
Submitted:
15 October 2025
Posted:
17 October 2025
You are already at the latest version
Abstract
Background: Fontan-associated liver disease (FALD) is a progressive condition resulting from chronic hepatic venous congestion following the Fontan procedure for univentricular heart defects. As survival improves in these patients, recognition and management of FALD have become increasingly important.
Objective: To describe the pathophysiological mechanisms, imaging findings, and diagnostic approach to FALD, with a focus on the role of ultrasonography, including contrast-enhanced ultrasound (CEUS).
Methods: This narrative review explores the evolution of FALD through a multidisciplinary lens, integrating cardiovascular and hepatic imaging data. Particular attention is paid to Doppler ultrasound and CEUS, both in early parenchymal changes and in the differential diagnosis of potential complications such as hepatic nodules.
Results: FALD is characterized by progressive fibrosis due to long-standing passive congestion, resulting in a wide spectrum of imaging findings. B-mode ultrasound reveals hepatomegaly, heterogeneous parenchyma, and gallbladder wall thickening. Doppler studies show altered hepatic venous flow patterns, while CEUS provides dynamic vascular evaluation, highlighting areas of altered perfusion. In advanced stages, hypovascular areas in the late phase may simulate malignant lesions, emphasizing the need for careful interpretation. The role of liver biopsy, though limited by invasiveness, remains crucial in selected cases. Surveillance strategies are not standardized but require close multidisciplinary follow-up.
Conclusion: FALD presents complex diagnostic challenges requiring integrated imaging and clinical assessment. CEUS emerges as a valuable, non-invasive tool in characterizing hepatic congestion and guiding management. Increased awareness and standardized protocols are essential for early detection and tailored care in this growing patient population.
Keywords:
fontan
; liver
; FALD
; heart
; hepatocellular carcinoma
1. Introduction
The Fontan procedure is a surgical intervention used to treat congenital heart defects resulting in a single functional ventricle, such as hypoplastic left heart syndrome or tricuspid atresia. This procedure diverts systemic venous return directly to the pulmonary arteries, bypassing the heart. The initial version of the Fontan procedure, known as the atrio-pulmonary connection or classical Fontan, was originally developed for patients with tricuspid atresia. This approach involved closing the atrial septal defect and directly linking the right atrium to the right pulmonary artery. Over time, several modifications were introduced (Figure 1), including the revised atrio-pulmonary technique by Kreutzer and the right atrial-to-pulmonary artery connection described by Björk et al. [1,2]. A significant evolution came in 1988 with the introduction of the total cavopulmonary connection, or lateral tunnel, by De Leval. In this method, the superior vena cava is connected to the right pulmonary artery (classical Glenn shunt), while the inferior vena cava is routed to the right atrium through an intracardiac tunnel. The most recent development is the extracardiac cavopulmonary connection, which involves a direct anastomosis between the superior vena cava and the right pulmonary artery. A vascular conduit is placed externally to link the inferior vena cava to the right pulmonary artery. This technique offers advantages such as avoiding myocardial ischemia, reducing the number of suture lines, and eliminating the use of foreign material within the right atrium.
The Fontan circulation, characterized by the absence of a subpulmonary ventricle, fundamentally alters cardiovascular dynamics. In this configuration, systemic venous blood is directed passively into the pulmonary arteries, relying on elevated central venous pressure (CVP) to drive pulmonary perfusion. This passive flow results in a reduced preload to the systemic ventricle, limiting stroke volume and cardiac output. Concurrently, the systemic ventricle faces increased afterload, as it must overcome both systemic and pulmonary vascular resistances without the assistance of a sub-pulmonary pump. Three main mechanisms facilitate the passage of blood from the systemic venous system to the left atrium in the Fontan circulation [3]:
- The suction effect generated by left atrial relaxation during diastole.
- The action of the respiratory and muscular pumps, driven by the negative intrathoracic pressure during inspiration, which enhances inferior vena cava return and promotes pulmonary vessel recruitment.
- The maintenance of low pulmonary vascular resistance, provided there is no mechanical obstruction within the Fontan conduit, the main pulmonary arteries, or the pulmonary veins.
These hemodynamic changes can lead to ventricular dysfunction over time, manifesting as decreased ejection fraction and diastolic impairment. Additionally, the elevated CVP inherent in the Fontan circulation contributes to complications such as hepatic congestion, protein-losing enteropathy, and decreased exercise tolerance. Understanding these alterations is crucial for optimizing long-term management and improving outcomes in patients with Fontan physiology.
These hemodynamic challenges predispose patients to long-term complications, including liver and kidney diseases. The Fontan physiology is characterized by chronically elevated CVP and reduced cardiac output, significantly altering normal organ perfusion and function[3]. These changes can progressively impair the liver and kidneys, organs highly sensitive to hemodynamic stress [3].
Fontan circulation can fail due to systolic or diastolic ventricular dysfunction, atrioventricular valve disease, elevated pulmonary vascular resistance, recurrent arrhythmias, lymphatic insufficiency, or end-organ complications [4]. Accordingly, symptoms may be related to heart failure and hypoxemia or end-organ complications, resulting in different clinical and hemodynamic Fontan failure phenotypes [4] (Table 1).
- Systolic Failure Phenotype (SFP): the single ventricle’s pumping ability deteriorates, leading to a reduced ejection fraction. Clinically, patients may experience fatigue, ascites and exercise intolerance. Hemodynamically, this group is characterized by a low cardiac index, often less than 2,2 L/min/m2, and variable Fontan pressures. These patients are typically the most ill and often require early evaluation for transplant due to poor outcomes with medical therapy alone.
- Preserved Systolic Function with Elevated Pressure (PFP): In this phenotype, the ventricle itself is functioning normally in terms of contractility, but the Fontan circuit develops resistance. Elevated pressures within the Fontan pathway—often due to increased pulmonary vascular resistance, conduit stenosis, or lack of compliance—lead to systemic venous congestion. Patients may present with peripheral edema, liver congestion, and ascites. Despite a preserved cardiac output, end-organ dysfunction progresses, and clinical management often focuses on relieving congestion or improving Fontan flow dynamics.
- Lymphatic Failure Phenotype (LFP): Some patients with Fontan circulation develop complications related to abnormal lymphatic flow, even in the absence of severe hemodynamic derangements. These patients may present with protein-losing enteropathy, plastic bronchitis, or chylous effusions. This phenotype is increasingly recognized because of chronic central venous hypertension impairing lymphatic drainage, especially from the gut and lungs. Management often requires targeted lymphatic interventions, such as lymphangiography-guided embolization or specialized dietary and pharmacologic therapies.
- Normal Hemodynamics Phenotype (NHP): A subset of patients may exhibit clinical symptoms of Fontan failure despite having normal cardiac function and pressures. These cases can be particularly challenging to diagnose and manage, as standard hemodynamic evaluations appear normal. The underlying mechanisms are not fully understood but may involve diastolic dysfunction, subtle microvascular issues, or autonomic imbalance. Despite “normal” measurements, these patients may have reduced exercise tolerance or quality of life and require a multidisciplinary approach to evaluation.
Fontan-associated liver disease (FALD) encompasses a broad spectrum of structural, functional, and clinical liver alterations secondary to Fontan hemodynamic changes [3,5] (Table 2). These changes are due to the pathological hemodynamic state that exists in any type of Fontan circulation from the first day of the surgical procedure, meaning that FALD can also occur in patients without Fontan circulatory failure [3,4]. Liver damage can start even before the Fontan procedure and is present in patients without Fontan circulatory failure [3,4] (Table 3). This review aims to provide an updated overview of FALD and to summarize current knowledge on the role of imaging modalities in the evaluation of liver disease in this population, with a particular focus on ultrasound-based techniques.
2. Fald Epidemiology
The number of individuals living with Fontan-type surgery in 2020 was estimated to be 66 per million, expected to rise to 79 per million by 2030 [6,7]. In 2020, this population comprised 55% adults, 17% adolescents, and 28% children. These proportions are projected to shift to 64%, 13% and 23% respectively, by 2030 [6]. The true incidence of FALD is not known and likely underrecognized since there is no consensus on a uniformly accepted definition of the disease. The reported prevalence of FALD is 13-86% [6]. However, the actual prevalence of some of these conditions could be higher due to subclinical disease presentation and the lack of a universal definition. Hispanic ethnicity was associated with increased all-cause mortality [6]. Furthermore, the prevalence of FALD is underrecognized, but there is evidence that its incidence increases with age [4]. FALD is associated with late mortality but excellent post-transplant survival [4]. This underscores the need for FALD-specific liver surveillance strategies in patients post-Fontan.
3. Pathophysiology
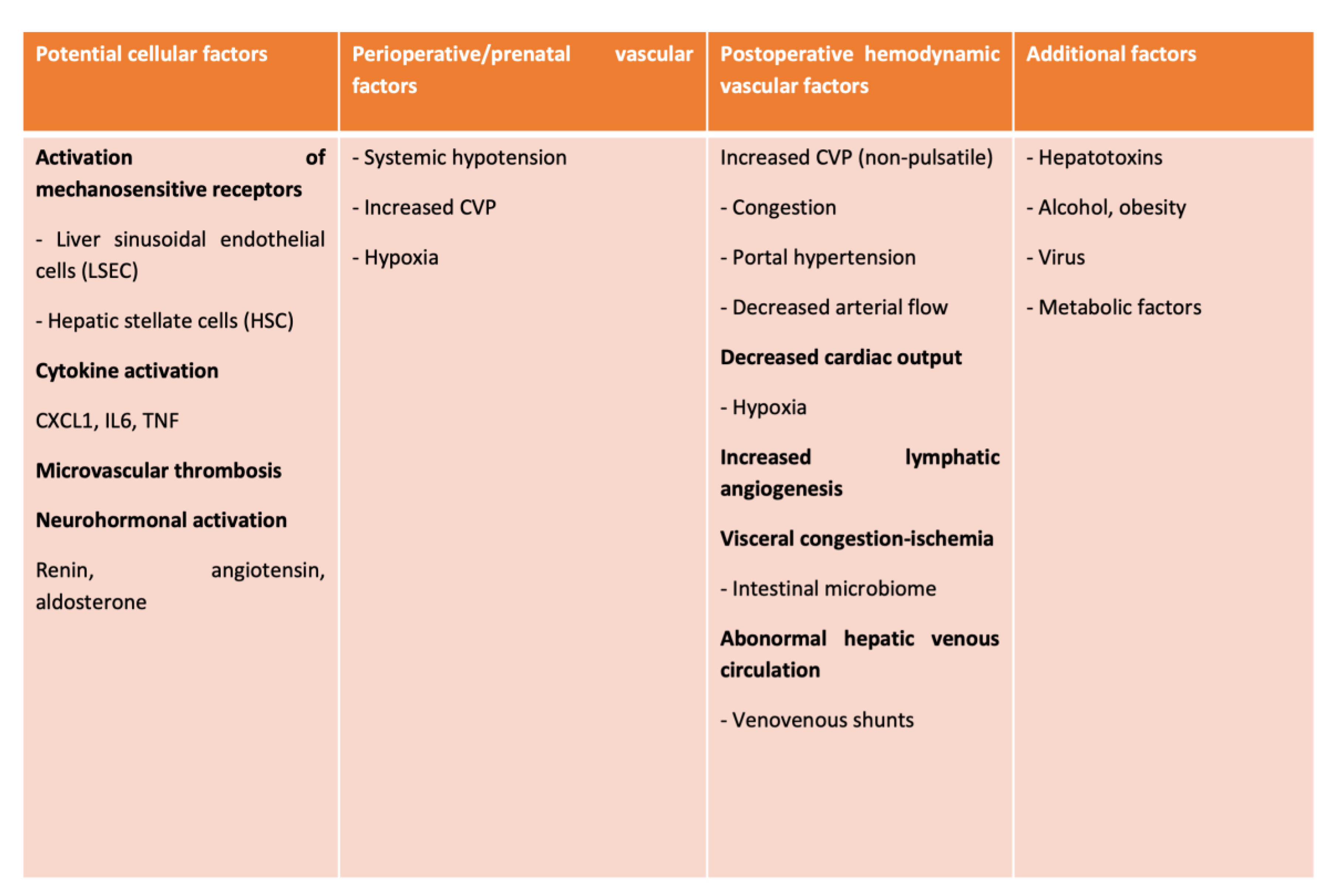
The mechanisms underlying the pathophysiology of FALD are multifactorial (Table 4). Different mechanisms related to the vascular supply and drainage of the liver have been linked to the development of hepatic damage in Fontan patients [7].
The hepatic veins transmit systemic venous hypertension to the sinusoid, leading to sinusoidal dilatation, hyperfiltration, and perisinusoidal edema [8,9]. In turn, sinusoidal shear stress promotes sinusoidal endothelial cell capillarization, decreases intrahepatic nitric oxide concentration, and facilitates the mechanical activation of mechanosensitive cell signaling pathways in hepatic stellate cells, resulting in liver fibrosis [10,11,12]. These changes also hamper the diffusion of oxygen and nutrients and promote centrilobular hepatocellular dropout and atrophy [13].
Elevated CVP may reduce the effectiveness of the hepatic arterial buffering response [5,14]. These changes put the liver at risk for hypoxic injury during an acute event (cardiac surgeries or cardiopulmonary collapse) [15,16]. Moreover, in the long term, chronic reduced cardiac output and the development of aberrant intrapulmonary shunts would perpetuate liver hypoxia [15,16].
The anatomical and functional characteristics of the Fontan circulation and the acquired thrombophilic state (low serum levels of antithrombin III, thrombomodulin, alpha-2-antiplasmin, and C and S proteins and high levels of thrombin-antithrombin complex) may facilitate intrahepatic microthrombosis [17,18,19].
Increased hepatic lymphangiogenesis and lymphatic stasis contribute to significant dilatation of hepatic sinusoids, the space of Disse, and channels passing through the limiting plate, potentially leading to collagen fiber deposition [20,21]. A state of latent microinflammation may promote end-organ fibrogenesis. Increased intestinal permeability secondary to venous and lymphatic congestion and chronic ischemia may play a central role in the inflammatory state.
Additional risk factors include an increased prevalence of hepatitis C and B virus infection and risk of hepatotoxic injury due to medications (i.e. amiodarone) [22].
4. Clinical Presentation
FALD most often develops subclinically during the early phases. Due to the distension of the Glisson capsule, some patients report discomfort in the upper right quadrant of the abdomen [7,23]. The liver edge is easily palpable, firm, smooth, and tender in these cases. Hepatojugular reflux may also be easily identified after applying compression over the liver [24]. Mild jaundice is common, yet severe jaundice is rare; however, it may occur at the end of an episode of hypoxic hepatitis [7,24]. Even in the advanced stages of FALD, with established but compensated cirrhosis, clinical symptoms may be absent or present with more nonspecific symptoms, such as anorexia, fatigue, and weight loss [24]. In late-stage and decompensated liver disease, ascites, jaundice, variceal bleeding, and hepatic encephalopathy may occur, suggesting the presence of portal hypertension (PHTN), which is associated with adverse outcomes in patients with a Fontan circulation [7,23]. Variceal bleeding has been reported after the Fontan procedure, with a variable incidence ranging from 9.3-38% [23]. In children, the prevalence of varices is even lower (about 9%), suggesting that their development is a late complication [25]. Given the high mortality risk associated with this complication (15%–20%), upper gastrointestinal endoscopy is commonly recommended for adult patients with cirrhosis or signs of PHTN [26].
5. Diagnosis
The diagnosis of FALD requires a comprehensive and integrated approach, as no single test can definitively identify or stage the condition. Evaluation typically begins with a thorough clinical assessment, including history and physical examination [27]. Clinicians look for signs of chronic liver disease such as hepatomegaly, ascites, jaundice, spider angiomas, and splenomegaly [27]. Symptoms may be subtle in early stages and include fatigue, abdominal discomfort, or evidence of portal hypertension, like gastrointestinal bleeding [27]. Laboratory testing plays a central role in the diagnostic process (Table 5). Liver enzymes such as ALT and AST may be normal or only mildly elevated, while markers of cholestasis (such as alkaline phosphatase and GGT) and bilirubin levels can provide additional insight [28]. Tests of synthetic liver function, including serum albumin and the international normalized ratio (INR), are useful for assessing disease severity [28]. A complete blood count may reveal thrombocytopenia, often a sign of portal hypertension, and serologic testing helps to exclude other causes of liver disease, such as viral hepatitis or autoimmune hepatitis [28]. Common fibrosis scores like APRI and FIB-4 are frequently used in other chronic liver diseases but have limited accuracy in FALD due to the unique hemodynamics of the Fontan circulation [28].
Imaging is a cornerstone of noninvasive evaluation. Abdominal ultrasound is often the first-line modality, allowing for assessment of liver size, texture, nodularity, and signs of portal hypertension such as splenomegaly or ascites [29,30]. Doppler ultrasound adds valuable information by evaluating hepatic and portal venous waveforms, which can reflect changes in venous congestion or progression toward cirrhosis [30,31]. Liver elastography, through either transient elastography or shear wave techniques, provides an estimate of liver stiffness [31]. However, stiffness values may be confounded by hepatic congestion and must be interpreted cautiously. Cross-sectional imaging with contrast-enhanced computed tomography (CT) or magnetic resonance (MR) offers detailed structural information and helps detect liver nodules, vascular changes, or collateral circulation [32]. MR with hepatobiliary contrast agents and MR elastography can offer superior tissue characterization, though their availability may be limited in some centers [32].
Endoscopic evaluation is recommended in patients at risk of portal hypertension [33]. Upper gastrointestinal endoscopy allows for direct visualization of esophageal and gastric varices, which may be asymptomatic until bleeding occurs [33]. In select cases, invasive testing is necessary [34]. Liver biopsy remains the gold standard for assessing fibrosis and confirming cirrhosis [34,35]. Histological findings in FALD typically include sinusoidal dilation, perivenular and perisinusoidal fibrosis, and in advanced stages, nodular regenerative hyperplasia [36]. However, in the case of FALD, this procedure is more challenging due to the potential for sampling errors caused by the heterogeneous nature and patchy distribution of fibrosis [36]. Additionally, because it is an invasive procedure, liver biopsy carries an increased risk of bleeding due to anticoagulant therapy and high CVP, making it unsuitable for routine longitudinal follow-up. In the pediatric population, sedation and general anesthesia are often required. Consequently, noninvasive diagnosis and staging could be an attractive alternative [37]. While hepatic venous pressure gradient (HVPG) is a standard tool in other liver diseases, it is less useful in the Fontan population due to altered vascular anatomy and hemodynamics. Conversely, cardiac catheterization remains an important tool to assess Fontan pressures and exclude hemodynamic contributors to liver congestion. Finally, in patients with advanced disease or cirrhosis, surveillance for hepatocellular carcinoma is crucial [38,39]. This typically involves regular imaging—such as ultrasound or MRI—every 6 to 12 months, sometimes paired with serum alpha-fetoprotein (AFP), although AFP alone has limited sensitivity and specificity [38,39].
7. Imaging
Imaging plays a valuable role in the diagnosis and surveillance of FALD [3]. Common imaging findings in patients with FALD include a heterogeneous liver texture. Initially, hepatomegaly is likely to develop because of venous congestion. With the development of advanced cirrhosis, atrophy of the right lobe with hypertrophy of the caudate lobe are seen, together with dilation of hepatic veins, IVC, and signs of PHTN, such as ascites, splenomegaly, and varices [3,7]. The specific atrophy of the right hepatic lobe in advanced cirrhosis can be explained by a combination of decreased portal and arterial inflow, intrahepatic anatomical changes and compensatory hypertrophy of the left lobe.
In advanced cirrhosis, there is significant disruption of hepatic blood flow, particularly a reduction in portal vein inflow to the right lobe. With the development of portal hypertension and portosystemic shunting, the right lobe becomes more susceptible to hypoperfusion, leading to chronic ischemia and atrophy. Structural changes in the liver (fibrosis, regenerative nodules, intrahepatic shunts) can compress portal branches supplying the right lobe. In some cases, a selective thrombosis of the right portal vein branch can be observed. As chronic liver disease progresses, the left lobe may become hypertrophic and more metabolically active, compensating for the reduced function of the right lobe. This is part of the compensatory atrophy-hypertrophy complex, where the right lobes shrink, and the left lobe enlarges.
Patients with imaging findings consistent with PHTN have a ninefold increased risk of HCC, liver transplantation, and death. While hepatomegaly can easily be seen on imaging methods, fibrosis remains undetectable until advanced stages. Typical manifestations of cirrhosis (fibrosis), such as regional atrophy, caudate lobe hypertrophy, and increased nodularity, are often masked in earlier stages due to liver swelling caused by congestion, which can obscure fibrotic shrinkage. The heterogeneous distribution of fibrosis is also characterized by multiple peripheral nodules of varying sizes in both early and late disease stages [3,7]. Over time, as cirrhosis progresses, right lobe atrophy and a nodular liver surface may become evident [3,7]. Typically, a patchy and uneven distribution of fibrosis or cirrhosis is seen [3,7]. Additionally, venovenous shunts, a dilated inferior vena cava, and engorged hepatic veins are frequently observed due to elevated CVP [3,7]. The combination of elevated CVP and low cardiac output leads to hepatic ischemia.
8. B-Mode Findings
Ultrasound can be used to detect heterogeneous echogenicity and hepatomegaly, which are early signs of congestive hepatopathy [40]. Several studies reported correlations between the severity of ultrasound features and the degree of hepatic fibrosis or cirrhosis (30, 41, 42). The most common ultrasound findings include a nodular liver surface, atrophy of the right lobe, rounded margins, and irregular profiles [43,44,45] (Figure 2). The echotexture appears granular and markedly heterogeneous, with hyperechogenic nodules of varying sizes [43,44,45] (Figure 3, Figure 4, Figure 5, Figure 6, Figure 7 and Figure 8).
