
Submitted:
19 September 2025
Posted:
22 September 2025
You are already at the latest version
Abstract
Context: Neglected Tropical Diseases (NTDs) are infectious illnesses prevalent in tropical and subtropical regions, disproportionately affecting vulnerable populations with limited access to healthcare. Understanding the spatial and temporal dynamics of these diseases in specific regions, such as northern Brazil, is crucial for guiding control strategies. The state of Pará, characterised by low human development indices, is a significant hotspot for NTDs. Development: This cross-sectional study analysed the spatio-temporal distribution of major autochthonous NTDs in Pará between 2016 and 2022, using data from Brazil’s Notifiable Diseases Information System (SINAN). Incidence rates were calculated for dengue, Chagas disease, leishmaniasis (cutaneous and visceral), leprosy, tuberculosis, and schistosomiasis, and used to generate spatial cluster maps. Results: The analysis revealed patterns of clustering and dispersion, with high-risk areas identified in the Southeast (Carajás), Marajó, and Belém Metropolitan regions. Cutaneous leishmaniasis was widespread in Marajó and southwestern Pará, while visceral leishmaniasis was concentrated in the southeast. Leprosy remained prevalent in urban and peri-urban zones, and schistosomiasis persisted in riverside communities. The Southeast region showed a high burden of four NTDs. Conclusion: Spatio-temporal analysis of NTDs in Pará revealed geographic clusters, socio-environmental influences, and diagnostic gaps, guiding targeted, adaptive public health strategies and future research priorities.
Keywords:
neglected tropical diseases
; spatial analysis
; geographic information systems
; Brazil
; health information systems
; leishmaniasis
; leprosy
; schistosomiasis
; dengue
; tuberculosis
1. Introduction
Neglected Tropical Diseases (NTDs) are a group of diverse infectious diseases caused by protozoa, fungi, helminths, bacteria, and viruses, which occur predominantly in areas with significant social vulnerabilities. Although they are found worldwide, countries in Africa, Asia, and Latin America are the most affected, due to the intrinsic link between these diseases and low socio-economic development indicators [1,2].
Furthermore, NTDs are more prevalent in tropical countries or territories, where they contribute to and are sustained by a cycle of poverty, leading to their continued spatial spread in vulnerable areas. In this context, controlling NTDs requires integrated interventions that are locally specific and based on up-to-date data [3].
A “Health in All Policies” approach is recommended as a model to integrate the social and economic conditions that influence the burden of multiple diseases [4]. Integrated mapping is essential for the success of NTD control programmes [1,5].
Brazil has a high prevalence of Neglected Tropical Diseases (NTDs), particularly in regions characterised by low socio-economic development and limited access to healthcare services. The distribution of these diseases is heterogeneous across the national territory, with certain illnesses being more common in specific regions — such as leishmaniasis in the North and Northeast, schistosomiasis in the Northeast and Southeast, and Chagas disease in the Central-West and Southeast. This pattern reflects a combination of environmental factors (such as the presence of vectors and reservoirs), social factors (including poverty and low levels of education), and structural issues (such as inadequate sanitation and weaknesses in local health surveillance and care systems), all of which directly influence the spread of these diseases [6].
NTDs are significant contributors to years of life lost due to premature death and years lived with disability, particularly among vulnerable populations and in Brazilian regions with lower socio-economic development[7].
In the Northern region of Brazil, there is a high incidence of these diseases, resulting from a complex interaction of environmental factors (such as a hot and humid climate conducive to the proliferation of vectors), geographical factors (including remote areas and low population density), and socio-economic factors (such as a high Gini index or low Human Development Index, low levels of education, and poor infrastructure). These structural determinants are strongly associated with persistent poverty, the absence of inadequacy of basic sanitation, and limited coverage of healthcare services—particularly the Family Health Strategy (FHS)which facilitates the persistence and spread of these diseases [6]. The North and Northeast regions of the country have the lowest Human Development Index (HDI) scores and the highest rates of NTDs, underscoring the correlation between social vulnerability and disease burden[8].
In the present study, the spatial distribution of certain notifiable diseases was analysed. These diseases are considered priorities in Brazil due to their high prevalence, significant impact on public health, and potential for control and elimination through appropriate interventions and effective public health strategies. Although tuberculosis is not officially classified as a neglected tropical disease, it was included in the study due to its association with overcrowded living conditions and its strong link to poverty.
The hypothesis of this study is that the spatio-temporal distribution of NTDs in the state of Pará exhibits heterogeneous patterns, with their presence and concentration potentially associated with socio-economic, environmental, and healthcare infrastructure factors.
Accordingly, the objective of this study was to analyse the spatio-temporal distribution of NTDs in the state, considering their occurrence over time and geographical dispersion, with the aim of identifying epidemiological patterns and possible associations with socio-environmental and structural factors.
2. Materials and Methods
2.1. Selected Diseases and Data
This is a cross-sectional, descriptive study covering all municipalities in the state of Pará and notifications of diseases from the period 2016 to 2022. The data on the diseases analysed—classified as notifiable—were obtained from Brazil’s Information System for Notifiable Diseases (SINAN), accessible via the website: http://portalsinan.saude.gov.br/doencas-e-agravos.
Information was collected on the following diseases: Tuberculosis (TB), Dengue, Leprosy, Cutaneous Leishmaniasis (CL), Visceral Leishmaniasis (VL), Acute Chagas Disease (ACD), and Schistosomiasis, considering the municipality of residence to construct the attribute table for statistical and Geographic Information System (GIS) analysis [9]
Based on the data obtained for each disease, annual incidence rates were calculated. These rates were then imported into QGIS 3.10 (A Coruña) and GeoDa 1.2 software to perform spatial correlation analyses, cluster detection, and significance testing, to determine spatial patterns and changes over the study period.
