
Submitted:
30 September 2025
Posted:
30 September 2025
You are already at the latest version
Abstract
Background: The current polio epidemiology in Pakistan poses a unique challenge for global eradication, with polio transmission dynamics influenced by regional variations in immunity and disparities in immunization coverage. This study assesses the immunity level for all three poliovirus types among children 6-11 months in polio high-risk regions of Pakistan. Methods: Four consecutive rounds of cross-sectional serological surveys were conducted in polio high-risk areas of Pakistan between November 2016 and October 2023. 12 high-risk areas were covered in the first three rounds of the survey, while 44 high-risk areas were covered in the fourth round. 25 clusters from each geographical stratum were selected utilizing probability proportional to size. Results: Across the four rounds of the survey, 32,907 children aged 6–11 months from 2,084 clusters and 32,371 households were covered. Temporal analysis showed that seroprevalence of poliovirus type 1 was high in provinces (>95%), albeit consistently lower in Balochistan (going down to 89.7% in Round 4). Type 2 seroprevalence was significantly lower and more heterogeneous, from 34.6% in Sindh to 83.4% in Punjab, with sharp declines by Round 4, particularly in Balochistan (40.4%). Type 3 seroprevalence was overall high (>94% in Punjab, Sindh, and KPK) but dropped in the last round, while Balochistan exhibited continually lower immunity (81.1%). Conclusion: The findings reflect the variations in population immunity to poliovirus in the country, with notable fluctuations over the years. The gaps in type 2 immunity over time and consistently lowest in Balochistan highlight the need for continued monitoring of immunity levels and adaptable vaccination strategies.
Keywords:
Poliovirus seroprevalence
; temporal trends
; serotype immunity
; Serological surveys
; Children 6-11 months
; Pakistan
1. Introduction
Poliomyelitis (polio) has been one of the infectious diseases targeted for global eradication since 1988 by the World Health Assembly, following the successful eradication of smallpox in 1980. In the same year, the Assembly launched the Global Polio Eradication Initiative (GPEI) with the ambitious goal of eradicating poliovirus worldwide by the year 2000 [1]. Since then, remarkable progress has been made in reducing global polio cases by over 99.9%, and the successful elimination of two of the three strains of the wild poliovirus, WPV2 and WPV3, in 2015 and 2019, respectively [2,3,4]. Nonetheless, complete eradication remains elusive, as Pakistan and Afghanistan continue to report cases of wild poliovirus type 1 (WPV1) transmission even today [5,6]. The unfinished journey of polio eradication in Pakistan represents a complex interplay of scientific, socio-political, cultural, systemic, and logistical challenges that have hindered the achievement of a polio-free status [7].
The ongoing circulation of poliovirus in Pakistan is attributed to multiple factors, including vaccine hesitancy, mobile, migrant, and displaced population, geographical isolation, security concerns, and operational challenges in outreach immunization campaigns and immunization service provisions at fixed sites in hard-to-reach areas [8,9]. These challenges are more pronounced in high-risk areas that serve as persistent reservoirs for poliovirus circulation in the country. These areas include regions in Balochistan, Khyber Pakhtunkhwa (KP), Sindh, and densely populated urban centers like Karachi [10].
In Pakistan and other countries, poliovirus eradication efforts have been further complicated with the emergence of vaccine-derived polioviruses (VDPVs), particularly type 2 (cVDPV2) [11,12]. The emergence of cVDPV2 is associated with the trivalent oral poliovirus vaccine (tOPV), which is comprised of live-attenuated strains of poliovirus 1, 2, and 3. This vaccine has the potential to induce vaccine-associated paralytic poliomyelitis (VAPP) in individuals who receive the vaccine and those in close contact with them. VAPP happens when attenuated oral poliovirus vaccine sometimes relapses to neurovirulence, leading to paralysis that clinically resembles poliomyelitis caused by wild poliovirus. This OPV virus circulates in under-immunized populations, resulting in outbreaks of VDPV [13,14,15].
The global switch from tOPV to bivalent OPV (bOPV, containing only types 1 and 3) implemented in April 2016 was meant to eliminate the risk of VAPP and the emergence of cVDPV2 from the type 2 component of tOPV [16,17]. However, the switch created new challenges for maintaining population immunity against type 2 poliovirus, as children born after the switch did not receive type 2 OPV in routine vaccination unless they were vaccinated with monovalent type 2 OPV (mOPV2) in supplementary immunization activities (SIAs) or with inactivated polio vaccine (IPV) in SIAs and routine vaccination [18,19]. Sabin-like type 2, which was circulating before the withdrawal of tOPV, could continue to cause outbreaks of type 2 cVDPV among these children [20,21,22]. In 2024, Pakistan reported 74 cases of WPV1, and as of September 2025, 24 cases have been reported. For cVDPV2, no cases have been reported in the country since 2021 [23].
The immunization landscape in Pakistan has evolved significantly over the study period (2016-2023). The country has adopted several strategies to strengthen both routine immunization and supplementary immunization campaigns, in addition to the inclusion of IPV into the routine immunization schedule in 2015, the use of monovalent and bivalent OPV formulations in targeted campaigns, and the implementation of context-specific innovative approaches to reach children in high-risk and security-compromised areas [24,25]. These efforts have been supported by enhanced environmental surveillance systems to detect poliovirus circulation in sewage samples. This surveillance approach has proven particularly valuable in identifying virus transmission in the absence of paralytic cases [26,27].
Like in other countries, the COVID-19 pandemic disrupted the polio eradication efforts in Pakistan [28]. Polio vaccination campaigns were temporarily suspended in early 2020, leading to an estimated 40 million children missing polio vaccinations during this period [29]. Although campaigns resumed later, the disruption likely created new immunity gaps, potentially reversing some of the progress made in previous years [30,31].
Moreover, regional disparities in healthcare access, socioeconomic status, and security conditions contribute to heterogeneity in immunization coverage and population-level immunity in the country [32]. Urban slums, hard-to-reach areas, and conflict-affected regions often exhibit low vaccination coverage and high susceptibility to poliovirus circulation [33,34]. The migrant and mobile population within the country and across its borders, particularly with Afghanistan, is one of the major challenges in a populous country like Pakistan that has been impacting the polio eradication efforts on a sustained basis [35]. Cross-border movement between Pakistan and Afghanistan has been an uninterrupted path for poliovirus transmission in both countries, attested by genetic sequencing of isolated viruses transmitted [36,37]. Internal migration, including seasonal movement patterns and displacement due to natural disasters or conflict, also transmits poliovirus into previously polio-free areas, creating risk for the communities to maintain higher population-level immunity [38,39].
