
Submitted:
03 October 2025
Posted:
06 October 2025
You are already at the latest version
Abstract
Background: Periodontitis is a chronic inflammatory disease characterized by progressive destruction of periodontal supporting tissues, strongly associated with shifts in the oral microbiota. Saliva has emerged as a promising diagnostic fluid; however, few studies have analyzed its microbial composition at the species level in the context of the 2018 classification of periodontal diseases. Objectives: To characterize the salivary microbial profiles in a systemically healthy Mexican population with different stages of periodontitis according to the 2018 AAP/EFP (American Academy of Periodontology/ European Federation of Periodontology) classification, and to evaluate sociodemographic, an-thropometric parameters and clinical characteristics as possible risk factors. Methods: A cross-sectional study was conducted in 138 adults classified as periodontal health (n = 33), gingivitis (n = 34), stage I-II periodontitis (n = 18), or stage III-IV periodontitis (n = 53). Unstimulated saliva samples were analyzed for 40 bacterial species using Checkerboard DNA–DNA hybridization technique. Microbial levels, prevalence, and proportions were compared, and multivariate ordinal logistic regression was used to identify independent predictors of disease severity. Results: Porphyromonas gingivalis and Tannerella forsythia exhibited significantly higher levels in advanced periodontitis (p< 0.001). Orange complex bacteria, including Campylobacter rectus and Campylobacter showae, also increased with severity, while commensals such as Gemella morbillorum and Streptococcus sanguinis de-creased. Ordinal logistic regression identified age (OR=1.10, p< 0.001), dental plaque (OR=1.03, p=0.008), C. rectus (OR=1.33, p=0.043), and P. gingivalis (OR=1.22, p< 0.001) as positive predictors of periodontitis. Conclusions: The salivary microbiota exhibits distinct microbial signatures by periodontal severity, with enrichment of pathogenic complexes and depletion of commensals. These findings support saliva as a feasible matrix for screening and prognosis, particularly in resource-limited laboratory clinical settings.
Keywords:
periodontitis
; microbiota
; saliva
; microbial profile
; oral dysbiosis
; checkerboard DNADNA hybridization
1. Introduction
Periodontitis is characterized by the progressive destruction of periodontal supporting tissues [1] and loss of clinical attachment [2]. The condition arises from dysbiosis of the oral microbial community and is closely linked to the accumulation of dental plaque on tooth surfaces [3,4]. This disease is one of the leading causes of tooth loss, which can contribute to the impairment of general health, as a significant association has been observed with various systemic diseases such as diabetes [5], hypertension [6], heart disease [7] and Alzheimer’s disease [8,9].
Saliva is the fluid that coats the entire oral cavity and plays important roles in chewing, swallowing, and speech [10]. The salivary microbiota consists of bacteria shed from different areas of the oral cavity, including the tongue, palate, mucosa, and teeth [10,11]. A few studies have detected subgingival periodontopathogenic bacteria from individuals with periodontitis through saliva [10,12], indicating that bacteria can be detected in saliva, reflecting shedding from multiple sites [13,14].
Most studies analyzing salivary microbiota associated with periodontitis have employed quantitative real-time polymerase chain reaction (qPCR) methods [15] sequencing of certain hypervariable regions of the 16S rRNA gene make it difficult to obtain these approaches are useful but can be limited either by their a priori target selection (qPCR) or by insufficient species-level resolution (some 16S regions). Although less comprehensive than next-generation sequencing, the DNA-DNA hybridization or ”Checkerboard” technique remains a robust tool for focused, species-level comparisons and has been applied to saliva as well as supragingival and subgingival biofilm sampling [16,17], described by Socransky in 1994 [18]. This technique has also been used to examine the microbial composition of saliva, supragingival and subgingival biofilm [17,19], and is still being used in the description of subgingival microbiota for periodontal disease [20,21]. Few studies have applied the 2018 staging system to salivary profiles, and none in systemically healthy Mexican cohorts using Checkerboard [22,23,24].
Moreover, the validation of saliva as a diagnostic matrix represents a significant advancement in the pursuit of non-invasive and accessible tools for the diagnosis and monitoring of periodontitis, particularly in clinical settings with limited resources [25].
Therefore, the aim of the present study was to characterize the salivary microbiota in individuals with periodontitis employing the Checkerboard DNA-DNA hybridization technique according to the 2018 Classification, considering and evaluate sociodemographic and clinical predictors of periodontitis severity (age, Oral Hygiene Index, Filled Teeth (DMFT) Index), in systematically healthy adults in Mexico City.
2. Materials and Methods
2.1. Ethics
This study was conducted in accordance with the Declaration of Helsinki [26] and was approved by the Research and Ethics Committee of the Faculty of Dentistry at the National Autonomous University of Mexico under the reference number CIE/0824/03/2024. All participants read and signed an informed consent form before joining the research project.
2.2. Study Population
A total of 138 unstimulated saliva samples were collected from adults aged 18 to 70 years. Participants were categorized as Periodontal Health, Gingivitis, stages I and II periodontitis, or stage III and IV periodontitis based on the criteria of the 2018 classification [27]. All individuals were recruited from the Division of Graduate Studies and Research at the Faculty of Dentistry, National Autonomous University of Mexico.
No formal sample size calculation was performed a priori, as the study was conceived as an exploratory cross-sectional analysis that included all eligible participants during the study period. However, a post hoc power calculation was performed under the following assumptions: four groups, Cohen’s f effect size = 0.30, α = 0.05, k = 4, N=138. The estimated power for a one-way ANOVA was 0.84 (84%), which provides reasonable evidence support given the sample size achieved.
The selection criteria were as follows:
Inclusion criteria
- Males and females aged 18–70 years.
- Residing in Mexico City or surrounding areas, systemically healthy (without self-reported chronic systemic diseases or conditions).
- With no oral hygiene performed 24 hours before sample collection and without additional use of antiseptic mouthwashes or oral hygiene aids (dental floss, interdental brushes).
- With at least 20 natural teeth (excluding third molars).
Exclusion criteria
- Individuals who have undergone periodontal treatment in the past 12 months.
- Those who had taken antibiotics within the last three months.
- Pregnant or lactating women.
- Individuals using orthodontic appliances.
Participants who did not undergo clinical examinations, had incomplete or contaminated samples, were excluded.
2.3. Sociodemographic Data
Demographic information such as sex (it refers to the participant’s birth sexual identity) and age (it refers to the age in completed years) were recorded. Educational level is classified into four categories: Complete Primary, Middle School, High school, University studies and Postgraduate school. Occupation (current occupation): Home, Student, Workman, Professional, Other. Marital status (Situation of natural persons determined by their family relationships, arising from marriage or kinship): Single and married. Anthropometric parameters were evaluated (weight and height), and the Body Mass Index (BMI) was calculated using the formula weight (kg)/ [height (m)]2.
2.4. Clinical Examination and Classification
The clinical examination was conducted by two standardized clinicians assessing Oral Hygiene Index (OHI) (a modification of the OHI was used, presenting the percentage of sites covered with different levels of biofilm and calculus) [28], Caries experience was assessed using the Decayed, Missing, and Filled Teeth (DMFT) Index [29], bleeding on probing (BoP) upon probing of teeth assessed using the Weijden Index [30], and periodontal measurements at six sites per tooth on all natural teeth except third molars, including probing depth and clinical attachment, measuring the distance from the cementoenamel junction (CEJ) to the pocket depth and the distance from the gingival margin to the CEJ were performed respectively. Along with a radiographic series (14 radiographs) using a digital sensor and portable X-ray device. The PCP11.5 probe was used for OHI and GB measurement, while the PCPUNC 15 probe was used for periodontal measurements. Calibration was performed prior to the study until achieving a Cohen’s kappa >0.7 for periodontal measurements and >0.8 for other indices. Re-standardization sessions were carried out every six months to maintain validity and reproducibility.
2.5. Periodontal Classification
Participants were classified according to the 2018 Classification of Periodontal and Peri-Implant Diseases and Conditions:
- Periodontal Health. No clinical attachment level (CAL) nor radiographical bone loss (RBL) and probing depths (PD) ≤3 mm, assuming no pseudo pockets [31].
- Gingivitis. No CAL nor radiographical bone loss (RBL) and BoP at >10% of the teeth. Including localized and generalized gingivitis [32].
- Periodontitis in stages I or II. Following the criteria for severity, interdental CAL of 1–2 mm (stage I) or 3–4 mm (stage II) and RBL affecting only the coronal third of the root (<15% for stage I and 15–33% for stage II) [2].
