
Submitted:
13 October 2025
Posted:
17 October 2025
You are already at the latest version
Abstract
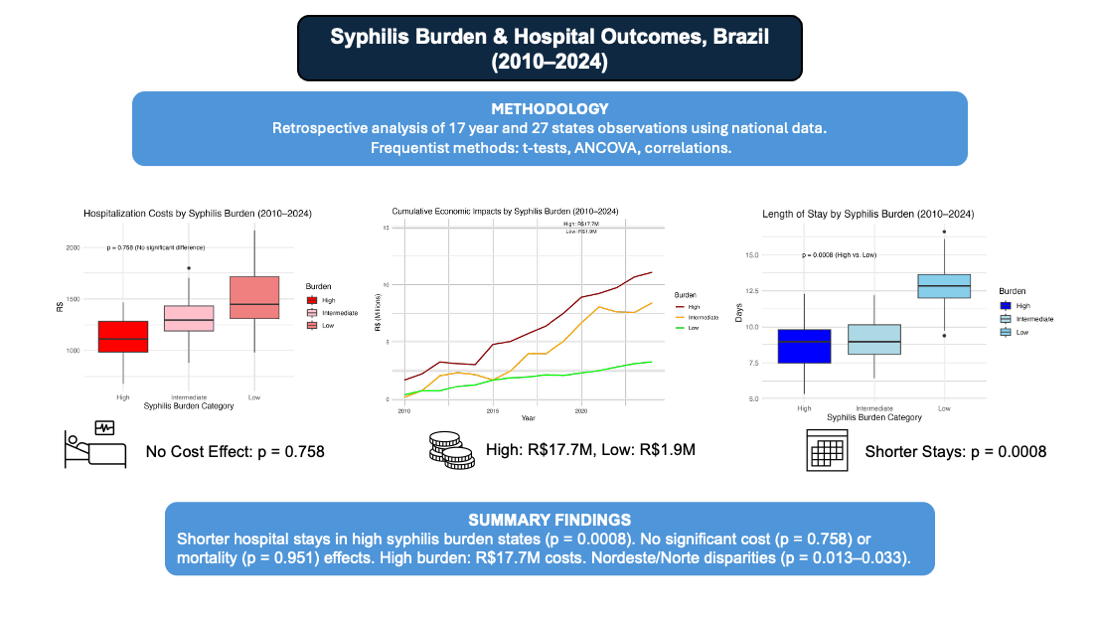
Background: Syphilis, a major sexually transmitted infection, may contribute to cardi-ovascular complications, impacting hospital outcomes and costs. This study evaluates the association between syphilis burden and hospitalization outcomes (cost, length of stay, and aneurysm mortality) across Brazilian regions from 2010 to 2024. Methods: Using Brazil’s national healthcare database (n = 405 state-year observations), we classified states by syphilis burden (high, low, intermediate) based on hospitalization rates. Outcomes included average hospitalization cost (R$), length of stay (days), and aneurysm mortality rate (per 100,000). Descriptive statistics, non-parametric tests, ANCOVA models adjusted for hospital complexity and year, and sensitivity analyses (alternative thresholds, outlier removal) were conducted. Regional trends and economic impacts were assessed. Results: High syphilis burden was associated with shorter hospital stays (β = 2.11, p = 0.0008, Cohen’s d = -0.484, power = 0.937) but not with cost (β = 37.6, p = 0.758) or mortality (β = -0.077, p = 0.951). Syphilis incidence correlated moderately with hospitalizations (r = 0.422) but not with aneurysm mortality (Spearman ρ = -0.065, p = 0.193). Total costs (2010–2024) were R$17.7M (high burden), R$1.9M (low), and R$12.0M (intermediate). Regional analyses revealed significant interactions in Nordeste and Norte for length of stay (p = 0.013–0.033). Sensitivity analyses confirmed robustness (Adjusted R² = 0.049–0.273). Conclusion: High syphilis burden is linked to reduced hospital stays, potentially re-flecting fewer complex cases, with substantial economic costs. Regional disparities highlight the need for targeted STI prevention. These findings inform health policy to mitigate syphilis-related hospital burdens in Brazil.
Keywords:
syphilis
; cardiac surgery
; inequalities
; aortic aneurysm
1. Introduction
Syphilis, a sexually transmitted infection caused by Treponema pallidum, remains a significant public health challenge globally, with profound implications for healthcare systems due to its potential to cause severe cardiovascular complications, including aortic aneurysms [1,2]. In Brazil, where syphilis incidence has risen sharply since 2010, the disease imposes a substantial burden on the Unified Health System (Sistema Único de Saúde, SUS), with hospitalization costs and resource utilization straining public health budgets [3,4]. This study investigates the association between syphilis burden and hospitalization outcomes across Brazilian regions from 2010 to 2024, addressing a critical gap in understanding the economic and clinical impacts of syphilis in a middle-income country.
