Submitted:
07 October 2025
Posted:
08 October 2025
You are already at the latest version
Abstract
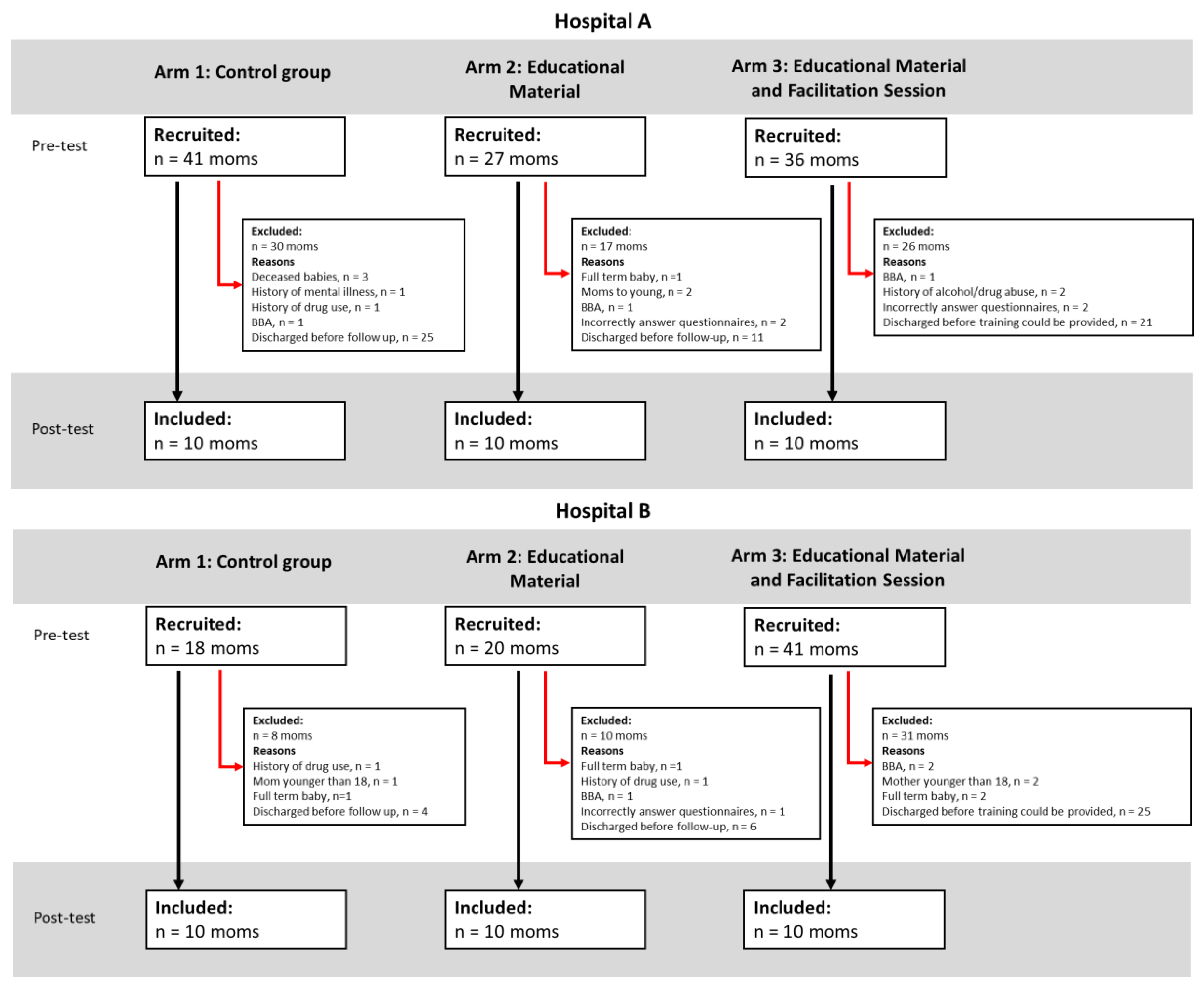
Introduction: Preterm birth and neonatal intensive care unit (NICU) admission may elevate parental stress and impair early parent-infant interaction. In low-resource settings, where staff and resources are limited, parental education programmes are often also limited, further complicating care engagement. This study piloted the NeuroSense PremmieEd parenting educational programme to assess its preliminary impact on maternal stress and knowledge in a South African public-sector NICU. Objectives: This study aims to pilot a contextually relevant parenting education intervention to enhance parental understanding of preterm infant behaviour, strengthen parents’ capacity to interpret and respond sensitively to infant cues, and reduce parental stress during NICU admission. Methodology: This sequential cohort pilot study involved 60 mothers of preterm infants (gestational age 24–36 weeks) admitted to two comparable NICUs. Mothers (aged 18–45 years) were allocated to three groups. Arm 1 received standard care (n = 20), Arm 2 received a printed educational booklet (n = 20), and Arm 3 received the booklet plus a facilitated education session (n = 20). Pre- and post-intervention data were collected using the Knowledge of Preterm Infant Behaviour (KPIB) questionnaire and the Parental Stressor Scale: NICU (PSS:NICU). Descriptive statistics were used to explore differences across arms.Results: Knowledge scores measured with the KPIB tool showed a positive trend across all groups, with the greatest improvement observed in Arm 3; however, changes were not statistically significant (p = .176). Maternal stress measured using the PSS:NICU increased significantly over time across all groups (F(1, 57) = 8.40, p = .005), with Arm 3 consistently reporting the lowest stress at both timepoints. The overall rise in stress likely reflects the cumulative burden of prolonged NICU exposure, including infant health concerns, environmental stressors, and the demands of acquiring new caregiving knowledge and skills. Discussion: The facilitated intervention was associated with a trend towards improved maternal knowledge of preterm infant behaviour. This pilot highlighted the potential of structured, culturally relevant education to support early parenting in a public