- Periodontitis in stages III or IV. Following the criteria for severity, interdental CAL ≥5mm and RBL extending to middle or apical third of the root. There should be evidence of tooth loss ≤4 teeth due to periodontal reasons in stage III, and ≥5 teeth in stage IV [2].
2.6. Saliva Samples
Saliva samples were collected in the morning between 8:00 and 11:00 AM to minimize variations in saliva viscosity. Participants were instructed to refrain from any oral hygiene procedures for 24 hours before collection and to observe a 6-hour fasting period. A total of 3 mL of unstimulated saliva was collected using the spitting method into a pre-labeled 15 mL Falcon tube and placed immediately in ice. 1 mL of saliva aliquots were centrifuged for 10 min at 10,000 RPM, the supernatant was discharged, and solutions were re-suspended in 150 µl of NaOH to lyse the cells and preserve them [33].
2.7. Microbial Evaluation
Complete genomic DNA probes labeled with digoxigenin were prepared using a random primer technique [34]. Samples were individually processed for the detection and quantification of 40 microbial species using DNA-DNA hybridization or “Checkerboard” technique [18], following previously described procedures [35]. The list of bacterial strains used for probe development is presented in Table S1. DNA was isolated and purified [36] from lyophilized stocks obtained from the American Type Culture Collection (ATCC, Rockville, MD). The specificity and sensitivity of DNA probes were assessed, and the assay sensitivity was adjusted to approximately from 104 to 107 cells of each species.
2.8. Statical Analysis
Data were analyzed using R software (R Foundation for Statistical Computing, Vienna, Austria). Descriptive statistics were used to summarize sociodemographic and clinical variables in the population study (N = 138). Frequencies and percentages were reported for categorical variables (sex, education level, marital status and occupation) with means and standard deviations. The Shapiro-Wilk test was used to evaluate the distribution of continuous data. Bivariate Analysis: Clinical and sociodemographic data were calculated by periodontal status group. Categorical variables were compared using Fisher’s exact tests. For continuous variables and microbial data Kruskal–Wallis tests were performed.
The microbial data available were the relative counts of each of the 40 test species from saliva samples of the participants. The analysis compared the composition of saliva between periodontal conditions, expressed as mean levels (DNA-probe count) ± SEM, prevalence (% positive saliva samples) ± SEM, and proportion (% total DNA-probe count) ± SEM of individual species. The proportion of microbial complexes was also determined by grouping the test species as similarly as possible to previous descriptions of microbial complexes, in subgingival plaque. Microbiological analyses were performed with adjustment for multiple comparisons. Post hoc multiple comparison correction was performed with the Benjamini–Hochberg procedure.
Additionally, a multivariate ordinal regression model [37] was constructed to evaluate the association between severity of periodontitis (classified into ordered categories) and sociodemographic, clinical, and microbiological variables. Odds ratios (ORs) with 95% confidence intervals (95% CI) and p-values were calculated. The variables of the final model were selected using a stepwise procedure based on the Akaike Information Criterion (AIC), choosing the model with the lowest AIC value as the most parsimonious. These variables were: age, marital status, DMFT index, body mass index (BMI), species (Aggregatibacter actinomycetemcomitans, Campylobacter rectus, Capnocytophaga ochracea, Cutibacterium acnes, Fusobacterium nucleatum sensu stricto, Porphyromonas endodontalis, Porphyromonas gingivalis, and Schaalia odontolytica).
3. Results
A total of 138 participants were included in the study (Table 1), comprising 33 individuals with periodontal health, 34 with gingivitis, 18 diagnosed with stage I or II periodontitis, and 53 diagnosed with stages III and IV. The mean age was 39.2 ± 13.7 years. Women accounted for 59.5% of the participants, and no significant differences were observed between periodontal conditions in terms of sex, marital status and education level. Significant differences were observed between the different stages of periodontitis and age (p<0.0001), occupation (p<0.001) and body mass index (BMI; p = 0.030).
The microbiological analysis revealed distinct microbial patterns across periodontal conditions (Figure 1A). Red complex species showed marked increases with disease severity. P. gingivalis reached significantly higher mean counts in stages III and IV compared to periodontal health or gingivitis groups (18.3 × 105 vs. 5.4 × 105; p < 0.001), and Tannerella forsythia also increased significantly in advanced disease (10.3 × 105 vs. 4.1 × 105; p = 0.001).
Orange complex species such as C. rectus and Campylobacter showae displayed higher levels in stage III and IV group (p = 0.002 and p = 0.006, respectively). Similarly, Eikenella corrodens and Fusobacterium periodonticum exhibited significantly higher levels in stage III and IV groups (p = 0.002 and p = 0.008, respectively) (Figure 1A).
In contrast, bacteria associated with periodontal health showed reduced levels with disease progression. For instance, Gemella morbillorum decreased in gingivitis and stage I and II groups; Actinomyces naeslundii and Streptococcus sanguinis showed lower proportions in Stage III and IV of periodontitis, although differences did not reach statistical significance.
Regarding the mean proportion of species (Figure 1B), red complex bacteria represented a significantly large fraction of the total salivary microbiota in subjects with periodontitis compared with healthy and gingivitis individuals. Conversely, commensal species such as Streptococcus mitis and S. sanguinis predominated in health but were reduced in disease groups.
Prevalence data (Figure 2) demonstrated similar patterns. The frequency of detection of P. gingivalis and T. forsythia increased in disease groups, while Veillonella parvula and C. ochracea decreased in prevalence in the stage III and IV group.
The analysis of the mean proportion of bacterial complexes showed distinct distribution patterns across periodontal conditions (Figure 1B and Table S5). The “Other” complex represented the largest fraction of the salivary microbiota (37.8%) in individuals with periodontal health (Figure 3A), followed by the Orange (19.1%) and Yellow complexes (18.3%). In gingivitis (Figure 3B), the overall distribution was similar, although an increase in the Orange complex (23.6%) and a slight elevation of the Red complex (7.4%) was observed. The “Other” complex remained abundant (33.6%), whereas the Yellow complex showed a reduction compared with health (14.9%). In stage I and II periodontitis (Figure 3C), there was a progressive increase in the proportion of Orange (20.5%) and Red (7.2%) complexes, accompanied by a decrease in commensal bacteria such as Actinomyces (2.6%) and the Green complex (8.1%). The “Other” complex remained the most abundant (33.3%). In stage III and IV periodontitis (Figure 3D), the Orange complex reached one of its highest values (22.4%), and the red complex showed an elevated proportion compared with the other groups (9.2%). However, the Yellow complex was reduced compared with periodontal health (15.5% vs. 18.3%). Additionally, the Actinomyces (3.9%) and green (8.6%) complexes, both associated with health, also presented lower proportions.
The ordinal logistic regression model (Table 2) identified several independent factors associated with periodontitis (stages of periodontitis as a dependent variable). Increasing age (OR = 1.10, 95% CI: 1.057–1.566, p < 0.001), presence of biofilm covering more than two-thirds of surfaces (OR = 1.03, 95% CI: 1.006–1.046, p = 0.008), S. odontolytica (OR = 1.13, 95% CI: 1.046–1.224, p = 0.002), C. rectus (OR = 1.33, 95% CI: 1.012–1.758, p = 0.043), and P. gingivalis (OR = 1.22, 95% CI: 1.100–1.349, p < 0.001) were positively associated with disease. In contrast, for each increase in DMFT, there was a 12.3% reduction in periodontitis (OR = 0.88, 95% CI: 0.802–0.956, p = 0.003), and C. ochracea (OR = 0.599, 95% CI: 0.430–0.907, p = 0.001), F. nucleatum sensu stricto (OR = 0.84, 95% CI: 0.772–0.907, p < 0.001), and P. endodontalis (OR = 0.94, 95% CI: 0.895–0.985, p = 0.009) are associated with a modest diminution of the likelihood of periodontitis.
Taken together, these findings indicate that the salivary microbiota varies significantly with periodontal status, with enrichment of pathogenic red and orange complex species in advanced stages and depletion of commensal taxa associated with health.
4. Discussion
The aim of the present study was to characterize the salivary microbiota in individuals with periodontitis according to the current Classification of Periodontal and Peri-Implant Diseases and Conditions proposed by the American Academy of Periodontology and the European Federation of Periodontology (AAP/EFP) in 2018. The findings reflect characteristic patterns of microbial dysbiosis associated with the progression of periodontal disease, confirming that saliva can be used as a diagnostic tool in oral microbiota research, and as a coadjutant of clinical periodontal diagnosis and prognosis and monitoring periodontitis.