In a study of 55 patients who had undergone the Fontan procedure, 67% exhibited heterogeneous hepatic echotexture or nodularity on the liver surface, findings that correlated with the time elapsed since the procedure. Severe congestion with PHTN may present with dilated portal veins (diameter >13 mm), enlarged paraumbilical veins, collateral circulation, splenomegaly (Figure 9), ascites, and reversal of portal vein flow [44,46,47].
Compared to liver cirrhosis secondary to hepatitis, extrahepatic portosystemic shunts in FALD are either uncommon or small, even in decompensated states. This is likely due to the high systemic venous pressure in Fontan circulation and the relatively low-pressure gradient between the portal and systemic veins, which limits the formation of large portosystemic collaterals [48]. Doppler ultrasonography is currently the most useful radiological tool for assessing liver disease. It provides useful information on blood flow and allows conclusions to be drawn about portal hypertension and thus about the cause of splenomegaly, hepatomegaly, ascites and liver nodules.
Doppler patterns in Fontan patients resemble those observed in chronic liver disease, including reduced portal flow velocity (mean flow velocity < 14 cm/sec) [49]. The Fontan procedure inevitably alters hepatic venous waveforms on Doppler US (Figure 10, Figure 11, Figure 12 and Figure 13). Inverted portal flow has a specificity of 100% for diagnosing PHTN [50] (Figure 12). The hepatopetal phase pattern in the hepatic vein differs between patients with total cavo-pulmonary anastomosis (including both lateral tunnels and extracardiac conduits) and those with atrio-pulmonary connection [51,52,53]. In atrio-pulmonary connection, hepatopetal flow is preserved (Figure 10), reflecting the exclusion of atrial contribution to venous circulation, whereas in total cavo-pulmonary anastomosis, flow reversal (Figure 11) occurs only during early expiration. Similar to congestive heart failure, hepatic veins and the IVC are dilated, with abnormally increased hepatic vein pulsatility, regardless of the anastomosis technique [48,54,55]. The loss of the normal three-phase Doppler pattern in hepatic veins is universal following bi-cavopulmonary surgery due to the absence of atrial contraction. The presence of a monophasic pattern indicates advanced liver injury [56].
In patients with Fontan circulation, the hepatic veins invariably demonstrate a blunted, hepatopetal monophasic flow pattern, consistent with chronic hepatic congestion. However, the flow velocity is lower than in the general population [56,57]. In contrast, in later stages characterized by cirrhosis and increased hepatic stiffness, further dampening or paradoxical changes in the venous flow pattern may be observed.
In particular, the hepatic venous Doppler waveform offers valuable insight into hemodynamic changes over time. In the early post-Fontan period, in the absence of atrial contraction and before structural liver damage is evident, the hepatic venous flow may display a relatively blunted monophasic or biphasic waveform with reduced phasicity, reflecting the lack of pulsatility and elevated central venous pressure.
As FALD progresses, and especially in the setting of developing cirrhosis, the Doppler waveform may become more dampened or even flat, corresponding to the increasing stiffness of the hepatic parenchyma, reduced compliance of the vascular bed, and worsening portal hypertension. Simultaneously, the hepatic veins may appear dilated in the early and mid-stages of disease due to chronic venous congestion but may show reduced caliber in later stages as fibrosis progresses and vascular remodeling occurs.
Tracking these Doppler changes, from waveform morphology to vein diameter, could provide a non-invasive, dynamic marker of FALD evolution. Including representative Doppler images at different timepoints post-Fontan would help clinicians recognize these transitions and potentially stratify risk or guide surveillance intensity.
Interestingly, hepatic vein waveform analysis can also serve as a surrogate marker for cardiac index, providing indirect insight into the hemodynamic status of Fontan circulation. Post-Fontan, IVC and hepatic vein dilation is common, but the main and intrahepatic portal veins tend to be small, likely due to reduced portal perfusion secondary to increased sinusoidal pressure and venous stasis [58]. The lumen width depends on the severity of the liver cirrhosis and, presumably, the duration of the disease. In FALD, the chronic elevation of central venous pressure leads to venous congestion and dilation of the hepatic veins and IVC due to the following reasons: the Fontan circulation results in chronically elevated systemic venous pressure, which is transmitted directly to the hepatic veins via the IVC. Over time, this causes passive venous dilatation, which can persist or even worsen despite progression to fibrosis and cirrhosis. Thus, even in advanced congestive cirrhosis from FALD, the hepatic veins and IVC often remain dilated. This is in contrast to classic cirrhosis from other etiologies, where fibrotic contraction can narrow venous structures.
A controlled study of 106 individuals by Kutty et al. found higher resistance and pulsatility indices in the celiac trunk and mesenteric artery, along with a significant decrease in portal velocity in Fontan patients [57]. These changes can be observed in cirrhosis of any etiology as they reflect hemodynamic consequences of cirrhosis in general. In advanced cirrhosis, increased intrahepatic vascular resistance leads to reduced portal inflow, which causes a compensatory increase in arterial inflow. Over time, changes in downstream compliance and resistance cause elevated RI and PI in splanchnic arteries. In FALD, the portal flow is often lower than in other cirrhosis types, and hepatic artery compensation may be more marked. Tellez et al. [59,60] describe that the portal hypertension model in FALD is characteristically hypodynamic and arterial splanchnic perfusion may also be impaired, as shown in Doppler studies. Indeed, this is what makes FALD a unique entity.
8.1. Ultrasound Differentiation of Liver Nodules
In FALD patients, these are typically multiple, hypervascular, hyperechoic nodules, smaller than 3 cm, and located at the liver’s outer margins. Hypervascular liver nodules are common in Fontan patients, with the vast majority representing benign regenerative nodules or focal nodular hyperplasia (FNH) [59] (Table 6). The exact pathophysiology underlying nodule formation remains unclear, but their peripheral location and radiological characteristics suggest a vascular origin. It has been hypothesized that central venous hypertension, transmitted directly to hepatic perivenular areas, reduces portal blood flow and promotes arterialization [61]. The prevalence of these nodules in adult Fontan patients ranges from 20% to 30% [59]. These nodules, often termed large regenerative nodules or FNH-like nodules, have also been identified in other conditions involving hepatic venous outflow obstruction, such as Budd-Chiari syndrome and right heart failure [59].
FNH-like nodules in FALD tend to be small, multiple, and predominantly located in the right lobe near the liver surface and within 2 cm (Figure 14 and Figure 15) [62]. On B-mode evaluation, FNH-like nodules often appear as small, hyperechoic, and sometimes multiple lesions, mostly located in the right hepatic lobe [61]. In contrast-enhanced ultrasound (CEUS), FNH-like nodules in FALD exhibit enhancement patterns similar to FNH, including hyperenhancement in the arterial phase, centrifugal enhancement, central stellate vasculature, and sustained enhancement without washout [61]. These nodules may demonstrate central hypoenhancement in the portal and late phase, corresponding to a central scar [61]. On CT, arterial phase nodules appear hyperenhancing compared to the surrounding liver parenchyma. In portal and delayed phases, they generally remain iso- or hyperattenuating, but occasional washout may be seen, due to background parenchymal congestion. On MRI T1- and T2-weighted sequences, the nodules are isointense or mildly hypointense on T1 and isointense or mildly hyperintense on T2 [63]. A central scar, hypointense on T1 and hyperintense on T2, may be present [63]. In the hepatobiliary phase, FNH-like nodules retain contrast and appear hyperintense [63]. This helps differentiate them from HCC, which usually appears hypointense in this phase. On DWI (Diffusion-weighted imaging), these nodules do not restrict diffusion, in contrast to HCC, which often shows diffusion restriction [63].
9. Hepatocellular Carcinoma (Hcc) in Fald
HCC can develop in adult patients with FALD [64]. Routine HCC surveillance in FALD has been recommended, but there is no consensus on surveillance frequency, imaging modalities, or the optimal timing after the Fontan procedure [3,59]. The progression from a dysplastic nodule to HCC is a potential stepwise pathway in Fontan-associated cirrhosis. Interval size increase, washout in the portal venous phase, mosaic architecture, and elevated alpha-fetoprotein levels may indicate malignancy [30,48].
HCC typically presents with arterial-phase hyperenhancement followed by mild late washout on dynamic contrast-enhanced imaging [23,65,66,67,68]. Suspicion of HCC increases with large nodule size, interval growth, echogenicity changes, a mass-like appearance, or nodules causing contour abnormalities on the liver surface. FNH-like nodules often show arterial hyperenhancement and no washout on CEUS, mimicking classic FNH. However, some may exhibit delayed washout, raising suspicion for HCC. Therefore, correlation with MRI and clinical context is essential to avoid misdiagnosis and unnecessary interventions [61,69]. Wells et al. argued that washout might not indicate an intrinsic abnormality of the nodule itself but rather reflect the background parenchymal contrast retention due to hepatic congestion and fibrosis [70]. Screening every 4–12 months using radiological techniques is cost-effective and improves survival in cirrhotic patients. Most experts recommend periodic surveillance, though the optimal imaging method and interval remain undetermined [71,72]. HCC treatment should follow standard clinical guidelines used for other cirrhosis etiologies [73].
10. Contrast-Enhanced Ultrasound (Ceus) in Fald
CEUS is valuable for characterizing the contrast enhancement patterns of liver nodules [74,75,76]. In Europe, the US contrast agent SonoVue® (sulfur hexafluoride; Bracco, Milan, Italy) is approved only for intravenous applications in patients over 18 years of age. CEUS use in Fontan patients remains limited due to their frequent collateral circulation with right-to-left shunts, which is considered a contraindication in Europe but not in the United States. Beyond structural liver changes, CEUS reveals markedly heterogeneous hepatic enhancement with mosaic or reticular patterns, mainly due to slow and reduced enhancement near congested hepatic veins—one of the most common imaging features of FALD [48,77]. Anecdotal experience suggests that CEUS demonstrates heterogeneous and decreased liver enhancement in the portal venous phase, similar to cirrhosis of other etiologies (Figure 16, Figure 17 and Figure 18). Abnormal enhancement is more prominent at the liver periphery than centrally, while the hypertrophic caudate lobe often shows more homogeneous enhancement. In patients with FALD, the altered hemodynamics resulting from chronic hepatic venous congestion and low cardiac output can significantly influence CEUS dynamics. Despite these circulatory changes, CEUS in FALD generally preserves the standard temporal enhancement pattern. The hepatic veins, although congested, do not typically show early enhancement, as microbubble distribution primarily reflects arterial input. The systemic hypokinetic circulation characteristic of FALD may lead to delayed arterial arrival times and a prolonged transit of contrast, especially in the background of the liver. Nonetheless, FNH-like nodules frequently exhibit intense and early arterial-phase hyperenhancement, suggesting preserved or increased arterial supply in these lesions. This contrast behavior is essential for lesion characterization.
CEUS plays a crucial role in evaluating hepatic nodules in FALD (Figure 19). In non-cardiac cirrhosis, contrast washout in the late phase is highly indicative of HCC. However, in FALD and other congestive hepatopathies like Budd-Chiari syndrome, FNH-like nodules can also exhibit delayed washout, leading to false positives if the LI-RADS system is strictly applied [78]. Washout in the portal venous phase, in contrast, is uncommon in FNH-like nodules and more specific for HCC [69]. Despite limitations, ancillary LI-RADS criteria and portal venous phase washout remain useful for identifying potentially malignant lesions [79,80].
Therefore, CEUS in FALD must be interpreted with awareness of the altered vascular physiology, and ideally integrated with MR findings and clinical context for accurate diagnosis and longitudinal monitoring.
11. Liver & Spleen Stiffness
Different elastography techniques have been investigated for liver stiffness measurement (LSM) in Fontan patients, including point shear-wave elastography (also known as point radiation force impulse), two-dimensional shear-wave elastography imaging, transient elastography (TE) (Fibroscan®), and MR elastography (MRE) [81,82,83,84,85,86,87]. However, their application in Fontan patients remains challenging because systemic venous congestion can lead to an overestimation of LSM (Table 7). Fontan surgery results in an immediate increase in liver stiffness (LS) due solely to hepatic congestion [88] (Figure 20). Over time, signs of Fontan failure typically emerge, leading to further increases in LS values, which may exceed 15 kPa levels indicative of advanced disease stages in non-congestive liver diseases. In these cases, fibrosis progression may play a role [25,71]. Real-time tissue elastography (RTE) has been shown to reflect liver fibrosis in FALD from the early stages. When combined with hepatic vein waveform analysis, RTE has proven to be a valuable non-invasive tool for evaluating clinical conditions in FALD patients [31].
US elastography, particularly shear-wave techniques, is increasingly being used for serial follow-up in these patients [89,90,91,92,93,94,95,96,97,98,99,100]. Longitudinal LSM assessment during follow-up could help monitor disease progression and predict clinical outcomes. However, elastography results must be interpreted with caution in the Fontan population, as no validated cut-off values for severe liver fibrosis exist for this specific group, unlike in other forms of chronic liver disease [89,90,91,92,93,94,95,96,97,98,99,100,101].
A few small studies have been published correlating spleen stiffness measurement (SSM) with liver fibrosis, but no firm conclusions can be drawn [100,104,105,106]. One prospective study reported that SSM was higher in children with Fontan circulation than in healthy controls [107].On the other hand, a retrospective study found SWE-SSM to be comparable to that of healthy controls [106]. Thus, more studies are needed to evaluate the role of spleen stiffness measurement in staging FALD.
12. Liver Ultrasound-Guided Biopsy
Liver biopsy is the gold standard diagnostic procedure and is still necessary to determine the extent of liver damage [42,108,109]. Typical histological features of FALD include sinusoidal dilation, centrilobular hemorrhagic necrosis, perisinusoidal fibrosis, ductular reaction, perivenular fibrous septa, central fibrous bridges, and nodular regenerative hyperplasia. Sinusoidal dilation is present in 90-97% of Fontan patients and is the earliest parenchymal change. Typically, it is more pronounced than in other causes of cardiogenic hepatopathy. The distribution of fibrosis in the early stages is typically perisinusoidal (in the space of Disse), which is not the case in other forms of cardiac-derived liver disease. Extensive bridges of centrilobular fibrosis associated with regenerative nodules are a late finding in patients with advanced liver disease. Periportal inflammation is usually minimal or absent, which helps differentiate FALD from other liver disease etiologies [110]. Some authors recommend a liver biopsy for all patients 10 years after Fontan surgery [71]. In a cohort of 67 patients, this strategy revealed that all patients developed hepatic fibrosis, and its extent increased over time. However, the authors found no correlation between the degree of fibrosis and clinically relevant events, hemodynamic, or analytical parameters [111], thereby questioning its utility in clinical practice. Liver biopsy is currently recommended when the etiology of liver disease is unclear or in candidates for heart and/or liver transplantation [57,112,113].
13. Ultrasound Follow-Up
In 2019, a statement from the American Heart Association acknowledged that there is insufficient evidence to develop clear recommendations, but that cardiac and end-organ surveillance in children and adults is warranted and clinically important [114] (Table 8). Monitoring should be performed by multidisciplinary Fontan/single-ventricle care clinics with healthcare personnel familiar with and experienced in managing Fontan circulation and complications. Cardiovascular imaging assessments are already common at many institutions and should be performed at regular intervals across all age groups. Cardiac MR, including anatomical and functional investigations, should be performed every 2–3 years, and CT angiography should be done when clinically indicated [115].Cardiac catheterization is recommended once every 10 years or when clinically indicated [116].End-organ status assessment is a newer concept, with imaging and frequency tailored to patient age: every 3–4 years for children under 12 years, and every 1–3 years for adolescents aged 12–18 years [116]. Findings at any test may alter the follow-up interval or trigger additional investigations. The general imaging strategy should be as follows [116]:
• Lymphatic and endocrine system: MR lymphography with T2-weighted MR imaging. Bone-age estimation and bone mineral density assessment are also recommended.
• Brain and neurocognitive function: Neurodevelopmental/cognitive testing and brain MRI can provide important information.
• Lungs: Chest radiography is recommended.
• Liver: Abdominal/liver ultrasound is recommended, including elastography if possible. MR, including liver biopsy, might be considered. Annual ultrasound imaging with elastography has been proposed, with more frequent controls if radiologic signs of fibrosis or nodules are found [116].
Some centers advocate annual liver MRI from adolescence onwards, later combined with ultrasound elastography when routine biopsy is proposed [116]. The risk of HCC in FALD should not be underestimated. Estimates of the cumulative incidence of HCC within 20 years after the Fontan procedure range from 0.6% to 4.9% and may be increasing over time [62,117,118]. HCC in this population also carries a poor prognosis, with less than 50% survival at 1 year, which is comparable to HCC secondary to other causes [119]. There is broad agreement on the need for liver imaging follow-up to detect possible malignancy. HCC is very unlikely within the first 10 years after Fontan-type surgery, with an exponential increase in risk over time [23]. However, according to LI-RADS criteria, imaging alone cannot accurately distinguish between malignant and benign nodules in the context of congestive hepatopathy, and biopsy is required for a definitive diagnosis [5]. Predictive factors for new-onset HCC include higher body mass index, worse NYHA functional class, poorer results on serological biomarkers of liver fibrosis (FIB-4 and APRI score), early Fontan circulatory failure, MELD score >19, and high levels of serum AFP [117]. Active HCC surveillance might be initiated at least 10 years after completion of the Fontan procedure and should be strongly considered earlier in the case of Fontan circulatory failure, even in the absence of cirrhosis. A practical approach could involve combining serial ultrasound (every 6 months) by experienced personnel with contrast-enhanced imaging at baseline (10 years after surgery) and periodically during follow-up to identify the full spectrum of liver nodules [120,121]. MR is generally preferred over CT, as hepatobiliary contrast agents offer advantages in diagnostic accuracy, and it is non-irradiating. However, a significant drawback is that MRI is contraindicated in many Fontan patients with older cardiac devices [121]. Although robust evidence is lacking, performing an MR at least every 1–2 years could be a practical and reasonable approach [122].
Serum AFP is a valuable complementary biomarker for diagnosing HCC in FALD, as it is elevated above the standard upper limit in 74–80% of patients diagnosed with HCC [122]. In a large prospective series with a high prevalence of non-neoplastic nodules (48%), no patient with Fontan-type surgery without HCC showed elevated AFP (defined as >7 ng/dl) [39]. Results from a large cohort of stable Fontan patients found that the likelihood of HCC was 26 times higher in patients with AFP levels > 10 ng/dl [36]. Interestingly, patients who did not develop HCC had a substantially lower AFP value (median: 2.9 ng/dl), supporting its role in predicting new-onset HCC in this population [36]. Consequently, elevated AFP levels in patients with FALD should always raise suspicion of HCC.
A 2023 EASL-ERN position paper emphasized the need for follow-up to be conducted within specialized multidisciplinary Fontan clinics [3] (figle 8). These teams should include hepatologists, cardiologists, and radiologists familiar with the unique pathophysiology of Fontan circulation and its complications. Cardiac MR is recommended every 2 to 3 years to evaluate ventricular function, flow dynamics, and Fontan pathway anatomy [3]. In patients with contraindications to MRI or when detailed hemodynamic data are required, cardiac catheterization is considered appropriate [3]. Annual liver ultrasound combined with elastography is advised as the first-line imaging modality [3]. At 10 years post-Fontan, a baseline liver MRI with hepatobiliary contrast is recommended to characterize hepatic architecture and detect potential nodules [3]. This should be repeated every 1 to 2 years, particularly in high-risk patients or when sonographic abnormalities are detected. In the event of suspicious lesions or inconclusive findings, contrast-enhanced CT or additional MR is warranted [3]. Given the limitations of standard LI-RADS criteria in the context of congestive hepatopathy, histological confirmation via liver biopsy is often necessary to distinguish benign nodules from HCC [3].
Serial AFP measurement should be incorporated into routine follow-up. An AFP value above 10 ng/mL has been identified as a strong predictor of HCC, and should prompt more aggressive diagnostic work-up, including advanced imaging or biopsy [3]. The timing of active HCC surveillance is typically initiated at least 10 years after Fontan completion, though earlier monitoring may be warranted in patients exhibiting Fontan circulatory failure or elevated non-invasive fibrosis scores such as FIB-4, APRI, or MELD >19 [3]. Surveillance intervals should remain flexible, with the frequency of imaging and biomarker assessment tailored to the patient's evolving risk profile and clinical findings.
14. Conclusion
Although the Fontan procedure has extended patients' lifespan, there remains a significant risk of morbidity and mortality. Patients undergoing the Fontan procedure at birth require lifelong follow-up with medical care, which has a considerable financial and societal impact. However, much remains unknown about how Fontan palliation affects patients differently. End-organ effects are increasingly recognized, with particular attention to cardiac, lymphatic, and liver changes, which require monitoring through radiological techniques to ensure optimal timing for treatment and, eventually, cardiac transplantation or combined liver-heart transplantation. FALD is an emerging liver disease that poses a significant clinical challenge. A FALD surveillance program should be recommended to detect liver disease progression at an early stage, allowing for interventions that optimize Fontan circulation and prevent advanced liver fibrosis. The lack of funding for research is a clear obstacle to expanding knowledge of FALD. Therefore, multi-institutional collaborative registries and prospective studies are essential.
Conflicts of Interest
authors declare no conflict of interest.