Understanding the immunological landscape across the diverse polio-high-risk regions is essential to understand geographic patterns of immunity and tailoring interventions to local contexts and prioritizing resources to areas at highest risk of poliovirus transmission [8,38]. It is also essential to assess the impact of disruptions like the COVID-19 pandemic on population immunity levels, particularly in regions already vulnerable to poliovirus circulation.
Serological surveys provide critical insights into population immunity levels by measuring the presence of neutralizing antibodies against each poliovirus serotype in the blood [40]. These surveys complement surveillance data on acute flaccid paralysis (AFP) cases and environmental sampling, offering a more direct measure of a population’s protection against poliovirus infection and disease [41]. In Pakistan, seroprevalence studies have been instrumental in identifying immunity gaps that may not be apparent from vaccination coverage data alone, as immunization effectiveness can be compromised by factors such as vaccine failure, improper vaccine handling, and interference from maternal antibodies or concurrent enteric infections [42,43].
This study presents the results of a series of four seroprevalence surveys conducted in polio high-risk areas in Pakistan from 2016 to 2023, targeting children between 6 to 11 months of age. The purpose of these surveys was to understand the change immunity level for all three poliovirus serotypes 1, 2, and 3 by geographical area of survey over the years.
By examining temporal trends in seroprevalence for all poliovirus serotypes, this study presents insights into the effectiveness of vaccination strategies implemented, the impact of program disruptions by external challenges, such as the COVID-19 pandemic, and the emergence of immunity gaps that may require targeted interventions [44]. Also, the longitudinal nature of the analysis allows for the identification of patterns and trends that may not be apparent from single cross-sectional assessments [45]. The findings from the first three rounds of the survey have already been reported in other studies [46,47].
2. Materials and Methods
2.1. Study Design and Setting
This study utilizes data from a series of cross-sectional serological surveys conducted between November 2016 and October 2023 by Aga Khan University (AKU), Karachi, in close coordination with the national and provincial emergency operations centers for polio eradication in Pakistan. Four rounds of the survey were conducted: the first round (R1) was conducted in 2016-2017, the second round (R2) in 2017, the third round (R3) in 2018-19, and the fourth round (R4) in 2022-23. The first three rounds of the surveys were conducted in 12 districts, and the fourth round included 44 districts, which were identified as the polio high-risk areas by the National Emergency Operations Cell (NEOC). A list of the districts for each round of the survey is provided in Supplementary Table 1a. These districts served as geographical strata for the surveys.
2.2. Sampling Procedure
For each round of the survey, the Lot Quality Assurance Sampling (LQAS) cluster database of the NEOC was used as the sampling frame. A two-stage cluster sampling technique was employed to select clusters from the geographical strata and eligible households from the selected clusters. The vaccination areas being assigned by the polio program in each geographical stratum were considered as clusters. 25 clusters were selected from each geographical stratum employing probability proportional to size (PPS). Following the selection of the clusters, household listing was conducted, and the required number of households with a child between the ages of 6 to 11 months were randomly selected using a fresh household listing. From each household, only one target child was selected. If a household had more than one child of the target age group, the Kish grid method was used to select one child.
2.3. Sample Size Estimation
For the first three rounds of the survey, to estimate seroprevalence with a 95% confidence margin of ± 5% assuming a true seroprevalence of 95%, a design effect of 1.5, and a 90% individual response rate was considered. This resulted in a sample size of 294 children per stratum (almost 12 children per cluster), and a sample of 300 children from each stratum was covered. For the fourth round, a true Seroprevalence of 90% was assumed for sampling size estimation, while the other factors for sample size estimation remained the same as those of the first three rounds. This resulted in a required sample size of 210 children aged between 6-11 months from each stratum (9 children from each cluster).
2.4. Data Collection
The surveys collected information on household demographics and socio-economic status, and child history on vaccination for all children enrolled in the study using a structured questionnaire. The immunization data were recorded from vaccination cards where cards were available, and in their absence, data were collected through mother/caregiver recall. The questionnaire was designed for administration to the mothers or caregivers of the target children. The questionnaire was translated into the national language (Urdu) and was pilot field-tested on 100 samples across five different locations, not part of the study. Along with this information, 2 mL of venous blood from each child was obtained by a trained phlebotomist. During the surveys, households that were locked or those that refused to participate were not replaced with other households.
Our survey team was comprised of data collectors, phlebotomists, team leaders, social mobilizers, lab technicians, medical officers, and regional supervisors. Each data collection team consisted of two female data collectors, two female phlebotomists, one male and one female social mobilizer, and a male team leader. The team leaders and supervisors received a comprehensive central training, conducted over five days. This training program was led by experienced investigators and faculty members from Aga Khan University. Subsequent cascading training sessions were held for the data collection teams at the regional level.
2.5. Laboratory Methodology
After collection, the blood sample was centrifuged, and the serum was isolated and put into sterile, labeled cryovials. The cryovials were kept in a cold box with ice packs and sent right away to the nearest laboratory collection point of AKU. From these collection points, the samples were transported to the Nutrition Research Laboratory at AKU in Karachi. During the transportation, the temperature of the samples was monitored using a digital thermometer attached to the lid of the ice box. At the laboratory at AKU, two distinct aliquots were prepared; one was kept as a backup, and the other was sent to the National Institute of Health (NIH), Pakistan, for neutralization assay examination [48]. For this study, seropositivity was defined as the titer of poliovirus neutralizing antibody >1:8 [49].
2.6. Statistical Analysis
The primary outcome of this study was to assess the level of serological protection (seropositivity) against poliovirus types 1, 2, and 3 in children aged 6-11 months. Seropositivity was analyzed by geography, serotype, and survey rounds. Trends in seropositivity across survey rounds were examined to identify patterns in immunity levels. Similar weights were assigned to different strata to ensure that the assessment of immunity represents all areas fairly without being influenced by areas with high-population averages like Karachi. The results were aggregated and presented at the provincial level. Also, the seropositivity was analyzed in the major cities of Pakistan for all three types by survey rounds. STAT (version 18) was used for analyses [50].
