
Submitted:
13 October 2025
Posted:
13 October 2025
You are already at the latest version
Abstract
Background: Oral squamous cell carcinoma (OSCC) is a major global health burden, with high recurrence and therapeutic resistance. α-Tocopherol, the most active form of vitamin E and a potent antioxidant, occurs in Stichopus hermanii together with other bioactive compounds. These natural agents have been proposed as adjunctive strategies with dual antioxidant and anticancer potentials. Objective: To map evidence of the antioxidant and anticancer activities of α-tocopherol, either as an isolated compound or within S. hermanii extracts, against molecular targets in OSCC. Methods: A scoping review was conducted according to the PRISMA-ScR guidelines. Searches in PMC, PubMed, ScienceDirect, ResearchGate, and Google Scholar (until July 2025) identified English- or Indonesian-language Scopus-indexed full-text studies. Eligible reports included original in vitro, in vivo, and clinical investigations of α-tocopherol and S. hermanii in OSCC models. Data on the design, interventions, molecular targets, and outcomes were charted and narratively synthesized. Results: Five studies were included (three in vitro, one in vivo, and one clinical study). In vitro, α-tocopherol decreased OSCC cell viability and induced apoptosis via caspase activation, Bax upregulation, and Bcl-2 suppression, with synergistic effects observed with combination therapy. In vivo, α-tocopherol upregulated PPARγ and inhibited PI3K/Akt signalling, whereas S. hermanii extract reduced oxidative stress. Clinically, supplementation during radiotherapy improves the oxidative balance. Common molecular targets include apoptotic regulators and oxidative stress markers; however, OSCC-specific oncogenic pathways remain unexplored. Conclusion: α-Tocopherol exhibits antioxidant and pro-apoptotic effects in OSCC, indicating its potential as an adjunct therapy. However, the evidence is limited and heterogeneous, necessitating standardized interventions and clinical trials to confirm these findings.
Keywords:
α-Tocopherol
; antioxidant
; anticancer
; oral squamous cell carcinoma
; Stichopus hermanii
1. Introduction
Oral squamous cell carcinoma (OSCC) is the most common malignancy worldwide, accounting for approximately 90% of all oral cancer cases. It is an aggressive neoplasm that arises from squamous epithelial cells of the oral mucosa and often leads to tissue destruction, functional impairment, and high mortality. The incidence of OSCC varies globally with a particularly high prevalence in parts of South and Southeast Asia. The etiology of OSCC is multifactorial, involving risk factors such as tobacco use, excessive alcohol consumption, genetic susceptibility, and viral infections (notably high-risk human papillomavirus (HPV) [1,2,3,4]. At the molecular level, OSCC development involves a cascade of genetic and epigenetic alterations that drives malignant transformation. Common events include mutations in tumor suppressor genes (e.g., TP53 with gain-of-function mutations or CDKN2A inactivation) and oncogenes (e.g., RAS family mutations), leading to disrupted cell cycle regulation and evasion of apoptosis. Dysregulation of key signaling pathways, such as the epidermal growth factor receptor (EGFR) and phosphoinositide 3-kinase/AKT (PI3K/Akt) pathways, is frequently observed, promoting unchecked cell proliferation and survival. OSCC progression is also supported by angiogenesis mediated by factors such as vascular endothelial growth factor (VEGF), which facilitates tumor growth and metastasis [3]. Despite advances in surgery, radiotherapy, and chemotherapy for OSCC, outcomes are undermined by high recurrence rates and therapeutic resistance [5,6], prompting interest in adjunctive treatments that can improve efficacy without severe toxicity.
In recent years, there has been a growing interest in the exploration of naturally derived bioactive compounds for the inhibition of OSCC progression. This approach aims to discover adjunct therapies that minimize long-term side effects associated with conventional drugs. Stichopus hermanii, an echinoderm native to Indonesian waters (locally known as “gamat”), has a rich history of use in traditional medicine across the Middle East and Asia [7,8,9,10]. S. hermanii is known for its high content of bioactive compounds that exhibit antioxidant and anticancer properties, making it a compelling candidate for cancer research. Among its key constituents is α-tocopherol, the most biologically active form of vitamin E. α-Tocopherol has a hydroxylated aromatic ring that confers potent lipophilic antioxidant activity. It can stabilize cell membranes by scavenging lipid peroxyl radicals, thereby protecting cells from oxidative damage [11]. Beyond its antioxidant role, α-tocopherol has demonstrated various anticancer mechanisms, such as inducing cytotoxic effects and apoptosis in cancer cells, causing cell cycle arrest, inhibiting tumor growth and metastasis, and even reversing certain drug resistance mechanisms [12,13,14,15]. For example, α-tocopherol enhances the expression of endogenous antioxidant enzymes, such as catalase and superoxide dismutase (SOD), which mitigate oxidative stress, a contributing factor in OSCC pathogenesis (particularly in smokers who experience chronic oxidative insult) [11,12]. By reducing reactive oxygen species (ROS) and associated DNA damage, antioxidants, such as α-tocopherol, may help interrupt the carcinogenic process and boost immune defence.
Although individual studies have reported promising findings on the antioxidant and anticancer effects of α-tocopherol, no comprehensive scoping review has mapped the landscape of evidence specifically for α-tocopherol derived from S. hermanii and its molecular targets in OSCC. Understanding the breadth of research on this topic is important for identifying the molecular pathways that have been explored, the outcomes that have been measured, and the gaps in knowledge that persist. Therefore, we conducted a scoping review following the PRISMA-ScR guidelines to collate and describe existing scientific evidence on α-tocopherol (as a pure compound or within S. hermanii extracts) in the context of OSCC. The objectives were to summarize the types of studies available, the interventions and molecular targets investigated, and the key findings (observed antioxidant and anticancer effects), and to highlight research trends and gaps that could inform future investigations or the eventual development of marine-based adjunctive therapies for OSCC.
2. Methods
2.1. Study Design and Protocol
This scoping review was conducted in accordance with the PRISMA-ScR (Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews) guidelines. We followed a predefined protocol based on the Arksey and O’Malley framework for scoping reviews, which included identifying the research question, relevant studies, study selection, data charting, collating and summarizing results, and consulting experts (if applicable). The core question guiding our review was as follows: What is the current state of evidence regarding the antioxidant and anticancer activities of α-tocopherol (alone or in Stichopus hermanii extracts) against molecular targets in OSCC models or patients? We did not register a formal review protocol for this review.
