Submitted:
14 October 2025
Posted:
14 October 2025
You are already at the latest version
Abstract
Bipolar spectrum disorders (BSD) are neuropsychiatric conditions that involve manic symptoms and depression symptoms. The prevalence of Bipolar Disorder (BD) is 1% to 3% in youth, which is known to undermine their cognitive, emotional, and social functions. Among the many biological mechanisms underlying BD, pro-inflammatory cytokines are small proteins that are active in the immune system, which can affect neuronal activity by altering blood-brain permeability, neurotransmitter activeness, and causing damage to the neuronal cells. This systematic review examines different types of cytokines and how their level varies in adolescent BD. Specifically, the review examined pro-inflammatory cytokines IL-6, IL-8, TNF-α, and IL-1β and an anti-inflammatory cytokine IL-10. A total of 9 studies were included from screening two databases, PsycInfo and PubMed. Overall, the levels of IL-6, IL-8, TNF-α, and IL-1β positively correlated with BD symptoms. While these findings have implications for treatment, counseling, medication, and prevention strategies specific to adolescent patients, future research must address the inconsistency around IL-10 levels as well as other biomarkers such as Brain-Derived Neurotrophic Factors (BDNF).
Keywords:
adolescent
; bipolar disoder
; bipolar spectrum disorder
; cytokine
; pro-inflammatory marker
; neuro-inflammatory marker
I. Introduction
Bipolar spectrum disorders (BSD) are neuropsychiatric conditions which are characterized by shifting mood, alternating highs (manic or hypomanic) and lows (depression) [1]. Diagnostic and Statistical Manual of Mental Disorders (DSM-5) is widely used to diagnose psychiatric symptoms, in which BSD are classified into three types: bipolar disorder (BD) I, II, and cyclothymia [1]. BD I is characterized by at least one manic episode, preceded or followed by hypomanic or major depressive episodes [2]. BD II is marked by at least one hypomanic and major depressive episode, yet lacking full manic episodes [2]. Lastly, cyclothymia is defined by a period of elevated mood symptoms and depressive symptoms for at least two years, yet is not included in major depressive, manic, or hypomanic criteria [2].
The prevalence of mood disorders worldwide is approximately 22%, with around 1% of BD and 7% of Major Depressive Disorder (MDD) [3]. BD occurs in 1% to 3% of youth, and 50 % of adolescents diagnosed with MDD convert to BSD [4,5]. Similar to other neuropsychiatric disorders like schizophrenia, researchers have indicated that 45% of first episodes of BD occur in an average age of 17 years [6]. Adolescence is a critical period, marked by the development of the nervous system, which is responsible for cognitive, emotional, and social functions [7]. One research highlighted that adolescents with the first episode of BD showed impaired cognitive function, as demonstrated by their memory, attention, and executive function [8].
Gene-environment interplays establish the epigenetic cause of BD, highlighting the complexity of its cause. Many mental disorders, including Schizophrenia (SCZ), BD, MDD, autism spectrum disorder (ASD), and attention deficit hyperactivity disorder (ADHD), have high heritability [9]. Specifically, heritability for BD ranges is estimated to be 44%, according to a family-based study [10].
In addition, family history for BD increases the risk of developing BD [11]. Other environmental factors for psychiatric disorders exist. Childhood traumatic experiences, such as physical, sexual, or emotional abuse can contribute to psychiatric disorders [12]. These environmental factors can contribute to the development of stress, which is a risk factor for depression [13].
In diagnosing BD, symptom-focused strategy is widely used, yet it is limited to recognizing patients whose early onset is depression episodes. According to one study, assessing BD in youth primarily relies on interview and observation, lacking objective criteria [4]. This can lead to exacerbation of BD in adolescents, as misdiagnosis of BD in early onset results in insufficient medication and more severe episodes [14]. Therefore, identifying biomarkers that contribute to BD is needed to accurately assess BD in adolescent patients.
Among the many biomarkers, pro-inflammatory markers (PIM) are neurological markers that are involved in physiological processes of BD, such as glucocorticoid resistance, blood-brain barrier dysfunction, changes in neurotransmitter activity, and damage in neuronal cells [15]. Cytokines are small proteins that are responsible for immune responses, as they affect neuronal activity, including excitability and plasticity [16,17]. Specifically, cytokines activate the HPA axis, which in turn releases corticotropin-releasing hormone (CRH), adrenocorticotropic hormone (ACTH), and cortisols, while reducing the function of glucocorticoid receptors [18].
Cytokines that are directly correlated with neurological functions include tumor necrosis factor alpha (TNF-α), interleukin-6 (IL-6), interleukin-1β (IL-1β), interleukin-10 (IL-10), and interleukin-8 (IL-8).
Tumor necrosis factor alpha (TNF-α) is a type of cytokine secreted by macrophages, glial cells, and neurons [19]. As a pro-inflammatory cytokine, TNF-α affects the function of neurons, the amount of neurotransmitters, and the synthesis of myelin in the central nervous system by increasing blood-brain barrier permeability [19]. One longitudinal study reported that TNF-α is negatively associated with cortical thickness of the prefrontal lobe of individuals who are at risk of developing a psychotic disorder [20]. The cytokine’s neurological role implies its correlation with Bipolar Disorder.
Another cytokine, Interleukin-6 (IL-6) has both beneficial and destructive potentials, contributing to the development, differentiation, regeneration, and degeneration of neurons [21]. IL-6 level was significantly correlated with mental disorders, as exemplified by a study that examined IL-6 gene expression in blood leukocytes, which was negatively correlated with hippocampal volume in schizophrenia patients [22].
