
Submitted:
20 September 2025
Posted:
22 September 2025
You are already at the latest version
Abstract
Trace elements are central for the accurate physiological functions of the body. However, these are possible only when they are maintained in a balanced state. Events like trauma, hereditary diseases, incorrect diets and polluted air or water may produce disruption, leading to their defficiency. This may trigger untold healthy implications. Hence, it is necessary to regain deficient trace elements through natural food or supplements, since the body cannot synthesize them. In this work, a thorough review of trace elements and updated knowledge on their potencial connections with common clinical disorders were provided. Consumption of trace elements as well as micronutrients were found to release intracellular substances. In addition, intake of the correct amount of these elements could provide oxidative protection while their defficiencies or excess amount may exacerbate oxidative damage in cells. Besides, imbalance of these elements is correlated with pathophysiology of clinical or degenerative diseases by disrupting the homeostatic status of the patients.
Keywords:
antioxidant
; dietary factors
; essential metals
; oxidative stress
; trace elements
1. Introduction
1.1. Trace Elements
The human body is gifted to adequately function in the presence of certain chemical elements and compounds. These chemical substances aid in the correct performance of many physiological activities such as metabolism, anti-oxidant action, reproduction, immune health and its boost, excretion, absorption, growth and homeostasis among others. In broad terms, they are divided into macromolecules, macroelements and trace elements. The difference between macroelements and trace elements depends on the amount of their daily requirements in the adult body [>100mg/day for macroelements and <100mg/day for trace elements]. The trace elements are further subdivided into potentially toxic, probably essential and essential elements.
Basically, the human body lacks the ability and machinery to endogenously fabricate these chemical substances when required. Hence, they have to be exogenously supplied, either through the ingestion of food rich in them or through mineral supplements. In the case of trace elements, their daily requirement for the body to carry out biological activities like development, adequate growth, anti-oxidant and physiological activities is minimal (<100mg/day) [1].
The essential trace elements, also called dietary elements, are extremely important for the body metabolic activities. Such activities include biochemical reactions and activities such as food digestion, hormone synthesis, immune system maintenance and cell división [2]. The balance of these chemical substances, especially the macroelements and trace elements, in the body is a key issue in the optimum function of the body systems and organs, since abnormal concentrations of them may lead to a disruption of the biochemical activities and reactions at celular level and hence, may underlie the onset of some diseases.
Macromolecules like carbohydrates [CH2O]n, protein [RCH[NH2]COOH], fat [CH3[CH2]nCOOH] and vitamins constitute the principal components of the staple food we consume. These macromolecules are formed by the four most common chemical elements designated as CHON [carbon, hydrogen, oxygen and nitrogen]. The covalent bond of these elements in addition with phosphorous and sulfur gives rise to the principal biomolecules in the living organisms. These biomolecules are biologically important in that they participate in the biochemical activities going on in the body.
The macroelements are non-metalic elements designated as macrominerals. These minerals are magnesium, chloride, phosphorus, sodium, sulfur, calcium, potassium, etc. They play crucial role in the day-to-day vital physiological functions of the body such as homeostasis; nerve impulses; muscle contraction and relaxation; tissue growth, maintenance and repair; biochemical reactions; transport and immune system health.
The trace elements are mainly minerals that function as enzymatic catalysts among others. Within this group we can highlight copper, iron, cobalt, iodine, manganese, zinc, etc. Their physiological functions include oxygen transport; metabolism, reproduction; tissue formation; regulation of blood sugar; erythropoiesis; maintenance of bone, nervous system health; immune boost; cell division and growth; tissue repair; catabolic activities of some macromolecules; and production and regulation of thyroid hormones. Recaping, both macroelements and trace elements found in the human body can be broadly grouped into two: trace elements and abundant elements [Table 1].
1.2. Trace elements and Metabolism
Over time, dietary transitions from naturally farmed products to chemically repleted industrialized food are associated with multiple health impacts in humans. Most of the junk foods we consume today are not properly enriched with trace elements and other health promoting nutrients and this could weaken the optimal physiological activities going on in the body. Consequently, the situation may have been responsable for the appearance of long-lasting diseases affecting the humans today today for its negative effect on cellular metabolism as well as the promotion of oxidative damage induction [3]. Some of the essential trace elements in animals with there biological relationship pinpointed in the literature are iron (Fe), an important component of hemoglobin; copper (Cu) associated with respiratory pigment; cobalt (Co), the central component of vitamin B12; manganese (Mn), a coenzyme that aids enzymes involved in carbohydrate and cholesterol metaboblism; and zinc associated with enzymes [4]. In humans elements such as Co [cobalt], Cu [copper], F [fluorine], I [iodine], Fe [iron], Mn [manganese], and Zn [zinc] [5], have been shown as the principal trace elements In cell metabolism, the role of selenium, zinc, iron and copper among others is very important. The metabolic process, just like other physiological activities, is laddened with enzymatic events and many trace elements are involved in these events. Notable in this function are the following trace elements depicted in Figure 1, Figure 2, Figure 3, Figure 4, Figure 5 and Figure 6.
In the metabolism of glucose, phosphate functional groups are responsible of providing the high energy in ATP to perform this metabolic activity. Also, magnesium plays active catalytic role in some of the reactions in this metabolism.
This cycle involves oxidation – reduction reactions that give rise to regeneration and condensation processes. The trace element, which participates in the mechanism that catalyzes some of these reactions is magnessium.
Electron transfer in biological oxidation–reduction reactions induces a change of GSH to GSSG. Selenium is found in the enzyme that catalyzes this reaction.
In lipid metabolism, Mn and Mg are involved in the mechanism that catalyzes some of the reactions. Here, many biological group-transfer reactions in form of ions participate in the reactions, for example, the transference of phosphoryl unit [−PO3−] from a donor molecule to the recipient molecule. In the above chemical process, hydrogen peroxide [H2O2] gives up a single ion to the hydroxyl ion, thereby neutralizing the ionic charge on the molecular reactant involved in the chemical process. For instance, in the movement of chemical species like O2, Fe and Cu are present in proteins and enzymes facilitating this process.
Zinc is a crucial part of the catalytic enzymes involved in water-assited bond cleavage for proteins, and for conversion of carbondioxide [CO2] to bicarbonate ion [HCO3−] and hydrogen ion [H+] as well as for all the chemical processes in the combination reaction, regeneration and replication of deoxyribonucleic acid [DNA] and ribonucleic acid [RNA].
1.3. Trace Elements and Environmental Factors
Blatant environmental pollution and contamination have shed many contaminants and pollutants into the air, land, aliments and water. Among these pollutants and conteminants are heavy metals, some of which belong to the toxic trace elements. Nowadays, some of the edible stuffs, for example grains [rice], seafood [fish] that the people consume, contain a large amount of metals like Pb [lead], Cd [cadmium] As [arsenic], Hb [mercury] and Co [cobalt] [6]. Most of these metals have deleterious health impacts on all living organisms, notably the humans.
Lead increases the risk of prevalent dyslipidemia. Studies have shown linear association of lead in antimony pulmonary hypertension, prevalent hypertension and dyslipidemia risk [7]. Likewise, lead was highly linked with elevated low-density lipoprotein cholesterol [LDL-C] concentration [8].
Prolonged arsenic exposure elevates the probability of bladder, skin, and lung cancers in humans. Arsenic detoxification route involves catalyzed transformation of inorganic arsenic by Arsenic [+3 oxidation state] methyltransferase [AS3MT] to mono- and dimethylated arsenic entities. One of these entities is arsenic trioxide [As2O3]. Drugs containing this trioxide have demonstrated their effectivenessin the management of cancer [9], and acute promyelocytic leukaemia [10]. ROS-induced stress is one of the routes for the propagation of arsenic toxicity. This allows arsenic penetration into the series of biochemical actions directed to identify, remove and replaced damaged/altered DNA as well as mitochondria integrity and efficient function. Consequently, this gives rise to disruption of these mechanisms, which may generate certain adverse health conditions. Regulation of p53 and the functions of mitogen/oncogenic both altered by ROS ascertain the result of the changes that affect cyclin-cdk complexes.
Likewise, chronic arsenic exposure affects growth transcription factor as c-myc, c-fos and c-Jun [11]. Arsenic trioxide in combination with pioglitazone, which is a catalyst of peroxisome proliferator-activated receptors gamma [PPARγ], induces important reaction retardation on the stability of NB4 even at a lower concentration [12]. This is possible because this combination reduces DNAs ability to duplicate in the synthesis phase of cell cycle.
Other elements with negative effects on the health include uranium [U]. This metal is responsible for the widespread of type2 diabetes with 30% [P=0.01] higher odds for this disease. Likewise, lead [Pb], thallium [Tl], arsenic [As], mercury [Hg], tungsten [W], cadmium [Cd], barium [Ba] and antimony [Sb] were linked with obesity and obesity comorbidities as well as high blood pressure and type-2 diabetes mellitus [T2DM] [13]. Yao et al.[14] demonstrated that, high exposure to As, Cd, Pb and Hg was associated to death-related high blood pressure, cardiovascular diseases and chronic lower respiratory disease. The normal concentrations of electrolyte minerals; Cl, Na, K, Ca, PO43- and Mg; constantly undergo changes and their imbalances usually have risky of these diseases. Sanders and cols, suggest that some exposure to combinations of these metals negatively affects renal parameters, thus, depicting the onset of of hypertension, kidney disease and renal dysfunction [15]. The chronic effects of these metals on brain tissues can cause additive/synergetic effects, because of their high binding constant with ligand-gated ion channel or N-mythyl-D-aspartate [NMDA] receptor [lead, Arsenic, methylmercury], Na+/K+-ATPase [Cadnium, methylmercury], biological Ca+2 [lead, Cadnium, methylmercury and Glu neurotransmitter [lead, methylmercury. This can bring about disequilibrium between the oxidizing agents [ROS] and the free radical scavengers [reducing elements]. In this process, ROS dominates the antioxidants factors such as GPx, GS, GSH, MT-III, Catalase, SOD, BDNF and Cyclic AMP response element-binding protein [CREB], and lastly gives rise to cognitive impairment [16]. Chronic lead, arsenic and MeHg exposures are linked with greater likelihood of developing neurodegenerative diseases. Proteomics, the study of proteomes, allows us to compare lead, arsenic and MeHg responses. Hence, it provides the key to evaluate potency differences of hippocampal cells. The response pattern of these heavy metals elucidate mRNA excision and ligation and on the role of ubiquitin pathway in neurodegeneration. Consequently, they could be employed as a valuable molecular biomarkers for certain disease states [17,18]. In fact, d-block and p-block elements are chiefly essential metals for the disease process [19].
