Submitted:
10 October 2025
Posted:
11 October 2025
You are already at the latest version
Abstract
Cancer is highly prevalent disease and one of the leading causes of global morbidity and mortality, however, about 50% of all cancer cases can be prevented through healthy living and policies that protect health. Stress, which has become an integral part of modern lifestyles, is considered as a hallmark of cancer. Chronic stress-related maladaptive response, immunosuppression, and inflammation – all directly increase the risk for the cancer development. Chronic stress also indirectly contributes by promoting unhealthy behaviours, such as overeating, smoking, drinking and hormonal imbalance – all of which induce inflammation promoting cancer development. Inflammation is also caused by many other factors, such as bacterial and viral infections, autoimmune diseases, and chemical exposure. This review is about stress and lifestyle-related behaviors and mechanisms that increase the risk for developing different types of cancer, and policies and strategies to educate people in early ages to take mindful decisions which can prevent the development of cancer in time.
Keywords:
stress
; risk factors
; prevention
; mechanisms
; inflammation
; cancer
1. Introduction
World Health Organization (WHO) states that About 1 in 5 people develop cancer in their lifetime and about 30–50% of all cancer cases are preventable. Emerging evidence suggests a role of chronic stress, which is an integral part of modern lifestyle, in higher incidences of cancer [1]. People experience stress or psychological stress when they are under mental, physical, or emotional pressure arising from daily routines associated with work, family or finances. Mechanistically, prolonged stress-associated maladaptive responses, a decline in immune surveillance and inflammation - directly promote cancer development and progression [2]. Stress indirectly promotes the development and progression of cancer by promoting unhealthy behaviours, such as overeating, smoking, drinking and hormonal imbalance – that also eventually leads to inflammation, which is considered as a hallmark of cancer [3]. In this review, we will discuss mutual direct and indirect crosstalk between stress-related different mechanisms and cancer, and also different measures to prevent development and progression of cancer.
1.1. Stress and Risk for Cancer
Stress is a new epidemic of the modern world and previously thought to be purely a mental reaction, but now research has established that prolonged or chronic stress adversely affects almost every part of the body. According to WHO, stress can be defined as a “state of worry or mental tension caused by a difficult situation” people feel when they are under psychological, physical or emotional pressure which may arise from people’s daily routine and responsibilities including work, family or finances. In a medical context, "stress" refers to the body's response to physical, mental, or emotional pressure, which can initiate the "fight-or-flight" response and lead to various physiological changes and potential health issues. Stress factors include external factors such as early life adversity, exposure to certain environmental conditions, poverty, discrimination, and inequities in the social determinants of health.
The body responds to external stressors by a variety of mental, physical and biochemical changes leading to release of stress hormones, such as epinephrine and norepinephrine, that increase blood pressure, heart rate, and blood sugar levels. This response, often referred to as the fight-or-flight response, helps a person act with greater strength and speed to escape and survive a perceived threat. Stress responses can be both adaptive or beneficial and maladaptive or deleterious depending upon the duration, intensity or nature of the stress [4]. Under repeated arousal of stress or chronic stress, the same beneficial fight-or-flight response becomes chronic and wears down body’s defenses, lowers immunity, making a body more vulnerable to all kind of sicknesses, such as, digestive problems, heart disease, high blood pressure, weakened immune system, headaches, sleep trouble, difficulty concentrating, depression, and anxiety as well as cancer. Accordingly, Drs. Thomas Holmes and Richard Rahe developed a scale based on 43 common stressful experiences, which indicate body’s vulnerability to illness under different types of stress [5]. It is important to note that people’s responses to stress are based on their mental, physiological and the environmental condition.
The idea of stress playing a role in cancer development is new, but it was noted as far back as the 2nd century by the Greek physician Galen, who noted that melancholy women appeared more likely to develop cancer than cheerful ones. Similarly, in the 18th and 19th centuries, physicians frequently noted an association between severe stress to occur before the onset of cancer. The same idea was further supported by Dr. Paget in 1870 and Dr. Parker in 1885, who observed an association between emotional disturbance and the development of cancer emphasizing the role of mind-body connection with cancer. This was further supported by Dr. Lawrence LeShan, who observed a distinct emotional life-history pattern in 76% of the cancer patients, which appeared only in 10% of a control healthy population. Similarly, in 2008, a comprehensive meta-analysis of 142 prospective studies (~87,000 subjects/study) observed a 6% increase of cancer incidence, poorer survival in patients with diagnosed cancer in individuals with psychosocial stress [6]. Several studies link stress directly or indirectly with cancer, where workplace stress is associated with an increased risk of prostate cancer [7], and greater odds of cancer at 5 out of 11 different cancer-types [7]. Work-related stress is also associated with an increased risk of lung, colorectal, and esophageal cancers in a meta-analysis of nine observational studies with a total of 281,290 participants [8]. There are several studies indicating a significant role of different type of stress in cancer progression and increased cancer-related mortality [1,6,9,10,11,12,13].
1.2. Mechanistic Link Between Stress and Risk for Cancer
There is sufficient evidence indicating the role of stress in the initiation and development of cancer, and accordingly, the biologic mechanisms and signaling pathways that may account for such observations are now being discovered through the convergence of relevant molecular, cellular, and clinical data. Studies show that hormones released as part of the body’s maladaptive response to chronic stress stimulates angiogenesis and metastasis [10]. These hormones may also activate immune cell, which can further promote initiate tumor and can also reactivate dormant tumors [14]. Furthermore, stress hormones also cause rapid release of proinflammatory cytokines, which can up-regulate the growth factor pathway initiating the formation of new tumor lesions and tumor cell exit from the dormancy [14]. These mechanisms are explained in detail as follows:
1.2.1. Mechanism of Stress-Related Maladaptive Response and Risk for Cancer
Initial adaptive stress response is coordinated by complex interaction between activation of the hypothalamic-pituitary-adrenal (HPA) axis, sympathetic-adreno-medullary (SAM) system, and the immune system [15]. The HPA axis facilitates physiological mechanisms of adaptation by secreting catecholamines and glucocorticoids [16]. Briefly, in HPA-mediated stress response, hypothalamus secretes corticotropin-releasing hormone (CRH) stimulating the anterior pituitary to secrete adrenocorticotropic hormone (ACTH), which eventually leads to the secretion of glucocorticoids, such as cortisol by the adrenal cortex. SAM system organizes the ‘fight or flight’ response during stress by modulating hormones such as epinephrine (adrenaline) and/or norepinephrine (noradrenaline). Together, HPA and SAM activate leukocyte trafficking to the specific brain areas and thereby modulating the immune system based on stress intensity and duration, which is mainly immunoenhansive under acute and immunosuppressive under chronic psychological stress condition [17,18]. Dysfunctional immune system contributes to sustained low-grade inflammation [19].
Emerging evidence provides a strong foundation for links between maladaptive response to chronic stress that is a continuous release of stress hormones, immunosuppression, and continuous low-grade inflammation [20], and an increased risk of cancer incidence and mortality [21]. Impaired HPA axis is associated with abnormal production of cortisol in cancer patients [22]. Chronic stress-associated prolonged activation of HPA and SAM leads to continuously higher level of stress hormones in different tissues including circulation [23] inducing DNA damage and inhibition of oncogenic p53 protein function, which may cause mutation and promote cancer growth [2]. Accordingly, it is reported that norepinephrine or cortisol-treatments induce DNA damage that is prevented by pharmacological inhibition of receptors for norepinephrine or cortisol [24]. In humans, psychological stress is associated with increased DNA damage (reviewed in [25]); however, DNA damage alone is not enough to promote cancer initiation, as mutations should be in oncogenes such as p53 and need to be maintained and accumulated throughout repeated cell divisions. Chronic restraint stress-associated increased glucocorticoid levels and beta-adrenergic signaling inhibit p53 expression and activity and promote tumorigenesis in mice [26,27]). Not only initiation but stress hormones such as catecholamines can also stimulate the proliferation of tumour cells and promote tumor growth by activation of extracellular signal-regulated kinases-1/2 (ERK1/2) signaling pathway by adrenergic signaling [28]. Role of catecholamines in cancer is further supported by the fact that inhibition of adrenergic signaling that inhibits ERK1/2 signaling inhibits proliferation and cancer growth [29,30,31]. Activation of adrenergic signaling also promotes angiogenesis that is required for sustained tumor growth and extracellular matrix degradation that is required for metastasis and growth factors secretion which enhances tumor microenvironment [23,32,33].
Additionally, approximately 13-15% of human cancer incidences are attributed to carcinogenic infections [34,35]. Chronic stress-associated glucocorticoids or catecholamines impair antiviral immunity [36,37,38] and appear to promote reactivation of human papillomaviruses (HPVs), Epstein–Barr virus, Kaposi sarcoma-associated herpesvirus and hepatitis B and C viruses [36] promoting the prevalence and outbreak of oncogenic viruses leading to an increased risk for cancer initiation. Accordingly, activation of stress-related SNS or HPA axis reactivated latent oncogenic viruses in humans [39,40]; and a higher incidence of HPV-related cancers was reported in a cohort of more than four million parents following child-loss [41]. There are also several animal studies demonstrating exacerbation of tumour initiation following carcinogenic exposure in stressed versus unstressed animal models [42,43,44,45,46].
1.2.2. Stress-Induced Immunosuppression and Risk for Cancer
Stress is shown to have immunosuppressive effects which prevents the body’s immune system from recognizing and fighting cancer cells [47]. Briefly, maladaptive chronic stress responses also lead to the accumulation of immunosuppressive immune cells, such as myeloid-derived suppressor cells, tumor-associated macrophages (M2 polarized), polymorphonuclear cells, type 2 and 3 of innate lymphoid cells, mast cells, regulatory T cells, and nucleated erythroid cells suppressing the number and function of immunoprotective (tumor-infiltrating lymphocytes, dendritic cells and natural killer cells are associated with an anti-tumor activity) cells leading to dysregulation of both innate and adaptive immune responses [48,49,50,51]. Additionally, chronic psychological stress stimulates the reprogramming of myeloid cells towards a hyperinflammatory state and induces production of proinflammatory cytokines, such as interleukin (IL)-6, IL-1β, or tumor necrosis factor (TNF)α [51].
1.2.3. Stress-Induced Inflammation and Risk for Cancer
Chronic stress promotes a persistent pro-inflammatory milieu by promoting production of pro-inflammatory cytokines [2], and persistent inflammation is often associated with the initiation, development, and progression of cancer [52,53,54]. Chronic inflammation is a hallmark of cancer, where cancer and inflammation both are driven by activation of common signaling pathways including signaling via nuclear factor kappa B (NF-kB), signal transducer and activator of transcription 3 (STAT3), and mammalian target of the rapamycin (mTOR) signaling pathways, which orchestrate the production and activation of proinflammatory cytokines [55]. Activation of NF-kB and STAT3 signaling pathways upregulate Ubiquitin D (UBD) expression which inhibits tumor suppressor p53 expression favouring tumorigenesis under inflammatory conditions [56]. P53 gene mutation is common in human cancers, and mutant p53 protein facilitates cancer cell survival by an enhanced production of intracellular reactive oxygen species (ROS), activation of mTOR signaling activation leading to reduced autophagic activity and secretion of proinflammatory cytokines which further activates proinflammatory and oncogenic signaling promoting a tumor-supportive milieu [55]. Cancer-associated hypoxia or metabolism and anticancer therapy can also induce proinflammatory cytokine production and release [57], which promotes cell proliferation, epithelial–mesenchymal transition (EMT), angiogenesis in tumor cells overall promoting progression of tumor growth and metastasis [57,58,59]. Additionally, in a normal inflammatory response, immune cells produce ROS that can kill a pathogen but can also induce DNA damage in a healthy cell, increasing the risk of mutations leading to cancer. In an acute optimal inflammatory response, the production of cells to replace injured tissue is normally delayed until ROS is no longer produced and/or active. However, in the case of chronic inflammation, ROS production can overlap with the production of cells that restore injured tissue, sustaining DNA damage leading to mutation and often creating an environment that is conducive to the development of cancer. Furthermore, animal studies have demonstrated a link between chronic stress, neuroinflammation and ROS production in brain [60,61], however, there are no studies directly evaluating the effect of stress-related neuroinflammation or ROS and incidence of cancer.