Interleukin 1β (IL-1β) is a pro-inflammatory cytokine in the CNS, released by peripheral and brain macrophages [23]. One study demonstrated that administering lipopolysaccharide caused the expression of IL-1β, which in turn contributed to depression and anxiety in healthy participants [24]. Another finding highlighted that increased IL-1β mRNA levels in schizophrenia patients induced a decrease in Broca’s area volume and verbal capability [25].
Interleukin 10 (IL-10) is an anti-inflammatory cytokine that maintains normal tissue homeostasis, thereby preventing autoimmune diseases [26]. According to one study, increased IL-10 levels effectively prevented neuronal degeneration, which is caused by neuroinflammation in diseases like Alzheimer’s Disease and Parkinson’s Disease [27].
Lastly, Interleukin 8 (IL-8) is a pro-inflammatory cytokine that is released by microglia, whose increased levels are found to be correlated with psychiatric diseases like BD, ASD, SCZ, and ASD [28].
For the adult group, an extensive amount of studies identified biomarkers that are associated with BD. One meta-analysis demonstrated that a pro-inflammatory marker, C-Reactive protein (CRP) was increased in adult BD patients compared to healthy controls (HC), especially highest during manic and depressive periods [29]. Another systematic review indicated that pro-inflammatory cytokines were elevated in the adult BD group compared to HC [30]. Yet, there are not enough studies that focus on cytokine levels within adolescent BD patients. Since cytokine levels in adults and adolescents differ significantly, findings from studies on adults cannot be fully generalized to youth patients [31].
This systematic review investigated the role of different inflammatory cytokines in bipolar disorder in adolescent patients.
II. Methods
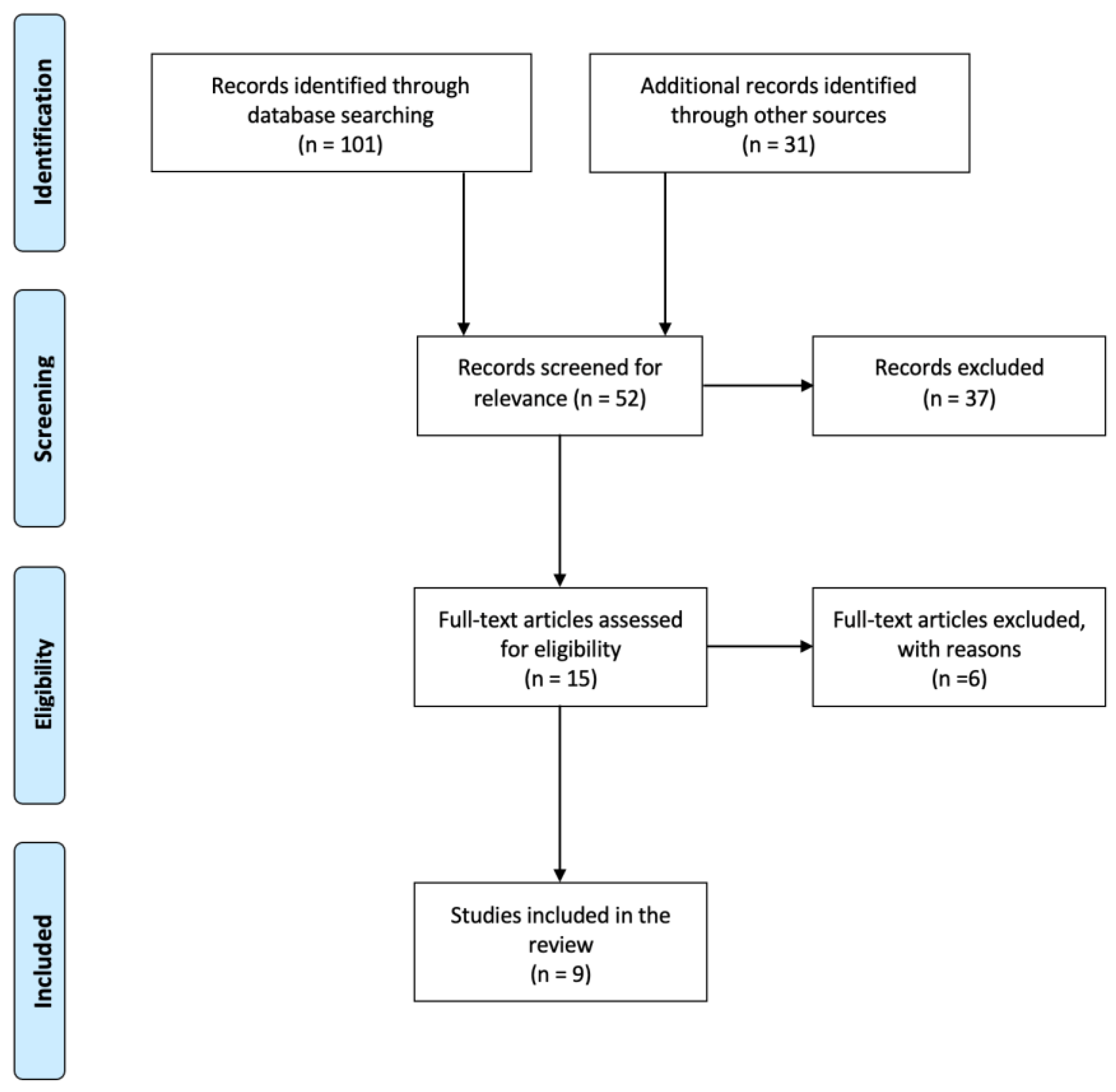
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. It conducted online searches of PubMed and PsycInfo, using keywords including “adolescent,” “bipolar disorder,” and “cytokines,” for studies from 1990 until May 2025.
