
Submitted:
29 September 2025
Posted:
30 September 2025
You are already at the latest version
Abstract
Background: Coronary artery bypass grafting (CABG) is a standard treatment for ad-vanced coronary artery disease (CAD). Despite its effectiveness, many patients devel-op recurrent ischemia requiring repeat revascularization. Residual platelet reactivity (RPR) and dyslipidemia are considered important contributors to graft failure and dis-ease progression. This study investigated the association of RPR and dyslipidemia with repeat revascularization in post-CABG patients. Methods: A observational cohort study was performed at a tertiary cardiology center in Kazakhstan. A total of 200 patients with prior CABG who underwent repeat coro-nary angiography between 2023 and 2024 for recurrent ischemic symptoms were in-cluded. Clinical data, comorbidities, lipid profiles, and antiplatelet response were ana-lyzed. RPR was measured with the VerifyNow P2Y12 assay where available. Dyslipidemia was defined according to current European guidelines, 2019/2021. Results: Elevated RPR was found in 45% (n = 90) of patients despite dual antiplatelet therapy. Poor lipid control, especially increased low-density lipoprotein cholesterol (LDL-C) and total cholesterol was common among patients undergoing repeat percu-taneous coronary intervention (PCI). Both RPR and dyslipidemia were independently associated with native coronary disease progression and graft failure. Conclusions: RPR and dyslipidemia are frequent and clinically relevant predictors of repeat revascularization after CABG. Optimizing antiplatelet and lipid-lowering ther-apy should be a priority in secondary prevention for this high-risk group. These results are particularly important in the Central Asian setting, where post-CABG management strategies require further improvement.
Keywords:
coronary artery bypass grafting
; residual platelet reactivity
; dyslipidemia
; repeat revascularization
; dual antiplatelet therapy
; Kazakhstan
1. Introduction
Coronary artery bypass grafting (CABG) remains a cornerstone in the management of advanced coronary artery disease (CAD), especially in patients with multivessel involvement. While surgical revascularization provides symptomatic relief and mortality benefit, a considerable proportion of patients continue to experience recurrent ischemic symptoms and adverse cardiovascular events during follow-up.
Platelets play a central role in the pathogenesis of atherosclerosis and arterial thrombosis. High residual platelet reactivity (HRPR), even under antiplatelet therapy, is a well-established predictor of major adverse cardiovascular events, including myocardial infarction (MI), stroke, and stent thrombosis [1,2]. Patients with multivessel CAD undergoing CABG have been shown to exhibit higher levels of HRPR compared to those with single-vessel disease. Several comorbidities—including dyslipidemia, anemia, chronic kidney disease (CKD), reduced left ventricular ejection fraction (LVEF), and overweight/obesity—are strongly associated both with HRPR and with the presence of extensive coronary disease, thereby amplifying the risk of recurrent ischemic events [3,4].
The prothrombotic role of platelets is particularly important in patients receiving long-term antiplatelet therapy aimed at reducing MI and stroke incidence. Anemia, common among patients with chronic heart failure (CHF), is linked to impaired response to clopidogrel, increased HRPR, higher hospitalization rates, and worse survival [5,6,7]. Renal dysfunction further diminishes antiplatelet efficacy and contributes to poor outcomes [8]. HRPR has consistently been recognized as a poor prognostic marker in acute coronary syndrome (ACS) [9]. Smoking, dyslipidemia, and elevated cholesterol levels additionally enhance platelet activation and thrombotic risk [4,5]. Moreover, obesity—particularly class I—has been associated with increased HRPR during antiplatelet therapy [10].
In the post-CABG setting, hemostatic alterations induced by cardiopulmonary bypass may further influence platelet function and predispose to enhanced platelet activation [11]. The pathophysiological mechanism linking HRPR to cardiovascular complications primarily involves exaggerated platelet aggregation and thrombus formation [12,13,14]. Consequently, HRPR is considered an independent risk factor for recurrent ischemic events, including MI, graft failure, stent thrombosis, and cardiovascular death [15,16].
Importantly, dyslipidemia represents a modifiable determinant of both platelet hyperreactivity and atherosclerotic progression. Failure to achieve guideline-recommended low-density lipoprotein cholesterol (LDL-C) targets—particularly <1.4 mmol/L in very-high-risk patients according to the 2019/2021 ESC guidelines—significantly increases the risk of recurrent ischemia and need for repeat revascularization. Thus, strict lipid control remains a cornerstone of secondary prevention in post-CABG patients and is crucial for improving long-term outcomes.
In this study, we analyzed 200 post-CABG patients from a tertiary cardiac center in Kazakhstan. Recurrent angina was observed in 94% (n=188), and 68% (n=136) required repeat percutaneous coronary intervention (PCI) after coronary angiography. Our aim was to identify the predominant clinical phenotypes associated with these outcomes, with particular emphasis on dyslipidemia and inadequate LDL-C control, residual platelet reactivity despite dual antiplatelet therapy, anemia, CKD, and heart failure (HF).
2. Materials and Methods
Study Design and Setting
This observational single-center cohort study was conducted from January 2023 to December 2024 at the Research Institute of Cardiology and Internal Medicine, a tertiary-level cardiovascular center in Almaty, Kazakhstan. The study aimed to evaluate residual platelet reactivity and dyslipidemia as risk factors for repeat revascularization in patients with established coronary artery disease (CAD) who previously underwent coronary artery bypass grafting (CABG).
Patient Population
Eligible participants were adult patients (≥18 years) with a documented history of coronary artery bypass grafting (CABG) and a diagnosis of stable coronary artery disease (CAD) who were admitted for repeat coronary angiography due to recurrent ischemic symptoms.
Inclusion Criteria:
Prior history of CABG
Documented stable CAD
Clinical and/or instrumental evidence of recurrent myocardial ischemia (e.g., angina, positive stress test, ischemic ECG changes)
Exclusion Criteria:
Presence of atrial fibrillation
Current use of oral anticoagulant therapy (e.g., rivaroxaban, apixaban, dabigatran)
Diagnosis of acute coronary syndrome (ACS) at the time of admission
A detailed flowchart of patient selection, including inclusion and exclusion criteria, is presented in Figure 1.
Residual Platelet Reactivity Assessment
Residual platelet reactivity (RPR) was evaluated using the VerifyNow P2Y12 assay (Instrumentation Laboratory, Bedford, MA, USA), a point-of-care system that quantifies platelet inhibition and reports results as P2Y12 Reaction Units (PRU). High residual platelet reactivity (HRPR) was defined as PRU ≥208, in accordance with current international consensus guidelines.
Clinical and Laboratory Data Collection
Baseline demographic, clinical, and pharmacological characteristics were extracted from electronic medical records. The following parameters were systematically evaluated:
Lipid profile: Total cholesterol, LDL-C, HDL-C, triglycerides
Renal function: Serum creatinine and estimated glomerular filtration rate (eGFR) to identify chronic kidney disease (CKD)
Hemoglobin level: Assessed for anemia according to WHO criteria
Left ventricular ejection fraction (LVEF): Measured via transthoracic echocardiography
Body mass index (BMI): Used to classify overweight and obesity
Cardiovascular complications: Including heart failure, diabetes mellitus, and prior myocardial infarction
All patients were treated with guideline-directed medical therapy in accordance with the 2024 European Society of Cardiology (ESC) recommendations for the management of chronic coronary syndromes.
Ethical Considerations
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. Ethical approval was obtained from the Local Ethics Committee of Asfendiyarov Kazakh National Medical University, Almaty, Republic of Kazakhstan (Protocol No. 11(134); Date: 04 November 2022). Written informed consent was obtained from all participants prior to enrollment.
Statistical Analysis
The data are presented as Median [Quartile 1; Quartile 3], as the majority of the quantitative variables do not follow a normal distribution. Between-group comparisons were performed using the Mann–Whitney U test for quantitative variables, or the chi-squared test (Fisher’s exact test when the number of observations was small) for qualitative variables. Categorical variables were expressed as frequencies and percentages. Normality of continuous variables, including PRU values, was assessed using the Shapiro–Wilk test. For comparisons of continuous variables between groups (e.g., HRPR vs. non-HRPR) Mann–Whitney U test was used as appropriate. Categorical variables were analyzed using the Chi-square test or Fisher’s exact test. A stepwise logistic regression analysis was performed to identify predictors associated with the risk of stenting after coronary artery bypass grafting (CABG). A p-value < 0.05 was considered statistically significant. All statistical tests were two-sided, and 95% confidence intervals (CIs) were reported when relevant.
