Submitted:
20 September 2025
Posted:
22 September 2025
You are already at the latest version
Abstract
Despite substantial progress in medical care, acute myocarditis remains a life-threatening disorder with a sudden onset, often unexpectedly complicating a simple and common upper respiratory tract infection. Myocarditis is most triggered by viral infections (over 80% of cases), with an estimated incidence of 10–106 per 100,000 annually. The clinical course may worsen in cases of mixed etiology, where a primary viral infection is complicated by secondary bacterial pathogens, leading to prolonged inflammation and an increased risk of progression to chronic active myocarditis or dilated cardiomyopathy. We included a case report as illustration of the clinical problem resulting from the progression of acute myocarditis into a chronic active disease. A central element of host defense is the inflammasome—an intracellular complex that activates pyroptosis and cytokine release (IL-1β, IL-18). While these processes help combat pathogens, their persistent activation may sustain inflammation and trigger heart failure and cardiac fibrosis, eventually leading to dilated cardiomyopathy. In this review, we summarize the current understanding of inflammasome pathways and their dual clinical role in myocarditis: essential for controlling acute infection but potentially harmful when over activated, contributing to chronic myocardial injury. Additionally, we discuss both novel and established therapeutic strategies targeting inflammatory pathways and anti-fibrotic mechanisms, including IL-1 receptor blockers (anakinra, canakinumab), NOD-like receptor protein 3 (NLRP3) inhibitors (colchicine, MCC950, dapansutrile, INF200), NF-κB inhibitors, angiotensin receptor-neprilysin inhibitors (ARNI). and microRNAs. Our aim is to highlight the clinical importance of early identification of patients at risk of progression from acute to chronic inflammation, role of inflammasomes and to present emerging therapies that may improve outcomes by balancing effective pathogen elimination with limitation of chronic cardiac damage.

Keywords:
myocarditis
; inflammasomes
; microRNAs
; Interleukins
; viral
; bacterial
; chronic active
; pharmacological strategies
1. Introduction
1.1. Epidemiology of Myocarditis
Despite substantial progress in medical care, acute myocarditis remains a life-threatening disorder with a sudden onset, often unexpectedly complicating a simple and common upper respiratory tract infection [1,2,3]. The annual incidence of myocarditis is reported to range from 10.2 to 105.6 per 100,000 population, with approximately 1.8 million cases occurring worldwide each year [4]. The etiology in the majority of cases is viral (over 85%) [5]. Bacterial myocarditis accounts for an estimated 3–6% of cases, though available data remain limited [6]. Sporadic cases result from parasitic (e.g., trichinosis, schistosomiasis) and protozoal infections (e.g., Trypanosoma cruzi, the causative agent of Chagas disease, and Toxoplasma gondii), as well as spirochetes such as Borrelia burgdorferi, the causative agent of Lyme disease [7,8]. Noninfectious myocarditis can be caused by drug toxicity or autoimmune disease [7,9].
Viral myocarditis (VMC) can be induced by various viruses. Coxsackievirus B3 (CVB3, an enterovirus) is the most common cause of myocardial injury globally (34.6 per 1000 cases), followed by influenza B (17.4 per 1000 cases), influenza A (11.7 per 1000 cases), Coxsackievirus A (CVA, 9.1 per 1000 cases), and cytomegalovirus (CMV) (8.0 per 1000 cases) [8,10].
In recent years, cardiotropic viruses utilizing angiotensin-converting enzyme 2 (ACE), such as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2, responsible for COVID-19), have also been implicated in acute myocarditis [7,11,12,13]. A pooled analysis by Zuin et al., involving more than 20 million individuals, revealed that myocarditis was nearly 2.5 times more prevalent in post-COVID-19 patients compared to controls [14]. Myocarditis occurred in 0.21 per 1000 patients recovering from COVID-19 (95% CI: 0.13–0.42), compared to 0.09 per 1000 control subjects (95% CI: 0.07–0.12) [14]. Thus, COVID-19 may predispose patients to cardiac complications following otherwise mild respiratory infections of various etiologies. Furthermore, patients recovered from COVID-19 showed an increased risk of incident myocarditis within one year of infection (HR: 5.16, 95% CI: 3.87–6.89; p < 0.0001) [15]. Conversely, COVID-19 vaccination has also been associated with myocarditis, with reported incidence ranging from 8.1 to 39 cases per 100,000 persons (or doses) [16].
Bacterial myocarditis is more frequently observed in immunocompromised individuals or as part of systemic infections. Among bacterial pathogens, Gram-positive organisms such as Staphylococcus aureus, Streptococcus pyogenes, and Corynebacterium diphtheriae are most identified. Less commonly, Gram-negative bacteria such as Neisseria meningitidis, Haemophilus influenzae, Salmonella spp., Klebsiella spp., and Borrelia burgdorferi are involved. The pathogenesis typically includes direct myocardial invasion or immune-mediated injury. Although bacterial myocarditis is less common than viral forms, early diagnosis is crucial due to its severity and the need for specific antimicrobial treatment [5,7,17].
Streptococcus pneumoniae is not typically described as a direct cause of myocarditis; however, it remains a leading cause of pneumonia—accounting for up to 15% of community-acquired pneumonia (CAP) cases in the United States and 27% globally [18]. Given the high incidence of pneumococcal pneumonia and frequent hospitalization, especially among elderly individuals, invasive pneumococcal disease is often accompanied by cardiac complications, most notably new-onset or worsening heart failure (HF) and cardiac arrhythmias [19,20,21].
1.2. Diagnostic Work-Ups
The initial diagnostic test upon admission to a cardiac care unit is typically a 12-lead electrocardiogram (ECG) [22]. This often reveals changes suggestive of myocardial ischemia, frequently resembling acute coronary syndrome (ACS) [23]. Recently, Ramantauskaitė et al. demonstrated that such ischemic ECG changes are clinically relevant [24]. The authors found that left ventricular (LV) ejection fraction (EF) in patients presenting with ST-segment elevation (STE) myocardial infarction (MI) was significantly lower compared to those with a non-STE pattern. The STE pattern was also associated with higher C-reactive protein (CRP) and troponin levels, along with reduced LV strain and lower LV-EF on echocardiography [24].
Echocardiography is the first-line imaging modality in all suspected cases of myocarditis, used to rule out alternative diagnoses and detect ventricular dysfunction, pericardial effusion, and complications such as intracardiac thrombus [25,26]. There is an increasing role for left ventricular (LV) strain assessment in providing important prognostic information regarding adverse outcomes in myocarditis [27]. Echocardiographic studies focus on both LV and right ventricular (RV) systolic function, the development of LV dilatation, and diastolic function. They also allow for the assessment of LV strain, which is fundamental for prognostication. This examination is highly valuable in predicting patient recovery or deterioration. Cardiac magnetic resonance (CMR) is recommended as the first-line diagnostic tool for establishing the diagnosis of uncomplicated myocarditis [28,29]. When acute myocarditis is suspected, CMR should be performed urgently and should include T1/T2 mapping to support a confirmatory diagnosis [29]. The diagnosis of myocarditis is based on the Lake Louise Criteria, which are applied during CMR to identify myocardial inflammation, edema, and fibrosis. It is highly recommended to confirm the diagnosis in clinically stable patients when the initial work-up suggests myocarditis. CMR should be performed on admission and repeated as necessary [23,25]. Cardiac biopsy is very useful in acute myocarditis for confirming the final diagnosis and predicting outcomes. However, it may carry an increased risk of pericardial hematoma. Endomyocardial biopsy remains necessary in high-risk cases to guide further therapy [23,30]. Both diagnostic tools provide insight into the extent of inflammation and fibrosis, which are crucial for predicting the future course of myocarditis [1,23,25,30,31,32].
1.3. Natural Course of Myocarditis
The natural course of myocarditis varies greatly between individuals, ranging from rapid and full recovery to the need for heart transplantation (HTx) in the most severe cases of dilated cardiomyopathy (DCM) and HF [2,4,7]. Aside from fulminant myocarditis, it is extremely difficult to predict at symptom onset who will deteriorate and who will recover quickly [33,34]. Myocarditis is a complex condition, with viral etiology playing a central role [1,2,3]. Standard treatment includes bed rest, management of the primary infection (antiviral or antibacterial therapy), and prevention and treatment of HF [24]. Treatment strategies may involve: no specific therapy, only symptomatic management (infusions, antipyretics), antibiotics, HF and antiarrhythmic therapy with beta-blockers, or a combination of optimal HF therapies such as ACE inhibitors, angiotensin II receptor blockers (ARBs), mineralocorticoid receptor antagonists (MRAs), diuretics, and other agents [5,7,24]. Beta-blockers should be considered for all patients with myocarditis due to their antiarrhythmic properties, which help prevent ventricular arrhythmias. Antibiotics are recommended only in cases of confirmed active bacterial infection, as viral infection is the usual cause of myocarditis.
Complicated myocarditis occurs in approximately 4% to 15% of cases, and around 1.2% of patients require durable mechanical circulatory support (MCS) [35,36]. The estimated mortality rate for acute myocarditis ranges from 1% to 7% [37,38,39]. In a Korean study involving nearly 3,000 patients, 30-day all-cause mortality was 6.6%, and was independently associated with complicated disease course (HR: 13.92, 95% CI: 8.43–22.97), diabetes (HR: 3.99, 95% CI: 1.79–8.92), connective tissue disease (HR: 2.90, 95% CI: 1.25–6.74), and concomitant malignancy (HR: 7.64, 95% CI: 3.04–19.17) [36]. In complicated cases, myocarditis may progress to LV dysfunction, end-stage chronic HF, and DCM, requiring assist devices and/or HTx. In the Lombardy Registry, a multicenter registry of patients with acute myocarditis, cardiac mortality and HTx rates were 11.3% and 14.7%, respectively, in patients with complicated presentation, and 0% in uncomplicated cases (log-rank P<0.0001) [37]. In contrast, multicenter data showed that among 419 patients admitted with fulminant myocarditis, 322 (77%) required temporary MCS upon intensive care unit admission, and one-third progressed to HTx or required ventricular support with LVAD/BiVAD during hospitalization [40]. Additionally, among 45,941 patients on the HTx waiting list in the Society for Heart and Lung Transplantation Registry, myocarditis was the primary diagnosis in 299 (0.7%) patients [41].
1.4. Elimination of the Pathogen Versus Progression to Chronic Active Inflammation
The long-term outcome of myocarditis survivors varies greatly. Most acute myocarditis cases resolve within a few days. However, when active inflammation persists for more than three months from onset, it is defined as chronic active myocarditis [39]. The residual risk associated with acute myocarditis was identified in the Danish national cohort [42]. Although pathogen elimination and healing from myocarditis are possible in most cases, VMC can persist and remain active for months or even years [38]. In the Danish study, all-cause mortality was 16.9% over 8.5 years. Even younger patients who recovered from acute myocarditis without complications were at increased risk of HF and death compared to age- and sex-matched controls [40]. Similarly, data from a Korean cohort reported a mortality rate of 25.5% during a 10-year follow-up [36]. In the latter study, patients hospitalized for acute myocarditis received standard intensive care (43% required IABP, ECMO, mechanical ventilation, CRRT, or cardiopulmonary resuscitation) and typical cardiovascular medications, including ACE inhibitors, angiotensin II receptor blockers, norepinephrine, inotropes, intravenous nitrates, diuretics, antiarrhythmics, MRAs, beta-blockers, and/or digoxin [34].
However, the management, considered the "standard of care," does not necessarily lead to complete recovery or full elimination of viral or bacterial material from cardiac cells [39]. The virus can persist in cardiac tissue, resulting in localized chronic myocarditis. Simultaneously, the innate immune system may remain activated, contributing to ongoing inflammation and myocardial fibrosis, which may eventually progress to DCM [39,43]. Both processes can occur simultaneously. Despite intensive medical treatment, some patients require left ventricular assist devices to enable cardiac recovery; if this fails, HTx may be necessary for survival [37].
Administration of antiviral, antibacterial, and anti-inflammatory medications appears to reduce mortality rates and should be prioritized in both the acute and chronic phases of myocarditis management [1,3,7,38,39]. Addressing infection-induced inflammation remains a major challenge. First, diagnosing the underlying etiology can be difficult. Second, even when the virus or bacteria has been neutralized, autoimmune mechanisms may persist and impede recovery. Among the two main mechanisms preventing myocardial recovery, excessive activation of inflammasomes and cardiac fibrosis come to the fore [40]. Recently, new therapies directly targeting inflammatory pathways and capable of preventing cardiac fibrosis are being evaluated. Some of these have entered randomized clinical trials (RCTs).
The following case of a 64-year-old woman highlights the clinical challenges faced by healthcare providers in managing a patient hospitalized with myocarditis. In this article, we aim to discuss: (1) the human immune defence mechanisms against infection; (2) the role of pyroptosis and excessive immune response in developing complications and chronic active myocarditis; and (3) the potential role of emerging medications in myocarditis management.
2. An illustrative Case Report
A 64-year-old woman with a significant history of internal medicine conditions—including hypertension, dyslipidemia, hypothyroidism, nicotine dependence, degenerative joint disease, and chronic venous insufficiency—presented to the Emergency Department with several days of upper respiratory tract symptoms. She reported sore throat, chest pain while coughing, generalized musculoskeletal pain and stiffness, and subjective fever.
Initial laboratory workup revealed signs of viral infection with elevated inflammatory markers: procalcitonin (PCT) 1.27 ng/mL (reference < 0.5 ng/mL), C-reactive protein (CRP) 98.7 mg/L (reference < 5.0 mg/L), and interleukin-6 (IL-6) 19.2 pg/mL (reference < 7.0 pg/mL). BioFire nasopharyngeal swab tested positive for human metapneumovirus (hMPV). Cardiac biomarkers were markedly elevated: NT-proBNP 6,978 pg/mL (reference < 125 pg/mL), troponin 786 ng/L (reference < 14 ng/L), creatine kinase (CK) 343 U/L (reference < 170 U/L), and CK-MB 20 U/L (reference < 24 U/L), without the dynamic profile typical of ACS.
Transthoracic echocardiography showed globally reduced LV-EF (45%) with hypokinesis of the mid and apical segments of the inferior wall, interventricular septum, and posterior wall (Supplementary 1-A), without pericardial effusion. The patient was admitted to the cardiac intensive care unit for further evaluation and treatment of suspected myocarditis. Following a consultation with an interventional cardiologist, coronary intervention was deferred.
On admission, the patient was conscious and hemodynamically stable. Physical examination revealed crackles in the lower fields of the right lung posteriorly and mid-axillary, and isolated basal crackles in the left lung. There was no peripheral oedema. ECG demonstrated sinus rhythm at 120 bpm, with normal axis and intervals and no significant ST-T abnormalities. Lung ultrasound revealed numerous confluent B-lines in the right lung’s lower posterior and mid-axillary fields, and isolated B- and A-lines in the scapular and paravertebral regions. The left lung showed isolated B-lines. No pleural effusion was observed.
Given her smoking history and occupational exposure to infections (working with children), a chest X-ray was performed (Fig.1A) and showed signs of concurrent pneumonia. Extensive microbiologic and immunologic testing (blood and urine cultures, and serologic IgA/IgG for Chlamydia pneumoniae, IgG for Bordetella pertussis, and Mycoplasma pneumoniae) yielded positive serum results. However, sputum PCR did not confirm bacterial presence, raising suspicion for atypical pneumonia.
Empirical antibiotic therapy was initiated with sulfamethoxazole/trimethoprim, followed by clarithromycin. Subsequent echocardiography showed progressive LVEF decline to 20–25% (Supplementary 1-B), pericardial effusion of 1.2 mm, and generalized hypokinesis, especially in the anterior wall and septum. ECG revealed negative T waves in leads V2–V6. Coronary CT angiography excluded ischemic causes of reduced EF. HRCT confirmed bilateral "tree-in-bud" opacities consistent with atypical pneumonia (Fig.1B). CMR indicated probable myocarditis (Fig.1C,D).
HF therapy was initiated, including an SGLT2 inhibitor, beta-blocker (for rate control), ACE inhibitor, and eplerenone. On day four, ACE inhibitor was replaced by sacubitril/valsartan (Sac/Val), an Angiotensin Receptor-Neprilysin Inhibitor (ARNI) at dose of 24/26 mg daily.
Laboratory parameters improved: CRP fell to 45 mg/L, CK to 247 U/L, troponin from 895 ng/L to 435 ng/L, and PCT to 0.43 ng/mL. IL-6 rose to 59.7 pg/mL. Follow-up echocardiography showed LVEF recovery to 60%.
Given the complete clinical and diagnostic picture, and after informed consent, a LV endomyocardial biopsy was performed (Fig.1E). During the final tissue sampling, the patient experienced angina progressing to cardiac shock with hypotension and tachycardia. Echocardiography revealed pericardial effusion without tamponade. Management included fluid resuscitation, dobutamine and norepinephrine infusions (5 mL/h and 2 mL/h, respectively), and protamine sulfate.
In the following days, the patient's condition worsened with cardiorespiratory failure. Passive oxygen therapy and escalating vasopressors (up to 10 mL/h and 7 mL/h) were required. Labs showed declining hemoglobin and GFR (down to 17 mL/min), necessitating therapy adjustments. Repeated microbiological tests revealed a new Streptococcus pneumoniae infection, complicating prior hMPV infection. Corticosteroids and azithromycin were initiated. The patient underwent cardiopulmonary rehabilitation. Vasopressors were gradually tapered, oxygen weaned, and heart failure therapy resumed. No significant arrhythmia occurred. Due to hypotension, Sac/Val was withheld.
Figure 1.
A. Initial chest X-ray showing inflammatory changes consistent with pneumonia (indicated by the red arrow). B. High-resolution chest CT (HRCT) showing bilateral inflammatory changes with a characteristic "tree-in-bud" pattern (marked by the red arrow). C. Cardiac magnetic resonance (CMR) in a SAX view demonstrating generalized myocardial oedema with late gadolinium enhancement (LGE) highlighted by the red arrow. D. CMR in a four-chamber view demonstrating generalized myocardial oedema with late gadolinium enhancement (LGE) highlighted by the red arrow. E. Fluoroscopic image of a left ventricular muscle biopsy from the apical region, performed under echocardiographic guidance. F. Follow-up chest X-ray at discharge showing gradual resolution of the inflammatory changes.
Figure 1.
A. Initial chest X-ray showing inflammatory changes consistent with pneumonia (indicated by the red arrow). B. High-resolution chest CT (HRCT) showing bilateral inflammatory changes with a characteristic "tree-in-bud" pattern (marked by the red arrow). C. Cardiac magnetic resonance (CMR) in a SAX view demonstrating generalized myocardial oedema with late gadolinium enhancement (LGE) highlighted by the red arrow. D. CMR in a four-chamber view demonstrating generalized myocardial oedema with late gadolinium enhancement (LGE) highlighted by the red arrow. E. Fluoroscopic image of a left ventricular muscle biopsy from the apical region, performed under echocardiographic guidance. F. Follow-up chest X-ray at discharge showing gradual resolution of the inflammatory changes.

Final echocardiography (Supplementary 1-C) showed gradual LVEF improvement and pericardial effusion regression (from 1.5 cm to 0.5 cm). Labs showed normalized inflammation and necrosis markers: NT-proBNP 3017 pg/mL, troponin 21 ng/L, IL-6 9.0 pg/mL, CRP 10 mg/L, PCT <0.05 ng/mL, CK-MB 9 U/L, CK 15 U/L, GFR 97 mL/min. Clinically, the patient remained stable. Chest X-ray showed inflammatory resolution (Fig.1F). She was discharged on bisoprolol 2.5 mg o.d., ramipril 5 mg o.d., dapagliflozin 10 mg o.d., eplerenone 25 mg o.d., and prednisone 20 mg o.d. with a tapering plan.
Histopathology confirmed focal necrosis, adipose infiltration, microvasculopathy with vascular smooth muscle cells (VSMCs) proliferation, and CD68+ macrophages damaging cardiomyocytes—findings consistent with myocarditis. The biopsy suggested the patient had entered chronic active myocarditis (CD68+) [44]. She remains under close cardiology follow-up with echocardiographic monitoring and guideline-directed therapy for HF and chronic myocarditis.
At first phone follow-up, the patient reported clinical improvement, no signs of HF decompensation, and only mild, improving fatigue. She tolerated treatment well. At the next follow-up, HF medications were titrated to maximum tolerated doses, and ARNI was reintroduced. A follow-up echocardiogram was scheduled after one month, and a control CMR at six months post-treatment.
3. Discussion and Literature Review
The presented case of myocarditis is, to our knowledge, the first reported instance of hMPV-induced myocarditis complicated by a subsequent Streptococcus pneumoniae infection in a woman without an underlying immunodeficiency. Following a severe disease course, the patient experienced ‘full recovery’, as demonstrated by normalization of LV-EF to 60% and normalization of inflammatory markers in laboratory tests. However, cardiac biopsy revealed that acute myocarditis had progressed to chronic active myocarditis with myocardial fibrosis and latent viral presence, suggesting incomplete viral clearance, or persistent activation of the innate immune system. In line, NT-pro-BNP levels remained significantly elevated exceeding 3,000 pg/mL. This condition can lead to irreversible chronic HF and DCM, potentially necessitating MCS or HTx.
This highlights the need to investigate novel approaches to immune-mediated myocarditis, in order to reduce chronic inflammation, and adverse cardiac remodeling. Therefore pro inflammatory cytokines engaged in myocarditis that are crucial for host defense, when disease progresses to chronic active inflammation, represents a potential target for pharmacological intervention against infective myocarditis [123].
3.1. Myocarditis Caused by Human Metapneumovirus (hMPV) and Opportunistic Bacterial Streptococcus pneumoniae Infection: A Brief Literature Review
hMPV is a paramyxovirus first identified in 2001 [45]. It is now recognized as a common cause of respiratory tract infections [46]. However, cardiac involvement in hMPV infections is extremely rare [47]. Only a few case reports describe hMPV-associated myocarditis, typically in immunocompromised individuals. Makhlouf et al. reported a case of a 14-year-old girl with Burkitt leukemia who developed severe hMPV-induced myocarditis, diagnosed using real-time PCR and CMR [48]. The patient was successfully treated with intravenous immunoglobulins. Wang et al. described hMPV-induced myocarditis complicated by Klebsiella pneumoniae co-infection in a 68-year-old man with liver cirrhosis [49]. The patient rapidly deteriorated, developed septic shock, and required intensive care, including ECMO, IABP, vasopressors, and broad-spectrum antibiotics. hMPV infections are known to be more severe in patients with immunodeficiency syndromes, autoimmune diseases (e.g., lupus, rheumatoid arthritis), HIV, cancer, or those receiving chemotherapy or immunosuppressive therapies [47]. The exact way in which hMPV invases cardiomyocytes is not well known. However, the G and the F proteins of hMPV play a crucial role in the initial stages of respiratory tract infection [50]. The first one, facilitates viral attachment and entry into host cells, whereas the F protein of hMPV mediates viral-host membrane fusion, transcription and subsequent infection [50]. Integrins and heparan sulfate proteoglycans (HSPGs) have been implicated in the fusion and internalization processes [51,52,53]. HSPGs are the same entry receptors for various viruses, such as respiratory syncytial virus: RSV, SARS-CoV-2, human immunodeficiency virus: HIV, and herpes simplex virus: HSV [50,52].