sector neonatal intensive care unit in South Africa. Maternal stress levels remained high across all groups. While this finding may be due to parent’s experience of changes in infant medical condition, fatigue, and other factors, it was not investigated in the study and therefore warrants further exploration in future work. Conclusion: The NeuroSense PremmieEd programme shows promise in improving maternal understanding of preterm infant behaviour. The results highlight the need for further adaptation of content delivery, inclusion of diverse populations (e.g., by preterm category) and scalable, low-resource approaches to improve engagement and long-term outcomes.
Keywords:
Background
Study Aim
Methods
Design
Recruitment of Participants
Inclusion Criteria
Exclusion Criteria
Sample Size
Procedures and Data Collection
Measures
Demographics and Clinical Descriptive Data
Arm Assignment
Arm 1: Control (Standard Care)
Arm 2: Educational Booklet
Arm 3: Booklet and In-Person Session
Data Analysis
Ethical Considerations
Results
Infant Characteristics

| Infants | ||||||||
| Hospital A | Hospital B | |||||||
| Variable |
Arm 1 (n = 11) |
Arm 2 (n = 11) |
Arm 3 (n = 12) |
Total (n = 34) |
Arm 1 (n = 11) |
Arm 2 (n = 12) |
Arm 3 (n = 11) |
Total (n = 34) |
| Gestational Age (weeks) | ||||||||
| Min | 24 | 26 | 26 | 24 | 26 | 31 | 27 | 26 |
| Max | 33 | 35 | 35 | 35 | 35 | 36 | 35 | 36 |
| Mean | 29.2 | 30.1 | 31 | 30.1 | 30.4 | 32.556 | 30.4 | 31.069 |
| Standard Deviation | 2.486 | 2.85 | 2.582 | 2.657 | 2.591 | 1.740 | 2.875 | 2.590 |
| Birth weight (in grams) | ||||||||
| Min | 950 | 705 | 1020 | 705 | 730 | 1060 | 760 | 730 |
| Max | 1690 | 2500 | 2500 | 2500 | 1700 | 2200 | 2390 | 2390 |
| Mean | 1275 | 1383 | 1537 | 1402 | 1224 | 1465 | 1185 | 1300 |
| Standard deviation | 210 | 470 | 393 | 380 | 311 | 323 | 599 | 428 |
| Head circumference (in cm) | ||||||||
| Min | 23 | 23 | 24 | 23 | 23 | 29 | - | 23 |
| Max | 29.5 | 37 | 33 | 37 | 30 | 34 | - | 34 |
| Mean | 27.363 | 28.714 | 27.857 | 27.88 | 27.4 | 31.5 | - | 28.571 |
| Standard Deviation | 1.9 | 4.31 | 3.338 | 2.981 | 2.702 | 3.536 | - | 3.309 |
| Missing Values | - | 4 | 4 | 8 | 6 | 10 | 11 | 27 |
| Apgar (1 min) | ||||||||
| Min | 2 | 3 | 6 | 2 | 1 | 2 | 0 | 0 |
| Max | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 |
| Mean | 6.556 | 6.75 | 7.667 | 6.913 | 7.454 | 7.5 | 7.143 | 7.4 |