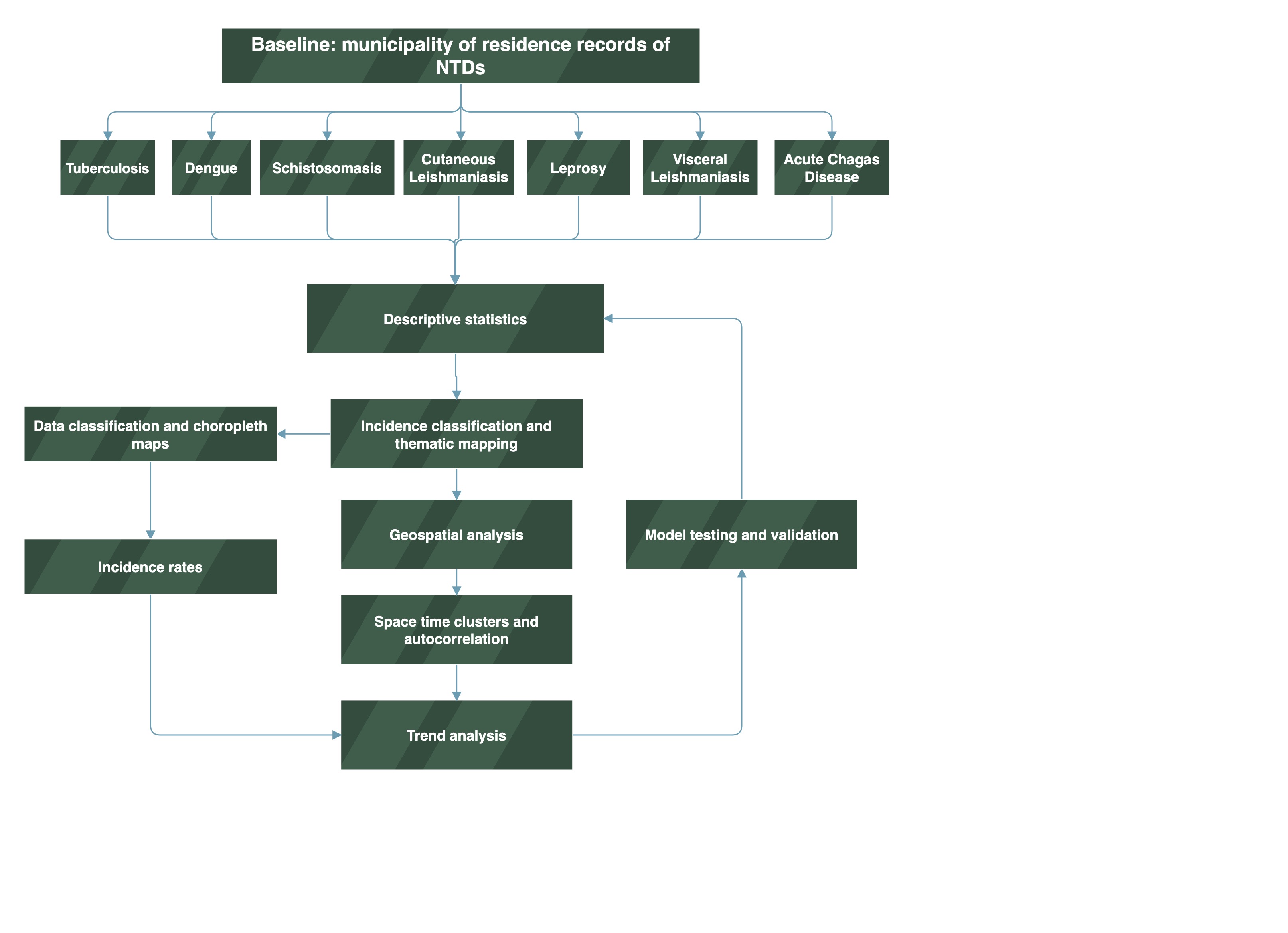
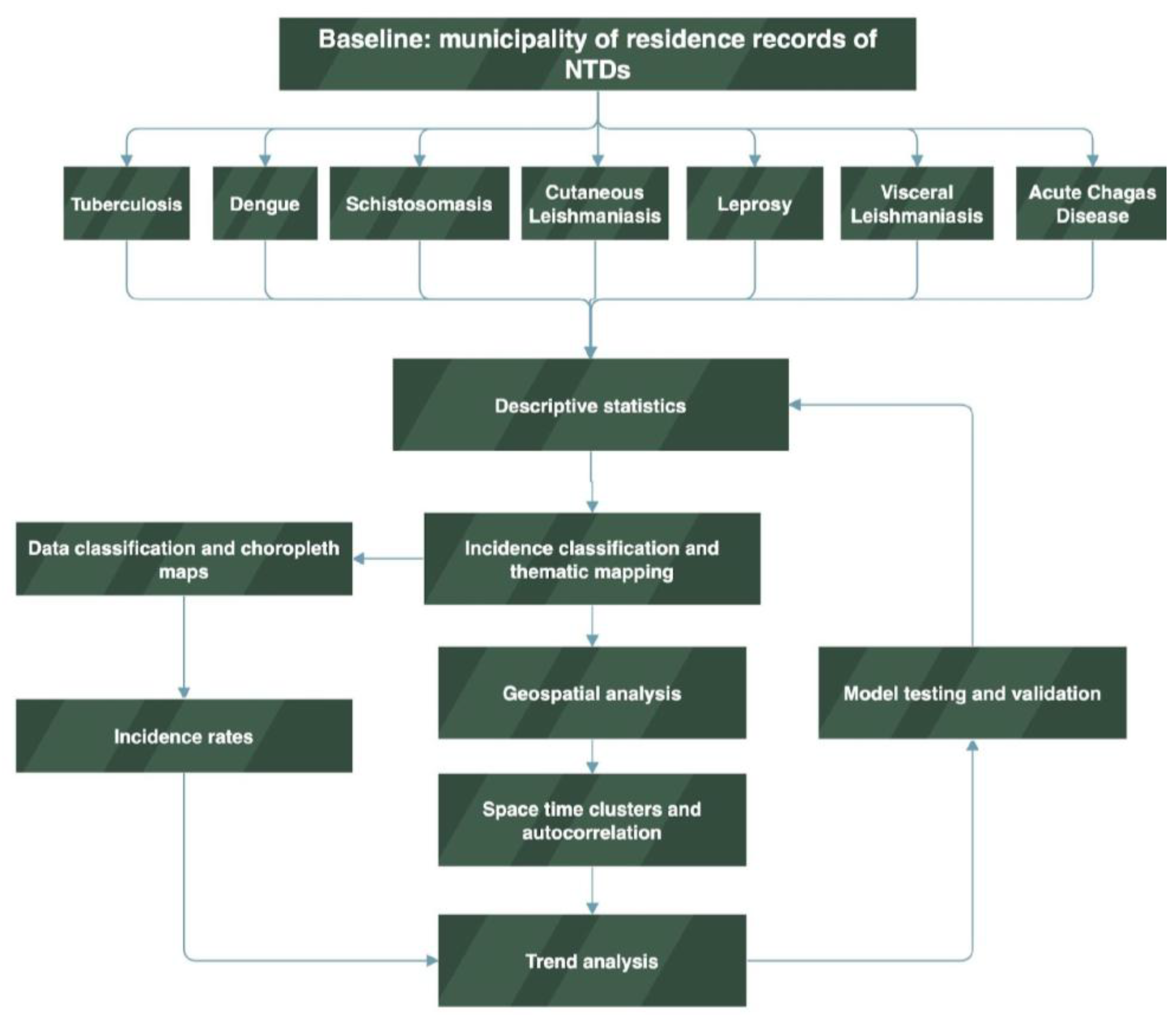
The methodology used in this study is summarised in the form of a flowchart. (Figure 1):
Figure 1.
Flowchart of the descriptive study and the initial collection of notification data; Data classification and choropleth maps, along with the organisation of data into categories and spatial representation by intensity; Incidence rates and the standardised calculation per population to allow comparisons between municipalities; Thematic mapping of case classification and the spatial visualisation of categorised data; Spatial analyses: in this study, we adopted spatial statistical methods of autocorrelation and space-time cluster detection; Trend verification; Repetition of the model with new parameters—this refers to the iterative process and adjustments to the final model. Source: prepared by the authors.
Figure 1.
Flowchart of the descriptive study and the initial collection of notification data; Data classification and choropleth maps, along with the organisation of data into categories and spatial representation by intensity; Incidence rates and the standardised calculation per population to allow comparisons between municipalities; Thematic mapping of case classification and the spatial visualisation of categorised data; Spatial analyses: in this study, we adopted spatial statistical methods of autocorrelation and space-time cluster detection; Trend verification; Repetition of the model with new parameters—this refers to the iterative process and adjustments to the final model. Source: prepared by the authors.
The study was structured into two complementary methodological steps. In the first step, mapping of the selected NTDs was carried out based on secondary sources of epidemiological data obtained from official health information systems.
In the second step, incidence rates, statistically significant clusters, and Moran’s I-LISA were calculated to analyse patterns of occurrence and identify areas of higher risk and co-location. For this purpose, spatial and geostatistical analysis techniques were employed, enabling a more robust understanding of the dynamics of NTDs in the region under study[10].
2.2. Incidence Rates and Statistical Analysis
The data were grouped by municipality of residence. The incidence rate was calculated by dividing the number of reported cases each year by the estimated number of residents in the municipality for the same year, then multiplying by 100,000 inhabitants. Population estimates available on the website of the Brazilian Institute of Geography and Statistics (IBGE) were used for each year in the series, as no demographic census was conducted during the study period (IBGE, 2023).
The incidence rates were used to generate graphs, cross-tabulations, and frequency tables. Additionally, the likelihood of two or more diseases occurring within the same municipality during the study period was calculated.
2.3. Mapping and Data Classification
Within the Geographic Information Systems (GIS) environment, thematic incidence maps were produced for each year of the historical series, as well as a map representing the average incidence rates over the analysed period. The incidence rates were classified using the natural breaks method (Jenks) [11].
Mapping was carried out using a GIS platform, which enabled the creation of choropleth maps, based on incidence rate values as a numerical attribute represented by graduated and ordered colours. Through the quantitative technique of legend scale homogenisation, coherent classification ranges were defined for the entire series, from 2016 to 2022.