3. Results
Throughout the four rounds of the survey, 68 polio high-risk districts were covered. Several districts were repeatedly surveyed, and additional districts were included in the fourth round after their reclassification as high-risk due to changing reports of polio cases. Altogether, 2,084 clusters, 32,371 households, and 32,907 children aged 6-11 months were covered. The proportion of male children was slightly higher than that of female children in all rounds. Vaccination card retention was higher in the initial rounds; however, there was a substantial decline in the fourth round (40%) (Table 1). OPV coverage ranged between 68% and 75% while IPV coverage varied between 55% and 82% across the survey rounds. Over two-thirds of the caregivers were literate. Round-wise, district-specific demographic and coverage indicators are presented in the supplementary material (Table 1a).
3.1. Seroprevalence of Polio Type-1 Across Provinces and Survey Rounds
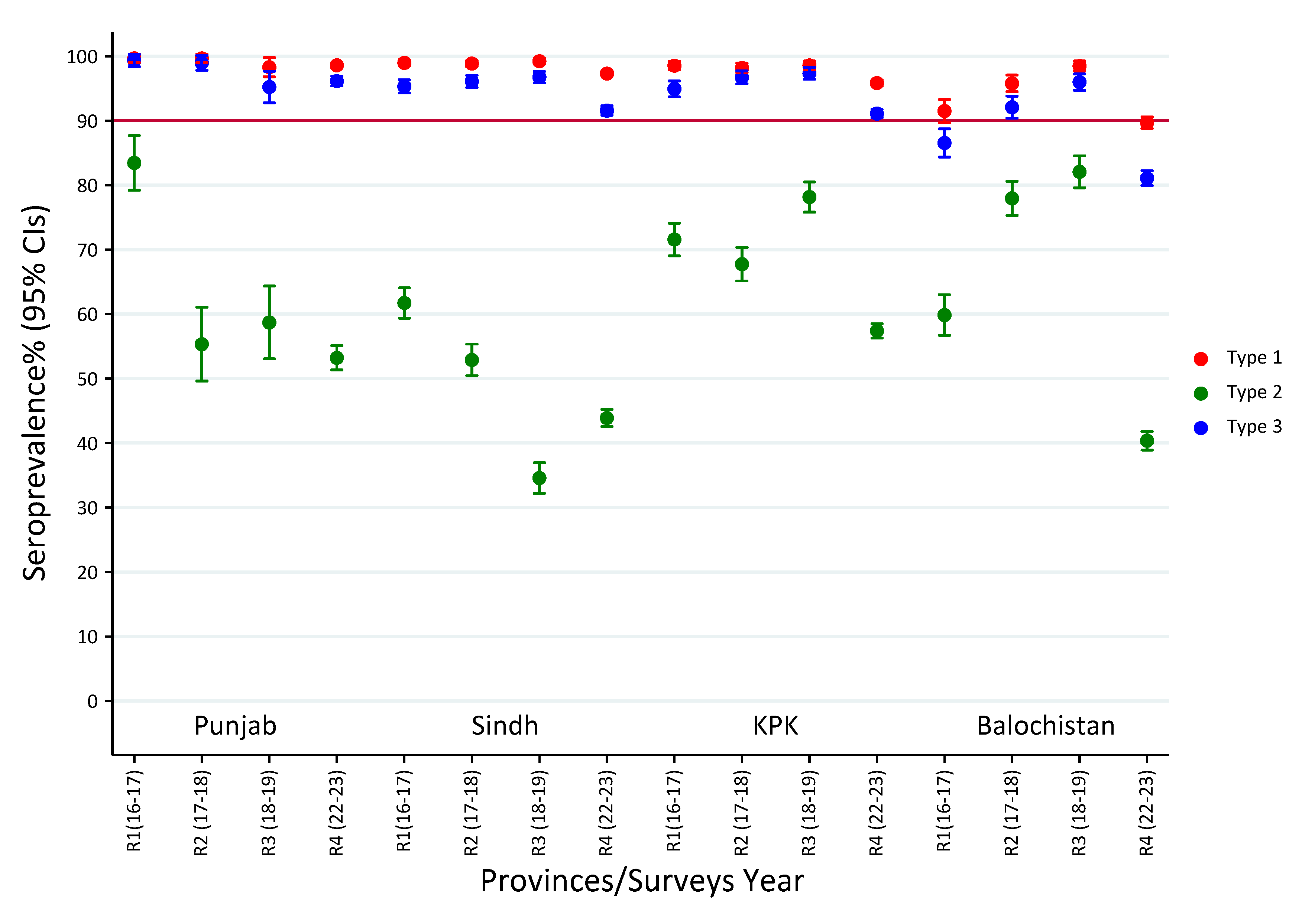
Poliovirus type 1 seroprevalence was consistently high in Punjab, Sindh, and KPK, with prevalence estimates over 95% in all four survey rounds. Immunity levels were between 98.3% and 99.7% in Punjab, and between 97.3% and 99.2% in Sindh. In KPK, it was consistently above 95%, though a minor drop was seen in the fourth round (95.8%). On the other hand, Balochistan showed more variability, the lowest coverage of 91.5% being reported in round 1 and another steep decline in round 4 (89.7%). These results reflect overall high immunity in Punjab, Sindh, and KPK, but persisting and high immunity gaps in Balochistan, especially in the latest round (Figure 1, Supplementary Table 2).
3.2. Seroprevalence of Polio Type-2 Across Provinces and Survey Rounds
The seroprevalence of poliovirus type 2 was found to be heterogeneous among provinces and survey rounds, with lower prevalences than type 1. Punjab had the highest prevalence in round 1 (83.4%, 95% CI: 79.2–87.7), followed by Sindh (61.7%, 95% CI: 59.4–64.1) and a comparatively lower level in Balochistan (59.8%, 95% CI: 56.7–63.0). In round 2, Punjab (55.3%, 95% CI: 49.6–61.0) and Sindh (52.9%, 95% CI: 50.4–55.3) showed a decline, whereas Balochistan (78.0%, 95% CI: 75.3–80.6) and KPK (67.7%, 95% CI: 65.1–70.3) recorded higher seroprevalence. Round 3 showed heterogeneity as Sindh continued to fall further to 34.6% (95% CI: 32.2-36.9), but Balochistan reached the highest level, 82.1% (95% CI: 79.6-84.5), while KPK had a prevalence of 78.1% (95% CI: 75.8-80.5). By round 4, every province displayed decreasing levels, Punjab (53.2%, 95% CI: 51.3-55.1), Sindh (43.9%, 95% CI: 42.6-45.2), and KPK (57.4%, 95% CI: 56.3-58.5) showing medium prevalence, while the lowest seroprevalence was in Balochistan (40.4%, 95% CI: 38.9-41.8) (Figure 1, Supplementary Table 2).