3. Results
A total of 195 post-CABG patients were included in the final analysis. Among them, 136 patients (69.7%) underwent repeat percutaneous coronary intervention (PCI), whereas 59 patients (30.3%) did not require reintervention. Baseline demographic, clinical, laboratory, and instrumental characteristics were systematically compared between the two groups (Table 1).
Demographic and Clinical Characteristics
Patients requiring repeat PCI were significantly older than those without reintervention (median age: 71.0 [IQR 65.8–75.0] vs. 66.0 [61.5–73.0] years; p = 0.016). No significant difference in sex distribution was observed (p = 0.431). Current smoking was more frequent in the non-reintervention group (54.2% vs. 28.7%; p = 0.001), whereas alcohol consumption rates were low and comparable (p = 0.164). Systolic blood pressure was higher in the repeat PCI group (130 [120–140] vs. 120 [110–130] mmHg; p = 0.041), while diastolic pressure did not differ significantly.
Comorbidities and Medical History
The prevalence of hypertension, diabetes mellitus, prior myocardial infarction, stroke, chronic kidney disease (CKD), anemia, and obesity was similar between groups. However, a higher frequency of prior CABG was noted among patients undergoing reintervention (96.3% vs. 83.1%; p = 0.003).
Biochemical and Hematological Parameters
No significant group differences were found in lipid profile (total cholesterol, LDL-C, HDL-C, triglycerides), glycemic control (glucose, HbA1c), renal function (creatinine, eGFR), liver enzymes (ALT, AST), inflammatory markers (CRP), or thyroid function (TSH, T4). Interestingly, cardiac troponin levels were lower in the reintervention group (14.3 [10.3–32.8] vs. 20.0 [13.4–95.4] ng/L; p = 0.002), possibly reflecting differences in post-CABG myocardial injury dynamics.
Platelet Reactivity
Patients undergoing repeat PCI exhibited significantly higher platelet reactivity. Median PRU was 230 [200–274] versus 145 [140–155] (p < 0.001). Moreover, high residual platelet reactivity (HRPR) was present in 66.2% of the reintervention group compared to 0% in the control group (p < 0.001).
Echocardiographic Findings
End-diastolic volume (EDV) was lower in the reintervention group (136 [113–179] vs. 162 [129–206] mL; p = 0.038). Posterior wall thickness (PWT) was also higher (1.10 [1.00–1.20] vs. 1.05 [0.90–1.20] cm; p = 0.030). No significant differences were observed for LVEF, stroke volume, left atrial/ventricular dimensions, or pulmonary artery pressure.
Coronary Angiographic Findings
Patients with repeat PCI demonstrated more extensive coronary artery disease. Significant stenosis was more frequently detected in:
LAD: 52.9% vs. 27.1% (p = 0.002)
LCx: 37.5% vs. 13.6% (p = 0.002)
Diagonal branch: 30.9% vs. 8.5% (p = 0.001)
PDA: 16.9% vs. 1.7% (p = 0.006)
SVGs: 25.0% vs. 5.1% (p = 0.002)
The number of bypass grafts (3.00 [2.00–3.00] vs. 2.00 [2.00–3.00]; p < 0.001) and diseased vessels (4.00 [3.75–5.00] vs. 3.00 [2.00–3.00]; p < 0.001) was also higher in the reintervention group.
Medical Therapy
All patients received statin therapy. Ezetimibe was prescribed more frequently in the reintervention group (34.6% vs. 0%; p < 0.001), suggesting intensified lipid-lowering strategies in patients with progressive disease.
Symptoms and Outcomes
Persistent angina post-CABG was reported in all reintervention patients compared to 88.1% in the control group (p < 0.001). No significant difference in post-CABG mortality was observed.
Summary of Key Findings
High residual platelet reactivity was strongly associated with repeat revascularization.
Older age, greater coronary involvement, and higher number of bypass grafts predicted the need for reintervention.
Despite similar baseline lipid levels, patients requiring repeat PCI were more frequently prescribed ezetimibe.
The prevalence of anemia, CKD, and diabetes was similar between groups, suggesting HRPR and coronary disease burden play a more central role in post-CABG ischemic recurrence.
A total of 195 patients with a history of coronary artery bypass grafting (CABG) were included in the analysis. Based on platelet reactivity (PRU) and clinical criteria, patients were stratified into two groups: those who achieved the therapeutic window for antiplatelet therapy (n = 105) and those classified as having a high residual thrombotic risk (HRTR; n = 90). Comparative analyses of demographic, clinical, laboratory, and angiographic characteristics were performed (Table 2).
Demographic and Clinical Characteristics
No significant differences were observed between the groups regarding age (69.0 [62.0–74.0] vs. 70.5 [65.2–75.0] years; p = 0.147), sex distribution (p = 0.871), or body mass index (BMI; p = 0.096). Interestingly, the prevalence of current smoking was lower in the HRTR group compared with the therapeutic window group (27.8% vs. 43.8%; p = 0.030). Patients in the HRTR group exhibited significantly higher systolic blood pressure (130 [120–140] vs. 120 [115–130] mmHg; p = 0.031) and fasting glucose levels (5.90 [5.23–7.10] vs. 5.54 [5.00–6.20] mmol/L; p = 0.022). A prior history of stroke was also more frequent in the HRTR group (13.3% vs. 3.81%; p = 0.031).
Angiographic Findings
Patients with HRTR had more extensive coronary artery disease, with significantly higher rates of multivessel involvement. Severe stenoses were more prevalent in the proximal left anterior descending artery (57.8% vs. 34.3%; p = 0.002), left circumflex artery (42.2% vs. 20.0%; p = 0.001), diagonal branches (34.4% vs. 15.2%; p = 0.003), posterior descending artery (21.1% vs. 4.76%; p = 0.001), and venous bypass grafts (33.3% vs. 6.67%; p < 0.001). Furthermore, the HRTR group had a higher number of diseased vessels (4.00 [4.00–5.00] vs. 3.00 [2.00–3.00]; p < 0.001) and bypass grafts (3.00 [2.00–4.00] vs. 2.00 [2.00–3.00]; p = 0.001).
Platelet Reactivity and Clinical Outcomes
Platelet reactivity was markedly elevated in the HRTR group (PRU: 255 [230–280] vs. 170 [141–200]; p < 0.001), indicating a suboptimal response to dual antiplatelet therapy. Consistently, all patients in the HRTR group underwent post-CABG stenting (100% vs. 43.8%; p < 0.001) and experienced recurrent angina (100% vs. 93.3%; p = 0.016).
Medical Therapy
All patients were treated with statins; however, ezetimibe was prescribed significantly more often in the HRTR group (47.8% vs. 3.81%; p < 0.001), reflecting attempts at intensified lipid-lowering therapy.
Summary of Findings
Patients classified as HRTR exhibited:
More extensive and severe coronary atherosclerosis;
Higher platelet reactivity despite dual antiplatelet therapy;
Increased frequency of recurrent angina and need for repeat revascularization;
Greater use of adjunctive lipid-lowering therapy.
These findings emphasize the role of HRTR as a marker of poor outcomes in post-CABG patients and underscore the importance of individualized antiplatelet and lipid-lowering strategies in this high-risk population.
A stepwise logistic regression analysis was performed to identify predictors associated with the risk of stenting after coronary artery bypass grafting (CABG). Due to the relatively small sample size (n = 195) and a large number of potential covariates, a stepwise forward/backward selection algorithm was employed (Table 3, picture 1).
Figure 2.
Stepwise logistic regression: predictors associated with the risk of developing stenting after CABG.
Figure 2.
Stepwise logistic regression: predictors associated with the risk of developing stenting after CABG.