2.4. Space-Time Clustering
To calculate spatial clusters, GeoDa software version 1.22, developed by the Center for Spatial Data Science at the University of Chicago, was used. The programme enables the identification of significant spatial patterns through Local Indicators of Spatial Association (LISA). The classification method used in the cluster maps was based on four categories: High-High: areas with high values surrounded by neighbours also with high values (hot spots); Low-Low: areas with low values surrounded by neighbours also with low values (cold spots); High-Low: areas with high values surrounded by neighbours with low values; Low-High: areas with low values surrounded by neighbours with high values.
In addition, the level of statistical significance was assessed, classifying areas into two categories: positive significance and negative significance. Positive significance indicates a tendency for spatial clustering of these diseases—i.e., areas where incidence is similar and geographically close. Conversely, negative significance indicates spatial dispersion, with low-incidence areas located near high-incidence areas. All data were analysed using a significance level of p = 0.05.
For each disease, a spatio-temporal cluster map, a corresponding significance map, and a scatterplot were generated. Based on the results of this mapping, a table and description of priority municipalities was compiled.
3. Results and Discussion
3.1. Geospatial Incidence of NTDs in Para State, 2016-2022
Spatio-temporal analysis has become an essential tool for understanding the dynamics of infectious diseases across different geographical contexts. This study on Neglected Tropical Diseases (NTDs) highlights distinct patterns of case concentration, influenced by environmental, climatic, and socio-economic factors.
Diseases such as Dengue, Cutaneous Leishmaniasis (CL), and Leprosy showed high standard deviations, indicating considerable variation in incidence across different locations or time periods. Diseases such as Tuberculosis (TB) and Schistosomiasis exhibited lower relative variation, suggesting a more uniform distribution (Table 1).

Table 1.
Incidence rates of NTDs in the state of Para.
| DTN | Incidence* (min) | Incidence* (max.) | Average | St. Dv. | Moran I |
|---|---|---|---|---|---|
| ACD | 1.90 | 342.50 | 172.20 | 240.84 | 0.645 |
| Dengue | 5.00 | 7,626.00 | 3,815.50 | 5,388.86 | 0.287 |
| VL | 2.95 | 818.00 | 410.48 | 576.32 | 0.312 |
| CL | 1.75 | 4,174.00 | 2,087.88 | 2,950.22 | 0.528 |
| Schistosomiasis | 0.46 | 3.40 | 1.93 | 2.07 | 0.018 |
| TB♦ | 12.50 | 31.19 | 21.85 | 13.21 | 0.206 |
| Leprosy | 26.00 | 2,386.00 | 1,206.00 | 1,668.00 | 0.228 |
Source: The authors – Adapted from the Notifiable Diseases Information System; Brazilian Institute of Geography and Statistics. *Incidence rates per 100,000 inhabitants. ♦ Tuberculosis was included due to poverty-related conditions.
In Table 2, the categorisation by clusters—High-High, Low-High, High-Low, and Low-Low—allows for the identification of high-risk areas, transitional zones, and regions of low incidence, contributing to a better understanding of the geographical distribution of diseases.
Dengue, VL, CL, Leprosy, TB, ACD, and Schistosomiasis all presented High-High clusters, indicating regions with high incidence surrounded by similarly affected areas. The southeast of Pará stands out as an epicentre for multiple diseases, particularly Dengue and Leishmaniasis. Since the 80s, sustainable dengue control in Brazil requires urban infrastructure improvements, technological innovation, and community engagement and Urbanization, poor sanitation, and high population density have created ideal conditions for Aedes aegypti proliferation[12]. The southeastern Pará, Brazil, urbanized rapidly due to migration, strategic river location, and extractive industries like rubber, nuts, and mining since the 20th century[13].
Leprosy and TB, diseases associated with poverty and urbanisation, showed concentration in the metropolitan region of Belém. Leprosy remains a public health concern in Tucuruí, with frequent cases among youth and working adults. Delayed diagnoses and disabilities highlight the need for education, early detection, and professional training[14].
Low-High clusters indicate municipalities with low incidence surrounded by areas of high incidence, suggesting epidemiological transition zones. Examples include the southeast of Pará for VL and Dengue, and the northeast for TB.
Low-Low clusters represent low-risk areas, encompassing municipalities and neighbouring regions with low incidence rates. These cover a large portion of Pará’s mesoregions, including the metropolitan region of Belém and the Baixo Amazonas. Some municipalities—such as Bagre, Bragança, Mãe do Rio, Redenção, Santa Izabel do Pará, São Sebastião da Boa Vista, and Vigia—did not present significant data, which may indicate absence of cases, underreporting, or limitations in data collection.
Table 2.
Municipalities that showed clusters and statistical significance for the incidence of Neglected Tropical Diseases (NTDs) in the state of Pará between 2016 and 2022.
Table 2.
Municipalities that showed clusters and statistical significance for the incidence of Neglected Tropical Diseases (NTDs) in the state of Pará between 2016 and 2022.
| Clusters | Dengue | Visceral Leishmaniasis | Cutaneous leishmaniasis | Leprosy | Tubersulosis♦ | Acute Chagas Disease | Schistosomiasis |
|---|---|---|---|---|---|---|---|
| High - High | 12 municipalities: SoutheastofPará | 10 municipalities: Southeast of Pará | 13 municipalities: Baixo amazonas | 7 municipalities: Southeast of Pará | 8 municipalities: Metropolitan of Belém | 13 municipalities: Metropolitan of Belém | 3 municipalities: Southeast of Pará |
| Low - High | 6 municipalities: Southeast e Southwestern of Pará | 3 municipalities: Southeast of Pará | 2 municipalities: Southeast of Pará | 5 municipalities: Southeast of Pará e Metropolitan of Belém | 3 municipalities: Nordeste paraense | Afua, Mocajuba, Ponta Pedras | 8 municipalities: Southeast of Pará |
| Low - Low | 28 municipalities: região Metropolitan of Belém. | 24 municipalities: Southwestern of Pará e baixo Amazonas | 50 municipalities: all mesoregions | 35 municipalities: all mesoregions | municipalities: Southeast of Pará | 8 municipalities: Southeast e Southwestern of Pará | 7 municipalities: Southeast of Pará |
| High - Low | inhagapi | Garrafão do Norte | NOT REPORTED | NOT REPORTED | Breves, Marabá, Redenção, Santa Cruz of Arari, Santarém, Tucuruí | NOT REPORTED | Bagre, Bragança, Mãe do Rio, Redenção, Santa Izabel of Pará, São Sebastião da Boa Vista, Vigia |
| P value | Dengue | Visceral Leishmaniasis | Cutaneous leishmaniasis | Leprosy | Tubersulosis | Acute Chagas Disease | Schistosomiasis |
| 0.05 | 36 municipalities | 32 municipalities | 31 municipalities | 39 municipalities | 19 municipalities | 38 municipalities | 10 municipalities |
| 0.01 | 14 municipalities | Santarém, São Geraldo do Araguaia, Piçarra, Xinguara, Iguarape Asul, Castanhal, Bannach, Breves | 21 municipalities | 10 municipalities | Inhangapi, Marabá, Piçarra, Portel, Xinguara | 9 municipalities | Parauapebas, Dom Eliseu |
| 0.001 | Anajás,Bagre, Breves, Redenção, Rio Maria | Garrafão do Norte, Floresta do Araguaia, Curionópolis | 15 municipalities | Santarém | Benevides, Breves, Santa Bárbara do Pará, Santo Antônio do Tauá | Santarém | Bragança, Mãe do Rio, Redenção, Santa Izabel do Pará, São Sebastião da Boa Vista, Vigia, Bagre |
Source: The authors – Adapted from the Notifiable Diseases Information System; Brazilian Institute of Geography and Statistics. ♦ Tuberculosis was included due to poverty-related conditions.
Through geospatial analysis, it was possible to identify areas with high incidence rates, as shown in the map (Figure 2), highlighting both high and low incidence areas for each of the diseases. This spatial information supports the understanding of the factors influencing the spread of Neglected Tropical Diseases (NTDs), such as the socio-economic, geographical, and environmental characteristics of different regions within the state of Pará.
