
Submitted:
06 October 2025
Posted:
07 October 2025
You are already at the latest version
Abstract
Background/Objectives: Delirium, an acute cognitive disturbance, is often unrecognized by family or friend care partners, contributing to delayed interventions and negative health outcomes. UnderstandingDelirium.ca is an e-learning lesson developed to address this gap by improving delirium knowledge among the public, patients, and family/friend care partners. Our objective was to evaluate the acceptability, intention to use, and perceived impact of Understanding Delirium among public users. Methods: A convergent mixed-methods evaluation was conducted using a brief post-lesson survey. The survey included the Net Promoter Score (NPS), the short-form Information Assessment Method for patients and consumers (IAM4all-SF), and an open-text feedback item. Descriptive statistics were used to summarize IAM4all-SF responses, assessing perceived relevance, understandability, intended use, and anticipated benefit. Open-text comments were analyzed thematically by two independent reviewers who reached consensus through discussion. Subgroup analysis of qualitative themes was performed by age, gender, and NPS category. Results: Among 629 survey respondents, over 90% of respondents agreed that the lesson was relevant, understandable, likely to be used, and beneficial. The NPS was rated ‘excellent’ (score of 71), and lesson uptake included over 7,000 unique users with a 35% completion rate. Qualitative analysis revealed themes of high educational value, emotional resonance, and perceived gaps in prior healthcare communication. Respondents emphasized the lesson’s clarity, intent to share, and potential for wider dissemination. Conclusions: UnderstandingDelirium.ca is a promising, guideline-aligned digital intervention that can enhance delirium literacy and reduce care partner distress. It may support prevention, earlier recognition, improved preparedness, and integration into clinical workflows and care partner education efforts.
Keywords:
delirium
; caregiver education
; e-learning
; internet-based intervention
; health literacy
; family care partners
; public health
; prevention
1. Introduction
Delirium is an acute cognitive disturbance commonly caused by underlying medical conditions, metabolic disturbances and medical interventions. This disorder is associated with increased morbidity and mortality. In the community, delirium prevalence is estimated at 1-2% and rises with age to 14% in individuals above 85 years-old [1]. In emergency department settings, delirium may be present in up to one-third of patients, depending on age and other factors, but is often unrecognized [2,3,4,5]. In hospitals 11-25% of older adults will have delirium on admission, and 29-31% will have developed delirium during their stay [6,7]. Since delirium symptoms fluctuate, and patients may have varied cognitive baselines, family/friend care partners are often best positioned to notice changes.
Family/friend care partners are often spouses, children, family members or friends who provide unpaid care to patients living with chronic illnesses. These individuals are often not formally trained or tied to any professional health organization. Family members and other care partners are interested in receiving information about delirium, including symptoms and causes, as well as what they can to do help [8,9]; however, such information is often not provided [8,10]. Evidence shows that the effectiveness of delirium detection and management improve when family care partners are engaged [11]. However, there is a limited number of evidence-based educational interventions to prepare family care partners for this role. Enhancing delirium literacy among the public and care partners is critical for early detection and better care outcomes. Furthermore, care partners for delirium patients are at risk of increased distress and adverse psychological impacts [12,13]. Improving delirium literacy has been shown to empower care partners and reduce emotional burden [14].
Understanding Delirium is a 15-minute, asynchronous, e-learning lesson developed to address the need for improving delirium knowledge among the public and family/friend care partners. The development phase involved a collaborative process with experts in delirium care, instructional design, and patient education, as well as people with lived experience as care partners. The lesson content included delirium signs and symptoms, prevention strategies, and guidance for how care partners can help.
Figure 1.
UnderstandingDelirium.ca e-learning lesson.
A user-centered approach ensured content was accessible, engaging, and culturally appropriate for diverse audiences. Best practices in multimedia learning instructional design were also used. Initial user testing took place in December 2022 – January 2023 and led to improvements to the case scenario of the lesson, amongst other enhancements. This study aims to analyze user feedback of the lesson for future improvements and to evaluate learners’ perceptions of its relevance, understandability, use, and perceived benefits.
2. Materials and Methods
A mixed-methods evaluation was used for this field trial. Potential respondents were recruited from the McMaster Optimal Aging Portal subscriber list with a link to the delirium e-learning lesson; the lesson was also made available publicly on the internet [15,16]. Following completion of the lesson, users were invited to complete a brief survey. Anonymous responses were collected from February 16, 2023–January 31, 2025.
Data were collected after lesson completion using the Net Promoter Score (NPS) and the short-form version of the Information Assessment Method for All Questionnaire (IAM4all-SF), both included in the post-lesson survey. The NPS was used as an outcome measure of overall satisfaction and willingness to recommend the lesson. It is a single question asking respondents: "How likely is it that you would recommend the lesson to a friend or colleague?" on a scale from 0 (not at all likely) to 10 (extremely likely) [17]. The IAM4all-SF assessed perceived relevance, understandability, intention to use the information, and anticipated benefit on a 5-point Likert scale from strongly disagree (1) to strongly agree (5). It is a short-form version of the Information Assessment Method (IAM4all), a content-validated tool used to assess and improve consumer-oriented health information [18]. We created the short form to minimize response burden and improve completion rates, particularly given the older adult demographic targeted by the intervention.