2.2. Data Sources and Search Strategy
A comprehensive literature search was performed using multiple databases to identify the relevant studies. The PubMed, PMC, ScienceDirect, ResearchGate, and Google Scholar databases were searched. We used combinations of Medical Subject Headings (MeSH) terms and keywords with Boolean operators to conduct the search. The primary search string is as follows:
(“α-tocopherol” OR “alpha-tocopherol” OR “vitamin E”)
AND (“Stichopus hermanii” OR “golden sea cucumber”)
AND (“oral squamous cell carcinoma” OR “OSCC”)
AND (antioxidant OR anticancer OR “molecular target”)
No restriction on publication year was applied, and all studies available up to July 2025 were considered. The language was limited to English or Indonesian (including articles with official English translations). To ensure a baseline level of quality and relevance, we focused on literature indexed in Scopus. We also manually screened the reference lists of relevant papers to identify additional studies that might have been missed in the database search.
2.3. Eligibility Criteria (Population Concept Context (PCC) Framework)
We defined the inclusion and exclusion criteria using (PCC) framework, which is recommended for scoping reviews.
- Population: Studies involving OSCC in any form. These included experiments on human oral cancer cell lines (e.g., ORL-48, SCC-9, and KB), animal models of oral/oropharyngeal carcinoma, and human subjects (patients) diagnosed with OSCC.
- Concept: This study investigated the antioxidant and anticancer activities of α-tocopherol and Stichopus hermanii extract. This encompassed α-tocopherol used as a single isolated compound (vitamin E) or as a component of crude extracts of S. hermanii. We included studies that measured relevant molecular or cellular outcomes such as oxidative stress markers (e.g., ROS levels, malondialdehyde [MDA], and antioxidant enzymes such as SOD, glutathione [GSH], and catalase) or cancer-related biomarkers/pathways (e.g., apoptosis induction, caspase activation, Bcl-2/Bax expression, cell proliferation, tumor growth, and expression of oncogenes or tumor suppressors).
- Context: Any research or clinical context relevant to oral squamous cell carcinoma was considered. These include in vitro laboratory experiments, in vivo studies in animal models, and clinical studies (including observational studies) involving patients with OSCC. We did not restrict the geographical location or setting.
Using these criteria, we included original research articles (experimental studies in vitro or in vivo and clinical studies) that were available in full text and addressed the above population and concepts within an OSCC context. Specifically, studies published in English (or Indonesian) until July 2025 were eligible if they examined α-tocopherol or S. hermanii extract in relation to OSCC.
The exclusion criteria were as follows: (1) articles that were not original research (e.g., review articles, meta-analyses, conference abstracts, editorials, or letters); (2) studies that did not explicitly involve α-tocopherol or Stichopus hermanii (for instance, studies on other sea cucumber species or vitamin E derivatives not derived from S. hermanii); (3) studies unrelated to OSCC (e.g., those focusing on other cancer types or general health effects not tied to oral carcinoma); and (4) studies with insufficient or unclear data on outcomes (e.g., missing quantitative results or lacking a clear method description to interpret findings). We initially aimed to be inclusive, given the exploratory nature of a scoping review; therefore, no studies were excluded solely based on perceived methodological quality. However, when screening the full texts, any study that lacked basic methodological clarity or outcome reporting was omitted because of the inability to confidently chart its findings.
2.4. Study Selection
All search results were imported into a reference management tool and duplicate records were excluded. The study selection process was conducted in two stages, by two independent reviewers (AA and IA). First, the titles and abstracts of all unique records were screened against the inclusion criteria (PCC). At this stage, irrelevant papers (for example, those not related to OSCC or those not involving α-tocopherol/S. hermanii) were excluded from analysis. Second, the full text of the remaining articles was retrieved and assessed for eligibility. Each reviewer independently evaluated whether the study met the inclusion criteria or not. Any disagreements or uncertainties regarding study inclusion were resolved through discussions between the reviewers and, if necessary, consultation with a third reviewer (AM). We maintained a PRISMA flow diagram to document the selection process, including the number of records identified, screened, excluded, and included. The final set of included studies was determined by consensus and is depicted in the PRISMA flowchart (Figure 1).
2.5. Data Charting and Extraction
A data charting form (spreadsheet) was developed to systematically extract key information from each included study. The charting process was performed by one reviewer and verified for accuracy by a second reviewer. The following details were extracted from each study:
- Citation details: Author(s), year of publication and title.
- Study design and context: Type of study (in vitro, in vivo, or clinical), specific model or population (cell line used, animal species and strain, patient population characteristics, etc.), and overall study aim related to OSCC.
- Intervention details: The form of α-tocopherol used (isolated α-tocopherol compound, synthetic vs. natural source, or S. hermanii extract containing α-tocopherol), dosage and duration of treatment, and route of administration (e.g., cell culture treatment, oral gavage in animals, and oral supplement in patients).
- Comparators: Description of control or comparison groups (such as untreated controls, vehicle controls, or alternative treatments such as standard antioxidants/drugs, if applicable).
- Outcomes measured: Molecular and biochemical targets or markers were assessed. These included antioxidant outcomes (e.g., levels of MDA and activities of SOD, GSH, and catalase), anticancer/cellular outcomes (e.g., cell viability, apoptosis rates, expression levels of apoptosis-related proteins such as caspase-3, caspase-9, Bcl-2, Bax, cell cycle phase distribution, tumor incidence, or size in animal models), and any other relevant OSCC-related molecular pathway data (e.g., signaling pathway activation/inhibition such as Akt phosphorylation status and expression of genes such as TP53 and VEGF, if reported).
- Key findings: A summary of the main results for these outcomes (for example, whether α-tocopherol treatment significantly reduced MDA levels or increased the apoptotic index compared to controls, including quantitative effects when reported).
- Conclusions of authors: The original study interpreted its findings (e.g., “α-tocopherol showed potential as an antiproliferative agent in OSCC cells by inducing apoptosis” or similar statements).
We did not formally appraise the risk of bias of the included studies, as the goal of a scoping review was to map all relevant evidence, regardless of quality. However, we have noted the general limitations of each study (such as small sample size or lack of controls, when applicable) in our narrative synthesis to provide context for the strength of evidence.
