1. Introduction
Gastrointestinal [GI] bleeding, a notable complication occurring more than 30 days after transcatheter aortic valve replacement [TAVR], is recognized as a significant predictor of long-term prognosis and mortality in TAVR patients. GI bleeding can be classified into upper GI bleeding [UGIB] and lower GI bleeding [LGIB]. UGIB occurs in the esophagus, stomach, or duodenum, proximal to the ligament of Treitz, and is typically manifested by hematemesis and melena. The most common causes of UGIB include peptic ulcer disease, esophagogastric varices, and esophagitis [
6].
In contrast, LGIB occurs in the jejunum, ileum, or large intestine, distal to the ligament of Treitz, with hematochezia being a common clinical presentation. Frequent causes of LGIB include diverticulosis and other colonic and small bowel diseases. The evaluation and diagnosis of UGIB are primarily conducted via endoscopy, while LGIB is typically assessed using colonoscopy. Risk factors for both UGIB and LGIB include the use of nonsteroidal anti-inflammatory drugs [NSAIDs], antiplatelet agents, and anticoagulants [
6,
7].
Management strategies for GI bleed primarily depend on identifying the underlying cause. For instance, the most common etiology of UGIB is peptic ulcer disease, often managed with proton pump inhibitors [PPIs] and discontinuation of NSAIDs if implicated. In cases of LGIB, diverticular disease is a frequent cause, with endoscopic interventions such as clipping and ligation commonly employed. Overall, PPIs are frequently used in the hospital setting for both the prevention and treatment of GI bleed [
8].
TAVR patients are uniquely predisposed to bleeding due to periprocedural acquired von Willebrand syndrome, routine antithrombotic therapy [dual antiplatelets or anticoagulants], and advanced age with multiple comorbidities such as chronic kidney disease and anemia [
3,
6]. In TAVR patients, the risk of GI bleeding can be indicated by findings from perioperative evaluations, including complete blood counts, coagulation assessments, and fecal occult blood tests. Baseline conditions also play a significant role, with factors such as prior GI bleeding, older age, atrial fibrillation, and female sex being associated with a higher risk of unfavorable postoperative outcomes [
8].
Given the potential predictors of GI bleeding risk in TAVR patients, understanding how these factors interact with anti-platelet therapy and re-evaluating these strategies is essential for optimizing patient outcomes following TAVR. This study aims to assess multiple mortality risks in patients receiving dual antiplatelet therapy [DAPT] compared to single antiplatelet therapy [SAPT] post-TAVR at a tertiary care medical center, with a specific focus on major bleeding risks, particularly gastrointestinal [GI] bleeding. The objectives of the study are twofold: [a] to determine whether a history of or new-onset GI bleeding in patients on antiplatelet therapy influences clinical outcomes in TAVR patients, and [b] to evaluate whether the selection of SAPT over DAPT [aspirin and clopidogrel] affects the incidence of adverse cardiac events in TAVR patients with a history of or de novo GI bleeding.
2. Materials and Methods
This study was conducted in a single tertiary care medical center that covers medical care for 150-mile radius including approximately 3 million people. This is a retrospective cohort study primarily conducted by chart review to identify patients fitting inclusive and exclusive criteria and to allow for adequate time to measure outcomes. Data was aggregated by researchers of the study from electronic patient chart review and organized using excel spreadsheet software. A total of 470 patients that underwent TAVR within 2018-2021 were screened for the study. Exclusion criteria included patients who had prior stent placements or those patients who had alternate indications for anticoagulant use, leaving 214 patients remaining. Data points collected included anti-platelet therapy [SAPT vs DAPT], non-GI bleed including type and time frame from procedure, GI bleed including type and time frame from procedure, EGD indications and findings, colonoscopy indications and findings, and interventions. Post TAVR adverse events were also recorded including non-fatal MI, arrythmia, stroke, and all-cause mortality including time frames from procedure. Demographics collected included age, gender, body mass index, hypertension, diabetes mellitus, coronary artery disease, peripheral artery disease, current smoker, atrial fibrillation or flutter, chronic kidney disease and stage. Prior history of all patients included history of GI bleed, prior endoscopy findings and prior colonoscopy findings.
