Submitted:
07 October 2025
Posted:
08 October 2025
You are already at the latest version
Abstract
Introduction: It is unclear in which patients’ bleomycin-induced pulmonary toxicity oc-curs at an increased rate in testicular cancer (TC). Objective: The aim of this study was to analyze the prognostic significance of lympho-cyte-associated inflammation markers that may predict bleomycin-related pulmonary toxicity in TC. Results: Clinical and laboratory data were recorded for 118 patients diagnosed with TC who received bleomycin, with a median age at diagnosis of 32.19±9.62. Symptomatic pulmonary toxicity was present in 19.49% (n=23) of patients. Of these, 66.67% had a DLCO decrease of more than 10%. When comparing patients with and without pulmo-nary toxicity, there were no differences in terms of age at diagnosis, performance status, histopathological subgroup, tumor size, lymphovascular invasion, diagnostic symptom, stage, number of adjuvant treatment cycles, and tumor marker levels. Patients with pul-monary toxicity were more likely to be active smokers than those without pulmonary tox-icity, and NLR>1.64, PLR>93.92, CLR>0.49, SII>444.25, and SIRI>0.66 were found to be statistically significant. Lymphocyte-related inflammation markers (NLR, PLR, LMR, CLR, SII, and SIRI) were found to be prognostic for pulmonary toxicity. There was 5.2 times more pulmonary toxicity in smokers than in non-smokers. The prognostic inflammation markers that enable us to predict pulmonary toxicity are TC. Conclusion: The employment of lymphocyte-related inflammation biomarkers at the commencement of treatment offers a means of predicting bleomycin-related pulmonary toxicity in TC.
Keywords:
bleomycin
; pulmonary toxicity
; testicular cancer
; lymphocyte-related inflammation markers
; NLR
; PLR
; LMR
; CLR
; SII
; SIRI
1. Introduction
Reactions to pharmaceutical agents used in the treatment of neoplastic diseases are a prevalent form of iatrogenic injury. The occurrence of toxicity is more frequently observed in organs with high blood flow, such as the lungs, and this damage is often unpredictable in patients. The following essay will provide a comprehensive overview of the relevant literature on the subject [1,2].
Although testicular cancer (TC) accounts for only 1% of male cancers, it is the most common solid tumor affecting young men (15-35 years old). There are two categories of TC established for treatment and diagnosis purposes. These are pure seminoma (no non-seminomatous histopathological elements) and nonseminomatous germ cell carcinoma (NSGCT) [3). The most common presenting complaints are painless mass, pain, swelling, cough, dyspnea, back pain, loss of appetite, nausea, bone pain, peripheral edema, and gynecomastia [4]. The treatment plan for TC patients is determined by the stage of the disease, tumor markers, and risk factors. Bleomycin is an important antineoplastic agent used in both the metastatic and adjuvant phases of TC treatment. Before starting treatment, the risk of developing bleomycin-related pulmonary toxicity should be assessed, and follow-up for late toxicity should be ensured after treatment [5].
Numerous pathophysiological mechanisms have been investigated to explain the cause of antineoplastic-induced pulmonary damage. Bleomycin promotes free radical formation, inhibits angiogenesis, and increases programmed cell death. In this way, it exerts its antitumor effect. The bleomycin hydrolase enzyme involved in bleomycin inactivation is not present in lung tissue. It is thought that bleomycin causes damage to the pulmonary vascular endothelium by increasing free radicals and cytokines. This pathophysiological process can progress to fibrosis [6].
The diagnosis is made by evaluating symptoms, radiological imaging, changes in lung volumes on spirometry (pulmonary function test; PFT), and carbon monoxide diffusion capacity (DLCO) in combination. Patients receive this diagnosis when it is considered and other differential diagnoses are ruled out. While many agents with pulmonary toxicity respond effectively to steroid treatment, similar results cannot be achieved with bleomycin. Although there is no proven treatment, patients who develop bleomycin-related pulmonary toxicity and enter the recovery process almost always experience complete recovery. Mechanisms causing antineoplastic-related pulmonary toxicity include treatment-induced direct damage to alveolar endothelium and pneumocytes, systemic cytokine release, increased oxidative stress, inflammatory cell migration, T cell activation, accompanying non-cardiogenic pulmonary edema, and cellular damage resulting from alveolar macrophage and lymphocyte activation [7,8,9,10]. Cough, shortness of breath, sputum, fever, weight loss, and hypoxemia are the most common accompanying symptoms and findings. Clinical signs may appear at different time intervals and are not specific to the treatment agent. Symptoms may be identified at the start of treatment or afterwards [7,8]. Abnormalities detected in the PFT and DLCO assist in the diagnostic process [11].
Bronchoalveolar lavage (BAL) of pulmonary toxicity frequently reveals lymphocytosis, neutrophilia, and eosinophilia [7]. Interstitial pneumonia, diffuse alveolar damage, hypersensitivity pneumonia, eosinophilic pneumonia, nonnecrotizing granulomatous inflammation, pulmonary veno-occlusive disease, and alveolar hemorrhage are the defined histopathological findings [12]. Atopic mice are resistant to bleomycin-related pulmonary toxicity. This demonstrates the importance of the inflammatory process in the pathogenesis of the disease [13]. The most common BAL finding is lymphocytosis, and based on this histopathological finding, the lymphocyte-related inflammation markers (neutrophil/lymphocyte ratio (NLR), platelet/lymphocyte ratio (PLR), lymphocyte/monocyte ratio (LMR), CRP/lymphocyte ratio (CLR), systemic immune inflammation score (SII), systemic inflammation response index (SIRI)) that could enable us to predict bleomycin-related pulmonary toxicity based on this histopathological finding. The effect of pulmonary toxicity on survival and prognosis in TC was evaluated.
2. Materials and Methods
Data Collection and Patient Characteristics
Adverse drug reactions associated with antineoplastic agents are a common form of iatrogenic injury, with the lungs being a frequent target. Although many are unpredictable in terms of toxicity, pulmonary toxicity accompanied by severe respiratory failure has been described in a small proportion of patients. Bleomycin is an important antineoplastic agent used in both the adjuvant and metastatic stages of testicular cancer treatment. Following up of testicular cancer patients after this treatment is important.
This study included 118 TC patients diagnosed with seminoma, NSGCT and mixed germ cell tumor (mGCT) who presented it to the Medical Oncology Clinic between January 2014 - January 2024 and received bleomycin at any stage of treatment. The clinical and demographic characteristics of the patients were retrospectively recorded from patient files and the hospital laboratory system. The systemic treatments administered to the patients, their treatment responses, progressions, and survival data were recorded. The SFT and DLCO values of patients who developed symptomatic pulmonary toxicity related to bleomycin were recorded.
The most common BAL finding in patients with pulmonary toxicity is lymphocytosis. Based on this histopathological finding, the prognostic value of lymphocyte-related inflammation markers (NLR, PLR, LMR, CLR, SII, SIRI) reported in the literature that may predict bleomycin-related pulmonary toxicity was analyzed. Roc curve analysis was performed for the cutoff value of prognostic markers (Figure 1, Figure 2). The effect of pulmonary toxicity on median overall survival (mOS). OS is the time from diagnosis to death or the last follow-up date.

The Purposes and Calculation of Prognostic Markers
Lymphocyte-Related Inflammation Markers (NLR, PLR, LMR, CLR, SII, SIRI)
NLR (neutrophil-lymphocyte ratio): A marker indicating inflammatory response, calculated by dividing the neutrophil count by the lymphocyte count (Neutrophil/Lymphocyte), which has been shown in the literature to be prognostic in solid tumors [14].
PLR (platelet-lymphocyte ratio): A prognostic marker indicating the inflammatory response, calculated by dividing the platelet count by the lymphocyte count (Platelet/Lymphocyte) [14].
LMR (lymphocyte-monocyte ratio): A prognostic marker indicating the inflammatory response, calculated by dividing the lymphocyte count by the monocyte count (Lymphocyte/Monocyte) [14].