Initially, 132 papers were reviewed through skimming, leaving 52 research papers that are relevant to the topic. The inclusion criteria applied were the following: (a) study type: longitudinal, cross-sectional, and prospective repeated-measures study; (b) age: adolescents and young adults (mean age of 12 to 25 years old); (c) diagnosis of subjects: any bipolar disorder (BD-I, BD-II, BSD, and not otherwise specified BD (NOS-BD)); (d) symptoms: any symptoms of BD as defined by DSM-5 Diagnostic and Statistical Manual of Mental Disorders (DSM); (e) studies that examined any neuro-inflammatory cytokines; and (f) language: English only.
The exclusion criteria applied were the following: (a) study type: narrative reviews, systematic reviews, and meta-analysis; (b) age: adults and infants (outside of range 12 to 25); (c) diagnosis of subjects: other mood disorders than BD (e.g., MDD); and (d) studies that focused on other biological markers than cytokines or only focused on neurotrophic factors.
After a full-text review of 15 papers, 9 studies were included in the final analysis. Figure 1 illustrates the screening process used in this research.
III. Results
The following is the table summarizing the findings of each reviewed source. Detailed results in accordance with each type of cytokine are presented after.

Table 1.
Detailed Findings of Reviewed Sources.
| Reference | Year | Study Design | No. of participants | Age of participants (mean and SD) |
No. of controls | Age of controls (mean and SD) |
Cytokines | Research Focus | Confounding Factor controlled |
| Skibinska et al. [32] | 2022 | Longitudinal | 25 | 18.28 (±2.82) | 31 | 21.1 (±2.76) | IL-8, TNF-α | Examined defensive mechanisms and cytokines | Age, gender |
| Goldstein et al. [33] | 2015 | Longitudinal | 123 | 20.4 (±3.8) | N/A | N/A | IL-6, TNF-α | Examined pro-inflammatory markers in lifetime characteristics, clinical characteristics, and metabolic syndrome variables | N/A |
| Goldstein et al. [34] | 2011 | Longitudinal | 30 | 15.5 (±2.3) | N/A | N/A | IL-6 | Examined bipolar subtypes and pro-inflammatory markers | N/A |
| Bai et al. [35] | 2024 | Longitudinal | 21 | 12-17 | 69 | 12-17 | TNF-α | Examined suicidal symptom severity and proinflammatory cytokines | Suicide severity, age, sex, BMI, education years, non-suicidal depressive symptoms |
| Karthikeyan et al. [36] | 2022 | Prospective repeated-measures study | 43 | 17.27 (±1.51) | 36 | 17.09 (±1.68) | IL-6, IL-10, TNF-α | Examined inflammatory markers as predictors of future mood symptoms and time for recovery | Age, sex, SES, BMI |
| Miklowitz et al. [37] | 2016 | Cross-sectional | 18 | 16.0 (±2.1) | 20 | 16.6 (±2.2) | IL-1β, IL-6, IL-8, IL-10, TNF-α | Examined systemic and cellular markers of inflammation in BD patients | N/A |
| Terczynska et al. [38] | 2025 | Longitudinal | 24 | 18.95 (±3.52) | N/A | N/A | TNF-α, IL-8 | Examined cytokines with temperament and character dimensions | N/A |
| Pearlstein et al. [39] | 2020 | Longitudinal | 25 | 15.03 (±1.90) | N/A | N/A | IL-6, IL-12, IL-1β, TNF-α | Examined the changes in cytokine levels between pre- and post-cognitive behavioral therapy (CBT) | N/A |
| Hatch et al. [40] | 2017 | Cross-sectional | 40 | 17.41 (±1.64) | 20 | 16.06 (±1.67) | IL-6, TNF-α | Examined the link between cytokine levels in BD patients and cardiovascular disease (CVD) risk | Age, BMI |
- 1)
- IL-6
IL-6 level increased for a longer duration of Bipolar Disorder (BD), maximum depressive severity, maximum hypo/manic severity, subthreshold mood symptom duration, and suicidal ideation [33]. Exposure to psychotic medication and obesity also led to higher IL-6 [33]. Family history of Attention Deficit Hyperactivity Disorder (ADHD) and substance use disorder (SUD) was negatively correlated with IL-6 level [33]. During euthymia, IL-6 level was lowered [33]. In addition, high levels of high-density lipoprotein (HDL) were associated with lower IL-6 [33]. There was no significant difference in IL-6 levels between BP-1 and BP-NOS patients, although obese subjects had higher IL-6 levels than nonobese subjects [34]. The ratio of IL-6/IL-10 was greater in the BD group compared to the HC [36]. There were no findings for IL-6 level as a predictor for future mood symptoms and time to recovery [36]. Controlling for age and BMI factors, IL-6 levels were increased in the BD group compared to the HC [40]. Adolescents with symptomatic BD resulted in the highest level of IL-6 [40]. There was a decreasing linear association of IL-6 between groups of symptomatic BD, asymptomatic BD, and HC [40].
- 2)
- IL-8
IL-8 level increased in the Bipolar Disorder (BD) group compared to the Major Depressive Disorder (MDD) group [32]. The study highlighted the negative correlations between IL-8 levels and immature defense mechanisms in the BD group [32].
IL-8 level did not show a significant correlation with temperament characteristics of individuals in the BD group [38].