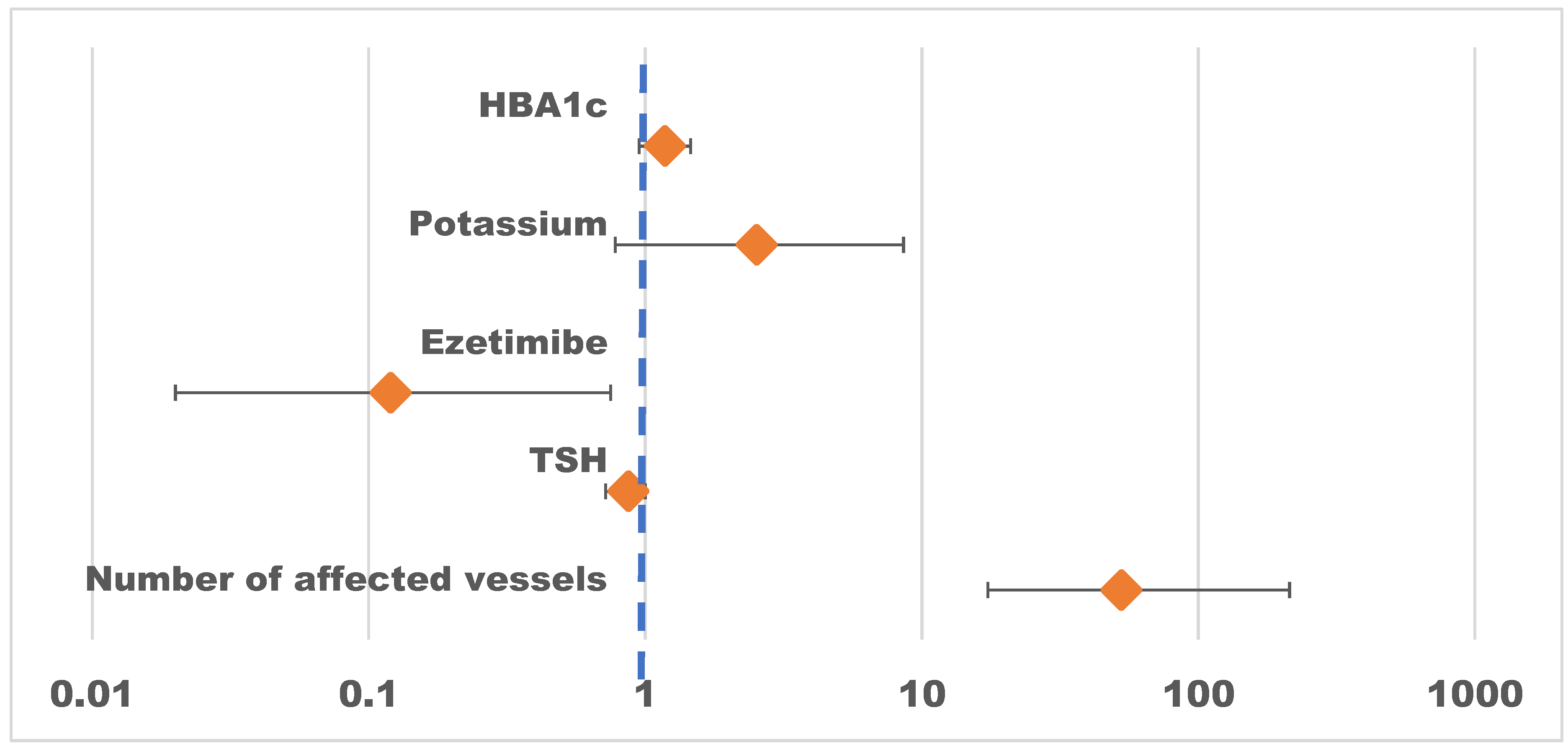
Among the variables included in the regression analysis, the number of affected vessels emerged as the strongest and statistically significant predictor of post-CABG stenting. Patients with more extensive coronary involvement had markedly higher odds of requiring stent implantation (Odds Ratio [OR] = 52.67; 95% CI: 17.33–213.77; p < 0.001).
Conversely, the use of ezetimibe was independently associated with a significantly lower risk of stenting (OR = 0.12; 95% CI: 0.02–0.75; p = 0.023), suggesting a potential protective effect of this lipid-lowering therapy in the postoperative setting.
Other factors, including thyroid-stimulating hormone (TSH) levels (OR = 0.87; 95% CI: 0.72–1.00; p = 0.116), serum potassium (OR = 2.53; 95% CI: 0.78–8.59; p = 0.127), and glycated hemoglobin (HbA1c) (OR = 1.18; 95% CI: 0.95–1.46; p = 0.138), did not reach statistical significance but were retained in the final model as clinically relevant covariates.
The regression model demonstrated good explanatory power, with a Tjur’s R² of 0.681, indicating that a substantial proportion of the variance in stenting risk was explained by the selected predictors.
Collectively, these findings emphasize the critical role of disease burden in determining the need for repeat revascularization, while also highlighting the potential benefit of ezetimibe as part of intensified secondary prevention strategies in post-CABG patients.
DISCUSSION
Our study highlights the substantial burden of recurrent ischemia and the high rate of re-intervention among post-CABG patients in a real-world clinical setting. Recurrent ischemic symptoms were observed in 94% (n = 188) of patients, with 68% requiring repeat PCI. These findings reflect the ongoing progression of atherosclerosis and/or incomplete revascularization, underscoring the challenges of long-term secondary prevention in this population. The role of platelets in arterial thrombosis is well established, particularly in patients with coronary heart disease (CHD) who are on antiplatelet therapy, which has been shown to reduce the risk of major adverse cardiovascular events. Hemoglobin levels also serve as a critical prognostic marker in patients with chronic heart failure (CHF), where anemia is a frequent comorbidity and is associated with increased risks of hospitalization and mortality [2]. Patients with HRPR who undergo percutaneous coronary intervention (PCI) with stent placement while receiving clopidogrel therapy are at elevated risk for recurrent ischemic events. Notably, residual platelet reactivity and HRPR levels have been found to increase in parallel with declining kidney function [3]. Smoking, a well-known risk factor for CHD and MI, is also strongly associated with increased platelet reactivity. When combined with HRPR, smoking further elevates the risk of stent thrombosis [4]. Dyslipidemia contributes to heightened platelet reactivity and thrombotic risk. Elevated cholesterol levels are known to enhance platelet activation and aggregation [5]. Similarly, the extent of coronary atherosclerosis correlates positively with platelet reactivity, suggesting that increased HRPR reflects more widespread atherosclerotic involvement [6]. Anemia has been shown to impair responsiveness to clopidogrel, thus contributing to elevated HRPR [7], while renal dysfunction is also independently associated with increased platelet reactivity [8]. HRPR is recognized as a poor prognostic marker in acute coronary syndrome (ACS) [9]. Moreover, grade 1 obesity has been linked to higher HRPR in patients undergoing antiplatelet therapy [10]. In patients undergoing CABG, alterations in the hemostatic system due to cardiopulmonary bypass may further contribute to increased platelet reactivity [11]. The primary association between HRPR and cardiovascular risk is mediated through enhanced platelet activation, which accelerates thrombus formation [12]. HRPR is therefore regarded as an independent risk factor for a range of serious complications, including myocardial infarction, stent thrombosis, and cardiovascular death [13]. Platelets are directly involved in thrombus formation following the rupture of atherosclerotic plaques in the coronary arteries [14], and individuals with HRPR are at significantly higher risk of recurrent ischemic events [15].
Despite adherence to the 2024 European Society of Cardiology (ESC) guidelines for the management of chronic coronary syndromes, a considerable proportion of patients continued to experience ischemic symptoms. This suggests the persistence of residual risk factors, including dyslipidemia and high platelet reactivity, as well as difficulties in achieving recommended LDL-C targets.
A key driver of recurrent ischemia was persistent dyslipidemia, with most patients failing to reach LDL-C goals despite statin therapy. Limited access to more potent lipid-lowering therapies (e.g., ezetimibe, PCSK9 inhibitors) further contributed to this gap. In Kazakhstan, these medications are not included in the national reimbursement list and are therefore not provided free of charge, which likely explains the underutilization of combination lipid-lowering therapy and the near-universal failure to achieve LDL-C targets [16].
Another important finding was the high prevalence of residual platelet reactivity, as measured by aggregometry in patients receiving dual antiplatelet therapy. This phenotype is known to be associated with increased thrombotic risk, recurrent ischemia, and a higher likelihood of stent failure, which is consistent with our observation of frequent post-CABG revascularization. In addition, comorbid conditions such as anemia, chronic kidney disease, and heart failure were common and likely amplified residual cardiovascular risk. These results are in line with previous reports demonstrating that non-cardiac comorbidities significantly impair long-term outcomes after surgical revascularization. Taken together, our findings point to distinct clinical phenotypes—such as dyslipidemic-thrombotic or cardio-renal-anemic—that may benefit from individualized post-operative management rather than uniform treatment protocols. This approach is particularly relevant in underrepresented regions such as Central Asia, where healthcare resource limitations further complicate secondary prevention.