The NTDs considered transitory include Dengue, ACD, Schistosomiasis, Leprosy, CL and VL. Previous studies that have conducted joint mapping of multiple diseases emphasise the importance of geographical space as a strategic unit for the development of public policies and decision-making in health, particularly in the context of multi-disease burdens [4,15,16].
Using the analytical method applied to identify areas with high NTD incidence within the state of Pará, it was observed that many of these diseases exhibit distinct concentration patterns, which can guide further studies aimed at reducing their impact on the health of the population in Pará. Moreover, the spatial analysis of incidence rates over the years 2016 to 2020 revealed trends and temporal variations in the occurrence of NTDs.
Figure 2.
Spatial Distribution of Neglected Tropical Disease Incidence Rates in Pará, Brazil (2016–2022). Source: The authors – Adapted from the Notifiable Diseases Information System; Brazilian Institute of Geography and Statistics.
Figure 2.
Spatial Distribution of Neglected Tropical Disease Incidence Rates in Pará, Brazil (2016–2022). Source: The authors – Adapted from the Notifiable Diseases Information System; Brazilian Institute of Geography and Statistics.
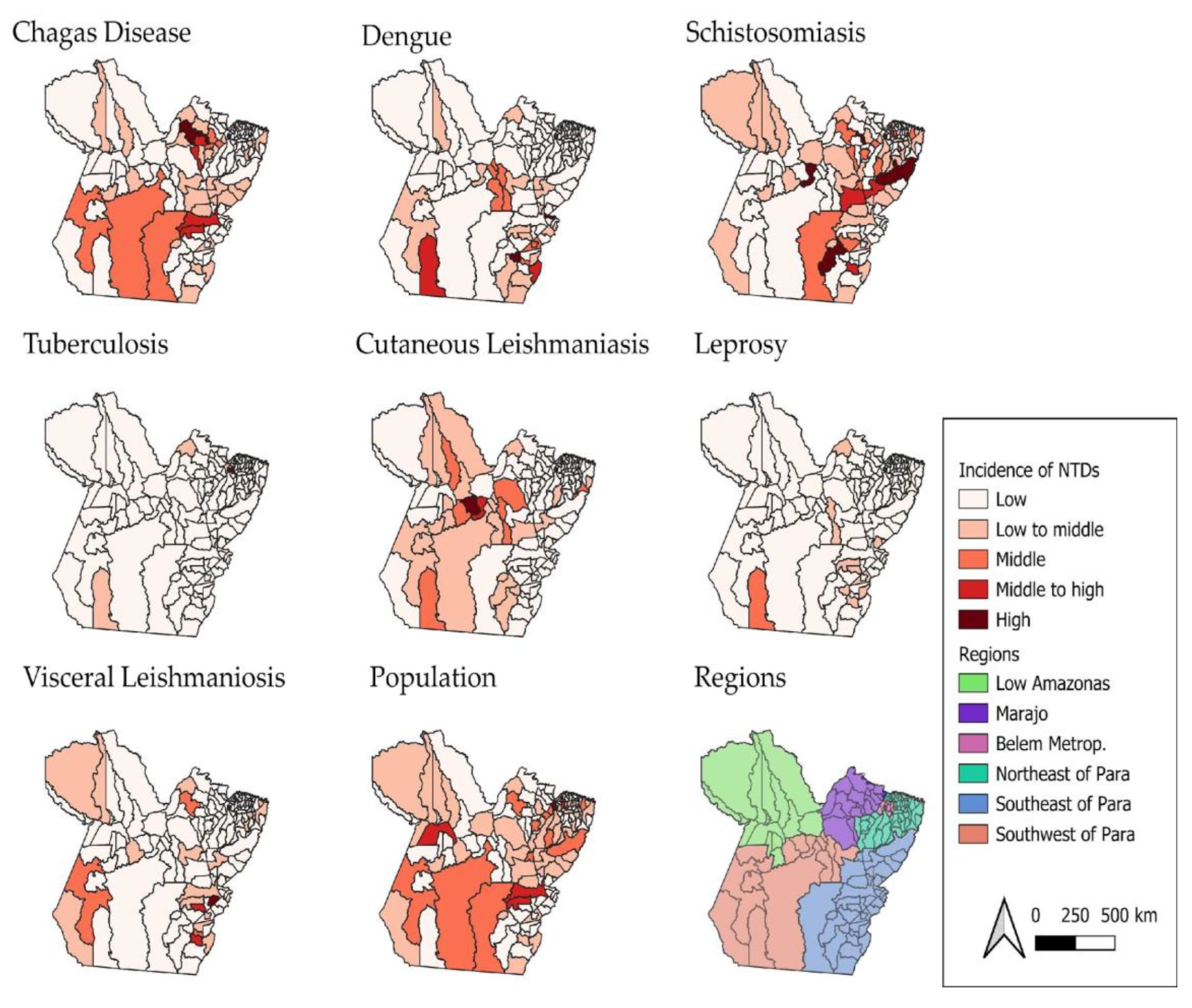
Figure 2 shows that the incidence rates of Neglected Tropical Diseases (NTDs) in the state of Pará vary from one disease to another. Acute Chagas disease (ACD) has a higher concentration of cases in the Metropolitan Region of Belém. This indicates that the area has a significant number of recorded cases of this disease compared to other regions of the state.
Regarding dengue, higher concentrations of cases were observed in the western and southern regions of the state, suggesting that these areas present environmental and urban conditions conducive to the proliferation of the Aedes aegypti vector. The high incidence may be associated with unplanned urbanisation, poor sanitation, and high population density in regional urban centres. Other studies highlighted that dengue in Pará peaks during the rainy season and climate-sensitive transmission demands targeted interventions in high-risk municipalities[17]. Also, the disease epidemics in Brazil follow seasonal traveling waves, typically starting in northwestern states like Acre and Rondônia, then moving eastward to coastal and northeastern regions[18].
Acute Chagas disease (ACD) stood out in High-High clusters in the Metropolitan Region of Belém and in southeastern Pará, respectively. Other study, when analyzing 696 cases of ACD from 2007 to 2015 in Belém, Abaetetuba and Breves, found that Belém alone accounted for 40.66% of reported cases, suggesting a shift from traditional rural transmission to urban outbreaks, likely driven by oral transmission, which accounted for 82.33% of cases[19].
For schistosomiasis, cases are mainly concentrated in the southern and southeastern municipalities of Pará—regions characterised by riverside areas and poor sanitation conditions. The presence of contaminated water bodies and the population’s frequent exposure to these environments favour the maintenance of the disease’s transmission cycle [20]. In this study, although detailed schistosomiasis data were less prominent in the sources, southeastern Pará is known for persistent endemic transmission, especially in rural and peri-urban communities with poor sanitation. In schistosomiasis cases, one remarkable characteristic of Pará state is that is not as prominent as the Northeast and Southeast of Brazil, indicating localized outbreaks or probable underreported endemicity[21].
Tuberculosis (TB), on the other hand, has the city of Belém as its main focus, showing the highest incidence rates. This pattern may be related to high population density, social vulnerability, and the concentration of at-risk populations, such as residents of peripheral areas and people deprived of liberty. It may also reflect a higher rate of case reporting compared to other municipalities in the state. TB remains a major public health challenge in Pará, showing regional disparities require tailored interventions and strengthening local health systems and addressing socioeconomic inequalitiesmesore[22]. In Tucurui area, a study highlighted that young, low-educated males are most affected and pulmonary TB was predominantly reported[23].
Although cases of cutaneous leishmaniasis (CL) have been recorded in various regions of the state, the highest concentration was identified in the Lower Amazon region. This area, with vast forest zones and extractive activities, facilitates human contact with disease vectors, especially in rural and riverside communities[24]. In Brazil, ACL incidence varies significantly across space and time, influenced by environmental conditions and rural settings contribute to this variability[25].