2.6. Synthesis of Results
The extracted data were collated and synthesized using a descriptive analytical approach. We grouped the evidence according to study type (in vitro, in vivo, and clinical) and main thematic outcomes (antioxidant activity outcomes versus anticancer/apoptotic outcomes), as these are the two prominent concepts across studies. Given the heterogeneity of the models and outcomes, no meta-analysis or quantitative pooling was conducted. Instead, we present a narrative summary that maps the findings across studies and highlights the patterns, consistencies, and discrepancies in the reported effects of α-tocopherol/S. hermanni extract on molecular targets in OSCC. We also constructed summary tables to provide an overview of each study’s characteristics and results, allowing for a visual comparison of interventions and outcomes (Table 1: in vitro studies; Table 2: in vivo studies; and Table 3: clinical studies). From this synthesis, we identified emerging trends (e.g., frequently studied biomarkers or common findings) and gaps (understudied aspects or inconsistencies) in the literature. These findings will inform the discussion of future research.
3. Results
3.1. Study Selection
The database search yielded 135 records. After removing 37 duplicate entries, 98 unique articles were retained for title and abstract screening. Of these, 50 were excluded from the initial screening phase because they were not relevant to our question (e.g., they were on unrelated topics or did not involve OSCC or α-tocopherol). We retrieved 48 articles for a full-text review, all of which were successfully obtained. Upon full-text eligibility assessment, 43 articles were excluded for the following reasons: they were reviews or commentary papers rather than original studies (9 articles); they did not specifically address OSCC or used non-OSCC cancer models (13 articles); they investigated sea cucumber species or substances unrelated to Stichopus hermanii (17 articles); or they failed to meet the inclusion criteria in terms of study design (e.g., not an in vitro/in vivo/clinical research study) or indexing criteria (four articles were in obscure journals not indexed in Scopus). Ultimately, five studies fulfilled all the inclusion criteria and were included in this scoping review. Figure 1 illustrates the study selection process using a PRISMA flow diagram.
3.2. Characteristics of Included Studies
The five included studies encompassed a mix of preclinical and clinical research, reflecting a multifaceted approach to investigating α-tocopherol in the context of OSCC. Three studies were in vitro experiments and one was a clinical observational study of patients with OSCC. Table 1, Table 2, and Table 3 summarize the key characteristics and findings of in vitro, in vivo, and clinical studies, respectively.
In all the in vitro studies, the Population was OSCC-related cell line. Zulkapli et al. used the ORL-48 human oral squamous carcinoma cell line to test the cytotoxic and pro-apoptotic effects of α-tocopherol [14]. Zhang et al. examined squamous carcinoma cells (derived from head and neck cancer) in a laboratory setting to evaluate combination therapy involving α-tocopherol [16]. Safithri et al. included an in vitro component measuring oxidative stress markers, although their study was also extended to an animal model [17]. The in vitro interventions included treatment with pure α-tocopherol at various concentrations (e.g., 100 µM in Zulkapli et al.’s study) and, in one case, α-tocopherol combined with other agents (13-cis-retinoic acid and interferon-α2a in the study by Zhang et al.) [14,16]. Control conditions were typically untreated cells or cells treated with standard comparators (for instance, Zhang et al. compared the triple combination against single agents, dual combinations, and untreated controls) [16]. The concepts/outcomes focused on in these cell studies were principally the antiproliferative and pro-apoptotic effects of the interventions. All three in vitro studies assessed cell viability and apoptosis-related endpoints. The techniques used included MTT or SRB assays for cell viability, flow cytometry with apoptosis markers (such as Annexin V staining or sub-G1 DNA content analysis), and measurement of apoptotic protein expression (caspase-3, caspase-9, and Bcl-2) via western blotting or ELISA. Key Findings from in vitro research have consistently indicated that α-tocopherol exposure reduces viability and increases apoptosis in OSCC cells. For example, Zulkapli et al. reported a dose-dependent decrease in cell viability and a more than two-fold increase in apoptotic cell count compared with untreated controls after treatment with α-tocopherol [14]. Similarly, Zhang et al. found that the combination of α-tocopherol with retinoic acid and interferon-α synergistically inhibited cell growth and induced significant G1 phase cell cycle arrest, accompanied by increased apoptosis rates and activation of caspase-3/-9 and downregulation of Bcl-2, surpassing the effects observed with any single agent alone [16]. These in vitro results indicate a clear trend that α-tocopherol can trigger apoptotic pathways in oral carcinoma cells, particularly when used at sufficiently high concentrations or in combination regimens.
In vivo evidence was obtained from two studies (including the in vivo portion of Safithri et al.). Xu et al. utilized a rat model of carcinogen-induced esophageal squamous cell carcinoma (which, while not oral cancer, is a closely related squamous carcinoma model) to investigate the chemopreventive effects of α-tocopherol [18]. Their intervention involved dietary supplementation with α-tocopherol in rats exposed to an OSCC-related carcinogen, N-nitrosomethylbenzylamine (NMBA). Safithri et al. used Sprague-Dawley rats with streptozotocin (STZ)-induced diabetes as a model of oxidative stress to test the antioxidant effect of S. hermanii extract, with α-tocopherol as a positive control comparator [17]. In these in vivo contexts, the measured outcomes included macroscopic tumor outcomes and molecular biomarkers. Xu et al. evaluated tumor incidence and histopathological changes as well as molecular signaling outcomes in esophageal tissues, notably the expression of peroxisome proliferator-activated receptor gamma (PPARγ) and components of the Akt signaling pathway, given their known roles in squamous cell carcinoma biology. They found that rats receiving α-tocopherol had a lower frequency of preneoplastic and neoplastic lesions, and mechanistically, α-tocopherol upregulated PPARγ expression while suppressing phosphorylated Akt levels, along with increasing pro-apoptotic markers such as Bax and cleaved caspase-3, relative to carcinogen-only controls [18]. These results suggest that α-tocopherol can interfere with carcinogenesis in vivo by modulating the key survival pathway (PI3K/Akt) and promoting apoptotic signaling. In contrast, Safithri et al.’s in vivo findings centered on oxidative stress parameters: in STZ-diabetic rats, treatment with S. hermanii extract significantly reduced markers of lipid peroxidation (with serum MDA levels reduced by approximately 86% compared to untreated diabetic controls) and improved antioxidant enzyme activities (such as SOD and catalase in red blood cells), with performance comparable to or better than that of the α-tocopherol-only group [17]. Although this study was not an OSCC tumor model, it provides insight into the antioxidant potency of S. hermanii extract in a living system and confirms that α-tocopherol is a major contributor to this effect. The inclusion of Safithri et al. in this review is valuable for mapping evidence on how S. hermanii (and by extension α-tocopherol) combats oxidative stress, a mechanism relevant to cancer prevention in general, and OSCC, in particular [17].