CLR (CRP-lymphocyte ratio): A prognostic marker indicating inflammatory response, calculated by dividing the CRP value by the lymphocyte count (CRP/Lymphocyte) [15].
SII (Systemic Inflammation Score): A prognostic marker indicating the inflammatory response, calculated using the ‘Platelet*Neutrophil/Lymphocyte’ formula [16].
SIRI (Systemic Inflammation Response Index): A prognostic marker indicating the inflammatory response, calculated using the ‘Neutrophil*Monocyte/Lymphocyte’ formula [17].
Statistical Analysis
Descriptive statistics of the data obtained from the study were presented as mean, standard deviation, median, minimum, and maximum values for numerical variables and as frequency and percentage analysis for categorical variables. The normality of numerical variables was examined using the Shapiro Wilk test. The Mann-Whitney U test was used to compare these variables according to pulmonary toxicity status. Additionally, differences between categorical variables were tested using the chi-square analysis. ROC analysis was used to determine the cutoff point for lymphocyte-related inflammation markers (NLR, PLR, LMR, CLR, SII, SIRI). Univariate and Multivariate Logistic regression analysis were used to analyze variables that could affect pulmonary toxicity. The analyses were performed using the SPSS 22.0 program. Statistically significant results (p<0.05) are indicated with a (*) sign next to the p value.
3. Results
The demographic characteristics of patients are presented in Table 1. According to this, 80.51% (n=95) had no symptomatic pulmonary toxicity, while 19.49% (n=23) had pulmonary toxicity. Among those with pulmonary toxicity, 66.67% had a DLCO decrease of more than 10%, while 33.33% had a DLCO decrease of 10% or less. In addition, GCSF was used in 54.55% of those with pulmonary toxicity. The diagnostic symptoms were mass in 44.92%, scrotal swelling in 29.66%, and pain in 25.42%. The median age at diagnosis was 32.19±9.62 years. In the age range analysis, the most common age group was 15-29 years (44.92%), followed by 30-39 years (36.44%), and the least common was 50 years and above (5.93%). The pathological subtypes, in order of frequency, are seminoma (36.44%), embryonal carcinoma (16.95%), and mixed GCT (45.76%). There was no epididymal invasion in 94.92%, tunica albuginea invasion in 85.59%, tunica vaginalis invasion in 94.92%, and lymphovascular invasion in 44.07%. The median tumor size was 42.61±24.7 mm. Progression was observed in 21.19% of clinical follow-ups (Table 1).
There were no significant differences between groups in terms of age at diagnosis, performance status, histopathological subtype, tumor size, lymphovascular invasion, diagnostic symptom, stage, number of adjuvant treatment cycles, and tumor marker levels. Patients with pulmonary toxicity were more likely to be active smokers than those without pulmonary toxicity and had NLR>1.64, PLR>93.92, CRP/Lymphocyte>0.49, SII>444.25, and SIRI>0.66 (Table 2).
Univariate and multivariate logistic regression analyses were performed for variables thought to predict pulmonary toxicity. Univariate analysis found that smoking and lymphocyte-related inflammation markers (NLR, PLR, LMR, CLR, SII, and SIRI) were statistically significant prognostic factors for pulmonary toxicity. Smokers had 5.2 times more pulmonary toxicity than non-smokers (Table 3).
Since all patients with pulmonary toxicity in this study survived, OS calculations could not be performed. The results of this study indicate that bleomycin-related pulmonary toxicity is not a poor prognostic indicator, contrary to survival data showing reduced survival in lung cancer patients who develop pulmonary toxicity.
4. Discussion
The diagnosis of pulmonary toxicity caused by antineoplastic agents is a comprehensive exclusion diagnosis and is therefore difficult. Prognostic inflammation markers that enable us to predict pulmonary toxicity are thought to be helpful in this process.
The levels of NLR, PLR, CLR, SII, and SIRI markers show statistically significant differences according to the status of pulmonary toxicity. Pulmonary toxicity was detected more frequently in smokers and in patients with higher values of lymphocyte-related inflammation markers at the time of initial diagnosis (NLR>1.64, PLR>93.92, CLR>0.49, SII>444.25 and SIRI>0.66). There were no significant differences between the groups in terms of age at diagnosis, performance status, histopathological subgroup, tumor size, lymphovascular invasion, diagnostic symptom, stage, number of adjuvant treatment cycles, and tumor marker levels. This indicates that the number of variables that could affect the grouping outcome was minimal. The most striking finding in this study was that, based on univariate analysis, lymphocyte-associated inflammation markers (NLR, PLR, LMR, CLR, SII, and SIRI) above the defined cutoff value and being an active smoker were statistically significant prognostic factors for pulmonary toxicity.
When considering drug-related toxicity, opportunistic lung infections, radiation damage, heart failure, lymphangitic carcinomatosis, pulmonary metastasis, and pulmonary tumor embolism should be considered in the differential diagnosis [18]. The suspected causative agent should be discontinued after preliminary diagnosis. There is no proven treatment in the literature other than glucocorticoid use and empirical supportive care [12,19]. Supportive care includes inhaled bronchodilators, supplemental oxygen, and mechanical ventilation. The degree of pulmonary toxicity determines the decision to reuse the causative drug [7,20].
Bleomycin is a significant antineoplastic agent employed in both adjuvant therapy and the metastatic stage of TC, the most prevalent solid malignancy in young males. Pulmonary damage has been observed in up to 10% cases involving the administration of bleomycin, an antitumor antibiotic [21,22,23].
In this study, a higher incidence of bleomycin-related symptomatic pulmonary toxicity (23 patients (19.49%)) was recorded than that reported in the literature. It is hypothesized that this increase can be attributed to several concomitant pathophysiological factors. The study revealed a high rate of granulocyte colony-stimulating factor (GCSF) use (12 patients (54.55%)) among patients who developed pulmonary toxicity. Retrospective records indicated that this was due to prolonged neutropenia. It was hypothesized that GCSF use may have increased the toxicity rate. The concomitant use of GCSF in bleomycin-containing treatment protocols is a risk factor for the development of bleomycin-related pulmonary damage in animal studies. However, human studies have yielded both positive and negative results. The rationale for this phenomenon, as elucidated by the extant literature, has been attributed to disparities in median age [24,25,26,27,28,29].
The primary rationale behind clinicians' hesitancy to employ GCSF during bleomycin-containing therapy pertains to its potential for pulmonary toxicity. However, should a patient have a documented history of febrile neutropenia, the prevailing treatment approach entails the administration of GCSF on the day of bleomycin infusion [30].
Another potential explanation may be the high prevalence of a history of smoking. The study found that 42 patients (35.59%) were active smokers, and pulmonary toxicity was observed in 13 of them (31%). Most cases of pulmonary toxicity were observed in patients who smoked (13 patients [56.52%]). The pulmonary toxicity levels in smokers were found to be 5.2 times higher than those observed in non-smokers. This finding indicated that smoking-related chronic inflammation may augment the risk of drug-related pulmonary toxicity. Despite the existence of studies within the extant literature which appear to support this finding [10,31,32,33], it should be noted that there have also been studies which have failed to obtain significant results [26,34].
Drug-related lung injury is more common in elderly patients [23]. In this study, pulmonary toxicity was most common in the 15-29 age group (10 patients (43.48%), with its frequency decreasing with increasing age. The positive aspect of this result is that none of the patients who developed pulmonary toxicity died. In the literature, the mean age of patients without fatal toxicity is 33, while the mean age of patients with fatal pulmonary toxicity is 55 [35]. This result supports the absence of mortality in our study, which is attributed to the low median age at diagnosis.
Drug-related pulmonary toxicity most commonly presents symptoms within one to six months after the start of treatment. Clinical signs, symptoms, physical examination findings, and radiological findings are nonspecific. A restrictive SFT pattern and decreased DLCO may be present. It is a diagnosis of exclusion. Resolution of symptoms following discontinuation of treatment supports the diagnosis [36].
