
Submitted:
26 September 2025
Posted:
30 September 2025
You are already at the latest version
Abstract
Radical drug therapy for schizophrenia is usually hard to achieve with one currently available antipsychotic agent. Indeed, it is the negative symptoms of this morbidity that are a dilemma to neutralize. Most of the first-generation agents can deal with the positive symptoms of the disease to a convincing degree, but not with its negative symptoms. The creation of so-called second-generation agents aimed to treat the negative symptoms, as these invisible barriers are the real reasons that isolate psychotic individuals and hinder their integration into society. Unfortunately, these newly designed drugs turned out to induce different categories of undesired effects; the most embarrassing of which is the metabolic drawbacks, such as insulin resistance, weight gain, and other subcategories of metabolic consequences. In this work, we discuss the reasons behind these undesired metabolic effects, how to deal with these, and how to choose the proper agent for each psychotic case separately. The choice of antipsychotics should be tailored separately for each case, as each patient responds variably to each neuroleptic.
Keywords:
intoxication
; weight gain
; insulin resistance
; free radicals
; mitochondrial dysfunction
; drug interactions
Introduction:
Psychosis, depression, and anxiety neurosis disorders are the three main classes of mental diseases that can affect humans. Schizophrenia is the major subclass of psychosis. Depression, both major depressive disorder and bipolar disorders, is another major subclass of mental diseases, and their incidence in different societies around the globe is higher than that of psychosis. Anxiety and insomnia are the third subclass of neuropsychiatric ailments that psychiatrists/neurologists can face in their clinics to provide help. According to available statistical data, more than 1/3 of individuals in any society at some point in their lives manifest clinical criteria sufficient for one or another form of psychiatric condition to be settled [1] . In the United States, about 46% of the population at some point qualifies for a mental illness diagnosis [2] .
Among the relatively newly designed antipsychotic agents is olanzapine (OLZ), which we are going to tackle in this work. In addition to its major therapeutic use as an antipsychotic, OLZ has other uses that we will mention briefly.
Antipsychotics and classification:
As the name indicates, an antipsychotic agent (also known as a neuroleptic) is a class of medications that is primarily used to treat schizophrenia. Antipsychotics, together or as an adjunct to mood stabilizers, are also used in the management of bipolar disorders. Dependent on the dose being therapeutically used, they also have many off-label uses, as is the case with quetiapine and OLZ. This major group of psychotropic agents includes many drugs; therefore, it was logical to classify these into 1st and 2nd generation agents. There also exist other classification methods; one can see this in detail in [3]. Because 1st generation agents are nonselective in their action, they cause a wide spectrum of undesired effects, some of which are associated with the drugs themselves, and some result from their interactions with other psychotropics, and many drugs that act on other systems of the body to treat different somatic morbidities that affect humans. Moreover, many 1st generation agents are impotent in their therapeutic actions [4]. Recall that some of the side effects exerted by these agents, dose independently (idiosyncratic), can be catastrophic and cause devastating side effects such as neuroleptic malignant syndrome, serotonin syndrome, blood dyscrasia, myocarditis, and others. All these factors motivated drug industry corporations, via the drug designers (molecular docking), to manufacture more selective and potent agents to deal with the dilemma of psychosis. One has to admit that these firms have made great efforts to create modern medicines that are highly effective therapeutically while having fewer side effects. They recruited their scientists to manufacture what is now known as 2nd generation agents. But, unfortunately, it turned out that these newly prepared agents can also exert the same side effects of 1st generation agents (probably to a lesser extent). Moreover, they also have their own drawbacks, especially of metabolic type, namely insulin resistance and the consequences of this, such as type 2 diabetes, an area in the spectrum of metabolic syndrome.
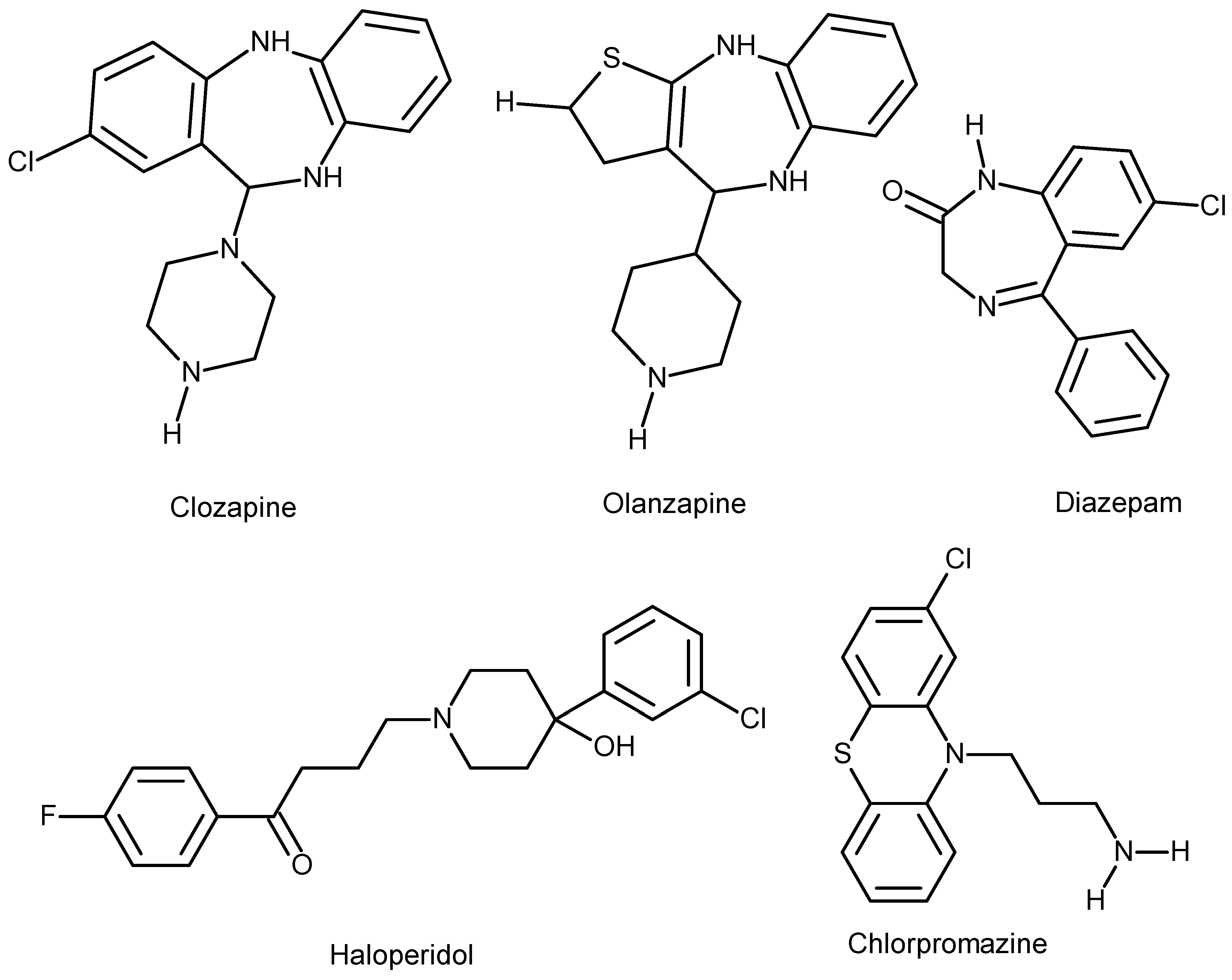
Olanzapine: is a thienobenzodiazepine derivative (water-insoluble), a 2nd generation antipsychotic agent, developed by Eli Lilly in 1971, and patented in the US in 1996. The chemical formula of the agent is C17H20N4S, has a molecular mass of 312.439 g/mole, and the PubChem CID is: 4585. OLZ is well-known under the trade name Zyprexa. It was basically developed to treat schizophrenia and bipolar affective disorders (drugs.com). The agent is administered both orally and parenterally (intramuscular IM), which is attributed to the fact that the drug is practically water-insoluble (see the chemical structure), Figure 1.
Diazepam, Olanzapine, and Clozapine are nearly insoluble in water, slightly soluble in alcohol, acetone, and dichloromethane, and highly soluble in chloroform because they are lipophilic nanoparticles.
Haloperidol is slightly soluble in water, soluble in alcohol, and freely soluble in chloroform.
