
Submitted:
11 October 2025
Posted:
14 October 2025
You are already at the latest version
Abstract
Background: Fluid overload (FO) is a frequent ICU complication and an important predictor of adverse outcomes. While classically attributed to resuscitative fluids, recent data emphasize the contribution of non-therapeutic “fluid creep” from medication diluents and carrier infusions. This study examined associations between fluid creep, FO, acute kidney injury (AKI), and mortality, and explored the predictive value of the modified Renal Angina Index (mRAI) for early AKI risk stratification; Methods: A retrospective cohort of 250 critically ill adults (ICU stay ≥72 h) admitted to a mixed medical–surgical ICU between May 2021 and November 2024 was analyzed. All fluids administered during the first 72 h were categorized and indexed to ideal body weight. Fluid creep included drug diluents, carriers, and flushes. FO% was calculated as [(Cumulative Fluid Balance)/IBW] × 100; Results: Fluid creep was higher in non-survivors (5,183 ± 2,541 vs. 4,354 ± 2,171 mL; p = 0.008) and correlated with FO, cumulative balance, and total input (r = 0.41–0.43; p < 0.001). Creep and FO independently predicted ICU mortality. Abnormal mRAI scores were associated with FO and early AKI; Conclusions: Fluid creep and FO were independent mortality predictors. Routine monitoring and minimization of creep, along with structured de-resuscitation protocols, may improve outcomes in critically ill adults.
Keywords:
fluid overload
; fluid creep
; acute kidney injury
; critical care
; renal angina index
; mortality
; de-resuscitation
1. Introduction
Intravenous fluid therapy is both lifesaving and potentially harmful in critical illness. While essential for restoring hemodynamic stability, excessive administration predisposes patients to fluid overload (FO)—commonly defined as a >10% increase in body weight—which is consistently associated with impaired oxygenation, organ dysfunction, prolonged ICU stay, and increased mortality [1,2,3].
Most studies have focused on total fluid balance without distinguishing between categories of fluid exposure [4]. Increasing evidence highlights the contribution of fluid creep—unintended fluids from drug diluents, carrier solutions, and catheter flushes [5]. Although FO is a well-established risk factor for acute kidney injury (AKI) [6] and prolonged mechanical ventilation [5,7,8], the independent role of fluid creep remains insufficiently defined.
Early identification of patients at risk for AKI is equally important to guide fluid management. The modified Renal Angina Index (mRAI), adapted from pediatric populations, integrates baseline risk factors and early markers of kidney injury into a composite score, improving prediction of severe AKI (9). Coupling such risk stratification with structured fluid stewardship—the systematic monitoring, rationalization, and reduction of unnecessary fluid exposure—may be critical to mitigating iatrogenic harm from hidden fluid burden.
Pediatric and experimental studies suggest that fluid creep may constitute 30–60% of daily intake and substantially increase sodium and chloride burden [10,11]. In adults, non-resuscitative fluids can account for up to 42% of intake during the first three ICU days, and minimizing their use has been associated with reduced FO [12,13]. One large adult study found fluid creep and maintenance fluids to be the predominant contributors to early fluid intake, particularly among mechanically ventilated patients [14]. Despite these signals, the prognostic relevance of fluid creep, independent of total fluid balance, has not been systematically evaluated [15,16].
To address these gaps, we investigated early fluid administration patterns and their associations with fluid overload FO and mortality in critically ill adults, with particular focus on fluid creep as a distinct, potentially modifiable contributor to hidden fluid burden. Exploratory analyses also assessed the predictive value of the modified Renal Angina Index (mRAI) for early AKI risk stratification and FO.
2. Materials and Methods
Study Design and Setting
This retrospective observational cohort study was conducted in the mixed medical–surgical ICU of the University General Hospital of Heraklion, a tertiary academic center in Greece. All adult patients admitted between May 1, 2021, and November 30, 2024, were screened for eligibility. The study was approved by the institutional review board (ID 17747/26-05-2023; 21549/18-10-2024), with informed consent waived owing to its retrospective design. All procedures adhered to the Declaration of Helsinki and institutional research guidelines.
Patient Selection
Eligible participants were adults (≥18 and ≤80 years) with an ICU stay of ≥72 hours. Exclusion criteria were pre-existing chronic kidney disease, heart failure requiring fluid restriction, palliative care admission, or incomplete data (e.g., missing admission creatinine).
Data Collection
Data were extracted from electronic health records, including: Demographics: age, sex, body weight, and height (used to calculate ideal body weight [IBW] for normalization across sex and BMI categories). Admission characteristics: primary diagnosis, comorbidities, admission type (medical/ surgical). Severity indices: APACHE II, SOFA, modified Renal Angina Index (mRAI), KDIGO stage. Laboratory/clinical data: admission and daily measurements for 72 hours. Interventions: mechanical ventilation, vasopressors, CRRT, nephrotoxic/contrast exposure.
Fluid Data
All fluids administered during the first 72 hours were quantified and indexed to IBW. Categories included: fluid creep (drug diluents, carrier infusions, flushes), maintenance, resuscitation (≥10 mL/kg crystalloids), replacement, nutrition, and blood products. Solutions were classified as balanced crystalloids or 0.9% sodium chloride (NS). Medication concentrations were maximized per protocol to reduce fluid burden. Fluid balance was calculated daily and cumulatively as: Fluid Balance (L) = Total Input (L) – Total Output (L). Fluid overload percentage (FO%) was defined using the formula: FO% = [(Cumulative Fluid Balance in L) / IBW in kg] × 100. FO >10% of IBW defined clinically significant FO, and FO >15% defined severe FO.
Acute Kidney Injury and mRAI
AKI was defined using KDIGO criteria, with severe AKI defined as stage ≥2 at admission or on day 3. Renal function was monitored daily (serum creatinine, urea, estimated creatinine clearance). The mRAI was calculated within 12 hours of admission by multiplying risk and injury domains [17,18]. A score ≥6 indicated high risk for severe AKI. A schematic of the scoring system is provided in Figure S1.
Statistical Analysis
Analyses were performed with SPSS v30 (IBM, Armonk, NY). Continuous variables were tested for normality (Shapiro–Wilk) and expressed as mean ± SD or median (IQR). Categorical variables were reported as n (%). Between-group comparisons used ANOVA or Kruskal–Wallis tests for continuous variables and chi-square or Fisher’s exact tests for categorical variables. Correlations were assessed with Pearson’s coefficient. Predictive performance of fluid creep, input, FO%, and fluid balance for ICU mortality was evaluated using ROC analysis. Multivariable logistic regression (backward stepwise) was used to identify independent predictors of ICU mortality, FO >10%, and severe AKI. Variables with p <0.10 in univariate analysis entered the model; significance was set at p <0.05..
3. Results
Demographic and Clinical Characteristics
Between May 2021 and November 2024, 2,000 patients were admitted to the ICU. After exclusions, 250 patients had complete datasets (Figure S2). Of these, 160 (64%) were male and 90 (36%) female, with a mean age of 64.8 ± 17 years, body weight 80.1 ± 17 kg, BMI 28.2 ± 5.6, and admission APACHE II score 21.9 ± 7.8. Mean ICU and hospital stays were 15.1 ± 16 and 35.6 ± 31 days, respectively (Table 1).
