Submitted:
27 September 2025
Posted:
29 September 2025
You are already at the latest version
Abstract
Lithium remains the first choice for long-term prophylaxis of mood episodes in bipolar disorder (BD), but only 30% of patients will respond, and there is no reliable method by which to predict treatment response. Ketamine is a rapid antidepressant therapy which ostensibly yields greater results in patients with clinical phenotypes that are classically associated with lithium non-response. Thus, we hypothesized an inverse relationship between acute ketamine response and efficacy of long-term prophylactic lithium therapy in BD. We conducted a scoping review of clinical and preclinical studies that examine convergent and divergent predictors and mechanisms of acute response to ketamine and long-term response to lithium. Preclinical data show mechanistic convergence of ketamine and lithium on the GSK-3β/mTOR pathways, and enhancement of synaptic plasticity. Furthermore, lithium appears to consistently limit ketamine-related oxidative stress and hyperlocomotion. However, clinical predictors diverge, with ketamine response associated with metabolic risk factors, anxiety/mixed features, and non-melancholic presentations, which are generally predictors of poorer prophylactic lithium response. No study directly tested ketamine response as a predictor of prophylactic lithium response. An important limitation is that clinical studies of ketamine are enriched for lithium-refractory populations and have often included mixed unipolar and bipolar cases. Overall, existing data support mechanistic overlap but clinical divergence between ketamine and lithium responders, which is only partially consistent with our hypothesized inverse relationship. We must therefore undertake longitudinal studies of prophylactic lithium therapy among patients with BD who received ketamine for acute antidepressant treatment. If this inverse relationship is validated, ketamine non-response could be used to rapidly identify lithium-responsive BD, thereby establishing control over this disease earlier in the course of illness.
Keywords:
bipolar disorder
; depression
; ketamine
; lithium
; treatment prediction
; maintenance therapy
1. Introduction
Bipolar disorder (BD) is a chronic neuropsychiatric disorder for which effective long-term maintenance treatment is critical to preventing relapses and reducing morbidity [1]. After more than seven decades, lithium remains the gold-standard prophylactic mood stabilizer in BD [2]. However, only one-third of patients achieve excellent response, which is characterized by full symptomatic remission and functional recovery [3,4]. Since an unsuccessful lithium trial can entail months of suboptimal treatment and side effects, psychiatrists and researchers must strive to find a priori or early markers of eventual response to lithium prophylaxis [5].
Decades of research suggest that patients with a more “classical” bipolar phenotype are the most likely to respond well to lithium maintenance [4,6,7]. Indeed, lithium-responsiveness is associated with completely episodic course (discrete episodes with full symptomatic remission and functional recovery in the inter-episode period), absence of rapid cycling, a strong family history of BD, and a later age of onset [4,5,8]. By contrast, lithium non-responsive BD patients typically exhibit a more atypical or “non-classical” clinical phenotype [6]., including the presence of mixed features, rapid cycling, and significant comorbidities, such as anxiety disorders [4,6,9]. Other studies have noted that metabolic comorbidities, such as insulin resistance, diabetes, and higher body mass index (BMI), are more common in lithium non-responders [8,10]. Lithium-nonresponders thus ostensibly show a more atypical and complicated clinical profile (e.g., mixed features, anxiety, metabolic comorbidities) compared to the classical episodic presentation of BD. Since clinicians currently cannot definitively determine lithium response before initiating therapy, many ultimately lithium non-responsive patients are subjected to lengthy lithium trials to determine effectiveness. These patients are at risk of experiencing many months of side-effects and illness recurrence if lithium ultimately proves ineffective.
In recent years, ketamine has emerged as a novel augmentation option for acute treatment-resistant bipolar depression [11]. Sub-anaesthetic doses of ketamine, an NMDA receptor antagonist produce rapid antidepressant effects within hours to days, which compares favourably to the 4–8 weeks typically required for response to conventional antidepressants [12,13]. Intriguingly, ketamine appears to benefit some subgroups of patients that are traditionally difficult to treat, such as patients with non-melancholic or “anxious” depressive subtypes [14], or patients with significant comorbid mixed mood features [15,16]. Furthermore, while a higher body mass index (BMI) has predicted positive response to ketamine [17], it is well known that higher BMI and related metabolic issues typically portend poorer prophylactic response to lithium [10,18]. Taken together, it these findings suggest that acute ketamine responders may phenotypically resemble prophylactic lithium non-responders, implying that ketamine’s mechanism of action (e.g., acute glutamatergic modulation and synaptogenesis) may potentially target acute depressive pathology in patient populations whose clinical phenotypes diverge from those typically observed in responders to long-term lithium prophylaxis.
Therefore, we asked whether there is substantial clinical/preclinical evidence to support an inverse relationship between ketamine responsiveness and lithium prophylactic response in BD. In other words, we sought to understand whether non-response to an acute ketamine trial could serve as a positive predictor of long-term lithium efficacy, and whether robust response to ketamine might predict lower probability of lithium maintenance success. The implications of such a relationship, if proven, would be highly significant. The rapid antidepressant effect of ketamine offers a unique opportunity to biologically “test” a patient’s treatment responsiveness within days, whereas evaluating lithium’s prophylactic effect requires months to years of observation. If a brief ketamine infusion series could reliably indicate whether a patient is more or less likely to respond to prophylactic lithium, the efficiency of long-term treatment decisions in BD could be greatly improved.
Up front, it is important to consider that an important methodological consideration arises from the inclusion criteria of most clinical trials of ketamine in bipolar depression. Specifically, that by the nature of studying treatment-resistant samples, the inclusion criteria will increase the probability that included patients had failed to respond to multiple prior pharmacologic interventions, including mood stabilizers such as lithium. As a result, these study populations may be likely enriched for individuals who are already known or presumed to be lithium non-responders. This could create a systematic sampling bias limiting the generalizability of findings and obscuring potential inverse relationships between ketamine and lithium response. Thus, we considered it important to consider the degree to which lithium and ketamine show overlapping vs. distinct preclinical mechanisms of action in order to evaluate their common and differential effects in patients with BD. This paper therefore presents a scoping review of the clinical and preclinical evidence supporting or refuting this proposed link between ketamine response and lithium maintenance outcomes in BD.
2. Methods
2.1. Data Collection
The Scopus database was searched from its inception until April 26th, 2025, using the following search query:
TITLE-ABS-KEY( ketamine AND (lithium OR anticonvuls* OR antipsychot* OR mood-stabiliz* OR (mood PRE/0 stabiliz*)) AND (bipolar OR depress*)). Additionally, reference lists from related reviews, commentaries, and editorials were manually examined to identify additional potentially relevant publications for inclusion.
2.2. Screening Process
Two authors (J.T. & A.N.) independently assessed titles and abstracts of the retrieved articles for potential inclusion. Conflicts were resolved via consensus discussion. One author (J.T.) then assessed full-text papers published in English for final inclusion. Articles were included in the present review if they met the following criteria: (1) Clinical trials that investigated the use of ketamine and a mood stabilizer in the treatment of bipolar depression, and which reported depressive symptom severity ratings over time; (2) Studies that administered ketamine in combination with a mood stabilizer to animals; (3) Preclinical translational studies that explored the mechanistic relationship between ketamine and mood stabilizers, examining both overlapping and distinct mechanisms; (4) Studies that specifically evaluated clinical predictors of ketamine response. Reviews, commentaries, and editorial articles were not eligible for inclusion in the present review. We included studies of other prophylactic treatments such as lamotrigine and clozapine in order to further explore the mechanistic overlap and divergence between ketamine, lithium, and these other prophylactic agents.