A clinical observational study by Chitra and Devi offered a glimpse into how α-tocopherol might affect patients with OSCC undergoing treatment [19]. This study was conducted in the context of radiotherapy for OSCC. Patients in the intervention group received oral α-tocopherol supplementation during their course of radiation treatment, while a comparison group of patients underwent radiotherapy without vitamin E supplementation. The outcomes of interest were oxidative stress and antioxidant status indicators measured in patient blood samples, including MDA (as a pro-oxidant marker) and antioxidant enzymes (SOD, GSH, and catalase), assessed before and after radiotherapy. The results showed that patients who received α-tocopherol had significantly more favorable changes in these biomarkers; post-radiotherapy, MDA levels were lower (indicating reduced lipid peroxidation) and their levels of SOD, GSH, and catalase were higher (indicating a bolstered antioxidant defense) than those who did not receive the supplement [19]. This suggests that α-tocopherol supplementation may mitigate radiation-induced oxidative stress in OSCC patients. It is worth noting that this was not a randomized trial, but rather an observational cohort study; therefore, the findings, while promising, should be interpreted with caution regarding causality. Nonetheless, this study provides supporting clinical evidence that aligns with the antioxidant effects observed in preclinical studies.
In summary, the concepts and molecular targets covered by the five included studies largely overlap in two domains: apoptosis-related pathways and oxidative stress-related markers. All studies, in one way or another, examined outcomes that fall into these categories, reinforcing the dual antioxidant and anticancer (specifically pro-apoptotic) effects of α-tocopherol. The interventions ranged from pure α-tocopherol (vitamin E) to crude S. hermanii extracts containing α-tocopherol among other compounds, and even combination therapies, including α-tocopherol. Despite this variety, a common trend is evident: α-Tocopherol exposure is associated with increased apoptosis in cancer cells and decreased oxidative damage in both cells and tissues. Key molecular indicators of these effects reported across studies include elevated caspase-3 and caspase-9 activity, higher Bax/Bcl-2 ratios favoring apoptosis, reduced MDA concentrations, and enhanced antioxidant enzyme levels. These findings span different experimental contexts (cell cultures, animal models, and human patients), suggesting a potentially robust phenomenon. However, it is also apparent that specific OSCC-related molecular pathways (e.g., EGFR, RAS-MAPK signaling, and p53 status) have not been thoroughly investigated in the current literature. Most studies have focused on general apoptosis and oxidative stress endpoints rather than tumor-specific oncogenic signaling. This observation highlights an evidence gap in linking the effects of α-tocopherol to the quintessential molecular drivers of OSCC, which we addressed in the Discussion section.
4. Discussion
To our knowledge, this is the first scoping review to map the evidence concerning α-tocopherol from Stichopus hermanii and its antioxidant and anticancer activities in the context of oral squamous cell carcinoma. We identified only five relevant studies, which indicates that this is an emerging research niche. Despite the limited number of studies, the findings collectively illustrate a consistent narrative: α-tocopherol, either as an isolated compound or within S. hermanii extracts, modulates the key processes of oxidative stress and apoptosis in OSCC models. The included studies, spanning in vitro cell experiments, animal models, and clinical observational studies, each contributed to the overall understanding of how α-tocopherol may influence OSCC pathophysiology. In this discussion, we synthesize these contributions, compare them with each other, and highlight the emerging trends and gaps in the broader scientific context.
4.1. Antioxidant and Pro-Apoptotic Effects of α-Tocopherol in OSCC Models
A prominent theme across these studies was the ability of α-tocopherol to induce apoptosis in OSCC cells. In in vitro investigations, α-tocopherol treatment led to significant apoptotic cell death in oral carcinoma cell lines. For instance, Zulkapli et al. reported that a 100 µM dose of α-tocopherol more than doubled the apoptosis rate in OSCC cells compared to untreated controls, as evidenced by the flow cytometric detection of apoptotic markers and morphological changes in DAPI-stained nuclei [14]. This finding aligns with the well-established role of vitamin E in triggering apoptosis through the mitochondrial pathway. Indeed, Zhang et al. found that α-tocopherol, especially when combined with 13-cis-retinoic acid and interferon-α2a, activated the intrinsic apoptotic pathway: treated cells showed increased activation of executioner caspases (caspase-3 and -9) and a concomitant decline in the anti-apoptotic protein Bcl-2, tipping the balance in favor of programmed cell death. Notably, the combination of agents in the study by Zhang et al. had a greater effect than α-tocopherol alone, suggesting a synergistic interaction that could be relevant for combination therapies. However, even as a single agent, the pro-apoptotic effect of α-tocopherol is evident. The ability of α-tocopherol to modulate Bcl-2/Bax rheostat (by downregulating Bcl-2 and likely upregulating pro-apoptotic Bax) is particularly important, as this rheostat governs mitochondrial outer membrane permeabilization, a point of no return in apoptosis induction [16].
An in vivo study by Xu et al. extended these findings to the organismal level. In the NMBA-induced carcinogenesis rat model, α-tocopherol supplementation was associated with higher expression of Bax and cleaved caspase-3 in esophageal tissues, indicating enhanced apoptotic activity in preneoplastic lesions [18]. Correspondingly, they observed the suppression of tumor development, implying that the pro-apoptotic pressure exerted by α-tocopherol counteracts the carcinogenic process. Xu et al. also highlighted the role of PPARγ and PI3K/Akt signaling in mediating these effects in the liver. PPARγ is a nuclear receptor that can promote differentiation and apoptosis in some cancer cells, whereas the PI3K/Akt pathway is a well-known survival pathway that is often overexpressed in OSCC and other cancers [18]. The finding that α-tocopherol upregulated PPARγ and concurrently inhibited Akt phosphorylation in vivo is highly significant, suggesting that α-tocopherol might shift the signaling landscape of cells towards one that favors growth arrest and apoptosis over survival and proliferation. This mechanistic insight complements the in vitro data, indicating that the anticancer activity of α-tocopherol in OSCC involves both direct induction of the apoptotic machinery and upstream modulation of survival pathways.