Respondents were also asked to share basic demographic data like age, gender and how they were directed to the e-learning website. Additionally, open text feedback was collected to allow respondents to elaborate on their answers, provide additional comments, or suggest improvements. Web and learning analytics, including pageviews, lesson starts, conversion rate, and completions were also collected.
A convergent mixed-methods research design was used to evaluate user feedback. The use of a convergent mixed-methods approach allowed for the triangulation of quantitative user ratings with qualitative feedback to better understand the perceived impact and areas for improvement of the e-learning lesson. Quantitative data from the IAM4all-SF questionnaire were collected using SurveyMonkey and exported to IBM SPSS Statistics version 30 for analysis. Descriptive statistics, including frequency counts and percentages, were used to summarize participants’ responses across four domains: perceived relevance, understandability, intention to use the information, and anticipated benefit. NPS was calculated to assess users’ likelihood of recommending the lesson to others. The NPS scoring question stratifies the respondents into three categories, promoters (score 9-10), passives (score 7-8) and detractors (score 0-6). NPS is calculated using the standard scoring method by subtracting the percentage of detractors from promoters, resulting in a single score for the entire program ranging from -100 to +100 [17]. Subgroup analyses of IAM4all-SF scores and NPS ratings were conducted by age, gender, and NPS category using the Kruskal-Wallis test. Due to the small number of respondents in the younger age bands, participants under age 55 were aggregated into a single category for the purposes of subgroup analysis. This approach ensured adequate cell sizes for comparison and improved the precision of statistical estimates.
Qualitative data were analyzed using thematic content analysis [19]. Using an inductive approach, free text comments were coded independently by two reviewers [RS + DH], with discrepancies resolved through discussions to reach consensus on the final coding framework. Analytic rigor was enhanced through formal comparisons of themes across participants and collaborative interpretation within the research team. Final themes and sub-themes were reviewed and approved by the wider research team. Subgroup analyses were conducted by age, gender and NPS category to explore thematic patterns in relation to participants’ demographics and satisfaction with the lesson. Triangulation was achieved both across analysts and across data sources.
Data integration occurred during both the design and interpretation phases. The project was structured around predefined research objectives that guided the integration of qualitative and quantitative strands [20]. After independent analysis, results from both components were merged in a narrative to provide a comprehensive understanding of the findings.
3. Results
3.1. e-Learning Lesson Uptake
The Understanding Delirium e-learning lesson landing page was accessed by 7,096 unique users, resulting in 10,794 pageviews. Of these users, 4,706 initiated the lesson, corresponding to a conversion rate of 66.3%. Among those who began the lesson, 1,650 individuals completed it, yielding a lesson completion rate of 35.1%.
