Submitted:
26 September 2025
Posted:
28 September 2025
You are already at the latest version
Abstract
Obesity in elderly individuals is associated with increased levels of inflammatory biomarkers, indicating a state of chronic low-grade inflammation, which has been recently termed as inflammaging and adipaging. Several studies have demonstrated this relationship: Overweight and obese middle-aged and elderly individuals show elevated levels of inflammatory markers like CXCL-16, IL-6, and adipokines compared to normal-weight counterparts. These markers positively correlate with anthropometric parameters indicating increased cardiovascular risk. C-reactive protein (CRP) and fibrinogen levels increase progressively with higher obesity classes in the general population, including the elderly . For instance, CRP levels nearly double with each increase in weight class compared to normal weight individuals. Additionally, the presence of obesity-related comorbidities like hypertension or diabetes further elevates these inflammatory markers. In conclusion, obesity in the elderly is characterized by elevated levels of various inflammatory biomarkers, reflecting a state of chronic low-grade inflammation. This inflammatory state may contribute to the development of obesity-related comorbidities. The clarification of the complementary or independent role of these biomarkers in aging and obesity could lead to targeted therapeutic interventions in this vulnerable population group.
Keywords:
obesity
; inflammatory markers
; ageing
; immune system
; inflammageing
; elderly population
1. Introduction
Obesity is an emerging worldwide problem. According to the WHO report, in 2022, 1 in 8 people in the world were living with obesity, meaning 16% of adults [1]. Its presence leads to the development of chronic diseases between others metabolic syndrome, cardiovascular disease, diabetes mellitus type 2, stroke and non-alcoholic fatty liver disease. The ageing population -with its challenges in public health concerning the multiple comorbidities that usually coexist-is another issue that will become more evident in the near future [2].By the late 2070s, the number of persons aged 65 years or older globally is estimated to overcome 2.2 billion, outweighing the number of children (under age 18). By the mid-2030s, it is estimated that there will be 265 million persons aged 80 years or older, more than the number of infants (1 year of age or less) [2]. The co-presence of obesity and ageing is a matter of intense research and various aspects of these two factors are addressed by researchers.
The phenomenon, known as the "obesity paradox," demonstrating improved short- and mid-term survival rates in overweight versus better long term survival outcomes in normal weight individuals, has also been studied as it was initially attributed to BMI’s inability to reflect fat distribution [3]. This paradox is more pronounced between people with chronic illnesses such as cancer, heart failure or kidney disease, but it seems to be caused by the lipolytic effect of cachexia. In other words, the detrimental effects of obesity is not linear, but also is a matter of general status of the patient and other factors such as the distribution of adipose tissue which seems to play a role in the interpretation of obesity impact in the elderly population.
Obesity in elderly individuals is associated with increased levels of inflammatory biomarkers, indicating a state of chronic low-grade inflammation that is evident through altered immune state in cellular and molecular level [4]. Several studies have demonstrated this relationship . On the other hand, conditions and comorbidities of obesity are a reflection of those of ageing and its related disease. Ageing and obesity have analogous phenotypes that also include enhanced systemic inflammation [5]. Obesity and ageing have been described as two sides of the same coin [6], whereas the term «adipaging» has also been used to show the common pathways of these two situations resulting in a dysfunctional adipose tissue [7]. In this narrative review we try to outline the obesity related inflammatory biomarkers in the elderly population and their possible clinical role.
2. Methodology
This review was documented using electronic databases (PubMed, Google Scholar, and Embase) with targeted search terms such as “obesity,” “inflammatory markers,” “ageing,” “immune system,” “inflammageing,” “elderly population” to identify relevant papers. Relevant material from grey literature was also included. Studies that were not in English or were not available in full text were not included in this study.
3. Changes of Adipose Tissue During Aging
The aging process is a lifelong process with gradual decline in (pre-)adipocyte function over time [8]. Chronic unresolved inflammation, in the adipose tissue, changes immune cell profiles and tissue homeostasis. [9]. These changes are not the same between the different types and depots of adipose tissue nor are they the same throughout life. Human adipose tissue (AT) is categorized into three primary types: white adipose tissue (WAT), which is mainly involved in energy storage; brown adipose tissue (BAT), which plays a role in non-shivering thermogenesis; and beige adipose tissue, which contains adipocytes with characteristics that are intermediate between white and brown fat. These tissue types are distributed throughout the human body [10].
Concerning WAT, it consists of subcutaneous adipose tissue (SAT) which lies in the hypodermis, and includes the subcutaneous thoracic, abdominal, gluteal, or femoral adipose tissue. Visceral adipose tissue (VAT) which is the adipose tissue located inside the abdominal or thoracic cavity, between the viscera can be sub-classified into thoracic adipose tissue (ThAT) (pericardial, non-pericardial, epicardial, and perivascular) and abdominal adipose tissue (intraperitoneal, retroperitoneal) [11]. SAT is decreasing with age whereas the abdominal and pericardial VAT increase with age [12]. Visceral AT, ("metabolically unhealthy") is considered metabolically harmful and associated with increased risk, whereas subcutaneous AT ("metabolically healthy") appears neutral or even beneficial.
An enhanced collection of senescent cells has been found in the visceral fat of obese individuals, that is an important source of inflammatory cytokines [13]. WAT is known to secrete multiple pro-inflammatory such as visfatin, leptin, chemerin, resistin, CRP and cytokines such as IL-6 and anti-inflammatory biomarkers, such as adiponectin. A chronic condition of subclinical inflammation in obesity has been shown to shift immune cells from anti-inflammatory to pro-inflammatory state, between others from B1 (anti-inflammatory) cells to B2 (pro-inflammatory) cells [14]. The two subsets of B cells perform nearly opposing functions in adipose tissue, in particular B-1 cells provide an early, innate-like defense and act as a brake on inflammation through natural IgM and IL-10 production whereas B-2 cells drive a later, adaptive immune response that, under conditions like high-fat diets or aging, can lead to heightened inflammation through the triggering or enhancement of the production of inflammatory cytokines such as IL-6 and TNF-α. This further propels the inflammatory cycle in adipose tissue and metabolic dysfunction, leading to conditions such as insulin resistance and atherosclerosis [14].
