Submitted:
16 October 2025
Posted:
17 October 2025
You are already at the latest version
Abstract
Background/Objectives: Ultrasonography (US) is a non-invasive and repeatable examination for evaluating chronic constipation. However, only few studies have investigated drug therapy decisions based on rectal US results. To date, the efficacy and safety of elobixibat have not been evaluated using rectal US classification in patients with chronic constipation. This study aimed to evaluate the efficacy and safety of elobixibat in patients with chronic constipation classified as “no fecal retention” by rectal US. Methods: We retrospectively analyzed 32 patients with chronic constipation who underwent rectal US and received elobixibat (10 mg/day) between May 2019 and December 2024. Patients were classified into four groups according to rectal US findings: no fecal retention, fecal retention without hard stools, fecal retention with hard stools, and gas retention. The primary endpoint was the response rate of spontaneous bowel movements (SBMs) within 3 days after starting elobixibat in the “no fecal retention” group. Results: Among 18 patients in the “no fecal retention” group, 94.4% achieved SBMs within 3 days after elobixibat administration, indicating a favorable response. Adverse events included abdominal distension and abdominal pain, each observed in one patient (3.1%). Conclusions: Elobixibat was effective and well tolerated in patients with chronic constipation classified by rectal US findings.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Observation Period and Data Collection