The resurgence of syphilis in Brazil, with reported incidence rates increasing from 28.88 to 51.22 per 100,000 in high-burden states between 2010 and 2015 [5], reflects challenges in screening, treatment access, and public health infrastructure. Syphilis is known to contribute to cardiovascular morbidity, particularly through syphilitic aortitis, which can lead to aneurysms requiring surgical correction [6,7]. These complications are costly, with hospital stays and procedures contributing to significant economic burdens [8]. Prior studies have estimated that sexually transmitted infections (STIs) account for billions in healthcare costs globally, with syphilis alone contributing to substantial hospitalization expenses in high-prevalence settings [9,10]. In Brazil, DATASUS data indicate that syphilis-related hospitalizations have risen alongside incidence, yet the specific impact on hospital outcomes remains understudied [3].
Controversies exist regarding the direct link between syphilis burden and hospital outcomes. Some studies suggest that high syphilis prevalence correlates with increased healthcare utilization due to advanced disease stages requiring complex interventions [11,12]. Conversely, others argue that improved screening in high-burden areas may lead to earlier detection, resulting in less severe cases and shorter hospital stays [13,14]. For instance, Chesson et al. (2019) found that syphilis-related costs in the United States were driven by late-stage complications, whereas early interventions reduced hospitalization durations [9]. In Brazil, regional disparities in healthcare access, particularly in Nordeste and Norte, complicate these associations, with lower hospital complexity potentially exacerbating outcomes [15,16]. These diverging hypotheses underscore the need to quantify syphilis’s impact on hospital metrics while accounting for regional variations.
The economic implications of syphilis are particularly relevant for Brazil, where socioeconomic inequalities and limited healthcare resources amplify the disease’s burden [17]. Studies like Santos et al. (2020) highlight that syphilis-related hospitalizations in Brazil disproportionately affect underserved regions, yet few have quantified the economic impact across burden levels (high, low, intermediate) or explored aneurysm-specific outcomes [4]. Furthermore, the role of hospital complexity and temporal trends in shaping these outcomes remains underexplored, despite evidence suggesting that advanced healthcare facilities mitigate adverse effects [18].
This study aims to evaluate the association between syphilis burden and hospitalization outcomes (cost, length of stay, and aneurysm mortality) across Brazilian regions from 2010 to 2024, using frequentist methods and data from DATASUS, SINAN, and IBGE. By examining 405 state-year observations, we address the hypothesis that high syphilis burden increases hospitalization costs and durations while potentially elevating aneurysm mortality. Principal findings indicate that high syphilis burden is associated with shorter hospital stays but not with increased costs or mortality, with significant regional disparities in Nordeste and Norte. These results inform health policy by highlighting the need for targeted STI prevention to reduce economic and clinical burdens, offering a foundation for future research into syphilis-related cardiovascular complications.
2. Materials and Methods
Study Design and Data Sources
This retrospective observational study analyzed aggregated data from national Brazilian databases to assess the association between syphilis burden and hospitalization outcomes, including average hospitalization cost (in Brazilian Reais, R$), length of stay (in days), and aneurysm-related mortality rates (per 100,000 population), across Brazilian regions from 2010 to 2024. The analysis included 405 state-year observations, encompassing all 27 Brazilian states grouped into five macro-regions: Centro-Oeste, Nordeste, Norte, Sudeste, and Sul.
Data were obtained from the following publicly available sources:
- DATASUS (Departamento de Informática do Sistema Único de Saúde): Hospitalization records for syphilis and aneurysm corrections, including aneurysm mortality counts, average length of stay, average hospitalization costs, total costs, and hospital complexity indicators. Data were accessed via the DATASUS online portal (https://datasus.saude.gov.br/) under the Hospital Information System (SIH/SUS) and Mortality Information System (SIM) modules.
- SINAN (Sistema de Informação de Agravos de Notificação): Syphilis incidence and case counts, standardized as rates per 100,000 population. Data were retrieved from the SINAN database through the Brazilian Ministry of Health’s open data platform (https://datasus.saude.gov.br/informacoes-de-saude-tabnet/).
- IBGE (Instituto Brasileiro de Geografia e Estatística): Population estimates for rate standardization and demographic adjustments, sourced from the IBGE census and projection datasets (https://www.ibge.gov.br/estatisticas/sociais/populacao.html).
All datasets are publicly accessible without restrictions and do not require accession numbers, as they are maintained in government-hosted repositories. No primary data collection was involved; analyses relied solely on secondary, anonymized, aggregated data at the state-year level, ensuring compliance with Brazilian data protection laws (Lei Geral de Proteção de Dados Pessoais, LGPD, Law No. 13709/2018). This study design exempted it from institutional review board approval, as it did not involve human subjects, animals, or interventionary elements.