| Standard Deviation | 2.79 | 1.91 | 1.033 | 2.109 | 2.77 | 2.28 | 3.237 | 2.608 |
| Missing Values | 1 | 3 | 5 | 9 | - | - | 3 | 3 |
| Apgar (5 min) | ||||||||
| Min | 6 | 5 | 8 | 6 | 5 | 3 | 0 | 0 |
| Max | 9 | 10 | 10 | 10 | 9 | 10 | 9 | 10 |
| Mean | 8.625 | 8.125 | 8.833 | 8.5 | 8.364 | 8.583 | 7.86 | 8.33 |
| Standard deviation | 1.06 | 1.46 | 0.753 | 1.144 | 1.689 | 2.065 | 3.485 | 2.279 |
| Missing values | 2 | 3 | 5 | 10 | - | - | 3 | 3 |
| Sex | ||||||||
| Male | 3 | 5 | 6 | 14 | 5 | 6 | 5 | 16 |
| Female | 8 | 6 | 6 | 20 | 6 | 6 | 6 | 18 |
KPIB Results
The Parental Stressor Scale: Neonatal Intensive Care Unit (PSS:NICU)
| Hospital A | Hospital B | Hospital A & B (pooled data) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Arm 1 | Arm 2 | Arm 3 | Total | Arm 1 | Arm 2 | Arm 3 | Total | Arm 1 | Arm 2 | Arm 3 | Total | |
| Pre-test KPIB | ||||||||||||
| Average Score out of 36 | 11.7 | 11.8 | 9.9 | 11.1 | 12.5 | 12.5 | 12.1 | 12.4 | 12.1 | 12.15 | 11 | 11.7 |
| Average percentage | 33% | 33% | 28% | 31% | 35% | 35% | 34% | 34% | 33.61% | 33.5% | 30.56% | 32.64% |
| Post-test KPIB | ||||||||||||
| Average Score out of 36 | 11.2 | 12.7 | 11.6 | 11.8 | 13.4 | 12.5 | 13.3 | 12.93 | 11.85 | 12.73 | 12.45 | 12.36 |
| Average percentage | 31% | 35% | 32% | 33% | 37% | 35% | 37% | 36% | 32.92% | 35.35% | 34.58% | 34.35% |
| Change between pre- and post-test (in %) | -2% | +2% | +4% | +2% | +2% | 0% | +3% | +2% | -0.69% | +1.85% | +4.02% | +1.71% |
| Pre-test NICU:PSS | ||||||||||||
| Average Score out of 170 | 128.7 | 112.6 | 99.1 | 113.5 | 88.3 | 101.9 | 104.2 | 98.13 | 108.50 | 107.25 | 101.65 | 105.81 |
| Average percentage | 76% | 66% | 58% | 67% | 52% | 60% | 61% | 58% | 63.82% | 63.09% | 59.79% | 62.24% |
| Post-test NICU:PSS | ||||||||||||
| Average Score out of 170 | 119.9 | 121.5 | 105.3 | 115.6 | 113.6 | 130 | 110.6 | 118.07 | 116.75 | 125.75 | 107.95 | 116.84 |
| Average percentage | 71% | 71% | 62% | 68% | 67% | 76% | 65% | 69% | 68.68% | 73.97% | 63.5% | 68.73% |
| Change between pre- and post-test | -4% | +5% | +4% | +1% | +15% | +16% | +4% | +11% | +4.86% | +10.88% | +3.71% | +6.49% |
Discussion
Limitations, Challenges, and Considerations for Future Research
Implications for Practice and Future Research
Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Use of Artificial Intelligence
Acknowledgments
Conflicts of Interest
References