1.3. Indirect Role of Stress in the Risk for Cancer
A more of indirect role of stress is that people under chronic stress may often develop certain unhealthy behaviors, such as smoking, overeating, becoming less active or alcoholic, that are themselves associated with increased risks for cancer (Figure 1). The mechanisms related to indirect role of stress-associated unhealthy behaviours in development of cancer is explained in detail as follows:
1.3.1. Diet
Chronic stress can disrupt normal appetite regulation, often leading to unhealthy eating behaviors. For example, many individuals cope with stress by consuming “comfort foods” high in sugar and fat, as these foods can momentarily alleviate stress and produce pleasurable feelings through neurochemical rewards. Studies show that higher perceived stress is associated with greater intake of ultra-processed and sugary foods of poor diet quality [62,63]. This stress-induced tendency toward nutrient-poor and high-calorie foods can result in weight gain and nutrients deficiencies [62]. Over time, such stress-driven dietary patterns, characterized by excess refined carbohydrates, saturated fats, and processed meats, create a metabolic environment of high insulin and glucose levels and may alter the gut microbiome causing inflammation and oxidative stress, which promotes the risk for cancer initiation [64,65]. Accordingly, poor is linked to higher incidence of colorectal, liver, gastric, and other cancers [66,67]. A large meta-analysis showed that an “unhealthy” dietary pattern i.e., high in processed meat, sugars, and refined grains, was associated with a ~14% increased risk of gastrointestinal cancers. Mechanistically, unhealthy diets can drive chronic inflammation and cell proliferation. Excess fat and sugar intake lead to hyperinsulinemia and elevated insulin-like growth factors, which encourage tumor cell growth [64]. Diet-related obesity further exacerbates inflammation by releasing pro-inflammatory cytokines from adipose tissue. Additionally, carcinogens formed during high-temperature cooking of meats (e.g., heterocyclic amines) and nitrosamines in processed meats, directly damage DNA in the gastrointestinal tract [68]. Overall, the pro-inflammatory milieu created by a poor diet is conducive to DNA damage and uncontrolled cell division, thereby increasing cancer risk. At the population level, preventive strategies include promoting a balanced diet rich in vegetables, fruits, and whole grains and low in processed foods. Public health guidelines recommend reducing red and processed meat and sugar intake and ensuring access to affordable, healthy foods to mitigate diet-related cancer risks [66].
1.3.2. Lifestyle
A chronically stressful lifestyle can erode healthy routines and biological rhythms. High stress often leads to sleep disturbances; for instance, rumination and anxiety can cause insomnia or fragmented sleep [69]. In a state of chronic stress, the HPA axis is hyper-activated, elevating cortisol levels that disturb normal circadian signals [36]. As a result, stressed individuals feel fatigued and lack time or energy for exercise, regular meals, or relaxation [70]. They may also engage in other poor “lifestyle” habits: working long and late hours, neglecting leisure activities, or using stimulants and screens late into the night, all of which further disrupt sleep–wake cycles. For example, job stress and shift-work schedules are linked to circadian misalignment, with long-term night shift work modestly increasing the risk of health problems [71]. This combination of insufficient sleep, sedentary behavior, and erratic daily patterns caused by stress can impair immune function and increase systemic inflammation [69].
An unhealthy, high-stress lifestyle contributes to cancer risk through both direct physiological pathways and indirect effects on other risk behaviors. Chronic sleep deprivation and circadian rhythm disruption are associated with higher risks of certain cancers, such as breast and colorectal cancer, potentially due to altered melatonin production and impaired DNA damage repair at night [71]. Epidemiological studies have noted that long-term night shift workers have a slightly increased incidence of breast cancer, presumably from years of circadian rhythm disruption and hormonal imbalance [71]. Moreover, chronic psychological stress can promote tumor development by weakening immune surveillance and creating a pro-tumorigenic milieu [36]. Stress hormones like norepinephrine and cortisol can inhibit apoptosis and stimulate angiogenesis in emerging tumors, facilitating their growth, and spread [36,72]. Indirectly, a stressful lifestyle often co-occurs with smoking, heavy drinking, poor diet, and inactivity, compounding cancer risk. Preventive strategies emphasize work–life balance, adequate sleep, and stress management. For example, workplace interventions to limit prolonged overtime and rotating night shifts, as well as public health initiatives promoting sleep hygiene and relaxation techniques that aims to reduce chronic stress load. By improving mental well-being, maintaining regular sleep patterns, and encouraging healthier daily routines, it is possible to lower inflammation and hormonal imbalances, thereby potentially reducing long-term cancer risk [69].
1.3.3. Smoking
Psychological stress is a major driver of tobacco use. Many individuals begin or intensify smoking as a coping mechanism to alleviate stress and anxiety [69]. Large cross-national studies have shown that higher perceived stress is associated with higher odds of heavy smoking [73]. Biologically, nicotine can transiently dampen stress responses by releasing dopamine, which smokers find calming. This reinforces the habit during stressful periods; for instance, someone under chronic work stress may smoke more cigarettes per day to self-soothe [73]. Unfortunately, the relief is temporary; nicotine withdrawal can increase stress, creating a vicious cycle. Stressed smokers also have more difficulty quitting, as stress can trigger cravings and relapse [63]. In summary, stress often fuels smoking behavior, embedding it as an unhealthy coping strategy.
Smoking is the single most potent preventable cause of cancer, responsible for an estimated 20-30% of all cancer deaths [74]. Tobacco smoke contains dozens of carcinogens that cause DNA mutations in cells of the lungs and other organs. Long-term cigarette smoking multiplies the risk of lung cancer more than 20-fold, and accounts for roughly 90% of lung cancer cases in men and 80% in women [74]. Smoking also contributes to cancers of the throat, esophagus, pancreas, bladder, kidney, cervix, and others [68]. Mechanistically, inhaled tobacco carcinogens (such as benzo[a]pyrene and nitrosamines) form DNA adducts that induce mutations in key oncogenes such as p53. In parallel, smoking creates a chronic inflammatory state in the airways and throughout the body, as tobacco particles and chemicals irritate tissues. This inflammation produces cytokines and free radicals that further damage DNA and inhibit its repair. Additionally, smoking impairs the immune system’s ability to eliminate cells with genetic damage. Beyond the lungs, tobacco toxins transported via blood can damage organs systemically. There is also a synergistic effect with stress; chronic psychological stress may impair the immune system’s ability to clear emerging precancerous cells in smokers, compounding the risk [36]. Reducing smoking prevalence is paramount for cancer prevention. This includes stress-management support for smokers to prevent stress-induced relapses, aggressive tobacco control policies (taxation, advertising bans, and smoke-free laws), and smoking cessation programs. Such measures have led to declining smoking rates and parallel drops in lung cancer incidence in many countries [74]. Helping individuals replace smoking with healthier coping mechanisms for stress is particularly important. Over time, eliminating tobacco use would dramatically lower the incidence of at least a dozen cancers and alleviate the inflammatory burden caused by smoking.
1.3.4. Drinking
Stress is a well-known catalyst for increased alcohol consumption. Faced with chronic stress or traumatic events, people may drink alcohol to “self-medicate” anxiety and tension, as ethanol has sedative effects on the central nervous system [69]. Studies in occupational settings have observed that high job-related stress correlates with higher rates of heavy or binge drinking [63]. In these cases, alcohol is used as a maladaptive coping strategy; for example, an individual under financial or relationship stress might start consuming several drinks in the evening to relax. Over time, this pattern can escalate to alcohol abuse or dependence. Physiologically, acute stress elevates cortisol, and alcohol can blunt the cortisol response, temporarily making the drinker feel more at ease. This relief reinforces the behavior, creating an association between stress and the urge to drink [75]. Unfortunately, reliance on alcohol can worsen stress in the long run by disrupting sleep and mood, creating a negative feedback loop. Thus, stress often contributes to higher alcohol intake and risky drinking behaviors, which are unhealthy both mentally and physically.
Regular heavy alcohol consumption significantly increases the risk of several cancers. Epidemiological evidence has established a causal link between alcohol intake and cancers of the oral cavity, pharynx, larynx, esophagus, liver, colon, rectum, and female breasts [68]. For example, chronic drinkers have about a 5-fold greater risk of cancers of the mouth and throat compared to nondrinkers, and even moderate alcohol use (as low as one drink per day) has been associated with a higher risk of breast cancer in women [68]. Alcohol (i.e., ethanol) itself is metabolized into acetaldehyde, a toxic compound that can bind to DNA and proteins, causing mutations and impairing DNA repair. In heavy drinkers, acetaldehyde accumulates and can initiate cancerous changes in cells of the upper digestive tract and liver. Alcohol also generates ROS that damage cell membranes and DNA. Moreover, alcohol disrupts hormonal regulation; it increases circulating estrogen, which may partly explain the elevated breast cancer risk in female drinkers [68]. Chronic alcohol abuse induces inflammation in tissues as well. For instance, in the liver, years of alcohol use cause alcoholic hepatitis and cirrhosis (a state of persistent inflammation and fibrosis), which predispose to hepatocellular carcinoma. In the esophagus, alcohol’s irritant effect combined with repeated inflammation can promote cellular changes leading to esophageal cancer. Notably, alcohol and smoking act synergistically: alcohol can act as a solvent for tobacco carcinogens, allowing them to penetrate mucosal cells more deeply, thereby jointly amplifying cancer risk in the aerodigestive tract [68]. To reduce alcohol-related cancers, public health guidelines advise limiting alcohol consumption or abstaining entirely. Population strategies include increasing awareness that even moderate drinking can be carcinogenic, implementing alcohol taxes and restrictions on sales to curb heavy drinking, and providing support for individuals to manage stress without alcohol through counseling or stress reduction programs. In clinical settings, screening for alcohol misuse and offering interventions like cognitive-behavioral therapy for coping skills are important. By lowering overall alcohol intake in the population and addressing the stressors that drive people to drink, the incidence of alcohol-associated cancers can be substantially reduced.
1.3.5. Sun Exposure
At first glance, sun exposure might not seem directly linked to psychological stress. However, stress can indirectly influence behaviors related to sun exposure and protection. Some individuals, for example, engage in indoor tanning as a coping mechanism to improve mood. Ultraviolet (UV) radiation produces feelings of relaxation and well-being [76]. This means that during times of stress or depression, a person might seek out excessive sun or tanning bed exposure for its “feel-good” effects. Research has shown that UV exposure can indeed become addictive in this way; in rodent models, chronic UV exposure causes the release of β-endorphin, leading to pain tolerance and withdrawal-like behaviors when UV is removed [76]. In humans, studies have noted that in a subset of people (sometimes called “tan seekers”) who report using tanning as a stress reliever or who feel compelled to tan frequently, exhibiting behavior similar to other addictions. High stress and fatigue can also lead to negligence in sun safety practices; someone who is emotionally drained may be less likely to apply sunscreen or wear protective clothing when outdoors. They might also have less bandwidth to plan around peak UV times or seek shade.