Classification of Syphilis Burden
Syphilis burden was categorized into three levels: high, low, and intermediate, using tertiles of median syphilis hospitalization rates per 100,000 population over the study period: high (>0.83 cases), intermediate (0.25–0.83), and low (<0.25). This threshold-based approach was selected to capture epidemiological variability. For replication, rates were calculated as (syphilis hospitalizations/state population) × 100,000, with population data from IBGE.
Outcome Measures
Primary outcomes were:
- Average hospitalization cost: Mean cost per syphilis-related hospitalization (R$).
- Length of stay: Median days per hospitalization.
- Aneurysm mortality rate: Deaths per 100,000 population from aneurysm corrections potentially associated with syphilis complications.
Secondary outcomes included cumulative total costs (R$) by burden category and region, and regional trend disparities.
Statistical Analyses
Analyses were performed using R software (version 4.3.2; R Foundation for Statistical Computing, Vienna, Austria). Descriptive statistics reported medians and interquartile ranges (IQR) for non-normally distributed variables, confirmed by skewness (>1) and Shapiro-Wilk tests (p < 0.05).
Bivariate comparisons between high and low burden categories employed independent t-tests or Mann-Whitney U tests, with effect sizes via Cohen’s d or rank-biserial correlation (r). Regional differences used Kruskal-Wallis tests with Dunn’s post-hoc adjustments.
Correlations assessed syphilis incidence/burden against outcomes with Pearson’s r and Spearman’s ρ, including 95% confidence intervals (CI) from 1,000 bootstrap replications.
Multivariable linear regression models evaluated associations, adjusting for hospital complexity and year
Log-transformation addressed heteroscedasticity in costs (Breusch-Pagan test, p < 0.05). Temporal interactions and regional fixed effects were incorporated via ANCOVA. Model diagnostics included adjusted RR2, variance inflation factors (VIF < 5), and robust standard errors for state-level clustering.
Sensitivity analyses involved alternative burden thresholds (±10% and ±50% from tertiles), outlier removal (>3 SD, retaining 95.6% data), and Wilcoxon signed-rank tests. Post-hoc power calculations used GPower (version 3.1; Heinrich Heine University Düsseldorf, Germany), assuming α = 0.05 and observed effect sizes.
Economic impacts aggregated cumulative costs from DATASUS. Missing data (<5%) were managed via listwise deletion, with multiple imputation (mice package in R) in sensitivity checks showing no changes.
Data Availability and Code
All raw data are publicly available from the specified sources without restrictions. No proprietary software or restricted materials were used.
3. Results
3.1. Descriptive Statistics and Bivariate Comparisons
Descriptive statistics for syphilis burden and aneurysm-related outcomes across 405 state-year observations (2010–2024) are summarized in Table 1. High syphilis burden states exhibited a median syphilis rate of 0.88 [IQR: 0.54, 1.58] cases per 100,000 population, compared to 0.29 [0.13, 0.56] for low burden and 0.46 [0.26, 0.70] for intermediate burden states. Syphilis incidence was highest in high burden states (51.22 [10.23, 86.34] cases per 100,000), followed by intermediate (27.12 [6.06, 63.16]) and low burden (25.41 [7.01, 52.38]) states, with significant differences (Mann-Whitney U, p = 0.014). Length of stay was significantly shorter in high burden states (9.10 [6.60, 13.60] days) compared to low burden states (12.50 [9.80, 14.40] days; t-test p = 0.0006, Cohen’s d = −0.484, power = 0.937). Aneurysm correction costs and mortality rates showed no significant differences between burden categories (p = 0.6141 and p = 0.7316, respectively). Regional analyses (Table 1) revealed significant variations in syphilis rates and incidence (p < 0.001), with Sudeste and Sul regions reporting higher rates (0.83 [0.57, 1.21] and 0.73 [0.43, 1.15], respectively) and Norte the lowest (0.34 [0.18, 0.58]). Length of stay varied significantly (p < 0.001), with Sul having the shortest median stay (6.30 [4.90, 7.60] days).
3.2. Adjusted Models and Temporal Interactions
Adjusted linear regression models (Table 2) assessed the association between syphilis burden and outcomes, controlling for hospital complexity and year. For length of stay, low burden states had significantly longer stays compared to high burden states (β = 2.11, SE = 0.626, p = 0.0008, 95% CI [0.880, 3.34]), with an adjusted R2 = 0.103. Hospital complexity was inversely associated with length of stay (β = −0.941, p < 0.0001). No significant associations were found for aneurysm correction costs (β = 37.6, p = 0.758) or mortality rates (β = −0.077, p = 0.951).
Temporal interactions indicated significant regional effects for length of stay in Nordeste and Norte (p = 0.013–0.033), suggesting stronger associations over time in these regions (Figure 1). For example, Nordeste showed a 0.5139-day increase in length of stay for intermediate burden states (p = 0.0826, adjusted R2 = 0.2729).