Non-survivors had lower body weight (p = 0.006), higher SOFA scores (p = 0.032), lower GCS (p = 0.049), and were more often admitted for medical indications (72.2% vs. 56.7%, p = 0.020). ICU-acquired infections and infections at admission were also more common in non-survivors (both p <0.05). ICU mortality was 20%; mortality among enrolled patients was 31.6%, and hospital mortality was 47.8%. Non-survivors required more vasoactive days (p <0.001) and had higher rates of mechanical ventilation and vasopressor use (both p <0.001).
Laboratory Findings
On day 3, non-survivors had lower pH (p = 0.042), bicarbonate (p = 0.009), base excess (p = 0.040), and PaO₂ (p = 0.025), with persistently higher lactate from day 2 onward (p <0.001) (Table S1). Longitudinally, sodium, chloride, and potassium increased (all p <0.001), while glucose and lactate declined in survivors (p <0.001). Arterial blood gases improved from day 1 except for PaO₂, which decreased (p <0.001). Sodium and chloride were not associated with fluid creep, FO%, input, creatinine clearance, or outcomes.
Acute Kidney Injury
At admission, 24.5% had KDIGO stage 2 and 26.6% stage 3 AKI. By day 3, severe AKI (KDIGO ≥2) decreased among survivors (14.6%) but rose in non-survivors (27.7%, p = 0.011). By day 7, the gap widened (12.8% vs. 32.0%, p <0.001) (Table 2). Creatinine clearance improved in survivors (p <0.001) but not in non-survivors. CRRT use was higher among non-survivors (34.2% vs. 14.8%, p <0.001). Nephrotoxic drug and diuretic exposure did not differ.
Abnormal mRAI (≥6) within 12 h was more common in ICU non-survivors (32.9% vs. 21.1%, p = 0.044) and hospital non-survivors (31.9% vs. 18.5%, p = 0.014). mRAI independently predicted severe AKI in medical (OR 0.93, 95% CI 0.87–0.99, p = 0.032) and emergency patients (OR 0.94, 95% CI 0.88–0.99, p = 0.023).
Categories of Administered Fluids
Pre-ICU
Among 73 patients with data, mean intake was 1,589 ± 1,351 mL crystalloids (25 ± 22 mL/kg IBW) and 957 ± 123 mL blood products/albumin (15 ± 14 mL/kg IBW), with no subgroup differences.
ICU Days 1–3
During the first three ICU days, fluid creep and maintenance fluids each contributed >40% of total intake, while resuscitation and replacement accounted for ~14% and nutrition/blood products ~5% (Table S2, Figure S3). Indexed to IBW, boluses, resuscitation fluids, albumin, and blood products decreased over time, whereas maintenance, creep, and nutrition increased (Table S3).
Cumulative fluid creep was higher in non-survivors (5,183 ± 2,541 vs. 4,354 ± 2,171 mL, p = 0.008), a difference persisting when nutrition and blood products were included (“fluid creep plus”: 6,342 ± 3,044 vs. 5,158 ± 2,565 mL, p = 0.002; Table S4). Among input categories, antibiotic diluents (day 2), vasoactive infusions (days 2–3), blood products (day 3), and enteral nutrition (day 1) were significantly higher in non-survivors (all p < 0.05) (Figure 1A). Other intake categories did not differ; therefore, overall input was greater in non-survivors (p = 0.002). Daily and cumulative output volumes were lower in non-survivors, though differences did not reach significance (Figure 1B).
Fluid Types
Before ICU, PlasmaLyte and Ringer’s Lactate predominated. During ICU stay, boluses were mostly NS (56–62% day 1, 80–90% days 2–3). Maintenance fluids were largely Ringer’s Lactate with 5–20% D/W. Creep consisted mainly of NS, D/W 5%, and sterile water, used as diluents. Overall composition (~50% balanced crystalloids, 25% NS, 25% D/W/nutrition/blood products) did not differ between survivors and non-survivors..
Fluid Overload
By day 3, clinically significant FO (>10%) and severe FO (>15%) were both significantly more frequent in non-survivors (34.2% and 15.2%, respectively; both p < 0.001) (Table 3). Non-survivors also had higher cumulative fluid creep, input, and positive balances.
Cumulative fluid creep correlated with FO (r = 0.41, p < 0.001), balance (r = 0.41, p < 0.001), and input (r = 0.43, p < 0.001), and more weakly with output (r = 0.17, p = 0.006) (Figure 2). It was also associated with longer ICU stay, prolonged mechanical ventilation, and increased vasoactive days (all p < 0.001).
In logistic regression, only APACHE II (OR 1.14, 95% CI 1.06–1.22, p < 0.001), mRAI (OR 1.08, 95% CI 1.03–1.14, p = 0.004), cumulative fluid creep (OR 1.04, 95% CI 1.02–1.06, p < 0.001), and maintenance fluid volume (OR 1.03, 95% CI 1.01–1.05, p = 0.005) independently predicted FO >10%. For FO >15%, the same predictors remained significant except for maintenance.
Outcomes
Multivariable regression identified cumulative fluid creep (OR 1.02, 95% CI 1.01–1.03, p = 0.012) and FO (OR 1.06, 95% CI 1.007–1.13, p = 0.028) as independent predictors of ICU mortality, whereas APACHE II, SOFA, KDIGO, and mRAI were not.
4. Discussion
In this retrospective adult ICU cohort, early fluid creep—unintended fluids from drug diluents, carrier solutions, and catheter flushes—was independently associated with FO and ICU mortality, even after adjusting for illness severity, conventional fluid categories, and early AKI markers. Fluid creep also correlated with prolonged mechanical ventilation, vasoactive support, and ICU length of stay, supporting a pathophysiologic role of hidden fluid burden in promoting interstitial edema and organ dysfunction.
These findings align with prior reports showing that maintenance fluids and fluid creep often exceed resuscitative boluses in their contribution to daily fluid, sodium, and chloride loads. In pediatric cohorts, higher intake—rather than reduced output—was the main driver of FO, which was associated with longer ICU stay, higher AKI incidence, fewer ventilator-free days, and increased mortality [2,19,20,21]. In a large mixed ICU cohort, creep accounted for ~33% of daily intake—fivefold greater than resuscitation fluids—and was a major source of electrolyte burden [22,23]. Likewise, among patients receiving respiratory support, fluid creep represented ~25% of intake within 24 hours and persisted in those with severe hypoxemia [14]. Our results extend these observations by demonstrating that fluid creep is not only common but also prognostically relevant in critically ill adults.
In our analysis, cumulative fluid creep independently predicted clinically significant FO (>10%) and severe FO (>15%), both of which were associated with mortality. Notably, both fluid creep and FO independently predicted ICU death. These findings highlight fluid creep as a modifiable early exposure, reinforcing the rationale for targeted interventions such as optimizing drug concentrations, minimizing carrier volumes, and preferentially using balanced diluents [24]. The SALT-ED and SMART trials support this biological plausibility, demonstrating reduced kidney injury with balanced fluids compared with saline [25]. Moreover, structured fluid stewardship—progressing through resuscitation, optimization, stabilization, and de-escalation phases—provides a framework to individualize volume targets, prevent FO, and improve outcomes [26].