2.3. Assessment of Bowel Movements
2.4. Stool Form and Constipation Scoring
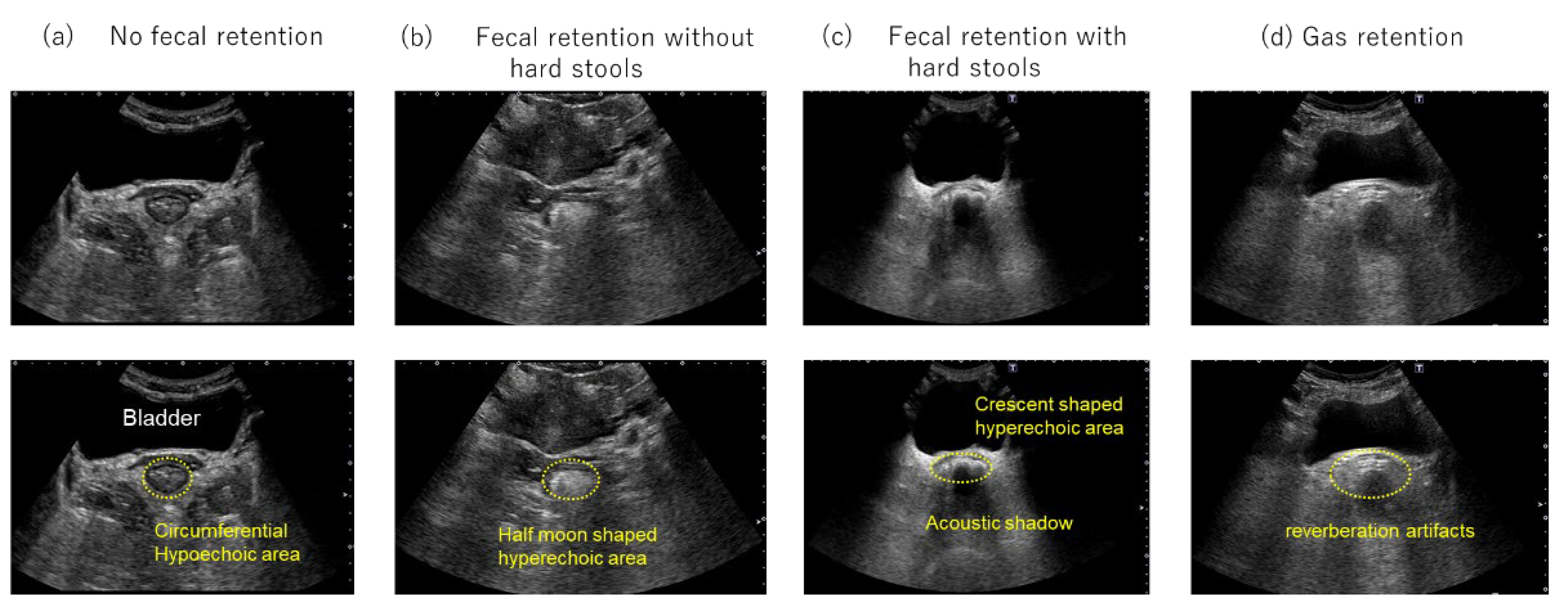
2.5. Ultrasonography (US)
2.6. Rectal US Classification
2.7. Measurement of Colonic Diameter
2.8. Statistical Analysis
3. Results
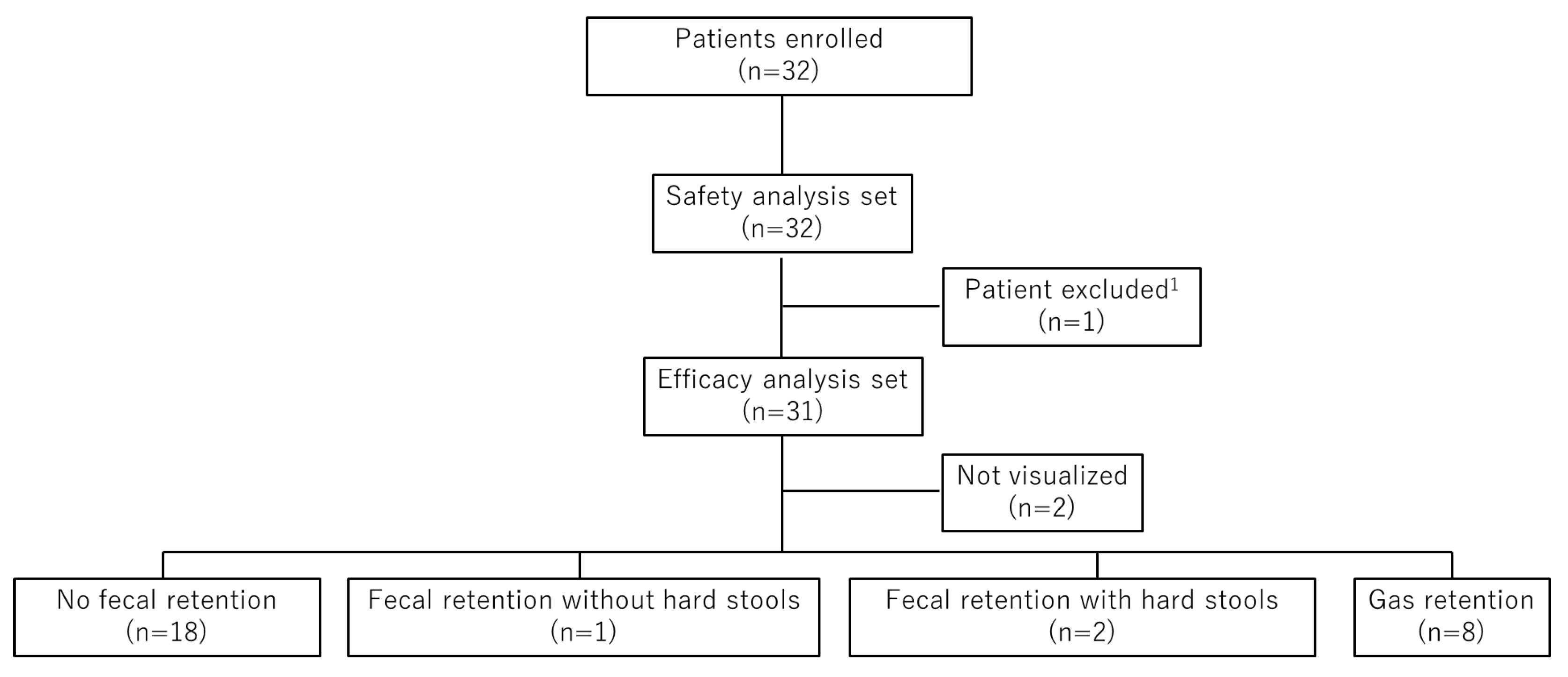
3.1. Patient Enrollment and Analysis Sets
3.2. Patient Characteristics
3.3. Proportion of Responders with SBMs Within 3 Days After the First Dose of Elobixibat
3.4. Proportion of Responders with SBMs on Day 1 Following the First Dose of Elobixibat
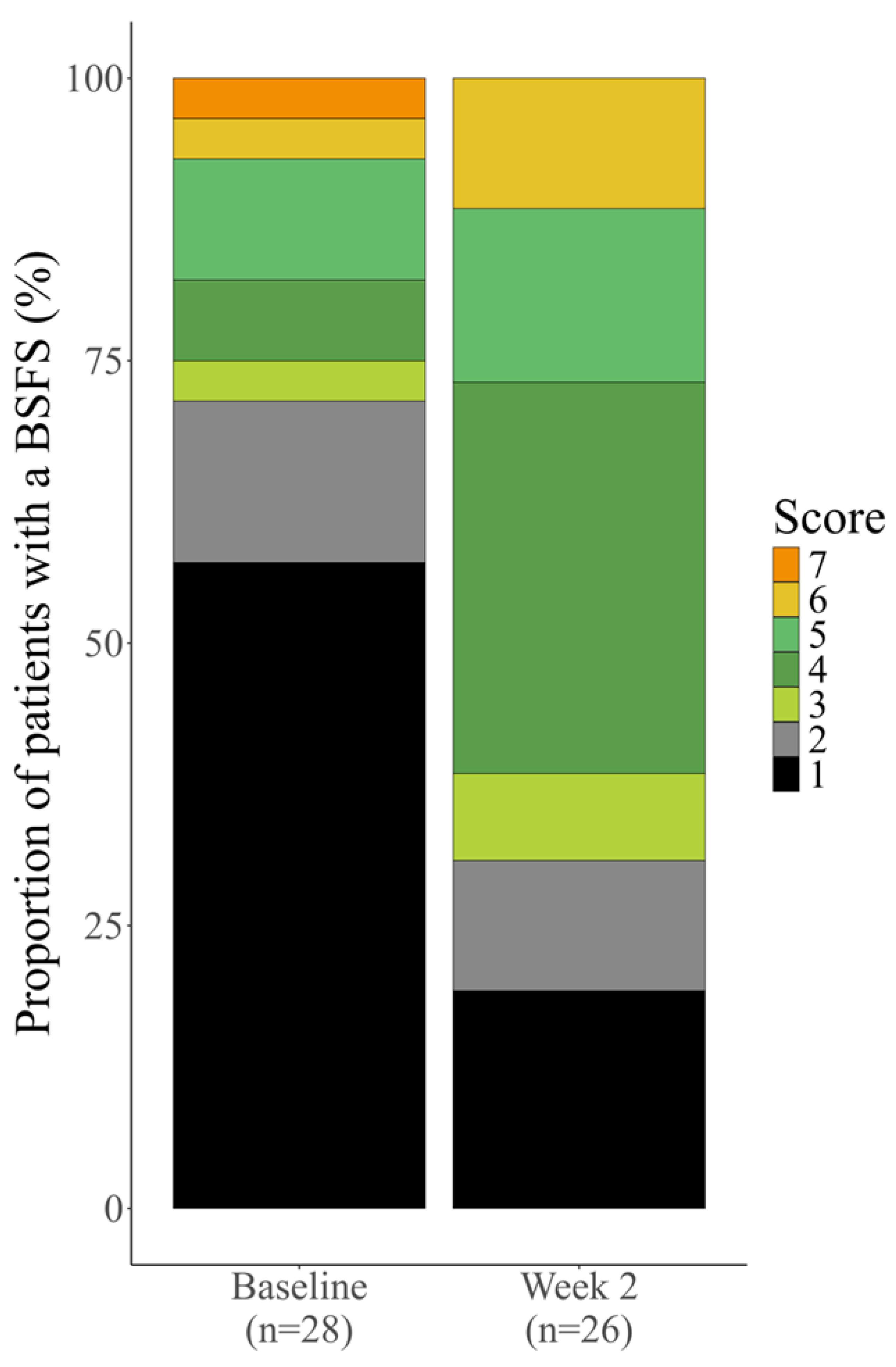
3.5. Stool Consistency Outcomes (BSFS)
3.6. Constipation Scoring System (CSS) Outcomes