The G and F proteins are involved in modulating the host immune response, evading immune surveillance [54]. These functions enable hMPV to infect host cells more efficiently and replicate successfully. hMPV avoids host immune response and apoptosis due to the small hydrophobic (SH) protein of hMPV [55,56]. Studies suggest SH protein may be a viroporin forming ion channels [57]. It is believed to regulate host immune response through the NF-kB and the NLRP3 inflammasome [57]. hMPV activates NOD-like receptor protein 3 inflammasome via its SH protein [57]. The contribution of NLRP3 inflammasome in the pathogenesis of RNA viruses occurs through its role as a trigger of inflammation, or both inflammation and viral replication [58,59].
Host immune factors can either promote or inhibit hMPV infection and replication. Among host restriction factors, leading to virus eliminations, are cellular proteins that inhibit viral replication and spread [50,51]. The key host restriction factors for hMPV include 1) interferon-induced transmembrane proteins (IFITMs) that prevent viral entry and membrane fusion; and 2) retinoic acid-inducible gene I (RIG-I); and 3) melanoma differentiation-associated gene 5 (MDA5) that activate NF-kB and IRF transcription factors [50,51,60,61,62]. Whereas, several host-promoting factors facilitate hMPV infection and replication within the host, including toll like receptor 4, and -7 (TLR4), protease-activated receptor 1 (PAR-1) and transmembrane protease, serine 2 (TMPRSS2) [63,64,65]. The TLR 4 and 7 reduce infiltration of inflammatory cells; facilitate viral entry; alter endosomal conditions. The PAR-1 promotes viral replication, while TMPRSS2 facilitates viral fusion.
Unfortunately, there is no solid treatment or vaccine for hMPV so far, the lack of vaccines is a significant factor leading to a large number of hospitalizations during the epidemic season [66]. After many attenuated vaccines failed due to insufficient attenuation or poor protective effects, subunit vaccine became the main focus of research [67]. Recently, Ma et al. presented a novel multi-epitope mRNA vaccine candidate to combat HMPV virus [68].
In the present case, hMPV-induced myocarditis was complicated by a secondary Streptococcus pneumoniae infection a few days later. Streptococcus pneumoniae is known to translocate into the myocardium and form microlesions that impair cardiac function [19]. Pneumolysin (PLY), a pore-forming toxin produced by S. pneumoniae, is a key factor in this process [69]. Experimental studies have shown that microlesion formation requires the interaction of bacterial adhesin CbpA with the host laminin receptor and the bacterial cell wall with platelet-activating factor receptor (PAFR). Pneumococci utilize PAFR to cross barriers, such as from lungs to bloodstream, facilitating progression from pneumonia to bacteremia [70]. In phagocytic cells, cell wall components interact with toll-like receptor 2 (TLR) to activate NF-κB signaling and cytokine production. Surprisingly, no significant changes were detected in classic NF-κB target genes including TNF-α, IL-1β, and I-κB meaning that the signal was too weak to activate enough the TLR-2 - NF-κB pathway [70]. These findings suggest that S. pneumoniae invades cardiac tissue in a PAFR-dependent but TLR2-independent manner and impairs myocardial contractility without causing cardiomyocyte death [70]. Microlesion formation also required PLY [19]. Importantly, despite specific for Pneumococci antibiotic treatment, a robust collagen deposition at former lesion sites, consistent with extensive scarring are reported. This may explain adverse cardiac events during and after invasive pneumococcal disease [19]. Like in hMPV infection, a vaccination against B Streptoccocus could protect the presented patient against cardiac complications [71].
3.2. Progression from Acute to Chronic Active Myocarditis
While acute immune activation is essential for host defense, excessive or prolonged responses may be harmful [72]. The possibility of myocarditis progressing from an acute to chronic phase, often with mixed etiology, is critical for patient management. It also highlights the need for targeted pathogen-specific treatment and understanding the variability of innate immune responses.
The immune system plays a central role in the pathogenesis and progression of cardiovascular disease (CVD) [72]. Macrophages are key players in the inflammatory cascade, secreting cytokines that fight pathogens through pyroptosis (a form of programmed cell death) while simultaneously recruiting other immune cells to the infection site [73,74]. Interleukin-1β (IL-1β) and IL-18 promote T lymphocyte activation and amplify cytokine and chemokine production [75]. Pathogen-specific immune responses converge on the activation of N-terminal gasdermin D (Nt-GSDMD), which forms pores in the cell membrane, disrupting membrane integrity, causing osmotic imbalance and leakage of intracellular contents—key features of pyroptosis [76]. In parallel, protein complexes cleave pro-caspase-1 to active caspase-1, which then processes pro-IL-1β and pro-IL-18 into their active forms IL-1β and IL-18 that are released during cell pyroptosis [77]. These cytokines amplify inflammation by recruiting more immune cells to the site [78]. IL-1 is linked to fever and leukocyte stimulation to release IL-6, IL-8, TNF-α, MCP-4, IP-10, CD40, RANTES (CCL5), and IL-18 [75]. These mediators further escalate the inflammatory response [79,80]. IL-18 is especially important in defending against intracellular pathogens via NK and Th1 cells, which produce interferon-γ (IFN-γ) [81]. Like IL-1, IL-18 is synthesized as an inactive precursor (pro-IL-18) that must be cleaved by caspase-1—an enzyme activated within the NLRP3 inflammasome complex, consisting of NLRP3, pro-caspase-1, and apoptosis-associated speck-like protein containing a caspase recruitment domain (ASC) [81,82].
Caspase-1 can also be activated by other inflammasomes that belong either to the AIM2-like receptors, NOD-like receptors, or the TRIM family, which contain PYD or CARD domains [83,84]. In the presence of IL-12, IL-18 activates Th1 cells, macrophages, NK cells, NKT cells, B cells, DCs, and naive T cells to produce IFN-γ, essential for clearing intracellular infections [85,86]. In the absence of IL-12, IL-18 and IL-2 induce Th2 cytokines in NK and NKT cells and stimulate IFN-γ secretion in CD3-activated Th1 cells [86]. IFN-γ is vital for microbial clearance via nitric oxide synthase 2 (NOS2) activation [87]. The pathways leading to cell death and cytokine release vary depending on the pathogen [88]. At least four major inflammasome pathways are currently recognized [89]. The key mechanisms by which inflammasomes oligomerize pro-caspase-1 into active caspase-1 and facilitate GSDMD cleavage, along with IL-1β and IL-18 maturation, are illustrated in Figure 2.
3.3. Role of Inflammasomes in Myocarditis
The innate immune system detects both microbial invaders and sterile danger signals via pattern recognition receptors (PRRs). PRRs are expressed on the cell surface, intracellular vesicles, and in the cytosol of monocytes, macrophages, neutrophils, mast cells, dendritic cells, and natural killer (NK) cells [90]. Microbial components detected by PRRs are termed pathogen-associated molecular patterns (PAMPs), while endogenous danger molecules are called damage-associated molecular patterns (DAMPs), often arising from tissue damage or oxidative stress [91]. PRRs are classified into several major families based on protein domain homology: toll-like receptors (TLRs), NOD-like receptors (NLRs), C-type lectin receptors (CLRs), absent in melanoma 2 (AIM2)-like receptors, retinoic acid-inducible gene-I (RIG-I)-like receptors, cyclic GMP-AMP synthase (cGAS)–stimulator of interferon genes (STING), and Pyrin [92]. TLRs and CLRs are transmembrane receptors, while NLRs are cytoplasmic [91].
Among NLRs, NLR family pyrin domain containing 3 (NLRP3) is the best studied in relation to myocarditis [92]. The NLRP3 pathway has also been implicated in various inflammatory conditions, including atherosclerosis, Alzheimer's disease, gut microbiota dysbiosis, and skin disorders such as urticaria [93,94,95,96,97,98]. Upon recognizing PAMPs or DAMPs, certain PRRs oligomerize and assemble with other proteins to form an inflammasome. A central component in this process is pro-caspase-1, which is activated via oligomerization to caspase-1 in mechanisms involving the NLRP3 pathway [99]. Other pathways include direct activation by cytosolic lipopolysaccharide (LPS) from Gram-negative bacteria, which activates caspase-11 (and its human homologs, caspase-4 and -5) [100].
3.3.1. The NLRP3 Pathway
The canonical NLRP3 pathway requires two steps: priming and activation. Priming begins with pathogen recognition by pyrin domain-containing PRRs such as NLRP3. Recognition of stimuli like viral RNA, bacterial toxins, toxins, drugs, K+ efflux, Ca2+ mobilization, ER stress, lysosomal rupture, or mitochondrial dysfunction primes NLRP3. Activation involves NF-κB pathway stimulation, which is initiated by degradation of the NF-κB inhibitor via IκB kinase [101,102]. Activated NF-κB leads to recruitment of ASC and pro-caspase-1 [103]. Cl- efflux enables NEK7 attachment, facilitating pro-caspase-1 oligomerization and forming the NLRP3-ASC-caspase-1 complex, known as the NLRP3 inflammasome. Caspase-1 has dual roles: (1) it cleaves and activates pro-inflammatory cytokines IL-1β and IL-18; (2) it processes full-length gasdermin D (GSDMD) into N-terminal (NT-GSDMD) and C-terminal fragments. NT-GSDMD forms membrane pores, initiating pyroptosis and cytokine release, including TNF-α and further NF-κB activation [96].
NLRP3 inflammasome activation has been demonstrated in myocarditis induced by CVA16, CVA10, and encephalomyocarditis virus (EMCV) [93]. EMCV-induced myocarditis relies on viral protein 2B, which promotes Ca2+ flux from the ER and Golgi into the cytoplasm, alongside K+ efflux [104,105,106]. SARS-CoV-2 enters cardiomyocytes via its spike protein binding to ACE2 with TMPRSS2, potentially activating NLRP3 inflammasomes and promoting inflammation [107,108].
3.3.2. CARD8 Pathway
In the CARD8 pathway, bacterial components induce proteasomal degradation of the CARD8 sensor, releasing the CARD-UPA domain. This domain recruits and activates pro-caspase-1, forming the CARD8 inflammasome. Caspase-1 then processes pro-IL-1β, pro-IL-18, and GSDMD, similar to the NLRP3 pathway [109].
3.3.3. AIM2 Pathway
AIM2 detects cytosolic double-stranded DNA (dsDNA), leading to ASC and pro-caspase-1 recruitment and inflammasome formation. Activated caspase-1 then processes IL-1β and IL-18, and cleaves GSDMD. The NT-GSDMD fragment forms membrane pores, facilitating cytokine release and pyroptosis [109].
3.3.4. Caspase-11 Inflammasome
In mice, caspase-11 (and human caspase-4 and -5) directly bind cytosolic LPS from Gram-negative bacteria such as Escherichia coli, Salmonella typhimurium, Shigella flexneri, and Burkholderia thailandensis [109]. When mice are infected by Gram-negative bacteria, LPS directly binds to the CARD of Caspase-11, thus activating Caspase-11, the activating progress of human Caspase-4 and Caspase-5 is the same as that of caspase-11 [109]. Inflammatory caspases-4/11 can directly bind the lipid A moiety of LPS, however, how LPS that sequestered in the membranes of cytosol-invading bacteria activates non-classical caspases remains not fully understood. In summary, in this mechanism under the stimulation of LPS, the caspase-11 inflammasome is formed, gains proteolytic activity, and cleave [109].
3.4. Post-Infectious Phase
The exact mechanisms underlying hMPV-induced myocarditis remain unclear [110]. Current evidence suggests it results from both direct viral invasion and immune-mediated mechanisms [111,112]. Immune evasion by the virus enables persistence and tissue damage. Altered immune responses may contribute via molecular mimicry or bystander activation [113,114,115]. In addition, the patient in this case was a regular smoker (one pack/day), which may have contributed to endothelial injury and HF progression [116]. Nicotine upregulates NLRP3 expression [117], promotes monocyte adhesion, and foam cell formation. After endothelial dysfunction, monocytes adhere to vascular lesions, differentiate into macrophages, and engulf lipoproteins like oxLDL and ChCs [118]. These macrophages become foam cells, which promote chronic inflammation [119,120].
3.5. Therapeutic Approaches in VMC Based on Pathogen and Disease Phase
During early acute myocarditis, the innate immune response facilitates pathogen clearance. At this stage, targeting viral or bacterial agents is essential. However, if the inflammatory response persists, myocarditis can evolve into chronic active myocarditis—a detrimental condition requiring more comprehensive immune-modulating strategies [120].
VMC typically begins with the infection of cardiomyocytes by cardiotropic viruses such as enteroviruses (e.g., CVB3), adenoviruses, or parvovirus B19 [117]. Viral entry into cardiomyocytes is mediated by specific cellular receptors such as the coxsackievirus and adenovirus receptor (CAR). Once inside the cell, viral replication causes direct cytopathic effects and the release of viral proteins and nucleic acids, which are recognized as PAMPs. These activate PRRs, mainly toll-like receptors (TLRs) including TLR3, TLR4, and TLR7, present on cardiomyocytes and resident immune cells.
TLR activation triggers downstream signaling pathways including NF-κB and interferon regulatory factors (IRFs), as well as the activation of the NLRP3 inflammasome. This promotes the maturation and secretion of IL-1β and IL-18, and upregulates other pro-inflammatory cytokines and chemokines such as TNF-α, IL-6, IFN-α, and IFN-β [121]. These mediators recruit innate immune cells (macrophages, neutrophils) into the myocardium. As inflammation progresses, dendritic cells present viral antigens to CD4+ and CD8+ T lymphocytes. CD8+ T cells kill infected cardiomyocytes, while CD4+ T cells coordinate cytokine production and support B-cell mediated antibody responses [122]. While this response is initially protective, sustained inflammation can cause myocardial injury, fibrosis, and progression to chronic cardiomyopathy or dilated cardiomyopathy (DCM) [123]. Thus, balancing effective viral clearance with limiting inflammation is crucial [124].
3.5.1. Specific Antiviral Therapy in Acute Phase of Myocarditis
Viruses commonly linked to myocarditis include adenoviruses, enteroviruses (CVA/B, echoviruses), parvovirus B19, human herpesvirus 6 (HHV6), Epstein-Barr virus, cytomegalovirus, HIV, hepatitis C virus, influenza A/B, MERS-CoV, SARS-CoV, and SARS-CoV-2 [125]. Most VMC is managed symptomatically or supportively. Some viruses such as adenoviruses and enteroviruses are readily cleared from cardiomyocytes, whereas others (e.g., parvovirus B19, HHV6, Epstein-Barr virus, cytomegalovirus) tend to persist, contributing to HF, DCM, and arrhythmias, depending on host immune function [126,127,128].
Specific therapy includes interferon and immunoglobulin-based immunomodulation. In a pilot study by Kuhl et al., IFN-β cleared enterovirus/adenovirus in 100% of patients and improved LV function in 68% [126]. IFN-β also reduced viral load in chronic myocarditis due to enterovirus, adenovirus, or B19V [127]. Intravenous immunoglobulin therapy (IVIG), with IgG, or polyvalent IgG/IgA/IgM, may improve survival in children and adults with VMC.
3.5.2. Immunosuppression in Active and Chronic Active Myocarditis
Glucocorticoids are first-line therapy in hemodynamically unstable or fulminant myocarditis [129]. A ‘Life support-based comprehensive treatment regimen” includes MCS devices, ventilation, dialysis, and high-dose glucocorticoids (200–400 mg methylprednisolone daily for several days) and IVIG, avoiding cytotoxic agents [130]. Without glucocorticoids/IVIG, benefits such as nitric oxide promotion, myocardial edema reduction, and cardiomyocyte survival are diminished [131]. Cytotoxic agents alone did not improve survival in fulminant myocarditis, as shown in the Myocarditis Treatment Trial [131]. The application of cytotoxic drugs could only gradually downregulate the cytokine levels. Immunosuppressive agents used in chronic active myocarditis include prednisolone alone or in combination with azathioprine or cyclosporine [132]. While some trials showed improved LV/RV function, survival benefits varied [133,134,135,136,137]. Long-term mortality was high, and routine immunosuppression was not supported by the Myocarditis Treatment Trial [137].
3.6. Targeting Inflammasomes: A Future for Myocarditis?
hMPV activates NLRP3 inflammasome via its SH protein [55]. Likewise, many other viruses activate infection through this pathway. Therefore, the blockade of IL-1β production by using NLRP3 inflammasome inhibitors or the inhibitors of cascade factors eventually leading to activation of NLRP3 might be a novel potential strategy for the therapy and prevention of hMPV infection (Table 1).
3.6.1. Inhibition of NF-κB Pathway
Inhibiting NF-κB is a potential therapeutic strategy, particularly in cancer [138]. Drugs like aspirin, salicylates, dexamethasone, and natural products including curcumin, resveratrol, and epigallocatechin gallate suppress NF-κB activity [138,139,140]. However, it is important to note that targeting NF-κB indirectly, for instance through proteasome inhibition, carries a risk of off-target effects. Bortezomib (BTZ), Ixazomib and Carfilzomib are proteasome inhibitors used in the treatment of multiple myeloma (MM) and other hematological malignancies; these agents block IκB degradation and thereby inhibit NF-κB activation. Despite their clinical efficacy, they have been associated with adverse cardiac effects, including arrhythmias, HF, and inflammatory complications such as pericarditis and myocarditis [141]. These observations highlighting the delicate balance between therapeutic benefit and cardiotoxicity when modulating key inflammatory pathways such as NF-κB in oncology.
3.6.2. Direct NLRP3 Inhibitors
Acute inflammasome activation is beneficial for infection defense but harmful when prolonged. Direct NLRP3 inhibition is thus a therapeutic option in chronic active myocarditis. In murine models of sepsis and LPS-induced cardiac injury, corticosteroids suppressed NLRP3 formation, cysteine asparaginase-1 activation, and IL-1β secretion [142]. This demonstrates that cortisone is a novel immunomodulatory factor with the ability to inactivate NLRP3 inflammasomes and protect the myocardium from septic injury. NLRP3 inhibition (e.g., MCC950) reduced arrhythmias and remodeling in myocarditis. In rats with myosin peptide-induced myocarditis (experimental group) treated with an NLRP3 inhibitor (MCC950; 10 mg/kg, daily for 14 days) for three weeks or left untreated (Table 1). MCC95 mitigated the myocarditis-induced leakage of Ca2+; this finding suggests that activation of CaMKII is crucial for the effects of myocarditis on RVOT cardiomyocytes [142].
3.6.3. Colchicine
Colchicine has broad anti-inflammatory effects and it is a potent inhibitor of tubule polymerization. Colchicine disrupts microtubules that are responsible for the subcellular transport of ASC and NLRP3 within macrophages and are necessary for proper cytosolic localization and activation of the NLRP3 inflammasome components. Recent studies suggest benefits in acute and chronic myocarditis (Table 1) [143,144,145,146,147]. In one study, colchicine reduced 90-day mortality, arrhythmia, and HF (193 [17.0 %] versus 279 [24.5 %], Log-rank p < 0.001; HR 0.66, 95%CI [0.55–0.79], respectively) [143]. Side effects were mild. Another study showed fewer recurrences (respectively, 19.2% vs 43.8%; p=0.001) and a longer event-free survival (p=0.005) in 175 patients with idiopathic/viral etiology of myocarditis receiving colchicine [144]. Colchicine was well-tolerated and colchicine-associated side effects were mild and occurred in 3 (1.7%) patients [144]. Pappritz et al. demonstrated that colchicine treatment significantly reduced cardiac inflammation and improved LV function in a murine model of autoimmune myocarditis [146]. As yet, the only published, randomized controlled trial (RCT) with colchicine in myocardial injury due to COVID 19 infection, the GRECCO-19 trial, showed that patients who received colchicine had significantly improved time to clinical deterioration [147]. Whereas, there were no significant differences in hs-Tn or CRP levels [147].
These findings support the hypothesis that targeting microtubule dynamics and inflammasome activation may translate into clinical benefit. Ongoing clinical trials, including NCT05855746 (Colchicine vs. placebo in acute myocarditis; https://clinicaltrials.gov/study/NCT05855746) and CMP-MYTHiC NCT06158698 (Colchicine in cardiomyopathy and myocarditis; https://cdek.pharmacy.purdue.edu/trial/NCT06158698/) aim to assess the efficacy and safety of colchicine in human myocarditis. Preliminary data and experimental results suggest that colchicine could become a valuable adjunctive therapy by reducing myocardial inflammation, limiting adverse remodeling, and potentially improving long-term cardiac outcomes.
3.6.4. Dapansutrile (OLT1177)
Dapansutrile is an oral NLRP3 inhibitor tested in phase 1B trial in 30 patients with stable HFrEF [148]. Improvements in LVEF [from 31.5% (27.5–39) to 36.5% (27.5–45), P = 0.039] and in exercise time [from 570 (399.5–627) to 616 (446.5–688) seconds, P = 0.039] were seen in the dapansutrile 2000 mg cohort (Table 1) [148]. It was well tolerated and reduced IL-1β and IL-18, supporting its use in inflammasome-driven cardiac inflammation [148]. Dapansutrile anti-inflammatory effect is obtained by directly blocking the assembly and activation of the NLRP3 inflammasome complex. Thus, dapansutrile prevents downstream release of pro-inflammatory cytokines such as IL-1β and IL-18, which are implicated in cardiac inflammation and remodeling.
If other studies support dapansutrile efficacy, it is potentially new drug for use in cardiovascular conditions associated with excessive inflammasome activation.
3.6.5. INF200
INF200 is a selective oral NLRP3 inflammasome inhibitor, a novel small-molecule inhibitor structurally based on the 1,3,4-oxadiazol-2-one scaffold. It in the experimental study by Wang et al. [149], it reduced inflammation, fibrosis, and cardiomyocyte apoptosis, and improved LV function (Table 1) [149]. These findings suggest that INF200 not only attenuates the inflammatory response but also protects against structural remodeling of the myocardium.
3.6.6. Canakinumab
Canakinumab is a monoclonal antibody targeting IL-1β. It is approved by the U.S. Food and Drug Administration for the treatment of systemic juvenile idiopathic arthritis, active Still disease, and certain types of auto inflammatory periodic fever syndromes. In the CANTOS trial (n=10,061), patients who received the intermediate canakinumab dose (150 mg) had reduced a primary endpoint, and a composite of cardiovascular death, nonfatal acute MI, or nonfatal stroke, and systemic inflammation (IL-6, CRP) (Table 1) [150].