Results revealed that type 2 immunity was always below type 1 in all provinces, with Sindh and Punjab showing the largest declines after the first round, whereas Balochistan generally exhibited variable but high seroprevalence until a steep decline in the fourth round.
3.3. Seroprevalence of Polio Type-3 Across Provinces and Survey Rounds
Seroprevalence of type 3 poliovirus was overall high in provinces and rounds, similar to type 1 but with greater provincial variation. Punjab reported the highest rates throughout, at nearly 99% in rounds 1 and 2. Sindh and KPK also had high rates (>94% for most rounds), although both fell to approximately 91% in round 4. Balochistan demonstrated considerably lower type 3 immunity, beginning at 86.5% (95% CI: 84.3–88.7) in round 1 and falling to 81.1% (95% CI: 79.9–82.2) in round 4 (Figure 1, Supplementary Table 2).
The results reflect that type 1 immunity across the country remained stable and high, type 2 immunity was stable yet lower with wide provincial variations, and type 3 immunity was moderately elevated but decreasing, where Balochistan lagged for all three serotypes consistently.
Figure 1.
Polio seroprevalence by types across provinces and survey rounds.
3.4. Seroprevalence of Polio Type-1 Across High-Risk Cities
Type 1 poliovirus seroprevalence was analyzed in high-risk cities across the survey rounds. Karachi and Peshawar demonstrated persistently high seroprevalence ranging between 97% and 99% throughout the study period. On the other hand, Quetta showed greater variability, with seroprevalence increasing from approximately 94.8% (CI:95%; 92.3 – 97.3) in round 1 to 99.7% (CI: 95%; 99.0-100.3) in round 3, followed by a decline to 96.4% (CI:95%: 94.7-98.1) in round 4. In Killa Abdullah, the prevalence remained fluctuated over time, increasing from 87.8% (CI:95%; 84.2-91.5) in round 1 to 97.5% (CI:95%; 95.7-99.2) in round 3 before a steep decline to 76.2% (CI: 95%; 72.2-80.1) in round 4. A similar trend was observed with seroprevalence in Pishin, where it increased from 91.9% (CI:95%; 88.8-94.4) in round 1 to 98.3% (CI: 95%; 96.99-99.8) in round 3, followed a decline to 91.7% (CI:95%; 89.2-94.3) in round 4 (Figure 2, Supplementary Table 3).
The prevalence rates indicate that while Karachi and Peshawar have maintained stable and high immunity against type 1 poliovirus, Quetta, Killa Abdullah, and Pishin experienced greater fluctuations and a notable decrease in seroprevalence in recent years.
3.5. Seroprevalence Trends of Polio Type-2 Across High-Risk Cities
Type 2 poliovirus seroprevalence showed a declining trend in the high-risk cities, with notable variability between the locations. In Karachi, the prevalence declined from 65.2% (CI:95%; 62.2-68.1) in round 1 to 38.5% (CI:95%; 35.4-41.6) in round 3, with a slight recovery to 46.8% (CI: 95%; 45.1-48.5) in round 4. Peshawar exhibited an initial decline from 64.6% (CI:95%; 60.8-68.3) in round 1 to 57.9% (CI: 95%; 54.1-61.7) in round 2, followed by a substantial improvement to 69.9% (CI:95%; 65.7-74.1) in round 4. In Quetta, the prevalence displayed variable patterns; increasing from 74.1% (CI:95%; 69.2-79) in round 1 to 93.1% (CI:95%; 90.2-95.9) in round 3, before it declined to 61.7% (CI:95%; 57.3-66.1) in round 4 (Figure 2, Supplementary Table 3). A similar trend was observed in Killa Abdullah, maintaining levels between 61-66% in the first three rounds, before it declined to 36.7% (CI:95%; 32.3-41.2) in round 4. Similarly, in Pishin, a quite dramatic improvement was witnessed in the prevalence, increasing from 44.5% (CI:95%; 38.9-50) in round 1 to 88.66% (CI:95%; 85-92.2) in round 2 and maintaining it at 87.4% (CI:95%; 83.7-91.2) in round 3 before it experienced a steady decline in round 4 [41.3% (CI:95%; 36.7-45.9) (Figure 2, Supplementary Table 3).
These prevalence rates indicate substantial variability in type 2 poliovirus immunity across the high-risk cities, highlighting potential gaps in vaccination coverage that may require targeted strategies for specific regions.
3.6. Seroprevalence of Polio Type-3 Across High-Risk Cities
The trends for poliovirus type 3 were nearly identical to type 1, with seroprevalence being consistently high in most districts. Karachi and Peshawar remained well above 93% through all rounds, even peaking at over 97% in rounds 2 and 3. In Quetta, the type 3 prevalence improved from 92.9% (CI:95%; 90-95.8) in round 1 to 96.7% (CI:95%; 94.7-98.7) in round 3, before slightly declining to 89.8% (CI:95%; 87-92.5) in round 4. Similarly, in Pishin, the prevalence increased from 86.7% (CI:95%; 82.9-90.5) in round 1 to 97% (CI:95%; 95.1-98.9) in round 3 and then decreased to 84.6% (CI:95%; 81.3-87.9) in round 4. On the other hand, Killa Abdullah had persistently lagged behind other districts, with seroprevalence for type 3 ranging from 80.1% (CI:95%; 75.7-84.6) in round 1 to a peak of 94.3% (CI:95%; 91.7-96.8) in round 3, followed by a steep drop to 67.5% (CI:95%; 63.1-71.8) in round 4 ) (Figure 2, Supplementary Table 3).