In this study, patients who developed antineoplastic-related pulmonary toxicity after differential diagnosis were identified from oncology file records. Patients with dyspnea after bleomycin administration were included in the pulmonary toxicity group. A DLCO decrease of more than 10% was observed in 66.67% of patients (n=14), while a DLCO decrease of 10% or less was observed in 33.33% (n=7). This result was consistent with literature. Bleomycin-related toxicity may be accompanied by a significant decrease in DLCO. However, small changes that are not correlated with symptoms may also occur [11,37,38]. If DLCO is shown to be below 30%-35% of the baseline value in drug toxicity, discontinuation of bleomycin use is recommended [39,40]. In 13% of patients (n:3), the DLCO decrease was above 30%-35%, but this did not affect the follow-up surveys.
It was noted that bleomycin use was discontinued in all symptomatic patients, and they completed the planned oncological treatment. Inhaler support therapy and intravenous steroids were administered. Symptoms subsided, and after completing treatment without bleomycin, they were placed on follow-up without treatment. Nineteen patients (82.61%) had received bleomycin during the adjuvant period, while the remainder had received it during first-line treatment in the postoperative relapse phase. Age at diagnosis, performance status, histopathological subgroup, tumor size, diagnostic symptom, stage, number of adjuvant treatment cycles, and tumor marker levels were similar in the groups with and without toxicity. Therefore, the prognostic value of lymphocyte-related inflammation markers (NLR, PLR, CLR, SII, and SIRI) was interpreted more reliably. Statistical analysis results showed that lymphocyte-associated inflammation markers (NLR>1.64, PLR>93.92, CLR>0.49, SII>444.25, and SIRI>0.66) evaluated at the time of initial diagnosis and before starting bleomycin treatment were prognostically useful for predicting pulmonary toxicity.
Radiographic findings of bleomycin-induced pulmonary toxicity are nonspecific, including ground-glass opacity, increased reticular markings, pleural effusion, focal consolidation areas, volume loss, and blunting of the costophrenic angle [7,41,42]. Chest X-ray is used to rule out differential diagnoses [43]. Restricted spirometry patterns, such as decreased forced vital capacity (FVC) and total lung capacity (TLC), is present. The clinical manifestation of this is a decrease in oxygen saturation and dyspnea at rest and during exertion due to abnormalities in gas Exchange [44]. As was the case with the initial complaint of all patients who developed bleomycin-related pulmonary toxicity in this study, the most common symptom of drug-related pulmonary toxicity is dyspnea [10].
In a study conducted in patients with non-small cell lung cancer, it was observed that the prognosis was poor in patients who developed pulmonary toxicity, with mOS of 3.5 months [45].
Pulmonary toxicity is one of the side effects that alarm clinicians. We don't know what's going to happen to these patients. So, the idea behind this study is to add to the existing knowledge on the subject. As all patients with pulmonary toxicity survived in this study, we couldn't calculate OS. This suggests that bleomycin-related pulmonary toxicity is not necessarily a sign of a poor prognosis, despite survival data showing that lung cancer patients who develop pulmonary toxicity have a shorter life expectancy.
BAL has frequently revealed lymphocytosis, neutrophilia, and eosinophilia in cases of pulmonary toxicity [7]. Histopathological findings include interstitial pneumonia, diffuse alveolar damage, hypersensitivity pneumonia, eosinophilic pneumonia, non necrotizing granulomatous inflammation, pulmonary Veno-occlusive disease, and alveolar hemorrhage [12]. The most common findings in BAL suggested that lymphocyte-associated inflammation markers (NLR, PLR, LMR, CLR, SII, and SIRI) may be prognostic markers that allow us to predict bleomycin-associated pulmonary toxicity. Atypical mice are resistant to bleomycin-related lung toxicity. This result demonstrates the importance of the inflammatory process in the pathogenesis of the disease [13].
All patients scheduled to receive bleomycin should be assessed for the risk of developing drug-related pulmonary toxicity prior to treatment. SFT and DLCO should be performed prior to treatment to determine lung capacity. They should be repeated when symptoms develop, and serial measurements should be taken. The optimal test frequency has not been determined. TC patients who will receive three/four courses of BEP (bleomycin, etoposide, cisplatin) are defined risk factors for concomitant GCSF use, a concurrent radiotherapy plan to the lung parenchyma, chronic lung disease, advanced age, and a history of smoking [46]. In addition, the use of lymphocyte-related inflammation markers (NLR, PLR, LMR, CLR, SII, and SIRI) in follow-up is thought to enable clinicians to predict patients with a high likelihood of developing pulmonary toxicity. Serial follow-up of prognostic tests is particularly important for patients with high risk factors. Reassessment before each treatment cycle is recommended.
Following the first publications suggesting that a decrease in DLCO is the earliest indicator of pulmonary toxicity leading to bleomycin discontinuation [47,48], studies emerged suggesting that SFT and DLCO are neither specific nor sensitive [10,49,50,51]. Finally, in a randomized controlled phase 3 trial, it was recommended that SFT be performed only in symptomatic patients and that computed tomography of the chest be performed early if deemed necessary [52]. In this patient group, where there is still no specific standardization, it is thought that the use of lymphocyte-related inflammation markers (NLR, PLR, CLR, SII, and SIRI), which can be calculated from the results of routine pre-treatment blood counts and biochemical tests, would be beneficial.
The most important limitations of our study are that it is a single-center experience and that the data were obtained from retrospective medical records. This is a common limitation in studies evaluating inflammatory markers. Future prospective studies will guide the prognostic value of lymphocyte-related inflammation markers (NLR, PLR, CLR, SII, and SIRI) in patients scheduled for bleomycin. The exclusion criteria for this study included obesity, chronic disease with lung parenchymal involvement, and a history of radiotherapy to the lung. This ensured that confounders that could affect the results of the inflammation scores were avoided. The absence of such exclusion criteria in studies in literature adds value to the results of this study.
5. Conclusions
The diagnosis of antineoplastic agent-related pulmonary toxicity is a detailed exclusion diagnosis. When drug toxicity is considered, the treatment agent should be discontinued. The reduction in symptoms following discontinuation of treatment supports the diagnosis. There is no proven treatment other than glucocorticoid use and empirical supportive care. The degree of pulmonary toxicity determines the decision to restart the drug. Lymphocyte-associated inflammation markers (NLR, PLR, CLR, SII, and SIRI) are prognostic in the development of drug-related pulmonary toxicity in testicular cancer patients receiving bleomycin therapy.
Author Contributions
“Conceptualization, methodology, software, validation, formal analysis, investigation, data curation, resources, writing—review and editing, M.Ö and G.G.D.; and all authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee. Non-interventional ethics committee approval was obtained from Pamukkale University Faculty of Medicine. (No: E60116787-020-521149, committee meeting dated 02.05.2024 and numbered E.521149).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study and the use of anonymized data, as approved by the Institutional Review Board.
Data Availability Statement
The data underlying this article will be shared at reasonable request to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| TC | Testicular cancer | |
| NSGCT | Nonseminomatous germ cell carcinoma | |
| PFT | Pulmonary function test | |
| BAL | Bronchoalveolar lavage | |
| DLCO | Carbon monoxide diffusion capacity | |
| NLR | Neutrophil/lymphocyte ratio | |
| PLR | Platelet/lymphocyte ratio | |
| LMR | Lymphocyte/monocyte ratio | |
| CLR | CRP/lymphocyte ratio | |
| SII | Systemic immune inflammation score | |
| SIRI | Systemic inflammation response index | |
| mGCT | Mixed germ cell tumor | |
| mOS | Median overall survival | |
| GCSF | Granulocyte colony-stimulating factor | |
| FVC | Forced vital capacity | |
| TLC | Total lung capacity | |
| BEP | Bleomycin, etoposide, cisplatin | |
| MDPI | Multidisciplinary Digital Publishing Institute | |
| DOAJ | Directory of open access journals | |
| TLA | Three letter acronym | |
| LD | Linear dichroism | |
References
- Ozkan M.; Dweik R.A.; Ahmad M. Drug-induced lung disease. Cleve clin j med. 2001; 68, 782-785, 789-795. https://doi:10.3949/ccjm.68.9.782.
