Policies and Organizational Support | (Anderson & Goldman, 2020; De Oliveira Trigo et al., 2023; Herweck et al., 2025; Jou et al., 2016; Kim & Parish, 2020; Lwin et al., 2024; Metcalfe et al., 2011; Rangel et al., 2022; Sabbath et al., 2024; Shreffler, 2016; Silverberg et al., 2009; Stanley & Foti, 2020; Steyn et al., 2022, 2024; Wang & Tan, 2024) | Paid/unpaid maternity leave, fertility benefits, family-supportive policies, flexible work arrangements, employer insurance, stigma policies | Fertility intentions, access to services, employee retention, morale, job satisfaction, wellbeing, fecundability, pregnancy complications, productivity and career outcomes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