Chlorpromazine (demonstrated for comparison) is an amphiphilic molecule, meaning it is soluble in both water and organic solvents.
Data from PubChem.
Pharmacopeia of olanzapine:
For oral use (including orally disintegrating tablets): 2.5mg, 7.5mg, 10mg, 15mg, and 20mg tablets are available.
For parenteral use: intramuscular (IM) as short-acting OLZ for the treatment of agitation episodes of acute schizophrenia, is an appropriate choice to start with, and then once the acute psychosis is controlled, one can switch to an oral preparation as maintenance therapy. Long-acting parenteral (IM) maintenance therapy as OLZ pamoate is also available and indicated where circumstances are not against such a procedure, as this is the new trend of deinstitutionalization of patients with chronic mental diseases.
Dedicated uses of olanzapine and the recommended doses:
Schizophrenia:
- 1.
- Initially started at a daily dose of 5-10 mg tablets; if necessary, can be titrated upward with increments of 5 mg/day at intervals of more than a week to reach the maintenance dose of 20mg daily but not more.
- 2.
- Based on oral dose, recommended (IM) doses are as follows:
- A.
- Daily oral dose of 10mg: is equivalent to 210 mg IM dose every 2 weeks, or 405 mg IM every 4 weeks (for 1st 8 weeks), so 150 mg every 2 weeks or 300 mg every 4 weeks.
- B.
- Daily oral dose of 15 mg: is equivalent to 300 mg IM dose (for the 1st 8 weeks) every 2 weeks, then 210mg IM (every 2 weeks) or 405 mg IM (every 4 weeks).
- C.
- Daily oral dose of 20 mg: is equivalent to 300 mg IM (every 2 weeks), for the 1st 8 weeks, if titration is optimal against therapeutic effects, the maintenance dose is 300mg IM (every 2 weeks). The data regarding OLZ doses dedicated to schizophrenia mentioned above is obtained from [5].
Mania of bipolar I disorder:
OLZ is indicated for the treatment of such a condition and also as a maintenance therapy of bipolar I disorder, especially when this is associated with manic or mixed episodes. It is sometimes used as an adjunct to lithium or valproate to treat manic and/or stabilize mixed episodes associated with bipolar I disorder [6].
OLZ is best to be prescribed as a monotherapy, as combination therapy of psychotropics is not recommended because of the possible augmentation of side effect panorama and the avoidance of drug interaction complications. Unfortunately, this practice is not always possible as individual patients respond variably to almost all antipsychotic agents; moreover, to get the desired therapeutic effect, one has to combine other agents.
As a monotherapy: daily oral 10-15 mg tablets to start with, if needed, titrated upward by 5mg daily at intervals of 24 hours.
As an add-on: to lithium or valproate, oral 10mg daily to start with.
As a maintenance therapy: daily 5-20 mg tablets, and this dose must not exceed 20 mg.
Agitation associated with schizophrenia and mania of bipolar I type: Short-acting 2.5-10 mg (IM) to start with and on-demand additional 10 mg (IM) at intervals of 2 hours after the initial dose, and if necessary another 10 mg 4 hours after the 2nd dose. This practice is dependent on the clinical outcomes of the individual case in question.
Depression of Bipolar I disorder: This is indicated as a combination therapy with fluoxetine (not more than 75mg daily), this is usually adjusted at daily doses of 5-12.5mg in the evening.
Off-label uses of olanzapine:
- Eating disorders, generalized anxiety disorder, panic disorder, delusional parasitosis, and post-traumatic stress. The use of OLZ in these disorders has not been evaluated rigorously enough.
- This agent has been used for Tourette syndrome and stuttering [7].
- Attention-deficient hyperactivity, aggressiveness, and repetitive behavior of autism [8].
- Insomnia, the effect is comparable to quetiapine and lurasidone [9]. In some cases, the sedation caused by OLZ impairs the ability of individuals to wake up at a steady, consistent time every day. Long-term studies of the safety of OLZ to treat insomnia are still to be done.
- As an antiemetic in individuals after receiving anticancer agents because of the high risk of vomiting [10]. As one can see, these off-label uses of the agent are an advantage for this drug, although nobody knows exactly how this agent cures all these different morbidities.
Olanzapine in pregnancy and lactation:
Overweight and obesity in pregnant women are risk factors for congenital malformations in their offspring. Results from a comprehensive meta-analysis support this claim. Specifically, women with a baseline body mass index (BMI > 30 kg/m²) are particularly vulnerable to giving birth to offspring with neural tube defects [11]. Olanzapine can complicate this issue because it has the highest placental exposure among atypical antipsychotics [12] and can induce obesity. This is due to its lipid solubility, as it is virtually insoluble in water. It easily crosses the placental barrier, leading to weight gain and increasing the risk of neural tube defects, such as spina bifida, in the offspring of OLZ-treated women [13]. Olanzapine is secreted into breast milk in very small amounts, so breastfeeding can generally be recommended if there are no alternatives to OLZ [14].
Olanzapine in the elderly and adolescents:
This agent (and risperidone) should not be prescribed for the elderly with dementia due to the increased risk of stroke according to UK Committee on the Safety Medicines (CSM). In the US the agent has a warning for increased death risk in elderly individuals. The agent is not recommended for dementia-related psychosis [15]. The elderly are more prone to experience obesity with this agent compared to risperidone or aripiprazole [16] . The agent causes EPS reactions of all categories in the elderly, but dystonia is more commonly seen in young adults.
In adolescents with precautions, OLZ may be indicated for the treatment of schizophrenia, and manic or mixed episodes associated with bipolar I disorder in individuals aged 13-17 years [17]. OLZ and other agents of the 2nd generation antipsychotics, such as risperidone and aripiprazole, are used to treat irritability, hyperactivity, inappropriate speech, social withdrawal, and stereotypy in autism spectrum disorders (ASD). The common side effects of these three agents are excessive sedation, sleepiness, and weight gain. These side effects are unfortunately more encountered with OLZ than the other 2nd generation agents [18] .
Metabolism: After the 1st pass and reaching the liver, OLZ binds to proteins by 90%. Almost 40% of the oral dose of the agent on average is removed by the hepatic 1st pass [19]. Peak plasma time after absorption is 6 hours (oral route), 15-45 minutes (short-acting I.M), and 7 days (extended-release IM). The half-life (t/2) of the agent is about 21-54 hours (for short-acting immediate release preparations and 30 days (for extended-release).
The clearance of OLZ varies according to sex and race. Women have an almost 25% lower clearance rate than men, and Afro-Americans have a clearance rate of 26% higher than Caucasians and Asian (Chinese or Japanese) individuals [20]. The drug is metabolized by the cytochrome P450 (CYP) system mainly via isozyme 1A2 (CYP1A2) and to a lesser degree by the isozyme CYP2D6. Metabolites of OLZ are inactive pharmacologically; they are metabolized by glucuronidation (water-soluble metabolites, after association with glucuronic acid) and thus mainly excreted via the renal route (57%) and to a lesser extent (30%) eliminated via feces. Monitoring of OLZ plasma levels is not reliable, but is sometimes requested to find out the patient’s adherence to the drug therapy [21] .
Side effects of the agent: a rapid check of (drugs.com) and literature [22,23] , one can realize that OLZ might cause any of the all known side effects that a typical (1st generation) and/or atypical (2nd generation) antipsychotic can exhibit, in addition to those of benzodiazepines (diazepam) potentiation. The latterly mentioned is because of the lipophilicity of the agent in other words, it can readily cross cellular biomembranes both cytoplasmic and the membranes of intracellular organelles such as the nucleus and mitochondria. Both agents (OLZ and diazepam) cause sedation, although by different cellular mechanisms. As a chemical structure, the agent resembles benzodiazepines see Figure 1. The major possible effects OLZ can cause include: extrapyramidal symptoms (EPS), neuroleptic malignant syndrome, blood dyscrasia, chest infections, CNS problems, mental side effects, autonomic nervous system side effects, balance problems, cardiovascular morbidities, musculoskeletal symptoms, urinary system problems, gastrointestinal discomforts, genito-sexual problems (both males and females), dermatological, and others to variable extents. As one can see here, although in different degrees, OLZ can cause side effects in all systems of the human body without exception. To discuss the details of all these is out of the scope of this review work, but it is worth mentioning the following subtopics in this context:
Obsessive-Compulsive Disorder (OCD) and Paradoxical Drawbacks
Many psychotropics used to treat various mental illnesses can induce or even cause OCD anew in individuals undergoing OLZ therapy [24,25,26]. As shown, treating one mental disorder can lead to the development of another psychological issue. Additionally, OLZ itself can sometimes produce other unwanted effects, though in a small subset of individuals. These effects include changes in thoughts, agitation, irritability, personality and behavior abnormalities, even hallucinations (the intended target of the drug), and the most severe of these are depression and intrusive thoughts about suicide [26].