LIMITATIONS
This study has several limitations. First, it was a retrospective, single-center analysis conducted at the National Research Institute of Cardiology and Internal Medicine, Almaty, Kazakhstan. Although patients were referred from diverse regions, many represented complex or refractory cases of coronary artery disease. Consequently, the findings may not be generalizable to the broader post-CABG population, especially those with less severe clinical presentations or treated at primary-level facilities. Additionally, key parameters such as inflammatory biomarkers or genetic determinants of platelet resistance were not consistently available due to real-world practice constraints.
CONCLUSIONS
Residual dyslipidemia and platelet hyperreactivity remain prevalent and clinically significant contributors to recurrent ischemia and repeat revascularization after CABG. Patients requiring repeat PCI had more extensive coronary involvement, elevated platelet reactivity reflecting suboptimal antiplatelet response, and were more frequently prescribed intensified lipid-lowering therapy. Importantly, the extent of vascular disease and ezetimibe use emerged as independent predictors of stenting risk. These results underscore the need for personalized strategies in lipid-lowering and antiplatelet therapy to optimize outcomes in this high-risk population. Tailored phenotype-guided approaches are especially critical in Kazakhstan, where limited access to advanced therapies may exacerbate residual risk and impede secondary prevention efforts.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org, Figure S1. The flow chart of patients; Figure S2: Stepwise logistic regression: predictors associated with the risk of developing stenting after CABG; Table S1: Descriptive statistics of the group without re-stenting and with re-stenting; Table S2: Descriptive statistics of the Therapeutic window/HRPR group; Table S3: Stepwise logistic regression: predictors associated with the risk of developing stenting after CABG.
Author Contributions
Conceptualization, A.M., L.D., Sh.Zh, F.N., D.K. and A.S; methodology, A.M., L.D., Sh.Zh, F.N., D.K. and A.S.; formal analysis, A.M., Sh.Zh, F.N., D.K., A.S., O.S., F.R. and D.A.; in-vestigation, A.M., Sh.Zh, F.N., D.K., O.S., F.R. and D.A.; resources, A.M., Sh.Zh., D.К., F.N., O.S. and D.A.; data curation, A.M., Sh.Zh., F.N., D.K. and D.A.; writing—original draft, A.M., Sh.Zh., F.N., D.К., O.S., D.A. and A.S.; writing—review and editing, A.M., F.N., O.S., D.K. and F.R..; visualization, L.D., Sh.Zh., D.K., F.N., O.S., F.R., and D.A; supervision, A.M., L.D. and Sh.Zh. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Committee of Science of the Ministry of Science and Higher Education of the Republic of Kazakhstan “Improving the outcomes of surgical myocardial revascularization based on the development of comprehensive innovative management of pa-tients after intervention”, grant number “IRN AR19680319”.
Institutional Review Board Statement
The study was conducted in accordance with the Declara-tion of Helsinki, and approved by the Local Ethics Committee of Asfendiyarov Kazakh national medical university, Almaty, Republic of Kazakhstan (protocol code 11(134), date of approval 04.11.2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
The authors would like to thank the JSC "Research Institute of Cardiology and Internal Medicine", Almaty, Republic of Kazakhstan, for support and assistance in initiating the study: Roza Kuanyshbekova, Marat Pashimov, Rustem Tuleutaev and a group of researchers who presented patient data: Asem Amantayeva, Madina Nurzhanova, Dania Sen-kibayeva, Irina Vorontsova, Gulnara Ospanova, Natalia Gordina, Talshyn Kalioldaeva, Әygerim Nagimatullaeva, Elvira Rakhmetulaeva, Zhanar Nurbay, and independent professor Dmitriy Polyakov.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ACS | Acute coronary syndrome |
| ASCVD | Atherosclerotic cardiovascular disease |
| BMI | Body mass index |
| CA | Circumflex artery |
| CABG | Coronary artery bypass grafting |
| CHD | Coronary heart disease |
| CHF | Congestive heart failure |
| CRP | C-reactive protein |
| CVDs | Cardiovascular diseases |
| DB | Diagonal branch |
| DBP | Diastolic blood pressure |
| EDD | End-diastolic dimension |
| EDV | End-diastolic volume |
| EF | Election fravtion |
| ESD | End-systolic dimension |
| ESV | End-systolic volume |
| GFR | Glomerular filtration rate |
| HRPR | High residual platelet reactivity |
| IA | Intermediate artery |
| IHD | Ischemic heart disease |
| IVS | Intraventricular septum |
| LA | Left atrium |
| LAD | Left anterior descending |
| LCA | Left coronary artery |
| LD | Linear dichroism |
| LDL-C | Low-density lipoprotein cholesterol |
| LV | Left ventricular |
| LVPW | Left ventricular posterior wall |
| МАСЕ | Major Adverse Cardiovascular Events |
| OMB | Obtuse marginal branch |
| PIVB | Posterior interventricular branch |
| RCA | Right coronary artery |
| RPR | Residual platelet reactivity |
| RV | Right ventricular |
| SBP | Systolic blood pressure |
| sPAP | Systolic pulmonary artery pressure |
| SV | Stroke volume |
| TG | Tryglicerides |
| MV | Mitral Valve |
| TV | Tricuspid Valve |
| AV | Aortic Valve |
| AH | Arterial Hypertension |
| TSH | thyroid-stimulating hormone |
| USD BCA | Ultrasound of Brachiocephalic Arteries |
References
- Mangiacapra, F., De Bruyne, B., Muller, O., Trana, C., Ntalianis, A., Bartunek, J., Heyndrickx, G., Di Sciascio, G., Wijns, W., & Barbato, E. (2010). High residual platelet reactivity after clopidogrel: extent of coronary atherosclerosis and periprocedural myocardial infarction in patients with stable angina undergoing percutaneous coronary intervention. JACC. Cardiovascular interventions, 3(1), 35–40. [CrossRef]
- Liu, L., Gong, B., Wang, W., Xu, K., Wang, K., & Song, G. (2024). Association between haemoglobin, albumin, lymphocytes, and platelets and mortality in patients with heart failure. ESC heart failure, 11(2), 1051–1060. [CrossRef]
- Franchi, F., Rollini, F., & Angiolillo, D. J. (2015). Defining the link between chronic kidney disease, high platelet reactivity, and clinical outcomes in clopidogrel-treated patients undergoing percutaneous coronary intervention. Circulation. Cardiovascular interventions, 8(6), e002760. [CrossRef]
- Gupta, R., Kirtane, A. J., Liu, Y., Crowley, A., Witzenbichler, B., Rinaldi, M. J., Metzger, D. C., Weisz, G., Stuckey, T. D., Brodie, B. R., Mehran, R., Ben-Yehuda, O., & Stone, G. W. (2019). Impact of Smoking on Platelet Reactivity and Clinical Outcomes After Percutaneous Coronary Intervention: Findings From the ADAPT-DES Study. Circulation. Cardiovascular interventions, 12(11), e007982. [CrossRef]
- Ma, Y., Ashraf, M. Z., & Podrez, E. A. (2010). Scavenger receptor BI modulates platelet reactivity and thrombosis in dyslipidemia. Blood, 116(11), 1932–1941. [CrossRef]
- Chirumamilla, A. P., Maehara, A., Mintz, G. S., Mehran, R., Kanwal, S., Weisz, G., Hassanin, A., Hakim, D., Guo, N., Baber, U., Pyo, R., Moses, J. W., Fahy, M., Kovacic, J. C., & Dangas, G. D. (2012). High platelet reactivity on clopidogrel therapy correlates with increased coronary atherosclerosis and calcification: a volumetric intravascular ultrasound study. JACC. Cardiovascular imaging, 5(5), 540–549. [CrossRef]
- Toma, C., Zahr, F., Moguilanski, D., Grate, S., Semaan, R. W., Lemieux, N., Lee, J. S., Cortese-Hassett, A., Mulukutla, S., Rao, S. V., & Marroquin, O. C. (2012). Impact of anemia on platelet response to clopidogrel in patients undergoing percutaneous coronary stenting. The American journal of cardiology, 109(8), 1148–1153. [CrossRef]
- Li, Q., Chen, Y., Liu, Y., Yu, L., Zheng, J., & Sun, Y. (2021). Impact of renal function on residual platelet reactivity and clinical outcomes in patients with acute coronary syndrome treated with clopidogrel. Clinical cardiology, 44(6), 789–796. [CrossRef]
- Dracoulakis, M. D. A., Gurbel, P., Cattaneo, M., Martins, H. S., Nicolau, J. C., & Kalil Filho, R. (2019). High Residual Platelet Reactivity during Aspirin Therapy in Patients with Non-St Segment Elevation Acute Coronary Syndrome: Comparison Between Initial and Late Phases. Arquivos brasileiros de cardiologia, 113(3), 357–363. [CrossRef]
- Lee, S., Eichelberger, B., Kopp, C. W., Panzer, S., & Gremmel, T. (2021). Residual platelet reactivity in low-dose aspirin-treated patients with class 1 obesity. Vascular pharmacology, 136, 106819. [CrossRef]
- Hertfelder, H. J., Bös, M., Weber, D., Winkler, K., Hanfland, P., & Preusse, C. J. (2005). Perioperative monitoring of primary and secondary hemostasis in coronary artery bypass grafting. Seminars in thrombosis and hemostasis, 31(4), 426–440. [CrossRef]
- Jiabing Wang, Xingliang Shi, Liuqing Chen, Ting Li, Chenttao Wu, and Mingwu Hu. Platelet Reactivity with MACE in Acute Coronary Syndrome Patients Post-PCI under Dual Antiplatelet Therapy: A Meta-Analysis. British Journal of Hospital Medicine 2024 85:10, 1-17. [CrossRef]
- Nurmukhammad, F.N., Zhangelova, Sh.B., Кapsultanova, D.A., Musagaliyeva, A.T., Danyarova, L.B., Rustamova, F.E,, Sugraliyev, A.B., Ospanova, G.E. Non-statin therapy in patients with elevated LDL-C and high platelet reactivity: a narrative review. Med J Malaysia. 2025 Mar;80(2):258-265. PMID: 40145170.