Apart from these behavioral links, sun exposure itself is a well-known environmental risk factor for cancer. UV radiation, especially UVB, can directly damage DNA in skin cells by inducing cyclobutane pyrimidine dimers and other mutagenic photoproducts, overwhelming the cell’s repair capacity. UV rays penetrate deeper and generate ROS that damages DNA and cellular structures [77]. Over years of frequent sunburns or intense sun exposure, these DNA lesions accumulate and can activate oncogenes or inactivate tumor suppressor genes in skin cells. For example, the hallmark mutation in many UV-induced melanomas is a UV-signature C→T transition in DNA [78]. In addition to causing mutations, UV radiation suppresses local skin immunity; it impairs the skin’s immune surveillance by affecting Langerhans cells, which may allow emerging malignant cells to evade destruction. Importantly, UV exposure triggers an inflammatory response in the skin (sunburn is essentially an acute inflammation) [79]. Repeated inflammation and subsequent tissue repair create a pro-tumor environment, as inflammatory mediators like prostaglandins can stimulate cell proliferation. In chronically sun-exposed sites, this can lead to actinic keratoses (premalignant lesions) and, occasionally, to multiple skin cancers arising close together, likely due to high mutation bursts [80,81]. Reducing UV overexposure is key to preventing skin cancers. This includes public education on sun safety: using broad-spectrum sunscreen (SPF 30 or higher), wearing protective clothing and hats, and avoiding peak midday sun [82]. For those who use tanning beds to cope with stress or for cosmetic reasons, raising awareness about the addictive nature of UV tanning [76] may help. Behavioral interventions can assist people in finding healthier stress-relief alternatives than tanning. Policies also play a role: many jurisdictions have banned indoor tanning for minors and mandated sunscreen use in schools and workplaces. Regular skin examinations and early treatment of precancerous lesions are additional strategies to catch problems early. Taken together, combining sun protection with attention to mental health factors (like addressing why someone might be tanning to cope) offers a more comprehensive approach to reducing skin cancer risk.
1.3.6. Weight and Obesity
Chronic stress can lead to unhealthy weight gain and obesity through a combination of hormonal and behavioral factors. Biologically, prolonged stress elevates cortisol over time, and cortisol is known to increase appetite and promote fat deposition, particularly visceral fat [83]. Stressed individuals often crave energy-dense foods, driven by cortisol and reward pathways, resulting in higher intake of sugary and fatty snacks [62]. This stress-induced “emotional eating” can cause a surplus of calories and subsequent weight gain. Research has shown that people under chronic stress (for instance, caregivers of ill family members) who consume high-fat and high-sugar diets tend to accumulate significantly more visceral fat than non-stressed individuals on similar diets. In addition, stress may reduce motivation for physical activity and regular meal planning, compounding the weight gain effect. Over time, these factors can lead to overweight and obesity, especially central obesity, as stress shifts metabolic balance towards fat storage [63]. Moreover, chronic stress can alter insulin sensitivity; elevated cortisol and stress-related behaviors often result in insulin resistance, which further promotes weight gain. Thus, persistent psychosocial stress is a risk factor for unhealthy weight gain via both increased caloric intake and metabolic changes [84].
Excess body weight is a significant contributor to cancer risk. Extensive evidence now links obesity with at least 13 types of cancer, including postmenopausal breast, endometrial, colorectal, kidney, pancreatic, liver, gallbladder cancer, and others [66]. For example, obese women have a 2-4 times higher risk of endometrial cancer compared to those at healthy weight, and obesity is estimated to account for ~20% or more of these cases [84]. The mechanisms by which adiposity increases cancer risk are multifaceted and rooted in the pro-inflammatory and hormonal effects of excess fat tissue. Adipose tissue is metabolically active: in obesity, enlarged fat cells and infiltrating macrophages secrete high levels of pro-inflammatory cytokines such as IL-6, TNF-α, and C-reactive protein (CRP), creating a state of chronic low-grade inflammation [84]. This inflammatory milieu can promote DNA damage and stimulate proliferation of cells, providing fertile ground for carcinogenesis. Obesity also alters levels of sex hormones and growth factors. In postmenopausal women, adipose tissue becomes the primary source of estrogen; obese women therefore have higher circulating estrogen, which drives the division of breast and endometrial cells and increases cancer risk in those tissues [84]. Similarly, obesity is associated with hyperinsulinemia and elevated insulin-like growth factor-1 (IGF-1), which have mitogenic and anti-apoptotic effects that can facilitate tumor development, particularly in the colon and pancreas. Another consequence of obesity is oxidative stress; the combination of excess nutrients and inflammation leads to more ROS production, causing DNA damage [84]. Furthermore, excess visceral fat mechanically and biochemically alters the tissue microenvironment; for instance, fatty liver disease due to obesity causes continuous liver cell injury and regeneration, contributing to liver cancer risk [84]. Importantly, many obesity-related cancers such as like colon, breast, and prostate cancers are also influenced by insulin resistance and adipokine imbalances, e.g., high leptin and low adiponectin levels in obesity favor tumor growth [66,84]. The good news is that weight loss and lifestyle interventions can partly reverse these adverse biological factors; weight reduction reduces inflammation and restores healthier hormone levels [84]. On a population level, preventing and reducing obesity can substantially decrease the cancer burden. Strategies include promoting physical activity and nutritious diets from early life, implementing policies to discourage consumption of ultra-processed, high-calorie foods, e.g., sugar-sweetened beverage taxes, and creating environments that support an active lifestyle [66,84]. For individuals, maintaining a healthy Body Mass Index (BMI) through balanced diet and regular exercise is recommended by cancer prevention guidelines [66]. In patients who are already obese, even moderate weight loss can lower levels of inflammatory markers and improve insulin sensitivity, likely reducing future cancer risk [84]. Bariatric surgery in extreme obesity has been associated with reduced incidence of obesity-related cancers, illustrating the profound impact of weight on carcinogenesis. Ultimately, addressing societal and behavioral factors that lead to chronic stress and obesity is crucial to lowering obesity-related cancer risk.
1.3.7. Physical Activity
Psychological stress can be a barrier to maintaining an active lifestyle [70]. When individuals are under chronic stress or time pressure, exercise and recreation are often the first activities to be curtailed [70]. Research indicates that higher stress levels are associated with lower levels of physical activity; for example, college students during exam stress or adults with demanding jobs report exercising less than usual [70]. Stress can induce fatigue, demotivation, and lack of pleasure in activities, all of which reduce the likelihood of engaging in regular workouts [70]. Additionally, stressed individuals often experience scheduling challenges or prioritize other urgent tasks over exercise, leading to a more sedentary routine. Physiologically, stress can also affect muscle tension and energy levels; people feeling anxious or depressed, which are common outcomes of chronic stress, may find it harder to initiate exercise due to lethargy. This cycle is self-perpetuating because physical activity is a known stress-reliever; so when stress causes inactivity, stress symptoms may worsen, further entrenching sedentary behavior [70]. For instance, a caregiver under chronic stress might spend prolonged periods sitting and forgo daily walks due to persistent worry and time constraints. Over time, stress-related physical inactivity contributes to weight gain, cardiovascular deconditioning, and worsened mood, establishing an unhealthy feedback loop [84].
Lack of physical activity or sedentariness is a recognized risk factor for certain cancers, whereas conversely, regular exercise exerts a protective effect [85]. Strong evidence links higher levels of physical activity to lower risks of colon cancer, breast cancer, and endometrial cancer, among others [85,86]. A meta-analysis of studies on physical activity and colon cancer found that the most active individuals had about a 24% reduced risk of developing colon cancer compared to the least active. Similar risk reductions (~20–30%) are observed for postmenopausal breast cancer and endometrial cancer with regular moderate-to-vigorous exercise [85]. Several biological mechanisms underlie this protective effect. Exercise helps regulate hormones and metabolic factors: it lowers circulating estrogen levels in women by reducing adipose tissue and altering metabolism and improving insulin sensitivity, thereby reducing insulin and IGF-1 levels that can promote tumor growth [86]. Physical activity also has immune-enhancing and anti-inflammatory effects. During exercise, muscles release anti-inflammatory cytokines (e.g., IL-6 in an acute, beneficial form and IL-10) and myokines that modulate immune function, leading to reduced chronic inflammation over time. Active individuals tend to have lower levels of systemic CRP and TNF-α than sedentary peers [86]. This matters because chronic inflammation is a driver of cancer development; by keeping inflammation in check, exercise creates a less cancer-promoting environment [86]. In the colon, regular exercise speeds gastrointestinal transit, which means potential carcinogens have less contact time with the intestinal lining [86]. It also improves the immune surveillance capacity; for example, moderate exercise is associated with more robust activity of natural killer cells that can eliminate nascent tumor cells [86]. Conversely, physical inactivity contributes to obesity, inflammation, and hyperinsulinemia, all of which raise cancer risk [66,84]. In terms of prevention, public health efforts encouraging adults to engage in at least 150 minutes of moderate or 75 minutes of vigorous physical activity per week or a combination of both for general health and cancer prevention [86]. Creating supportive environments, such as safe walking paths, exercise programs at workplaces, and community sports facilities, can reduce barriers to exercise [86]. Importantly, incorporating stress-reduction techniques can help individuals overcome the motivational challenges; for instance, yoga or group exercises may provide both stress relief and physical activity [70]. Regular exercise not only lowers the risk of developing cancers but is also associated with better outcomes in cancer survivors, highlighting its role in both prevention and health maintenance [86]. In summary, keeping physically active helps maintain healthy body weight, reduces inflammatory mediators, improves immune function, and leads to favorable metabolic profiles, thereby significantly lowering the risk of various cancers [86].
1.3.8. Family History
A family history of cancer is a significant risk factor for developing cancer, usually due to inherited genetic mutations or shared lifestyle/environmental factors. While “family history” itself is not a behavior, it can influence behavior and stress levels. Individuals who know that a close family member or multiple family members had cancer often experience increased anxiety and perceived vulnerability regarding their own cancer risk [86]. This cancer-related worry can in some cases motivate positive health changes; for example, someone with a family history of colon cancer might adopt a healthier diet or adhere to screening colonoscopies earlier. However, studies have found that many people with a strong family cancer history do not significantly change their behaviors; some may even develop a sense of fatalism that “cancer is inevitable” [86]. This fatalistic outlook, driven by stress and fear, can lead to neglect of prevention, e.g., continuing to smoke or avoiding doctor visits due to fear of a bad outcome. Additionally, the stress of caring for a relative with cancer or the grief of losing a family member to cancer can take a psychological toll. Chronic stress in these familial situations may manifest as post-traumatic stress or prolonged anxiety. Such stress can indirectly affect cancer risk; for instance, via stress-induced behaviors like poor diet or alcohol use, as previously discussed. There is emerging evidence that severe stress, especially early in life, can produce epigenetic changes, such as DNA methylation or telomere shortening, that might interact with genetic predispositions to elevate cancer risk [87]. For example, women caring for children with chronic illnesses were found to have shorter leukocyte telomeres, equivalent to a decade of additional aging, compared to low-stress controls [87]. Shorter telomeres and increased oxidative stress in cells can facilitate genomic instability, potentially compounding inherited cancer risk. Thus, while the primary driver in family history is genetics, the accompanying stress and behavioral patterns in families can modulate how that risk is expressed.