- 3)
- TNF-α
Compared to the healthy control (HC) group, the BD group showed higher TNF-α levels [32]. The BD group also showed a higher level of TNF-α compared to the MDD group [32]. The study highlighted the negative correlations between TNF-α levels and immature defense mechanisms in the BD group [32]. Other variables, including low socioeconomic status, lifetime suicide attempts, lifetime self-injurious behavior, family history of SUD, psychosis duration, and high triglyceride, were correlated with higher levels of TNF-α [33]. Patients in the BD group had higher TNF-α levels compared to MDD and HC [35]. There were no findings for TNF-α level as a predictor for future mood symptoms and time to recovery [36]. TNF-α level did not show a significant correlation with temperament characteristics of individuals in the BD group [38]. Controlling for age and BMI factors, TNF-α levels were increased in the BD group compared to the HC [40]. There was a decreasing linear association of TNF-α between groups of symptomatic BD, asymptomatic BD, and HC [40].
- 4)
- IL-10
IL-10 was lower in patients’ symptomatic periods [36]. There were no findings for IL-10 as a predictor of time to recovery [36]. IL-10 was positively associated with increased severity of mood symptoms in the future phase [36].
- 5)
- IL-1β
Plasma levels reported that IL-1β was higher in the BD youth group than in controls [37].
IV. Discussion
Studies of cytokine levels in adolescent BD patients are insufficient. This study aimed to investigate changes in inflammatory cytokine levels for adolescent BD patients, aged 18 or younger.
IL-6 levels positively correlated with the mood symptoms across adolescent BD groups, as confirmed by several studies [33,40]. These findings are congruent with the fact that the increased level of IL-6 is linked with other mental disorders such as Alzheimer’s Disease (AD), Parkinson’s Disease (PD), and brain cancer [41]. Goldstein et al. confirmed the positive correlation between IL-6 levels and symptomatic duration, which can be explained by the findings that overproduction of IL-6 leads to longer periods of neuroinflammatory multiple sclerosis (MS) (33,41). As exposure to medication and obesity had implications on IL-6 levels [33,34], future studies must control such factors when examining IL-6 levels in BD.
Although IL-8 levels increased in the BD group compared to the MDD group [32], there were no studies that examined the difference in IL-8 levels between the BD and HC groups. IL-8 levels are positively correlated with body mass, waist circumference, and lean body mass, but not significantly affected by sex [42], and these factors must be considered in future research comparing BD and HC.
Confirmed by multiple studies, it is evident that TNF-α levels increase across adolescent HC, MDD, and BD groups [32,35,40]. These findings are also congruent in adult BD patients, as a myriad of studies have found increased TNF-α levels [43,44]. It is known that TNF-α dysfunctions the brain blood-brain barrier (BBB); that is, it allows more inflammatory mediator cells and peripheral immune cells to infiltrate into the CNS, which leads to mood disorders [45]. These findings indicate that TNF-α can be an objective biomarker that can distinguish between BD and MDD diagnosis.
Hatch et al. found that TNF-α is the highest in the adolescent symptomatic BD group, followed by asymptomatic and HC [40], which implies that if medications are applied effectively to patients, TNF-α levels can be decreased accordingly. In fact, in an experiment using mice, antipsychotic drugs demonstrated anti-inflammatory effects, thereby decreasing the synthesis of IL-6 and TNF-α by lipopolysaccharides [46]. Therefore, the future direction of research that focuses on treatment for bipolar and mood disorders needs to effectively regulate TNF-α levels.
There exists a notable inconsistency around IL-10 levels in adolescent BD patients. Karthikeyan et al. found the lowered level of IL-10 in symptomatic periods [36], yet some studies found the elevated level of IL-10 in the adult BD group [47,48,49]. These discrepancies can be attributed to the detectability of IL-10. One research indicated that more than IL-10 was not detectable within 90% of elderly subjects [50]. As IL-10 levels are detectable at low levels in humans, the sensitivity of the bioassay also affects the IL-10 [51], which could also be attributed to past studies’ inconsistency. In addition, according to Wiener et al., IL-10 levels are found to be dynamic: in earlier stages of mood disorder, IL-10 levels increased, while during the course of the disorder, the levels decreased [52]. To address these discrepancies, future researchers can examine the pro- to anti-inflammatory marker ratio, rather than examining solely IL-10 levels, as one study reported that the ratios have higher sensitivity than individual markers in BD youth [36]. In addition, they may examine the level of IL-10 based on symptoms during the course of the BD, which may yield specific changes in IL-10 levels.
A single study examined the increased IL-1β level in adolescent BD patients [37]. Similarly, one study found that IL-1β level is proportional to the severity of illness, and the level also increased in elderly BD patients compared to HC [53]. These findings can be attributed to the fact that IL-1β is known to be a biological marker that is central to explaining different human behaviors. One experiment using rats confirmed the positive correlation between acute stress and the level of IL-1β [54].
This study examined cytokines as primary biomarkers for adolescent BD, yet did not examine brain-derived neurotrophic factor (BDNF). According to Karthikeyan et al., BDNF did not have statistical differences in adolescent BD compared to HC [36]. In addition, another research confirmed reduced levels of BDNF at ages 10-19 years compared to 0-9 years and 30-39 years, which implies the age-related difference in the BDNF level [55]. There also lie other variables, such as age, weight, and gender, that affect BDNF levels, as one study reported lower platelet BDNF levels in women than men [56]. Still, BDNF must not be eclipsed as an inconsequential factor for other mental disorders, as a study showed its association with autism [57].