These Findings indicate that while most cities maintained a high level of immunity (above 90%) against type 3 poliovirus, Killa Abdullah showed a concerning situation, with a suboptimal seroprevalence level. The 95% confidence intervals suggest that these patterns are statistically significant, especially for the sharp decline in Killa Abdullah. Overall, these findings underscore the need for targeted interventions in Killa Abdullah and continued vigilance in other regions to sustain and strengthen immunity against type 3 poliovirus in these high-risk populations.
Figure 2.
Polio seroprevalence trends by types across high-risk cities and survey rounds.

4. Discussion
This study assesses the immunity levels among children aged 6-11 months for all three strains of poliovirus in Pakistan’s high-risk region between 2016 and 2023. The results identify gaps in immunity and regional disparities influenced by national immunization efforts and operational challenges. The findings provide valuable insights into the effectiveness of current strategies for delivering immunization services in the region.
Throughout the study period, the consistently high seroprevalence for type 1 poliovirus (>90%) was observed in most areas, especially in Punjab and Sindh (98–99%), which was a major programmatic success. This stability in immunity levels reflects the continued focus on type 1 poliovirus in both routine immunization and supplementary vaccination campaigns, since it is the only endemic wild poliovirus serotype still present in Pakistan [6,33,51]. However, the decline in poliovirus type 1 immunity in Balochistan to 89% in 2022-23 reflects challenges of maintaining immunity level posed by security situations, remote geography, and health system constraints [33,34].
Among high-risk cities, the type 1 immunity in Karachi and Peshawar – historical poliovirus reservoirs- remained remarkably high and stable, demonstrating that intensive vaccination campaigns in these urban centers have been largely successful in building and maintaining population immunity [10,25]. Conversely, the decline in immunity in Quetta despite past improvements indicates vulnerability to immunity gaps, a concern supported by environmental surveillance findings that could potentially sustain virus transmission [26,32]. The overall stability of type 1 seroprevalence, even during periods of programmatic disruption due to the COVID-19 pandemic, suggests that prioritization of type 1 vaccination activities has been effective [29,30]. However, the decreasing trend in several regions during the 2022-23 survey indicates for continued vigilance, particularly in densely populated areas with inadequate sanitation infrastructure [52,53]. Similar patterns have been reported in Afghanistan, where continuous WPV1 transmission in border regions is associated with pockets of low immunity to type 1 poliovirus caused by insecurity, limited access, and difficult geographical terrains [38]. On the other hand, countries such as India have effectively eliminated WPV1 through the implementation of targeted national SIAs, a robust, regular vaccination program, and efficient surveillance [41,54]. These comparative experiences demonstrate the importance of health system strength, community trust, logistical reach, and robust monitoring to maintain high immunity and eradicate polioviruses.
Type 2 poliovirus immunity displayed a relatively high temporal variation, caused by the 2016 global switch from tOPV to bOPV, which excluded vaccination for type 2 poliovirus [16,17]. As anticipated, nonetheless, concerning, this global switch led to declines in type 2 seroprevalence in Pakistan, with rates dropping below 40% in Balochistan and Sindh in 2022–23. This declining trend across the provinces leaves a substantial population vulnerable to type 2 poliovirus infection, including vaccine-derived strains [11,12], and also highlights a systemic challenge rather than region-specific issues, underscoring the impact of the global OPV switch on population immunity level [18].
Our findings reflect that among polio high-risk cities, type 2 immunity patterns varied greatly. In Karachi, the immunity level was low and continued to decline throughout the study period, whereas in Pishin, it remarkably improved (90%) and remained stable post-2017- 18, likely due to the implementation of SIAs with mOPV2 or IPV in response to cVDPV2 outbreaks [19,25]. Our findings related to type 2 immunity levels and patterns are aligned with the epidemiological reality of cVDPV2 outbreaks in Pakistan during the study period [12]. The persistent low immunity in multiple regions created conditions favorable for the emergence and circulation of vaccine-derived strains, complicating eradication efforts [13]. The partial recovery observed in some regions by 2022-23 may reflect the impact of targeted type 2 vaccination responses, but the continued low levels in other areas suggest that maintaining adequate type 2 immunity remains a significant challenge in the post-switch period [19].
Similar to the findings of our study, post-switch type 2 immunity declines were reported in Nigeria and the Democratic Republic of the Congo, where cVDPV2 outbreaks occurred due to inadequate IPV coverage and delayed mOPV2 responses [13,14]. However, countries that swiftly implemented mOPV2 in their immunization campaigns, such as Benin and Egypt, demonstrated more promising control of cVDPV2 spread, highlighting the importance of a timely response for evolving issues around poliovirus circulation following the 2016 global switch [11,18]. These proven strategies reinforce the need for a strategic implementation of mOPV2 in Pakistan in areas with low type 2 immunity.
For type 3 poliovirus, immunity level generally improved over the study period in most regions, likely due to continued inclusion of bOPV containing type 1 and 3 strains in routine immunization and supplementary campaigns in the post-switch era [16]. However, by 2022-23, several areas experienced a significant decline; for instance, in Killa Abdullah, type 3 immunity dropped from 94% in 2017-18 to 69% in 2022-23, creating a significant immunity gap that could potentially facilitate virus transmission if type 3 strains were introduced [55,56]. The timing of this reduction can be associated with the distortion in routine immunization activities in the wake of the COVID-19 pandemic, which could have influenced the immunity level in the population. This also highlights how high-risk communities are vulnerable to external programmatic shocks [29,30]. Aligned with our findings, studies from Yemen and Indonesia also recorded a decline in immunity level for type 3 poliovirus in the aftermath of type poliovirus eradication in 2019, mainly due to reduced focus on it [40,57,58]. These findings suggest that eradication certification must not lead to contentment in immunization efforts, especially in polio high-risk areas and under-immunized communities like Pakistan.
The pronounced regional disparities in immunity level for all three strains of polio viruses in our study mirror the underlying differences in access to immunization services, health system capacity, and operational reach [32]. Urban centers like Karachi maintained high type 1 and type 3 immunity and maintained consistency in type 2 protection level. Peripheries and border districts in Balochistan, like Killa Abdullah, demonstrated more volatile immunity patterns across all serotypes, likely due to challenges related to cross-border movement, accessibility, and security concerns [36,38,59].
These patterns underscore the need for granular and context-specific strategies in delivering immunization services. Though national-level coverage may appear adequate, gaps in immunity at the subnational level and certain pockets can reinforce virus circulation [60].