Having a family history of specific cancers often signifies the presence of inherited mutations in cancer susceptibility genes, e.g., BRCA1/2 for breast and ovarian cancer, MLH1/MSH2 for Lynch syndrome colorectal and endometrial cancers, APC for familial polyposis, etc. [88,89]. These mutations can confer very high lifetime cancer risks. For instance, women with a BRCA1 gene mutation face about a 65–75% lifetime risk of breast cancer and up to a 40–50% risk of ovarian cancer, far above population averages [88,90,91]. Carriers of mismatch repair gene mutations, such as Lynch syndrome, have ~20–70% elevated risks for colorectal cancer and also higher risks for uterine and other cancers [88]. When such genetic predispositions exist, they initiate carcinogenesis more readily; fewer mutations are needed for a cell to become malignant. However, the actual development of cancer still can be influenced by environment and lifestyle. Chronic inflammation or hormonal exposures can accelerate cancer in predisposed individuals [84]. For example, an obese person with a hereditary colon cancer risk may develop polyps and cancer at younger ages because obesity-driven inflammation and insulin resistance promote additional tumor growth on top of the genetic tendency [84]. Family history is also often accompanied by shared environmental factors; families might have similar diets, smoking habits, or exposures (like radon or certain infections) that contribute to risk [69]. Preventive strategies for those with a strong family history or known genetic mutations are two-fold: medical and lifestyle interventions. Medically, there are high-risk surveillance programs, e.g., earlier and more frequent screenings such as mammography/MRI starting at age 25 for BRCA mutation carriers, or colonoscopy every 1–2 years starting in young adulthood for Lynch syndrome [88]. These can identify cancers at an early, treatable stage or even prevent them by removing precancerous lesions. In some cases, risk-reducing prophylactic surgeries are recommended, such as prophylactic mastectomy or oophorectomy in BRCA carriers [88]. Alongside, individuals with familial risk are counseled to rigorously modify any additional risk factors, e.g., not smoking, maintaining healthy weight, exercising, and eating a protective diet, to mitigate the environmental component of risk [66,84]. Managing stress and anxiety in these high-risk persons is also important: genetic counseling and support groups can alleviate excessive distress and encourage proactive health behaviors rather than fatalism [69]. While we cannot change the genes we inherit, evidence suggests that a healthy lifestyle can delay or even prevent some genetically predisposed cancers perhaps by reducing background inflammation and allowing the immune system to better counter nascent tumors [36]. Therefore, at the population level, offering genetic screening to families with strong cancer histories, providing them with tailored prevention plans, and addressing psychosocial stress through counseling are key strategies. By empowering individuals with familial risk to take medical and behavioral preventive actions, impact of hereditary cancer can be reduced.
1.3.9. Hormones
Chronic stress disrupts the body’s normal hormonal balance through the activation of stress response systems [92]. The HPA axis, when persistently stimulated by stress, leads to prolonged elevation of stress hormones in the bloodstream [92]. These stress hormones have wide-ranging effects on other endocrine pathways as previously described [36]. For example, high cortisol levels over time can cause insulin resistance and hyperinsulinemia, as well as relative suppression of gonadotropins, potentially altering sex hormone levels [36]. Women under chronic stress have been observed to sometimes experience menstrual irregularities, an indication that stress may affect estrogen–progesterone dynamics, although the relationship is complex [36]. Stress can also lower melatonin secretion due to disrupted circadian rhythms, removing a hormone that has antioxidant and oncostatic (cancer-protective) properties in tissues [36]. Moreover, stress-related behaviors such as poor sleep and diet further skew hormonal profiles; insufficient sleep raises cortisol and ghrelin (a hunger hormone) and reduces leptin levels, while a high sugar diet elevates insulin, together contributing to an endocrine environment that can be considered “pro-cancer” [84]. Notably, stress hormones themselves directly interact with cancer biology: many tumor cells, especially in breast, ovarian, and prostate cancers, express receptors for adrenergic stress hormones [72]. Norepinephrine released during stress can bind β-adrenergic receptors on tumor and stromal cells, activating signaling pathways that enhance formation of new blood vessels and inhibit anoikis (detachment-induced cell death), thereby facilitating tumor growth and metastasis [72]. In essence, chronic stress tilts the internal hormonal milieu toward one that favors inflammation, cell proliferation, and reduced immune surveillance [36,72].
Hormones play a critical role in the development of many cancers, and stress-related hormonal changes can intersect with these pathways [36]. Some of the most common hormone-driven cancers are those of the breast, uterus, prostate, and thyroid [93]. For instance, lifetime exposure to estrogen is a known driver of breast and endometrial cancer risk; factors like early menarche, late menopause, or postmenopausal hormone replacement therapy (HRT) that increase cumulative estrogen exposure all raise risk [93]. Stress may indirectly contribute by affecting body weight; as noted, stress-induced obesity increases peripheral estrogen production through aromatase activity in adipose tissue [84]. High insulin levels, often seen in chronically stressed or depressed individuals with poor lifestyle, can promote colon and endometrial cancer because insulin and IGF-1 provide growth signals to epithelial cells [84]. Additionally, adipokines from stress-related weight gain (such as elevated leptin and lower adiponectin) create a pro-inflammatory, pro-proliferative environment [84]. Stress hormones themselves can inhibit p53 and other tumor suppressor functions: experiments have shown that cortisol can render immune cells less responsive, leading to higher levels of inflammatory cytokines that foster DNA damage [36]. Meanwhile, adrenaline can mobilize neutrophils that release enzymes and ROS aiding tumor invasion and metastasis [72]. The net effect is that chronic stress hormones reduce cell apoptosis and promote angiogenesis and tumor dissemination [36,72]. Clinically, it’s observed that cancers can progress faster in patients with severe chronic stress, likely through these biological mechanisms [72]. On the other hand, exogenous hormone use is another aspect: for example, prolonged HRT with combined estrogen–progestin increases breast cancer risk, and high-dose testosterone use (e.g., anabolic steroids) can increase prostate abnormalities [72]. Stress might influence individuals’ decisions to use or not use such therapies, e.g., stress from menopausal symptoms leading to HRT use, which in turn affects cancer risk. To mitigate hormone-related cancer risks, managing both exogenous and endogenous hormone exposures is the key. On the exogenous side, guidelines recommend using the lowest effective doses of hormone therapy for the shortest duration necessary or seeking non-hormonal options for conditions like menopausal symptoms [93]. Endogenously, healthy lifestyle choices, e.g. regular exercise, weight control, high-fiber diets, help maintain balanced insulin and sex hormone levels, reducing cancer-promoting signaling [84]. Importantly, stress reduction is a complementary strategy: by lowering chronic stress, individuals can normalize cortisol and adrenaline output, which may improve immune function and reduce inflammation [36]. Techniques such as mindfulness, cognitive-behavioral therapy, or yoga have been shown to modulate stress hormone levels [69]. While the direct impact of stress reduction on cancer incidence needs more research, it likely contributes to a hormonal and immune environment less conducive to cancer [36,72]. In people with known high hormonal risks, such as BRCA mutation carriers or those with precancerous lesions, combining medical preventive measures, e.g., prophylactic surgeries or chemoprevention, with lifestyle and stress management offers the best approach [88]. Overall, recognizing the mind–body connection, that chronic psychological stress can translate into biochemical changes influencing tumor biology, underscores the importance of holistic cancer prevention strategies that include mental well-being as a component [36,72].
1.3.10. Environment
Environmental factors, such as pollution, occupational chemicals, and radiation, are major contributors to cancer risk, and these often intersect with social stressors [36,94]. Individuals living in lower socioeconomic conditions typically face both higher chronic stress and greater environmental carcinogen exposure [36,69]. For example, high-stress communities may be located in industrial areas with polluted air and water [94]. Economic stress can force people to live in substandard housing with carcinogens like radon or asbestos or to work in hazardous jobs, such as mining, construction, chemical manufacturing, where toxic exposures are higher [94]. Chronic stress might also reduce one’s capacity to avoid or mitigate environmental risks; a person juggling multiple jobs and financial strain may not have the time or resources to, say, test their home for radon or advocate for cleaner local air [36,69]. Moreover, stress can physiologically amplify the damage from environmental toxins; research suggests that stress hormones can diminish DNA repair capacity and antioxidant defenses, increasing susceptibility to environmental mutagens [36]. Thus, when a stressed individual is exposed to a carcinogen like benzo[a]pyrene in air pollution or aflatoxin in food, their body might be less efficient at repairing the DNA lesions, increasing the likelihood of mutations [36]. Additionally, stress-related immune suppression can impair the clearance of virally infected or transformed cells that result from environmental insults, further compounding cancer risk [36]. In occupational settings, a stressed or fatigued worker might be less vigilant about using protective equipment, inadvertently increasing their exposure to harmful substances [36]. In these ways, psychosocial stress and environment interplay: stress can cluster with higher exposure, and potentially worsen the biological impact of that exposure [36,69].
Numerous environmental agents are carcinogenic, often act through DNA damage or long-term inflammation [94]. For instance, airborne particulate matter and traffic-related air pollution are firmly linked to lung cancer; large cohort studies have found that areas with higher fine particulate (PM2.5) concentrations have elevated lung cancer incidence, even among nonsmokers [94]. In 2013, the International Agency for Research on Cancer classified outdoor air pollution (and PM2.5 specifically) as Group 1 (carcinogenic to humans) after evidence showed a clear dose-dependent increase in lung cancer risk with rising pollution levels [94]. Similarly, contamination of drinking water with arsenic (in parts of Bangladesh and other regions) has caused epidemics of skin, bladder, and lung cancers [94]. Occupational exposures like asbestos fibers cause mesothelioma and lung cancer by lodging in lung tissue and inducing chronic inflammatory scarring [94]. UV radiation in sunlight, discussed earlier, is an environmental carcinogen for skin, causing DNA mutations and inflammation [95]. Ionizing radiation, whether from nuclear fallout, radon gas seeping into basements, or medical X-rays, can break DNA strands and has been implicated in leukemias, thyroid cancer, and others [94]. Environmental tobacco smoke (secondhand smoke) increases lung cancer risk in nonsmokers, as it contains many of the same carcinogens as direct smoking [94]. Certain infectious agents are also considered environmental: for example, Helicobacter pylori (H. pylori) infection that is facilitated by sanitation conditions causes stomach cancer via chronic gastritis, and HPV spread in the community causes cervical and other cancers [96,97]. A common thread is inflammation; many environmental carcinogens cause tissue injury and long-standing inflammation that promotes cancer through the release of cytokines and growth factors [36,94]. Silica dust in mines causes silicosis (lung inflammation and fibrosis) and lung cancer; asbestos causes chronic pleural inflammation [94]. Air pollution particulates can induce oxidative stress in lung cells and an influx of inflammatory cells, contributing to carcinogenesis in the respiratory tract [94]. Industrial solvent and pollutant like benzene can cause bone marrow toxicity and subsequent leukemic changes [94]. Environmental risk factors often operate synergistically with lifestyle factors; for example, heavy smokers exposed to radon have a multiplicative lung cancer risk compared to non-smokers [94]. Mitigating environmental cancer risk requires policy-level interventions to reduce exposure in the population. This includes enforcing clean air and water standards, e.g., limiting industrial emissions of carcinogens, banning asbestos, reducing vehicle exhaust through emissions controls [94]. Urban planning can help by creating green buffers and relocating high-traffic corridors away from residential areas [94]. Workplace regulations are crucial: use of personal protective equipment, fume hoods, and exposure limits for chemicals like benzene or formaldehyde have lowered occupational cancer rates [94]. On an individual level, awareness and testing are important; for instance, homeowners in high-radon areas should test and remediate their houses [94]. Community stress and environmental justice also need addressing; often, marginalized communities face disproportionate pollution and stress; policies to ensure environmental equity can reduce both stress and exposure for those groups [69]. Another key strategy is vaccination and infection control (covered in the next section): by vaccinating against oncogenic viruses and treating infections like H. pylori, certain environmental causes of cancer can be removed [96,97]. Reducing chronic stress in communities through social support and economic improvements may indirectly bolster residents’ resilience to environmental risks by improving overall health and engagement in prevention [36,69]. In summary, while individuals have limited control over many environmental exposures, societal actions to create a cleaner, safer environment have a proven payoff in cancer prevention, evidenced by declines in lung cancers as air quality improves and mesothelioma reductions after asbestos bans [94]. Combining these efforts with stress reduction and healthy living will maximize protection against environmentally linked cancers [36,69].
