Submitted:
10 October 2025
Posted:
13 October 2025
You are already at the latest version
Abstract
[Objective]: The objective is to assess the effectiveness and safety of doxycycline for treating macrolide-resistant Mycoplasma pneumoniae pneumonia (MRMPP) in pediatric patients across various age ranges, and to explore the value of early switching to doxycycline therapy in children aged <8 years. [Methods] This retrospective cohort study included children diagnosed with MRMPP due to mutations in the 23S rRNA V domain confirmed by sputum PCR, admitted to our hospital from January 2023 to April 2024. The children were grouped by age and treatment regimen: Children aged ≥8 years were divided into the oral doxycycline treatment group (DX group) and the intravenous azithromycin treatment group (AZ1 group); Children aged <8 years were divided into the azithromycin-to-doxycycline switching group (AD group, further subdivided into subgroup AD1 [switching time ≤3 days] and subgroup AD2 [switching time >3 days]) and the intravenous azithromycin group (AZ2 group). The length of hospital stay, duration of fever, time to cough relief, rate of imaging improvement, and adverse drug reactions were compared among the groups. [Results] A total of 173 patients were included, with 42 patients aged ≥8 years (DX group: 27 cases, AZ1 group: 15 cases) and 131 patients aged <8 years (AD group: 52 cases, including AD1 group: 22 cases, AD2 group: 30 cases; AZ2 group: 79 cases). For patients aged ≥8 years, those in the DX group experienced a markedly reduced duration of hospitalization when compared to the AZ1 group (7.11±1.78 days vs. 8.33±0.97 days, P=0.007). Furthermore, the DX group had a shorter period of fever (3.37±1.18 days vs. 4.33±0.72 days, P=0.011) and achieved cough relief more quickly (5.96±1.76 days vs. 7.33±0.97 days, P=0.008). Additionally, the rate of improvement seen in imaging results was greater in the DX group (63.0% vs. 20.0%, P=0.011), and the length of time for glucocorticoid treatment was reduced (2.15±1.81 days vs. 4.07±2.49 days, P=0.013). For patients aged <8 years, the AD group had a shorter hospital stay compared to the AZ2 group (8.12±1.56 days vs. 8.76±1.75 days, P=0.029) and a faster resolution of fever (3.85±1.60 days vs. 4.65±1.51 days, P=0.005). Analysis of subgroups showed that the efficacy metrics for the AD1 group outperformed those of the AD2 group (P<0.05). In the cohort of severe patients (aged <8 years): the ADsp group (n=27) experienced notably shorter hospital stays (9.04±1.61 days vs. 10.93±1.34 days, P<0.001), a reduced duration of fever (4.52±1.87 days vs. 5.73±1.58 days, P=0.032), and a decreased incidence of glucocorticoid administration (74.1% vs. 100%, P=0.038) relative to the AZ2sp group (n=15). Regarding safety, the doxycycline group experienced mild adverse reactions (1 case of vomiting in the ≥8 years group and 2 cases of rash in the <8 years group), which were alleviated after symptomatic treatment, demonstrating good tolerance. [Conclusion] Doxycycline is effective and safe for treating pediatric MRMPP. It can be used as a first-line initial treatment for patients ≥8 years old. For patients <8 years old who do not respond to azithromycin within 72 hours (especially severe cases), switching to doxycycline early is beneficial for shortening the disease course and reducing the risk of complications.
Keywords:
macrolide-resistant
; Mycoplasma pneumoniae
; doxycycline
; azithromycin
1. Introduction
Mycoplasma pneumoniae (MP) is one of the significant pathogens responsible for Community-Acquired Pneumonia (CAP) in children, with infections widely prevalent across the globe, posing a severe threat to child health [1,2]. Macrolides, including azithromycin and erythromycin, have historically been recognized as the primary treatment option for Mycoplasma pneumoniae pneumonia (MPP) because of their remarkable safety profile and effectiveness [3]. However, the widespread use of macrolide antibiotics in various infected patients has led to a continuous rise in the prevalence of Macrolide-resistant Mycoplasma pneumoniae (MRMP) globally, with notable regional differences [4,5]. Systematic reviews and meta-analyses indicate that the highest proportion of MP infections occurs in the Western Pacific region (53.4%), followed by Southeast Asia (9.8%), the Americas (8.4%), and Europe (5.1%). The infection rate among children (37.0%) is significantly higher than that among adults (15.9%), and the proportion of MP infections in CAP patients (38.8%) exceeds that in general respiratory infections (23.0%) [6]. Particularly alarming is the fact that multiple domestic studies have reported that the resistance rate of MP isolated from pediatric patients in certain regions of China has surged to over 90.0% for macrolides [7]. Specifically, the proportion of resistant strains in Shanghai has reached 90.2% [8], in Wuhan it is as high as 96.0% [9], and in Beijing, the mutation rate of resistant genes has soared to 97.1% [7]. This high resistance rate directly leads to a significantly increased risk of treatment failure with macrolides, manifested by persistent fever, prolonged clinical symptoms, and progression in pulmonary imaging, as well as an increased risk of severe pneumonia and extrapulmonary complications, presenting a severe challenge to clinical management [10,11,12,13].
In the face of the challenges posed by MRMP infections, there is an urgent need to find safe and effective alternative treatment options. Tetracycline antibiotics (such as doxycycline and minocycline) and fluoroquinolone antibiotics (such as levofloxacin and moxifloxacin) are considered important choices due to their good antibacterial activity against MRMP [7,14]. Nevertheless, the administration of fluoroquinolones in pediatric patients is severely restricted because of their possible chondrotoxic effects and the associated risk of tendon rupture. They are generally prescribed with caution, only in cases where alternative treatment methods are either ineffective or deemed inappropriate [15,16]. In contrast, doxycycline, as a second-generation tetracycline antibiotic, has advantages such as a broad antibacterial spectrum, good tissue penetration, a long half-life, and high oral bioavailability [17]. It exerts significant antibacterial activity against MP (including resistant strains) by binding to the 30S subunit of bacterial ribosomes and inhibiting protein synthesis [18,19]. To date, there are no reported cases of MRMP developing resistance to tetracycline antibiotics [20]. Moreover, doxycycline has the capability to inhibit the secretion of various inflammatory mediators, such as tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6), thereby diminishing the inflammatory response induced by infections [21,22,23]. Despite the traditional view that tetracycline antibiotics may affect dental development in children under the age of 8 (leading to tooth discoloration and enamel hypoplasia), existing evidence from evidence-based medicine indicates that the risk of significant tooth staining from short-term doxycycline treatment (typically ≤21 days) in children is extremely low. It has been recommended by the American Academy of Pediatrics for the treatment of specific severe infections [16,24,25]. In recent years, multiple clinical studies and meta-analyses have also suggested that doxycycline has good efficacy and acceptable safety in treating MRMP infections in children and adolescents [26,27].
However, the current evidence regarding the use of doxycycline in the treatment of pediatric macrolide-resistant Mycoplasma pneumoniae pneumonia (MRMPP) remains significantly limited: 1) Most studies included a mixed age range, lacking systematic comparisons of efficacy and safety specifically targeting different age groups (especially a strict distinction between children ≥8 years and <8 years); 2) For the critical group of children <8 years, doxycycline is considered an off-label medication, and its optimal administration strategy (such as the timing of switching) and its impact on severe cases in this age group have not been fully elucidated. Therefore, this study aims to evaluate the efficacy and safety of doxycycline in the treatment of MRMPP in children of different age groups through a retrospective analysis of clinical data, with the intention of providing more optimized treatment options and reference for clinical practice.
2. Materials and Methods
2.1. Study Subjects
This study is a retrospective analysis that included hospitalized patients with CAP at the Seventh Affiliated Hospital of Sun Yat-sen University (Shenzhen) from January 2023 to April 2024, all of whom had no underlying diseases. All patients exhibited typical clinical manifestations of pneumonia (fever, cough) and imaging abnormalities [28]. Sputum specimens were collected upon admission and sent to the Guangzhou KingMed Diagnostics Group for polymerase chain reaction (PCR) testing for MP to confirm the infection. Exclusion criteria included: (1) concomitant congenital diseases (such as congenital heart disease, genetic disorders, congenital pulmonary hypoplasia, immunodeficiency diseases); (2) concomitant chronic diseases (such as tuberculosis, asthma, hematological diseases, chronic liver disease, chronic kidney disease); (3) infections with pathogens other than MP (viruses, bacteria, etc.); (4) prior treatment with macrolides or doxycycline before admission; (5) withdrawal from treatment midway or missing clinical data. The study protocol was approved by the Medical Ethics Committee of our hospital (Approval No.: KY-2025-026-01). The off-label use of doxycycline for patients under 8 years old has been double-filed with the Pharmacy Management and Pharmacotherapy Committee and the Medical Ethics Committee of our hospital. Before treatment, the researchers fully informed the legal guardians of all patients about the treatment plan, potential risks, and benefits, and obtained their understanding and signed informed consent for off-label drug use.
3. Methods
In this research, participants received either azithromycin via intravenous infusion or doxycycline orally. The intravenous administration of azithromycin was established at a dosage of 10 mg/kg, provided once each day, whereas the oral dosage of doxycycline was set at 2.2 mg/kg, given every 12 hours, in strict adherence to the guidelines specified in the medication instructions [29]. The choice of primary antibiotics was determined by the attending pediatrician based on the patient's condition. Prior to microbiological diagnosis and resistance testing: for suspected MPP patients aged ≥8 years with a clear history of MRMP exposure, initial treatment was with oral doxycycline; for suspected MPP patients of all ages (regardless of prior resistance exposure history), intravenous azithromycin was the preferred initial treatment. After obtaining laboratory evidence of MRMP infection (including identification of relevant resistance mutation sites): some patients had their treatment adjusted from intravenous azithromycin to oral doxycycline based on test results; another group of patients continued intravenous azithromycin treatment due to the guardians' refusal to use doxycycline.