In addition to inducing apoptosis, α-tocopherol and Stichopus hermanii extracts consistently demonstrated antioxidant effects in the included studies. OSCC and carcinogenesis are strongly linked to oxidative stress; excessive ROS can cause DNA damage and activate pro-tumorigenic signaling pathways while also creating an environment of chronic inflammation that supports cancer progression [19]. α-Tocopherol, a chain-breaking antioxidant, directly neutralizes lipid peroxides and stabilizes cell membranes, which are vital in tissues undergoing inflammatory or radiation-induced oxidative damage [11]. A clinical study by Chitra & Devi provided real-world evidence of this antioxidant action: OSCC patients who received α-tocopherol during radiotherapy had markedly lower levels of MDA, a byproduct of lipid peroxidation, than those who did not. Simultaneously, their antioxidant enzyme levels (SOD, GSH, and catalase) were higher, indicating that α-tocopherol either preserved these endogenous defenses or stimulated their up-regulation. These results are congruent with our understanding that vitamin E protects cells from oxidative damage; here, it seemingly helped patients better withstand the oxidative stress caused by RT [19].
Safithri et al. further reinforced the antioxidant capacity of α-tocopherol using experimental models. Using in vitro chemical assays, they demonstrated that S. hermanii extract and pure α-tocopherol could inhibit MDA formation (a measure of antioxidant activity) in a controlled system. In vivo experiments in rats showed dramatic reductions in MDA levels in vital organs when treated with S. hermanii extract, approaching the effect magnitude of standard antioxidants or hypoglycemic agents in a diabetic model [17]. This highlights an important point: the whole extract of S. hermanii may confer additional antioxidant benefits beyond those provided by α-tocopherol alone, owing to other bioactive constituents, such as saponins, glycosaminoglycans, or triterpenoids present in the sea cucumber [21]. Such compounds may act synergistically with α-tocopherol or cover different aspects of oxidative stress (for instance, some could be more effective in aqueous environments than in lipid environments where α-tocopherol operates).
4.2. Trends, Heterogeneity, and Knowledge Gaps
The evidence mapped in this scoping review revealed several trends and notable heterogeneity among the approaches. A clear trend is the dual focus on antioxidants and apoptotic/cancer markers as outcome measures. This duality perfectly aligns with the purported dual role of α-tocopherol as an antioxidant and anticancer agent. Despite their different designs, all included studies measured at least one parameter of oxidative stress and one parameter of cell survival or apoptosis. This indicates that researchers in this area are consistently interested in how α-tocopherol addresses the two fundamental hallmarks of cancer: the avoidance of cell death and oxidative stress damage.
Another trend is the use of α-tocopherol in combination with other compounds, or as part of a complex natural mixture. Only one study [14] looked at pure α-tocopherol in isolation; others either combined it with conventional agents (a differentiation agent and cytokine) [16] or used it in the form of a crude extract [17] or as a supplement during standard care (with radiotherapy) [19]. This suggests that, in practical scenarios, α-tocopherol is considered an adjunct rather than a standalone therapy. The combination approach is logical: the antioxidant action of α-tocopherol might protect normal tissues or sensitize cancer cells to other treatments, while its pro-apoptotic influence could enhance the overall anticancer effect when used with chemotherapy, radiation, or other drugs. However, the heterogeneity in the application of these interventions (different doses, combinations, and formulations) makes it challenging to directly compare results across studies. For example, the doses used in vitro (tens to hundreds of micromolars) do not directly translate to the doses administered to rats (which were dietary and resulted in systemic levels) or to human supplementation (which was a certain mg/day oral dose). This variability points to the need for standardization; researchers should aim to report doses in comparable units (e.g., mg/kg or µM) and justify their dose choices against known therapeutic or physiological levels.
The molecular targets examined across studies were mostly general markers (caspases, MDA, antioxidant enzymes, etc.), and not OSCC-specific oncogenic pathways. Key drivers of OSCC, such as EGFR, cyclin D1, TP53 mutations, RAS mutations, and pathways such as NF-κB and MAPK, have not been investigated in these studies. This is a significant gap because, while demonstrating that α-tocopherol can induce apoptosis and reduce oxidative stress, understanding the specific cancer pathways it affects in OSCC is crucial for positioning α-tocopherol in the landscape of cancer therapeutics. It might be informative, for instance, to know if α-tocopherol downregulates EGFR expression or activity in OSCC cells (since EGFR overexpression is common in OSCC) or whether it interferes with NF-κB activation (a pathway linking inflammation and cancer survival). The current evidence does not answer these questions, which identifies a clear direction for future research: targeted studies investigating the impact of α-tocopherol on OSCC-specific molecular signals (e.g., those mentioned above, as well as angiogenesis-related factors like VEGF, or invasion/metastasis-related markers like MMPs).
Another limitation is the lack of clinical data. Only one observational study in humans was included, and no randomized controlled trials (RCTs) have been conducted on patients with OSCC to test α-tocopherol or S. hermanii extract as an intervention. The lack of RCTs means that there is no high-level evidence for actual efficacy or patient outcomes (such as survival and tumor response). The existing human data suggest biochemical effects (reduced oxidative damage during therapy), which are encouraging but insufficient to draw any conclusions about clinical benefits, such as tumor control or patient quality of life. Additionally, an observational design is subject to confounding factors; for example, patients who took supplements might differ in other ways (diet, overall health) from those who did not. Thus, while the trend in biochemical markers is favorable, there is a critical need for clinical trials to evaluate whether these biochemical improvements translate into meaningful clinical improvements in OSCC treatment (e.g., fewer mucositis side effects, improved tumor response to radiotherapy, and better recurrence rates).
The limitations of the included studies are worth discussing because they reflect the state of evidence. Although in vitro studies are excellent for mechanistic understanding, they cannot capture the complexity of a living organism; factors such as the bioavailability of α-tocopherol, metabolism, immune system interactions, and long-term effects have not been addressed. The in vivo studies each had limitations: Xu et al.’s model was esophageal rather than oral cancer (although similar in histologic type, the tissue context differs), and Safithri et al.’s model did not involve cancer at all, but rather systemic oxidative stress. To date, no animal study has specifically tested S. hermanii extract or α-tocopherol in an oral cancer-bearing animal (such as a mouse oral xenograft model or a hamster cheek pouch model of OSCC). This represents a gap in preclinical evidence; bridging the gap between cell culture and human trials using a dedicated OSCC animal model study would be highly beneficial. Finally, the clinical study had a small sample size (exact numbers were not given in the summary but were likely modest) and short-term follow-up was limited to the radiation treatment period; long-term outcomes were not reported.