3.6.1. Modified CSS Total Score
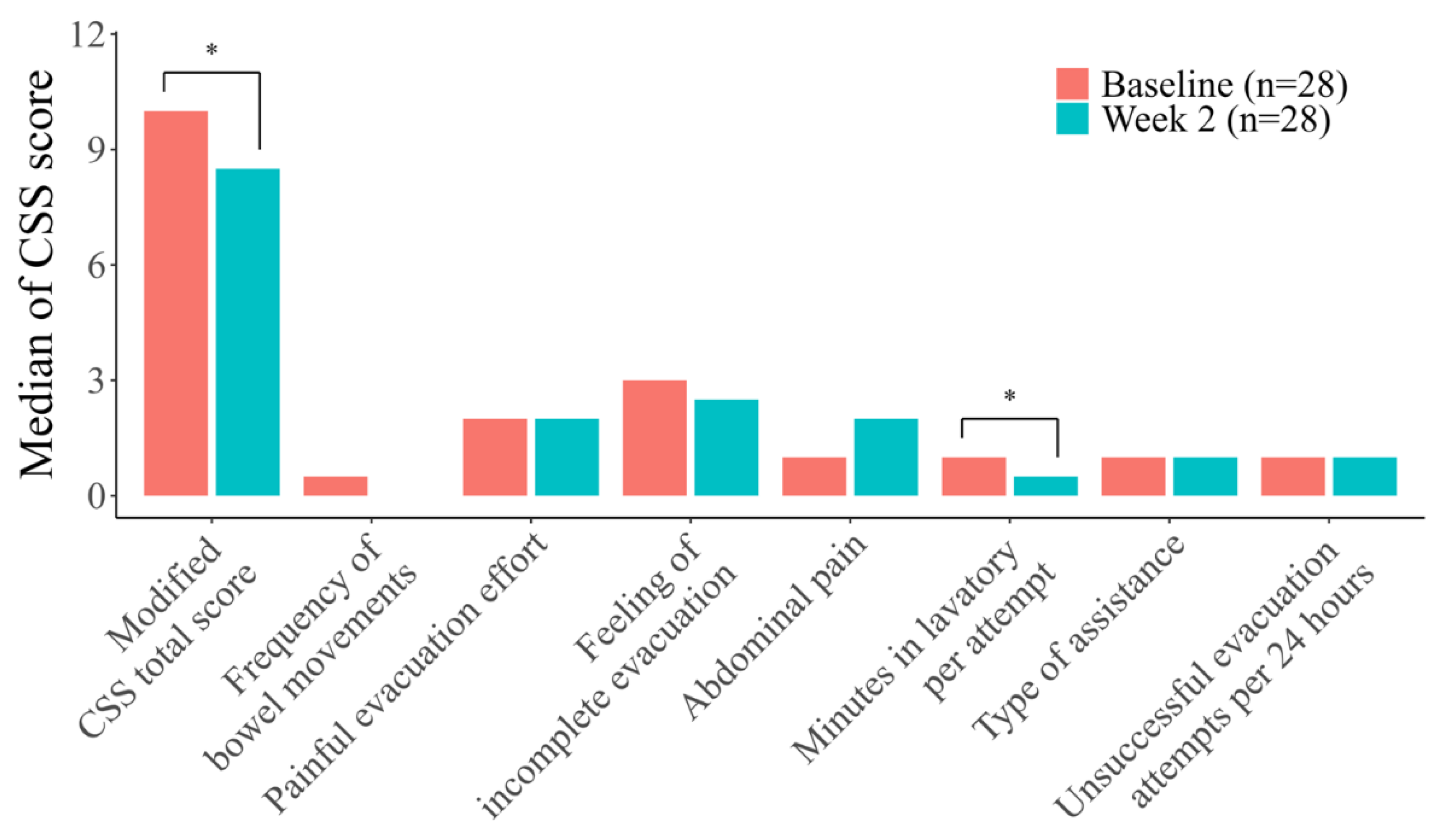
3.6.2. Modified CSS Sub-Scores
3.7. Relationship Between Colonic Diameter and Rectal US Classification
3.8. Safety
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BSFS | Bristol stool form scale |
| CSS | Constipation scoring system |
| CI | Confidence Interval |
| IBAT | Ileal bile acid transporter |
| MedDRA/J | Medical Dictionary for Regulatory Activities/J |
| QOL | Quality of life |
| RED | Rectal evacuation disorder |
| SBM | Spontaneous bowel movement |
| US | Ultrasonography |
References
- Summary Report of Comprehensive Survey of Living Conditions 2022. Available online: https://www.mhlw.go.jp/english/database/db-hss/dl/report_gaikyo_2022.pdf (accessed on 05 Sep 2025).