Post-injection delirium syndrome: is one of the potential unwanted effects that is unique for OLZ among other 2nd generation long-acting injectable antipsychotic agents. The syndrome is also known as (post-injection delirium/sedation syndrome, abbreviated as PDSS) as it manifests the clinical picture of both delirium and sedation. This undesired effect exhibited by OLZ pamoate is not seen with other similar injectable long-acting preparations of antipsychotic agents of the same class, such as paliperidone palmitate. The syndrome includes the symptoms and signs of delirium (uncoordinated movements, difficulty of speech, confusion) and sedation. Although it is believed that this pharmacodynamic effect occurs as a result of the mishap of accidental intravenous administration of OLZ pamoate, which is designated for deep intramuscular use as a long-acting medication, as a measure to help deinstitutionalized schizophrenic individuals. The incidence of the syndrome indeed is very low, estimated as 0.07% of parenteral administrations [27].
The unwanted effects of OLZ are not only confined to the drug’s direct side effects, but also to its interactions with other drugs acting on the CNS, including other psychotropics (antipsychotics, antidepressants, and others) and even other groups of drugs devoted to treating somatic diseases. The registered and known drug-drug interactions with OLZ are about 592 (drugs.com). It is worth mentioning that OLZ can also cause an undesired effect, which is a sort of overlapping of Neuroleptic Malignant Syndrome (NMS) and serotonin syndrome [28], a condition that can create a diagnostic challenge.
Discontinuation: As is the case with other psychotropics, gradual dose tapering is indicated also with this antipsychotic agent. This is necessary to avoid acute withdrawal syndrome and rapid relapse of psychosis [29]. The risk of relapse on neuroleptics can be minimized via a planned gradual tapering, which is attributed to the fact that adaptation to antipsychotic agents can last for months or years after the cessation of such agents. Dopaminergic (especially D2 receptors) hypersensitivity related to the administration of antipsychotic agents results in upregulation of dopamine receptors, which are the proposed reason behind tardive symptoms of antipsychotic abrupt discontinuation and the relapse of symptoms. Therefore, it will be wise to taper antipsychotics, including olanzapine, gradually over months or even years [30]. The chemical structure of the agent is very similar to benzodiazepines, see Figure 1, a fact that, although partially, may explain why these two agents potentiate the pharmacodynamic effects of each other (both action and side effects) in such a way that they induce deeper sedation and hypotension [31].
Titration of therapeutic serum concentration of olanzapine:
It is generally accepted that OLZ is a safe drug provided the therapeutic serum level of the agent is titrated carefully against its therapeutic effects. The agent’s optimal therapeutic effect lies around "20-40 ng/ml". Although the dose and serum concentration are linearly correlated, therapeutic doses may result in great variability in serum levels. As it has been mentioned elsewhere in this work, OLZ can interact with many drugs (agents) of different classes; these drugs either increase or decrease olanzapine’s serum levels, thus augmenting or decreasing its therapeutic potency. For example, smoking and carbamazepine decrease OLZ serum levels by inducing the cytochrome P450 via mainly its isozyme (CYP1A2), thus decreasing OLZ concentration. Fluvoxamine (an SSRI antidepressant) inhibits CYP1A2, so it increases the agent’s concentration. The other P450 cytochrome isozyme, namely CYP2D6, which is also a clinically relevant one, is inhibited by other factors such as female gender and/or senility [32].
Management of olanzapine Intoxication:
Serum concentrations of above 80ng/ml is considered the threshold for the occurrence of toxic effects of the drug, although research studies showed that the lethal plasma levels are much higher than this. The management of intoxication generally includes the following broad lines:
first, neuroleptic and serotonin syndrome should be ruled out. Fatalities have been documented with plasma concentrations greater than 1000 ng/ml. Bear in mind that to date, there exists no effective specific antidote to revert intoxication caused by OLZ. This is a disadvantage for OLZ [22]. Clinical signs and symptoms mimic those of poisoning with opioids. This includes agitation, tachycardia, dysarthria, and a decrease in the level of consciousness, which terminates with coma. Suicide or attempts to suicide with this agent, if happens, would be attributed to dose-related heavy intoxications, or when the drug is combined heavily with other agents such as alcohol and or opiates. In this sense, the agent is safe provided its serum levels are titrated correctly versus therapeutic effects tailored individually for each patient.
Treatment of an overdose is done mainly by supportive measures in an intensive care unit. The steps include endotracheal intubation, intravenous fluids, observation of cardiopulmonary signs, and mental status [33]. It is worth mentioning that the outcome of poisoning with OLZ is more dangerous than that caused by quetiapine and aripiprazole [34]. This is attributed to the prolonged clearance of the drug [30].
Patients who are on olanzapine therapy should be monitored regularly, especially for fasting blood sugar every 3 months, 6 months, and 9 months. Weight should be also monitored, especially in those who are putting on a lot of weight during the period of drug therapy. Alcohol should be avoided at the start of OLZ treatment as this causes augmented drowsiness and affects alertness and concentration, in addition to the consequences of these. Moreover, it can cause agitation, aggression, and amnesia. Before administration of OLZ for therapeutic purposes or even when another antipsychotic is added as an adjunct to OLZ, the patient should have his/her blood glucose and cholesterol levels checked in addition to a physical check of the heart function (pulse, blood pressure, and EKG). To be on the safe side, a complete blood picture (CBP) and a survey of hepatorenal functions is usually also requested.
Discussion:
The metabolic drawbacks of OLZ were the main reason for the rigorous investigation of this lipophilic 2nd generation antipsychotic and especially its pharmacodynamics. Otherwise, this agent is potent against the negative symptoms of schizophrenia (which are treatment difficult and the real problems of schizophrenic individuals). The drug is also one of the alternatives to treat affective disorders (although as an add-on) in patients with depressive symptoms, in addition to its many important off-label uses.