- Snoep, J. D., Roest, M., Barendrecht, A. D., De Groot, P. G., Rosendaal, F. R., & Van Der Bom, J. G. (2010). High platelet reactivity is associated with myocardial infarction in premenopausal women: a population-based case-control study. Journal of thrombosis and haemostasis : JTH, 8(5), 906–913. [CrossRef]
- Franchi, F., Rollini, F., & Angiolillo, D. J. (2015). Defining the link between chronic kidney disease, high platelet reactivity, and clinical outcomes in clopidogrel-treated patients undergoing percutaneous coronary intervention. Circulation. Cardiovascular interventions, 8(6), e002760. [CrossRef]
- François Mach, Konstantinos C Koskinas, Jeanine E Roeters van Lennep, Lale Tokgözoğlu, Lina Badimon, Colin Baigent, Marianne Benn, Christoph J Binder, Alberico L Catapano, Guy G De Backer, Victoria Delgado, Natalia Fabin, Brian A Ference, Ian M Graham, Ulf Landmesser, Ulrich Laufs, Borislava Mihaylova, Børge Grønne Nordestgaard, Dimitrios J Richter, Marc S Sabatine, ESC/EAS Scientific Document Group , 2025 Focused Update of the 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Developed by the task force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS), European Heart Journal, 2025; ehaf190. [CrossRef]
Figure 1.
The flow chart of patients.
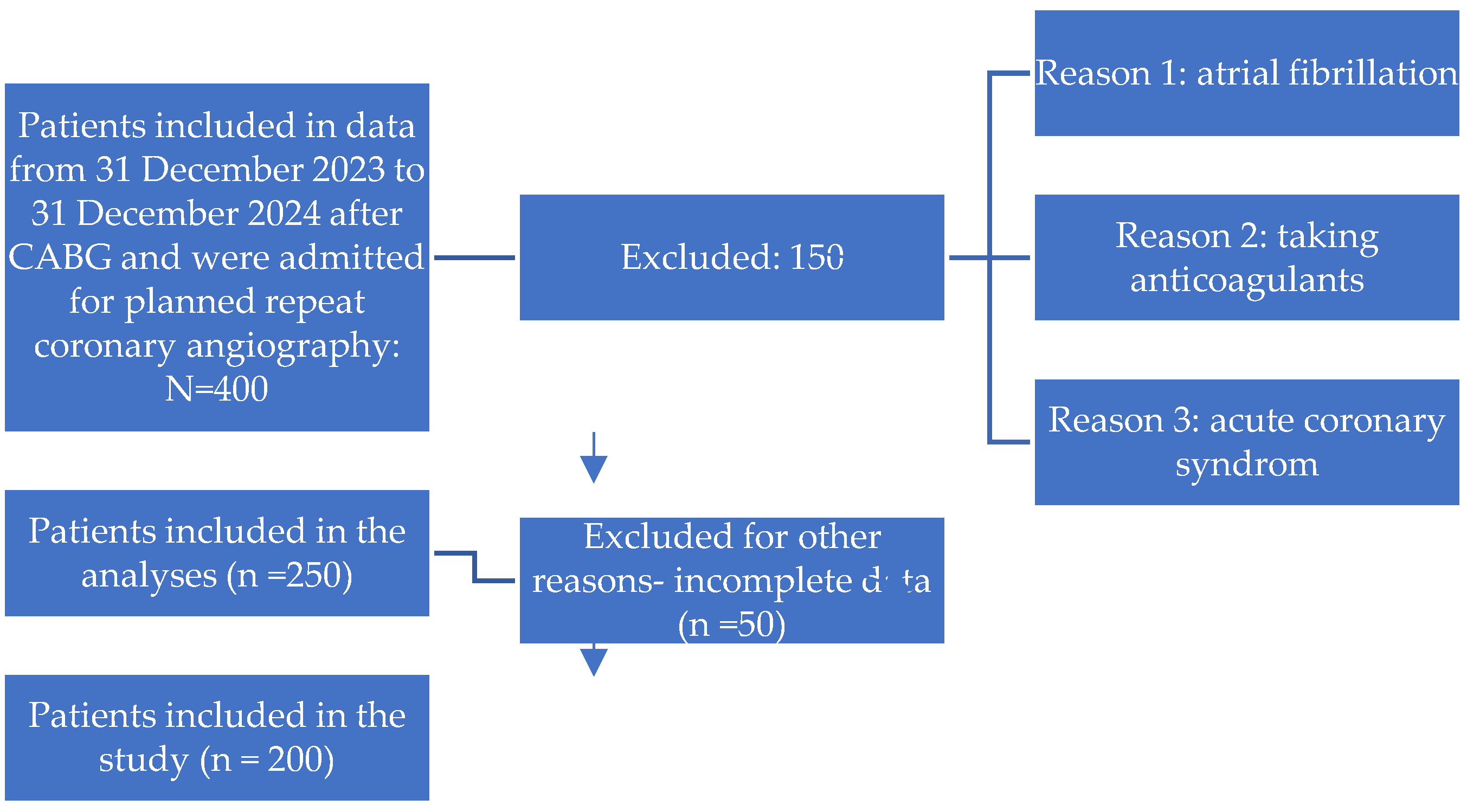

Table 1.
Descriptive statistics of the group without re-stenting and with re-stenting.
