
Submitted:
09 October 2025
Posted:
10 October 2025
You are already at the latest version
Abstract
Intestinal protozoa are a common cause of morbidity in people living with HIV (PLWH), particularly in tropical regions with poor sanitation. We conducted a cross-sectional study in 315 PLWH from Iquitos, Peru, between October/2023-May/2024, to assess their prevalence and risk factors. Stool samples were examined using Lugol’s iodine, modi-fied Ziehl Neelsen (MZN) staining, and immunochromatography (ICT). Epidemiologi-cal and clinical data were collected. The mean age was 41 years, with a median CD4+ count of 431 cells/µL; 12.4% were in AIDS stage (CD4+ < 200) and 21.5% had a detectable viral load. 51.4% of participants tested positive for any intestinal protozoa. Pathogenic protozoa prevalence was 25.7% for Cryptosporidium spp., 2.9% for Giardia spp., and 1.9% for Entamoeba spp. Diagnostic agreement was almost perfect between Lugol and ICT for Giardia and Entamoeba (κ = 0.87; p < 0.001 and κ = 0.91; p < 0.001, respectively), but only slight between MZN and ICT. Homosexual practices were identified as a significant risk factor for pathogenic protozoa infection (AOR 2.52; 95% CI: 1.04–6.12). In conclusion, the high prevalence of protozoa infection reflects ongoing exposure to fecal–oral transmission, underscoring the need for public health education, routine diagnosis, and treatment in similar settings.
Keywords:
Intestinal protozoa
; parasite
; Cryptosporidium
; Giardia
; Entamoeba
; HIV
; Peru
1. Introduction
Intestinal protozoa are common in immunocompromised patients and an important cause of diarrhea in patients living with HIV (PWH) worldwide [1], particularly in tropical low-resources countries that are challenged by scarce access to potable water and/or robust sanitation infrastructure [2,3].
Cryptosporidium spp. is a well-recognized opportunistic intestinal protozoa that cause acute or chronic enterocolitis, with severity varying according to the host’s immune status [4]. In fact, it is classified as an Acquired Immuno-Deficiency Syndrome (AIDS)-defining illness, as it predominantly affects PWH with profound immunosuppression, in whom it can lead to severe, life-threatening diarrheal disease [5,6,7,8]. Besides, it can cause epidemic outbreaks linked to water sources [9]. Giardia duodenalis can cause similar gastrointestinal manifestations, particularly diarrhea and malabsorption, that can be more persistent and difficult to treat in immunocompromised, although it is less frequently associated with life-threatening disease in immunocompromised hosts [10]. Entamoeba histolytica is a well-recognized pathogenic intestinal protozoan capable of causing amebic colitis, with disease severity largely determined by the host’s immune status. In immunocompromised patients, such as those with advanced HIV infection, E. histolytica infection may progress to more severe manifestations, including amebic liver abscesses and fulminant amebic dysentery [11].
Blastocystis spp., traditionally known as a commensal parasite, is a parasite frequently found in human fecal samples [12,13]. Its pathogenicity remains uncertain; however, certain subtypes (such as ST1 and ST7) have been associated with gastrointestinal symptoms—including diarrhea, bloating or abdominal pain—and, in some reports, with irritable bowel syndrome and pruritus, possibly mediated through alterations of the intestinal microbiome [14]. This suggests that the clinical relevance of Blastocystis may be limited to specific populations and clinical contexts. Entamoeba coli, Endolimax nana and Iodamoeba bütschlii are believed to not cause pathogenic human infections, but their presence in stool can sentinel co-infection with true pathogens [15].
The prevalence of intestinal protozoa is likely underestimated given the high proportion of asymptomatic infections, low sensitivity of standard microscopy and scarcity of personnel who are competent in parasitology diagnosis [5]. Despite this, it is consistently reported to be high among PWH in Peru [16], sometimes reaching levels twice as high as in healthy individuals [17]. Even if there are some reports about intestinal protozoa in PWH in Lima, with 47.5% of overall prevalence and Cryptosporidium spp., Blastocystis spp. and Giardia duodenalis leading the top three positions (prevalences around 20%, 11% and 8% [18,19] respectively), no studies have been found on HIV population in the Peruvian Amazon basin.
Iquitos, Peru, the largest city in the Peruvian Amazon (Loreto Department), presents a unique context for studying the prevalence of intestinal protozoa in PWH. It has the second-highest prevalence of PWH in Peru, after Lima; more than 1,000 patients presented to Iquitos’ public hospitals and 272 new HIV cases were diagnosed in the last part of 2023 alone [20]. The city has distinctive environmental and socio-economic factors (hot and humid conditions, limited access to healthcare and drinkable water, high levels of poverty), which could contribute to a high burden of intestinal parasitic infections. Despite the favorable environment for intestinal protozoa infections, their epidemiology in PWH is understudied. Addressing this knowledge gap is crucial for developing targeted clinical and public health interventions to improve the care of PWH.
The objective of this study was to assess the parasitological prevalence and risk factors for intestinal protozoa infection in established outpatients attending HIV-dedicated clinics in Iquitos, Peru.
2. Materials and Methods
We conducted a cross-sectional study of PWH receiving care at one of two hospitals in Iquitos, Loreto Department, Peru: (1) the Regional Hospital of Loreto "Felipe Santiago Arriola Iglesias" (referral center for patients from the north of the city or rural communities), and (2) the Hospital of Iquitos “César Garayar García” (referral center for patients from the south of the city), from October 20, 2023 to May 20, 2024.
2.1. Study Population and Inclusion/Exclusion Criteria
We included adult outpatients (≥18 years) with confirmed HIV infection who were attending HIV-dedicated clinics for routine follow-up at either the Regional Hospital of Loreto or the Hospital of Iquitos and were able to provide stool specimens. Previously enrolled patients were excluded from re-entry during the study period.
2.2. Enrollment Procedures
The study staff recruited PWH by providing them with information about the study when they presented to either hospital for routine follow-up visits. After informed consent, they collected the participant’s socio-epidemiological, clinical, and HIV-associated factors through a structured interview and registered via an electronic Excel spreadsheet, given the absence of a stable internet connection. The presence of diarrhea was classified according to the patient's opinion, while frequency was categorized into three categories (at least once a day, at least once a week, at least once a month). Next, study participants submitted a fresh stool specimen which was preserved under cold-chain conditions and processed for copro-parasitological examination on the same day. If participants were unable to submit the stool sample at the clinic, a driver collected it from their home within the following week, provided they consented to a home visit, which all participants agreed to.
2.3. Stool Specimen Processing, Staining and Microscopy
Stool samples were examined using Lugol’s iodine solution for the identification of intestinal protozoa, modified Ziehl–Neelsen (MZN) stain for Cryptosporidium spp. oocysts, a technique not routinely performed in Iquitos, and immunochromatographic test (ICT) for Cryptosporidium parvum, Giardia duodenalis and Entamoeba histolytica/dispar. All the positive samples were assessed by two technicians, together with the 20% negative stool (control quality) and the MZN stains.
- -
- Lugol’s iodine solution: Each fecal specimen was analyzed using Lugol’s iodine solution to enhance the diagnostic accuracy of direct microscopy of wet mounts, looking for Giardia spp., Entamoeba spp., Blastocystis spp., Entamoeba coli, Endolimax nana, and Iodamoeba bütschlii. We did not perform a concentration technique before Lugol’s iodine solution because some studies reported a non-significant difference in sensitivity between direct examination and the formalin ether concentration technique [21]. Lugol’s iodine stains glycogen and other cytoplasmic structures, enhancing the visualization of protozoan cysts and trophozoites. Giardia cysts typically appear oval with internal nuclei and axonemes [22], while Entamoeba cysts show characteristic nuclear structures and chromatoid bodies, and the trophozoite could appear with red blood cells in the cytoplasm, what allow it to be sometimes distinguished from the commensal E. dispar [23]. Commensal protozoa, including Blastocystis, display variable shapes and internal granularity, whereas E. coli, E. nana, and I. bütschlii cysts can be distinguished by their size, number of nuclei, and cytoplasmic inclusions. [24]. This technique is simple, fast and useful, and provides a cost-effective approach for preliminary identification of intestinal protozoa in laboratory settings.
