Submitted:
18 September 2025
Posted:
23 September 2025
You are already at the latest version
Abstract
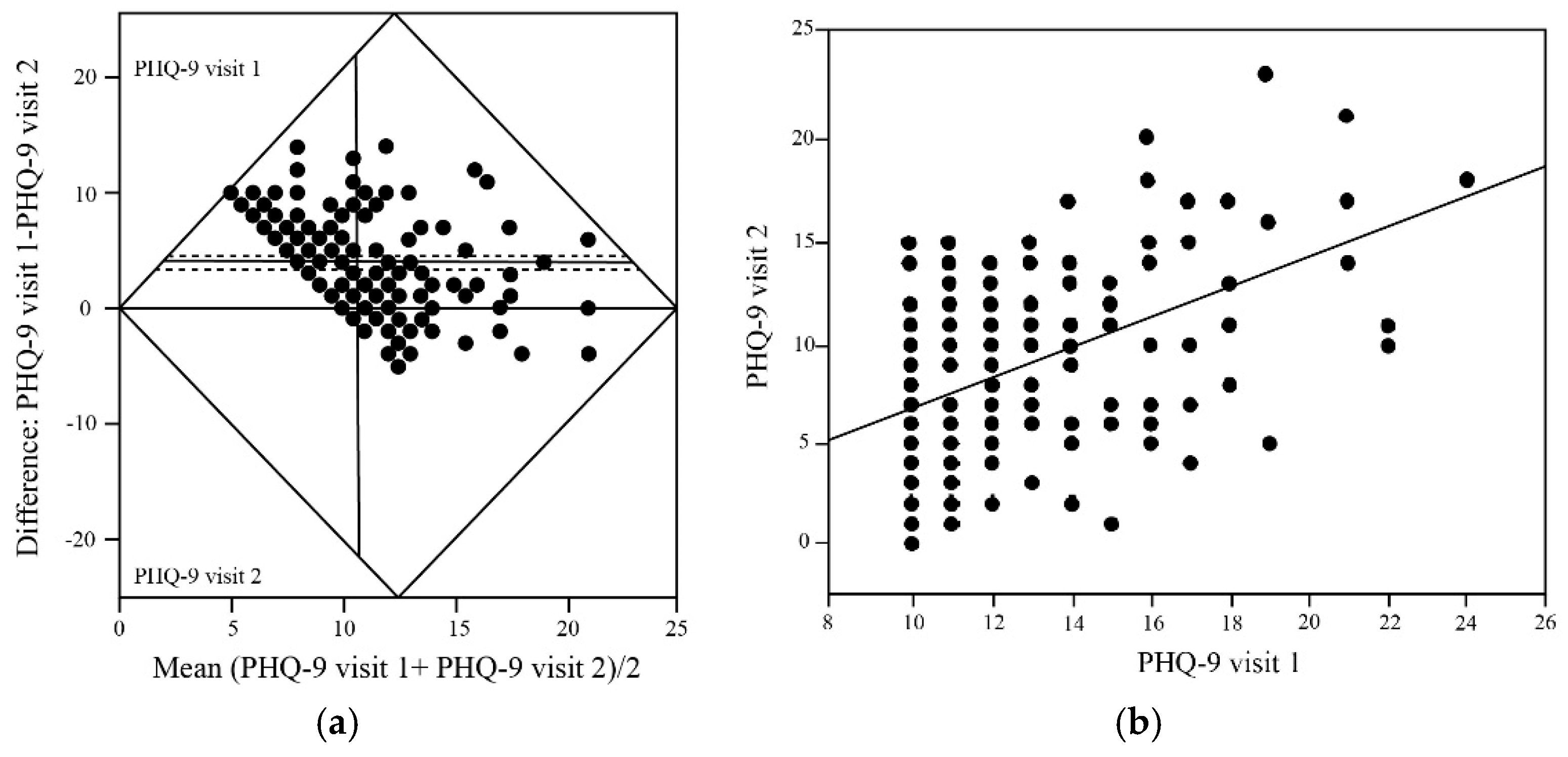
Background/Objectives: The ReCODE (Reversal of Cognitive Decline) protocol, a precision medicine program, designed for patients with Alzheimer's disease, has shown promising results in improving cognitive function. Depression, which is common among individuals with mild cognitive impairment and Alzheimer’s disease, shares some risk and exacerbating factors (such as systemic inflammation), and can negatively affect quality of life and disease trajectory. We set out to assess whether participation in the ReCODE program is associated with improvement in depressive symptoms, as measured by the Patient Health Questionnaire-9 (PHQ-9). Methods: A total of 170 individuals diagnosed with mild to moderate Alzheimer’s disease were enrolled in the ReCODE program. Each participant received consultations with clinical practitioners and a detailed orientation to the program. Follow-up visits were conducted 31 days post-enrollment, during which participants received further guidance on diet, lifestyle modifications, medications, and supplements. These visits also included mood assessment using the Patient Health Questionnaire-9 (PHQ-9). Pre- and post-intervention data were analyzed using the non-parametric Wilcoxon signed-rank test. Results: Participants demonstrated a statistically and clinically significant reduction in PHQ-9 scores, with improvement observed across mild, moderate, and severe baseline depression categories. The proportion of participants above the clinical threshold for depression decreased substantially following the intervention. Conclusions: Our results suggest that the ReCODE program not only benefits cognitive and biological measures, as shown in prior work, but also significantly alleviates depressive symptoms. These findings highlight ReCODE’s potential as a successful multifaceted therapeutic approach addressing both cognitive decline and mental health in Alzheimer’s disease.
Keywords:
1. Introduction
2. Methods
2.1. ReCODE Protocol Components, Software and Program Implementation
2.2. Patient Health Questionnaire-9 (PHQ-9)