Brown adipose tissue (BAT) decline with aging especially in male adults, with interscapular areas being the first to decline [15]. Other areas of BAT are the supraclavicular areas which are more active in the females but the detection of BAT in humans is generally difficult [16]. Also beige adipose tissue becomes dysfunctional with aging due to several mechanisms such as chronic inflammation, and senescence of different adipose cell compartments [16]. Their role in local inflammation as compared to WAT is less pronounced, but enhanced production of TNF-a and MCP-1 is caused due to obesity related metabolic derangement [17]. Of note is the role of the beige-like epicardial adipose tissue (adipose tissue between the myocardium and the visceral side of the pericardium) that changes function in obesity. From being a protective thermogenetic tissue to the myocardium, it becomes inflammatory, secreting pro-inflammatory cytokines (e.g. MCP-1, TNFa, and IL-1b) into the adjacent myocardium and coronary arteries, with a possible damaging role in the coronary vasculature [18].
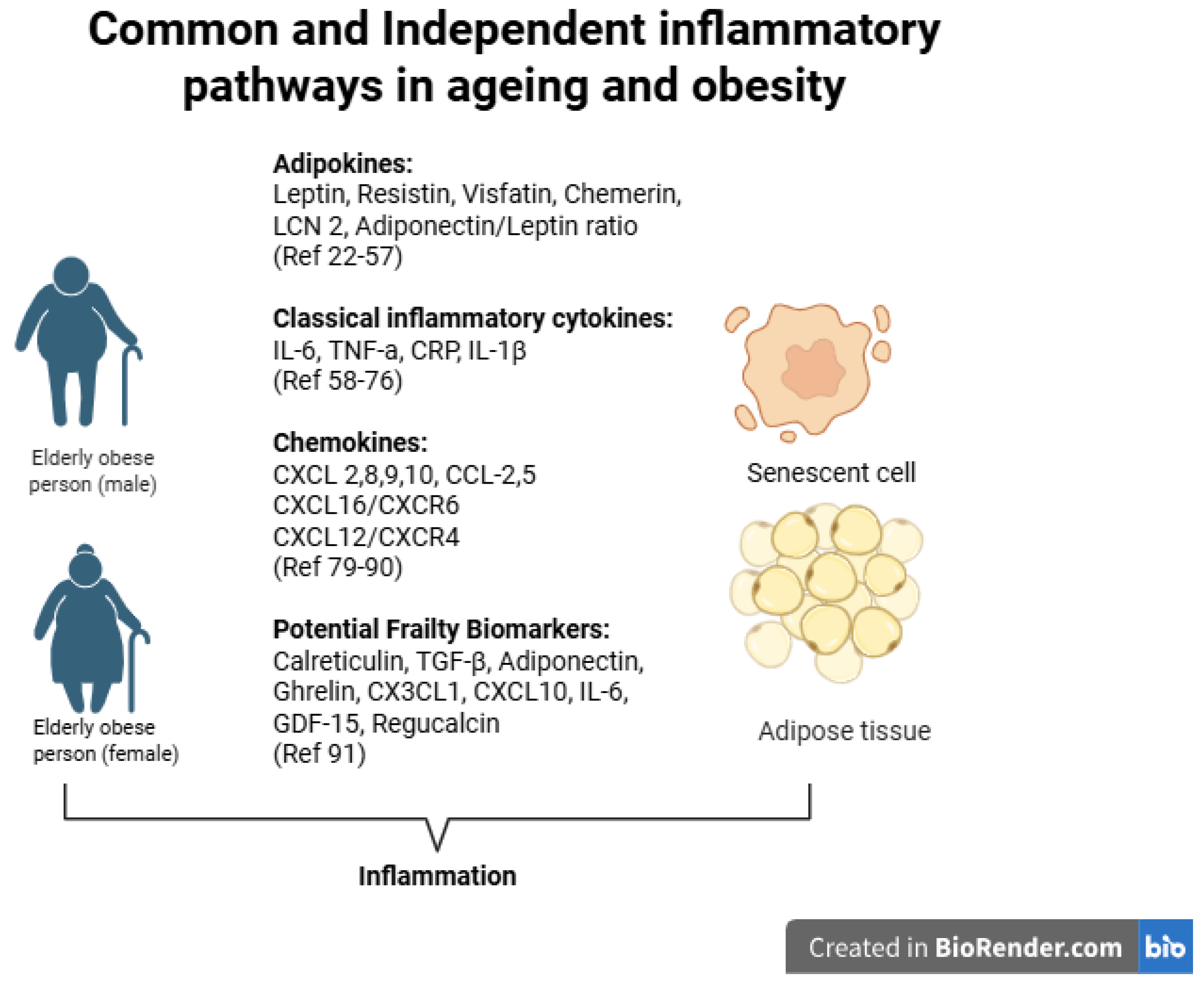
Overall there is a variety of common and novel inflammatory biomarkers [19]. Present and various studies have focused in the description of these markers in obesity [20] or in ageing [21]. In this narrative review a description of the existent evidence of obesity related inflammatory biomarkers in the elderly population is following, trying to highlight their possible clinical value in the daily clinical practice (Figure 1).
4. Plasma Visfatin Levels in Obesity and Ageing
Visfatin is a protein mainly secreted from VAT not only by adipocytes, but also by macrophages infiltrating adipose tissue [22]. An affinity of this protein for the insulin receptor has been shown in animal models by binding to the receptor at a different, from insulin, linking site [23] thus implying a possible role of this protein in abnormal glucose metabolism [24] which was not confirmed in clinical studies [25]. Conflicting evidence exists as to whether visfatin levels are related to the amount of VAT. Higher levels of mRNA visfatin have been shown in VAT in obese versus lean subjects which was also positively related to BMI [25]. Moreover Jurdana M et al [26] have shown significantly higher baseline levels of fasting visfatin in overweight versus normal weight subjects and confirmed statistically that physical fitness was the best significant predictor of the baseline visfatin concentration in male participants, while alanine, omega-3 fatty acid intakes and C-reactive protein levels were significant predictors of baseline visfatin concentrations independent of age, body mass index, and % of trunk fat in females. In morbidly obese adults plasma visfatin levels were significantly increased compared to lean subjects [27] also when morbid obesity was associated with glucose metabolic abnormalities [28].
Concerning the correlation of Visfatin with anthropometric parameters again various studies have shown divergent results. In a study of obese adults (BMI>30) without a previous diagnosis of abnormal glucose metabolism the only-negative-correlation was found with waist to hip ratio (WHR) [24] suggesting an association with the gynoid pattern of adipose tissue distribution, but commented that their study included 70% women who usually exhibit the gynoid adipose tissue pattern obesity. In another study [29] plasma visfatin levels and visfatin mRNA expression were measured in 189 adults with a wide range of obesity, body fat distribution, insulin sensitivity, and glucose tolerance. The authors conclude that visfatin plasma concentration correlates positively with the visceral visfatin mRNA expression, BMI and percent body fat, but not with WHR.