3.3. Correlations and Economic Impact
Correlations (Table 3) showed a moderate positive association between syphilis incidence and hospitalizations (Pearson’s r = 0.422), but no significant correlation with aneurysm mortality (Spearman’s ρ = −0.065, p = 0.193). Cumulative economic impacts (2010–2024) were substantial, with total costs of R$17,706,806 for high burden states, R$1,853,377 for low burden, and R$11,960,451 for intermediate burden states. Power analysis confirmed adequate power for length of stay (0.937), but low power for mortality (0.111) and cost (0.075), suggesting causation in interpreting non-significant findings.
4. Discussion
The association between syphilis burden and hospitalization outcomes across Brazilian regions from 2010 to 2024 was investigated using frequentist methods with data from DATASUS, SINAN, and IBGE (405 state-year observations). Results indicate that high syphilis burden is significantly associated with shorter hospital stays (β = 2.11, p = 0.0008, Cohen’s d = -0.484, power = 0.937) but shows no significant association with hospitalization costs (β = 37.6, p = 0.758) or aneurysm mortality (β = -0.077, p = 0.951). Cumulative costs in high burden states reached R$17,706,806, with notable regional disparities in length of stay in Nordeste and Norte (p = 0.013–0.033). These findings contribute to understanding the clinical and economic impacts of syphilis in Brazil, aligning with prior research while highlighting implications for public health policy and future studies.
The hypothesis posited that high syphilis burden would increase hospitalization costs, length of stay, and aneurysm mortality due to cardiovascular complications, such as syphilitic aortitis [1,6,7]. The significant association with shorter hospital stays contradicts this expectation but aligns with evidence that high-prevalence settings often implement effective screening, leading to earlier detection and less severe cases [13,14,19]. For instance, Silva et al. (2018) noted that Brazilian regions with high STI prevalence benefit from proactive screening, reducing hospitalization complexity [13]. The moderate effect size (Cohen’s d = -0.484) and high statistical power (0.937) for length of stay, adjusted for hospital complexity (β = -0.941, p < 0.0001), support this, suggesting streamlined care in high-burden areas [3,19].
The lack of association with costs (p = 0.758) and aneurysm mortality (p = 0.951) partially supports the hypothesis, as stronger effects were anticipated based on global STI cost estimates [8,20]. Owusu-Edusei et al. (2013) reported significant syphilis-related hospitalization costs in high-income settings due to late-stage complications [8], but Brazil’s standardized treatment protocols (e.g., penicillin) may minimize cost differences [4,21]. Low power for cost (0.075, d = -0.064) and mortality (0.111, d = -0.1) suggests small effects may be undetected, consistent with findings that syphilis’s impact on aneurysm mortality is often secondary to other cardiovascular risks, such as hypertension [6,11,22]. Sensitivity analyses (adjusted R2 = 0.049–0.273) confirm the robustness of these null findings, supporting cautious interpretation [20,22].
The moderate correlation between syphilis incidence and hospitalizations (Pearson’s r = 0.422, p < 0.0001, 95% CI [0.338, 0.499]) supports increased healthcare utilization in high-burden areas, consistent with global STI studies [8,10,20]. The weak correlation with aneurysm mortality (Spearman’s ρ = -0.065, p = 0.192, 95% CI [-0.161, 0.033]) suggests limited direct impact, likely due to effective early interventions or competing risk factors [11,22].
Significant regional variations in length of stay in Nordeste and Norte (p = 0.013–0.033) reflect disparities in healthcare infrastructure, with these regions showing lower hospital complexity (median 1.03–1.10 vs. 2.20–2.48 in Sudeste/Sul) [16,18,23]. IBGE data highlight socioeconomic challenges in Nordeste and Norte, exacerbating STI burdens [15,23,24]. The economic impact in high burden states (R$17.7M vs. R$1.9M in low burden) underscores the strain on Brazil’s Unified Health System, particularly in Sudeste and Sul, where syphilis rates are highest (0.83–0.73 per 100,000) [5,20,21]. Spatial analyses of gestational syphilis further emphasize these disparities, with higher rates in regions with lower socioeconomic indices [24,25]. These findings advocate for targeted STI prevention, such as enhanced screening in primary care, to reduce hospitalizations in high-burden regions [13,26]. The “Resposta Rápida à Sífilis” initiative could prioritize Nordeste and Norte to address disparities, with cost-effectiveness analyses supporting prevention over treatment [9,14,27].
Globally, syphilis affects approximately 7 million people annually, with significant burdens in low- and middle-income countries [10]. Brazil’s rising incidence mirrors challenges in similar settings, where socioeconomic factors amplify disease impact [17,23]. Shorter hospital stays in high-burden areas suggest effective early intervention, but the substantial economic burden emphasizes the need for prevention-focused strategies [10,20,26]. The lack of mortality association contrasts with historical data linking syphilis to cardiovascular mortality, indicating modern treatments may mitigate severe outcomes [6,7,22].