References
- Kreutzer G, Galíndez E, Bono H, De Palma C, Laura JP. An operation for the correction of tricuspid atresia. J Thorac Cardiovasc Surg. 1973, 66, 613–621. [Google Scholar] [CrossRef]
- Björk VO, Olin CL, Bjarke BB, Thorén CA. Right atrial-right ventricular anastomosis for correction of tricuspid atresia. J Thorac Cardiovasc Surg. 1979, 77, 452–458. [Google Scholar] [CrossRef]
- Téllez L, Payancé A, Tjwa E, Del Cerro MJ, Idorn L, Ovroutski S, et al. EASL-ERN position paper on liver involvement in patients with Fontan-type circulation. J Hepatol. 2023, 79, 1270–1301. [Google Scholar] [CrossRef] [PubMed]
- Cao JY, Wales KM, d'Udekem Y, Celermajer DS, Cordina R, Majumdar A. Prevalence, Risk Factors, and Prognosis for Fontan-Associated Liver Disease: A Systematic Review and Exploratory Meta-Analysis. JACC Adv. 2025, 4, 101694. [Google Scholar] [CrossRef]
- Gordon-Walker TT, Bove K, Veldtman G. Fontan-associated liver disease: A review. J Cardiol. 2019, 74, 223–232. [Google Scholar] [CrossRef]
- Emamaullee J, Martin S, Goldbeck C, Rocque B, Barbetta A, Kohli R, et al. Evaluation of Fontan-associated Liver Disease and Ethnic Disparities in Long-term Survivors of the Fontan Procedure: A Population-based Study. Ann Surg. 2022, 276, 482–490. [Google Scholar] [CrossRef]
- Hilscher MB, Johnson JN. Fontan-Associated Liver Disease. Semin Liver Dis. 2025, 45, 114–128. [Google Scholar] [CrossRef] [PubMed]
- Ignee A, Gebel M, Caspary WF, Dietrich CF. [Doppler imaging of hepatic vessels - review]. Z Gastroenterol. 2002, 40, 21–32. [Google Scholar]
- Dietrich CF, Lee JH, Gottschalk R, Herrmann G, Sarrazin C, Caspary WF, et al. Hepatic and portal vein flow pattern in correlation with intrahepatic fat deposition and liver histology in patients with chronic hepatitis C. AJR Am J Roentgenol. 1998, 171, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Simonetto DA, Yang HY, Yin M, de Assuncao TM, Kwon JH, Hilscher M, et al. Chronic passive venous congestion drives hepatic fibrogenesis via sinusoidal thrombosis and mechanical forces. Hepatology. 2015, 61, 648–659. [Google Scholar] [CrossRef]
- Hilscher MB, Sehrawat T, Arab JP, Zeng Z, Gao J, Liu M, et al. Mechanical Stretch Increases Expression of CXCL1 in Liver Sinusoidal Endothelial Cells to Recruit Neutrophils, Generate Sinusoidal Microthombi, and Promote Portal Hypertension. Gastroenterology. 2019, 157, 193–209.e9. [Google Scholar] [CrossRef] [PubMed]
- Thomas, H. LSEC stretch promotes fibrosis during hepatic vascular congestion. Nat Rev Gastroenterol Hepatol. 2019, 16, 262–263. [Google Scholar] [CrossRef] [PubMed]
- Dietrich CF, Trenker C, Fontanilla T, Görg C, Hausmann A, Klein S, et al. New Ultrasound Techniques Challenge the Diagnosis of Sinusoidal Obstruction Syndrome. Ultrasound Med Biol. 2018, 44, 2171–2182. [Google Scholar] [CrossRef]
- Dijkstra H, Wolff D, van Melle JP, Bartelds B, Willems TP, Oudkerk M, et al. Diminished liver microperfusion in Fontan patients: A biexponential DWI study. PLoS One. 2017, 12, e0173149. [Google Scholar]
- Durongpisitkul K, Driscoll DJ, Mahoney DW, Wollan PC, Mottram CD, Puga FJ, et al. Cardiorespiratory response to exercise after modified Fontan operation: determinants of performance. J Am Coll Cardiol. 1997, 29, 785–790. [Google Scholar] [CrossRef] [PubMed]
- Ohuchi H, Mori A, Nakai M, Fujimoto K, Iwasa T, Sakaguchi H, et al. Pulmonary Arteriovenous Fistulae After Fontan Operation: Incidence, Clinical Characteristics, and Impact on All-Cause Mortality. Front Pediatr. 2022, 10, 713219. [Google Scholar] [CrossRef]
- Daems JJN, Attard C, Van Den Helm S, Breur J, D'Udekem Y, du Plessis K, et al. Cross-sectional assessment of haemostatic profile and hepatic dysfunction in Fontan patients. Open Heart.
- Skubera M, Gołąb A, Plicner D, Natorska J, Ząbczyk M, Trojnarska O, et al. Properties of Plasma Clots in Adult Patients Following Fontan Procedure: Relation to Clot Permeability and Lysis Time-Multicenter Study. J Clin Med.
- McCrindle BW, Michelson AD, Van Bergen AH, Suzana Horowitz E, Pablo Sandoval J, Justino H, et al. Thromboprophylaxis for Children Post-Fontan Procedure: Insights From the UNIVERSE Study. J Am Heart Assoc. 2021, 10, e021765. [Google Scholar] [CrossRef]
- Jeong J, Tanaka M, Iwakiri Y. Hepatic lymphatic vascular system in health and disease. J Hepatol. 2022, 77, 206–218. [Google Scholar] [CrossRef]
- Tanaka M, Iwakiri Y. Lymphatics in the liver. Curr Opin Immunol. 2018, 53, 137–142. [Google Scholar] [CrossRef]
- Cox DA, Ginde S, Tweddell JS, Earing MG. Outcomes of a hepatitis C screening protocol in at-risk adults with prior cardiac surgery. World J Pediatr Congenit Heart Surg. 2014, 5, 503–506. [Google Scholar] [CrossRef]
- de Lange C, Möller T, Hebelka H. Fontan-associated liver disease: Diagnosis, surveillance, and management. Front Pediatr. 2023, 11, 1100514. [Google Scholar] [CrossRef]
- Kiesewetter CH, Sheron N, Vettukattill JJ, Hacking N, Stedman B, Millward-Sadler H, et al. Hepatic changes in the failing Fontan circulation. Heart. 2007, 93, 579–584. [Google Scholar] [CrossRef]
- Agnoletti G, Ferraro G, Bordese R, Marini D, Gala S, Bergamasco L, et al. Fontan circulation causes early, severe liver damage. Should we offer patients a tailored strategy? Int J Cardiol. 2016, 209, 60–65. [Google Scholar] [CrossRef]
- D'Amico G, De Franchis R. Upper digestive bleeding in cirrhosis. Post-therapeutic outcome and prognostic indicators. Hepatology. 2003, 38, 599–612. [Google Scholar] [CrossRef] [PubMed]
- Ohuchi, H. What are the mechanisms for FALD and how can we prevent the progression? Int J Cardiol. 2018, 273, 121–122. [Google Scholar] [CrossRef] [PubMed]
- Hansen JH, Khodami JK, Moritz JD, Rinne K, Voges I, Scheewe J, et al. Surveillance of Fontan Associated Liver Disease in Childhood and Adolescence. Semin Thorac Cardiovasc Surg. 2022, 34, 642–650. [Google Scholar] [CrossRef]
- Dillman JR, Trout AT, Alsaied T, Gupta A, Lubert AM. Imaging of Fontan-associated liver disease. Pediatr Radiol. 2020, 50, 1528–1541. [Google Scholar] [CrossRef]
- Bae JM, Jeon TY, Kim JS, Kim S, Hwang SM, Yoo SY, et al. Fontan-associated liver disease: Spectrum of US findings. Eur J Radiol. 2016, 85, 850–856. [Google Scholar] [CrossRef] [PubMed]
- Koizumi Y, Hirooka M, Tanaka T, Watanabe T, Yoshida O, Tokumoto Y, et al. Noninvasive ultrasound technique for assessment of liver fibrosis and cardiac function in Fontan-associated liver disease: diagnosis based on elastography and hepatic vein waveform type. J Med Ultrason (2001). 2021, 48, 235–244. [Google Scholar] [CrossRef]
- Brown MJ, Kolbe AB, Hull NC, Hilscher M, Kamath PS, Yalon M, et al. Imaging of Fontan-Associated Liver Disease. J Comput Assist Tomogr. 2024, 48, 1–11. [Google Scholar] [CrossRef]
- Griffiths ER, Lambert LM, Ou Z, Shaaban A, Rezvani M, Carlo WF, et al. Fontan-associated liver disease after heart transplant. Pediatr Transplant. 2023, 27, e14435. [Google Scholar] [CrossRef]
- Shahid MU, Frenkel Y, Kuc N, Golowa Y, Cynamon J. Transfemoral-Transcaval Liver Biopsy (TFTC) and Transjugular Liver Biopsy (TJLB) in Patients with Fontan-Associated Liver Disease (FALD). Cardiovasc Intervent Radiol. 2024, 47, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Borquez AA, Silva-Sepulveda J, Lee JW, Vavinskaya V, Vodkin I, El-Sabrout H, et al. Transjugular liver biopsy for Fontan associated liver disease surveillance: Technique, outcomes and hemodynamic correlation. Int J Cardiol. 2021, 328, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Francalanci P, Giovannoni I, Tancredi C, Gagliardi MG, Palmieri R, Brancaccio G, et al. Histopathological Spectrum and Molecular Characterization of Liver Tumors in the Setting of Fontan-Associated Liver Disease. Cancers (Basel).
- Emamaullee J, Khan S, Weaver C, Goldbeck C, Yanni G, Kohli R, et al. Non-invasive biomarkers of Fontan-associated liver disease. JHEP Rep. 2021, 3, 100362. [Google Scholar] [CrossRef]
- Feeley M, Hopkins K, Grinspan LT, Schiano T, Love B, Chan A, et al. Challenges in Accurate Diagnosis of HCC in FALD: A Case Series. Pediatr Cardiol. 2023, 44, 1447–1453. [Google Scholar] [CrossRef]
- D'Amato J, Bianco EZ, Camilleri J, Debattista E, Ellul P. Hepatocellular carcinoma in Fontan-associated liver disease. Ann Gastroenterol. 2025, 38, 133–142. [Google Scholar]
- Dietrich CF, Shi L, Löwe A, Dong Y, Potthoff A, Sparchez Z, et al. Conventional ultrasound for diagnosis of hepatic steatosis is better than believed. Z Gastroenterol. 2022, 60, 1235–1248. [Google Scholar] [CrossRef]
- Salvatore V, Borghi A, Peri E, Colecchia A, Li Bassi S, Montrone L, et al. Relationship between hepatic haemodynamics assessed by Doppler ultrasound and liver stiffness. Dig Liver Dis. 2012, 44, 154–159. [Google Scholar] [CrossRef]
- Zheng RQ, Wang QH, Lu MD, Xie SB, Ren J, Su ZZ, et al. Liver fibrosis in chronic viral hepatitis: an ultrasonographic study. World journal of gastroenterology. 2003, 9, 2484–2489. [Google Scholar] [CrossRef]
- Seol JH, Song J, Kim SJ, Ko H, Na JY, Cho MJ, et al. Clinical predictors and noninvasive imaging in Fontan-associated liver disease: A systematic review and meta-analysis. Hepatol Commun.
- Garagiola ML, Tan SB, Alonso-Gonzalez R, O'Brien CM. Liver Imaging in Fontan Patients: How Does Ultrasound Compare to Cross-Sectional Imaging? JACC Adv. 2024, 3, 101357. [Google Scholar] [CrossRef] [PubMed]
- Thrane KJ, Müller LSO, Suther KR, Thomassen KS, Holmström H, Thaulow E, et al. Spectrum of Fontan-associated liver disease assessed by MRI and US in young adolescents. Abdom Radiol (NY). 2021, 46, 3205–3216. [Google Scholar] [CrossRef] [PubMed]
- Liu X, Han L, Zhou Z, Tu J, Ma J, Chen J. Effect of liver abnormalities on mortality in Fontan patients: a systematic review and meta-analysis. BMC Cardiovasc Disord. 2024, 24, 385. [Google Scholar]
- Heering G, Lebovics N, Agarwal R, Frishman WH, Lebovics E. Fontan-Associated Liver Disease: A Review. Cardiol Rev.
- Wells ML, Fenstad ER, Poterucha JT, Hough DM, Young PM, Araoz PA, et al. Imaging Findings of Congestive Hepatopathy. Radiographics. 2016, 36, 1024–1037. [Google Scholar] [CrossRef]
- Nakatsuka T, Soroida Y, Nakagawa H, Shindo T, Sato M, Soma K, et al. Identification of liver fibrosis using the hepatic vein waveform in patients with Fontan circulation. Hepatol Res. 2019, 49, 304–313. [Google Scholar] [CrossRef]
- Giannini E, Botta F, Borro P, Risso D, Romagnoli P, Fasoli A, et al. Platelet count/spleen diameter ratio: proposal and validation of a non-invasive parameter to predict the presence of oesophageal varices in patients with liver cirrhosis. Gut. 2003, 52, 1200–1205. [Google Scholar] [CrossRef] [PubMed]
- Hsia TY, Khambadkone S, Deanfield JE, Taylor JF, Migliavacca F, De Leval MR. Subdiaphragmatic venous hemodynamics in the Fontan circulation. J Thorac Cardiovasc Surg. 2001, 121, 436–447. [Google Scholar] [CrossRef]
- Hsia TY, Khambadkone S, Redington AN, De Leval MR. Instantaneous pressure-flow velocity relations of systemic venous return in patients with univentricular circulation. Heart. 2000, 83, 583. [Google Scholar]
- Hsia TY, Khambadkone S, Redington AN, de Leval MR. Effect of fenestration on the sub-diaphragmatic venous hemodynamics in the total-cavopulmonary connection. Eur J Cardiothorac Surg. 2001, 19, 785–792. [Google Scholar] [CrossRef]
- McNaughton DA, Abu-Yousef MM. Doppler US of the liver made simple. Radiographics. 2011, 31, 161–188. [Google Scholar] [CrossRef]
- Moreno FL, Hagan AD, Holmen JR, Pryor TA, Strickland RD, Castle CH. Evaluation of size and dynamics of the inferior vena cava as an index of right-sided cardiac function. Am J Cardiol. 1984, 53, 579–585. [Google Scholar] [CrossRef]
- Camposilvan S, Milanesi O, Stellin G, Pettenazzo A, Zancan L, D'Antiga L. Liver and cardiac function in the long term after Fontan operation. Ann Thorac Surg. 2008, 86, 177–182. [Google Scholar] [CrossRef]
- Kutty SS, Peng Q, Danford DA, Fletcher SE, Perry D, Talmon GA, et al. Increased hepatic stiffness as consequence of high hepatic afterload in the Fontan circulation: a vascular Doppler and elastography study. Hepatology. 2014, 59, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Cura M, Haskal Z, Lopera J. Diagnostic and interventional radiology for Budd-Chiari syndrome. Radiographics. 2009, 29, 669–681. [Google Scholar] [CrossRef] [PubMed]
- Téllez L, Rodríguez de Santiago E, Minguez B, Payance A, Clemente A, Baiges A, et al. Prevalence, features and predictive factors of liver nodules in Fontan surgery patients: The VALDIG Fonliver prospective cohort. J Hepatol. 2020, 72, 702–710. [Google Scholar] [CrossRef]
- Wallihan DB, Podberesky DJ. Hepatic pathology after Fontan palliation: spectrum of imaging findings. Pediatr Radiol. 2013, 43, 330–338. [Google Scholar] [CrossRef]
- Çolaklar A, Lehnert SJ, Tirkes T. Benign Hepatic Nodules Mimicking Hepatocellular Carcinoma in the Setting of Fontan-associated Liver Disease: A Case Report. Euroasian J Hepatogastroenterol. 2020, 10, 42–44. [Google Scholar]
- Kogiso T, Tokushige K. Fontan-associated liver disease and hepatocellular carcinoma in adults. Sci Rep. 2020, 10, 21742. [Google Scholar] [CrossRef] [PubMed]
- Shiina Y, Inai K, Sakai R, Tokushige K, Nagao M. Hepatocellular carcinoma and focal nodular hyperplasia in patients with Fontan-associated liver disease: characterisation using dynamic gadolinium ethoxybenzyl diethylenetriamine pentaacetic acid-enhanced MRI. Clin Radiol. 2023, 78, e197–e203. [Google Scholar] [CrossRef]
- Nandwana SB, Olaiya B, Cox K, Sahu A, Mittal P. Abdominal Imaging Surveillance in Adult Patients After Fontan Procedure: Risk of Chronic Liver Disease and Hepatocellular Carcinoma. Curr Probl Diagn Radiol. 2018, 47, 19–22. [Google Scholar] [CrossRef]
- Josephus Jitta D, Wagenaar LJ, Mulder BJ, Guichelaar M, Bouman D, van Melle JP. Three cases of hepatocellular carcinoma in Fontan patients: Review of the literature and suggestions for hepatic screening. Int J Cardiol. 2016, 206, 21–26. [Google Scholar] [CrossRef]
- Rosenbaum J, Vrazas J, Lane GK, Hardikar W. Cardiac cirrhosis and hepatocellular carcinoma in a 13-year-old treated with doxorubicin microbead transarterial chemoembolization. J Paediatr Child Health. 2012, 48, E140–E143. [Google Scholar]
- Möller T, Klungerbo V, Diab S, Holmstrøm H, Edvardsen E, Grindheim G, et al. Circulatory Response to Rapid Volume Expansion and Cardiorespiratory Fitness in Fontan Circulation. Pediatr Cardiol. 2022, 43, 903–913. [Google Scholar] [CrossRef] [PubMed]
- Grosch IB, Andresen B, Diep LM, Diseth TH, Möller T. Quality of life and emotional vulnerability in a national cohort of adolescents living with Fontan circulation. Cardiol Young. 2022, 32, 874–882. [Google Scholar] [CrossRef] [PubMed]
- Kim TH, Yang HK, Jang HJ, Yoo SJ, Khalili K, Kim TK. Abdominal imaging findings in adult patients with Fontan circulation. Insights Imaging. 2018, 9, 357–367. [Google Scholar] [CrossRef]
- Wells ML, Hough DM, Fidler JL, Kamath PS, Poterucha JT, Venkatesh SK. Benign nodules in post-Fontan livers can show imaging features considered diagnostic for hepatocellular carcinoma. Abdom Radiol (NY). 2017, 42, 2623–2631. [Google Scholar] [CrossRef] [PubMed]
- Rychik J, Veldtman G, Rand E, Russo P, Rome JJ, Krok K, et al. The precarious state of the liver after a Fontan operation: summary of a multidisciplinary symposium. Pediatr Cardiol. 2012, 33, 1001–1012. [Google Scholar] [CrossRef]
- Wu FM, Kogon B, Earing MG, Aboulhosn JA, Broberg CS, John AS, et al. Liver health in adults with Fontan circulation: A multicenter cross-sectional study. J Thorac Cardiovasc Surg. 2017, 153, 656–664. [Google Scholar] [CrossRef]
- Reig M, Forner A, Ávila MA, Ayuso C, Mínguez B, Varela M, et al. Diagnosis and treatment of hepatocellular carcinoma. Update of the consensus document of the AEEH, AEC, SEOM, SERAM, SERVEI, and SETH. Med Clin (Barc). 2021, 156, 463.e1–e30. [Google Scholar] [CrossRef]
- Zander T, Zadeh ES, Möller K, Goerg C, Correas JM, Chaubal N, et al. Comments and illustrations of the WFUMB CEUS liver guidelines: Rare focal liver lesion - infectious parasitic, fungus. Med Ultrason. 2023, 25, 423–434. [Google Scholar] [CrossRef]
- Dong Y, Wang WP, Zadeh ES, Möller K, Görg C, Berzigotti A, et al. Comments and illustrations of the WFUMB CEUS liver guidelines: Rare benign focal liver lesion, part I. Med Ultrason. 2024, 26, 50–62. [Google Scholar]
- Dong Y, Guggisberg E, Wang WP, Zadeh ES, Görg C, Möller K, et al. Comments and illustrations of the WFUMB CEUS liver guidelines: Rare benign focal liver lesion, part II. Med Ultrason. 2024, 26, 168–177. [Google Scholar] [CrossRef]
- Bulut OP, Romero R, Mahle WT, McConnell M, Braithwaite K, Shehata BM, et al. Magnetic resonance imaging identifies unsuspected liver abnormalities in patients after the Fontan procedure. J Pediatr. 2013, 163, 201–206. [Google Scholar] [CrossRef]
- Van Wettere M, Purcell Y, Bruno O, Payancé A, Plessier A, Rautou PE, et al. Low specificity of washout to diagnose hepatocellular carcinoma in nodules showing arterial hyperenhancement in patients with Budd-Chiari syndrome. J Hepatol. 2019, 70, 1123–1132. [Google Scholar] [CrossRef]
- Tang A, Abukasm K, Moura Cunha G, Song B, Wang J, Wagner M, et al. Imaging of hepatocellular carcinoma: a pilot international survey. Abdom Radiol (NY). 2021, 46, 205–215. [Google Scholar] [CrossRef]
- Dietrich CF, Dong Y, Kono Y, Caraiani C, Sirlin CB, Cui XW, et al. LI-RADS ancillary features on contrast-enhanced ultrasonography. Ultrasonography. 2020, 39, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Ferraioli G, Barr RG, Berzigotti A, Sporea I, Wong VW, Reiberger T, et al. WFUMB Guideline/Guidance on Liver Multiparametric Ultrasound: Part 1. Update to 2018 Guidelines on Liver Ultrasound Elastography. Ultrasound Med Biol. 2024, 50, 1071–1087. [Google Scholar]
- Ferraioli G, Barr RG, Farrokh A, Radzina M, Cui XW, Dong Y, et al. How to perform shear wave elastography. Part I. Med Ultrason. 2022, 24, 95–106. [Google Scholar] [CrossRef] [PubMed]
- Ferraioli G, Barr RG, Farrokh A, Radzina M, Cui XW, Dong Y, et al. How to perform shear wave elastography. Part II. Med Ultrason. 2022, 24, 196–210. [Google Scholar] [CrossRef]
- Dietrich CF, Shi L, Wei Q, Dong Y, Cui XW, Löwe A, et al. What does liver elastography measure? Technical aspects and methodology. Minerva Gastroenterol (Torino). 2021, 67, 129–140. [Google Scholar]
- Dietrich CF, Ferraioli G, Sirli R, Popescu A, Sporea I, Pienar C, et al. General advice in ultrasound based elastography of pediatric patients. Med Ultrason. 2019, 21, 315–326. [Google Scholar] [CrossRef]
- Ferraioli G, Wong VW, Castera L, Berzigotti A, Sporea I, Dietrich CF, et al. Liver Ultrasound Elastography: An Update to the World Federation for Ultrasound in Medicine and Biology Guidelines and Recommendations. Ultrasound Med Biol. 2018, 44, 2419–2440. [Google Scholar] [CrossRef]
- Dietrich CF, Bamber J, Berzigotti A, Bota S, Cantisani V, Castera L, et al. EFSUMB Guidelines and Recommendations on the Clinical Use of Liver Ultrasound Elastography, Update 2017 (Long Version). Ultraschall Med. 2017, 38, e16–e47. [Google Scholar] [CrossRef]
- Deorsola L, Aidala E, Cascarano MT, Valori A, Agnoletti G, Pace Napoleone C. Liver stiffness modifications shortly after total cavopulmonary connection. Interact Cardiovasc Thorac Surg. 2016, 23, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Egbe A, Miranda WR, Connolly HM, Khan AR, Al-Otaibi M, Venkatesh SK, et al. Temporal changes in liver stiffness after Fontan operation: Results of serial magnetic resonance elastography. Int J Cardiol. 2018, 258, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Munsterman ID, Duijnhouwer AL, Kendall TJ, Bronkhorst CM, Ronot M, van Wettere M, et al. The clinical spectrum of Fontan-associated liver disease: results from a prospective multimodality screening cohort. Eur Heart J. 2019, 40, 1057–1068. [Google Scholar] [CrossRef]
- Schleiger A, Salzmann M, Kramer P, Danne F, Schubert S, Bassir C, et al. Severity of Fontan-Associated Liver Disease Correlates with Fontan Hemodynamics. Pediatr Cardiol. 2020, 41, 736–746. [Google Scholar] [CrossRef]
- Chemello L, Padalino M, Zanon C, Benvegnu L, Biffanti R, Mancuso D, et al. Role of Transient Elastography to Stage Fontan-Associated Liver Disease (FALD) in Adults with Single Ventricle Congenital Heart Disease Correction. J Cardiovasc Dev Dis.