There are few studies addressing the relationship between age and plasma visfatin levels. Kaminska et al [24] showed a decrease of plasma visfatin levels with age and glycated haemoglobin levels in 68 obese adults without previous diagnosis of abnormal glucose metabolism. In another study by de Luis et al, plasma visfatin levels were also found to be inversely correlated with age in an interventional longitudinal study analyzing a population of 80 obese non-diabetic outpatients. , showing a steady decrease in levels for each year of age [30].
5. Leptin
Leptin is a16 kDa protein containing 160 amino acids that is responsible for food intake, body mass, reproductive functioning and fetal development [31]. It is primarily produced in white adipose tissue and in smaller concentrations also in brown adipose tissue, placenta, stomach, fetal tissue, bone marrow, muscles, teeth and brain. Hyperleptinemia is found in obesity as its secretion is proportional to body mass and nutritional status. Its secretion is more pronounced in the subcutaneous rather than in the visceral adipose tissue [32]. There is a feedback loop explaining the increased production of multiple inflammatory cytokines (IL-6, IL-12, TNF-a) from leptin and the increased expression of leptin from others (e.g. IL-1, TNF-a) leading to a chronic inflammatory state due to obesity [33]. There is also evidence that obesity impairs the effects of leptin, leading to resistance that encompasses also its receptor’s function LEP-R [32]. This also explains the diminished effects of exogenous leptin administration and the need for leptin sensitizers [31] as leptin resistance occurs due to the leptin’s inability to reach the target cells, reduced Lep-R expression, or disturbed Lep-R signaling [34,35].
Τhe elevated levels of circulating leptin in older adults primarily result from increased fat mass when compared to younger adults. Another reason for this elevation has been suggested to be due to decreased leptin responsiveness with advancing age as a result of impaired signaling of hypothalamic leptin receptors, a phenomenon that has been observed in aged rats [36]. In older humans a reduction in the expression of the short form of the leptin receptor (LepRa) in peripheral blood monocytes has been documented. LepRa is recognized for its role in transporting leptin across the blood-brain barrier [37]. Whether aging reduces hypothalamic leptin responsiveness in humans remains to be determined, as it is linearly correlated with total body fat and BMI.
It has been shown that adiponectin/leptin ratio is a better diagnostic marker for classifying subjects with metabolic syndrome than leptin or adiponectin alone [38]. Increased adiponectin is associated with increased mortality in the elderly, perhaps related to production by the vascular system in atherosclerosis [39,40]. More needs to be done to understand whether there are age-related changes in adiponectin production by cells in fat tissue and what the consequences are.
6. Retinol Binding Protein 4 (RBP4) in Obesity and Aging
RBP4 is known as a negative acute inflammatory reactant and as a new adipokine, which levels increase in insulin resistant conditions such as obesity, metabolic syndrome, type 2 diabetes mellitus [41] as well as cardiovascular diseases [42]. It is also produced in the liver and in macrophages [41]. In elderly patients as those studied in the PIVUS study (Prospective Investigation of the Vasculature in Uppsala Seniors) circulating RBP4 concentrations were inversely associated with intima media and plaque echogenicity in carotid arteries, implying its role in the development of atherosclerosis [43]. RBP4 contributes to the advancement of insulin resistance via immune and inflammatory processes in adipose and vascular tissues [44].
According to a study by Gavi S et al [45] comparing a young and an elderly small group of adults, in the elderly subjects there was no correlation between RBP4 levels and insulin sensitivity, percent trunk fat, triglycerides, and low-density lipoprotein and its levels in the elderly seem to be independent of central adiposity [45].
7. Chemerin in Obesity and Ageing
Chemerin, is a recently discovered adipose tissue-specific adipokine that has a pivotal function in the differentiation and development of adipocytes, in addition to glucose and lipid metabolism [46]. Elevated levels of chemerin were detected in overweight individuals, in prediabetic states, and in lean, overweight, and obese individuals with T2DM [47].
In elderly patients with type 2 DM, circulating chemerin levels are elevated and are independent of the length of disease and BMI, probably due to adipocyte dysfunction enhancement with aging [48]. Chemerin is directly associated with age but it is uncertain if elevated chemerin is a result of aging or of the higher concentration of visceral adipose tissue in the aging population [49].
8. Resistin in Obesity and Ageing
Resistin has been initially described as an adipokine of the mice by Steppan et al [50] linking obesity and diabetes. Its role as an adipokine has not been established in humans, where its site of production are mainly in the monocytes and macrophages [32], and shows an increased risk for atherosclerosis [51] and a propensity for insulin resistance in elderly patients with previous coronary interventions [52].
9. Lipocalin 2 in Obesity and Ageing
Lipocalin 2 (LCN2), also known as neutrophil gelatinase-associated lipocalin (NGAL) [53], has been studied in various conditions such as inflammation, infection and metabolic diseases. It is a 25-kDa glycoprotein derived from neutrophil granules and is a member of the lipocalin superfamily [54]. It is produced abundantly in adipocytes, particularly after preadipocytes mature, but is also secreted by other tissues such as liver and kidney tissue. Despite LCN2 levels increase under a large number of inflammatory conditions, both pro- and anti-inflammatory properties of this adipokine have been reported [55].
A study by Daoud et al [56] examining the correlation between LCN2 and other adipokines in obese adults undergoing a 12 month lifestyle and diet induced weight reduction before and after this intervention showed that LCN2 was positively correlated with resistin and adiponectin. These results imply a role of LCN2 in adipose tissue dysregulation and could recognize LCN2 as a biomarker for diagnosing obesity associated metabolic disorders [56].
Increased LCN-2 expression is seen in the adipose tissue of obese individuals and is linked to obesity-related variables, between others fasting glucose and the HOMA-IR index [57]. LCN-2 is induced by various pro- and anti-inflammatory cytokines and has been identified as pivotal in glucose homeostasis and insulin sensitivity. Its association with body fat mass and metabolic indices underlines its role for evaluating the severity of obesity [58].
In ageing the role of LCN2 is not yet clarified. In LCN2 deficient KO mice [59] lipocalin-2 deficiency protects mice from developing aging- and obesity-induced insulin resistance largely by modulating 12-lipoxygenase and TNF- levels in adipose tissue. Conversely ap2-promoter-driven Lcn2 transgenic (Tg) mice and aged Lcn2 Tg mice showed that overexpression of Lcn2 in adipose tissue not only preserves adipose tissue function during aging but also promotes maintenance of glucose tolerance, decreases dyslipidemia, and prevents liver lipid accumulation and steatosis [59].