- Abbasinia, N.; Rad, Z.A.; Qalehsari, M.Q.; Gholinia, H.; Arzani, A. The effect of instructing mothers in attachment behaviors on short-term health outcomes of premature infants in NICU. Journal of Education and Health Promotion 2023, 12, 1–8. [Google Scholar] [CrossRef]
- Aboud, F.E.; Choden, K.; Tusiimi, M.; Gómez, R.; Hatch, R.; Dang, S.; Betancourt, T.S.; Dyenka, K.; Umulisa, G.; Omoeva, C. A tale of two programs for parents of young children: Independently-conducted case studies of workforce contributions to scale in Bhutan and Rwanda. Children 2023, 10. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, K.; Haque, M.; Khatoon, S. Kangaroo Mother Care: A simple method to care for low-birth-weight infants in developing countries. Journal of Shaheed Suhrawardy Medical College 2013, 5, 49–54. [Google Scholar] [CrossRef]
- Baker, B.J.; McGrath, J. Parent education: The cornerstone of excellent neonatal nursing care. Newborn and Infant Nursing Reviews 2011, 11, 6–7. [Google Scholar] [CrossRef]
- Bastani, F.; Rajai, N.; Farsi, Z.; Als, H. The effects of kangaroo care on the sleep and wake states of preterm infants. Journal of Nursing Research 2017, 25, 231–239. [Google Scholar] [CrossRef]
- Black, S.E.; Devereux, P.J.; Salvanes, K.G. Does grief transfer across generations? Bereavements during pregnancy and child outcomes. American Economic Journal: Applied Economics 2016, 8, 193–223. [Google Scholar] [CrossRef]
- Brett, J.; Staniszewska, S.; Newburn, M.; Jones, N.; Taylor, L. A systematic mapping review of effective interventions for communicating with, supporting and providing information to parents of preterm infants. BMJ Open 2011, 1, 1–11. [Google Scholar] [CrossRef]
- Browne, J.V.; Talmi, A. Family-based intervention to enhance infant–parent relationships in the neonatal intensive care unit. Journal of Pediatric Psychology 2005, 30, 667–677. [Google Scholar] [CrossRef]
- Campbell-Yeo, M.L.; Disher, T.C.; Benoit, B.L.; Johnston, C.C. Understanding kangaroo care and its benefits to preterm infants. Pediatric Health Medicine and Therapeutics 2015, 6, 15–32. [Google Scholar] [CrossRef]
- Carozza, S.; Leong, V. The role of affectionate caregiver touch in early neurodevelopment and parent–infant interactional synchrony. Frontiers in Neuroscience 2021, 14, 1–11. [Google Scholar] [CrossRef]
- Creswell, J.W. (2009). Research design: Qualitative, Quantitative and Mixed Methods Approaches. (3rd ed.). Sage.