- -
- Modified Ziehl-Neelsen stain (MZN): Briefly, each stool sample was homogenized with a spatula and, taking a small amount at the edge, spread elliptically over the central part of a slide. The slide was heat-fixed and placed on a support to facilitate washing, then coated with phenolated fuchsin for 5 minutes and gently rinsed with running water to remove the reagent. The slide was incubated in 3% acid alcohol for 1 minute, rinsed, incubated in methylene blue as a contrast stain for 5 minutes, rinsed, and allowed to dry at room temperature on paper towels. Once dry, a drop of immersion oil was added to the center of the extended slide for microscopic observation with the 100X objective. To assure high-quality microscopy results, the two study staff microscopists were trained by the Cayetano Heredia University’s Microbiology Service and Selva Amazonica Civil Association before study initiation.
- -
- Crypto + Giardia + Entamoeba ICT (CerTest ®, Certest Biotec, Zaragoza, Spain): This one step combo card test is a colored chromatographic immunoassay for the simultaneous qualitative detection of Cryptosporidium spp. (via Anti-Crypto MAb (clone CR23) and Inactivated Cryptosporidium parvum antigen (native extract)), Giardia duodenalis and Entamoeba histolytica/dispar in stool samples. It is used by mixing a small amount of stool sample with the provided buffer, applying the mixture to the test cassette, and waiting the specified time (usually 10–15 minutes). The appearance of lines in the result window indicates the presence of antigens from Cryptosporidium spp. and/or Giardia duodenalis and/or Entamoeba histolytica/dispar.
2.4. Data Analysis
Statistical analyses were performed via SPSS Statistics version 22.0 (IBM, Armonk, EEUU). For descriptive statistics, categorical variables were expressed as frequencies and percentages, while continuous variables were presented as medians with interquartile range (IQRs). The 95% confidence intervals (CIs) were calculated using the Newcombe method [25]. Categorical variables were compared using Chi-square tests, while continuous variables were analyzed using student t-tests (for variables with a normal distribution like age) and U-Mann Whitney tests (for other quantitative variables without a normal distribution). Prevalences were given by overall cohort and in the sub analysis of people referring diarrhea.
To compare the agreement between two diagnostic tests (MZN versus ICT for Cryptosporidium spp. and Lugol´s iodine solution versus ICT for other protozoa), we calculated Cohen’s kappa coefficient, which measures concordance beyond chance. Kappa values were interpreted as slight (0–0.20), fair (0.21–0.40), moderate (0.41–0.60), substantial (0.61–0.80), or almost perfect (0.81–1.00) agreement.
Risk factors were calculated for the overall prevalence of pathogenic intestinal protozoa (Cryptosporidium, Giardia, Entamoeba). Initially, we evaluated them through bivariate analysis, with associations quantified using odds ratios (ORs). Subsequently, multivariable logistic regression models were constructed to identify independent risk factors for the infection. This model included variables that showed statistical significance (p<0.05) in the univariate analyses, adjusted by age and sex. The models’ goodness of fit were assessed using CoxSnell R2 and Nagelkerke R2 statistics to determine the strength of association between the dependent variable (protozoa infection) and independent variables (socio-epidemiological, clinical, and HIV-associated factors).
2.5. Ethical Considerations
The Ethics Committee of Loreto Regional Hospital in Iquitos (Peru) (EXP: ID-018-CIEI-2013) and the Responsible Research Office of the Miguel Hernández University of Elche approved the study (DMC.JMRR.230908). Individuals who volunteered for the study provided informed consent. All study results were kept strictly confidential and released only to the participants’ HIV healthcare provider, who offered treatment and follow-up to those who tested positive for intestinal parasites (protozoa or helminths) at no cost.
3. Results
3.1. Description of the Cohort
315 patients were enrolled (Figure 1). The mean age of the PWH cohort was 41 years (+/-11), with a median of CD4+ of 431 (288, 584) cells/uL. 12.4% had CD4+ < 200 cells/uL (AIDS stage), while 21,5% had a detectable viral load.
Most participants (267/315, 85%) were enrolled from Loreto Regional Hospital, which has the largest PWH cohort in Iquitos. Most (227/315, 76.7%) were heterosexual men, with few comorbidities. 103/315 (32.7%) lived on an unpaved road, 150/315 (47.6%) lived in a wood-made house and 220/315 (70.0%) reported close contact with animals. 21.6% (68/315) reported diarrhea (76.5% once a month, 10.3% once a week, 13.2% once a day). Baseline characteristics were comparable before and after patient exclusion, with no significant differences observed.
3.2. Stool Diagnosis
We received stool samples from 315 PWH. All samples underwent direct examination with Lugol’s iodine staining, MZN and ICT. Among the 315 samples, 162 (51.4%) stool were positive for any pathogenic/commensal protozoa.
3.2.1. Prevalence of Giardia, Entamoeba, Blastocystis, and Commensal Pathogens
Among the 315 samples that underwent by Lugol´s iodine staining, 35 (prevalence 11.1%; 95% CI 8.1-15.1%) were positive for Blastocystis spp., 8 (prevalence 2.5%; 95% CI 1.2-4.9%) for Giardia spp., and 5 (prevalence 1.6%; 95% CI 0.7-3.7%) for Entamoeba spp. For commensal pathogens, 64 (prevalence 20.3%; 95% CI 16.3-25.1%) were positive for Entamoeba coli, 24 (prevalence 7.6%; 95% CI 5.2-11.1%) for Endolimax nana and 6 (prevalence 1.9%; 95% CI 0.8-4.1%) for Iodamoeba buetschlii.
Among the 315 samples that underwent by ICT, 8 (prevalence 2.5%; 95% CI 1.2-4.9%) were positive for Giardia duodenalis, and 6 (prevalence 1.9%; 95% CI 0.8-4.1%) for Entamoeba histolytica/dispar.
The overall prevalence for pathogenic protozoa was: 9/315 samples positive for Giardia spp. (prevalence 2.9%; 95% CI 1.5-5.3%)) and 6 (prevalence 1.9%; 95% CI 0.8-4.1%) for Entamoeba spp.
3.2.2. Prevalence of Cryptosporidium spp.
Among the 315 samples that underwent by MZN, 73 were positive for Cryptosporidium spp. (prevalence 23.2%; 95% CI 18.9-28.1%). Among the 315 samples that underwent by ICT, 11 were positive for Cryptosporidium (prevalence 3.5%; 95% CI 2.0-6.1%).
Overall prevalence for Cryptosporidium spp. was: 81/315 (prevalence 25.7%; 95% CI 21.2-30.8%).
3.2.3. Evaluation of Diagnostic Test Agreement
Agreement between Lugol’s iodine microscopy and ICT for the detection of Giardia spp. and Entamoeba spp. was almost perfect (κ = 0.87; 95% CI 0.70 – 1.00); p <0.001) and κ = 0.91; 95% CI 0.73 – 1.00; p < 0.001, respectively). Agreement between MZN and ICT for the detection of Cryptosporidium spp. was slight (κ = 0.11; 95% CI 0.04 – 0.18; p < 0.74) (Figure 2).