10. TNF-a, IL-1β and IL-6 in Obesity and Ageing
The aging immune system undergoes quantitative and qualitative changes, leading to a reduced ability to fight infections and increased susceptibility to cancer and autoimmune disorders. Key features include altered T-cell populations, a diminished ability to recognize diverse antigens, reduced effector functions, and a chronic, low-grade inflammatory state [60] as already mentioned before. The role of circulating pro-inflammatory cytokines (interleukin (IL)-6, tumor necrosis factor (TNF) or IL-1b) as risk factor in cardiovascular and neurodegenerative diseases is well established as also its association with sarcopenia and frailties [61]. Many studies have examined the relation of these cytokines with age [62,63], though a clear association cannot be established due to differences in the characteristics of the subpopulations studied. Nevertheless in a small population of healthy nonobese adults study a trend in the increase of TNF-a levels with age was found, whereas for IL-6 levels there was a positive correlation [63]. The role of these cytokines in aging seems to be dichotomal since studies have shown that cytokines, like IL-1β, IL-6 and TNF positively regulate macroautophagy, mitochondrial function, anti-tumor immune responses and skeletal muscle biogenesis, possibly contributing to longevity. Contradictory, there is also a detrimental and antagonistic role of these cytokines including the induction of sarcopenia, tissue damage and promotion of tumorigenesis [64].
Ghanemi et al [65] have shown shared patterns in the aging and obesity process in cellular, molecular and epigenetic pathways that impact health outcomes. In obese older adults, higher levels of adiposity are associated with higher blood levels of inflammatory markers such as interleukin (IL)-1 receptor antagonist (IL-1RA), IL-6 and TNF-α [66] . These proinflammatory cytokines inhibit preadipocyte differentiation and maturation, and promote adipocyte aging [67]. IL-1β, IL-6 and TNF-α secreted by adipose tissue macrophages reduce PPAR-γ expression, an important transcription factor that induces adipogenesis [68], while finally there is a shift in macrophage migration and expression resulting in enhanced expression of M1 macrophages (classically activated CD40+ and/or CD11c+), a proinflammatory macrophage phenotype, in aged obese individuals which is formed with aberrant adipose tissue [68].
Concerning the role of IL-6 in ageing and obesity a positive and significant association between serum IL-6 and visceral fat mass has been shown in a small cohort with 77 patients aged ≥ 65 years old [69]. Furthermore, the authors have exhibited that moderately increased IL-6 level during the aging process inhibits PKA/HSL- mediated lipolysis in KO mice and consequently leads to an increase of lipid accumulation in visceral adipose tissue [69]. The role of IL-6 in insulin resistance remains controversial although elevated levels of IL-6 have been linked to the development of type 2 diabetes [70]. It is possible that the different actions of IL-6 on insulin signaling may be due to its divergent actions in variable organs (liver versus muscle) or the different sources of IL-6 (muscle versus fat) [71].
11. CRP Levels in Obesity and Ageing
The ageing process is associated with senescence of the immune system [72], particularly with T-lymphocyte dysfunction [73] as well as with a recently described phenotype called SCAP (senescence associated secretory phenotype) [21]. It is known that in healthy normal weight subjects, abdominal obesity is associated with hs-CRP, irrespective of age and BMI [74]. A value of hs-CRP over 3mg/dl is linked to elevated cardiovascular risk [75] and the proportion of people with elevated hs-CRP is significantly higher in those with abdominal obesity than in control subjects, in addition to a higher BMI [74]. Concerning the trend of CRP levels in elderly people of the general population Hutchinson et al have shown that there is an increase (approximately a doubling of the median CRP levels in the oldest from 1 to 2 mg/dl) with higher values in the female subjects [76]. In obese older adults, higher levels of adiposity are associated with higher blood levels of the acute phase reactant, C-reactive protein, especially in female nonagenarians [66] .
CRP is an established biomarker of IL-1β/IL-6/CRP axis [77]. Although its genetic variations have not been directly linked to CVD risk [75], newer genetic studies have found that less common recessive genotypes of two single nucleotide polymorphisms in the CRP gene (rs1800947 and rs11265263) were associated with significantly higher mortality risk in heart failure patients [78].
12. The Role of Chemokines in Obesity and Ageing
Chemokines are signaling proteins that guide white blood cells to locations of injury or infection by initiating a process called chemotaxis. As a type of "cytokine," chemokines bind to receptors on immune cells, stimulating them to move toward specific sites to fight inflammation. They have a pivotal role in the proper functioning of the immune system, collaborating to orchestrate immune responses by navigation the migration and activating immune cells [79]. Currently, more than 50 chemokines and 18 chemokine receptors having various physiological and pathological properties have been discovered and their receptors can be common (shared receptors) but with divergent functions [80]. They are distinguished into inflammatory and homeostatic chemokines, the former being responsible for recruiting neutrophils and monocytes to sites of active inflammation, whereas the latter seem to have a more qualitative (highly specific) control on immune cells migration [80].
In obesity pro-inflammatory cytokines and chemokines involved in the recruitment of immune cells to the adipose tissue from bone marrow are secreted so that consequently macrophage infiltration within the adipose tissue becomes one of the major sources of inflammation[80]. Adipocytes release pro-inflammatory biomarkers as well (cytokines, chemokines, and adipokines) and in larger amounts compared with immune cells [81]. Another source of chemokine production in the adipose tissue is interferon-γ, the signature Th1 cytokine, which causes macrophages and T cells to release chemokines, which in turn recruit immune cells to the obese adipose tissue [82]. Despite extensive trials scarce evidence has been found as to the differential expression of chemokines that account for the chronic inflammatory state in obesity.
In brief, in obesity, adipose tissue secretes several chemokines, including MCP-1(also known as CCL2) and CCL5 , which can trigger signaling pathways and result in inflammatory reactions and insulin resistance. These elements can likewise influence the management of obesity. Weight reduction has demonstrated a decrease in serum levels of chemokine MCP-1 in obese males with metabolic syndrome and enhances indicators related to kidney damage [83]. The up-regulation of CCL2 results in an increased recruitment of macrophages into adipose tissue, worsening metabolic inflammation though CCL2 deficient mice do not show decreased macrophage infiltration into the adipose tissue [84].
