Submitted:
03 October 2025
Posted:
07 October 2025
You are already at the latest version
Abstract
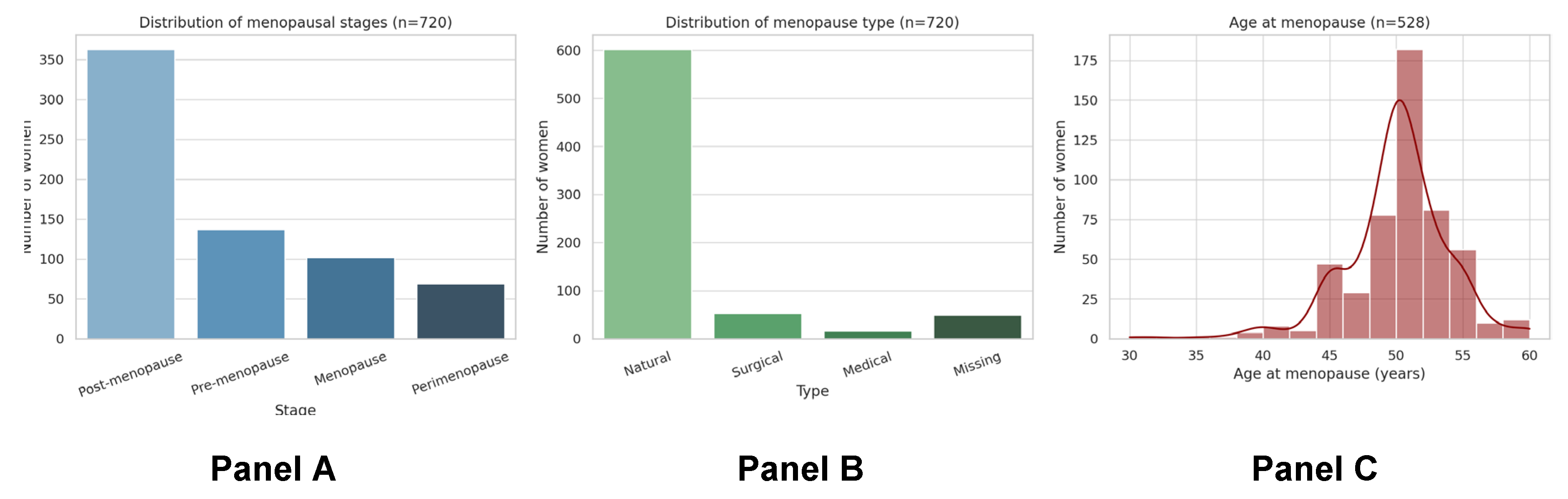
Background: Menopause is a critical life stage for women’s health, yet it remains under-recognised in Sri Lanka despite an ageing female population. Previous studies have reported symptom prevalence and mean age at menopause but lacked an integrated, population-level approach to understanding biological, sociocultural, and health system determinants. Methods: We conducted a cross-sectional analysis of baseline data from 720 women enrolled in the Sri Lanka arm of the Menopause and Ageing Research in International Environments (MARIE) study. Menopause type was classified as natural, medical, or surgical using direct self-reports supplemented by rule-based derivation from hysterectomy, premature ovarian insufficiency (POI), and gonadotrophin-releasing hormone (GnRH) analogue use. Descriptive statistics, Wilson confidence intervals, and multivariable logistic regression with cluster-robust standard errors were used to examine associations with age, ethnicity, education, employment, and urban versus non-urban residence. A burden index was developed to assess cumulative disadvantage across clinical, treatment, and sociocultural domains. Results: The mean age at menopause was 49.7 years (SD±4.1). Natural menopause predominated (83.5%), with 7.4% experiencing surgical and 2.2% medical menopause. The use of traditional remedies was 6.9%, and HRT was 3.4%.The composite burden score (range 0–8) quantified cumulative disadvantage across clinical, treatment, and sociocultural domains. The overall mean burden score was 1·1 (SD 0·7), with a median of 1 (range 0–4). Burden scores were broadly similar across stages: 1·05 in pre-menopausal, 1·10 in perimenopausal, 1·12 in menopause, and 1·11 in post-menopausal women. Conclusion: These findings highlight substantial ethnic and contextual disparities in menopause pathways and treatment access. Addressing inequities through improved access to conservative care, culturally sensitive services, and integrated women’s health policies is urgently needed.
Keywords:
Introduction
Methods
Study Design and ๒
Case Definitions
Data Collection and Variables
Ethics
Data Cleaning and Quality Control
Statistical Analysis
- Clinical burden (0–3 points): presence of long-term conditions, premature ovarian insufficiency, or surgical menopause.
- Treatment burden (0–3 points): ≥2 concurrent medications, reported barrier or contraindication to HRT use, or use of GnRH analogues.
- Socio-cultural burden (0–2 points): reliance on traditional remedies or residence outside Colombo.