Consistent with broader ICU evidence, FO in our study was associated with impaired creatinine clearance and greater CRRT use among non-survivors [27,28]. Importantly, abnormal mRAI scores within 12 h were more frequent in non-survivors and independently predicted severe AKI in medical and emergency subgroups. This supports prior validation studies demonstrating that mRAI outperforms serum creatinine change alone in identifying patients at risk for AKI progression [9,28,29]. While exploratory, our findings support incorporating mRAI into fluid stewardship to identify high-risk patients in whom limiting creep and maintenance may be most beneficial [17,30].
Fluid composition also matters. A meta-analysis of five ICU studies (n=1,105) found that balanced crystalloids, when used for creep and maintenance, significantly reduced daily sodium burden compared with saline [31]. Similarly, a prospective before–after study showed that substituting 5% glucose for maintenance and diluent fluids halved daily sodium load and lowered daily fluid balance [32]. In our cohort, predominant use of balanced crystalloids maintained acid–base homeostasis and preserved normal sodium and chloride levels, with no association between electrolyte trends and outcomes. In line with this, a randomized controlled trial found higher chloride concentrations with saline compared with balanced crystalloids (111 vs. 108 mmol/L) but no difference in AKI or mortality [33]. A recent systematic review, however, suggested that balanced crystalloids probably reduce 90-day mortality compared with saline, underscoring the importance of fluid type even in hidden sources such as diluents [34].
From a clinical perspective, our results argue for explicit accounting of fluid creep in early ICU care and its incorporation into fluid stewardship bundles. Practical measures include daily reporting of creep volumes, use of concentrated infusions, balanced diluents when compatible, and integration with the “four D’s” (drug, dosing, duration, de-escalation) [35,36,37]. Equally important, structured deresuscitation protocols—emphasizing active fluid removal with diuretics or timely initiation of renal replacement therapy—are a complementary step to prevent progression from clinically significant to severe FO and thereby reduce morbidity and mortality [38,39,40]. Although our ROC analyses showed only modest discrimination (AUC 0.62–0.67), creep- and FO-related variables may still function as operational triggers to reassess volume status, initiate deresuscitation, or minimize creep exposure, rather than as strict prognostic thresholds.
This study systematically disaggregated fluid categories indexed to IBW, evaluated early exposures, and linked creep to patient-centered outcomes while adjusting for illness severity and early AKI indices [41]. Limitations include its retrospective, single-center design, potential residual confounding from illness severity and medication burden, and restricted ability to evaluate the impact of fluid type. Granular data on pre-ICU fluid administration were unavailable, which may have influenced early balances. Finally, mRAI analyses were exploratory, not powered for mortality prediction, and ROC performance was modest.
5. Conclusions
Fluid creep is an underrecognized but modifiable driver of fluid overload and ICU mortality. Incorporating its measurement and reduction into fluid stewardship programs offers a pragmatic strategy to minimize unintended harm. Prospective trials—testing concentration protocols, balanced diluents, and automated monitoring—are warranted to determine whether reducing hidden fluid exposure can improve outcomes in critically ill patients.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1 (Supplement): Modified Renal Angina Index (mRAI). The mRAI was calculated 12 hours after ICU admission as the product of risk and injury domains. The creatinine score was defined as the difference between serum creatinine at ICU admission and the most recent value within the preceding 3 days. An mRAI score ≥6 indicated high risk for acute kidney injury (AKI); Figure S2 (Supplement): Flowchart of patient screening, exclusions, and final study cohort, according to STROBE recommendations; Table S1: Laboratory Tests During the First Three Days of ICU Stay; Table S2: Distribution of daily fluid intake categories stratified by outcome category; Table S3: Distribution of daily fluid intake indexed by ideal body weight (IBW), stratified by outcome category; Figure S3 (Supplement): Distribution of cumulative fluid input categories by ICU day 3, indexed to IBW. Fluid creep and maintenance fluids each accounted for >40% of total intake, whereas resuscitation, replacement, and nutrition/blood products contributed smaller proportions; Table S4: Distribution of cumulative fluid categories by outcome category: Table S5: Predictive ability of cumulative fluid variables by day 3, indexed to ideal body weight (IBW) for ICU mortality, based on ROC analysis.
Author Contributions
Conceptualization, GB, SI, and EK.; methodology, GB and SI.; software, GB and SI.; validation, GB and SI.; formal analysis, TA and IV.; investigation, TA and IV.; resources, TA and IV.; data curation, GB and SI.; writing—original draft preparation, GB.; writing—review and editing, GB, TA, IV, and SI; visualization, EK.; supervision, GB and SI.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the University Hospital of Heraklion, Crete (ID 17747/26-05-2023; 21549/18-10-2024).
Informed Consent Statement
Patient consent was waived due to its retrospective design.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The Special Account for Research Funds of the University of Crete (KA 3650) supported publication fees.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AKI | Acute Kidney Injury |
| FO | Fluid Overload |
| ICU | Intensive Care Unit |
| mRAI | modified Renal Angina Index |
| IBM | Ideal Body Weight |
References