The results showed a gradual increase in the levels and prevalence of red complex species (P. gingivalis and T. forsythia) in relation to the clinical severity of periodontitis. This trend has been observed in other populations on subgingival microbiota samples [38,39]. Similarly, previous studies in the Mexican population have revealed the same pattern for this bacterial complex [40,41]. Moreover, regarding the bacterial variables included in the model, the levels of P. gingivalis and C. rectus were confirmed as positive predictors of periodontitis, reaching an area under the curve (AUC) of 86.8% at 80.8% sensitivity and 80% specificity for the Stage III and IV group, and a AUC of 89% at 93% sensitivity and 74% specificity for Periodontal health group, allowing to discriminate between health and disease status. These results are consistent with the bivariate analysis and with previous investigations that employ PCR [42] and Next Generation Sequencing (NGS) [23,43,44] detection methods since these bacteria, belonging to the red and orange complexes, respectively, are recognized as key pathogens in disease progression [45]. Previous studies have shown that P. gingivalis promotes biofilm maturation [46], sustained dysbiosis, attenuation of antimicrobial response [47], and subversion of immunological response [48], furthermore it has been shown its ecological dominance, in saliva, where its presence reflects continuous shedding from subgingival biofilms and highlights its utility as a salivary biomarker for periodontal disease. These results suggest that dysbiosis may not be limited to the subgingival habitat but can also be detected in the salivary microbiota [49] which is clinically relevant since salivary sampling is less invasive than subgingival sampling [50].
Similarly, orange complex species such as F. nucleatum sensu stricto and P. intermedia also increased in individuals with periodontal disease, suggesting their role as secondary colonizers that promote the adhesion and co-aggregation of more periodonto-pathogenic species [51]. In contrast, bacteria considered commensal or associated with periodontal health, such as S. sanguinis, A. naeslundii and G. morbillorum showed a notable decrease in both proportion and prevalence in the periodontitis groups [52], indicating a shift toward dysbiosis and the development of a more pathogenic oral ecosystem [51]. Moreover, bacteria such as C. ochracea (green complex) and F. nucleatum sensu stricto (orange complex) exhibited OR values <1, suggesting no association in this model. This finding is noteworthy and contrasts with the established role of F. nucleatum sensu stricto as a facilitator in the colonization of late pathogens [53].
An important finding of this study is that, although the overall proportions of the yellow and green complexes decreased in periodontitis groups compared with health, some individual species from the yellow complex, such as S. oralis and S. gordonii, were found at higher proportions and levels in the most severe stages of periodontitis (stages III and IV) [54]. This may reflect secondary recolonization following periodontal tissue destruction and the expansion of ecological habitats [55], whereby certain commensal bacteria recolonize the oral cavity without exerting the same beneficial effects as in health [56]. Furthermore, some bacteria traditionally considered associated with periodontal health may adapt to inflamed environments and participate in dysbiotic biofilms [57], shifting their role from commensals to opportunists. For example, S. gordonii can contribute to heme acquisition, an essential iron source that supports the growth and proliferation of P. gingivalis [58,59].
Additional factors were positively associated with periodontitis in the ordinal logistic regression analysis, specifically, increasing age (OR = 1.10; p < 0.001) and the presence of biofilm covering more than two-thirds of tooth surfaces (OR = 1.02; p = 0.008) were positively associated with periodontitis. This is consistent with reports from other authors describing periodontitis as a chronic disease that progresses over time [60,61] with the risk of advanced stages increasing with age [62]. In line with this, the direction and magnitude align with population data showing higher salivary bacterial loads and inflammatory markers in older individuals, and increased counts of periodontopathogens in those with generalized bone loss suggesting age-related changes in the salivary milieu beyond periodontal status, which may partly mediate the age effect we observe [63]. In addition, periodontitis is directly related to the accumulation of dental biofilm [60,64], as this ecological niche supports the further accumulation of bacteria that promote early inflammation stages related to periodontitis in susceptible hosts [60,65].
Body mass index was observed with a positive OR however, it did not show significance within the model (OR = 1.06; p=0.14). Although several studies report that a higher BMI is associated with greater severity of periodontitis [66,67,68,69], other studies have shown that when adjusted for variables such as age and oral hygiene habits, the association decreases or is not statistically significant [70].
The ordinal regression showed that for each one unit increase in DMFT, the presence of periodontitis decreased by 12.3%. In other words, a higher number of decayed, missing, and filled teeth was associated with less periodontitis. Although caries and periodontitis share similar environmental conditions, such as biofilm accumulation, substrate availability, and poor oral hygiene, the main types of microorganisms involved are different [71].
The use of saliva samples instead of subgingival biofilm represents a potential logistical and clinical advantage, as it is a non-invasive procedure and easier to standardize. Our findings support previous studies suggesting that salivary analysis can accurately reflect the microbial composition of the oral environment and differentiate between periodontal health and disease states [12,72]. However, it is also acknowledged that saliva represents a mixture of multiple ecological niches, and therefore its interpretation must be appropriately contextualized [22].
By identifying specific microbial signatures associated with different stages of periodontitis, our results could support the development of population-level screening strategies, particularly in resource-limited settings where traditional periodontal assessments may not be feasible [25]. In addition, the stratification of microbial patterns by disease stage could contribute to therapeutic monitoring by providing a non-invasive means to assess treatment outcomes over time [12,73]. In which sociodemographic, oral hygiene, and clinical monitoring must be evaluated together through microbial screening to clarify the risk factors of individuals for presenting periodontitis.
4.1. Limitations
Among the main limitations of the study are its cross-sectional design, which prevents the establishment of causal relationships, as well as the limited sample size and the exclusion of patients with systemic conditions, which may restrict the generalizability of the findings. In addition, although the Checkerboard DNA–DNA hybridization technique is robust and validated, with a detection threshold above 10,000 bacterial cells and providing reliable semi-quantification that allows the association of bacterial load with endogenous infections, it offers a more limited overview of the oral microbiota compared to more recent molecular techniques such as NGS.
5. Conclusions
The salivary microbiota exhibits distinct microbial signatures according to periodontal severity, with enrichment of pathogenic red and orange complex species and depletion of commensals in advanced disease resulting in a higher risk of presenting periodontitis, particularly in older individuals with biofilm coverage, with a higher risk to present periodontitis according to age and biofilm covering. These findings support the use of saliva as a feasible diagnostic matrix for screening, as a coadjutant of clinical periodontal diagnosis and prognosis and monitoring periodontitis, particularly in resource-limited laboratory clinical settings.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Reference strains employed for the development of DNA-probes ; Table S2: Average levels (bacterial counts x 105 ± SEM) of 40 bacterial species evaluated in subjects with periodontal health vs gingivitis vs subjects with periodontitis stage I and II vs subjects with periodontitis stage III and IV.; Table S3: Prevalence (% of colonized sites) of 40 bacterial species evaluated in subjects with periodontal health (n=33) vs. subjects with gingivitis (n=34) vs. subjects with stage I-II periodontitis (n=18) vs. subjects with stage III-IV periodontitis (n=53).; Table S4: Mean individual proportion (%) of 40 bacterial species evaluated in subjects with periodontal health (n=33) vs. subjects with gingivitis (n=34) vs. subjects with stage I-II periodontitis (n=18) vs. subjects with stage III-IV periodontitis (n=53).; Table S5: Average proportion by bacterial complexes (%) of 40 bacterial species in subjects with Periodontal Health (n=33), Gingivitis (n=34), Stage I–II periodontitis (n=18), and Stage III–IV periodontitis (n=53).