- de Góes Salvetti, M.; Lauretti, L.G.; Muniz, R.C.; Dias, T.Y.S.F.; Gomes de Oliveira, A.A.D.; Gouveia, L.M.R. Characteristics of pregnant women at risk and relationship with type of delivery and complications. Revista Brasileira de Enfermagem 2021, 74. [Google Scholar] [CrossRef] [PubMed]
- Franck, L.S.; Gay, C.; Hoffmann, T.J.; Kriz, R.M.; Bisgaard, R.; Cormier, D.M.; Joe, P.; Lothe, B.; Sun, Y. Maternal mental health after infant discharge: A quasi-experimental clinical trial of family integrated care versus family-centered care for preterm infants in U.S. NICUs. BMC Pediatrics 2023, 23. [Google Scholar] [CrossRef] [PubMed]
- Givrad, S.; Dowtin, L.L.; Scala, M.; Hall, S.L. Recognizing and mitigating infant distress in Neonatal Intensive Care Unit (NICU). Journal of Neonatal Nursing 2020, 27. [Google Scholar] [CrossRef]
- Hendricks, M.R. How a frightened mother of a preterm newborn eventually flourished. Nursing for Women’s Health 2021, 25, 156–158. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Warre, R.; Qiu, X.; O’Brien, K.; Lee, S.K. Parents as practitioners in preterm care. Early Human Development 2014, 90, 781–785. [Google Scholar] [CrossRef]
- Kim, S.; Kim, A.R. Attachment- and relationship-based interventions during NICU hospitalization for families with preterm/low-birth weight infants: A systematic review of RCT data. International Journal of Environmental Research and Public Health 2022, 19, 1–13. [Google Scholar] [CrossRef]
- Kristensen, I.H.; Juul, S.; Kronborg, H. What are the effects of supporting early parenting by newborn behavioral observations (NBO)? A cluster randomised trial. BMC Psychology 2020, 8. [Google Scholar] [CrossRef]
- Kristiawati, K.; Rustina, Y.; Budi, I.B.; Hariyati Rr, T.S. How to prepare your preterm baby before discharge. Sri Lanka Journal of Child Health 2020, 49, 390–395. [Google Scholar] [CrossRef]
- Loewenstein, K.; Barroso, J.; Phillips, S. The experiences of parent dyads in the neonatal intensive care unit: A qualitative description. Journal of Pediatric Nursing 2021, 60, 1–10. [Google Scholar] [CrossRef]
- Melançon, J.; Aita, M.; Belzile, S.; Lavallée, A. Clinical intervention involving parents in their preterm infant’s care to promote parental sensitivity: A case study. Journal of Neonatal Nursing 2020, 27, 58–62. [Google Scholar] [CrossRef]
- Milgrom, J.; Martin, P.R.; Newnham, C.; Holt, C.J.; Anderson, P.J.; Hunt, R.W.; Reece, J.; Ferretti, C.; Achenbach, T.; Gemmill, A.W. Behavioural and cognitive outcomes following an early stress-reduction intervention for very preterm and extremely preterm infants. Pediatric Research 2019, 86, 92–99. [Google Scholar] [CrossRef]
- Miller, P.M.; Commons, M.L. The benefits of attachment parenting for infants and children: A behavioral developmental view. Behavioral Development Bulletin 2010, 16, 1–14. [Google Scholar] [CrossRef]
- Möller, E.L.; de Vente, W.; Rodenburg, R. Infant crying and the calming response: Parental versus mechanical soothing using swaddling, sound, and movement. PLoS ONE 2019, 14, e0214548. [Google Scholar] [CrossRef] [PubMed]
- Mosher, S.L. Comprehensive NICU parental education: Beyond baby basics. Neonatal Network 2017, 36, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Naeem, N.; Zanca, R.M.; Weinstein, S.; Urquieta, A.; Sosa, A.; Yu, B.; Sullivan, R.M. The neurobiology of infant attachment-trauma and disruption of parent–infant interactions. Frontiers in Behavioral Neuroscience 2022, 16, 1–14. [Google Scholar] [CrossRef]
- Ndjomo, G.; Njiengwe, E.; Moudze, B.; Guifo, O.; Blairy, S. Posttraumatic stress, anxiety, and depression in mothers after preterm delivery and the associated psychological processes. Research Square 2024. [Google Scholar] [CrossRef]
- Nickolls, B.J.; Relton, C.; Hemkens, L.; Zwarenstein, M.; Eldridge, S.; McCall, S.J.; Griffin, X.L.; Sohanpal, R.; Verkooijen, H.M.; Maguire, J.L.; McCord, K.A. Randomised trials conducted using cohorts: A scoping review. BMJ Open 2024, 14, e075601. [Google Scholar] [CrossRef]