| Without re-stenting |
With re-stenting |
p-value | N | |
|---|---|---|---|---|
| N=59 | N=136 | |||
| Age | 66.0 [61.5;73.0] | 71.0 [65.8;75.0] | 0.016 | 195 |
| Gender: | 0.431 | 195 | ||
| female | 13 (22.0%) | 39 (28.7%) | ||
| male | 46 (78.0%) | 97 (71.3%) | ||
| Smoking: | 0.001 | 195 | ||
| No | 27 (45.8%) | 97 (71.3%) | ||
| Yes | 32 (54.2%) | 39 (28.7%) | ||
| Alcohol: | 0.164 | 195 | ||
| No | 56 (94.9%) | 134 (98.5%) | ||
| Yes | 3 (5.08%) | 2 (1.47%) | ||
| Weight | 79.0 [70.0;86.5] | 78.5 [70.0;85.8] | 0.903 | 195 |
| Height | 170 [164;174] | 168 [162;173] | 0.438 | 195 |
| BMI | 27.3 [24.9;29.4] | 27.6 [25.0;30.2] | 0.411 | 195 |
| Heredity: | 0.874 | 195 | ||
| No | 37 (62.7%) | 82 (60.3%) | ||
| Yes | 22 (37.3%) | 54 (39.7%) | ||
| Dyspnea: | 0.776 | 194 | ||
| No | 5 (8.47%) | 10 (7.41%) | ||
| Yes | 54 (91.5%) | 125 (92.6%) | ||
| Edema: | 0.190 | 195 | ||
| No | 55 (93.2%) | 116 (85.3%) | ||
| Yes | 4 (6.78%) | 20 (14.7%) | ||
| Pain: | 0.726 | 195 | ||
| No | 2 (3.39%) | 7 (5.15%) | ||
| Yes | 57 (96.6%) ? | 129 (94.9%) | ||
| Weakness: | 0.104 | 195 | ||
| No | 0 (0.00%) | 7 (5.15%) | ||
| Yes | 59 (100%) | 129 (94.9%) | ||
| Heartbeat: | 0.451 | 195 | ||
| No | 53 (89.8%) | 115 (84.6%) | ||
| Yes | 6 (10.2%) | 21 (15.4%) | ||
| Short of breath: | 0.961 | 195 | ||
| No | 43 (72.9%) | 97 (71.3%) | ||
| Yes | 16 (27.1%) | 39 (28.7%) | ||
| SBP | 120 [110;130] | 130 [120;140] | 0.041 | 195 |
| DBP | 80.0 [70.0;80.0] | 80.0 [70.0;80.0] | 0.201 | 195 |
| History of myocardial infarction: | 0.145 | 195 | ||
| No | 33 (55.9%) | 59 (43.4%) | ||
| Yes | 26 (44.1%) | 77 (56.6%) | ||
| АH: | 0.133 | 195 | ||
| No | 5 (8.47%) | 4 (2.94%) | ||
| Yes | 54 (91.5%) | 132 (97.1%) | ||
| DM type 2: | 0.603 | 195 | ||
| No | 42 (71.2%) | 90 (66.2%) | ||
| Yes | 17 (28.8%) | 46 (33.8%) | ||
| History of Stroke: | 0.400 | 195 | ||
| No | 56 (94.9%) | 123 (90.4%) | ||
| Yes | 3 (5.08%) | 13 (9.56%) | ||
| CKD: | 0.068 | 195 | ||
| No | 39 (66.1%) | 69 (50.7%) | ||
| Yes | 20 (33.9%) | 67 (49.3%) | ||
| Stenting: | 0.712 | 195 | ||
| No | 47 (79.7%) | 113 (83.1%) | ||
| Yes | 12 (20.3%) | 23 (16.9%) | ||
| CABG: | 0.003 | 195 | ||
| No | 10 (16.9%) | 5 (3.68%) | ||
| Yes | 49 (83.1%) | 131 (96.3%) | ||
| IHD, duration | 3.00 [1.00;6.50] | 2.50 [1.00;10.0] | 0.364 | 195 |
| Hemoglobin | 142 [132;154] | 145 [135;155] | 0.542 | 195 |
| СRP | 2.00 [1.24;3.56] | 2.45 [1.03;4.22] | 0.487 | 195 |
| Glucose | 5.54 [5.12;6.30] | 5.80 [5.16;6.93] | 0.293 | 195 |
| HbA1c | 6.01 [5.30;6.70] | 6.05 [5.40;7.33] | 0.403 | 195 |
| Creatinine | 80.4 [70.6;90.2] | 79.0 [70.8;92.2] | 0.952 | 195 |
| GFR | 88.0 [75.8;96.0] | 81.0 [69.8;94.2] | 0.279 | 195 |
| Potassium | 4.40 [4.20;4.60] | 4.30 [4.10;4.60] | 0.590 | 195 |
| Sodium | 142 [140;144] | 142 [141;144] | 0.268 | 195 |
| ALT | 19.0 [14.1;28.5] | 18.1 [12.9;25.7] | 0.453 | 195 |
| AST | 17.3 [13.8;25.9] | 17.9 [14.9;23.1] | 0.977 | 195 |
| TC | 4.24 [3.41;5.25] | 4.50 [3.70;5.22] | 0.419 | 195 |
| LDL | 2.58 [2.00;3.17] | 2.42 [2.00;3.20] | 0.569 | 195 |
| HDL | 1.00 [0.99;1.00] | 1.00 [0.96;1.03] | 0.809 | 195 |
| ТG | 1.50 [1.00;1.98] | 1.29 [1.00;1.75] | 0.083 | 195 |
| Troponin I | 20.0 [13.4;95.4] | 14.3 [10.3;32.8] | 0.002 | 195 |
| TSH | 2.00 [1.47;2.90] | 2.00 [1.39;3.15] | 0.773 | 195 |
| Thyroxine | 14.1 [12.0;16.0] | 14.0 [11.6;16.2] | 0.945 | 193 |
| PTI | 94.9 [80.3;103] | 95.8 [77.5;105] | 0.627 | 195 |
| INR | 1.07 [1.04;1.17] | 1.04 [0.99;1.14] | 0.039 | 195 |
| APTT | 31.1 [28.8;36.5] | 31.6 [28.7;35.7] | 0.737 | 195 |
| EDV | 162 [129;206] | 136 [113;179] | 0.038 | 195 |
| ESV | 80.0 [45.5;116] | 61.5 [45.8;95.2] | 0.222 | 195 |
| SV | 78.0 [69.5;87.5] | 77.5 [59.8;92.2] | 0.466 | 195 |
| sPAP | 32.0 [23.0;44.0] | 35.0 [24.5;42.0] | 0.917 | 194 |
| EF | 47.0 [41.5;59.0] | 52.0 [44.0;59.2] | 0.235 | 195 |
| LA | 3.80 [3.60;4.55] | 3.90 [3.50;4.40] | 0.638 | 195 |
| EDD | 5.70 [5.20;6.30] | 5.30 [4.97;6.00] | 0.081 | 195 |
| ESD | 4.20 [3.35;4.90] | 3.80 [3.30;4.60] | 0.240 | 195 |
| LVPW | 1.05 [0.90;1.20] | 1.10 [1.00;1.20] | 0.030 | 195 |
| IVS | 1.10 [0.95;1.27] | 1.10 [1.00;1.30] | 0.924 | 195 |
| МV: | 0.858 | 195 | ||
| No | 4 (6.78%) | 13 (9.56%) | ||
| 1 degree. | 36 (61.0%) | 75 (55.1%) | ||
| 2 degree. | 13 (22.0%) | 36 (26.5%) | ||
| 3 degree. | 6 (10.2%) | 11 (8.09%) | ||
| 4 degree. | 0 (0.00%) | 1 (0.74%) | ||
| ТV: | 0.437 | 195 | ||
| No | 9 (15.3%) | 22 (16.2%) | ||
| 1 degree. | 32 (54.2%) | 67 (49.3%) | ||
| 2 degree. | 16 (27.1%) | 46 (33.8%) | ||
| 3 degree. | 2 (3.39%) | 1 (0.74%) | ||
| AV: | 0.309 | 195 | ||
| No | 30 (50.8%) | 71 (52.2%) | ||
| 1 degree. | 22 (37.3%) | 49 (36.0%) | ||
| 2 degree. | 5 (8.47%) | 15 (11.0%) | ||
| 3 degree. | 0 (0.00%) | 1 (0.74%) | ||
| Stenosis | 2 (3.39%) | 0 (0.00%) | ||
| RV | 3.00 [2.80;3.40] | 3.10 [2.90;3.40] | 0.566 | 195 |
| LV aneurysm: | 0.990 | 195 | ||
| No | 50 (84.7%) | 117 (86.0%) | ||
| Yes | 9 (15.3%) | 19 (14.0%) | ||
| Heart Rate | 75.0 [66.0;82.0] | 71.5 [65.0;83.2] | 0.496 | 195 |
| USD of BCA: | 1.000 | 195 | ||
| No | 24 (40.7%) | 56 (41.2%) | ||