Statistical analysis was conducted using R Version 3.6.3 [R Foundation for Statistical Computing] and Microsoft Excel [Microsoft, Corp]. An initial analysis of baseline variables between the 2 groups was conducted using Wilcox rank sum tests for continuous variables, chi-square test of independence for categorical variables with counts ≥10 in either group, and Fisher exact test for categorical variables with counts <10 in either group. Results were considered statistically significant when p < 0.05.
The primary outcome was to compare the incidence of adverse cardiac events between patients with and without history of or de novo GI bleed. Secondary outcomes included: incidence and description of postoperative GI and non-GI bleeds, bleeding and endoscopic interventions, and all-cause mortality. Exempt determination was granted from the Institutional Review Board.
3. Results
3.1. Cohort Overview and Antiplatelet Exposure
3.1.1. Summary of Therapy Groups
The study compared clinical outcomes among patients receiving single antiplatelet therapy [SAPT] versus dual antiplatelet therapy [DAPT] following transcatheter aortic valve replacement [TAVR]. Patients without pre-existing indications for oral anticoagulation were included, reflecting contemporary practice in which SAPT or DAPT is prescribed to mitigate thrombotic risk after TAVR [
3,
4]. Within this cohort, treatment selection with SAPT or DAPT did not result in meaningful differences in the incidence of adverse cardiac outcomes.
3.2. History of Gastrointestinal [GI] Bleeding and Outcomes
3.2.1. Impact on Post-TAVR Prognosis
A prior history of GI bleeding did not adversely affect mortality or composite adverse cardiac outcomes following TAVR. Patients with antecedent GI bleeds did not demonstrate higher rates of post-procedural events compared with those without such history, indicating that remote GI bleeding is not a contraindication to TAVR in appropriately selected candidates.
3.2.2. Recurrence of GI Bleeding
The incidence of recurrent GI bleeding within 12 months after TAVR was uncommon among patients with a history of GI bleeding. These findings suggest that, under current care pathways, prior GI bleeding alone should not preclude TAVR nor mandate deviation from standard antiplatelet strategies solely on the basis of historical bleeding risk.
3.3. Comparative Effectiveness: SAPT vs DAPT
3.3.1. Adverse Cardiac and Cerebrovascular Events
Across the study population, selection of SAPT or DAPT in patients with prior or de novo GI bleeding had no measurable impact on the incidence of major adverse cardiac or cerebrovascular events. This aligns with accumulating evidence that has failed to show a clear reduction in stroke, myocardial infarction, or death with DAPT compared with SAPT after TAVR and has instead suggested greater bleeding liability with DAPT [
3,
9,
10,
11,
12].
3.4. Bleeding Phenotypes and Mortality Context
3.4.1. Access-Site Versus Non-Access-Site Bleeding
In the Bern TAVR registry, both access-site and non-access-site bleeding were independently associated with higher mortality, with non-access-site bleeding conferring a greater risk than access-site events [
5]. Notably, GI bleeding constituted the majority of non-access-site bleeds in that registry. In contrast to the aggregated non-access-site classification used in Bern, our analysis isolated GI bleeding specifically and found that it did not independently worsen cardiac outcomes, thereby refining the understanding of bleeding phenotypes after TAVR.
3.5. Safety Signals over Time
3.5.1. Contemporary Procedural Risk
Although procedural outcomes after TAVR have improved with operator experience and device iterations, bleeding remains a clinically relevant complication, particularly in the context of antiplatelet therapy [
3]. Within our 12-month follow-up window, observed bleeding rates were consistent with modern series, and recurrent GI bleeding events remained infrequent even among previously affected patients.