3.6.7. Anakinra and IL-1 Receptor Accessory Protein Monoclonal Antibody
Anakinra inhibits IL-1 receptor 1, thereby inhibiting both IL-1β and IL-1α. It is already approved for other inflammatory conditions [151]. In the MRC-ILA (Medical Royal Council InterLeukin-1 Antagonist) heart study, patients with non–ST-segment elevation ACS were randomized to daily administration of anakinra or matching placebo for 2 weeks (Table 1) [152]. Anakinra reduced CRP and IL-6, but increased major adverse cardiac events at 1 year [152]. In VCU-ART3 trial (Virginia Commonwealth University Anakinra Remodeling Trial 3), anakinra reduced HF incidence in STEMI patients when given within 12 hours after the onset of symptoms [153].
Formerly published case reports of fulminant myocarditis showed the spectacular efficacy of IL-1 blockade with anakinra [154,155]. Promising results led to the ARAMIS trial investigating anakinra in acute myocarditis [156]. The ARAMIS trial is pending a multicenter, randomized, placebo-controlled study designed to assess the efficacy and safety of anakinra in patients with acute myocarditis. Patients receive anakinra for 14 days, with the aim of reducing myocardial inflammation by blocking IL-1α and IL-1β signaling. Preliminary results have shown a significant reduction in systemic inflammatory markers such as CRP and IL-6, along with encouraging trends toward improved LV function. While long-term clinical outcomes are still under investigation, the study supports the potential role of IL-1 blockade as a targeted therapy in acute myocarditis.
In addition, a recent study demonstrated an advantage of IL-1 receptor accessory protein (IL1RAP) blockade with a monoclonal antibody [157]. IL1RAP (also called IL1R3) is a shared subunit for the IL-1, IL-33 and IL-36 isoform receptors. An IL1RAP blockade might be a potential therapeutic strategy in viral and autoimmune myocarditis. IL1RAP blockade reduced inflammatory monocytes, T cells, neutrophils, and eosinophils in the heart in CVB3-mediated VMC in mice compared with placebo and IL1Ra (anakinra) treatment alone [157]. In conclusion, IL1RAP blockade reduced cardiac inflammation and disease severity in VMC and protected against cardiac dysfunction in autoimmune myocarditis, with higher efficacy compared with anti-IL-1 treatment alone.
3.6.8. Monoclonal Antibodies and Drugs Targeting IL-18
Recently, a novel humanized monoclonal anti-human IL-1R7 antibody that specifically blocks and suppresses the inflammatory signaling of IL-18 was developed [158,159,160]. It acts by reducing IL-18 induced NF-κB and IFN-γ activation and IL-6 production in human cell lines. As yet, many researchers use IL-18 as a marker of inflammasome activation [160]. In recent studies, the strategy of blocking IL-1R7 in hyperinflammation in vivo using animal models was explored (Table 1) [158,159]. It is important to note that IL-1R7 is a potential virgin therapeutic strategy for the investigation of its clinical potential in treating IL-18 mediated diseases as this area remains to be explored [158,159,160].
3.7. Angiotensin Receptor-Neprilysin Inhibitor (ARNI)
Sacubitril/valsartan (Sac/Val) is an angiotensin receptor-neprilysin inhibitor (ARNI) that has an established role in chronic HFrEF as it decreases the risk of death and hospitalization [161,162,163,164,165]. In RCT, Sac/Val reduced cardiovascular mortality (by 20%) and all-cause mortality (by 16%) compared to enalapril [165]. However, RCT excluded patients with ACS <4 weeks, primary hypertrophic or infiltrative DCM, acute myocarditis, constrictive pericarditis or tamponade, active infection, planned LVAD, and other specific conditions [165,166,167]. Furthermore, data for Sac/Val use in patients in NYHA class IV and requiring inotropic therapy are limited [165]. In PARADIGM-HF and OUTSTEP-HF trials, only 0.7% of patients had New York Heart Association (NYHA) functional class IV symptoms [165,166]. The multicenter PIONEER-HF trial assessed the impact of Sac/Val on NT-pro-BNP and high-sensitivity cardiac troponin T (hs-TnT) levels, and HF hospital admissions in patient hospitalized for acute HF after obtaining HF stabilization [167]. A greater reduction in the NT-pro-BNP, hs-TnT, and lower rate of re-hospitalization for HF in Sac/Val arm compared to enalapril arm was observed at 4 and 8 weeks (Table 2). LIFE trial that was scheduled to assess Sac/Val in patients with HFrEF and recently advanced HF (NYHA class IV) have not randomized a predefined group of 400 patients, as it was terminated prematurely due to COVID-19 pandemic [168]. The results of LIFE trial in a group of 335 patients showed that Sac/Val was not superior to valsartan and had a 29% discontinuation rate during the 24 weeks of the trial [168,169]. Compared to valsartan, treatment with Sac/Val have not improved the clinical composite of number of days alive, out of hospital, and free from HF events [169].
3.7.1. Off-Label Use of ARNI
There is no evidence of benefits from the prescription of Sac/Val in patients in acute HF, non-ischemic cardiomyopathy such as chemotherapy induced DCM, or acute myocarditis [170]. Despite limited data, clinicians often prescribe Sac/Val based on its beneficial mechanisms, such as enhancing bioavailability of circulatory and myocardial nitric oxide, which leads to an increase in cyclic guanosine monophosphate (cGMP) and the activation of the protein kinase G, reducing fibrosis and inflammation [171,172,173]. CMR studies show reduced LV scarring, improved LV contractility, and faster recovery [174].
3.7.2. ARNI in Acute Myocardial Infarction: RCT Results
In patients who suffered from MI, use of ARNI occurred superior compared with the use of ACE inhibitors or ARBs alone [175]. The use of ARNI in patients with acute MI was not associated with a significantly lower incidence of death from cardiovascular causes or incident HF than ramipril [176]. The PARADISE-MI trial was a large randomized study evaluating the effects of Sac/Val compared to ramipril in patients following acute MI with reduced LVEF (≤ 40%) and signs of HF or pulmonary congestion. A total of 5661 patients underwent randomization within 7 days post-MI; 2830 were assigned to receive Sac/Val and 2831 to receive Ramipril [176]. Over a median of 22 months, a primary-outcome (cardiovascular death, HF hospitalization, or outpatient HF) occurred in 338 patients (11.9%) in the Sac/Val group and in 373 patients (13.2%) in the ramipril group (NS). However, compared to ramipril, Sac/Val showed a trend toward fewer HF events and a lower incidence of hypotension.
3.7.3. ARNI in Doxorubicin-Induced DCM
Doxorubicin, an anthracycline chemotherapeutic agent used in various cancers, is well-known for its dose-dependent cardiotoxicity leading to DCM. Established doxorubicin cardiomyopathy is often fatal, with mortality reaching approximately 50% after the onset of HF [177]. Therefore, patients receiving doxorubicin should be closely monitored with regular HF symptom assessment, echocardiography, and biomarkers such as NT-proBNP, as DCM is typically irreversible once it occurs. Currently, there is no effective treatment for established doxorubicin-induced cardiomyopathy. This is due to the complex mechanisms of doxorubicin cardiotoxicity, including ROS generation, NLRP3 inflammasome activation, IL-1β secretion, pyroptosis, matrix metalloproteinase activity, mitochondrial dysfunction, apoptosis and autophagy of cardiomyocytes, resulting in progressive LV dilation and systolic dysfunction [178,179,180]. It is postulated that both doxorubicine-related cardiac toxicity can be attenuated by Sac/Val administration [181,182]. Experimental studies have shown promising results with Sac/Val. In rodents, ARNI therapy reduced cardiac toxicity and fibrosis more effectively than valsartan alone, and this benefit was associated with modulation of matrix metalloproteinases activity [181]. In a Sac/Val treated rats an attenuated histological evidence of cellular toxicity and fibrosis was found [181]. In mice, Sac/Val attenuated inflammation, fibrosis, and apoptosis while promoting autophagy via the AMPKα–mTORC1 pathway [183]. Dindas et al. also showed that Sac/Val reduced oxidative stress and caspase-3 activation [184]. Moreover, combined low-dose ARNI with SGLT2 inhibitors showed the highest survival rates and minimal toxicity in mice models [185]. The survival rate, of acute doxorubicin-injected mice, in treatment groups including SGLT2i only, ARNI only, and ARNI/SGLT2i combination, increased up to 66.7%, 50%, and 66.7%, respectively, from 25% in doxorubicin + vehicle group [186]. Of note, low-dose ARNI/SGLT2i group showed the highest survival (85.7%), whereas high-dose ARNI was associated with high cardiac toxicity [186]. Also, a recent study showed that low dose of Val/Sac leads to successful reversal of acute HF in chemotherapy-induced cardiomyopathy [187].
These findings suggest translational potential for ARNI therapy in myocarditis, which shares similar inflammatory and fibrotic pathways with doxorubicin cardiotoxicity.
3.7.4. Potential of ARNIs in Acute Myocarditis: A Review of the Literature
Although ACE inhibitors remain foundational in HF treatment, ARNIs such as Sac/Val are increasingly used when ACE inhibitors therapy is insufficient [188,189,190]. In acute myocarditis, Sac/Val has shown superior outcomes in improving LV contractility and reducing dilation compared to ACE inhibitors. Nesukay et al. demonstrated improved outcomes with Sac/Val compared to ACE inhibitors after six months treatment in patients with reduced initial LV-EF ≤ 40% (β=0.601; р=0.016), decreased longitudinal and circular global LV systolic deformation of ≤ 8.5% (β=0.687; р=0.012) and ≤9.0% (β=0.611; р=0.024), respectively, LV dilatation with end-diastolic volume index ≥ 102 ml/m2 (β=0.712; р=0.006), NYHA III or higher functional class (β=0.425; р=0.047), the presence of LV delayed enhancement in at least five segments or more according to CMR data (β=0.548; p=0.031) [191].
The anti-inflammatory effects of Sac/Val have been further elucidated in the study by Liang et al. who demonstrated that beyond its established role as a neoprilysin inhibitor and angiotensin receptor blocker, Sac/Val inhibits the NLRP3 thus IL-1β–mediated inflammatory pathway in the myocardium [192]. In experimental models, treatment with Sac/Val reduced levels of key inflammatory cytokines, including IL-6 and TNF-α, and attenuated cardiac fibrosis and adverse remodeling [193]. Of note, Zile et al. reported that aldosterone, ST2 (soluble tumorigenicity suppressor 2, a receptor from the interleukin-1 family associated with cardiac remodeling and fibrosis), TIMP-1 (metallopeptidase inhibitor 1), MMP-9, PINP (aminoterminal propeptide of type I collagen), and N-terminal propeptide of procollagen type III had decreased more in the Sac/Val group than in the enalapril group eight months after randomization [194]. Liang et al. demonstrated that Sac/Val alleviates myocarditis by inhibiting Th17 cell differentiation independently of the NLRP3 inflammasome pathway [192]. Reduction in levels of all aforementioned biomarkers might have beneficial pleiotropic effect in myocarditis, reducing fibrosis, inflammation and arhythmogenesis.
These anti-inflammatory properties support Sac/Val's role in mitigating myocardial inflammation and improving long-term cardiac function following injury.
3.8. Role of Cardiac Fibrosis and Anti-fibrotic Treatment Approaches
Cardiac fibrosis is a maladaptive process marked by excessive extracellular matrix (ECM) deposition, primarily of collagens I and III [195,196]. This increases myocardial stiffness, reduces compliance, and impairs systolic and diastolic function, contributing to HF progression. In clinical practice, the effect of cardiac fibrosis can be observed on CMR and biochemical markers of HF [197,198]. Fibrosis arises from interactions among inflammatory, neurohormonal, molecular and profibrotic signaling pathways [199,200,201]. Injury or chronic stress activates immune cells (macrophages, mast cells), which secrete pro-inflammatory cytokines (IL-1β, IL-6, TNF-α), promoting fibroblast activation. A pivotal mediator of fibrogenesis is transforming growth factor-beta (TGF-β), which promotes the differentiation of resident cardiac fibroblasts into activated myofibroblasts cells that secrete large quantities of ECM components. TGF-β signals through canonical Smad-dependent pathways and alternative non-canonical pathways, leading to transcriptional upregulation of genes involved in collagen synthesis and fibrosis [202,203,204]. The renin–angiotensin–aldosterone system (RAAS), in particular angiotensin II via the angiotensin type 1 (AT1) receptor, promotes fibroblast activation, and TGF-β upregulation [201,204]. Moreover, angiotensin II activates NADPH oxidase, resulting in the generation of reactive oxygen species (ROS), which further amplify pro-inflammatory and profibrotic signaling cascades.
Therefore, targeting fibroblasts’ proliferation might have potential to confer myocardial fibrosis [205]. Previous studies in HFpEF patients using antifibrotic medications, such as ACE inhibitors, ARBs and aldosterone antagonists showed some long-term benefit in reducing fibrosis but do not reduce mortality [206,207]. In 35 patients with acute myocarditis and normalized LV-EF from the initial LV-EF < 45% taking ACE inhibitors, prolonged treatment with ACE inhibitors was associated with lower incidence of new episodes of HFrEF < 45%, compared with patients who stopped taking ACE inhibitors (5% vs 33%, P=0.064), and their LV-EF was higher at 3-years follow-up (57±11% vs 47±12%, P=0.002), with no difference in mortality rate [206]. These results suggest that ACE inhibitors should be continued over the long term in these patients. The results of a meta-analysis of six studies including in total 706 patients suggested that ACE inhibitors can effectively inhibit collagen synthesis and deposition in the myocardium, potentially preventing, or even reversing, the progression of myocardial fibrosis [207]. ARBs mitigate fibrosis by inhibiting AT1 receptor and reducing cytokine expression. This blockade not only reduces afterload and blood pressure but also directly attenuates fibroblast activation and decreases TGF-β–driven collagen synthesis. Additionally, ARBs have been shown to dampen the production of pro-inflammatory cytokines, highlighting their dual hemodynamic and anti-inflammatory effects [208]. Seko et al. demonstrated an anti-inflammatory effect of the ARB olmesartan on the development of murine acute myocarditis caused by viral infection with CVB3 [208]. In the mice model, treatment with olmesartan was associated with decreased expression of IFN-γ, iNOS, Fas ligand and pore-forming protein, as well as lowered the expression of CVB3 genomes [208]. ARNIs provide added anti-fibrotic effects by inhibiting noeprilysin leading to increasing natriuretic peptides levels such as BNP, which act via cGMP to inhibit fibroblast proliferation and stimulate ECM degradation [209,210].
However, antifibrotic properties of ACE inhibitors, ARBs and ARNI are moderate. One of potential stronger experimental treatments against myocardial fibrosis involve C-type natriuretic peptide (CNP) administration [211]. Cardiac fibroblasts treated with TGF-β with or without CNP, showed CNP activated cGMP–PKG signaling, inhibiting TGF-β–induced myofibroblast differentiation and ECM production [211]. Tranilast, a synthetic derivate of a tryptophan metabolite, reduces cardiomyocyte injury induced by ischemia-reperfusion via Nrf2/HO-1/NF-κB signaling [212]. Tranilast, in a mice model of CVB3-induced myocarditis, showed reduced myocardial fibrosis by decreasing the number of mast cells, inhibiting the expression of TGF-β1 and osteopontin a biomarker of outcomes [213].
Pirfenidone, a small oral anti-fibrotic agent that inhibits the activation of cardiac fibroblasts and the production of peptides, such as TGF-β, was investigated in preclinical studies, then two small RCTs showed a mild, yet significant reduction in extracellular volume in patients receiving pirfenidone compared with placebo on CMR (Table 2) [214,215,216]. Pirfenidone, an oral antifibrotic agent without hemodynamic effect, was investigated in phase 2 RCT in 94 patients with HF with preserved EF (>45%) and elevated levels of natriuretic peptides [215]. Authors found that among patients with myocardial fibrosis and HFpEF, administration of pirfenidone for 52 weeks reduced myocardial fibrosis on CMR [215]. However, reduction in myocardial extracellular volume was mild compared with placebo group (-1.21%, 95% CI, -2.12 to -0.31%) [215].
3.9. MicroRNAs in VMC
MicroRNAs (miRNAs, miRs) are short, non-coding regulatory ribonucleic acids (RNAs) that inhibit translation by binding to target messenger RNA (mRNA) sequences [216,217,218,219]. As a result, they modulate the secretion of proteins and cytokines, significantly impacting metabolic homeostasis [220]. The expression of miRs during VMC is critically important as miRs are implicated in the viral replication, immune responses and severity of disease pathogenesis, as well as they can be a therapeutic target to confer VMC [220]. Thus, they are key regulators of gene expression and play significant roles in host–virus interactions. Depending on the context, they can either promote or inhibit viral infections. Depending on the viral pathogen, a variety of miRs were described (Table 3) [221].
MicroRNAs identified in VMC in peripheral blood can reflect either degree of cardiomyocytes damage, or can be pathogen-specific depending on invasion pathways, and disease phase [221,222]. With regard to first group, Goldberg et al. showed that, in children, levels of cardiac associated miRNA such as miR-208a, miR-208b, miR-499, and miR-21 present upward or downward dynamics depending on the phase of enteroviral, adenoviral or parvoviral B19 myocarditis [223]. Similarly to myocardial infarction, miRs: -1, -208a/b, and -499 are highly sensitive markers of cardiac necrosis [224,225,226]. In particular, miR-208b and miR-499 are located in close vicinity to myosin chains, therefore cardiomyocyte death leads to the release of these microRNAs into blood stream [96,227]. miR-21 is produced by many various cell-lines, including endothelial, inflammatory, vascular smooth muscle cells and fibroblasts [96]. Therefore, their action depends on the sourced cells. miR-21 downregulation could protect myocardial cells against LPS-induced apoptosis and inflammation [228,229]. Whereas, Yang et al. reported that miR-21 deficiency promoted inflammatory cytokine production and worsened cardiac function in cardiac ischemia [230]. In late phase of VMC, miR-155, miR-135b, miR-190, miR-422a, miR-489, miR-590, miR-601, and miR-1290 were strongly induced in the hearts of patients with late viral persistence and progressive DCM [231].
In enteroviral CVB3 myocarditis, the most common cause of myocardial injury, many microRNAs promote CVB3 replication, including miR-19a/b, -22, -30a, -107, -126, -203, -590 [232]. microRNAs, involved in inflammatory process identified in VMC, include miR-1, miR-155, miR-141-3p, miR-142-3p, miR-203, the miR-221/222 cluster, and miR-21 [233].
miR-155 and miR-148a were shown to reduce cardiac injury during acute phase in humans by inhibiting the NF-κB pathway [234]. Results for miR-155 have been inconsistent in myocarditis, particularly regarding therapeutic interventions aimed at modulating its expression. It is important to notice that miR-155, that regulates the differentiation of macrophages, is highly upregulated and localized in heart-infiltrating macrophages and CD4+T lymphocytes during CVB3-induced myocarditis [235,236]. M1 macrophages, induced by LPS and IFN-γ, typically produce copious amounts of pro-inflammatory cytokines (TNF-α, IL-12) and generate ROS. As such, M1 macrophages are associated with inflammation and tissue destruction. In Corsten et al. study, cardiac microRNAs were profiled in both human myocarditis and in CVB3-injected mice, comparing myocarditis-susceptible with nonsusceptible mouse strains longitudinally [235]. MiR-155, -146b, and -21 were consistently and strongly upregulated during acute myocarditis in both humans and susceptible mice. Inhibition of miR-155 by a systemically delivered LNA-anti-miR attenuated cardiac infiltration by monocyte-macrophages, decreased T lymphocyte activation, and reduced myocardial damage during acute myocarditis in mice. Beyond the acute phase, miR-155 inhibition reduced mortality and improved cardiac function during 7 weeks of follow-up [235]. Despite this, there is currently limited evidence supporting the use of antagomirs targeting miR-155 outside of preclinical studies related to cardiac ischemia and atherosclerosis, where miR-155 is a key regulator of macrophage-driven inflammation.
Interestingly, some microRNAs appear to be specific to myocarditis and are associated with Th17 cell responses [236,237,238,239]. The Th17 cells are of particular importance as they secrete IL-17, therefore mediates myeloid cells recruitment, fibrosis, and favors DCM evolution [123]. Among Th17 cell-associated microRNAs, miR-1, miR-21, miR-146b, and miR-721 are candidates for antagomir-based therapy—with the potential to silence Th17 cells and thus suppress inflammatory pathways in VMC [236,237,238,239]. According to Liu et al., miR-146b is highly expressed in mice with CVB myocarditis [237]. Its inhibition reduced inflammatory lesions and suppressed Th17 differentiation. Inhibiting miR-146b may lead to a reduction in the severity of myocarditis [236]. A similar beneficial influence of miR-21 silencing on DCM evolution was demonstrated by Xu et al. [238]. Blanco-Domínguez et al. reported increased expression levels of miR-721 in a murine model of viral/autoimmune myocarditis compared with mice with induced myocardial infarction [239]. Notably, miR-721, synthesized by Th17 cells, was detectable uniquely in the plasma of mice with myocarditis but absent in infarcted mice [239].
Some, microRNAs were identified with anti-inflammatory potential like miR-425 and miR1/133a [240,241]. In CVB3-infected mice, delivery of miR-425-3p reduced levels of IL-6, IL-12, TNF-α, resulting in the inhibited myocardial inflammation and cardiomyocyte apoptosis [240]. IL-6 is fundamental for Th17 cells differentiation [123]. VMC rat models treated with miR-133a showed lower levels of inflammatory factors than non-treated groups [241]. Noteworthy, the highest levels of these cytokines were observed in the miR-133a-silenced rats [241].
However, CVB3-induced inflammatory pathways can diverse from other viral pathogens with regard to the expression levels of microRNAs [242,243,244,245,246,247,248,249,250,251]. For instance, in hMPV infection, 142 miRs were upregulated, and 32 were downregulated [244]. Notably, let-7f was significantly upregulated and exhibited antiviral effects: its inhibitors increased viral replication, whereas its mimics reduced it. The viral M2-2 protein regulated miRNAs such as miR-16 and miR-30a: miR-16 regulation depended on type I IFN signaling, whereas miR-30a was IFN independent, suggesting potential therapeutic targets [243]. Furthermore, hsa-miR-4634 enhances viral immune evasion by inhibiting type I IFN responses and interferon-stimulated genes, increasing viral replication in macrophages and epithelial cells [246]. In hMPV production of neutralizing antibodies depends on CD4+ T cells, therefore can lead to the development of new therapeutic strategies, through attenuation of Th17 cells and production of IL-17, thus preventing progression of VMC into DCM.
In patients with SARS-CoV-2 infection, high miR-335-3p expression level was potential biomarker to predict disease severity [247]. In Parvovirus B19 infection, five top microRNAs associated with infection progression identified miR-4799-5p, miR-5690, miR-335-3p, miR-193b-5p, and miR-6771-3p were highly expressed in the B19V transcripts [248]. In respiratory syncytial virus (RSV), miR-146a-5p and miR-29a were up-regulated, whereas let-7c, miR-345-5p, and miR-221 were downregulated by prolonged RSV infection [249,250]. miR-29a facilitated RSV replication [250].