Overweight: Many agents, including drugs and hormone groups, are known to cause overweight or obesity, see Table 2. Psychotropics (antipsychotic agents) have a big impact on this issue, see Table 1. Indeed, one of the most significant drawbacks of 2nd generation antipsychotics is weight gain. The medical literature includes dozens of documents to confirm this undesired pharmacodynamic effect of OLZ. The multiple treatment meta-analysis conducted by Leucht et al using 6-week data elucidated that most of the currently available antipsychotics, both 1st & 2nd generation agents cause weight gain; the exception is with haloperidol, lurasidone, and ziprasidone. Among these, OLZ and clozapine caused the highest (significant) weight gain, while quetiapine, risperidone, and sertindole caused milder effects according to a head-to-head meta-analysis [35]. An Indian study confirms that 66.6% of 80 patients received OLZ had gain weight by 1-5 kg over a period of 4 weeks, this was neither dependent of OLZ dose being administered nor BMI (body mass index) of these individuals being included in the study. The other significant finding in this study, the weight gain was related to females of 40 years of age and upwards [36]. Indeed, weight gain attributed to OLZ therapy is a serious drawback psychiatrists should consider when deciding to prescribe OLZ to their patients, at least to those who already suffer from metabolic conditions such as hyperlipidemia and/or insulin resistance [20]. OLZ affects almost all classes (and their subclasses) of human membrane receptors [37], among these, the histamine receptor subclasses (H1, H2, H3, and H4). Antagonism of these receptors by OLZ causes weight gain [38]. It is possible to reverse weight gain to a certain extent, but not completely, according to a meta-analysis conducted on 12,279 patients of 40 randomized and 15 uncontrolled trials. The measures that have been applied to reverse the weight gain included drug discontinuation, dose reduction, switch to monotherapy, or switch to a partial agonist agent [39]. Switching from OLZ to asenapine might reverse OLZ-induced obesity to a certain degree, according to a case report, but unfortunately, this agent also has its own drawbacks, such as sedation and somnolence. Switching of medication might be an option, but one has to take into consideration the relapse of the illness [40]. It’s best that the tapering of OLZ should be intermingled synchronously with the dose escalation of the alternative antipsychotic agent to which it is to switch. The other significant factor that causes weight gain in schizophrenic individuals using OLZ as therapy is that the drug, per se, acts as an appetizer; some individuals taking neuroleptics report craving for sweet and fatty food [41]. It is worth mentioning that the regulation of appetite in the human body is a sophisticated and not well-elucidated physiological process, which is mainly regulated by the hypothalamus. The action of the hypothalamus is integrated with the signals received from other parts of the brain and, via hormones released from the adipose tissue and the gastrointestinal tract. The most significant signal transducer ligands (hormones) in this context are leptin and ghrelin [42]. How antipsychotics disrupt this pathway is yet to be elucidated. But it is believed that certain neurotransmitter receptors play a role in this complex process. The evidences indicate the implication of serotonin 5-HT2C and 5-HT1A receptors, histamine H1 and dopamine D2 receptors in addition to many other receptors. Antipsychotic agents differ in their potency to block these receptors, a fact that may explain their different propensities to induce weight gain. Olanzapine and clozapine antagonize the action of these receptors, thus these agents have higher risk to develop overweight in individuals who use these agents for therapy [43], see Table 1. The ratio of weight gain also varies among patients who use these agents, a fact that implies differences between individuals regarding their dietary habits, level of daily physical activity, and their genetic makeup. Polymorphism in the gene that codes the 5-HT2C has been blamed mostly in this context, in addition to other genes [44,45]. Recent research has elucidated the contribution of serotonin signaling in the regulation of glucose homeostasis via sertonylation of certain proteins known as Rab4 [46]. Another issue that should be noted here is that the selective antagonism of 5-HT2 (mainly by 2nd generation antipsychotic agents, which include olanzapine) impairs insulin sensitivity. These nonconventional antipsychotics, moreover, induce abnormal differentiation of adipocytes [47], increase the accumulation of lipids in hepatocytes [48], upregulate the synthesis of sterol regulatory element-binding protein [49], and inhibit the accumulation of glycogen in skeletal myocytes [50]. Despite these proposed mechanisms to explain the induction of insulin resistance (consequently, the weight gains), the issue of weight gain is indeed a matter of debate and controversy among clinicians, endocrinologists, and drug designers.

Table 1.
Antipsychotic agents that can cause weight gain, sequenced in increasing order.
| Antipsychotic agent | Weight gain risk |
|---|---|
| Haloperidol | Low |
| Ziprasidone | Low |
| Lurasidone | Low |
| Aripiprazole | Low |
| Amisulpride | Low |
| Asenapine | Low |
| Paliperidone | Medium |
| Risperidone | Medium |
| Quetiapine | Medium |
| Chlorpromazine | Medium/high |
| Clozapine | High |
| Olanzapine | High |
Table 2.
Agents (drugs/hormones) that induce weight gain, with references.
| SN | Type of drug | Examples | Mechanism | References |
|---|---|---|---|---|
| 1. | Anti-diabetic drugs | |||
| Insulin (hormone) | Circulating insulin is an anabolic hormone. In type 2 diabetes, the induced weight gain is due to a reduction in the signaling of satiety to the arcuate nucleus of the hypothalamus. |
[92, 105 & 106]. | ||
| Sulfonylurea agents, such as glyburide, glipizide, and glimepiride | These increase endogenous insulin levels. | 105 & 108]. | ||
| Thiazolidinediones, such as pioglitazone & rosiglitazone | They induce weight gain due to fluid retention, the promotion of lipid storage, and adipogenesis through the activation of peroxisome proliferator-activated receptor gamma (PPARγ). | [91, 97 & 112]. | ||
| 2. | Antihypertensive drugs | |||
|
Beta-blockers, such as propranolol and atenolol. |
These affect body weight through two main mechanisms: 1) reductions in total energy expenditure through lowering of the basal metabolic rate and thermogenic response to meals, and 2) inhibition of lipolysis in response to adrenergic stimulation. Moreover, these agents can promote fatigue and reductions in patient activity. | [99, 104 & 111]. | ||
| Calcium channel blockers, such as Flunarizine | Body weight gain is linked to its blocking effects on calcium channels and dopamine receptors. | [101 & 109]. | ||
| 3. | Drugs acting on CNS | |||
|
Antipsychotics |
Olanzapine, clozapine, chlorpromazine, quetiapine, risperidone, and paliperidone. | [42]. | ||
|
Anticonvulsants, such as: Valproate, carbamazepine, pregabalin and gabapentin |
Valproate causes weight gain through: 1) Central mechanism: via interactions with appetite-regulating neuropeptides and cytokines within the hypothalamus, as well as effects on energy expenditure 2) Peripheral actions: perturbation of glucose and lipid metabolism that contribute to weight-independent worsening of insulin resistance and risk for type 2 diabetes. |
[94 & 110]. | ||
|
Mood stabilizers: lithium |
The possible mechanisms include: 1) direct effect on hypothalamic centers that control appetite, increased thirst, and increased intake of high-calorie drinks, changes in food preference, 2) its influence on thyroid function with increased incidence of hypothyroidism. | [95 & 100]. | ||
| Sulpiride | It blocks 1) D2 dopamine receptors in the lateral hypothalamus are involved in satiety. 2) It also blocks the pituitary D2 receptors involved in the inhibition of prolactin secretion, which results in hyperprolactinemia, creating a condition similar to a functional ovariectomy, which in turn induces hyperphagia and weight gain. |
[93, 105 & 108]. | ||
| Antidepressants | TCA: Amitriptyline and Nortriptyline |
1) Block different classes of histamine receptors. 2) Interfere with the reuptake of serotonin, which controls appetite, and increases craving for carbohydrate-rich food. 3) They cause hypoglycemia by increasing circulating blood insulin, inducing insulin resistance. |
[103 & 107]. | |
|
Serotonin agents: 1) SSRIs such as citalopram, fluoxetine, and sertraline. 2) SNRIs: such as venlafaxine and duloxetine |
Indeed, these are associated with a slight weight loss to start with, but, with prolonged therapy, many of these agents have been shown to cause weight gain in individuals who use them for treatment. | [102 & 107]. | ||
| 4. | Endocrine agents | |||
| Glucocorticoids: | these may induce an increase in food intake and dietary preference for high-calorie, high-fat (comfort foods) through changes in the activity of AMP-activated protein kinase in the hypothalamus. | [83 & 98]. |
This table is adapted from the guidelines of the British Association of Psychopharmacology (reference 42, a summary of 10 cross references); the drugs are listed in order of their risk of causing weight gain from lowest to highest.
One must admit that the data currently available in the medical literature regarding the molecular mechanisms behind the toxicity exerted by 2nd generation antipsychotics is limited and cannot provide a plausible explanation for the wide-spectrum side effect profile these agents exhibit as a pharmacodynamic parameter. In fact, in vivo studies in rodents have shown that OLZ impairs insulin sensitivity in hepatocytes [51], skeletal myocytes, and adipocytes [52,53,54]. Additionally, recent research has demonstrated that OLZ reduces insulin-mediated glucose uptake through mechanisms involving impaired hypothalamic insulin sensing, as shown by pancreatic glycemic clamp studies [54]. Overall, in vitro research suggests that OLZ can induce insulin resistance in tissues throughout the body [48,49,50].
The problem with these agents is that we don’t know precisely how they operate at the cellular level, a fact attributed to that we don’t know the pathophysiology and the biochemical changes that occur in neurons of psychotic and to be more precise in neurons of schizophrenic individuals. In other words, it is not OLZ alone that should be blamed.
Indeed, people with schizophrenia are more liable to gain weight, almost twice as much as individuals in the general population, because of antipsychotic therapy and other adjunct drugs that are frequently needed in combination to get the most benefit of the antipsychotic therapy, or because of coexisting symptoms (signs) that might be difficult to control with a single psychotropic agent. The other moment of schizophrenia spectrum is isolation from society and physical inactivity because of psychosis and its consequences, even in those who are drug naïve. In fact, individuals who are on antipsychotic therapy consider the weight gain as the most fundamental drawback of these agents. Moreover, we have to realize that being overweight increases the risk of developing heart attack, stroke, and many other physical illnesses such as hypertension, insulin resistance (thus type 2 diabetes), osteoarthritis, and sleep apnea [55]. All these consequential morbidities enhance physical inactivity and make things much worse. It is an accepted fact that the maximal antipsychotic induced weight gain occurs within the 1st 6 months of the therapy period (especially the 1st month, an indicator for greater weight gain in the long run, then the rate declines [56]. The weight gain is more prominent in individuals who use antipsychotics for the first time (acute episode of psychosis) than in those who have to start the same medication again. This could be attributed to the relapse of symptoms after discontinuation or because of uncooperative adherence to the same antipsychotic for the same disease or other mental condition that necessitates the reiteration of the same antipsychotic. Bear in mind that we are talking about 7% increase or more of the starting weight [57].