3.6. Figures, Tables and Schemes
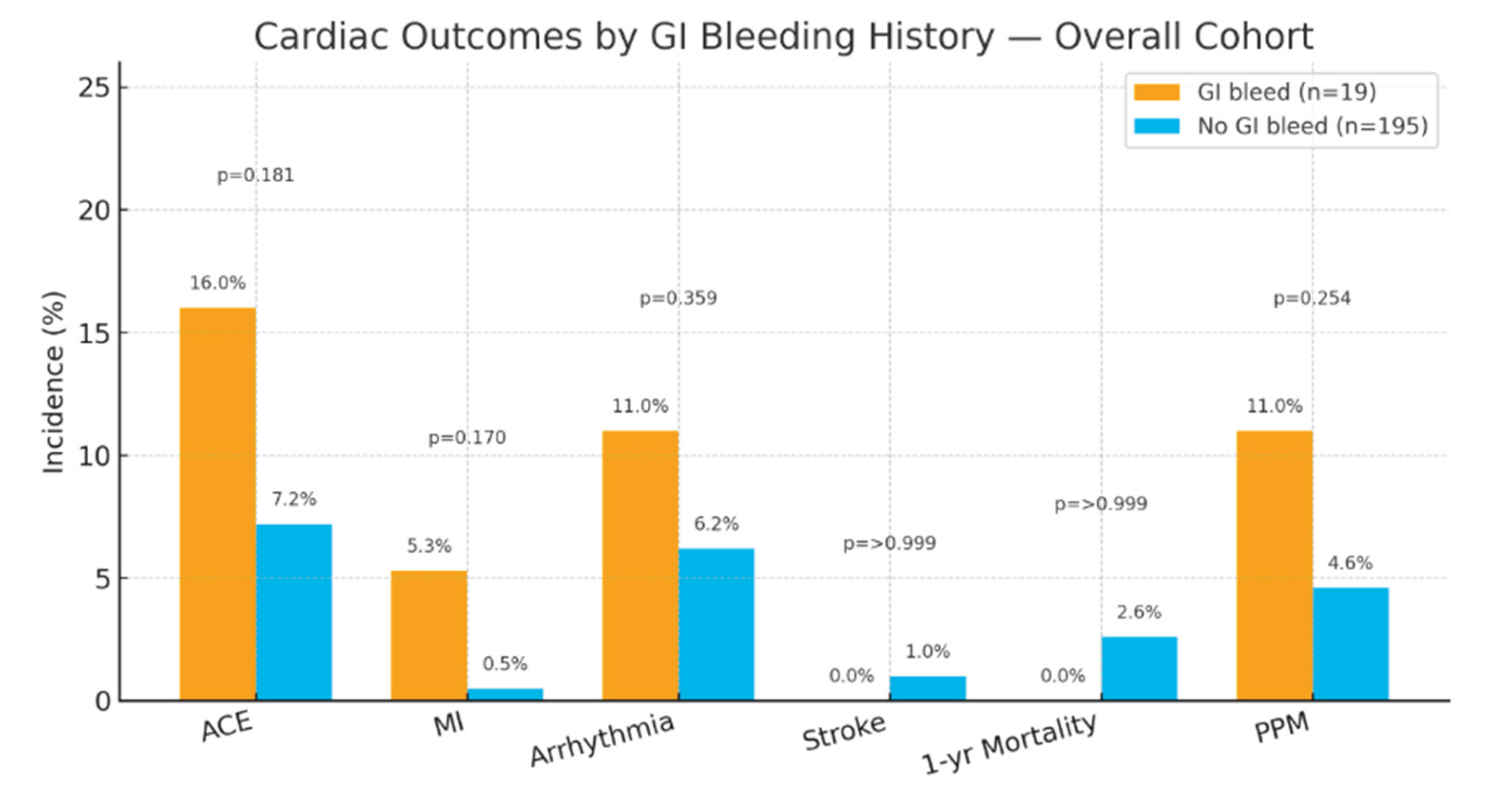
Figure 3.
Cardiac outcomes by GI bleeding history—overall cohort (n=214). Bars show incidence (%) in patients with prior/de novo GI bleed (n=19) versus no GI bleed (n=195). Labels indicate percentages; p-values from Fisher’s exact or Wilcoxon tests as reported. ACE, adverse cardiac events; PPM, permanent pacemaker placement.
Figure 3.
Cardiac outcomes by GI bleeding history—overall cohort (n=214). Bars show incidence (%) in patients with prior/de novo GI bleed (n=19) versus no GI bleed (n=195). Labels indicate percentages; p-values from Fisher’s exact or Wilcoxon tests as reported. ACE, adverse cardiac events; PPM, permanent pacemaker placement.