Chen et al. investigated patients suffering from fulminant myocarditis, comparing them to healthy individuals. The increased levels of miR-29b and miR-125b in plasma were observed in the first group. Interestingly, this upregulation was positively correlated with the area of myocardial edema and was negatively correlated with the LVEF [251]. However, miR-29b demonstrated higher sensitivity and specificity for the fulminant myocarditis diagnosis than miR-125b [251].
Finally, a major group of microRNAs is involved in cardiac fibrosis [200]. This group is diverse, but special attention has recently focused on miR-132, a pro-fibrotic microRNA, and currently the only one under RCT investigation as a potential target to inhibit fibroblast proliferation [252,253]. A first-in-human trial confirmed the safety and tolerability of a novel antisense oligonucleotide directed against miR-132-3p [254]. The antagomir CDR132L, currently under investigation in phase 2 RCT, demonstrated cardioprotective effects by preventing post-MI remodeling in both murine and porcine models of acute ischemia [252,253,254,255]. A phase I clinical trial further supported its therapeutic potential, showing preserved cardiac function and reversal of structural remodeling in patients with HF (Table 1) [253]. Based on these promising findings, the antagomir against miR-132-3p has entered phase 2 trials and is considered one of the few microRNA-based therapies with high potential for clinical application [255]. However, recently published data did not show and benefit from anti-miR-132 on ventricular function in humans.
In conclusion, the identification of virus pathogen is a key determinant of immune cell and microRNA engagement. Therefore, only identification of the causal pathogen can lead to effective pathogen elimination through the anti-pathogen-specific treatment.

Table 3.
Expression of microRNAs associated with viral pathogen.
| Study | Pathogen | microRNA | Down vs Up-regulated |
Rationale for use of individual microRNA | Therapeutic approach |
|---|---|---|---|---|---|
| Goldberg et al. 2018 [223] | enteroviral, adenoviral or parvoviral B19 myocarditis | miR-208a, miR-208b, miR-499, and miR-21 | Up or Down | upward or downward dynamics depending on the phase of infection | No data |
| Gong et al. 2023 [228] |
miR-21 |
Down | miR-21 downregulation protects myocardial cells against LPS-induced apoptosis and inflammation through Rcan1 signaling | No data | |
| Li et al. 2022 [229] | miR-21 | Down | miR-21 downregulation protects myocardial cells against LPS-induced apoptosis and inflammation by targeting Bcl-2 and CDK6 | No data | |
| Yang et al. 2018 [230] | miR-21 | Down | miR-21 deficiency promoted inflammatory cytokine production and worsened cardiac function in cardiac ischemia through targeting KBTBD7 | No data | |
| Bao et al. 2014 [234] | Coxsackie B3 myocarditis | miR-155, miR-148 | Up | miR-155 and miR-148a were shown to reduce cardiac injury during acute phase in humans by inhibiting the NF-κB pathway | miR-155 reduced cardiac myoblast cytokines expression. Increased survival in miR-155 treated mice |
| Corsten MF et al. 2012 [235] | CVB3 myocarditis in humans and susceptible mice | miR-155, miR-146b, miR-21 | Up | Inhibition of miR-155 by a systemically delivered LNA-anti-miR attenuated cardiac infiltration by monocyte-macrophages, decreased T lymphocyte activation, and reduced myocardial damage during acute myocarditis in mice | LNA-anti-miR-155 may reduce inflammation activity in mice with CVB3 |
| Zhang Y, et al 2016 [236] |
CVB3 myocarditis | miR-155 | Up | miR-155 is upregulated in CVB3 myocarditis, and localized primarily in heart-infiltrating macrophages and CD4+ T lymphocytes, promoting macrophage polarization to pro inflammatory M1. Silencing miR-155 led to increased levels of alternatively-activated macrophages (anti-inflammatory M2) | miR-155 may be a potential therapeutic target for VMC |
| Liu et al. 2013 [237] |
CVB3 myocarditis | miR-146b | Up | miR-146b was highly expressed in mice with CVB3. Its inhibition reduced inflammatory lesions and suppressed Th17 cells differentiation. | inhibiting miR-146b may lead to a reduction in the severity of myocarditis |
| Blanco-Domínguez et al. [239] | A murine model of viral/autoimmune myocarditis in mice | miR-721 | Up | Increased expression levels of miR-721 in a murine model of viral/autoimmune myocarditis. miR-721, synthesized by Th17 cells, was detectable in the plasma of mice with myocarditis but absent in infarcted mice. A murine model of viral/autoimmune myocarditis in mice | antagomir-miR-721: potential to silence Th17 cells and thus suppress inflammatory pathways in VMC |
| Li, J. et al. 2021 [240] | CVB3-infected mice | miR-425-3p | Up | Reduction in IL-6, IL-12, TNF-α in VMC mice treated with miR-425-3p compared to non-treated VMC mice | MiR-425-3p inhibits myocardial inflammation and cardiomyocyte apoptosis in CVB3 myocarditis |
| Li W et al. 2020 [241] | CVB3-infected mice | miR-1/133a | Up | miR-1/133 mimics up-regulated the expression of miR-1 and miR-133, the potassium channel genes Kcnd2 and Kcnj2, as well as Bcl-2, and down-regulated the expression of the potassium channel suppressor gene Irx5, L-type calcium channel subunit gene a1c (Cacna1c), Bax, and caspase-9 in the myocardium of VMC mice. MiR-1/133 also up-regulated the protein levels of Kv4.2 and Kir2.1, and down-regulated the expression of CaV1.2 |
miR-1/133 mimics attenuates cardiomyocyte apoptosis and electrical remodeling in mice with VMC |
| Deng et al., 2014 [244] | hMPV infection |
142 miRs upregulated 32 miRs downregulated let-7f |
Up Down Up |
let-7f was significantly upregulated and exhibited antiviral effects: its inhibitors increased viral replication | Let-7f mimics reduced viral replication |
| Wu et al., 2020 [245] | hMPV infection | miR-16, miR-30a | Up | miR-16 regulation depended on type I IFN signaling, whereas miR-30a was IFN independent, suggesting potential therapeutic targets | No data |
| Martínez-Espinoza et al. 2023 [246] | hMPV infection | miR-4634 | Up | hsa-miR-4634 enhances viral immune evasion by inhibiting type I IFN responses and IFN-stimulated genes, increasing viral replication in macrophages and epithelial cells | No data |
| Srivastava et al. 2023 [247] | SARS-CoV-2 | miR-335-3p | Up | miR-335-3p expression level predicted COVID infection severity | No data |
| Salvado et al 2025 [248] | Parvovirus B19 |
miR-4799-5p, miR-5690, miR-335-3p, miR-193b-5p, and miR-6771-3p were highly expressed in the B19V transcripts | Up | promising biomarkers of infection progression | No data |
| Eilam-Frenkel et al 2018 [249] | Respiratory syncytial virus (RSV) |
miR-146a let-7c, miR-345, miR-221 |
Up Down |
miR-146a-5p were up-regulated, whereas let-7c, miR-345-5p, and miR-221 were downregulated by prolonged RSV infection | No data |
| Zhang Y et al. 2016 [250] | Respiratory syncytial virus (RSV) | miR-29a | Up | Respiratory syncytial virus non-structural protein 1 facilitates virus replication through miR-29a-mediated inhibition of IFN-alpha receptor. | No data |
| Chen et al. 2022 [251] | Fulminant myocarditis | miR-29b, miR-125b | Up | miR-29b demonstrated higher sensitivity and specificity for the fulminant myocarditis. Upregulation of miR-29b and miR-125b in plasma of patients with fulminant myocarditis positively correlated with the area of myocardial edema and was negatively correlated with the LVEF. | No data |
| Taubel et al., 2021 [254] | HF | miR-132 | Up | Randomized, phase 1b controlled trial evaluating the impact of CDR132L (antagomir-miR-132) on cardiac function over 3 months in a chronic HF model. Treatment with CDR132L significantly improved systolic and diastolic cardiac function, reduced cardiac fibrosis, and attenuated adverse remodeling | Demonstrated the therapeutic potential of targeting microRNA-132 for HF management |
| HF-REVERT, 2025 [255] | HF after myocardial infarction | miR-132 | Up | Randomized, phase 2, controlled study in patients with HFrEE following myocardial infarction showed safety of antagomir-132 treatment, without the effect on left ventricular remodeling | Demonstrated safety of the treatment with antagomir-132 |
CVB3, coxsackievirus B3; HF, heart failure; IFN, interferon; miR, microRNA; VMC, viral myocarditis;.
4. Conclusions and Future Perspectives
A progression from VMC to DCM has long been hypothesized [256]. It is sad that since late XX Century, despite huge progress in immunology, virology and diagnostic work-ups, still we are far from solutions to effectively treat this disease [257,258].
Since pharmacological treatment, including adrenergic blocking agents, carteolol, verapamil, sartans and ACE inhibitors, new pharmacological agents were developed resulting from deepen knowledge on an immune system–mediated mechanism [256]. The rather discouraging results obtained to date with immunosuppressive agents, anti-viral treatment, and the limited role of immunomodulating therapy in the treatment of VMC indicated the importance to target pathogen-specific replication and persistence mechanisms, as well as develop therapies to cease the exaggerated immune responses activity resulting in cardiac fibrosis [123,258].
New knowledge on inflammasomes, T-cell–mediated immune responses, role of cytokines like IL-1, IL-6, IL-12, IL-17, IL-18 and TGF-β in murine VMC has contributed greatly to the understanding of the mechanisms of disease processes. Pyroptotic cell death may provide new concept to explain the pathogenesis of DCM, in addition to persistent viral RNA and excessive fibrosis in the heart tissue, and an immune system–mediated mechanism.
The immune response to the pathogen might differ and be more pathogen-specific, despite similar symptoms of infection (like rhinorrhea, cough, fever, and respiratory distress, or clinical course of myocarditis that are often indistinguishable in patients). Therefore, the concept to target the pathway, not the pathogen, seems fully justified [123]. This individualized approach might lead to improved prognosis in patients [259]. VMC became important clinical issue in the era of COVID infection, as SARS-CoV-2 might either be a causal pathogen of myocarditis, as well as can make a patient susceptible to myocarditis of other etiology. The importance of upgrading management in myocarditis was addressed in just released 2025 ESC Scientific Guidelines for the management of myocarditis [260].
Our review paper has identified key cellular immune responses, including inflammasomes activation resulting in pyroptosis, Th cells differentiation, macrophages polarization, and microRNAs that can potentially be targets in myocarditis [123]. Of those, ARNI, that are already approved to therapy in HF, should be highly considered as first line treatment due to their anti-inflammatory and anti-fibrotic properties, regardless of VMC etiology. Dapansutrile, an oral NLRP3 inhibitor was already tested in phase 1B trial in patients with chronic HFrEF, and have shown good tolerability and clinical improvement as well as the increase in LVEF. If further clinical trials confirmed its efficacy, dapansutrile might become an important tool to reduce the activity of this most popular inflammasome pathway. According to present evidence, pirfenidone, a small oral agent that inhibits the activation of cardiac fibroblasts and the production of TGF-β demonstrated some potential to reduce fibrosis in humans on CMR. More evidence is needed for the treatment with anti-IL-1R7 antibody that might inhibit IL-18–induced NF-κB activation and downstream cytokines production. The inhibition of this pathway would limit Th17 cells differentiation into M1 macrophages. microRNAs-based therapies are still far from the use in clinical practice, although antagomir-132 is currently tested in RCTs for its potential property in reversing adverse left ventricular remodeling. Antagomir against miR-155, a strong driver of inflammation in VMC, might be considered for further research. Among Th17 cell-associated microRNAs, miR-146b and miR-721 are candidates for antagomir-based therapy—with the potential to silence Th17 cells and thus suppress inflammatory pathways in CVB3 myocarditis.
In conclusion, understanding the complex interactions between the pathogen virus and genetic and immune pathways can provide new insights into their use as therapeutic targets for developing antiviral therapies and vaccines. However, further studies are necessary to validate their roles experimentally in samples and humans.
Author Contributions
N.P., J.P., T.P., P.P., and A.K-Z. have equally contributed in writing this review and have approved the submitted version and agree to be personally accountable for the contributions and for ensuring that questions related to the accuracy or integrity of any part of the work. Conceptualization, N.P. and A.K.-Z.; Visualization, N.P. and J.P.; Editing, J.P., T.P., and P.P.; Obtaining fund, N.P.; Critical revision, T.P., P.P., Supervision, A.K.-Z. Final version revision, P.P. And A.K.-Z.
All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by grants from the St. John Paul II Hospital to Natalia Przytuła (grant number: FN/16/2025).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
The patient signed an informed consent to present a case report
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy.
Acknowledgments
none.
Conflicts of Interest
The authors declare that there is no conflict of interest regarding the publication of this article.
References
- Ammirati, E. , Moslehi J.J. Diagnosis and Treatment of Acute Myocarditis. JAMA. 2023;329:1098. [CrossRef]
- Golpour, A.; Patriki, D.; Hanson, P.J.; McManus, B.; Heidecker, B. Epidemiological Impact of Myocarditis. J. Clin. Med. 2021, 10, 603. [Google Scholar] [CrossRef]
- Brociek E, Tymińska A, Giordani AS, Caforio AL, Wojnicz R, Grabowski M, Ozierański K. Myocarditis: Etiology, Pathogenesis, and Their Implications in Clinical Practice. Biology. 2023;12:874. [CrossRef]
- Pollack, A. , Kontorovich A.R., Fuster V., Dec G.W. Viral myocarditis—diagnosis, treatment options, and current controversies. Nat. Rev. Cardiol. 2015;12:670. [CrossRef]
- Caforio AL, Pankuweit S, Arbustini E, et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2013;34(33):2636-2648d. [CrossRef]
- Bacterial cardiomyopathy: A review of clinical status and meta-analysis of diagnosis and clinical management. Trends in Research 2019, 2(3). [CrossRef]
- Tschöpe, C. , Ammirati, E., Bozkurt, B., Caforio, A. L. P., Cooper, L. T., Felix, S. B., Hare, J. M., Heidecker, B., Heymans, S., Hübner, N., Kelle, S., Klingel, K., Maatz, H., Parwani, A. S., Spillmann, F., Starling, R. C., Tsutsui, H., Seferovic, P., Van Linthout, S. Myocarditis and inflammatory cardiomyopathy: current evidence and future directions. Nature reviews. Cardiology, 2021, 18(3), 169–193. [CrossRef]
- Golpour, A.; Patriki, D.; Hanson, P.J.; McManus, B.; Heidecker, B. Epidemiological Impact of Myocarditis. J. Clin. Med. 2021, 10, 603. [Google Scholar] [CrossRef] [PubMed]
- Giordani, A.S.; Simone, T.; Baritussio, A.; Vicenzetto, C.; Scognamiglio, F.; Donato, F.; Licchelli, L.; Cacciavillani, L.; Fraccaro, C.; Tarantini, G.; et al. Hydrocarbon Exposure in Myocarditis: Rare Toxic Cause or Trigger? Insights from a Biopsy-Proven Fulminant Viral Case and a Systematic Literature Review. Int. J. Mol. Sci. 2025, 26, 4006. [Google Scholar] [CrossRef]
- Blauwet, L.A. , Cooper L.T. Antimicrobial agents for myocarditis: Target the pathway, not the pathogen. Heart. 2009;96:494–495. [CrossRef]
- Siripanthong, B. , Nazarian, S., Muser, D., Deo, R., Santangeli, P., Khanji, M. Y., Cooper, L. T., Jr, & Chahal, C. A. A. Recognizing COVID-19-related myocarditis: The possible pathophysiology and proposed guideline for diagnosis and management. Heart rhythm, 2020, 17(9), 1463–1471. [CrossRef]
- Chen, T. , Dai, Z., Mo, P., Li, X., Ma, Z., Song, S., Chen, X., Luo, M., Liang, K., Gao, S., Zhang, Y., Deng, L., Xiong, Y. Clinical Characteristics and Outcomes of Older Patients with Coronavirus Disease 2019 (COVID-19) in Wuhan, China: A Single-Centered, Retrospective Study. J Gerontol A Biol Sci Med Sci. 2020;75(9):1788-1795. [CrossRef]
- Ammirati, E; Lupi, L; Palazzini, M; et al. Prevalence, characteristics, and outcomes of COVID-19 associated acute myocarditis. Circulation 2022, 145, 1123–1139.
- Zuin, M. , Rigatelli, G., Bilato, C., Porcari, A., Merlo, M., Roncon, L., Sinagra, G. One-Year Risk of Myocarditis After COVID-19 Infection: A Systematic Review and Meta-analysis. Can J Cardiol. 2023; 39(6): 839-844. [CrossRef]
- Magyar K, Halmosi R, Toth K, Alexy T. Myocarditis after COVID-19 and influenza infections: insights from a large data set. Open Heart. 2024 Nov 14;11(2):e002973. [CrossRef]
- Knudsen B, Prasad V. COVID-19 vaccine induced myocarditis in young males: A systematic review. Eur J Clin Invest. 2023;53(4):e13947. [CrossRef]
- Yao Z, Liang M, Zhu S. Infectious factors in myocarditis: a comprehensive review of common and rare pathogens. Egypt Heart J. 2024;76(1):Published 2024. 24 May. [CrossRef]
- Dion CF, Ashurst JV. Streptococcus pneumoniae. In: StatPearls. Treasure Island (FL): StatPearls Publishing; , 2023. 8 August.
- Brown, A. O. , Mann, B., Gao, G., Hankins, J. S., Humann, J., Giardina, J., Faverio, P., Restrepo, M. I., Halade, G. V., Mortensen, E. M., et al. Streptococcus pneumoniae Translocates into the Myocardium and Forms Unique Microlesions That Disrupt Cardiac Function. PLoS Pathog. 2014;10(9):ePublished 2014 Sep 18. [CrossRef]
- Shenoy, A.T. , Orihuela, C. J. Anatomical site-specific contributions of pneumococcal virulence determinants. Pneumonia 2016, 8, 7. [Google Scholar] [CrossRef]
- Im, H. , Kruckow, K. L., D'Mello, A., Ganaie, F., Martinez, E., Luck, J. N., Cichos, K. H., Riegler, A. N., Song, X., Ghanem, E., Saad, J. S., Nahm, M. H., Tettelin, H., & Orihuela, C. J. Anatomical Site-Specific Carbohydrate Availability Impacts Streptococcus pneumoniae Virulence and Fitness during Colonization and Disease. Infect Immun. 2022;90(1):e0045121. [CrossRef]
- Piazza, I.; Ferrero, P.; Marra, A.; Cosentini, R. Early Diagnosis of Acute Myocarditis in the ED: Proposal of a New ECG-Based Protocol. Diagnostics 2022, 12, 481. [Google Scholar] [CrossRef]
- Drazner, M, Bozkurt, B. et al. 2024 ACC Expert Consensus Decision Pathway on Strategies and Criteria for the Diagnosis and Management of Myocarditis: A Report of the American College of Cardiology Solution Set Oversight Committee. JACC. 2025 Feb, 85 (4) 391–431. doi.org/10.1016/j.jacc.2024.10.
- Ramantauskaitė, G; Okeke, K.A.; Mizarienė, V. Myocarditis: Differences in Clinical Expression between Patients with ST-Segment Elevation in Electrocardiogram vs. Patients without ST-Segment Elevation. J Pers Med. 2024 Oct 13;14(10):1057. [CrossRef]
- Arbelo E, Protonotarios A, Gimeno JR, et al. 2023 ESC Guidelines for the management of cardiomyopathies. Eur Heart J. 2023;44(37):3503-3626. [CrossRef]
- Khanna, S. , Li, C., Amarasekera, A. T., Bhat, A., Chen, H. H. L., Gan, G. C. H., & Tan, T. C. Echocardiographic parameters of cardiac structure and function in the diagnosis of acute myocarditis in adult patients: A systematic review and meta-analysis. Echocardiography. 2024;41(2):e15760. [CrossRef]
- Supeł, K.; Wieczorkiewicz, P.; Przybylak, K.; Zielińska, M. 2D Strain Analysis in Myocarditis—Can We Be Any Closer to Diagnose the Acute Phase of the Disease? J. Clin. Med. 2023, 12, 2777. [Google Scholar] [CrossRef]
- Joudar I, Aichouni N, Nasri S, Kamaoui I, Skiker I. Diagnostic criteria for myocarditis on cardiac magnetic resonance imaging: an educational review. Ann Med Surg (Lond). 2023;85(8):3960-Published 2023 Jul 6. [CrossRef]
- Domínguez, F.; Uribarri, A.; Larrañaga-Moreira, J.M.; Ruiz-Guerrero, L.; Pastor-Pueyo, P.; Gayán-Ordás, J.; Fernández-González, B.; Esteban-Fernández, A.; Barreiro, M.; López-Fernández, S.; et al. Diagnosis and treatment of myocarditis and inflammatory cardiomyopathy. Consensus document of the SEC-Working Group on Myocarditis. Revista Española de Cardiología (English Edition) 2024, 77, 667–679. [Google Scholar] [CrossRef]
- Ammirati, E. , Buono, A., Moroni, F., Gigli, L., Power, J.R., Ciabatti, M., Garascia, A., Adler, E.D., Pieroni, M. State-of-the-Art of Endomyocardial Biopsy on Acute Myocarditis and Chronic Inflammatory Cardiomyopathy. Curr Cardiol Rep. 2022;24(5):597-609. [CrossRef]
- E, Kaur S, Jaber WA. Modern tools in cardiac imaging to assess myocardial inflammation and infection. Eur Heart J Open. 2023;3(2):oead019. [CrossRef]
- Gao Q, Yi W, Gao C, Qi T, Li L, Xie K, Zhao W, Chen W. Cardiac magnetic resonance feature tracking myocardial strain analysis in suspected acute myocarditis: diagnostic value and association with severity of myocardial injury. BMC Cardiovasc Disord. 2023;23(1):162. [CrossRef]
- Kociol, R.D. , Cooper L.T., Fang J.C., Moslehi J.J., Pang P.S., Sabe M.A., Shah R.V., Sims D.B., Thiene G., Vardeny O., et al. Recognition and Initial Management of Fulminant Myocarditis. Circulation. 2020;141:E69–E92. [CrossRef]
- Lasica, R.; Djukanovic, L.; Savic, L.; Krljanac, G.; Zdravkovic, M.; Ristic, M.; Lasica, A.; Asanin, M.; Ristic, A. Update on Myocarditis: From Etiology and Clinical Picture to Modern Diagnostics and Methods of Treatment. Diagnostics 2023, 13, 3073. [Google Scholar] [CrossRef]
- Al-Kindi, S.G. , Xie, R., Kirklin, J.K., Cowger, J., Oliveira, G.H., Krabatsch, T., Nakatani, T., Schueler, S., Leet, A., Golstein, D., et al. Outcomes of Durable Mechanical Circulatory Support in Myocarditis: Analysis of the International Society for Heart and Lung Transplantation Registry for Mechanically Assisted Circulatory Support Registry. ASAIO J. 2022;68(2):190-196. [CrossRef]
- Kim, M.J.; Jung, H.O.; Kim, H.; Bae, Y.; Lee, S.Y.; Jeo, D.S. 10-year survival outcome after clinically suspected acute myocarditis in adults: A nationwide study in dunishthe pre-COVID-19 era. PLoS ONE 18(1): e0281296. [CrossRef]
- Ammirati, E. , Cipriani, M., Moro, C., Raineri, C., Pini, D., Sormani, P., Mantovani, R., Varrenti, M., Pedrotti, P., Conca, C., et al. Clinical Presentation and Outcome in a Contemporary Cohort of Patients With Acute Myocarditis: Multicenter Lombardy Registry. Circulation. 2018;138(11):1088-1099. [CrossRef]
- Hashmani, S.; Manla, Y.; Al Matrooshi, N.; Bader, F. Red Flags in Acute Myocarditis, Cardiac Failure Review 2024;10:e02. doi.org/10.15420/cfr.2023.