- Nagasawa T, Kuroda H, Abe T, Saiki H, Takikawa Y. Shear wave dispersion to assess liver disease progression in Fontan-associated liver disease. PLoS One. 2022, 17, e0271223. [Google Scholar]
- Gill M, Mudaliar S, Prince D, Than NN, Cordina R, Majumdar A. Poor correlation of 2D shear wave elastography and transient elastography in Fontan-associated liver disease: A head-to-head comparison. JGH Open. 2023, 7, 690–697. [Google Scholar] [CrossRef]
- Jarasvaraparn C, Thoe J, Rodenbarger A, Masuoka H, Payne RM, Markham LW, et al. Biomarkers of fibrosis and portal hypertension in Fontan-associated liver disease in children and adults. Dig Liver Dis. 2024, 56, 1335–1342. [Google Scholar] [CrossRef]
- Bolia R, Alremawi S, Noble C, Justo R, Ward C, Lewindon PJ. Shear-wave elastography for monitoring Fontan-associated liver disease: A prospective cohort study. J Pediatr Gastroenterol Nutr. 2024, 79, 126–130. [Google Scholar] [CrossRef] [PubMed]
- Téllez L, Rincón D, Payancé A, Jaillais A, Lebray P, Rodríguez de Santiago E, et al. Non-invasive assessment of severe liver fibrosis in patients with Fontan-associated liver disease: The VALDIG-EASL FONLIVER cohort. J Hepatol. 2025, 82, 480–489. [Google Scholar] [CrossRef]
- Cuadros M, Abadía M, Castillo P, Martín-Arranz MD, Gonzalo N, Romero M, et al. Role of transient elastography in the diagnosis and prognosis of Fontan-associated liver disease. World journal of gastroenterology. 2025, 31, 103178. [Google Scholar]
- Imoto K, Goya T, Azuma Y, Hioki T, Aoyagi T, Nagata H, et al. Strain elastography for detecting advanced Fontan-associated liver disease: a retrospective study. BMC Gastroenterol. 2025, 25, 341. [Google Scholar] [CrossRef] [PubMed]
- Sakae H, Tanoue S, Mawatari S, Oda K, Taniyama O, Toyodome A, et al. Fontan-Associated Liver Disease: Predictors of Elevated Liver Stiffness and the Role of Transient Elastography in Long-Term Follow-Up. Cureus. 2025, 17, e85336. [Google Scholar]
- Abadeer M, Greer J, Reddy S, Divekar A, Schooler GR, Fares M, et al. The Importance of Hepatic Surveillance After Single-Ventricle Palliation: An Interventional Study Validating Liver Elastography. Pediatr Cardiol.
- Lo Yau Y, Coppola JA, Lopez-Colon D, Purlee M, Vyas H, Saulino DM, et al. Correlation of Liver Fibrosis on Ultrasound Elastography and Liver Biopsy After Fontan Operation: Is Non-invasive Always Better? Pediatr Cardiol. Pediatr Cardiol. 2025.
- Yau YL, Purlee MS, Brinkley LM, Gupta D, Saulino DM, Lopez-Colon D, et al. A Tense Race: Correlation of Liver Stiffness with Ultrasound Elastography and Hemodynamics in Fontan Patients. Congenit Heart Dis. 2025, 20, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Serai SD, Elsingergy MM, Hartung EA, Otero HJ. Liver and spleen volume and stiffness in patients post-Fontan procedure and patients with ARPKD compared to normal controls. Clin Imaging. 2022, 89, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Padalino MA, Chemello L, Cavalletto L, Angelini A, Fedrigo M. Prognostic Value of Liver and Spleen Stiffness in Patients with Fontan Associated Liver Disease (FALD): A Case Series with Histopathologic Comparison. J Cardiovasc Dev Dis.
- Venkatakrishna SSB, Ghosh A, Gonzalez IA, Wilkins BJ, Serai SD, Rand EB, et al. Spleen shear wave elastography measurements do not correlate with histological grading of liver fibrosis in Fontan physiology: a preliminary investigation. Pediatr Radiol. 2024, 54, 1998–2005. [Google Scholar] [CrossRef]
- Aliyev B, Bayramoglu Z, Nişli K, Omeroğlu RE, Dindar A. Quantification of Hepatic and Splenic Stiffness After Fontan Procedure in Children and Clinical Implications. Ultrasound Q. 2020, 36, 350–356. [Google Scholar] [CrossRef]
- Jenssen C, Hocke M, Fusaroli P, Gilja OH, Buscarini E, Havre RF, et al. EFSUMB Guidelines on Interventional Ultrasound (INVUS), Part IV - EUS-guided Interventions: General aspects and EUS-guided sampling (Long Version). Ultraschall Med. 2016, 37, E33–E76. [Google Scholar]
- Dietrich CF, Lorentzen T, Appelbaum L, Buscarini E, Cantisani V, Correas JM, et al. EFSUMB Guidelines on Interventional Ultrasound (INVUS), Part III - Abdominal Treatment Procedures (Long Version). Ultraschall Med. 2016, 37, E1–e32. [Google Scholar]
- Kendall TJ, Stedman B, Hacking N, Haw M, Vettukattill JJ, Salmon AP, et al. Hepatic fibrosis and cirrhosis in the Fontan circulation: a detailed morphological study. J Clin Pathol. 2008, 61, 504–508. [Google Scholar] [CrossRef]
- Goldberg DJ, Surrey LF, Glatz AC, Dodds K, O'Byrne ML, Lin HC, et al. Hepatic Fibrosis Is Universal Following Fontan Operation, and Severity is Associated With Time From Surgery: A Liver Biopsy and Hemodynamic Study. J Am Heart Assoc.
- Castéra L, Foucher J, Bernard PH, Carvalho F, Allaix D, Merrouche W, et al. Pitfalls of liver stiffness measurement: a 5-year prospective study of 13,369 examinations. Hepatology. 2010, 51, 828–835. [Google Scholar] [CrossRef]
- D'Souza BA, Fuller S, Gleason LP, Hornsby N, Wald J, Krok K, et al. Single-center outcomes of combined heart and liver transplantation in the failing Fontan. Clin Transplant.
- Rychik J, Atz AM, Celermajer DS, Deal BJ, Gatzoulis MA, Gewillig MH, et al. Evaluation and Management of the Child and Adult With Fontan Circulation: A Scientific Statement From the American Heart Association. Circulation. 2019, 140, e234–e84. [Google Scholar]
- Yoon JS, Lee DH, Cho EJ, Song MK, Choi YH, Kim GB, et al. Risk of Liver Cirrhosis and Hepatocellular Carcinoma after Fontan Operation: A Need for Surveillance. Cancers (Basel).
- Pundi K, Pundi KN, Kamath PS, Cetta F, Li Z, Poterucha JT, et al. Liver Disease in Patients After the Fontan Operation. Am J Cardiol. 2016, 117, 456–460. [Google Scholar] [CrossRef]
- Kogiso T, Sagawa T, Taniai M, Shimada E, Inai K, Shinohara T, et al. Risk factors for Fontan-associated hepatocellular carcinoma. PLoS One. 2022, 17, e0270230. [Google Scholar]
- Sagawa T, Kogiso T, Sugiyama H, Hashimoto E, Yamamoto M, Tokushige K. Characteristics of hepatocellular carcinoma arising from Fontan-associated liver disease. Hepatol Res. 2020, 50, 853–862. [Google Scholar] [CrossRef] [PubMed]
- Yamamura K, Sakamoto I, Morihana E, Hirata Y, Nagata H, Yamasaki Y, et al. Elevated non-invasive liver fibrosis markers and risk of liver carcinoma in adult patients after repair of tetralogy of Fallot. Int J Cardiol. 2019, 287, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Kogiso T, Tokushige K. Fontan-associated liver disease and hepatocellular carcinoma in adults. Scientific Reports. 2020, 10, 21742. [Google Scholar] [CrossRef]
- Possner M, Gordon-Walker T, Egbe AC, Poterucha JT, Warnes CA, Connolly HM, et al. Hepatocellular carcinoma and the Fontan circulation: Clinical presentation and outcomes. Int J Cardiol. 2021, 322, 142–148. [Google Scholar] [CrossRef]
- Téllez L, Payancé A, Tjwa E, del Cerro MJ, Idorn L, Ovroutski S, et al. EASL-ERN position paper on liver involvement in patients with Fontan-type circulation. Journal of Hepatology. 2023, 79, 1270–1301. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Fontan-type surgical approaches.
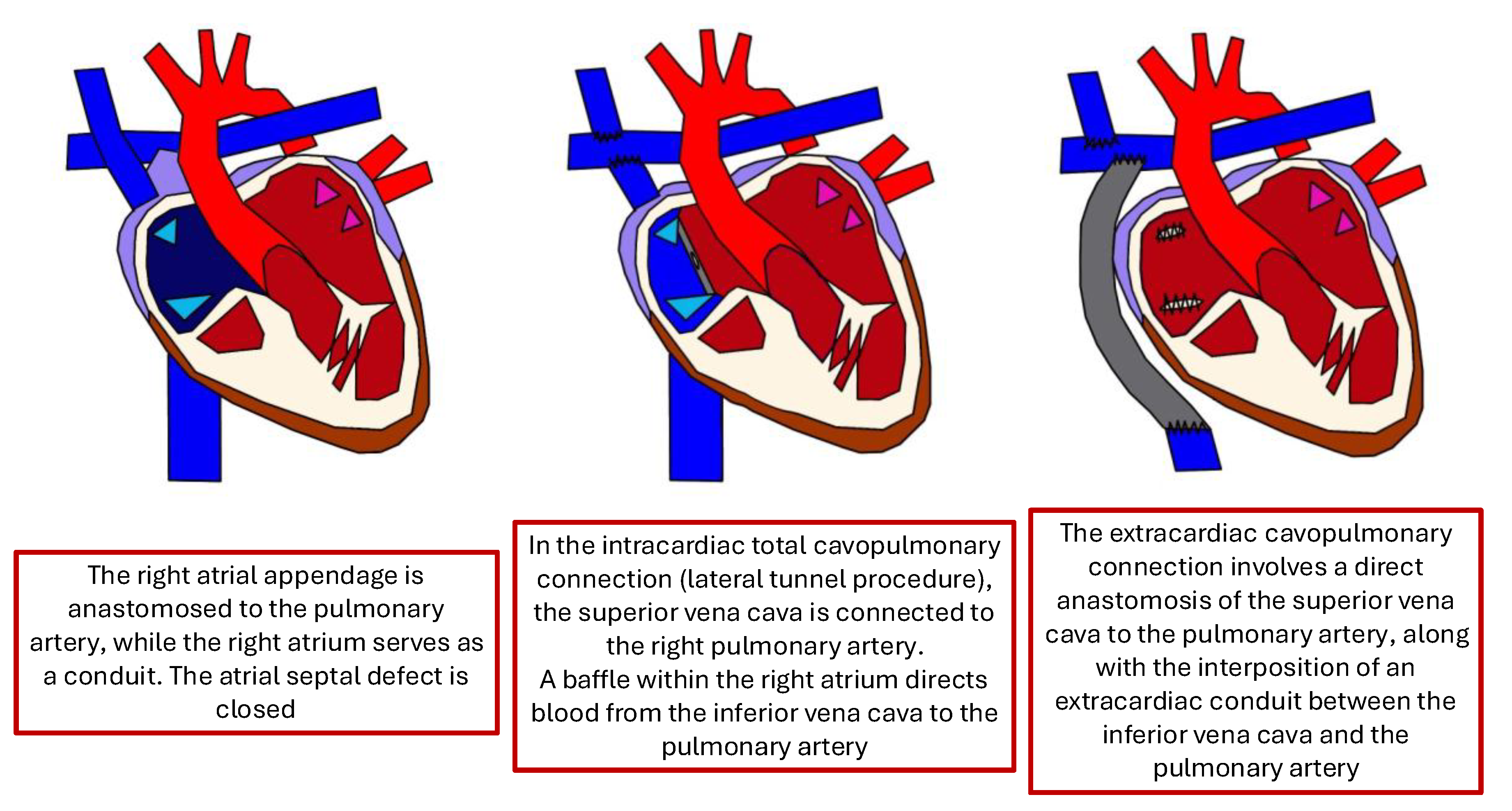
Figure 2.
Detail with convex probe in oblique subcostal scan: note the rounded margins, the heterogeneous echotexture, particularly in the left segments, and a marked hypotrophy of the right lobe.
Figure 2.
Detail with convex probe in oblique subcostal scan: note the rounded margins, the heterogeneous echotexture, particularly in the left segments, and a marked hypotrophy of the right lobe.
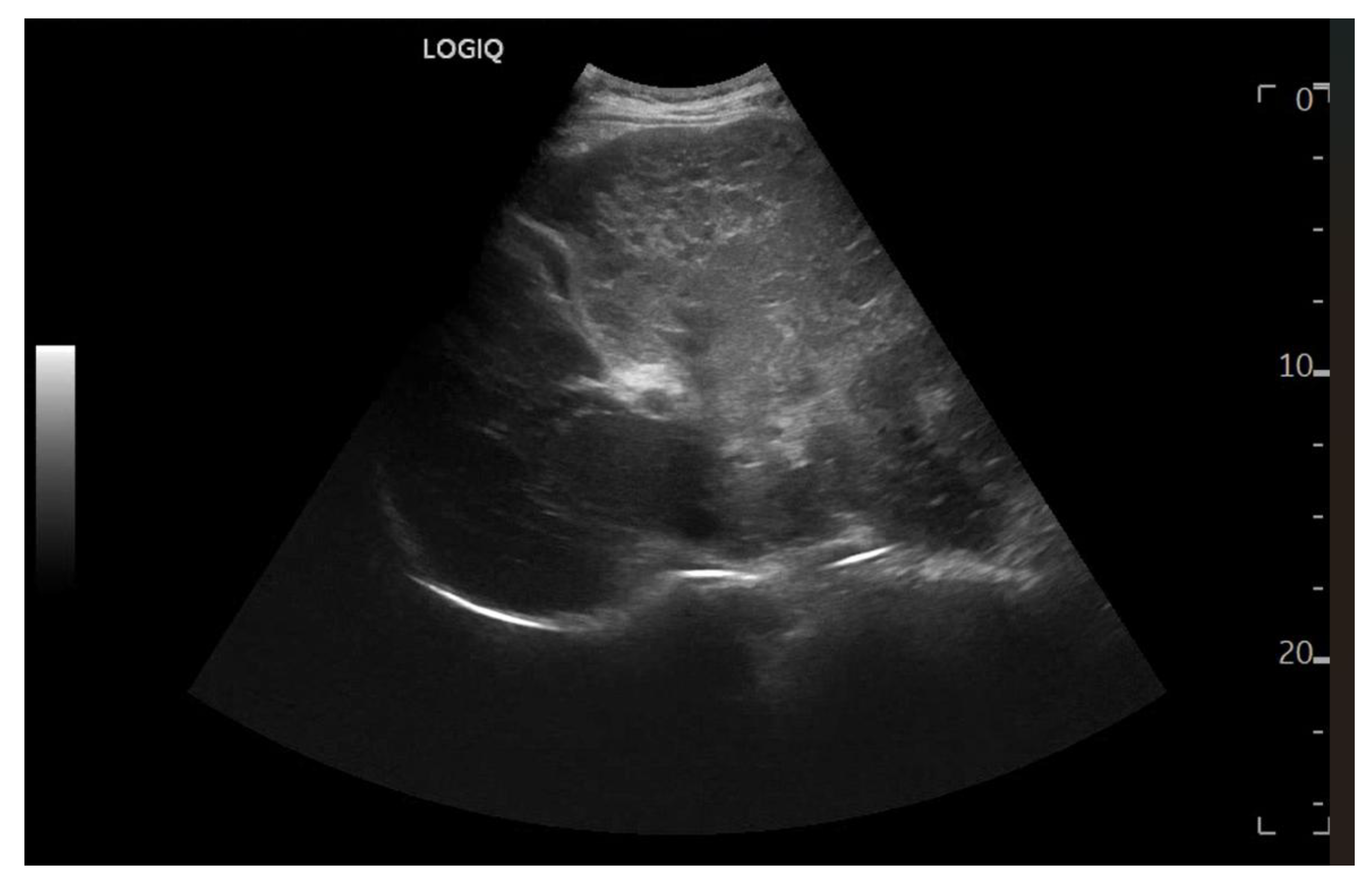
Figure 3.
Subcostal scan with convex probe showing symmetrical thickening of the gallbladder walls, consistent with congestion.
Figure 3.
Subcostal scan with convex probe showing symmetrical thickening of the gallbladder walls, consistent with congestion.
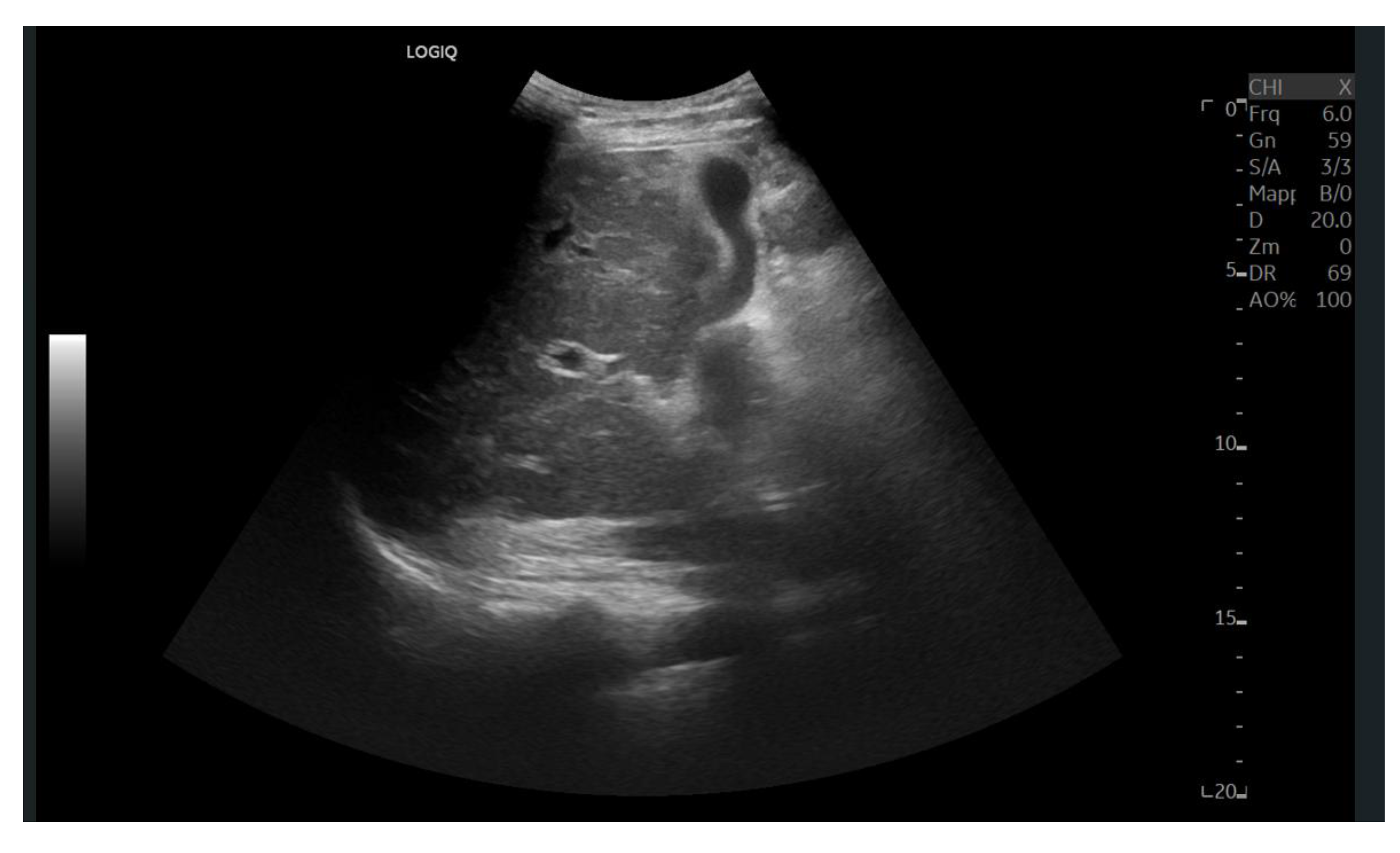
Figure 4.