1.3.11. Mental and Physical Wellbeing
Mental wellbeing is an integral component of overall health, and its absence, e.g., chronic stress, depression, or anxiety can indirectly heighten cancer risk [69]. Chronic psychological stress and certain psychiatric disorders produce physiological changes, often termed an “allostatic load,” that include elevated inflammatory markers, impaired immunity, and dysregulated endocrine function [69]. For instance, long-term depression has been associated with higher levels of CRP and IL-6, indicating a state of persistent inflammation [98]. Such inflammation can contribute to the initiation and progression of cancer by causing DNA damage and promoting a microenvironment that supports tumor growth [36,69]. Additionally, poor mental health can lead to adverse health behaviors: depressed or highly stressed individuals are more likely to smoke, drink excessively, have sedentary lifestyles, and neglect preventive healthcare [36,69]. These behaviors, as detailed above, are risk factors for various cancers [69]. There is evidence that people with severe chronic stress or post-traumatic stress disorder (PTSD) exhibit lower adherence to cancer screening; they might avoid mammograms or colonoscopies due to medical anxiety or hopelessness, resulting in later detection of cancers [69]. Furthermore, mental distress can shorten sleep and elevate cortisol, weakening immune surveillance against nascent tumor cells [36]. Physical wellbeing is often intertwined; chronic mental stress can exacerbate physical conditions like hypertension or ulcerative colitis, which themselves carry cancer risks; for example, long-standing ulcerative colitis raises colorectal cancer risk through constant colon inflammation [36]. Conversely, chronic physical illnesses and pain can cause psychological stress, forming a bidirectional relationship [69]. A person with diabetes and obesity may experience chronic stress, which then hamper their ability to manage those conditions, potentially accelerating complications including cancer [69,84].
While mental ill-health is not typically a direct carcinogen, it creates internal conditions that can facilitate cancer development and worsen outcomes [69]. Population studies have observed modest associations between stress-related psychiatric disorders and higher cancer incidence, particularly for stress-sensitive cancers like lung that is possibly mediated by smoking and some infection-related cancers, suggesting immune effects [69]. Notably, one Swedish cohort found that patients with PTSD had a slightly elevated risk of certain cancers, but much of that association was explained by behavioral and familial factors when controlling for siblings, implying that shared genetics or upbringing which affect both mental health and cancer propensity and unhealthy behaviors were driving the risk more than stress per se [69]. However, cancer progression seems more clearly affected by mental and emotional wellbeing. For example, in cancer patients, depression and lack of social support have been linked to poorer survival, likely due to a mix of biologic effects and reduced treatment adherence [72]. Chronic psychological stress can activate the sympathetic nervous system, leading to tumor angiogenesis and metastasis, thereby potentially accelerating progression in those who already have microscopic cancers [72]. On the positive side, improving mental and physical wellbeing can enhance resilience against cancer [36,69]. Regular physical activity; a boon for mental health via endorphin release and improved mood is also an independent protective factor against cancer, as previously noted [86]. Interventions such as stress management programs, counseling, or antidepressant treatment in those who need it might indirectly reduce cancer risk by promoting healthier lifestyles and reducing inflammation [69]. In one remarkable trial among melanoma patients, a psychological intervention to reduce stress improved immune parameters and was associated with better long-term outcomes [99]. From a public health perspective, promoting mental health, through community programs, access to mental healthcare, and reduction of stigma, is seen as part of comprehensive cancer prevention [69]. Ensuring people have the resources to cope with life stressors, e.g., social support networks, stable housing, employment, can reduce chronic stress loads in the population [69]. Preventive strategies in this domain include incorporating mental health screenings into primary care so that issues like depression can be treated early, workplace wellness initiatives to manage stress and encourage work-life balance and integrating behavioral health into oncology care for high-risk individuals [69]. In conclusion, while mental and physical wellbeing factors are often indirect, they set the stage upon which other carcinogenic factors act [36]. A healthy mind and body strengthen the immune system’s ability to find and destroy emerging cancer cells and foster lifestyles that minimize exposure to known risks [36,69]. By addressing mental health as a core component of public health, we not only improve quality of life but may also achieve modest reductions in cancer incidence and better outcomes for those diagnosed [69].
1.3.12. Vaccination
Vaccines play a pivotal role in preventing cancers caused by infectious agents [96,97]. However, psychological and social factors can influence vaccine uptake [69]. High stress levels or chaotic life circumstances may lead individuals to deprioritize preventive healthcare such as vaccinations [69]. For example, adolescents or adults under significant socioeconomic stress might miss HPV vaccination windows due to limited healthcare engagement or logistical difficulties, indirectly increasing their future cancer risk [69]. Additionally, chronic stress and mistrust can affect health behaviors; someone experiencing high stress or depression could be less likely to follow through with multi-dose vaccine regimens or might avoid medical visits altogether [69]. It’s also worth noting that stress can transiently dampen immune responses; studies have shown that people vaccinated when severely stressed may produce a somewhat weaker antibody response [100]. While this typically does not negate vaccine efficacy, it suggests that stress management might even benefit the immunogenicity of vaccines [100]. Despite these influences, the main issue connecting stress and vaccination is behavioral: ensuring that individuals, even those facing life stresses, receive timely cancer-preventive vaccines [69]. Public health campaigns aim to increase vaccination rates by making access easy and framing vaccination as a routine part of care so that acute stress does not derail it [69].
Several common cancers are caused by infections that are now vaccine-preventable [96,97]. The clearest example is human HPV, a sexually transmitted virus responsible for virtually all cervical cancers and a majority of anal, oropharyngeal, penile, vaginal, and vulvar cancers [97]. HPV vaccines such as the 9-valent HPV vaccine are highly effective in preventing infections with the high-risk HPV strains like HPV16 and 18 that cause these malignancies [97]. Widespread vaccination of adolescents has been shown to drastically reduce the incidence of cervical precancers, projecting large drops in cervical cancer in coming decades [97]. Another example is hepatitis B virus (HBV), which can cause chronic hepatitis and liver cirrhosis that often leads to hepatocellular carcinoma [96]. Universal HBV vaccination in infancy and in high-risk adults has led to marked declines in liver cancer rates in countries with endemic HBV infection [96]. In addition, vaccination against Epstein-Barr virus (EBV) is under development and if successful could reduce nasopharyngeal carcinoma and certain lymphomas [96]. Beyond vaccinations, preventing infection through other means also counts: there is no vaccine available for H. pylori yet, but its eradication with antibiotics in infected individuals reduces stomach cancer risk [96]. Human immunodeficiency virus (HIV), which causes AIDS, indirectly raises risk for several cancers like Kaposi sarcoma and certain lymphomas by immunosuppression; controlling HIV with antiretroviral therapy lowers those cancer risks significantly [96]. All these illustrate that reducing the burden of carcinogenic infections via vaccination or treatment is an effective cancer prevention strategy [96,97]. Stress does not cause these infections, but as mentioned, it could influence whether someone accesses vaccination or adheres to treatment [69]. Ensuring high vaccination coverage requires addressing barriers, some of which are structural such as healthcare access, cost and others behavioral such as misinformation and fear [69]. Many countries have implemented school-based HPV vaccination programs to reach adolescents regardless of individual stress or healthcare utilization [97]. Education campaigns target parents and young adults to increase acceptance of the HPV vaccine by emphasizing cancer prevention [97]. For HBV, global initiatives aim to vaccinate all infants and catch-up vaccinate unprotected adults, e.g., healthcare workers or those in endemic regions [96]. In communities under high stress or with mistrust of the medical system, culturally tailored outreach and combining vaccination with other supportive services can improve uptake [69]. It’s also important to integrate vaccination into routine visits so that even those with other health concerns like mental health issues or chronic stress conditions receive preventative care [69]. When successful, vaccination virtually eliminates certain cancer causes; for instance, Australia is on track to eradicate cervical cancer in the next decade thanks to high HPV vaccine coverage and screening [97]. In summary, vaccines are powerful tools to prevent infection-driven cancers and overcoming psychosocial hurdles to vaccination is an essential public health task [69,97]. Reducing the incidence of HPV, HBV, and other infections can eliminate the chronic inflammation, cell turnover, and genetic damage those infections cause, thereby preventing many cancers before they can even begin [96,97].
1.3.13. Risky Behaviors
Chronic stress, especially during adolescence and early adulthood, can increase propensity for risky behaviors, some of which elevate cancer risk [63,69]. In stressful environments or when coping resources are overwhelmed, individuals may engage in impulsive or sensation-seeking activities as an escape or form of self-regulation [69]. For example, high stress or trauma has been linked to higher likelihood of risky sexual behaviors, such as unprotected sex or multiple partners [69]. This may be due to impaired judgment under stress or using sexual activity as a temporary stress relief without considering safety [69]. Such behaviors can lead to infection with oncogenic viruses like HPV or HIV, both of which are associated with increased cancer risk [96,97]. Similarly, injection drug use can be a risky coping behavior in people facing severe psychological distress or substance use disorders; using non-sterile needles places them at risk for hepatitis B and C viruses and HIV, which are linked to liver cancer and Kaposi sarcoma/lymphomas, respectively [96]. Chronic HCV infection that is often acquired through injection drug use leads to cirrhosis and is a leading cause of liver cancer worldwide alongside HBV [96]. Another behavior is indoor tanning especially among young women facing body image stress, which significantly raises melanoma risk, though this overlaps with the sun exposure category [95]. Even poor diet and alcohol abuse are sometimes termed risky behaviors; those have been addressed earlier as they contribute to cancer via metabolic and inflammatory mechanisms [66,84]. What ties these behaviors together is that they are often adopted in contexts of psychosocial stress, peer influence, or mental health struggles, and they expose individuals to carcinogenic viruses or chemicals [69].
Preventing cancer linked to risky behaviors involves both behavior modification and biomedical interventions [96,97]. Comprehensive sex education and free or accessible condoms can reduce unprotected sexual encounters, thereby lowering HPV and HIV spread [97]. More directly, HPV vaccination of adolescents’ boys and girls provides immunity regardless of future sexual behavior, essentially decoupling the risky behavior from cancer outcome as discussed in the Vaccination section [97]. Similarly, needle exchange programs and opioid substitution therapy help prevent spread of hepatitis C and B among people who inject drugs; these harm reduction approaches have been shown to decrease new infections and thus future liver cancers [96]. Substance abuse treatment and mental health services for at-risk populations (such as trauma survivors) are crucial to addressing underlying stressors that lead to risky practices [69]. For HIV, widespread testing and treatment not only improves individual health but also dramatically lowers transmission, indirectly preventing AIDS-related cancers [96]. Laws and regulations also play a role: many places have age restrictions or bans on indoor tanning to protect youth, and enforcement of driving under influence (DUI) and drug laws can curb some risky behaviors though the relationship to cancer is indirect [95]. Outreach to high-stress communities, such as adolescents in foster care or people in poverty, can provide coping resources and education so that stress does not translate into health-compromising decisions [69]. In medical settings, counseling is key: physicians now routinely counsel patients on safe sex and avoidance of tobacco/alcohol, and there is growing emphasis on screening for social determinants of health like housing instability, abuse, etc. that may signal someone is at risk for unhealthy coping behaviors [69]. In summary, by reducing high-risk behaviors through education, supportive services, and preventive tools like vaccines and needle exchanges, we can interrupt the pathway by which stress and social adversity often lead to infections or exposures that cause cancer [96,97]. These interventions, combined with broader efforts to alleviate socioeconomic and psychological stress, aim to create conditions where individuals are less likely to engage in or suffer from cancer-causing risky behaviors [69].
1.4. Conclusion
This review discusses the link between chronic stress and cancer and provides evidence supporting stress as a promoter of cancer initiation and progression. Mechanistic insights from animal models and some clinical observations underscore how stress and maladaptive responses to stress foster tumor progression, impair immune function, and diminish the efficacy of cancer therapies. Accordingly, many epidemiological studies and clinical trials evaluating stress-reducing interventions have shown modest but significant results. Future studies investigating link between stress and cancer should be tailored to patient-specific stress profiles and should be rigorously tested through multicenter randomized controlled trials. To dissect this complex crosstalk, integrative multi-omics approaches - encompassing genomics, proteomics, and metabolomics - are proposed to identify biomarkers of cancer susceptibility and progression. Particularly, profiling cytokine signatures particularly in peripheral blood cells may facilitate early identification of individuals at heightened risk for stress-induced oncological outcomes. Advancing this line of research may yield novel prognostic tools and therapeutic targets, ultimately enhancing personalized cancer prevention and care. This review proposes that targeted psychosocial and pharmacological interventions can optimally disrupt the stress–cancer axis. Given that majority of cancers are diagnosed in people with 45 years and older, it is necessary to educate young adults about the heightened risk and ways to prevent cancer in time by making lifestyle changes. This review also recommends cancer-related funding to promote and allocate a portion of funding towards cancer prevention-related research.