3.2.4. Prevalence of Co-Infection with Giardia spp., Entamoeba spp., Cryptosporidium spp. and Blastocystis spp.
Among the overall protozoa prevalence, 8 patients were co-infected with Cryptosporidium spp. + Blastocystis spp., 3 with Cryptosporidium spp. + Giardia spp. and 2 with Giardia spp. + Blastocystis spp.
3.2.5. Epidemiological Risk Factors Associated with Pathogenic Intestinal Protozoa Positivity
We compared demographic and epidemiological characteristics, comorbidities and HIV infection features by pathogenic protozoa (overall Cryptosporidium spp., Giardia spp. and Entamoeba spp. positivity) (Table 1).
After adjusting for sex, age, and variables with p-values <0.10 in the bivariate analysis (hospital, current CD4 count <200 cells/uL, viral load uncontrolled >20 copies/ml, daily diarrhea, homosexual practices, prior intestinal parasite infection, gonococcal infection, or toxoplasmosis), homosexual practices (compared to heterosexual, bisexual, or transgender practices) were significantly associated with a higher risk of pathogenic protozoa positivity (adjusted OR: 2.52; 95% CI: 1.04–6.12).
3.2.6. Prevalence Pattern of Protozoa in People Referring Diarrhea
Among patients with diarrhea, the prevalence pattern of pathogenic agents was higher to those asymptomatic; Cryptosporidium spp. was the most frequent parasite isolated: 19/68 (27.9%), followed by Blastocystis spp.: 8/68 (11.8%), Giardia spp.: 4/68 (5.9%) and Entamoeba spp.: 3/68 (4.4%).
Presence of overall Giardia spp. was close to signification with having diarrhea the previous month (p=0.091; OR 3.03; 95% CI 0.79-11, similar for Entamoeba spp. (p=0.088; OR 3.754; IC 0.74-19.04), without significant differences in the sub-analysis by Lugol’s iodine and ICT techniques. A prior diagnosis of gonorrhea was significantly associated with diarrhea (p=0.012; OR 2.41; 95% CI 1.20–4.86), as was a history of digestive disease (p<0.001; OR 4.09; 95% CI 1.63–10.28).
4. Discussion
This study provides an epidemiologic evaluation of intestinal protozoa infections among a vulnerable population, PWH, in Iquitos, Peru. The global prevalence of intestinal parasitosis is reported at approximately 50% in patients with HIV-AIDS and diarrhea, with various studies identifying Cryptosporidium spp. as the most common protozoan pathogen, followed by Giardia [17,18,26], which is consistent with our results.
4.1. Cryptosporidium spp. Prevalence in Stool
Our study demonstrated a notable prevalence of Cryptosporidium spp. in both general cohort (25.7%) and people with diarrhea (27.9%), relatively high compared to reports from similar population in Peru, where prevalence usually ranges between 10–20% depending on diagnostic methods and setting [17,18,19,27], reaching 25% in PWH reporting poor hygienic habits [28]. We found only one study of Cryptosporidium spp. in Amazonian populations without HIV [29], in children living in the Colombian Amazon, which identified a 2% prevalence, suggesting that our results are among the first describing Cryptosporidium infections in PWH in the Peruvian Amazon.
The discrepancy between MZN (23.2%) and ICT (3.5%) results can be attributed to two main factors. First, MZN is a sensitive tool for detecting Cryptosporidium spp., but sensitivity can vary (60-100%) depending on the staining process, infection stage and laboratorian’s expertise [9,30]. Its specificity is reported as higher than 90%. Without a competent microscopist, misdiagnosis may be possible with other acid-fast microorganism, such as Cyclospora cayetanensis or Cystoisospora (Isospora) belli, endemic in the region [31,32], even with substantial differences in size. Second, while MZN detects oocysts from any Cryptosporidium species, some of the ICT targets are based on Cryptosporidium parvum antigens. This species is considered more relevant than others in low-resource countries and rural areas due to its zoonotic transmission, accounting for up to 70% of infections in some HIV Asiatic cohorts [33]. However, in a study conducted among HIV-infected patients in Lima, C. parvum represented only 11.3% of the identified genotypes, whereas C. hominis (67.5%) and C. meleagridis (12.6%) predominated [34]. Even if there is no evidence from Iquitos regarding the predominance of this species, the relatively low ICT positivity may reflect a true predominance of non-parvum species. While molecular techniques have an important complementary role in the diagnosis of intestinal protozoa, they are challenging to implement in the clinical laboratories of most low-resources settings.
4.2. Giardia and Entamoeba spp. Prevalence in Stool
Prevalence of Giardia spp. and Entamoeba spp. was relatively low, but agreement between Lugol’s iodine microscopy and ICT for detection of Giardia duodenalis and Entamoeba histolytica/dispar was almost perfect, underscoring the validity of the diagnostic approach [21].
The prevalence of Giardia spp. observed in this study is notably lower than global estimates. A meta-analysis in HIV/AIDS patients reported a pooled prevalence of giardiasis of 5% [35]. Studies in Peru have reported considerable variability depending on population, area and associated symptomatology, with prevalence rates as high as 20% in Trujillo (northern Peru) [36] and 15-4% in HIV in Lima [19,37]. One possible explanation is that the presence of other opportunistic microorganisms, such as Cryptosporidium, could compete with and displace Giardia, especially in individuals with more advanced immunosuppression [38]. Furthermore, Cryptosporidium oocysts are more resistant to conventional cleaning methods than Giardia oocysts, and they can be more easily acquired in recreational settings such as swimming pools and rivers, which are very common in Iquitos [39]. Finally, children, a population not included in our study, seem to be more susceptible to Giardia acquisition [40].
Entamoeba is usually found less frequently than Giardia, and its prevalence in some studies may be overestimated due to the difficulty of distinguishing it from Entamoeba dispar, a non-pathogenic amoeba. In Peru, only a few studies have assessed its prevalence, and none have been conducted in Iquitos. One study in Lima reported a prevalence of 1.9% among people living with HIV [37], consistent with our results.
Although the associations between the presence of Giardia or Entamoeba and diarrhea were not statistically significant, our study suggests a trend toward increased risk. Moreover, a prior diagnosis of gonorrhea and a history of gastrointestinal disease—both significantly associated with diarrhea—may indicate that diarrhea occurrence in our population is multifactorial and not solely driven by enteric protozoa. Furthermore, the typical diet in Iquitos is fatty and high in calories, so many people report diarrhea after heavy meals, which could affect data accuracy.
4.3. Blastocystis, and Commensal Pathogens Prevalence in Stool
Blastocystis spp. prevalence was high (11.5%) in Iquitos’ PWH. Globally, estimations vary from 10 to 50% depending on the geographical area [41]. In Peru, studies of in PWH are mostly restricted to Lima reporting prevalences between 11% [19] and 24.6% [42], consistent with our findings. In our study, Blastocystis spp. was not associated with diarrhea but it was identified as a risk factor for co-infection with commensal protozoa, similar to previous reports suggesting that Blastocystis may serve as a sentinel of fecal contamination [15] due to its association with limited access to potable water and animal contact [41,43,44].
4.4. Risk Factors for Pathogenic Intestinal Protozoa Acquisition
PWH are well-known to be a vulnerable population for intestinal parasitosis, particularly opportunistic protozoa such as Cryptosporidium spp. in patients with low number of CD4+ [45]. Additional commonly reported risk factors for intestinal protozoan infections include young age, male sex, low educational level, lack of sanitary facilities, previous infection with other protozoa, living in suburban areas or an HIV viral load of > 1,000 copies/mL [45,46].