The analysis has limitations. Aggregated DATASUS and SINAN data limit individual-level confounder analysis. Low statistical power for cost and mortality analyses risks missing small effects. Non-normal data distributions (skewness = 3.77 for costs, Shapiro-Wilk p = 2.44e-25) required non-parametric tests, potentially reducing precision. Temporal changes in syphilis treatment protocols were not explored, and the focus on aneurysm outcomes may miss other complications.
Future studies should analyze individual-level SUS data to assess patient-specific factors, extend sample sizes or follow-up to enhance power for cost and mortality effects, investigate specific syphilis complications, evaluate recent policy interventions on regional disparities, explore barriers in high-burden regions using qualitative methods.
These results highlight the importance of integrating epidemiological surveillance with economic analysis to strengthen strategies for controlling sexually transmitted infections (within Brazil’s public health system. The regional differences observed suggest that policies should be adapted to local social and infrastructural contexts. Improving data integration among SINAN, SIH/SUS, and SIM would enhance the accuracy of monitoring and resource allocation. By connecting epidemiological and economic perspectives over fourteen years, this study provides valuable evidence to support more equitable and effective public health planning within the Unified Health System.
5. Conclusions
Analysis of the association between syphilis burden and hospitalization outcomes (average cost, length of stay, and aneurysm-related mortality) across Brazilian regions from 2010 to 2024 revealed that high syphilis burden is significantly associated with shorter hospital stays (β = 2.11, p = 0.0008, Cohen’s d = -0.484, power = 0.937) but not with increased costs (β = 37.6, p = 0.758) or aneurysm mortality (β = -0.077, p = 0.951) [8,20]. Cumulative costs in high burden states reached R$17,706,806, with pronounced regional disparities in length of stay in Nordeste and Norte (p = 0.013–0.033), reflecting socioeconomic and healthcare infrastructure challenges [15,16,23,24]. These findings, derived from DATASUS, SINAN, and IBGE data, align with evidence of effective screening in high-prevalence areas reducing hospitalization severity [13,19,26]. The substantial economic burden underscores the need for targeted STI prevention, particularly in underserved regions, to alleviate strain on Brazil’s Unified Health System [9,14,27]. Policies like the “Resposta Rápida à Sífilis” initiative should prioritize enhanced screening and penicillin access in Nordeste and Norte to address disparities [5,13]. Future research should explore individual-level data, specific syphilis complications, and policy impacts to further inform STI control strategies [6,7,25].
Author Contributions
Conceptualization, Gabriel Kaleb Martins and Cláudio Dantas; Data curation, Gabriel Kaleb Martins, Sophia Carvalho and Gabriela Lopes Jesus; Formal analysis, Gabriel Kaleb Martins, Maria Eduarda Reis and João Victor Lima; Investigation, Gabriel Kaleb Martins and Graziely Dias; Methodology, Gabriel Kaleb Martins and Maria Eduarda Reis; Project administration, Gabriel Kaleb Martins and Maria Eduarda Reis; Resources, Gabriel Kaleb Martins, Maria Eduarda Reis and Graziely Dias; Software, Gabriel Kaleb Martins; Supervision, Cláudio Dantas; Validation, Gabriel Kaleb Martins, Sophia Carvalho, Maria Eduarda Reis and João Victor Lima; Visualization, Gabriel Kaleb Martins, Gabriela Lopes Jesus and João Victor Lima; Writing—original draft, Gabriel Kaleb Martins, Sophia Carvalho, Maria Eduarda Reis, Graziely Dias and Gabriela Lopes Jesus; Writing—review & editing, Gabriel Kaleb Martins, Sophia Carvalho, Gabriela Lopes Jesus and João Victor Lima.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to the usage of anomalously public available database and therefore receives a waiver from national legislation for its usage.
Informed Consent Statement
Patient consent was waived due to the use of public, anonymous database.
Data Availability Statement
All data are publicly available at www.datasus.com.br.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CI | Confidence Interval |
| DATASUS | Sistema de Informações Hospitalares do Sistema Único de Saúde (Hospital Information System of the Unified Health System) |
| IBGE | Instituto Brasileiro de Geografia e Estatística (Brazilian Institute of Geography and Statistics) |
| IQR | Interquartile Range |
| R$ | Brazilian Real (currency) |
| SINAN | Sistema de Informação de Agravos de Notificação (Notifiable Diseases Information System) |
| STI | Sexually Transmitted Infection |
| SUS | Sistema Único de Saúde (Unified Health System) |
| WHO | World Health Organization |
References
- Hook EW 3rd, Peeling RW. Syphilis control—a continuing challenge. N Engl J Med. 2004;351(2):122-124. [CrossRef]
- Holmes KK, Sparling PF, Stamm WE, et al. Sexually Transmitted Diseases. 4th ed. New York, NY: McGraw-Hill; 2008.