- Chang, J.Y.; Locke, G.R. 3rd; McNally, M.A.; Halder, S.L.; Schleck, C.D.; Zinsmeister, A.R.; Talley, N.J. Impact of functional gastrointestinal disorders on survival in the community. Am J Gastroenterol 2010, 105, 822–832. [Google Scholar] [CrossRef] [PubMed]
- Tomita, T.; Kazumori, K.; Baba, K.; Zhao, X.; Chen, Y.; Miwa, H. Impact of chronic constipation on health-related quality of life and work productivity in Japan. J Gastroenterol Hepatol 2021, 36, 1529–1537. [Google Scholar] [CrossRef] [PubMed]
- Manabe, N.; Kamada, T.; Kusunoki, H.; Hata, J.; Haruma, K. Usefulness of ultrasonographic evaluation of stool and/or gas distribution for the treatment strategy of chronic constipation. JGH Open 2019, 3, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, M.; Misawa, N.; Tsuda, M.; Manabe, N.; Kessoku, T.; Tamai, N.; Kawamoto, A.; Sugama, J.; Tanaka, H.; Kato, M.; et al. Expert consensus document: diagnosis for chronic constipation with faecal retention in the rectum using ultrasonography. Diagnostics (Basel) 2022, 12, 300. [Google Scholar] [CrossRef]
- Ihara, E.; Manabe, N.; Ohkubo, H.; Ogasawara, N.; Ogino, H.; Kakimoto, K.; Kanazawa, M.; Kawahara, H.; Kusano, C.; Kuribayashi, S.; et al. Evidence-based clinical guidelines for chronic constipation 2023. Digestion 2025, 106, 62–89. [Google Scholar] [CrossRef]
- Kessoku, T.; Matsumoto, M.; Misawa, N.; Tsuda, M.; Miura, Y.; Uchida, A.; Toriumi, Y.; Onodera, T.; Arima, H.; Kawamoto, A.; et al. Expert consensus document: an algorithm for the care and treatment of patients with constipation based on ultrasonographic findings in the rectum. Diagnostics (Basel) 2024, 14, 1510. [Google Scholar] [CrossRef]
- Acosta, A.; Camilleri, M. Elobixibat and its potential role in chronic idiopathic constipation. Ther Adv Gastroenterol 2014, 7, 167–175. [Google Scholar] [CrossRef]
- Manabe, N.; Umeyama, M.; Ishizaki, S.; Ota, T.; Kuratani, S.; Katsumata, R.; Fujita, M.; Haruma, K.; Camilleri, M. Elobixibat improves rectal sensation in patients with chronic constipation aged ≥60 years: A randomised placebo-controlled study. BMJ Open Gastroenterol 2023, 10, e001257. [Google Scholar] [CrossRef]
- Ishikawa, T.; Fukuzawa, M. Efficacy of elobixibat on defecation desire in patients with chronic constipation: a single center, retrospective, observational study [in Japanese]. Shinryo Shinyaku 2021, 58, 865–872. [Google Scholar]
- Park, S.Y.; Khemani, D.; Nelson, A.D.; Eckert, D.; Camilleri, M. Rectal gas volume measured by computerized tomography identifies evacuation disorders in patients with constipation. Clin Gastroenterol Hepatol 2017, 15, 543–552.e4. [Google Scholar] [CrossRef]
- Seike, K.; Koda, K.; Takiguchi, N.; Oda, K.; Miyazaki, M. Gas volume analysis and postoperative bowel functional disorders in patients who received anterior resection for rectal cancer. Dis Colon Rectum 2003, 46, 661–666. [Google Scholar] [CrossRef]
- Lewis, S.J.; Heaton, K.W. Stool form scale as a useful guide to intestinal transit time. Scand J Gastroenterol 1997, 32, 920–924. [Google Scholar] [CrossRef]
- Agachan, F.; Chen, T.; Pfeifer, J.; Reissman, P.; Wexner, S.D. A constipation scoring system to simplify evaluation and management of constipated patients. Dis Colon Rectum 1996, 39, 681–685. [Google Scholar] [CrossRef]