Patients were divided into two age groups: those aged ≥8 years and those aged <8 years. The age cutoff of 8 years was established based on the recommendations regarding the use of doxycycline in the 'Guidelines for the Diagnosis and Treatment of Mycoplasma Pneumonia in Children (2023 Edition)' issued by the National Health Commission [15]. According to the treatment regimens, patients aged ≥8 years were further categorized into the oral doxycycline group (DX group) and the intravenous azithromycin group (AZ1 group); patients aged <8 years were categorized into two groups: one receiving intravenous azithromycin transitioned to oral doxycycline (AD group) and the other receiving only intravenous azithromycin (AZ2 group). The AD group was additionally divided into two subgroups according to the length of intravenous azithromycin treatment: the AD1 subgroup, consisting of patients who received treatment for three days or fewer, and the AD2 subgroup, which included those who underwent treatment for more than three days. The three-day cutoff was chosen based on the suggested duration for macrolide antibiotics mentioned in the previously referenced guidelines [15]. Additionally, patients with severe pneumonia aged <8 years were separately classified into the ADsp group and the AZ2sp group.
3.1. Data Collection
Clinical data were collected retrospectively from the medical records of patients in this study. This included demographic details, the duration of hospitalization, the length of fever and cough (encompassing the days leading up to treatment with azithromycin or doxycycline, as well as the time needed for resolution of fever and relief from cough post-treatment), laboratory test results obtained upon admission, findings from chest imaging, and any adverse reactions related to treatment. All patients underwent chest imaging examinations before the start of treatment and were re-examined when their temperature returned to normal and clinical symptoms stabilized, recording the time of imaging improvement. The chest imaging results were independently reviewed by two radiologists, who classified the findings into pulmonary consolidation, interstitial lesions, mixed lesions, and the presence of pleural effusion. If the area of absorption of the imaging lesions was >30%, it was determined to be an improvement.
3.2. Statistical Analysis
Statistical analysis was performed using SPSS 25.0 software. Measurement data conforming to a normal distribution were expressed as mean ± standard deviation (?X±S). Normality and homogeneity of variance tests were conducted first. Should the data meet the criteria for normal distribution and variance homogeneity, comparisons between two groups would be carried out using Student's t-test. In contrast, for multiple group comparisons, one-way ANOVA would be utilized. On the other hand, when these assumptions are not satisfied, non-parametric rank-sum tests like the Mann-Whitney U test or the Kruskal-Wallis H test would be applied. Frequencies (percentages) [n (%)] were used to present categorical data, with inter-group comparisons being assessed through the χ² test. A p-value below 0.05 was deemed statistically significant.
4. Results
4.1. Demographic and Clinical Characteristics
From January 2023 to April 2024, a total of 590 patients who were hospitalized due to clinically suspected MPP and underwent sputum PCR testing for MP were included in the study. Among them, 292 patients tested positive for MP PCR, accounting for 49.49% of the total number of tests (292/590). In the positive cases, 192 cases (65.75%, 192/292) exhibited point mutations in the 23S rRNA V domain. The main mutation types were A2063G (183 cases) and A2064G (9 cases), with the A2063G mutation accounting for 95.31% of the mutated cases (183/192). Analysis showed that the peak incidence of MPP occurred in the autumn and winter seasons; similarly, the peak incidence of MRMPP was also observed in the autumn and winter. In contrast, the peak incidence of macrolide-susceptible Mycoplasma pneumoniae pneumonia (MSMPP) occurred in the summer and autumn. Figure 1 illustrates the seasonal distribution characteristics of MPP.
This research involved 173 patients following the removal of 19 cases due to specific exclusion criteria established for MRMPP patients. When categorized by age, there were patients aged ≥8 years (42 cases), subdivided into the DX group (27 cases) and the AZ1 group (15 cases). In contrast, patients aged <8 years totalled 131 cases, consisting of the AD group (52 cases, which included 22 cases from the AD1 subgroup and 30 cases from the AD2 subgroup) and the AZ2 group (comprising 79 cases). Additionally, among patients aged <8 years, a severe subgroup was delineated based on the severity of the condition: the ADsp group (27 cases) and the AZ2sp group (15 cases). The enrollment and grouping process of the study subjects is shown in Figure 2, while the demographic and clinical characteristics are presented in Table 1.
For patients aged ≥8 years, the DX group (n=27) had an average age of 9.00±1.33 years, compared to 9.20±1.47 years for the AZ1 group (n=15). The male representation in these groups was 59.3% (16/27) in the DX group and 53.3% (8/15) in the AZ1 group. All patients exhibited symptoms of fever and cough. Prior to treatment, the duration of fever (DX group: 3.37±1.57 days; AZ1 group: 3.40±1.29 days) and the duration of cough (DX group: 5.67±1.75 days; AZ1 group: 5.20±1.52 days) were compared between the two groups, and no statistically significant differences were found (P>0.05). Imaging findings (such as pulmonary consolidation, interstitial changes, mixed lesions, and pleural effusion) and laboratory indicators (including white blood cell count, percentage of neutrophils, platelet count, hemoglobin, C-reactive protein, procalcitonin, lactate dehydrogenase, and erythrocyte sedimentation rate) also showed no statistically significant differences between the two groups (P>0.05). The proportion of severe pneumonia caused by MRMP in the two groups was similar [DX group: 44.4% (12/27); AZ1 group: 40.0% (6/15)], with no statistically significant difference (P=1.000).
For patients aged <8 years, the AD group's average age (n=52) was 5.75±1.29 years, in contrast to the AZ2 group's average (n=79), which was 5.33±1.30 years. The proportion of males was 53.8% (28/52) in the AD group and 49.4% (39/79) in the AZ2 group. All patients exhibited fever and cough symptoms. Before treatment, the duration of fever (AD group: 3.27±1.65 days; AZ2 group: 3.14±1.68 days) and cough (AD group: 5.08±2.35 days; AZ2 group: 5.73±2.11 days) did not show any statistically significant differences between the two groups (P>0.05). In a similar vein, no statistically significant variations were observed in the imaging results and laboratory metrics between the two groups (P>0.05). Nonetheless, there was a notable difference in the rates of severe pneumonia resulting from MRMP infection between the two groups [AD group: 51.9% (27/52); AZ2 group: 19.0% (15/79)], with the AD group exhibiting a significantly higher percentage compared to the AZ2 group, a difference that reached statistical significance (P<0.001).
In the AD group of patients (stratified by doxycycline conversion time), the average age of the AD1 group (n=22) and the AD2 group (n=30) was 5.50±1.50 years and 5.93±1.11 years, respectively, with male proportions of 40.9% (9/22) and 63.3% (19/30). Before treatment, the duration of fever in both groups (AD1 group: 3.23±1.37 days; AD2 group: 3.30±1.86 days) and the duration of cough (AD1 group: 5.64±2.17 days; AD2 group: 4.67±2.44 days) showed no statistically significant differences (P>0.05). The imaging findings and laboratory indicators also did not show statistically significant differences between the two groups (P>0.05). The proportion of severe pneumonia in the two groups [AD1 group: 54.5% (12/22); AD2 group: 50.0% (15/30)] was similar, with no statistically significant difference (P=0.785). A comparison of the baseline clinical characteristics between the AD1 and AD2 patient groups is presented in Table 2.
In patients aged <8 years suffering from severe pneumonia attributed to MRMP, the mean ages for the ADsp cohort (n=27) and the AZ2sp cohort (n=15) were found to be 5.74±1.37 years and 4.80±2.04 years, respectively. Additionally, the male proportions in these groups were 59.3% (16/27) and 33.3% (5/15). Before treatment, there were no statistically significant differences (P>0.05) between the two groups in terms of the duration of fever, duration of cough, imaging findings, and related laboratory indicators. A detailed comparison of baseline characteristics before treatment in patients aged <8 years with MRMP severe pneumonia can be found in Table 3.
4.2. Comparisons of Clinical Courses After Therapy
In patients aged ≥8 years, the average length of hospital stay in the DX group (7.11±1.78 days) was significantly shorter than that in the AZ1 group (8.33±0.97 days) (P=0.007). After treatment, the duration of fever resolution in the DX group (3.37±1.18 days) and the time to cough relief (5.96±1.76 days) were both significantly shorter than those in the AZ1 group (4.33±0.72 days and 7.33±0.97 days, respectively) (P<0.05). Furthermore, the percentage of patients experiencing fever resolution within 72 hours, as well as the rate of enhancement in chest imaging for the DX group, was considerably greater than that observed in the AZ1 group (P<0.05). The usage rate of glucocorticoids showed no statistically significant difference between the two groups [DX group: 74.1% (20/27); AZ1 group: 80.0% (12/15), P=1.000], but the number of days of glucocorticoid use in the DX group (2.15±1.81 days) was significantly lower than that in the AZ1 group (4.07±2.49 days) (P=0.013). Additionally, the rate of immunoglobulin administration in the DX group [14.8% (4/27)] was notably lesser compared to that in the AZ1 group [46.7% (7/15)] (P=0.034). Figure 3 illustrates the comparison of hospital stay duration, fever length, and the time taken for cough relief between the DX and AZ1 groups. A detailed comparison of the clinical efficacy between the two groups is presented in Table 4.
In patients aged <8 years, the average hospitalization duration for the AD group (8.12±1.56 days) was significantly shorter than that of the AZ2 group (8.76±1.75 days) (P=0.029). After treatment, the duration of fever resolution in the AD group (3.85±1.60 days) was significantly shorter than that in the AZ2 group (4.65±1.51 days) (P=0.005). Furthermore, the proportion of patients achieving defervescence within 72 hours was significantly higher in the AD group than in the AZ2 group (P < 0.001). The glucocorticoid usage rate was significantly lower in the AD group [75.0% (39/52)] than in the AZ2 group [91.1% (72/79)] (P < 0.05). However, there were no statistically significant differences between the two groups in the time to cough resolution after treatment, the rate of radiographic improvement, the duration of glucocorticoid use, or the rate of immunoglobulin use (P > 0.05). These results may be attributed to the higher proportion of severe pneumonia in the AD group compared to the AZ2 group. Comparisons of hospitalization duration, time to defervescence after treatment, and time to cough resolution between the AD and AZ2 groups are shown in Figure 4. A detailed comparison of the clinical efficacy between the AD and AZ2 groups is presented in Table 5.
Among patients aged <8 years who have severe pneumonia due to MRMP infection, the ADsp group demonstrated a significantly better performance compared to the AZ2sp group regarding hospital stay duration, time taken for defervescence post-treatment, duration until cough relief, improvement rates in chest imaging, usage rates of glucocorticoids, and immunoglobulin administration, all showing statistically significant differences (P<0.05). Figure 5 illustrates a comparison between the ADsp and AZ2sp groups regarding hospital duration, time taken for defervescence post-treatment, and the duration until cough relief occurs. A detailed comparison of the efficacy between the two groups is presented in Table 6.