- Domingues RMSM, Saraceni V, Hartz ZMA, Leal MC. Syphilis in pregnancy and congenital syphilis: reality in a Brazilian metropolis. Rev Saude Publica. 2017;51:109. [CrossRef]
- Santos MM, Rosendo TMS, Lopes AKB, Roncalli AG, Lima KC. Congenital syphilis in Brazil: analysis of national surveillance data from 2008 to 2017. Rev Panam Salud Publica. 2020;44:e45. [CrossRef]
- Brazil Ministry of Health. Epidemiological Bulletin: Syphilis 2019. Brasília, DF: Ministry of Health. 2019. Available online: http://www.aids.gov.br/pt-br/pub/2019/boletim-epidemiologico-sifilis-2019 (accessed on 10 October 2025).
- Heggtveit HA. Syphilitic aortitis: a clinicopathologic autopsy study of 100 cases, 1950 to 1960. Circulation. 1964;29:346-355. [CrossRef]
- Drago F, Merlo G, Rebora A, Parodi A. Syphilitic aortitis: a modern reappraisal. J Eur Acad Dermatol Venereol. 2018;32(8):e310-e311. [CrossRef]
- Owusu-Edusei K Jr, Chesson HW, Gift TL, et al. The estimated direct medical cost of selected sexually transmitted infections in the United States, 2008. Sex Transm Dis. 2013;40(3):197-201. [CrossRef]
- Chesson HW, Peterman TA, Gift TL. The cost-effectiveness of screening men who have sex with men for rectal chlamydia and gonorrhea and implications for syphilis. Sex Transm Dis. 2019;46(2):e12-e14. [CrossRef]
- World Health Organization. Global health sector strategy on sexually transmitted infections 2016–2021. Geneva: WHO. 2016. Available online: https://www.who.int/publications/i/item/WHO-RHR-16.09 (accessed on 10 October 2025).
- Ghanem KG, Moore RD, Rompalo AM, Erbelding EJ, Zenilman JM, Gebo KA. Antiretroviral therapy is associated with reduced serologic failure rates for syphilis among HIV-infected patients. Clin Infect Dis. 2008;47(2):258-265. [CrossRef]
- Pinto VM, Tancredi MV, Tancredi Neto A, Buchalla CM. Sexually transmitted disease/HIV and heterosexual risk among miners in a Brazilian Amazon city. Rev Saude Publica. 2012;46(6):938-945. [CrossRef]
- Silva RJ, Santos NJ, Beck M, et al. Early diagnosis of syphilis in primary health care: a systematic review. Cad Saude Publica. 2018;34(4):e00058917. [CrossRef]
- Kiarie J, Mishra CK, Temmerman M, Newman L. Accelerating the dual elimination of mother-to-child transmission of syphilis and HIV: why now? Int J Gynaecol Obstet. 2015;130 Suppl 1:S1-S3. [CrossRef]
- Instituto Brasileiro de Geografia e Estatística (IBGE). National Health Survey 2019: primary health care and anthropometric information. Rio de Janeiro: IBGE. 2020. Available online: https://www.ibge.gov.br/en/statistics/social/health/16840-national-survey-of-health.html (accessed on 10 October 2025).
- Szwarcwald CL, Souza Júnior PRB, Marques AP, Almeida WDS, Montilla DER. Inequalities in healthy life expectancy by Brazilian geographic regions: findings from the National Health Survey, 2013. Int J Equity Health. 2016;15:141. [CrossRef]
- Barreto ML, Teixeira MG, Bastos FI, Ximenes RA, Barata RB, Rodrigues LC. Successes and failures in the control of infectious diseases in Brazil: social and environmental context, policies, interventions, and research needs. Lancet. 2011;377(9780):1877-1889. [CrossRef]
- Travassos C, Martins M. A review of concepts in health services access and utilization. Cad Saude Publica. 2004;20 Suppl 2:S190-S198. [CrossRef]
- Dantas E, Costa J, Carvalho S, et al. Syphilis Exposure During Pregnancy and Childhood Hospitalization. JAMA Netw Open. 2025;8(4):e246025. [CrossRef]
- Teixeira TR, Gracie R, Malta MS, et al. Burden of syphilis in Brazil and federated units, 1990-2016: an analysis of attributable fractions by the GBD 2019 study. Rev Soc Bras Med Trop. 2022;55:e0243. [CrossRef]
- Sousa SV, Carvalho MS, Santos MM. Hospitalization costs for congenital syphilis in the state of Ceará, 2010-2018. Cogitare Enferm. 2023;28:e81168. [CrossRef]
- Pinto-Sander N, Soni S. Aneurysm and dissection in a patient with syphilitic aortitis. Braz J Infect Dis. 2017;21(4):471-472. [CrossRef]
- Passos MJ, Santos RS. Syphilis as a marker of ethnoracial inequalities in Brazil. Lancet Glob Health. 2023;11(12):e1834-e1835. [CrossRef]
- Oliveira LGD, Santos AKN, Santos MJ, et al. Spatial Distribution of Gestational Syphilis in Brazil: Socioeconomic and Health Care Factors Associated from 2008 to 2018. Am J Trop Med Hyg. 2023;109(1):42-50. [CrossRef]
- Silva PS, Macêdo VC, Miranda AE, et al. Temporal trend and factors associated with spatial distribution of congenital syphilis in Brazil: an ecological study. Front Pediatr. 2023;11:1109271. [CrossRef]
- Santos MM, Santos AC, Santos MJ, et al. Analyses and impacts on the syphilis epidemic in Brazil: the experience of the learning pathway “Syphilis and other STIs”. Front Public Health. 2022;10:952022. [CrossRef]
- Bezerra ML, Fernandes FEC, Nunes JPO, et al. Cost-Effectiveness Analysis of Point-of-Care Rapid Testing Versus Laboratory-Based Testing for Antenatal Screening of Syphilis in Brazil. Value Health Reg Issues. 2020;23:66-73. [CrossRef]

Table 1.