For all studies, data extracted by J.T. included study information (e.g., author, publication details), participant/animal population, study design, intervention details, and relevant depressive outcomes. Study data were then categorized, summarized, and qualitatively synthesized by the study team.
3. Results
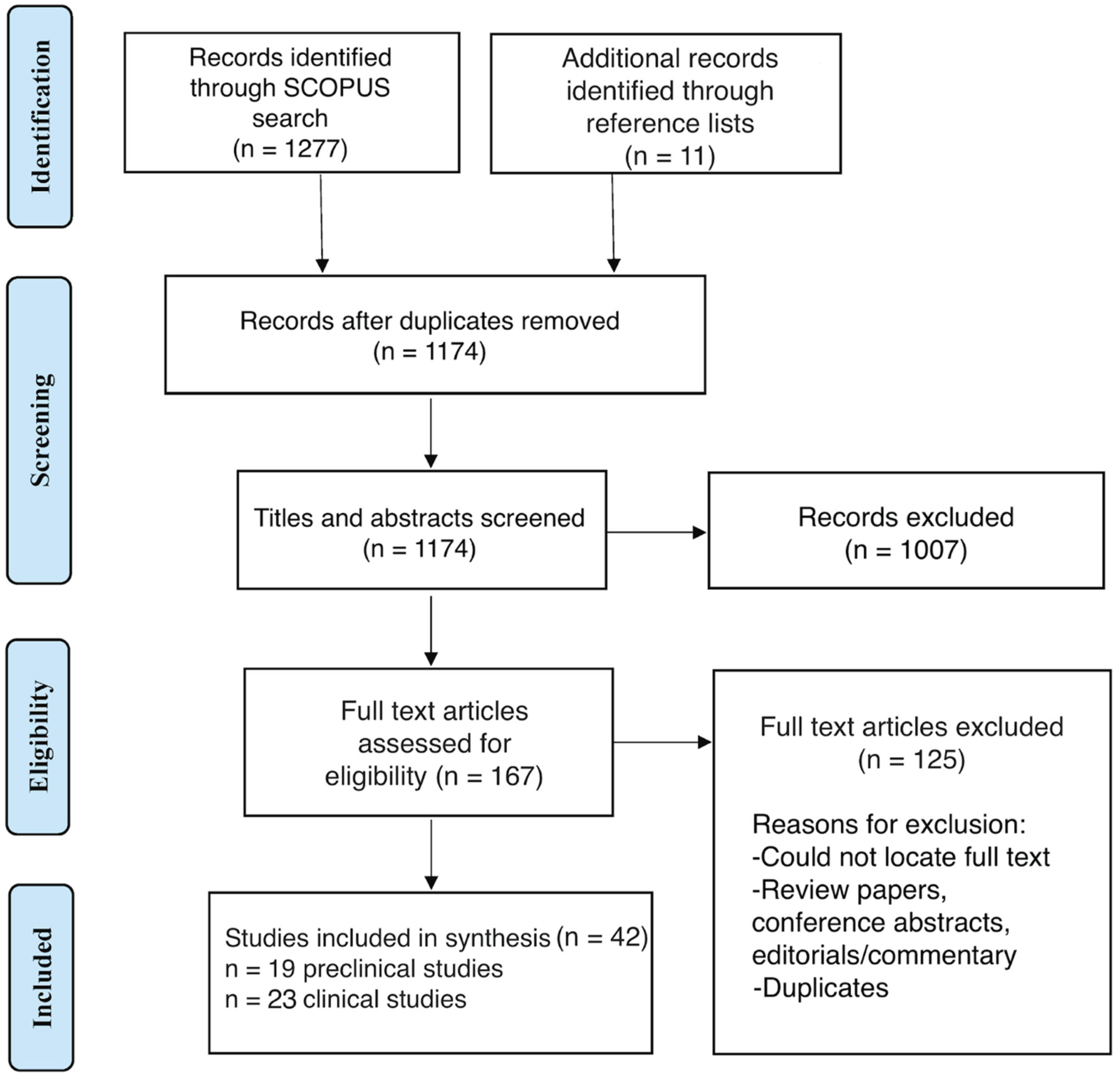
The initial search yielded a total of 1277 records, with 11 additional records identified from relevant reference lists (Figure 1). After removing 114 duplicates, 1174 records were screened for relevance based on titles and abstracts, with 1007 excluded at this stage. Following full-text review of 167 articles, 125 studies were excluded based on the eligibility criteria previously outlined. In total, 42 records that met the inclusion criteria were included in the qualitative synthesis, 19 of which were preclinical studies and 23 of which were clinical studies.
3.1. Preclinical Studies
3.1.1. Lithium Augmentation of the Rapid Antidepressant Effect of Ketamine
Chiu et al. [20] showed that a single high-dose ketamine (50 mg/kg delivered intraperitoneally [i.p.]) reverses depressive-like behavior in chronically stressed mice (measured as a reduction of immobility in forced swim and tail suspension tests). However, this antidepressant effect is transient and accompanied by increased oxidative stress markers in the brain. Notably, low-dose lithium given before ketamine enabled a previously ineffective subthreshold ketamine dose (2.5 mg/kg) to produce antidepressant-like behavioral effects. Likewise, lithium delivered post-ketamine (at therapeutic levels) sustained ketamine’s antidepressant action and synaptic enhancements for at least 2 weeks. Furthermore, Chiu et al. found that lithium pretreatment completely abolished ketamine-induced oxidative damage (lipid peroxidation, glutathione oxidation) in the stressed mouse brain [20]. Mechanistically, lithium enhanced ketamine-mediated activation of the mTOR–BDNF pathway in the prefrontal cortex, resulting in increased dendritic spine density associated with antidepressant response. This suggests that combining ketamine with lithium can both potentiate the acute antidepressant effect and limit ketamine-related adverse oxidative stress, aligning with a “proof-of-concept” for using lithium to maintain ketamine responders. With respect to the question approached by the present study, the results of Chiu et al. [20] support alignment, and not divergence of ketamine’s and lithium’s mechanisms of action.
Ketamine’s antidepressant action may be related to GSK-3β inhibition and consequent increases in synaptic plasticity. Liu et al. [21] demonstrated that blocking GSK-3, either with lithium or a selective inhibitor, markedly potentiates ketamine’s effects at low doses. In their study, a normally subthreshold ketamine dose produced robust antidepressant-like effects only when combined with lithium/GSK-3 inhibitor, resulting in rapid mTORC1 activation, elevated BDNF–TrkB signaling, and increased density/strength of synaptic spines. The combination (low dose ketamine + lithium) was as effective as a higher ketamine dose alone, highlighting GSK-3 as a mediator of ketamine’s synaptogenic and behavioral effects. As a clinical corollary, this may also support a treatment strategy for patients who may not be able to tolerate normally therapeutic ketamine doses (i.e., potentiation with a low dose of lithium). In line with this, do Vale et al. [22] found that lithium (5 mg/kg) synergized with ketamine to enhance antidepressant outcomes and anti-inflammatory signaling. Low-dose ketamine (2 mg/kg) had only modest effects on forced-swim immobility, but when paired with lithium it yielded a reduction in immobility time comparable to a 10 mg/kg ketamine dose. This combination also potentiated ketamine-mediated reduction of pro-inflammatory markers (TNF-α, iNOS, COX-2) and increased inhibitory GSK-3β phosphorylation in peripheral tissue. These findings suggest that GSK-3 inhibition is a critical mechanism that boosts ketamine-driven antidepressant response and synaptic plasticity.