This study analyzes the clinical efficacy of transitioning to doxycycline treatment at different stages in patients with MRMPP aged <8 years. In terms of efficacy indicators, the length of hospital stay in the AD1 group (7.50±1.10 days), time to defervescence after treatment (3.23±1.31 days), and time to cough relief (6.50±1.10 days) were significantly shorter than those in the AD2 group (8.57±1.70 days, 4.30±1.66 days, and 7.47±1.81 days, respectively) (P<0.05); the proportion of patients in the AD1 group who achieved defervescence within 72 hours [77.3% (17/22)] was significantly higher than that in the AD2 group [46.7% (14/30)] (P=0.044); the improvement rate of chest imaging in the AD1 group [81.8% (18/22)] was significantly higher than that in the AD2 group [43.3% (13/30)] (P=0.009); the usage rate of glucocorticoids in the AD1 group [59.1% (13/22)] and the usage rate of immunoglobulin [9.1% (2/22)] were significantly lower than those in the AD2 group [86.7% (26/30) and 36.7% (11/30), respectively] (P=0.049), and the number of days of glucocorticoid use in the AD1 group (3.14±2.78 days) was significantly less than that in the AD2 group (4.57±2.22 days) (P=0.045). The comparison of hospitalization duration, time to fever resolution after treatment, and time to cough relief between the AD1 group and the AD2 group is illustrated in Figure 6. A detailed comparison of the efficacy between the two groups can be found in Table 7.
In patients treated with intravenous azithromycin, the following adverse reactions were recorded: 3 cases of abdominal pain, 2 cases of vomiting, and 2 cases of rash. All patients treated with oral doxycycline exhibited good tolerance. During the treatment period, 1 patient aged ≥8 years experienced vomiting, and 2 patients aged <8 years developed a rash. After symptomatic treatment, the aforementioned symptoms were alleviated and did not recur. During the treatment period and the following follow-up, no negative reactions associated with oral doxycycline were noted in the other patients.
5. Discussion
This study systematically evaluated the efficacy and safety of doxycycline in treating pediatric MRMPP through age stratification (≥8 years vs. <8 years). The core findings indicate that doxycycline significantly outperforms azithromycin as a first-line treatment in patients aged ≥8 years; for patients aged <8 years, an early switch to doxycycline (within 3 days of intravenous azithromycin treatment) can significantly improve clinical outcomes, particularly benefiting critically ill patients. These results provide important evidence for optimizing treatment strategies for pediatric MRMPP.
MP is a minimal prokaryote lacking a cell wall that adheres to respiratory epithelial cells, releasing CARDS toxins and reactive oxygen species that directly damage cells and activate host immune responses, leading to inflammatory reactions and lung tissue injury [30]. Among school-aged children and adolescents, pneumonia cases caused by MP account for as much as 10%-40% of total cases, with significant regional and seasonal variations in its epidemiology [31,32]. For instance, in Japan, MP infections peak during the summer and autumn seasons, with a macrolide resistance rate as high as 86.3% [33]; in the United States, peaks are commonly observed in the autumn and winter, with a resistance rate of approximately 10% [34]; while in Beijing, China, the peak period is concentrated from August to January of the following year, with a macrolide resistance rate exceeding 90% [35]. This study also observed that the overall incidence of MPP peaks in the autumn and winter, and found differences in the peak periods of MRMPP and MSMPP: MSMPP cases peak more often in the summer and autumn, whereas MRMPP is more commonly seen in the autumn and winter. This seasonal difference provides a new perspective for understanding the epidemiological characteristics of MPP.
Resistance to macrolide antibiotics in MP primarily arises from specific point mutations within the 23S ribosomal RNA (rRNA) gene. Among these mutations, the A2063G alteration is the most frequently observed variant. The A2064G mutation closely follows, also contributing to the resistance mechanism [36]. These mutations can lead to modifications in the ribosomal target site, preventing macrolide antibiotics from effectively binding to the ribosome, thereby diminishing their antibacterial efficacy [19]. Research has demonstrated that clinical isolates harboring mutations at the A2063 or A2064 loci exhibit high levels of resistance to both 14-membered and 15-membered macrolides, with a minimum inhibitory concentration (MIC) of ≥32 μg/ml. Remarkably, the A2063G variation can provide significantly elevated resistance to 14-membered, 15-membered, and ketolide antibiotics, whereas only a moderate degree of resistance is noted for 16-membered macrolides [37]. A multi-center epidemiological study conducted in Beijing from 2015 to 2020 revealed that the A2063G mutation accounted for 99.0% of MRMP infections [35]. From 2020 to 2022, the predominant strain of MPP in children in Wuhan was type P1, with a resistance rate to macrolides reaching 96%, all attributed to the A2063G mutation [9]. The findings of this study are highly consistent with the aforementioned reports, with the A2063G mutation accounting for 95.31%. The elevated resistance rate directly escalates the risk of treatment failure with macrolide antibiotics, necessitating the exploration of safe and effective alternatives.
In this study, patients aged ≥8 years in the doxycycline group (DX group) demonstrated significant advantages compared to those in the azithromycin group (AZ1 group): reduced duration of hospitalizations (7.11 ± 1.78 days vs. 8.33 ± 0.97 days, P = 0.007), quicker resolution of fever (3.37 ± 1.18 days vs. 4.33 ± 0.72 days, P = 0.011), and a greater percentage of radiological improvement (63.0% vs. 20.0%, P = 0.011). Furthermore, the DX group significantly reduced the duration of glucocorticoid use and the rate of immunoglobulin administration. These findings are consistent with previous studies and support doxycycline as the preferred treatment for MRMPP patients in this age group [20,26].
The findings of this study hold significant clinical implications for the critical population of patients aged <8 years, who require particularly cautious medication management. Although the proportion of severe pneumonia was significantly higher in the azithromycin-to-doxycycline switch group (AD group) than in the azithromycin-only group (AZ2 group) (51.9% vs. 19.0%, P < 0.001), the AD group still demonstrated a shorter length of hospital stay (8.12 ± 1.56 days vs. 8.76 ± 1.75 days, P = 0.029), a shorter time to defervescence (3.85 ± 1.60 days vs. 4.65 ± 1.51 days, P = 0.005), and a lower glucocorticoid use rate (75.0% vs. 91.1%, P = 0.015). Crucially, subgroup analysis revealed that early treatment switching (intravenous azithromycin ≤ 3 days, AD1 group) further optimized efficacy compared to late switching (> 3 days, AD2 group), manifested as a shorter hospitalization duration (7.50 ± 1.10 days vs. 8.57 ± 1.70 days, P = 0.013), a reduced time to defervescence (3.23 ± 1.31 days vs. 4.30 ± 1.66 days, P = 0.015), and a higher radiographic improvement rate (81.8% vs. 43.3%, P = 0.009). In severe patients aged <8 years (ADsp group), the benefits of early switching to doxycycline were even more pronounced, not only significantly shortening the hospital stay (9.04 ± 1.61 days vs. 10.93 ± 1.34 days, P < 0.001) and the time to symptom resolution but also significantly reducing the rates of glucocorticoid and immunoglobulin use. Therefore, for patients aged <8 years with MRMPP, especially severe cases, early switching to doxycycline therapy within 72 hours if the initial azithromycin treatment shows inadequate response is a crucial strategy for improving prognosis.
The significant efficacy of doxycycline can be attributed to its dual mechanism of action. On one hand, doxycycline effectively inhibits protein synthesis by blocking the bacterial ribosomal 30S subunit, demonstrating precise antibacterial activity against MRMP, including strains harboring common resistance mutations such as A2063G [27,38]. Conversely, doxycycline has the ability to inhibit the secretion of important inflammatory mediators like TNF-α and IL-6, thus mitigating the intense inflammatory reactions occurring in the lungs [23]. This synergistic effect of antibacterial and anti-inflammatory actions may be a key reason why the doxycycline group significantly outperformed the azithromycin group in terms of rapid symptom relief, promoting radiological absorption, and reducing the need for supportive therapy.
Concerning the safety of doxycycline in patients aged <8 years, the findings of this study, along with evidence-based data, suggest that the risks associated with short-course treatment (ranging from 7 to 10 days in this study) are manageable. Traditional concerns have primarily focused on its potential impact on tooth development (such as tooth discoloration and enamel hypoplasia). However, substantial evidence suggests that the risk of significant tooth staining from short-course doxycycline therapy (≤21 days) is extremely low [39,40]. Population pharmacokinetic studies also support the safety of doxycycline in children aged 2–8 years, demonstrating pharmacokinetic profiles similar to those in older children, with body weight being the primary influencing factor [41]. According to the American Academy of Pediatrics (AAP), when the advantages surpass the risks, short-term doxycycline is applicable for treating severe infections in all pediatric age categories [42]. In this study, all patients receiving doxycycline tolerated it well, with only three mild adverse events recorded (one vomiting in the ≥8-year group and two rashes in the <8-year group). These resolved with symptomatic treatment and did not recur, consistent with the safety profile reported in the literature [40,43]. Although doxycycline may cause adverse effects such as gastrointestinal discomfort or photosensitivity, these are generally mild and manageable [44,45]. Furthermore, desensitization protocols can be implemented for patients allergic to doxycycline [46].
This research presents various limitations. First, the retrospective nature of the study could introduce selection bias; for instance, the percentage of severe cases in the AD group aged <8 years is considerably greater than that found in the AZ2 group. Although baseline characteristics (such as age, gender, duration of symptoms, laboratory indicators, and imaging findings) did not show significant differences between groups, not all potential confounding factors could be fully controlled. Second, the sample size is relatively small (a total of 173 cases, with only 42 cases in the ≥8 years old group), which may weaken the statistical power of the tests. Third, the long-term safety (such as the potential long-term impact on dental development) was not assessed, although short-term adverse reactions were mild and consistent with previous reports. Fourth, the resistance detection methods have limitations, as they are based solely on sputum PCR testing for common mutation sites in 23S rRNA (A2063G/A2064G), which may overlook resistant strains caused by other rare resistance mechanisms. Finally, the duration of the study was relatively short (from January 2023 to April 2024), which may make it difficult to fully reflect the long-term epidemiological trends or seasonal variations of the disease. Future research should focus on conducting prospective randomized controlled trials (RCTs), particularly paying attention to the efficacy and timing of conversion in younger age groups, expanding the sample size to improve the reliability of inferences, systematically conducting long-term follow-up to assess the long-term safety of doxycycline, and exploring combination treatment strategies with anti-inflammatory drugs such as corticosteroids, in order to further improve the treatment outcomes of severe MRMPP.