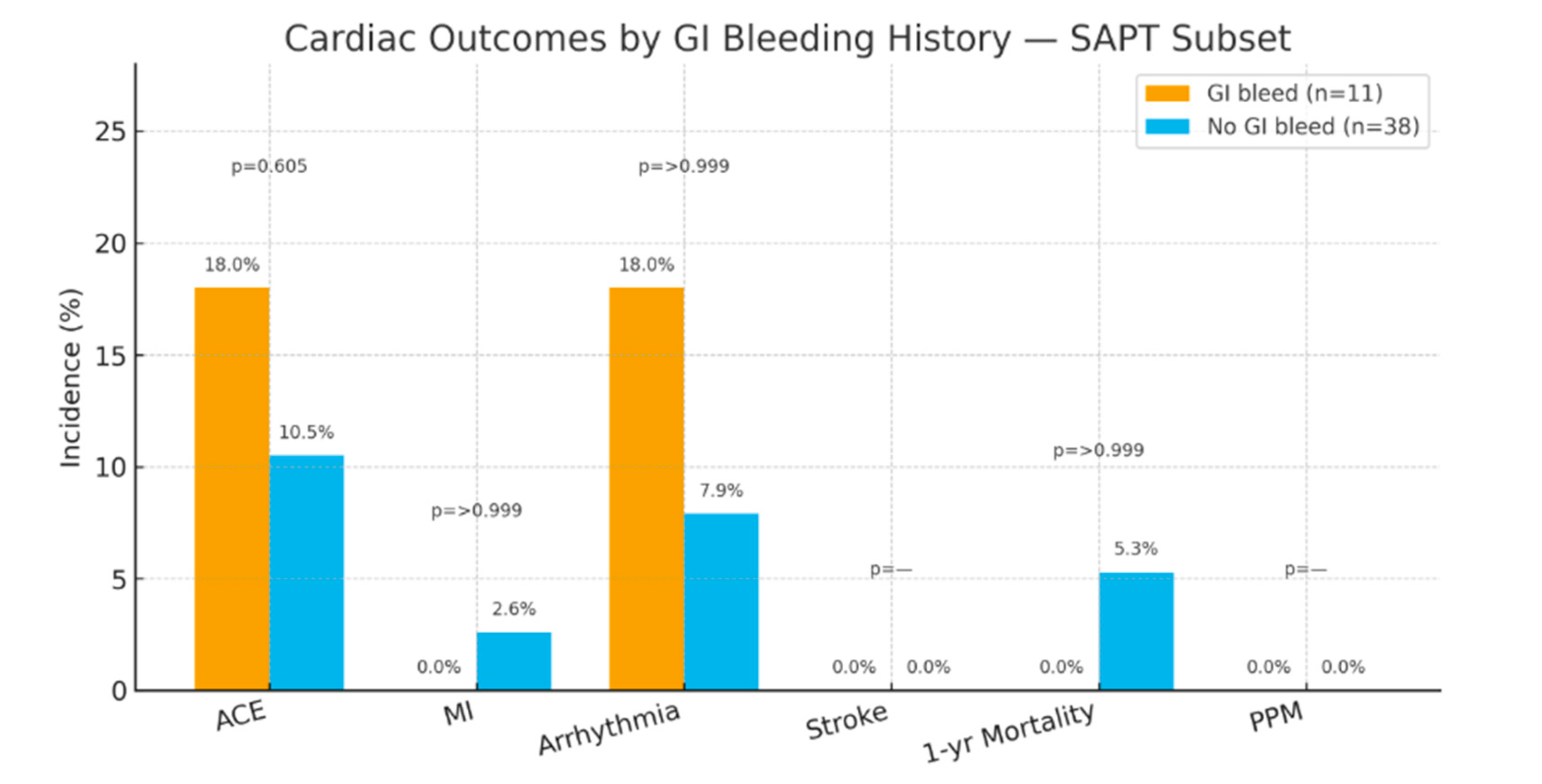
Figure 4.
Cardiac outcomes by GI bleeding history—SAPT subset (n=49). Incidence (%) in GI bleed (n=11) versus no GI bleed (n=38) with reported p-values. ACE, adverse cardiac events; PPM, permanent pacemaker placement.
Figure 4.
Cardiac outcomes by GI bleeding history—SAPT subset (n=49). Incidence (%) in GI bleed (n=11) versus no GI bleed (n=38) with reported p-values. ACE, adverse cardiac events; PPM, permanent pacemaker placement.