| Yes | 35 (59.3%) | 80 (58.8%) | ||
| RCA, degree: | 0.117 | 195 | ||
| minor | 44 (74.6%) | 84 (61.8%) | ||
| significant | 15 (25.4%) | 52 (38.2%) | ||
| LAD, degree: | 0.002 | 195 | ||
| Minor | 43 (72.9%) | 64 (47.1%) | ||
| Significant | 16 (27.1%) | 72 (52.9%) | ||
| LCA, degree: | 0.235 | 195 | ||
| Minor | 55 (93.2%) | 117 (86.0%) | ||
| Significant | 4 (6.78%) | 19 (14.0%) | ||
| CА, degree: | 0.002 | 195 | ||
| Minor | 51 (86.4%) | 85 (62.5%) | ||
| significant | 8 (13.6%) | 51 (37.5%) | ||
| DB, degree: | 0.001 | 195 | ||
| Minor | 54 (91.5%) | 94 (69.1%) | ||
| significant | 5 (8.47%) | 42 (30.9%) | ||
| PIVB, degree: | 0.006 | 195 | ||
| Minor | 58 (98.3%) | 113 (83.1%) | ||
| Significant | 1 (1.69%) | 23 (16.9%) | ||
| IА, degree: | 0.369 | 195 | ||
| Minor | 56 (94.9%) | 133 (97.8%) | ||
| significant | 3 (5.08%) | 3 (2.21%) | ||
| OMB, degree: | 0.002 | 195 | ||
| Minor | 56 (94.9%) | 102 (75.0%) | ||
| Significant | 3 (5.08%) | 34 (25.0%) | ||
| Number of shunts | 2.00 [2.00;3.00] | 3.00 [2.00;3.00] | <0.001 | 195 |
| Number of affected vessels | 3.00 [2.00;3.00] | 4.00 [3.75;5.00] | <0.001 | 195 |
| Statins: Yes | 59 (100%) | 136 (100%) | . | 195 |
| Ezetimibe: | <0.001 | 195 | ||
| No | 59 (100%) | 89 (65.4%) | ||
| Yes | 0 (0.00%) | 47 (34.6%) | ||
| Angina after CABG: | <0.001 | 195 | ||
| No | 7 (11.9%) | 0 (0.00%) | ||
| Yes | 52 (88.1%) | 136 (100%) | ||
| Mortality after CABG: | 1.000 | 195 | ||
| No | 58 (98.3%) | 132 (97.1%) | ||
| Yes | 1 (1.69%) | 4 (2.94%) | ||
| Stenting after CABG: | <0.001 | 195 | ||
| No | 59 (100%) | 0 (0.00%) | ||
| Yes | 0 (0.00%) | 136 (100%) | ||
| PRU | 145 [140;155] | 230 [200;274] | <0.001 | 195 |
| Dyslipidemia: | 1.000 | 195 | ||
| No | 2 (3.39%) | 4 (2.94%) | ||
| Yes | 57 (96.6%) | 132 (97.1%) | ||
| Anemia: | 0.941 | 195 | ||
| No | 52 (88.1%) | 122 (89.7%) | ||
| Yes | 7 (11.9%) | 14 (10.3%) | ||
| CKD: | 0.977 | 195 | ||
| No | 53 (89.8%) | 124 (91.2%) | ||
| Yes | 6 (10.2%) | 12 (8.82%) | ||
| Obesity: | 0.406 | 195 | ||
| No | 17 (28.8%) | 30 (22.1%) | ||
| Yes | 42 (71.2%) | 106 (77.9%) | ||
| RPR: | <0.001 | 195 | ||
| Therapeutic window | 59 (100%) | 46 (33.8%) | ||
| HRPR | 0 (0.00%) | 90 (66.2%) |
Table 2.
Descriptive statistics of the Therapeutic window/HRPR group.
| Therapeutic window | HRPR | p-value | N | |
|---|---|---|---|---|
| N=105 | N=90 | |||
| Age | 69.0 [62.0;74.0] | 70.5 [65.2;75.0] | 0.147 | 195 |
| Gender: | 0.871 | 195 | ||
| female | 29 (27.6%) | 23 (25.6%) | ||
| male | 76 (72.4%) | 67 (74.4%) | ||
| Smoking: | 0.030 | 195 | ||
| No | 59 (56.2%) | 65 (72.2%) | ||
| Yes | 46 (43.8%) | 25 (27.8%) | ||
| Alcohol: | 1.000 | 195 | ||
| No | 102 (97.1%) | 88 (97.8%) | ||
| Yes | 3 (2.86%) | 2 (2.22%) | ||
| Weight | 78.0 [69.0;85.0] | 80.0 [70.2;88.0] | 0.199 | 195 |
| Height | 168 [163;174] | 170 [162;173] | 0.838 | 195 |
| BMI | 27.2 [25.0;29.4] | 28.1 [25.9;30.6] | 0.096 | 195 |
| Heredity: | 0.475 | 195 | ||
| No | 67 (63.8%) | 52 (57.8%) | ||
| Yes | 38 (36.2%) | 38 (42.2%) | ||
| Dyspnea: | 0.739 | 194 | ||
| No | 7 (6.67%) | 8 (8.99%) | ||
| Yes | 98 (93.3%) | 81 (91.0%) | ||
| Edema: | 0.801 | 195 | ||
| No | 91 (86.7%) | 80 (88.9%) | ||
| Yes | 14 (13.3%) | 10 (11.1%) | ||
| Pain: | 0.510 | 195 | ||
| No | 6 (5.71%) | 3 (3.33%) | ||
| Yes | 99 (94.3%) | 87 (96.7%) | ||
| Weakness: | 0.252 | 195 | ||
| No | 2 (1.90%) | 5 (5.56%) | ||
| Yes | 103 (98.1%) | 85 (94.4%) | ||
| Heartbeat: | 1.000 | 195 | ||
| No | 90 (85.7%) | 78 (86.7%) | ||
| Yes | 15 (14.3%) | 12 (13.3%) | ||
| Short of breath: | 0.778 | 195 | ||
| No | 74 (70.5%) | 66 (73.3%) | ||
| Yes | 31 (29.5%) | 24 (26.7%) | ||
| SBP | 120 [115;130] | 130 [120;140] | 0.031 | 195 |
| DBP | 80.0 [70.0;80.0] | 80.0 [70.0;80.0] | 0.320 | 195 |
| History of myocardial infarction: | 0.394 | 195 | ||
| No | 53 (50.5%) | 39 (43.3%) | ||
| Yes | 52 (49.5%) | 51 (56.7%) | ||
| АH: | 0.510 | 195 | ||
| No | 6 (5.71%) | 3 (3.33%) | ||
| Yes | 99 (94.3%) | 87 (96.7%) | ||
| DM type 2: | 0.293 | 195 | ||
| No | 75 (71.4%) | 57 (63.3%) | ||
| Yes | 30 (28.6%) | 33 (36.7%) | ||
| History of Stroke: | 0.031 | 195 | ||
| No | 101 (96.2%) | 78 (86.7%) | ||
| Yes | 4 (3.81%) | 12 (13.3%) | ||
| CKD: | 0.697 | 195 | ||
| No | 60 (57.1%) | 48 (53.3%) | ||
| Yes | 45 (42.9%) | 42 (46.7%) | ||
| Stenting: | 0.897 | 195 | ||
| No | 87 (82.9%) | 73 (81.1%) | ||
| Yes | 18 (17.1%) | 17 (18.9%) | ||
| CABG: | 0.065 | 195 | ||
| No | 12 (11.4%) | 3 (3.33%) | ||
| Yes | 93 (88.6%) | 87 (96.7%) | ||
| IHD, duration | 2.00 [1.00;8.00] | 3.00 [1.00;9.75] | 0.888 | 195 |
| Hemoglobin | 142 [132;154] | 150 [136;156] | 0.053 | 195 |
| СRP | 2.36 [1.27;4.10] | 2.29 [1.02;4.13] | 0.853 | 195 |
| Glucose | 5.54 [5.00;6.20] | 5.90 [5.23;7.10] | 0.022 | 195 |
| HbA1c | 6.01 [5.38;6.70] | 6.06 [5.52;7.83] | 0.282 | 195 |
| Creatinine | 80.0 [71.0;91.8] | 79.0 [70.3;92.7] | 0.890 | 195 |
| GFR | 87.0 [74.0;96.0] | 81.0 [70.0;92.5] | 0.361 | 195 |
| Potassium | 4.30 [4.10;4.50] | 4.35 [4.10;4.60] | 0.267 | 195 |
| Sodium | 142 [141;144] | 142 [140;144] | 0.931 | 195 |