- Norholt, H. Revisiting the roots of attachment: A review of the biological and psychological effects of maternal skin-to-skin contact and carrying of full-term infants. Infant Behavior and Development 2020, 60, 1–19. [Google Scholar] [CrossRef]
- Pineda, R.; Bender, J.; Hall, B.; Shabosky, L.; Annecca, A.; Smith, J. Parent participation in the neonatal intensive care unit: Predictors and relationships to neurobehavior and developmental outcomes. Early Human Development 2018, 117, 32–38. [Google Scholar] [CrossRef]
- Polizzi, C.; Perricone, G.; Morales, M.R.; Burgio, S. A study of maternal competence in preterm birth condition, during the transition from hospital to home: An early intervention program’s proposal. International Journal of Environmental Research and Public Health 2021, 18, 1–24. [Google Scholar] [CrossRef]
- Quiñones-Preciado, J.A.; Peña-García, Á.A.; Vallecilla-Zambrano, D.G.; Yama-Oviedo, J.A.; Hernández-Gutiérrez, N.L.; Ordoñez-Hernández, C.A. Strategies and educational needs of parents of premature infants in a third level hospital in Cali, Colombia. Interface 2023, 27, 1–17. [Google Scholar] [CrossRef]
- Reddy, U.M.; Rice, M.M.; Grobman, W.A.; Bailit, J.L.; Wapner, R.J.; Varner, M.W.; Thorp, J.M.; Leveno, K.J.; Caritis, S.N.; Prasad, M.; Tita, A.T.N.; Saade, G.R.; Sorokin, Y.; Rouse, D.J.; Blackwell, S.C.; Tolosa, J.E. Serious maternal complications after early preterm delivery (24–33 weeks’ gestation). American Journal of Obstetrics and Gynecology 2015, 213. [Google Scholar] [CrossRef] [PubMed]
- Roque, A.T.F.; Lasiuk, G.C.; Radünz, V.; Hegadoren, K. Scoping Review of the Mental Health of Parents of Infants in the NICU. Journal of Obstetric Gynecologic & Neonatal Nursing 2017, 46, 576–587. [Google Scholar] [CrossRef]
- Séassau, A.; Munos, P.; Gire, C.; Tosello, B.; Carchon, I. Neonatal care unit interventions on preterm development. Children 2023, 10, 1–15. [Google Scholar] [CrossRef]
- Shaw, R.J.; Givrad, S.; Poe, C.; Loi, E.C.; Hoge, M.K.; Scala, M. Neurodevelopmental, mental health, and parenting issues in preterm infants. Children 2023, 10, 1–17. [Google Scholar] [CrossRef]
- Springer, C.; Elleman, B.; Cooper, O. The effectiveness of parental education programs within neonatal intensive care units: A systematic review. Research Directs in Therapeutic Sciences 2023, 2. [Google Scholar] [CrossRef]
- Turner, M.; Chur-Hansen, A.; Winefield, H.; Stanners, M. The assessment of parental stress and support in the neonatal intensive care unit using the Parent Stress Scale—Neonatal Intensive Care Unit. Women and Birth 2015, 28, 252–258. [Google Scholar] [CrossRef]
- Ünal, N.; Küçükdağ, M.; Şengun, Z. Evaluation of stress levels in both parents of newborns hospitalized in the neonatal intensıve care unit. Mathews Journal of Pediatrics 2023, 8. [Google Scholar] [CrossRef]
- University of Witwatersrand. (2023). Admissions registers of hospital complex, prepared by nursing services manager. https://www.wits.ac.za/clinicalmed/departments/paediatrics-and-child-health/hospital-services/klerksdorp-hospital/.
- Urizar, G.G.; Nguyen, V.; Devera, J.; Saquillo, A.J.; Dunne, L.A.; Brayboy, C.; Dixon-Hamlett, A.; Clanton-Higgins, V.; Manning, G. Destined for greatness: A Family-based stress management intervention for African-American mothers and their children. Social Science & Medicine 2021, 280, 114058. [Google Scholar] [CrossRef]
- Voulgaridou, A.; Paliouras, D.; Deftereos, S.; Skarentzos, K.; Tsergoula, E.; Miltsakaki, I.; Oikonomou, P.; Aggelidou, M.; Kambouri, K. Hospitalization in neonatal intensive care unit: Parental anxiety and satisfaction. The Pan African Medical Journal 2023, 44, 1–11. [Google Scholar] [CrossRef]
- World Health Organization. (2022). WHO recommendations for care of the preterm or low birth weight infant. World Health Organization. https://www.who.int/publications/i/item/9789240068041.