6. Conclusions
This study confirms that doxycycline has significant therapeutic advantages for patients with MRMPP. For patients aged ≥8 years, it is recommended as the first-line initial treatment drug. For patients <8 years old, if the initial treatment with azithromycin shows inadequate efficacy within 72 hours (especially in severe cases), timely conversion to doxycycline treatment should be implemented. This strategy helps to rapidly control the infection and reduce the inflammatory response, thereby shortening the course of the disease, decreasing complications, and reducing dependence on supportive treatment, ultimately contributing to the improvement of patients' clinical prognosis.
Author Contributions
Conception and Design: Jiawen Zhu,Jiezhen Mo and Xiaojing Mao; Extraction of Data: Jiawen Zhu, Tianqi Liang and Junbin Huang; Drafting the Article: Jiawen Zhu; Revising It for Intellectual Content: Jiawen Zhu, Hongman Xue, and Chun Chen; Final Approval of the Completed Article: Xiaoyi Fang. All authors read and approved the final manuscript.
Funding
The authors did not receive support from any organization for the submitted work.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The Ethical Committee of the Seventh Affiliated Hospital of Sun Yat-Sen University approved the study. Since this study was non-interventional and retrospective in nature, the ethical committee waived the need for written informed consent provided by patients or their legal guardians.
Consent for Publication
Not applicable.
Competing Interests
The authors declare no conflict of interest.
References
- Oishi T, Ouchi K: Recent Trends in the Epidemiology, Diagnosis, and Treatment of Macrolide-Resistant Mycoplasma pneumoniae. Journal of Clinical Medicine 2022, 11, 1–8.
- Gu H, Zhu Y, Zhou Y, Huang T, Zhang S, Zhao D, Liu F: LncRNA MALAT1 Affects Mycoplasma pneumoniae Pneumonia via NF-κB Regulation. Frontiers in Cell and Developmental Biology 2020, 8, 1–12.
- Beeton ML, Zhang X-S, Uldum SA, Bébéar C, Dumke R, Gullsby K, Ieven M, Loens K, Nir-Paz R, Pereyre S et al: Mycoplasma pneumoniae infections, 11 countries in Europe and Israel, 2011 to 2016. Eurosurveillance 2020, 25, 1–13.
- Lee H, Yun KW, Lee HJ, Choi EH: Antimicrobial therapy of macrolide-resistantMycoplasma pneumoniaepneumonia in children. Expert Review of Anti-infective Therapy 2017, 16, 23–34.
- Tanaka T, Oishi T, Miyata I, Wakabayashi S, Kono M, Ono S, Kato A, Fukuda Y, Saito A, Kondo E et al: Macrolide-Resistant Mycoplasma pneumoniae Infection, Japan, 2008–2015. Emerging Infectious Diseases 2017, 23, 1703–1706. [CrossRef] [PubMed]
- Kim K, Jung S, Kim M, Park S, Yang H-J, Lee E: Global Trends in the Proportion of Macrolide-Resistant Mycoplasma pneumoniae Infections. JAMA Network Open 2022, 5, 1–12.
- Yan C, Xue G-H, Zhao H-Q, Feng Y-L, Cui J-H, Yuan J: Current status of Mycoplasma pneumoniae infection in China. World Journal of Pediatrics 2024, 20, 1–4. [CrossRef]
- Zhou Y, Shan Y, Cui Y, Shi J, Wang F, Miao H, Wang C, Zhang Y: Characteristics and Outcome of Severe Mycoplasma pneumoniae Pneumonia Admitted to PICU in Shanghai: A Retrospective Cohort Study. Critical Care Explorations 2021, 3, 1–8.
- Xu M, Li Y, Shi Y, Liu H, Tong X, Ma L, Gao J, Du Q, Du H, Liu D et al: Molecular epidemiology of Mycoplasma pneumoniae pneumonia in children, Wuhan, 2020–2022. BMC Microbiology 2024, 24, 1–11.
- Yang H-J: Benefits and risks of therapeutic alternatives for macrolide resistant Mycoplasma pneumoniae pneumonia in children. Korean Journal of Pediatrics 2019, 62, 199–205. [CrossRef]
- Chen Y-C, Hsu W-Y, Chang T-H: Macrolide-Resistant Mycoplasma pneumoniae Infections in Pediatric Community-Acquired Pneumonia. Emerging Infectious Diseases 2020, 26, 1382–1391. [CrossRef]
- Lanata MM, Wang H, Everhart K, Moore-Clingenpeel M, Ramilo O, Leber A: Macrolide-Resistant Mycoplasma pneumoniae Infections in Children, Ohio, USA. Emerging Infectious Diseases 2021, 27, 1588–1597. [CrossRef]
- Wang Y-S, Zhou Y-L, Bai G-N, Li S-X, Xu D, Chen L-N, Chen X, Dong X-Y, Fu H-M, Fu Z et al: Expert consensus on the diagnosis and treatment of macrolide-resistant Mycoplasma pneumoniae pneumonia in children. World Journal of Pediatrics 2024, 20, 901–914. [CrossRef]
- Cheng J, Liu Y, Zhang G, Tan L, Luo Z: Azithromycin Effectiveness in Children with Mutated Mycoplasma Pneumoniae Pneumonia. Infection and Drug Resistance 2024, 17, 2933–2942. [CrossRef]
- Commission NH: Guidelines for the Diagnosis and Treatment of Mycoplasma Pneumoniae Pneumonia in Children.
- (2023 Edition). Infect Dis Info 2023, 36, 291–297.
- Ahn JG, Cho H-K, Li D, Choi M, Lee J, Eun B-W, Jo DS, Park SE, Choi EH, Yang H-J, Kim KH: Efficacy of tetracyclines and fluoroquinolones for the treatment of macrolide-refractory Mycoplasma pneumoniae pneumonia in children: a systematic review and meta-analysis. BMC Infectious Diseases 2021, 21, 1–10.
- Cunha TA, Sibley CM, Ristuccia AM: Doxycycline. Therapeutic Drug Monitoring 1982, 4, 115–135.
- Zhu H, Wen Q, Bhangu SK, Ashokkumar M, Cavalieri F: Sonosynthesis of nanobiotics with antimicrobial and antioxidant properties. Ultrasonics Sonochemistry 2022, 86, 1–8.
- Lee H, Choi YY, Sohn YJ, Kim YK, Han MS, Yun KW, Kim K, Park JY, Choi JH, Cho EY, Choi EH: Clinical Efficacy of Doxycycline for Treatment of Macrolide-Resistant Mycoplasma pneumoniae Pneumonia in Children. Antibiotics 2021, 10, 1–11.
- Chen Y, Zhang Y, Tang Q-N, Shi H-B: Efficacy of doxycycline therapy for macrolide-resistant Mycoplasma pneumoniae pneumonia in children at different periods. Italian Journal of Pediatrics 2024, 50, 1–8.
- Fredeking TM, Zavala-Castro JE, González-Martínez P, Moguel-Rodríguez W, Sanchez EC, Foster MJ, Diaz-Quijano FA: Dengue Patients Treated with Doxycycline Showed Lower Mortality Associated to a Reduction in IL-6 and TNF Levels. Recent Patents on Anti-Infective Drug Discovery 2015, 10, 51–58. [CrossRef] [PubMed]
- Singh B, Ghosh N, Saha D, Sarkar S, Bhattacharyya P, Chaudhury K: Effect of doxycyline in chronic obstructive pulmonary disease - An exploratory study. Pulmonary Pharmacology & Therapeutics 2019, 58, 1–9.
- Patel A, Khande H, Periasamy H, Mokale S: Immunomodulatory Effect of Doxycycline Ameliorates Systemic and Pulmonary Inflammation in a Murine Polymicrobial Sepsis Model. Inflammation 2020, 43, 1035–1043. [CrossRef] [PubMed]
- Zhu Z, Yu Q, Qi G, Yang J, Ni Y, Ruan W, Fang L: Tigecycline-Induced Tooth Discoloration in Children Younger than Eight Years. Antimicrobial Agents and Chemotherapy 2021, 65, 1–4.
- Kim SJ, Kim EH, Lee M, Baek JY, Lee JY, Shin JH, Lim SM, Kim MY, Jung I, Ahn JG et al: Risk of Dental Discoloration and Enamel Dysplasia in Children Exposed to Tetracycline and Its Derivatives. Yonsei Medical Journal 2022, 63, 1113–1120. [CrossRef]
- Bolormaa E, Park JY, Choe YJ, Kang CR, Choe SA, Mylonakis E: Treatment of Macrolide-resistant Mycoplasma pneumoniae Pneumonia in Children: A Meta-analysis of Macrolides Versus Tetracyclines. Pediatric Infectious Disease Journal 2024, 44, 200–206.
- Song X, Zhou N, Lu S, Gu C, Qiao X: New-generation tetracyclines for severe macrolide-resistant Mycoplasma pneumoniae pneumonia in children: a retrospective analysis. BMC Infectious Diseases 2024, 24, 1–10.
- Meyer Sauteur PM: Childhood community-acquired pneumonia. European Journal of Pediatrics 2023, 183, 1129–1136. [CrossRef] [PubMed]
- The Subspecialty Group of Respiratory tSoP, Chinese Medical Association; China National Clinical Research Center of Respiratory Diseases; the Editorial Board, Chinese Journal of Pediatrics: Evidence-based guideline for the diagnosis and treatment of Mycoplasma pneumoniae pneumonia in children (2023). Chin J Pediatr 2024, 62, 1137–1144.
- Kumar S, Kumar S: Mycoplasma pneumoniae: Among the smallest bacterial pathogens with great clinical significance in children. Indian Journal of Medical Microbiology 2023, 46, 1–5.
- Jiang T-t, Sun L, Wang T-y, Qi H, Tang H, Wang Y-c, Han Q, Shi X-q, Bi J, Jiao W-w, Shen Ad: The clinical significance of macrolide resistance in pediatric Mycoplasma pneumoniae infection during COVID-19 pandemic. Frontiers in Cellular and Infection Microbiology 2023, 13, 01–09.
- Song Z, Jia G, Luo G, Han C, Zhang B, Wang X: Global research trends of Mycoplasma pneumoniae pneumonia in children: a bibliometric analysis. Frontiers in Pediatrics 2023, 11, 01–16.