Table 1.
Cardiac Outcomes Comparing TAVR patients with and without Prior GI Bleed.
Table 1.
Cardiac Outcomes Comparing TAVR patients with and without Prior GI Bleed.
| Variable |
Setting |
|
History or Denovo GI Bleed
n=19 |
No GI bleed
n=195 |
p-value1
|
| Adverse Cardiac Events |
3 [16%] |
14 [7.2%] |
0.181 |
| MI |
1 [5.3%] |
1 [0.5%] |
0.170 |
| Arrythmia |
2 [11%] |
12 [6.2%] |
0.359 |
| Stroke |
0 [0%] |
2 [1.0%] |
>0.999 |
| 1-year Mortality |
0 [0%] |
5 [2.6%] |
>0.999 |
| Permanent Pacemaker Placement |
2 [11%] |
9 [4.6%] |
0.254 |
| Other Bleeds |
|
|
0.730 |
| Access Site Bleed |
1 [14%] |
5 [25%] |
|
| Access Site Hematoma |
3 [43%] |
8 [40%] |
|
Femoral Artery
Pseudoaneurysm |
2 [29%] |
3 [15%] |
|
| Pericardial Effusion |
0 [0%] |
1 [5%] |
|
1Statistical tests performed: Wilcoxon rank-sum test; Fisher’s exact test
GI: Gastrointestinal; MI: Myocardial Infarction; |
Table 2.
Cardiac Outcomes Comparing TAVR patients on SAPT with and without Prior GI Bleed.
Table 2.
Cardiac Outcomes Comparing TAVR patients on SAPT with and without Prior GI Bleed.
| Variable |
Setting |
|
History or De novo GI Bleed
n = 11 |
No GI bleed
n = 38 |
p-value1
|
| Adverse Cardiac Events |
2 [18%] |
4 [11%] |
0.605 |
| MI |
0 [0%] |
1 [2.6%] |
>0.999 |
| Arrythmia |
2 [18%] |
3 [7.9%] |
>0.999 |
| Stroke |
0 [0%] |
0 [0%] |
|
| 1-year Mortality |
0 [0%] |
2 [5.3%] |
>0.999 |
| Permanent Pacemaker Placement |
0 [0%] |
0 [0%] |
|
| Other Bleeds |
|
|
0.365 |
| Access Site Bleed |
0 [0%] |
0 [0%] |
|
| Access Site Hematoma |
3 [60%] |
2 [40%] |
|
Femoral Artery
Pseudoaneurysm |
2 [40%] |
0 [0%] |
|
| GU hematuria |
0 [0%] |
2 [40%] |
|
| Retroperitoneal Bleed |
0 [0%] |
1 [20%] |
|
1Statistical tests performed: Wilcoxon rank-sum test; Fisher’s exact test
GI: Gastrointestinal; MI: Myocardial Infarction; |
4. Discussion
4.1. Rationale for Antiplatelet Therapy After TAVR
4.1.1. Historical Framework and Evolving Evidence
TAVR has expanded to lower-risk surgical candidates while maintaining high procedural success rates; however, thrombotic and ischemic complications such as stroke, bleeding, and myocardial infarction remain important considerations [
1,
3]. Historically, DAPT—low-dose aspirin plus clopidogrel for 3–6 months followed by lifelong aspirin—was recommended for patients without another indication for anticoagulation [
3]. Emerging data have challenged the routine use of DAPT by demonstrating no superiority over SAPT for ischemic prevention and higher risks of major or life-threatening bleeding with DAPT [
3,
9,
10,
11,
12]. Reflecting these findings, the 2021 ACC/AHA guideline endorses lifelong low-dose aspirin after TAVR [Class IIa, LOE B-NR] and allows DAPT for 3–6 months to be considered only in select patients at low bleeding risk who are not on oral anticoagulation [
4].
4.2. Synthesis with Prior Literature
4.2.1. Meta-Analyses and Randomized Data
A meta-analysis of 12 studies including 20,766 patients associated DAPT with significantly higher rates of combined life-threatening and major bleeding compared with SAPT without clear reductions in ischemic endpoints [
3]. Randomized and prospective data converge on similar conclusions: the POPular TAVI program showed increased bleeding when clopidogrel was added to oral anticoagulation without ischemic benefit [
11], and the ARTE trial demonstrated fewer major or life-threatening events with SAPT relative to DAPT, with no increase in myocardial infarction or stroke [
12]. Additional studies suggest aspirin alone is associated with fewer bleeding events and a lower composite of bleeding and thromboembolism than DAPT over 12 months, though definitions and follow-up horizons vary [
10].