1.4. Trace Elements with Pathological Consequences
Essential trace elements are required in only minute quantities. Therefore, their concentration or availability in the body might be easily disrupted. Both events can give rise to metabolic aberrations like glucose intolerance and lipid disorder. Likewise, the association of micronutrients with long-term liver diseases, such as liver fibrotic diseases, autoimmune liver diseases, chronic inflammatory liver disease and NAFLD [nonalcoholic fatty liver disease] have been reported [20].
Iron is the main component of hemoglobin [Hb]. Therefore, it is a very important trace element. Hemoglobin is one of the parameters in red blood counts [RBCs], whose principal function is oxygen transport due to its high affinity with this element. So, iron deficiency may tragger an array of physiological disorders that give way to disease onset.
It was reported that maternal iron deficiency [ID] and excess body weight during gestation [BMI≥25 kg/m2] negatively affect the brain development of the children; thus, highlighting the need for Fe supplementation in pregnant women [21]. Infants serum and urine analysis have revealed that loss of trace elements and deficient storage of body mineral were strongly marked in the earlier life stage [at 23.8th day] than later in life [22].
Ions of the trace elements play key roles in some neurological disorders, such as glaucoma. This disorder is a disparate group of chronic conditions involving progressive neuronal cell death. Generally, patients with glaucoma suffer the damage of retinal ganglion cells [RGCs] including their axons. This event brings about axon loss and alteration in the visual field. In one study, it was reported that glaucoma is associated with anomalies of orgasmic functions in charge of regulating ionic elements specifically micronutrients crucials for the functioning of the cells [23].
In the disorders of the thyroid, it was found that concentrations of elements, such as Ni, Cu and Cd, were significantly higher than normal while elements like Cr and Zn were lower [24]. Pathological samples of patients with multinodular goiter [MNG], thyroid adenoma [TA] and thyroid cancer [TC], showed decreased content of Mn, Co, Ni, Cu, Zn, Se and Pb is decreased [25].
Iron deficiency was associated with impaired antioxidant defense system and oxidative damage of erythrocytes in the neonatal age [26]. This was demonstrated in anemic neonatal calves. These animals depicted a more severe oxidative stress than their counterparts without anemia. The principal regulator of Fe is hepcidin, a peptide hormone. This hormone is extremely essential for the survival of the cells. The concentration of serum hepcidin increase in certain disease pathogenesis. This event may be owed to secondary anemia-linked HAMP gene transcription. HAMP gene transcription is a common event in redox imbalance and in the elevation of inflammatory cytokines. The role of genetic alterations in tissue iron overload has been demonstrated since these kind of alterations may lead to lower concentration of serum hepcidin [27]. This situation consequently causes iron-dependent lipid peroxidation-mediated cell death, which is a new form of apoptosis that features ROS accumulation [28]. Retinal iron accumulation can be seen in a broad spectrum of retinopathies. Today, Deferiprone, a 1,2-dimethyl-3,4-hydroxypyridinone, is the principal manage for hemochromatosis or elevated tisuue iron level [29]. In addition, dysfunction of blood-retinal barrier may cause retinal iron accumulation and hence, retinal degeneration [30].
Indeed, the impacts of iron deficiency on health are untold. It can weaken the patient and aggravate any underlying pathological conditions, although anemia is not present. Iron deficiency is usually accompanied by chronic inflammatory disease [31]. Joint treatment with free-radical scavenger and supplement of micronutrients positively declined burn stress-induced inflammation markers in patients [32]. Intravenous iron therapy showed significant beneficial effects in patients with iron deficiency [33]. However, excess consumption of Fe is a risk for the development of lower esophagus cancer [EC]. On the contrary, Se has been found to offer protection against EC [34]. In a studies conducted by Iqbal and Ali [35], it was reported the predisposing factor effect of excessive heme iron consumption on reast cancer.
Iron therapy have been found to fully restore iron-deficiency anemia [IDA] in infants, however, this restoration was partial in children with the same condition [36]. One of the events in blood transfusion is significant iron overload. Blood transfusion is normally accompany by hemolysis. This event leads to the increased free heme levels and this coupled with the inability of detoxification systems to sufficiently scavenge heme and iron creates iron overload [37]. Normally, this overload is deleterous to the arterial wall, because of its affectation of cells involved in atherosclerotic process [monocytes/macrophages, endothelial cells, vascular smooth muscle cells and platelets] [38].
In this reaction, the labile iron pool constitutes the source of iron for cells. The common event in this reaction is induction of redox imbalance, because of the liberation of excess of free irons. Living organisms circumvent surplus unbound irons by strict regulation of iron homeostasis [39]. Erythrocyte breakdown is the principal source deleterious intravascular cytotoxic molecules. These molecules intensify, modulate and maintain the inflammatory response [40], thus, giving rise to altered iron imbalance. This problem has been lately associated cancer and neurodegenerative diseases [41].
In sick people suffering from multiple sclerosis [MS], iron-binding molecules demomstrated to exacerbated redox imbalance [42]. Furthermore, plasma increase of hepcidin and ferritin is a frequent event in people with breast cancer; however, in those with non-cancerous breast conditions, this is not the case. The increase in hepcidin is usually tackled with the administration of estrogen hormone. This treatment not only reduces the expression of hepcidin in an important manner, but also increases HIF-1α [hypoxia-inducible factor 1 alpha] [43]. The changes in body iron equilibrium, so far outlined, could be provoked by negative changes in various iron-related proteins such as ferritin, transferrin, and hemoglobin. These proteins performs fundamental functions in breast cancer, where they function like STAT5, BMP6, CD7, TFRC and INHA. Indeed, there is a strong link between iron-related proteins and tumor tissue type [44].
Different severe diseases, such as leukemias, tumors, brain injuries, lymphomas, neurological diseases, burns and trauma, alter the dynamic equilibrium maintained by the body to keep trace element concentrations within specific physiological ranges. In children and adults, Mn and Se concentrations were 0.97±0.67 μg/L and 13.3±3.5 μg/L respectively [45]. The concentration of Cu and Zn was found to be elevated in children with epilepsy; however, Se concentration remained normal [46]. This suggests that high selenoprotein concentrations may be important for normal mental development. In Table 2, we show a summary of the report of recent studies on the role of micronutrients in health and disease in the organism.
Combined administration of trace elements and antioxidant is reported to reduce inflammatory biomarkers associated with burn trauma and decrease increased metabolic activity, as well as shorten the inpatient stay and improve bacterial elimination [79]. Deficient micronutrients can lead to adverse mental manifestations, such as depression, anxiety, schizophrenia and autism [80]
In idiopathic pulmonary fibrosis [IPF], an uncommon pulmonary disorder, sputum trace element concentrations of non-invassive type of this disease are clinically valuable biomarkers for the disease. The gender relationship of Cd, Cr and Cu in IPF patients phlegm were reported to be higher in males when compared with females. In severe stages of IPF, Zn level was found to be higher than normal [81].
Trace elements have a crucial function in the pathogenesis of psoriasis, a common inflammatory skin disease. A decreased Se and increased Cu serum concentrations were found in patients with this disease [82]. Findings from a study by Shahidi-Dadras et al. [83], in a group of patients, Fe, Cu, Transferrin [Trf] and Ceruloplasmin [Cp] serum levels were lower with respect to the controls. In addition, these authors reported that the action of Cp decreased Molybdenum [Mo] levels. Though required in small amounts, high dietary concentrations of trace elements can induce adverse health outcomes [84]. In patients with Alzheimer Disease, serum levels of Cu and Fe are usually high while Se level is very insignificant [85]. The cytochrome oxidase enzyme contains a substantial amount of copper. Also, enzymes such as ascorbic acid oxidase and ceruloplasmin contain a good amount of Cu. This element is extremely fundamental for for normal biologic development. It has a very high redox potential and this has been associated to human hepatopathies [86]. Despite its great beneficial effects, Cu could be deleterious to proteins and DNA. In free state, it can stimulate the release of a large amount of free radicals, which can damage proteins and DNA [87,88]. Synergistic effects have been reported with Cu and As, which hike up disturbance in the homeostasis of micronutrients and oxidative stress in the blood [89]. Moreover, combined decrease in the levels of Cu and Zn is related with an elevated likelihood of preeclampsia [90]. Indeed, Cu and Zn enhance the immune system and are beneficial in the treatment of tuberculosis [91]. Specific minerals play an active role in keeping the structural integrity of skin and mucus membranes. In addition, they aide in immune cell recruitment and activation, complement cascade activation and in inflammatory cascade [92].
1.5. Trace Element Metabolism and Redox Imbalance
Reactive oxygen species (ROS) imbalance is produced due to a disequilibrium in the internal oxidation system and antioxidant system. This situation has been linked to many vascular diseases and their prognosis; hence, it can be used as a biomarker for these diseases [93]. Age-related diseases, such as aterosclerosis, are associated with metal exposure and decreased PON1 activity. In these situations, ROS imbalance and inflammation mechanisms are fundamental. The protective effect of Zn has been reported in plaque buildup in arteries outside of the heart and shows that Zn-PON1interactions are potent anti-inflammatory and antioxidant agent [94].
The joint use of bioactive agents with Se and plant compounds such as bioflavonoids or polyphenols has attracted a great interest for their potential in decreasing the activities of antioxidant enzymes, for example, GSH peroxidase, superoxide dismutase [SOD] and hydroperoxidase in mice and rats brain. In addition, selenium-rich nanoparticles in small size [5-15 nm] have been shown to deplete Aβ formation by decreasing the production of ROS [95].
Zinc [Zn2+] is an important constituent of many enzymes [>2700 in number] among which hydrolytic enzymes, group transfer enzymes (transferases), synthases, lysases isomerization catalysts and oxy-reductases can be mentioned. In addition, zinc(II) ion functions as intracellular signaling molecule as well as provides stability to polypeptides (proteins) during intermolecular interactions. It acts as a structural element in nucleic acids or other gene-regulating proteins [96]. Likewise, it functions as a promoter of cell survival in various conditions. On the other hand, the release of zinc during synaptic transmission enhances neuronal resistance to programmed cell death [97]. In the context of depressive disorders and neuroplasticity, the interaction of Zn and monoaminergic system displays mood-stabilizing effects [98]. However, elevated levels of zinc is associated with disruption of mitochondrial quality control and induction of oxidative stress caused by Ca-induced mitochondrial depolarization as a result of ephemeral and persistent openings of the mitochondrial permeability transition pore [mPTP] [99]. Therefore, disruption of tissue Zn levels could function as a part of the defense mechanism of the host against infectious agents in times of sepsis through different mechanisms as well as serving as a diagnostic marker [100].