- Alobaidi, R.; Morgan, C.; Basu, R.K.; Stenson, E.; Featherstone, R.; Majumdar, S.R.; Bagshaw, S.M. Association Between Fluid Balance and Outcomes in Critically Ill Children: A Systematic Review and Meta-Analysis. JAMA Pediatr 2018, 172, 257–268. [CrossRef]
- Lintz, V.C.; Vieira, R.A.; Carioca, F. de L.; Ferraz, I. de S.; Silva, H.M.; Ventura, A.M.C.; de Souza, D.C.; Brandão, M.B.; Nogueira, R.J.N.; de Souza, T.H. Fluid Accumulation in Critically Ill Children: A Systematic Review and Meta-Analysis. EClinicalMedicine 2024, 74, 102714. [CrossRef]
- Renaudier, M.; Lascarrou, J.-B.; Chelly, J.; Lesieur, O.; Bourenne, J.; Jaubert, P.; Paul, M.; Muller, G.; Leprovost, P.; Klein, T.; et al. Fluid Balance and Outcome in Cardiac Arrest Patients Admitted to Intensive Care Unit. Crit Care 2025, 29, 152. [CrossRef]
- Pfortmueller, C.A.; Dabrowski, W.; Wise, R.; van Regenmortel, N.; Malbrain, M.L.N.G. Fluid Accumulation Syndrome in Sepsis and Septic Shock: Pathophysiology, Relevance and Treatment-a Comprehensive Review. Ann Intensive Care 2024, 14, 115. [CrossRef]
- Sharif, S.; Flindall, H.; Basmaji, J.; Ablordeppey, E.; Díaz-Gómez, J.L.; Lanspa, M.; Nikravan, S.; Piticaru, J.; Lewis, K. Critical Care Ultrasonography for Volume Management: A Systematic Review, Meta-Analysis, and Trial Sequential Analysis of Randomized Trials. Crit Care Explor 2025, 7, e1261. [CrossRef]
- Woodward, C.W.; Lambert, J.; Ortiz-Soriano, V.; Li, Y.; Ruiz-Conejo, M.; Bissell, B.D.; Kelly, A.; Adams, P.; Yessayan, L.; Morris, P.E.; et al. Fluid Overload Associates With Major Adverse Kidney Events in Critically Ill Patients With Acute Kidney Injury Requiring Continuous Renal Replacement Therapy. Crit Care Med 2019, 47, e753–e760. [CrossRef]
- Vignon, P.; Evrard, B.; Asfar, P.; Busana, M.; Calfee, C.S.; Coppola, S.; Demiselle, J.; Geri, G.; Jozwiak, M.; Martin, G.S.; et al. Fluid Administration and Monitoring in ARDS: Which Management? Intensive Care Med 2020, 46, 2252–2264. [CrossRef]
- Charaya, S.; Angurana, S.K.; Nallasamy, K.; Jayashree, M. Restricted versus Usual/Liberal Maintenance Fluid Strategy in Mechanically Ventilated Children: An Open-Label Randomized Trial (ReLiSCh Trial). Indian J Pediatr 2025, 92, 7–14. [CrossRef]
- Ortiz-Soriano, V.; Kabir, S.; Claure-Del Granado, R.; Stromberg, A.; Toto, R.D.; Moe, O.W.; Goldstein, S.L.; Neyra, J.A. Assessment of a Modified Renal Angina Index for AKI Prediction in Critically Ill Adults. Nephrol Dial Transplant 2022, 37, 895–903. [CrossRef]
- Langer, T.; D’Oria, V.; Spolidoro, G.C.I.; Chidini, G.; Scalia Catenacci, S.; Marchesi, T.; Guerrini, M.; Cislaghi, A.; Agostoni, C.; Pesenti, A.; et al. Fluid Therapy in Mechanically Ventilated Critically Ill Children: The Sodium, Chloride and Water Burden of Fluid Creep. BMC Pediatr 2020, 20, 424. [CrossRef]
- Van Regenmortel, N.; Verbrugghe, W.; Roelant, E.; Van den Wyngaert, T.; Jorens, P.G. Maintenance Fluid Therapy and Fluid Creep Impose More Significant Fluid, Sodium, and Chloride Burdens than Resuscitation Fluids in Critically Ill Patients: A Retrospective Study in a Tertiary Mixed ICU Population. Intensive Care Med 2018, 44, 409–417. [CrossRef]
- Messmer, A.; Pietsch, U.; Siegemund, M.; Buehler, P.; Waskowski, J.; Müller, M.; Uehlinger, D.E.; Hollinger, A.; Filipovic, M.; Berger, D.; et al. Protocolised Early De-Resuscitation in Septic Shock (REDUCE): Protocol for a Randomised Controlled Multicentre Feasibility Trial. BMJ Open 2023, 13, e074847. [CrossRef]
- Gamble, K.C.; Smith, S.E.; Bland, C.M.; Sikora Newsome, A.; Branan, T.N.; Hawkins, W.A. Hidden Fluids in Plain Sight: Identifying Intravenous Medication Classes as Contributors to Intensive Care Unit Fluid Intake. Hosp Pharm 2022, 57, 230–236. [CrossRef]
- Sakuraya, M.; Yoshihiro, S.; Onozuka, K.; Takaba, A.; Yasuda, H.; Shime, N.; Kotani, Y.; Kishihara, Y.; Kondo, N.; Sekine, K.; et al. A Burden of Fluid, Sodium, and Chloride Due to Intravenous Fluid Therapy in Patients with Respiratory Support: A Post-Hoc Analysis of a Multicenter Cohort Study. Ann Intensive Care 2022, 12, 100. [CrossRef]
- Bihari, S.; Prakash, S.; Potts, S.; Matheson, E.; Bersten, A.D. Addressing the Inadvertent Sodium and Chloride Burden in Critically Ill Patients: A Prospective before-and-after Study in a Tertiary Mixed Intensive Care Unit Population. Crit Care Resusc 2018, 20, 285–293.
- Van Regenmortel, N.; Moers, L.; Langer, T.; Roelant, E.; De Weerdt, T.; Caironi, P.; Malbrain, M.L.N.G.; Elbers, P.; Van den Wyngaert, T.; Jorens, P.G. Fluid-Induced Harm in the Hospital: Look beyond Volume and Start Considering Sodium. From Physiology towards Recommendations for Daily Practice in Hospitalized Adults. Ann Intensive Care 2021, 11, 79. [CrossRef]
- Matsuura, R.; Srisawat, N.; Claure-Del Granado, R.; Doi, K.; Yoshida, T.; Nangaku, M.; Noiri, E. Use of the Renal Angina Index in Determining Acute Kidney Injury. Kidney Int Rep 2018, 3, 677–683. [CrossRef]
- Basu, R.K.; Kaddourah, A.; Goldstein, S.L.; AWARE Study Investigators Assessment of a Renal Angina Index for Prediction of Severe Acute Kidney Injury in Critically Ill Children: A Multicentre, Multinational, Prospective Observational Study. Lancet Child Adolesc Health 2018, 2, 112–120. [CrossRef]
- Mohoric, S.; Alobaidi, R.; McGraw, T.; Joffe, A.R. The Determinants of Fluid Accumulation in Critically Ill Children: A Prospective Single-Center Cohort Study. Pediatr Nephrol 2025. [CrossRef]
- Rajendran, A.; Bamne, P.; Upadhyay, N.; Pandwar, U.; Shrivastava, J. Impact of Fluid Overload on Mortality Among Critically Ill Pediatric Patients: An Observational Study at a Tertiary Care Hospital in Central India. Cureus 2025, 17, e82178. [CrossRef]
- Rao, S.B.; Akhondi-Asl, A.; Mehta, N.; Yang, Y. Association between Early Fluid Overload and Clinical Outcomes in a Pediatric ICU. Pediatr Res 2025. [CrossRef]
- Van Regenmortel, N.; Verbrugghe, W.; Roelant, E.; Van den Wyngaert, T.; Jorens, P.G. Maintenance Fluid Therapy and Fluid Creep Impose More Significant Fluid, Sodium, and Chloride Burdens than Resuscitation Fluids in Critically Ill Patients: A Retrospective Study in a Tertiary Mixed ICU Population. Intensive Care Med 2018, 44, 409–417. [CrossRef]