Clinicians believe there is no clear link between antipsychotic dose and weight gain [56]. Fortunately, many agents within what is known as the 2nd generation drugs are available. Clinicians can choose among these drugs, which generally provide similar therapeutic effects but differ in their likelihood to cause weight gain [42,56]; as demonstrated in Table 1. The exception is clozapine, which is ideal for treating negative symptoms of schizophrenia (such as avolition, anhedonia, and inability to act spontaneously) as well as resistant schizophrenia and mania, despite its serious potential side effects [22]. The cellular mechanisms behind weight gain are not fully understood, but it is well known that this agent can cause hyperglycemia (insulin resistance) and hyperlipidemia through different mechanisms discussed in this review. According to the US FDA -1440 x 810, it is believed that combining OLZ with samidorphan (Lybalvi) reduces the risk of weight gain compared to OLZ alone as monotherapy [58]. Additionally, metformin, an oral hypoglycemic agent, has been used as an adjunct to olanzapine to prevent weight gain associated with this and other 2nd generation antipsychotics that may have metabolic side effects [59].
Insulin resistance:
Why OLZ causes obesity, or at least increases weight, is attributed to the predisposition of insulin resistance [16,60,61,62]. Insulin resistance is a state of prediabetes where glucose transporters GLUTs (mainly GLUT1, GLUT2, GLUT3, and GLUT4) will not respond to the action of the hormone insulin on insulin receptors (a defect in the signal transduction cascade initiated by insulin). The increase in insulin levels in the circulation causes lipogenesis within cells, especially in lipocytes, and consequently leads to weight gain [63]. The two main known contributing factors to insulin resistance are excess body fat around the waist and lack of physical activity. The etiology of insulin resistance has not been elucidated hitherto, but it is generally accepted that the underlying causes are either genetic or acquired. What concerns us in this context is the acquired factors, namely, the drug-induced ones. There are many drug groups known to cause insulin resistance; these include: steroids, certain antihypertensive drugs, some antivirals that are used in HIV treatments, and certain neuroleptics (antipsychotic agents), see Table 2. To discuss all these drug groups falls outside the scope of this mini-review work; therefore, our concerns will be limited to antipsychotics and especially on OLZ. One has to admit that insulin resistance is a complex morbidity because the condition does not exhibit prominent symptoms until it progresses into prediabetes or type 2 diabetes. But once it occurs, the best-known scientific methods to prevent/reverse the condition is via changing the dietary habits to healthy one, regular physical exercising to keep the body healthy and lean, a condition unfortunately not easily achieved in psychotic patients.
Indeed, insulin resistance and especially drug induced ones is a complicated subject of debate in endocrinology and diabetology. This is attributed to that its mechanism and pathophysiology is not elucidated convincingly. Genetic factors, including mitochondrial dysfunction, have been blamed as being among the most important contributing factors to induce this prediabetic metabolic disturbance resulting from resistance to the function of insulin [64,65,66,67]. In other words, insulin resistance can occur in schizophrenia even before the administration of antipsychotic agents; therefore, many clinicians and scientists classify schizophrenia under mitochondrial diseases [65]. Results obtained from both preclinical and clinical studies have shown that among the 2nd generation antipsychotic agents, OLZ is the strongest to induce metabolic toxicity via its effects on plasma glucose levels, weight gain, and many other metabolic parameters [68]. Despite their wide-spectrum metabolic adverse effects, clozapine, risperidone, OLZ, quetiapine, and aripiprazole have been among the top-selling pharmaceuticals worldwide over the last decade [69,70].
Mitochondrial dysfunction: For decades, mitochondrial dysfunction has been recognized as a potential predisposing factor to both psychosis and affective disorders [65,71]. Intact and sound mitochondria in neurons is a must for energy production (oxidative phosphorylation) and Ca++ homeostasis, which are crucial for the action of neurons. A deviation in mitochondria-related intracellular biological pathways that regulate neuronal survival, apoptosis, oxidative stress, plasticity, and neuronal transmission has been observed both in psychosis and affective disorders [37,64,72,73,74,75,76]. In other words, malfunctioning neuronal mitochondria distort the connectivity of neuronal networks, which might be the reason behind the abnormal emotional and cognitive behaviors that manifest clinically both in schizophrenia and affective disorders. In this connection, in an animal model, transplantation of intact healthy mitochondria into neurons has improved the aberrant mitochondrial function and restored the behavioral deficits in animals [77].
The interesting issue here is that mitochondria are a target for psychotropic agents, which contribute to the modulatory effects on mitochondrial gene expression and thus synthesis of proteins that are fundamental for the mitochondrial machinery to drive citric acid cycle, oxidative phosphorylation, apoptosis, autophagy, and other dynamics of the mitochondrial network [37,43,78,79,80,81]. OLZ releases free radicals in neurons and thus causes oxidative stress; accordingly, it induces depolarization of mitochondrial membranes and subsequently their damage, thus causing neuronal apoptosis as neurons cannot survive without intact and sound mitochondria to synthesize ATP [82]. Regarding the release of free radicals, one has to admit that the 2nd generation agent OLZ has a milder propensity than the 1st generation agents, such as haloperidol [83] and even other 2nd generation agents, such as clozapine [22] and quetiapine [84], to release reactive oxygen species. As psychotic individuals respond differently to different antipsychotic agents, recent studies apply mitochondrial function as a parameter to choose the best currently available antipsychotic for each psychotic patient separately [85]. In other words, the agent (agents) should be customized for each patient, because patients respond differently to each antipsychotic agent. Still, neither the 1st nor the 2nd generation agents are optimal. The reason for this is that we know very little about the biochemical changes that stand behind the pathophysiology of psychosis [22], as mentioned elsewhere in this work.
Is olanzapine addictive?
Although it shares features that mimic other agents that can cause abuse, such as benzodiazepines, Z-drugs (nonbenzodiazepines, used to treat insomnia), and barbiturates, there exists no clear and strong evidence based on a reliable systematic study to demonstrate that OLZ is an addictive agent. One of the arguments that backs the assumption that OLZ may not possess the high potential to cause abuse is that the agent has a long elimination half-life (t/2), in humans, about 33 hours [30]. Moreover, the abusive drugs usually have a shorter duration of action, as is the case with amphetamine, cocaine, etc. Yet clinicians should be cautious when prescribing this thienobenzodiazepine derivative to individuals who have records of substance abuse. Bear in mind that this substance is water-insoluble and readily passes the blood-barrier in a manner that mimics that of diazepam, and both of these agents have CNS depressant properties, which is why it is expected that OLZ could be misused as a recreational drug.
Tapering off olanzapine and withdrawal symptoms of olanzapine cutoff:
Similar to other psychotropic agents, both antipsychotics and antidepressants, OLZ should be tapered off gradually under supervision of a psychiatrist. This is attributed to the fact that abrupt cutoff of OLZ can cause rebound symptoms, which means relapse of the symptoms of psychosis the drug was originally prescribed to treat [86,87]. The other serious issue here is the emergence of withdrawal symptoms. These include: dizziness, restlessness, agitation, anxiety (insomnia), muscle spasms, dyskinesia, and GIT symptoms (nausea, vomiting, diarrhea) [88,89,90].