- Nebeker J.R.; Barach P.; Samore M.H. Clarifying adverse drug events: a clinician's guide to terminology, documentation, and reporting. Ann intern med. 2004; 140, 795-801. [CrossRef]
- Dieckmann K.P.; Richter-Simonsen H.; Kulejewski M.; Ikogho R.; Zecha H.; Anheuser P.; Pichlmeier U.; Isbarn H. Testicular Germ-Cell Tumours: A Descriptive Analysis of Clinical Characteristics at First Presentation. Urol int. 2018; 100, 09-419. [CrossRef]
- Shah Y.B.; Goldberg H.; Hu B.; Daneshmand S.; Chandrasekar T. Metastatic Testicular Cancer Patterns and Predictors: A Contemporary Population-based SEER Analysis. Urology. 2023; 180, 182-189. [CrossRef]
- Haugnes H.S.; Aass N.; Fosså S.D.; Dahl O.; Brydøy M.; Aasebø U.; Wilsgaard T.; Bremnes R.M. Pulmonary function in long-term survivors of testicular cancer. J clin oncol. 2009; 27, 2779-2786. [CrossRef]
- Lauritsen J.; Kier M.G.; Mortensen M.S.; Bandak M.; Gupta R.; Holm N.V.; Agerbaek M.; Daugaard G. Germ Cell Cancer and Multiple Relapses: Toxicity and survival. j clin oncol. 2015; 33, 3116-3123. [CrossRef]
- Vahid B.; Marik P.E. Pulmonary complications of novel antineoplastic agents for solid tumors. Chest. 2008; 133, 528-538. [CrossRef]
- Limper A.H. Chemotherapy-induced lung disease. Clin chest med. 2004; 25, 53-64. [CrossRef]
- Possick J.D. Pulmonary Toxicities from Checkpoint Immunotherapy for Malignancy. Clin Chest Med. 2017; 38, 223-232. [CrossRef]
- Sleijfer S. Bleomycin-induced pneumonitis. Chest. 2001; 120, 617-624. [CrossRef]
- Yerushalmi R.; Kramer M.R.; Rizel S.; Sulkes A.; Gelmon K.; Granot T.; Neiman V.; Stemmer S.M. Decline in pulmonary function in patients with breast cancer receiving dose-dense chemotherapy: A prospective study. Ann oncol. 2009; 20, 437-440. [CrossRef]
- Camus P.; Bonniaud P.; Fanton A.; Camus C.; Baudaun N.; Foucher P. Drug-induced and iatrogenic infiltrative lung disease. Clin chest med. 2004; 25, 479-519. https://doi:10.1016/j.ccm.2004.05.006.
- Schrier D.J.; Phan S.H.; McGarry B.M. The effects of the nude (nu/nu) mutation on bleomycin-induced pulmonary fibrosis. A biochemical evaluation. Am rev respir dis. 1983; 127, 614-617. [CrossRef]
- Otsuka R.; Hayashi H.; Uesato M.; Hayano K.; Murakami K.; Toyozumi T.; Matsumoto Y.; Kurata Y.; Nakano A.; Takahashi Y.; Arasawa T.; Matsubara H. Inflammatory and Nutritional Indices as Prognostic Markers in Elderly Patients With Gastric Cancer. Anticancer Res. 2023; 43, 5261-5267. [CrossRef]
- Ruan G.T.; Xie H.L.; Yuan K.T.; Lin S.Q.; Zhang H.Y.; Liu C.A.; Shi J.Y.; Ge Y.Z.; Song M.M.; Hu C.L.; Zhang X.W.; Liu X.Y.; Yang M.; Wang K.H.; Zheng X.; Chen Y.; Hu W.; Cong M.H.; Zhu L.C.; Deng L.; Shi H.P.; Prognostic value of systemic inflammation and for patients with colorectal cancer cachexia. J cachexia sarcopenia muscle. 2023; 14, 2813-2823. [CrossRef]
- Nøst T.H.; Alcala K.; Urbarova I.; Byrne K.S.; Guida F.; Sandanger T.M.; Johansson M. Systemic inflammation markers and cancer incidence in the UK Biobank. Eur j epidemiol. 2021; 36, 841-848. [CrossRef]
- Zhang S.; Cheng T. Prognostic and clinicopathological value of systemic inflammation response index (SIRI) in patients with breast cancer: a meta-analysis. Ann med. 2024; 56, 2337729. [CrossRef]
- Blumenschein G.R. Jr.; Gatzemeier U.; Fossella F.; Stewart D.J.; Cupit L.; Cihon F.; O'Leary J.; Reck M. Phase II, multicenter, uncontrolled trial of single-agent sorafenib in patients with relapsed or refractory, advanced non-small-cell lung cancer. J clin oncol. 2009; 27, 4274-4280. [CrossRef]
- Nicolls M.R.; Terada L.S.; Tuder R.M.; Prindiville S.A.; Schwarz M.I. Diffuse alveolar hemorrhage with underlying pulmonary capillaritis in the retinoic acid syndrome. Am j respir crit care med. 1998; 158, 1302-1305. [CrossRef]
- Lee C.; Gianos M.; Klaustermeyer W.B. Diagnosis and management of hypersensitivity reactions related to common cancer chemotherapy agents. Ann Allergy Asthma Immunol. 2009; 102, 179-187. [CrossRef]
- Meadors M.; Floyd J.; Perry M.C. Pulmonary toxicity of chemotherapy. Semin oncol. 2006; 33, 98-105. [CrossRef]
- Jules-Elysee K.; White D.A. Bleomycin-induced pulmonary toxicity. Clin chest med. 1990; 11, 1-20.
- O'Sullivan J.M.; Huddart R.A.; Norman A.R.; Nicholls J.; Dearnaley D.P.; Horwich A. Predicting the risk of bleomycin lung toxicity in patients with germ-cell tumours. Ann oncol. 2003; 14, 91-96. [CrossRef]
- Lazo J.S.; Merrill W.W.; Pham E.T.; Lynch T.J.; McCallister J.D.; Ingbar D.H. Bleomycin hydrolase activity in pulmonary cells. J pharmacol exp ther. 1984; 231, 583-588.