Goldstein et al. reported higher levels of high-sensitivity C-Reactive protein (hsCRP) for adolescents’ longer duration of BD [33]. Yet, this study did not examine CRP levels as a valuable biomarker for adolescent BD because CRP can increase non-specifically in various conditions. Factors including infections, autoimmune conditions, cardiovascular events, past trauma or injury, cancer, diet, obesity, smoking, and alcohol were found to affect CRP levels [58], making it difficult to control for confounding variables and to accurately attribute changes in CRP levels specifically to adolescent BD patients compared to HCs. This suggests that cytokine levels may be influenced by such confounding variables; hence, blood tests to detect cytokine levels must not be conducted on BD patients with autoimmune diseases, a history of steroid use, or alcohol or drug consumption [59,60,61].
One study found that TNF-α and IL-6 levels did not show any statistical difference for adult BD patients, compared to HC [48,59]. This implies the uniqueness of such markers in adolescent BD patients, which will be crucial in future studies specifically investigating medications, treatments, and prevention plans for adolescent BD.
Exemplified by some articles, cytokine levels are influenced by treatment and symptom variations [33,40]. Therefore, a single blood test alone has limitations in sufficiently reflecting the diversity of symptoms and changes in cytokine levels following psychiatric drug treatment. This must be considered in future research as well as other reviews of cytokine levels in adolescent BD patients.
A limitation of this systematic review is the small number of studies included. Also, due to the inaccessibility of specific patient data, studies including both adults and adolescents without disaggregated individual information could not be considered. Although Table 1 indicates whether the confounding variables were controlled for each study, future studies must effectively account for factors such as sex, gender, obesity, history of abuse, and family history, among others.
V. Conclusion
This systematic review included studies that reported differences in levels of cytokines, including IL-6, IL-8, TNF-α, IL-10, and IL-1β, for adolescents with bipolar disorder (BD). The levels of pro-inflammatory cytokines (IL-6, IL-8, TNF-α, and IL-1β) positively correlate with adolescents' symptoms of bipolar disorder, which corroborates the preliminary findings about the effect of neuro-inflammation on neuronal activities. Further research is needed to address the inconsistency of the anti-inflammatory cytokine IL-10. Overall, this examination of multiple biomarkers will be useful in future research to implement treatment, counseling, medication, and prevention strategies specific to adolescents with bipolar disorder.
References
- Digiovanni, A., Ajdinaj, P., Russo, M., Sensi, S. L., Onofrj, M., & Thomas, A. (2022). Bipolar spectrum disorders in neurologic disorders. Frontiers in psychiatry, 13, 1046471. [CrossRef]
- American Psychiatric Association. DSM-5 Task Force., Diagnostic and Statistical Manual of Mental Disorders : DSM-5. 5th ed. Washington, DC: American Psychiatric Association; (2013). 947 p.
- Waraich P, Goldner EM, Somers JM, Hsu L. Prevalence and incidence studies of mood disorders: a systematic review of the literature. Can J Psychiatry. (2004) 49:124–38. [CrossRef]
- Birmaher, B. (2013), Bipolar disorder in children and adolescents. Child Adolesc Ment Health, 18: 140-148.
- Birmaher B, Axelson D, Strober M, Gill MK, Valeri S, Chiappetta L, et al. Clinical course of children and adolescents with bipolar spectrum disorders. Arch Gen Psychiatry. (2006) 63:175–83. [CrossRef]
- Bolton, S., Warner, J., Harriss, E., Geddes, J., & Saunders, K. E. A. (2021). Bipolar disorder: Trimodal age-at-onset distribution. Bipolar disorders, 23(4), 341–356.
- Foulkes, L., & Blakemore, S. J. (2018). Studying individual differences in human adolescent brain development. Nature neuroscience, 21(3), 315–323. [CrossRef]
- Bombin, I., Mayoral, M., Castro-Fornieles, J., Gonzalez-Pinto, A., de la Serna, E., Rapado-Castro, M., Barbeito, S., Parellada, M., Baeza, I., Graell, M., Payá, B., & Arango, C. (2013). Neuropsychological evidence for abnormal neurodevelopment associated with early-onset psychoses. Psychological medicine, 43(4), 757–768. [CrossRef]
- Polderman, T. J., Benyamin, B., de Leeuw, C. A., Sullivan, P. F., van Bochoven, A., Visscher, P. M., & Posthuma, D. (2015). Meta-analysis of the heritability of human traits based on fifty years of twin studies. Nature genetics, 47(7), 702–709. [CrossRef]
- O'Connell, K. S., & Coombes, B. J. (2021). Genetic contributions to bipolar disorder: current status and future directions. Psychological medicine, 51(13), 2156–2167. [CrossRef]
- Mortensen PB, Pedersen CB, Melbye M, Mors O, Ewald H. Individual and familial risk factors for bipolar affective disorders in Denmark. Arch Gen Psychiatry. 2003;60:1209–1215. [CrossRef]
- Arango, C., Dragioti, E., Solmi, M., Cortese, S., Domschke, K., Murray, R. M., Jones, P. B., Uher, R., Carvalho, A. F., Reichenberg, A., Shin, J. I., Andreassen, O. A., Correll, C. U., & Fusar-Poli, P. (2021). Risk and protective factors for mental disorders beyond genetics: an evidence-based atlas. World psychiatry : official journal of the World Psychiatric Association (WPA), 20(3), 417–436. [CrossRef]
- McGowan, P.O., Kato, T. Epigenetics in mood disorders. Environ Health Prev Med 13, 16–24 (2008). [CrossRef]
- Dudek, D., Siwek, M., Zielińska, D., Jaeschke, R., & Rybakowski, J. (2013). Diagnostic conversions from major depressive disorder into bipolar disorder in an outpatient setting: results of a retrospective chart review. Journal of affective disorders, 144(1-2), 112–115. [CrossRef]
- Goldstein, B. I., Collinger, K. A., Lotrich, F., Marsland, A. L., Gill, M. K., Axelson, D. A., & Birmaher, B. (2011). Preliminary findings regarding proinflammatory markers and brain-derived neurotrophic factor among adolescents with bipolar spectrum disorders. Journal of child and adolescent psychopharmacology, 21(5), 479–484. [CrossRef]
- Medzhitov, R. Origin and physiological roles of inflammation. Nature 454, 428–435 (2008). [CrossRef]
- Dantzer, R., O'Connor, J., Freund, G. et al. From inflammation to sickness and depression: when the immune system subjugates the brain. Nat Rev Neurosci 9, 46–56 (2008). [CrossRef]
- Allan, S., Rothwell, N. Cytokines and acute neurodegeneration. Nat Rev Neurosci 2, 734–744 (2001).