In our study, homosexual practices were associated with a higher prevalence of pathogenic protozoa. In the literature, certain high-risk practices that also facilitate HIV transmission, such as unprotected anal intercourse, also significantly increase the likelihood of acquiring specific enteropathogens. These include Giardia spp., Entamoeba spp., and some helminths such as Strongyloides stercoralis, whose transmission can be enhanced by exposure to fecal material during sexual activity [47,48]. Our findings suggest that the transmission routes of some intestinal protozoa may overlap with HIV risk factors, highlighting the importance of comprehensive prevention strategies that address both viral and parasitic infections.
Furthermore, a poor immunovirological control of HIV and a previous diagnosis of toxoplasmosis —which also reflects impaired immunity—were identified as risk factors for protozoan acquisition in our bivariate analysis [18,49,50], even if they did not emerge as risk factors in the multivariable analysis. This was likely due to the large proportion of missing HIV viral load data that substantially reduced the number of participants included. Other important associations, such as a prior diagnosis of intestinal parasites or experiencing daily diarrhea, also reached significance in the bivariate analysis but not in the multivariate, suggesting trends that could be confirmed with larger cohorts.
4.5. Strengths and Limitations
This study is the first epidemiological evaluation of intestinal protozoa—including Cryptosporidium spp., Giardia duodenalis, and E. hystolitica/dispar—in PWH in the Peruvian Amazon. It identifies risk factors for protozoan acquisition in this vulnerable population and may inform clinical and public health interventions. Strengths include rigorous staff training in stool processing and microscopy, use of gold-standard techniques for Cryptosporidium detection, and inclusion of participants from both major hospitals in Iquitos, representing about one-third of the city’s PWH population.
However, it has several limitations. First, resource limitations precluded us from combining traditional staining and microscopic diagnosis with newer molecular techniques (PCR), that would have improved the specificity and sensitivity of our results [32]. In this regard, E. histolytica was not possible to distinguish from E. dispar, although this does not appear to have led to overdiagnosis. Other limitations include the exclusion of out-of-care PWH, which may have led to an underestimation of intestinal protozoa prevalence in the broader population; a substantial amount of missing data for CD4 counts and HIV viral load, restricting the scope of our multivariable analysis; and the potential recall or reporting bias for diarrhea and exposure history. Additionally, findings may not be generalizable to other regions with different epidemiological contexts.
5. Conclusions
Our study demonstrates a higher-than-expected prevalence of Cryptosporidium spp. infection among PWH in Iquitos, affecting nearly one in four participants, while Giardia spp. and Entamoeba spp. were less common. Moreover, individuals reporting homosexual practices showed an increased risk of acquiring pathogenic protozoa. These findings underscore the importance of implementing affordable laboratory techniques, such as Lugol’s iodine staining and MZN, to ensure accurate screening for intestinal protozoal infections, particularly in patients with poor immunovirological control of HIV.
Author Contributions
Conceptualization, Silvia Otero-Rodriguez, Viviana Pinedo-Cancino, Martin Casapia-Morales and José Ramos-Rincón; Data curation, Silvia Otero-Rodriguez and José Ramos-Rincón; Formal analysis, Silvia Otero-Rodriguez and José Ramos-Rincón; Funding acquisition, José Ramos-Rincón; Investigation, Silvia Otero-Rodriguez, Victoria-Ysabel Villacorta-Pezo, Seyer Mego-Campos and Jorge Parráguez-de-la-Cruz; Methodology, Silvia Otero-Rodriguez, Martin Casapia-Morales and José Ramos-Rincón; Project administration, Viviana Pinedo-Cancino, Martin Casapia-Morales, Esperanza Merino, Eva Clark and José Ramos-Rincón; Resources, Silvia Otero-Rodriguez; Software, Silvia Otero-Rodriguez; Supervision, José Ramos-Rincón; Validation, Silvia Otero-Rodriguez, Viviana Pinedo-Cancino and José Ramos-Rincón; Visualization, José Ramos-Rincón; Writing – original draft, Silvia Otero-Rodriguez and José Ramos-Rincón; Writing – review & editing, Viviana Pinedo-Cancino, Martin Casapia-Morales, Victoria-Ysabel Villacorta-Pezo, Seyer Mego-Campos, Jorge Parráguez-de-la-Cruz, Esperanza Merino, Eva Clark and José Ramos-Rincón.
Funding
This research was funded by Miguel Hernández University of Elche (UMH), grant number UMH-GVA 2022/0005; 11-134-4- 2023-0133, Alicante Health and Biomedical Research Institute (ISABIAL), grant number 2024-0181 and Instituto de Salud Carlos III (ISCIII), grant number CM23/00050.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Loreto Regional Hospital, Iquitos, Peru, protocol code ID-018-CIEI-2013, May 11, 2023.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The dataset used and/or analyzed during the current study are available in Zenodo Repository, under the ORCID: 10.5281/zenodo.14864472.
Acknowledgments
We want to thank the medical staff of the Infectious Diseases Service in Loreto Regional Hospital and Iquitos Hospital, together with the laboratory staff of LIPNAA-CIRNA and Asociación Civil Selva Amazónica for the support on the field.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results”.
Abbreviations
The following abbreviations are used in this manuscript:
| HIV | Human Immunodeficiency Virus |
| PWH | People with HIV |
| MZN | Modified Ziehl Neelsen staining |
| ICT | Immunochromatography |
| CI | Confidence Interval |
| AOR | Adjusted Odds Ratio |
| ELISA | Enzyme-Linked Immunosorbent Assay |
| IQRs | Interquartile Ranges |
| N/A | Not Applicable. |
| ART | Anti-retroviral therapy. |
References
- Zorbozan O, Quliyeva G, Tunalı V, Özbilgin A, Turgay N, Gökengin AD Intestinal Protozoa in Hiv-Infected Patients: A Retrospective Analysis. Turk. J. Parasitol. 2018, 42, 187–190. [CrossRef]
- Bednarska, M.; Jankowska, I.; Pawelas, A.; Piwczyńska, K.; Bajer, A.; Wolska-Kuśnierz, B.; Wielopolska, M.; Welc-Falęciak, R. Prevalence of Cryptosporidium, Blastocystis, and Other Opportunistic Infections in Patients with Primary and Acquired Immunodeficiency. Parasitol. Res. 2018, 117, 2869–2879. [Google Scholar] [CrossRef]
- Bahmani, P.; Maleki, A.; Sadeghi, S.; Shahmoradi, B.; Ghahremani, E. Prevalence of Intestinal Protozoa Infections and Associated Risk Factors among Schoolchildren in Sanandaj City, Iran. Iran. J. Parasitol. 2017, 12, 108–116. [Google Scholar]
- Darlan, D.M.; Rozi, M.F.; Nurangga, M.A.; Amsari, L.C. Cryptosporidium Sp. and Blastocystishominis Findings: A Cross-Sectional Study among Healthy Versus Immunocompromised Individuals. Int. J. Psychosoc. Rehabil. 2020, 24, 2346–2351. [Google Scholar] [CrossRef]
- Gerace, E.; Lo Presti, V.D.M.; Biondo, C. Cryptosporidium Infection: Epidemiology, Pathogenesis, and Differential Diagnosis. Eur. J. Microbiol. Immunol. 2019, 9, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Panel on Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents With HIV. Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents With HIV. National Institutes of Health, HIV Medicine Association, and Infectious Diseases Society of America. Available at Https://Clinicalinfo.Hiv.Gov/En/Guidelines/Adult-and-Adolescent-Opportunistic-Infection. Accessed May 2025 [I-1, I-6].