Conclusion
We have discussed the plausible and possible mechanisms behind insulin resistance and overweight in individuals who are on OLZ therapy to combat psychosis or other mental diseases that necessitate drug therapy with OLZ. We have attempted to assemble the pieces of the puzzle to understand the spectrum of undesired metabolic effects associated with these agents. We believe that considerable effort should be made to fill the gaps in our understanding of the etiology of the unwanted metabolic effects that this drug exerts. Fortunately, clinicians have many alternative agents within 2nd generation antipsychotics they can choose to prescribe for each patient, a condition that necessitates cooperation between the individual patients and the psychiatrist. That is to say, the prescribed antipsychotic should be fitted to the individual patient. Patients respond variably to different agents; in other words, what is convenient for one patient does not necessarily fit the other one for therapy. OLZ is one of the best antipsychotics we have to combat the negative symptoms of schizophrenia. Monitoring of weight and the other accompanying metabolic parameters is necessary before starting olanzapine therapy. This is necessary in cases when we have to switch to another agent (or other agents when a combination therapy is in question) to obtain the desired therapeutic response. There is a lot to be done to understand the real biochemical changes that occur in neurons (and the mitochondria they possess) of schizophrenic individuals. This is important as certain agents of 2nd generation antipsychotics, such as OLZ, are lipophilic nanoparticles that can easily cross the blood-brain barrier and cellular and organelle membranes, such as mitochondria (the energy house of neurons). As schizophrenic individuals already have dysfunctional mitochondria in their neurons, the future (optimal) antipsychotic agents should devoid the property of free radical release that can jeopardize mitochondrial function and aggravates psychotic symptoms. Moreover, they should be more selective in such a way they only antagonize the receptors they are designed to block, because OLZ and almost all currently available psychotropic agents affect almost all classes of neuronal membrane receptors to various degrees.
OBS: The references [91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112] do not appear in the main manuscript; these belong to Table 2.
Conflicts of interest: none
Funding
The authors extend their sincere thanks to the Deanship of Scientific Research (DSR) at Najran University for funding this work.
Abbreviations
Antipsychotic (s) = APC (s); OLZ = Olanzapine; EPS = Extrapyramidal symptoms; NMS = Neuroleptic Malignant Syndrome; Serotonin syndrome =(SS).
References
- Kessler, R.C., et al., Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry, 2005. 62(6): p. 593-602. [CrossRef]
- Brunton, L.; Chabner, B.; Knollmann, B. Goodman and Gillman's The Pharmacological Basis of Therapeutics. 12th Ed. 2010. New York: McGraw-Hill Professional. ISBN: 978-0-07-16244-8.
- Oruch R. Psychosis and Antipsychotics: A Short Résumé. Austin J Pharmacol Ther. 2014; 2 (7).3.
- Mann SK; Marawah R. Chlorpromazine. 2022 May 17. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan. PMID: 31971720.
- https://reference.medscape.com/drug/zyprexa-relprevv-olanzapine-342979.
- Attia, E., et al., Olanzapine Versus Placebo in Adult Outpatients With Anorexia Nervosa: A Randomized Clinical Trial. Am J Psychiatry, 2019. 176(6): p. 449-456. [CrossRef]
- Stephens, R.J., C. Bassel, and P. Sandor, Olanzapine in the treatment of aggression and tics in children with Tourette's syndrome--a pilot study. J Child Adolesc Psychopharmacol, 2004. 14(2): p. 255-66. [CrossRef]
- Tural Hesapcioglu, S., et al., Olanzapine, risperidone, and aripiprazole use in children and adolescents with Autism Spectrum Disorders. Research in Autism Spectrum Disorders, 2020. 72: p. 101520. [CrossRef]
- Khaledi-Paveh B, Maazinezhad S, Rezaie L, Khazaie H. Treatment of chronic insomnia with atypical antipsychotics: results from a follow-up study. Sleep Sci. 2021 Jan-Mar;14(1):27-32. PMID: 34104334; PMCID: PMC8157779.
- Saudemont, G., et al., The use of olanzapine as an antiemetic in palliative medicine: a systematic review of the literature. BMC Palliat Care, 2020. 19(1): p. 56. [CrossRef]
- Huang, H.Y., H.L. Chen, and L.P. Feng, Maternal obesity and the risk of neural tube defects in offspring: A meta-analysis. Obes Res Clin Pract, 2017. 11(2): p. 188-197. [CrossRef]
- Prakash, S. and R.K. Chadda, Teratogenicity with olanzapine. Indian J Psychol Med, 2014. 36(1): p. 91-3. [CrossRef]
- Rasmussen, S.A., et al., Maternal obesity and risk of neural tube defects: a meta-analysis. Am J Obstet Gynecol, 2008. 198(6): p. 611-9.
- Uguz F. A New Safety Scoring System for the Use of Psychotropic Drugs During Lactation. Am J Ther. 2021 Jan-Feb 01;28(1):e118-e126. PMID: 30601177. [CrossRef]
- Caution with olanzapine use in dementia. Aust Prescr. 2021 Apr;44(2):40. Epub 2021 Apr 1. PMID: 33911330; PMCID: PMC8075751. [CrossRef]
- Yeung, E.Y., et al., Effect of atypical antipsychotics on body weight in geriatric psychiatric inpatients. SAGE Open Med, 2017. 5: p. 2050312117708711. [CrossRef]
- McCormack, P.L., Olanzapine: in adolescents with schizophrenia or bipolar I disorder. CNS Drugs, 2010. 24(5): p. 443-52.
- Tural Hesapcioglu, S., et al., Frequency and Correlates of Acute Dystonic Reactions After Antipsychotic Initiation in 441 Children and Adolescents. J Child Adolesc Psychopharmacol, 2020. 30(6): p. 366-375. [CrossRef]
- Lexi-Comp Inc. (2010). Lexi-Comp Drug Information Handbook (19th North American ed.). Hudson, OH: Lexi-Comp Inc. ISBN 978-1-59195-278-7.
- Leong, I., Neuropsychiatric disorders: Side effects of olanzapine worsened by metabolic dysfunction. Nat Rev Endocrinol, 2018. 14(3): p. 129.
- Schwenger, E., J. Dumontet, and M.H. Ensom, Does olanzapine warrant clinical pharmacokinetic monitoring in schizophrenia? Clin Pharmacokinet, 2011. 50(7): p. 415-28. [CrossRef]
- Ramadhan Oruch, Ian F Pryme, Anders Lund. The Ideal Antipsychotic: Hybrid between Typical Haloperidol And the Atypical Clozapine Antipsychotic. Journal of Bioanalysis & Biomedicine, 2015, 07, ⟨10.4172/1948-593x.1000134⟩. ⟨hal-04023320⟩.
- Chen, J., et al., Molecular Mechanisms of Antipsychotic Drug-Induced Diabetes. Front Neurosci, 2017. 11: p. 643. [CrossRef]
- Alevizos, B., C. Papageorgiou, and G.N. Christodoulou, Obsessive-compulsive symptoms with olanzapine. Int J Neuropsychopharmacol, 2004. 7(3): p. 375-7.
- Kulkarni, G., J.C. Narayanaswamy, and S.B. Math, Olanzapine induced de-novo obsessive compulsive disorder in a patient with schizophrenia. Indian J Pharmacol, 2012. 44(5): p. 649-50. [CrossRef]
- Lykouras, L., et al., Olanzapine and obsessive-compulsive symptoms. Eur Neuropsychopharmacol, 2000. 10(5): p. 385-7.
- Luedecke, D., et al., Post-injection delirium/sedation syndrome in patients treated with olanzapine pamoate: mechanism, incidence, and management. CNS Drugs, 2015. 29(1): p. 41-6. [CrossRef]
- Kontaxakis, V.P., et al., Olanzapine-associated neuroleptic malignant syndrome: Is there an overlap with the serotonin syndrome? Ann Gen Hosp Psychiatry, 2003. 2(1): p. 10. [CrossRef]
- Horowitz, M.A., et al., A Method for Tapering Antipsychotic Treatment That May Minimize the Risk of Relapse. Schizophr Bull, 2021. 47(4): p. 1116-1129. [CrossRef]
- Callaghan, J.T., et al., Olanzapine. Pharmacokinetic and pharmacodynamic profile. Clin Pharmacokinet, 1999. 37(3): p. 177-93.
- Diazepam/olanzapine/valproate semisodium interaction. Reactions Weekly, 2012. 1384(1): p. 23-23.
- Rao, M.L., et al., [Olanzapine: pharmacology, pharmacokinetics and therapeutic drug monitoring]. Fortschr Neurol Psychiatr, 2001. 69(11): p. 510-7.