CXC chemokines (including CXCL16/CXCR6, CXCL10, and CXCL12/CXCR4,) influence inflammation linked to obesity, affect immune cell migration, tumor development, and metabolic processes [85]. CXCL12, a chemokine secreted by adipocytes, attracts macrophages into adipose tissue, impairing insulin sensitivity [86]. On the other hand CXCL16/CXCR6 axis in adipocytes differentiated from human adipose derived mesenchymal stem cells regulates macrophage polarization making it a possible target as a modulator of immune response in adipose tissue [85]. Patients with obesity have been noted to have increased circulating levels of the CXCL10 chemokine. These levels are associated with indicators of obesity, including BMI, waist circumference, and Homeostatic Model Assessment of Insulin Resistance (HOMA-IR) [82]. Increased CXCL10 levels might boost leukocyte attachment to endothelial cells, leading to dysfunctional endothelial activity. This mechanism may play a role in the onset of insulin resistance and cardiovascular issues associated with obesity [87].
Concerning aging, overweight and obese middle-aged and elderly individuals show elevated levels of inflammatory chemokine CXCL-16 compared to normal-weight counterparts [88]. This marker positively correlates with anthropometric parameters indicating increased cardiovascular risk. CXCL16 could potentially serve as an early marker for the transition from normal weight to overweight in this age group [88]. Bonfante et al have shown that serum levels of CCL2, CXCL8, CXCL9, and CXCL10 increase with aging, considering them as potential aging biomarkers[89]. Also Inadera et al elicited a profound age-dependent increase of CCL2 levels both in males and females most possibly due to the correlation of CCL2 levels with atherosclerotic burden although no difference was found in patients with coronary artery disease compared to healthy age-matched controls. Furthermore CXCL9 has a distinct role in cardiovascular aging and vascular dysfunction which is associated with cellular senescence and arterial stiffness. Its silencing reverses these phenotypes and most probably it could serve as an early indicator of aging [90]. Cardoso et al have highlighted CX3CL1 and CXCL10, along with other factors, such as IL-6, GDF15, regucalcin, calreticulin, TGF-β, adiponectin, and ghrelin as potential frailty biomarkers [91]. In their review Chaudhary et al describe recent findings about the role of chemokines in the aging process of different organs and underline the crucial importance of targeting these mechanisms in order to delay and/or modulate the aging process and prevent age-related diseases [92].
13. Conclusions
There is a plethora of obesity related inflammatory biomarkers that play a role in the chronic low grade inflammation in elderly obese adults leading to various related comorbidities. Inflammaging and adipaging are interrelated and enhance the vulnerability of this group population. Targeted therapies are needed to improve the health status of an age group that is expected to rise disproportionally in the near future.
References
- Obesity and overweight [Internet]. [cited 2025 May 1]. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
- World Population Ageing 2019.
- Aune D, Sen A, Prasad M, Norat T, Janszky I, Tonstad S, et al. BMI and all cause mortality: systematic review and non-linear dose-response meta-analysis of 230 cohort studies with 3.74 million deaths among 30.3 million participants. BMJ. 2016 May 4;353:i2156. [CrossRef]
- Khanna D, Khanna S, Khanna P, Kahar P, Patel BM. Obesity: A Chronic Low-Grade Inflammation and Its Markers. Cureus. 2022 Feb;14(2):e22711. [CrossRef]
- Trim WV, Walhin JP, Koumanov F, Bouloumié A, Lindsay MA, Chen YC, et al. Divergent immunometabolic changes in adipose tissue and skeletal muscle with ageing in healthy humans. The Journal of Physiology. 2022;600(4):921–47.
- Tam BT, Morais JA, Santosa S. Obesity and ageing: Two sides of the same coin. Obes Rev. 2020 Apr;21(4):e12991. [CrossRef]
- Pérez LM, Pareja-Galeano H, Sanchis-Gomar F, Emanuele E, Lucia A, Gálvez BG. ‘Adipaging’: ageing and obesity share biological hallmarks related to a dysfunctional adipose tissue. J Physiol. 2016 June 15;594(12):3187–207. [CrossRef]
- Schosserer M, Grillari J, Wolfrum C, Scheideler M. Age-Induced Changes in White, Brite, and Brown Adipose Depots: A Mini-Review. Gerontology. 2017 Dec 7;64(3):229–36. [CrossRef]
- Reyes-Farias M, Fos-Domenech J, Serra D, Herrero L, Sánchez-Infantes D. White adipose tissue dysfunction in obesity and aging. Biochem Pharmacol. 2021 Oct;192:114723. [CrossRef]
- Cinti S. The adipose organ at a glance. Dis Model Mech. 2012 Sept;5(5):588–94. [CrossRef]
- Antoniades C, Tousoulis D, Vavlukis M, Fleming I, Duncker DJ, Eringa E, et al. Perivascular adipose tissue as a source of therapeutic targets and clinical biomarkers. Eur Heart J. 2023 Oct 12;44(38):3827–44. [CrossRef]
- Kuk JL, Saunders TJ, Davidson LE, Ross R. Age-related changes in total and regional fat distribution. Ageing Research Reviews. 2009 Oct 1;8(4):339–48. [CrossRef]
- Tchkonia T, Morbeck DE, Von Zglinicki T, Van Deursen J, Lustgarten J, Scrable H, et al. Fat tissue, aging, and cellular senescence. Aging Cell. 2010 Oct;9(5):667–84. [CrossRef]
- Srikakulapu P, McNamara CA. B Lymphocytes and Adipose Tissue Inflammation. Arteriosclerosis, Thrombosis, and Vascular Biology. 2020 May;40(5):1110–22. [CrossRef]
- Pfannenberg C, Werner MK, Ripkens S, Stef I, Deckert A, Schmadl M, et al. Impact of Age on the Relationships of Brown Adipose Tissue With Sex and Adiposity in Humans. Diabetes. 2010 Apr 27;59(7):1789–93. [CrossRef]
- Zoico E, Rubele S, De Caro A, Nori N, Mazzali G, Fantin F, et al. Brown and Beige Adipose Tissue and Aging. Front Endocrinol [Internet]. 2019 June 20 [cited 2025 Apr 27];10. Available from: https://www.frontiersin.orghttps://www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2019.00368/full. [CrossRef]
- Villarroya F, Cereijo R, Gavaldà-Navarro A, Villarroya J, Giralt M. Inflammation of brown/beige adipose tissues in obesity and metabolic disease. Journal of Internal Medicine. 2018;284(5):492–504. [CrossRef]
- Hirata Y, Tabata M, Kurobe H, Motoki T, Akaike M, Nishio C, et al. Coronary Atherosclerosis Is Associated With Macrophage Polarization in Epicardial Adipose Tissue. Journal of the American College of Cardiology. 2011 July 12;58(3):248–55. [CrossRef]
- Menzel A, Samouda H, Dohet F, Loap S, Ellulu MS, Bohn T. Common and Novel Markers for Measuring Inflammation and Oxidative Stress Ex Vivo in Research and Clinical Practice—Which to Use Regarding Disease Outcomes? Antioxidants (Basel). 2021 Mar 9;10(3):414.