- Akashi Y, Hayashi D, Suzuki H, Shiigai M, Kanemoto K, Notake S, Ishiodori T, Ishikawa H, Imai H: Clinical features and seasonal variations in the prevalence of macrolide-resistant Mycoplasma pneumoniae. Journal of General and Family Medicine 2018, 19, 191–197. [CrossRef]
- Rothstein TE, Cunningham SA, Rieke RA, Mainella JM, Mutchler MM, Patel R: Macrolide Resistance in Mycoplasma pneumoniae, Midwestern United States, 2014 to 2021. Antimicrob Agents Chemother 2022, 66, 1–5.
- Wang X, Li M, Luo M, Luo Q, Kang L, Xie H, Wang Y, Yu X, Li A, Dong M et al: Mycoplasma pneumoniae.
- triggers pneumonia epidemic in autumn and winter in Beijing: a multicentre, population-based epidemiological study between 2015 and 2020. Emerging Microbes & Infections 2022, 11, 1508–1517. [CrossRef] [PubMed]
- Zhao F, Li J, Liu J, Guan X, Gong J, Liu L, He L, Meng F, Zhang J: Antimicrobial susceptibility and molecular characteristics of Mycoplasma pneumoniae isolates across different regions of China. Antimicrobial Resistance & Infection Control 2019, 8, 1–8.
- Morozumi M, Ubukata K, Takahashi T: Macrolide-resistant Mycoplasma pneumoniae: characteristics of isolates and clinical aspects of community-acquired pneumonia. Journal of Infection and Chemotherapy 2010, 16, 78–86. [CrossRef]
- Gianvecchio C, Lozano NA, Henderson C, Kalhori P, Bullivant A, Valencia A, Su L, Bello G, Wong M, Cook E et al: Variation in Mutant Prevention Concentrations. Frontiers in Microbiology 2019, 10, 1–9.
- Stultz JS, Eiland LS: Doxycycline and Tooth Discoloration in Children: Changing of Recommendations Based on Evidence of Safety. Annals of Pharmacotherapy 2019, 53, 1162–1166. [CrossRef]
- Qiao Y, Chen Y, Wang Q, Liu J, Guo X, Gu Q, Ding P, Zhang H, Mei H: Safety profiles of doxycycline, minocycline, and tigecycline in pediatric patients: a real-world pharmacovigilance analysis based on the FAERS database. Frontiers in Pharmacology 2024, 15, 01–14.
- Thompson EJ, Wu H, Melloni C, Balevic S, Sullivan JE, Laughon M, Clark KM, Kalra R, Mendley S, Payne EH et al: Population Pharmacokinetics of Doxycycline in Children. Antimicrobial Agents and Chemotherapy 2019, 63, 1–12.
- Kuriakose K, Pettit AC, Schmitz J, Moncayo A, Bloch KC: Assessment of Risk Factors and Outcomes of Severe Ehrlichiosis Infection. JAMA Network Open 2020, 3, 1–12.
- Zhao Q, Sang X, Gao D, Zhang Z, Xuan A, Peng W: Efficacy and safety of doxycycline for severe Mycoplasma pneumoniae pneumonia in pediatric patients. Clinical and Experimental Medicine 2025, 25, 1–18.
- Velušček M, Bajrović FF, Strle F, Stupica D: Doxycycline-induced photosensitivity in patients treated for erythema migrans. BMC Infectious Diseases 2018, 18, 1–5.
- Dou W, Liu X, An P, Zuo W, Zhang B: Real-world safety profile of tetracyclines in children younger than 8 years old: an analysis of FAERS database and review of case report. Expert Opinion on Drug Safety 2024, 23, 885–892. [CrossRef] [PubMed]
- Maciag MC, Ward SL, O’Connell AE, Broyles AD: Hypersensitivity to tetracyclines. Annals of Allergy, Asthma & Immunology 2020, 124, 589–593.
Figure 1.
Seasonal distribution of MPP cases stratified by macrolide susceptibility.
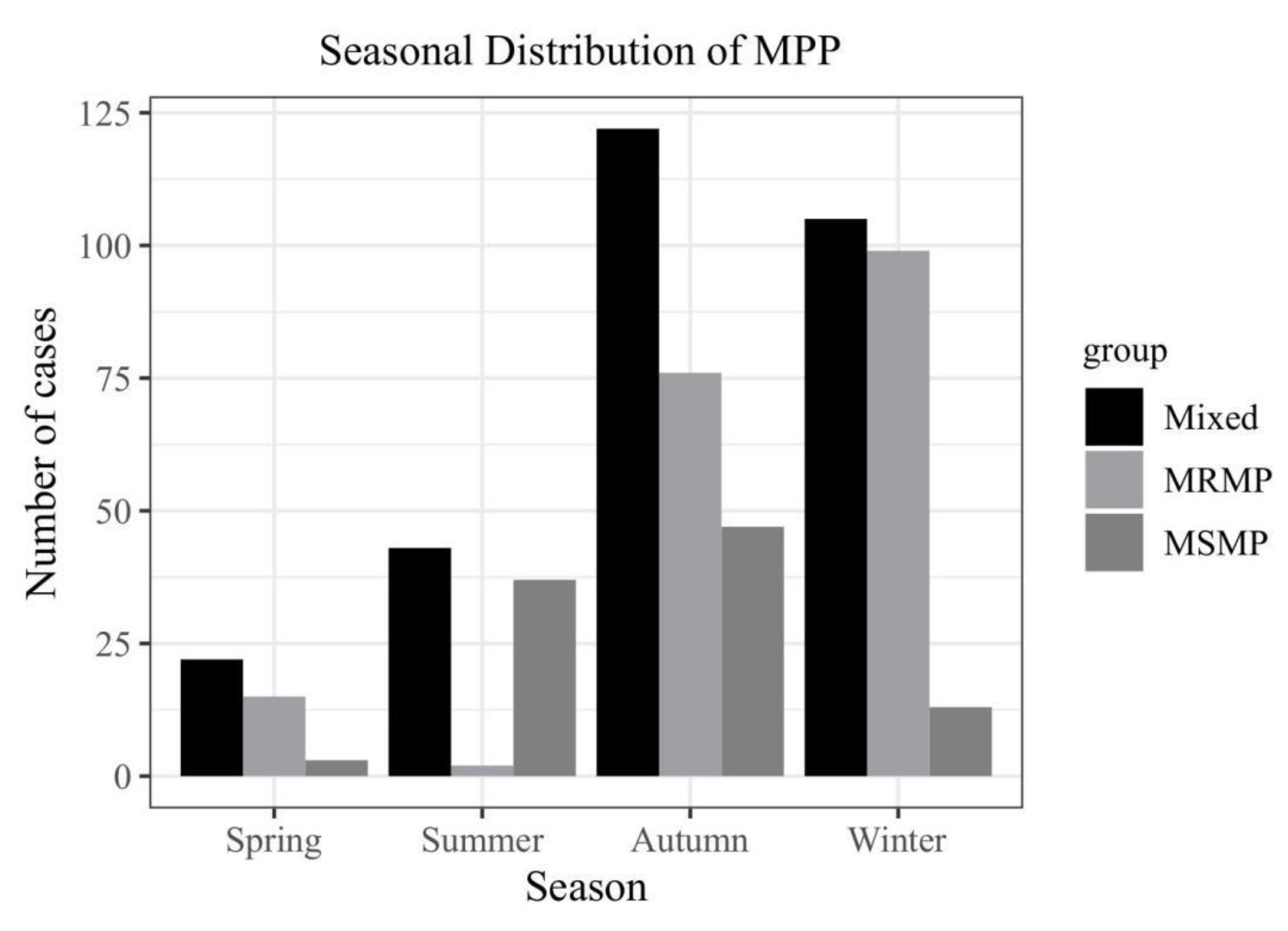
Figure 2.
Flow diagram of study participant recruitment and classification.
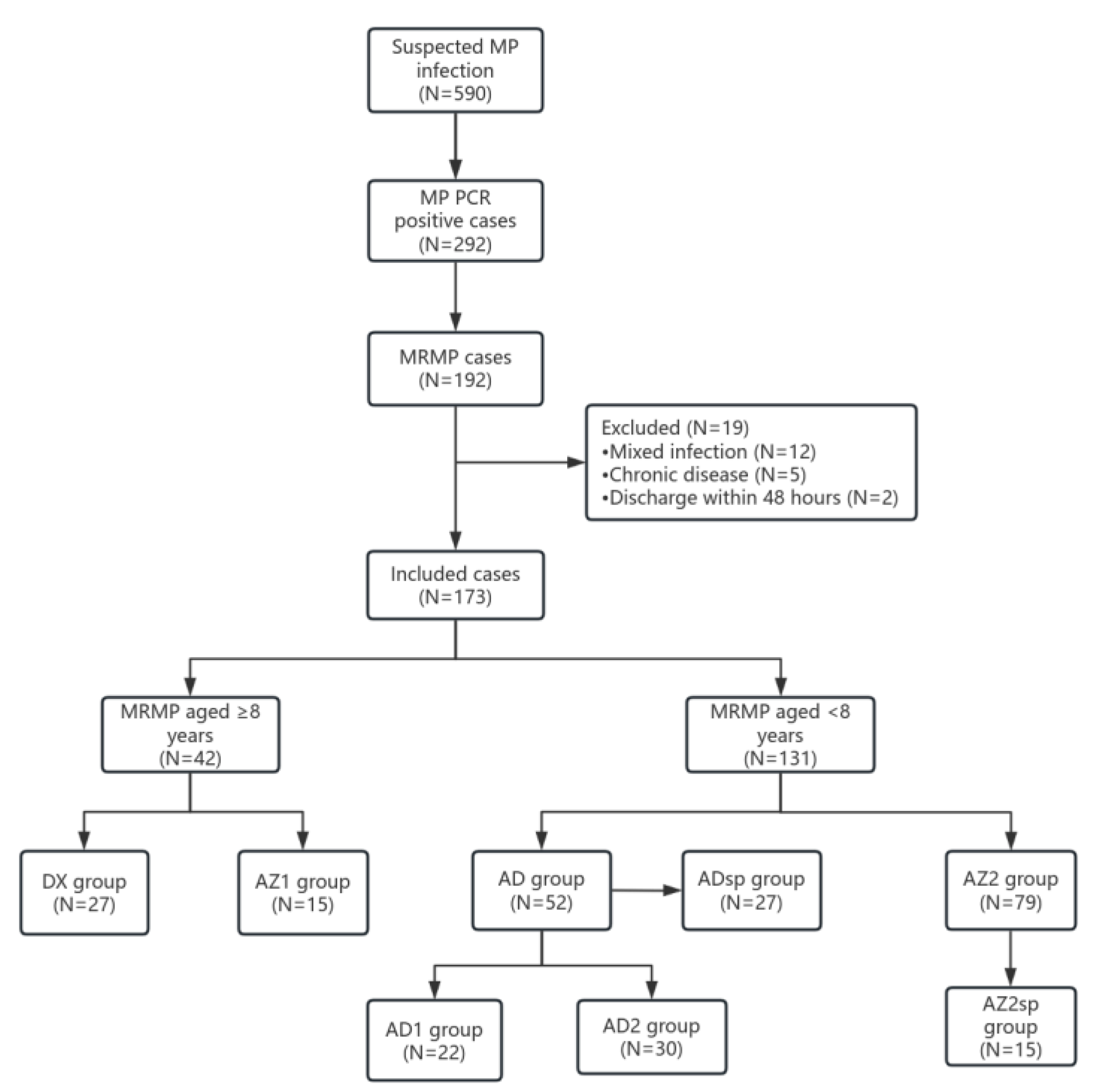
Figure 3.