Recent data implicate insulin–Akt signaling in ketamine’s sustained antidepressant effect. In a rodent model of ketamine treatment-resistant depression, Price et al. [23] showed that adding lithium to ketamine not only reduced immobility time and increased latency to immobility in the forced swim test, but also uniquely upregulated insulin pathway signaling. Rats receiving ketamine and lithium had significantly higher plasma insulin levels and mTOR activation, along with increased phosphorylation of insulin-linked kinases (Akt) in the prefrontal cortex. Blood insulin levels correlated inversely with depression-like immobility in these animals receiving both ketamine and lithium (i.e., higher insulin predicted greater antidepressant response). Increased insulin signaling in infralimbic PFC also correlated with the behavioral improvement. These results suggest lithium’s augmentation may recruit metabolic signaling pathways to support antidepressant effects.
At the circuit level, ketamine’s antidepressant action appears to be related to its acute psychotomimetic effects. For example, Maltbie et al. [24] used fMRI in awake nonhuman primates to map ketamine-induced brain activation. Ketamine infusion broadly increased BOLD activation, with the strongest activations in the cingulate gyrus, supplementary motor area (SMA), and thalamus, but this was reduced in both extent and magnitude by risperidone pretreatment. Interestingly, there was no deactivation of the subgenual cingulate observed. It is thus possible that disinhibition of PFC networks is a shared mechanism for the rapid antidepressant effect of ketamine and its transient psychotic symptoms. The lack of effect of acute antipsychotic effects of lithium in humans may thus suggest that divergence in effect of ketamine and lithium could relate to mechanisms related to psychotomimesis.
Further circuit-related findings suggest that ketamine and lithium may overlap in their effects on stress-related brain circuits. Specifically, in a study of rats by Stepan et al. [25] using hippocampal slice imaging, the authors found that chronic stress impairs propagation of neural activity through the hippocampus, whereas lithium, ketamine, and BDNF ameliorate this impairment. Such findings suggest that ketamine and lithium both reinforce synaptic connectivity in stress-sensitive circuits, further supporting convergent mechanistic targets for these agents.
3.1.2. Studies Related to Ketamine as a Preclinical Model of Mania/Psychosis
Repeated low-dose ketamine in rodents can produce hyperactivity and dysregulation thought to be analogous to manic episodes. This ketamine-induced “mania-like” behavior is typically characterized by increased locomotor activity, risk-taking, and dysregulated neurotransmitter signaling. A consistent finding across such studies is that ketamine triggers oxidative stress and inflammation in brain regions involved in mood regulation (prefrontal cortex, hippocampus, striatum), and therefore many interventions that prevent ketamine’s “mania-like” side-effects are thought to have potent antioxidant or neuroprotective properties.
For example, a series of studies from Gazal and colleagues explored dietary antioxidants as prophylactics in a ketamine mania model. In multiple studies, pre-treatment with lithium or a blueberry extract markedly protected rats against ketamine-induced hyperlocomotive and oxidative/inflammatory effects in cortex, striatum, and hippocampus [26,27]. Similar to lithium, pretreatment with an extract from blackberry (another anthocyanin-rich berry) could attenuate ketamine-induced hyperlocomotion and brain oxidative stress markers [28]. Pretreatment with curcumin [29] (the active component of turmeric), an extract of Cecropia pachystachya [30] (a traditional medicinal plant which the authors cite has been associated with sedative, antioxidant, hypoglycemic, anti-inflammatory, and cytotoxic activities), or gallic acid [31] (a polyphenolic compound found in plants, fruits, wine, and green tea which has antitumour, antiviral, and neuroprotective properties) have also been shown to limit ketamine’s hyperlocomotive effects and oxidative/inflammatory markers, particularly in the cortex, hippocampus, and striatum, to a degree similar to pretreatment with lithium. Gallic acid (like lithium) was also able to normalize acetylcholinesterase activity in the hippocampus and striatum, countering ketamine’s increase of acetylcholinesterase activity [31]. However, in another study, ederavone (a potent free-radical scavenger which exhibits antioxidant activity by inhibition of hydroxyl radical-dependent and radical-independent lipid peroxidation), unlike lithium, failed to prevent hyperlocomotion in the open-field test [32]. Given that edaravone functions by inhibition of lipid peroxidation, its lack of effect in this study may have been attributable to the ketamine not inducing increases in TBARS, although the reason for this is unclear in this specific study. Taken together, these findings suggest that lithium and ketamine may diverge in the degree to which they affect oxidative/inflammatory responses, with lithium and other antioxidants particularly limiting ketamine’s hyperlocomotive effects (i.e., the model for mania). However, the degree to which the hyperlocomotive effects are necessary to observe an acute antidepressant effect of ketamine is unclear.
Beyond oxidative/inflammatory pathways, lithium may limit ketamine-induced hyperlocomotion through other mechanisms. For example lithium has been shown to limit widespread ketamine-induced forebrain activation (measured by c-FOS expression, which is a marker of a neural firing) in limbic regions such as the hippocampus, amygdala, lateral septum, and hypothalamus [33], suggesting that lithium can dampen aberrant circuit excitability underlying ketamine’s “mania-like” effect, potentially explaining lithium’s clinical antimanic efficacy. To some degree, lithium related attenuation of ketamine induced hyperlocomotion may be related to lithium downregulating PI3K-AKT signalling in mPFC [34]. That same study found that pharmacological inhibition of mTOR (with rapamycin) had no effect on hyperlocomotion [34]. It is therefore possible that lithium counteracts ketamine’s hyperlocomotive effects not only via antioxidant mechanisms mentioned in the previous section, but also via dampening of neural excitability, potentially via activity in the PI3K-AKT pathway.
To better understand the convergence and divergence of the effects of ketamine and lithium, it is also important to examine the mechanisms of alternative mood stabilizers, and antipsychotics when co-administered with ketamine. For example, lamotrigine has been found to prevent ketamine-induced deficits in prepulse inhibition (PPI), which is an operational measure of sensorimotor gating that is reduced in mania and schizophrenia [35]. Interestingly, in that study, lamotrigine did not reduce amphetamine-induced PPI deficit, implying that lamotrigine specifically antagonizes glutamate/NMDA-related gating disturbance (i.e., ketamine’s PPI effect) but not dopamine-driven PPI deficit (i.e., due to amphetamine). Clinically, this may align with lamotrigine’s efficacy in bipolar maintenance, supporting a glutamatergic modulation role in normalizing circuit function. On the other hand, the atypical antipsychotic clozapine may reverse hippocampal-prefrontal impairments in long term potentiation (LTP) induced by administration of ketamine [36]. Interestingly, in that study, while both ketamine and clozapine increased phospho-GSK3β in PFC, clozapine uniquely increased GluA1 phosphorylation in PFC and hippocampus (enhancing AMPA channel conductance at those sites). This pattern indicates an interesting overlap between ketamine, clozapine, and lithium with respect to effects on GSK3β, while indicating that clozapine and lamotrigine’s effects on countering ketamine-related mania/psychosis may be mediated by effects on glutamatergic transmission.
On the EEG level, Bowman et al. [37] used freely moving rats to examine how clozapine and another modulator, naltrexone, influence ketamine-induced network oscillations. Ketamine alone produced distinct resting-state EEG abnormalities, including a reduction in low-beta power and an increase in gamma and high-frequency oscillations during resting states (identified via head-mounted accelerometers). Interestingly, clozapine and naltrexone had differential reversal effects depending on EEG frequency band and behavioral state. During inactivity, clozapine restored the diminished beta power and potentiated ketamine’s gamma and high-frequency oscillation increases. In contrast, naltrexone suppressed the ketamine induced high-frequency oscillation increase. The clinically important implication of this study is that ketamine’s EEG signature of psychosis vs. antidepressant response might be separable. Specifically, clozapine reversed the low-beta deficit, which may be related to its antipsychotic action, whereas naltrexone (which in human patients blocks ketamine’s antidepressant and anti-suicidal effects) [38] specifically blunted the high-frequency oscillation component, which may thus be a marker of ketamine’s antidepressant action.