Although our study did not explicitly analyze the impact of COVID-19 disruptions, the declines in immunity level between 2018-19 and 2022-23 provide insights into potential consequences of the pandemic on immunity level for all three serotypes. These disruptions likely contributed to missed vaccinations and weakened the health system outreach, disproportionately impacting the already underserved communities [28,29,30,31].
The findings of this study highlight several policy considerations. Maintaining high immunity for type 1 should be the cornerstone of eradication efforts with robust monitoring in areas showing early signs of decline, and for type 3 immunity, the eradication certification should not derail the immunity maintenance, and efforts must be sustained to uphold the immunity level in under-immunized communities. For type 2 immunity gaps, demand integrated approaches including administration of mOPV in SIAs and IPV in both routine nd outreach sessions with enhanced surveillance. Monitoring of immunity level supported by environmental and AFP surveillance is needed for informed data-driven decision making and to close the immunity gaps contributing towards the ultimate goal of a polio-free Pakistan.
The study has several limitations. Although data were collected through multiple rounds from 2016 to 2023, the survey design was cross-sectional, which limits the ability to draw causal inferences about changes in immunity at the individual level. The vaccination history was in part captured through caregiver recall, in the absence of vaccination cards. This could result in the unintentional bias of recall about vaccination status. Even though this timeframe also included the COVID-19 epidemic, its particular effects on immunization activities and the subsequent immunity gaps were not specifically captured during this study. Thus, any interpretation with regard to the disruptions of the pandemic remains inferential. In spite of these limitations, our study provides trends and inequities in poliovirus immunity across the ‘at-risk’ regions of Pakistan, highlighting the gaps that demand programmatic efforts.
5. Conclusions
The findings from this series of serological evaluations indicate a promising yet variable progression in the developing and maintaining immunity to all three strains of polioviruses in polio high-risk areas of Pakistan. These results underscore the necessity for ongoing vigilance and the implementation of context-specific strategies to preserve the high type 1 immunity, improve and stabilize type 3 immunity, and address gaps in type 2 immunity through targeted interventions utilizing mOPV2 and IPV. Moreover, the establishment of robust surveillance mechanisms, tailored outreach initiatives directed at underserved populations, and improving immunization coverage are critical for closing immunity gaps and ultimately eradicating poliovirus in the country.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org.
Author Contributions
SBS conceptualized and designed the survey and assisted with interpreting the results. IH developed the sampling strategy and tools and supervised the field activities. IH, AK, and HA drafted the manuscript. MU assisted with study design, formulating contextually relevant survey tools, and oversaw data collection activity. MS performed the statistical analysis. MMA supervised the laboratory analysis of the samples. MAH, AB, RH, JF, and all authors reviewed and approved the final manuscript for submission.
Funding
The study was supported by the Bill & Melinda Gates Foundation [grant number OPP1156736].
Institutional Review Board Statement
Ethical approval was obtained from the Ethical Review Committee of Aga Khan University, Pakistan (2024-7646), and the National Bioethics Committee, Pakistan (NBC-814). Informed consent was obtained from the caregivers of the participants included in the study.
Informed Consent Statement
Written Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data will be made available on request.
Acknowledgments
We are immensely grateful to all participants for their cooperation during the survey.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization. World Health Assembly. Global eradication of poliomyelitis by the year 2000: resolution of the 41st World Health Assembly. Geneva: WHO; 1988.
- Haqqi A, Zahoor S, Aftab MN, Tipu I, Rehman Y, Ahmed H, et al. COVID-19 in Pakistan: impact on global polio eradication initiative. J Med Virol. 2020, 93, 141–143. [CrossRef]
- Bandyopadhyay AS, Garon J, Seib K, Orenstein WA. Polio vaccination: past, present and future. Future Microbiol. 2015, 10, 791–808. [CrossRef]
- Pons-Salort M, Molodecky NA, O’Reilly KM, Wadood MZ, Safdar RM, Etsano A, et al Population immunity against Serotype-2 poliomyelitis leading up to the global withdrawal of the Oral poliovirus vaccine: Spatio-temporal modelling of surveillance data. PLoS Med. 2016, 13, e1002140. [CrossRef]
- Hsu CH, Kader M, Mahamud A, et al. Progress Toward Poliomyelitis Eradication — Pakistan, January 2022–July 2023. MMWR Morb Mortal Wkly Rep. 2023, 72, 1057–1062. [Google Scholar]
- Chard AN, Datta SD, Gumede N, et al. Progress Toward Global Polio Eradication — Worldwide, January 2021–March 2023. MMWR Morb Mortal Wkly Rep. 2023, 72, 533–538. [Google Scholar]
- Akseer N, Rizvi A, Bhatti Z, et al. Association of Polio Eradication Initiative with the Delivery of Essential Maternal and Child Health Interventions in Pakistan: A Population-Based Cross-Sectional Study. Lancet Glob Health. 2022, 10, e1302–e1312. [Google Scholar]
- Ghafoor S, Sheikh N. Eradication and Current Status of Poliomyelitis in Pakistan: Ground Realities. J Immunol Res. 2016, 2016, 6837824. [Google Scholar]
- Raza F, Svensson J, Shehzad S, et al. Endemic Polio in Peshawar, Pakistan: Perceptions, Practices, and Risk Analysis. Health Policy Plan. 2021, 36, 383–394. [Google Scholar]
- Shah M, Khan MK, Shakeel S, et al. Resistance of Polio to Its Eradication in Pakistan. Virol J. 2021, 18, 108. [Google Scholar]
- Mbaeyi C, Alleman MM, Ehrhardt D, et al. Update on Vaccine-Derived Poliovirus Outbreaks — Worldwide, January 2020–June 2021. MMWR Morb Mortal Wkly Rep. 2021, 70, 1691–1699. [Google Scholar] [CrossRef] [PubMed]
- Macklin GR, O’Reilly KM, Grassly NC, et al. Evolving Epidemiology of Poliovirus Serotype 2 Following Withdrawal of the Type 2 Oral Poliovirus Vaccine. Science. 2020, 368, 401–405. [Google Scholar] [CrossRef]
- Burns CC, Diop OM, Sutter RW, Kew OM. Vaccine-Derived Polioviruses. J Infect Dis. 2014, 210 (Suppl. 1), S283–S293.