Ariaee et al. [101], demonstrated lower serum zinc and selenium levels in type 2 asthmatic people than was found in the controls, and a little higher copper level in the same group of patients. Moreover, blood zinc was found to increase in people suffering from smoke-inhalation-induced acute lung injury (SI-ALI). Xie et al. [102], found an association between elevated serum Zn level during perchloroethane/zinc chloride [HC/ZnCl] smoke inhalation with the severity of lung and liver injuries. In patients suffering from brucellosis, serum zinc showed a decreasing tendency [103]. D. dendriticum parasitosis caused a decrease of serum levels of zinc and iron in a group infected by this parasite. This result suggests that erythrocyte destruction in naturally parasite infected sheep may be associated with oxidative stress [104]. In a controlled study performed in diabetic patients, zinc and coper levels increased when compared with the healthy controls [105]. This confirms the association of redox imbalance with diabetes is a metabolic disorder. However, recent studies, involving patients with non-insulin-dependent diabetes mellitus (NIDDM), showed a decrease in the levels of in new studies in diabetes type 2, nitric oxide [NO] and magnesium [Mg]. This suggests the influence of blood glucose levels on the concentrations of micronutrients as was put forward by Mishra S and Mishra BB [106], on finding inverse relationship between Zn and Mg with fasting blood glucose (FBG). Certain micronutrients have been linked with the likelihood of the loss of immunological tolerance to self-antigens, particularly non-insulin-dependent diabetes mellitus (NIDDM) and disseminated sclerosis, which participate in antibody-mediated immunity and cell-mediated immunity. In these disease events, some trace elements functions like coenzymes for ubiquitous enzymes and antioxidant molecules [107].
Zn and cadmium [Cd] exposures to yeasts provide protection against oxidative stress to these fungai. These elements are efficient inhibitors of gene expressions related with Cd-triggered redox imbalance, and in this way, displays a protective role against imbalance in iron and zinc ion levels, GSH, and partially restoring mitochondrial membrane potential. Zinc suppresses negative changes in Cd-induced ribosomal proteins, S-containing amino acids, S-rich proteins and the synthesis of antioxidant enzymes [108].
In conditions of hypoxia and ischemia, a buid-up of Zn and ROS has been demonstrated, suggesting a novel cross communication between Zn2+ and mROS through positive feedback processes that eventually induce excess free Zn2+ as well as ROS when there is ischemic stress [109]. In order to keep the stability of intracellular micronutrients, as well as Cu, free radical scavenger, apoptosis inhibitor, metal-binding protein or Metallothionein [MT] has been proposed [110]. Metal-binding protein or MT is non-membrane-bound protein that has low molecular mass, enriched with cysteine [110]. Redox imbalance and blood vessel genesis are shown to be fundamental factors in breast cancer growth. In this process, and vascular endothelial growth factor [VEGF] is used as the best discriminatory biomarker for the presence of breast cancer [111].
2. Conclusion
Macromolecules, Macroelements and dietary elements are important chemical substances that guarantee adequacy and efficiency of the various physiological activities going on in the body. Trace elements, particularly the essential group, when under normal concentrations act as enzymatic body that catalyze many biological processes, such as transport, regulation, metabolism, organogenesis, tissue repair, homeostasis and maintenance etc. as function as biomarkers in various disease state. However, excessive amount of them could trigger deleterious effects, such as disruption of the above mentioned processes including oxidative stress, apoptosis or set the bases for the onset of degenerative diseases. We propose that more prospective studies that would evaluate the impact of abnormal micronutrients and the possible therapeutic value of intervention be conducted. This would improve and strengthen the international guideline recommendations on trace elements and their monitoring.
Author Contributions
DCGa,b,c,d,e, NOBb,c,d,e, MOHb,c,d,e, AVPb,c,d,e, FTJb,c,d,e, EHGb,c,d,e, HJOb,c,d,e, [a] Collaborated in the conception and research design. [b] Assisted in data collection, analysis, or interpretation. [c] Thoroughly reviewed the manuscript for important innovative insights. [d] Wrote the manuscript. [e] Gave final approval.
Funding
This article received no kind of economical support
Authors’ information
Each and every participant in this work is qualified Medical Science Researcher, acknowledged by the Health Ministry of Mexico.
Ethics Statements
Not relevant.
Acknowledgements
We extend our gratitude to Dr. Nwoye Nnamezie Cyril Ndidi, an expert medical research translator and first-language English speaker. The authors extend their sincere appreciation to the National Institute of Pediatrics [NIP] for supporting medical research efforts and for the publication of this article issued on the Program A022.
Conflicts of Interest
The authors have no financial or other competing interests to declare.
References
- Food and nutrition aboard [FNA], National Research Council. Recommended Dietary Allowances. 10th ed. Washington D.C. National Academy Press, 1989.
- Irlam, J.H.; Visser, M.M.; Rollins, N.N.; Siegfried, N. Micronutrient supplementation in children and adults with HIV infection. Cochrane Database Syst Rev 2010, 8, CD003650. [Google Scholar]
- Henche Morilla, A.L.; Romero Montero, C.; Llorente González, C. Levels of oligo-elements and trace elements in patients at the time of admission in intensive care units. Nutr Hosp 1990, 5, 338–344. [Google Scholar]
- Bowen, Humphrey John Moule. Trace elements in biochemistry. Academic Press 1966, ISBN 9780121209506.
- Shier Butler; Lewis David; Jackie Ricki. Hole’s Human Anatomy. Fourteenth Edition; McGraw Hill Education: New York, 2016; p. 59. ISBN 978-0-07-802429-0. [Google Scholar]
- Stephanie L Raehsler; Rok Seon Choung; Eric V Marietta; et al. Accumulation of heavy metals in people on a gluten-free diet. Clin Gastroenterol Hepatol 2018, 16, 244–251. [Google Scholar] [CrossRef]
- Sarah Swayze; Michael Rotondi; Jennifer L Kuk. The association between blood and urinary concentrations of metal metabolites, obesity, hypertension, type 2 diabetes, and dyslipidemia among US Adults: NHANES 1999-2016. J Environ Public Health 2021, 2358060, eCollection 2021. [CrossRef]
- Can Qu; Ruixue Huang. Linking the low-density lipoprotein-cholesterol [LDL] level to arsenic acid, dimethylarsinic, and monomethylarsonic: Results from a National Population-Based Study from the NHANES, 2003-2020. Nutrients 2022, 14, 3993. [Google Scholar] [CrossRef]
- Islam Khairul; Qian Qian Wang; Yu Han Jiang; et al. Metabolism, toxicity and anticancer activities of arsenic compounds. Oncotarget 2017, 8, 23905–23926. [Google Scholar] [CrossRef]
- Maneka Hoonjan; Vaibhav Jadhav; Purvi Bhatt. Arsenic trioxide: Insights into its evolution to an anticancer agent. J Biol Inorg Chem 2018, 23, 313–329. [Google Scholar] [CrossRef]
- Nandita Medda, Subrata Kumar De, Smarajit Maiti. Different mechanisms of arsenic related signaling in cellular proliferation, apoptosis and neo-plastic transformation. Ecotoxicol Environ Saf 2021, 208, 111752. [Google Scholar] [CrossRef]
- Shadi Esmaeili; Ava Safaroghli-Azar; Atieh Pourbagheri-Sigaroodi; et al. Activation of PPARγ intensified the effects of arsenic trioxide in acute promyelocytic leukemia through the suppression of PI3K/Akt pathway: Proposing a novel anticancer effect for pioglitazone. Int J Biochem Cell Biol 2020, 122, 105739. [Google Scholar] [CrossRef]
- Xin Wang; Bhramar Mukherjee; Sung Kyun Park. Associations of cumulative exposure to heavy metal mixtures with obesity and its comorbidities among U.S. adults in NHANES 2003-2014. Environ Int 2018, Pt 1, 683–694. [CrossRef]
- Xu Yao; Xu Steven Xu; Yaning Yang; et al. Stratification of population in NHANES 2009-2014 based on exposure pattern of lead, cadmium, mercury, and arsenic and their association with cardiovascular, renal and respiratory outcomes. Environ Int 2021, 149, 106410. [Google Scholar] [CrossRef]
- Alison P Sanders; Matthew J Mazzella; Ashley J Malin; et al. Combined exposure to lead, cadmium, mercury, and arsenic and kidney health in adolescents age 12-19 in NHANES 2009-2014. Environ Int 2019, 131, 104993. [Google Scholar] [CrossRef]
- Venkatanaidu Karri; Marta Schuhmacher; Vikas Kumar. Heavy metals [Pb, Cd, As and MeHg] as risk factors for cognitive dysfunction: A general review of metal mixture mechanism in brain. Environ Toxicol Pharmacol 2016, 48, 203–213. [Google Scholar] [CrossRef] [PubMed]
- Venkatanaidu Karri; David Ramos; Julia Bauzá Martinez; et al. Differential protein expression of hippocampal cells associated with heavy metals [Pb, As, and MeHg] neurotoxicity: Deepening into the molecular mechanism of neurodegenerative diseases. J Proteomics 2018, 187, 106–125. [Google Scholar] [CrossRef]
- Venkatanaidu Karri; Marta Schuhmacher Professor; Vikas Kumar. A systems toxicology approach to compare the heavy metal mixtures [Pb, As, MeHg] impact in neurodegenerative diseases. Food Chem Toxicol 2020, 139, 111257. [Google Scholar] [CrossRef] [PubMed]