- Martin W.G.; Ristow K.M.; Habermann T.M.; Colgan J.P.; Witzig T.E.; Ansell S.M. Bleomycin pulmonary toxicity has a negative impact on the outcome of patients with Hodgkin's lymphoma. J clin oncol. 2005; 23, 7614-7620. [CrossRef]
- Stamatoullas A.; Brice P.; Bouabdallah R.; Mareschal S.; Camus V.; Rahal I.; Franchi P.; Lanic H.; Tilly H. Outcome of patients older than 60 years with classical Hodgkin lymphoma treated with front line ABVD chemotherapy: frequent pulmonary events suggest limiting the use of bleomycin in the elderly. Br j haematol. 2015; 170-184. [CrossRef]
- Fosså S.D.; Kaye S.B.; Mead G.M.; Cullen M.; de Wit R.; Bodrogi I.; van Groeningen C.J.; De Mulder P.H.; Stenning S.; Lallemand E.; De Prijck L.; Collette L. Filgrastim during combination chemotherapy of patients with poor-prognosis metastatic germ cell malignancy. European Organization for Research and Treatment of Cancer, Genito-Urinary Group, and the Medical Research Council Testicular Cancer Working Party, Cambridge, United Kingdom. j clin oncol. 1998; 16, 716-724. [CrossRef]
- Saxman S.B.; Nichols C.R.; Einhorn L.H. Pulmonary toxicity in patients with advanced-stage germ cell tumors receiving bleomycin with and without granulocyte colony stimulating factor. Chest. 1997; 111, 657-660. [CrossRef]
- Evens A.M.; Cilley J.; Ortiz T.; Gounder M.; Hou N.; Rademaker A.; Miyata S.; Catsaros K.; Augustyniak C.; Bennett C.L.; Tallman M.S.; Variakojis D.; Winter J.N.; Gordon L.I. G-CSF is not necessary to maintain over 99% dose-intensity with ABVD in the treatment of Hodgkin lymphoma: low toxicity and excellent outcomes in a 10-year analysis. Br j haematol. 2007; 137, 545-552. [CrossRef]
- Nichols C.R.; Catalano P.J.; Crawford E.D.; Vogelzang N.J.; Einhorn L.H.; Loehrer P.J. Randomized comparison of cisplatin and etoposide and either bleomycin or ifosfamide in treatment of advanced disseminated germ cell tumors: an Eastern Cooperative Oncology Group, Southwest Oncology Group, and Cancer and Leukemia Group B Study. J clin oncol. 1998; 16, 1287-1293. [CrossRef]
- Lauritsen J.; Kier M.G.; Bandak M.; Mortensen M.S.; Thomsen F.B.; Mortensen J.; Daugaard G. Pulmonary Function in Patients With Germ Cell Cancer Treated With Bleomycin, Etoposide, and Cisplatin. J clin oncol. 2016; 34, 1492-1499. [CrossRef]
- Chaudhary U.B.; Haldas J.R. Long-term complications of chemotherapy for germ cell tumours. Drugs. 2003; 63, 1565-1577. [CrossRef]
- Lower E.E.; Strohofer S.; Baughman R.P. Bleomycin causes alveolar macrophages from cigarette smokers to release hydrogen peroxide. Am j med sci. 1988; 295, 193-197. [CrossRef]
- Thomas T.S.; Luo S.; Reagan P.M.; Keller J.W.; Sanfilippo K.M.; Carson K.R. Advancing age and the risk of bleomycin pulmonary toxicity in a largely older cohort of patients with newly diagnosed Hodgkin Lymphoma. J geriatr oncol. 2020; 11, 69-74. [CrossRef]
- Simpson A.B.; Paul J.; Graham J.; Kaye S.B. Fatal bleomycin pulmonary toxicity in the west of Scotland 1991-95: a review of patients with germ cell tumours. Br j cancer. 1998; 78, 1061-1066. [CrossRef]
- Uzel I.; Ozguroglu M.; Uzel B.; Kaynak K.; Demirhan O.; Akman C.; Oz F.; Yaman M. Delayed onset bleomycin-induced pneumonitis. Urology. 2005; 66, 195. [CrossRef]
- Dimopoulou I.; Efstathiou E.; Samakovli A.; Dafni U.; Moulopoulos L.A.; Papadimitriou C.; Lyberopoulos P.; Kastritis E.; Roussos C.; Dimopoulos M.A. A prospective study on lung toxicity in patients treated with gemcitabine and carboplatin: clinical, radiological and functional assessment. Ann oncol. 2004; 15, 1250-1255. [CrossRef]
- Rivera M.P.; Detterbeck F.C.; Socinski M.A.; Moore D.T.; Edelman M.J.; Jahan T.M.; Ansari R.H.; Luketich J.D.; Peng G.; Monberg M.; Obasaju C.K.; Gralla R.J. Impact of preoperative chemotherapy on pulmonary function tests in resectable early-stage non-small cell lung cancer. Chest. 2009; 135, 1588-1595. [CrossRef]
- Buchler T.; Bomanji J.; Lee S.M. FDG-PET in bleomycin-induced pneumonitis following ABVD chemotherapy for Hodgkin's disease--a useful tool for monitoring pulmonary toxicity and disease activity. Haematologica. 2007; 92, 120-121. [CrossRef]
- von Rohr L.; Klaeser B.; Joerger M.; Kluckert T.; Cerny T.; Gillessen S. Increased pulmonary FDG uptake in bleomycin-associated pneumonitis. Onkologie. 2007; 30, 320-323. [CrossRef]
- Cleverley J.R.; Screaton N.J.; Hiorns M.P.; Flint J.D.; Müller N.L. Drug-induced lung disease: high-resolution CT and histological findings. Clin radiol. 2002; 57, 292-299. [CrossRef]
- Torrisi J.M.; Schwartz L.H.; Gollub M.J.; Ginsberg M.S.; Bosl G.J.; Hricak H. CT findings of chemotherapy-induced toxicity: what radiologists need to know about the clinical and radiologic manifestations of chemotherapy toxicity. Radiology. 2011; 258, 41-56. [CrossRef]
- Sikdar T.; MacVicar D.; Husband J.E. Pneumomediastinum complicating bleomycin related lung damage. Br j radiol. 1998; 71, 1202-1204. [CrossRef]
- Bossi G.; Cerveri I.; Volpini E.; Corsico A.; Baio A.; Corbella F.; Klersy C.; Arico M. Long-term pulmonary sequelae after treatment of childhood Hodgkin's disease. Ann oncol. 1997; 19-24.
- Fujimoto D.; Kato R.; Morimoto T.; Shimizu R.; Sato Y.; Kogo M.; Ito J.; Teraoka S.; Nagata K.; Nakagawa A.; Otsuka K.; Tomii K. Characteristics and Prognostic Impact of Pneumonitis during Systemic Anti-Cancer Therapy in Patients with Advanced Non-Small-Cell Lung Cancer. PLoS one. 2016; 11, 0168465. [CrossRef]
- Watson R.A.; De La Peña H.; Tsakok M.T.; Joseph J.; Stoneham S.; Shamash J.; Joffe J.; Mazhar D.; Traill Z.; Ho L.P.; Brand S.; Protheroe A.S. Development of a best-practice clinical guideline for the use of bleomycin in the treatment of germ cell tumours in the UK. Br j cancer. 2018; 119, 1044-1051. [CrossRef]
- Comis R.L.; Kuppinger M.S.; Ginsberg S.J.; Crooke S.T.; Gilbert R.; Auchincloss J.H.; Prestayko A.W. Role of single-breath carbon monoxide-diffusing capacity in monitoring the pulmonary effects of bleomycin in germ cell tumor patients. Cancer res. 1979; 39, 5076-5080.
- Pascual R.S.; Mosher M.B.; Sikand R.S.; De Conti R.C.; Bouhuys A. Effects of bleomycin on pulmonary function in man. Am rev respir dis. 1973; 108, 211-217. [CrossRef]
- Villani F.; De Maria P.; Bonfante V.; Viviani S.; Laffranchi A.; Dell'oca I.; Dirusso A.; Zanini M. Late pulmonary toxicity after treatment for Hodgkin's disease. Anticancer res. 1997; 4739-4742.
- McKeage M.J.; Evans B.D.; Atkinson C.; Perez D.; Forgeson G.V.; Dady P.J. Carbon monoxide diffusing capacity is a poor predictor of clinically significant bleomycin lung. New Zealand Clinical Oncology Group. J clin oncol. 1990; 779-783. [CrossRef]
- Ng A.K.; Li S.; Neuberg D.; Chi R.; Fisher D.C.; Silver B.; Mauch P.M. A prospective study of pulmonary function in Hodgkin's lymphoma patients. Ann oncol. 2008; 19, 1754-1758. [CrossRef]
- Shamash J.; Sarker S.J.; Huddart R.; Harland S.; Joffe J.K.; Mazhar D.; Birtle A.; White J.; Chowdhury K.; Wilson P.; Marshall M.R.; Vinnicombe S. A randomized phase III study of 72 h infusional versus bolus bleomycin in BEP (bleomycin, etoposide and cisplatin) chemotherapy to treat IGCCCG good prognosis metastatic germ cell tumours (TE-3). Ann oncol. 2017; 28, 1333-1338. [CrossRef]
Figure 1.
Roc curve analysis of lymphocyte-related inflammation markers (neutrophil/lymphocyte ratio (NLR), platelet/lymphocyte ratio (PLR), lymphocyte/monocyte ratio (LMR), CRP/lymphocyte ratio (CLR), systemic immune inflammation score (SII), systemic inflammation response index (SIRI)).
Figure 1.
Roc curve analysis of lymphocyte-related inflammation markers (neutrophil/lymphocyte ratio (NLR), platelet/lymphocyte ratio (PLR), lymphocyte/monocyte ratio (LMR), CRP/lymphocyte ratio (CLR), systemic immune inflammation score (SII), systemic inflammation response index (SIRI)).