- Darlan, D.M.; Rozi, M.F.; Nurangga, M.A.; Amsari, L.C. Cryptosporidium Sp. and Blastocystishominis Findings: A Cross-Sectional Study among Healthy Versus Immunocompromised Individuals. Int. J. Psychosoc. Rehabil. 2020, 24, 2346–2351. [Google Scholar] [CrossRef]
- Shirley, D.-A.T.; Moonah, S.N.; Kotloff, K.L. Burden of Disease from Cryptosporidiosis. Curr. Opin. Infect. Dis. 2012, 25, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Aghamolaie, S.; Rostami, A.; Fallahi, S.; Tahvildar Biderouni, F.; Haghighi, A.; Salehi, N. Evaluation of Modified Ziehl-Neelsen, Direct Fluorescent-Antibody and PCR Assay for Detection of Cryptosporidium Spp. in Children Faecal Specimens. J. Parasit. Dis. Off. Organ Indian Soc. Parasitol. 2016, 40, 958–963. [Google Scholar] [CrossRef]
- Nash, T.E.; Ohl, C.A.; Thomas, E.; Subramanian, G.; Keiser, P.; Moore, T.A. Treatment of Patients with Refractory Giardiasis. Clin. Infect. Dis. 2001, 33, 22–28. [Google Scholar] [CrossRef]
- Chakrabarti, S. Multiple Amoebic Liver Abscess As Initial Manifestation in Hiv Sero-Positive Male. J. Clin. Diagn. Res. JCDR 2015, 9, OD04–OD05. [Google Scholar] [CrossRef]
- Khorshidvand, Z.; Khazaei, S.; Amiri, M.; Taherkhani, H.; Mirzaei, A. Worldwide Prevalence of Emerging Parasite Blastocystis in Immunocompromised Patients: A Systematic Review and Meta-Analysis. Microb. Pathog. 2021, 152, 104615. [Google Scholar] [CrossRef]
- Ocaña-Losada C, et al. Características Clínicas y Epidemiológicas de La Parasitación Intestinal Por Blastocystis Hominis. Rev Clin Esp. 2018;218(3):115-120. [CrossRef]
- Wawrzyniak, I.; Poirier, P.; Viscogliosi, E.; Dionigia, M.; Texier, C.; Delbac, F.; Alaoui, H.E. Blastocystis, an Unrecognized Parasite: An Overview of Pathogenesis and Diagnosis. Ther. Adv. Infect. Dis. 2013, 1, 167–178. [Google Scholar] [CrossRef]
- Espinosa Aranzales, A.F.; Radon, K.; Froeschl, G.; Pinzón Rondón, Á.M.; Delius, M. Prevalence and Risk Factors for Intestinal Parasitic Infections in Pregnant Women Residing in Three Districts of Bogotá, Colombia. BMC Public Health 2018, 18, 1071. [Google Scholar] [CrossRef] [PubMed]
- Marcos, L.A.; Gotuzzo, E. Intestinal Protozoan Infections in the Immunocompromised Host. Curr. Opin. Infect. Dis. 2013, 26, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Cárcamo, C.; Hooton, T.; Wener, M.H.; Weiss, N.S.; Gilman, R.; Arevalo, J.; Carrasco, J.; Seas, C.; Caballero, M.; Holmes, K.K. Etiologies and Manifestations of Persistent Diarrhea in Adults with HIV-1 Infection: A Case-Control Study in Lima, Peru. J. Infect. Dis. 2005, 191, 11–19. [Google Scholar] [CrossRef]
- García C, Rodríguez E, Do N, López de Castilla D, Terashima A, Gotuzzo E. Parasitosis Intestinal En El Paciente Con Infección VIH-SIDA [Intestinal Parasitosis in Patients with HIV-AIDS]. Rev Gastroenterol Peru. 2006;26(1):21-24.
- Vergaray, S.; Paima-Olivari, R.; Runzer-Colmenares, F.M. Parasitosis intestinal y estado inmunológico en pacientes adultos con infección por VIH del Centro Médico Naval "Cirujano Mayor Santiago Távara. Horiz. Méd. Lima 2019, 19, 32–36. [Google Scholar] [CrossRef]
- Centro Nacional de Epidemiología, Prevención y Control de Enfermedades. Situación Epidemiológica Del VIH - Sida En El Perú. Boletín VIH, II Trimestre - 2024. Available at: Https://Www.Dge.Gob.Pe/Epipublic/Uploads/Vih-Sida/Vih-Sida_20246_16_153419.Pdf. Consultado El 20 de Febrero de 2025.
- Wahdini, S.; Putra, V.P.; Sungkar, S. The Prevalence of Intestinal Protozoan Infections among Children in Southwest Sumba Based on the Type of Water Sources. Infect. Chemother. 2021, 53, 519. [Google Scholar] [CrossRef]
- Calchi L, C. Martinella, Acurero E, et al. Comparación de Técnicas Parasitológicas. Kasmera, 42(1): 32-40, Enero-Junio 2014. ISSN 0075-5222.
- Botero D, Restrepo M. Parasitosis Humanas. 5.a Edición. Medellín, Corporación Para Investigaciones Biológicas, 2012: 38-56.
- Flórez, A.C.; García, D.A.; Moncada, L.; Beltrán, M. Prevalencia de microsporidios y otros parásitos intestinales en pacientes con infección por VIH, Bogotá, 2001. Biomédica 2003, 23, 274. [Google Scholar] [CrossRef]
- Newcombe, R.G. Two-Sided Confidence Intervals for the Single Proportion: Comparison of Seven Methods. Stat. Med. 1998, 17, 857–872. [Google Scholar] [CrossRef]
- Benson, C.A.; Kaplan, J.E.; Masur, H.; Pau, A.; Holmes, K.K. ; CDC; National Institutes of Health; Infectious Diseases Society of America Treating Opportunistic Infections among HIV-Infected Adults and Adolescents: Recommendations from CDC, the National Institutes of Health, and the HIV Medicine Association/Infectious Diseases Society of America. MMWR Recomm. Rep. Morb. Mortal. Wkly. Rep. Recomm. Rep. 2004, 53, 1–112. [Google Scholar]
- Cama, V.A.; Bern, C.; Sulaiman, I.M.; Gilman, R.H.; Ticona, E.; Vivar, A.; Kawai, V.; Vargas, D.; Zhou, L.; Xiao, L. Cryptosporidium Species and Genotypes in HIV-Positive Patients in Lima, Peru. J. Eukaryot. Microbiol. 2003, 50 Suppl, 531–533. [Google Scholar] [CrossRef]
- Dankwa, K.; Nuvor, S.V.; Obiri-Yeboah, D.; Feglo, P.K.; Mutocheluh, M. Occurrence of Cryptosporidium Infection and Associated Risk Factors among HIV-Infected Patients Attending ART Clinics in the Central Region of Ghana. Trop. Med. Infect. Dis. 2021, 6, 210. [Google Scholar] [CrossRef]
- Sánchez, A.; Munoz, M.; Gómez, N.; Tabares, J.; Segura, L.; Salazar, Á.; Restrepo, C.; Ruíz, M.; Reyes, P.; Qian, Y.; et al. Molecular Epidemiology of Giardia, Blastocystis and Cryptosporidium among Indigenous Children from the Colombian Amazon Basin. Front. Microbiol. 2017, 8, 248. [Google Scholar] [CrossRef]
- Ahmed, S.A.A.; Quattrocchi, A.; Elzagawy, S.M.; Karanis, P.; Gad, S.E.M. Diagnostic Performance of Toluidine Blue Stain for Direct Wet Mount Detection of Cryptosporidium Oocysts: Qualitative and Quantitative Comparison to the Modified Ziehl-Neelsen Stain. Diagn. Basel Switz. 2023, 13, 2557. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention Stool Specimens – Staining Procedures [Internet]. Atlanta (GA): Centers for Disease Control and Prevention; 2023 Aug 31 [Cited 2025 Sep 30]. Available from: Https://Www.Cdc.Gov/Dpdx/Diagnosticprocedures/Stool/Staining.Html.