- Nagai, T. , Katsuki, M., Amemiya, K., Takahashi, A., Oyama-Manabe, N., Ohta-Ogo, K., Imanaka-Yoshida, K., Ishibashi-Ueda, H., Anzai, T. Chronic Active Myocarditis and Inflammatory Cardiomyopathy - Challenges in Diagnosis and Treatment. Circ J. Published online , 2025. 31 May. [CrossRef]
- Florent Huang, for the FULLMOON Study Group. Fulminant myocarditis proven by early biopsy and outcomes. Eur. Heart J., 2023, 44, 5110–5124. [CrossRef]
- Al-Kindi SG, Outcomes of Durable Mechanical Circulatory Support in Myocarditis: Analysis of the International Society for Heart and Lung Transplantation Registry for Mechanically Assisted Circulatory Support Registry. ASAIO J. 2022 Feb 1;68(2):190-196. [CrossRef]
- Ghanizada M, Kristensen SL, Bundgaard H, Rossing K, Sigvardt F, Madelaire C, et al. Long-term prognosis following hospitalization for acute myocarditis—a matched nationwide cohort study. Scand Cardiovasc J. 2021; 55(5):264–9. doi.org/10.1080/14017431.2021. 1900.
- Martens CR, Accornero F. Viruses in the Heart: Direct and Indirect Routes to Myocarditis and Heart Failure. Viruses. 2021;13(10):Published 2021 Sep 24. [CrossRef]
- Falleti J, Orabona P, Municinò M, Castellaro G, Fusco G, Mansueto G. An Update on Myocarditis in Forensic Pathology. Diagnostics (Basel). 2024 Apr 3;14(7):760. [CrossRef]
- van den Hoogen, B. G., J. C. de Jong, J. Groen, T. Kuiken, R. de Groot, R. A. Fouchier, and A. D. Osterhaus. A newly discovered human pneumovirus isolated from young children with respiratory tract disease. Nat. Med. 2001, 7, 719-724.
- Uddin S, Thomas M. Human Metapneumovirus. [Updated 2023 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.
- Hennawi HA, Khan A, Shpilman A, Mazzoni JA. Acute myocarditis secondary to human metapneumovirus: a case series and mini-review. Glob Cardiol Sci Pract. 2024 Dec 31;2024(6):e202452. [CrossRef]
- Makhlouf A, Peipoch L, Duport P, Darrieux E, Reguerre Y, Ramful D, Alessandri JL, Levy Y. First Case of Acute Myocarditis Caused by Metapneumovirus in an Immunocompromised 14-year-old Girl. Indian J Crit Care Med. 2022 Jun;26(6):745-747. [CrossRef]
- Wang SH, Lee MH, Lee YJ, Liu YC. Metapneumovirus-Induced Myocarditis Complicated by Klebsiella pneumoniae Co-Infection: A Case Report. Am J Case Rep. 2024 Dec 27;25:e946119. [CrossRef]
- Dong, Y.; Xie, Z.; Xu, L. Receptors and host factors: key players in human metapneumovirus infection. Front. Cell. Infect. Microbiol. 2025, 15, 1557880. [Google Scholar] [CrossRef]
- Harburger, D. S. , and Calderwood, D. A. Integrin signalling at a glance. J. Cell Sci. 2009, 122, 159–163. [Google Scholar] [CrossRef]
- De Pasquale, V. , Quiccione, M. S., Tafuri, S., Avallone, L., and Pavone, L. M. Heparan sulfate proteoglycans in viral infection and treatment: A special focus on SARS-coV-Int. J. Mol. Sci. 2021, 22(12):6574. [CrossRef]
- Ballegeer, M.; Saelens, X. Cell-Mediated Responses to Human Metapneumovirus Infection. Viruses 2020, 12, 542; [Google Scholar] [CrossRef]
- Bao, X. , Liu, T. , Shan, Y., Li, K., Garofalo, R. P., and Casola, A. Human metapneumovirus glycoprotein G inhibits innate immune responses. PloS Pathog. 2008, 4, e1000077. [Google Scholar] [CrossRef]
- Wilson RL, Fuentes SM, Wang P, Taddeo EC, Klatt A, Henderson AJ, He B. Function of small hydrophobic proteins of paramyxovirus. J Virol. 2006;80(4):1700–9.
- Bao X, Kolli D, Liu T, Shan Y, Garofalo RP, Casola A. Human metapneumovirus small hydrophobic protein inhibits NF-kappaB transcriptional activity. J Virol. 2008 Aug;82(16):8224-9. [CrossRef]
- Lê VB, Dubois J, Couture C, Cavanagh MH, Uyar O, Pizzorno A, et al. Human metapneumovirus activates NOD-like receptor protein 3 inflammasome via its small hydrophobic protein which plays a detrimental role during infection in mice. PLoS Pathog 15(4): e1007689. [CrossRef]
- Ren R, Wu S, Cai J, Yang Y, Ren X, Feng Y, et al. The H7N9 influenza A virus infection results in lethal inflammation in the mammalian host via the NLRP3-caspase-1 inflammasome. Sci Rep. 2017; 7 (1):7625. [CrossRef]
- Shrivastava G, Leo´n-Jua´rez M, Garcı´a-Cordero J, Meza-Sa´nchez DE, Cedillo-Barro´n L. Inflammasomes and its importance in viral infections. Immunol Res. 2016; 64(5):1101–17. [CrossRef]
- Guo, L., Li, L., Liu, L., Zhang, T., and Sun, M. (2023). Neutralising antibodies against human metapneumovirus. Lancet Microbe 4, e732–e744. https://doi.org/10.1016/S2666-5247(23)00134-9. [CrossRef]
- Martı́nez-Espinoza, I. , Bungwon, A. D., and Guerrero-Plata, A. Human metapneumovirus-induced host microRNA expression impairs the interferon response in macrophages and epithelial cells. Viruses 2023, 15, v15112272. [Google Scholar] [CrossRef]
- Baños-Lara Mdel, R. , Ghosh, A. , and Guerrero-Plata, A. Critical role of MDA5 in the interferon response induced by human metapneumovirus infection in dendritic cells and in vivo. J. Virol. 2013, 87, 1242–1251. [Google Scholar] [CrossRef] [PubMed]
- McMichael, T. M. , Zhang, Y. , Kenney, A. D., Zhang, L., Zani, A., Lu, M., et al. IFITM3 restricts human metapneumovirus infection. J. Infect. Dis. 2018, 218, 1582–1591. [Google Scholar] [CrossRef]
- Lê, V. B. , Riteau, B. , Alessi, M. C., Couture, C., Jandrot-Perrus, M., Rhéaume, C., et al. Protease-activated receptor 1 inhibition protects mice against thrombindependent respiratory syncytial virus and human metapneumovirus infections. Br. J. Pharmacol. 2018, 175, 388–403. [Google Scholar] [CrossRef]
- Shirogane,Y. Takeda,M., Iwasaki, M., Ishiguro,N.,Takeuchi, H., Nakatsu,Y., et al. Efficient multiplication of human metapneumovirus in Vero cells expressing the transmembrane serine protease. TMPRSSJ. Virol. 2008, 82, 8942–8946. [CrossRef]
- Ogonczyk Makowska D, Hamelin ME, Boivin G. Engineering of live chimeric vaccines against human metapneumovirus. Pathogens. 2020;9(2):135. [CrossRef]
- August A, Shaw CA, Lee H, Knightly C, Kalidindia S, Chu L, Essink BJ, Seger W, Zaks T, Smolenov I, et al. Safety and immunogenicity of an mRNA-based human metapneumovirus and parainfluenza virus type 3 combined vaccine in healthy adults. Open Forum Infect Dis. 2022, 9(7), ofac206. [CrossRef]
- Ma S, Zhu F, Xu Y, Wen H, Rao M, Zhang P, Peng W, Cui Y, Yang H, Tan C, Chen J, Pan P. Development of a novel multi-epitope mRNA vaccine candidate to combat HMPV virus. Hum Vaccin Immunother. 2023 Dec 15;19(3):2293300. [CrossRef]
- Pereira JM, Xu S, Leong JM, Sousa S. The Yin and Yang of Pneumolysin During Pneumococcal Infection. Front Immunol. 2022;13:Published 2022 Apr 22. [CrossRef]
- Fillon S, Soulis K, Rajasekaran S, Benedict-Hamilton H, Radin JN, et al. Platelet-activating factor receptor and innate immunity: uptake of Gram-positive bacterial cell wall into host cells and cell-specific pathophysiology. J Immunol 2006, 177: 6182–6191. doi.org/10.4049/jimmunol.177.9. 6182.
- Zhang Y, Liang S, Zhang S, Zhang S, Yu Y, Yao H, Liu Y, Zhang W, Liu G. Development and evaluation of a multi-epitope subunit vaccine against group B Streptococcus infection. Emerg Microbes Infect. 2022;11(1):2371–82.
- Chen, R. , Zhang, H., Tang, B. et al. Macrophages in cardiovascular diseases: molecular mechanisms and therapeutic targets. Sig Transduct Target Ther 9, 130 (2024). [CrossRef]
- Hu M, Deng F, Song X, Zhao H, Yan F. The crosstalk between immune cells and tumor pyroptosis: advancing cancer immunotherapy strategies. J Exp Clin Cancer Res. 2024 Jul 10;43(1):190. [CrossRef]
- Xu J, Zhou Z, Zheng Y, Yang S, Huang K, Li H. Roles of inflammasomes in viral myocarditis. Front Cell Infect Microbiol. 2023 ;13:1149911. 15 May. [CrossRef]
- Turner MD, Nedjai B, Hurst T, Pennington DJ. Cytokines and chemokines: At the crossroads of cell signalling and inflammatory disease. Biochim Biophys Acta. 2014 Nov;1843(11):2563-2582. [CrossRef]
- Zhu, C. , Xu, S. , Jiang, R. et al. The gasdermin family: emerging therapeutic targets in diseases. Sig Transduct Target Ther 2024, 9, 87. [Google Scholar] [CrossRef]
- Van de Veerdonk FL, Netea MG, Dinarello CA, Joosten LA. Inflammasome activation and IL-1β and IL-18 processing during infection. Trends Immunol. 2011 Mar;32(3):110-6. [CrossRef]
- Al-Qahtani AA, Alhamlan FS, Al-Qahtani AA. Pro-Inflammatory and Anti-Inflammatory Interleukins in Infectious Diseases: A Comprehensive Review. Trop Med Infect Dis. 2024 Jan 4;9(1):13. [CrossRef]
- Han Xiao, Hao Li, Jing-Jing Wang, Jian-Shu Zhang, Jing Shen, Xiang-Bo An, Cong-Cong Zhang, Ji-Min Wu, Yao Song, Xin-Yu Wanget al. IL-18 cleavage triggers cardiac inflammation and fibrosis upon β-adrenergic insult, European Heart Journal, Volume 39, Issue 1, , Pages 60–69. 01 January. [CrossRef]
- Liu, Y.; Zhang, D.; Yin, D. Pathophysiological Effects of Various Interleukins on Primary Cell Types in Common Heart Disease. Int. J. Mol. Sci. 2023, 24, 6497. [Google Scholar] [CrossRef]
- Yasuda, K.; Nakanishi, K.; Tsutsui, H. Interleukin-18 in Health and Disease. Int. J. Mol. Sci. 2019, 20, 649. [Google Scholar] [CrossRef]
- Martinon F, Mayor A, Tschopp J. The inflammasomes: guardians of the body. Annu Rev Immunol. 2009;27:229-65. [CrossRef]
- Jorgensen I, Miao EA. Pyroptotic cell death defends against intracellular pathogens. Immunol Rev. 2015 May;265(1):130-42. [CrossRef]
- Latz E, Xiao TS, Stutz A. Activation and regulation of the inflammasomes. Nat Rev Immunol. 2013 Jun;13(6):397-411. [CrossRef]
- Ihim SA, Abubakar SD, Zian Z, Sasaki T, Saffarioun M, Maleknia S, Azizi G. Interleukin-18 cytokine in immunity, inflammation, and autoimmunity: Biological role in induction, regulation, and treatment. Front Immunol. 2022 Aug 11;13:919973. [CrossRef]
- Nakanishi K, Yoshimoto T, Tsutsui H, Okamura H. Interleukin-18 is a unique cytokine that stimulates both Th1 and Th2 responses depending on its cytokine milieu. Cytokine Growth Factor Rev. 2001 Mar;12(1):53-72. [CrossRef]
- Chattopadhyay, A.; Shyam, S. ; Das, S; Nandi, D. Global transcriptome analysis identifies nicotinamide metabolism to play key roles in IFN-γ and nitric oxide modulated responses. bioRxiv 2025.01.17.633516; [CrossRef]
- Camilli G, Blagojevic M, Naglik JR, Richardson JP. Programmed Cell Death: Central Player in Fungal Infections. Trends Cell Biol. 2021 Mar;31(3):179-196. [CrossRef]
- Yao, J. , Sterling, K., Wang, Z. et al. The role of inflammasomes in human diseases and their potential as therapeutic targets. Sig Transduct Target Ther 9, 10 (2024). [CrossRef]
- Li, D. , Wu, M. Pattern recognition receptors in health and diseases. Sig Transduct Target Ther 6, 291 (2021). [CrossRef]
- Olsen MB, Gregersen I, Sandanger Ø, Yang K, Sokolova M, Halvorsen BE, Gullestad L, Broch K, Aukrust P, Louwe MC. Targeting the Inflammasome in Cardiovascular Disease. JACC Basic Transl Sci. 2021 Nov 3;7(1):84-98. [CrossRef]
- Wen Y, Liu Y, Liu W, Liu W, Dong J, Liu Q, Hao H, Ren H. Research progress on the activation mechanism of NLRP3 inflammasome in septic cardiomyopathy. Immun Inflamm Dis. 2023 Oct;11(10):e1039. [CrossRef]
- Hu Y, Zhao W, Lv Y, Li H, Li J, Zhong M, Pu D, Jian F, Song J, Zhang Y. NLRP3-dependent pyroptosis exacerbates coxsackievirus A16 and coxsackievirus A10-induced inflammatory response and viral replication in SH-SY5Y cells. Virus Res. 2024 Jul;345:199386. [CrossRef]
- El Gendy A, Abo Ali FH, Baioumy SA, Taha SI, El-Bassiouny M, Abdel Latif OM. NOD-like receptor family pyrin domain containing 3 (rs10754558) gene polymorphism in chronic spontaneous urticaria: A pilot case-control study. Immunobiology. 2025 Jan;230(1):152868. [CrossRef]
- Remnitz, A.D.; Hadad, R.; Keane, R.W.; Dietrich, W.D.; de Rivero Vaccari, J.P. Comparison of Methods of Detecting IL-1β in the Blood of Alzheimer’s Disease Subjects. Int. J. Mol. Sci. 2025, 26, 831. [Google Scholar] [CrossRef]
- Badacz, R.; Przewłocki, T.; Legutko, J.; Żmudka, K.; Kabłak-Ziembicka, A. microRNAs Associated with Carotid Plaque Development and Vulnerability: The Clinician’s Perspective. Int. J. Mol. Sci. 2022, 23, 15645. [Google Scholar] [CrossRef] [PubMed]
- Pagliaro, P.; Penna, C. Inhibitors of NLRP3 Inflammasome in Ischemic Heart Disease: Focus on Functional and Redox Aspects. Antioxidants 2023, 12, 1396. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Ma, X.; Yang, X.; Xiao, S.; Ouyang, S.; Hu, Z.; Zhou, Z.; Jiang, Z. E. coli Nissle 1917 improves gut microbiota composition and serum metabolites to counteract atherosclerosis via the homocitrulline/Caspase 1/NLRP3/GSDMD axis. International Journal of Medical Microbiology 2025, 318, 151642. [Google Scholar] [CrossRef] [PubMed]
- Yang J, Zhao Y, Shao F. Non-canonical activation of inflammatory caspases by cytosolic LPS in innate immunity. Curr Opin Immunol. 2015 Feb;32:78-83. [CrossRef]
- Fernández-Duran, I. , Quintanilla, A., Tarrats, N. et al. Cytoplasmic innate immune sensing by the caspase-4 non-canonical inflammasome promotes cellular senescence. Cell Death Differ 29, 1267–1282 (2022). [CrossRef]
- Lupino E, Ramondetti C, Piccinini M. IκB kinase β is required for activation of NF-κB and AP-1 in CD3/CD28-stimulated primary CD4(+) T cells. J Immunol. 2012 Mar 15;188(6):2545-55. [CrossRef]
- Abdrabou, A.M. The Yin and Yang of IκB Kinases in Cancer. Kinases Phosphatases 2024, 2, 9–27. [Google Scholar] [CrossRef]
- Sánchez KE, Bhaskar K, Rosenberg GA. Apoptosis-associated speck-like protein containing a CARD-mediated release of matrix metalloproteinase 10 stimulates a change in microglia phenotype. Front Mol Neurosci. 2022 Oct 11;15:976108. [CrossRef]
- Bazzone LE, King M, MacKay CR, Kyawe PP, Meraner P, Lindstrom D, Rojas-Quintero J, Owen CA, Wang JP, Brass AL, Kurt-Jones EA, Finberg RW. A Disintegrin and Metalloproteinase 9 Domain (ADAM9) Is a Major Susceptibility Factor in the Early Stages of Encephalomyocarditis Virus Infection. mBio. 2019 Feb 5;10(1):e02734-18. [CrossRef]
- Spector, Lauren1,2; Subramanian, Naeha1,2,*. Revealing the dance of NLRP3: spatiotemporal patterns in inflammasome activation. Immunometabolism 7(1):p e00053, January 2025. [CrossRef]
- Choudhury SM, Ma X, Abdullah SW, Zheng H. Activation and Inhibition of the NLRP3 Inflammasome by RNA Viruses. J Inflamm Res. 2021 Mar 26;14:1145-1163. [CrossRef]
- Beyerstedt S, Casaro EB, Rangel ÉB. COVID-19: angiotensin-converting enzyme 2 (ACE2) expression and tissue susceptibility to SARS-CoV-2 infection. Eur J Clin Microbiol Infect Dis. 2021 May;40(5):905-919. [CrossRef]
- Sagris, M.; Theofilis, P.; Antonopoulos, A.S.; Tsioufis, C.; Oikonomou, E.; Antoniades, C.; Crea, F.; Kaski, J.C.; Tousoulis, D. Inflammatory Mechanisms in COVID-19 and Atherosclerosis: Current Pharmaceutical Perspectives. Int. J. Mol. Sci. 2021, 22, 6607. [Google Scholar] [CrossRef]
- Sun J, Li Y. Pyroptosis and respiratory diseases: A review of current knowledge. Front Immunol. 2022 Sep 30;13:920464. [CrossRef]
- Ingram T, Evbuomwan MO, Jyothidasan A. A case report of sepsis-induced dilated cardiomyopathy secondary to human metapneumovirus infection. Cureus. e: 2024;16(4), 2024.
- Wang SH, Lee MH, Lee YJ, Liu YC. Metapneumovirus-Induced Myocarditis Complicated by Klebsiella pneumoniae Co-Infection: A Case Report. Am J Case Rep. 2024 Dec 27;25:e946119.
- Hennawi HA, Khan A, Shpilman A, Mazzoni JA. Acute myocarditis secondary to human metapneumovirus: a case series and mini-review. Glob Cardiol Sci Pract. 2024 Dec 31;2024 (6):e202452. [CrossRef]
- Cox RG, Mainou BA, Johnson M, et al. Human metapneumovirus is capable of entering cells by fusion with endosomal membranes. PLoS Pathog. e: 2015;11(12), 2015.
- Soto JA, Galvez NMS, Benavente FM, et al. Human metapneumovirus: Mechanisms and molecular targets used by the virus to avoid the immune system. Front Immunol. 2018;9:2466.
- Van Den Bergh A, Bailly B, Guillon P, et al. Antiviral strategies against human metapneumovirus: Targeting the fusion protein. Antiviral Res. 1: 2022;207, 2022.
- Tsigkou, V.; Oikonomou, E.; Anastasiou, A.; Lampsas, S.; Zakynthinos, G.E.; Kalogeras, K.; Katsioupa, M.; Kapsali, M.; Kourampi, I.; Pesiridis, T.; Marinos, G.; Vavuranakis, M.-A.; Tousoulis, D.; Vavuranakis, M.; Siasos, G. Molecular Mechanisms and Therapeutic Implications of Endothelial Dysfunction in Patients with Heart Failure. Int J Mol Sci 2023, 24, 4321. [Google Scholar] [CrossRef]
- Wu, X. , Tian, Y. , Wang, H. et al. Dual Regulation of Nicotine on NLRP3 Inflammasome in Macrophages with the Involvement of Lysosomal Destabilization, ROS and α7nAChR. Inflammation 2025, 48, 61–74. [Google Scholar] [CrossRef]
- Wang, Z.; Li, X.; Moura, A.K.; Hu, J.Z.; Wang, Y.-T.; Zhang, Y. Lysosome Functions in Atherosclerosis: A Potential Therapeutic Target. Cells 2025, 14, 183. [Google Scholar] [CrossRef] [PubMed]
- Padmanaban, A.M.; Ganesan, K.; Ramkumar, K.M. A Co-Culture System for Studying Cellular Interactions in Vascular Disease. Bioengineering 2024, 11, 1090. [Google Scholar] [CrossRef] [PubMed]
- Casella M, Gasperetti A, Compagnucci P, Narducci ML, Pelargonio G, Catto V, Carbucicchio C, Bencardino G, Conte E, Schicchi N, Andreini D, Pontone G, Giovagnoni A, Rizzo S, Inzani F, Basso C, Natale A, Tondo C, Russo AD, Crea F. Different Phases of Disease in Lymphocytic Myocarditis: Clinical and Electrophysiological Characteristics. JACC Clin Electrophysiol. 2023 Mar;9(3):314-326. [CrossRef]
- Heymans S, et al. Inflammation as a therapeutic target in heart failure? Cardiovasc Res. 2019;115(7):1189-1201. [CrossRef]
- Ying, C. Viral Myocarditis. Yale J Biol Med. 2024 Dec 19;97(4):515-520. [CrossRef]
- Vicenzetto C, Giordani AS, Menghi C, Baritussio A, Scognamiglio F, Pontara E, Bison E, Peloso-Cattini MG, Marcolongo R, Caforio ALP. Cellular Immunology of Myocarditis: Lights and Shades-A Literature Review. Cells. 2024, 13(24), 2082. [CrossRef]
- Badrinath A, Bhatta S, Kloc A. Persistent viral infections and their role in heart disease. Front Microbiol. 2022;13:1030440].