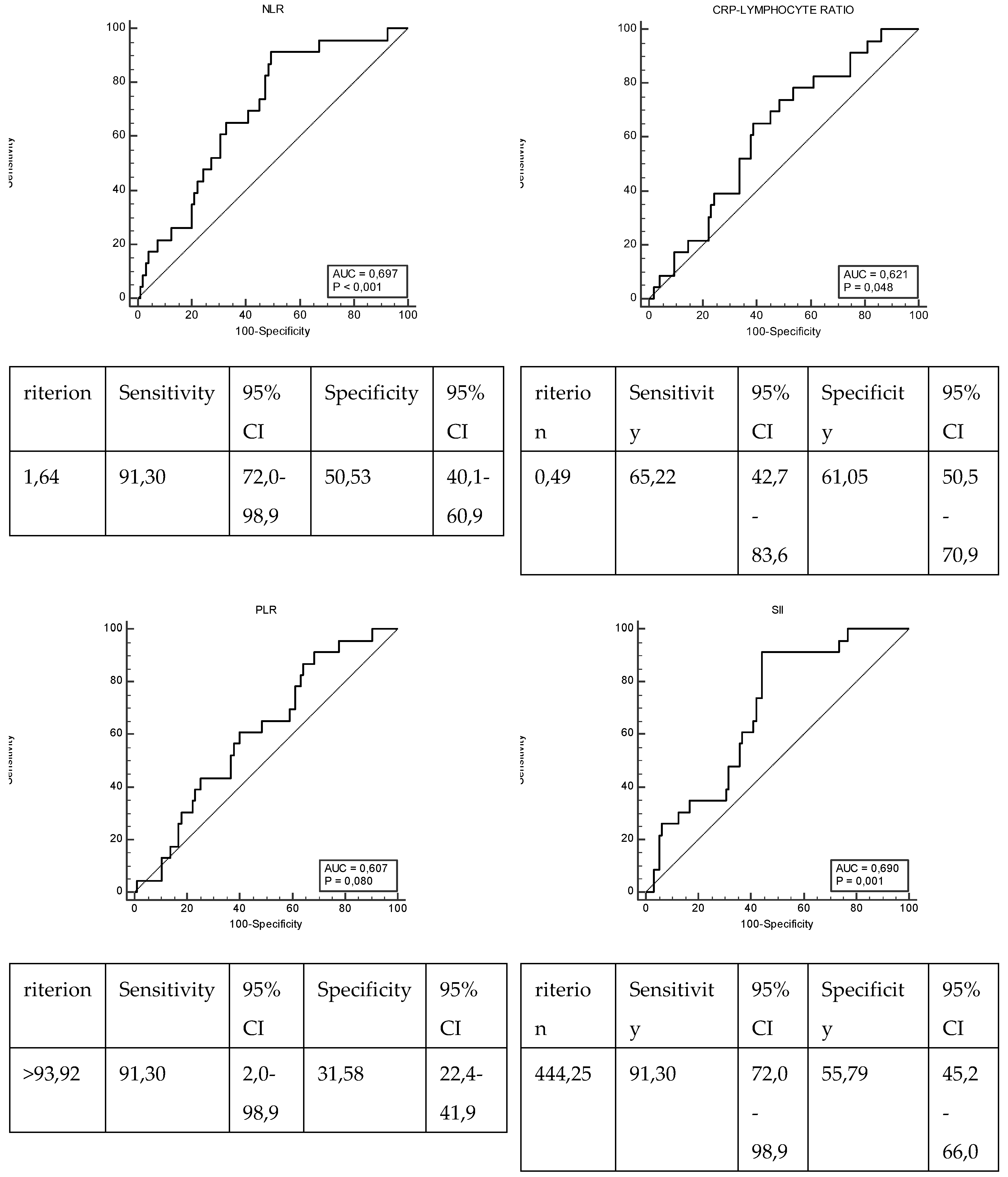
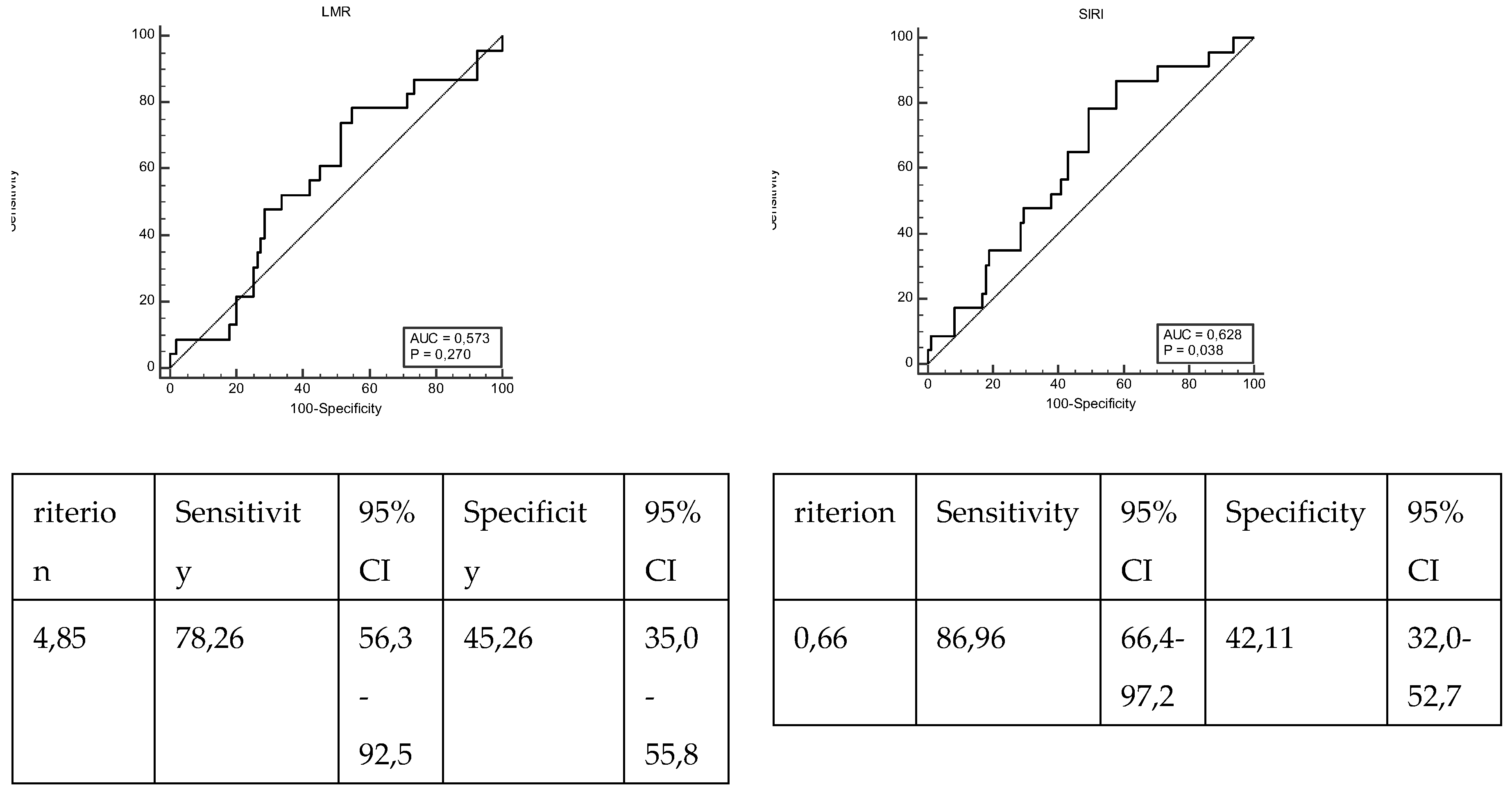
Figure 2.
Roc curve analysis of lymphocyte-related inflammation markers (neutrophil/lymphocyte ratio (NLR), platelet/lymphocyte ratio (PLR), lymphocyte/monocyte ratio (LMR), CRP/lymphocyte ratio (CRP-L), systemic immune inflammation score (SII), systemic inflammation response index (SIRI)).
Figure 2.