- Savulescu-Fiedler I, Mihalcea R, Dragosloveanu S, Scheau C, Baz RO, Caruntu A, et al. The Interplay between Obesity and Inflammation. Life. 2024 July;14(7):856.
- Spray L, Richardson G, Haendeler J, Altschmied J, Rumampouw V, Wallis SB, et al. Cardiovascular inflammaging: Mechanisms, consequences, and therapeutic perspectives. Cell Reports Medicine [Internet]. [cited 2025 Aug 17]. [CrossRef]
- Curat CA, Wegner V, Sengenès C, Miranville A, Tonus C, Busse R, et al. Macrophages in human visceral adipose tissue: increased accumulation in obesity and a source of resistin and visfatin. Diabetologia. 2006 Apr 1;49(4):744–7. [CrossRef]
- Skoczylas A. [The role of visfatin in the pathophysiology of human]. Wiad Lek. 2009;62(3):190–6.
- Kamińska A, Kopczyńska E, Bronisz A, Żmudzińska M, Bieliński M, Borkowska A, et al. An evaluation of visfatin levels in obese subjects. Endokrynologia Polska. 2010;61(2):169–73.
- Pagano C, Pilon C, Olivieri M, Mason P, Fabris R, Serra R, et al. Reduced Plasma Visfatin/Pre-B Cell Colony-Enhancing Factor in Obesity Is Not Related to Insulin Resistance in Humans. The Journal of Clinical Endocrinology & Metabolism. 2006 Aug 1;91(8):3165–70. [CrossRef]
- Jurdana M, Petelin A, Černelič Bizjak M, Bizjak M, Biolo G, Jenko-Pražnikar Z. Increased serum visfatin levels in obesity and its association with anthropometric/biochemical parameters, physical inactivity and nutrition. e-SPEN Journal. 2013 Apr 1;8(2):e59–67. [CrossRef]
- Haider DG, Schindler K, Schaller G, Prager G, Wolzt M, Ludvik B. Increased Plasma Visfatin Concentrations in Morbidly Obese Subjects Are Reduced after Gastric Banding. The Journal of Clinical Endocrinology & Metabolism. 2006 Apr 1;91(4):1578–81. [CrossRef]
- García-Fuentes E, García-Almeida JM, García-Arnés J, García-Serrano S, Rivas-Marín J, Gallego-Perales JL, et al. Plasma Visfatin Concentrations in Severely Obese Subjects Are Increased After Intestinal Bypass. Obesity. 2007;15(10):2391–5. [CrossRef]
- Berndt J, Klöting N, Kralisch S, Kovacs P, Fasshauer M, Schön MR, et al. Plasma Visfatin Concentrations and Fat Depot–Specific mRNA Expression in Humans. Diabetes. 2005 Oct 1;54(10):2911–6.
- de Luis DA, Gonzalez Sagrado M, Conde R, Aller R, Izaola O, Romero E. Effect of a hypocaloric diet on serum visfatin in obese non-diabetic patients. Nutrition. 2008 June 1;24(6):517–21. [CrossRef]
- Farr OM, Gavrieli A, Mantzoros CS. Leptin applications in 2015: what have we learned about leptin and obesity? Current Opinion in Endocrinology, Diabetes and Obesity. 2015 Oct;22(5):353.
- Obradovic M, Sudar-Milovanovic E, Soskic S, Essack M, Arya S, Stewart AJ, et al. Leptin and Obesity: Role and Clinical Implication. Front Endocrinol (Lausanne). 2021 May 18;12:585887.
- Faggioni R, Feingold KR, Grunfeld C. Leptin regulation of the immune response and the immunodeficiency of malnutrition. The FASEB Journal. 2001;15(14):2565–71. [CrossRef]
- Myers MG, Heymsfield SB, Haft C, Kahn BB, Laughlin M, Leibel RL, et al. Challenges and opportunities of defining clinical leptin resistance. Cell Metab. 2012 Feb 8;15(2):150–6. [CrossRef]
- Izquierdo AG, Crujeiras AB, Casanueva FF, Carreira MC. Leptin, Obesity, and Leptin Resistance: Where Are We 25 Years Later? Nutrients. 2019 Nov 8;11(11):2704. [CrossRef]
- La Cava A, Matarese G. The weight of leptin in immunity. Nat Rev Immunol. 2004 Dec;4(5):371–9. [CrossRef]
- Laule C, Rahmouni K. Leptin and Associated Neural Pathways Underlying Obesity-Induced Hypertension. Comprehensive Physiology. 2025;15(1):e8. [CrossRef]
- Zhuo Q, Wang Z, Fu P, Piao J, Tian Y, Xu J, et al. Comparison of adiponectin, leptin and leptin to adiponectin ratio as diagnostic marker for metabolic syndrome in older adults of Chinese major cities. Diabetes Research and Clinical Practice. 2009 Apr 1;84(1):27–33. [CrossRef]
- Rizza RA. Pathogenesis of fasting and postprandial hyperglycemia in type 2 diabetes: implications for therapy. Diabetes. 2010 Nov;59(11):2697–707. [CrossRef]
- Bik W, Baranowska-Bik A, Wolinska-Witort E, Kalisz M, Broczek K, Mossakowska M, et al. Assessment of adiponectin and its isoforms in Polish centenarians. Experimental Gerontology. 2013 Apr 1;48(4):401–7. [CrossRef]
- Moraes-Vieira PM, Yore MM, Dwyer PM, Syed I, Aryal P, Kahn BB. RBP4 Activates Antigen-Presenting Cells, Leading to Adipose Tissue Inflammation and Systemic Insulin Resistance. Cell Metabolism. 2014 Mar 4;19(3):512–26.