Regarding leprosy, although it does not present the highest absolute number of cases, it is distributed across many municipalities, with Altamira standing out. This indicates a wide territorial dispersion of the disease, even with moderate incidence, which reinforces the need for active surveillance and early diagnosis strategies. This study found the Belém Metropolitan Area emerging as the most prominent transmission zone, with statistically significant clusters, highlighting the need for targeted surveillance and intervention strategies in urban centers (Figure 2). Other study between 2019 and 2023 showed that Pará reported 12,231 leprosy cases, with 2019 having the highest count (3,554). Marituba, with a specialized treatment center, accounted for 13.4% of cases, followed by Belem and Parauapebas [26].
The highest incidences of visceral leishmaniasis (VL) were recorded in the region known as South and Southeast Pará—areas that historically present favourable conditions for disease transmission, such as the presence of vectors, animal reservoirs, and social vulnerabilities that hinder access to healthcare services and vector control. In the case of VL in the Amazonian cities, the presence of open peridomestic yards increases the contact vector-host and these behaviors, especially with dogs contributed to the spread of Leishmania chagasi[27]. Understanding sandfly communication helps explain spatial patterns of infection and can inform vector control strategies.
It is worth noting that the southeastern region of the state of Pará stands out as an area with a high epidemiological burden for four major Neglected Tropical Diseases (NTDs): dengue, schistosomiasis, VL, and leprosy (see Figure 2). This pattern of concentration may be attributed to a combination of environmental, socioeconomic, and structural factors.
The Marajó region presented a very specific pattern of ACD (acute Chagas disease) incidence throughout the study period. This can be explained by the strong association with oral transmission of the etiological agent (Trypanosoma cruzi), particularly through the consumption of contaminated food such as açaí, as this region is a major producer. Additionally, Marajó has geographical and socioeconomic characteristics conducive to the spread of the disease, such as relative isolation, low sanitation coverage, and challenges in sanitary inspection[28].
Dengue and visceral leishmaniasis (VL) showed greater territorial spread compared to other diseases, affecting a wide range of regions across the state. The former is classically associated with unplanned urbanisation, which facilitates the proliferation of Aedes aegypti; deficiencies in basic sanitation; and high population mobility, which reintroduces susceptible individuals to new serotypes[12]. The latter has a different profile, linked to deforestation and environmental degradation, agricultural expansion and mining, and recent spatial transformations in land use, which ultimately promote contact between humans, sandflies, and wild and/or domestic reservoir [29].
Dengue and CL had the highest number of municipalities classified as High-High, indicating strong spatial concentration. CL also had the highest number of municipalities in Low-Low, suggesting large areas with low incidence. Leprosy and tuberculosis showed more distributed patterns, with presence across multiple types of clusters.
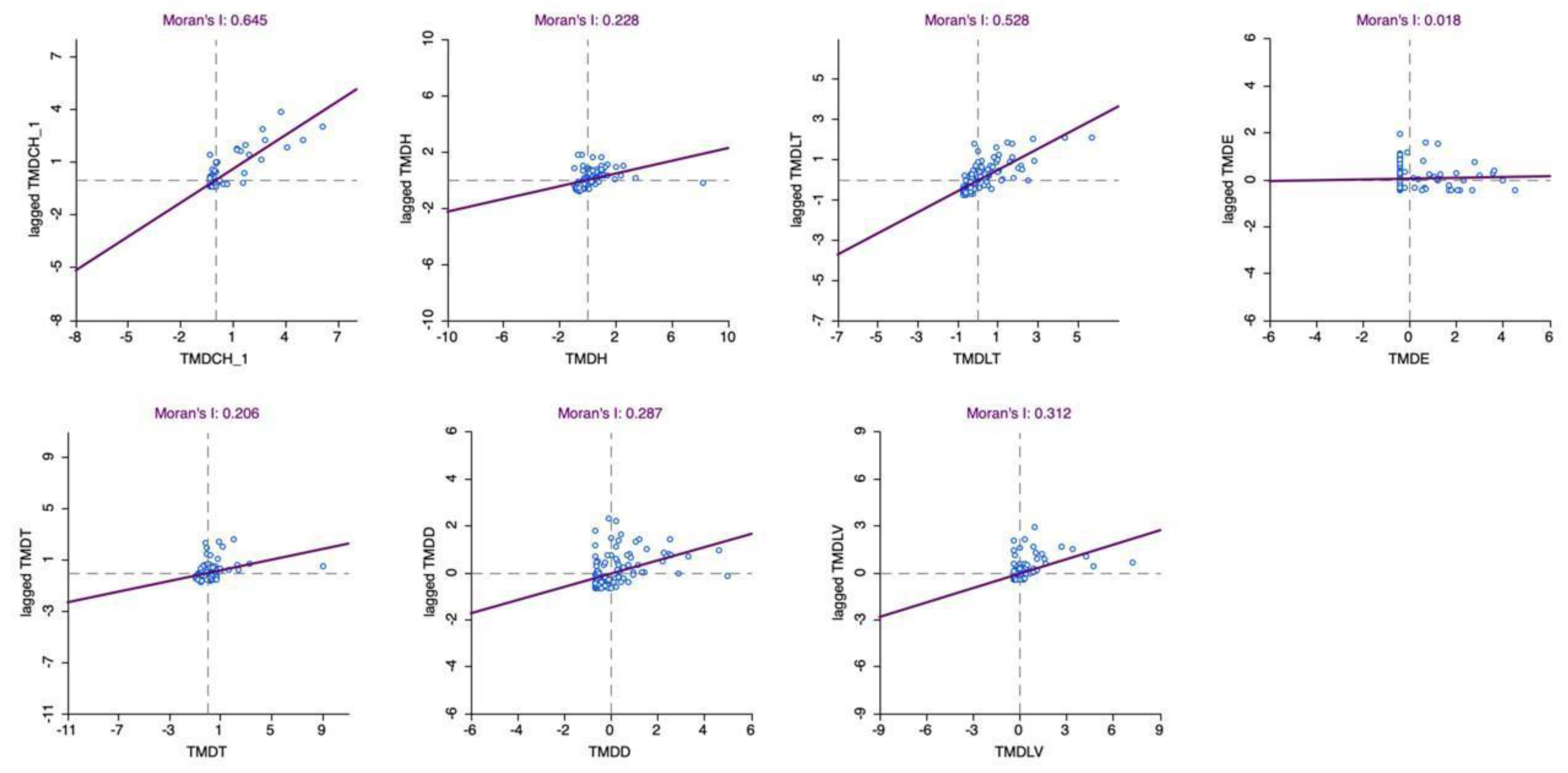
The analysis of statistical significance in the spatial distribution using the Moran’s I LISA index, applied to the average incidence of NTDs in the state of Pará between 2016 and 2022, enabled the identification of statistically significant spatial autocorrelation patterns (Table 1). Through the detection of local clusters, it was possible to identify areas with high concentrations of cases (High-High), as well as regions with low incidence (Low-Low), revealing critical and priority zones for public health intervention.
When analysing the map (Figure 3) showing the significance level of the Moran’s I LISA distribution, it is possible to observe areas where the incidence of NTDs presents either positive or negative spatial significance. Darker areas on the map indicate regions of positive significance, that is, where high incidence rates occur in neighbouring regions. Conversely, lighter areas represent regions of negative significance, indicating a dispersion of NTD cases—areas of low incidence located near those with high incidence.
Figure 3.
Spatial Distribution of Moran’s I LISA Significance Levels for the Average Incidence of Neglected Tropical Diseases in Pará, Brazil (2016–2022). Source: Notifiable Diseases Information System; Brazilian Institute of Geography and Statistics. Legend: The maps represent statistical significance based on the incidence rates of acute Chagas disease, dengue, leprosy, cutaneous leishmaniasis, visceral leishmaniasis, schistosomiasis, and tuberculosis. The areas were classified into three categories: “Not significant”, “Low significance”, and “High significance”, according to the green colour scale. All data were considered at a significant level of p = 0.05.
Figure 3.
Spatial Distribution of Moran’s I LISA Significance Levels for the Average Incidence of Neglected Tropical Diseases in Pará, Brazil (2016–2022). Source: Notifiable Diseases Information System; Brazilian Institute of Geography and Statistics. Legend: The maps represent statistical significance based on the incidence rates of acute Chagas disease, dengue, leprosy, cutaneous leishmaniasis, visceral leishmaniasis, schistosomiasis, and tuberculosis. The areas were classified into three categories: “Not significant”, “Low significance”, and “High significance”, according to the green colour scale. All data were considered at a significant level of p = 0.05.