References
- Hamer, M.; Chida, Y.; Molloy, G.J. Psychological distress and cancer mortality. J. Psychosom. Res. 2009, 66, 255–258. [Google Scholar] [CrossRef]
- Petrinović, S.V.; Milošević, M.S.; Marković, D.; Momčilović, S. Interplay between stress and cancer—A focus on inflammation. Front. Physiol. 2023, 14, 1119095. [Google Scholar] [CrossRef]
- Hanahan, D. and R.A. Weinberg, Hallmarks of cancer: the next generation. Cell, 2011. 144(5): p. 646-74.
- Suri, D.; Vaidya, V.A. The adaptive and maladaptive continuum of stress responses – a hippocampal perspective. Prog. Neurobiol. 2015, 26, 415–442. [Google Scholar] [CrossRef]
- 5.Holmes, T.H. and R.H. Rahe, The Social Readjustment Rating Scale. J Psychosom Res, 1967. 11(2): p. 213-8.
- Chida, Y.; Hamer, M.; Wardle, J.; Steptoe, A. Do stress-related psychosocial factors contribute to cancer incidence and survival? Nat. Clin. Pr. Oncol. 2008, 5, 466–475. [Google Scholar] [CrossRef] [PubMed]
- Blanc-Lapierre, A.; Rousseau, M.-C.; Weiss, D.; El-Zein, M.; Siemiatycki, J.; Parent, M. Lifetime report of perceived stress at work and cancer among men: A case-control study in Montreal, Canada. Prev. Med. 2017, 96, 28–35. [Google Scholar] [CrossRef]
- Yang, T.; Qiao, Y.; Xiang, S.; Li, W.; Gan, Y.; Chen, Y. Work stress and the risk of cancer: A meta-analysis of observational studies. Int. J. Cancer 2019, 144, 2390–2400. [Google Scholar] [CrossRef]
- McDonald, P.G.; Antoni, M.H.; Lutgendorf, S.K.; Cole, S.W.; Dhabhar, F.S.; E Sephton, S.; Stefanek, M.; Sood, A.K. A biobehavioral perspective of tumor biology. . 2005, 5, 520–6. [Google Scholar] [PubMed]
- Moreno-Smith, M.; Lutgendorf, S.K.; Sood, A.K. Impact of Stress on Cancer Metastasis. Futur. Oncol. 2010, 6, 1863–1881. [Google Scholar] [CrossRef]
- Eckerling, A.; Ricon-Becker, I.; Sorski, L.; Sandbank, E.; Ben-Eliyahu, S. Stress and cancer: mechanisms, significance and future directions. Nat. Rev. Cancer 2021, 21, 767–785. [Google Scholar] [CrossRef] [PubMed]
- Sloan, E.K., et al., The sympathetic nervous system induces a metastatic switch in primary breast cancer. Cancer Res, 2010. 70(18): p. 7042-52.
- Lu, D.; Andrae, B.; Valdimarsdóttir, U.; Sundström, K.; Fall, K.; Sparén, P.; Fang, F. Psychologic Distress Is Associated with Cancer-Specific Mortality among Patients with Cervical Cancer. Cancer Res. 2019, 79, 3965–3972. [Google Scholar] [CrossRef]
- Perego, M.; Tyurin, V.A.; Tyurina, Y.Y.; Yellets, J.; Nacarelli, T.; Lin, C.; Nefedova, Y.; Kossenkov, A.; Liu, Q.; Sreedhar, S.; et al. Reactivation of dormant tumor cells by modified lipids derived from stress-activated neutrophils. Sci. Transl. Med. 2020, 12. [Google Scholar] [CrossRef]
- Godoy, L.D.; Rossignoli, M.T.; Delfino-Pereira, P.; Garcia-Cairasco, N.; de Lima Umeoka, E.H. A Comprehensive Overview on Stress Neurobiology: Basic Concepts and Clinical Implications. Front. Behav. Neurosci. 2018, 12, 127. [Google Scholar] [CrossRef] [PubMed]
- McEwen, B.S.; Gianaros, P.J. Central role of the brain in stress and adaptation: Links to socioeconomic status, health, and disease. Ann. New York Acad. Sci. 2010, 1186, 190–222. [Google Scholar] [CrossRef]
- Poller, W.C.; Downey, J.; Mooslechner, A.A.; Khan, N.; Li, L.; Chan, C.T.; McAlpine, C.S.; Xu, C.; Kahles, F.; He, S.; et al. Brain motor and fear circuits regulate leukocytes during acute stress. Nature 2022, 607, 578–584. [Google Scholar] [CrossRef]
- Dhabhar, F.S. Psychological stress and immunoprotection versus immunopathology in the skin. Clin. Dermatol. 2013, 31, 18–30. [Google Scholar] [CrossRef] [PubMed]
- Demers, M.; Suidan, G.L.; Andrews, N.; Martinod, K.; Cabral, J.E.; Wagner, D.D. Solid peripheral tumor leads to systemic inflammation, astrocyte activation and signs of behavioral despair in mice. PLOS ONE 2018, 13, e0207241. [Google Scholar] [CrossRef]
- Dai, S.; Mo, Y.; Wang, Y.; Xiang, B.; Liao, Q.; Zhou, M.; Li, X.; Li, Y.; Xiong, W.; Li, G.; et al. Chronic Stress Promotes Cancer Development. Front. Oncol. 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.X.; Andrzejak, S.E.; Bevel, M.S.; Jones, S.R.; Tingen, M.S. Exploring racial disparities on the association between allostatic load and cancer mortality: A retrospective cohort analysis of NHANES, 1988 through 2019. SSM - Popul. Health 2022, 19, 101185. [Google Scholar] [CrossRef]
- Weinrib, A.Z.; Sephton, S.E.; DeGeest, K.; Penedo, F.; Bender, D.; Zimmerman, B.; Kirschbaum, C.; Sood, A.K.; Lubaroff, D.M.; Lutgendorf, S.K. Diurnal cortisol dysregulation, functional disability, and depression in women with ovarian cancer. Cancer 2010, 116, 4410–4419. [Google Scholar] [CrossRef]
- Tian, W.; Liu, Y.; Cao, C.; Zeng, Y.; Pan, Y.; Liu, X.; Peng, Y.; Wu, F. Chronic Stress: Impacts on Tumor Microenvironment and Implications for Anti-Cancer Treatments. Front. Cell Dev. Biol. 2021, 9. [Google Scholar] [CrossRef]
- Valente, V.B.; Cardoso, D.d.M.; Kayahara, G.M.; Nunes, G.B.; Tjioe, K.C.; Biasoli, É.R.; Miyahara, G.I.; Oliveira, S.H.P.; Mingoti, G.Z.; Bernabé, D.G. Stress hormones promote DNA damage in human oral keratinocytes. Sci. Rep. 2021, 11, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Gidron, Y.; Russ, K.; Tissarchondou, H.; Warner, J. The relation between psychological factors and DNA-damage: A critical review. Biol. Psychol. 2006, 72, 291–304. [Google Scholar] [CrossRef]
- Biometry of the temporomandibular joint]. Orthod Fr, 1990. 61 Pt 1: p. 265-78.
- Zong, C.; Yang, M.; Guo, X.; Ji, W. Chronic restraint stress promotes gastric epithelial malignant transformation by activating the Akt/p53 signaling pathway via ADRB2. Oncol. Lett. 2022, 24, 1–11. [Google Scholar] [CrossRef]
- Lin, Q.; Wang, F.; Yang, R.; Zheng, X.; Gao, H.; Zhang, P. Effect of Chronic Restraint Stress on Human Colorectal Carcinoma Growth in Mice. PLOS ONE 2013, 8, e61435. [Google Scholar] [CrossRef]
- Koh, M.; Takahashi, T.; Kurokawa, Y.; Kobayashi, T.; Saito, T.; Ishida, T.; Serada, S.; Fujimoto, M.; Naka, T.; Wada, N.; et al. Propranolol suppresses gastric cancer cell growth by regulating proliferation and apoptosis. Gastric Cancer 2021, 24, 1037–1049. [Google Scholar] [CrossRef] [PubMed]
- Obeid, E.I.; Conzen, S.D. The role of adrenergic signaling in breast cancer biology. Cancer Biomarkers 2013, 13, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Yap, A.; Lopez-Olivo, M.; Dubowitz, J.; Pratt, G.; Hiller, J.; Gottumukkala, V.; Sloan, E.; Riedel, B.; Schier, R. Effect of beta-blockers on cancer recurrence and survival: a meta-analysis of epidemiological and perioperative studies. Br. J. Anaesth. 2018, 121, 45–57. [Google Scholar] [CrossRef]
- Calvani, M.; Pelon, F.; Comito, G.; Taddei, M.L.; Moretti, S.; Innocenti, S.; Nassini, R.; Gerlini, G.; Borgognoni, L.; Bambi, F.; et al. Norepinephrine promotes tumor microenvironment reactivity through β3-adrenoreceptors during melanoma progression. Oncotarget 2015, 6, 4615–4632. [Google Scholar] [CrossRef]
- Martins, J.M.A.; Rabelo-Santos, S.H.; Westin, M.C.D.A.; Zeferino, L.C. Tumoral and stromal expression of MMP-2, MMP-9, MMP-14, TIMP-1, TIMP-2, and VEGF-A in cervical cancer patient survival: a competing risk analysis. BMC Cancer 2020, 20, 1–11. [Google Scholar] [CrossRef]
- Plummer, M.; de Martel, C.; Vignat, J.; Ferlay, J.; Bray, F.; Franceschi, S. Global burden of cancers attributable to infections in 2012: a synthetic analysis. Lancet Glob. Heal. 2016, 4, e609–e616. [Google Scholar] [CrossRef]
- de Martel, C. , et al., Global burden of cancer attributable to infections in 2018: a worldwide incidence analysis. Lancet Glob Health, 2020. 8(2): p. e180-e190.