- Lambadiari V, Kadoglou NP, Stasinos V, Maratou E, Antoniadis A, Kolokathis F, et al. Serum levels of retinol-binding protein-4 are associated with the presence and severity of coronary artery disease. Cardiovasc Diabetol. 2014 Dec;13(1):121. [CrossRef]
- Ingelsson E, Lind L. Circulating Retinol-Binding Protein 4 and Subclinical Cardiovascular Disease in the Elderly. Diabetes Care. 2009 Apr 1;32(4):733–5. [CrossRef]
- Zabetian-Targhi F, Mahmoudi MJ, Rezaei N, Mahmoudi M. Retinol Binding Protein 4 in Relation to Diet, Inflammation, Immunity, and Cardiovascular Diseases. Advances in Nutrition. 2015 Nov 1;6(6):748–62.
- Gavi S, Qurashi S, Stuart LM, Lau R, Melendez MM, Mynarcik DC, et al. Influence of age on the association of retinol-binding protein 4 with metabolic syndrome. Obesity. 2008;16(4):893–5. [CrossRef]
- Sell H, Laurencikiene J, Taube A, Eckardt K, Cramer A, Horrighs A, et al. Chemerin Is a Novel Adipocyte-Derived Factor Inducing Insulin Resistance in Primary Human Skeletal Muscle Cells. Diabetes. 2009 Dec;58(12):2731–40. [CrossRef]
- Ernst MC, Issa M, Goralski KB, Sinal CJ. Chemerin Exacerbates Glucose Intolerance in Mouse Models of Obesity and Diabetes. Endocrinology. 2010 May 1;151(5):1998–2007. [CrossRef]
- Coimbra S, Brandão Proença J, Santos-Silva A, Neuparth MJ. Adiponectin, Leptin, and Chemerin in Elderly Patients with Type 2 Diabetes Mellitus: A Close Linkage with Obesity and Length of the Disease. Biomed Res Int. 2014;2014:701915. [CrossRef]
- Aronis KN, Sahin-Efe A, Chamberland JP, Spiro A, Vokonas P, Mantzoros CS. Chemerin levels as predictor of acute coronary events: A case–control study nested within the veterans affairs normative aging study. Metabolism. 2014 June;63(6):760–6. [CrossRef]
- Steppan CM, Bailey ST, Bhat S, Brown EJ, Banerjee RR, Wright CM, et al. The hormone resistin links obesity to diabetes. Nature. 2001 Jan 18;409(6818):307–12.
- Gencer B, Auer R, de Rekeneire N, Butler J, Kalogeropoulos A, Bauer DC, et al. Association between resistin levels and cardiovascular disease events in older adults: The health, aging and body composition study. Atherosclerosis. 2016 Feb;245:181–6. [CrossRef]
- Ohmori R, Momiyama Y, Kato R, Taniguchi H, Ogura M, Ayaori M, et al. Associations between serum resistin levels and insulin resistance, inflammation, and coronary artery disease. J Am Coll Cardiol. 2005 July 19;46(2):379–80. [CrossRef]
- Krizanac M, Mass Sanchez PB, Weiskirchen R, Asimakopoulos A. A Scoping Review on Lipocalin-2 and Its Role in Non-Alcoholic Steatohepatitis and Hepatocellular Carcinoma. International Journal of Molecular Sciences. 2021 Jan;22(6):2865. [CrossRef]
- Wang M, Zhang Q, Zhao X, Dong G, Li C. Diagnostic and prognostic value of neutrophil gelatinase-associated lipocalin, matrix metalloproteinase-9, and tissue inhibitor of matrix metalloproteinases-1 for sepsis in the Emergency Department: an observational study. Critical Care. 2014 Nov 19;18(6):634. [CrossRef]
- Abella V, Scotece M, Conde J, Gómez R, Lois A, Pino J, et al. The potential of lipocalin-2/NGAL as biomarker for inflammatory and metabolic diseases. Biomarkers. 2015 Nov 17;20(8):565–71. [CrossRef]
- Daoud MS, Alshareef FH, Alnaami AM, Amer OE, Hussain SD, Al-Daghri NM. Prospective changes in lipocalin-2 and adipocytokines among adults with obesity. Sci Rep. 2025 Aug 6;15(1):28794. [CrossRef]
- Lögdberg L, Wester L. Immunocalins: a lipocalin subfamily that modulates immune and inflammatory responses. Biochim Biophys Acta. 2000 Oct 18;1482(1–2):284–97. [CrossRef]
- Auguet T, Quintero Y, Terra X, Martínez S, Lucas A, Pellitero S, et al. Upregulation of lipocalin 2 in adipose tissues of severely obese women: positive relationship with proinflammatory cytokines. Obesity (Silver Spring). 2011 Dec;19(12):2295–300. [CrossRef]
- Law IKM, Xu A, Lam KSL, Berger T, Mak TW, Vanhoutte PM, et al. Lipocalin-2 Deficiency Attenuates Insulin Resistance Associated With Aging and Obesity. Diabetes. 2010 Apr;59(4):872–82. [CrossRef]
- Oh SJ, Lee JK, Shin OS. Aging and the Immune System: the Impact of Immunosenescence on Viral Infection, Immunity and Vaccine Immunogenicity. Immune Netw. 2019 Nov 14;19(6):e37. [CrossRef]
- Tylutka A, Walas Ł, Zembron-Lacny A. Level of IL-6, TNF, and IL-1β and age-related diseases: a systematic review and meta-analysis. Frontiers in Immunology. 2024 Mar 1;15. [CrossRef]
- Álvarez-Rodríguez L, López-Hoyos M, Muñoz-Cacho P, Martínez-Taboada VM. Aging is associated with circulating cytokine dysregulation. Cellular Immunology. 2012 Jan 1;273(2):124–32.
- Milan-Mattos JC, Anibal FF, Perseguini NM, Minatel V, Rehder-Santos P, Castro CA, et al. Effects of natural aging and gender on pro-inflammatory markers. Braz J Med Biol Res. 2019;52:e8392. [CrossRef]
- Silva RCMC. The dichotomic role of cytokines in aging. Biogerontology. 2024 Dec 2;26(1):17. [CrossRef]
- Ghanemi A, Yoshioka M, St-Amand J. Ageing and Obesity Shared Patterns: From Molecular Pathogenesis to Epigenetics. Diseases. 2021 Nov 29;9(4):87. [CrossRef]
- Lisko I, Tiainen K, Stenholm S, Luukkaala T, Hurme M, Lehtimäki T, et al. Inflammation, adiposity, and mortality in the oldest old. Rejuvenation Res. 2012 Oct;15(5):445–52.
- Tchkonia T, Morbeck DE, Von Zglinicki T, Van Deursen J, Lustgarten J, Scrable H, et al. Fat tissue, aging, and cellular senescence. Aging Cell. 2010 Oct;9(5):667–84.