Comparative analysis of clinical outcomes between DX and AZ1 groups in ≥8-year-old MRMPP patients. (A) Hospitalization duration (days); (B) Time to defervescence post-treatment (days); (C) Cough improvement duration post-treatment (days).
Figure 3.
Comparative analysis of clinical outcomes between DX and AZ1 groups in ≥8-year-old MRMPP patients. (A) Hospitalization duration (days); (B) Time to defervescence post-treatment (days); (C) Cough improvement duration post-treatment (days).
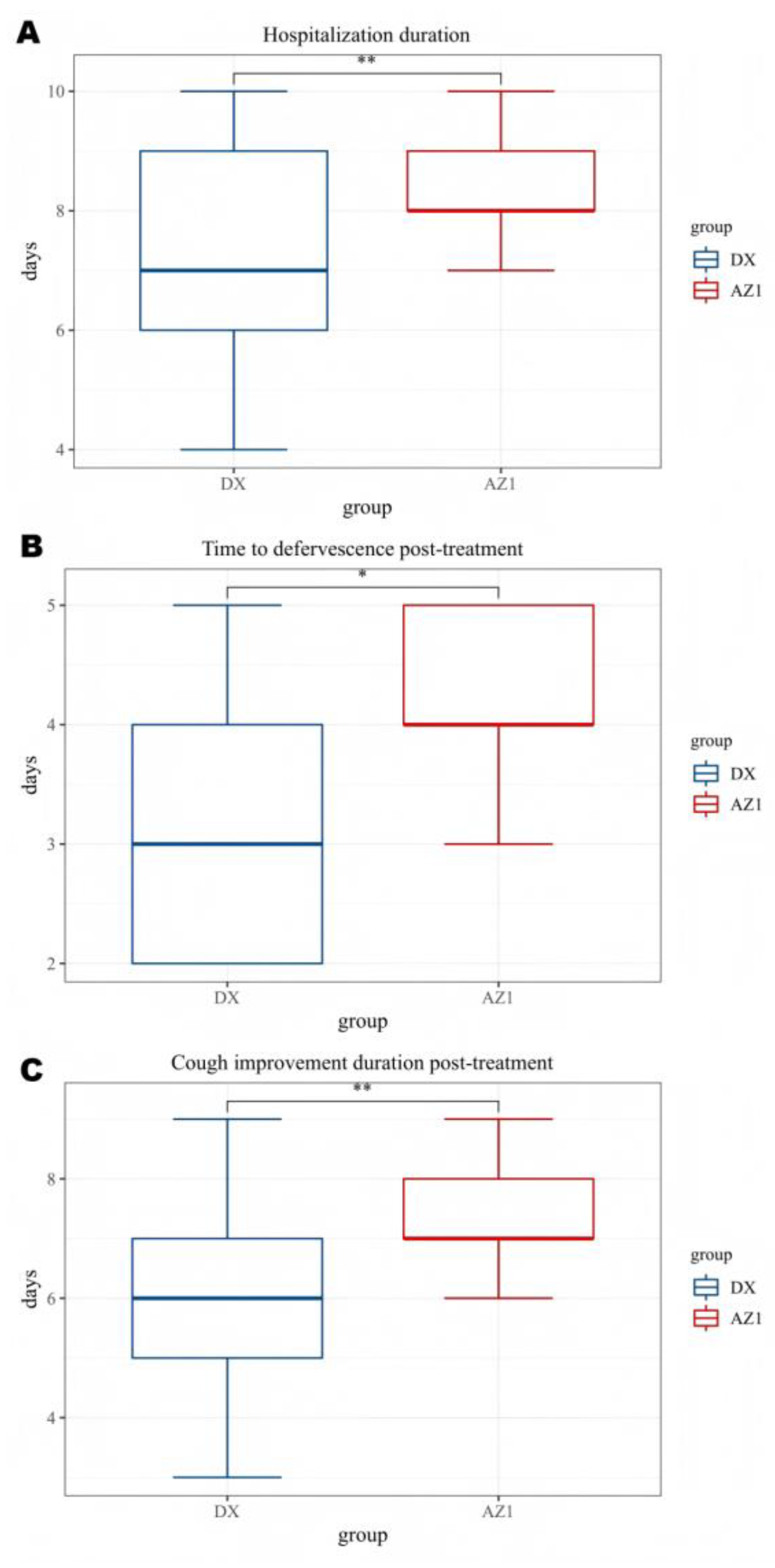
Figure 4.
Comparative clinical outcomes between AD and AZ2 groups in <8-year-old MRMPP patients. (A) Hospitalization duration (days); (B) Time to defervescence post-treatment (days); (C) Cough improvement duration post-treatment (days).
Figure 4.
Comparative clinical outcomes between AD and AZ2 groups in <8-year-old MRMPP patients. (A) Hospitalization duration (days); (B) Time to defervescence post-treatment (days); (C) Cough improvement duration post-treatment (days).
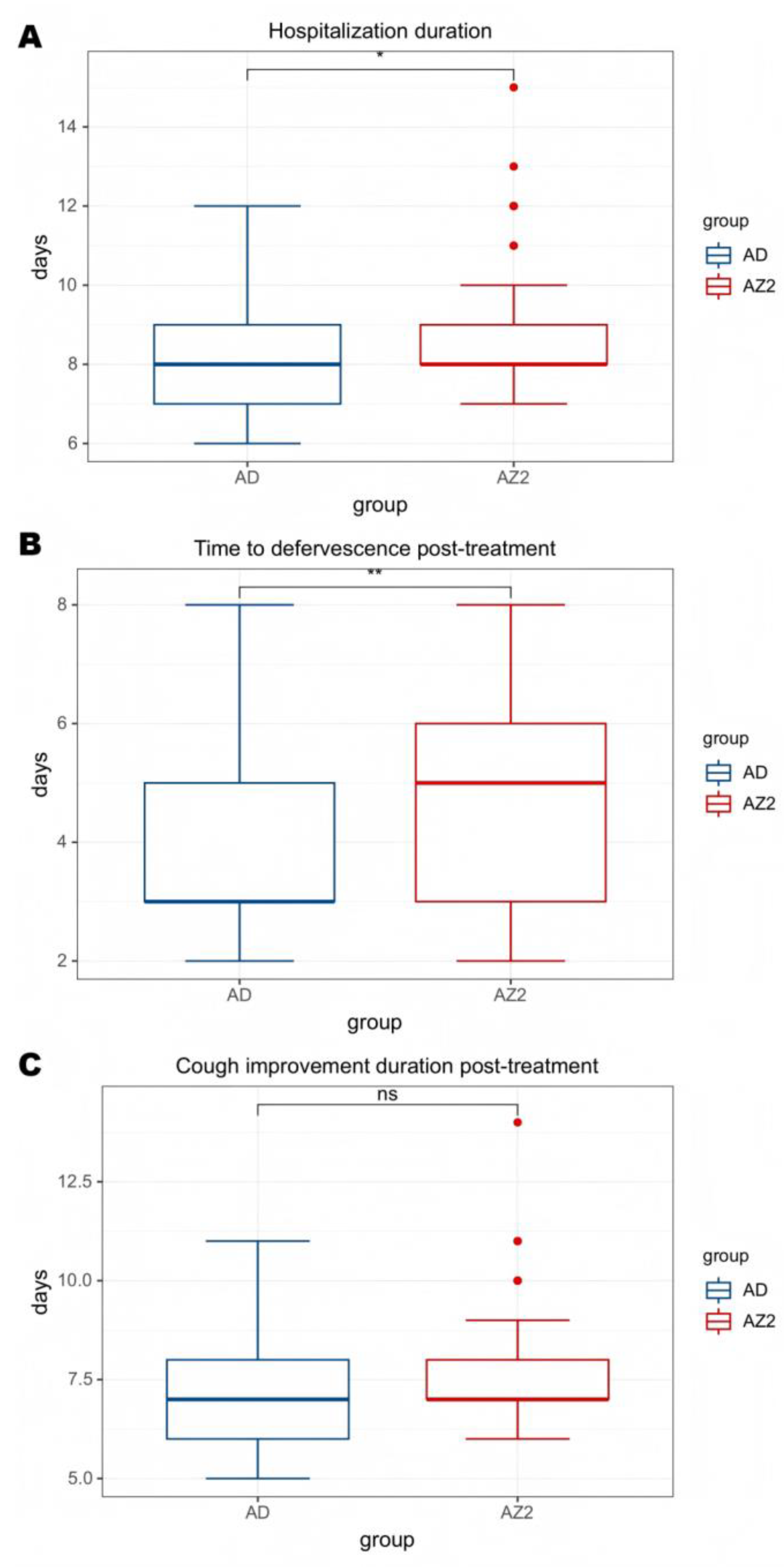
Figure 5.
Comparative outcomes in severe MRMPP patients <8 years: ADsp vs AZ2sp. (A) Hospitalization duration (days); (B) Time to defervescence post-treatment (days); (C) Cough resolution time post-treatment (days).
Figure 5.