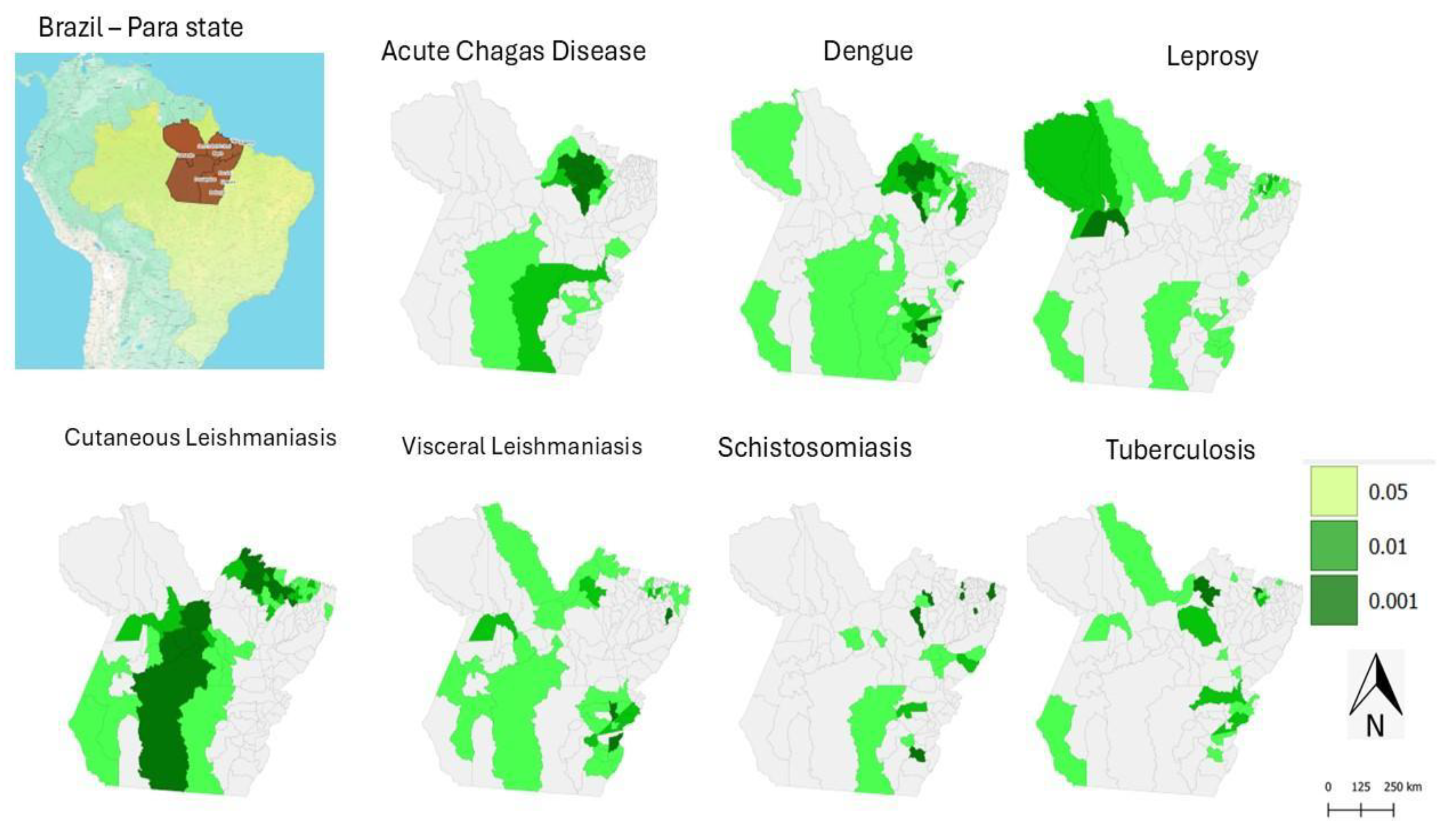
Therefore, this distribution highlights the regions in the state of Pará where the incidence of NTDs shows a significant pattern of spatial organisation. These areas may indicate the presence of common risk factors or environmental characteristics that favour the persistence of these diseases. It is important to emphasise that the interpretation of results from this method should consider other factors, such as demographic characteristics, socioeconomic conditions, the presence of vectors, and public health policies. These additional elements can help in understanding the observed spatial patterns and in guiding strategies for the prevention and control of NTDs in Pará.
Through geospatial analysis, it was possible to identify areas with high incidence rates for different NTDs, as illustrated in the maps (Figure 2). For example, dengue showed a high concentration pattern (High-High cluster) in 12 municipalities in southeastern Pará, while cutaneous leishmaniasis (CL) had a wide dispersion, with 13 municipalities of high local incidence mainly located in the Lower Amazon region.
In contrast, leprosy and tuberculosis displayed distinct patterns: leprosy was concentrated in 7 municipalities in the southeast, while tuberculosis had higher incidence in the Metropolitan Region of Belém, with 8 municipalities classified as High-High. Acute Chagas disease and schistosomiasis showed more localised patterns, with emphasis on the Metropolitan Region of Belém and the southeast of the state, respectively.
When jointly analysing the maps in Figure 2 and Figure 3, it becomes evident that some diseases, such as dengue and CL, have a greater capacity for territorial spread, while others, such as ACD, tend to occur in more restricted clusters. These spatial insights are essential for understanding the factors influencing the spread of NTDs, such as the socioeconomic, geographic, and environmental characteristics of different regions in Pará. Moreover, they enable the identification of priority areas for intervention, contributing to the planning of more effective surveillance and control actions.
Figure 4: Maps of the state of Pará showing the spatial clustering of acute Chagas disease, dengue, leprosy, cutaneous leishmaniasis, visceral leishmaniasis, schistosomiasis, and tuberculosis, measured by the categories High-High, representing neighbourhoods with high values (Hot Spot); Low-Low, representing neighbourhoods with low values (Cold Spot). Additionally, High-Low indicates a hot spot surrounded by low values, and Low-High represents a cold spot surrounded by high values. Source: The authors – Adapted from the Notifiable Diseases Information System; Brazilian Institute of Geography and Statistics.
Figure 4.
Municipal-level Spatial Clustering of Neglected Tropical Diseases in Pará, Brazil, Based on Local Indicators of Spatial Association (Anselin Local Moran’s I), 2016–2022.
Figure 4.
Municipal-level Spatial Clustering of Neglected Tropical Diseases in Pará, Brazil, Based on Local Indicators of Spatial Association (Anselin Local Moran’s I), 2016–2022.