Author Contributions
Conceptualization, PEGV. and EHL.; methodology, PEGVG.; software, MAP-G.; Formal analysis, PEGV, MAP-G and EHL.; investigation, PEGV.; EHL., SABY. and APRH.; data curation, PEGV, MAP-G and EHL.; writing—original draft preparation, PEGV.; writing—review and editing, PEGV, MAP-G, MMG, SABY, EHL and APRH.; visualization, EHL and MMG.; supervision, EHL.; project administration, EHL.; funding acquisition, SABY, EHL. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by a grant from the General Directorate of Academic Personnel Affairs (DGAPA), National Autonomous University of Mexico, grant number PAPIIT IN219524 as well as intramural funds from the National Institute of Genomic Medicine.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, was approved by the Research and Ethics Committee of the Faculty of Dentistry at the National Autonomous University of Mexico under the reference number CIE/0824/03/2024.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Acknowledgments
Paola E. García Vázquez is a PhD student in Dental Sciences in the Master’s and Doctorate Program in Medical, Dental and Health Sciences at the National Autonomous University of Mexico, with a scholarship from the Secretariat of Science, Humanities, Technology and Innovation (SECIHTI) CVU 1068944. Quality management systems ISO: 9001:2015 of the Molecular Genetics Laboratory.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Chapple, I.L.; Mealey, B.L.; Van Dyke, T.E.; Bartold, P.M.; Dommisch, H.; Eickholz, P.; Geisinger, M.L.; Genco, R.J.; Glogauer, M.; Goldstein, M. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri--Implant Diseases and Conditions. Journal of periodontology 2018, 89, S74–S84. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri--Implant Diseases and Conditions. Journal of periodontology 2018, 89, S173–S182. [Google Scholar]
- Preshaw, P.M.; Alba, A.L.; Herrera, D.; Jepsen, S.; Konstantinidis, A.; Makrilakis, K.; Taylor, R. Periodontitis and diabetes: A two-way relationship. Diabetologia 2012, 55, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Socransky, S.; Haffajee, A. Periodontal microbial ecology. Periodontology 2000 2005, 38. [Google Scholar] [CrossRef]
- Serón, C.; Olivero, P.; Flores, N.; Cruzat, B.; Ahumada, F.; Gueyffier, F.; Marchant, I. Diabetes, periodontitis, and cardiovascular disease: Towards equity in diabetes care. Frontiers in Public Health 2023, 11, 1270557. [Google Scholar] [CrossRef]
- Del Pinto, R.; Pietropaoli, D.; Munoz-Aguilera, E.; D’Aiuto, F.; Czesnikiewicz-Guzik, M.; Monaco, A.; Guzik, T.J.; Ferri, C. Periodontitis and hypertension: Is the association causal? High Blood Pressure & Cardiovascular Prevention 2020, 27, 281–289. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice, C.; American Diabetes Association Professional Practice, C. 10. Cardiovascular disease and risk management: Standards of Medical Care in Diabetes—2022. Diabetes care 2022, 45, S144–S174. [Google Scholar] [CrossRef] [PubMed]
- Dioguardi, M.; Crincoli, V.; Laino, L.; Alovisi, M.; Sovereto, D.; Mastrangelo, F.; Lo Russo, L.; Lo Muzio, L. The role of periodontitis and periodontal bacteria in the onset and progression of Alzheimer’s disease: A systematic review. Journal of clinical medicine 2020, 9, 495. [Google Scholar] [CrossRef]
- Liccardo, D.; Marzano, F.; Carraturo, F.; Guida, M.; Femminella, G.D.; Bencivenga, L.; Agrimi, J.; Addonizio, A.; Melino, I.; Valletta, A. Potential bidirectional relationship between periodontitis and Alzheimer’s disease. Frontiers in physiology 2020, 11, 683. [Google Scholar] [CrossRef] [PubMed]
- Yamanaka, W.; Takeshita, T.; Shibata, Y.; Matsuo, K.; Eshima, N.; Yokoyama, T.; Yamashita, Y. Compositional stability of a salivary bacterial population against supragingival microbiota shift following periodontal therapy. 2012. [CrossRef]
- Rasiah, I.A.; Wong, L.; Anderson, S.A.; Sissons, C.H. Variation in bacterial DGGE patterns from human saliva: Over time, between individuals and in corresponding dental plaque microcosms. Archives of oral biology 2005, 50, 779–787. [Google Scholar] [CrossRef]
- Belstrøm, D.; Sembler-Møller, M.L.; Grande, M.A.; Kirkby, N.; Cotton, S.L.; Paster, B.J.; Holmstrup, P. Microbial profile comparisons of saliva, pooled and site-specific subgingival samples in periodontitis patients. PLoS ONE 2017, 12, e0182992. [Google Scholar] [CrossRef] [PubMed]
- Soares Nunes, L.A.; Mussavira, S.; Sukumaran Bindhu, O. Clinical and diagnostic utility of saliva as a non-invasive diagnostic fluid: A systematic review. Biochemia medica 2015, 25, 177–192. [Google Scholar] [CrossRef]
- Yoshizawa, J.M.; Schafer, C.A.; Schafer, J.J.; Farrell, J.J.; Paster, B.J.; Wong, D.T. Salivary biomarkers: Toward future clinical and diagnostic utilities. Clinical microbiology reviews 2013, 26, 781–791. [Google Scholar] [CrossRef]
- Singer, E.; Bushnell, B.; Coleman-Derr, D.; Bowman, B.; Bowers, R.M.; Levy, A.; Gies, E.A.; Cheng, J.-F.; Copeland, A.; Klenk, H.-P. High-resolution phylogenetic microbial community profiling. The ISME journal 2016, 10, 2020–2032. [Google Scholar] [CrossRef]
- Sakamoto, M.; Umeda, M.; Benno, Y. Molecular analysis of human oral microbiota. Journal of periodontal research 2005, 40, 277–285. [Google Scholar] [CrossRef]
- Socransky, S.S.; Haffajee, A.D.; Smith, C.; Martin, L.; Haffajee, J.A.; Uzel, N.G.; Goodson, J.M. Use of checkerboard DNA–DNA hybridization to study complex microbial ecosystems. Oral microbiology and immunology 2004, 19, 352–362. [Google Scholar] [CrossRef]
- Socransky, S.; Smith, C.; Martin, L.; Paster, B.; Dewhirst, F.; Levin, A. “ Checkerboard” DNA-DNA hybridization. Biotechniques 1994, 17, 788–792. [Google Scholar]
- Castro-Casarrubias, R.; Castro-Alarcón, N.; Reyes-Fernández, S.; Salazar-Hernández, E.; Vázquez-Villamar, M.; Romero-Castro, N.S. Subgingival microbiota and genetic factors (A-2570G, A896G, and C1196T TLR4 polymorphisms) as periodontal disease determinants. Frontiers in Dental Medicine 2025, 6, 1576429. [Google Scholar] [CrossRef] [PubMed]
- Mager, D.L.; Ximenez--Fyvie, L.A.; Haffajee, A.D.; Socransky, S.S. Distribution of selected bacterial species on intraoral surfaces. Journal of clinical periodontology 2003, 30, 644–654. [Google Scholar] [CrossRef] [PubMed]
- Ximénez--Fyvie, L.A.; Haffajee, A.D.; Socransky, S.S. Comparison of the microbiota of supra--and subgingival plaque in health and periodontitis. Journal of clinical periodontology 2000, 27, 648–657. [Google Scholar] [CrossRef]
- Chew, R.J.J.; Tan, K.S.; Chen, T.; Al--Hebshi, N.N.; Goh, C.E. Quantifying periodontitis--associated oral dysbiosis in tongue and saliva microbiomes—An integrated data analysis. Journal of Periodontology 2025, 96, 55–66. [Google Scholar] [CrossRef]