Oblique subcostal scan with convex probe showing diffuse periportal edema.
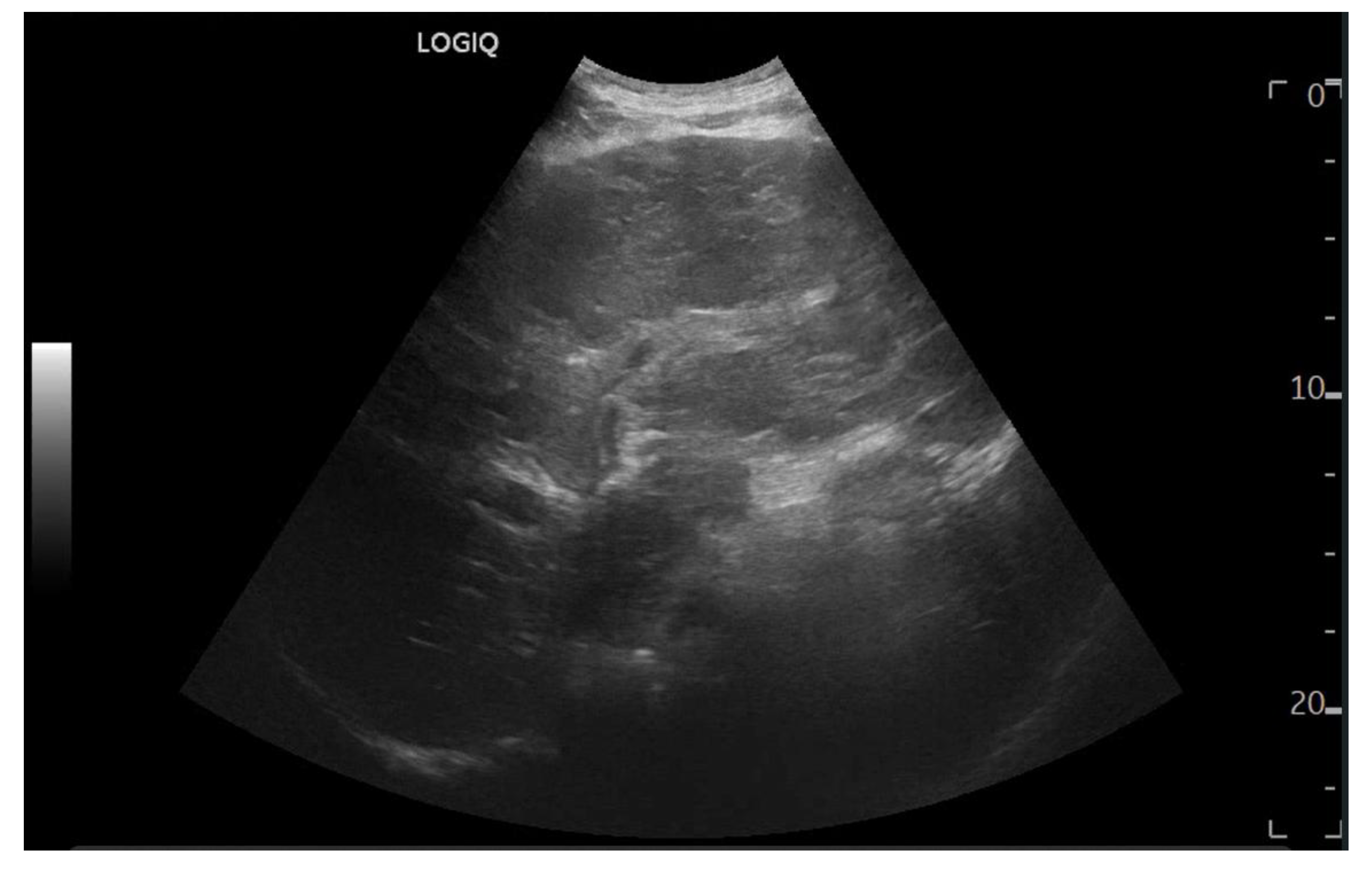
Figure 5.
Linear Probe (9 MHz) with trapezoidal scan. Diffusely dense and heterogeneous echostructure due to the presence of multiple and diffuse hyperechoic areas, suggestive of peri-portal fibrosis.
Figure 5.
Linear Probe (9 MHz) with trapezoidal scan. Diffusely dense and heterogeneous echostructure due to the presence of multiple and diffuse hyperechoic areas, suggestive of peri-portal fibrosis.
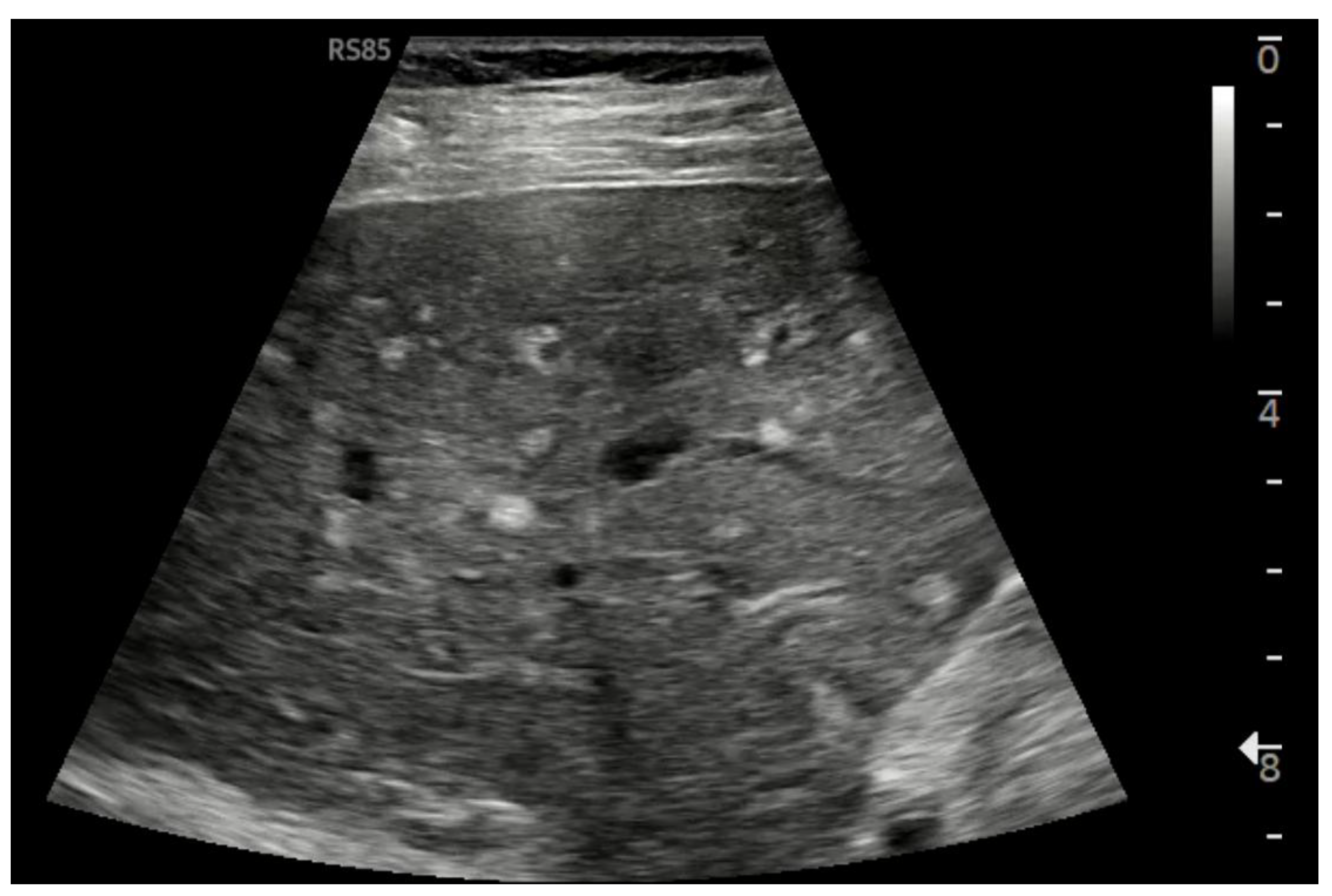
Figure 6.
Diffuse echostructural change of the left lobe with a heterogeneous hyperechoic area measuring 89 x 81 mm.
Figure 6.
Diffuse echostructural change of the left lobe with a heterogeneous hyperechoic area measuring 89 x 81 mm.
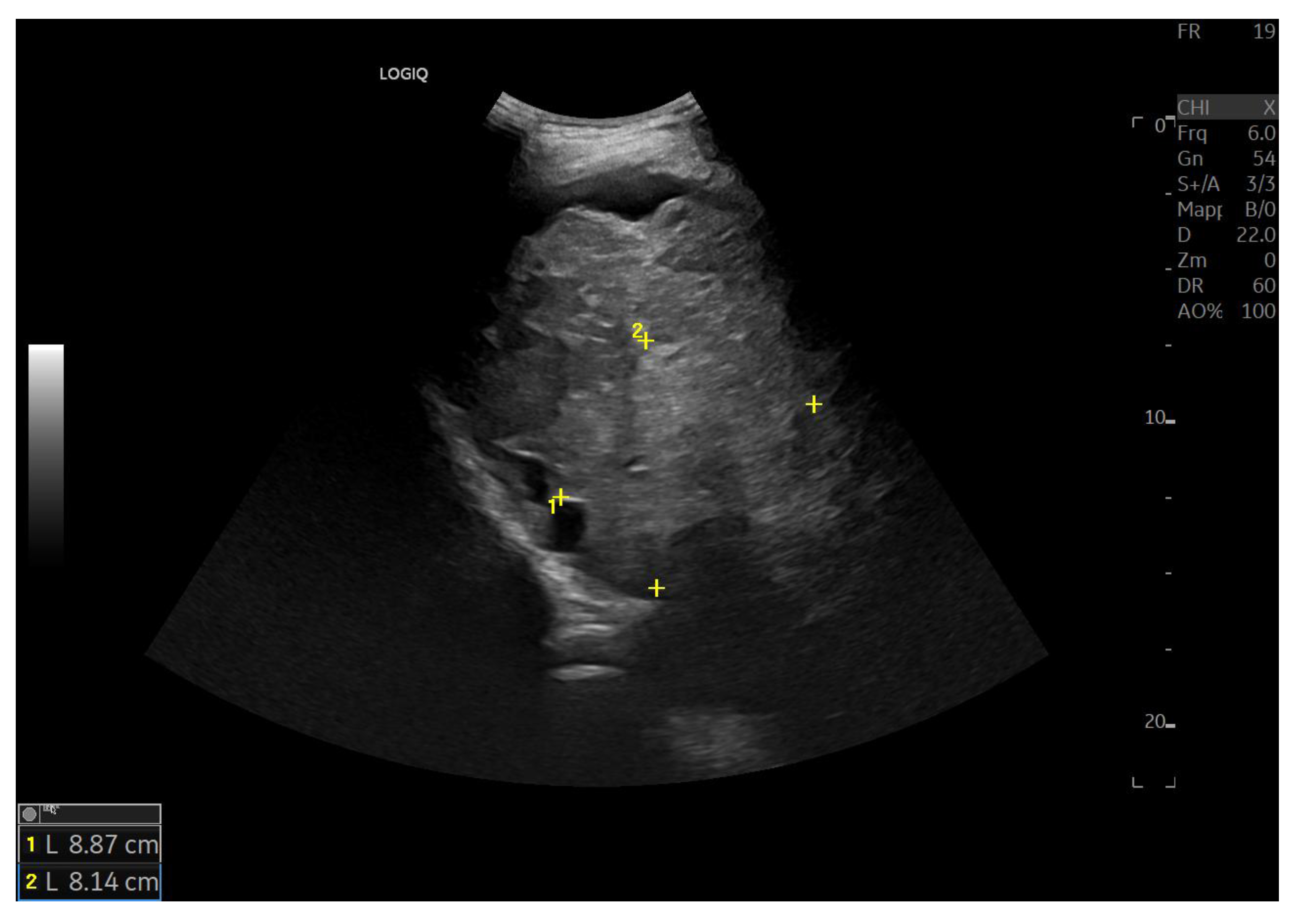
Figure 7.
Hypotrophy of the right lobe. Nodular profiles. Markedly heterogeneous echostructure, with increased fibrous component and fibrous trabeculae delimiting pseudo-nodular areas, within the context of a vascular-type cirrhosis.
Figure 7.
Hypotrophy of the right lobe. Nodular profiles. Markedly heterogeneous echostructure, with increased fibrous component and fibrous trabeculae delimiting pseudo-nodular areas, within the context of a vascular-type cirrhosis.

Figure 8.
Marked hypertrophy of the left lobe, which partially occupies the left hypochondrium.
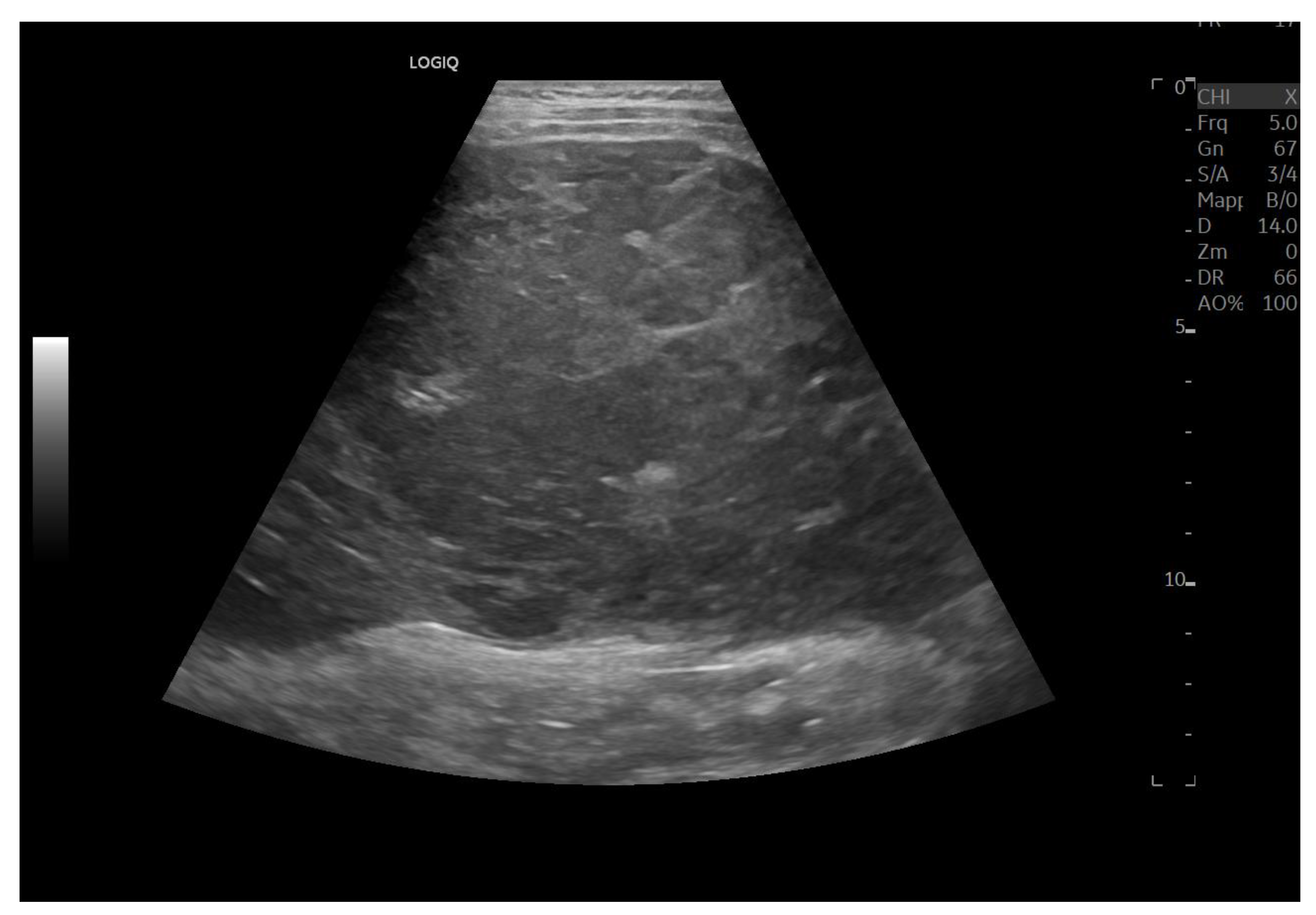
Figure 9.
Splenomegaly: bipolar diameter 16 cm (normal value: 12 cm); sectional area 81 cm2 (normal value: 45 cm2).
Figure 9.
Splenomegaly: bipolar diameter 16 cm (normal value: 12 cm); sectional area 81 cm2 (normal value: 45 cm2).
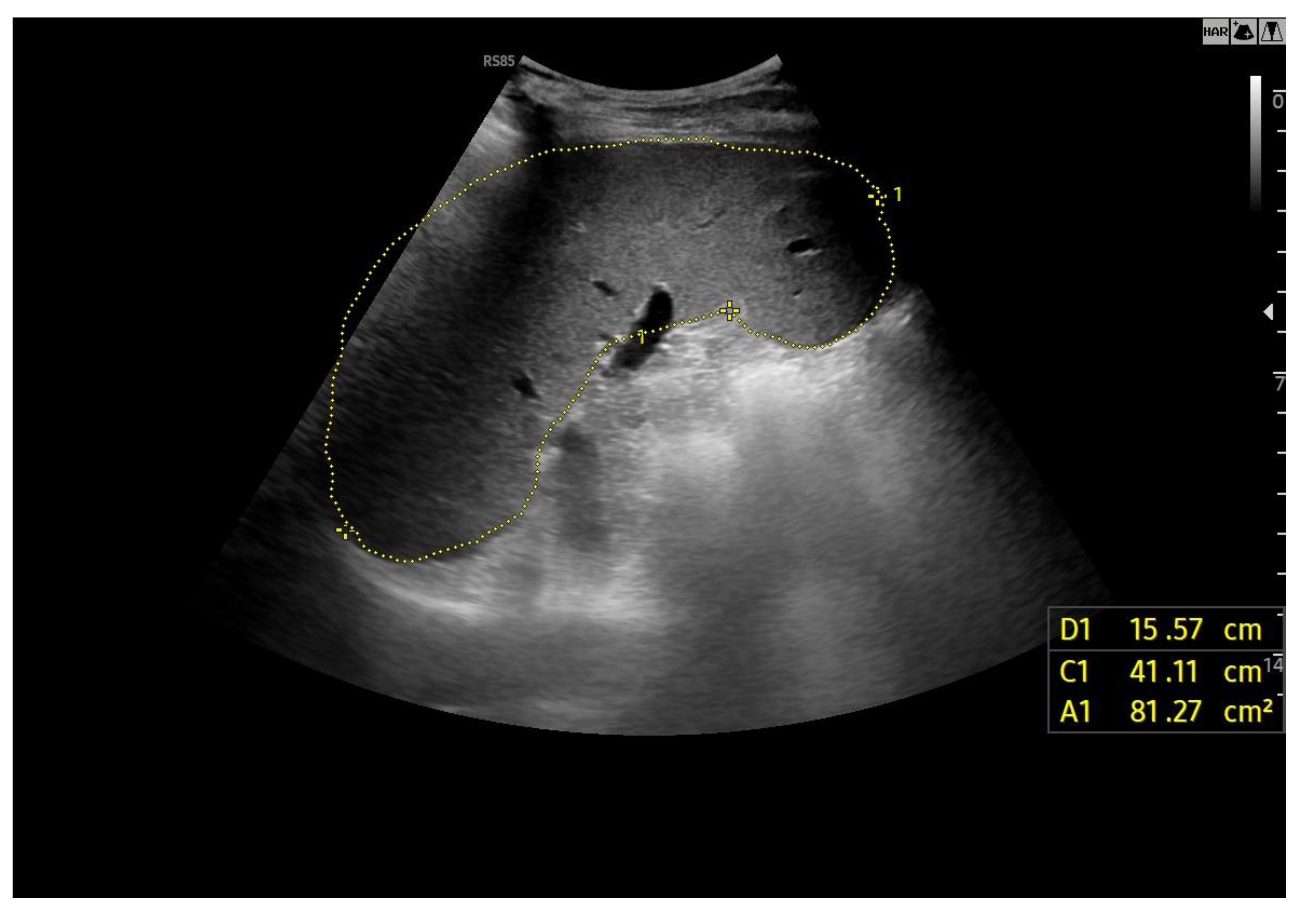
Figure 10.