- Nakajima, A.; Seki, M.; Taniguchi, S.; Ohta, A.; Gillberg, P.G.; Mattsson, J.P.; Camilleri, M. Safety and efficacy of elobixibat for chronic constipation: results from a randomised, double-blind, placebo-controlled, phase 3 trial and an open-label, single-arm, phase 3 trial. Lancet Gastroenterol Hepatol 2018, 3, 537–547. [Google Scholar] [CrossRef] [PubMed]
- Kessoku, T.; Ishihara, Y.; Takahashi, K.; Dang, T.H.; Ohira, M.; Horiuchi, M.; Shibata, C.; Uchida, A.; Toriumi, Y.; Misawa, N.; et al. Comparison of the effectiveness of magnesium oxide and elobixibat on improving rectal sensitivity and colonic transit time in patients with chronic constipation: an observational study. Neurogastroenterol Motil 2025, e70106. [Google Scholar] [CrossRef] [PubMed]
- Uno, J.; Tsuboi, S.; Fujita, K. The utilization of elobixibat against Stimulant Laxatives administration to psychiatric disordered patients with chronic constipation: a single-center, retrospective observational study[in Japanese]. Jpn J Clin Psychopharmacol 2023, 26, 197–206. [Google Scholar]
- Eguchi, T.; Inatomi, O.; Shintani, S.; Momose, K.; Sako, T.; Takagi, M.; Fumihara, D.; Inoue, K.; Katayama, N.; Morisawa, T.; et al. Efficacy and safety of elobixibat in combination with or switched from conventional treatments of chronic constipation: A retrospective observational study. JGH Open 2024, 8, e70019. [Google Scholar] [CrossRef]
- Vollebregt, P.F.; Burgell, R.E.; Hooper, R.L.; Knowles, C.H.; Scott, S.M. Clinical impact of rectal hyposensitivity: a cross-sectional study of 2,876 patients with refractory functional constipation. Am J Gastroenterol 2021, 116, 758–768. [Google Scholar] [CrossRef]
- Kohno, T.; Okanobu, H.; Boda, K. Efficacy and safety of elobixibat for chronic constipation: a single-center prospective study [in Japanese]. Journal of Japanese Gastroenteroogical Association 2022, 6, 36–42. [Google Scholar]
- Nakajima, A.; Umeyama, M.; Higashikawa, M.; Shimada, Y.; Arai, Y. A multicenter, postmarketing surveillance of elobixibat in patients with chronic constipation in Japan: A final analysis report. Sage Open Med 2025, 13, 20503121251321659. [Google Scholar] [CrossRef]
- Shono, T.; Hyakutake, H. Efficacy and safety of long-term treatment with elobixibat in hemodialysis patients with chronic constipation: an observational study. Ren Replace Ther 2024, 10, 53. [Google Scholar] [CrossRef]

| Data | Efficacy Analysis Set | Safety Analysis Set | ||
|---|---|---|---|---|
| N | Variable | N | Variable | |
| Subjects | 31 | 32 | ||
| Male, n (%)1 | 6 (19.4) | 6 (18.8) | ||
| Female, n (%)1 | 25 (80.6) | 26 (81.3) | ||
| Age (years), mean ± SD | 31 | 56.8 ± 14.7 | 32 | 56.5 ± 14.6 |
| Height (cm), mean ± SD | 31 | 157.68 ± 7.19 | 32 | 157.56 ± 7.10 |
| Weight (kg), mean ± SD | 31 | 55.51 ± 11.96 | 32 | 55.18 ± 11.91 |
| Rectal US classification | 31 | 32 | ||
| No fecal retention, n (%)1 | 18 (58.1) | 18 (56.3) | ||
| Fecal retention without hard stools, n (%)1 | 1 (3.2) | 1 (3.1) | ||
| Fecal retention with hard stools, n (%)1 | 2 (6.5) | 2 (6.3) | ||
| Gas retention, n (%)1 | 8 (25.8) | 8 (25.0) | ||
| Not visualized, n (%)1, 2 | 2 (6.5) | 3 (9.4) | ||
| BSFS, median (IQR) | 30 | 1.0 (1.0–3.0) | 31 | 1.0 (1.0–4.0) |
| CSS | ||||