- Ji, S.; Kook, J.-K.; Park, S.-N.; Lim, Y.K.; Choi, G.H.; Jung, J.-S. Characteristics of the salivary microbiota in periodontal diseases and potential roles of individual bacterial species to predict the severity of periodontal disease. Microbiology Spectrum 2023, 11, e04327-22. [Google Scholar] [CrossRef]
- Pianeta, R.; Iniesta, M.; Castillo, D.M.; Lafaurie, G.I.; Sanz, M.; Herrera, D. Characterization of the subgingival cultivable microbiota in patients with different stages of periodontitis in Spain and Colombia. A cross-sectional study. Microorganisms 2021, 9, 1940. [Google Scholar] [CrossRef]
- Ji, S.; Choi, Y. Point-of-care diagnosis of periodontitis using saliva: Technically feasible but still a challenge. Frontiers in cellular and infection microbiology 2015, 5, 65. [Google Scholar] [CrossRef]
- World Medical, A. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. Jama 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri--implant diseases and conditions–Introduction and key changes from the 1999 classification. 2018, 89, S1–S8. [Google Scholar] [CrossRef] [PubMed]
- Greene, J.C.; Vermillion, J.R. The oral hygiene index: A method for classifying oral hygiene status. The Journal of the American Dental Association 1960, 61, 172–179. [Google Scholar] [CrossRef]
- World Health, O. Oral health surveys: Basic methods. World Health Organization, 2013. [Google Scholar]
- Van der Weijden, G.A.; Timmerman, M.F.; Saxton, C.A.; Russell, J.I.; Huntington, E.; Van der Velden, U.; Van der Weijden, F. Intra--/inter--examiner reproducibility study of gingival bleeding. Journal of periodontal research 1994, 29, 236–241. [Google Scholar] [CrossRef]
- Chapple, I.; Mealey, B.; Van Dyke, T.; Bartold, P.; Dommisch, H.; Eickholz, P.; Geisinger, M.; Genco, R.; Glogauer, M.; Goldstein, M. set al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol 89. [CrossRef]
- Trombelli, L.; Farina, R.; Silva, C.O.; Tatakis, D.N. Plaque--induced gingivitis: Case definition and diagnostic considerations. Journal of clinical periodontology 2018, 45, S44–S67. [Google Scholar] [CrossRef]
- Navazesh, M.; Christensen, C. A comparison of whole mouth resting and stimulated salivary measurement procedures. Journal of dental research 1982, 61, 1158–1162. [Google Scholar] [CrossRef]
- Feinberg, A.P.; Vogelstein, B. A technique for radiolabeling DNA restriction endonuclease fragments to high specific activity. Analytical biochemistry 1983, 132, 6–13. [Google Scholar] [CrossRef]
- Salinas-Azuceno, C.; Martínez-Hernández, M.; Maldonado-Noriega, J.-I.; Rodríguez-Hernández, A.-P.; Ximenez-Fyvie, L.-A. Probiotic monotherapy with Lactobacillus reuteri (Prodentis) as a coadjutant to reduce subgingival dysbiosis in a patient with periodontitis. International Journal of Environmental Research and Public Health 2022, 19, 7835. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.; Socransky, S.; Sansone, C. “Reverse” DMA hybridization method for the rapid identification of subgingival microorganisms. Oral microbiology and immunology 1989, 4, 141–145. [Google Scholar] [CrossRef]
- Fagerland, M.W.; Hosmer, D.W. Tests for goodness of fit in ordinal logistic regression models. Journal of Statistical Computation and Simulation 2016, 86, 3398–3418. [Google Scholar] [CrossRef]
- Griffen, A.L.; Beall, C.J.; Campbell, J.H.; Firestone, N.D.; Kumar, P.S.; Yang, Z.K.; Podar, M.; Leys, E.J. Distinct and complex bacterial profiles in human periodontitis and health revealed by 16S pyrosequencing. The ISME journal 2012, 6, 1176–1185. [Google Scholar] [CrossRef]
- Wara--Aswapati, N.; Pitiphat, W.; Chanchaimongkon, L.; Taweechaisupapong, S.; Boch, J.A.; Ishikawa, I. Red bacterial complex is associated with the severity of chronic periodontitis in a Thai population. Oral diseases 2009, 15, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Ximenez--Fyvie, L.A.; Almaguer--Flores, A.; Jacobo--Soto, V.; Lara--Cordoba, M.; Moreno--Borjas, J.Y.; Alcantara--Maruri, E. Subgingival microbiota of periodontally untreated Mexican subjects with generalized aggressive periodontitis. Journal of Clinical Periodontology 2006, 33, 869–877. [Google Scholar] [CrossRef]
- Ximenez--Fyvie, L.A.; Almaguer--Flores, A.; Jacobo--Soto, V.; Lara--Cordoba, M.; Sanchez--Vargas, L.O.; Alcantara--Maruri, E. Description of the subgingival microbiota of periodontally untreated Mexican subjects: Chronic periodontitis and periodontal health. Journal of periodontology 2006, 77, 460–471. [Google Scholar] [CrossRef]
- Lee, J.; Lee, J.-B.; Song, H.-Y.; Son, M.J.; Li, L.; Rhyu, I.-C.; Lee, Y.-M.; Koo, K.-T.; An, J.-S.; Kim, J.S. Diagnostic models for screening of periodontitis with inflammatory mediators and microbial profiles in saliva. Diagnostics 2020, 10, 820. [Google Scholar] [CrossRef]
- Chigasaki, O.; Aoyama, N.; Sasaki, Y.; Takeuchi, Y.; Mizutani, K.; Ikeda, Y.; Gokyu, M.; Umeda, M.; Izumi, Y.; Iwata, T. Porphyromonas gingivalis, the most influential pathogen in red--complex bacteria: A cross--sectional study on the relationship between bacterial count and clinical periodontal status in Japan. Journal of Periodontology 2021, 92, 1719–1729. [Google Scholar] [CrossRef] [PubMed]
- Damgaard, C.; Danielsen, A.K.; Enevold, C.; Massarenti, L.; Nielsen, C.H.; Holmstrup, P.; Belstrøm, D. Porphyromonas gingivalis in saliva associates with chronic and aggressive periodontitis. Journal of oral microbiology 2019, 11, 1653123. [Google Scholar] [CrossRef]
- Kim, E.-H.; Kim, S.; Kim, H.-J.; Jeong, H.-o.; Lee, J.; Jang, J.; Joo, J.-Y.; Shin, Y.; Kang, J.; Park, A.K. Prediction of chronic periodontitis severity using machine learning models based on salivary bacterial copy number. Frontiers in Cellular and Infection Microbiology 2020, 10, 571515. [Google Scholar] [CrossRef]
- Nakayama, M.; Ohara, N. Molecular mechanisms of Porphyromonas gingivalis-host cell interaction on periodontal diseases. Japanese Dental Science Review 2017, 53, 134–140. [Google Scholar] [CrossRef]
- de Jongh, C.A.; de Vries, T.J.; Bikker, F.J.; Gibbs, S.; Krom, B.P. Mechanisms of Porphyromonas gingivalis to translocate over the oral mucosa and other tissue barriers. Journal of oral microbiology 2023, 15, 2205291. [Google Scholar] [CrossRef] [PubMed]
- Messina, B.M.; Grippaudo, C.; Polizzi, A.; Blasi, A.; Isola, G. The Key Role of Porphyromonas gingivalis in the Pathogenesis of Periodontitis Linked with Systemic Diseases. Applied Sciences 2025, 15, 6847. [Google Scholar] [CrossRef]
- Kim, Y.-T.; Jeong, J.; Mun, S.; Yun, K.; Han, K.; Jeong, S.-N. Comparison of the oral microbial composition between healthy individuals and periodontitis patients in different oral sampling sites using 16S metagenome profiling. Journal of Periodontal & Implant Science 2022, 52, 394. [Google Scholar] [CrossRef]
- Na, H.S.; Kim, S.Y.; Han, H.; Kim, H.-J.; Lee, J.-Y.; Lee, J.-H.; Chung, J. Identification of potential oral microbial biomarkers for the diagnosis of periodontitis. Journal of clinical medicine 2020, 9, 1549. [Google Scholar] [CrossRef] [PubMed]