- O'Malley, G.F., et al., Olanzapine overdose mimicking opioid intoxication. Ann Emerg Med, 1999. 34(2): p. 279-81. [CrossRef]
- Michie, P.T., et al., The neurobiology of MMN and implications for schizophrenia. Biol Psychol, 2016. 116: p. 90-7. [CrossRef]
- Dayabandara, M., et al., Antipsychotic-associated weight gain: management strategies and impact on treatment adherence. Neuropsychiatr Dis Treat, 2017. 13: p. 2231-2241. [CrossRef]
- Jain, S., M. Bhargava, and S. Gautam, Weight gain with olanzapine: Drug, gender, or age? Indian J Psychiatry, 2006. 48(1): p. 39-42. [CrossRef]
- Ben-Shachar, D., Mitochondrial multifaceted dysfunction in schizophrenia; complex I as a possible pathological target. Schizophr Res, 2017. 187: p. 3-10. [CrossRef]
- Ratliff, J.C., et al., Association of prescription H1 antihistamine use with obesity: results from the National Health and Nutrition Examination Survey. Obesity (Silver Spring), 2010. 18(12): p. 2398-400. [CrossRef]
- Speyer, H., et al., Reversibility of Antipsychotic-Induced Weight Gain: A Systematic Review and Meta-Analysis. Front Endocrinol (Lausanne), 2021. 12: p. 577919. [CrossRef]
- Okazaki, K., K. Yamamuro, and T. Kishimoto, Reversal of olanzapine-induced weight gain in a patient with schizophrenia by switching to asenapine: a case report. Neuropsychiatr Dis Treat, 2017. 13: p. 2837-2840. [CrossRef]
- Huang, J., et al., Increased Appetite Plays a Key Role in Olanzapine-Induced Weight Gain in First-Episode Schizophrenia Patients. Front Pharmacol, 2020. 11: p. 739. [CrossRef]
- Haddad, P. "Antipsychotic medication and weight gain". March 31, 2017. https://bap.org.uk/articles/antipsychotic-medication-and-weight-gain/.
- Maurer, I.C., P. Schippel, and H.P. Volz, Lithium-induced enhancement of mitochondrial oxidative phosphorylation in human brain tissue. Bipolar Disord, 2009. 11(5): p. 515-22. [CrossRef]
- Kaur, G. and S.K. Kulkarni, Studies on modulation of feeding behavior by atypical antipsychotics in female mice. Prog Neuropsychopharmacol Biol Psychiatry, 2002. 26(2): p. 277-85. [CrossRef]
- Zai, C.C., et al., Association study of GABAA alpha2 receptor subunit gene variants in antipsychotic-associated weight gain. J Clin Psychopharmacol, 2015. 35(1): p. 7-12. [CrossRef]
- Al-Zoairy, R., et al., Serotonin improves glucose metabolism by Serotonylation of the small GTPase Rab4 in L6 skeletal muscle cells. Diabetol Metab Syndr, 2017. 9: p. 1. [CrossRef]
- Oh, J.E., et al., Inhibition of mouse brown adipocyte differentiation by second-generation antipsychotics. Exp Mol Med, 2012. 44(9): p. 545-53. [CrossRef]
- Sertie, A.L., et al., Effects of antipsychotics with different weight gain liabilities on human in vitro models of adipose tissue differentiation and metabolism. Prog Neuropsychopharmacol Biol Psychiatry, 2011. 35(8): p. 1884-90. [CrossRef]
- Hu, Y., E. Kutscher, and G.E. Davies, Berberine inhibits SREBP-1-related clozapine and risperidone induced adipogenesis in 3T3-L1 cells. Phytother Res, 2010. 24(12): p. 1831-8.
- Engl, J., et al., Olanzapine impairs glycogen synthesis and insulin signaling in L6 skeletal muscle cells. Mol Psychiatry, 2005. 10(12): p. 1089-96. [CrossRef]
- Chintoh, A.F., et al., Insulin resistance following continuous, chronic olanzapine treatment: an animal model. Schizophr Res, 2008. 104(1-3): p. 23-30. [CrossRef]
- Albaugh, V.L., et al., Olanzapine promotes fat accumulation in male rats by decreasing physical activity, repartitioning energy and increasing adipose tissue lipogenesis while impairing lipolysis. Mol Psychiatry, 2011. 16(5): p. 569-81. [CrossRef]
- Houseknecht, K.L., et al., Acute effects of atypical antipsychotics on whole-body insulin resistance in rats: implications for adverse metabolic effects. Neuropsychopharmacology, 2007. 32(2): p. 289-97. [CrossRef]
- Kowalchuk, C., et al., In male rats, the ability of central insulin to suppress glucose production is impaired by olanzapine, whereas glucose uptake is left intact. J Psychiatry Neurosci, 2017. 42(6): p. 424-431. [CrossRef]
- De Hert, M., et al., Cardiovascular disease and diabetes in people with severe mental illness position statement from the European Psychiatric Association (EPA), supported by the European Association for the Study of Diabetes (EASD) and the European Society of Cardiology (ESC). Eur Psychiatry, 2009. 24(6): p. 412-24. [CrossRef]
- Cooper, S.J., et al., BAP guidelines on the management of weight gain, metabolic disturbances and cardiovascular risk associated with psychosis and antipsychotic drug treatment. J Psychopharmacol, 2016. 30(8): p. 717-48. [CrossRef]
- McEvoy, J.P., et al., Efficacy and tolerability of olanzapine, quetiapine, and risperidone in the treatment of early psychosis: a randomized, double-blind 52-week comparison. Am J Psychiatry, 2007. 164(7): p. 1050-60.
- Paik, J., Olanzapine/Samidorphan: First Approval. Drugs, 2021. 81(12): p. 1431-1436. [CrossRef]
- de Silva, V.A., et al., Metformin in prevention and treatment of antipsychotic induced weight gain: a systematic review and meta-analysis. BMC Psychiatry, 2016. 16(1): p. 341.
- Martins, P.J., M. Haas, and S. Obici, Central nervous system delivery of the antipsychotic olanzapine induces hepatic insulin resistance. Diabetes, 2010. 59(10): p. 2418-25. [CrossRef]
- Yang, N., et al., Insulin Resistance-Related Proteins Are Overexpressed in Patients and Rats Treated With Olanzapine and Are Reverted by Pueraria in the Rat Model. J Clin Psychopharmacol, 2019. 39(3): p. 214-219. [CrossRef]
- Yu, L., et al., Insulin resistance induced by olanzapine and other second-generation antipsychotics in Chinese patients with schizophrenia: a comparative review and meta-analysis. Eur J Clin Pharmacol, 2019. 75(12): p. 1621-1629.
- Aedh, A.I., et al., A Glimpse into Milestones of Insulin Resistance and an Updated Review of Its Management. Nutrients, 2023. 15(4). [CrossRef]
- Kato, T., Neurobiological basis of bipolar disorder: Mitochondrial dysfunction hypothesis and beyond. Schizophr Res, 2017. 187: p. 62-66. [CrossRef]
- Rajasekaran, A., et al., Mitochondrial dysfunction in schizophrenia: pathways, mechanisms and implications. Neurosci Biobehav Rev, 2015. 48: p. 10-21. [CrossRef]
- Scaglia, F., The role of mitochondrial dysfunction in psychiatric disease. Dev Disabil Res Rev, 2010. 16(2): p. 136-43. [CrossRef]
- Tobe, E.H., Mitochondrial dysfunction, oxidative stress, and major depressive disorder. Neuropsychiatr Dis Treat, 2013. 9: p. 567-73. [CrossRef]
- Del Campo, A., et al., Metabolic Syndrome and Antipsychotics: The Role of Mitochondrial Fission/Fusion Imbalance. Front Endocrinol (Lausanne), 2018. 9: p. 144. [CrossRef]
- Geddes, J., Generating evidence to inform policy and practice: the example of the second generation "atypical" antipsychotics. Schizophr Bull, 2003. 29(1): p. 105-14. [CrossRef]
- Monasterio, E. and D. Gleeson, Pharmaceutical industry behaviour and the Trans Pacific Partnership Agreement. N Z Med J, 2014. 127(1389): p. 6-12.
- Clay, H.B., S. Sillivan, and C. Konradi, Mitochondrial dysfunction and pathology in bipolar disorder and schizophrenia. Int J Dev Neurosci, 2011. 29(3): p. 311-24. [CrossRef]
- Ben-Shachar, D. and D. Laifenfeld, Mitochondria, synaptic plasticity, and schizophrenia. Int Rev Neurobiol, 2004. 59: p. 273-96.
- Iwata, K., Mitochondrial Involvement in Mental Disorders; Energy Metabolism, Genetic, and Environmental Factors, in Pre-Clinical Models: Techniques and Protocols, P.C. Guest, Editor. 2019, Springer New York: New York, NY. p. 41-48.