| Frequency of bowel movements, median (IQR) | 30 | 1.0 (0.0–2.0) | 31 | 1.0 (0.0–2.0) |
| Painful evacuation effort, median (IQR) | 30 | 2.0 (0.0–3.0) | 31 | 2.0 (0.0–3.0) |
| Feeling of incomplete evacuation, median (IQR) | 30 | 3.0 (2.0–4.0) | 31 | 3.0 (2.0–4.0) |
| Abdominal pain, median (IQR) | 30 | 1.0 (0.0–2.0) | 31 | 1.0 (0.0–2.0) |
| Minutes in lavatory per attempt, median (IQR) | 30 | 1.0 (1.0–2.0) | 30 | 1.0 (1.0–2.0) |
| Type of assistance, median (IQR) | 30 | 1.0 (1.0–2.0) | 31 | 1.0 (1.0–2.0) |
| Unsuccessful evacuation attempts per 24 hours, median (IQR) | 30 | 1.0 (1.0–1.0) | 30 | 1.0 (1.0–1.0) |
| Duration of constipation, median (IQR) | 30 | 3.0 (2.0–4.0) | 31 | 3.0 (2.0–4.0) |
| CSS total score, median (IQR) | 30 | 13.5 (10.0–17.0) | 30 | 13.5 (10.0–17.0) |
| Modified CSS total score, median (IQR) | 30 | 10.0 (8.0–13.0) | 30 | 10.0 (8.0–13.0) |
| Colonic diameter | ||||
| Rectum (mm), mean ± SD | 20 | 34.15 ± 13.18 | 20 | 34.15 ± 13.18 |
| Ascending colon (mm), mean ± SD | 24 | 35.70 ± 6.83 | 25 | 35.58 ± 6.72 |
| Transverse colon (mm), mean ± SD | 20 | 24.29 ± 3.34 | 21 | 24.35 ± 3.26 |
| Descending colon (mm), mean ± SD | 22 | 22.49 ± 4.02 | 23 | 22.26 ± 4.08 |
| Sigmoid colon (mm), mean ± SD | 22 | 21.80 ± 3.49 | 23 | 21.71 ± 3.43 |
| Mean colonic diameter (mm), mean ± SD | 24 | 28.32 ± 6.36 | 25 | 28.14 ± 6.29 |
| Comorbidities3 | 31 | 32 | ||
| Yes, n (%)1 | 13 (41.9) | 14 (43.8) | ||
| Mental disorder, n (%)1 | 3 (9.7) | 3 (9.4) | ||
| After cancer surgery, n (%)1 | 2 (6.5) | 3 (9.4) | ||
| Cholecystectomy, n (%)1 | 1 (3.2) | 1 (3.1) | ||
| Others, n (%)1, 4 | 8 (25.8) | 8 (25.0) | ||
| No, n (%)1 | 18 (58.1) | 18 (56.3) | ||
| Prior medications for constipation3, 5 | 31 | 32 | ||
| Yes, n (%)1 | 22 (71.0) | 23 (71.9) | ||
| Osmotic laxatives, n (%)1 | 12 (38.7) | 12 (37.5) | ||
| Stimulant laxatives, n (%)1 | 13 (41.9) | 14 (43.8) | ||
| Intestinal secretagogues, n (%)1, 6 | 2 (6.5) | 2 (6.3) | ||
| Others, n (%)1, 7 | 4 (12.9) | 4 (12.5) | ||
| No, n (%)1 | 9 (29.0) | 9 (28.1) | ||
| Prior medications for other comorbidities5 | 31 | 32 | ||
| Yes, n (%)1 | 17 (54.8) | 18 (56.3) | ||
| No, n (%)1 | 14 (45.2) | 14 (43.8) | ||
| Rectal US Classification | N | Responder, (n) | Non-Responder, (n) | Proportion of Responders1, 2 (%) |
95% CI3 (%) |
|---|---|---|---|---|---|
| No fecal retention | 18 | 17 | 1 | 94.4 | 74.2–99.0 |
| Fecal retention without hard stools | 1 | 1 | 0 | 100.0 | 20.7–100.0 |
| Fecal retention with hard stools | 2 | 2 | 0 | 100.0 | 34.2–100.0 |
| Gas retention | 8 | 8 | 0 | 100.0 | 67.6–100.0 |
| Total of 4 categories | 29 | 28 | 1 | 96.6 | 82.8– 99.4 |
| Rectal US Classification | N | Responder, (n) | Non-Responder, (n) | Proportion of Responders1, 2 (%) |
95% CI3 (%) |
|---|---|---|---|---|---|
| No fecal retention | 18 | 15 | 3 | 83.3 | 60.8–94.2 |
| Fecal retention without hard stools | 0 | 0 | 0 | - | - |
| Fecal retention with hard stools | 2 | 2 | 0 | 100.0 | 34.2–100.0 |
| Gas retention | 8 | 8 | 0 | 100.0 | 67.6–100.0 |
| Total of 4 categories | 28 | 25 | 3 | 89.3 | 72.8–96.3 |
| Rectal US Classification | Baseline | Week 2 | |||
|---|---|---|---|---|---|
| N | Variable | N | Variable | p1 | |
| No fecal retention, median (IQR) | 18 | 1.5 (1.0–5.0) | 16 | 4.0 (2.5–5.0) | 0.1078 |