- Emel Koseoglu; Rahmi Koseoglu; Murat Kendirci; et al. Trace metal concentrations in hair and nails from Alzheimer’s disease patients: Relations with clinical severity. J Trace Elem Med Biol 2017, 39, 124–128. [Google Scholar] [CrossRef]
- Takashi Himoto; Tsutomu Masaki. Current trends of essential trace elements in patients with chronic liver diseases. Nutrients 2020, 12, 2084. [Google Scholar] [CrossRef]
- Berglund, S.K.; Torres-Espínola, F.J.; García-Valdés, L.; et al. The impacts of maternal iron deficiency and being overweight during pregnancy on neurodevelopment of the offspring. Br J Nutr 2017, 118, 533–540. [Google Scholar] [CrossRef]
- Bocca, B.; Ciccarelli, S.; Agostino, R.; et al. Trace elements, oxidative status and antioxidant capacity as biomarkers in very low birth weight infants. Environ Res 2017, 156, 705–713. [Google Scholar] [CrossRef]
- Agnieszka Kamińska; Giovanni Luca Romano; Robert Rejdak; et al. Influence of trace elements on neurodegenerative diseases of the eye-the glaucoma model. Int J Mol Sci 2021, 22, 4323. [Google Scholar] [CrossRef]
- Maha M Al-Bazi; Taha A Kumosani; Abdulrahman L Al-Malki; et al. Association of trace elements abnormalities with thyroid dysfunction. Afr Health Sci 2021, 21, 1451–1459. [Google Scholar] [CrossRef] [PubMed]
- Aleksandar Stojsavljević; Branislav Rovčanin; Jovana Jagodić; et al. Alteration of trace elements in multinodular goiter, thyroid adenoma, and thyroid cancer. Biol Trace Elem Res 2021, 199, 4055–4065. [Google Scholar] [CrossRef]
- Rajabian, F.; Mohri, M.; Heidarpour, M. Relationships between oxidative stresses, haematology and iron profile in anaemic and non-anaemic calves. Vet Rec 2017, 181, 265. [Google Scholar] [CrossRef]
- Reichert, C.O.; da Cunha, J.; Levy, D.; et al. Hepcidin: Homeostasis and diseases related to iron metabolism. Acta Haematol 2017, 137, 220–236. [Google Scholar]
- Bai, T.; Wang, S.; Zhao, Y.; et al. Haloperidol, a sigma receptor 1 antagonist, promotes ferroptosis in hepatocellular carcinoma cells. Biochem Biophys Res Commun 2017, 491, 919–925. [Google Scholar] [CrossRef]
- Cusnir, R.; Imberti, C.; Hider, R.C.; et al. Hydroxypyridinone chelators: From iron scavenging to radiopharmaceuticals for PET imaging with gallium-68. Int J Mol Sci 2017, 18, E116. [Google Scholar] [CrossRef]
- Baumann, B.; Sterling, J.; Song, Y.; et al. Conditional müller cell ablation leads to retinal iron accumulation. Invest Ophthalmol Vis Sci 2017, 58, 4223–4234. [Google Scholar] [CrossRef] [PubMed]
- Cappellini, M.D.; Comin-Colet, J.; de Francisco, A.; et al. Iron deficiency across chronic inflammatory conditions: International expert opinion on definition, diagnosis, and management. Am J Hematol 2017, 92, 1068–1078. [Google Scholar] [CrossRef]
- Rehou, S.; Shahrokhi, S.; Natanson, R.; et al. Antioxidant and trace element supplementation reduce the inflammatory response in critically ill burn patients. J Burn Care Res Aug 2017, 31. [Google Scholar] [CrossRef]
- Çavuşoğlu, Y.; Altay, H.; Çetiner, M.; et al. Iron deficiency and anemia in heart failure. Turk Kardiyol Dern Ars 2017, 45, 1–38. [Google Scholar] [PubMed]
- Xin Yang; Zhe Tang; Jing Li; et al. Esophagus cancer and essential trace elements. Front Public Health 2022, 10, 1038153. [Google Scholar] [CrossRef]
- Sehar Iqbal; Inayat Ali. Dietary trace element intake and risk of breast cancer: A mini review. Biol Trace Elem Res 2022, 200, 4936–4948. [Google Scholar] [CrossRef]
- Hassan, R.H.; Kandil, S.M.; Zeid, M.S.; et al. Kidney injury in infants and children with iron-deficiency anemia before and after iron treatment. Hematology 2017, 22, 565–570. [Google Scholar] [CrossRef]
- Coates, T.D.; Wood, J.C. How we manage iron overload in sickle cell patients. Br J Haematol 2017, 177, 703–716. [Google Scholar]
- Kraml, P. The role of iron in the pathogenesis of atherosclerosis. Physiol Res 2017, 66, S55–S67. [Google Scholar] [CrossRef] [PubMed]
- Jamnongkan, W.; Thanan, R.; Techasen, A.; et al. Upregulation of transferrin receptor-1 induces cholangiocarcinoma progression via induction of labile iron pool. Tumour Biol 2017, 39, 1010428317717655. [Google Scholar] [CrossRef] [PubMed]
- Guarda, C.C.D.; Santiago, R.P.; Fiuza, L.M.; et al. Heme-mediated cell activation: The inflammatory puzzle of sickle cell anemia. Expert Rev Hematol 2017, 10, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Crielaard, B.J.; Lammers, T.; Rivella, S. Targeting iron metabolism in drug discovery and delivery. Nat Rev Drug Discov 2017, 16, 400–423. [Google Scholar] [CrossRef]
- Ferreira, K.P.; Oliveira, S.R.; Kallaur, A.P.; et al. Disease progression and oxidative stress are associated with higher serum ferritin levels in patients with multiple sclerosis. J Neurol Sci 2017, 373, 236–241. [Google Scholar] [CrossRef]
- Bajbouj, K.; Shafarin, J.; Abdalla, M.Y.; et al. Estrogen-induced disruption of intracellular iron metabolism leads to oxidative stress, membrane damage, and cell cycle arrest in MCF-7 cells. Tumour Biol 2017, 39, 1010428317726184. [Google Scholar] [CrossRef]
- Pizzamiglio, S.; De Bortoli, M.; Taverna, E.; et al. Expression of iron-related proteins differentiate non-cancerous and cancerous breast tumors. Int J Mol Sci 2017, 18, 410. [Google Scholar] [CrossRef]
- Franěk, T.; Kotaška, K.; Průša, R. Manganese and selenium concentrations in cerebrospinal fluid of seriously ill children. J Clin Lab Anal 2017, 31. [Google Scholar] [CrossRef]
- Christian L Görlich; Qian Sun; Viola Roggenkamp; et al. Selenium status in paediatric patients with neurodevelopmental diseases. Nutrients 2022, 14, 2375. [Google Scholar] [CrossRef]
- Sandstead, H.H.; Prasad, A.S.; Penland, J.G.; et al. Zinc deficiency in Mexican American children: Influence of zinc and other micronutrients on T cells, cytokines, and antiinflammatory plasma proteins. Am J Clin Nutr 2008, 88, 1067–1073. [Google Scholar] [CrossRef]
- Long, K.Z.; Rosado, J.L.; Montoya, Y.; et al. Effect of vitamin A and zinc supplementation on gastrointestinal parasitic infections among Mexican children. Pediatrics 2007, 120, e846–e855. [Google Scholar] [CrossRef] [PubMed]
- Villalpando, S.; Pérez-Expósito, A.B.; Shamah-Levy, T.; et al. Distribution of anemia associated with micronutrient deficiencies other than iron in a probabilistic sample of Mexican children. Ann Nutr Metab 2006, 50, 506–511. [Google Scholar] [CrossRef]
- Flynn, A. Minerals and trace elements in milk. Adv Food Nutr Res 1992, 36, 209–252. [Google Scholar] [PubMed]
- Singh, M.; Das, R.R. Zinc for the common cold. Cochrane Database Syst Rev 2011, 16, CD001364. [Google Scholar]
- Vernacchio, L.; Kelly, J.P.; Kaufman, D.W.; et al. Vitamin, fluoride, and iron use among US children younger than 12 years of age: Results from the Slone Survey 1998-2007. J Am Diet Assoc 2011, 111, 285–289. [Google Scholar] [CrossRef]
- Razi CH, Akin O., Harmanci K; et al. (2011) Serum heavy metal and antioxidant element levels of children with recurrent wheezing. Allergol Immunopathol [Madr] Jan 12. Epub ahead of print.
- Van Santen, S.; de Mast, Q.; Luty, A.J.; et al. Iron homeostasis in mother and child during placental malaria infection. Am J Trop Med Hyg 2011, 84, 148–151. [Google Scholar] [CrossRef]
- Habib, M.A.; Soofi, S.B.; Bhutta, Z.A. Effect of zinc in tablet and suspension formulations in the treatment of acute diarrhoea among young children in an emergency setting of earthquake affected region of Pakistan. J Coll Physicians Surg Pak 2010, 20, 837–838. [Google Scholar]
- Troesch, B.; van Stujivenberg, M.E.; Smuts, C.M.; et al. A micronutrient powder with low doses of highly absorbable iron and zinc reduces iron and zinc deficiency and improves weight-for-age Z-scores in South African children. J Nutr 2011, 141, 237–242. [Google Scholar] [CrossRef]
- Christian, P.; Murray-Kolb, L.E.; Khatry, S.K.; et al. Prenatal micronutrient supplementation and intellectual and motor function in early school-aged children in Nepal. JAMA 2010, 304, 2716–2723. [Google Scholar] [CrossRef] [PubMed]
- Muhsen, K.; Barak, M.; Henig, C.; et al. Is the association between Helicobacter pylori infection and anemia age dependent? Helicobacter 2010, 15, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Habis, A.; Hobson, W.L.; Greenberg, R. Cerebral sinovenous thrombosis in a toddler with iron deficiency anemia. Pediatr Emerg Care 2010, 26, 848–851. [Google Scholar] [CrossRef] [PubMed]
- Pasricha, S.R.; Flecknoe-Brown, S.C.; Allen, K.J.; et al. Diagnosis and management of iron deficiency anaemia: A clinical update. Med J Aust 2010, 193, 525–532. [Google Scholar] [CrossRef]
- Arlet, J.B.; Hermine, O.; Darnige, L.; et al. Iron-deficiency anemia in Castleman disease: Implication of the interleukin 6/hepcidin pathway. Pediatrics 2010, 126, e1608–e1612. [Google Scholar] [CrossRef]
- Kelishadi, R.; Hashemipour, M.; Adeli, K.; et al. Effect of zinc supplementation on markers of insulin resistance, oxidative stress, and inflammation among prepubescent children with metabolic syndrome. Metab Syndr Relat Disord 2010, 8, 505–510. [Google Scholar] [CrossRef]
- Tascilar, M.E.; Ozgen, I.T.; Abaci, A.; et al. Trace elements in obese Turkish children. Biol Trace Elem Res.