- Xi, M.; Ruan, Q.; Zhong, S.; Li, J.; Qi, W.; Xie, C.; Wang, X.; Abuduxiku, N.; Ni, J. Periodontal bacteria influence systemic diseases through the gut microbiota. Frontiers in Cellular and Infection Microbiology 2024, 14, 1478362. [Google Scholar] [CrossRef]
- del Pilar Angarita-Díaz, M.; Fong, C.; Medina, D. Bacteria of healthy periodontal tissues as candidates of probiotics: A systematic review. European journal of medical research 2024, 29, 328. [Google Scholar] [CrossRef]
- Nayak, S.; Shetty, N.D.; Kamath, D.G. Commensalism of Fusobacterium nucleatum-The dilemma. Journal of Indian Society of Periodontology 2024, 28, 427–430. [Google Scholar] [CrossRef]
- Riggen-Bueno, V.; Del Toro-Arreola, S.; Baltazar-Díaz, T.A.; Vega-Magaña, A.N.; Peña-Rodríguez, M.; Castaño-Jiménez, P.A.; Sánchez-Orozco, L.V.; Vera-Cruz, J.M.; Bueno-Topete, M.R. Intestinal dysbiosis in subjects with obesity from western mexico and its association with a proinflammatory profile and disturbances of folate (B9) and carbohydrate metabolism. Metabolites 2024, 14, 121. [Google Scholar] [CrossRef]
- Lenartova, M.; Tesinska, B.; Janatova, T.; Hrebicek, O.; Mysak, J.; Janata, J.; Najmanova, L. The oral microbiome in periodontal health. Frontiers in Cellular and Infection Microbiology 2021, 11, 629723. [Google Scholar] [CrossRef]
- Rashid, M.H.; Kumar, S.P.; Rajan, R.; Mamillapalli, A. Salivary microbiota dysbiosis and elevated polyamine levels contribute to the severity of periodontal disease. BMC Oral Health 2025, 25, 2. [Google Scholar] [CrossRef] [PubMed]
- Bagaitkar, J.; Daep, C.A.; Patel, C.K.; Renaud, D.E.; Demuth, D.R.; Scott, D.A. Tobacco smoke augments Porphyromonas gingivalis-Streptococcus gordonii biofilm formation. PLoS ONE 2011, 6, e27386. [Google Scholar] [CrossRef]
- Hajishengallis, G.; Lamont, R.J. Polymicrobial communities in periodontal disease: Their quasi--organismal nature and dialogue with the host. Periodontology 2000 2021, 86, 210–230. [Google Scholar] [CrossRef]
- Park, O.-J.; Kwon, Y.; Park, C.; So, Y.J.; Park, T.H.; Jeong, S.; Im, J.; Yun, C.-H.; Han, S.H. Streptococcus gordonii: Pathogenesis and host response to its cell wall components. Microorganisms 2020, 8, 1852. [Google Scholar] [CrossRef]
- Abdulkareem, A.A.; Al-Taweel, F.B.; Al-Sharqi, A.J.B.; Gul, S.S.; Sha, A.; Chapple, I.L.C. Current concepts in the pathogenesis of periodontitis: From symbiosis to dysbiosis. Journal of Oral Microbiology 2023, 15, 2197779. [Google Scholar] [CrossRef]
- Ana, D.-P.; O, S.J.; Flavia, T.; Zhang, Y.; Jorge, F.-L. Longitudinal host-microbiome dynamics of metatranscription identify hallmarks of progression in periodontitis. Microbiome 2025, 13, 119. [Google Scholar] [CrossRef] [PubMed]
- Xiao, L.; Pu, Y.; Cui, Y.; Chen, C.; Xiao, Q.; Wang, Y.; Wei, Y.; Feng, M.; Zhang, T.; Yang, S. Elongation factor Tu promotes the onset of periodontitis through mediating bacteria adhesion. npj Biofilms and Microbiomes 2025, 11, 47. [Google Scholar] [CrossRef] [PubMed]
- Lira-Junior, R.; Åkerman, S.; Klinge, B.; Boström, E.A.; Gustafsson, A. Salivary microbial profiles in relation to age, periodontal, and systemic diseases. PLoS ONE 2018, 13, e0189374. [Google Scholar] [CrossRef]
- Yang, H.; Qin, Y.; Geng, J.; Qu, J.; Cheng, Q.; Li, K.; Zhang, D. Effect of age and systemic inflammation on the association between severity of periodontitis and blood pressure in periodontitis patients. BMC Oral Health 2025, 25, 273. [Google Scholar] [CrossRef]
- Kwon, T.; Lamster, I.B.; Levin, L. Current concepts in the management of periodontitis. International dental journal 2021, 71, 462–476. [Google Scholar] [CrossRef]
- Lee, B.; Mun, S. Association of Body Mass Index and Waist Circumference with Periodontal Disease. Oral Health & Preventive Dentistry 2025, 23, 271. [Google Scholar] [CrossRef]
- Nilsen, A.; Thorsnes, A.; Lie, S.A.; Methlie, P.; Bunaes, D.F.; Reinholtsen, K.K.; Leknes, K.N. Periodontitis in obese adults with and without metabolic syndrome: A cross-sectional study. BMC Oral Health 2023, 23, 439. [Google Scholar] [CrossRef]
- Rajasekar, A.; Marrapodi, M.M.; Russo, D.; Uzunçıbuk, H.; Ronsivalle, V.; Cicciù, M.; Minervini, G. Correlation of Body Mass Index With Severity of Periodontitis: A Cross--Sectional Study. Clinical and Experimental Dental Research 2025, 11, e70058. [Google Scholar] [CrossRef]
- Reytor-González, C.; Parise-Vasco, J.M.; González, N.; Simancas-Racines, A.; Zambrano-Villacres, R.; Zambrano, A.K.; Simancas-Racines, D. Obesity and periodontitis: A comprehensive review of their interconnected pathophysiology and clinical implications. Frontiers in Nutrition 2024, 11, 1440216. [Google Scholar] [CrossRef]
- Venkat, M.; Janakiram, C. Association between body mass index and severity of periodontal disease among adult South Indian population: A Cross-sectional study. Indian Journal of Community Medicine 2023, 48, 902–908. [Google Scholar] [CrossRef] [PubMed]
- Sedghi, L.; DiMassa, V.; Harrington, A.; Lynch, S.V.; Kapila, Y.L. The oral microbiome: Role of key organisms and complex networks in oral health and disease. Periodontology 2000 2021, 87, 107–131. [Google Scholar] [CrossRef] [PubMed]
- Belstrøm, D.; Holmstrup, P.; Nielsen, C.H.; Kirkby, N.; Twetman, S.; Heitmann, B.L.; Klepac-Ceraj, V.; Paster, B.J.; Fiehn, N.-E. Bacterial profiles of saliva in relation to diet, lifestyle factors, and socioeconomic status. Journal of oral microbiology 2014, 6, 23609. [Google Scholar] [CrossRef] [PubMed]
- Regueira-Iglesias, A.; Suárez-Rodríguez, B.; Blanco-Pintos, T.; Relvas, M.; Alonso-Sampedro, M.; Balsa-Castro, C.; Tomas, I. The salivary microbiome as a diagnostic biomarker of periodontitis: A 16S multi-batch study before and after the removal of batch effects. Frontiers in Cellular and Infection Microbiology 2024, 14, 1405699. [Google Scholar] [CrossRef]
Figure 1.
A) Mean total individual levels (total DNA Probe counts x 105) and B) mean proportion (% total DNA probe count) of 40 individual bacterial species across the 138 participants of the study diagnosed with Periodontal Health, Gingivitis, Stage I and II and Stage III and IV Periodontitis. Differences of mean total levels (* p < 0.05) and Mean proportions ( † p < 0.05) between periodontal conditions were determined using Kruskal-Wallis and were further corrected.
Figure 1.
A) Mean total individual levels (total DNA Probe counts x 105) and B) mean proportion (% total DNA probe count) of 40 individual bacterial species across the 138 participants of the study diagnosed with Periodontal Health, Gingivitis, Stage I and II and Stage III and IV Periodontitis. Differences of mean total levels (* p < 0.05) and Mean proportions ( † p < 0.05) between periodontal conditions were determined using Kruskal-Wallis and were further corrected.