4.3. Interpreting Our Findings in the Context of Bleeding Phenotypes
4.3.1. GI Bleeding as a Distinct Non-Access-Site Entity
The Bern registry reported higher mortality with non-access-site bleeding than with access-site bleeding after TAVR, and GI bleeding accounted for most non-access-site events [
5]. Our analysis disentangled GI bleeding from the broader non-access-site category and found that GI bleeding, whether antecedent or de novo, did not independently worsen cardiac outcomes. This distinction suggests heterogeneity within non-access-site bleeding and supports more nuanced risk stratification, in which GI bleeding—particularly when promptly recognized and managed—may not carry the same prognostic weight as other non-access-site hemorrhages.
4.4. Clinical Implications for Antiplatelet Selection
4.4.1. Individualized Therapy and Guideline-Concordant Care
Taken together, our results support a default strategy of SAPT for most patients after TAVR, consistent with contemporary guidelines and trial evidence, with DAPT reserved for carefully selected, low-bleeding-risk individuals who have compelling thrombotic concerns [
4,
9,
10,
11,
12]. A prior history of GI bleeding should not be viewed as a categorical barrier to TAVR, and routine escalation from SAPT to DAPT solely on the basis of remote GI bleeding is not supported by our data. Where clinically appropriate, strategies to mitigate GI bleeding risk, including optimized gastroprotection and management of modifiable contributors such as anemia or occult ulcer disease, may further improve safety.
4.5. Study Limitations
4.5.1. Design, Sample, and Data Constraints
This single-center, retrospective study with a modest sample size limits generalizability and reduces power to detect small differences in uncommon events. The 12-month follow-up horizon may underestimate late bleeding or thrombotic complications. We lacked systematic data on proton pump inhibitor use, baseline anemia severity, and frailty indices, all of which can influence bleeding and ischemic risk. Medication adherence to SAPT or DAPT could not be strictly verified, introducing exposure misclassification. These constraints temper causal inference and underscore the need for prospective validation.
4.6. Future Directions
4.6.1. Targeted Prospective Evaluation
Future investigations should prospectively evaluate GI bleeding as a distinct endpoint with standardized definitions, adjudication, and extended follow-up beyond 12 months. Trials comparing SAPT versus DAPT in predefined GI-bleed–risk strata, coupled with systematic assessment of gastroprotective strategies such as proton pump inhibitor co-therapy and optimization of anemia and frailty, would clarify the net clinical benefit of antiplatelet regimens after TAVR. Pragmatic designs embedded in TAVR programs could also delineate how patient selection, access techniques, and contemporary valve platforms interact with bleeding phenotypes to influence long-term outcomes.
5. Conclusions
This study demonstrates that selection of treatment between SAPT and DAPT did not predict adverse cardiac events in TAVR patients. Furthermore, patients with history of versus no history of prior GI bleeding were without a difference in adverse cardiac events after TAVR. Our data suggest no large difference in post-TAVR MACE between SAPT and DAPT, but a larger prospective trial is needed to confirm equivalence. These findings further demonstrate that a history of GI bleed in a patient is not a contraindication to TAVR. Consequently, treatment selection of SAPT versus DAPT post-operatively for TAVR patients with history of prior or post-de novo GI bleed has no impact on incidence of adverse cardiac outcomes.
Perspectives:
Competency in Medical Knowledge: A history of gastrointestinal bleeding in TAVR patients does not contraindicate the procedure, and the selection between SAPT and DAPT does not significantly impact adverse cardiac outcomes.
Competency in Patient Care and Procedural Skills: Clinicians should consider that patients with a history of GI bleeding can undergo TAVR without increased risk of adverse cardiac events and can be managed effectively on SAPT, potentially reducing bleeding risks.