3.2. Demographics
Of the 1,650 individuals who completed the delirium e-learning lesson, 739 agreed to participate in the post-lesson survey, and 629 (85.1%) completed it. Most respondents (79.8%) accessed the lesson via the McMaster Optimal Aging Portal e-newsletter. The majority of respondents were female (85.4%), and over 70% were aged 65 or older, including more than one-third who were 75 years or older.

Table 1.
Key demographic characteristics of survey respondents.
| Variables | Responses, n (%) |
|
Arrived at lesson through (N = 621) McMaster Optimal Aging Portal e-newsletter links from friends healthcare professional recommendation other websites search engine links on social media |
496 (79.8) 36 (5.8) 35 (5.6) 14 (2.3) 12 (1.9) 8 (1.3) |
|
Gender (N = 619) Female Male Prefer not to say Other |
528 (85.4) 85 (13.8) 4 (0.7) 1 (0.2) |
|
Age (N = 610) ≥ 75 years old 65-74 years old 55-64 years old 45-54 years old 35-44 years old 25-34 years old 18-24 years old |
216 (35.4) 222 (36.4) 99 (16.2) 35 (5.7) 22 (3.6) 12 (2.0) 4 (0.7) |
3.3. Quantitative Analysis
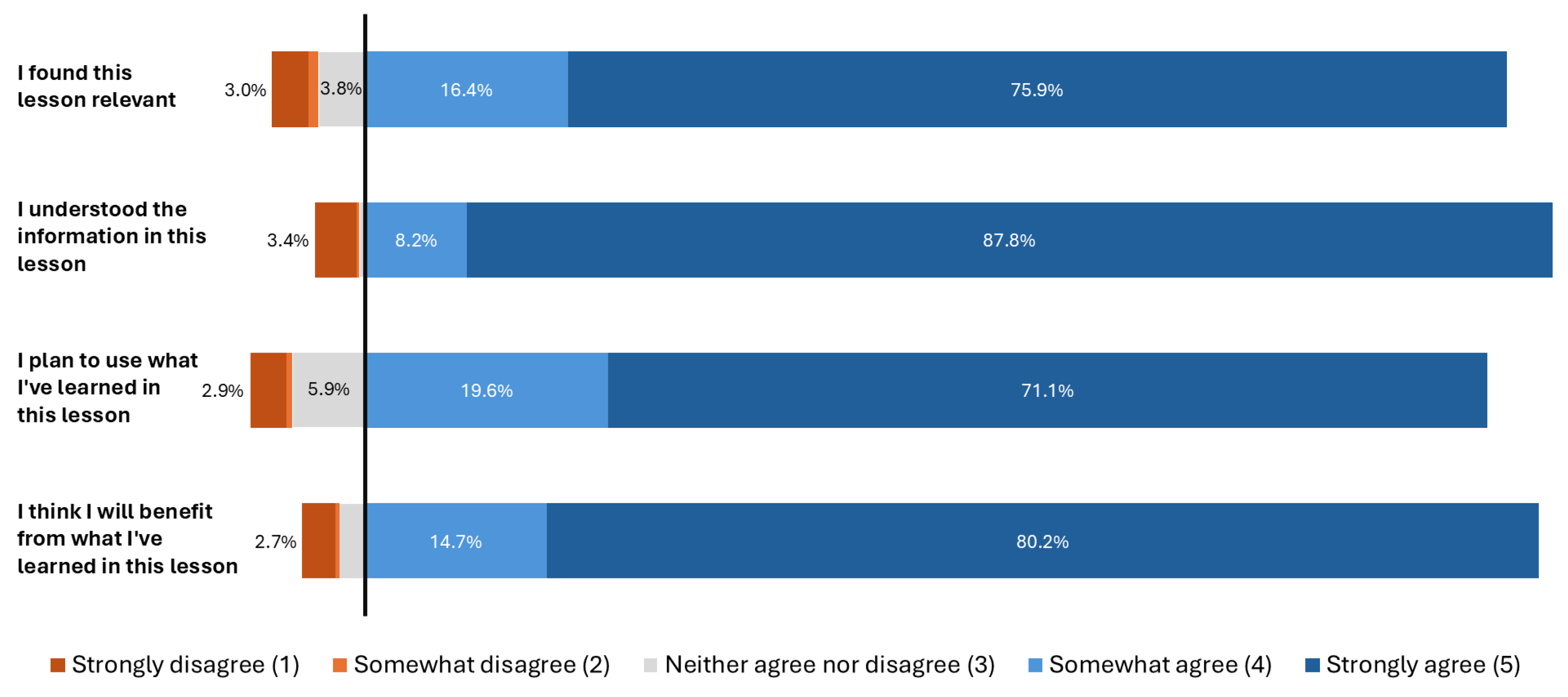
Results from the IAM4all-SF questionnaire indicated high levels of user endorsement and impact across all domains. The median and mode for each domain was 5 (strongly agree). Specifically, 579 of 627 (92%) of respondents somewhat or strongly agreed that the lesson was relevant; 599 (96%) found the information understandable; 569 (91%) intended to use what they had learned; and 594 (95%) believed they would benefit from it. The NPS was rated as ‘excellent,’ with a score of 71 on a scale from –100 to +100. Detailed results are presented in Table 2 and Table 3.
Figure 2.
IAM4all-SF summary chart.
For analysis purposes, age groups were collapsed into four broader categories, with all respondents under 55 combined into a single group to ensure sufficient sample size for statistical testing.
A Kruskal-Wallis test indicated a statistically significant difference in Net Promoter Score (NPS) by age group, H(3) = 16.45, p < .001, as well as in NPS category (promoter, passive, detractor) by age group, H(3) = 14.59, p = .002. However, post-hoc comparisons could not be conducted due to tied median values and insufficient valid cases in some groups. Analysis of IAM4all-SF responses by age group showed a statistically significant difference for the item related to intended use of information (H(3) = 9.86, p = .020), but not for the other IAM4all-SF domains. Similarly, significant differences in IAM4all-SF scores were observed across NPS categories, with higher ratings consistently reported among promoters. Due to the limited variability in responses and the presence of tied ranks, post-hoc analyses were not feasible.
3.4. Qualitative Analysis
A total of 423 respondents provided open-text comments. Of these, 62 were deemed non-contributory (e.g., blank, irrelevant, or unintelligible), resulting in 361 responses included in the qualitative analysis. Thematic content analysis identified five major themes and 20 subthemes. The five themes were: (1) educational value of the lesson; (2) personal and professional relevance; (3) suggestions for improvement; (4) emotional and psychological impact; and (5) healthcare system and professional support. These themes are summarized in Table 4.