- Manji, H.K., et al., The underlying neurobiology of bipolar disorder. World Psychiatry, 2003. 2(3): p. 136-46.
- Ross, C.A., et al., Neurobiology of schizophrenia. Neuron, 2006. 52(1): p. 139-53.
- Scaini, G., et al., Mitochondrial dysfunction in bipolar disorder: Evidence, pathophysiology and translational implications. Neurosci Biobehav Rev, 2016. 68: p. 694-713. [CrossRef]
- Robicsek, O., et al., Isolated Mitochondria Transfer Improves Neuronal Differentiation of Schizophrenia-Derived Induced Pluripotent Stem Cells and Rescues Deficits in a Rat Model of the Disorder. Schizophr Bull, 2018. 44(2): p. 432-442. [CrossRef]
- Chen, G. and H.K. Manji, The extracellular signal-regulated kinase pathway: an emerging promising target for mood stabilizers. Curr Opin Psychiatry, 2006. 19(3): p. 313-23. [CrossRef]
- Kazemi, H., et al., Lithium prevents cell apoptosis through autophagy induction. Bratisl Lek Listy, 2018. 119(4): p. 234-239. [CrossRef]
- Sarkar, S., et al., Lithium induces autophagy by inhibiting inositol monophosphatase. J Cell Biol, 2005. 170(7): p. 1101-11. [CrossRef]
- Scaini, G., et al., Second generation antipsychotic-induced mitochondrial alterations: Implications for increased risk of metabolic syndrome in patients with schizophrenia. Eur Neuropsychopharmacol, 2018. 28(3): p. 369-380. [CrossRef]
- Vucicevic, L., et al., Autophagy inhibition uncovers the neurotoxic action of the antipsychotic drug olanzapine. Autophagy, 2014. 10(12): p. 2362-78. [CrossRef]
- Singh, O.P., et al., A comparative study of oxidative stress and interrelationship of important antioxidants in haloperidol and olanzapine treated patients suffering from schizophrenia. Indian J Psychiatry, 2008. 50(3): p. 171-6. [CrossRef]
- Ramadhan Oruch., et al. “Quetiapine: An Objective Evaluation of Pharmacology, Clinical Uses and Intoxication”. EC Pharmacology and Toxicology 8.4 (2020): 01-26.
- Bar-Yosef, T., et al., Mitochondrial function parameters as a tool for tailored drug treatment of an individual with psychosis: a proof of concept study. Sci Rep, 2020. 10(1): p. 12258. [CrossRef]
- Chouinard, G., et al., Antipsychotic-Induced Dopamine Supersensitivity Psychosis: Pharmacology, Criteria, and Therapy. Psychother Psychosom, 2017. 86(4): p. 189-219. [CrossRef]
- Seeman, P., All roads to schizophrenia lead to dopamine supersensitivity and elevated dopamine D2(high) receptors. CNS Neurosci Ther, 2011. 17(2): p. 118-32. [CrossRef]
- Brandt, L., et al., Antipsychotic Withdrawal Symptoms: A Systematic Review and Meta-Analysis. Front Psychiatry, 2020. 11: p. 569912. [CrossRef]
- Dilsaver, S.C. and N.E. Alessi, Antipsychotic withdrawal symptoms: phenomenology and pathophysiology. Acta Psychiatr Scand, 1988. 77(3): p. 241-6. [CrossRef]
- Lacoursiere, R.B., H.E. Spohn, and K. Thompson, Medical effects of abrupt neuroleptic withdrawal. Compr Psychiatry, 1976. 17(2): p. 285-94. [CrossRef]
- Aleman-Gonzalez-Duhart, D., et al., Current Advances in the Biochemical and Physiological Aspects of the Treatment of Type 2 Diabetes Mellitus with Thiazolidinediones. PPAR Res, 2016. 2016: p. 7614270. [CrossRef]
- Allison, D.B., et al., Antipsychotic-induced weight gain: a comprehensive research synthesis. Am J Psychiatry, 1999. 156(11): p. 1686-96. [CrossRef]
- Banini, B.A. and A.J. Sanyal, Current and future pharmacologic treatment of nonalcoholic steatohepatitis. Curr Opin Gastroenterol, 2017. 33(3): p. 134-141. [CrossRef]
- Belcastro, V., et al., Metabolic and endocrine effects of valproic acid chronic treatment. Epilepsy Res, 2013. 107(1-2): p. 1-8. [CrossRef]
- Chen, Y. and T. Silverstone, Lithium and weight gain. Int Clin Psychopharmacol, 1990. 5(3): p. 217-25. [CrossRef]
- Christ-Crain, M., et al., AMP-activated protein kinase mediates glucocorticoid-induced metabolic changes: a novel mechanism in Cushing's syndrome. FASEB J, 2008. 22(6): p. 1672-83. [CrossRef]
- Cignarelli, A., F. Giorgino, and R. Vettor, Pharmacologic agents for type 2 diabetes therapy and regulation of adipogenesis. Arch Physiol Biochem, 2013. 119(4): p. 139-50. [CrossRef]
- Harfstrand, A., et al., Regional differences in glucocorticoid receptor immunoreactivity among neuropeptide Y immunoreactive neurons of the rat brain. Acta Physiol Scand, 1989. 135(1): p. 3-9. [CrossRef]
- Koch, G., I.W. Franz, and F.W. Lohmann, Effects of short-term and long-term treatment with cardio-selective and non-selective beta-receptor blockade on carbohydrate and lipid metabolism and on plasma catecholamines at rest and during exercise. Clin Sci (Lond), 1981. 61 Suppl 7: p. 433s-435s. [CrossRef]
- Livingstone, C. and H. Rampes, Lithium: a review of its metabolic adverse effects. J Psychopharmacol, 2006. 20(3): p. 347-55. [CrossRef]
- Manconi, F.M., et al., Behavioural And Biochemical Effects Of Flunarizine On The Dopaminergic System In Rodents. Cephalalgia, 1987. 7(6_suppl): p. 420-421. [CrossRef]
- Masand, P.S. and S. Gupta, Long-term side effects of newer-generation antidepressants: SSRIS, venlafaxine, nefazodone, bupropion, and mirtazapine. Ann Clin Psychiatry, 2002. 14(3): p. 175-82. [CrossRef]
- Nakra, B.R., et al., Amitriptyline and weight gain: a biochemical and endocrinological study. Curr Med Res Opin, 1977. 4(8): p. 602-6. [CrossRef]
- Newsom, S.A., et al., Short-term sympathoadrenal inhibition augments the thermogenic response to beta-adrenergic receptor stimulation. J Endocrinol, 2010. 206(3): p. 307-15. [CrossRef]
- Russell-Jones, D. and R. Khan, Insulin-associated weight gain in diabetes--causes, effects and coping strategies. Diabetes Obes Metab, 2007. 9(6): p. 799-812.
- Seeman, P., et al., Antipsychotic drug doses and neuroleptic/dopamine receptors. Nature, 1976. 261(5562): p. 717-9. [CrossRef]
- Serretti, A. and L. Mandelli, Antidepressants and body weight: a comprehensive review and meta-analysis. J Clin Psychiatry, 2010. 71(10): p. 1259-72.
- Van Gaal, L. and A. Scheen, Weight management in type 2 diabetes: current and emerging approaches to treatment. Diabetes Care, 2015. 38(6): p. 1161-72.
- Vecsei, L., et al., Drug safety and tolerability in prophylactic migraine treatment. Expert Opin Drug Saf, 2015. 14(5): p. 667-81. [CrossRef]
- Verrotti, A., et al., Weight gain following treatment with valproic acid: pathogenetic mechanisms and clinical implications. Obes Rev, 2011. 12(5): p. e32-43. [CrossRef]
- Welle, S., R.G. Schwartz, and M. Statt, Reduced metabolic rate during beta-adrenergic blockade in humans. Metabolism, 1991. 40(6): p. 619-22. [CrossRef]
- Wilding, J., Thiazolidinediones, insulin resistance and obesity: Finding a balance. Int J Clin Pract, 2006. 60(10): p. 1272-80. [CrossRef]
Figure 1.
Chemical structure of the drugs discussed in this work, illustrating their solubility properties.
Figure 1.
Chemical structure of the drugs discussed in this work, illustrating their solubility properties.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