- Molin, C.; Wichmann, S.; Schønemann-Lund, M.; Møller, M.H.; Bestle, M.H. Sodium and Chloride Disturbances in Critically Ill Adult Patients: A Protocol for a Sub-Study of the FLUID-ICU Cohort Study. Acta Anaesthesiol Scand 2025, 69, e70028. [CrossRef]
- Gamble, K.C.; Smith, S.E.; Bland, C.M.; Sikora Newsome, A.; Branan, T.N.; Hawkins, W.A. Hidden Fluids in Plain Sight: Identifying Intravenous Medication Classes as Contributors to Intensive Care Unit Fluid Intake. Hosp Pharm 2022, 57, 230–236. [CrossRef]
- Self, W.H.; Semler, M.W.; Wanderer, J.P.; Wang, L.; Byrne, D.W.; Collins, S.P.; Slovis, C.M.; Lindsell, C.J.; Ehrenfeld, J.M.; Siew, E.D.; et al. Balanced Crystalloids versus Saline in Noncritically Ill Adults. N Engl J Med 2018, 378, 819–828. [CrossRef]
- Messina, A.; Matronola, G.M.; Cecconi, M. Individualized Fluid Optimization and De-Escalation in Critically Ill Patients with Septic Shock. Curr Opin Crit Care 2025. [CrossRef]
- Bouchard, J.; Soroko, S.B.; Chertow, G.M.; Himmelfarb, J.; Ikizler, T.A.; Paganini, E.P.; Mehta, R.L.; Program to Improve Care in Acute Renal Disease (PICARD) Study Group Fluid Accumulation, Survival and Recovery of Kidney Function in Critically Ill Patients with Acute Kidney Injury. Kidney Int 2009, 76, 422–427. [CrossRef]
- Wang, N.; Jiang, L.; Zhu, B.; Wen, Y.; Xi, X.-M.; Beijing Acute Kidney Injury Trial (BAKIT) Workgroup Fluid Balance and Mortality in Critically Ill Patients with Acute Kidney Injury: A Multicenter Prospective Epidemiological Study. Crit Care 2015, 19, 371. [CrossRef]
- Bouchard, J.; Soroko, S.B.; Chertow, G.M.; Himmelfarb, J.; Ikizler, T.A.; Paganini, E.P.; Mehta, R.L.; Program to Improve Care in Acute Renal Disease (PICARD) Study Group Fluid Accumulation, Survival and Recovery of Kidney Function in Critically Ill Patients with Acute Kidney Injury. Kidney Int 2009, 76, 422–427. [CrossRef]
- Sakaguchi, E.; Naruse, H.; Ishihara, Y.; Hattori, H.; Yamada, A.; Kawai, H.; Muramatsu, T.; Tsuboi, Y.; Fujii, R.; Suzuki, K.; et al. Assessment of the Renal Angina Index in Patients Hospitalized in a Cardiac Intensive Care Unit. Sci Rep 2024, 14, 75. [CrossRef]
- Waskowski, J.; Salvato, S.M.; Müller, M.; Hofer, D.; van Regenmortel, N.; Pfortmueller, C.A. Choice of Creep or Maintenance Fluid Type and Their Impact on Total Daily ICU Sodium Burden in Critically Ill Patients: A Systematic Review and Meta-Analysis. J Crit Care 2023, 78, 154403. [CrossRef]
- Bihari, S.; Prakash, S.; Potts, S.; Matheson, E.; Bersten, A.D. Addressing the Inadvertent Sodium and Chloride Burden in Critically Ill Patients: A Prospective before-and-after Study in a Tertiary Mixed Intensive Care Unit Population. Crit Care Resusc 2018, 20, 285–293.
- Verma, B.; Luethi, N.; Cioccari, L.; Lloyd-Donald, P.; Crisman, M.; Eastwood, G.; Orford, N.; French, C.; Bellomo, R.; Martensson, J. A Multicentre Randomised Controlled Pilot Study of Fluid Resuscitation with Saline or Plasma-Lyte 148 in Critically Ill Patients. Crit Care Resusc 2016, 18, 205–212.
- Hammond, N.E.; Zampieri, F.G.; Di Tanna, G.L.; Garside, T.; Adigbli, D.; Cavalcanti, A.B.; Machado, F.R.; Micallef, S.; Myburgh, J.; Ramanan, M.; et al. Balanced Crystalloids versus Saline in Critically Ill Adults - A Systematic Review with Meta-Analysis. NEJM Evid 2022, 1, EVIDoa2100010. [CrossRef]
- Malbrain, M.L.N.G.; Van Regenmortel, N.; Saugel, B.; De Tavernier, B.; Van Gaal, P.-J.; Joannes-Boyau, O.; Teboul, J.-L.; Rice, T.W.; Mythen, M.; Monnet, X. Principles of Fluid Management and Stewardship in Septic Shock: It Is Time to Consider the Four D’s and the Four Phases of Fluid Therapy. Ann Intensive Care 2018, 8, 66. [CrossRef]
- Malbrain, M.L.N.G.; Van Regenmortel, N.; Saugel, B.; De Tavernier, B.; Van Gaal, P.-J.; Joannes-Boyau, O.; Teboul, J.-L.; Rice, T.W.; Mythen, M.; Monnet, X. Principles of Fluid Management and Stewardship in Septic Shock: It Is Time to Consider the Four D’s and the Four Phases of Fluid Therapy. Ann Intensive Care 2018, 8, 66. [CrossRef]
- Malbrain, M.L.N.G.; Martin, G.; Ostermann, M. Everything You Need to Know about Deresuscitation. Intensive Care Med 2022, 48, 1781–1786. [CrossRef]
- Gist, K.M.; Selewski, D.T.; Brinton, J.; Menon, S.; Goldstein, S.L.; Basu, R.K. Assessment of the Independent and Synergistic Effects of Fluid Overload and Acute Kidney Injury on Outcomes of Critically Ill Children. Pediatr Crit Care Med 2020, 21, 170–177. [CrossRef]
- Vaara, S.T.; Korhonen, A.-M.; Kaukonen, K.-M.; Nisula, S.; Inkinen, O.; Hoppu, S.; Laurila, J.J.; Mildh, L.; Reinikainen, M.; Lund, V.; et al. Fluid Overload Is Associated with an Increased Risk for 90-Day Mortality in Critically Ill Patients with Renal Replacement Therapy: Data from the Prospective FINNAKI Study. Crit Care 2012, 16, R197. [CrossRef]
- Liu, C.; Lu, G.; Wang, D.; Lei, Y.; Mao, Z.; Hu, P.; Hu, J.; Liu, R.; Han, D.; Zhou, F. Balanced Crystalloids versus Normal Saline for Fluid Resuscitation in Critically Ill Patients: A Systematic Review and Meta-Analysis with Trial Sequential Analysis. Am J Emerg Med 2019, 37, 2072–2078. [CrossRef]
- Van Regenmortel, N.; Verbrugghe, W.; Roelant, E.; Van den Wyngaert, T.; Jorens, P.G. Maintenance Fluid Therapy and Fluid Creep Impose More Significant Fluid, Sodium, and Chloride Burdens than Resuscitation Fluids in Critically Ill Patients: A Retrospective Study in a Tertiary Mixed ICU Population. Intensive Care Med 2018, 44, 409–417. [CrossRef]
Figure 1.
Distribution of daily (A) fluid input and (B) fluid output by category through ICU day 3, indexed to ideal body weight (IBW) and stratified by survival status. Non-survivors received higher proportions of fluid creep, blood products (day 3), and enteral nutrition (day 1), and demonstrated lower effective output. *p < 0.05.
Figure 1.
Distribution of daily (A) fluid input and (B) fluid output by category through ICU day 3, indexed to ideal body weight (IBW) and stratified by survival status. Non-survivors received higher proportions of fluid creep, blood products (day 3), and enteral nutrition (day 1), and demonstrated lower effective output. *p < 0.05.