- Antoni, M.H.; Lutgendorf, S.K.; Cole, S.W.; Dhabhar, F.S.; Sephton, S.E.; McDonald, P.G.; Stefanek, M.; Sood, A.K. The influence of bio-behavioural factors on tumour biology: pathways and mechanisms. Nat. Rev. Cancer 2006, 6, 240–248. [Google Scholar] [CrossRef]
- Irwin, M.R.; Cole, S.W. Reciprocal regulation of the neural and innate immune systems. Nat. Rev. Immunol. 2011, 11, 625–632. [Google Scholar] [CrossRef]
- Collado-Hidalgo, A.; Sung, C.; Cole, S. Adrenergic inhibition of innate anti-viral response: PKA blockade of Type I interferon gene transcription mediates catecholamine support for HIV-1 replication. Brain, Behav. Immun. 2006, 20, 552–563. [Google Scholar] [CrossRef] [PubMed]
- Cacioppo, J.T.; Kiecolt-Glaser, J.K.; Malarkey, W.B.; Laskowski, B.F.; Rozlog, L.A.; Poehlmann, K.M.; Burleson, M.H.; Glaserb, R. Autonomic and Glucocorticoid Associations with the Steady-State Expression of Latent Epstein–Barr Virus. Horm. Behav. 2002, 42, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Glaser, R.; Friedman, S.B.; Smyth, J.; Ader, R.; Bijur, P.; Brunell, P.; Cohen, N.; Krilov, L.R.; Lifrak, S.T.; Stone, A.; et al. The Differential Impact of Training Stress and Final Examination Stress on Herpesvirus Latency at the United States Military Academy at West Point. Brain, Behav. Immun. 1999, 13, 240–251. [Google Scholar] [CrossRef] [PubMed]
- Fang, F.; Fall, K.; Sparén, P.; Adami, H.-O.; Valdimarsdóttir, H.B.; Lambe, M.; Valdimarsdóttir, U. Risk of Infection-Related Cancers after the Loss of a Child: A Follow-up Study in Sweden. Cancer Res. 2011, 71, 116–122. [Google Scholar] [CrossRef]
- Feng, Z.; Liu, L.; Zhang, C.; Zheng, T.; Wang, J.; Lin, M.; Zhao, Y.; Wang, X.; Levine, A.J.; Hu, W. Chronic restraint stress attenuates p53 function and promotes tumorigenesis. Proc. Natl. Acad. Sci. USA 2012, 109, 7013–7018. [Google Scholar] [CrossRef]
- Saul, A.N.; Oberyszyn, T.M.; Daugherty, C.; Kusewitt, D.; Jones, S.; Jewell, S.; Malarkey, W.B.; Lehman, A.; Lemeshow, S.; Dhabhar, F.S. Chronic Stress and Susceptibility to Skin Cancer. JNCI J. Natl. Cancer Inst. 2005, 97, 1760–1767. [Google Scholar] [CrossRef]
- Renz, B.W.; Takahashi, R.; Tanaka, T.; Macchini, M.; Hayakawa, Y.; Dantes, Z.; Maurer, H.C.; Chen, X.; Jiang, Z.; Westphalen, C.B.; et al. β2 Adrenergic-Neurotrophin Feedforward Loop Promotes Pancreatic Cancer. Cancer Cell 2018, 33, 75–90.e7. [Google Scholar] [CrossRef]
- Hermes, G.L.; Delgado, B.; Tretiakova, M.; Cavigelli, S.A.; Krausz, T.; Conzen, S.D.; McClintock, M.K. Social isolation dysregulates endocrine and behavioral stress while increasing malignant burden of spontaneous mammary tumors. Proc. Natl. Acad. Sci. USA 2009, 106, 22393–22398. [Google Scholar] [CrossRef]
- Hasen, N.S.; O'LEary, K.A.; Auger, A.P.; Schuler, L.A. Social Isolation Reduces Mammary Development, Tumor Incidence, and Expression of Epigenetic Regulators in Wild-type and p53-Heterozygotic Mice. Cancer Prev. Res. 2010, 3, 620–629. [Google Scholar] [CrossRef]
- He, X.Y. , et al., Stressing Out about Cancer Immunotherapy. Cancer Cell, 2019. 36(5): p. 468-470.
- Heidt, T.; Sager, H.B.; Courties, G.; Dutta, P.; Iwamoto, Y.; Zaltsman, A.; Muhlen, C.v.Z.; Bode, C.; Fricchione, G.L.; Denninger, J.; et al. Chronic variable stress activates hematopoietic stem cells. Nat. Med. 2014, 20, 754–758. [Google Scholar] [CrossRef]
- Petrinović, S.V.; Budeč, M.; Marković, D.; Ajtić, O.M.; Jovčić, G.; Milošević, M.; Momčilović, S.; Čokić, V. Nitric oxide-dependent expansion of erythroid progenitors in a murine model of chronic psychological stress. Histochem. Cell Biol. 2020, 153, 457–468. [Google Scholar] [CrossRef]
- Dhabhar, F.S. Effects of stress on immune function: the good, the bad, and the beautiful. Immunol. Res. 2014, 58, 193–210. [Google Scholar] [CrossRef]
- Barrett, T.J.; Corr, E.M.; van Solingen, C.; Schlamp, F.; Brown, E.J.; Koelwyn, G.J.; Lee, A.H.; Shanley, L.C.; Spruill, T.M.; Bozal, F.; et al. Chronic stress primes innate immune responses in mice and humans. Cell Rep. 2021, 36, 109595–109595. [Google Scholar] [CrossRef]
- Liu, X.; Yin, L.; Shen, S.; Hou, Y. Inflammation and cancer: paradoxical roles in tumorigenesis and implications in immunotherapies. Genes Dis. 2023, 10, 151–164. [Google Scholar] [CrossRef] [PubMed]
- Nøst, T.H.; Alcala, K.; Urbarova, I.; Byrne, K.S.; Guida, F.; Sandanger, T.M.; Johansson, M. Systemic inflammation markers and cancer incidence in the UK Biobank. Eur. J. Epidemiology 2021, 36, 841–848. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.S.; Apple, C.G.; Kannan, K.B.; Funk, Z.M.; Plazas, J.M.; Efron, P.A.; Mohr, A.M. Chronic stress induces persistent low-grade inflammation. Am. J. Surg. 2019, 218, 677–683. [Google Scholar] [CrossRef] [PubMed]
- D’orazi, G.; Cordani, M.; Cirone, M. Oncogenic pathways activated by pro-inflammatory cytokines promote mutant p53 stability: clue for novel anticancer therapies. Cell. Mol. Life Sci. 2020, 78, 1853–1860. [Google Scholar] [CrossRef]
- Choi, Y.; Kim, J.K.; Yoo, J.-Y. NFκB and STAT3 synergistically activate the expression of FAT10, a gene counteracting the tumor suppressor p53. Mol. Oncol. 2014, 8, 642–655. [Google Scholar] [CrossRef]
- Kartikasari, A.E.R.; Huertas, C.S.; Mitchell, A.; Plebanski, M. Tumor-Induced Inflammatory Cytokines and the Emerging Diagnostic Devices for Cancer Detection and Prognosis. Front. Oncol. 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Yadav, A. , et al., IL-6 promotes head and neck tumor metastasis by inducing epithelial-mesenchymal transition via the JAK-STAT3-SNAIL signaling pathway. Mol Cancer Res, 2011. 9(12): p. 1658-67.
- Chung, S.S.; Wu, Y.; Okobi, Q.; Adekoya, D.; Atefi, M.; Clarke, O.; Dutta, P.; Vadgama, J.V. Proinflammatory Cytokines IL-6 and TNF-αIncreased Telomerase Activity through NF-κB/STAT1/STAT3 Activation, and Withaferin A Inhibited the Signaling in Colorectal Cancer Cells. Mediat. Inflamm. 2017, 2017, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Weber, M.D.; Godbout, J.P.; Sheridan, J.F. Repeated Social Defeat, Neuroinflammation, and Behavior: Monocytes Carry the Signal. Neuropsychopharmacology 2016, 42, 46–61. [Google Scholar] [CrossRef]
- Ramirez, K., J. Fornaguera-Trias, and J.F. Sheridan, Stress-Induced Microglia Activation and Monocyte Trafficking to the Brain Underlie the Development of Anxiety and Depression. Curr Top Behav Neurosci, 2017. 31: p. 155-172.
- Ulrich-Lai, Y.M.; Fulton, S.; Wilson, M.; Petrovich, G.; Rinaman, L. Stress exposure, food intake and emotional state. 2015, 18, 381–399. [CrossRef]
- Cortes, M.L.; Louzado, J.A.; Oliveira, M.G.; Bezerra, V.M.; Mistro, S.; Medeiros, D.S.; Soares, D.A.; Silva, K.O.; Kochergin, C.N.; Carvalho, V.C.H.S.; et al. Association between perceived stress and health-risk behaviours in workers. Psychol. Heal. Med. 2020, 27, 746–760. [Google Scholar] [CrossRef]
- Jayedi, A.; Emadi, A.; Shab-Bidar, S. Dietary Inflammatory Index and Site-Specific Cancer Risk: A Systematic Review and Dose-Response Meta-Analysis. Adv. Nutr. Int. Rev. J. 2018, 9, 388–403. [Google Scholar] [CrossRef] [PubMed]
- Asensi, M.T.; Napoletano, A.; Sofi, F.; Dinu, M. Low-Grade Inflammation and Ultra-Processed Foods Consumption: A Review. Nutrients 2023, 15, 1546. [Google Scholar] [CrossRef]
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Grosse, Y.; Bianchini, F.; Straif, K. Body Fatness and Cancer — Viewpoint of the IARC Working Group. N. Engl. J. Med. 2016, 375, 794–798. [Google Scholar] [CrossRef]
- Abebe, Z.; Wassie, M.M.; Mekonnen, T.C.; Reynolds, A.C.; Melaku, Y.A. Difference in Gastrointestinal Cancer Risk and Mortality by Dietary Pattern Analysis: A Systematic Review and Meta-Analysis. Nutr. Rev. 2025, 83, e991–e1013. [Google Scholar] [CrossRef]
- Boffetta, P. and M. Hashibe, Alcohol and cancer. Lancet Oncol, 2006. 7(2): p. 149-56.
- Schneiderman, N.; Ironson, G.; Siegel, S.D. Stress and Health: Psychological, Behavioral, and Biological Determinants. Annu. Rev. Clin. Psychol. 2005, 1, 607–628. [Google Scholar] [CrossRef]
- Stults-Kolehmainen, M.A.; Sinha, R. The Effects of Stress on Physical Activity and Exercise. Sports Med. 2014, 44, 81–121. [Google Scholar] [CrossRef]
- Walser, T.; Cui, X.; Yanagawa, J.; Lee, J.M.; Heinrich, E.; Lee, G.; Sharma, S.; Dubinett, S.M. Smoking and Lung Cancer: The Role of Inflammation. Proc. Am. Thorac. Soc. 2008, 5, 811–815. [Google Scholar] [CrossRef]
- Lutgendorf, S.K. and A.K. Sood, Biobehavioral factors and cancer progression: physiological pathways and mechanisms. Psychosom Med, 2011. 73(9): p. 724-30.