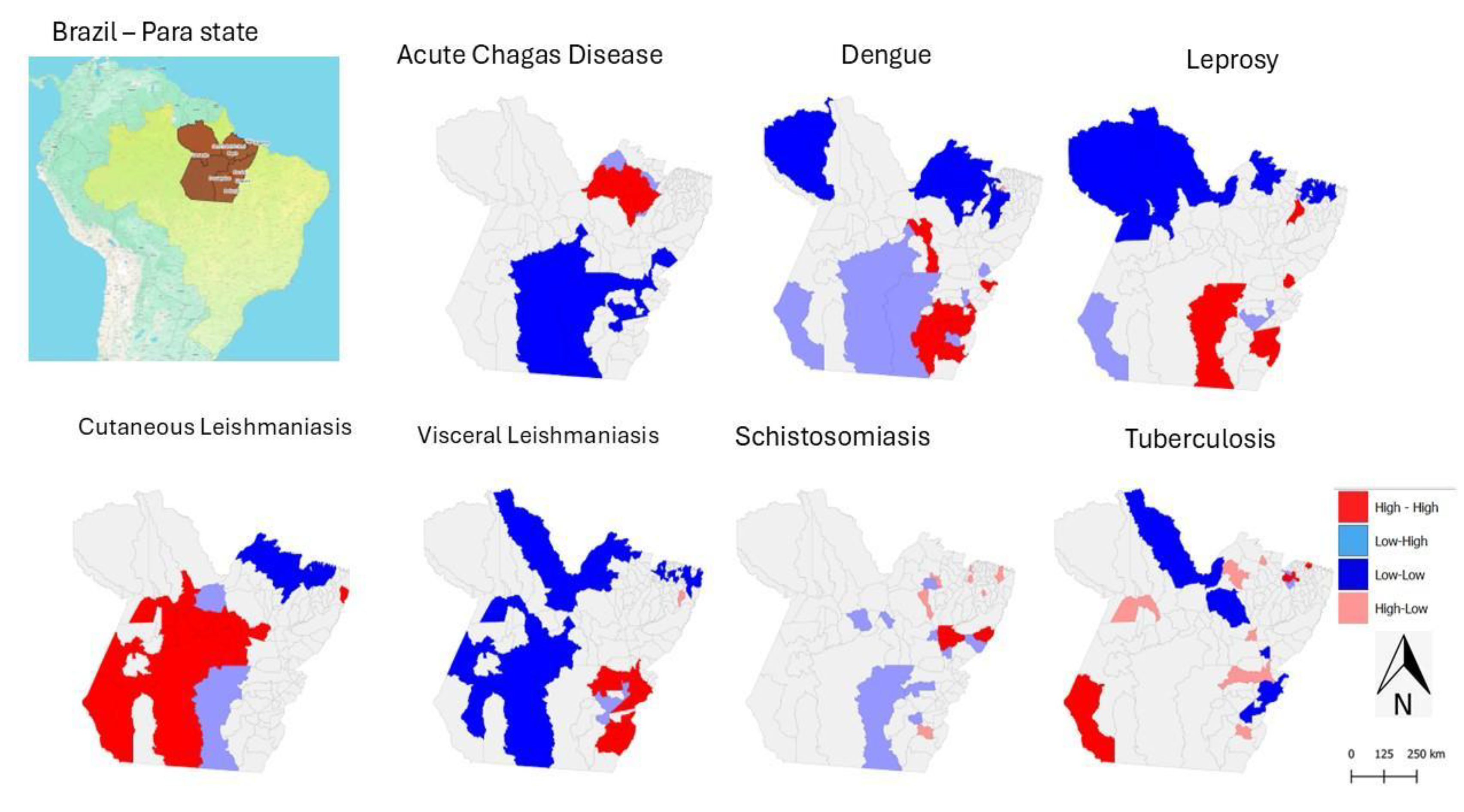
The maps in Figure 4 provide strategic information for identifying priority areas for intervention, as they show a high concentration of multiple diseases (High-High) or the simultaneous presence of diseases in different critical clusters.
In this context, southeastern Pará is a priority region due to the high incidence of dengue, visceral leishmaniasis (VL), leprosy, acute Chagas disease (ACD), and schistosomiasis. Municipalities such as Redenção, Marabá, Xinguara, Parauapebas, and Rio Maria appear in multiple significant clusters (p < 0.01 or p < 0.001) (Figure 5).
Figure 5.
Scatterplot of Neglected Tropical Diseases Incidence in Pará, Brazil (2016–2022). Source: The authors – Adapted from the Notifiable Diseases Information System; Brazilian Institute of Geography and Statistics.
Figure 5.
Scatterplot of Neglected Tropical Diseases Incidence in Pará, Brazil (2016–2022). Source: The authors – Adapted from the Notifiable Diseases Information System; Brazilian Institute of Geography and Statistics.
3.2. Targeted areas for intervention to NTDs in Para state
Based on the data analysed, it was possible to carry out a synthesis exercise that highlighted priority areas for multi-disease intervention, revealing territories with overlapping incidence of different Neglected Tropical Diseases (NTDs) and, therefore, greater epidemiological vulnerability. In the Lower Amazon, a high concentration of cutaneous leishmaniasis (CL) was observed. Municipalities such as Santarém stood out in High-High clusters with statistical significance (p < 0.001).
In the Metropolitan Region of Belém, there was a high incidence of tuberculosis (TB) and acute Chagas disease (ACD). Municipalities such as Santa Izabel do Pará, Bagre, Vigia, and Bragança appeared in critical clusters.
Each graph displays Moran’s I index, indicating the degree of spatial association between observed values and their neighbours. The axes represent the values of the variables (e.g., ACD, leprosy, CL, schistosomiasis, TB, dengue, and visceral leishmaniasis) and their respective lagged values.
A relevant aspect of NTDs in the state of Pará is the marked difference compared to the national pattern. For example, between 2000 and 2019, the highest burden of mortality from NTDs in Brazil was concentrated in the Central-West, particularly due to Chagas disease and schistosomiasis, with hotspots in Goiás, Minas Gerais, Bahia, Tocantins, and Piauí. Notably, the North region, including Pará, is rarely mentioned in these national studies, which may reflect limitations in data coverage or the scale of analysis[30].
This issue of scale is crucial: when Pará is analysed in isolation, distinct epidemiological patterns emerge that are not evident in national-level analyses. For example, Southeast Pará shows a high burden of dengue, schistosomiasis, visceral leishmaniasis, and leprosy (see Figure 2).
Furthermore, according to the Global Burden of Disease Study (GBD 2016), the profile of NTDs in Brazil underwent significant changes between 1990 and 2016, with a reduction in some diseases and the emergence of others. However, data from Pará suggest a coexistence of diseases associated with the older profile (such as leprosy and schistosomiasis) and emerging diseases (such as dengue and leishmaniasis), indicating an incomplete process of epidemiological transition.
4. Conclusions
The spatio-temporal analysis of Neglected Tropical Diseases (NTDs) in the state of Pará from 2016 to 2022 revealed distinct patterns in the distribution and progression of these illnesses. The Metropolitan Region of Belém stood out as a priority area for acute Chagas disease and tuberculosis, while the western and southern regions showed a higher concentration of dengue cases. Urban schistosomiasis was more prevalent in the southern and southeastern regions, and cutaneous leishmaniasis predominated in the Lower Amazon. Although visceral leishmaniasis had a lower absolute number of cases, it was more frequent in the southern and southeastern regions of the state.
These findings underscore the importance of considering the geographical distribution of NTDs, in addition to their incidence, when planning public health actions. The spatio-temporal approach proved to be an effective tool for identifying critical areas and guiding resource allocation, contributing to more targeted strategies for prevention, control, and treatment.
Additionally, the results highlight the significant influence of socio-environmental factors in the spread of NTDs, such as housing conditions, basic sanitation, and access to healthcare services. These findings support the need for intersectoral and place-based public policies that integrate social, environmental, and structural aspects into strategies to tackle these diseases.
It is worth noting that spatio-temporal surveillance should be continuous and adaptive, incorporating new data and analytical methodologies. Future research should aim to expand these analyses by including additional variables that allow for a more comprehensive understanding of the determinants of NTDs and support the formulation of more effective and sustainable public policies.
Author Contributions
Conceptualisation, data curation, formal analysis, funding acquisition – ESF and JALL. Conceptualisation, data curation, formal analysis – PPLM, FOS, SSS, SR, and SS. Conceptualisation, formal analysis – LMA and RKR. Writing, review, and editing – All authors.
Funding
The authors would like to thank the Federal University of Southern and Southeastern Pará (UNIFESSPA), the project entitled “Use of Geoprocessing for Public Health in Southern and Southeastern Pará”, under CALL 06/2023-PROEG – General Monitoring Programme (PMG 2023), and CALL PROPIT No. 02/2022 – PIBIC/PNAES.
Institutional Review Board Statement
The study did not require ethical approval, as it was conducted using archival data from official sources.