- Bandyopadhyay AS, Garon J, Seib K, Orenstein WA. Polio vaccination: past, present and future. Future Microbiol. 2015, 10, 791–808. [Google Scholar] [CrossRef]
- Pons-Salort M, Molodecky NA, O’Reilly KM, Wadood MZ, Safdar RM, Etsano A, et al. Population immunity against Serotype-2 poliomyelitis leading up to the global withdrawal of the Oral poliovirus vaccine: Spatio-temporal modelling of surveillance data. PLoS Med. 2016, 13, e1002140. [Google Scholar] [CrossRef]
- Hampton LM, Farrell M, Ramirez-Gonzalez A, et al. Cessation of Trivalent Oral Poliovirus Vaccine and Introduction of Inactivated Poliovirus Vaccine — Worldwide, 2016. MMWR Morb Mortal Wkly Rep. 2016, 65, 934–938. [Google Scholar] [CrossRef] [PubMed]
- Sutter RW, Platt L, Mach O, et al. The New Polio Eradication End Game: Rationale and Supporting Evidence. J Infect Dis. 2014, 210 (Suppl. 1), S434–S438. [Google Scholar] [CrossRef] [PubMed]
- Bandyopadhyay AS, Garon J, Seib K, Orenstein WA. Polio Vaccination: Past, Present and Future. Future Microbiol. 2015, 10, 791–808. [Google Scholar] [CrossRef]
- Duintjer Tebbens RJ, Hampton LM, Thompson KM. Implementation of Coordinated Global Serotype 2 Oral Poliovirus Vaccine Cessation: Risks of Potential Non-Synchronous Cessation. BMC Infect Dis. 2016, 16, 237. [Google Scholar]
- Garon J, Seib K, Orenstein WA, Gonzalez AR, Blanc DC, Zaffran M, et al. Polio endgame: the global switch from tOPV to bOPV. Expert Rev Vaccines. 2016, 15, 693–708. [CrossRef]
- Taniuchi M, Famulare M, Zaman K, Uddin MJ, Upfill-Brown AM, Ahmed T, et al. Community transmission of type 2 poliovirus after cessation of trivalent oral polio vaccine in Bangladesh: an open-label cluster-randomised trial and modelling study. Lancet Infect Dis. 2017, 17, 1069–1079. [CrossRef]
- Concepción FE, Mark AP, Abhijeet A, Steven GFW, Roland WS, Jay DW, et al. Poliovirus vaccination options for achieving eradication and securing the endgame. Curr Opin Virol. 2013, 3, 309–315. [CrossRef]
- Pakistan Polio Eradication Programme. (2025). Polio cases in provinces. Available at: https://www.endpolio.com.pk/polioin-pakistan/polio-cases-in-provinces.
- Mir F, Quadri F, Mach O, et al. Monovalent Type-1 Oral Poliovirus Vaccine Given at Short Intervals in Pakistan: A Randomised Controlled, Four-Arm, Open-Label, Non-Inferiority Trial. Lancet Infect Dis. 2015, 15, 889–897. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Pakistan Polio Update—January-December 2022. WHO Regional Office for the Eastern Mediterranean; 2023.
- Asghar H, Diop OM, Weldegebriel G, et al. Environmental Surveillance for Polioviruses in the Global Polio Eradication Initiative. J Infect Dis. 2014, 210 (Suppl. 1), S294–S303. [Google Scholar] [CrossRef]
- Alam MM, Shaukat S, Sharif S, et al. Detection of Multiple Cocirculating Wild Poliovirus Type 1 Lineages Through Environmental Surveillance: Impact and Progress During 2011-2013 in Pakistan. J Infect Dis.
- Zafar M, Ullah MA, Zahoor MA, et al. COVID-19 and Polio in Pakistan: Challenges, Efforts, and Recommendations. Int J Infect Dis. 2022, 115, 172–179. [Google Scholar]
- Chandir S, Siddiqi DA, Mehmood M, et al. Impact of COVID-19 Pandemic on Polio Vaccination in Pakistan: A Retrospective Cross-Sectional Study. BMJ Open. 2020, 10, e043813. [Google Scholar]
- Zainab SM, Khowaja S, Akhtar I, et al. Polio Vaccination Amidst COVID-19 in Pakistan: What Are the Efforts and Challenges? J Glob Health. 2022, 12, 03023. [Google Scholar]
- Rana MS, Usman M, Salman M, et al. Impact of COVID-19 Pandemic on Polio Surveillance in Pakistan. J Infect. 2021, 82, 414–451. [Google Scholar] [CrossRef]
- Khan MT, Zaheer S, Shafique K. Maternal Education, Empowerment, Economic Status and Child Polio Vaccination Uptake in Pakistan: A Population Based Cross Sectional Study. BMJ Open. 2017, 7, e013853. [Google Scholar] [CrossRef]
- Khan AJ, Akber A, Nawaz M, et al. Transmission Dynamics of Wild Poliovirus Type 1 in a High-Risk District of Pakistan with Continuously High Vaccination Coverage. BMC Infect Dis. 2022, 22, 677. [Google Scholar]
- Naqvi AA, Naqvi SBS, Zehra F, et al. Estimation of the Burden of Children Affected by Poliomyelitis in Pakistan and an Assessment of the Physical Limitations Faced by these Children. J Taibah Univ Med Sci. 2018, 13, 241–246. [Google Scholar]
- Hsu CH, Mahamud A, Morales M, et al. Progress Toward Poliomyelitis Eradication — Afghanistan, January 2021–May 2023. MMWR Morb Mortal Wkly Rep. 2023, 72, 683–688. [Google Scholar]
- Jorba J, Diop OM, Iber J, et al. Update on Vaccine-Derived Poliovirus Outbreaks — Worldwide, January 2018–June 2019. MMWR Morb Mortal Wkly Rep. 2019, 68, 1024–1028. [Google Scholar] [CrossRef]
- Cowger TL, Burns CC, Sharif S, et al. The Role of Supplementary Environmental Surveillance to Complement Acute Flaccid Paralysis Surveillance for Wild Poliovirus in Pakistan – 2011-2013. PLoS One. 2017, 12, e0180608. [Google Scholar]
- Hsu CH, Rehman MS, Ray P, et al. Progress Toward Poliomyelitis Eradication — Pakistan, January 2021–July 2022. MMWR Morb Mortal Wkly Rep. 2022, 71, 1359–1364. [Google Scholar]
- Ahmad SO, Bux R, Yousuf F. Health Care in Pakistan—A Systems Perspective. In: Cockerham WC, ed. The Wiley Blackwell Encyclopedia of Health, Illness, Behavior, and Society. Chichester: John Wiley & Sons.