Respondents overwhelmingly highlighted the educational value of the e-learning lesson. Many described the lesson as informative, well-structured, and clearly presented:“The lesson was informative, well-presented, and useful. I was not aware of the prevalence and will review the information to enhance my knowledge base." (ID 600)
Respondents also highlighted how the lesson clarified previously held misconceptions by providing a clearer understanding of delirium and its distinction from dementia:
“It was helpful to understand how it is different from dementia. Dementia is such a well-discussed topic, and I’m sure so many lay people are not very familiar with delirium and simply assume their loved one is experiencing dementia." (ID 629)
The lesson also enabled respondents to make sense of past experiences involving delirium in loved ones. Some expressed regret at not having had access to this information earlier:
“My husband died of pancreatic cancer a year ago. I wish I’d known more about delirium then, because that knowledge would’ve helped me understand what he was going through in the weeks before his death. Now, in retrospect and with the information presented in these lessons, it all makes so much more sense. Thank you.” (ID529)
This retrospective clarity frequently provided respondents with a sense of relief and, in some cases, a sense of closure. Many expressed gratitude for finally understanding what had occurred during distressing experiences with loved ones:
“Almost 18 months ago I experienced delirium while in hospital. I am just now coming to terms with all the pieces this was complicated by system becoming septic twice ….actually did almost die twice. Still feel fearful…..cannot remember much of 1st year of recovery. Finally understanding what happened…and be less fearful.” (ID 103)
While many respondents were learning about delirium for the first time, some viewed the lesson as a helpful refresher, a reinforcement of knowledge they had previously encountered, particularly among those with prior familiarity with delirium or clinical experience:
“This is part of my onboarding experience as a nurse at my local hospital. It was a good refresher on delirium, since it's something I'm likely to encounter in the general medicine unit.” (ID 12)
Beyond the educational content, respondents consistently praised the clarity and accessibility of the lesson format. The presentation style, visual layout, and lesson design were praised for supporting engagement and comprehension:
“This was organized in a way that was easy to follow and offered bite-sized information about delirium.” (ID 15)
Respondents frequently indicated an intention to share the lesson among family members, friends, and caregiving networks, particularly those supporting older adults with dementia or individuals who had recently experienced episodes of delirium:
“I will share this lesson with family members and friends who have parents experiencing delirium.” (ID 313)
Others expressed plans to incorporate the knowledge into caregiving practices or to apply it for proactive health monitoring, both for others and for themselves:
“I now know what to watch for, for both of us, and I will recommend that my husband listens to the lesson too.” (ID 64)
Several respondents reported that they were not informed about the condition during critical moments of care, which contributed to confusion and distress:
“My father experienced delirium after surgery to remove stomach cancer 10 yrs ago...No one on the team explained what was happening. The amount of stress we suffered trying to figure out what was happening was immense.” (ID 62)
Others described instances in which their concerns were dismissed or overlooked by medical staff despite observable changes in their loved ones’ behaviour.
“This could have helped me years ago when my mother began having bouts of delirium. I eventually realized these bouts were associated with her frequent UTIs. I encourage you to as much as possible to publicize these information modules. You are correct to state that family members often recognize early signs of delirium in loved ones. At one time, my expressions of concern were ignored when Mom was in a rehab institution following hip surgery. My concerns were rebuffed, and Mom ended up returning to the hospital for many days with a severe UTI. Thank you for all that you do.” (ID 521)
In response to these experiences, respondents advocated for systemic improvements, including the integration of delirium education into hospital protocols, caregiving teams, and broader public health initiatives. Many emphasized that delirium awareness and training should be incorporated into standard education for both family/friend care partners and healthcare professionals. This was also echoed by professionals, including nurses and health workers, who recognized the lesson’s clinical value, with some proposing its integration into staff training and orientation programs:
“This is a fantastic module! I would love to use this module as part of new employee orientation (health authority). This brilliantly touches on all the important aspects of delirium from prevention through treatment and would be suitable for all new employees from Housekeeping to direct care Clinical staff.” (ID 481)
While overall feedback was highly positive, respondents provided several constructive suggestions to improve the lesson. These included technical enhancements, such as incorporating autoplay functionality and streamlining transitions between sections. Others recommended expanding the content to cover additional topics, including alcohol withdrawal delirium, and more specific, actionable strategies for care partners. Suggestions also addressed accessibility and interactivity, such as adjusting font size for readability and including final knowledge checks to reinforce learning.
When analyzing responses by subgroups of gender, age, and NPS rating, minor but notable differences emerged. Female respondents more frequently referenced the lesson’s value in helping them understand prior experiences with delirium and in supporting proactive health management for others, compared to male respondents. Age-related trends were also observed: respondents under the age of 65 more often emphasized the educational and informative aspects of the lesson, while those aged 65 and older more frequently discussed its usefulness in retrospectively understanding previous experiences with delirium and in guiding proactive health management for both themselves and others. Respondents aged 75 and older were particularly likely to express intentions to share the knowledge they had gained with family and friends.
Analysis by NPS category revealed that both promoters (n = 271) and passives (n = 72) commonly mentioned the lesson’s usefulness in understanding prior experiences with delirium, raising awareness, and supporting proactive health behaviours. These groups also expressed feelings of relief and gratitude for understanding what had occurred during distressing experiences. Promoters, in particular, frequently praised the clarity and organization of the content. In contrast, detractors (n = 12) were more likely to highlight the need for improved professional support, particularly noting a lack of communication from healthcare providers during delirium-related experiences.
4. Discussion
This study aimed to evaluate learners’ perceptions of the value and impact of the UnderstandingDelirium.ca asynchronous e-learning lesson and to gather feedback for future improvements. Overall, the quantitative analysis demonstrated strong positive ratings across all IAM4all-SF domains, with over 90% of respondents agreeing that the lesson was relevant and understandable Furthermore, they intended to use the information, and anticipated benefit. The NPS was also rated as ‘excellent,’ further supporting the positive reception and learners’ willingness to recommend the lesson to others.
Although IAM4all-SF scores varied significantly by NPS category – as expected given the alignment between satisfaction and perceived benefit – other subgroup comparisons yielded few statistically significant differences. These findings should be interpreted cautiously, given the skewed distribution of responses, limited variability, and small sample sizes in some age subgroups.
However, one age-related trend that did emerge across multiple measures – namely, higher NPS ratings and greater intention to use the lesson among younger respondents – may reflect differences in caregiving context. Younger participants may be more likely to be actively involved in caregiving roles for older adults, such as parents or grandparents. As a result, they may find the content more immediately relevant and actionable, which could account for their slightly greater likelihood of intending to use and recommending the information. In contrast, older respondents may be more likely to reflect on past experiences with delirium or view the lesson as less directly applicable to their current role. Future studies should consider capturing caregiving status to better understand how care context influences perceptions of value and engagement with digital education tools.