- Uzzan, S., & Azab, A. N. (2021). Anti-TNF-α Compounds as a Treatment for Depression. Molecules (Basel, Switzerland), 26(8), 2368. [CrossRef]
- Cannon, T. D., Chung, Y., He, G., Sun, D., Jacobson, A., van Erp, T. G., McEwen, S., Addington, J., Bearden, C. E., Cadenhead, K., Cornblatt, B., Mathalon, D. H., McGlashan, T., Perkins, D., Jeffries, C., Seidman, L. J., Tsuang, M., Walker, E., Woods, S. W., Heinssen, R., … North American Prodrome Longitudinal Study Consortium (2015). Progressive reduction in cortical thickness as psychosis develops: a multisite longitudinal neuroimaging study of youth at elevated clinical risk. Biological psychiatry, 77(2), 147–157. [CrossRef]
- Kummer, K. K., Zeidler, M., Kalpachidou, T., & Kress, M. (2021). Role of IL-6 in the regulation of neuronal development, survival and function. Cytokine, 144, 155582. [CrossRef]
- Mondelli, V., Cattaneo, A., Murri, M. B., Di Forti, M., Handley, R., Hepgul, N., Miorelli, A., Navari, S., Papadopoulos, A. S., Aitchison, K. J., Morgan, C., Murray, R. M., Dazzan, P., & Pariante, C. M. (2011). Stress and inflammation reduce brain-derived neurotrophic factor expression in first-episode psychosis: a pathway to smaller hippocampal volume. The Journal of clinical psychiatry, 72(12), 1677–1684.
- Ghafelehbashi, H., Pahlevan Kakhki, M., Kular, L., Moghbelinejad, S., & Ghafelehbashi, S. H. (2017). Decreased Expression of IFNG-AS1, IFNG and IL-1B Inflammatory Genes in Medicated Schizophrenia and Bipolar Patients. Scandinavian journal of immunology, 86(6), 479–485.
- Rossi, S., Sacchetti, L., Napolitano, F., De Chiara, V., Motta, C., Studer, V., Musella, A., Barbieri, F., Bari, M., Bernardi, G., Maccarrone, M., Usiello, A., & Centonze, D. (2012). Interleukin-1β causes anxiety by interacting with the endocannabinoid system. The Journal of neuroscience : the official journal of the Society for Neuroscience, 32(40), 13896–13905. [CrossRef]
- Fillman, S. G., Weickert, T. W., Lenroot, R. K., Catts, S. V., Bruggemann, J. M., Catts, V. S., & Weickert, C. S. (2016). Elevated peripheral cytokines characterize a subgroup of people with schizophrenia displaying poor verbal fluency and reduced Broca's area volume. Molecular psychiatry, 21(8), 1090–1098. [CrossRef]
- Iyer, S. S., & Cheng, G. (2012). Role of interleukin 10 transcriptional regulation in inflammation and autoimmune disease. Critical reviews in immunology, 32(1), 23–63. [CrossRef]
- Porro, C., Cianciulli, A., & Panaro, M. A. (2020). The Regulatory Role of IL-10 in Neurodegenerative Diseases. Biomolecules, 10(7), 1017. [CrossRef]
- Tsai S. J. (2021). Role of interleukin 8 in depression and other psychiatric disorders. Progress in neuro-psychopharmacology & biological psychiatry, 106, 110173.