- Omoruyi, B.E.; Nwodo, U.U.; Udem, C.S.; Okonkwo, F.O. Comparative Diagnostic Techniques for Cryptosporidium Infection. Mol. Basel Switz. 2014, 19, 2674–2683. [Google Scholar] [CrossRef] [PubMed]
- Ghafari, R.; Rafiei, A.; Tavalla, M.; Moradi Choghakabodi, P.; Nashibi, R.; Rafiei, R. Prevalence of Cryptosporidium Species Isolated from HIV/AIDS Patients in Southwest of Iran. Comp. Immunol. Microbiol. Infect. Dis. 2018, 56, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Cama, V.A.; Bern, C.; Roberts, J.; Cabrera, L.; Sterling, C.R.; Ortega, Y.; Gilman, R.H.; Xiao, L. Cryptosporidium Species and Subtypes and Clinical Manifestations in Children, Peru - Volume 14, Number 10—October 2008 - Emerging Infectious Diseases Journal - CDC. [CrossRef]
- Mahdavi, F.; Shams, M.; Sadrebazzaz, A.; Shamsi, L.; Omidian, M.; Asghari, A.; Hassanipour, S.; Salemi, A.M. Global Prevalence and Associated Risk Factors of Diarrheagenic Giardia Duodenalis in HIV/AIDS Patients: A Systematic Review and Meta-Analysis. Microb. Pathog. 2021, 160, 105202. [Google Scholar] [CrossRef]
- Peréz Cordón, G.; Cordova Paz Soldan, O.; Vargas Vásquez, F.; Velasco Soto, J.R.; Sempere Bordes, L.; Sánchez Moreno, M.; Rosales, M.J. Prevalence of Enteroparasites and Genotyping of Giardia Lamblia in Peruvian Children. Parasitol. Res. 2008, 103, 459–465. [Google Scholar] [CrossRef]
- Chincha L, O.; Bernabé-Ortiz, A.; Samalvides C, F.; Soto A, L.; Gotuzzo H, E.; Terashima I, A. Parasite Intestinal Infection and Factors Associated with Coccidian Infection in Adults at Public Hospital in Lima, Peru. Rev. Chil. Infectol. 2009, 26, 440–444. [Google Scholar] [CrossRef]
- Sannella, A.R.; Suputtamongkol, Y.; Wongsawat, E.; Cacciò, S.M. A Retrospective Molecular Study of Cryptosporidium Species and Genotypes in HIV-Infected Patients from Thailand. Parasit. Vectors 2019, 12. [Google Scholar] [CrossRef]
- Adeyemo, F.E.; Singh, G.; Reddy, P.; Bux, F.; Stenström, T.A. Efficiency of Chlorine and UV in the Inactivation of Cryptosporidium and Giardia in Wastewater. PLOS ONE 2019, 14, e0216040. [Google Scholar] [CrossRef] [PubMed]
- Han, M.; Xiao, S.; An, W.; Sang, C.; Li, H.; Ma, J.; Yang, M. Co-Infection Risk Assessment of Giardia and Cryptosporidium with HIV Considering Synergistic Effects and Age Sensitivity Using Disability-Adjusted Life Years. Water Res. 2020, 175, 115698. [Google Scholar] [CrossRef]
- Robles-Cabrera, M.X.; Maguiña, J.L.; Gonzales-Huerta, L.; Panduro-Correa, V.; Dámaso-Mata, B.; Pecho-Silva, S.; Navarro-Solsol, A.C.; Rabaan, A.A.; Rodríguez-Morales, A.J.; Arteaga-Livias, K. Blastocystis Species and Gastrointestinal Symptoms in Peruvian Adults Attended in a Public Hospital. Infect. Chemother. 2021, 53, 374–380. [Google Scholar] [CrossRef]
- Chincha, O.; Bernabé-Ortiz, A.; Samalvides, F.; Soto, L.; Gotuzzo, E.; Terashima, A. Infecciones parasitarias intestinales y factores asociados a la infección por coccidias en pacientes adultos de un hospital público de Lima, Perú [Parasite intestinal infection and factors associated with coccidian infection in adults at public hospital in Lima, Peru] [published correction appears in Rev Chilena Infectol. 2009 Dec;26(6):571]. Rev Chil. Infectol 2009, 26, 440–444. [Google Scholar]
- Fontanelli Sulekova, L.; Gabrielli, S.; Furzi, F.; Milardi, G.L.; Biliotti, E.; De Angelis, M.; Iaiani, G.; Fimiani, C.; Maiorano, M.; Mattiucci, S.; et al. Molecular Characterization of Blastocystis Subtypes in HIV-Positive Patients and Evaluation of Risk Factors for Colonization. BMC Infect. Dis. 2019, 19, 876. [Google Scholar] [CrossRef]
- Salazar-Sánchez, R.S.; Ascuña-Durand, K.; Ballón-Echegaray, J.; Vásquez-Huerta, V.; Martínez-Barrios, E.; Castillo-Neyra, R. Socio-Demographic Determinants Associated with Blastocystis Infection in Arequipa, Peru. Am. J. Trop. Med. Hyg. 2020, 104, 700–707. [Google Scholar] [CrossRef]
- Ntonifor, N.H.; Tamufor, A.S.W.; Abongwa, L.E. Prevalence of Intestinal Parasites and Associated Risk Factors in HIV Positive and Negative Patients in Northwest Region, Cameroon. Sci. Rep. 2022, 12, 16747. [Google Scholar] [CrossRef]
- Feleke, D.G.; Ali, A.; Bisetegn, H.; Andualem, M. Intestinal Parasitic Infections and Associated Factors among People Living with HIV Attending Dessie Referral Hospital, Dessie Town, North-East Ethiopia: A Cross-Sectional Study. AIDS Res. Ther. 2022, 19, 19. [Google Scholar] [CrossRef]
- Nahn Junior, E.P.; Oliveira, E.C. de; Barbosa, M.J.; Mareco, T.C. de S.; Brígido, H.A.; Nahn Junior, E.P.; Oliveira, E.C. de; Barbosa, M.J.; Mareco, T.C. de S.; Brígido, H.A. Protocolo Brasileño Para Infecciones de Transmisión Sexual 2020: Infecciones Entéricas de Transmisión Sexual. Epidemiol. E Serviços Saúde 2021, 30. [CrossRef]
- Sorvillo, F.; Mori, K.; Sewake, W.; Fishman, L. Sexual Transmission of Strongyloides Stercoralis among Homosexual Men. Sex. Transm. Infect. 1983, 59, 342–342. [Google Scholar] [CrossRef] [PubMed]
- Mohebali, M.; Yimam, Y.; Woreta, A. Cryptosporidium Infection among People Living with HIV/AIDS in Ethiopia: A Systematic Review and Meta-Analysis. Pathog. Glob. Health 2020, 114, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Tian, L.-G.; Wang, T.-P.; Lv, S.; Wang, F.-F.; Guo, J.; Yin, X.-M.; Cai, Y.-C.; Dickey, M.K.; Steinmann, P.; Chen, J.-X. HIV and Intestinal Parasite Co-Infections among a Chinese Population: An Immunological Profile. Infect. Dis. Poverty 2013, 2, 18. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow chart illustrating sample availability for the study.