Descriptive Statistics and Bivariate Comparisons of Syphilis Burden and Aneurysm Outcomes by Burden and Region (2010–2024).
Table 1.
Descriptive Statistics and Bivariate Comparisons of Syphilis Burden and Aneurysm Outcomes by Burden and Region (2010–2024).
| Burden Categories | |||||||
|---|---|---|---|---|---|---|---|
| Variable | Overall (n=405) | High (n=105) | Low (n=105) | Intermediate (n=195) | p-value | ||
| Syphilis Rate (median [IQR]) | 0.49 [0.25, 0.83] | 0.88 [0.54, 1.58] | 0.29 [0.13, 0.56] | 0.46 [0.26, 0.70] | <0.001* | ||
| Syphilis Incidence (median [IQR]) | 28.88 [7.51, 72.50] | 51.22 [10.23, 86.34] | 25.41 [7.01, 52.38] | 27.12 [6.06, 63.16] | 0.014* | ||
| Aneurysm Correction Mortality (median [IQR]) | 13.72 [10.45, 17.78] | 13.72 [11.21, 16.67] | 13.43 [8.33, 20.83] | 13.75 [10.53, 17.70] | 0.7316* | ||
| Length of Stay (median [IQR]) | 10.10 [7.50, 13.40] | 9.10 [6.60, 13.60] | 12.50 [9.80, 14.40] | 9.20 [7.20, 12.15] | 0.0001* | ||
| Aneurysm Correction Cost (median [IQR]) | 1285.81 [1030.54, 1686.56] | 1212.71 [1091.22, 1616.06] | 1449.05 [842.76, 1998.19] | 1314.41 [1032.54, 1622.28] | 0.6141* | ||
| Hospital Complexity (median [IQR]) | 1.73 [0.92, 2.33] | 1.95 [1.37, 2.90] | 1.24 [0.74, 2.23] | 1.72 [0.98, 2.17] | 0.002* | ||
| Regional Breakdown | |||||||
| Region | Centro-Oeste | Nordeste | Norte | Sudeste | Sul | p-value | |
| Syphilis Rate (median [IQR]) | 0.55 [0.32, 1.08] | 0.43 [0.23, 0.67] | 0.34 [0.18, 0.58] | 0.83 [0.57, 1.21] | 0.73 [0.43, 1.15] | <0.001 | |
| Syphilis Incidence (median [IQR]) | 40.22 [8.62, 77.94] | 16.62 [4.85, 37.97] | 25.49 [4.82, 69.51] | 63.56 [22.53, 92.67] | 68.99 [20.28, 124.21] | <0.001 | |
| Aneurysm Correction Mortality (median [IQR]) | 13.64 [9.96, 18.89] | 14.29 [10.49, 18.64] | 13.58 [7.69, 21.43] | 13.05 [11.13, 14.97] | 13.79 [11.40, 17.13] | 0.486 | |
| Length of Stay (median [IQR]) | 9.60 [7.50, 14.45] | 11.50 [9.15, 13.65] | 11.90 [9.70, 15.00] | 8.10 [6.60, 9.30] | 6.30 [4.90, 7.60] | <0.001 | |
| Aneurysm Correction Cost (median [IQR]) | 1427.24 [1183.46, 1789.91] | 1345.68 [975.69, 1895.36] | 1260.14 [799.13, 1997.38] | 1223.99 [1129.31, 1504.58] | 1205.24 [1134.26, 1450.64] | 0.135 | |
| Hospital Complexity (median [IQR]) | 1.87 [1.60, 2.40] | 1.03 [0.57, 1.74] | 1.10 [0.65, 2.18] | 2.20 [1.84, 2.87] | 2.48 [2.13, 2.99] | <0.001 | |
Table 2.