3.2. Clinical Studies
3.2.1. Rapid Antidepressant Efficacy in Mood Disorders (Clinical Outcomes)
Ketamine has demonstrated significant antidepressant effects in both treatment-resistant bipolar and unipolar depression. In the first randomized placebo controlled trial in bipolar depression, a single sub-anesthetic IV dose of ketamine (0.5 mg/kg) administered to patients receiving stable levels of lithium or valproate produced significantly improved depressive symptoms within 40 minutes, with 71% of patients responding at 2 weeks (compared to only 6% in the placebo arm) [39]. There was no treatment response stratification by lithium or valproate treatment status. A replication study confirmed these findings [40], and overall these add-on trials (with patients maintained on lithium or valproate throughout) indicate that ketamine’s efficacy is compatible with concurrent mood stabilizer therapy. Furthermore, no relationship has been found between blood levels of lithium or valproate and the antidepressant response to ketamine [41] (although this study may have been underpowered). An open-label clinical series in 53 patients with bipolar depression on stable mood stabilizers further corroborated the effectiveness of ketamine, with no clear stratification of response across bipolar subtypes and illness histories, number of prior episodes, or concomitant lithium/quetiapine use [42]. Still another study found that lithium or anticonvulsant use was unrelated to response trajectories in patients with severe depression (in a mixed sample of unipolar and bipolar depression) [43]. Taken together, these studies suggest that acute antidepressant effects of ketamine are not affected by mood stabilizer use.
3.2.2. Symptom Subtypes and Clinical Predictors of Response
Interestingly, ketamine’s antidepressant efficacy may differ depending on depression subtype. In an observational study of 97 patients with treatment-resistant depression, Wang et al. [14] found that those with melancholic features were significantly less likely to respond or achieve remission, and improved more slowly, from 6 ketamine infusions compared to patients with anxious or non-melancholic depression. These findings suggest that patients with melancholic features might require additional measures or may respond less robustly to ketamine’s antidepressant mechanism, whereas those with significant anxious distress (at least in the absence of melancholic signs) could be particularly good candidates for ketamine therapy. This is of particular interest given that prior studies have suggested that melancholic features during depression may predict favourable outcomes with lithium prophylaxis [44], indicating a further clinical divergence between predictors of lithium and ketamine response, respectively. Similarly, in bipolar depression, anxiety comorbidity does not appear to diminish ketamine’s efficacy. A post-hoc analysis focusing on bipolar patients with high baseline anxiety found that patients with anxious bipolar depression (n=21) derived a similar magnitude and timing of benefit from ketamine as those with non-anxious (n=15) bipolar depression [45]. This efficacy of ketamine in anxious bipolar depression indicates it may bypass some of the limitations of conventional treatments in these populations.
Beyond mood subtype, other clinical factors like personality and trauma history have emerged as potential moderators of ketamine response. A recent study of intranasal ketamine (esketamine) in depressed inpatients reported that patients with a co-morbid personality disorder (the most common of which was borderline personality disorder) had a significantly lower response rate to ketamine, whereas patients with a history of childhood trauma had a higher likelihood of responding [46]. Although this study was (A) exploratory in nature and prone to the risk of uncorrected multiple comparisons, and (B) inclusive of a mixed unipolar/bipolar sample, it poses an interesting further potential contrast between the clinical predictors of response to IV ketamine and prophylactic lithium therapy, since it is well known that histories of childhood trauma are predictive of poorer prophylactic response to lithium [47]. Given that there is some evidence that childhood maltreatment may not deter responsiveness to anticonvulsant mood stabilizers, it is of potential interest to consider whether acute ketamine antidepressant response may be subsequently differentially predictive of response to prophylactic anticonvulsant therapy [48].
An analysis by Pennybaker et al.[49] examined what clinical features distinguished longer-lasting (what they called “extended”) antidepressant responses to ketamine, finding that extended responders (A) were more likely to have a family history of alcohol use disorder in first-degree relatives, and (B) experience greater acute dissociation during the ketamine infusion [49]. Another study found that ketamine responders may have a higher intra-infusion increase in systolic blood pressure compared to non-responders, although the effect on duration of response was not reported [50]. No clinical predictors that are known to influence prophylactic lithium response in bipolar disorder were identified. Thus, it remains unclear whether the duration of ketamine’s antidepressant response provides any information about the likelihood of subsequent prophylactic lithium response. There has also been mixed evidence of clinical laboratory measures predicting response to ketamine [51,52], with no known overlap with predictors of lithium response.
3.2.3. Adjunctive Treatments to Sustain Ketamine’s Effects
Because ketamine’s antidepressant benefit is often transient, adjunctive strategies to prolong its effect have been tested. A randomized controlled trial in TRD investigated lithium continuation following ketamine response in patients with treatment resistant unipolar depression. Specifically, Costi et al. [53] found that lithium (mean plasma level 0.61 mEq/L, with mean dosage of 800mg/day) offered no advantage over placebo in maintaining antidepressant response by day 28, with nearly identical MADRS scores across groups. This suggests that lithium alone, started immediately after ketamine, does not reliably prevent early relapse. By contrast, in a 5-year observational follow-up study in n=16 patients, Amiaz et al. [54] found that patients receiving quetiapine experienced a longer time until relapse compared to patients receiving other neuroleptics. Patients (a mixed sample of unipolar and bipolar disorder) who received ketamine while on quetiapine had a median time to relapse of ~966 days compared to ~80 days for those on other antipsychotics (aripiprazole, olanzapine, ziprasidone, perphenazine, and clozapine).
3.2.4. Neuroimaging and Neurophysiological Mechanisms
Neuroimaging studies have suggested that ketamine’s antidepressant response in BD may be related to rapid reorganization of brain networks. In a PET imaging study of depressed bipolar patients who did not respond to 4 week trials of either lithium or valproate, and who subsequently underwent a double-blind crossover trial of ketamine vs. saline placebo, Nugent et al. [55] showed that antidepressant responders exhibited the greatest post-infusion increases in ventral striatal metabolism, while higher activity in the subgenual anterior cingulate cortex (sgACC) following the placebo infusion predicted greater symptom relief following ketamine. Along these lines, resting-state fMRI findings in patients with MDD have found that ketamine responders showed lower baseline functional connectivity between the lateral prefrontal cortex and the sgACC, as well as larger increases following treatment. Indeed, Chen et al. [56] also found that patients with treatment resistant depression showed lower fronto-striatal functional connectivity, and that the magnitude of this connectivity was inversely related to the degree of antidepressant improvement following IV ketamine [56]. Furthermore, in a repeated-infusion protocol, patients with unipolar depression who responded to IV ketamine demonstrated elevated baseline resting state functional connectivity between various regions and the amygdala [57]. These differences may be related to oscillatory patterns of activity in depression, since Cao et al. [58] reported that responders to IV ketamine showed lower frontal power in theta band at baseline, but higher treatment related increases in alpha power, as well as lower alpha asymmetry and theta cordance. The degree to which these findings are associated with prophylactic response to lithium is unclear to us, since we are unaware of evidence demonstrating that functional connectivity and EEG-biomarkers serve as reliable markers of prophylactic mood stabilizer response.