- Tavazzi G, Pellegrini C, Maurelli M, Belliato M, Sciutti F, Bottazzi A, et al. Myocardial localization of coronavirus in COVID-19 cardiogenic shock. Eur J Heart Fail. 2020 May;22(5):911–5.
- Kühl U, Pauschinger M, Schwimmbeck PL, Seeberg B, Lober C, Noutsias M, et al. Interferon-β treatment eliminates cardiotropic viruses and improves left ventricular function in patients with myocardial persistence of viral genomes and left ventricular dysfunction. Circulation. 2: 2003 Jun;107(22), 2003.
- Schultheiss HP, Piper C, Sowade O, Waagstein F, Kapp JF, Wegscheider K, et al. Betaferon in chronic viral cardiomyopathy (BICC) trial: effects of interferon-β treatment in patients with chronic viral cardiomyopathy. Clin Res Cardiol. 2016 Sep;105(9):763–73.
- Hang, W. , Chen, C., Seubert, J.M. et al. Fulminant myocarditis: a comprehensive review from etiology to treatments and outcomes. Sig Transduct Target Ther 5, 287 (2020). [CrossRef]
- Hafezi-Moghadam, A.; et al. Acute cardiovascular protective effects of corticosteroids are mediated by non-transcriptional activation of endothelial nitric oxide synthase. Nat. Med. 8, 473–479 (2002).
- Mason, J. W.; et al. A clinical trial of immunosuppressive therapy for myocarditis. The Myocarditis Treatment Trial Investigators. N. Engl. J. Med. 1995. [Google Scholar]
- Chimenti C, Russo MA, Frustaci A. Immunosuppressive therapy in virus-negative inflammatory cardiomyopathy: 20-year follow-up of the TIMIC trial. Eur Heart J 2022; 43: 3463 – 3473.
- Wojnicz R, Nowalany-Kozielska E, Wojciechowska C, Glanowska G, Wilczewski P, Niklewski T, et al. Randomized, placebocontrolled study for immunosuppressive treatment of inflammatory dilated cardiomyopathy: Two-year follow-up results. Circulation 2001; 104: 39 – 45. 55.
- Frustaci A, Chimenti C, Calabrese F, Pieroni M, Thiene G, Maseri A. Immunosuppressive therapy for active lymphocytic myocarditis: Virological and immunologic profile of responders versus nonresponders. Circulation 2003; 107: 857 – 863. 56.
- Frustaci A, Russo MA, Chimenti C. Randomized study on the efficacy of immunosuppressive therapy in patients with virusnegative inflammatory cardiomyopathy: The TIMIC study. Eur Heart J 2009; 30: 1995 – 2002. 57.
- Merken J, Hazebroek M, Van Paassen P, Verdonschot J, Van Empel V, Knackstedt C, et al. Immunosuppressive therapy improves both short- and long-term prognosis in patients with virus-negative nonfulminant inflammatory cardiomyopathy. Circ Heart Fail 2018; 11: e004228.
- Caforio ALP, Giordani AS, Baritussio A, Marcolongo D, Vicenzetto C, Tarantini G, et al. Long-term efficacy and safety of tailored immunosuppressive therapy in immune-mediated biopsy-proven myocarditis: A propensity-weighted study. Eur J Heart Fail 2024; 26: 1175 – 1185.
- Hahn EA, Hartz VL, Moon TE, O'Connell JB, Herskowitz A, McManus BM, Mason JW. The Myocarditis Treatment Trial: design, methods and patients enrollment. Eur Heart J. 1995 Dec;16 Suppl O:162-7. [CrossRef]
- Gupta SC, Sundaram C, Reuter S, Aggarwal BB. Inhibiting NF-κB activation by small molecules as a therapeutic strategy. Biochim Biophys Acta. 2010 Oct-Dec;1799(10-12):775-87. [CrossRef]
- Yu, H. , Lin, L., Zhang, Z. et al. Targeting NF-κB pathway for the therapy of diseases: mechanism and clinical study. Sig Transduct Target Ther 2020, 5, 209. [Google Scholar] [CrossRef]
- Freitas RHCN, Fraga CAM. NF-κB-IKKβ Pathway as a Target for Drug Development: Realities, Challenges and Perspectives. Curr Drug Targets. 2018;19(16):1933-1942. [CrossRef]
- Georgiopoulos G, Makris N, Laina A, Theodorakakou F, Briasoulis A, Trougakos IP, Dimopoulos MA, Kastritis E, Stamatelopoulos K. Cardiovascular Toxicity of Proteasome Inhibitors: Underlying Mechanisms and Management Strategies: JACC: CardioOncology State-of-the-Art Review. JACC CardioOncol. 2023 Feb 21;5(1):1-21. [PubMed]
- Chin, CG. , Chen, YC. , Lin, FJ. et al. Targeting NLRP3 signaling reduces myocarditis-induced arrhythmogenesis and cardiac remodeling. J Biomed Sci 2024, 31, 42. [Google Scholar] [CrossRef]
- Golino M, Coe A, Aljabi A, Talasaz AH, Van Tassell B, Abbate A, Markley R. Effect of colchicine on 90-day outcomes in patients with acute myocarditis: a real-world analysis. Am Heart J Plus. 2024 Oct 24;47:100478. [CrossRef]
- Collini, V. , De Martino M. Efficacy and safety of colchicine for the treatment of myopericarditis. Heart. Jan 18 2024. [CrossRef]
- Kavgacı A, Incedere F, Terlemez S, Kula S. Successful treatment of two cases of acute myocarditis with colchicine. Cardiology in the Young. 2023;33(9):1741-1742. [CrossRef]
- Pappritz, K. , Lin J., El-Shafeey M., et al. Colchicine prevents disease progression in viral myocarditis via modulating the NLRP3 inflammasome in the cardiosplenic axis. ESC Heart Fail. Apr 2022;9(2):925–941. [CrossRef]
- Deftereos SG, Giannopoulos G, Vrachatis DA, et al. Effect of Colchicine vs Standard Care on Cardiac and Inflammatory Biomarkers and Clinical Outcomes in Patients Hospitalized With Coronavirus Disease 2019: The GRECCO-19 Randomized Clinical Trial. JAMA Netw Open. 2020;3(6):e2013136. [CrossRef]
- Wohlford, George F et al. “Phase 1B, Randomized, Double-Blinded, Dose Escalation, Single-Center, Repeat Dose Safety and Pharmacodynamics Study of the Oral NLRP3 Inhibitor Dapansutrile in Subjects With NYHA II-III Systolic Heart Failure.” Journal of cardiovascular pharmacology vol. 77,1 49-60. 24 Oct. 2020. [CrossRef]
- Wang, Shuangcui et al. “NLRP3 inflammasome as a novel therapeutic target for heart failure.” Anatolian journal of cardiology vol. 26,1 (2022): 15-22. [CrossRef]
- Ridker, Paul M et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. NEJM 2017, 377, 1119–1131. [CrossRef]
- Silvis MJM, Demkes EJ, Fiolet ATL, Dekker M, Bosch L, van Hout GPJ, Timmers L, de Kleijn DPV. Immunomodulation of the NLRP3 Inflammasome in Atherosclerosis, Coronary Artery Disease, and Acute Myocardial Infarction. J Cardiovasc Transl Res. 2021 Feb;14(1):23-34. [CrossRef]
- Morton AC, Rothman AM, Greenwood JP, Gunn J, Chase A, Clarke B, Hall AS, Fox K, Foley C, Banya W, Wang D, Flather MD, Crossman DC. The effect of interleukin-1 receptor antagonist therapy on markers of inflammation in non-ST elevation acute coronary syndromes: the MRC-ILA Heart Study. Eur Heart J. 2015 Feb 7;36(6):377-84. [CrossRef]
- Abbate A, Trankle CR, Buckley LF, Lipinski MJ, Appleton D, Kadariya D, Canada JM, Carbone S, Roberts CS, Abouzaki N, et al. Interleukin-1 Blockade Inhibits the Acute Inflammatory Response in Patients With ST-Segment-Elevation Myocardial Infarction. J Am Heart Assoc. 2020 Mar 3;9(5):e014941. [CrossRef]
- Cavalli G, Foppoli M, Cabrini L, Dinarello CA, Tresoldi M, Dagna L. Interleukin-1 Receptor Blockade Rescues Myocarditis-Associated End-Stage Heart Failure. Front Immunol. 2017 Feb 9;8:131.
- Ma, P.; et al. IL-1 Signaling Blockade in Human Lymphocytic Myocarditis. Circ Res 2025, doi.org/10.1161/CIRCRESAHA.125. 3265. [Google Scholar]
- Kerneis, M.; Cohen, F.; Combes, A.; Amoura, Z.; Pare, C.; Brugier, D.; Puymirat, E.; Abtan, J.; Lattuca, B.; Dillinger, J.-G.; et al. ACTION Study Group, Rationale and design of the ARAMIS trial: Anakinra versus placebo, a double blind randomized controlled trial for the treatment of acute myocarditis, Volume 1267, Issue 1, 7/2023, Pages 1-73, ISSN 1875-2136. [CrossRef]
- Lema, D.A.; et al. IL1RAP Blockade With a Monoclonal Antibody Reduces Cardiac Inflammation and Preserves Heart Function in Viral and Autoimmune Myocarditis. Circ Heart Fail. e: 2024;17, 2024. [Google Scholar] [CrossRef]
- Li S, Jiang L, Beckmann K, Højen JF, Pessara U, Powers NE, de Graaf DM, Azam T, Lindenberger J, Eisenmesser EZ, Fischer S, Dinarello CA. A novel anti-human IL-1R7 antibody reduces IL-18-mediated inflammatory signaling. J Biol Chem. 2021 Jan-Jun;296:100630. [CrossRef]
- Jiang L, Lunding LP, Webber WS, Beckmann K, Azam T, Højen JF, Amo-Aparicio J, Dinarello A, Nguyen TT, Pessara U, et al. An antibody to IL-1 receptor 7 protects mice from LPS-induced tissue and systemic inflammation. Front Immunol. 2024, 15, 1427100. [CrossRef]
- Uchida, Y. , Nariai, Y. , Obayashi, E., Tajima, Y., Koga, T., Kawakami, A., Urano, T., Kamino, H. Generation of antagonistic monoclonal antibodies against the neoepitope of active mouse interleukin (IL)-18 cleaved by inflammatory caspases. Archives of biochemistry and biophysics, 2022, 727, 109322. [Google Scholar] [CrossRef]
- Bhattacharjee P, Khan Z. Sacubitril/Valsartan in the Treatment of Heart Failure With Reduced Ejection Fraction Focusing on the Impact on the Quality of Life: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Cureus. 2023, 15(11), e48674. [CrossRef]
- McMurray JJ, Packer M, Desai AS, et al. Dual angiotensin receptor and neprilysin inhibition as an alternative to angiotensin-converting enzyme inhibition in patients with chronic systolic heart failure: rationale for and design of the Prospective comparison of ARNI with ACEI to Determine Impact on Global Mortality and morbidity in Heart Failure trial (PARADIGM-HF). Eur J Heart Fail 2013, 15, 1062–1073.
- Song Y, Zhao Z, Zhang J, Zhao F, Jin P. Effects of sacubitril/valsartan on life quality in chronic heart failure: A systematic review and meta-analysis of randomized controlled trials. Front Cardiovasc Med. 2022 Aug 3;9:922721. [CrossRef]
- Tsutsui H, Momomura SI, Saito Y, et al. Efficacy and safety of sacubitril/valsartan in Japanese patients with chronic heart failure and reduced ejection fraction- results from the PARALLEL-HF study. Circ J. 2021, 85, 584–594.
- McMurray JJ, Packer M, Desai AS, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med 2014, 371, 993–1004.
- Piepoli MF, Hussain RI, Comin-Colet J, Dosantos R, Ferber P, Jaarsma T, Edelmann F: OUTSTEP-HF: randomised controlled trial comparing short-term effects of sacubitril/valsartan versus enalapril on daily physical activity in patients with chronic heart failure with reduced ejection fraction. Eur J Heart Fail. 2021, 23, 127–135.
- Velazquez, E. J. , Morrow, D. A., DeVore, A. D., Duffy, C. I., Ambrosy, A. P., McCague, K., Rocha, R., Braunwald, E., PIONEER-HF Investigators. Angiotensin-Neprilysin Inhibition in Acute Decompensated Heart Failure. N Engl J Med. 2019;380(6):539-548. [CrossRef]
- Mann, D.L.; et al. Sacubitril/Valsartan in Advanced Heart Failure With Reduced Ejection Fraction Rationale and Design of the LIFE Trial. J Am Coll Cardiol HF. 2020, 8(10), 789–799. [Google Scholar] [CrossRef]
- Mann DL, Givertz MM, Vader JM, et al.Effect of treatment with sacubitril/valsartan in patients with advanced heart failure and reduced ejection fraction: a randomized clinical trial. JAMA Cardiol. 2022, 7, 17–25.
- Manzi L, Buongiorno F, Narciso V, Florimonte D, Forzano I, Castiello DS, Sperandeo L, Paolillo R, Verde N, Spinelli A, et al. Acute Heart Failure and Non-Ischemic Cardiomyopathies: A Comprehensive Review and Critical Appraisal. Diagnostics (Basel). 2025 Feb 23;15(5):540. [CrossRef]
- Trivedi RK, Polhemus DJ, Li Z, Yoo D, Koiwaya H, Scarborough A, et al. Combined angiotensin receptor-neprilysin inhibitors improve cardiac and vascular function via increased NO bioavailability in heart failure. J Am Heart Assoc. 2018, 7:8268. [CrossRef]
- Shi YJ, Yang CG, Qiao WB, Liu YC, Dong GJ. Sacubitril/valsartan attenuates myocardial inflammation, hypertrophy, and fibrosis in rats with heart failure with preserved ejection fraction. Eur J Pharmacol. 2023;961:176170. [CrossRef]
- Volpe, M. , Rubattu, S. , & Battistoni, A. ARNi: A Novel Approach to Counteract Cardiovascular Diseases. Int. J. Mol. Sci. 2019, 20, 2092; [Google Scholar] [CrossRef]
- Caobelli F, Cabrero JB, Galea N, et al. Cardiovascular magnetic resonance (CMR) and positron emission tomography (PET) imaging in the diagnosis and follow-up of patients with acute myocarditis and chronic inflammatory cardiomyopathy : A review paper with practical recommendations on behalf of the European Society of Cardiovascular Radiology (ESCR). Int J Cardiovasc Imaging. 2023;39(11):2221-2235. [CrossRef]
- She J, Lou B, Liu H, Zhou B, Jiang GT, Luo Y, Wu H, Wang C, Yuan Z. ARNI versus ACEI/ARB in Reducing Cardiovascular Outcomes after Myocardial Infarction. ESC Heart Fail. 2021 Dec;8(6):4607-4616. [CrossRef]
- Pfeffer MA, Claggett B, Lewis EF, Granger CB, Køber L, Maggioni AP, Mann DL, McMurray JJV, Rouleau JL, Solomon SD, et al.; PARADISE-MI Investigators and Committees. Angiotensin Receptor-Neprilysin Inhibition in Acute Myocardial Infarction. N Engl J Med. 2021 Nov 11;385(20):1845-1855. [CrossRef]
- Chatterjee, K.; Zhang, J.; Honbo, N.; Karliner, J.S. Doxorubicin cardiomyopathy. Cardiology 2010, 115(2), 155–162. [Google Scholar] [CrossRef] [PubMed]
- Hahn VS, Sharma K. Angiotensin Receptor-Neprilysin Inhibition for Doxorubicin-Mediated Cardiotoxicity: Time for a Paradigm Shift. JACC CardioOncol. 2020, 2(5), 788-790. [CrossRef]
- Wei S, Ma W, Li X, et al. Involvement of ROS/NLRP3 Inflammasome Signaling Pathway in Doxorubicin-Induced Cardiotoxicity. Cardiovasc Toxicol. 2020;20(5):507-519. [CrossRef]
- Polegato BF, Minicucci MF, Azevedo PS, et al. Acute doxorubicin-induced cardiotoxicity is associated with matrix metalloproteinase-2 alterations in rats. Cell Physiol Biochem. 2015;35(5):1924-1933. [CrossRef]
- Boutagy, N.E. , Feher A., Pfau D. Dual angiotensin receptor neprilysin inhibition with sacubitril/valsartan attenuates systolic dysfunction in experimental doxorubicin-induced cardiotoxicity. J Am Coll Cardiol CardioOnc. 2020;2:774–787. [CrossRef]
- Bell E, Desuki A, Karbach S, Göbel S. Successful treatment of doxorubicin-induced cardiomyopathy with low-dose sacubitril/valsartan: a case report. Eur Heart J Case Rep. 2022 Sep 23;6(10):ytac396. [PubMed]
- Hu, F. , Yan, S., Lin, L. et al. Sacubitril/valsartan attenuated myocardial inflammation, fibrosis, apoptosis and promoted autophagy in doxorubicin-induced cardiotoxicity mice via regulating the AMPKα–mTORC1 signaling pathway. Mol Cell Biochem 480, 1891–1908 (2025). [CrossRef]
- Dindas, F.; Turkey, U.; Gungor, H.; Ekici, M.; Akokay, P.; Erhan, F.; Dogdus, M.; Yilmaz, M.B. Angiotensin receptor-neprilysin inhibition by sacubitril/valsartan attenuates doxorubicin-induced cardiotoxicity in a pretreatment mice model by interfering with oxidative stress, inflammation, and Caspase 3 apoptotic pathway. Anatol. J. Cardiol. 2021, 25, 821–828. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Jang, G.; Hwang, J.; Wei, X.; Kim, H.; Son, J.; Rhee, S.-J.; Yun, K.-H.; Oh, S.-K.; Oh, C.-M.; et al. Combined Therapy of Low-Dose Angiotensin Receptor–Neprilysin Inhibitor and Sodium–Glucose Cotransporter-2 Inhibitor Prevents Doxorubicin-Induced Cardiac Dysfunction in Rodent Model with Minimal Adverse Effects. Pharmaceutics 2022, 14, 2629. [Google Scholar] [CrossRef]
- Quagliariello V, Di Mauro A, Ferrara G, Bruzzese F, Palma G, Luciano A, Canale ML, Bisceglia I, Iovine M, Cadeddu Dessalvi C, et al. Cardio-Renal and Systemic Effects of SGLT2i Dapagliflozin on Short-Term Anthracycline and HER-2-Blocking Agent Therapy-Induced Cardiotoxicity. Antioxidants (Basel). 2025, 20, 14(5), 612. [CrossRef]
- Lo SH, Liu YC, Dai ZK, Chen IC, Wu YH, Hsu JH. Case Report: Low Dose of Valsartan/Sacubitril Leads to Successful Reversal of Acute Heart Failure in Chemotherapy-Induced Cardiomyopathy. Front Pediatr. 2021 Feb 25;9:639551. [CrossRef]
- Hernandez AV, Pasupuleti V, Scarpelli N, Malespini J, Banach M, Bielecka-Dabrowa AM. Efficacy and safety of sacubitril/valsartan in heart failure compared to renin–angiotensin–aldosterone system inhibitors: a systematic review and meta-analysis of randomised controlled trials. Arch Med Sci. 2023;3:565-76. [CrossRef]
- Cemin R, Casablanca S, Foco L, Schoepf E, Erlicher A, Di Gaetano R, Ermacora D. Reverse Remodeling and Functional Improvement of Left Ventricle in Patients with Chronic Heart Failure Treated with Sacubitril/Valsartan: Comparison between Non-Ischemic and Ischemic Etiology. J Clin Med. 2023;12:621. [CrossRef]
- Zhang M, Zou Y, Li Y, Wang H, Sun W, Liu B. The history and mystery of sacubitril/ valsartan: From clinical trial to the real world. Front Cardiovasc Med. 2023;10:1102521. [CrossRef]
- Nesukay, E.G.; Kovalenko, V.M.; Cherniuk, S.V.; Kyrychenko, R.M.; Titov, I.Y.; Hiresh, I.I.; Dmytrychenko, O.V.; Slyvna, A.B. Choice of RAAS Blocker in the treatment of Heart Failure in Acute Myocarditis”. Ukrainian Journal of Cardiology, 2024, 31, 32–40. [Google Scholar] [CrossRef]
- Liang W, Xie BK, Ding PW, Wang M, Yuan J, Cheng X, Liao YH, Yu M. Sacubitril/Valsartan Alleviates Experimental Autoimmune Myocarditis by Inhibiting Th17 Cell Differentiation Independently of the NLRP3 Inflammasome Pathway. Front Pharmacol. 2021, 12, 727838. [CrossRef]
- Bellis, A.; Mauro, C.; Barbato, E.; Trimarco, B.; Morisco, C. The Rationale for Angiotensin Receptor Neprilysin Inhibitors in a Multi-Targeted Therapeutic Approach to COVID-Int. J. Mol. Sci. 2020, 21, 8612. [Google Scholar] [CrossRef]
- Zile MR, O’Meara E, Claggett B, Prescott MF, Solomon SD, Swedberg K, et al. Effects of sacubitril/valsartan on biomarkers of extracellular matrix regulation in patients with HFrEF. J Am Coll Cardiol. 2019, 73, 795–806. [CrossRef]
- Rao W, Li D, Zhang Q, Liu T, Gu Z, Huang L, Dai J, Wang J, Hou X. Complex regulation of cardiac fibrosis: insights from immune cells and signaling pathways. J Transl Med. 2025 Feb 28;23(1):242. [CrossRef]
- Thomas TP, Grisanti LA. The Dynamic Interplay Between Cardiac Inflammation and Fibrosis. Front Physiol. 2020 Sep 15;11:529075. [CrossRef]
- Dziewięcka, E.; Banyś, R.; Wiśniowska-Śmiałek, S.; Winiarczyk, M.; Urbańczyk-Zawadzka, M.; Krupiński, M.; Mielnik, M.; Lisiecka, M.; Gąsiorek, J.; Kyslyi, V.; et al. Prevalence and prognostic implications of the longitudinal changes of right ventricular systolic function on cardiac magnetic resonance in dilated cardiomyopathy. Kardiol Pol. 2025, 83(1), 62–69. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.; Bayes-Genis, A.; Bodegård, J.; Mullin, K.; Gustafsson, S.; Rosano, G.M.C.; Sundström, J. Suspected de novo heart failure in outpatient care: the REVOLUTION HF study. Eur Heart J. 2025, 46(16), 1493–1503. [Google Scholar] [CrossRef] [PubMed]
- Podolec, J.; Baran, J.; Siedlinski, M.; Urbanczyk, M.; Krupinski, M.; Bartus, K.; Niewiara, L.; Podolec, M.; Guzik, T.; Tomkiewicz-Pajak, L.; et al. Serum rantes, transforming growth factor-1 and interleukin-6 levels correlate with cardiac muscle fibrosis in patients with aortic valve stenosis. J. Physiol. Pharmacol. 2018, 69, 615–623. [Google Scholar]
- Kablak-Ziembicka, A.; Badacz, R.; Okarski, M.; Wawak, M.; Przewłocki, T.; Podolec, J. Cardiac microRNAs: diagnostic and therapeutic potential. Arch Med Sci 2023; 19 (5): 1360–1381.