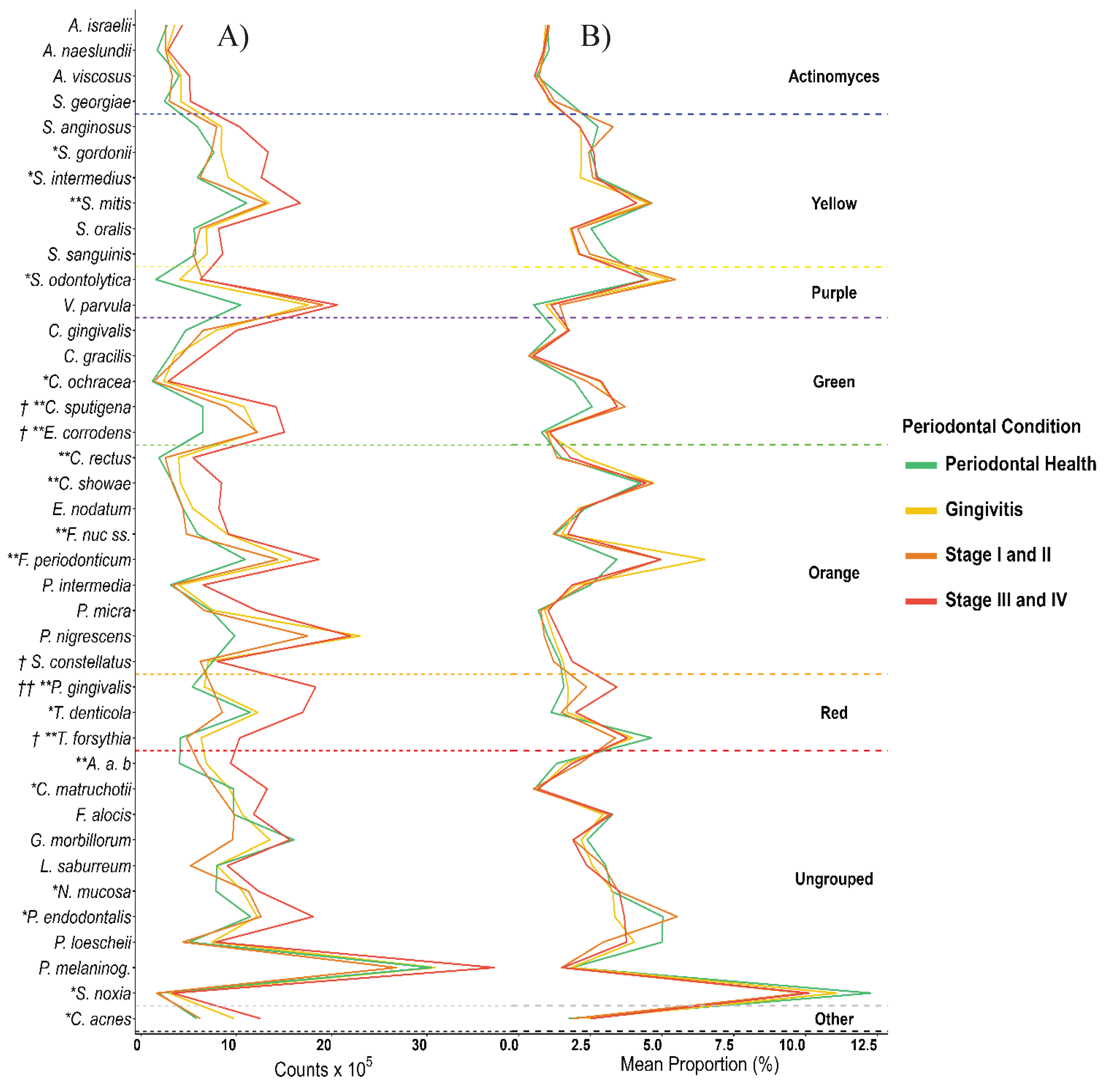
Figure 2.
Prevalence of bacterial species in each periodontal condition ± standard error through the Checkerboard DNA-DNA hybridization technique. Differences of prevalence between groups was determined using Kruskal-Wallis with post hoc multiple comparison correction was performed with the Benjamini–Hochberg procedure: * p < 0.00125.
Figure 2.
Prevalence of bacterial species in each periodontal condition ± standard error through the Checkerboard DNA-DNA hybridization technique. Differences of prevalence between groups was determined using Kruskal-Wallis with post hoc multiple comparison correction was performed with the Benjamini–Hochberg procedure: * p < 0.00125.
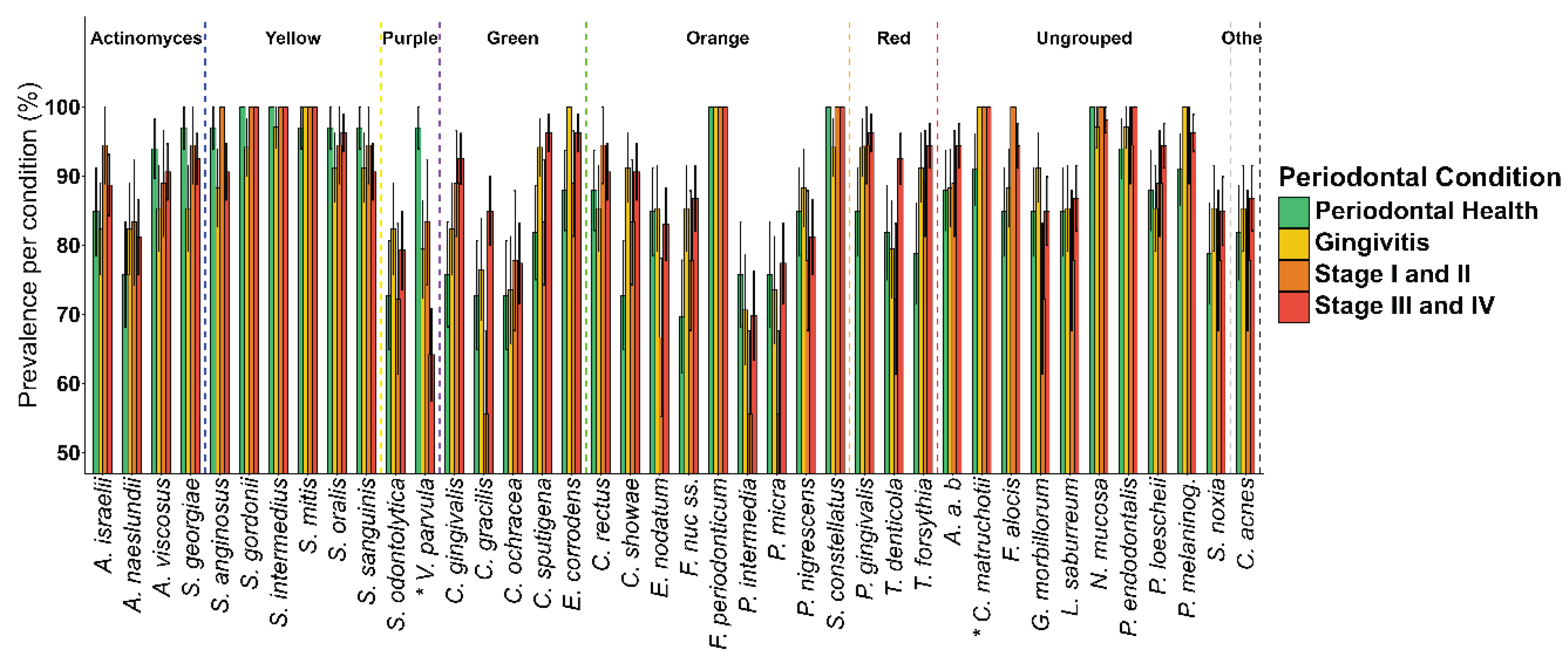
Figure 3.
Distribution of the bacterial complexes identified through the Checkerboard DNA—DNA hybridization technique according to periodontal condition: A) Periodontal health, B) Gingivitis, C) Periodontitis in Stage I and II and D) Periodontitis in Stage III and IV. Each circle represents the relative proportions of classical bacterial complexes (Yellow, Purple, Green, Orange and Red) as well as members of the Actinomyces genus (dark blue), the Ungrouped (light blue) and other bacterial species grouped as Others (grey).
Figure 3.
Distribution of the bacterial complexes identified through the Checkerboard DNA—DNA hybridization technique according to periodontal condition: A) Periodontal health, B) Gingivitis, C) Periodontitis in Stage I and II and D) Periodontitis in Stage III and IV. Each circle represents the relative proportions of classical bacterial complexes (Yellow, Purple, Green, Orange and Red) as well as members of the Actinomyces genus (dark blue), the Ungrouped (light blue) and other bacterial species grouped as Others (grey).