Doppler Ultrasound of the middle hepatic vein showing the loss of the normal three-phase pattern due to the absence of atrial contraction.
Figure 10.
Doppler Ultrasound of the middle hepatic vein showing the loss of the normal three-phase pattern due to the absence of atrial contraction.
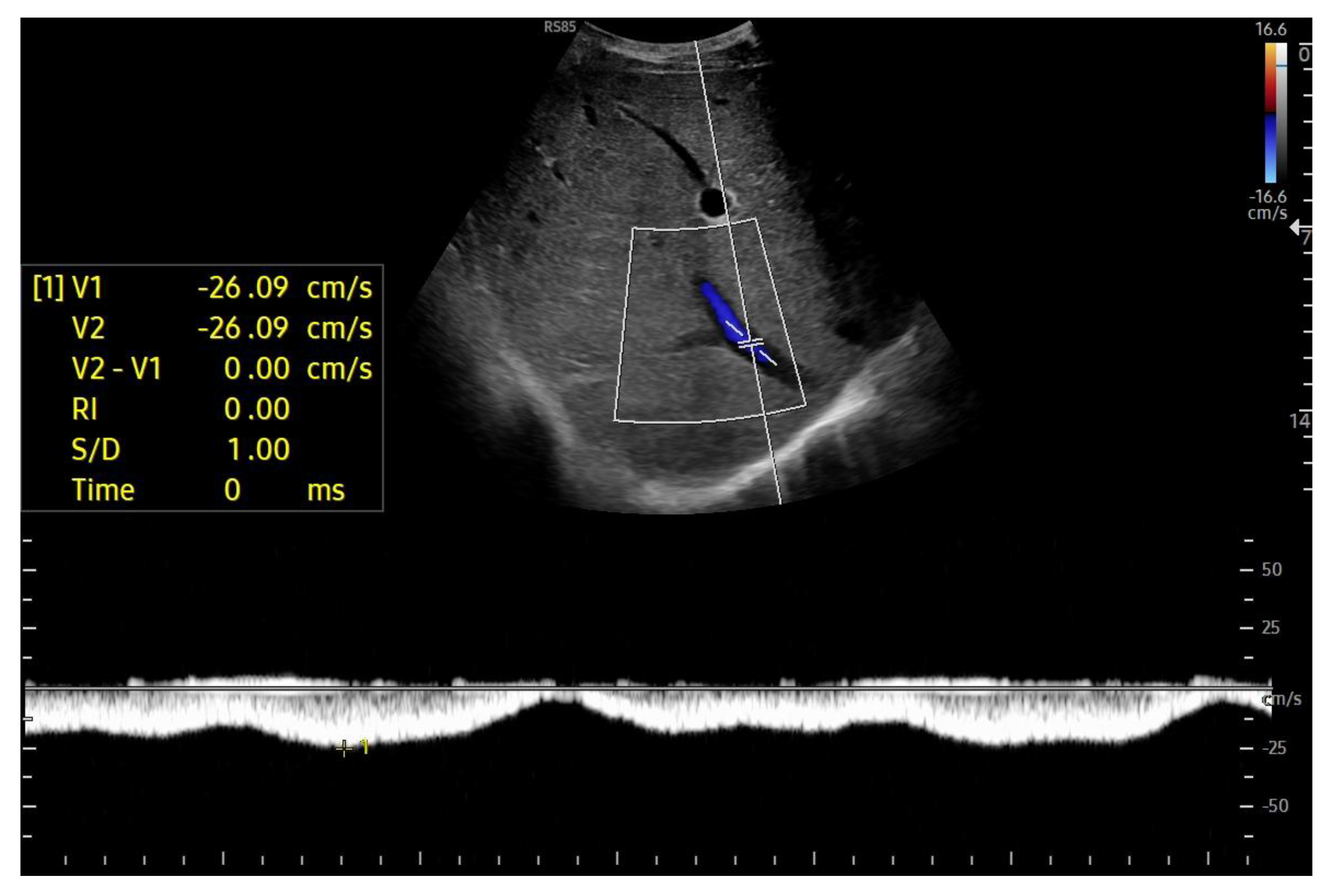
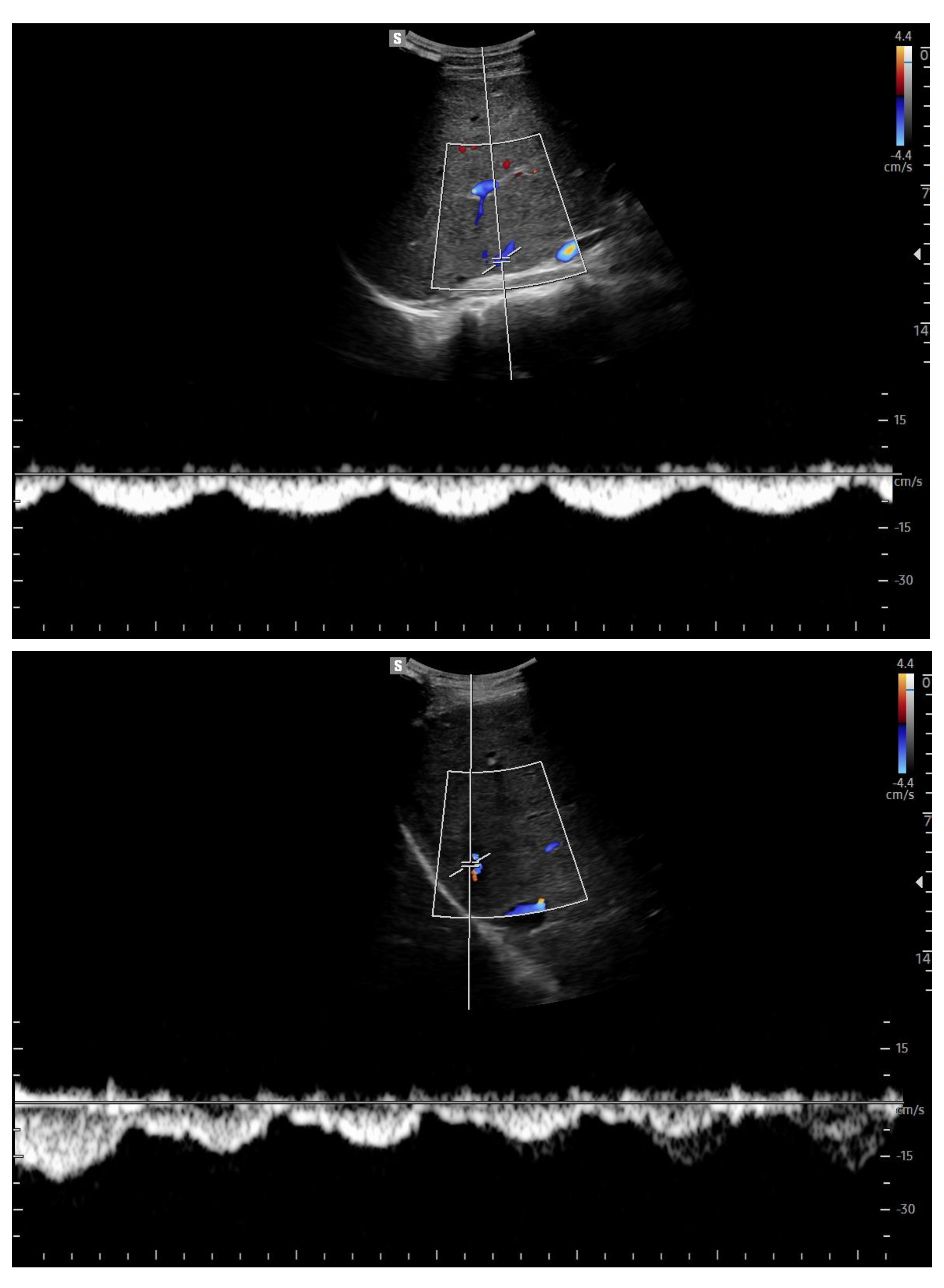
Figure 11.
Preserved hepatopetal portal flow in atrio-pulmonary connection.
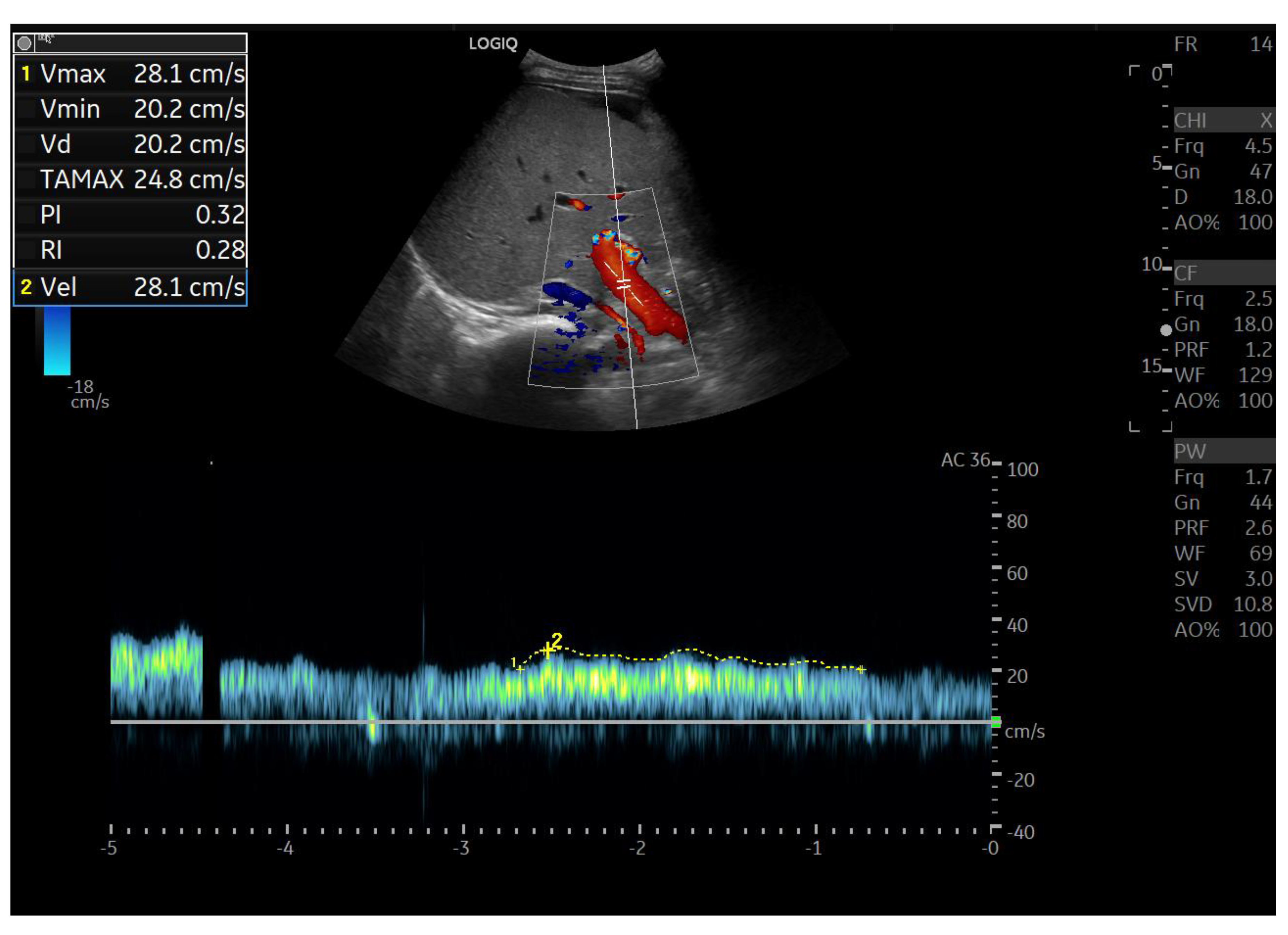
Figure 12.
Inverted portal flow in cavopulmonary anastomosis.
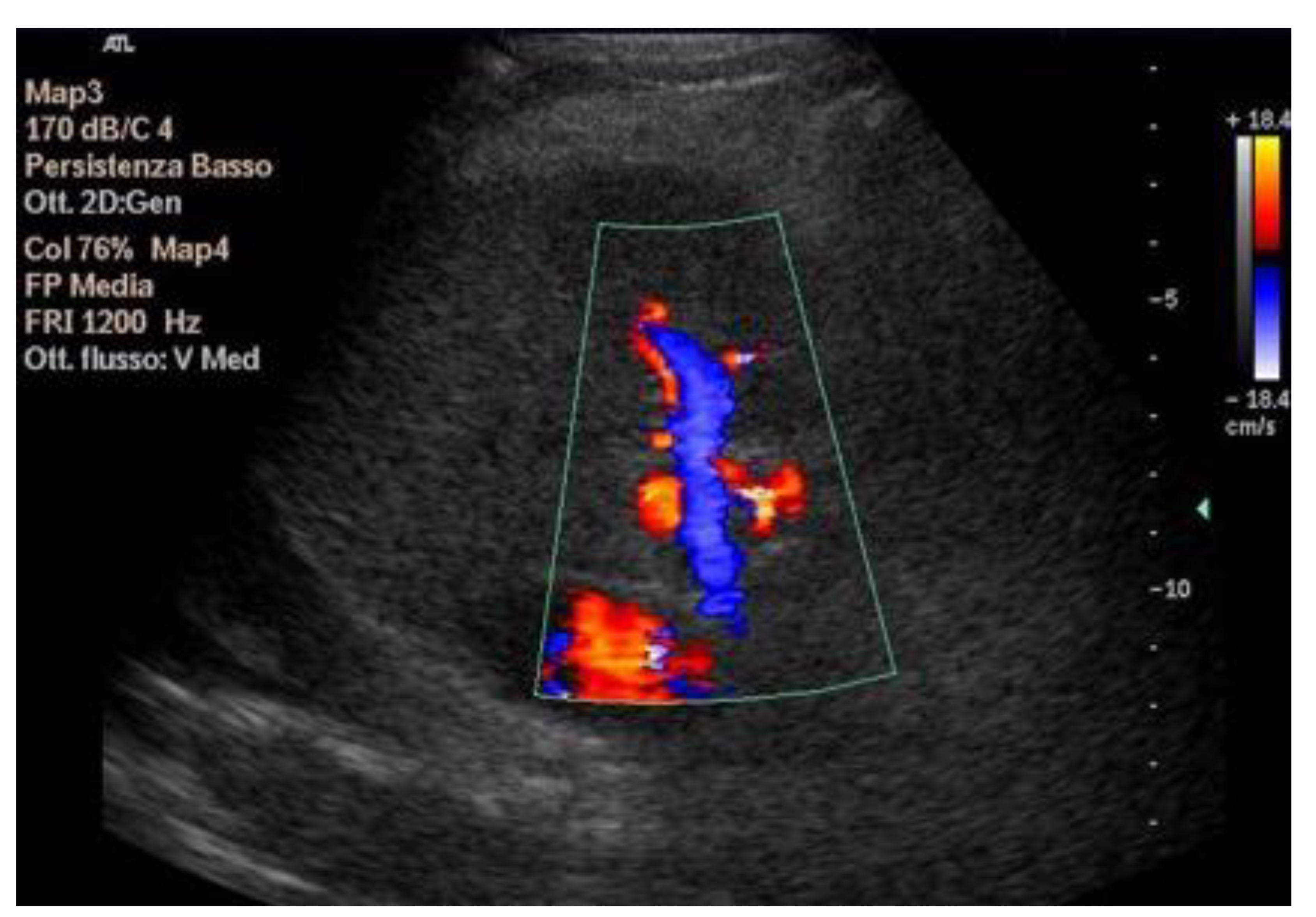
Figure 13.
Changes in hepatic vascularization in a patient with FALD. The middle hepatic vein is patent, although irregular, within the context of the parenchymal nodularity.
Figure 13.
Changes in hepatic vascularization in a patient with FALD. The middle hepatic vein is patent, although irregular, within the context of the parenchymal nodularity.
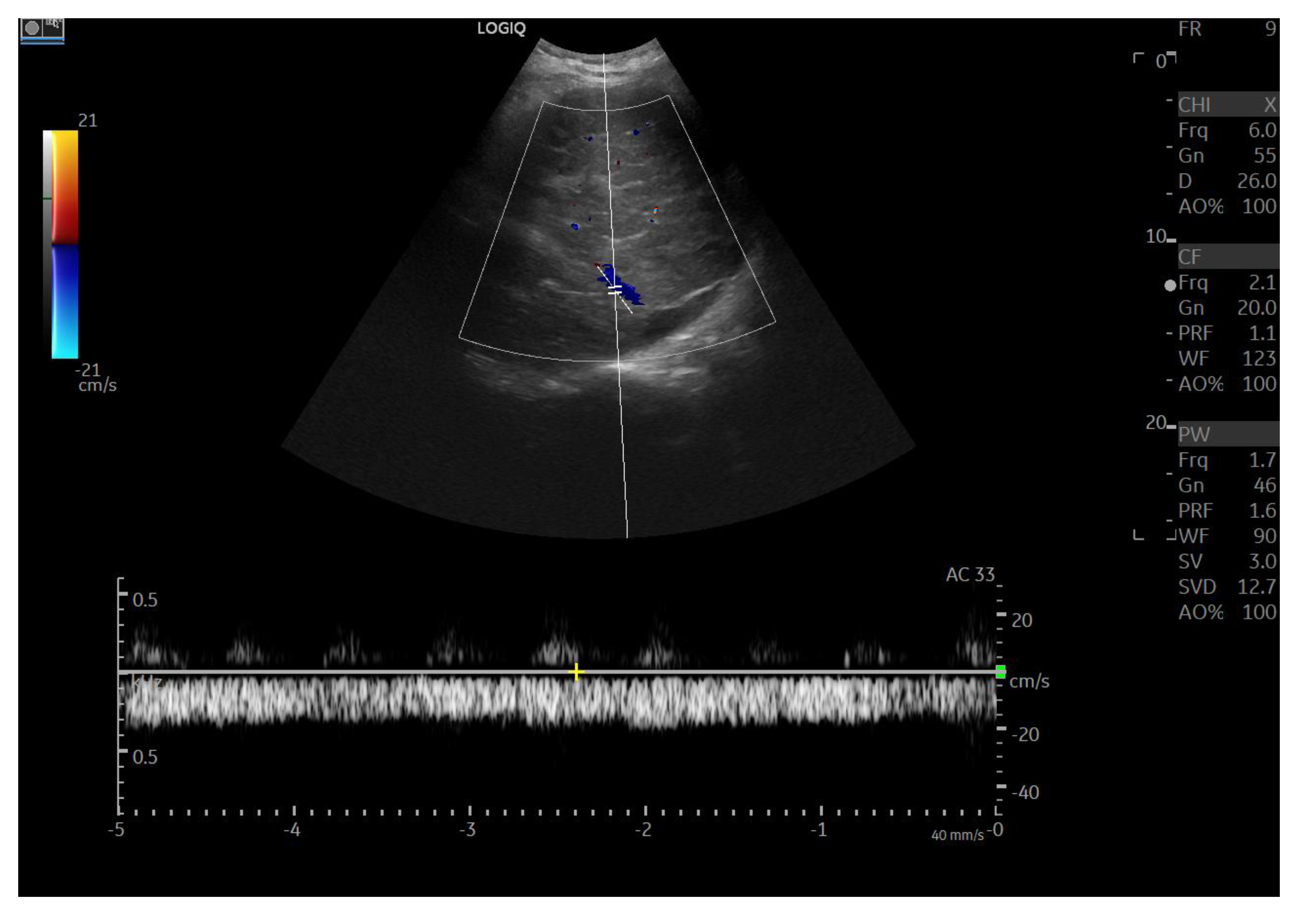
Figure 14.
Diffusely dense and heterogeneous echostructure due to the presence of multiple and diffuse hyperechoic areas consistent with FNH-like nodules.
Figure 14.
Diffusely dense and heterogeneous echostructure due to the presence of multiple and diffuse hyperechoic areas consistent with FNH-like nodules.