3.2.5. Peripheral Biomarkers and Molecular Pathways
One striking finding involves ketamine’s effect on the glutamate–mTOR signaling pathway, which is involved in synaptic plasticity, and may be a significant mediator of ketamine’s antidepressant action. In a small study of 27 depressed women, Berner et al. [59] found that higher baseline levels of phosphorylated p70S6 kinase (p70S6K, a downstream effector of mTORC1 whose phosphorylation levels served as a proxy for MTORC1 activation in monocytes) were correlated with better antidepressant outcomes from ketamine, although the study used a machine learning method that in such a small sample would be prone to overfitting. Notwithstanding this limitation, the implication here may be that individuals with higher baseline MTORC1 activity may be potentially more “primed” to respond to the antidepressant effects of ketamine, which involves synaptogenesis and may depend on mTOR-mediated pathways. mTOR may also serve as a convergence point between the acute antidepressant effects of ketamine and the longer-term prophylactic effects of lithium in bipolar disorder, since a key mechanism of the latter involves GSK3β inhibition, an upstream regulator of mTOR activity.
In a placebo-controlled clinical study, a single ketamine infusion significantly increased vascular endothelial growth factor A (VEGFA) gene expression in whole blood of depressed patients compared to a midazolam (sedative) control [60]. Ketamine also selectively increased the ratio of VEGFA to its anti-angiogenic counterpart PEDF (pigment epithelial–derived factor, with gene name SERPINF1) in peripheral blood, measured about 4 hours post-infusion [60]. The specificity of these biomarker changes in the ketamine infusion group may suggest that ketamine engages pro-angiogenic growth factor signalling. Interestingly, in rats, it has been demonstrated that lithium promotes VEGF expression in brain endothelium and astrocytes [61].
In a study by Permoda-Osip et al. [52] of 42 depressed patients, personal/family history of alcohol abuse, elevated serum vitamin B12 concentrations, and elevated serum vascular endothelial growth factor predicted response to ketamine. Villaseñor et al. [62] found that lysophosphatidylethanolamines and lysophosphatidylcholines were increased in ketamine responders relative to non-responders in a sample of patients with bipolar depression, suggesting that mitochondrial fatty acid metabolism may predict response to ketamine. Słupski et al. [63] showed that repeated ketamine infusions decreased serum copper concentrations in depressed patients, though no clear connection to treatment response was found. Reduced copper concentrations may be due to a reduction in the acute phase response, further suggesting ketamine exerts anti-inflammatory effects.
4. Discussion
This review examined the relationship between acute antidepressant effects of ketamine and long-term prophylactic outcomes with lithium in bipolar disorder (BD). We found that while ketamine and lithium share convergent molecular targets that enhance structural plasticity, their clinical predictors of efficacy largely diverge. In this section, we synthesize this evidence, attempt to consider why such divergence may exist, and discuss implications for clinical prediction and the design of future studies leveraging ketamine response to predict prophylactic response to lithium.
Ketamine and lithium ultimately act on overlapping molecular pathways implicated in neuroplasticity. Ketamine produces rapid antidepressant effects through NMDA receptor antagonism, resulting in glutamate surges and AMPA receptor activation, and ultimately downstream mTORC1–BDNF signaling, which together promote rapid synaptogenesis [64,65]. Over a longer time-scale, lithium exerts pro-synaptic effects via GSK-3β inhibition, disinhibiting mTOR and supporting neurotrophic and gene-expression changes that sustain long-term mood stabilization [20,66]. Rodent studies have suggested that these mechanisms may compound eachother’s effects. Indeed, lithium potentiates and prolongs the antidepressant effects of subthreshold ketamine doses, and reduces ketamine-induced oxidative stress [20,21,22]. Both agents upregulate phosphorylation of GSK-3β and mTOR in the prefrontal cortex, reinforcing structural plasticity [20]. As a result, lithium attenuates ketamine-induced hyperlocomotion and limbic hyperactivation, potentially consistent with its anti-manic effects in humans [33,34]. These findings support a shared capacity to enhance synaptic strength and, especially for lithium, protect against excitotoxicity, suggesting some mechanistic overlap among biological responders. In terms of clinical overlap in function, it is notable that both agents reduce suicidal ideation, albeit over different time scales (ketamine within hours [40,67] and lithium across years of maintenance [68]). A corollary question that arises from this overlap therefore concerns the degree to which synaptic plasticity is involved in the pathophysiology of suicidal ideation and behaviour.
Despite the aforementioned clinical overlaps, the clinical phenotypes of ketamine and lithium responders differ significantly. Excellent lithium responders typically present with “classical” BD, characterized by episodic euphoric manias, discrete illness episodes, complete inter-episode remission, later onset, and strong family history [69,70]. This stands in stark contrast to the atypical clinical phenotypes that are ostensibly characteristic of ketamine responders and lithium non-response. Indeed, while high body mass index (BMI) ostensibly predicts ketamine response [17,71], factors such as insulin resistance and metabolic syndrome are associated with chronic course of BD and lithium non-response [10,72]. Similarly, while comorbid anxiety and mixed features limit lithium prophylaxis [4,6,9], they are associated with positive ketamine response [15,16]. Childhood trauma predicts poor lithium outcomes [47] but may enhance ketamine responsiveness [46]. Finally, depression subtypes diverge: melancholic features favor lithium [44], whereas non-melancholic or anxious depressions respond preferentially to ketamine [14]. Taken together, these findings suggest that ketamine responders are overrepresented with respect to the features that portend worse prognosis for longer-term prophylactic lithium responsiveness.
Ultimately, our review failed to identify clear preclinical evidence explaining the divergent phenotypic profiles of responders to acute ketamine treatment and long-term lithium prophylaxis. Animal models reliably show that ketamine produces rapid acute antidepressant effects which can be extended or modulated by lithium, but do not provide clinically-relevant approaches to identify whether and which ketamine responders are less likely to benefit from lithium prophylaxis. For example, while oxidative stress and inflammatory changes accompany ketamine’s behavioral effects in rodents [26,27,28], these findings do not straightforwardly map onto the clinical observation that ketamine responders often show the phenotypic predictors of lithium non-responders. Similarly, while insulin and metabolic pathways are implicated in both ketamine and lithium’s actions [23], animal studies do not yet clarify why metabolic dysregulation (e.g., high BMI) would favor acute ketamine response but undermine lithium prophylaxis [10].
One possible explanation for our failure to reconcile the preclinical and clinical data is that preclinical models largely capture acute effects of ketamine and lithium, such as how lithium extends the duration of the antidepressant effect of ketamine or counteracts ketamine-induced hyperlocomotion. By contrast, the clinical divergence in response emerges over years of illness course (since lithium responsiveness requires more than 1-2 years to elucidate), reflecting potential differences in understanding the mechanisms of long-term disease stabilization versus the mechanisms of short-term symptom relief. Unfortunately, animal models are not well-suited to capture these long-horizon prophylactic outcomes. This limits our ability to test hypotheses about divergent predictors of response at the biological level. Thus, while the clinical data suggest an inverse predictive relationship between ketamine response and prophylactic lithium response, the preclinical literature remains largely neutral on this matter.
Several limitations must be acknowledged. First, no clinical study has directly tested ketamine response as a predictor of lithium prophylaxis, so all inferences remain indirect. Secondly, many of the clinical studies included herein included mixed unipolar/bipolar samples, which were not disentangled in post-hoc analyses. Third, ketamine trials are likely enriched for treatment-resistant patients, implying that they may contain a higher proportion of lithium non-responders, which may inflate the appearance of divergence. Furthermore, many predictor studies, both for ketamine and lithium, are small, underpowered, and heterogeneous in design, complicating interpretation. Finally, one must also note that preclinical studies, while mechanistically valuable, cannot model the full complexity of BD or the longitudinal trajectories that are required to understand prophylactic lithium response, limiting their utility in understanding this critical element of disease management in humans.