2.3. Participants, Assessment and Statistical analysis
3. Results
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- El-Hayek, Y.H.; Wiley, R.E.; Khoury, C.P.; Daya, R.P.; Ballard, C.; Evans, A.R.; Karran, M.; Molinuevo, J.L.; Norton, M.; Atri, A. Tip of the Iceberg: Assessing the Global Socioeconomic Costs of Alzheimer's Disease and Related Dementias and Strategic Implications for Stakeholders. J Alzheimers Dis 2019, 70, 323-341. [CrossRef]
- James, B.D.; Leurgans, S.E.; Hebert, L.E.; Scherr, P.A.; Yaffe, K.; Bennett, D.A. Contribution of Alzheimer disease to mortality in the United States. Neurology 2014, 82, 1045-1050. [CrossRef]
- Alzheimer's, A. 2024 Alzheimer's disease facts and figures. Alzheimers Dement 2024, 20, 3708-3821. [CrossRef]
- Yiannopoulou, K.G.; Anastasiou, A.I.; Zachariou, V.; Pelidou, S.H. Reasons for Failed Trials of Disease-Modifying Treatments for Alzheimer Disease and Their Contribution in Recent Research. Biomedicines 2019, 7, 97-112. [CrossRef]
- Dubois, B.; Hampel, H.; Feldman, H.H.; Scheltens, P.; Aisen, P.; Andrieu, S.; Bakardjian, H.; Benali, H.; Bertram, L.; Blennow, K.; et al. Preclinical Alzheimer's disease: Definition, natural history, and diagnostic criteria. Alzheimers Dement 2016, 12, 292-323. [CrossRef]
- Calabro, M.; Rinaldi, C.; Santoro, G.; Crisafulli, C. The biological pathways of Alzheimer disease: a review. AIMS neuroscience 2021, 8, 86-132. [CrossRef]
- Peng, Y.; Gao, P.; Shi, L.; Chen, L.; Liu, J.; Long, J. Central and Peripheral Metabolic Defects Contribute to the Pathogenesis of Alzheimer's Disease: Targeting Mitochondria for Diagnosis and Prevention. Antioxid Redox Signal 2020, 32, 1188-1236. [CrossRef]
- Merlo, S.; Spampinato, S.; Canonico, P.L.; Copani, A.; Sortino, M.A. Alzheimer's disease: brain expression of a metabolic disorder? Trends in endocrinology and metabolism: TEM 2010, 21, 537-544. [CrossRef]
- Ishii, M.; Iadecola, C. Metabolic and Non-Cognitive Manifestations of Alzheimer's Disease: The Hypothalamus as Both Culprit and Target of Pathology. Cell metabolism 2015, 22, 761-776. [CrossRef]
- Bredesen, D.E. Reversal of cognitive decline: a novel therapeutic program. Aging (Albany NY) 2014, 6, 707-717.