- Riojas-Rodríguez, H.; Solís-Vivanco, R.; Schilmann, A.; et al. Intellectual function in Mexican children living in a mining area and environmentally exposed to manganese. Environ Health Perspect 2010, 118, 1465–1470. [Google Scholar] [CrossRef]
- Mahyar, A.; Ayazi, P.; Fallahi, M.; et al. Correlation between serum selenium level and febrile seizures. Pediatr Neurol 2010, 43, 331–334. [Google Scholar] [CrossRef]
- Gara, S.N.; Madaki, A.J.; Thacher, T.D. A comparison of iron and folate with folate alone in hematologic recovery of children treated for acute malaria. Am J Trop Med Hyg 2010, 83, 843–847. [Google Scholar] [CrossRef]
- Savino, W.; Dardenne, M. Nutritional imbalances and infections affect the thymus: Consequences on T-cell-mediated immune responses. Proc Nutr Soc 2010, 69, 636–643. [Google Scholar] [CrossRef]
- Harrington, M.; Hotz, C.; Zeder, C.; et al. A comparison of the bioavailability of ferrous fumarate and ferrous sulfate in non-anemic Mexican women and children consuming a sweetened maize and milk drink. Eur J Clin Nutr 2011, 65, 20–25. [Google Scholar] [CrossRef]
- Dylewski, M.L.; Bender, J.C.; Smith, A.M.; et al. The selenium status of pediatric patients with burn injuries. J Trauma 2010, 69, 584–588. [Google Scholar] [CrossRef]
- Takuma, Y.; Nouso, K.; Makino, Y.; et al. Clinical trial: Oral zinc in hepatic encephalopathy. Aliment Pharmacol Ther 2010, 32, 1080–1090. [Google Scholar] [CrossRef]
- Afridi, H.I.; Kazi, T.G.; Kazi, N.; et al. Evaluation of essential trace and toxic elements in biological samples of normal and night blindness children of age groups 3-7 and 8-12 years. Biol Trace Elem Res 2010. Sep 4. Epub ahead of print. [Google Scholar]
- Remer, T.; Johner, S.A.; Gärtner, R.; et al. Iodine deficiency in infancy - a risk for cognitive development. Dtsch Med Wochenschr, 1551. [Google Scholar]
- Balay, K.S.; Hawthorne, K.M.; Hicks, P.D.; et al. Orange but not apple juice enhances ferrous fumarate absorption in small children. J Pediatr Gastroenterol Nutr 2010, 50, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Pinto, R.B.; Fröehlich, P.E.; Pitrez, E.H.; et al. MR findings of the brain in children and adolescents with portal hypertension and the relationship with blood manganese levels. Neuropediatrics 2010, 41, 12–17. [Google Scholar] [CrossRef]
- Ralston, N.V.; Raymond, L.J. Dietary selenium’s protective effects against methylmercury toxicity. Toxicology 2010, 278, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Hegazy, A.A.; Zaher, M.M.; Abd El-Hafez, M.A.; et al. Relation between anemia and blood levels of lead, copper, zinc and iron among children. BMC Res Notes 2010, 12, 133. [Google Scholar] [CrossRef]
- Tondo, M.; Moreno, J.; Casado, M.; et al. Selenium concentration in cerebrospinal fluid samples from a pediatric population. Neurochem Res 2010, 35, 1290–1293. [Google Scholar] [CrossRef] [PubMed]
- Alireza Mohammadi; Ehsan Rashidi; Vahid Ghasem Amooeian. Brain, blood, cerebrospinal fluid, and serum biomarkers in schizophrenia. Psychiatry Res 2018, 265, 25–38. [Google Scholar] [CrossRef] [PubMed]
- Sarah Rehou; Shahriar Shahrokhi; Rimona Natanson; et al. Antioxidant and trace element supplementation reduce the inflammatory response in critically ill burn patients. J Burn Care Res 2018, 39, 1–9. [Google Scholar] [CrossRef]
- Mehran Shayganfard. Are essential trace elements effective in modulation of mental disorders? Update and perspectives. Biol Trace Elem Res 2022, 200, 1032–1059. [Google Scholar] [CrossRef]
- Giovanni Forte; Beatrice Bocca; Andrea Pisano; et al. Trace elements in sputum as biomarkers for idiopathic pulmonary fibrosis. The levels of trace. Chemosphere 2021, 271, 129514. [Google Scholar] [CrossRef]
- Wacewicz, M.; Socha, K.; Soroczyńska, J.; et al. Concentration of selenium, zinc, copper, Cu/Zn ratio, total antioxidant status and c-reactive protein in the serum of patients with psoriasis treated by narrow-band ultraviolet B phototherapy: A case-control study. J Trace Elem Med Biol 2017, 44, 109–114. [Google Scholar] [CrossRef]
- . Shahidi-Dadras, M.; Namazi, N.; Younespour, S. Comparative analysis of serum copper, iron, ceruloplasmin, and transferrin levels in mild and severe psoriasis vulgaris in Iranian patients. Indian Dermatol Online J 2017, 8, 250–253. [Google Scholar]
- Shi, L.; Cao, H.; Luo, J.; et al. Effects of molybdenum and cadmium on the oxidative damage and kidney apoptosis in Duck. Ecotoxicol Environ Saf 2017, 145, 24–31. [Google Scholar] [CrossRef]
- Vaz, F.N.C.; Fermino, B.L.; Haskel, M.V.L.; et al. The relationship between copper, iron, and selenium levels and alzheimer disease. Biol Trace Elem Res 2018, 181, 185–191. [Google Scholar] [CrossRef]
- Dirksen, K.; Spee, B.; Penning, L.C.; et al. Gene expression patterns in the progression of canine copper-associated chronic hepatitis. PLoS ONE 2017, 12, e0176826. [Google Scholar] [CrossRef]
- Meramat, A.; Rajab, N.F.; Shahar, S.; et al. DNA damage, copper and lead associates with cognitive function among older adults. J Nutr Health Aging 2017, 21, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Ogórek, M.; Gąsior, Ł.; Pierzchała, O.; et al. Role of copper in the process of spermatogenesis. Postepy Hig Med Dosw 2017, 71, 663–683. [Google Scholar] [CrossRef]
- Li, S.W.; Shao, Y.Z.; Zhao, H.J.; et al. Analysis of 28 trace elements in the blood and serum antioxidant status in chickens under arsenic and/or copper exposure. Environ Sci Pollut Res Int 2017, 24, 27303–27313. [Google Scholar] [CrossRef]
- Keshavarz, P.; Nobakht, M.; Mirhafez, S.R.; et al. Alterations in lipid profile, zinc and copper levels and superoxide dismutase activities in normal pregnancy and preeclampsia. Am J Med Sci 2017, 353, 552–558. [Google Scholar] [CrossRef]
- Bahi, G.A.; Boyvin, L.; Méité, S.; et al. Assessments of serum copper and zinc concentration, and the Cu/Zn ratio determination in patients with multidrug resistant pulmonary tuberculosis [MDR-TB] in Côte d’Ivoire. BMC Infect Dis 2017, 17, 257. [Google Scholar] [CrossRef]
- Malak Alghamdi; Janelle Gutierrez; Slavko Komarnytsky. Essential minerals and metabolic adaptation of immune cells. Nutrients 2022, 15, 123. [Google Scholar] [CrossRef]
- Yu-Jing Huang; Guang-Xian Nan. Oxidative stress-induced angiogénesis. J Clin Neurosc 2019, 63, 13–16. [Google Scholar] [CrossRef]
- Joaquim Rovira; Anna Hernández-Aguilera; Fedra Luciano-Mateo; et al. Trace elements and paraoxonase-1 activity in lower extremity artery disease. Biol Trace Elem Res 2018, 186, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Nazıroğlu, M.; Muhamad, S.; Pecze, L. Nanoparticles as potential clinical therapeutic agents in Alzheimer’s disease: Focus on selenium nanoparticles. Expert Rev Clin Pharmacol 2017, 10, 773–782. [Google Scholar] [CrossRef] [PubMed]
- Baltaci, A.K.; Yuce, K.; Mogulkoc, R. Zinc metabolism and metallothioneins. Biol Trace Elem Res 2018, 183, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Qiu, M.; Shentu, Y.P.; Zeng, J.; et al. Zinc mediates the neuronal activity-dependent anti-apoptotic effect. PLoS ONE 2017, 12, e0182150. [Google Scholar] [CrossRef] [PubMed]
- Doboszewska, U.; Wlaź, P.; Nowak, G. Zinc in the monoaminergic theory of depression: Its relationship to neural plasticity. Neural Plast 2017, 3682752. [Google Scholar] [CrossRef] [PubMed]
- Sharaf, M.S.; Stevens, D.; Kamunde, C. Zinc and calcium alter the relationship between mitochondrial respiration, ROS and membrane potential in rainbow trout [Oncorhynchus mykiss] liver mitochondria. Aquat Toxicol 2017, 189, 170–183. [Google Scholar] [CrossRef]
- Wiebke Alker; Hajo Haase. Zinc and sepsis. Nutrients 2018, 10, 976. [Google Scholar] [CrossRef]
- Ariaee, N.; Farid, R.; Shabestari, F.; et al. Trace elements status in sera of patients with allergic asthma. Rep Biochem Mol Biol 2016, 5, 20–25. [Google Scholar]
- Xie, F.; Zhang, X.; Xie, L. Prognostic value of serum zinc levels in patients with acute HC/zinc chloride smoke inhalation. Medicine [Baltimore] 2017, 96, e8156. [Google Scholar] [CrossRef] [PubMed]
- Zanganeh, N.; Siahpoushi, E.; Kheiripour, N.; et al. Brucellosis causes alteration in trace elements and oxidative stress factors. Biol Trace Elem Res 2018, 182, 204–208. [Google Scholar] [CrossRef]
- Samadieh, H.; Mohammadi, G.R.; Maleki, M.; et al. Relationships between oxidative stress, liver, and erythrocyte injury, trace elements and parasite burden in sheep naturally infected with dicrocoelium dendriticum. Iran J Parasitol 2017, 12, 46–55. [Google Scholar]
- Eljaoudi, R.; Elomri, N.; Laamarti, M.; et al. Antioxidants status in type 2 diabetic patients in Morocco. Turk J Med Sci 2017, 47, 782–788. [Google Scholar] [CrossRef]
- Mishra, S.; Mishra, B.B. Study of lipid peroxidation, nitric oxide end product, and traceelement status in type 2 diabetes mellitus with and without complications. Int J Appl Basic Med Res 2017, 7, 88–93. [Google Scholar] [CrossRef]
- Daniela Cannas; Eleonora Loi; Matteo Serra; et al. Relevance of essential trace elements in nutrition and drinking water for human health and autoimmune disease risk. Nutrients 2020, 12, 2074. [Google Scholar] [CrossRef]
- Pan, J.; Huang, X.; Li, Y.; et al. Zinc protects against cadmium-induced toxicity by regulating oxidative stress, ions homeostasis and protein synthesis. Chemosphere 2017, 188, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Slepchenko, K.G.; Lu, Q.; Li, Y.V. Cross talk between increased intracellular zinc [Zn2+] and accumulation of reactive oxygen species in chemical ischemia. Am J Physiol Cell Physiol 2017, 313, C448–C459. [Google Scholar] [CrossRef] [PubMed]
- Ono, S.I. Metallothionein is a potential therapeutic strategy for amyotrophic lateral sclerosis. Curr Pharm Des 2017, 23, 5001–5009. [Google Scholar] [CrossRef] [PubMed]
- Kanchan Karki; Shahi, K.S.; Rashmi Bisht; et al. Biochemical investigation of tissue oxidative stress and angiogenesis with associated trace elements in breast disease patients in Uttarakhand, India. J Environ Pathol Toxicol Oncol 2019, 38, 377–390. [Google Scholar] [CrossRef]
Figure 1.