- Sutter RW, John TJ, Jain H, et al. Immunogenicity of Bivalent Types 1 and 3 Oral Poliovirus Vaccine: A Randomised, Double-Blind, Controlled Trial. Lancet. 2010, 376, 1682–1688. [Google Scholar] [CrossRef]
- Grassly, NC. The Final Stages of the Global Eradication of Poliomyelitis. Philos Trans R Soc Lond B Biol Sci. 2013, 368, 20120140. [Google Scholar] [CrossRef] [PubMed]
- Habib MA, Soofi SB, Sheraz A, et al. Evaluation of Immunogenicity and Safety of the 13-Valent Pneumococcal Conjugate Vaccine in Pakistani Children. Vaccine. 2016, 34, 4739–4744. [Google Scholar]
- Estivariz CF, Pallansch MA, Anand A, et al. Poliovirus Vaccination Options for Achieving Eradication and Securing the Endgame. Curr Opin Virol. 2013, 3, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Hussain I, Mach O, Habib A, et al. Seroprevalence of Anti-Polio Antibodies in Children from Polio High-Risk Areas of Pakistan: A Cross-Sectional Survey 2015-2016. BMJ Open. 2017, 7, e013014. [Google Scholar]
- Grassly NC, Wadood MZ, Safdar RM, et al. Effect of Inactivated Poliovirus Vaccine Campaigns, Pakistan, 2014-2017. Emerg Infect Dis. 2018, 24, 2113–2115. [Google Scholar] [CrossRef]
- Voorman A, Habib MA, Hussian I, Safdar RM, Ahmed JA, Weldon WC, et al. Immunity and field efficacy of type 2-containing polio vaccines after cessation of trivalent oral polio vaccine: a population-based serological study in Pakistan. Vaccine. 2020, 5, 100067. [CrossRef]
- Hussain I, Umer M, Khan A, Sajid M, Ahmed I, Begum K, Iqbal J, Alam MM, Safdar RM, Baig S, Voorman A, Partridge J and Soofi S. Exploring the path to polio eradication: insights from consecutive seroprevalence surveys among Pakistani children. Front. Public Health 2024, 12, 1384410. [CrossRef]
- Weldon WC, Oberste MS, MA P. Standardized methods for detection of poliovirus antibodies. New York: Springer (2016).
- Plotkin, SA. Correlates of protection induced by vaccination. Clin Vaccine Immunol. 2010, 17, 1055–1065. [Google Scholar] [CrossRef] [PubMed]
- StataCorp. Stata Statistical Software: Release 18. College Station, TX: StataCorp LLC.; 2024.
- Chandir S, Siddiqi DA, Mehmood M, et al. Impact of COVID-19 Pandemic on Polio Vaccination in Pakistan: A Retrospective Cross-Sectional Study. BMJ Open. 2020, 10, e043813. [Google Scholar]
- Fatima M, Khan MA, Ali S, et al. Projection of Spatial Spread of Wild Polio Virus Type 1 in Pakistan. Commun Nonlinear Sci Numer Simul. 2022, 113, 106523. [Google Scholar]
- Bigouette JP, Wilkinson AL, Tallis G, et al. Progress Toward Polio Eradication — Worldwide, January 2019–June 2021. MMWR Morb Mortal Wkly Rep. 2021, 70, 1129–1135. [Google Scholar] [CrossRef]
- O’Reilly KM, Durry E, ul Islam O, et al. The Effect of Mass Immunisation Campaigns and New Oral Poliovirus Vaccines on the Incidence of Poliomyelitis in Pakistan and Afghanistan, 2001–2011: A Retrospective Analysis. Lancet. 2012, 380, 491–498. [Google Scholar] [CrossRef]
- Shaikh NB, Soomro TR, Ghouri A, et al. Key Determinants of Polio Immunity Gaps in Areas of High Risk in Pakistan. J Infect Dis. 2020, 221, 744–750. [Google Scholar]
- Minor, PD. Polio Vaccines and the Eradication of Poliomyelitis. Lancet. 2021, 398, 1731–1740. [Google Scholar] [CrossRef]
- World Health Organization. Certification of the Global Eradication of Wild Poliovirus Type 3. Wkly Epidemiol Rec. 2019, 94, 545–547.
- Kew OM, Cochi SL, Jafari HS, et al. Possible Eradication of Wild Poliovirus Type 3 — Worldwide, 2012. MMWR Morb Mortal Wkly Rep. 2014, 63, 1031–1033. [Google Scholar]
- Rehman AU, Sahito A, Alvi ZA, et al. Geographical Disparities in the Access of Polio Vaccination in Pakistan: A Secondary Analysis. J Prim Care Community Health. 2021, 12, 21501327211027735. [Google Scholar]
- Molodecky NA, Blake IM, O’Reilly KM, et al. Risk Factors and Short-term Projections for Serotype-1 Poliomyelitis Incidence in Pakistan: A Spatiotemporal Analysis. PLoS Med. 2017, 14, e1002323. [Google Scholar]

Table 1.
Survey round-wise demographic information and vaccination coverage.
| Survey rounds | Number of Districts | Clusters covered | Households covered | Number of children surveyed (N) | Male (%) | Vaccination Card (%) | OPV3 Coverage (%) | IPV Coverage (%) | Caregiver Education level (Illiteracy rate- %) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 10 | 326 | 4143 | 4146 | 52.0 | 65.3 | 75.3 | 69.2 | 73.3 |
| 2 | 10 | 325 | 4093 | 4094 | 52.2 | 60.3 | 69.0 | 74.0 | 76.6 |
| 3 | 10 | 324 | 3985 | 3987 | 53.0 | 70.8 | 68.8 | 81.9 | 73.2 |
| 4 | 38 | 1109 | 20150 | 20680 | 51.9 | 40.0 | 74.1 | 55.4 | 67.5 |
Abbreviations: IPV: Inactivated Poliovirus Vaccine; OPV: Oral Poliovirus Vaccine.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