| ALT | 18.0 [12.0;27.5] | 19.0 [14.0;26.4] | 0.473 | 195 |
| AST | 17.6 [13.8;25.8] | 17.7 [15.0;22.7] | 0.934 | 195 |
| TC | 4.30 [3.67;5.27] | 4.50 [3.63;5.20] | 0.571 | 195 |
| LDL | 2.43 [2.00;3.10] | 2.64 [2.00;3.39] | 0.546 | 195 |
| HDL | 1.00 [0.98;1.01] | 1.00 [0.96;1.04] | 0.684 | 195 |
| ТG | 1.37 [1.00;1.80] | 1.38 [1.00;1.79] | 0.981 | 195 |
| Troponin I | 15.0 [11.0;58.7] | 15.0 [11.0;40.0] | 0.635 | 195 |
| TSH | 2.00 [1.60;3.00] | 1.96 [1.25;3.18] | 0.517 | 195 |
| Thyroxine | 13.9 [11.5;16.2] | 14.7 [12.3;16.3] | 0.335 | 193 |
| PTI | 94.5 [80.0;103] | 96.3 [78.5;106] | 0.209 | 195 |
| INR | 1.06 [1.01;1.16] | 1.04 [1.00;1.15] | 0.189 | 195 |
| APTT | 31.4 [29.0;35.9] | 31.4 [28.6;36.0] | 0.524 | 195 |
| EDV | 157 [119;194] | 131 [113;174] | 0.053 | 195 |
| ESV | 72.0 [44.0;108] | 60.0 [46.0;91.2] | 0.256 | 195 |
| SV | 78.0 [65.0;91.0] | 77.0 [59.0;90.0] | 0.268 | 195 |
| sPAP | 34.0 [23.8;44.0] | 35.0 [20.8;40.8] | 0.624 | 194 |
| EF | 49.0 [41.0;60.0] | 51.7 [45.0;58.9] | 0.459 | 195 |
| LA | 3.80 [3.50;4.40] | 3.80 [3.60;4.40] | 0.907 | 195 |
| EDD | 5.60 [5.10;6.20] | 5.20 [4.90;5.90] | 0.043 | 195 |
| ESD | 4.00 [3.30;4.80] | 3.74 [3.40;4.38] | 0.394 | 195 |
| LVPW | 1.10 [0.90;1.20] | 1.10 [1.00;1.20] | 0.087 | 195 |
| IVS | 1.10 [1.00;1.30] | 1.10 [0.90;1.30] | 0.366 | 195 |
| МV: | 0.291 | 195 | ||
| No | 7 (6.67%) | 10 (11.1%) | ||
| 1 degree. | 62 (59.0%) | 49 (54.4%) | ||
| 2 degree. | 24 (22.9%) | 25 (27.8%) | ||
| 3 degree. | 12 (11.4%) | 5 (5.56%) | ||
| 4 degree. | 0 (0.00%) | 1 (1.11%) | ||
| ТV: | 0.717 | 195 | ||
| No | 14 (13.3%) | 17 (18.9%) | ||
| 1 degree. | 55 (52.4%) | 44 (48.9%) | ||
| 2 degree. | 34 (32.4%) | 28 (31.1%) | ||
| 3 degree. | 2 (1.90%) | 1 (1.11%) | ||
| AV: | 0.070 | 195 | ||
| No | 51 (48.6%) | 50 (55.6%) | ||
| 1 degree. | 44 (41.9%) | 27 (30.0%) | ||
| 2 degree. | 7 (6.67%) | 13 (14.4%) | ||
| 3 degree. | 1 (0.95%) | 0 (0.00%) | ||
| Stenosis | 2 (1.90%) | 0 (0.00%) | ||
| RV | 3.00 [2.90;3.40] | 3.10 [2.90;3.30] | 0.893 | 195 |
| LV aneurysm: | 0.862 | 195 | ||
| No | 89 (84.8%) | 78 (86.7%) | ||
| Yes | 16 (15.2%) | 12 (13.3%) | ||
| Heart Rate | 74.0 [66.0;83.0] | 70.5 [65.0;82.0] | 0.483 | 195 |
| USD of BCA: | 0.196 | 195 | ||
| No | 48 (45.7%) | 32 (35.6%) | ||
| Yes | 57 (54.3%) | 58 (64.4%) | ||
| RCA, degree: | 0.022 | 195 | ||
| minor | 77 (73.3%) | 51 (56.7%) | ||
| significant | 28 (26.7%) | 39 (43.3%) | ||
| LAD, degree: | 0.002 | 195 | ||
| Minor | 69 (65.7%) | 38 (42.2%) | ||
| Significant | 36 (34.3%) | 52 (57.8%) | ||
| LCA, degree: | 0.694 | 195 | ||
| Minor | 94 (89.5%) | 78 (86.7%) | ||
| Significant | 11 (10.5%) | 12 (13.3%) | ||
| CА, degree: | 0.001 | 195 | ||
| Minor | 84 (80.0%) | 52 (57.8%) | ||
| significant | 21 (20.0%) | 38 (42.2%) | ||
| DB, degree: | 0.003 | 195 | ||
| Minor | 89 (84.8%) | 59 (65.6%) | ||
| significant | 16 (15.2%) | 31 (34.4%) | ||
| PIVB, degree: | 0.001 | 195 | ||
| Minor | 100 (95.2%) | 71 (78.9%) | ||
| Significant | 5 (4.76%) | 19 (21.1%) | ||
| IА, degree: | 0.688 | 195 | ||
| Minor | 101 (96.2%) | 88 (97.8%) | ||
| significant | 4 (3.81%) | 2 (2.22%) | ||
| OMB, degree: | <0.001 | 195 | ||
| Minor | 98 (93.3%) | 60 (66.7%) | ||
| Significant | 7 (6.67%) | 30 (33.3%) | ||
| Number of shunts | 2.00 [2.00;3.00] | 3.00 [2.00;4.00] | 0.001 | 195 |
| Number of affected vessels | 3.00 [2.00;3.00] | 4.00 [4.00;5.00] | <0.001 | 195 |
| Statins: Yes | 105 (100%) | 90 (100%) | . | 195 |
| Ezetimibe: | <0.001 | 195 | ||
| No | 101 (96.2%) | 47 (52.2%) | ||
| Yes | 4 (3.81%) | 43 (47.8%) | ||
| Angina after CABG: | 0.016 | 195 | ||
| No | 7 (6.67%) | 0 (0.00%) | ||
| Yes | 98 (93.3%) | 90 (100%) | ||
| Mortality after CABG: | 0.183 | 195 | ||
| No | 104 (99.0%) | 86 (95.6%) | ||
| Yes | 1 (0.95%) | 4 (4.44%) | ||
| Stenting after CABG: | <0.001 | 195 | ||
| No | 59 (56.2%) | 0 (0.00%) | ||
| Yes | 46 (43.8%) |
90 (100%) !!! |
||
| PRU | 170 [141;200] | 255 [230;280] | <0.001 | 195 |
| Dyslipidemia: | 0.688 | 195 | ||
| No | 4 (3.81%) | 2 (2.22%) | ||
| Yes | 101 (96.2%) | 88 (97.8%) | ||
| Anemia: | 0.310 | 195 | ||
| No | 91 (86.7%) | 83 (92.2%) | ||
| Yes | 14 (13.3%) | 7 (7.78%) | ||
| CKD: | 0.689 | 195 | ||
| No | 94 (89.5%) | 83 (92.2%) | ||
| Yes | 11 (10.5%) | 7 (7.78%) | ||
| Obesity: | 0.462 | 195 | ||
| No | 28 (26.7%) | 19 (21.1%) | ||
| Yes | 77 (73.3%) | 71 (78.9%) | ||
| RPR: | <0.001 | 195 | ||
| Therapeutic window | 105 (100%) | 0 (0.00%) | ||
| HRPR | 0 (0.00%) | 90 (100%) |
Table 3.
Stepwise logistic regression: predictors associated with the risk of developing stenting after CABG.
Table 3.
Stepwise logistic regression: predictors associated with the risk of developing stenting after CABG.
| HRPR | |||
|---|---|---|---|
| Predictors | Odds Ratios | CI | p |
| Number of affected vessels | 52.67 | 17.33 – 213.77 | <0.001 |
| ТSH | 0.87 | 0.72 – 1.00 | 0.116 |
| Ezetimibe: Yes | 0.12 | 0.02 – 0.75 | 0.023 |
| Potassium | 2.53 | 0.78 – 8.59 | 0.127 |
| Hb A 1 c | 1.18 | 0.95 – 1.46 | 0.138 |
| Observations | 195 | ||
| R2 Tjur | 0.681 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