Glycolysis.
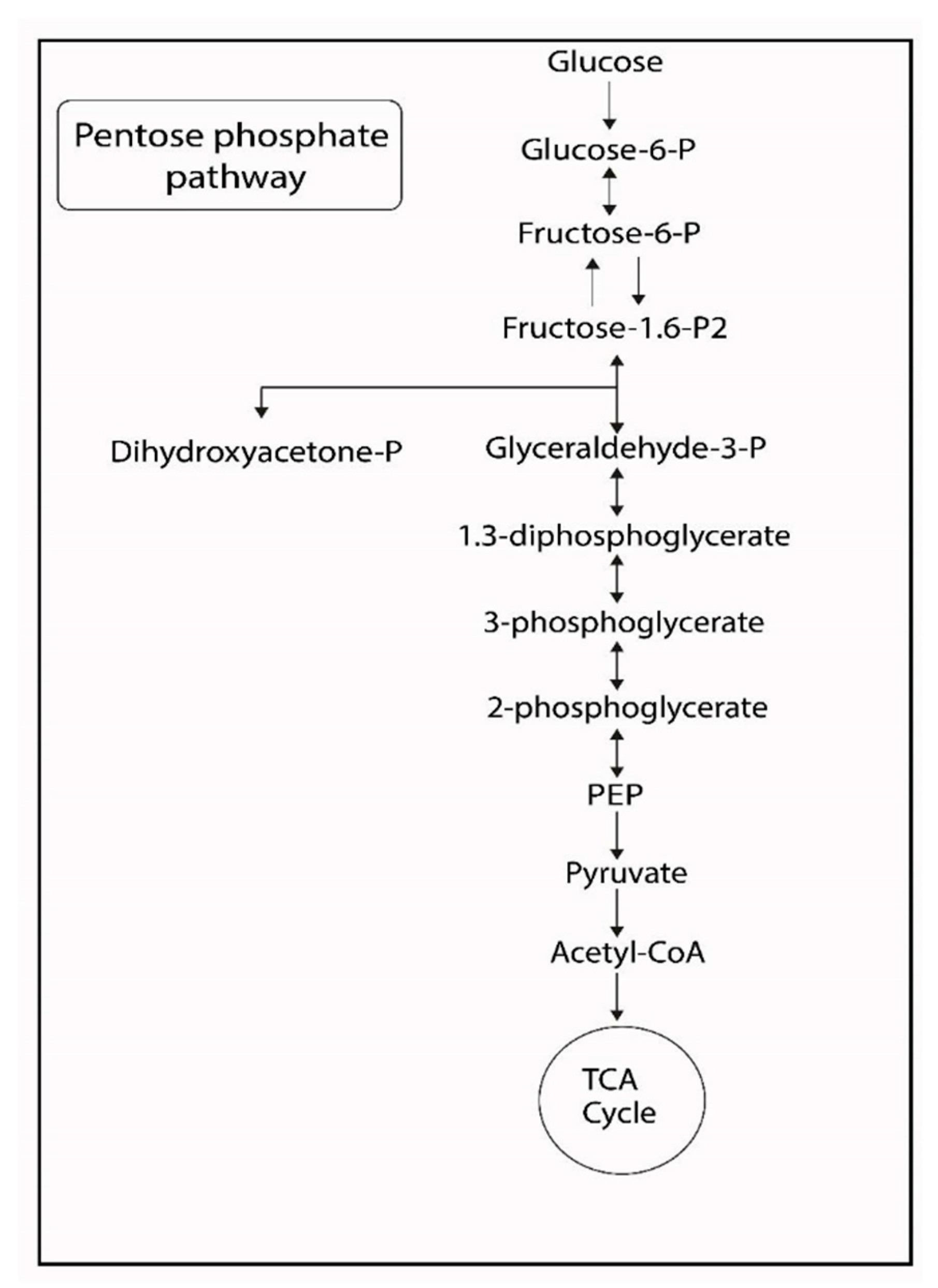
Figure 2.
Tricarboxilic acid cycle.
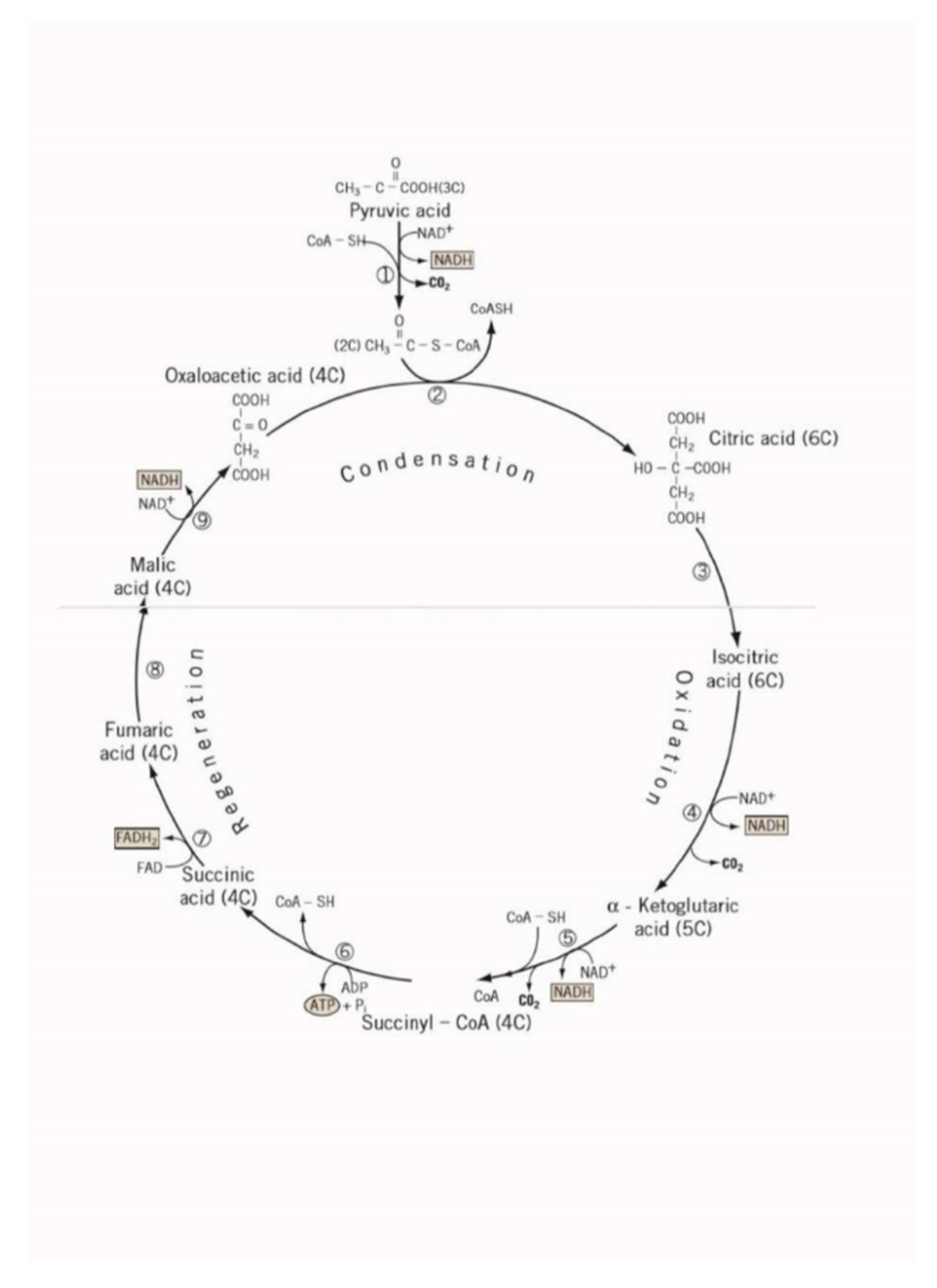
Figure 3.
Glutathione.