- Heidenreich, P.A., Bozkurt, B., Aguilar, D., Allen, L.A., Byun, J.J., Colvin, M.M., Deswal, A., Drazner, M.H., Dunlay, S.M., Evers, L.R., et al, ACC/AHA Joint Committee Members. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation, 2022, 145(18), e895–e1032.
- Huang S, Chen B, Su Y, Alex L, Humeres C, Shinde AV, Conway SJ, Frangogiannis NG. Distinct roles of myofibroblast-specific Smad2 and Smad3 signaling in repair and remodeling of the infarcted heart. J Mol Cell Cardiol, 2019, 132, 84–97.
- Nevers T, Salvador AM, Velazquez F, Ngwenyama N, Carrillo-Salinas FJ, Aronovitz M, Blanton RM, Alcaide P, Th1 effector T cells selectively orchestrate cardiac fibrosis in nonischemic heart failure. J Exp Med, 2017, 214, 3311–3329. [CrossRef]
- Duangrat, Ratchanee et al. Dual Blockade of TGF-β Receptor and Endothelin Receptor Synergistically Inhibits Angiotensin II-Induced Myofibroblast Differentiation: Role of AT1R/Gαq-Mediated TGF-β1 and ET-1 Signaling. Int J Mol Scie 2023, 24, 8 6972. [CrossRef]
- Zhao, X. , Kwan, J. Y.Y., Yip, K. et al. Targeting metabolic dysregulation for fibrosis therapy. Nat Rev Drug Discov 2020, 19, 57–75. [Google Scholar] [CrossRef]
- Anguita-Sánchez M, Castillo-Domínguez JC, Mesa-Rubio D, Ruiz-Ortiz M, López-Granados A, Suárez de Lezo J. Se deben mantener los inhibidores de la enzima de conversión de la angiotensina a largo plazo en pacientes que normalizan la fracción de eyección tras un episodio de miocarditis aguda? [Should Angiotensin-converting enzyme inhibitors be continued over the long term in patients whose left ventricular ejection fraction normalizes after an episode of acute myocarditis?]. Rev Esp Cardiol. 2006, 59(11), 1199-1201.
- Kayyale, A.A.; Timms, P.; Xiao, H.B. ACE inhibitors reduce the risk of myocardial fibrosis post-cardiac injury: a systematic review. Br J Cardiol 2025;32:72–6. [CrossRef]
- Seko, Y. Effect of the angiotensin II receptor blocker olmesartan on the development of murine acute myocarditis caused by coxsackievirus BClin Sci (Lond). 2006, 110, 379-86. [CrossRef]
- Burke, R. M. , Lighthouse, J. K., Mickelsen, D. M., Small, E. M. Sacubitril/Valsartan Decreases Cardiac Fibrosis in Left Ventricle Pressure Overload by Restoring PKG Signaling in Cardiac Fibroblasts. Circulation. Heart failure, 2019, 12(4), e005565. [CrossRef]
- Liu C, Long Q, Yang H, Yang H, Tang Y, Liu B, Zhou Z, Yuan J. Sacubitril/Valsartan inhibits M1 type macrophages polarization in acute myocarditis by targeting C-type natriuretic peptide. Biomed Pharmacother. 2024 May;174:116535. [CrossRef]
- Ding N, Wei B, Fu X, Wang C, Wu Y. Natural Products that Target the NLRP3 Inflammasome to Treat Fibrosis. Front Pharmacol. 2020 Dec 17;11:591393. [CrossRef]
- Wang W, Shen Q. Tranilast reduces cardiomyocyte injury induced by ischemia-reperfusion via Nrf2/HO-1/NF-κB signaling. Exp Ther Med. 2023 Feb 22;25(4):160. [CrossRef]
- Huang LF, Wen C, Xie G, Chen CY. [Effect of tranilast on myocardial fibrosis in mice with viral myocarditis]. Zhongguo Dang Dai Er Ke Za Zhi. 2014 Nov;16(11):1154-61.
- AbdelMassih A, Agha H, El-Saiedi S, El-Sisi A, El Shershaby M, Gaber H, Ismail HA, El-Husseiny N, Amin AR, ElBoraie A, et al. The role of miRNAs in viral myocarditis, and its possible implication in induction of mRNA-based COVID-19 vaccines-induced myocarditis. Bull Natl Res Cent. 2022;46(1):267. [CrossRef]
- Lewis, G.A., Dodd, S., Clayton, D. et al. Pirfenidone in heart failure with preserved ejection fraction: a randomized phase 2 trial. Nat Med 2021, 27, 1477–1482 (). [CrossRef]
- Młynarska, E.; Badura, K.; Kurcinski, S.; Sinkowska, J.; Jakubowska, P.; Rysz, J.; Franczyk, B. The Role of MicroRNA in the Pathophysiology and Diagnosis of Viral Myocarditis. Int. J. Mol. Sci. 2024, 25, 10933. [Google Scholar] [CrossRef] [PubMed]
- Kabłak-Ziembicka A, Badacz R, Przewłocki T. Clinical Application of Serum microRNAs in Atherosclerotic Coronary Artery Disease. J Clin Med. 2022 Nov 20;11(22):6849. [CrossRef]
- Grodzka, O.; Procyk, G.; Gąsecka, A. The Role of MicroRNAs in Myocarditis—What Can We Learn from Clinical Trials? Int. J. Mol. Sci. 2022, 23, 16022. [Google Scholar] [CrossRef] [PubMed]
- Singh, D. Next-generation miRNA therapeutics: from computational design to translational engineering. Naunyn-Schmiedeberg's Arch Pharmacol 2025. [CrossRef]
- Bruscella, P.; Bottini, S.; Baudesson, C.; Pawlotsky, J.M.; Feray, C.; Trabucchi, M. Viruses and MiRNAs: More Friends than Foes. Front. Microbiol. 2017, 8, 824. [Google Scholar] [CrossRef] [PubMed]
- Pasławska, M.; Grodzka, A.; Peczyńska, J.; Sawicka, B.; Bossowski, A.T. Role of miRNA in Cardiovascular Diseases in Children—Systematic Review. Int. J. Mol. Sci. 2024, 25, 956. [Google Scholar] [CrossRef]
- Wang J and Han, B. Dysregulated CD4+ T Cells and microRNAs in Myocarditis. Front. Immunol. 2020, 11, 539. [Google Scholar] [CrossRef]
- Goldberg, L.; Tirosh-Wagner, T.; Vardi, A.; Abbas, H.; Pillar, N.; Shomron, N.; Nevo-Caspi, Y.; Paret, G. Circulating MicroRNAs: A Potential Biomarker for Cardiac Damage, Inflammatory Response, and Left Ventricular Function Recovery in Pediatric Viral Myocarditis. J. Cardiovasc. Transl. Res. 2018, 11, 319–328. [Google Scholar] [CrossRef]
- Abdou DM, Aziz EE, Kazem YS. Elgabrty S, Taha HS. The diagnostic value of circulating microRNA-499 versus high-sensitivity cardiac troponin T in early diagnosis of ST segment elevation myocardial infarction. Comp Clin Pathol 2021; 30: 565-70.
- Gacoń, J.; Badacz, R.; Stępień, E.; Karch, I.; Enguita, F.J.; Żmudka, K.; Przewłocki, T.; Kabłak-Ziembicka, A. Diagnostic and prognostic micro-RNAs in ischaemic stroke due to carotid artery stenosis and in acute coronary syndrome: A four-year prospective study. Kardiol. Pol. 2018, 76, 362–369. [Google Scholar] [CrossRef]
- Wang J, Xu L, Tian L, Sun Q. Circulating microRNA-208 family as early diagnostic biomarkers for acute myocardial infarction: a meta-analysis. Medicine 2021; 100: e27779.
- Badacz, R.; Przewlocki, T.; Gacoń, J.; Stępień, E.; Enguita, F.J.; Karch, I.; Żmudka, K.; Kabłak-Ziembicka, A. Circulating miRNA levels differ with respect to carotid plaque characteristics and symptom occurrence in patients with carotid artery stenosis and provide information on future cardiovascular events. Adv. Interv. Cardiol. 2018, 14, 75–84. [Google Scholar] [CrossRef]
- Gong, M.; Tao, L.; Li, X. MicroRNA-21-3p/Rcan1 Signaling Axis Affects Apoptosis of Cardiomyocytes of Sepsis Rats. Gen. Physiol. Biophys. 2023, 42, 217–227. [Google Scholar] [CrossRef]
- Li, Y.; Sun, G.; Wang, L. MiR-21 Participates in LPS-Induced Myocardial Injury by Targeting Bcl-2 and CDKInflamm. Res. 2022, 71, 205–214. [Google Scholar]
- Yang, L.; Wang, B.; Zhou, Q.; Wang, Y.; Liu, X.; Liu, Z.; Zhan, Z. MicroRNA-21 Prevents Excessive Inflammation and Cardiac Dysfunction after Myocardial Infarction through Targeting KBTBDCell Death Dis. 2018, 9, 769.
- Wang J, Han B. Front. Immunol., 2020 Sec. T Cell Biology Volume 2020, 1. 2020. [CrossRef]
- Kang Z, Zhang L, Yang Z. Role of non-coding RNAs in the pathogenesis of viral myocarditis. Virulence. 2025 Dec;16(1):2466480.
- Procyk, G.; Grodzka, O.; Procyk, M.; Gąsecka, A.; Głuszek, K.; Wrzosek, M. MicroRNAs in Myocarditis—Review of the preclinical In Vivo Trials. Biomedicines 2023, 11, 2723. [Google Scholar] [CrossRef]
- Bao JL, Lin L. MiR-155 and miR-148a reduce cardiac injury by inhibiting NF-κB pathway during acute viral myocarditis. Eur Rev Med Pharmacol Sci. 2014 Aug;18(16):2349-56.
- Corsten, M.F.; Papageorgiou, A.; Verhesen, W.; Carai, P.; Lindow, M.; Obad, S. ; Summer, G; et al. MicroRNA Profiling Identifies MicroRNA-155 as an Adverse Mediator of Cardiac Injury and Dysfunction During Acute Viral Myocarditis. Circulation Research 2012, 111. [CrossRef]
- Zhang, Y. , Zhang, M. , Li, X. et al. Silencing MicroRNA-155 Attenuates Cardiac Injury and Dysfunction in Viral Myocarditis via Promotion of M2 Phenotype Polarization of Macrophages. Sci Rep 2016, 6, 22613. [Google Scholar] [CrossRef]
- Liu, Y.L. ;Wu,W. F.; Xue, Y.; Gao, M.; Yan, Y.; Kong, Q.; Pang, Y.; Yang, F. MicroRNA-21 and -146b Are Involved in the Pathogenesis of Murine Viral Myocarditis by Regulating TH-17 Differentiation. Arch. Virol. 2013, 158, 1953–1963. [Google Scholar]
- Xu HF, Ding YJ, Zhang ZX, et al. MicroRNA-21 regulation of the progression of viral myocarditis to dilated cardiomyopathy. Mol Med Rep. 2014;10(1):161–168. [CrossRef]
- Blanco-Domínguez R, Sánchez-Díaz R, de la Fuente H, et al. A novel circulating MicroRNA for the detection of acute myocarditis. N Engl J Med. 2021;384 (21):2014–2027. [CrossRef]
- Li J, Tu J, Gao H, et al. MicroRNA-425-3p inhibits myocardial inflammation and cardiomyocyte apoptosis in mice with viral myocarditis through targeting tgf-βImmun Inflamm Dis. 2021;9(1):288–298. [CrossRef]
- Li W, Liu M, Zhao C, Chen C, Kong Q, Cai Z, Li D. MiR-1/133 attenuates cardiomyocyte apoptosis and electrical remodeling in mice with viral myocarditis. Cardiol J. 2020;27(3):285-294. [CrossRef]
- Baños-Lara, M.D.R.; Zabaleta, J.; Garai, J.; Baddoo, M.; Guerrero-Plata, A. Comparative analysis of miRNA profile in human dendritic cells infected with respiratory syncytial virus and human metapneumovirus. BMC Res Notes 2018, 11, 432. [Google Scholar] [CrossRef] [PubMed]
- Pasławska, M.; Grodzka, A.; Peczyńska, J.; Sawicka, B.; Bossowski, A.T. Role of miRNA in Cardiovascular Diseases in Children—Systematic Review. Int. J. Mol. Sci. 2024, 25, 956. [Google Scholar] [CrossRef] [PubMed]
- Deng, J. , Ptashkin, R. N., Wang, Q., Liu, G., Zhang, G., Lee, I., et al. Human metapneumovirus infection induces significant changes in small noncoding RNA expression in airway epithelial cells. Mol. Ther. Nucleic Acids 2014, 3, e163. [Google Scholar] [CrossRef]
- Wu, W.; Choi, E.-J.; Lee, I.; Lee, Y.S.; Bao, X. Non-Coding RNAs and Their Role in Respiratory Syncytial Virus (RSV) and Human Metapneumovirus (hMPV) Infections. Viruses 2020, 12, 345. [Google Scholar] [CrossRef]
- Martínez-Espinoza I, Bungwon AD, Guerrero-Plata A. Human Metapneumovirus-Induced Host microRNA Expression Impairs the Interferon Response in Macrophages and Epithelial Cells. Viruses. 2023, 15(11):2272. [CrossRef]
- Srivastava, S.; Garg, I.; Singh, Y.; Meena, R.; Ghosh, N.; Kumari, B.; Kumar, V.; Eslavath, M.R.; Singh, S.; Dogra, V.; et al. Evaluation of Altered MiRNA Expression Pattern to Predict COVID-19 Severity. Heliyon 2023, 9, e13388. [Google Scholar] [CrossRef]
- Salvado, V.d.A.; Alves, A.D.R.; Coelho, W.L.d.C.N.P.; Costa, M.A.; Guterres, A.; Amado, L.A. Screening out microRNAs and Their Molecular Pathways with a Potential Role in the Regulation of Parvovirus B19 Infection Through In Silico Analysis. Int. J. Mol. Sci. 2025, 26, 5038. [Google Scholar] [CrossRef]
- Eilam-Frenkel, B.; Naaman, H.; Brkic, G.; Veksler-Lublinsky, I.; Rall, G.; Shemer-Avni, Y.; Gopas, J. MicroRNA 146–5p, miR-let-7c-5p, miR-221 and miR-345–5p are differentially expressed in Respiratory Syncytial Virus (RSV) persistently infected HEp-2 cells. Virus Res. 2018, 251, 34–39. [Google Scholar] [CrossRef]
- Zhang, Y.; Yang, L.; Wang, H.; Zhang, G.; Sun, X. Respiratory syncytial virus non-structural protein 1 facilitates virus replication through miR-29a-mediated inhibition of interferon-alpha receptor. Biochem. Biophys. Res. Commun. 2016, 478, 1436–1441. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.H.; He, J.; Zhou, R.; Zheng, N. Expression and Significance of Circulating microRNA-29b in Adult Fulminant Myocarditis. Zhongguo Yi Xue Ke Xue Yuan Xue Bao 2022, 44, 102–109. [Google Scholar] [PubMed]
- Maruyama, K.; Imanaka-Yoshida, K. The Pathogenesis of Cardiac Fibrosis: A Review of Recent Progress. Int. J. Mol. Sci. 2022, 23, 2617. [Google Scholar] [CrossRef] [PubMed]
- Foinquinos, A. , Batkai, S. , Genschel, C. et al. Preclinical development of a miR-132 inhibitor for heart failure treatment. Nat Commun 2020, 11, 633. [Google Scholar] [CrossRef]
- Täubel J, Hauke W, Rump S, Viereck J, Batkai S, Poetzsch J, Rode L, Weigt H, Genschel C, Lorch U, Theek C, Levin AA, Bauersachs J, Solomon SD, Thum T. Novel antisense therapy targeting microRNA-132 in patients with heart failure: results of a first-in-human Phase 1b randomized, double-blind, placebo-controlled study. Eur Heart J. 2021 Jan 7;42(2):178-188. [CrossRef]
- Bauersachs J, Solomon SD, Anker SD, Antorrena-Miranda I, Batkai S, Viereck J, Rump S, Filippatos G, Granzer U, Ponikowski P, de Boer RA, Vardeny O, Hauke W, Thum T. Efficacy and safety of CDR132L in patients with reduced left ventricular ejection fraction after myocardial infarction: Rationale and design of the HF-REVERT trial. Eur J Heart Fail. 2024 Mar;26(3):674-682. [CrossRef]
- Kawai, C. From Myocarditis to Cardiomyopathy: Mechanisms of Inflammation and Cell Death Learning From the Past for the Future. Circulation. 1999;99:1091-1100.
- Martens, P.; Cooper, L.T.; Tang, W.H.W. Diagnostic Approach for Suspected Acute Myocarditis: Considerations for Standardization and Broadening Clinical Spectrum. J Am Heart Assoc. 2023, 12, e. [Google Scholar] [CrossRef]
- Shinge SAU, Zhang B, Zheng B, Qiang Y, Ali HM, Melchiade YTV, Zhang L, Gao M, Feng G, Zeng K, Yang Y. Unveiling the Future of Infective Endocarditis Diagnosis: The Transformative Role of Metagenomic Next-Generation Sequencing in Culture-Negative Cases. J Epidemiol Glob Health. 2025 Aug 22;15(1):108. [CrossRef]
- Podolec, J.; Przewłocki, T.; Kabłak-Ziembicka, A. Optimization of Cardiovascular Care: Beyond the Guidelines. J. Clin. Med. 2025, 14, 2406. [Google Scholar] [CrossRef]
- Schulz-Menger J, Collini V, Gröschel J, Adler Y, Brucato A, Christian V, Ferreira VM, Gandjbakhch E, Heidecker B, Kerneis M, Klein AL, Klingel K, Lazaros G, Lorusso R, Nesukay EG, Rahimi K, Ristić AD, Rucinski M, Sade LE, Schaubroeck H, Semb AG, Sinagra G, Thune JJ, Imazio M; ESC Scientific Document Group. 2025 ESC Guidelines for the management of myocarditis and pericarditis. Eur Heart J. 2025 Aug 29:ehaf192. [CrossRef]
Figure 2.
Pathways of innate response through inflammasomes formation and potential targets for medical therapy (adopted from: Xu et al. [74]). The key mechanisms by which inflammasomes oligomerize pro-caspase-1 into active caspase-1 and caspase-11 that facilitate GSDMD cleavage, along with IL-1β and IL-18 maturation. For detailed description of inflammatory pathways see the text. Abbreviations: AIM2, absent in melanoma 2; ARNI, angiotensin receptor-neprilysin inhibitor; ASC, apoptosis-associated speck-like protein containing a CARD; CARD8, caspase recruitment domain-containing protein 8; DAMPs, damage-associated molecular patterns; GSDMD, gasdermin D; IFN-γ, Interferon gamma; pro-IL-1b, pro-forms of interleukin 1b, IL-18; LPS, lipopolysaccharide; Nt-GSDMD, N-terminal gasdermin D; PAMPs, pathogen associated molecular patterns; dsDNA, double-stranded DNA; dsRNA, double-stranded RNA; NLRP, NOD-like receptor family pyrin domain; ROS, reactive oxygen species; TNF-α, Tumor Necrosis Factor alpha; VMC, viral myocarditis.
Figure 2.
Pathways of innate response through inflammasomes formation and potential targets for medical therapy (adopted from: Xu et al. [74]). The key mechanisms by which inflammasomes oligomerize pro-caspase-1 into active caspase-1 and caspase-11 that facilitate GSDMD cleavage, along with IL-1β and IL-18 maturation. For detailed description of inflammatory pathways see the text. Abbreviations: AIM2, absent in melanoma 2; ARNI, angiotensin receptor-neprilysin inhibitor; ASC, apoptosis-associated speck-like protein containing a CARD; CARD8, caspase recruitment domain-containing protein 8; DAMPs, damage-associated molecular patterns; GSDMD, gasdermin D; IFN-γ, Interferon gamma; pro-IL-1b, pro-forms of interleukin 1b, IL-18; LPS, lipopolysaccharide; Nt-GSDMD, N-terminal gasdermin D; PAMPs, pathogen associated molecular patterns; dsDNA, double-stranded DNA; dsRNA, double-stranded RNA; NLRP, NOD-like receptor family pyrin domain; ROS, reactive oxygen species; TNF-α, Tumor Necrosis Factor alpha; VMC, viral myocarditis.
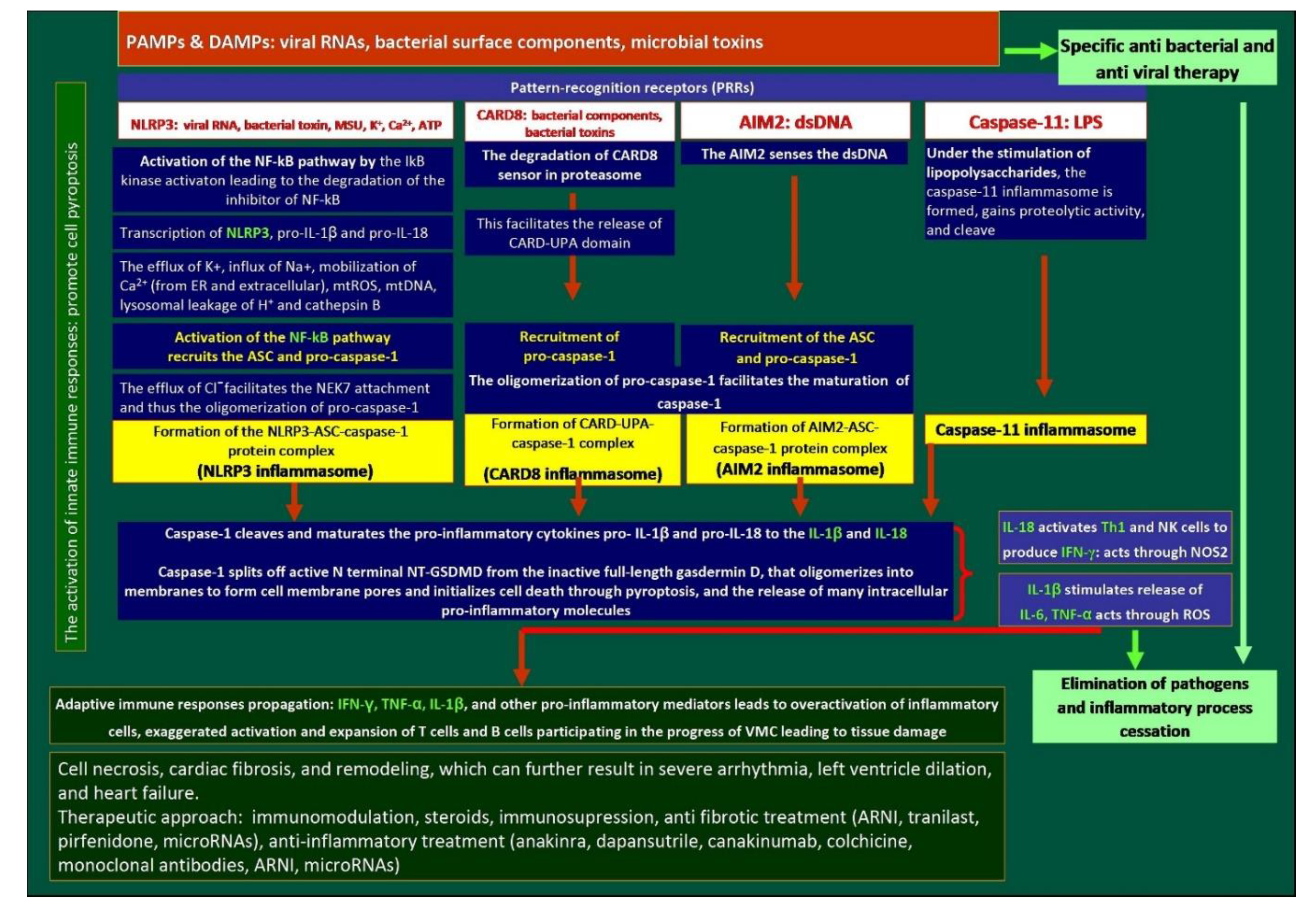
Table 1.