Competency in Systems-Based Practice: Healthcare providers should integrate these findings into antiplatelet therapy decision-making post-TAVR to minimize unnecessary bleeding risk without compromising cardiac outcomes
Translational Outlook 1: Future research should explore patient-specific risk stratification models to better guide antiplatelet therapy selection post-TAVR, particularly for those with a bleeding history.
Translational Outlook 2: Additional studies could evaluate long-term outcomes of SAPT versus DAPT in broader populations, assessing whether SAPT could become the standard for patients with high bleeding risk post-TAVR.
Abbreviations
The following abbreviations are used in this manuscript:
| Transcatheter Aortic Valve Replacement |
(TAVR) |
| Dual Anti-Platelet Therapy |
(DAPT) |
| Single Anti-Platelet Therapy |
(SAPT) |
| Aspirin |
(ASA) |
| Gastrointestinal |
(GI) |
| Upper Gastrointestinal Bleed |
(UGIB) |
| Lower Gastrointestinal Bleed |
(LGIB) |
| Myocardial Infarction |
(MI) |
| Oral Anti-Coagulation |
(OAC) |
| Proton Pump Inhibitor |
(PPI) |
References
- Eckstein J, Liu S, Toleva O, Yanagawa B, Verma S, Cheema AN. Antithrombotic therapy after transcatheter aortic valve replacement: current perspective. Curr Opin Cardiol. 2021 Mar 1;36[2]:117-124. [CrossRef]
- Keskinbora KH, Keskinbora K. A systematic review of Ibn Sina's [Avicenna] studies: reflections on anatomy. Eur J Anat. 2016;20[1]:99–105.
- Zhang Y, Shen L, Yang W, He B. Dual antiplatelet therapy vs. single antiplatelet therapy after transcatheter aortic valve replacement: an updated systematic review and meta-analysis. Front Cardiovasc Med. 2021;8:679703. [CrossRef]
- Moey MYY, Udani K, Nifong LW, Carabello BA, Morris DL, Shah NN. Optimal antiplatelet and antithrombotic regimen post-transcatheter aortic valve replacement. Eur J Clin Invest. 2023;53:e14071. [CrossRef]
- Piccolo R, Pilgrim T, Franzone A, Valgimigli M, Haynes A, Asami M, Lanz J, Räber L, Praz F, Langhammer B, Roost E, Windecker S, Stortecky S. Frequency, timing, and impact of access-site and non-access-site bleeding on mortality among patients undergoing transcatheter aortic valve replacement. JACC Cardiovasc Interv. 2017;10[14]:1436-1446. [CrossRef]
- Kamboj AK, Hoversten P, Leggett CL. Upper gastrointestinal bleeding: etiologies and management. Mayo Clin Proc. 2019;94[4]:697-703. [CrossRef]
- Aoki T, Hirata Y, Yamada A, Koike K. Initial management for acute lower gastrointestinal bleeding. World J Gastroenterol. 2019;25[1]:69-84. [CrossRef]
- Lu C, Zhang Y. Gastrointestinal bleeding during the transcatheter aortic valve replacement perioperative period: A review. Medicine [Baltimore]. 2022;101[48]:e31953. [CrossRef]
- Raheja H, Garg A, Goel S, et al. Comparison of single versus dual antiplatelet therapy after TAVR: A systematic review and meta-analysis. Catheter Cardiovasc Interv. 2018;00:1–9. [CrossRef]
- Brouwer J, Nijenhuis VJ, Delewi R, et al. Aspirin with or without Clopidogrel after Transcatheter Aortic-Valve Implantation. N Engl J Med. 2020;383[15]:1447-1457. [CrossRef]
- Nijenhuis VJ, Brouwer J, Delewi R, et al. Anticoagulation with or without Clopidogrel after Transcatheter Aortic-Valve Implantation. N Engl J Med. 2020;382[18]:1696-1707. [CrossRef]
- Rodés-Cabau J, Masson JB, Welsh RC, et al. Aspirin Versus Aspirin Plus Clopidogrel as Antithrombotic Treatment Following Transcatheter Aortic Valve Replacement With a Balloon-Expandable Valve: The ARTE [Aspirin Versus Aspirin + Clopidogrel Following Transcatheter Aortic Valve Implantation] Randomized Clinical Trial. JACC Cardiovasc Interv. 2017;10[13]:1357-1365. [CrossRef]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).