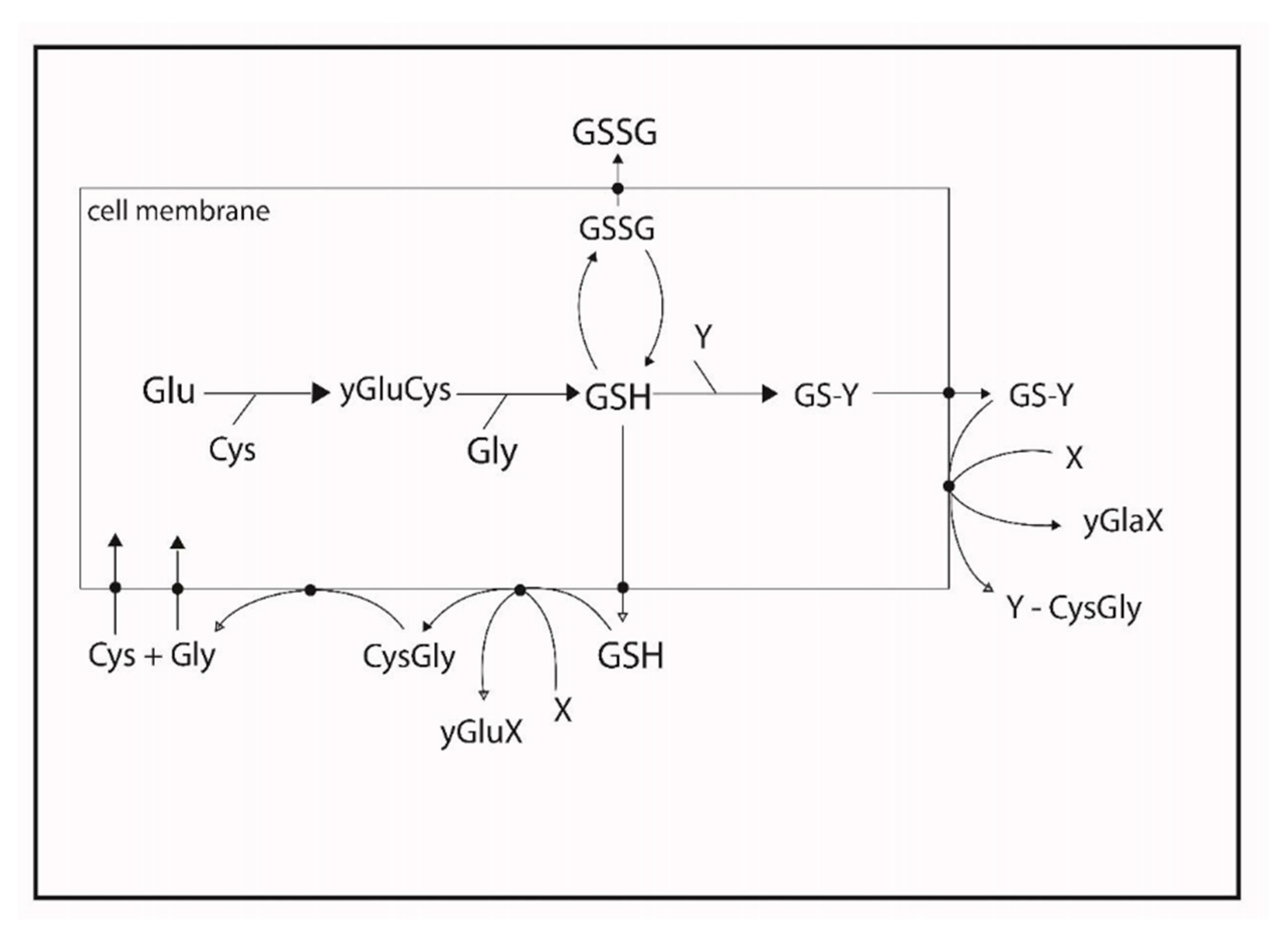
Figure 4.
Lipids.
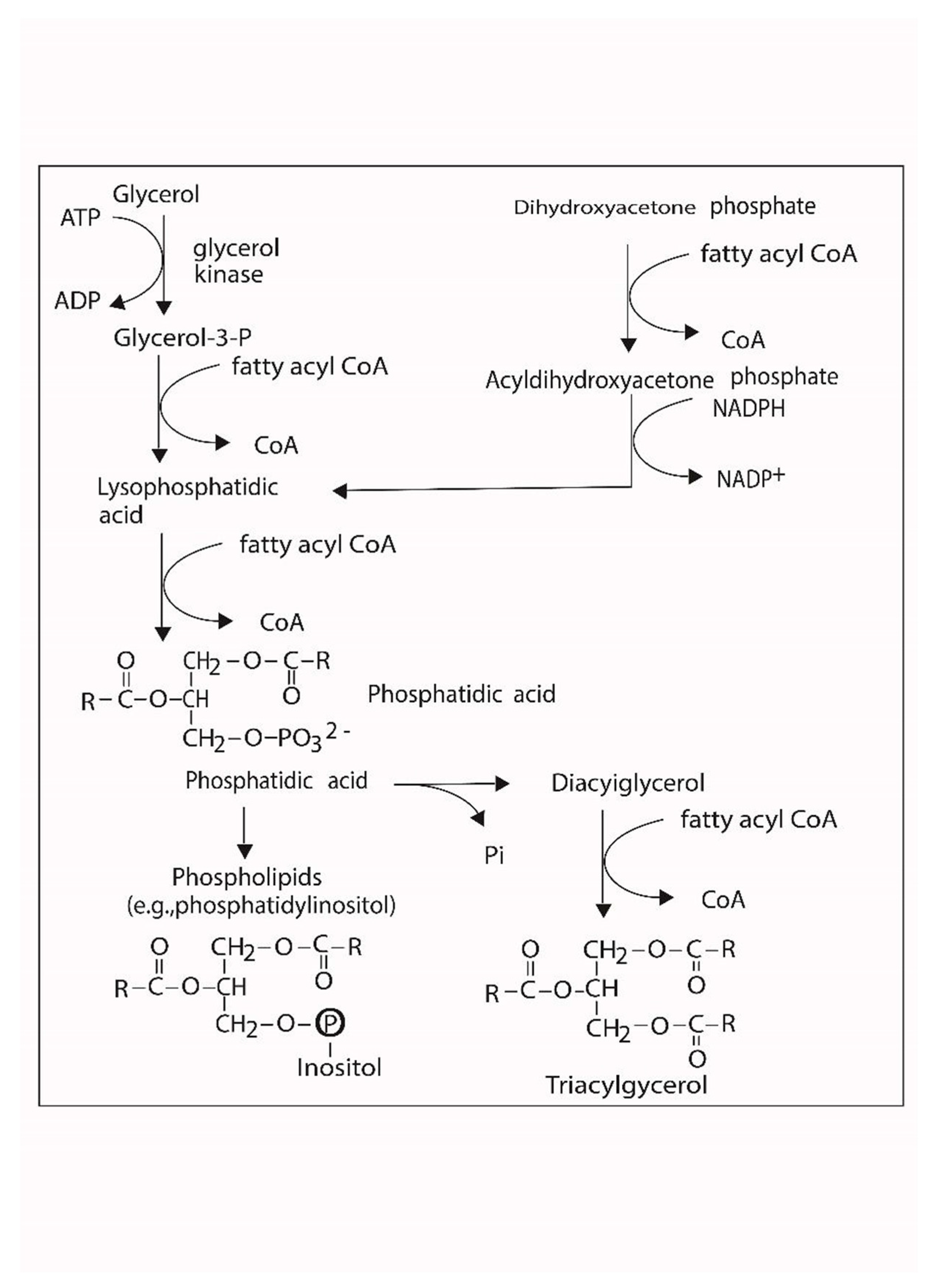
Figure 5.
Reactive oxygen species.
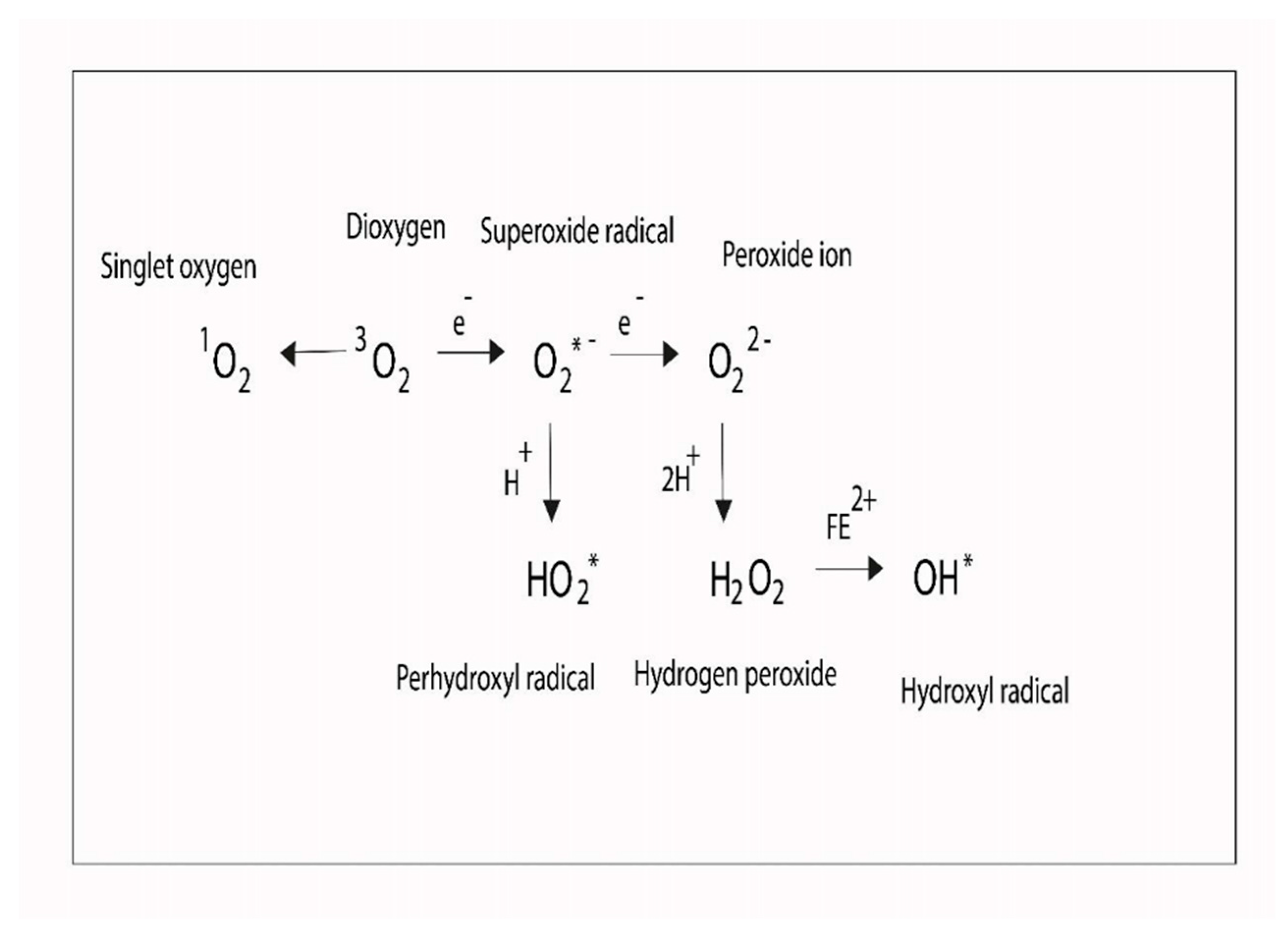
Figure 6.
DNA Damage.