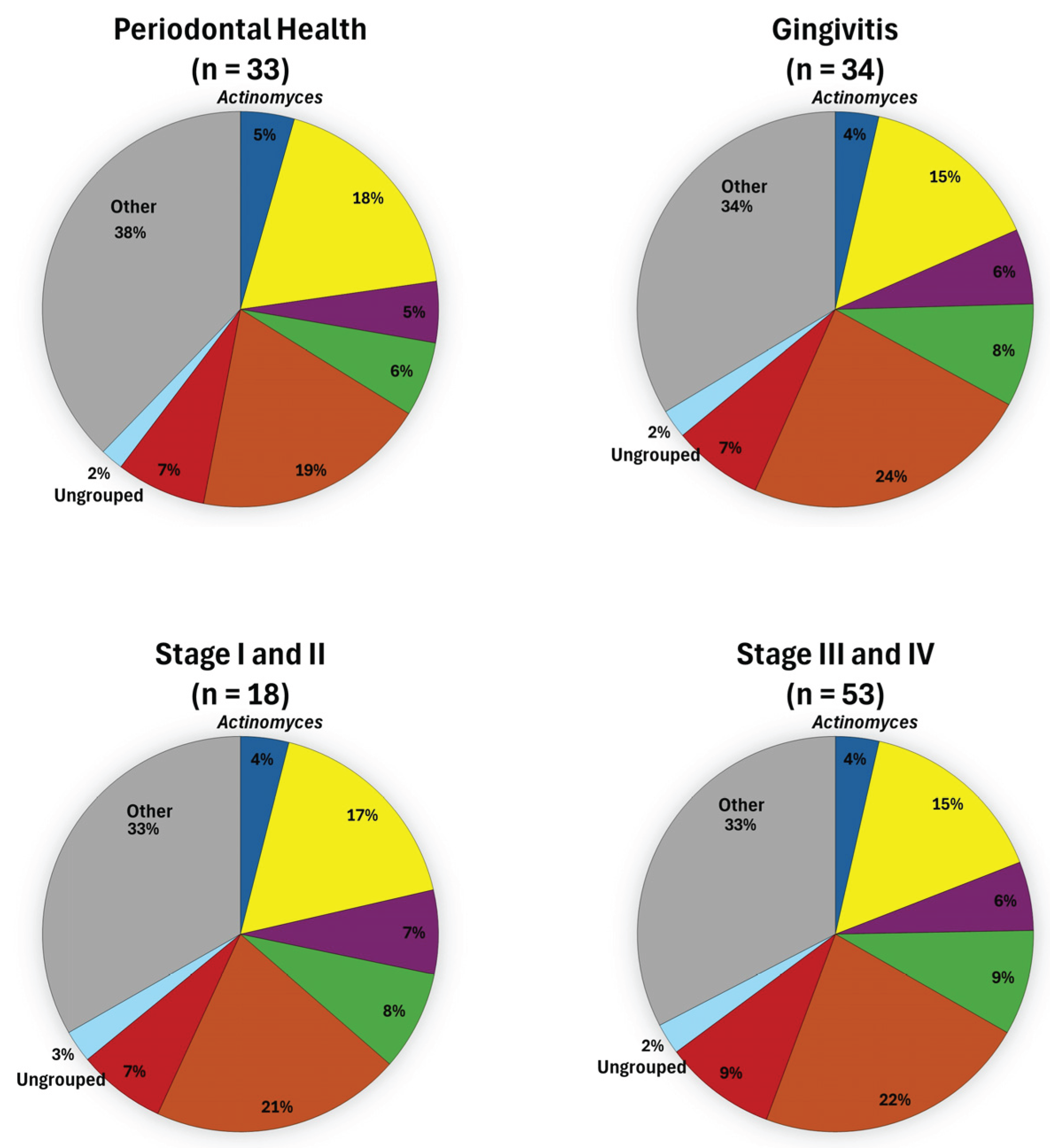

Table 1.
Sociodemographic and clinical characteristics of the studied population and by periodontal condition.
Table 1.
Sociodemographic and clinical characteristics of the studied population and by periodontal condition.
| Population (n = 138) |
Periodontal Health (n = 33) |
Gingivitis (n = 34) |
Stage I-II (n = 18) |
Stage III-IV (n = 53) |
p | |
|---|---|---|---|---|---|---|
| Age(μ±sd) | 39.23±13.72 | 30.82±10.84 | 39.68±13.46 | 31.28±10.85 | 46.8±11.9 | 2.1x10-7 |
| Sex | 0.61* | |||||
| Male (n (%)) | 56(40.57) | 13(39.3) | 16(47.05) | 5(27.7) | 22(41.5) | |
| Female (n (%)) | 82(59.43) | 20(60.7) | 18(52.95) | 13(72.3) | 31(58.5) | |
| Marital status | 0.25* | |||||
| Single (n (%)) | 88 (63.76) | 26 (78.8) | 24 (70.5) | 11 (61.1) | 27 (50.9) | |
| Married (n (%)) | 50 (36.23) | 7 (22.2) | 10 (29.5) | 7 (38.9) | 26 (49.1) | |
| Education | 0.052* | |||||
| Complete primary (n (%)) | 8 (5.7) | 0 (0) | 5 (14.71) | 0 (0) | 3 (5.66) | |
| Middle school (n (%)) | 25 (18.1) | 4 (12.12) | 9 (26.47) | 4 (22.22) | 8 (15.09) | |
| High school (n (%)) | 17 (12.3) | 3 (9.09) | 3 (8.82) | 3 (16.67) | 8 (15.09) | |
| University (n (%)) | 71 (51.4) | 22 (66.67) | 14 (41.18) | 7 (38.89) | 26 (49.06) | |
| Postgraduate (n (%)) | 17 (12.3) | 4 (12.12) | 3 (8.82) | 2 (11.11) | 8 (15.09) | |
| Occupation | 0.001* | |||||
| Homework (n (%)) | 17 (12.3) | 2 (6.06) | 4 (11.76) | 1 (5.56) | 10 (18.87) | |
| Student (n (%)) | 26(18.8) | 11 (33.33) | 6 (17.65) | 6 (33.33) | 3 (5.66) | |
| Workman (n (%)) | 16(11.5) | 1 (3.03) | 2 (5.88) | 3 (16.67) | 10 (18.87) | |
| Professional (n (%)) | 57 (41.3) | 18 (54.55) | 13(38.24) | 7 (38.89) | 19 (35.85) | |
| Other (n (%)) | 22 (15.9) | 1 (3.03) | 9 (26.47) | 1 (5.56) | 11 (20.75) | |
| Clinical variables | ||||||
| BMI (μ±sd) | 26.56±4.87 | 25.20±4.65 | 25.86±4.16 | 25.73±3.9 | 28.1±5.3 | 0.029* |
| CAL (μ±sd) | 4.89±2.32 | 3.63±1.59 | 4.17±1.6 | 4±0 | 6.4±2.6 | 1.4x10-14 |
| RBL (μ±sd) | 19.09±7.43 | 14.96±2.7 | 17.4±5.9 | 16.61±2.6 | 20.4±8.9 | 9.02x10-8 |
| PD (μ±sd) | 4.18±1.36 | 3.1±0.44 | 3.4±0.6 | 4±0 | 5.3±1.4 | 2.09x10-19 |
| BoP (μ±sd) | 25.15±21.1 | 3±3.4 | 27.8±15.8 | 30.1±20.8 | 35.5±20.7 | 1.23x10-14 |
| Surfaces with biofilm greater than 2/3 (μ±sd) | 27.5±22.7 | 14.3±14.6 | 22.1±18.7 | 31.6±21.37 | 37.9±24.6 | 2.4x10-5 |
| DMFT | 9.9±5.37 | 9.2±5.3 | 9.9±6 | 8.3±5.6 | 10.9±4.7 | 0.27 |
| Missing teeth (μ±sd) | 0.6±1.4 | 0.8±1.5 | 0.6±1.22 | 0.1±0.64 | 0.7±1.5 | 0.53 |
BMI = Body Mass Index. CAL = Clinical Attachment Level. RBL = Radiographic Bone Loss. PD =Pocket Deep. BoP = Bleeding on Probing. DMFT = Decayed, Missing, and Filled Teeth. n = number of patients. µ = mean. sd = standard deviation. p = p-value associated to Kruskal-Wallis test. * = p-value associated to Fisher’s exact test.
Table 2.
Ordinal logistic regression model of periodontitis severity adjusted for sociodemographic, clinical, and microbiological variables.
Table 2.
Ordinal logistic regression model of periodontitis severity adjusted for sociodemographic, clinical, and microbiological variables.
| OR | (95% CI) | p | |
|---|---|---|---|
| Age Marital status Surfaces with biofilm greater than 2/3 |
1.103 | (1.057–1.566) | < 0.001 |
| 0.335 | (0.117–0.956) | 0.034 | |
| 1.025 | (1.006–1.046) | 0.008 | |
| DMFT BMI |
0.877 | (0.802–0.956) | 0.003 |
| 1.067 | (0.977–1.167) | 0.149 | |
|
A. actinomycetemcomitans C. acnes C. ochracea C. rectus |
1.106 | (0.982–1.254) | 0.101 |
| 1.060 | (0.998 -1.130) | 0.043 | |
| 0.599 | (0.430–0.907) | 0.001 | |
| 1.326 | (1.012–1.758) | 0.057 | |
|
F. nucleatum sensu stricto P. endodontalis |
0.838 | (0.772–0.907) | < 0.001 |
| 0.939 | (0.895–0.985) | 0.009 | |
| P. gingivalis | 1.218 | (1.10–1.349) | < 0.001 |
| S. odontolytica | 1.130 | (1.046–1.224) | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