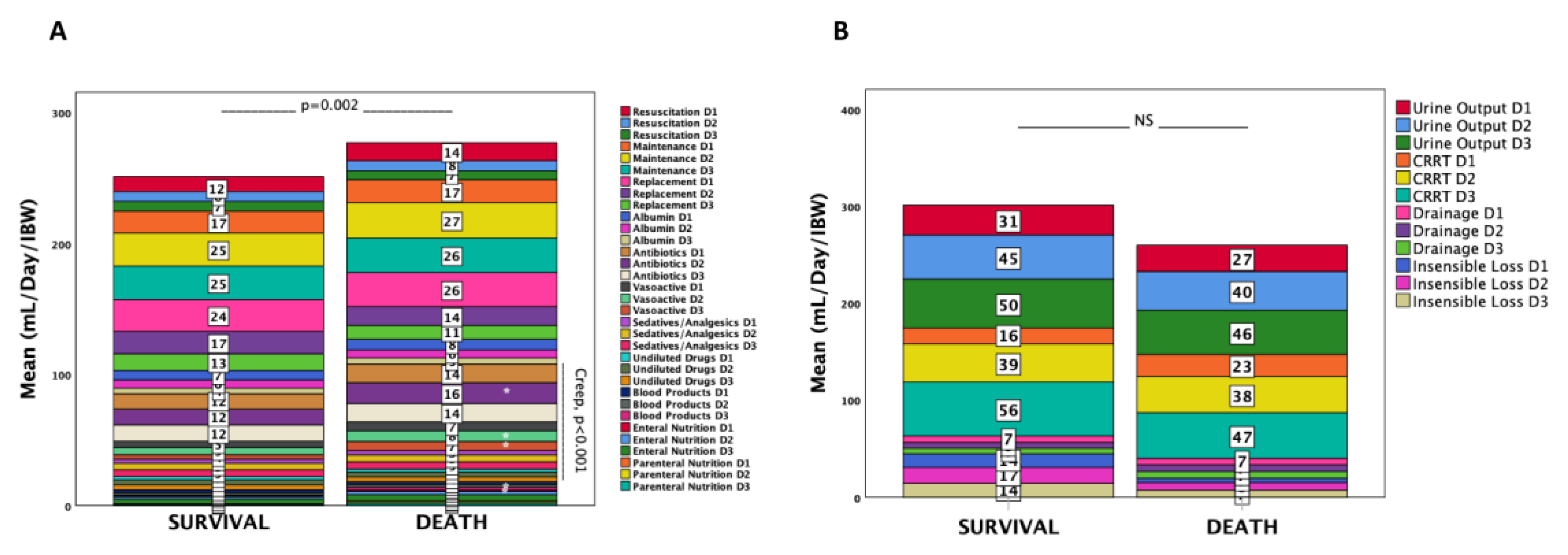
Figure 2.
Correlation of cumulative fluid creep with (A) total input and (B) fluid balance through ICU day 3, both indexed to IBW. Fluid creep correlated strongly with intake and fluid balance and more weakly with output, underscoring its role in fluid accumulation.
Figure 2.
Correlation of cumulative fluid creep with (A) total input and (B) fluid balance through ICU day 3, both indexed to IBW. Fluid creep correlated strongly with intake and fluid balance and more weakly with output, underscoring its role in fluid accumulation.
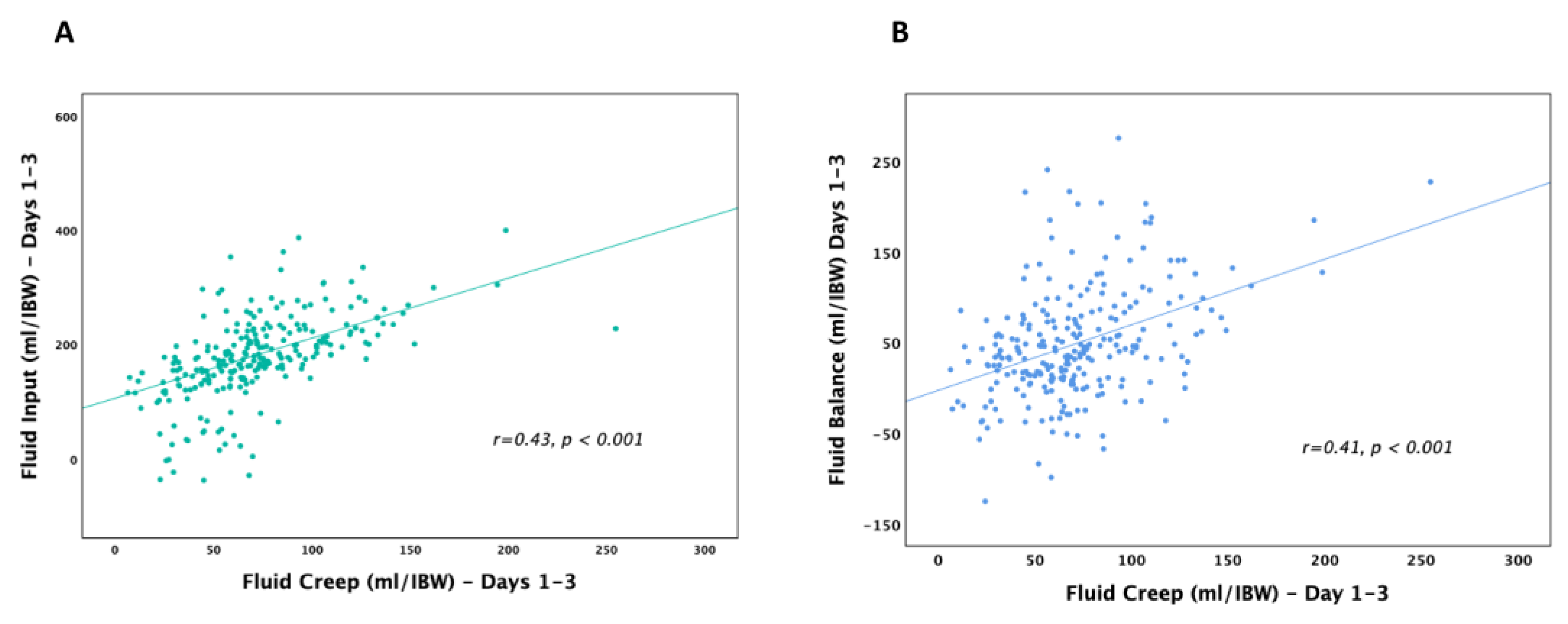
Figure 3.
Receiver operating characteristic (ROC) curves for cumulative fluid indices indexed to IBW in predicting ICU mortality. Total input, FO%, fluid balance, maintenance fluids, and cumulative fluid creep showed modest but significant discriminatory ability.
Figure 3.
Receiver operating characteristic (ROC) curves for cumulative fluid indices indexed to IBW in predicting ICU mortality. Total input, FO%, fluid balance, maintenance fluids, and cumulative fluid creep showed modest but significant discriminatory ability.