- Theendakara, V.; Peters-Libeu, C.A.; Spilman, P.; Poksay, K.S.; Bredesen, D.E.; Rao, R.V. Direct Transcriptional Effects of Apolipoprotein E. J Neurosci 2016, 36, 685-700. [CrossRef]
- Seto, M.; Weiner, R.L.; Dumitrescu, L.; Hohman, T.J. Protective genes and pathways in Alzheimer's disease: moving towards precision interventions. Mol Neurodegener 2021, 16, 29-44. [CrossRef]
- Schechter, G.; Azad, G.K.; Rao, R.; McKeany, A.; Matulaitis, M.; Kalos, D.M.; Kennedy, B.K. A Comprehensive, Multi-Modal Strategy to Mitigate Alzheimer's Disease Risk Factors Improves Aspects of Metabolism and Offsets Cognitive Decline in Individuals with Cognitive Impairment. Journal of Alzheimer's disease reports 2020, 4, 223-230. [CrossRef]
- Toups, K.; Hathaway, A.; Gordon, D.; Chung, H.; Raji, C.; Boyd, A.; Hill, B.D.; Hausman-Cohen, S.; Attarha, M.; Chwa, W.J.; et al. Precision Medicine Approach to Alzheimer's Disease: Successful Pilot Project. J Alzheimers Dis 2022, 88, 1411-1421. [CrossRef]
- Bredesen, D.E.; Toups, K.; Hathaway, A.; Gordon, D.; Chung, H.; Raji, C.; Boyd, A.; Hill, B.D.; Hausman-Cohen, S.; Attarha, M.; et al. Precision Medicine Approach to Alzheimer's Disease: Rationale and Implications. J Alzheimers Dis 2023, 96, 429-437. [CrossRef]
- Sandison, H.; Callan, N.G.L.; Rao, R.V.; Phipps, J.; Bradley, R. Observed Improvement in Cognition During a Personalized Lifestyle Intervention in People with Cognitive Decline. J Alzheimers Dis 2023. [CrossRef]
- Keawtep, P.; Sungkarat, S.; Boripuntakul, S.; Sa-Nguanmoo, P.; Wichayanrat, W.; Chattipakorn, S.C.; Worakul, P. Effects of combined dietary intervention and physical-cognitive exercise on cognitive function and cardiometabolic health of postmenopausal women with obesity: a randomized controlled trial. Int J Behav Nutr Phys Act 2024, 21, 28. [CrossRef]
- Ornish, D.; Madison, C.; Kivipelto, M.; Kemp, C.; McCulloch, C.E.; Galasko, D.; Artz, J.; Rentz, D.; Lin, J.; Norman, K.; et al. Effects of intensive lifestyle changes on the progression of mild cognitive impairment or early dementia due to Alzheimer's disease: a randomized, controlled clinical trial. Alzheimers Res Ther 2024, 16, 122. [CrossRef]
- Thunborg, C.; Wang, R.; Rosenberg, A.; Sindi, S.; Andersen, P.; Andrieu, S.; Broersen, L.M.; Coley, N.; Couderc, C.; Duval, C.Z.; et al. Integrating a multimodal lifestyle intervention with medical food in prodromal Alzheimer's disease: the MIND-AD(mini) randomized controlled trial. Alzheimers Res Ther 2024, 16, 118. [CrossRef]
- Rao, R.V.; Kumar, S.; Gregory, J.; Coward, C.; Okada, S.; Lipa, W.; Kelly, L.; Bredesen, D.E. ReCODE: A Personalized, Targeted, Multi-Factorial Therapeutic Program for Reversal of Cognitive Decline. Biomedicines 2021, 9, 1348-1356. [CrossRef]
- Rao, R.V.; Subramaniam, K.G.; Gregory, J.; Bredesen, A.L.; Coward, C.; Okada, S.; Kelly, L.; Bredesen, D.E. Rationale for a Multi-Factorial Approach for the Reversal of Cognitive Decline in Alzheimer's Disease and MCI: A Review. International journal of molecular sciences 2023, 24, 1659-1681. [CrossRef]
- Schneider, N.; Yvon, C. A review of multidomain interventions to support healthy cognitive ageing. The journal of nutrition, health & aging 2013, 17, 252-257. [CrossRef]
- Bredesen, D.E.; Sharlin, K.; Jenkins, D.; Okuno, M.; Youngberg, W.; Cohen, S.H.; Stefani, A.; Brown, R.L.; Conger, S.; Tanio, C.; et al. Reversal of Cognitive Decline: 100 Patients. Journal of Alzheimer’s Disease & Parkinsonism 2018, 8, 1-6. [CrossRef]