Results
Menopause

| Menopause type | n | % (95% CI) |
| Natural | 602 | 83·5 (80·7–86·0) |
| Surgical | 53 | 7·4 (5·7–9·6) |
| Medical | 16 | 2·2 (1·4–3·7) |
| Missing/not reported | 49 | 6·8 (—) |
Inequalities in Menopausal Status and Type
| Panel | Category | Range min (%) | Range max (%) | Number of groups |
| Status by city | Pre-menopause | 0·0 | 66·7 | 21 |
| Status by city | Perimenopause | 0·0 | 33·3 | 21 |
| Status by city | Menopause | 0·0 | 33·3 | 21 |
| Status by city | Post-menopause | 33·3 | 100·0 | 21 |
| Status by ethnicity | Pre-menopause | 6·9 | 33·3 | 3 |
| Status by ethnicity | Perimenopause | 0·0 | 13·8 | 3 |
| Status by ethnicity | Menopause | 0·0 | 20·7 | 3 |
| Status by ethnicity | Post-menopause | 60·0 | 93·1 | 3 |
| Type by city | Natural | 57·9 | 100·0 | 21 |
| Type by city | Surgical | 3·9 | 40·0 | 14 |
| Type by city | Medical | 1·4 | 15·8 | 3 |
| Type by ethnicity | Natural | 60·0 | 93·1 | 3 |
| Type by ethnicity | Surgical | 6·9 | 40·0 | 3 |
| Type by ethnicity | Medical | 1·6 | 1·6 | 1 |
Exploratory Burden Score
| Characteristic | n | Summary |
| *Age (years) | 673 | Mean: 54·1±13.0; median: 56 (IQR 49–62) |
| Menopausal status | 720 | 100% |
| Pre-menopausal | 137 | 19·0% |
| Perimenopausal | 69 | 9·6% |
| Menopause | 49 | 6·8% |
| Post-menopausal | 465 | 64·6% |
| *Age at menopause (years)† | 546 | Mean: 49·7±4.1; median 50 (48–52) |
| *Age at menarche (years)† | 712 | Mean: 13.2±1.6; median: 13 (12-14) |
| Race | 680 | 94.4% |
| Sinhala | 626 | 92% |
| Tamil | 43 | 6.3% |
| Muslim | 6 | 0.8% |
| Burger | 1 | 0.1% |
| Other | 4 | 0.5% |
| Missing values | 40 | 5.6% |
| Religion | 720 | 100% |
| Buddhism | 635 | 88.2% |
| Hindu | 39 | 5.4% |
| Catholic | 35 | 4.9% |
| Islam | 6 | 0.8% |
| Christian | 4 | 0.5% |
| Other | 1 | 0.1% |
| Marital Status | 720 | 100% |
| Married | 530 | 73.6% |
| Single | 103 | 14.3% |
| Widowed | 73 | 10.1% |
| Divorced | 10 | 1.4% |
| Live-in | 3 | 0.4% |
| Other | 1 | 0.1% |
| Family Status | 720 | 100% |
| Nuclear | 583 | 81% |
| Single parenting | 25 | 34.7% |
| Other (Extended or living with other family) | 112 | 15.5% |
| *Number of Children | 569 | Mean: 2.5±1.3 |
| Education level | 720 | 100% |
| A-level, higher grade or equivalent | 306 | 42.5% |
| O-level, higher grade or equivalent | 170 | 23.6% |
| Undergraduate (e.g., BA or BSc) or equivalent | 118 | 16.4% |
| Postgraduate (e.g., MA or PhD) or equivalent | 34 | 4.7% |
| No formal educational qualifications | 92 | 12.8% |
| Employment status | 720 | 100% |
| Employed full-time | 221 | 30.7% |
| Employed part-time | 34 | 4.7% |
| Employed casually | 35 | 4.9% |
| Retired | 77 | 10.7% |
| Home maker | 123 | 17.1% |
| Cared for a family member | 16 | 2.2% |
| Unemployed | 214 | 29.7% |
| Setting | 642 | 89.2% |
| Urban | 193 | 30% |
| Semi-urban | 332 | 51.7% |
| Remote | 117 | 18.2% |
| Missing values | 78 | 10.8% |
| *Comorbidities | 206 | 28.6% |
| Hypertension | 83 | 40.3% |
| Diabetes | 72 | 34.9% |
| Dyslipidaemia | 58 | 28.1% |
| Endometriosis | 33 | 16% |
| Arthritis | 24 | 11.6% |
| Back pain | 8 | 11.6 |
| Hypothyroidism | 8 | 3.9% |
| Cancer | 2 | 1% |
| Vision problems | 2 | 1% |
| Hyperthyroidism | 1 | 0.5% |
| Group | n | Mean | SD | Median | Min | Max |
| Overall | 720 | 1·10 | 0·68 | 1 | 0 | 4 |
| Pre-menopausal | 137 | 1·05 | 0·66 | 1 | 0 | 3 |
| Perimenopausal | 69 | 1·10 | 0·61 | 1 | 0 | 3 |
| Menopause | 49 | 1·12 | 0·64 | 1 | 0 | 3 |
| Post-menopausal | 465 | 1·11 | 0·70 | 1 | 0 | 4 |
Discussion
Population Science
Regional Differences and Environmental Factors
Comorbidity–Menopause Interaction
Contextualisation
Clinical Implications
Comorbidity Impact Profile & Contextualisation
Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgements
Consent for Publication
Conflicts of Interest
References
- Delanerolle, G.; Phiri, P.; Elneil, S.; Talaulikar, V.; Eleje, G.U.; Kareem, R.; Shetty, A.; Saraswath, L.; Kurmi, O.; Benetti-Pinto, C.L. Menopause: a global health and wellbeing issue that needs urgent attention. The Lancet Global Health 2025, 13, e196–e198. [Google Scholar] [CrossRef] [PubMed]
- Rathnayake, N.; Lenora, J.; Alwis, G.; Lekamwasam, S. Prevalence and severity of menopausal symptoms and the quality of life in middle—aged women: A study from Sri Lanka. Nursing research and practice 2019, 2019, 2081507. [Google Scholar] [CrossRef] [PubMed]
- Ilankoon, I.; Samarasinghe, K.; Elgán, C. Menopause is a natural stage of aging: a qualitative study. BMC women’s health 2021, 21, 47. [Google Scholar] [CrossRef] [PubMed]
- Rao, D.B. Status and Advancement of women; APH Publishing: 2000.