Despite these limitations, the overarching insight from this scoping review is that research consistently indicates towards α-tocopherol has beneficial biological effects in the context of OSCC, particularly by reducing oxidative stress and promoting apoptosis. None of the studies reported adverse or pro-carcinogenic effects of α-tocopherol; on the contrary, all outcomes were in a direction that would be considered favorable (e.g., decreased tumor cells and decreased oxidative damage). This consistency is encouraging and supports continued interest in this topic.
4.3. Research Gaps and Future Directions
Given the identified findings and limitations, several avenues for future research are important to fully elucidate the potential of α-tocopherol in OSCC. Key recommendations for future studies include the following.
- Investigation of OSCC-Specific Pathways: Studies should investigate how α-tocopherol influences key oncogenic pathways (e.g., EGFR, MAPK, NF-κB, TP53, RAS, and angiogenesis) to determine whether its effects are broad-spectrum or pathway-specific.
- Standardization of Interventions: Future studies should standardize formulations and dosages, directly compare pure α-tocopherol with S. hermanii extracts, and establish equivalent dosing to guide preclinical and clinical applications.
- Expanded Preclinical Models: Dedicated OSCC animal models, including immune-competent and xenograft systems, should be used to evaluate molecular, histological, and therapeutic outcomes as well as long-term safety and toxicity.
- Clinical Trials in Patients with OSCC: Randomized controlled trials are urgently needed to test α-tocopherol and S. hermanii supplementation in patients with OSCC, assessing not only biochemical endpoints but also clinical outcomes, such as mucositis, tumor response, recurrence, and survival, with careful patient stratification and dosing strategies.
- Long-Term and Synergistic Effects: Research should explore the potential risks of high-dose antioxidants, their long-term safety, and their possible synergies with standard therapies (e.g., enhancing cisplatin cytotoxicity or protecting normal tissues during radiotherapy).
Addressing these gaps will not only strengthen the evidence base, but also clarify whether α-tocopherol from S. hermanii can be moved from the bench to the bedside as a legitimate adjunct in OSCC therapy. Although the current evidence is promising, it is preliminary. To progress, the field requires more rigorous and focused studies to build on the findings of this scoping review.
5. Conclusions
In summary, this scoping review mapped the current evidence on α-tocopherol, particularly from Stichopus hermanii, in relation to oral squamous cell carcinoma (OSCC). Studies have consistently demonstrated dual antioxidant and pro-apoptotic activities, as reflected by reduced oxidative damage (lower MDA and higher antioxidant enzyme activity) and enhanced apoptosis via caspase activation, Bcl-2 family modulation, and PI3K/Akt pathway inhibition. These findings support the potential use of α-tocopherol as an adjunct for OSCC management by targeting oxidative stress and apoptotic resistance.
However, the evidence base remains limited, with only five heterogeneous studies ranging from in vitro to clinical observations. The lack of controlled clinical trials precludes conclusions regarding therapeutic efficacy in patients. Current data provide preliminary mechanistic and clinical insights, but highlight significant gaps, including the need for standardized interventions, exploration of OSCC-specific molecular pathways, and rigorous clinical validation of the findings.
Future research addressing these gaps will determine whether the promising antioxidant and anticancer properties of α-tocopherol alone or within S. hermanii extract can be translated into effective adjunctive strategies to improve OSCC outcomes.
Funding
The authors declare that no funding was received for this study.
Acknowledgements
The authors have no acknowledgements to declare.
Conflict of Interest
The authors declare no conflict of interest.
References
- Riskayanti NP, Riyanto D, Winias S. Manajemen multidisiplin oral squamous cell carcinoma (OSCC): laporan kasus. Intisari Sains Med. 2021;12(2):621–626. [CrossRef]
- Matsuo K, Akiba J, Kusukawa J, Yano H. Squamous cell carcinoma of the tongue: subtypes and morphological features affecting prognosis. Am J Physiol Cell Physiol. 2022;323:C1611–C1623. [CrossRef]
- Cabral LGS, Martins IM, Paulo EPA, Pomini KT, Poyet JL, Maria DA. Molecular mechanisms in the carcinogenesis of oral squamous cell carcinoma: a literature review. Biomolecules. 2025;15(5): Article 621.
- Gamal-Eldeen AM, Raafat BM, Alrehaili AA, El-Daly SM, Hawsawi N, Banjer HJ, et al. Anti-hypoxic effect of polysaccharide extract of brown seaweed Sargassum dentifolium in tongue squamous cell carcinoma. Front Nutr. 2022;9:854780. [CrossRef]
- Warnakulasuriya S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009;45(4–5):309–316. [CrossRef]
- Rivera C. Essentials of oral cancer. Int J Clin Exp Pathol. 2015;8(9):11884–11894. PMID: 26617944.
- Fatwati K, Amin A, Indriani L, Ladju RB, Akbar FH, Hamrun N. GC-MS analysis and in silico approaches to Stichopus hermanii as anti-inflammatory through PKC-β inhibition. Results Chem. 2025;??:102086. [CrossRef]
- Fachry MF, Damayanti I, Damoro P, Jubhari EH, Thalib B, Habibie A. Effectiveness of golden sea cucumber (Stichopus hermanii) extract gel on increasing RANKL expression process modeling in post-extraction tooth. Makassar Dent J. 2025;14(1):35–39.