- Bredesen, D.E.; Amos, E.C.; Canick, J.; Ackerley, M.; Raji, C.; Fiala, M.; Ahdidan, J. Reversal of cognitive decline in Alzheimer's disease. Aging (Albany NY) 2016, 8, 1250-1258. [CrossRef]
- Kivipelto, M.; Solomon, A.; Ahtiluoto, S.; Ngandu, T.; Lehtisalo, J.; Antikainen, R.; Backman, L.; Hanninen, T.; Jula, A.; Laatikainen, T.; et al. The Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER): study design and progress. Alzheimers Dement 2013, 9, 657-665. [CrossRef]
- Lista, S.; Dubois, B.; Hampel, H. Paths to Alzheimer's disease prevention: from modifiable risk factors to biomarker enrichment strategies. The journal of nutrition, health & aging 2015, 19, 154-163. [CrossRef]
- Ross, M.K.; Raji, C.; Lokken, K.L.; Bredesen, D.E.; Roach, J.C.; Funk, C.C.; Price, N.; Rappaport, N.; Hood, L.; Heath, J.R. Case Study: A Precision Medicine Approach to Multifactorial Dementia and Alzheimer's Disease. Journal of Alzheimer's disease & Parkinsonism 2021, 11, 18-36.
- Fotuhi, M.; Lubinski, B.; Trullinger, M.; Hausterman, N.; Riloff, T.; Hadadi, M.; Raji, C.A. A Personalized 12-week "Brain Fitness Program" for Improving Cognitive Function and Increasing the Volume of Hippocampus in Elderly with Mild Cognitive Impairment. The journal of prevention of Alzheimer's disease 2016, 3, 133-137. [CrossRef]
- Nguyen, S.A.; Oughli, H.A.; Lavretsky, H. Complementary and Integrative Medicine for Neurocognitive Disorders and Caregiver Health. Current psychiatry reports 2022, 24, 469-480. [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606-613. [CrossRef]
- Levis, B.; Sun, Y.; He, C.; Wu, Y.; Krishnan, A.; Bhandari, P.M.; Neupane, D.; Imran, M.; Brehaut, E.; Negeri, Z.; et al. Accuracy of the PHQ-2 Alone and in Combination With the PHQ-9 for Screening to Detect Major Depression: Systematic Review and Meta-analysis. JAMA 2020, 323, 2290-2300. [CrossRef]
- Wu, Y.; Levis, B.; Riehm, K.E.; Saadat, N.; Levis, A.W.; Azar, M.; Rice, D.B.; Boruff, J.; Cuijpers, P.; Gilbody, S.; et al. Equivalency of the diagnostic accuracy of the PHQ-8 and PHQ-9: a systematic review and individual participant data meta-analysis. Psychol. Med. 2020, 50, 1368-1380. [CrossRef]
- Chi, S.; Wang, C.; Jiang, T.; Zhu, X.C.; Yu, J.T.; Tan, L. The prevalence of depression in Alzheimer's disease: a systematic review and meta-analysis. Curr Alzheimer Res 2015, 12, 189-198. [CrossRef]
- Dafsari, F.S.; Jessen, F. Depression-an underrecognized target for prevention of dementia in Alzheimer's disease. Translational psychiatry 2020, 10, 160. [CrossRef]
- Wang, X.; Ye, T.; Alzheimer's Disease Neuroimaging, I.; Zhou, W.; Zhang, J. Sex-specific association of depressive symptom trajectories with cognitive decline and clinical progression in mild cognitive impairment. Alzheimers Dement 2025, 21, e70548. [CrossRef]
- Byers, A.L.; Yaffe, K. Depression and risk of developing dementia. Nat Rev Neurol 2011, 7, 323-331. [CrossRef]
- Wragg, R.E.; Jeste, D.V. Overview of depression and psychosis in Alzheimer's disease. A. J. Psychiatry 1989, 146, 577-587. [CrossRef]
- Bredesen, D.E.; John, V. Next generation therapeutics for Alzheimer's disease. EMBO Mol Med 2013, 5, 795-798. [CrossRef]
- Bredesen, D.E. Metabolic profiling distinguishes three subtypes of Alzheimer's disease. Aging (Albany NY) 2015, 7, 595-600.