Roc curve analysis of lymphocyte-related inflammation markers (neutrophil/lymphocyte ratio (NLR), platelet/lymphocyte ratio (PLR), lymphocyte/monocyte ratio (LMR), CRP/lymphocyte ratio (CRP-L), systemic immune inflammation score (SII), systemic inflammation response index (SIRI)).
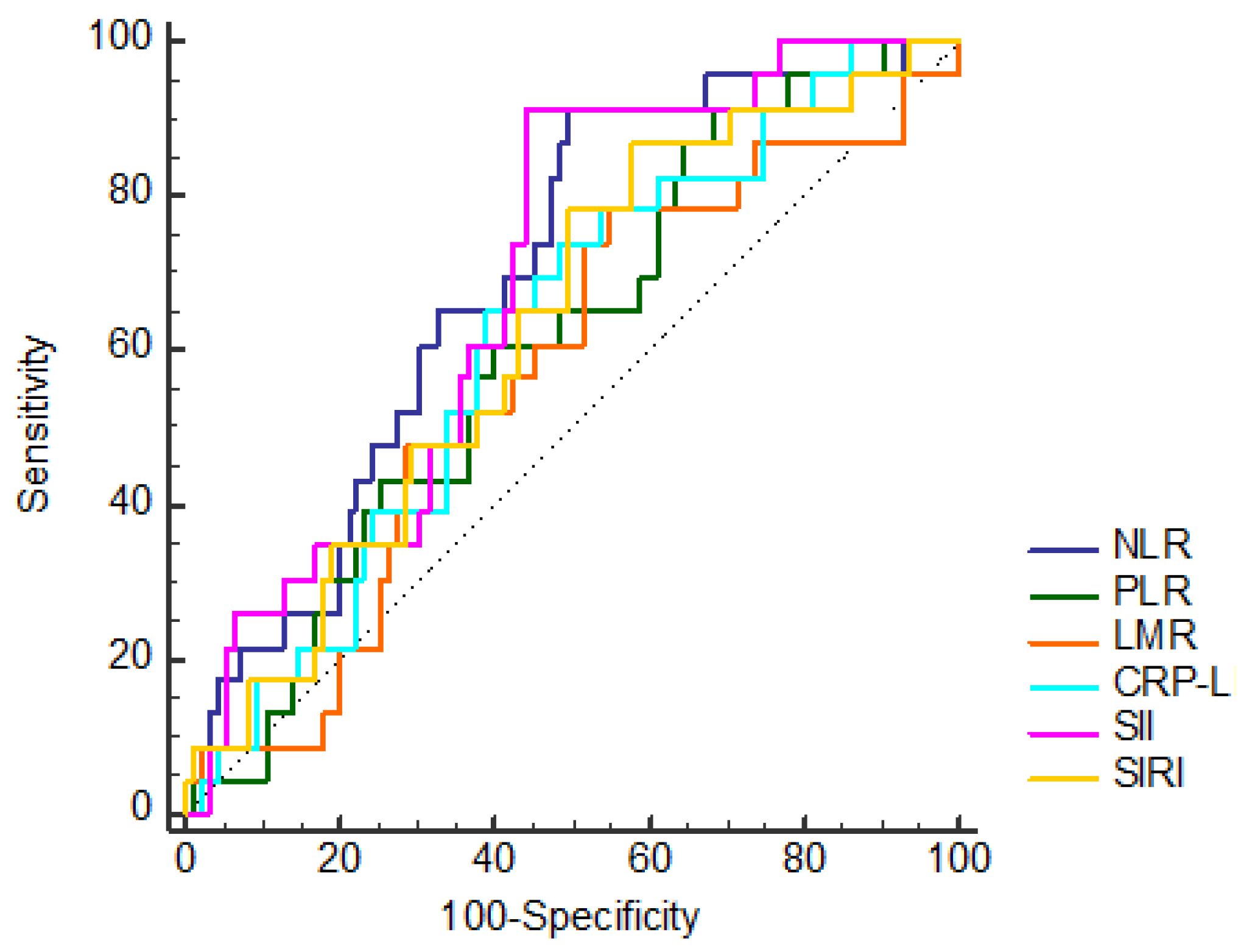

Table 1.
Clinical and demographic characteristics of testicular cancer patients receiving bleomycin in oncological treatment.
Table 1.
Clinical and demographic characteristics of testicular cancer patients receiving bleomycin in oncological treatment.
| Variables | N (%) | |
|---|---|---|
| Age at Diagnosis (median±SS) | 32.19±9.62 | 30.79 (15.73-65.33) |
| Age at Diagnosis | 15-29 years | 53 (44.92) |
| 30-39 years | 43 (36.44) | |
| 40-49 years | 15 (12.71) | |
| ≥ 50 years | 7 (5.93) | |
| Eastern Cooperative Oncology Group (ECOG) Performance Status | 0 | 112 (94.92) |
| 1 | 3 (2.54) | |
| 2 | 1 (0.85) | |
| 3 | 2 (1.69) | |
| Histopathology | Seminoma | 43 (36.44) |
| Embryonal carcinoma | 20 (16.95) | |
| Mixed germ cell carcinoma | 54 (45.76) | |
| Epididymal invasion | No | 112 (94.92) |
| Yes | 6 (5.08) | |
| Tunica albuginea invasion | No | 101 (85.59) |
| Yes | 17 (14.41) | |
| Tunica vaginalis invasion | No | 112 (94.92) |
| Yes | 6 (5.08) | |
| Lymphovascular invasion | No | 52 (44.07) |
| Yes | 66 (55.93) | |
| Tumor localization | Right | 56 (47.46) |
| Left | 59 (50) | |
| Bilateral | 3 (2.54) | |
| Diagnostic symptom | Mass | 53 (44.92) |
| Swelling | 35 (29.66) | |
| Pain | 30 (25.42) | |
| Stage | Stage 1 | 69 (58.47) |
| Stage 2 | 29 (24.58) | |
| Stage 3 | 20 (16.95) | |
| Tumor size | 42.61±24.7 | 35 (6-120) |
| Radiotherapy | No | 113 (95.76) |
| Yes | 5 (4.24) | |
| Surgery | No | 4 (3.39) |
| Yes | 114 (96.61) | |
| Retroperitoneal lymph node dissection | No | 86 (72.88) |
| Yes | 32 (27.12) | |
| Adjuvant therapy | No | 19 (16.1) |
| Yes | 99 (83.9) | |
| Number of adjuvant cycles | 2.96±0.94 | 3 (1-6) |
| Pulmonary toxicity | No | 95 (80.51) |
| Yes | 23 (19.49) | |
| Decrease in DLCO in patients with pulmonary toxicity | ≤%10 | 7 (33.33) |
| >%10 | 14 (66.67) | |
| Use of GCSF in Patients Developing Pulmonary Toxicity | No | 10 (45.45) |
| Yes | 12 (54.55) | |
| Progression | No | 93 (78.81) |
| Yes | 25 (21.19) | |
| Living Situation | Alive | 107 (90.68) |
| Exitus | 11 (9.32) | |
| Median overall survival (mOS) | 159,86±4,34(min/max:151,346-168,364) | |
| NLR | ≤1.64 | 50 (42.37) |
| >1.64 | 68 (57.63) | |
| PLR | ≤93.92 | 32 (27.12) |
| >93.92 | 86 (72.88) | |
| LMR | ≤4.85 | 70 (59.32) |
| >4.85 | 48 (40.68) | |
| CLR | ≤0.49 | 66 (55.93) |
| >0.49 | 52 (44.07) | |
| SII | ≤444.25 | 55 (46.61) |
| >444.25 | 63 (53.39) | |
| SIRI | ≤0.66 | 43 (36.44) |
| >0.66 | 75 (63.56) | |
| Median Forced Vital Capacity (FVC) | 85.96±7.41 | 87 (73-105) |
| Median Carbon Monoxide Diffusion Capacity (DLCO) | 68.18±13.44 | 70 (34-88) |
NLR: neutrophil/lymphocyte ratio, PLR: platelet/lymphocyte ratio, LMR: lymphocyte/monocyte ratio, CLR: CRP/lymphocyte ratio, SII: systemic immune inflammation score, SIRI: systemic inflammation response index.