To resolve these uncertainties, prospective, longitudinal studies must be conducted in which individuals with BD who have received acute courses of ketamine for depression are followed prospectively while receiving lithium prophylaxis. Incorporating biomarkers such as inflammatory and metabolic measures, neuroimaging, and electrophysiology may help link clinical observations to mechanistic pathways, and induced pluripotent stem-cell based assays may help qualify overlapping and diverging mechanistic pathways at the individual level [73,74,75,76,77]. Preclinical work should additionally focus on developing animal models of the longitudinal relapsing and remitting trajectory of BD, in order to better understand prophylaxis. Ultimately, such studies would serve to determine whether ketamine response, which could be a rapid and easily identified predictor, predicts poor lithium prophylaxis, thereby potentially saving patients the trouble and side-effects of years of ineffective trials of prophylactic therapy. This could help us establish control over the disease early, and improving morbidity and mortality in this patient population who are often struck by BD in the prime years of their lives.
Author Contributions
JT and AN conducted the data collection and screening, as well as manuscript preparation. JEAC assisted with manuscript edits.
Conflicts of Interest
JEAC—none; JT—none; AN—Funding received by the QEII Foundation (Translating Research Into Care [TRIC] Grant), Nova Scotia Health Research Fund, Nova Scotia Health Innovation Catalyst Fund, and the Canadian Institutes of Health Research.
References
- Yatham L, Kennedy S, Parikh S, Schaffer A, Bond D, Frey B, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disorders. 2018;20, 97–170. [CrossRef]
- Grof P. Sixty Years of Lithium Responders. Neuropsychobiology. 2010 May 7;62, 8–16. [CrossRef]
- Garnham J, Munro A, Slaney C, MacDougall M, Passmore M, Duffy A, et al. Prophylactic treatment response in bipolar disorder: Results of a naturalistic observation study. Journal of Affective Disorders. 2007;104(1–3):185–90. [CrossRef]
- Nunes A, Ardau R, Berghöfer A, Bocchetta A, Chillotti C, Deiana V, et al. Prediction of lithium response using clinical data. Acta Psychiatrica Scandinavica. 2020;141, 131–41. [CrossRef]
- Scott K, Khayachi A, Alda M, Nunes A. Prediction of Treatment Outcome in Bipolar Disorder: When Can We Expect Clinical Relevance? Biological Psychiatry. 2025 Aug 15;98, 285–92. [CrossRef]
- Nunes A, Stone W, Ardau R, Berghöfer A, Bocchetta A, Chillotti C, et al. Exemplar scoring identifies genetically separable phenotypes of lithium responsive bipolar disorder. Transl Psychiatry. 2021 June;11, 36. [CrossRef]
- Gershon S, Chengappa K, Malhi G. Lithium specificity in bipolar illness: A classic agent for the classic disorder. Bipolar Disorders. 2009;11(SUPPL. 2):34–44. [CrossRef]
- Hui TP, Kandola A, Shen L, Lewis G, Osborn DPJ, Geddes JR, et al. A systematic review and meta-analysis of clinical predictors of lithium response in bipolar disorder. Acta Psychiatr Scand. 2019 Aug;140, 94–115. [CrossRef]
- Lin Y, Maihofer AX, Stapp E, Ritchey M, Alliey-Rodriguez N, Anand A, et al. Clinical predictors of non-response to lithium treatment in the Pharmacogenomics of Bipolar Disorder (PGBD) study. Bipolar Disorders. 2021;23, 821–31. [CrossRef]
- Calkin CV, Ruzickova M, Uher R, Hajek T, Slaney CM, Garnham JS, et al. Insulin resistance and outcome in bipolardisorder. The British Journal of Psychiatry. 2015 Jan;206, 52–7.
- Fancy F, Haikazian S, Johnson DE, Chen-Li DCJ, Levinta A, Husain MI, et al. Ketamine for bipolar depression: an updated systematic review. Ther Adv Psychopharmacol. 2023 Sept 26;13:20451253231202723. [CrossRef]
- Kraus C, Rabl U, Vanicek T, Carlberg L, Popovic A, Spies M, et al. Administration of ketamine for unipolar and bipolar depression. International Journal of Psychiatry in Clinical Practice. 2017 Jan 2;21, 2–12. [CrossRef]
- Lam RW. Onset, time course and trajectories of improvement with antidepressants. European Neuropsychopharmacology. 2012 Jan 1;22:S492–8. [CrossRef]
- Wang C, Zhou Y, Zheng W, Liu W, Zhan Y, Li H, et al. Association between depression subtypes and response to repeated-dose intravenous ketamine. Acta Psychiatrica Scandinavica. 2019;140, 446–57. [CrossRef]
- Ionescu DF, Luckenbaugh DA, Niciu MJ, Richards EM, Zarate CA. A single infusion of ketamine improves depression scores in patients with anxious bipolar depression. Bipolar Disord. 2015 June;17, 438–43. [CrossRef]
- McIntyre RS, Lipsitz O, Rodrigues NB, Lee Y, Cha DS, Vinberg M, et al. The effectiveness of ketamine on anxiety, irritability, and agitation: Implications for treating mixed features in adults with major depressive or bipolar disorder. Bipolar Disorders. 2020;22, 831–40. [CrossRef]
- Rong C, Park C, Rosenblat JD, Subramaniapillai M, Zuckerman H, Fus D, et al. Predictors of Response to Ketamine in Treatment Resistant Major Depressive Disorder and Bipolar Disorder. Int J Environ Res Public Health. 2018 Apr 17;15, 771. [CrossRef]
- Hui T, Kandola A, Shen L, Lewis G, Osborn D, Geddes J, et al. A systematic review and meta-analysis of clinical predictors of lithium response in bipolar disorder. Acta Psychiatrica Scandinavica. 2019;140, 94–115. [CrossRef]
- McIntyre RS, Lipsitz O, Rodrigues NB, Lee Y, Cha DS, Vinberg M, et al. The effectiveness of ketamine on anxiety, irritability, and agitation: Implications for treating mixed features in adults with major depressive or bipolar disorder. Bipolar Disorders. 2020;22, 831–40. [CrossRef]
- Chiu CT, Scheuing L, Liu G, Liao HM, Linares GR, Lin D, et al. The Mood Stabilizer Lithium Potentiates the Antidepressant-Like Effects and Ameliorates Oxidative Stress Induced by Acute Ketamine in a Mouse Model of Stress. International Journal of Neuropsychopharmacology. 2015 Apr 1;18, pyu102. [CrossRef]
- Liu RJ, Fuchikami M, Dwyer JM, Lepack AE, Duman RS, Aghajanian GK. GSK-3 Inhibition Potentiates the Synaptogenic and Antidepressant-Like Effects of Subthreshold Doses of Ketamine. Neuropsychopharmacol. 2013 Oct;38, 2268–77. [CrossRef]
- do Vale EM, Xavier CC, Nogueira BG, Campos BC, de Aquino PEA, da Costa RO, et al. Antinociceptive and Anti-Inflammatory Effects of Ketamine and the Relationship to Its Antidepressant Action and GSK3 Inhibition. Basic & Clinical Pharmacology & Toxicology. 2016;119, 562–73. [CrossRef]
- Price JB, Yates CG, Morath BA, Van De Wakker SK, Yates NJ, Butters K, et al. Lithium augmentation of ketamine increases insulin signaling and antidepressant-like active stress coping in a rodent model of treatment-resistant depression. Transl Psychiatry. 2021 Nov 25;11, 1–12. [CrossRef]