The qualitative findings reinforced and expanded upon the quantitative results. Themes related to the educational value of the lesson, intent to share knowledge, proactive health behaviors, and improved understanding of past experiences emerged prominently. These insights align closely with the IAM4all-SF domains, suggesting consistency across data sources. Additionally, themes addressing emotional burden and perceived gaps in healthcare communication underscore the need for caregiver-centered education. Reports of psychological relief, clarity, and gratitude further suggest the intervention may help reduce care partner distress. Suggestions for technical, content, and accessibility improvements will inform iterative lesson improvements.
Interpretation of qualitative subgroup analyses by gender, age, and NPS category should also be approached with caution due to the overrepresentation of women, older adults (aged 65+), and those who rated the lesson highly (NPS promoters). Despite this, observed differences may offer early insights into varying information needs or preferences. For example, participants aged 75 and older were more likely to report intentions to share the lesson with others, particularly family members or caregivers. This aligns with a more advocacy-oriented form of engagement, even as their quantitative responses indicated a slightly lower intent to personally use the information. Dissemination strategies that leverage this motivation, such as targeting older adults in retirement or long-term care settings, may help amplify the reach and impact of the intervention. Future research is needed to confirm these patterns in more diverse populations.
The intervention was designed primarily for family and friend care partners of older adults, as well as members of the public seeking to improve delirium literacy. Recruitment through the McMaster Optimal Aging Portal likely attracted participants already motivated to engage with health-related content [21]. Notably, several health professionals, including nurses and other clinical staff, also participated and reported finding the lesson useful as a refresher. This suggests an opportunity to develop complementary educational materials tailored to healthcare providers.
4.1. Comparison with Previous Research
This study evaluated the intervention using the IAM4all-SF, a short-form version of the Information Assessment Method designed to assess user responses to consumer-oriented health education. We created the short form to minimize response burden and improve completion rates, particularly in the context of a slightly longer educational intervention (a 15-minute multimedia lesson) instead of a web page or short article, which are more common health information formats to which the questionnaire has been linked. Use of the IAM4all to evaluate e-learning was informed by previous work assessing the iGeriCare dementia education program. In this work, the IAM4all questionnaire was also used to assess public-facing e-learning content [22]. In both cases, the instruments demonstrated strong uptake and yielded highly positive ratings across key domains, supporting their appropriateness for evaluating web-based health education.
Two systematic reviews have examined the implementation and impact of delirium education for family care partners, identifying nine relevant studies [14,23]. These interventions typically involved printed materials or in-person psychoeducational sessions. Three studies that directly assessed delirium knowledge reported significant gains, while others found improvements in caregiver confidence, satisfaction, or emotional well-being. However, randomized trials comparing delirium outcomes across intervention and control groups yielded mixed results. While some showed no effect, Martinez et al. reported a reduction in delirium incidence when family-delivered, nonpharmacologic interventions were supported through education [11]. These findings underscore the need for rigorous evaluation of scalable, evidence-based caregiver education tools.
Future evaluations could incorporate validated tools such as the Caregiver Delirium Knowledge Questionnaire (CDKQ) to directly assess knowledge gains [24]. For example, Wong et al. successfully used a modified CDKQ in a quality improvement initiative to evaluate the impact of a delirium education handout [25]. Other promising instruments, such as the delirium knowledge, risk factors, and attitudes questionnaire used in recent studies from Saudi Arabia [26,27], may offer broader content coverage or greater applicability across diverse cultural contexts and could also be considered. Applying such tools in future studies of UnderstandingDelirium.ca would enable objective measurement of learning outcomes.
Overall, existing delirium education programs for care partners have shown promise but have relied primarily on in-person or paper-based formats. To our knowledge, this is the first study to evaluate an asynchronous, multimedia, internet-based delirium education intervention specifically designed for both the public and family/friend care partners. Such tools have potential for wide-scale dissemination, not only in acute care but also in outpatient and community settings, where early awareness may aid in prevention and timely recognition.
e-Learning offers key advantages, including scalability, low marginal cost, and seamless integration into existing care workflows. There is also growing evidence that digital health interventions can improve caregiver well-being by reducing anxiety and enhancing self-efficacy [28]. The emotional responses observed in this study, including relief, clarity, and gratitude, support this potential psychosocial benefit.
4.2. Alignment with Clinical Guidelines and Implications for Practice
Our findings are especially relevant in light of the recent second edition of the American Psychiatric Association delirium guidelines [29], which call for increased involvement and education of family and friend care partners in delirium care. As Shrestha and Fick and others have shown, care partners often identify symptoms earlier than healthcare providers but lack sufficient knowledge or support [9]. Care partners not only seek education about delirium but also experience substantial psychological distress. Digital education tools may be particularly well-positioned to address both the informational and emotional needs of caregivers. Chuen et al. highlight that delirium is frequently under-documented at discharge, missing a key opportunity for caregiver education, especially during transitions of care [10]. Integrating resources into transitions such as peri-operative care, Intensive Care Unit admissions, or discharge protocols may improve care partner readiness to support patient management. Our evaluation demonstrates that a brief, user-centered, web-based lesson may help to fulfill this need, aligning care practices with guideline-recommended strategies to better engage caregivers as partners in care.