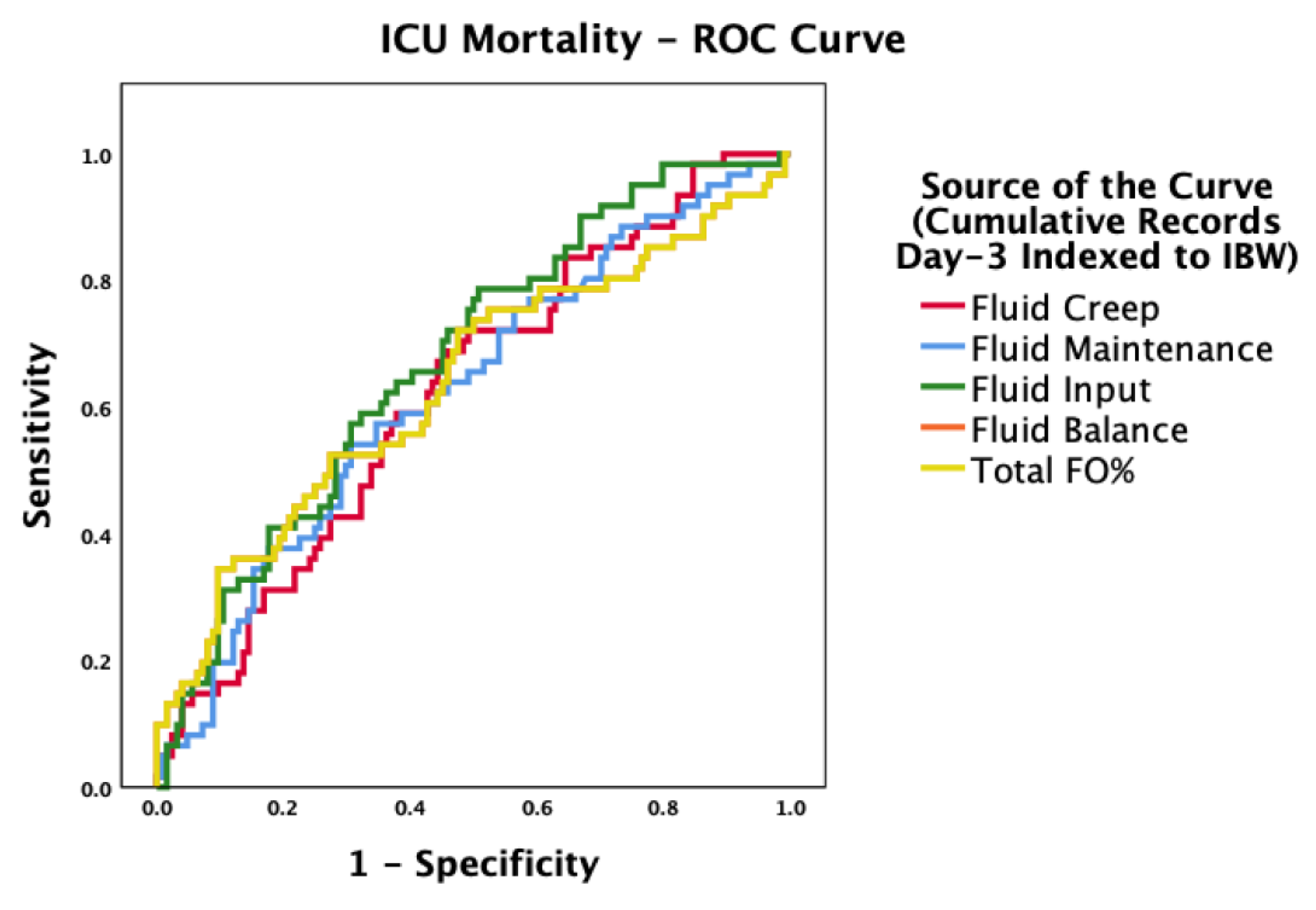

Table 1.
Demographic and clinical characteristics of the study population stratified by survival status.
Table 1.
Demographic and clinical characteristics of the study population stratified by survival status.
| Patient Characteristics | Total | Survival | Death | |
|---|---|---|---|---|
| Patients, n (%) | 250 (100) | 171 (68.4) | 79 (31.6) | p-value |
| Gender, n (%) | 0.115 | |||
| • Male | 160 (64.0) | 115 (67.3) | 45 (57.0) | |
| • Female | 90 (36.0) | 56 (32.7) | 34 (43.0) | |
| Age (years), mean ± SD | 64.8 ± 17 | 63.6 ± 17 | 67.5 ± 16 | 0.081 |
| Body weight (kg), mean ± SD | 80.1 ± 17 | 82.1 ± 17 | 75.8 ± 16 | 0.006 |
| BMI (kg/m²), mean ± SD | 28.2 ± 5.6 | 28.6 ± 5.6 | 27.4 ± 5.6 | 0.124 |
| BMI Nutritional Status, n (%) | 0.156 | |||
| • Undernutrition | 8 (3.2) | 7 (4.1) | 1 (1.3) | |
| • Normal weight | 118 (47.2) | 73 (42.7) | 45 (57.0) | |
| • Overweight | 93 (37.2) | 69 (40.4) | 24 (30.4) | |
| • Obesity | 31 (12.4) | 22 (12.9) | 9 (11.4) | |
| APACHE II score, mean ± SD | 21.9 ± 7.8 | 21.1 ± 7.5 | 23.8 ± 8.4 | 0.068 |
| SOFA score, mean ± SD | 8.45 ± 7.8 | 8.18 ± 2.9 | 9.05 ± 3.0 | 0.032 |
| Glascow Coma Scale, mean ± SD | 6.6 ± 4.9 | 7.0 ± 5.2 | 5.7 ± 4.2 | 0.049 |
| Comorbidities, n (%) | 231 (92.4) | 156 (91.2) | 75 (94.9) | 0.560 |
| Admission Type, n (%) | 0.020 | |||
| Medical, n (%) | 154 (61.6) | 97 (56.7) | 57 (72.2) | |
| Surgical, n (%) | 96 (38.4) | 74 (43.3) | 22 (27.8) | |
| Nosocomial Infection, n (%) | 89 (35.6) | 49 (28.7) | 40 (50.6) | <0.001 |
| Primary Clinical Diagnoses | 0.125 | |||
| Respiratory | 90 (36.0) | 55 (32.2) | 35 (44.3) | |
| Cardiac | 8 (3.2) | 6 (3.5) | 2 (2.5) | |
| Sepsis/Septic Shock | 47 (18.8) | 27 (15.8) | 20 (25.3) | |
| Traumatic Brain Injury | 17 (6.8) | 13 (7.6) | 4 (5.1) | |
| Surgery | 43 (17.2) | 35 (20.5) | 8 (10.1) | |
| Neurological | 21 (8.4) | 17 (9.9) | 4 (5.1) | |
| Other | 19 (7.6) | 14 (8.2) | 5 (6.3) | |
| Admission day worst value | ||||
| Heart rate,mean±SD | 80.1 ± 32 | 78.6 ± 30 | 83.5 ± 35 | 0.253 |
| Respiratory rate,mean±SD | 26.3 ± 5.8 | 26.2 ± 31 | 26.6 ± 6.1 | 0.566 |
| Systolic blood pressure,mean±SD | 115 ± 29.3 | 114 ± 27.7 | 115 ± 32 | 0.740 |
| Diastolic blood pressure,mean±SD | 58.4 ± 15 | 59.0 ± 15 | 57.1 ± 15 | 0.343 |
| Mean Blood Pressure,mean±SD | 77.1 ± 17 | 77.5 ± 17 | 76.3 ± 19 | 0.612 |
| SpO2 (%), mean±SD | 94.6 ± 4.5 | 94.9 ± 4.3 | 94.1 ± 4.9 | 0.179 |
| Therapeutic Interventions, n (%) | ||||
| • Mechanical ventilation | 97 (39.6) | 28 (16.9) | 69 (87.3) | <0.001 |
| • Vasoactive agents | 71 (28.5) | 10 (5.9) | 61 (77.2) | <0.001 |
| ICU stay (days), mean ± SD | 15.1 ± 16 | 14.2 ± 16 | 16.9 ± 16 | 0.220 |
| Hospital stays (days), mean ± SD | 35.6 ± 31 | 39.3 ± 31 | 27.7 ± 29 | 0.006 |
| Mechanical ventilation (days), mean ± SD | 14.5 ± 16 | 13.3 ± 16 | 16.9 ± 16 | 0.098 |
| Vasoactive therapy (days), mean ± SD | 11.8 ± 12 | 9.9 ± 11 | 15.5 ± 14 | <0.001 |
Abbreviations: BMI, body mass index; SOFA, Sequential Organ Failure Assessment; APACHE II, Acute Physiology and Chronic Health Evaluation II; ICU, intensive care unit; SpO₂, oxygen saturation. Related-Samples Friedman's Two-Way Analysis of Variance by Ranks, p<0.05: *D2 or D3 vs. D1, ** D2 vs. D3.