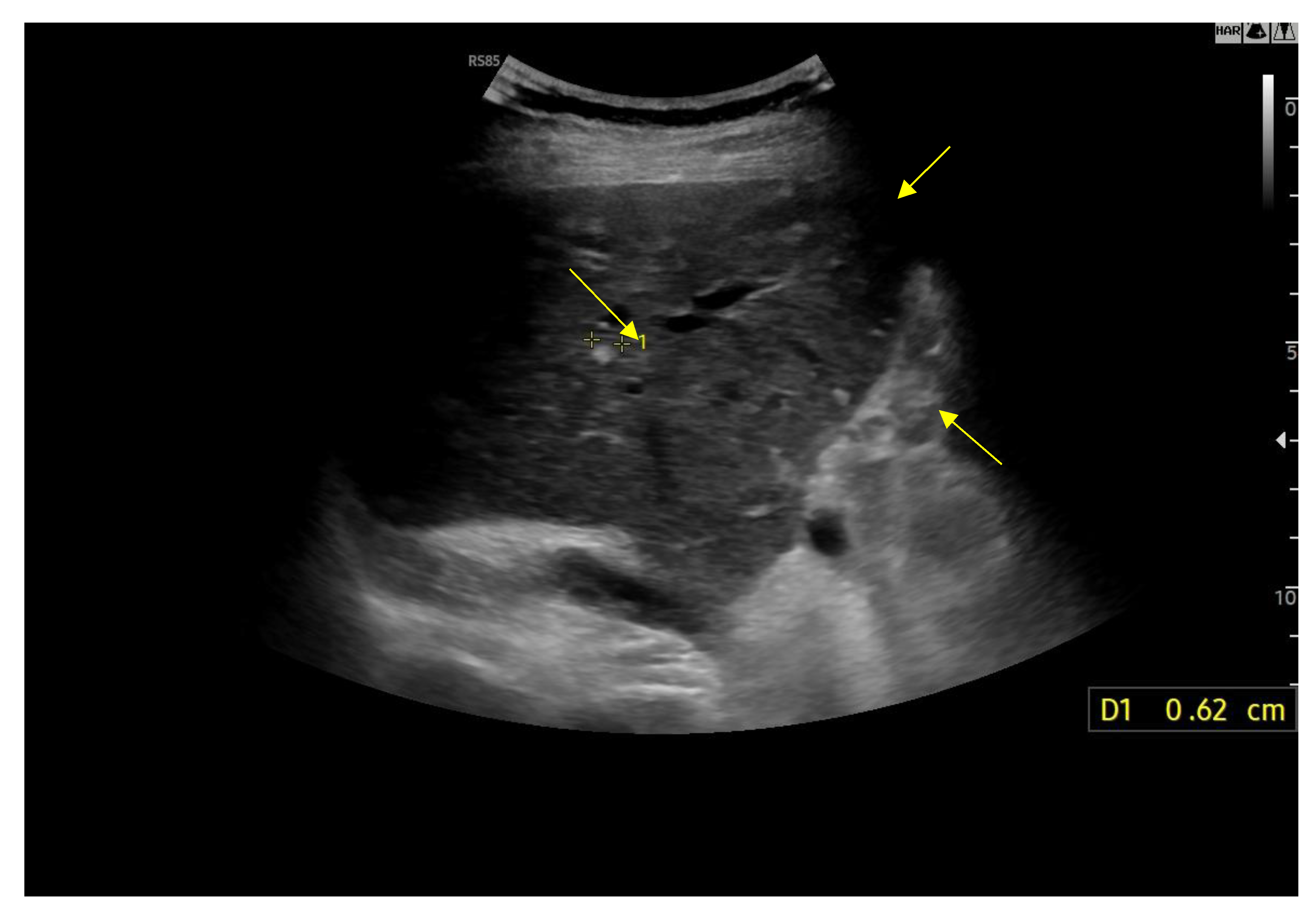
Figure 15.
Hyperechoic oval lesion of 2.7 mm, compatible with a FNH-like nodule, identified using a high-frequency linear probe.
Figure 15.
Hyperechoic oval lesion of 2.7 mm, compatible with a FNH-like nodule, identified using a high-frequency linear probe.
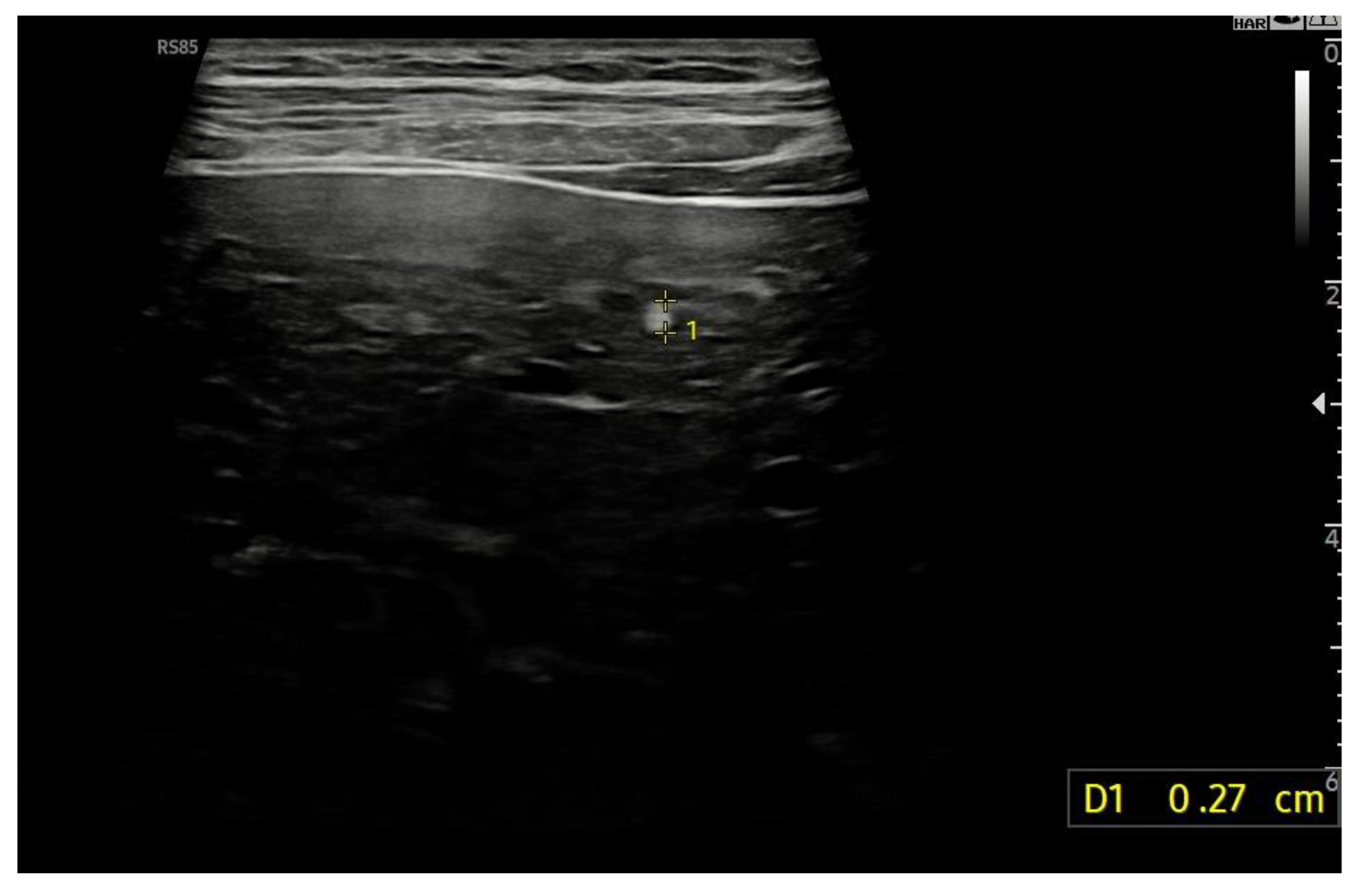
Figure 16.
Contrast-enhanced ultrasound (CEUS) in the arterial phase; note the heterogeneous wash-in of multiple hepatic areas.
Figure 16.
Contrast-enhanced ultrasound (CEUS) in the arterial phase; note the heterogeneous wash-in of multiple hepatic areas.
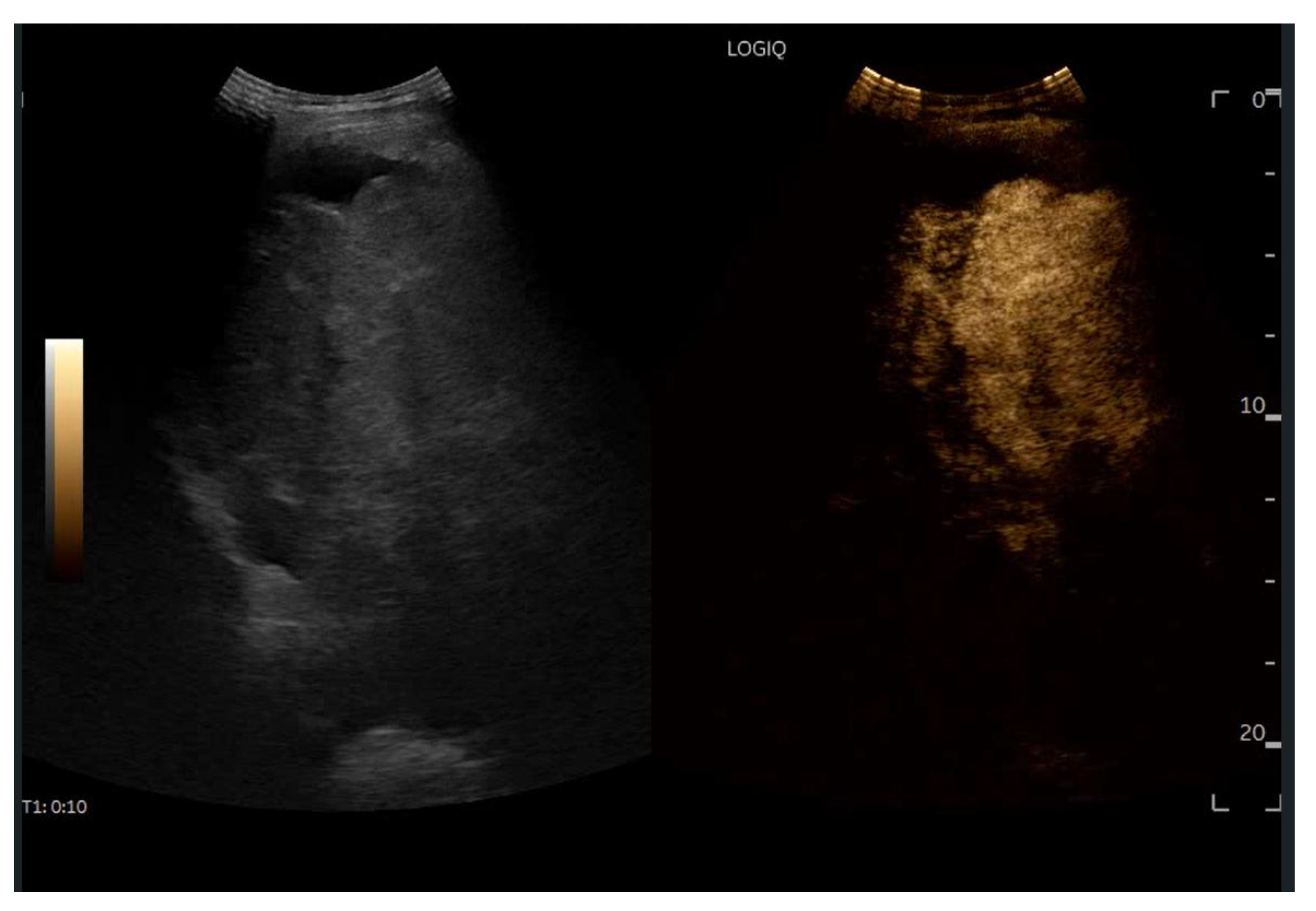
Figure 17.
Contrast-enhanced ultrasound (CEUS) in the portal phase; The enhancement of the different hepatic regions becomes homogeneous.
Figure 17.
Contrast-enhanced ultrasound (CEUS) in the portal phase; The enhancement of the different hepatic regions becomes homogeneous.
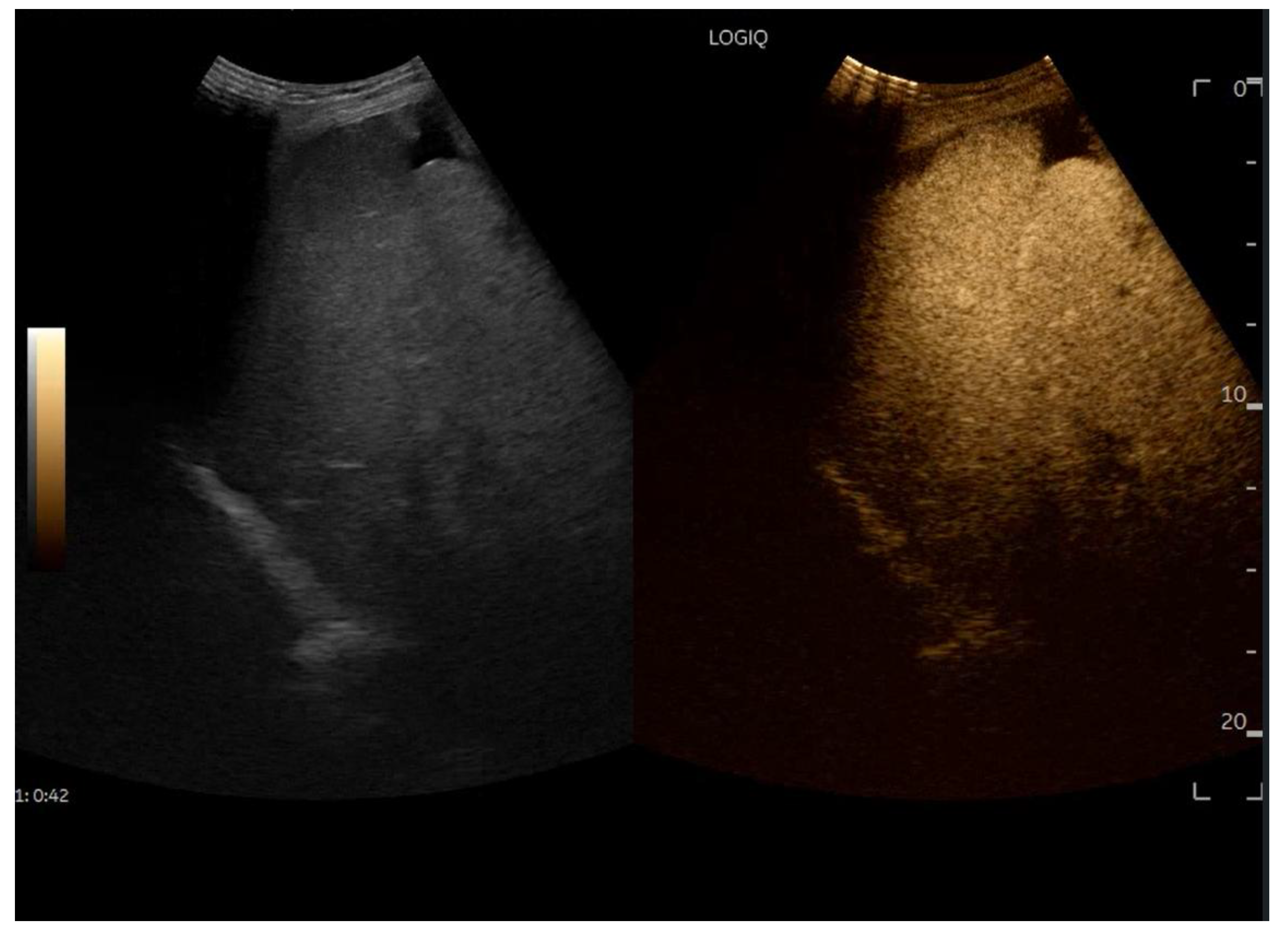
Figure 18.
Contrast-enhanced ultrasound (CEUS) in the late phase shows the appearance of hypovascular areas due to varying degrees of congestion and hepatic alteration. These areas may mimic malignant nodular lesions with early washout.
Figure 18.
Contrast-enhanced ultrasound (CEUS) in the late phase shows the appearance of hypovascular areas due to varying degrees of congestion and hepatic alteration. These areas may mimic malignant nodular lesions with early washout.
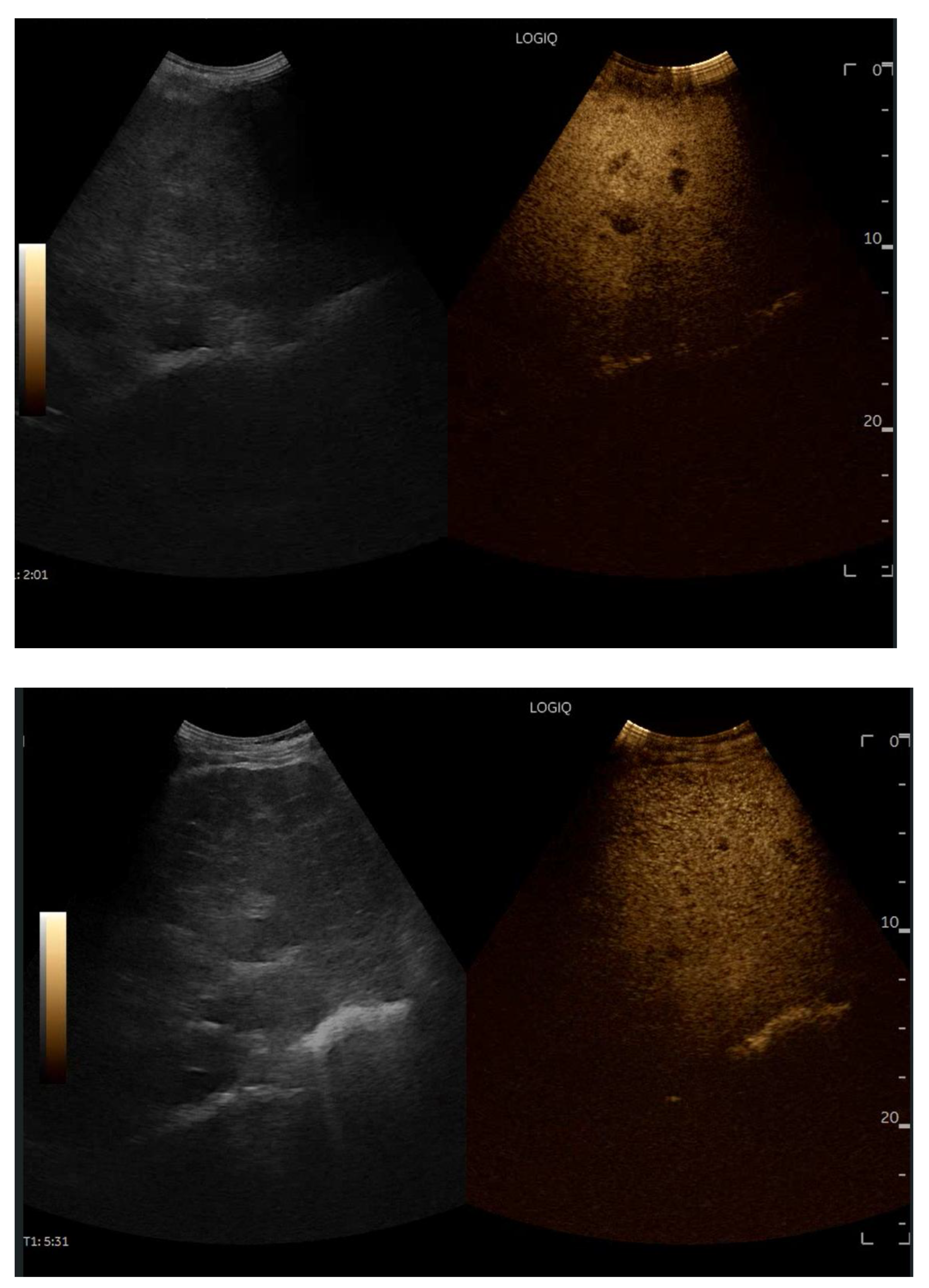
Figure 19.
CEUS exam showing late heterogeneous enhancement in the arterial phase with evidence of hypo-enhanced areas, thus mimicking a malignant wash-out.
Figure 19.
CEUS exam showing late heterogeneous enhancement in the arterial phase with evidence of hypo-enhanced areas, thus mimicking a malignant wash-out.
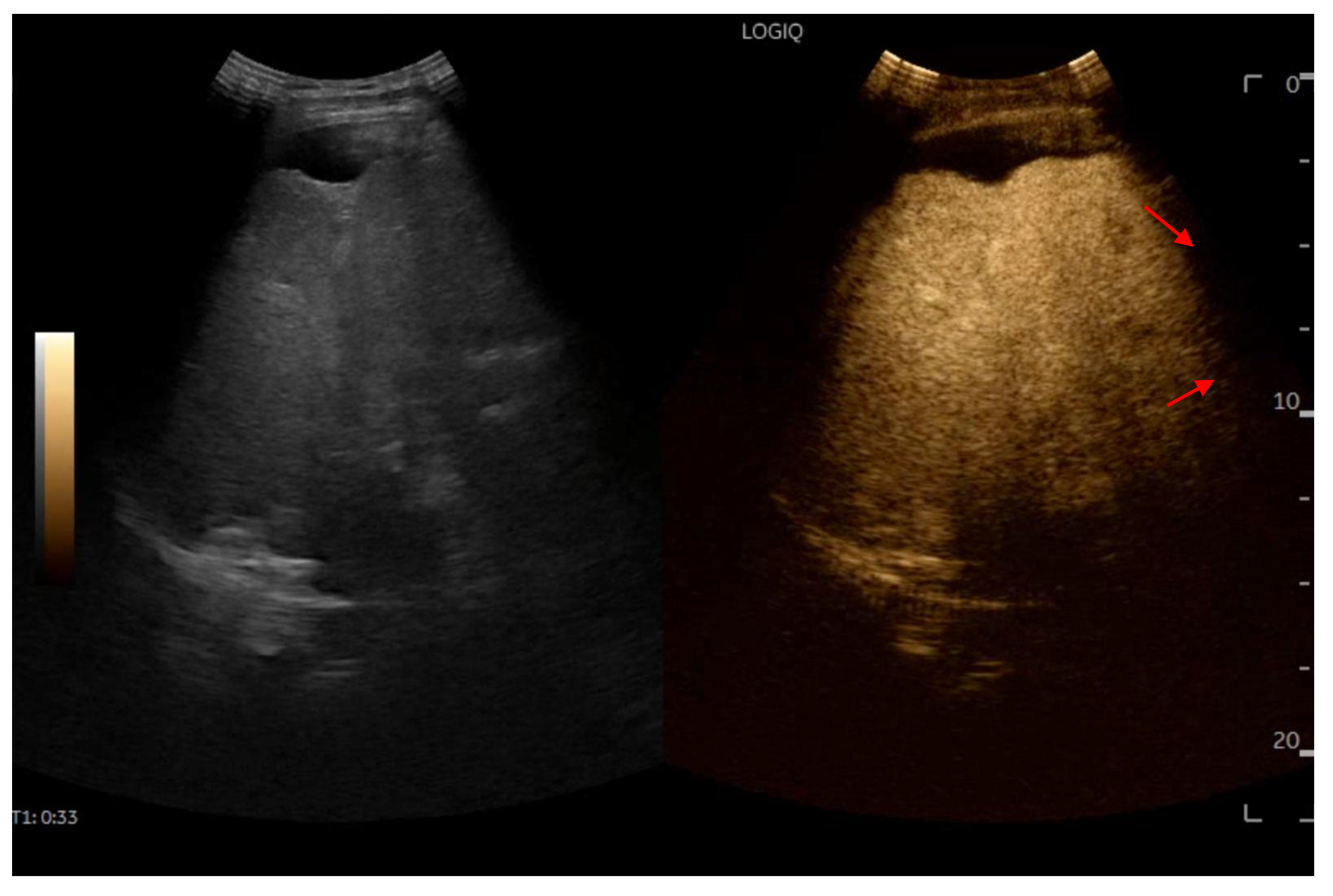
Figure 20.