4.3. Limitations
This study has several limitations. First, the self-selected sample and reliance on voluntary survey participation may introduce selection bias, particularly given that most participants were recruited through the McMaster Optimal Aging Portal, a source likely to attract health-motivated individuals [21]. Additionally, only those who completed the lesson and opted into the survey were included, potentially biasing responses toward those with more positive impressions. Second, the study assessed perceived rather than objective outcomes, such as knowledge gain or behavioral change. Lastly, as a web-based intervention, UnderstandingDelirium.ca may be less accessible to individuals with limited internet access, poor bandwidth, low digital literacy, or language barriers. Future adaptations should explore multimodal formats including printed materials, translated content, and audio-based tools, to ensure equitable access for diverse caregiver populations.
4.4. Future Directions
Future studies should assess the lesson with larger and more diverse samples in real-world settings. Implementation science and quality improvement methodologies could support integration into healthcare workflows. Randomized controlled trials or quasi-experimental designs may also help evaluate the lesson’s impact on care partner knowledge, self-efficacy, and potentially on delirium-related outcomes such as detection, duration, and severity.
5. Conclusions
The UnderstandingDelirium.ca e-learning lesson demonstrates strong potential as an accessible and effective tool for improving delirium literacy among the public and family/friend care partners. Findings from this pilot evaluation support its broader integration into public health and caregiver education initiatives. Future research with more diverse populations and rigorous study designs is needed to confirm these results and to assess the intervention’s impact on additional outcomes, including delirium prevention, early recognition, and caregiver well-being.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: title; Table S1: title; Video S1: title.
Author Contributions
Conceptualization, A.J.L., S.A, S.C..; methodology, A.J.L., D.H., S.A., S.C, R.G.; data curation, R.W.; formal analysis, R.S. and D.H..; writing—original draft preparation, R.S., S.A., and A.J.L; writing—review and editing, R.S., S.A., D.H., and A.J.L..; supervision, A.J.L.; project administration, S.A. S.C., and A.J.L.; funding acquisition, A.J.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The Hamilton Integrated Research Ethics Board reviewed the study protocol and granted exemption from full reviewer per their review process, as this was considered a quality improvement initiative.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available upon reasonable request from the corresponding author.
Acknowledgments
This work was supported by the research team at the Division of e-Learning Innovation at McMaster University. The authors would like to thank Dr Amy Schneeberg for her feedback with respect to the quantitative reporting. A.J.L. receives support through the John R Evans Chair in Health Sciences Educational Research and Instructional Development, Faculty of Health Sciences, McMaster University. The authors would like to thank all who participated in this project for their time.
Conflicts of Interest
A.J.L. and McMaster University are the co-owners of UnderstandingDelirium.ca.
Abbreviations
The following abbreviations are used in this manuscript:
| IAM4all-SF | Information Assessment Method for patients and consumers short form version |
| IAM4all | Information Assessment Method for patients and consumers |
| NPS | Net Promoter Score |
Information Assessment Method For All – Short Form (IAM4all-SF)
Thank you for your interest in the lesson. Please tell us more about your experience with this short feedback survey. All of your responses are anonymous. Your answers will help improve this e-learning lesson and identify future topics for enhanced multimedia content like videos and e-learning.
Thank you for considering.
--
Please rate your level of agreement to the following statements about the lesson.
- I found this lesson relevant. (single select)
Strongly Disagree
Disagree
Neither agree nor disagree
Agree
Strongly Agree
- 2.
- I understood the information in this lesson. (single select)
Strongly Disagree
Disagree
Neither agree nor disagree
Agree
Strongly Agree
- 3.
- I plan to use what I’ve learned in this lesson. (single select)
Strongly Disagree
Disagree
Neither agree nor disagree
Agree
Strongly Agree
- 4.
- I think I will benefit from what I’ve learned in this lesson. (single select)
Strongly Disagree
Disagree
Neither agree nor disagree
Agree
Strongly Agree
- 5.
- Is there anything else you would like to tell us about your experience of this lesson or suggestions to improve it? Feel free to comment further on any of your responses if you wish. For example, tell us more about how you will use this lesson or how you expect to benefit. (open text)
- 6.
- Please tell us a bit about yourself. What is your age? (single select)
- 75+
- 65-74
- 55-64
- 45-54
- 35-44
- 25-34
- 18-24
- Under 18
- 7.