Pharmacological strategies against excessive activity of inflammasomes. Inhibitors of NLRP3 and Interleukins: a novel therapeutic approach.
Table 1.
Pharmacological strategies against excessive activity of inflammasomes. Inhibitors of NLRP3 and Interleukins: a novel therapeutic approach.
| Study | Medication / comparator | Type of the study | Study design | Main findings | Outcomes | Remarks / limitations |
|---|---|---|---|---|---|---|
| Inhibitors of the NLRP3 pathway | ||||||
| Chin, CG et al., 2024 [142] | MCC950 vs placebo | Experimental, animal model | Rats with myosin peptide–induced myocarditis (experimental group) were treated with an NLRP3 inhibitor (MCC950; 10 mg/kg, daily for 14 days) or left untreated | Rats treated with MCC950 improved their LV-EF and reduced the frequency of premature ventricular contraction | Changes in heart structure may be mitigated by inhibiting NLRP3 signaling. | A study on animal model |
| Golino M et al. 2024 [143] | Colchicine vs placebo in 1:1 proportion | Retrospective multi-center study in the US of patients hospitalized with acute myocarditis |
In total 1137 patients with acute myocarditis treated with colchicine within 14 days of diagnosis vs whose not obtaining colchicine | The incidence of the all-cause death was 3.3% vs. 6.6% (HR, 0.48, 95% CI, 0.33–0.71; p < 0.001), ventricular arrhythmias: 6.1% vs. 9.1% (HR, 0.65, 95% CI, 0.48–0.88; p < 0.01), and acute HF: 10.9% vs. 14.7% (HR 0.72, 95% CI, 0.57–0.91; p < 0.01) in patients treated with colchicine or not, respectively. | Patients with acute myocarditis treated with colchicine within 14 days of diagnosis have better outcomes at 90 days | Short-term outcomes |
| Collini et al., 2024 [144] | 45.1% of patients were treated with colchicine | Retrospective cohort study | A total of 175 patients with pericarditis and myocarditis, 88.6% with idiopathic/viral aetiology of myocarditis | In multivariable Cox regression analysis, women (HR 1.97, 95% CI 1.04 to 3.73; p=0.037) and corticosteroid use (HR 2.27, 95% CI 1.15 to 4.47; p=0.018) were risk factors of recurrence, and colchicine use prevented recurrences (HR 0.39, 95% CI 0.21 to 0.76; p=0.005). | After a median follow-up of 25.3 (IQR 8.3–45.6) months, colchicine use was associated with a lower incidence of recurrences (respectively, 19.2% vs 43.8%; p=0.001) and a longer event-free survival (p=0.005) |
Concomitant pericarditis and myocarditis |
| Pappritz et al 2022 [146] | Colchicine (5 µmol/kg p.o. daily) vs vehicle (PBS) | Preclinical, experimental | Murine model of CVB3-induced myocarditis; treatment started 24 h post-infection for 7 days | Colchicine significantly improved LV-EF, reduced viral load, and decreased inflammatory cell infiltration (ASC⁺, caspase-1⁺, IL-1β⁺ cells) in myocardium and spleen. | Reduced fibrosis markers, cardiac troponin I, and lower collagen deposition. | Preclinical only |
| GRECCO-19 trial, 2020 [147] | 52.4% of a total 105 patients were treated with colchicine | RCT phase 3 | to explore the potential of colchicine to attenuate COVID-19–related myocardial injury | Patients who received colchicine had significantly improved time to clinical deterioration. There were no significant differences in hs-Tn or CRP levels | a significant clinical benefit from colchicine in patients hospitalized with COVID-19 | Cardiac complications of COVID-19 infection |
| NCT05855746 [ https://clinicaltrials.gov/study/NCT05855746] | Colchicine vs placebo | RCT phase 3 | Three-hundred adults with acute myocarditis; primary endpoint at 6 months: composite of re-hospitalization, recurrent chest pain, arrhythmias, changes in LGE percentage by CMR | No results, as yet | Results expected post 2028 | Results not yet available |
| CMP-MYTHiC NCT06158698 [https://cdek.pharmacy.purdue.edu/trial/NCT06158698/] |
Colchicine vs placebo | RCT phase 3 | In total 80 adults with chronic inflammatory cardiomyopathy and impaired LV-EF or ventricular arrhythmias to receive colchicine or placebo for 6 months, with outcomes assessed by imaging, biomarkers, and arrhythmic burden. | No results, as yet | Results expected post 2026 | Chronic myocarditis, small population |
| Wohlford GF, et al, 2020 [148] | Dapansutrile (OLT1177) | RCT phase 1B |
Patients with HFrEF, dose escalation, single-center, repeat dose safety and pharmacodynamics study of dapansutrile in stable patients with HFrEF | Improvements in LV-EF [from 31.5% (27.5–39) to 36.5% (27.5–45), P = 0.039] and in exercise time [from 570 (399.5–627) to 616 (446.5–688) seconds, P = 0.039] were seen in the dapansutrile 2000 mg cohort. | Treatment with dapansutrile was well tolerated and safe over a 14-day treatment period. | A study for HFrEF, not specifically in myocarditis |
| Wang et al. 2022 [149] | INF200 (1,3,4-oxadiazol-2-one) | preclinical | Experiments on heart stress in rats | INF200 works by inhibiting the NLRP3 inflammasome, which in turn reduces inflammation and its associated detrimental effects on the heart | Reduced cardiac biomarkers and ischemia–reperfusion injury in diet-induced metabolic heart stress in rats | A study on animal models |
| IL-1 receptor antagonists | ||||||
| CANTOS TRIAL [150] | Canakinumab: IL-1 receptor antagonist given s.c. in dose 50mg, 150 mg, or 300 mg, vs placebo |
RCT phase 3 | A total of 10,061 patients with prior MI and high hsCRP (≥2 mg/L) given s.c. canakinumab at 50 mg, 150 mg, or 300 mg every 3 months |
The 150 mg dose of canakinumab significantly reduced the incidence of recurrent cardiovascular events compared to placebo. |
the canakinumab dose of 150 mg was associated with a reduced occurrence of the primary endpoint, and reduction in IL-6 and CRP levels | A study for myocardial infraction, not specifically in myocarditis |
| MRC-ILA [152] | Anakinra given s.c. IL-1ra vs placebo, 1:1 allocation | RCT phase 2 | 182 patients with NSTEMI; treatment for 14 days; primary endpoint: 7-day CRP | Significant CRP reduction (≈ 50% vs placebo); no difference in 30-day or 3-month MACE. | Lower inflammation; no clinical benefit; unexpected rise in CV events at one-year follow-up | A study for myocardial infraction, not specifically in myocarditis |
| VCU-ART3 [153] | Anakinra 100 mg once daily or twice daily vs placebo | RCT phase 2 | 99 STEMI patients within 12 h of symptom onset; 14-day treatment; primary endpoint: CRP level to day 14; follow-up to 12 months for echocardiographic remodeling and MACE | Not yet fully published, but early phase results showed significant CRP reduction during treatment | Primary: reduced inflammation (CRP AUC); secondary: pending data on LV remodeling and MACE over 12 months. | A study for myocardial infraction, not specifically in myocarditis |
| ARA-MIS Trial (Kerneis et al) [156] | Anakinra (IL-1 receptor antagonist: IL-1ra) 100 mg vs placebo | RCT phase 2 | 120 patients hospitalized with CMR-proven acute myocarditis, without severe hemodynamic instability or cardiogenic shock | No significant difference from myocarditis complications within 28 days. Significant reduction in systemic inflammatory markers such as CRP and IL-6. | Safety confirmed; well tolerated, but no efficacy signal in low-risk patients | Short course, low-risk population, low incidence of complicated myocarditis in both groups. |
| Lema et al. 2024 [157] | IL1RAP monoclonal antibody vs placebo, or vs anakinra/IL-1Ra | Preclinical, mice model | Induced CVB3-mediated myocarditis or experimental autoimmune myocarditis in mice, followed by the treatment with anti-mouse IL1RAP monoclonal antibody vs placebo, or IL-1Ra treatment | IL1RAP blockade with a monoclonal antibody, compared with placebo and IL1Ra, reduced inflammatory monocytes, T cells, neutrophils, and eosinophils in the heart in CVB3-mediated VMC, and preserved heart function on echocardiography in autoimmune myocarditis | The effect on the reduction in inflammation was higher in IL1RAP blockade compared with anti-IL-1Ra treatment alone, and placebo | Study in viral and autoimmune myocarditis |
| Interleukin-18 inhibitors | ||||||
| Li et al. 2021 [158] | Anti–IL-1R7 monoclonal antibody vs isotype control | Preclinical, in vitro human cells + in vivo mouse models | Assessed suppression of IL-18–mediated signaling in human PBMCs and whole blood; in mice, evaluated protection against LPS- or Candida-induced hyperinflammation | Blockade of IL-1R7 strongly inhibited IL-18–induced NF-κB activation and downstream cytokines (IFNγ, IL-6, TNFα) in mice, significantly reduced systemic inflammation and protected tissues (lung, liver) from LPS-induced injury | Demonstrated proof-of-concept that IL-1R7 blockade effectively attenuates IL-18–driven inflammation. | No direct myocarditis model used. |
| Jiang L et al. 2024 [159] | anti-human IL-1R7 antibody | Mice model | A novel humanized monoclonal antibody which specifically blocks the activity of human IL-18 and its inflammatory signaling in human cell and whole blood cultures was tested in hyperinflammation in acute lung injury model | In the current study, anti-IL-1R7 supressed LPS-induced inflammatory cell infiltration in lungs and inhibited subsequent IFN- γ production | An IL-1R7 antibody protects mice from LPS-induced tissue and systemic inflammation | Aimed to combat macrophage activation syndrome and COVID-19 infection |
Abbreviations: ASC, apoptosis-associated speck-like protein containing a CARD; CMR, cardiac magnetic resonance; CRP, C-Reactive Protein; CVB3, Coxsackievirus B3; hs-CRP, high-sensitivity C-Reactive Protein; HFrEF, heart failure with reduced ejection fraction; hs-Tn, high-sensitivity troponin T; IFN- γ, interferon gamma; IL, interleukin; IL-1R7, interleukin-1 receptor 7; LGE, late gadolinium enhancement; LPS, lipopolysaccharide; LV-EF, left ventricular ejection fraction; MACE, major cardiac adverse events; NSTEMI, Non ST Elevation Myocardial Infarction; NLRP3, NLR family pyrin domain containing 3; PBMCs, peripheral blood mononuclear cells; s.c., subcutaneous; STEMI, ST Elevation Myocardial Infarction; VCM, viral myocarditis
Table 2.
Approaches for ARNI use and anti-fibrotic treatment in heart failure and myocarditis.
| Study | Medication / comparator | Type of the study | Study design | Main findings | Outcomes | Remarks / limitations |
|---|---|---|---|---|---|---|
| ARNI | ||||||
| PARADIGM-HF [165] | Sac/Val vs. enalapril | RCT phase 3 | In total 8442 patients with chronic HF, NYHA class II–IV symptoms, an elevated plasma BNP or NT-proBNP level, and an LVEF of ≤35% | The primary outcome of CVD or hospitalization for HF was significantly lower in ARNI arm compared with enalapril arm (21.8% vs 26.5%; HR, 0.80; 95% CI, 0.73 to 0.87; P<0.001). | ARNI use reduced risk of CVD by 16%, hospitalization for HF by 21% and decreased the symptoms and physical limitations of HF. | Study terminated earlier due to high benefits from ARNI use. Only 0.7% of patients in NYHA functional class IV symptoms |
| OUT-STEP [166] | Sac/Val vs. enalapril | Observational study | A total of 621 ambulatory patients with stable symptomatic HFrEF randomised 1:1 to Sac/Val (n = 310) or enalapril (n = 311) | The study found no difference between the effect of Sac/Val vs. enalapril on 6-min walk test (6MWT) distance, non-sedentary daytime physical activity and HF symptoms | No significant benefit of Sac/Val compared with enalapril on either 6MWT or daytime physical activity after 12 weeks | Only 0.7% of patients in NYHA functional class IV symptoms |
| PIONEER-HF trial [167] | Sac/Val vs enalapril | RCT phase 3 | 736 hospitalized patients for acute decompansated HF with HFrEF after stabilization. | A greater reduction in the NTproBNP, hs-TnT, and lower rate of rehospitalization for HF in Sac/Val treatment compared to enalapril treatment was observed at 4 and 8 weeks | Fewer hospital admissions for HF in Sac/Val arm | patients hospitalized for acute HF after stabilization irrespective of HF background |
| LIFE trial [168] | Sac/Val vs valsartan | RCT phase 3 | In total 335 patients with HFrEF and recently advanced HF (NYHA class IV) | Compared to valsartan, treatment with Sac/Val have not improved the clinical composite of number of days alive, out of hospital, and free from HF events (p = 0.450). | The results showed that Sac/Val was not superior to valsartan and had a 29% discontinuation rate during the 24 weeks of the trial | not enrolled a predefined group of 400 patients, as it was terminated prematurely due to COVID-19 pandemic |
| She et al. 2021 [175] | ARNI, ACEI, and ARB groups | Propensity score of patients included in the Hospital of Xi’an Jiaotong University database | A total of 646 eligible patients with AMI assigned to ARNI, ACEI, and ARB group, respectively. |
Patients receiving ARNI had significantly lower rates of the composite cardiovascular outcome of CVD, MI, HF hospitalization and IS than ACEI [HR, 0.51, 95% CI, 0.27–0.95, P = 0.02], and ARB users [HR 0.47, 95% CI, 0.24–0.90, P = 0.02]. Patients receiving ARNI showed lower rates of CVD than ACEI [HR, 0.37, 95% CI, 0.18–0.79, P = 0.01] and ARB users [HR, 0.41, 95% CI, 0.18–0.95), P = 0.04]. |
Subgroup analysis indicated that patients with LVEF <40% benefit more from ARNI as compared with ACEI [HR 0.30, (95%CI, 0.11–0.86), P = 0.01] or ARB [HR 0.21, (95%CI, 0.04–1.1), P = 0.05]. Patients aged <60 years exhibited reduced composite endpoints [HR for ARNI vs. ARB: 0.11, (95%CI, 0.03–0.46), P = 0.002]. | not randomized, not specific for myocarditis |
| PARADISE-MI [176] | Sac/Val vs ramipril | RCT phase 3 | 5,661 post-MI patients with reduced LVEF (≤40%) ± pulmonary congestion, randomized within 0.5–7 days post-infarction, followed for ~23 months | No significant difference in the primary endpoint (CV death, first HF hospitalization, or outpatient HF: 11.9% vs 13.2%, p = 0.17) | Numerically fewer total HF events and coronary events with sac/val; higher incidence of hypotension (28% vs 22%). | A study for myocardial infraction, not specifically in myocarditis |
| Doxorubicine-induced DCM | ||||||
| Boutagy et al. 2020 [181] | Sac/Val vs. valsartan vs. placebo |
Preclinical experimental study | DOX-induced cardiotoxicity in rats. The study aimed to compare a cardioprotective effect of ARNI, valsartan, vs placebo | The treatment with ARNI caused lower LVEF reduction compared with valsartan alone, and placebo (p < 0.05). Cardiac fibrosis was similar in rats treated with valsartan alone, compared with Sac/Val, and significantly lower compared to DOX alone |
Preservation of LVEF in group with ARNI. Sac/Val occured more cardioprotective than Val in a rodent model of progressive DOX-induced cardiotoxicity. Val therapy alone only attenuated DOX-induced toxicity and fibrosis at the cellular level, whereas ARNI therapy preserved LVEF and inhibited myocardial MMP activation. |
A study on animal models |
| Dindas et al. 2021 [184] | Sac/Val pretreatment vs. doxorubicin | Preclinical experimental study | Four groups in mice (control; DOX only; Sac/Val only; Sac/Val pretreatment + DOX); Sac/Val given 80 mg/kg from day 1 before DOX (20 mg/kg at day 5) | Pretreatment with Sac/Val significantly attenuated DOX-induced ECG changes, oxidative stress, inflammation, compared with DOX alone (p<0.001). NT-proBNP levels were lower in the Sac/Val+DOX group compared with the DOX group along with less Caspase 3 apoptosis. | Sac/Val protects the cardiac electrophysiology, reduced biochemical and histologic markers of injury during DOX therapy. | A study on animal models |
| Kim et al. 2022 [185] | Low-dose ARNI + SGLT2i vs. monotherapy or placebo | Preclinical experimental study | Mouse model of doxorubicin-induced cardiotoxicity | Low-dose ARNI + SGLT2i improved survival, cardiac function, and reduced myocardial damage more than monotherapies or full-dose combo. | … | A study on animal models |
| Myocarditis | ||||||
| Nesukay et al. 2024 [191] | Sac/Val vs. enalapril | Prospective observational | Patients with acute myocarditis and HFrEF ≤40% treated with either enalapril (n=48) or sac/val (n=42), followed for 12 months with echocardiography and CMR | Sac/val group showed greater improvement in EF, myocardial strain, and functional capacity than enalapril group | Improved cardiac function and exercise tolerance with sac/val | Non-randomized design and more longer-term safety data is needed |
| Liang et al. 2022 [192] | Sac/Val vs valsartan alone | Preclinical, experimental animal study | Mice induced with experimental autoimmune myocarditis; treated with sac/val or valsartan during disease course. | Sac/val significantly reduced myocardial inflammation, decreased Th17 cell differentiation, and lowered IL-1β and IL-6 expression | Reduced inflammatory cell infiltration, improved histology. |
A study on animal models |
| Anti-fibrotic treatment | ||||||
| Liu et al. 2024 [204] |
Sac/Val vs placebo | In vitro | In total 30 patients diagnosed with AMC Autoimmune acute myocarditis | Sac/Val alleviated myocardial inflammation while augmenting circulating CNP levels rather than BNP and ANP, accompanied by reduction in intracardial M1 macrophage infiltration and expression of inflammatory cytokines IL-1β, TNF-α, and IL-6 | Sac/Val exerts a protective effect in myocarditis by increasing CNP concentration and inhibiting M1 macrophages polarization | C-type natriuretic peptide (CNP) |
| Wang et al., 2023 [212] | Tranilast | Experimental cell culture | A H/R model of H9c2 cardiomyocytes was established to simulate I/R-induced cardiomyocyte injury | Tranilast increased the viability of H9c2 cells, while decreased I/R injury-induced cardiomyocyte apoptosis through reduction the expression levels of the Nrf2/HO-1/NF-κB signalling pathway | Tranilast decreased apoptosis, oxidative stress and inflammatory response in H/R-induced H9c2 cells by activating Nrf2/HO-1/NF-κB signalling | |
| Huang et al., 2014 [213] | Tranilast | Experimental (mice) | Three subgroups of mice with CVB3-induced myocarditis, receiving tranilast (n =24), placebo (n=24), and 24 controls | The mRNA and protein expression of TGF-β1 and OPN was lower in tranilast group than the other groups | Tranilast reduced myocardial fibrosis by decreasing the number of mast cells, inhibiting the expression of TGF-β1 and OPN | |
| Levis et al., 2021 (PIROUETTE, NCT02932566) [215] |
Pirfenidone vs placebo | RCT phase 2 | A total of 94 patients with stable symptomatic HFpEF (≥45%) , elevated levels of natriuretic peptides, and CMR documented myocardial fibrosis (ECV ≥27%), randomised 1:1 to oral pirfenidone (n = 47) or placebo (n = 47) for 52 weeks | The primary outcome of the change in myocardial extracellular volume, from baseline to 52 weeks was higher in pirfenidone receiving group compared with placebo (between-group difference, −1.21%; 95%CI, −2.12 to −0.31; P = 0.009), | In comparison to placebo, pirfenidone significantly reduced myocardial extracellular volume | 26%) in the pirfenidone group and 30% in the placebo group experienced serious adverse event (nausea, rash, insomnia) |
Abbreviations: 6MWT, 6-Minute Walk Test; ACE, Angiotensin-Converting Enzyme; ARB, Angiotensin Receptor Blocker; ARNI, Angiotensin Receptor-Neprilysin Inhibitor; BNP, B-Type Natriuretic Peptide; CI, confidence interval; CMR – Cardiac Magnetic Resonance; CNP, C-Type Natriuretic Peptide; CVD, cardiovascular death; DOX, doxorubicin; ECG, Electrocardiogram; ECM, Extracellular Matrix; HF, Heart Failure; HO-1, heme oxygenase-1; HR, hazard ratio; HFrEF, Heart Failure with Reduced Ejection Fraction; H/R, hypoxia/reoxygenation; hs-TnT, high-sensitivity Troponin T; I/R, ischemia-reperfusion; LVEF – Left Ventricular Ejection Fraction; MI – Myocardial Infarction; MMP, matrix metalloproteinases; NF-κB, Nuclear Factor kappa B; NLRP3, NOD-Like Receptor P3; Nrf2, nuclear factor erythroid 2-related factor 2; NT-proBNP, N-Terminal Pro B-Type Natriuretic Peptide; NYHA, New York Heart Association; OPN, Osteopontin; RCT, Randomized Controlled Trial; ROS, Reactive Oxygen Species; Sac/Val, Sacubitril/valsartan, SGLT2i – Sodium-Glucose Co-Transporter 2 Inhibitors, TGF-18 – Transforming Growth Factor Beta-18,.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