- Maltbie E, Gopinath K, Urushino N, Kempf D, Howell L. Ketamine-induced brain activation in awake female nonhuman primates: a translational functional imaging model. Psychopharmacology (Berl). 2016 Mar;233, 961–72. [CrossRef]
- Stepan J, Hladky F, Uribe A, Holsboer F, Schmidt MV, Eder M. High-Speed imaging reveals opposing effects of chronic stress and antidepressants on neuronal activity propagation through the hippocampal trisynaptic circuit. Front Neural Circuits. 2015 Nov 6;9:70. [CrossRef]
- Debom G, Gazal M, Soares MSP, do Couto CAT, Mattos B, Lencina C, et al. Preventive effects of blueberry extract on behavioral and biochemical dysfunctions in rats submitted to a model of manic behavior induced by ketamine. Brain Research Bulletin. 2016 Oct 1;127:260–9. [CrossRef]
- Spohr L, Soares MSP, Oliveira PS, da Silveira de Mattos B, Bona NP, Pedra NS, et al. Combined actions of blueberry extract and lithium on neurochemical changes observed in an experimental model of mania: exploiting possible synergistic effects. Metab Brain Dis. 2019 Apr;34, 605–19. [CrossRef]
- Chaves VC, Soares MSP, Spohr L, Teixeira F, Vieira A, Constantino LS, et al. Blackberry extract improves behavioral and neurochemical dysfunctions in a ketamine-induced rat model of mania. Neuroscience Letters. 2020 Jan 1;714:134566. [CrossRef]
- Gazal M, Valente MR, Acosta BA, Kaufmann FN, Braganhol E, Lencina CL, et al. Neuroprotective and antioxidant effects of curcumin in a ketamine-induced model of mania in rats. European Journal of Pharmacology. 2014 Feb 5;724:132–9. [CrossRef]
- Gazal M, Kaufmann FN, Acosta BA, Oliveira PS, Valente MR, Ortmann CF, et al. Preventive Effect of Cecropia pachystachya Against Ketamine-Induced Manic Behavior and Oxidative Stress in Rats. Neurochem Res. 2015 July 1;40, 1421–30. [CrossRef]
- Recart VM, Spohr L, Soares MSP, de Mattos B da S, Bona NP, Pedra NS, et al. Gallic acid protects cerebral cortex, hippocampus, and striatum against oxidative damage and cholinergic dysfunction in an experimental model of manic-like behavior: Comparison with lithium effects. International Journal of Developmental Neuroscience. 2021;81, 167–78. [CrossRef]
- Arslan FC, Tiryaki A, Yıldırım M, Özkorumak E, Alver A, Altun İK, et al. The effects of edaravone in ketamine-induced model of mania in rats. Acta Neurobiol Exp (Wars). 2016;76, 192–8. [CrossRef]
- Gao TH, Ni RJ, Liu S, Tian Y, Wei J, Zhao L, et al. Chronic lithium exposure attenuates ketamine-induced mania-like behavior and c-Fos expression in the forebrain of mice. Pharmacology Biochemistry and Behavior. 2021 Mar 1;202:173108. [CrossRef]
- Ni RJ, Gao TH, Wang YY, Tian Y, Wei JX, Zhao LS, et al. Chronic lithium treatment ameliorates ketamine-induced mania-like behavior via the PI3K-AKT signaling pathway. Zoological Research. 2022;43, 989–1004. [CrossRef]
- Brody SA, Geyer MA, Large CH. Lamotrigine prevents ketamine but not amphetamine-induced deficits in prepulse inhibition in mice. Psychopharmacology. 2003 Sept 1;169, 240–6. [CrossRef]
- Rame M, Caudal D, Schenker E, Svenningsson P, Spedding M, Jay TM, et al. Clozapine counteracts a ketamine-induced depression of hippocampal-prefrontal neuroplasticity and alters signaling pathway phosphorylation. PLOS ONE. 2017 May 4;12, e0177036. [CrossRef]
- Bowman C, Richter U, Jones CR, Agerskov C, Herrik KF. Activity-State Dependent Reversal of Ketamine-Induced Resting State EEG Effects by Clozapine and Naltrexone in the Freely Moving Rat. Front Psychiatry. 2022 Jan 27;13:737295. [CrossRef]
- Williams NR, Heifets BD, Blasey C, Sudheimer K, Pannu J, Pankow H, et al. Attenuation of Antidepressant Effects of Ketamine by Opioid Receptor Antagonism. AJP. 2018 Dec;175, 1205–15. [CrossRef]
- Diazgranados N, Ibrahim L, Brutsche NE, Newberg A, Kronstein P, Khalife S, et al. A Randomized Add-on Trial of an N-methyl-d-aspartate Antagonist in Treatment-Resistant Bipolar Depression. Arch Gen Psychiatry. 2010 Aug;67, 793–802. [CrossRef]
- Zarate CA, Brutsche NE, Ibrahim L, Franco-Chaves J, Diazgranados N, Cravchik A, et al. Replication of Ketamine’s Antidepressant Efficacy in Bipolar Depression: A Randomized Controlled Add-On Trial. Biological Psychiatry. 2012 June 1;71, 939–46. [CrossRef]
- Xu AJ, Niciu MJ, Lundin NB, Luckenbaugh DA, Ionescu DF, Richards EM, et al. Lithium and Valproate Levels Do Not Correlate with Ketamine’s Antidepressant Efficacy in Treatment-Resistant Bipolar Depression. Neural Plasticity. 2015 June 7;2015:e858251. [CrossRef]
- Rybakowski JK, Permoda-Osip A, Bartkowska-Sniatkowska A. Ketamine augmentation rapidly improves depression scores in inpatients with treatment-resistant bipolar depression. Int J Psychiatry Clin Pract. 2017 June;21, 99–103. [CrossRef]
- O’Brien B, Lijffijt M, Lee J, Kim YS, Wells A, Murphy N, et al. Distinct trajectories of antidepressant response to intravenous ketamine. Journal of Affective Disorders. 2021 May 1;286:320–9. [CrossRef]
- Serretti A, Lattuada E, Franchini L, Smeraldi E. Melancholic features and response to lithium prophylaxis in mood disorders. Depression and Anxiety. 2000;11, 73–9. [CrossRef]
- Ionescu DF, Luckenbaugh DA, Niciu MJ, Richards EM, Zarate Jr CA. A single infusion of ketamine improves depression scores in patients with anxious bipolar depression. Bipolar Disorders. 2015;17, 438–43.
- Peters EM, Halpape K, Cheveldae I, Jacobson P, Wanson A. Predictors of response to intranasal ketamine in patients hospitalized for treatment-resistant depression. Personalized Medicine in Psychiatry. 2024 Mar 1;43–44:100119. [CrossRef]
- Etain B, Lajnef M, Brichant-Petitjean C, Geoffroy PA, Henry C, Gard S, et al. Childhood trauma and mixed episodes are associated with poor response to lithium in bipolar disorders. Acta Psychiatr Scand. 2017 Apr;135, 319–27. [CrossRef]
- Cascino G, D’Agostino G, Monteleone AM, Marciello F, Caivano V, Monteleone P, et al. Childhood maltreatment and clinical response to mood stabilizers in patients with bipolar disorder. Human Psychopharmacology: Clinical and Experimental. 2021;36, e2783. [CrossRef]
- Pennybaker SJ, Niciu MJ, Luckenbaugh DA, Zarate CA. Symptomatology and Predictors of Antidepressant Efficacy in Extended Responders to a Single Ketamine Infusion. J Affect Disord. 2017 Jan 15;208:560–6. [CrossRef]
- Keith KM, Geller J, Froehlich A, Arfken C, Oxley M, Mischel N. Vital Sign Changes During Intravenous Ketamine Infusions for Depression: An Exploratory Study of Prognostic Indications. J Clin Psychopharmacol. 2022 May;42, 254–9.