- Ouchi N, Parker JL, Lugus JJ, Walsh K. Adipokines in inflammation and metabolic disease. Nat Rev Immunol. 2011 Feb;11(2):85–97. [CrossRef]
- Zhang X, Wang Q, Wang Y, Ma C, Zhao Q, Yin H, et al. Interleukin-6 promotes visceral adipose tissue accumulation during aging via inhibiting fat lipolysis. International Immunopharmacology. 2024 May 10;132:111906. [CrossRef]
- Pradhan AD, Manson JE, Rifai N, Buring JE, Ridker PM. C-reactive protein, interleukin 6, and risk of developing type 2 diabetes mellitus. JAMA. 2001 July 18;286(3):327–34.
- Mooney RA. Counterpoint: Interleukin-6 does not have a beneficial role in insulin sensitivity and glucose homeostasis. J Appl Physiol (1985). 2007 Feb;102(2):816–8; discussion 818-819.
- Gruver A, Hudson L, Sempowski G. Immunosenescence of ageing. The Journal of Pathology. 2007;211(2):144–56. [CrossRef]
- Salam N, Rane S, Das R, Faulkner M, Gund R, Kandpal U, et al. T cell ageing: Effects of age on development, survival & function. Indian Journal of Medical Research. 2013 Nov;138(5):595.
- Lapice E, Maione S, Patti L, Cipriano P, Rivellese AA, Riccardi G, et al. Abdominal Adiposity Is Associated With Elevated C-Reactive Protein Independent of BMI in Healthy Nonobese People. Diabetes Care. 2009 Sept 1;32(9):1734–6. [CrossRef]
- Casas JP, Shah T, Hingorani AD, Danesh J, Pepys MB. C-reactive protein and coronary heart disease: a critical review. J Intern Med. 2008 Oct;264(4):295–314. [CrossRef]
- Hutchinson WL, Koenig W, Fröhlich M, Sund M, Lowe GD, Pepys MB. Immunoradiometric assay of circulating C-reactive protein: age-related values in the adult general population. Clin Chem. 2000 July;46(7):934–8. [CrossRef]
- Direct Proinflammatory Effect of C-Reactive Protein on Human Endothelial Cells [Internet]. [cited 2025 Aug 17]. Available from: https://www.ahajournals.org/doi/epub/10.1161/01.CIR.102.18.2165. [CrossRef]
- Kittel-Schneider S, Kaspar M, Berliner D, Weber H, Deckert J, Ertl G, et al. CRP genetic variants are associated with mortality and depressive symptoms in chronic heart failure patients. Brain, Behavior, and Immunity. 2018 July;71:133–41. [CrossRef]
- Hughes CE, Nibbs RJB. A guide to chemokines and their receptors. FEBS J. 2018 Aug;285(16):2944–71.
- Xue W, Fan Z, Li L, Lu J, Zhai Y, Zhao J. The chemokine system and its role in obesity. Journal of Cellular Physiology. 2019;234(4):3336–46. [CrossRef]
- Kern PA, Saghizadeh M, Ong JM, Bosch RJ, Deem R, Simsolo RB. The expression of tumor necrosis factor in human adipose tissue. Regulation by obesity, weight loss, and relationship to lipoprotein lipase. J Clin Invest. 1995 May 1;95(5):2111–9. [CrossRef]
- He W, Wang H, Yang G, Zhu L, Liu X. The Role of Chemokines in Obesity and Exercise-Induced Weight Loss. Biomolecules. 2024 Sept 4;14(9):1121. [CrossRef]
- Bai Y, Sun Q. Macrophage recruitment in obese adipose tissue. Obes Rev. 2015 Feb;16(2):127–36. [CrossRef]
- Inouye KE, Shi H, Howard JK, Daly CH, Lord GM, Rollins BJ, et al. Absence of CC chemokine ligand 2 does not limit obesity-associated infiltration of macrophages into adipose tissue. Diabetes. 2007 Sept;56(9):2242–50. [CrossRef]
- Lee SC, Lee YJ, Choi I, Kim M, Sung JS. CXCL16/CXCR6 Axis in Adipocytes Differentiated from Human Adipose Derived Mesenchymal Stem Cells Regulates Macrophage Polarization. Cells. 2021 Dec 3;10(12):3410. [CrossRef]
- Kim D, Kim J, Yoon JH, Ghim J, Yea K, Song P, et al. CXCL12 secreted from adipose tissue recruits macrophages and induces insulin resistance in mice. Diabetologia. 2014 July;57(7):1456–65. [CrossRef]
- Moreno B, Hueso L, Ortega R, Benito E, Martínez-Hervas S, Peiro M, et al. Association of chemokines IP-10/CXCL10 and I-TAC/CXCL11 with insulin resistance and enhance leukocyte endothelial arrest in obesity. Microvasc Res. 2022 Jan;139:104254. [CrossRef]
- Ribeiro SMTL, Lopes LR, Paula Costa G de, Figueiredo VP, Shrestha D, Batista AP, et al. CXCL-16, IL-17, and bone morphogenetic protein 2 (BMP-2) are associated with overweight and obesity conditions in middle-aged and elderly women. Immunity & Ageing. 2017 Mar 11;14(1):6. [CrossRef]
- Bonfante H de L, Almeida C de S, Abramo C, Grunewald STF, Levy RA, Teixeira HC. CCL2, CXCL8, CXCL9 and CXCL10 serum levels increase with age but are not altered by treatment with hydroxychloroquine in patients with osteoarthritis of the knees. Int J Rheum Dis. 2017 Dec;20(12):1958–64.
- Sayed N, Huang Y, Nguyen K, Krejciova-Rajaniemi Z, Grawe AP, Gao T, et al. An inflammatory aging clock (iAge) based on deep learning tracks multimorbidity, immunosenescence, frailty and cardiovascular aging. Nat Aging. 2021 July;1:598–615. [CrossRef]
- Cardoso AL, Fernandes A, Aguilar-Pimentel JA, De Angelis MH, Guedes JR, Brito MA, et al. Towards frailty biomarkers: Candidates from genes and pathways regulated in aging and age-related diseases. Ageing Research Reviews. 2018 Nov;47:214–77. [CrossRef]
- Chaudhary JK, Danga AK, Kumari A, Bhardwaj A, Rath PC. Role of chemokines in aging and age-related diseases. Mechanisms of Ageing and Development. 2025 Feb 1;223:112009. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