Hepatic elastography, performed using the 2D-SWE method, showed a mean stiffness of 11.4 kPa, with an IQR/M of 9%, consistent with F4 fibrosis.
Figure 20.
Hepatic elastography, performed using the 2D-SWE method, showed a mean stiffness of 11.4 kPa, with an IQR/M of 9%, consistent with F4 fibrosis.
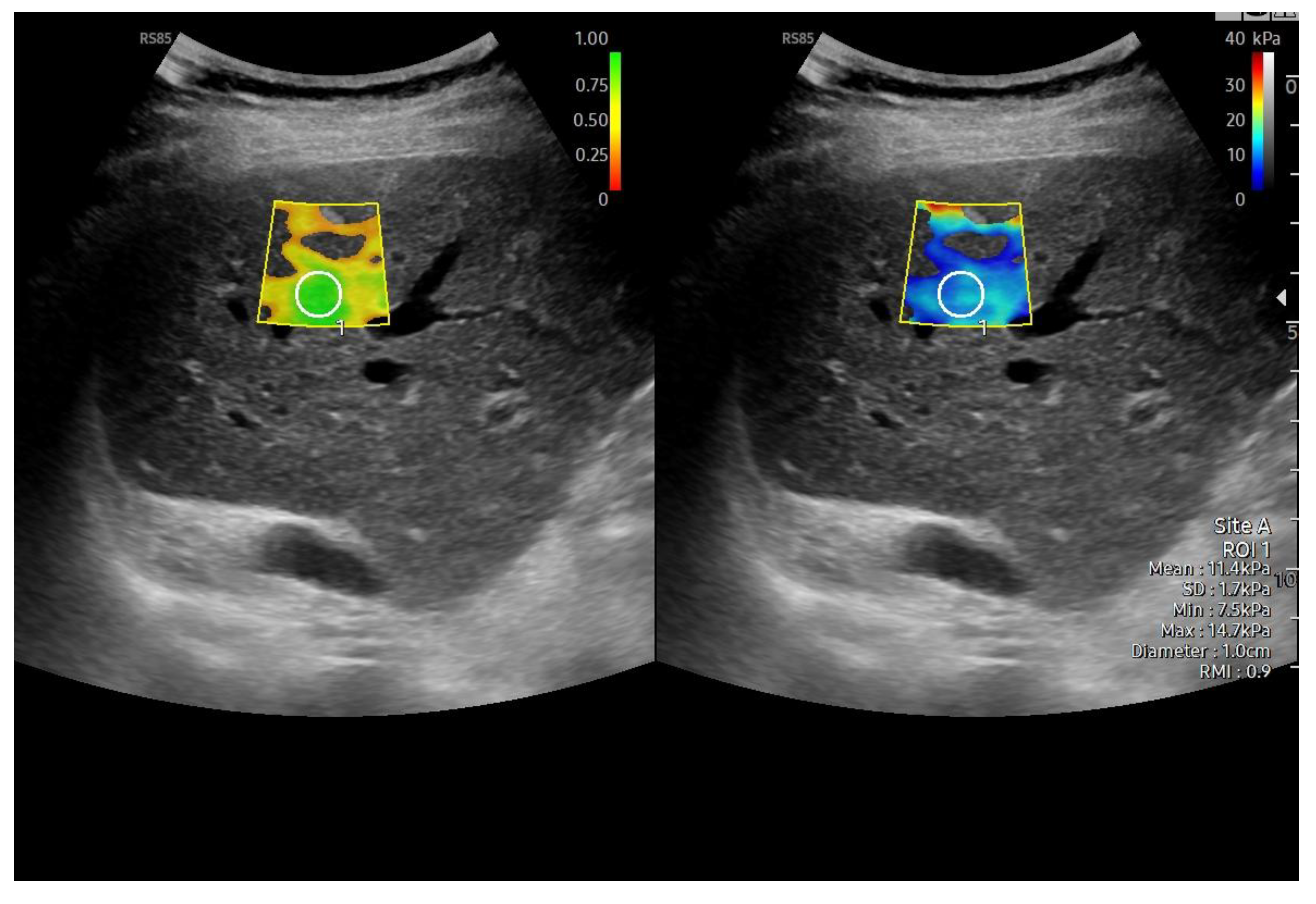

Table 1.
clinical and hemodynamic phenotypes of Fontan Circulation Failure.
| Phenotype | Ventricular Function | Fontan Pressure | Cardiac Index | Key clinical features | Prognosis |
|---|---|---|---|---|---|
| SFP (Systolic) | Reduced | Variable | Low | Heart failure symptoms | Poor, high transplant risk |
| PFP (Preserved) | Normal | Elevated | Normal or mildly low | Systemic congestion | Intermediate |
| LFP (Lymphatic) | Variable | Normal or low | Variable | Protein-losing enteropathy, plastic bronchitis | High morbidity |
| NHP (Normal) | Normal | Normal | Normal | Nonspecific symptoms | Variable, challenging diagnosis |
Table 2.
Similarities between FALD, cardiac cirrhosis and non-cardiac cirrhosis.
| Feature | FALD vs Cardiac Cirrhosis | FALD vs Other Cirrhosis (e.g. viral, metabolic) |
|---|---|---|
| Pathophysiology | Passive hepatic congestion due to chronically elevated central venous pressure | Chronic injury leads to progressive fibrosis and cirrhosis |
| Histological findings | Sinusoidal dilation and perivenular fibrosis | Development of bridging fibrosis and nodular architecture in all |
| Imaging features | Hepatomegaly, heterogeneous liver texture, signs of venous congestion | Nodular surface, altered vascular flow patterns, and signs of portal hypertension |
| Clinical progression | Often indolent onset with progression over years | Progressive decompensation common to all advanced cirrhosis |
| Complications | Risk of HCC present in all advanced stages | HCC risk shared across etiologies |
| Portal hypertension | May develop in late stages due to sinusoidal and post-sinusoidal resistance | Common in all cirrhotic patterns, but from different hemodynamic origins. |
Table 3.
Key differences between FALD, cardiac cirrhosis and non-cardiac cirrhosis.
| Feature | FALD vs Cardiac Cirrhosis | FALD vs Other Cirrhosis (e.g. viral, metabolic) |
|---|---|---|
| Etiology | Congenital heart disease with Fontan circulation | Non-cardiac: viral hepatitis, alcohol, MASLD, autoimmune causes |
| Hemodynamics | Consistently elevated CVP due to absent sub-pulmonary ventricle | Typically unrelated to central venous pressure |
| Age of onset | Pediatric or adolescent onset due to congenital heart repair | Usually manifests in adulthood |
| Liver biochemistry | Mild, non-specific transaminase elevation; often preserved synthetic function | May show higher AST/ALT, and impaired bilirubin, albumin, INR in advanced stages |
| Histopathology | Patchy fibrosis with central congestion and sinusoidal dilation; portal tracts relatively spared | Portal-based fibrosis, lobular inflammation, steatosis or bile duct injury |
| Fibrosis pattern | Predominantly centrilobular with variable progression | Diffuse or periportal depending on underlying disease |
| Progressive dynamics | Slow, heterogeneous; shaped by Fontan physiology and systemic venous congestion | Related to ongoing inflammatory, toxic or metabolic insult |
Table 4.
The most common proposed mechanisms influencing the development of FALD.
Table 5.
Laboratory scoring systems. ALT, alanine transaminase; AST, aspartate aminotransferase; APRI, aspartate aminotransferase to platelet ratio index; FIB-4, fibrosis-4; MELD, model for end-stage liver disease; MELD XI, model for end-stage liver disease excluding the international normalized ratio; FALD, Fontan-associated liver disease; INR, International Normalized Ratio; GGT, gamma-glutamyl transferase.
Table 5.
Laboratory scoring systems. ALT, alanine transaminase; AST, aspartate aminotransferase; APRI, aspartate aminotransferase to platelet ratio index; FIB-4, fibrosis-4; MELD, model for end-stage liver disease; MELD XI, model for end-stage liver disease excluding the international normalized ratio; FALD, Fontan-associated liver disease; INR, International Normalized Ratio; GGT, gamma-glutamyl transferase.
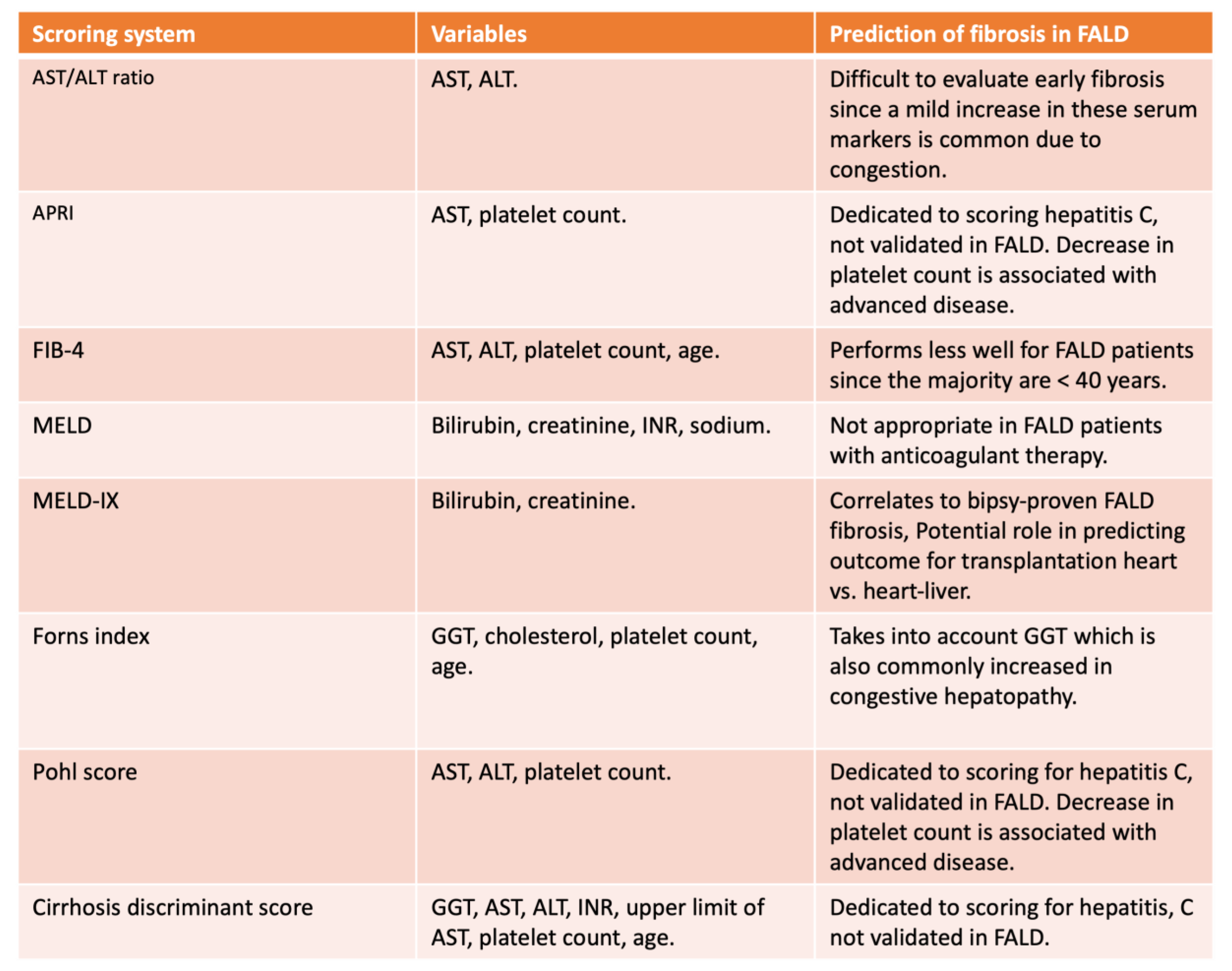
Table 6.
This table summarizes the distinguishing imaging characteristics of FNH-like nodules observed in Fontan-associated liver disease (FALD) compared with typical findings in hepatocellular carcinoma (HCC). Modalities include standard ultrasound (B-mode), contrast-enhanced ultrasound (CEUS), computed tomography (CT), and magnetic resonance imaging (MRI).
Table 6.
This table summarizes the distinguishing imaging characteristics of FNH-like nodules observed in Fontan-associated liver disease (FALD) compared with typical findings in hepatocellular carcinoma (HCC). Modalities include standard ultrasound (B-mode), contrast-enhanced ultrasound (CEUS), computed tomography (CT), and magnetic resonance imaging (MRI).
| Imaging | Imaging Modality | FNH-like Nodules Features | Differential Clues from HCC |
|---|---|---|---|
| Ultrasound | B-mode | Small, hyperechoic, sometimes multiple lesions | HCC may be iso- or hypoechoic, larger, with irregular margins |
| CEUS (Contrast-Enhanced Ultrasound) | Hyperenhancement in arterial phase; centrifugal enhancement; central stellate vasculature; no washout | HCC often shows rapid washout in portal/late phase and lacks central stellate pattern | |
| CT | Arterial Phase | Hyperenhancing compared to liver parenchyma | HCC may also be hyperenhancing, but more likely to show irregular margins or washout later |
| Portal/Delayed Phase | Generally iso- or hyperattenuating; occasional mild washout due to parenchymal congestion | HCC often shows true washout, distinguishing it from regenerative nodules | |
| MRI | T1-weighted | Iso- or mildly hypointense; central scar hypointense | HCC is often more heterogeneous and may have intense arterial enhancement |
| T2-weighted | Iso- or mildly hyperintense; central scar hyperintense | HCC may be more heterogeneous, with areas of necrosis or hemorrhage | |
| Hepatobiliary Phase | Hyperintense due to hepatobiliary contrast retention (differentiates from HCC) | HCC typically appears hypointense due to lack of contrast uptake | |
| DWI | No diffusion restriction (helps distinguish from HCC) | HCC typically restricts diffusion (appears hyperintense on DWI) |
Table 7.
This table provides a detailed comparative overview of key studies evaluating liver stiffness in Fontan-associated liver disease (FALD). List of Abbreviations: FALD (Fontan-Associated Liver Disease), LSM (Liver Stiffness Measurement), TE (Transient Elastography), SWE (Shear Wave Elastography), 2D SWE (Two-Dimensional Shear Wave Elastography), SWD (Shear Wave Dispersion), MRE (Magnetic Resonance Elastography), MRI (Magnetic Resonance Imaging), CT (Computed Tomography), US (Ultrasound), LFI (Liver Fibrosis Index), APRI (AST to Platelet Ratio Index), FIB-4 (Fibrosis-4 Index), LSPS (Liver Stiffness-Spleen Diameter to Platelet Ratio Score), MELD (Model for End-Stage Liver Disease), AFP (Alpha-Fetoprotein), AUROC (Area Under the Receiver Operating Characteristic Curve), HCC (Hepatocellular Carcinoma).
Table 7.
This table provides a detailed comparative overview of key studies evaluating liver stiffness in Fontan-associated liver disease (FALD). List of Abbreviations: FALD (Fontan-Associated Liver Disease), LSM (Liver Stiffness Measurement), TE (Transient Elastography), SWE (Shear Wave Elastography), 2D SWE (Two-Dimensional Shear Wave Elastography), SWD (Shear Wave Dispersion), MRE (Magnetic Resonance Elastography), MRI (Magnetic Resonance Imaging), CT (Computed Tomography), US (Ultrasound), LFI (Liver Fibrosis Index), APRI (AST to Platelet Ratio Index), FIB-4 (Fibrosis-4 Index), LSPS (Liver Stiffness-Spleen Diameter to Platelet Ratio Score), MELD (Model for End-Stage Liver Disease), AFP (Alpha-Fetoprotein), AUROC (Area Under the Receiver Operating Characteristic Curve), HCC (Hepatocellular Carcinoma).
| Study | Sample Size | Modality | Comparator | Main Findings |
| Sakae et al. (2025) [100] | 37 | TE (FibroScan®) | Serum markers (FIB-4, GGT), clinical parameters | FIB-4, GGT, and age at Fontan were independently associated with elevated LSM; TE correlated with liver fibrosis risk. |
| Imoto et al. (2025) [99] | 46 | SWE, Platelet count, LFI | Liver biopsy results | Platelet <185k + LFI >2.21 predicted aFALD with high sensitivity; proposed a 2-step algorithm for screening. |
| Lo Yau et al. (2025) [102] | 29 | US elastography, Liver biopsy | METAVIR vs congestive hepatic fibrosis score | Weak correlation between US elastography and histologic fibrosis. 86% had METAVIR > F2; median shear wave 1.97 m/s. |
| Yau et al. (2025) [103] | 56 | SWE, Hemodynamic assessment | Cardiac catheterization, Echocardiography parameters | No significant correlation between SWE and pre-/post-Fontan hemodynamics. No association with systolic function or AV valve regurgitation on echo. Liver stiffness measurements appear independent of cardiac output parameters. |
| Cuadros et al. (2025) [98] | 91 | TE (FibroScan®) | Clinical outcomes, fibrosis markers | Elevated LSM predicted major events and mortality in Fontan patients; validated prognostic value of TE. |
| Téllez et al. (2025) [97] | 217 | TE, Biopsy, FonLiver score | Other non-invasive tests (APRI, FIB-4, MELD) | FonLiver score outperformed traditional markers; strong diagnostic tool combining TE and platelet count. |
| Bolia et al. (2024) [96] | 48 | SWE | Liver stiffness, biomarkers | SWE showed weak correlation with established FALD markers; limited predictive utility. |
| Jarasvaraparn et al. (2024) [95] | 66 | APRI, FIB-4, TE | Histologic and imaging findings | APRI and FIB-4 were moderately predictive in adults but not effective in children. |
| Gill et al. (2023) [94] | 25 | 2D SWE, TE | Liver stiffness measurements | Poor concordance between SWE and TE; questioned reliability of elastography. |
| Nagasawa et al. (2022) [93] | 27 | SWD, 2D SWE | Fibrosis stage (biopsy) | SWD more accurate than SWE for detecting significant fibrosis. |
| Chemello et al. (2021) [92] | 52 | TE | Portal hypertension and clinical stage | LS and LSPS effectively staged FALD and identified portal hypertension risk. |
| Schleiger et al. (2020) [91] | 145 | TE, FibroTest®, US | Fontan duration, clinical severity | Fibrosis scores strongly associated with Fontan duration and clinical severity. |
| Munsterman et al. (2019) [90] | 49 | US, TE, MRI/CT, Biopsy | Histology and imaging findings | Universal fibrosis found; varices and nodules inconsistently reflected severity. |
| Egbe et al. (2018) [89] | 22 | MRE | MELD score, outcomes | Annual MRE-LS progression correlated with worsening MELD and clinical outcomes. |
Table 8.
This comparative table outlines the practical follow-up and surveillance strategies recommended by the American Heart Association (AHA, 2019) and the European Association for the Study of the Liver/European Reference Network (EASL-ERN, 2023) for patients with Fontan circulation. It includes guidance on multidisciplinary care, imaging modalities, timing of surveillance, and use of biomarkers to monitor Fontan-associated liver disease (FALD) and hepatocellular carcinoma (HCC).
Table 8.
This comparative table outlines the practical follow-up and surveillance strategies recommended by the American Heart Association (AHA, 2019) and the European Association for the Study of the Liver/European Reference Network (EASL-ERN, 2023) for patients with Fontan circulation. It includes guidance on multidisciplinary care, imaging modalities, timing of surveillance, and use of biomarkers to monitor Fontan-associated liver disease (FALD) and hepatocellular carcinoma (HCC).
| Surveillance Component | AHA Recommendations (2019) | EASL-ERN Recommendations (2023) |
|---|---|---|
| Multidisciplinary Care Team | Fontan/single-ventricle clinics with experienced personnel | Specialized clinics with hepatologist, cardiologist, radiologist |
| Cardiac MRI | Every 2–3 years for anatomic and functional assessment | Every 2–3 years to evaluate Fontan flow and anatomy |
| CT Angiography | When clinically indicated | Not specifically emphasized unless MRI is contraindicated |
| Cardiac Catheterization | Every 10 years or when clinically indicated | When MRI contraindicated or invasive data needed |
| Liver Ultrasound + Elastography | Annual ultrasound with elastography | Annual surveillance as first-line imaging tool |
| Liver MRI with Hepatobiliary Contrast | Annual MRI from adolescence; use hepatobiliary contrast if biopsy is considered | Baseline at 10 years; repeat every 1–2 years in high-risk |
| Liver Biopsy | If imaging is inconclusive and LI-RADS fails to differentiate | Mandatory when malignancy cannot be ruled out by imaging alone |
| Serum AFP Monitoring | Use AFP >7 ng/dl as alert threshold; >10 ng/dl = high risk | AFP >10 ng/mL requires advanced imaging or biopsy |
| Timing of HCC Surveillance | Start 10 years after Fontan; consider earlier in high-risk patients | Begin at 10 years post-Fontan; earlier if MELD >19, APRI/FIB-4 elevated |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