- Lundin NB, Niciu MJ, Luckenbaugh DA, Ionescu DF, Richards EM, Voort JLV, et al. Baseline Vitamin B12 and Folate Levels Do Not Predict Improvement in Depression After a Single Infusion of Ketamine. Pharmacopsychiatry. 2014 July;47, 141–4. [CrossRef]
- Permoda-Osip A, Skibińska M, Bartkowska-Sniatkowska A, Kliwicki S, Chłopocka-Woźniak M, Rybakowski JK. [Factors connected with efficacy of single ketamine infusion in bipolar depression]. Psychiatr Pol. 2014 Feb;48, 35–47. [CrossRef]
- Costi S, Soleimani L, Glasgow A, Brallier J, Spivack J, Schwartz J, et al. Lithium continuation therapy following ketamine in patients with treatment resistant unipolar depression: a randomized controlled trial. Neuropsychopharmacol. 2019 Sept;44, 1812–9. [CrossRef]
- Amiaz R, Saporta R, Noy A, Berkenstadt H, Weiser M. Can Quetiapine Prolong the Antidepressant Effect of Ketamine?: A 5-Year Follow-up Study. J Clin Psychopharmacol. 2021 Nov;41, 673–5.
- Nugent AC, Diazgranados N, Carlson PJ, Ibrahim L, Luckenbaugh DA, Brutsche N, et al. Neural correlates of rapid antidepressant response to ketamine in bipolar disorder. Bipolar Disorders. 2014;16, 119–28. [CrossRef]
- Chen MH, Chang WC, Lin WC, Tu PC, Li CT, Bai YM, et al. Functional Dysconnectivity of Frontal Cortex to Striatum Predicts Ketamine Infusion Response in Treatment-Resistant Depression. International Journal of Neuropsychopharmacology. 2020 Dec 1;23, 791–8. [CrossRef]
- Liu H, Wang C, Lan X, Li W, Zhang F, Hu Z, et al. Functional connectivity of the amygdala subregions and the antidepressant effects of repeated ketamine infusions in major depressive disorder. Eur Psychiatry. 2024 Apr 4;67, e33. [CrossRef]
- Cao Z, Lin CT, Ding W, Chen MH, Li CT, Su TP. Identifying Ketamine Responses in Treatment-Resistant Depression Using a Wearable Forehead EEG. IEEE Transactions on Biomedical Engineering. 2019 June;66, 1668–79. [CrossRef]
- Berner K, Oz N, Kaya A, Acharjee A, Berner J. mTORC1 activation in presumed classical monocytes: observed correlation with human size variation and neuropsychiatric disease. Aging. 2024;16, 11134–50. [CrossRef]
- McGrory CL, Ryan KM, Gallagher B, McLoughlin DM. Journal of Affective Disorders. 2020m 273:380–3.
- Guo S, Arai K, Stins MF, Chuang DM, Lo EH. Lithium Upregulates Vascular Endothelial Growth Factor in Brain Endothelial Cells and Astrocytes. Stroke. 2009 Feb;40, 652–5. [CrossRef]
- Villaseñor A, Ramamoorthy A, Silva dos Santos M, Lorenzo MP, Laje G, Zarate Jr C, et al. A pilot study of plasma metabolomic patterns from patients treated with ketamine for bipolar depression: evidence for a response-related difference in mitochondrial networks. British Journal of Pharmacology 2014;171, 2230–42.
- Słupski J, Cubała WJ, Górska N, Słupska A, Gałuszko-Węgielnik M. Copper Concentrations in Ketamine Therapy for Treatment-Resistant Depression. Brain Sciences. 2020 Dec;10(12):971. [CrossRef]
- Duman RS, Li N, Liu RJ, Duric V, Aghajanian G. Signaling Pathways Underlying the Rapid Antidepressant Actions of Ketamine. Neuropharmacology. 2012 Jan;62(1):35–41. [CrossRef]
- Zanos P, Gould TD. Intracellular signaling pathways involved in (S)- and (R)-ketamine antidepressant actions. Biol Psychiatry. 2018 Jan 1;83(1):2–4. [CrossRef]
- Quiroz JA, Gould TD, Manji HK. Molecular effects of lithium. Mol Interv. 2004 Oct;4(5):259–72.
- Wilkinson ST, Katz RB, Toprak M, Webler R, Ostroff RB, Sanacora G. Acute and Longer-Term Outcomes Using Ketamine as a Clinical Treatment at the Yale Psychiatric Hospital. J Clin Psychiatry. 2018 July 24;79(4):10099.
- Cipriani A, Hawton K, Stockton S, Geddes JR. Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis. BMJ. 2013 June 27;346:f3646. [CrossRef]
- Grof P, Duffy A, Cavazzoni P, Grof E, Garnham J, MacDougall M, et al. Is response to prophylactic lithium a familial trait? J Clin Psychiatry. 2002 Oct;63(10):942–7. [CrossRef]
- Manchia M, Adli M, Akula N, Ardau R, Aubry JM, Backlund L, et al. Assessment of Response to Lithium Maintenance Treatment in Bipolar Disorder: A Consortium on Lithium Genetics (ConLiGen) Report. PLoS One. 2013;8(6):e65636. [CrossRef]
- McIntyre RS, Rosenblat JD, Nemeroff CB, Sanacora G, Murrough JW, Berk M, et al. Synthesizing the Evidence for Ketamine and Esketamine in Treatment-Resistant Depression: An International Expert Opinion on the Available Evidence and Implementation. Am J Psychiatry. 2021 May 1;178(5):383–99. [CrossRef]
- Rybakowski JK, Suwalska A. Excellent lithium responders have normal cognitive functions and plasma BDNF levels. Int J Neuropsychopharmacol. 2010 June 1;13(5):617–22. [CrossRef]
- Khayachi A, Ase A, Liao C, Kamesh A, Kuhlmann N, Schorova L, et al. Chronic lithium treatment alters the excitatory/ inhibitory balance of synaptic networks and reduces mGluR5–PKC signalling in mouse cortical neurons. JPN. 2021 May 1;46(3):E402–14. [CrossRef]
- Khayachi A, Abuzgaya M, Liu Y, Jiao C, Dejgaard K, Schorova L, et al. Akt and AMPK activators rescue hyperexcitability in neurons from patients with bipolar disorder. EBioMedicine. 2024 June;104:105161. [CrossRef]
- Stern S, Santos R, Marchetto M, Mendes A, Rouleau G, Biesmans S, et al. Neurons derived from patients with bipolar disorder divide into intrinsically different sub-populations of neurons, predicting the patients’ responsiveness to lithium. Molecular Psychiatry. 2018;23(6):1453–65. [CrossRef]
- Stern S, Sarkar A, Galor D, Stern T, Mei A, Stern Y, et al. A Physiological Instability Displayed in Hippocampal Neurons Derived From Lithium-Nonresponsive Bipolar Disorder Patients. Biological Psychiatry. 2020 July;88(2):150–8. [CrossRef]
- Stern S, Sarkar A, Stern T, Mei A, Mendes APD, Stern Y, et al. Mechanisms Underlying the Hyperexcitability of CA3 and Dentate Gyrus Hippocampal Neurons Derived From Patients With Bipolar Disorder. Biological Psychiatry. 2020 July;88(2):139–49. [CrossRef]
Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of study selection.
Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of study selection.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