- Zanta, N.C.; Assad, N.; Suchecki, D. Neurobiological mechanisms involved in maternal deprivation-induced behaviours relevant to psychiatric disorders. Frontiers in Molecular Neuroscience 2023, 16, 1–11. [Google Scholar] [CrossRef]
| Mothers | ||||||||
|---|---|---|---|---|---|---|---|---|
| Hospital A | Hospital B | |||||||
| Variable | Arm 1 (n = 10) | Arm 2 (n = 10) | Arm 3 (n = 10) | Total (n = 30) | Arm 1 (n = 10) | Arm 2 (n = 10) | Arm 3 (n = 10) | Total (n = 30) |
| Marital status | ||||||||
| Single | 10 | 10 | 9 | 29 | 7 | 7 | 10 | 24 |
| Married | - | - | 1 | 1 | 2 | 3 | - | 5 |
| Separated | - | - | - | - | 1 | - | - | 1 |
| Maternal age | ||||||||
| Min | 18 | 19 | 20 | 18 | 21 | 21 | 20 | 20 |
| Max | 42 | 38 | 45 | 45 | 43 | 41 | 37 | 43 |
| Mean | 30,8 | 30.9 | 29.3 | 30.333 | 29.6 | 31.5 | 26.4 | 29.679 |
| Standard Deviation |
7.495 | 5.744 | 8.179 | 6.999 | 7.792 | 6.519 | 6.239 | 6.978 |
| Number of Pregnancies | ||||||||
| Min | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Max | 8 | 4 | 7 | 8 | 3 | 9 | 4 | 9 |
| Mean | 3.1 | 2.7 | 3.2 | 3.0 | 1.9 | 2.778 | 2.7 | 2.448 |
| Standard Deviation |
2.12 | 0.90 | 1.78 | 1.69 | 0.876 | 2.386 | 0.949 | 1.526 |
| Ethnicity | ||||||||
| African | 10 | 10 | 10 | 30 | 9 | 9 | 10 | 28 |
| Coloured | - | - | - | - | - | 1 | - | 1 |
| White | - | - | - | - | 1 | - | - | 1 |
| Pregnancy History | ||||||||
| No pregnancy and birth complications | 6 | 5 | 8 | 19 | 4 | 4 | 5 | 13 |
| High Blood Pressure |
2 | 2 | 1 | 5 | 3 | 4 | - | 7 |
| Bleeding | 1 | 1 | - | 2 | - | - | - | - |
| Foetal distress | - | 2 | 1 | 3 | 2 | - | 2 | 4 |
| Other | - | - | - | - | 1 | 2 | 2 | 5 |
| Not reported | 1 | - | - | 1 | - | - | 1 | 1 |
| Type of delivery | ||||||||
| Vaginal | 7 | 4 | 4 | 15 | 3 | 3 | 4 | 10 |
| Planned c-section | 1 | 1 | 1 | 3 | 1 | 1 | 1 | 3 |
| Emergency c-section | 2 | 5 | 5 | 12 | 6 | 6 | 5 | 17 |
| Education level | ||||||||
| Primary School | - | - | - | - | - | 1 | - | 1 |
| Secondary School | 8 | 7 | 7 | 22 | 7 | 7 | 9 | 23 |
| Certificate (after school) | - | 1 | 1 | 2 | 2 | 1 | 1 | 4 |
| Diploma | - | 1 | 1 | 2 | - | - | - | - |
| Degree | 2 | - | 1 | 3 | 1 | - | - | 1 |
| Not recorded | - | 1 | - | 1 | - | 1 | - | 1 |
| Number of babies | ||||||||
| Singleton | 9 | 8 | 8 | 25 | 8 | 8 | 9 | 25 |
| Twins | 1 | 2 | 2 | 5 | 2 | 2 | 1 | 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