Table 2.
Comparison of clinical and demographic characteristics according to the severity of bleomycin-related pulmonary toxicity.
Table 2.
Comparison of clinical and demographic characteristics according to the severity of bleomycin-related pulmonary toxicity.
| Variables | Pulmonary toxicity | p | ||
|---|---|---|---|---|
| No | Yes | |||
| N (%) | N (%) | |||
| Age at Diagnosis | 15-29 years | 43 (45,26) | 10 (43,48) | 0,880 |
| 30-39 years | 35 (36,84) | 8 (34,78) | ||
| 40-49 years | 12 (12,63) | 3 (13,04) | ||
| ≥ 50 years | 5 (5,26) | 2 (8,7) | ||
| Smoking History | No | 66 (69,47) | 10 (43,48) | 0,028* |
| Yes | 29 (30,53) | 13 (56,52) | ||
| Eastern Cooperative Oncology Group (ECOG) Performance Status | 0 | 89 (93,68) | 23 (100) | 1,000 |
| 1 | 3 (3,16) | 0 (0) | ||
| 2 | 1 (1,05) | 0 (0) | ||
| 3 | 2 (2,11) | 0 (0) | ||
| Histopathology | Seminoma | 34 (35,79) | 9 (39,13) | 0,716 |
| Embryonal carcinoma | 15 (15,79) | 5 (21,74) | ||
| Mixed germ cell carcinoma | 45 (47,37) | 9 (39,13) | ||
| Epididymal invasion | No | 90 (94,74) | 22 (95,65) | 1,000 |
| Yes | 5 (5,26) | 1 (4,35) | ||
| Tunica albuginea invasion | No | 82 (86,32) | 19 (82,61) | 0,741 |
| Yes | 13 (13,68) | 4 (17,39) | ||
| Tunica vaginalis invasion | No | 89 (93,68) | 23 (100) | 0,596 |
| Yes | 6 (6,32) | 0 (0) | ||
| Lymphovascular invasion | No | 43 (45,26) | 9 (39,13) | 0,646 |
| Yes | 52 (54,74) | 14 (60,87) | ||
| Tumor localization | Right | 46 (48,42) | 10 (43,48) | 0,818 |
| Left | 46 (48,42) | 13 (56,52) | ||
| Bilateral | 3 (3,16) | 0 (0) | ||
| Diagnostic symptom | Mass | 40 (42,11) | 13 (56,52) | 0,362 |
| Swelling | 31 (32,63) | 4 (17,39) | ||
| Pain | 24 (25,26) | 6 (26,09) | ||
| Stage | Stage 1 | 56 (58,95) | 13 (56,52) | 0,381 |
| Stage 2 | 25 (26,32) | 4 (17,39) | ||
| Stage 3 | 14 (14,74) | 6 (26,09) | ||
| Radiotherapy | No | 90 (94,74) | 23 (100) | 0,582 |
| Yes | 5 (5,26) | 0 (0) | ||
| Surgery | No | 4 (4,21) | 0 (0) | 1,000 |
| Yes | 91 (95,79) | 23 (100) | ||
| Retroperitoneal lymph node dissection | No | 69 (72,63) | 17 (73,91) | 1,000 |
| Yes | 26 (27,37) | 6 (26,09) | ||
| Adjuvant therapy | No | 15 (15,79) | 4 (17,39) | 1,000 |
| Yes | 80 (84,21) | 19 (82,61) | ||
| NLR | ≤1,64 | 48 (50,53) | 2 (8,7) | 0,001* |
| >1,64 | 47 (49,47) | 21 (91,3) | ||
| PLR | ≤93,92 | 30 (31,58) | 2 (8,7) | 0,035* |
| >93,92 | 65 (68,42) | 21 (91,3) | ||
| LMR | ≤4,85 | 52 (54,74) | 18 (78,26) | 0,057 |
| >4,85 | 43 (45,26) | 5 (21,74) | ||
| CLR | ≤0,49 | 58 (61,05) | 8 (34,78) | 0,034* |
| >0,49 | 37 (38,95) | 15 (65,22) | ||
| SII | ≤444,25 | 53 (55,79) | 2 (8,7) | 0,001* |
| >444,25 | 42 (44,21) | 21 (91,3) | ||
| SIRI | ≤0,66 | 40 (42,11) | 3 (13,04) | 0,014* |
| >0,66 | 55 (57,89) | 20 (86,96) | ||
NLR:neutrophil/lymphocyte ratio, PLR:platelet/lymphocyte ratio, LMR:lymphocyte/monocyte ratio, CLR:CRP/lymphocyte ratio, SII:systemic immune inflammation score, SIRI:systemic inflammation response index; Fisher-Freeman-Halton Exact Test, Statistically significant results (p<0.05) are indicated with a (*) sign next to the p value.
Table 3.
Univariate and Multivariate Logistic regression for Pulmonary toksisity.
| Variables | Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|
| OR(95%CI) | p | OR(95%CI) | p | ||
| Age at Diagnosis | 15-29 years | 1 (reference) | 0,941 | ||
| 30-39 years | 0,983 (0,35-2,756) | 0,974 | |||
| 40-49 years | 1,075 (0,255-4,538) | 0,922 | |||
| ≥ 50 years | 1,72 (0,291-10,182) | 0,550 | |||
| Smoking History | Yes | 2,959 (1,164-7,52) | 0,023* | 5,23(1,536-17,814) | ,008* |
| Histopathology | Seminoma | 1 (reference) | 0,872 | ||
| Embryonal carcinoma | 1,259 (0,361-4,398) | 0,718 | |||
| Mixed germ cell carcinoma | 0,756 (0,271-2,107) | 0,592 | |||
| Lymphovascular invasion | No | 1 (reference) | |||
| Yes | 1,286 (0,508-3,259) | 0,596 | |||
| Tumor localization | Right | 1 (reference) | 0,855 | ||
| Left | 1,3(0,518-3,263) | 0,576 | |||
| Diagnostic symptom | Mass | 1 (reference) | 0,329 | ||
| Swelling | 0,397 (0,118-1,338) | 0,136 | |||
| Pain | 0,769 (0,258-2,292) | 0,638 | |||
| Stage | Stage 1 | 1 (reference) | 0,374 | ||
| Stage 2 | 0,689 (0,204-2,325) | 0,549 | |||
| Stage 3 | 1,846 (0,596-5,72) | 0,288 | |||
| Retroperitoneal lymph node dissection | No | 1 (reference) | |||
| Yes | 0,937 (0,333-2,635) | 0,901 | |||
| NLR | ≤1,64 | 1 (reference) | |||
| >1,64 | 10,723 (2,38-48,306) | 0,002* | 3,811 (0,389-37,314) | ,250 | |
| PLR | ≤93,92 | 1 (reference) | |||
| >93,92 | 4,846 (1,067-22,015) | 0,041* | 1,863 (0,296-11,727) | ,507 | |
| LMR | ≤4,85 | 1 (reference) | |||
| >4,85 | 0,336 (0,115-0,979) | 0,046* | 1,038 (0,215-5,016) | ,963 | |
| CLR | ≤0,49 | 1 (reference) | |||
| >0,49 | 2,939 (1,134-7,615) | 0,026* | 3,24 (0,995-10,547) | ,051 | |
| SII | ≤444,25 | 1 (reference) | |||
| >444,25 | 13,25 (2,939-59,731) | 0,001* | 8,011 (0,933-68,809) | ,058 | |
| SIRI | ≤0,66 | 1 (reference) | |||
| >0,66 | 4,848 (1,348-17,439) | 0,016* | 0,536 (0,061-4,671) | ,572 | |
NLR: neutrophil/lymphocyte ratio, PLR: platelet/lymphocyte ratio, LMR: lymphocyte/monocyte ratio, CLR: CRP/lymphocyte ratio, SII: systemic immune inflammation score, SIRI: systemic inflammation response index; statistically significant results (p<0.05) are indicated with a (*) sign next to the p value.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