- What is your gender? (single select)
- Female
- Male
- Non-binary
- Prefer not to say
- Not listed (please specify) __________
References
- De Lange, E.; Verhaak, P.F.M.; Van Der Meer, K. Prevalence, Presentation and Prognosis of Delirium in Older People in the Population, at Home and in Long Term Care: A Review. Int J Geriatr Psychiatry 2013, 28, 127–134. [CrossRef]
- Chen, F.; Liu, L.; Wang, Y.; Liu, Y.; Fan, L.; Chi, J. Delirium Prevalence in Geriatric Emergency Department Patients: A Systematic Review and Meta-Analysis. Am J Emerg Med 2022, 59, 121–128. [CrossRef]
- Lee, J.S.; Tong, T.; Chignell, M.; Tierney, M.C.; Goldstein, J.; Eagles, D.; Perry, J.J.; McRae, A.; Lang, E.; Hefferon, D.; et al. Prevalence, Management and Outcomes of Unrecognized Delirium in a National Sample of 1,493 Older Emergency Department Patients: How Many Were Sent Home and What Happened to Them? Age Ageing 2022, 51, 16. [CrossRef]
- Oliveira J. e Silva, L.; Berning, M.J.; Stanich, J.A.; Gerberi, D.J.; Murad, M.H.; Han, J.H.; Bellolio, F. Risk Factors for Delirium in Older Adults in the Emergency Department: A Systematic Review and Meta-Analysis. Ann Emerg Med 2021, 78, 549–565. [CrossRef]
- O’Regan, N.A.; Fitzgerald, J.; Adamis, D.; Molloy, D.W.; Meagher, D.; Timmons, S. Predictors of Delirium Development in Older Medical Inpatients: Readily Identifiable Factors at Admission. J Alzheimers Dis 2018, 64, 775–785. [CrossRef]
- Vasilevskis, E.E.; Han, J.H.; Hughes, C.G.; Ely, E.W. Epidemiology and Risk Factors for Delirium across Hospital Settings. Best Pract Res Clin Anaesthesiol 2012, 26, 277–287. [CrossRef]
- Gibb, K.; Seeley, A.; Quinn, T.; Siddiqi, N.; Shenkin, S.; Rockwood, K.; Davis, D. The Consistent Burden in Published Estimates of Delirium Occurrence in Medical Inpatients over Four Decades: A Systematic Review and Meta-Analysis Study. Age Ageing 2020, 49, 352–360. [CrossRef]
- Meyer, G.; Mauch, M.; Seeger, Y.; Burckhardt, M. Experiences of Relatives of Patients with Delirium Due to an Acute Health Event - A Systematic Review of Qualitative Studies. Applied Nursing Research 2023, 73, 151722. [CrossRef]
- Shrestha, P.; Fick, D.M. Family Caregiver’s Experience of Caring for an Older Adult with Delirium: A Systematic Review. Int J Older People Nurs 2020, 15, e12321. [CrossRef]
- Chuen, V.L.; Chan, A.C.H.; Ma, J.; Alibhai, S.M.H.; Chau, V. The Frequency and Quality of Delirium Documentation in Discharge Summaries. BMC Geriatr 2021, 21, 1–10. [CrossRef]
- Martinez, F.T.; Tobar, C.; Beddings, C.I.; Vallejo, G.; Fuentes, P. Preventing Delirium in an Acute Hospital Using a Non-Pharmacological Intervention. Age Ageing 2012, 41, 629–634. [CrossRef]
- Rosgen, B.K.; Krewulak, K.D.; Davidson, J.E.; Ely, E.W.; Stelfox, H.T.; Fiest, K.M. Associations between Caregiver-Detected Delirium and Symptoms of Depression and Anxiety in Family Caregivers of Critically Ill Patients: A Cross-Sectional Study. BMC Psychiatry 2021, 21. [CrossRef]
- Williams, S.T.; Dhesi, J.K.; Partridge, J.S.L. Distress in Delirium: Causes, Assessment and Management. Eur Geriatr Med 2020, 11, 63–70. [CrossRef]
- Carbone, M.K.; Gugliucci, M.R. Delirium and the Family Caregiver: The Need for Evidence-Based Education Interventions. Gerontologist 2015, 55, 345–352. [CrossRef]
- Barbara, A.M.; Dobbins, M.; Haynes, R.B.; Iorio, A.; Lavis, J.N.; Raina, P.; Levinson, A.J. The McMaster Optimal Aging Portal: Usability Evaluation of a Unique Evidence-Based Health Information Website. JMIR Hum Factors 2016, 3, e14. [CrossRef]
- Levinson, A. Understanding Delirium | McMaster Optimal Aging Portal Available online: https://www.mcmasteroptimalaging.org/e-learning/delirium (accessed on 10 September 2025).
- Reichheld, F.F. The One Number You Need to Grow. Harv Bus Rev 2003, 81, 46–54.