Informed Consent Statement
The study did not require informed consent from subjects, as it was conducted using archival data from official sources.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| NTDs | Neglected Tropical Diseases |
| FHS | Family Health Strategy |
| HDI | Human Development Index |
| ISND | Information System for Notifiable Diseases |
| TB | Tuberculosis |
| CL | Cutaneous Leishmaniasis |
| VL | Visceral Leishmaniasis |
| ACD | Acute Chagas Disease |
| GIS | Geographic Information System |
References
- Hotez, P. A New Voice for the Poor. PLoS Negl Trop Dis. 2007, 1, e77. [Google Scholar] [CrossRef]
- Hotez, P.J. Neglected infections of poverty in the United States of America. PLoS Negl Trop Dis. 2008, 2. [Google Scholar] [CrossRef] [PubMed]
- Brooker, S.; Utzinger, J. Integrated disease mapping in a polyparasitic world. Geospat Health. 2007. [CrossRef] [PubMed]
- Booth, M.; Clements, A. Neglected Tropical Disease Control – The Case for Adaptive, Location-specific Solutions. Trends Parasitol. 2018, xx, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Hotez, P.J.; Fujiwara, R.T. Brazil’s neglected tropical diseases: an overview and a report card. Microbes and infection / Institut Pasteur [Internet]. 2014, 16, 601–6. [Google Scholar] [CrossRef]
- Martins-Melo, F.R.; Carneiro, M.; Ramos, A.N.; Heukelbach, J.; Ribeiro, A.L.P.; Werneck, G.L. The burden of Neglected Tropical Diseases in Brazil, 1990-2016: A subnational analysis from the Global Burden of Disease Study 2016. PLoS Negl Trop Dis. 2018, 12. [Google Scholar] [CrossRef]
- Martins-Melo, F.R.; Ramos, A.N.; Alencar, C.H.; Heukelbach, J. Trends and spatial patterns of mortality related to neglected tropical diseases in Brazil. Parasite Epidemiol Control. 2016, 1, 56–65. [Google Scholar] [CrossRef]
- Lindoso, J.A.L.; Lindoso, A.A.B.P. Neglected tropical diseases in Brazil. Rev Inst Med Trop Sao Paulo [Internet]. 2009, 51, 247–53. [Google Scholar] [CrossRef]
- IBGE Pesquisa de Informações Básicas Estaduais Pesquisa de Informações Básicas Municipais. 2021. 103p.
- Anselin, L. Local Indicators of Spatial Association-LISA. Geogr Anal. 2010, 27, 93–115. [Google Scholar] [CrossRef]
- Davenhall, B. Helping Shape Global Health. Esri Health and Human Services. 2010, 1. [Google Scholar]
- GTeixeira, C.M.; Glória Teixeira, M.; da Conceição Costa, M.N.; Barreto, F.; Lima Barreto, M. Dengue: twenty-fi ve years since reemergence in Brazil Dengue: vinte e cinco anos da reemergência no Brasil [Internet]. 2009. Available from: http://w3.datasus.gov.br/siasih/siasih.php,.
- Silva Sde, S. Production of urban space in Marabá (PA): trajectories and processes. Geopauta. 2022, 6, e10094. [Google Scholar] [CrossRef]
- Silva, D.R.X.; Ignotti, E.; Souza-Santos, R.; Hacon Sde, S. Hanseníase, condições sociais e desmatamento na Amazônia brasileira. Revista Panamericana de Salud Pública. 2010, 27, 268–75. [Google Scholar] [CrossRef]
- Brooker, S.; Utzinger, J. Integrated disease mapping in a polyparasitic world. Geospat Health. 2007, 1, 141–6. [Google Scholar] [CrossRef] [PubMed]
- Titosse, A.C.; Fonseca Eda, S.; Rodrigues, M.V.P.; Ramos, A.P.M.; Giuffrida, R.; Arana, A.R.A. Distribuição espacial das doenças tropicais negligenciadas na região oeste do estado de São Paulo. Caminhos de Geografia. 2020, 12–26. [Google Scholar]
- Serra, E.M.F.; Ferreira DBda, S.; Silva Jr Jde, A.; Moraes BCde Lima AMMde Silva BCSda et, a.l. Mapping the Incidence of Dengue Fever in the State of Pará, Eastern Amazon: Epidemiology and Relationships with Climate. Reports. 2025, 8, 61. [Google Scholar] [CrossRef] [PubMed]
- Churakov, M.; Villabona-Arenas, C.J.; Kraemer, M.U.G.; Salje, H.; Cauchemez, S. Spatio-temporal dynamics of dengue in Brazil: Seasonal travelling waves and determinants of regional synchrony. PLoS Negl Trop Dis. 2019, 13. [Google Scholar] [CrossRef]
- Vilhena AOde Pereira, W.M.M.; Oliveira SSde Fonseca, P.F.L.; Ferreira, M.S.; Oliveira TNda, C.; et al. Doença de Chagas aguda no estado do Pará, Brasil: série histórica de aspectos clínicos e epidemiológico em três municípios, no período de 2007 a 2015. Rev Panamazonica Saude. 2020, 11. [Google Scholar]
- Katz, N.; Peixoto, S.V. Análise crítica da estimativa do número de portadores de esquistossomose mansoni no Brasil. Revista de Sociedade Brasileira de Medicina Tropical. 2000, 3, 303–8. [Google Scholar] [CrossRef]
- Cardoso, D.T.; Magalhães, F.D.C.; Enk, M.J.; Geiger, S.M.; Barbosa, D.S. Challenges to Schistosomiasis Control Program in Brazil: setbacks in the control program and critical analysis of the disease notification. Rev Soc Bras Med Trop. 2024, 57. [Google Scholar] [CrossRef]
- Marcos, W.; Lobato Dda, C.; Garcez, J.C.D.; Sardinha, D.M.; Marinho, R.L.; Júnior, A.M.D.F.; et al. Profile of Tuberculosis Deaths by Mesoregion in the State of Pará from 2012 to 2022: An Ecological Study. J Adv Med Med Res. 2025, 37, 104–18. [Google Scholar] [CrossRef]
- Sousa Júnior CPde Oliveira EMde Marques VGPda, S.; Castro ASde Aguiar LCde Bizari, L.; et al. Análise epidemiológica dos casos de tuberculose na Região de Integração do Lago de Tucuruí – PA. Research, Society and Development. 2021, 10, e50510615916. [Google Scholar]
- Bensabath, G. Espaço-tempo no processo da saúde na Amazônia brasileira. Rev Panamazonica Saude. 2014, 5, 9–10. [Google Scholar] [CrossRef]
- Machado-Coelho, G.L.; Assunção, R.; Mayrink, W.; Caiaffa, W.T. American cutaneous leishmaniasis in Southeast Brazil: space-time clustering. Int J Epidemiol. 1999, 28, 982–9. [Google Scholar] [CrossRef]
- Barbosa, M.V.L.; Campêlo, C.B.; Vasconcellos, D.M.; Menin, G.A.W.; Neto, J.O.O.; Santos MVdos et, a.l. Epidemiological Profile of Leprosy in the State of Pará between the Years 2019 and 2023. J Adv Med Med Res. 2025, 37, 139–49. [Google Scholar] [CrossRef]
- Dye, C.; Davies, C.R.; Lainson, R. Communication among phlebotomine sandflies: a field study of domesticated Lutzomyia longipalpis populations in Amazonian Brazil. Anim Behav. 1991, 42, 183–92. [Google Scholar] [CrossRef]
- Nóbrega, A.A.; Garcia, M.H.; Tatto, E.; Obara, M.T.; Costa, E.; Sobel, J.; et al. Oral transmission of chagas disease by consumption of Açaí palm fruit, Brazil. Emerg Infect Dis. 2009, 15, 653–5. [Google Scholar] [CrossRef] [PubMed]
- Profeta da Luz, Z.M.; Pimenta, D.N.; Cabral, A.L.; Fiúza, V.O.; Rabello, A. A urbanização das leishmanioses e a baixa resolutividade diagnóstica em municípios da Região Metropolitana de Belo Horizonte. Rev Soc Bras Med Trop. 2001, 34, 249–54. [Google Scholar]
- Trindade Bezerra, J.M.; Etelvina, V.; De Araú Jo, M.; Soeiro Barbosa, D.; Rogerlândio Martins-Melo, F.; Werneck, G.L.; et al. Burden of leishmaniasis in Brazil and federated units, 1990-2016: Findings from Global Burden of Disease Study 2016. PLoS Negl Trop Dis. 2018, 12, 1–19. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