Comparative outcomes in severe MRMPP patients <8 years: ADsp vs AZ2sp. (A) Hospitalization duration (days); (B) Time to defervescence post-treatment (days); (C) Cough resolution time post-treatment (days).
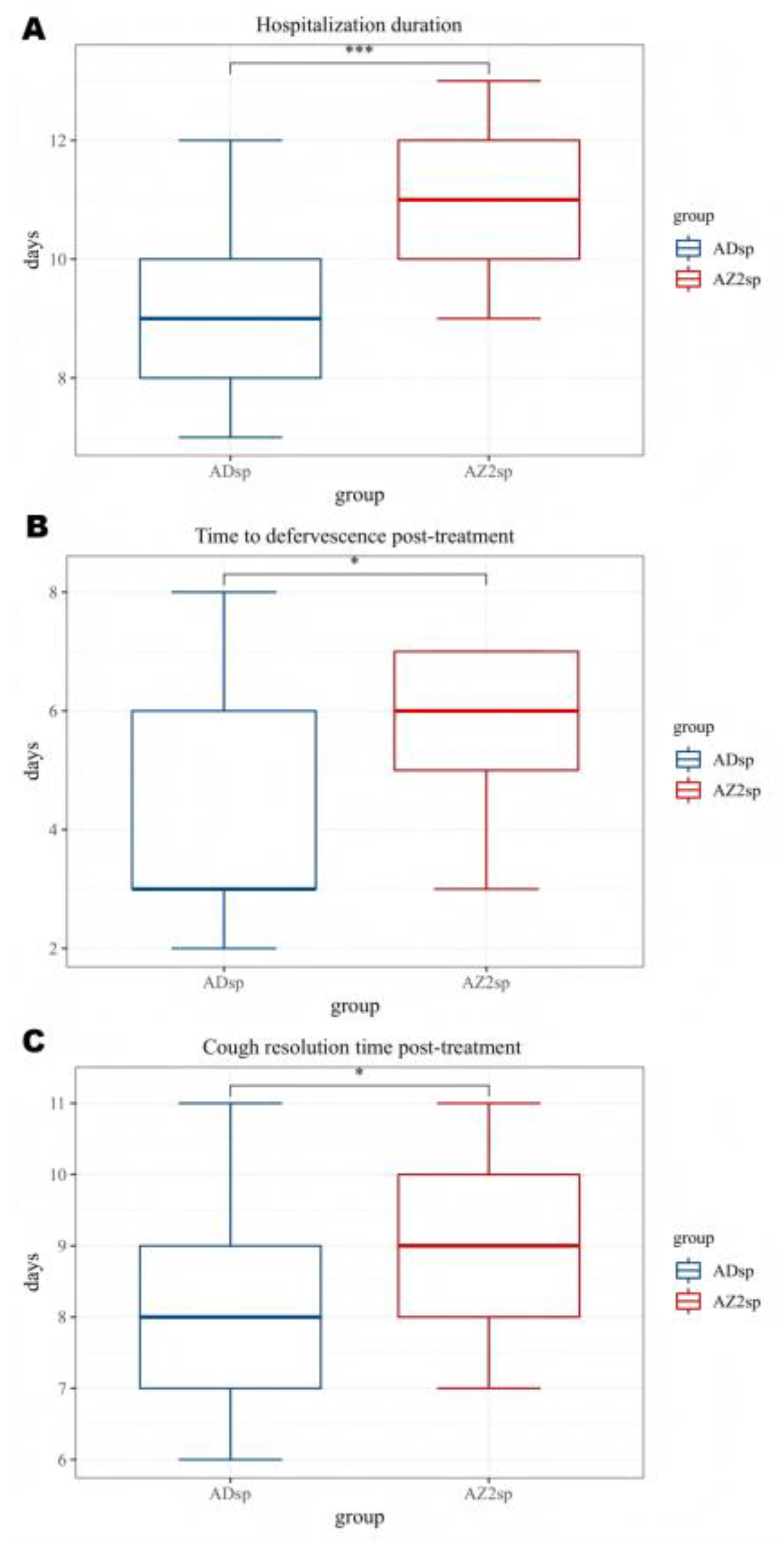
Figure 6.
Comparison of clinical outcomes between the AD1 and AD2 groups. (A) Hospitalization duration (days); (B) Time to defervescence post-treatment (days); (C) Cough resolution time post-treatment (days).
Figure 6.
Comparison of clinical outcomes between the AD1 and AD2 groups. (A) Hospitalization duration (days); (B) Time to defervescence post-treatment (days); (C) Cough resolution time post-treatment (days).
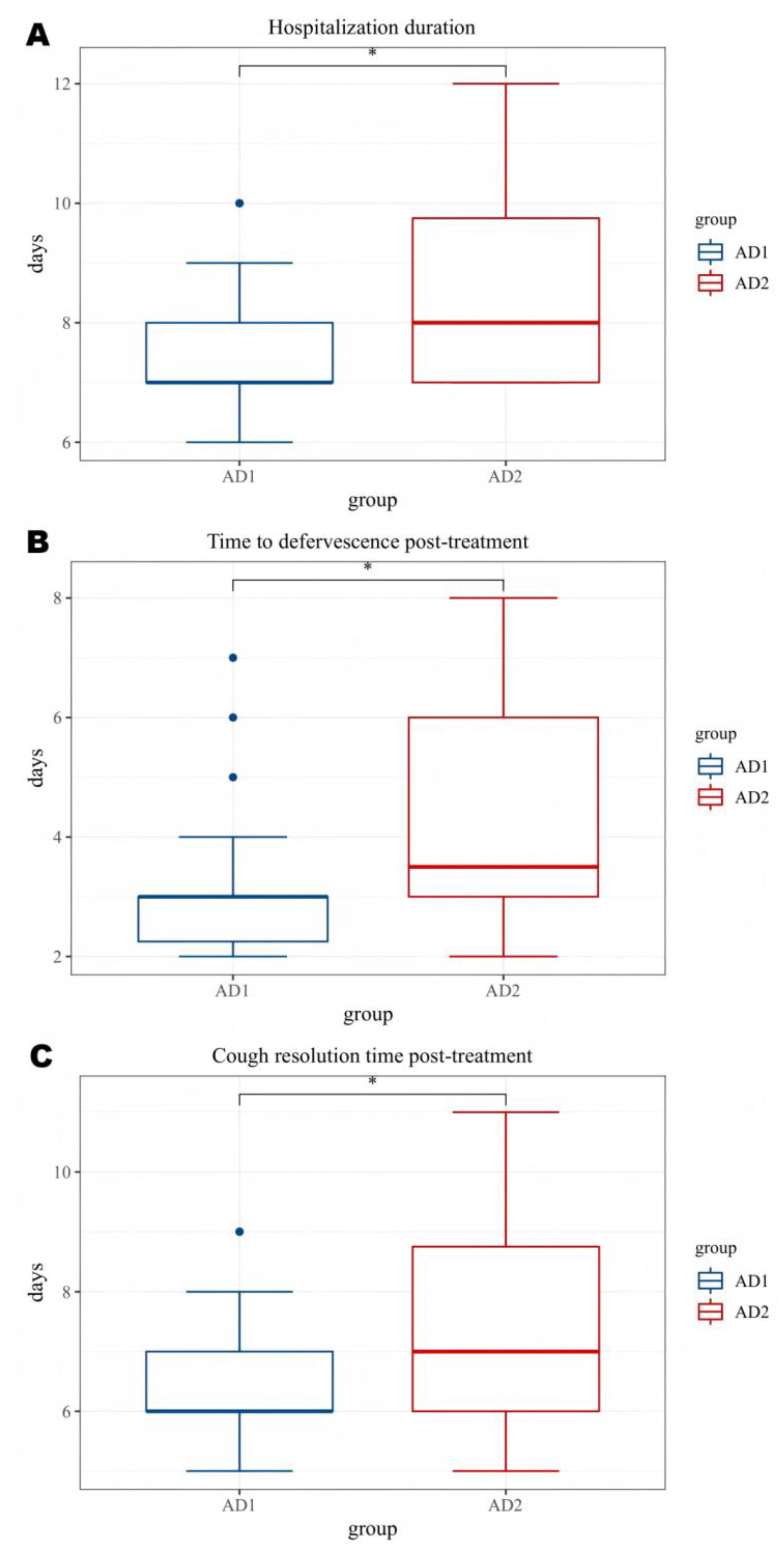

Table 1.
Age-stratified comparison of baseline characteristics between MRMPP patients (≥8 years: DX group vs AZ1 group; <8 years: AD group vs AZ2 group).
Table 1.
Age-stratified comparison of baseline characteristics between MRMPP patients (≥8 years: DX group vs AZ1 group; <8 years: AD group vs AZ2 group).
| ≥8 years | P value | <8 years | P value | |||
|---|---|---|---|---|---|---|
| DX group | AZ1 group | AD group | AZ2 group | |||
| N=27 | N=15 | N=52 | N=79 | |||
| Age, years | 9.00±1.33 | 9.20±1.47 | 0.725 | 5.75±1.29 | 5.33±1.30 | 0.066 |
| Male gender (n,%) | 16(59.3%) | 8(53.3%) | 0.710 | 28(53.8%) | 39(49.4%) | 0.616 |
| Fever (n, %) | 27(100%) | 15(100%) | - | 52(100%) | 79(100%) | - |
| Cough (n, %)) | 27(100%) | 15(100%) | - | 52(100%) | 79(100%) | - |
| Duration of fever before treatment (d) | 3.37±1.57 | 3.40±1.29 | 0.286 | 3.27±1.65 | 3.14±1.68 | 0.664 |
| Cough duration before treatment (d) | 5.67±1.75 | 5.20±1.52 | 0.392 | 5.08±2.35 | 5.73±2.11 | 0.099 |
| Chest imaging findings(n, %) | 0.800 | 0.975 | ||||
| pulmonary consolidation | 14(51.9%) | 9(60.0%) | 22(42.3%) | 35(44.3%) | ||
| Interstitial Disease | 1(3.7%) | 1(6.7%) | 5(9.6%) | 8(10.1%) | ||
| Mixed Lesions | 7(25.9%) | 4(26.7%) | 19(36.5%) | 29(36.7%) | ||
| Pleural Effusion | 5(18.5%) | 1(6.7%) | 6(11.5%) | 7(8.9%) | ||
| Laboratory findings | ||||||
| White blood cell(×10^9/L) |
8.26±3.06 | 9.68±4.57 | 0.291 | 8.16±3.63 | 8.39±4.08 | 0.836 |
| Neutrophil (%) | 66.22±9.18 | 61.04±18.09 | 0.313 | 67.01±11.96 | 65.46±11.55 | 0.459 |
| Platelets (×10^9/L) | 296.03±92.50 | 311.86±113.52 | 0.627 | 293.96±106.97 | 308.84±106.72 | 0.317 |
| Hemoglobin (g/L) | 123.33±10.76 | 123.60±8.66 | 0.935 | 118.58±9.29 | 119.51±9.52 | 0.582 |
| C-reactive protein(mg/L) |
23.38±19.53 | 25.18±26.13 | 0.815 | 22.69±15.67 | 24.65±33.98 | 0.273 |
| Procalcitonin (ng/mL) | 0.19±0.35 | 0.47±1.02 | 0.790 | 0.26±0.43 | 0.26±0.49 | 0.447 |
| Lactate dehydrogenase (U/L) |
332.14±185.51 | 325.12±97.74 | 0.893 | 317.78±84.33 | 315.16±80.23 | 0.959 |
| Erythrocyte sedimentation rate (mm/h) | 49.77±27.97 | 48.40±12.99 | 0.829 | 48.87±18.64 | 48.39±16.54 | 0.821 |
| Severe pneumonia (n, %) |
12(44.4%) | 6(40.0%) | 1.000 | 27(51.9%) | 15(19.0%) | 0.000 |
Table 2.