- Hamoda, H.; Sharma, A. Premature ovarian insufficiency, early menopause, and induced menopause. Best practice & research Clinical endocrinology & metabolism 2024, 38, 101823. [Google Scholar]
- Nelson, L.M.; Covington, S.N.; Rebar, R.W. An update: spontaneous premature ovarian failure is not an early menopause. Fertility and sterility 2005, 83, 1327–1332. [Google Scholar] [CrossRef] [PubMed]
- Pillay, O.C.; Manyonda, I. The surgical menopause. Best practice & research clinical obstetrics & gynaecology 2022, 81, 111–118. [Google Scholar]
- Sochocka, M.; Karska, J.; Pszczołowska, M.; Ochnik, M.; Fułek, M.; Fułek, K.; Kurpas, D.; Chojdak-Łukasiewicz, J.; Rosner-Tenerowicz, A.; Leszek, J. Cognitive decline in early and premature menopause. International journal of molecular sciences 2023, 24, 6566. [Google Scholar] [CrossRef]
- Samuel, R.L. From Menarche to Menopause: A Systematic Review of Black and Asian Minority Ethnic (BAME) Women’s Reproductive Health Challenges in the UK. University of Wales Trinity Saint David (United Kingdom), 2024.
- Angaye, U.S.; Sibiri, E.A. Between stigma and support: how socio-cultural norms shape health decisions among perimenopausal women in bayelsa central, Nigeria. African journal for the psychological studies of social issues 2025, 28. [Google Scholar]
- Stevens, B.; Watt, K.; Brimbecombe, J.; Clough, A.; Judd, J.; Lindsay, D. The role of seasonality on the diet and household food security of pregnant women living in rural Bangladesh: a cross-sectional study. Public health nutrition 2017, 20, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Hunter, M.; Gupta, P.; Chedraui, P.; Blümel, J.; Tserotas, K.; Aguirre, W.; Palacios, S.; Sturdee, D. The international menopause study of climate, altitude, temperature (IMS-CAT) and vasomotor symptoms. Climacteric 2012, 16, 8–16. [Google Scholar] [CrossRef]
- Mishra, G.D.; Pandeya, N.; Dobson, A.J.; Chung, H.-F.; Anderson, D.; Kuh, D.; Sandin, S.; Giles, G.G.; Bruinsma, F.; Hayashi, K. Early menarche, nulliparity and the risk for premature and early natural menopause. Human Reproduction 2017, 32, 679–686. [Google Scholar] [CrossRef] [PubMed]
| Domain | Recommendation | Public health perspective | Clinical perspective |
| Awareness and education | Normalise menopause as a health issue, not just a life stage | Community-based programmes to educate women, families, and communities; leverage well-woman clinics at ages 35 and 45 for counselling | Routine primary care consultations to validate symptoms, provide anticipatory guidance, and promote healthy ageing |
| Support for induced menopause | Dedicated follow-up for women with surgical or medical menopause | Integrate counselling into surgical pathways; ensure continuity between tertiary care and community follow-up | Offer counselling on HRT, non-hormonal options, and lifestyle advice to reduce immediate symptoms and long-term risks |
| Screening and preventive care | Proactive assessment at midlife | Implement population-level screening campaigns for osteoporosis, cardiovascular risk, and cancers; reduce stigma to improve clinic attendance | Embed midlife screening in primary care, gynaecology, and oncology; link findings to tailored preventive interventions |
| Research and policy | Strengthen evidence base and allocate resources | Conduct epidemiological studies across rural and urban areas; assess socioeconomic inequalities | Train healthcare providers in menopausal medicine; ensure consistent supply of MHT and alternatives; embed menopause care in national health strategies |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