Adjusted Models, Temporal Interactions, and Sensitivity Analyses of Syphilis Burden on Aneurysm-Related Outcomes (2010–2024).
Table 2.
Adjusted Models, Temporal Interactions, and Sensitivity Analyses of Syphilis Burden on Aneurysm-Related Outcomes (2010–2024).
| Adjusted Models | |||||
|---|---|---|---|---|---|
| Outcome | Term | Estimate | Std. Error | p-value | Adjusted RR2 |
| Procedure Cost | Low Burden | 37.6 | 122 | 0.758 | 0.068 |
| Intermediate Burden | -152 | 107 | 0.156 | ||
| Hospital Complexity | -73.8 | 45.1 | 0.102 | ||
| Year | 58.5 | 10.7 | <0.001 | ||
| Procedure Mortality | Low Burden | -0.077 | 1.26 | 0.951 | 0.073 |
| Intermediate Burden | 0.194 | 1.10 | 0.861 | ||
| Hospital Complexity | -2.46 | 0.466 | <0.001 | ||
| Year | -0.0609 | 0.111 | 0.583 | ||
| Length of Stay | Low Burden | 2.11 | 0.626 | 0.0008 | 0.103 |
| Intermediate Burden | -0.948 | 0.549 | 0.0849 | ||
| Hospital Complexity | -0.941 | 0.232 | <0.001 | ||
| Year | 0.112 | 0.0552 | 0.0425 | ||
| Temporal Interactions | |||||
| Outcome | Term | Estimate | Std. Error | p-value | Adjusted RR2 |
| Procedure Mortality | Intermediate Burden | 0.170 | 0.665 | 0.798 | 0.0556 |
| Procedure Cost | Intermediate Burden | -50.39 | 62.42 | 0.420 | 0.107 |
| Length of Stay | Intermediate Burden | 0.5139 | 0.2953 | 0.0826 | 0.2729 |
| Sensitivity (Alternative Thresholds) | |||||
| Outcome | Term | Estimate | Std. Error | p-value | Adjusted RR2 |
| Cost | Low Burden | 256 | 144 | 0.0764 | 0.0703 |
| Mortality | Intermediate Burden | -2.92 | 0.952 | 0.0023 | 0.0939 |
| Length of Stay | Low Burden | 2.59 | 0.757 | 0.0007 | 0.0643 |
| Sensitivity (No Outliers) | |||||
| Outcome | Term | Estimate | Std. Error | p-value | Adjusted RR2 |
| Cost | Low Burden | 43.4 | 84.2 | 0.607 | 0.1040 |
| Mortality | Low Burden | 0.485 | 1.09 | 0.657 | 0.0494 |
| Length of Stay | Low Burden | 1.64 | 0.535 | 0.0024 | 0.0997 |
Table 3.
Correlations, Economic Impact, Power Analysis, and Diagnostic Statistics for Syphilis-Aneurysm Associations (2010–2024).
Table 3.
Correlations, Economic Impact, Power Analysis, and Diagnostic Statistics for Syphilis-Aneurysm Associations (2010–2024).
| Correlations (Pearson) | ||
|---|---|---|
| Metric | Value [95% CI] | p-value |
| Incidence vs. Syphilis Hospitalizations | 0.422 [0.338, 0.499] | <0.0001 |
| Syphilis Burden vs. Mortality | -0.051 [-0.147, 0.0469] | 0.308 |
| Correlations (Spearman) | ||
| Syphilis Burden vs. Mortality | -0.065 [-0.161, 0.033] | 0.192 |
| Syphilis Rate vs. Incidence | 0.542 [0.462, 0.614] | <0.0001 |
| Syphilis Rate vs. Mortality | -0.065 [-0.161, 0.033] | 0.192 |
| Length of Stay vs. Cost | 0.297 [0.204, 0.385] | <0.0001 |
| Economic Impact | ||
| Metric | Value [95% CI] | p-value |
| Total Cost (High) | R$17,706,806 | -- |
| Total Cost (Low) | R$1,853,377 | -- |
| Total Cost (Intermediate) | R$11,960,451 | -- |
| Cost Difference (High vs. Low) | -236.34 R$ [- 529.48, 56.80] | 0.6141 |
| Cost Difference (High vs. Intermediate) | -101.70 R$ [-398.54, 195.14] | 0.682 |
| Power Analysis | ||
| Metric | Value | p-value |
| Aneurysm Mortality Rate (d=-0.1) | 0.111 | -- |
| Length of Stay (d=-0.484) | 0.937 | -- |
| Average Hospitalization Cost (d=-0.064) | 0.075 | -- |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