- Fernandes, B. S., Steiner, J., Molendijk, M. L., Dodd, S., Nardin, P., Gonçalves, C. A., Jacka, F., Köhler, C. A., Karmakar, C., Carvalho, A. F., & Berk, M. (2016). C-reactive protein concentrations across the mood spectrum in bipolar disorder: a systematic review and meta-analysis. The lancet. Psychiatry, 3(12), 1147–1156. [CrossRef]
- Sayana, P., Colpo, G. D., Simões, L. R., Giridharan, V. V., Teixeira, A. L., Quevedo, J., & Barichello, T. (2017). A systematic review of evidence for the role of inflammatory biomarkers in bipolar patients. Journal of psychiatric research, 92, 160–182. [CrossRef]
- Elsässer-Beile, U., Dursunoglu, B., Gallati, H., Mönting, J. S., & von Kleist, S. (1995). Comparison of cytokine production in blood cell cultures of healthy children and adults. Pediatric allergy and immunology : official publication of the European Society of Pediatric Allergy and Immunology, 6(3), 170–174. [CrossRef]
- Skibinska, M., Rajewska-Rager, A., Dmitrzak-Weglarz, M., Kapelski, P., Lepczynska, N., Kaczmarek, M., & Pawlak, J. (2022). Interleukin-8 and tumor necrosis factor-alpha in youth with mood disorders-A longitudinal study. Frontiers in psychiatry, 13, 964538. [CrossRef]
- Goldstein, B. I., Lotrich, F., Axelson, D. A., Gill, M. K., Hower, H., Goldstein, T. R., Fan, J., Yen, S., Diler, R., Dickstein, D., Strober, M. A., Iyengar, S., Ryan, N. D., Keller, M. B., & Birmaher, B. (2015). Inflammatory markers among adolescents and young adults with bipolar spectrum disorders. The Journal of clinical psychiatry, 76(11), 1556–1563. [CrossRef]
- Goldstein, B. I., Collinger, K. A., Lotrich, F., Marsland, A. L., Gill, M. K., Axelson, D. A., & Birmaher, B. (2011). Preliminary findings regarding proinflammatory markers and brain-derived neurotrophic factor among adolescents with bipolar spectrum disorders. Journal of child and adolescent psychopharmacology, 21(5), 479–484. [CrossRef]
- Bai, Y. M., Chen, M. H., Hsu, J. W., Huang, H. H., Jeng, J. S., & Tsai, S. J. (2024). Distinct Effects of Major Affective Disorder Diagnoses and Suicidal Symptom Severity on Inhibitory Control Function and Proinflammatory Cytokines: Single-Site Analysis of 800 Adolescents and Adults. The international journal of neuropsychopharmacology, 27(10), pyae043. [CrossRef]
- Karthikeyan, S., Dimick, M. K., Fiksenbaum, L., Jeong, H., Birmaher, B., Kennedy, J. L., Lanctôt, K., Levitt, A. J., Miller, G. E., Schaffer, A., Young, L. T., Youngstrom, E. A., Andreazza, A. C., & Goldstein, B. I. (2022). Inflammatory markers, brain-derived neurotrophic factor, and the symptomatic course of adolescent bipolar disorder: A prospective repeated-measures study. Brain, behavior, and immunity, 100, 278–286. [CrossRef]
- Miklowitz, D. J., Portnoff, L. C., Armstrong, C. C., Keenan-Miller, D., Breen, E. C., Muscatell, K. A., Eisenberger, N. I., & Irwin, M. R. (2016). Inflammatory cytokines and nuclear factor-kappa B activation in adolescents with bipolar and major depressive disorders. Psychiatry research, 241, 315–322. [CrossRef]
- Terczynska, M., Bargiel, W., Grabarczyk, M., Kozlowski, T., Zakowicz, P., Bojarski, D., Wasicka-Przewozna, K., Kapelski, P., Rajewska-Rager, A., & Skibinska, M. (2025). Circulating Growth Factors and Cytokines Correlate with Temperament and Character Dimensions in Adolescents with Mood Disorders. Brain sciences, 15(2), 121. [CrossRef]
- Pearlstein, J. G., Staudenmaier, P. J., West, A. E., Geraghty, S., & Cosgrove, V. E. (2020). Immune response to stress induction as a predictor of cognitive-behavioral therapy outcomes in adolescent mood disorders: A pilot study. Journal of psychiatric research, 120, 56–63. [CrossRef]
- Hatch, J. K., Scola, G., Olowoyeye, O., Collins, J. E., Andreazza, A. C., Moody, A., Levitt, A. J., Strauss, B. H., Lanctot, K. L., & Goldstein, B. I. (2017). Inflammatory Markers and Brain-Derived Neurotrophic Factor as Potential Bridges Linking Bipolar Disorder and Cardiovascular Risk Among Adolescents. The Journal of clinical psychiatry, 78(3), e286–e293. [CrossRef]
- Kummer, K. K., Zeidler, M., Kalpachidou, T., & Kress, M. (2021). Role of IL-6 in the regulation of neuronal development, survival and function. Cytokine, 144, 155582. [CrossRef]
- Lagzdina, R., Rumaka, M., Gersone, G., & Tretjakovs, P. (2023). Circulating Levels of IL-8 and MCP-1 in Healthy Adults: Changes after an Acute Aerobic Exercise and Association with Body Composition and Energy Metabolism. International journal of molecular sciences, 24(19), 14725. [CrossRef]
- Elhaik, E., & Zandi, P. (2015). Dysregulation of the NF-κB pathway as a potential inducer of bipolar disorder. Journal of psychiatric research, 70, 18–27. [CrossRef]
- Goldstein, B. I., Kemp, D. E., Soczynska, J. K., & McIntyre, R. S. (2009). Inflammation and the phenomenology, pathophysiology, comorbidity, and treatment of bipolar disorder: a systematic review of the literature. The Journal of clinical psychiatry, 70(8), 1078–1090.
- Uzzan, S., & Azab, A. N. (2021). Anti-TNF-α Compounds as a Treatment for Depression. Molecules (Basel, Switzerland), 26(8), 2368. [CrossRef]
- Sugino, H., Futamura, T., Mitsumoto, Y., Maeda, K., & Marunaka, Y. (2009). Atypical antipsychotics suppress production of proinflammatory cytokines and up-regulate interleukin-10 in lipopolysaccharide-treated mice. Progress in neuro-psychopharmacology & biological psychiatry, 33(2), 303–307. [CrossRef]
- Hsu, J. W., Lirng, J. F., Wang, S. J., Lin, C. L., Yang, K. C., Liao, M. H., & Chou, Y. H. (2014). Association of thalamic serotonin transporter and interleukin-10 in bipolar I disorder: a SPECT study. Bipolar disorders, 16(3), 241–248. [CrossRef]
- Kunz, M., Ceresér, K. M., Goi, P. D., Fries, G. R., Teixeira, A. L., Fernandes, B. S., Belmonte-de-Abreu, P. S., Kauer-Sant'Anna, M., Kapczinski, F., & Gama, C. S. (2011). Serum levels of IL-6, IL-10 and TNF-α in patients with bipolar disorder and schizophrenia: differences in pro- and anti-inflammatory balance. Revista brasileira de psiquiatria (Sao Paulo, Brazil : 1999), 33(3), 268–274.