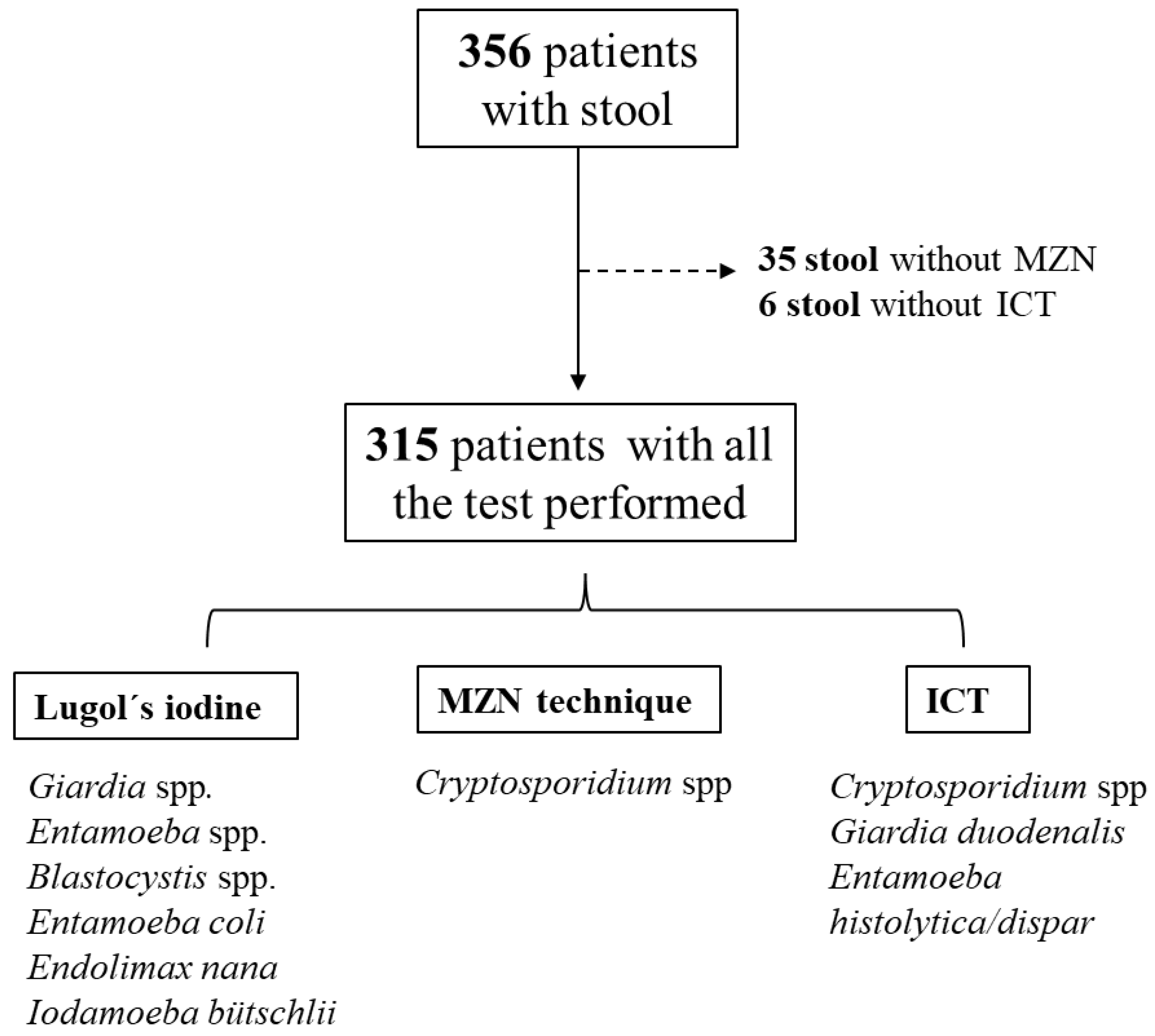
Figure 2.
Cross-tabulations and Cohen’s Kappa for Giardia, Entamoeba and Cryptosporidium.
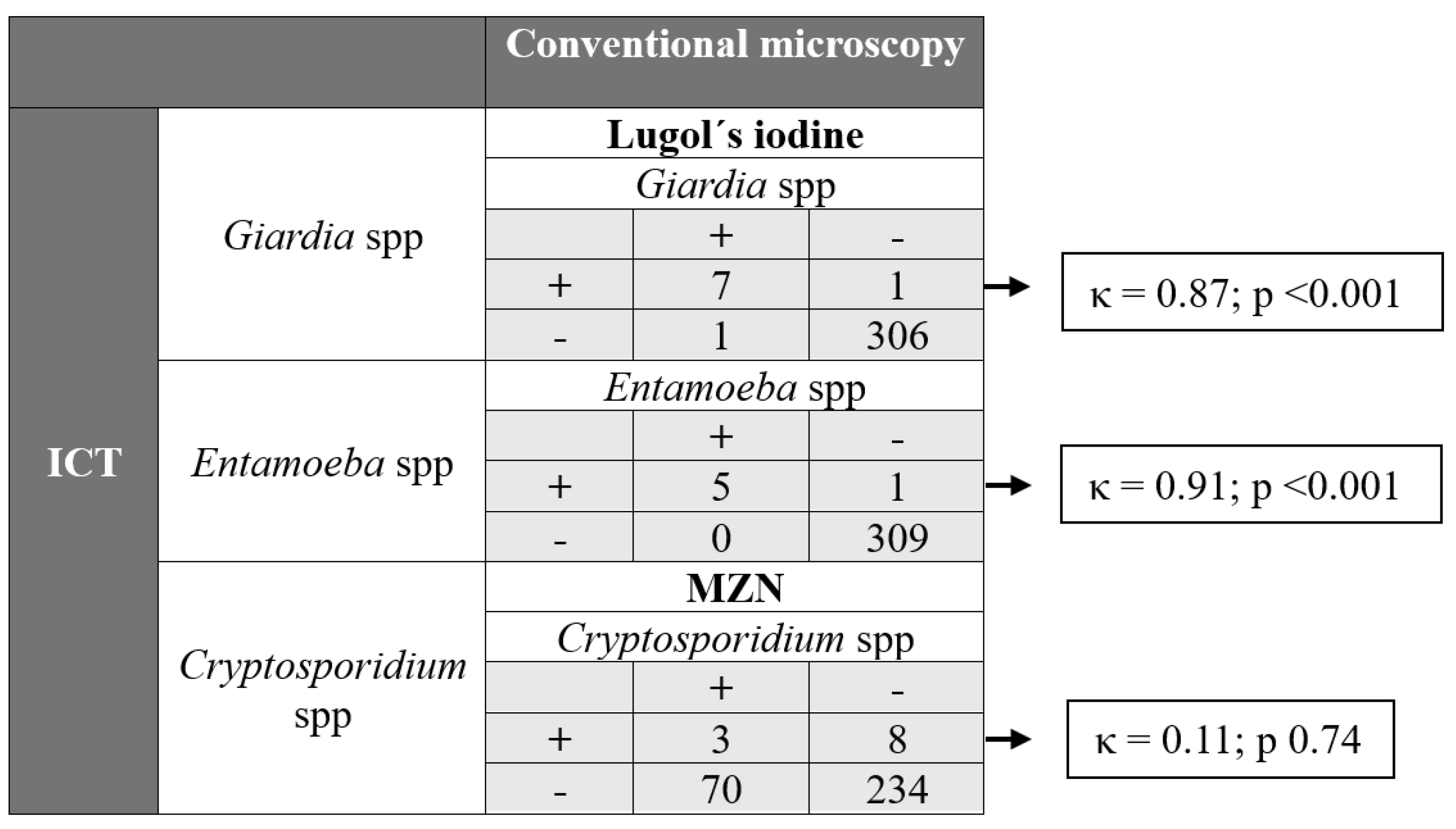

Table 1.