- Pluye, P.; Granikov, V.; Bartlett, G.; Grad, R.M.; Tang, D.L.; Johnson-Lafleur, J.; Shulha, M.; Galvão, M.C.B.; Ricarte, I.L.M.; Stephenson, R.; et al. Development and Content Validation of the Information Assessment Method for Patients and Consumers. JMIR Res Protoc 2014, 3. [CrossRef]
- Braun, V.; Clarke, V. Braun, V. and Clarke, V. (2006) Using Thematic Analysis in Psychology. Qualitative Research in Psychology, 3 (2). Pp. 77-101. ISSN 1478-0887 Available from: Http://Eprints.Uwe.Ac.Uk/11735. Qual Res Psychol 2006, 3. [CrossRef]
- Creswell, J.W.; Fetters, M.D.; Ivankova, N. V. Designing A Mixed Methods Study In Primary Care. The Annals of Family Medicine 2004, 2, 7–12. [CrossRef]
- Neil-Sztramko, S.E.; Farran, R.; Watson, S.; Levinson, A.J.; Lavis, J.N.; Iorio, A.; Dobbins, M. If You Build It, Who Will Come? A Description of User Characteristics and Experiences With the McMaster Optimal Aging Portal. Gerontol Geriatr Med 2017, 3. [CrossRef]
- Scott, A.F.; Ayers, S.; Pluye, P.; Grad, R.; Sztramko, R.; Marr, S.; Papaioannou, A.; Clark, S.; Gerantonis, P.; Levinson, A.J. Impact and Perceived Value of IGeriCare E-Learning Among Dementia Care Partners and Others: Pilot Evaluation Using the IAM4all Questionnaire. JMIR Aging 2022, 5, e40357. [CrossRef]
- Bull, M.J.; Boaz, L.; Jermé, M. Educating Family Caregivers for Older Adults About Delirium: A Systematic Review. Worldviews Evid Based Nurs 2016, 13, 232–240. [CrossRef]
- Bull, M.J.; Avery, J.S.; Boaz, L.; Oswald, D. Psychometric Properties of the Family Caregiver Delirium Knowledge Questionnaire. Res Gerontol Nurs 2015, 8, 198–207. [CrossRef]
- Wong, S.P.; Tu, J.; Downie, S.; Heflin, M.T.; McDonald, S.R.; Yanamadala, M. Delirium Education for Geriatric Patients and Their Families: A Quality Improvement Initiative✰. Aging Health Res 2023, 3, 100123. [CrossRef]
- Alaujan, R.; Alhinti, S.; Alharbi, M.; Basakran, F.; Ahmed, M.; Almodaimegh, H. Delirium Knowledge, Risk Factors, and Attitude among General Public in Riyadh, Saudi Arabia, a Cross-Sectional Study. International Journal of Medicine in Developing Countries 2022. [CrossRef]
- Alshurtan, K.; Ali Alshammari, F.; Alshammari, A.B.; Alreheili, S.H.; Aljassar, S.; Alessa, J.A.; Al Yateem, H.A.; Almutairi, M.; Altamimi, A.F.; Altisan, H.A. Delirium Knowledge, Risk Factors, and Attitude Among the General Public in Saudi Arabia: A Cross-Sectional Study. Cureus 2024, 16. [CrossRef]
- Zhai, S.; Chu, F.; Tan, M.; Chi, N.C.; Ward, T.; Yuwen, W. Digital Health Interventions to Support Family Caregivers: An Updated Systematic Review. Digit Health 2023, 9. [CrossRef]
- Crone, C.; Fochtmann, L.J.; Ahmed, I.; Balas, M.C.; Boland, R.; Escobar, J.I.; Heinrich, T.; Jackson-Triche, M.; Levenson, J.L.; Mattison, M.; et al. The American Psychiatric Association Practice Guideline for the Prevention and Treatment of Delirium. Am J Psychiatry 2025, 182, 880–884. [CrossRef]
Table 2.
Frequency of responses to items in the IAM4all-SF questionnaire.
| Responses, n (%) | ||||||
| Strongly disagree (1) | Somewhat disagree (2) | Neither agree nor disagree (3) | Somewhat agree (4) | Strongly agree (5) | Total | |
| I found this lesson relevant. | 19 (3.0) | 5 (0.8) | 24 (3.8) | 103 (16.4) | 476 (75.9) | 627 (100) |
| I understood the information in this lesson. | 21 (3.4) | 1 (0.2) | 3 (0.5) | 51 (8.2) | 548 (87.8) | 624 (100) |
| I plan to use what I've learned in this lesson. | 18 (2.9) | 3 (0.5) | 37 (5.9) | 123 (19.6) | 446 (71.1) | 627 (100) |
| I think I will benefit from what I've learned in this lesson. | 17 (2.7) | 2 (0.3) | 13 (2.1) | 92 (14.7) | 502 (80.2) | 626 (100) |
Table 3.
IAM4all-SF mean (standard deviation), median, mode, mode frequency and interquartile range.
Table 3.
IAM4all-SF mean (standard deviation), median, mode, mode frequency and interquartile range.
| Mean (SD) | Median | Mode | Frequency of the Mode (%) | Interquartile Range | |
| I found this lesson relevant. | 4.61 (0.85) | 5.0 | 5 | 476 (63.2) | 0 |
| I understood the information in this lesson. | 4.77 (0.78) | 5.0 | 5 | 548 (72.8) | 0 |
| I plan to use what I've learned in this lesson. | 4.56 (0.86) | 5.0 | 5 | 446 (59.2) | 1 |
| I think I will benefit from what I've learned in this lesson. | 4.69 (0.78) | 5.0 | 5 | 501 (66.5) | 0 |
Table 4.
Themes and subthemes from the qualitative analysis of open-text comments.
| Themes | Subthemes |
| 1. Educational value of the lesson | a. Informative and educational b. Better understanding of delirium vs dementia c. Useful to better understanding of prior experiences with delirium d. Refresher/reinforcement of knowledge e. Clarity and organization of content |
| 2. Personal and professional relevance | a. Personal use: Intend to share lesson/knowledge dissemination b. Personal use: Awareness and proactive health management for others c. Personal use: Awareness and proactive health management for themselves d. Professional use: Awareness and proactive health management for patients/clients |
| 3. Suggestions for improvements | a. Technical issues/suggestions b. Formatting issues/suggestions c. Content expansion/suggestions |
| 4. Emotional and psychological impact | a. Relief, clarification and gratitude b. Anxiety, fear and sadness - induced by lesson content c. Anxiety, fear and sadness - induced by experience/recollection |
| 5. Healthcare system and professional support | a. Need for better professional support: General b. Lack of information in the healthcare and professional support system c. Lack of communication in the healthcare and professional support system d. Missed diagnosis/ignored brought up concerns e. This lesson as candidate for training professionals and patients |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