Table 2.
Distribution of acute kidney injury (AKI) markers, treatments, and nephrotoxic exposures by outcome group.
Table 2.
Distribution of acute kidney injury (AKI) markers, treatments, and nephrotoxic exposures by outcome group.
| Clinical characteristics | Total | Survivors | Non-survivors | p-value |
|---|---|---|---|---|
| Patients, n (%) | 250 (100) | 171 (68.4) | 79 (31.6) | |
| Urea D1 (mg/dL), mean±SD | 65.4 ± 48 | 61.4 ± 48 | 73.9 ± 48 | 0.056 |
| Urea D2 (mg/dL), mean±SD | 59.1 ± 40 * | 55.2 ± 40 * | 67.5 ± 39 | 0.023 |
| Urea D3 (mg/dL), mean±SD | 51.5 ± 33 *,** | 47.1 ± 30 *,** | 60.9 ± 36 * | 0.0092 |
| Creatinine D1 (mg/dL), mean±SD | 1.42 ± 1.2 | 1.40 ± 1.3 | 1.44 ± 1.1 | 0.836 |
| Creatinine D2 (mg/dL), mean±SD | 1.36 ± 1.0 | 1.33 ± 0.9 | 1.44 ± 1.0 | 0.421 |
| Creatinine D3 (mg/dL), mean±SD | 1.22 ± 0.7 *,** | 1.17 ± 0.7 *,** | 1.33 ± 0.8 ** | 0.107 |
| ClCr D1 (ml/min/1.73m2),mean±SD | 51.7 ± 37 | 53.5 ± 37 | 47.6 ± 37 | 0.244 |
| ClCr D2 (ml/min/1.73m2),mean±SD | 51.9 ± 38 | 54.2 ± 37 | 47.1 ± 39 | 0.173 |
| ClCr D3 (ml/min/1.73m2), mean±SD | 55.0 ± 39 *,** | 57.8 ± 38 *,** | 49.1 ± 40 | 0.101 |
| AKI at admission, n (%) | ||||
| KDIGO 1 | 46 (48.9) | 28 (50.9) | 18 (46.2) | 0.901 |
| KDIGO 2 | 23 (24.5) | 13 (23.6) | 10 (25.6) | |
| KDIGO 3 | 25 (26.6) | 14 (25.5) | 11 (28.2) | |
| KDIGO2 (day 3), n (%) | 52 (20.8) | 19 (14.6) | 33 (27.7) | 0.011 |
| KDIGO2 (day 7), n (%) | 48 (21.8) | 15 (12.8) | 33 (32.0) | <0.001 |
| mRAI (score), mean±SD | 7.1 ± 7.8 | 6.4 ± 7.1 | 8.6 ± 8.9 | 0.043 |
| mRAI (6–40), n (%) | 62 (24.8) | 36 (21.1) | 26 (32.9) | 0.044 |
| Nephrotoxicity, n (%) | 0.164 | |||
| Nephrotoxic (NF) Drugs | 49 (19.6) | 40 (23.4) | 9 (11.4) | |
| Contrast Agents (CA) | 80 (32) | 51 (29.8) | 29 (36.7) | |
| AC and NF drugs | 31 (12.4) | 20 (11.7) | 11 (13.9) | |
| None | 90 (36) | 60 (35.1) | 30 (38.0) | |
| Diuretics, n (%) | 184 (93.9) | 134 (92.4) | 50 (98.0) | 0.150 |
| CRRT, n (%) | 59 (24.1) | 19 (14.8) | 40 (34.2) | <0.001 |
| Diuretics, (days), mean±SD | 11.1 ± 14 | 10.7 ± 15 | 11.9 ± 13 | 0.559 |
| CRRT, (days), mean±SD | 10.5 ± 10 | 8.7 ± 7.4 | 12.9 ± 13 | 0.201 |
Abbreviations: AKI, acute kidney injury; KDIGO, Kidney Disease: Improving Global Outcomes; ClCr, creatinine clearance; CRRT, continuous renal replacement therapy; FO, fluid overload; mRAI, modified Renal Angina Index. Related-Samples Friedman's Two-Way Analysis of Variance by Ranks, p<0.05: *D2 or D3 vs. D1.
Table 3.
Cumulative input, output, fluid balance, and fluid overload by ICU day 3, stratified by survival status.
Table 3.
Cumulative input, output, fluid balance, and fluid overload by ICU day 3, stratified by survival status.
| Clinical characteristics | Total | Survivors | Non-survivors | p-value |
|---|---|---|---|---|
| Patients, n (%) | 250 (100) | 171 (68.4) | 79 (31.6) | |
| Total Input (ml), mean±SD | 11561 ± 5366 | 11024 ± 5943 | 12724 ± 3599 | 0.020 |
| Total Input (ml/IBW), mean±SD | 180.7 ± 85.5 | 169.3 ± 91.5 | 205.5 ± 64.8 | 0.002 |
| Total Output (ml), mean±SD | 9627 ± 4226 | 10007 ± 4426 | 8804 ± 3649 | 0.036 |
| Total Output (ml/IBW), mean±SD | 148.9 ± 60.3 | 152.7 ± 62.0 | 140.5 ± 54.1 | 0.137 |
| Fluid Balance (ml), mean±SD | 3038 ± 3877 | 2327 ± 3298 | 4577 ± 4556 | <0.001 |
| Fluid Balance (ml/IBW), mean±SD | 48.8 ± 62.0 | 36.6 ± 52.1 | 75.1 ± 73.1 | <0.001 |
| FO%, mean±SD | 4.9 ± 6.2 | 3.7 ± 5.2 | 7.5 ± 7.3 | <0.001 |
| FO > 10% (clinically significant), n (%) | 43 (17.2) | 16 (9.4) | 27 (34.2) | <0.001 |
| FO > 15% (severe), (%) | 17 (6.8) | 5 (2.9) | 12 (15.2) | <0.001 |
Abbreviations: FO, fluid overload; IBW, ideal body weight. Clinically significant FO was defined as >10% IBW, and severe FO as >15% IBW.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