- Sun, Y.; Fu, Z.; Bo, Q.; Mao, Z.; Ma, X.; Wang, C. The reliability and validity of PHQ-9 in patients with major depressive disorder in psychiatric hospital. BMC Psychiatry 2020, 20, 474. [CrossRef]
- Levis, B.; Benedetti, A.; Thombs, B.D.; Collaboration, D.E.S.D. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: individual participant data meta-analysis. BMJ 2019, 365, l1476. [CrossRef]
- Karyotaki, E.; Efthimiou, O.; Miguel, C.; Bermpohl, F.M.G.; Furukawa, T.A.; Cuijpers, P.; Individual Patient Data Meta-Analyses for Depression, C.; Riper, H.; Patel, V.; Mira, A.; et al. Internet-Based Cognitive Behavioral Therapy for Depression: A Systematic Review and Individual Patient Data Network Meta-analysis. JAMA Psychiatry 2021, 78, 361-371. [CrossRef]
- Kendrick, T.; Moore, M.; Leydon, G.; Stuart, B.; Geraghty, A.W.A.; Yao, G.; Lewis, G.; Griffiths, G.; May, C.; Dewar-Haggart, R.; et al. Patient-reported outcome measures for monitoring primary care patients with depression (PROMDEP): study protocol for a randomised controlled trial. Trials 2020, 21, 441. [CrossRef]
- Yao, X.; Wang, Y.; Zhou, Y.; Li, Z. A nurse-led positive psychological intervention among elderly community-dwelling adults with mild cognitive impairment and depression: A non-randomized controlled trial. Int. J. Geriatr. Psychiatry 2023, 38, e5951. [CrossRef]
- Manea, L.; Gilbody, S.; McMillan, D. Optimal cut-off score for diagnosing depression with the Patient Health Questionnaire (PHQ-9): a meta-analysis. CMAJ 2012, 184, E191-196. [CrossRef]
- Pettit, R.S.; Sakon, C.M.; Kinney, K.E.; Brown, C.; Gallaway, K.A.; Wagner, S.A.; Tillman, E.M. Predictors of Selective Serotonin Reuptake Inhibitor Treatment Failure in Persons With Cystic Fibrosis. Pediatr. Pulmonol. 2025, 60, e27402. [CrossRef]
- Yi, J.; Lu, J.; Yang, A.; Marsh, E.B. In-hospital predictors of post-stroke depression for targeted initiation of Selective Serotonin Reuptake Inhibitors (SSRIs). BMC Psychiatry 2022, 22, 722. [CrossRef]
- Lewis, G.; Duffy, L.; Ades, A.; Amos, R.; Araya, R.; Brabyn, S.; Button, K.S.; Churchill, R.; Derrick, C.; Dowrick, C.; et al. The clinical effectiveness of sertraline in primary care and the role of depression severity and duration (PANDA): a pragmatic, double-blind, placebo-controlled randomised trial. Lancet Psychiatry 2019, 6, 903-914. [CrossRef]
- Kampf-Sherf, O.; Zlotogorski, Z.; Gilboa, A.; Speedie, L.; Lereya, J.; Rosca, P.; Shavit, Y. Neuropsychological functioning in major depression and responsiveness to selective serotonin reuptake inhibitors antidepressants. J. Affect. Disord. 2004, 82, 453-459. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