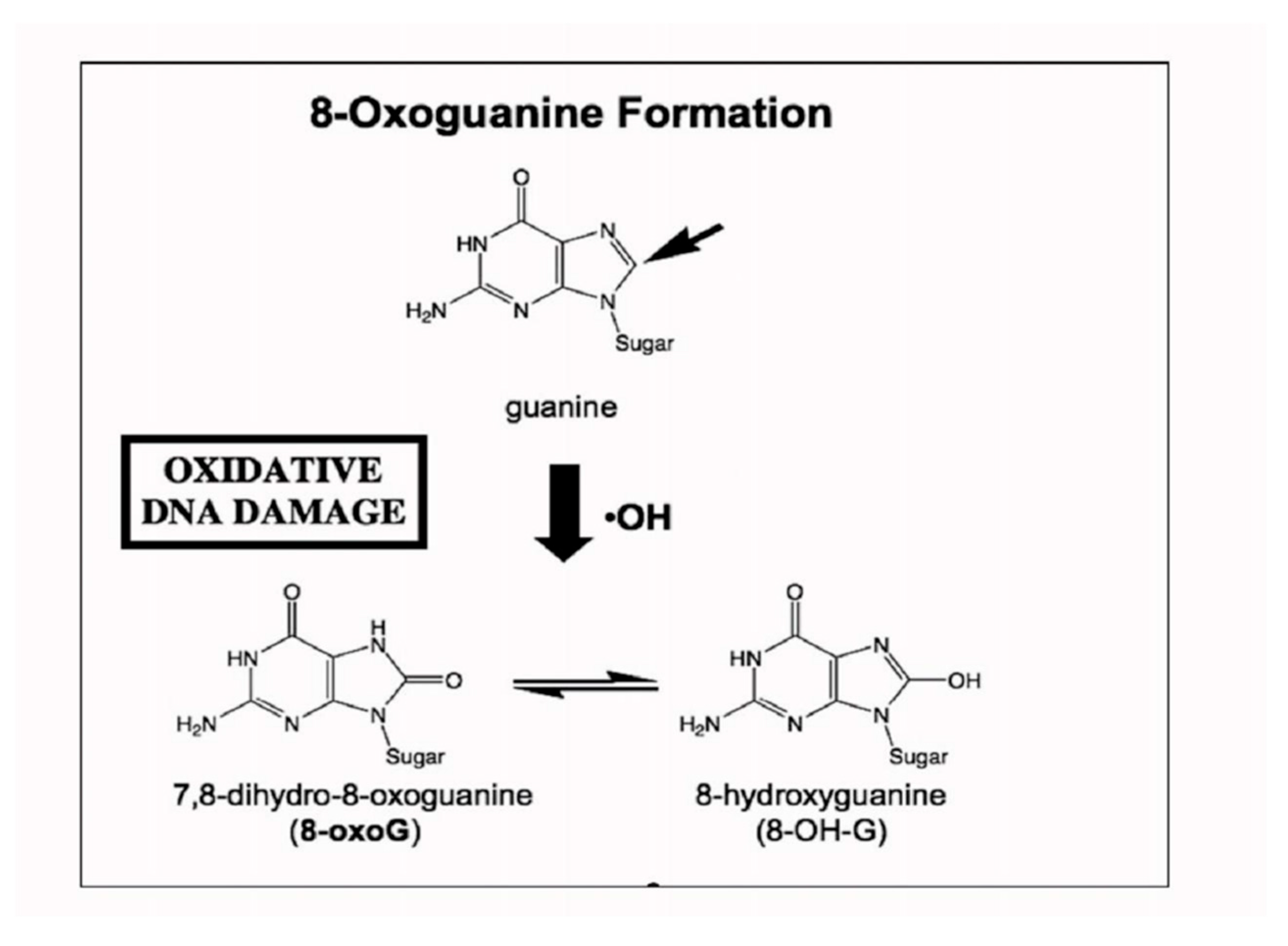

Table 1.
Trace elements and abundant elements.
| Major Elements [mg/L] | Trace Elements [µg/L] | ||
|---|---|---|---|
| Cl- | 19,295 ± 135 | Mn | 5.235 ± 0.046 |
| Na | 10,690 ± 110 | Fe | 1.773 ± 0.012 |
| SO₄²⁻ | 2701 ± 37 | Zn | 0.785 ± 0.002 |
| Ca | 416 ± 15 | Cu | 0.635 ± 0.025 |
| K | 390 ± 10 | V (Vanadium) | 1.45 ± 0.7 |
| HCO3⁻ | 145 ± 12 | Ni (Nickel) | 0.327 ± 0.012 |
| Mg | 128 ± 5 | Pb | 0.045 ± 0.025 |
| Br | 62 ± 5 | Cd (Cadmium) | 0.035 ± 0.008 |
| BO3−3 (Borate) | 27 ± 2 | Hg | Undetected |
| Sr (Strontium) | 13.2 ± 0.5 | As (Arsenic) | Undetected |
| F⁻ | 1.35 ± 0.02 | ||
Elements such as Silver [Ag], arsenic [As], cadmium [Cd], chromo [Cr], mercury [Hg], lead [Pb] and tin [Sn] have no known biological function and they can be toxic even at low concentration.
Table 2.
Studies of trace elements in patients.
| Symbol | Biological Effects | Ref. |
|---|---|---|
| Zn | Joint tx involving Zn and micronutrients elevates neutrophil-to-lymphocyte ratio of T helper cells/CD8-positive T cells, and of CD4[+] to CD8[+] and CD4[+]CD45RA[+] to CD4[+]CD45RO[+]. | [47] |
| Zn | Retinol in combination wih Zn decreases Giardiasis. Zn intake elevates the incidence of Ascaris lumbricoides and lessens Entamoeba histolytica-associated diarrhea. | [48] |
| Fe | Erythrocytopenia is linked to Iron-depleted state, lower concentration do folic acid and retinol deficiency. | [49] |
| Se | Mineral and micronutrients proportions in infant formulas for full-term infants are generally higher than in human breast milk. However, Se levels in these formulas is far from adequate and needs to be increased in some formulas. | [50] |
| Zn | The incidence rate ratio [IRR] of developing a cold [IRR 0.64; 95% CI 0.47 to 0.88] [P = 0.006], school absence [P = 0.0003] and prescription of antibiotics [P < 0.00001] was lower in people using Zn supplement. | [51] |
| Fe | Approximately a quarter of US children less than 12-year old, and 30% of 2-year-olds, use dietary supplements, F- and Fe at least once a week. | [52] |
| Se, Zn | Increeased blood Pb and Hg, and Elevated levels of serum lead and mercury, and Zn and Se deficiency could infer antioxidant system alterations in children with recurrent wheezing. | [53] |
| Fe | Maternal iron regulatory hormone did not show a statistically significant change in thee course of infection in the placenta as well as in erythropenia. | [54] |
| Zn | Zn diminishes the occurrence of diarrhea as well as optimizes recovery outcomes of this sickness. | [55] |
| Fe, Zn | The powder form of these micronutrients promotes high native iron absorption in cereal/legume-based complementary foods. | [56] |
| Zn | Prenatal iron/folic acid supplementation has been positively linked with some features of cognitive capacity, e.g., active memory, response inhibition and fine motor functioning in children living in iron-deficient areas. | [57] |
| Zn | Zn is not affected by human immunodeficiency infection in both children and adults, rather it is found to be benefitial in these patients with diarrhea. | [58] |
| Fe | H. pylori infection is linked with increased rate of anemia in school children independently of socioeconomic variables. | [59] |
| Fe | Severe anemia due to inadequate dietary iron intake is associated with sagittal sinus venous thrombosis in children. | [60] |
| Fe | Oral iron therapy, in appropriate doses and for a sufficient duration, is an effective first-line strategy for most patients. The same happens in selected patients for whom intravenous [IV] iron therapy is indicated. | [61] |
| Fe | Iron-regulatory hormone (hepcidin) production in humans is regulated by Interleukin-6 (IL-6). This means that iron deficiency is a causal link between IL-6 and anemia of chronic disease. | [62] |
| Zn | Zinc supplement exhibits a considerable diminution in the mean BMI. However, this promising benefit has not been explore in obese children and needs to be an object of study. | [63] |
| Se, Fe | These micronutrients probably induce changes in the profile of trace elements in the blood of patients with childhood obesity. | [64] |
| Mn | Environmental inhalation exposure to manganese is negatively correlated with cognitive capacity in school children. | [65] |
| Se | Se blood level in febrile-seizure pediatric patients was substantially decreased when compared with nonseizure control group. This suggests a probable link between low serum selenium concentration and simple febrile seizures. | [66] |
| Fe | Iron administration improved hematologic recovery in children with malarial anemia. Children 6-60 months of age with blood film-positive malaria and anemia [hematocrit < 33%] should receive iron [2 mg/kg/day] plus folate [5 mg/day] or folate alone. | [67] |
| Zn | A combined vitamin and micronutrients can induce deep alterations in the thymus as seen in thymus-zinc associated atrophy. | [68] |
| Fe | In healthy children and those with non-anemic iron deficient, iron(II) fumarate and iron(II) sulfate are well absorbed and could serve as a useful fortification compound for complementary foods designed to prevent iron deficiency. | [69] |
| Se | In children with burns, selenium status is decreased showing that selenium intake for healthy children is likely insufficient for this population. | [70] |
| Zn | In hepatic encephalopathy, Zn administrationconstitutes an effective treatment and improves the quality of life of these patients. | [71] |
| Zn | In the scalp and blood of children suffering from night blindness, Zn, Ca, K, and Mg levels were found to be low. | [72] |
| I | It is recommended that iodine intake of 4-month old infants should be increased from the current dose of 40 µg/d to at least 60 µg/d. | [73] |
| Fe | The administration of ferrous fumarate with orange juice enhances the absorption of iron by almost 2-folds in more than six-year old children. | [74] |
| Mn | In the basal ganglia of patients with portal hypertension, magnetic resonance imaging (MRI) of the brain depicted high T1 hyperintensity frequency [64%] correlating positively with blood manganese levels. | [75] |
| Se | Studies of populations exposed to Methyl-Mercury [MeHg] by eating Se-rich ocean fish observed improved child IQs instead of harm. | [76] |
| Fe | Lead level >/= 10 µg/dl strongly correlated with anemia, decreased iron absorption and affectation of hematological parameters. High serum Pb levels were linked with decreased blood iron and ferritin. | [77] |
| Se | Selenium concentrations in Cerebrum Spinal Fluid (CSF) were 32 times lower versus plasma values. There was an association observed between CSF Se and GPX activity. | [78] |
Zn [Zinc], Fe [Iron], Se [Selenium], Mn [Manganese], I [Iodine].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