Baseline characteristics of the AD1 and AD2 subgroups before treatment.
| AD1 group | AD2 group | P value | |
|---|---|---|---|
| N=22 | N=30 | ||
| Age, years | 5.50±1.50 | 5.93±1.11 | 0.360 |
| Male gender (n,%) | 9(40.9%) | 19(63.3%) | 0.160 |
| Duration of fever before treatment (d) | 3.23±1.37 | 3.30±1.86 | 0.878 |
| Cough duration before treatment (d) | 5.64±2.17 | 4.67±2.44 | 0.145 |
| Chest imaging findings(n, %) | 0.373 | ||
| pulmonary consolidation | 8(36.4%) | 14(46.7%) | |
| Interstitial Disease | 1(4.5%) | 0(0.0%) | |
| Mixed Lesions | 10(45.5%) | 9(30.0%) | |
| Pleural Effusion | 3(13.6%) | 7(23.3%) | |
| Laboratory findings | |||
| White blood cell(×10^9/L) |
8.52±4.18 | 7.90±3.23 | 0.549 |
| Neutrophil (%) | 66.70 ±12.45 | 67.24±11.80 | 0.875 |
| Platelets (×10^9/L) | 300.14±109.48 | 289.43±106.74 | 0.725 |
| Hemoglobin (g/L) | 118.36±7.82 | 118.73±10.36 | 0.889 |
| C-reactive protein(mg/L) |
20.38±12.98 | 24.39±17.4 | 0.368 |
| Procalcitonin (ng/mL) | 0.20±0.35 | 0.30±0.48 | 0.590 |
| Lactate dehydrogenase (U/L) |
294.89±59.48 | 334.57±96.21 | 0.176 |
| Erythrocyte sedimentation rate (mm/h) | 43.14±13.81 | 53.07±20.73 | 0.057 |
| Severe pneumonia (n, %) |
12(54.5%) | 15(50.0%) | 0.785 |
Table 3.
Comparison of baseline characteristics before treatment in severe MRMPP patients aged <8 years (ADsp group vs. AZ2sp group).
Table 3.
Comparison of baseline characteristics before treatment in severe MRMPP patients aged <8 years (ADsp group vs. AZ2sp group).
| AD group | AZ2 group | P value | |
|---|---|---|---|
| N=27 | N=15 | ||
| Age, years | 5.74±1.37 | 4.80±2.04 | 0.129 |
| Male gender (n,%) | 16(59.3%) | 5(33.3%) | 0.107 |
| Duration of fever before treatment (d) | 2.85±1.70 | 3.00±1.85 | 0.799 |
| Cough duration before treatment (d) | 5.07±2.40 | 5.80±2.17 | 0.338 |
| Chest imaging findings(n, %) | 0.203 | ||
| pulmonary consolidation | 12(44.4%) | 4(26.7%) | |
| Interstitial Disease | 1(3.7%) | 3(20.0%) | |
| Mixed Lesions | 9(33.3%) | 7(46.7%) | |
| Pleural Effusion | 5(18.5%) | 1(6.7%) | |
| Laboratory findings | |||
| White blood cell(×10^9/L) |
8.32±4.23 | 7.83±3.15 | 0.865 |
| Neutrophil (%) | 65.83±13.99 | 60.94±8.87 | 0.230 |
| Platelets (×10^9/L) | 265.22±99.73 | 294.87±113.25 | 0.351 |
| Hemoglobin (g/L) | 119.30±8.41 | 119.93±7.30 | 0.807 |
| C-reactive protein(mg/L) |
20.28±18.91 | 23.40±19.48 | 0.487 |
| Procalcitonin (ng/mL) | 0.38±0.57 | 0.23±0.48 | 0.351 |
| Lactate dehydrogenase (U/L) |
334.00±99.66 | 324.95±62.15 | 0.752 |
| Erythrocyte sedimentation rate (mm/h) | 46.74±18.21 | 49.13±15.45 | 0.670 |
Table 4.
Comparison of clinical effectiveness in MRMPP patients aged ≥8 years between the DX and AZ1 groups.
Table 4.
Comparison of clinical effectiveness in MRMPP patients aged ≥8 years between the DX and AZ1 groups.
| DX group | AZ1 group | P value | |
|---|---|---|---|
| N=27 | N=15 | ||
| Hospitalization duration(d) | 7.11±1.78 | 8.33±0.97 | 0.007 |
| Fever duration after treatment(d) |
3.37±1.18 | 4.33±0.72 | 0.011 |
| Antipyretic period | 0.020 | ||
| Defervescence within 72 h (n,%) | 14(51.9%) | 2(13.3%) | |
| Fever lasts more than 72 hours(n,%) | 13(48.1%) | 13(86.7%) | |
| Cough Improvement Duration After Treatment (d) | 5.96±1.76 | 7.33±0.97 | 0.008 |
| Improved chest imaging(n,%) | 17(63.0%) | 3(20.0%) | 0.011 |
| Glucocorticoids(n,%) | 20(74.1%) | 12(80.0%) | 1.000 |
| Glucocorticoids(d) | 2.15±1.81 | 4.07±2.49 | 0.013 |
| Immunoglobulin(n,%) | 4(14.8%) | 7(46.7%) | 0.034 |
Table 5.
Comparison of clinical efficacy between AD and AZ2 groups in MRMPP patients aged <8 years.
| AD group | AZ2 group | P value | |
|---|---|---|---|
| N=52 | N=79 | ||
| Hospitalization duration(d) | 8.12±1.56 | 8.76±1.75 | 0.029 |
| Fever duration after treatment(d) |
3.85±1.60 | 4.65±1.51 | 0.005 |
| Antipyretic period | 0.000 | ||
| Defervescence within 72 h (n,%) | 32(61.5%) | 21(26.6%) | |
| Fever lasts more than 72 hours(n,%) | 20(38.5%) | 58(73.4%) | |
| Cough Improvement Duration After Treatment (d) | 7.06±1.61 | 7.61±1.56 | 0.056 |
| Improved chest imaging(n,%) | 31(59.6%) | 38(48.1%) | 0.215 |
| Glucocorticoids(n,%) | 39(75.0%) | 72(91.1%) | 0.015 |
| Glucocorticoids(d) | 3.96±2.55 | 4.14±1.91 | 0.649 |
| Immunoglobulin(n,%) | 13(25.0%) | 13(16.5%) | 0.266 |
Table 6.
Comparison of clinical efficacy between ADsp and AZ2sp groups in patients aged <8 years with severe MRMP pneumonia.
Table 6.
Comparison of clinical efficacy between ADsp and AZ2sp groups in patients aged <8 years with severe MRMP pneumonia.
| ADsp group | AZ2sp group | P value | |
|---|---|---|---|
| N=27 | N=15 | ||
| Hospitalization duration(d) | 9.04±1.61 | 10.93±1.34 | 0.000 |
| Fever duration after treatment(d) | 4.52±1.87 | 5.73±1.58 | 0.032 |
| Antipyretic period | 0.000 | ||
| Defervescence within 72 h (n,%) | 14(51.9%) | 3(20.0%) | |
| Fever lasts more than 72 hours(n,%) | 13(48.1%) | 12(80.0%) | |
| Cough Improvement Duration After Treatment (d) | 8.04±1.61 | 9.00±1.31 | 0.043 |
| Improved chest imaging(n,%) | 18(66.7%) | 4(26.7%) | 0.023 |
| Glucocorticoids(n,%) | 20(74.1%) | 15(100%) | 0.038 |
| Glucocorticoids(d) | 4.52±2.86 | 6.07±0.88 | 0.049 |
| Immunoglobulin(n,%) | 7(25.9%) | 9(60.0%) | 0.047 |
Table 7.
Comparison of clinical efficacy of doxycycline conversion at different times in MRMPP patients aged <8 Years (AD1 group vs AD2 group).
Table 7.
Comparison of clinical efficacy of doxycycline conversion at different times in MRMPP patients aged <8 Years (AD1 group vs AD2 group).
| AD1 group | AD2 group | P value | |
|---|---|---|---|
| N=22 | N=30 | ||
| Hospitalization duration(d) | 7.50±1.10 | 8.57±1.70 | 0.013 |
| Fever duration after treatment(d) | 3.23±1.31 | 4.30±1.66 | 0.015 |
| Antipyretic period | 0.044 | ||
| Defervescence within 72 h (n,%) | 17(77.3%) | 14(46.7%) | |
| Fever lasts more than 72 hours(n,%) | 5(22.7%) | 16(53.3%) | |
| Cough Improvement Duration After Treatment (d) | 6.50±1.10 | 7.47±1.81 | 0.031 |
| Improved chest imaging(n,%) | 18(81.8%) | 13(43.3%) | 0.009 |
| Glucocorticoids(n,%) | 13(59.1%) | 26(86.7%) | 0.049 |
| Glucocorticoids(d) | 3.14±2.78 | 4.57±2.22 | 0.045 |
| Immunoglobulin(n,%) | 2(9.1%) | 11(36.7%) | 0.049 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