| Fecal retention without hard stools, median (IQR) | 1 | 1.0 (1.0–1.0) | 0 | - | - |
| Fecal retention with hard stools, median (IQR) | 2 | 1.5 (1.0–2.0) | 2 | 1.0 (1.0–1.0) | 1.0000 |
| Gas retention, median (IQR) | 7 | 1.0 (1.0–3.0) | 8 | 4.0 (2.5–4.5) | 0.0350* |
| Total of 4 categories, median (IQR) | 28 | 1.0 (1.0–3.5) | 26 | 4.0 (2.0–5.0) | 0.0104* |
| Rectal US Classification | Baseline | Week 2 | |||
|---|---|---|---|---|---|
| N | Variable | N | Variable | p1 | |
| No fecal retention, median (IQR) | 18 | 10.0 (7.0–14.0) | 17 | 8.0 (6.0–12.0) | 0.2206 |
| Fecal retention without hard stools, median (IQR) | 1 | 10.0 (10.0–10.0) | 1 | 11.0 (11.0–11.0) | 1.0000 |
| Fecal retention with hard stools, median (IQR) | 2 | 16.5 (13.0–20.0) | 2 | 11.5 (11.0–12.0) | 0.3711 |
| Gas retention, median (IQR) | 7 | 10.0 (6.0–10.0) | 8 | 6.0 (3.0–11.5) | 0.0502 |
| Total of 4 categories, median (IQR) | 28 | 10.0 (7.5–13.5) | 28 | 8.5 (5.0–12.0) | 0.0231* |
| Rectal US Classification |
CSS Sub-Score | Timepoint | N | Variable, Median (IQR) | p1 |
|---|---|---|---|---|---|
| Total of 4 categories | Total score (excluding the duration of constipation)2 | Baseline | 28 | 10.0 (7.5–13.5) | 0.0231* |
| Week 2 | 28 | 8.5 (5.0–12.0) | |||
| Frequency of bowel movements | Baseline | 28 | 0.5 (0.0–1.5) | 0.3543 | |
| Week 2 | 28 | 0.0 (0.0–1.0) | |||
| Painful evacuation effort | Baseline | 28 | 2.0 (0.0–3.0) | 0.6806 | |
| Week 2 | 28 | 2.0 (0.0–3.0) | |||
| Feeling of incomplete evacuation | Baseline | 28 | 3.0 (2.0–4.0) | 0.0615 | |
| Week 2 | 28 | 2.5 (1.0–3.0) | |||
| Abdominal pain | Baseline | 28 | 1.0 (0.0–2.0) | 0.1078 | |
| Week 2 | 28 | 2.0 (0.5–2.0) | |||
| Minutes in lavatory per attempt | Baseline | 28 | 1.0 (0.5–2.0) | 0.0046* | |
| Week 2 | 28 | 0.5 (0.0–1.0) | |||
| Type of assistance | Baseline | 28 | 1.0 (1.0–2.0) | 0.0782 | |
| Week 2 | 28 | 1.0 (0.0–1.0) | |||
| Unsuccessful evacuation attempts per 24 hours | Baseline | 28 | 1.0 (1.0–1.0) | 0.0519 | |
| Week 2 | 28 | 1.0 (0.5–1.0) |
| Rectal US Classification | Number of Patients | Mean Transverse Diameter of the Colon and Rectum1 (mm) |
|---|---|---|
| N2 | Variable | |
| No fecal retention, Mean ± SD | 9 | 25.00 ± 1.23 |
| Fecal retention without hard stools, Mean ± SD | - | - |
| Fecal retention with hard stools, Mean ± SD | 2 | 33.09 ± 5.88 |
| Gas retention, Mean ± SD | 6 | 28.86 ± 1.43 |
| Total of 4 categories, Mean ± SD | 17 | 27.31 ± 3.41 |
| Factor | Estimated Difference1 | 95% CI | p |
|---|---|---|---|
| Rectal US classification: fecal retention without hard stools | - | - | - |
| Rectal US classification: fecal retention with hard stools | 8.09 | [4.705–11.468] | 0.0002* |
| Rectal US classification: gas retention | 3.86 | [1.579–6.139] | 0.0027* |
| Total | Severity | |||||
|---|---|---|---|---|---|---|
| Mild | Moderate | Severe | ||||
| n (%) | n (%) | n (%) | n (%) | |||
| Number | 32 | 32 | 32 | 32 | ||
| Adverse event | 2 (6.3) | 2 (6.3) | 0 (0.0) | 0 (0.0) | ||
| Gastrointestinal disorders | 2 (6.3) | 2 (6.3) | 0 (0.0) | 0 (0.0) | ||
| Abdominal distension | 1 (3.1) | 1 (3.1) | 0 (0.0) | 0 (0.0) | ||
| Abdominal pain | 1 (3.1) | 1 (3.1) | 0 (0.0) | 0 (0.0) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