- Damaiyanti DW, Soesilowati P, Arundina I, Sari RP. Effectiveness of gold sea cucumber (Stichopus hermanii) extracts in accelerating the healing process of oral traumatic ulcer in rats. Padjadjaran J Dent. 2019;31(3):208–214. [CrossRef]
- Salindeho N, Nurkolis F, Gunawan WB, Handoko MN, Samtiya M, Muliadi RD. Anticancer and anticholesterol attributes of sea cucumbers: an opinion in terms of functional food applications. Front Nutr. 2022;9:986986. [CrossRef]
- Niki E. Role of vitamin E as a lipid-soluble peroxyl radical scavenger: in vitro and in vivo evidence. Free Radic Biol Med. 2014;66:3–12. [CrossRef]
- Bei MF, Domocoş D, Szilágyi G, Varga DM, Pogan MD. Influence of vitamins and antioxidants in oral carcinogenesis – a review. Pharmacophore. 2023;14(6):39–45. [CrossRef]
- Talib WH, Jum’ah DAA, Athamneh K, Jallad MS, Kury LTA, Hadi F, et al. Role of vitamins A, C, D, E in cancer prevention and therapy: therapeutic potentials and mechanisms of action. Front Nutr. 2024;10:1281879. [CrossRef]
- Zulkapli R, Razak FA, Zain RB. Vitamin E (α-tocopherol) exhibits antitumour activity on oral squamous carcinoma cells ORL-48. Integr Cancer Ther. 2016;16(3):414–425. [CrossRef]
- Rajendran P, Athira AP, Yin OF, Swathy SS, Nishanth R, Sakthivel KM, et al. PI3K/Akt signaling pathway-mediated autophagy in oral carcinoma: a comprehensive review. Int J Med Sci. 2024;21(6):1165–1175. [CrossRef]
- Zhang X, Zhuo X, Khuri FR, Shin DM. Induction of cell cycle arrest and apoptosis by a combined treatment with 13-cis-retinoic acid, interferon-α2a, and α-tocopherol in squamous cell carcinoma of the head and neck. Head Neck. 2007;29(4):351–361. [CrossRef]
- Safithri M, Tarman K, Setyaningsih I, Fajarwati Y, Dittama IYE. In vitro and in vivo malondialdehyde inhibition activities of Stichopus hermanii and Spirulina platensis. Hayati J Biosci. 2022;29(6):771–781.
- Xu M, Yang H, Zhang Q, Lu P, Feng Y, Geng X, et al. α-Tocopherol prevents esophageal squamous cell carcinoma by modulating PPARγ–Akt signaling pathway at the early stage of carcinogenesis. Oncotarget. 2017;8(56):95914–95930. [CrossRef]
- Chitra S, Devi SS. Effect of α-tocopherol on pro-oxidant and antioxidant enzyme status in radiation-treated oral squamous cell carcinoma. Indian J Med Sci. 2008;62(4):141–148. PMID: 18445980.
- Reuter S, Gupta SC, Chaturvedi MM, Aggarwal BB. Oxidative stress, inflammation, and cancer: how are they linked? Free Radic Biol Med. 2010;49(11):1603–1616. [CrossRef]
- Hossain A, Dave D, Shahidi F. Antioxidant potential of sea cucumbers and their beneficial effects on human health. Mar Drugs. 2022;20(8):521. [CrossRef]
Figure 1.
PRISMA flow diagram illustrating the inclusion and exclusion processes of the studies across various screening phases.
Figure 1.
PRISMA flow diagram illustrating the inclusion and exclusion processes of the studies across various screening phases.
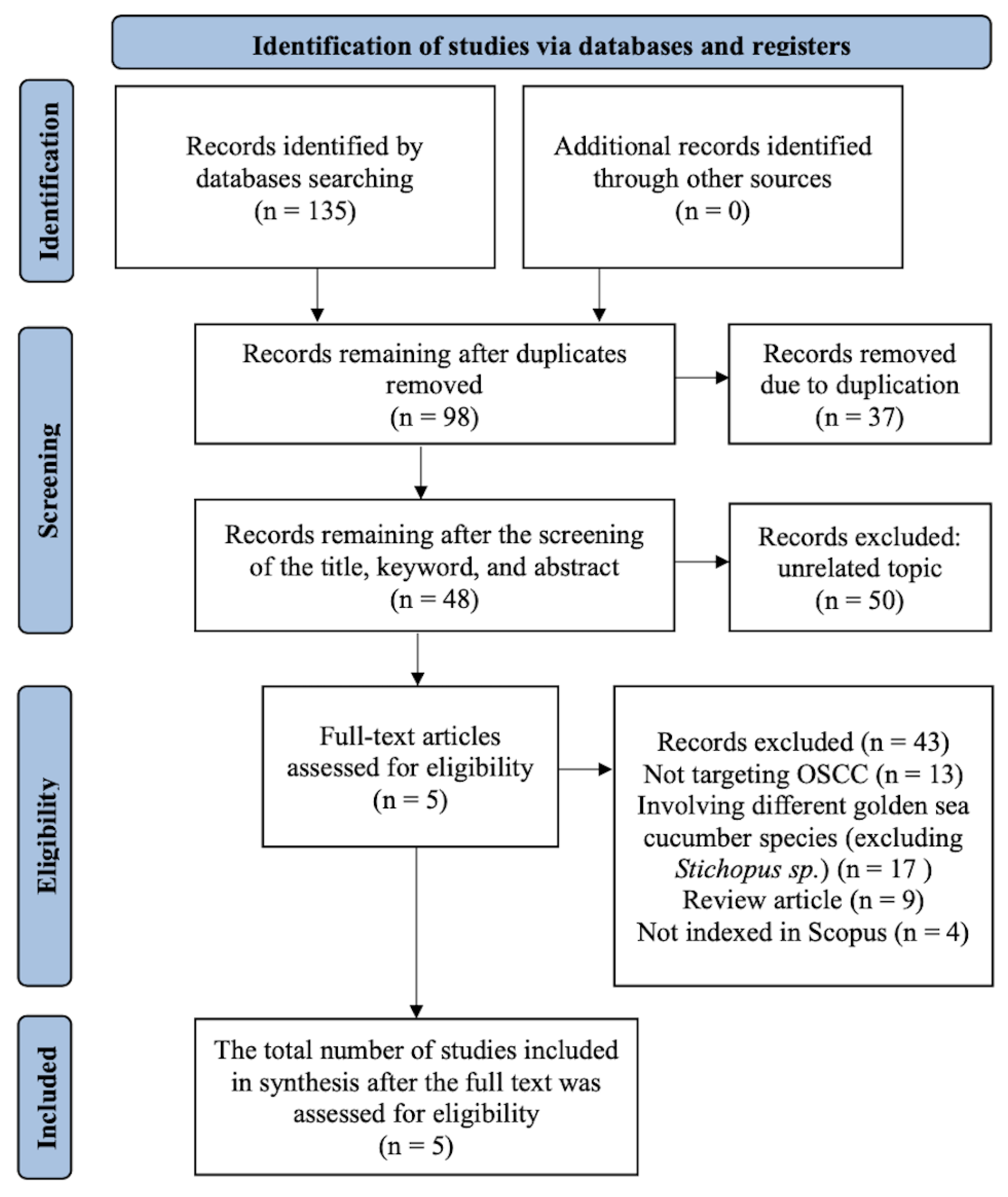

Table 1.