- Stubbs, B.; Veronese, N.; Vancampfort, D.; Prina, A.M.; Lin, P.-Y.; Tseng, P.-T.; Evangelou, E.; Solmi, M.; Kohler, C.; Carvalho, A.F.; et al. Perceived stress and smoking across 41 countries: A global perspective across Europe, Africa, Asia and the Americas. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef]
- Islami, F.; Marlow, E.C.; Thomson, B.; McCullough, M.L.; Rumgay, H.; Gapstur, S.M.; Patel, A.V.; Soerjomataram, I.; Jemal, A. Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States, 2019. CA: A Cancer J. Clin. 2024, 74, 405–432. [Google Scholar] [CrossRef]
- Clay, J.M.; Parker, M.O. The role of stress-reactivity, stress-recovery and risky decision-making in psychosocial stress-induced alcohol consumption in social drinkers. Psychopharmacology 2018, 235, 3243–3257. [Google Scholar] [CrossRef] [PubMed]
- Fell, G.L.; Robinson, K.C.; Mao, J.; Woolf, C.J.; Fisher, D.E. Skin β-Endorphin Mediates Addiction to UV Light. Cell 2014, 157, 1527–1534. [Google Scholar] [CrossRef] [PubMed]
- Agar, N.S.; Halliday, G.M.; Barnetson, R.S.; Ananthaswamy, H.N.; Wheeler, M.; Jones, A.M. The basal layer in human squamous tumors harbors more UVA than UVB fingerprint mutations: A role for UVA in human skin carcinogenesis. Proc. Natl. Acad. Sci. USA 2004, 101, 4954–4959. [Google Scholar] [CrossRef]
- Brash, D.E. Sunlight and the onset of skin cancer. Trends Genet. 1997, 13, 410–414. [Google Scholar] [CrossRef]
- Clydesdale, G.J.; Dandie, G.W.; Muller, H.K. Ultraviolet light induced injury: Immunological and inflammatory effects. Immunol. Cell Biol. 2001, 79, 547–568. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, J.; Seidler, A.; Diepgen, T.; Bauer, A. Occupational ultraviolet light exposure increases the risk for the development of cutaneous squamous cell carcinoma: a systematic review and meta-analysis. Br. J. Dermatol. 2011, 164, 291–307. [Google Scholar] [CrossRef]
- Whiteman, D.C.; Whiteman, C.A.; Green, A.C. Childhood sun exposure as a risk factor for melanoma: a systematic review of epidemiologic studies. Cancer Causes Control. 2001, 12, 69–82. [Google Scholar] [CrossRef]
- Geller, A.C.; Rutsch, L.; Kenausis, K.; Selzer, P.; Zhang, Z. Can an hour or two of sun protection education keep the sunburn away? Evaluation of the Environmental Protection Agency's Sunwise School Program. Environ. Health 2003, 2, 13–13. [Google Scholar] [CrossRef] [PubMed]
- Aschbacher, K.; Kornfeld, S.; Picard, M.; Puterman, E.; Havel, P.J.; Stanhope, K.; Lustig, R.H.; Epel, E. Chronic stress increases vulnerability to diet-related abdominal fat, oxidative stress, and metabolic risk. Psychoneuroendocrinology 2014, 46, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Pati, S.; Irfan, W.; Jameel, A.; Ahmed, S.; Shahid, R.K. Obesity and Cancer: A Current Overview of Epidemiology, Pathogenesis, Outcomes, and Management. Cancers 2023, 15, 485. [Google Scholar] [CrossRef]
- McTiernan, A. Mechanisms linking physical activity with cancer. Nat. Rev. Cancer 2008, 8, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Wolin, K.Y.; Yan, Y.; Colditz, G.A.; Lee, I.-M. Physical activity and colon cancer prevention: a meta-analysis. Br. J. Cancer 2009, 100, 611–616. [Google Scholar] [CrossRef]
- Epel, E.S.; Blackburn, E.H.; Lin, J.; Dhabhar, F.S.; Adler, N.E.; Morrow, J.D.; Cawthon, R.M. Accelerated telomere shortening in response to life stress. Proc. Natl. Acad. Sci. USA 2004, 101, 17312–17315. [Google Scholar] [CrossRef]
- Kuchenbaecker, K.B.; Hopper, J.L.; Barnes, D.R.; Phillips, K.-A.; Mooij, T.M.; Roos-Blom, M.-J.; Jervis, S.; Van Leeuwen, F.E.; Milne, R.L.; Andrieu, N.; et al. Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2 Mutation Carriers. JAMA 2017, 317, 2402–2416. [Google Scholar] [CrossRef]
- Singh, S.; Nguyen, H.; Michels, D.; Bazinet, H.; Matkar, P.N.; Liu, Z.; Esene, L.; Adam, M.; Bugyei-Twum, A.; Mebrahtu, E.; et al. BReast CAncer susceptibility gene 2 deficiency exacerbates oxidized LDL-induced DNA damage and endothelial apoptosis. Physiol. Rep. 2020, 8, e14481. [Google Scholar] [CrossRef]
- Singh, A.; Ravendranathan, N.; Frisbee, J.C.; Singh, K.K. Complex Interplay between DNA Damage and Autophagy in Disease and Therapy. Biomolecules 2024, 14, 922. [Google Scholar] [CrossRef]
- Nikfarjam, S.; Singh, K.K. DNA damage response signaling: A common link between cancer and cardiovascular diseases. Cancer Med. 2022, 12, 4380–4404. [Google Scholar] [CrossRef]
- Dedovic, K.; Duchesne, A.; Andrews, J.; Engert, V.; Pruessner, J.C. The brain and the stress axis: The neural correlates of cortisol regulation in response to stress. NeuroImage 2009, 47, 864–871. [Google Scholar] [CrossRef]
- Collaborative Group on Hormonal Factors in Breast, C. , Menarche, menopause, and breast cancer risk: individual participant meta-analysis, including 118 964 women with breast cancer from 117 epidemiological studies. Lancet Oncol, 2012. 13(11): p. 1141-51.
- Loomis, D.; Grosse, Y.; Lauby-Secretan, B.; El Ghissassi, F.; Bouvard, V.; Benbrahim-Tallaa, L.; Guha, N.; Baan, R.; Mattock, H.; Straif, K. The carcinogenicity of outdoor air pollution. Lancet Oncol. 2013, 14, 1262–1263. [Google Scholar] [CrossRef]
- Takagi, H.; Kawai, N.; Umemoto, T. Preoperative Inspiratory Muscle Training and Postoperative Complications. JAMA 2007, 297, 697–699. [Google Scholar] [CrossRef]
- Chang, M.-H.; You, S.-L.; Chen, C.-J.; Liu, C.-J.; Lee, C.-M.; Lin, S.-M.; Chu, H.-C.; Wu, T.-C.; Yang, S.-S.; Kuo, H.-S.; et al. Decreased Incidence of Hepatocellular Carcinoma in Hepatitis B Vaccinees: A 20-Year Follow-up Study. JNCI J. Natl. Cancer Inst. 2009, 101, 1348–1355. [Google Scholar] [CrossRef]
- Falcaro, M.; Castañon, A.; Ndlela, B.; Checchi, M.; Soldan, K.; Lopez-Bernal, J.; Elliss-Brookes, L.; Sasieni, P. The effects of the national HPV vaccination programme in England, UK, on cervical cancer and grade 3 cervical intraepithelial neoplasia incidence: a register-based observational study. Lancet 2021, 398, 2084–2092. [Google Scholar] [CrossRef] [PubMed]
- Howren, M.B.; Lamkin, D.M.; Suls, J. Associations of Depression With C-Reactive Protein, IL-1, and IL-6: A Meta-Analysis. Psychosom. Med. 2009, 71, 171–186. [Google Scholar] [CrossRef] [PubMed]
- Fawzy, F.I. , et al., Malignant melanoma. Effects of an early structured psychiatric intervention, coping, and affective state on recurrence and survival 6 years later. Arch Gen Psychiatry, 1993. 50(9): p. 681-9.
- Glaser, R.; Kiecolt-Glaser, J.K. Stress-induced immune dysfunction: implications for health. Nat. Rev. Immunol. 2005, 5, 243–251. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Chronic stress influences cancer initiation and progression through behavioral, physiological, and biological pathways. Chronic psychosocial stress initiates a cascade of behavioral and environmental changes that increase cancer risk. Stress-induced behaviors include unhealthy dietary patterns, physical inactivity, tobacco use, excessive alcohol consumption, increased sun exposure, and engagement in risky activities such as unprotected sex or intravenous drug use. Stress also contributes to psychological and physical deterioration, including sleep disruption, emotional distress, and weight gain, while indirectly influencing hormonal decisions and reducing adherence to preventive healthcare such as vaccinations. These behavioral and exposure factors lead to a range of biological alterations: persistent systemic inflammation, direct DNA damage and genomic instability, hormonal and metabolic dysregulation, e.g., hyperinsulinemia and elevated estrogen, suppression of immune surveillance, and chronic infections with oncogenic pathogens such as HPV, HBV, and H. pylori. These biological disturbances, individually and in synergy, drive the initiation of tumorigenesis via mutagenesis and loss of genomic integrity, promote tumor growth (through proliferative and anti-apoptotic signaling, and tumor progression via immune evasion, angiogenesis, and tissue invasion. The diagram depicts the interconnected pathways by which chronic stress translates into elevated cancer risk, emphasizing the compounding and multi-factorial nature of stress-mediated carcinogenesis.
Figure 1.
Chronic stress influences cancer initiation and progression through behavioral, physiological, and biological pathways. Chronic psychosocial stress initiates a cascade of behavioral and environmental changes that increase cancer risk. Stress-induced behaviors include unhealthy dietary patterns, physical inactivity, tobacco use, excessive alcohol consumption, increased sun exposure, and engagement in risky activities such as unprotected sex or intravenous drug use. Stress also contributes to psychological and physical deterioration, including sleep disruption, emotional distress, and weight gain, while indirectly influencing hormonal decisions and reducing adherence to preventive healthcare such as vaccinations. These behavioral and exposure factors lead to a range of biological alterations: persistent systemic inflammation, direct DNA damage and genomic instability, hormonal and metabolic dysregulation, e.g., hyperinsulinemia and elevated estrogen, suppression of immune surveillance, and chronic infections with oncogenic pathogens such as HPV, HBV, and H. pylori. These biological disturbances, individually and in synergy, drive the initiation of tumorigenesis via mutagenesis and loss of genomic integrity, promote tumor growth (through proliferative and anti-apoptotic signaling, and tumor progression via immune evasion, angiogenesis, and tissue invasion. The diagram depicts the interconnected pathways by which chronic stress translates into elevated cancer risk, emphasizing the compounding and multi-factorial nature of stress-mediated carcinogenesis.
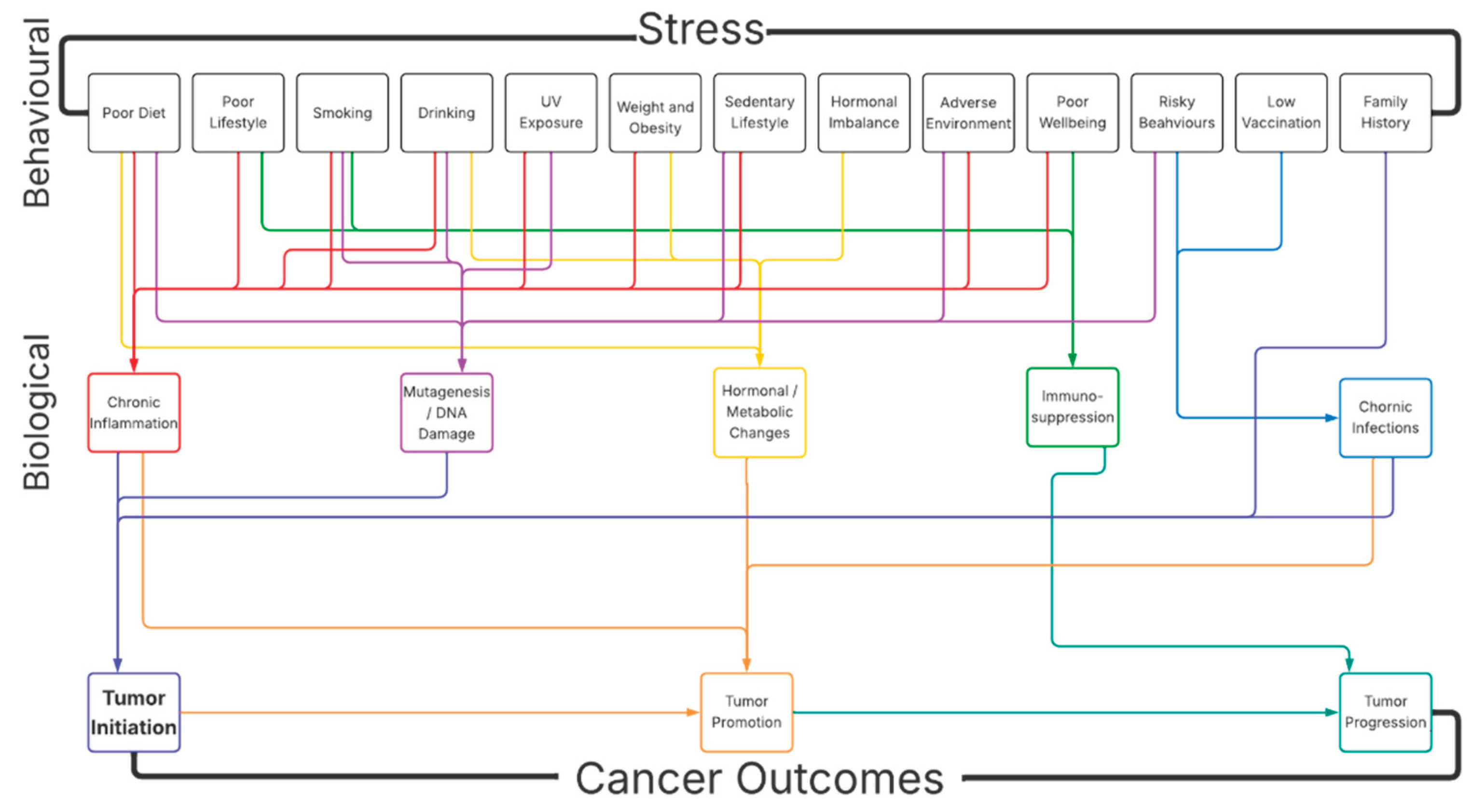
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