- Remlinger-Molenda, A., Wojciak, P., Michalak, M., Karczewski, J., & Rybakowski, J. K. (2012). Selected cytokine profiles during remission in bipolar patients. Neuropsychobiology, 66(3), 193–198. [CrossRef]
- Nematollahi, H. R., Hosseini, R., Bijani, A., Akhavan-Niaki, H., Parsian, H., Pouramir, M., Saravi, M., Bagherzadeh, M., Mosapour, A., Saleh-Moghaddam, M., Rajabian, M., Golpour, M., & Mostafazadeh, A. (2019). Interleukin 10, lipid profile, vitamin D, selenium, metabolic syndrome, and serum antioxidant capacity in elderly people with and without cardiovascular disease: Amirkola health and ageing project cohort-based study. ARYA atherosclerosis, 15(5), 233–240. [CrossRef]
- Schlaak, J. F., Schmitt, E., Hüls, C., Meyer zum Büschenfelde, K. H., & Fleischer, B. (1994). A sensitive and specific bioassay for the detection of human interleukin-10. Journal of immunological methods, 168(1), 49–54. [CrossRef]
- Wiener, C. D., Moreira, F. P., Portela, L. V., Strogulski, N. R., Lara, D. R., da Silva, R. A., Souza, L. D. M., Jansen, K., & Oses, J. P. (2019). Interleukin-6 and Interleukin-10 in mood disorders: A population-based study. Psychiatry research, 273, 685–689. [CrossRef]
- Thomas, A. J., Davis, S., Morris, C., Jackson, E., Harrison, R., & O'Brien, J. T. (2005). Increase in interleukin-1beta in late-life depression. The American journal of psychiatry, 162(1), 175–177. [CrossRef]
- Nguyen, K. T., Deak, T., Owens, S. M., Kohno, T., Fleshner, M., Watkins, L. R., & Maier, S. F. (1998). Exposure to acute stress induces brain interleukin-1beta protein in the rat. The Journal of neuroscience : the official journal of the Society for Neuroscience, 18(6), 2239–2246. [CrossRef]
- Katoh-Semba, R., Wakako, R., Komori, T., Shigemi, H., Miyazaki, N., Ito, H., Kumagai, T., Tsuzuki, M., Shigemi, K., Yoshida, F., & Nakayama, A. (2007). Age-related changes in BDNF protein levels in human serum: differences between autism cases and normal controls. International journal of developmental neuroscience : the official journal of the International Society for Developmental Neuroscience, 25(6), 367–372. [CrossRef]
- Lommatzsch, M., Zingler, D., Schuhbaeck, K., Schloetcke, K., Zingler, C., Schuff-Werner, P., & Virchow, J. C. (2005). The impact of age, weight and gender on BDNF levels in human platelets and plasma. Neurobiology of aging, 26(1), 115–123.
- Taurines, R., Segura, M., Schecklmann, M., Albantakis, L., Grünblatt, E., Walitza, S., Jans, T., Lyttwin, B., Haberhausen, M., Theisen, F. M., Martin, B., Briegel, W., Thome, J., Schwenck, C., Romanos, M., & Gerlach, M. (2014). Altered peripheral BDNF mRNA expression and BDNF protein concentrations in blood of children and adolescents with autism spectrum disorder. Journal of neural transmission (Vienna, Austria : 1996), 121(9), 1117–1128. [CrossRef]
- Landry, A., Docherty, P., Ouellette, S., & Cartier, L. J. (2017). Causes and outcomes of markedly elevated C-reactive protein levels. Canadian family physician Medecin de famille canadien, 63(6), e316–e323.
- Lovell, D. J., Giannini, E. H., Reiff, A., Cawkwell, G. D., Silverman, E. D., Nocton, J. J., Stein, L. D., Gedalia, A., Ilowite, N. T., Wallace, C. A., Whitmore, J., & Finck, B. K. (2000). Etanercept in children with polyarticular juvenile rheumatoid arthritis. Pediatric Rheumatology Collaborative Study Group. The New England journal of medicine, 342(11), 763–769. [CrossRef]
- Imhof, A., Froehlich, M., Brenner, H., Boeing, H., Pepys, M. B., & Koenig, W. (2001). Effect of alcohol consumption on systemic markers of inflammation. Lancet (London, England), 357(9258), 763–767. [CrossRef]
- Pacifici, R., Zuccaro, P., Pichini, S., Roset, P. N., Poudevida, S., Farré, M., Segura, J., & De la Torre, R. (2003). Modulation of the immune system in cannabis users. JAMA, 289(15), 1929–1931. [CrossRef]
- Hope, S., Melle, I., Aukrust, P., Steen, N. E., Birkenaes, A. B., Lorentzen, S., Agartz, I., Ueland, T., & Andreassen, O. A. (2009). Similar immune profile in bipolar disorder and schizophrenia: selective increase in soluble tumor necrosis factor receptor I and von Willebrand factor. Bipolar disorders, 11(7), 726–734. [CrossRef]
Figure 1.
PRISMA Flow Diagram showing the process of literature review in this study.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