Characteristics and Main Findings (In Vitro Studies).
| No. | Author (Year) | Title | Study Design | Intervention | Comparison | Analysis Technique | Outcome Measures | Conclusion |
|---|---|---|---|---|---|---|---|---|
| 1. | Zulkapli et al. (2017) [11] | Vitamin E (α-Tocopherol) Exhibits Antitumour Activity on Oral Squamous Carcinoma Cells ORL-48 | In vitro (cell culture of OSCC ORL-48 cells) | Treatment with pure α-tocopherol | Control group (untreated ORL-48 cells) | MTT assay (cell viability), flow cytometry (apoptosis), DAPI staining (nuclear morphology) | Cell viability percentage, number of apoptotic cells, nuclear morphology | α-Tocopherol significantly reduced ORL-48 cell viability and induced dose-dependent apoptosis |
| 2. | Zhang et al. (2007) [12] | Induction of Cell Cycle Arrest and Apoptosis by a Combined Treatment with 13-Cis-Retinoic Acid, Interferon-α2a, and α-Tocopherol in Squamous Cell Carcinoma of the Head and Neck | In vitro (lab study on squamous cell carcinoma of the head and neck) | Combination of 13cRA, IFN-α, and α-tocopherol | Single agents, dual combinations and untreated control | SRB assay, FACS, Western blot, ELISA, Annexin V staining | Cell growth inhibition, apoptosis %, G1/S arrest, caspase and Bcl-2 expression | Triple combination synergistically induced apoptosis and cell cycle arrest |
| 3. | Safithri et al. (2022) [13] | In Vitro and In Vivo Malondialdehyde Inhibition Activities of Stichopus hermanii and Spirulina platensis | Combined in vitro and in vivo study (STZ-induced diabetic rats) | Methanolic extracts of S. hermanii and S. platensis; α-tocopherol as positive control | In vitro: α-tocopherol 200 ppm; In vivo: normal, STZ only, +SH, +SP, +glibenclamide | MDA-TBA assay, serum/liver MDA, RBC SOD & CAT via ELISA | MDA inhibition (%), serum/liver MDA (nmol/ml), SOD, CAT activity | SH reduced serum MDA (~86%), SP reduced liver MDA (~59%) |
ORL: Oral Squamous Cell Carcinoma Line; MTT Assay: 3-(4,5-Dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide assay; DAPI Staining: 4’,6-Diamidino-2-phenylindole staining; 13cRA: 13-CIS-retinoic acid; IFN-α: Interferon Alpha; SRB Assay: Sulforhodamine B assay; FACS: Fluorescence-Activated Cell Sorting; ELISA: Enzyme-Linked Immunosorbent Assay; Bcl-2: B-cell lymphoma 2; STZ: Streptozotocin; SH: Stichopus hermanii; SP: Stichopus sp.; MDA: Malondialdehyde; RBC SOD&CAT: Red blood cell superoxide dismutase.
Table 2.
Characteristics and Main Findings (In Vivo Studies).
| No. | Author (Year) | Title | Study Design | Intervention | Comparison | Analysis Technique | Outcome Measures | Conclusion |
|---|---|---|---|---|---|---|---|---|
| 1. | Xu et al. (2017) [14] | Alpha-Tocopherol Prevents Esophageal Squamous Cell Carcinoma by Modulating PPARγ-Akt Signaling Pathway at the Early Stage of Carcinogenesis | In vivo (study on F344 rats induced with NMBA carcinogen) | Dietary administration of pure α-tocopherol | Negative control, NMBA only, NMBA + α-Tocopherol | Western blot, IHC, qPCR, H&E staining, pathology scoring | Lesion count and severity, expression of PPARγ, Akt, p-Akt, caspase-3, Bcl-2, Bax | α-Tocopherol inhibited carcinogenesis via PPARγ upregulation and Akt phosphorylation suppression |
| 2. | Safithri et al. (2022) [13] | In Vitro and In Vivo Malondialdehyde Inhibition Activities of Stichopus hermanii and Spirulina platensis | Combined in vitro and in vivo study (STZ-induced diabetic rats) | Methanolic extracts of S. hermanii and S. platensis; α-tocopherol as positive control | In vitro: α-tocopherol 200 ppm; In vivo: normal, STZ only, +SH, +SP, +glibenclamide | MDA-TBA assay, serum/liver MDA, RBC SOD & CAT via ELISA | MDA inhibition (%), serum/liver MDA (nmol/ml), SOD, CAT activity | SH reduced serum MDA (~86%), SP reduced liver MDA (~59%) |
PPARγ-Akt: Peroxisome Proliferator-Activated Receptor Gamma–AKT pathway; NMBA: N-Nitrosomethylbenzylamine; IHC: Immunohistochemistry; qPCR: Quantitative Polymerase Chain Reaction; H&E Staining: Hematoxylin and Eosin staining; Bcl-2: B-cell lymphoma 2; STZ: Streptozotocin; SH: Stichopus hermanii; SP: Stichopus sp.; MDA: Malondialdehyde; RBC SOD&CAT: Red Blood Cell Superoxide Dismutase & Catalase.
Table 3.
Characteristics and Main Findings (Clinical Observational Studies).
| No. | Author (Year) | Title | Study Design | Intervention | Comparison | Analysis Technique | Outcome Measures | Conclusion |
|---|---|---|---|---|---|---|---|---|
| 1. | Chitra et al. (2008) [15] | Effect of α-Tocopherol on Pro-Oxidant and Antioxidant Enzyme Status in Radiation-treated Oral Squamous Cell Carcinoma | Clinical observational study (OSCC patients undergoing radiotherapy) | Oral supplementation of α-tocopherol during radiotherapy | OSCC patients without vitamin E supplementation | Spectrophotometry: estimation of MDA, SOD, GSH, and catalase activity | MDA levels, SOD, GSH, and catalase activity before and after radiotherapy | α-Tocopherol significantly reduced MDA and enhanced antioxidant enzyme activity |
MDA: Malondialdehyde; SOD: Superoxide Dismutase; GSH: Glutathione.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