Epidemiological characteristics of study participants (N = 315) by pathogenic protozoa (overall Cryptosporidium spp., Giardia spp. and Entamoeba spp. positivity)
Table 1.
Epidemiological characteristics of study participants (N = 315) by pathogenic protozoa (overall Cryptosporidium spp., Giardia spp. and Entamoeba spp. positivity)
| Variables |
Pathogenic protozoa positive (N = 92) |
Pathogenic Protozoa negative (N = 223) |
OR | p |
| Male, % (n/N) | 60.9 (56/92) | 64.6 (144/223) | 0.85 | 0.54 |
| Age, mean±SD, years | 42 ± 12 | 41 ± 12 | 1.26 | 0.39 |
| Hospital attended, % (n/N) | ||||
| Hospital of Iquitos | 26.1 (24/92) | 10.8 (24/223) | 2.93 | <0.001 |
| Regional Hospital of Loreto | 73.9 (68/92) | 89.2 (199/223) | ||
| Residence, % (n/N) | ||||
| Iquitos district | 33.7 (31/92) | 34.5 (77/223) | N/A | 0.58 |
| Punchana district | 29.3 (27/92) | 25.1 (56/223) | ||
| Belen district | 15.2 (14/92) | 15.7 (35/223) | ||
| San Juan district | 16.3 (15/92) | 22.0 (49/223) | ||
| Outside of Iquitos | 5.4 (5/92) | 2.7 (6/223) | ||
| Occupation, % (n/N) | ||||
| Unemployed or student (yes) | 38.1 (35/92) | 46.2 (103/223) | N/A | 0.19 |
| Cattle, agriculture or construction (yes) | 16.3 (15/92) | 15.2 (34/223) | ||
| Craft work (yes) | 4.3 (4/92) | 4.5 (10/223) | ||
| Intellectual worka(yes) | 15.2 (14/92) | 6.7 (15/223) | ||
| Self-employment (yes) | 26.1 (24/92) | 27.4 (61/223) | ||
| Education, % (n/N) | ||||
| None (yes) | 3.3 (3/92) | 2.7 (6/223) | N/A | 0.31 |
| Attended primary school (yes) | 22.2 (20/92) | 14.3 (32/223) | ||
| Attended secondary school (yes) | 48.9 (45/92) | 59.2 (132/223) | ||
| Attended university (yes) | 26.1 (24/92) | 23.8 (53/223) | ||
| Epidemiological risk factors, % (n/N) | ||||
| Lives with dogs/cats/farm animals (yes) | 69.6 (64/92) | 70.0 (156/223) | 0.98 | 0.94 |
| Walks barefoot (yes) | 33.7 (31/92) | 26.0 (58/223) | 1.45 | 0.17 |
| Resid in rural locationb (yes) | 30.4 (28/92) | 33.6 (75/223) | 0.86 | 0.58 |
| Lives in a house made of wood/leaves (yes) | 44.6 (41/92) | 48.9 (109/223) | 0.84 | 0.49 |
| Alcohol or tobacco consumption (yes) | 55.4 (51/92) | 51.6 (115/223) | 1.17 | 0.53 |
| Comorbidity, % (n/N) | ||||
| Diabetes or high blood pressure (yes) | 6.5 (6/92) | 7.6 (17/223) | 0.85 | 0.73 |
| Other cardiovascular disease (yes) | 1.0 (1/92) | 3.6 (8/223) | 0.30 | 0.23 |
| Digestive disease (yes) | 8.7 (8/92) | 5.4 (12/223) | 1.68 | 0.27 |
| Urinary disease (yes) | 3.3 (3/92) | 0.9 (2/223) | 3.73 | 0.13 |
| Dermatological disease (yes) | 1.0 (1/92) | 0.4 (1/223) | 2.44 | 0.52 |
| Other (yes) | 0.0 (0/92) | 0.9 (2/223) | 1.42 | 0.36 |
| Previous infections, % (n/N) | ||||
| Tuberculosis (yes) | 20.7 (19/92) | 22.0 (49/223) | 0.92 | 0.80 |
| Intestinal parasitosis (yes) | 18.5 (17/92) | 9.0 (20/223) | 2.30 | 0.017 |
| Gonorrhea (yes) | 19.6 (18/92) | 10.3 (23/223) | 2.12 | 0.026 |
| Syphilis (yes) | 18.5 (17/92) | 13.5 (30/223) | 1.46 | 0.26 |
| Chronic hepatitis (yes) | 8.7 (8/92) | 5.8 (13/223) | 1.54 | 0.35 |
| Cerebral toxoplasmosis (yes) | 0.0 (0/92) | 4.9 (11/223) | 1.43 | 0.038 |
| Symptoms, % (n/N) | ||||
| Cough, cold symptoms (yes) | 14.1 (13/92) | 8.1 (18/223) | 1.87 | 0.10 |
| Fever (yes) | 1.1 (1/92) | 2.2 (5/223) | 0.48 | 0.68 |
| Diarrhea (yes) | 26.1 (24/92) | 19.7 (44/223) | 1.44 | 0.21 |
| Frequency of diarrhea, % (n/N) | ||||
| No diarrhea | 73.9 (68/92) | 80.3 (179/223) | N/A | 0.014 |
| Once a month | 16.3 (15/92) | 16.6 (37/223) | ||
| Once a week | 2.2 (2/92) | 2.2 (5/223) | ||
| Once a day | 7.6 (7/92) | 0.9 (2/223) | ||
| Risk group, % (n/N) | ||||
| Heterosexual | 70.9 (61/86) | 79.0 (166/210) | N/A |
0.046 |
| Homosexual | 27.9 (24/86) | 15.7 (33/210) | ||
| Transexual/Bisexual | 1.2 (1/86) | 5.2 (11/210) | ||
|
6.5 (6/92) | 5.8 (13/223) | ||
| HIV acquisition, % (n/N) | ||||
| Sexual | 92.4 (85/92) | 88.8 (198/223) | N/A | 0.64 |
| Vertical | 0.0 (0/92) | 0.9 (2/223) | ||
| Parenteral | 0.0 (0/92) | 0.4 (1/223) | ||
| Unknown | 7.6 (7/92) | 9.9 (22/223) | ||
| CD4+ nadir, median (IQR), /uL | 234 (131, 369) | 261 (117, 378) | N/A | 0.84 |
|
46.7 (43/92) | (92/223) | ||
| Current CD4+, median (IQR), /uL | 427 (265, 574) | 431 (293, 592) | N/A | 0.61 |
|
30.4 (28/92) | 31.4 (70/223) | ||
| Current CD4+ < 200/ml, % (n/N), /ml | 18.8 (12/64) | 9.8 (15/153) | 2.12 | 0.069 |
|
30.4 (28/92) | 31.4 (70/223) | ||
|
Uncontrolled HIV viral load, (> 20 copies/ml), % (n/N) |
29.4 (25/85) | 18.4 (40/217) | 1.84 | 0.037 |
|
7.6 (7/92) | 2.7 (6/223) | ||
| Poor ART adherence ≤ 95%, % (n/N) | 14.8 (12/81) | 14.2 (26/183) | 1.05 | 0.90 |
|
12.0 (11/92) | 17.9 (40/223) |
Data shown as % (n/N) or median (interquartile range: IQR), unless specified otherwise. Variables with a p value < 0.10 are shown in bold and were included in the multivariable analysis. Percentages may not total 100 due to rounding. aScientific work, teaching, architecture or politics. bDefined as absence of paved streets. Abbreviations: N/A: Not Applicable. ART: anti-retroviral therapy.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



