Submitted:
17 September 2025
Posted:
18 September 2025
You are already at the latest version
Abstract
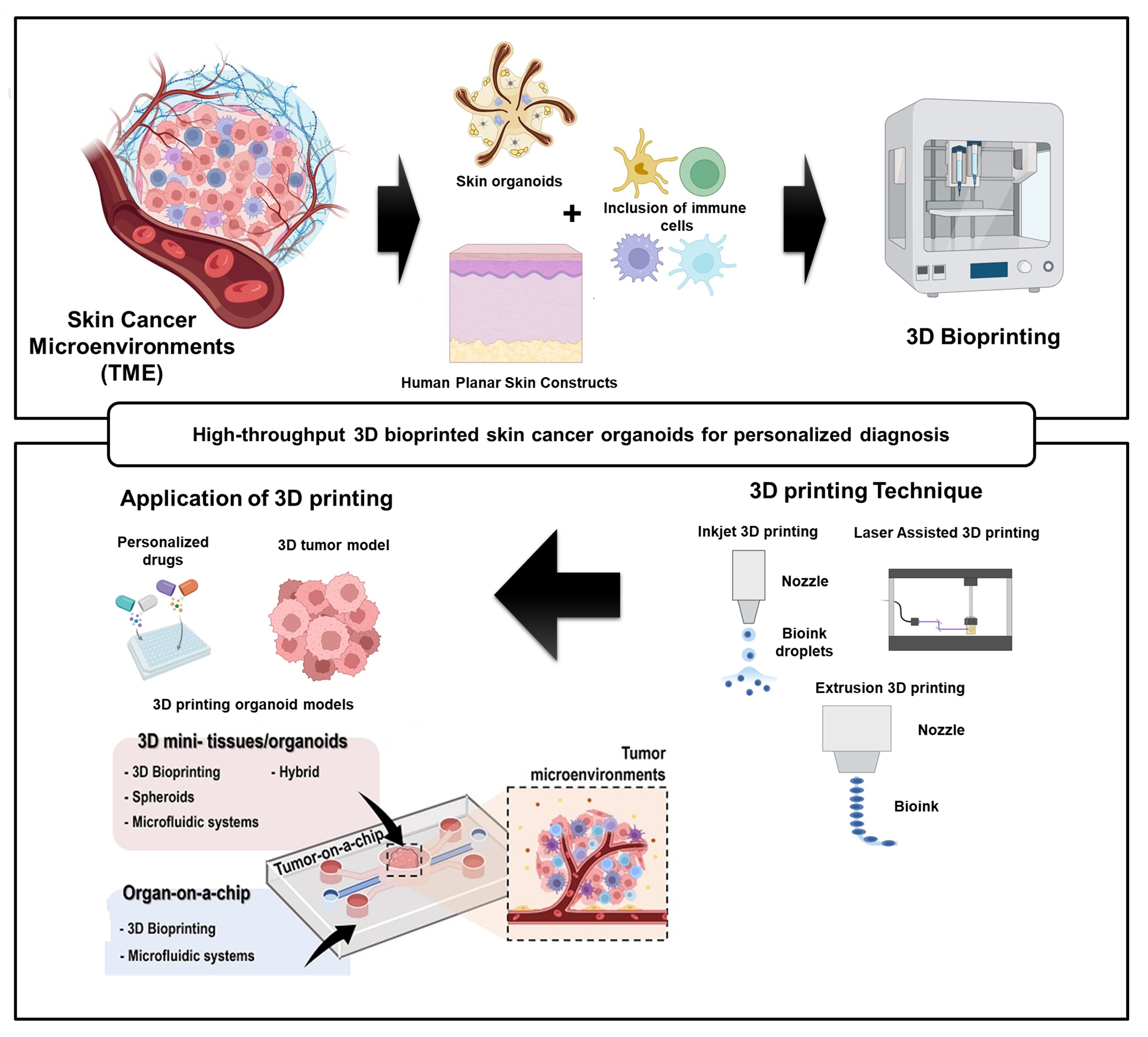
Skin cancer remains a major global health burden, necessitating more accurate models for understanding disease mechanisms, drug responses, and patient variability. Recent advancements in three-dimensional (3D) bioprinting have enabled the development of high-throughput, patient-specific organoids that closely mimic the structural and functional characteristics of native skin tumors. This review highlights the integration of 3D bioprinting technologies with bioengineered extracellular matrices and patient-derived cells to fabricate skin cancer organoids for diagnostic screening and personalized medicine applications. We discuss key bioinks, printing strategies, and biomimetic approaches used to replicate the tumor microenvironment, as well as the incorporation of immune and stromal components for enhanced physiological relevance. The utility of these organoids in high-throughput drug screening, mutation-specific therapy design, and biomarker discovery is also evaluated. Furthermore, we explore current challenges and future directions for translating bioprinted skin cancer models into clinical workflows. Collectively, this review underscores the transformative potential of 3D bioprinted organoids in the precision oncology landscape for skin cancer.
Keywords:
3D bioprinting
; skin cancer organoids
; high-throughput screening
; personalized therapy
; tumor microenvironment
; precision oncology
1. Introduction
The most common cancer in the world, skin cancer, includes a wide range of neoplastic conditions that originate from different types of skin cells. The three main types are melanoma, squamous cell carcinoma (SCC), and basal cell carcinoma (BCC). Although melanoma is less common, it accounts for the majority of skin cancer-related deaths. Different cellular lineages give rise to these cancers: melanocytes cause melanoma, squamous cells cause SCC, and basal keratinocytes cause BCC [1,2,3]. Melanoma is particularly aggressive among them because of its high potential for metastasis, intricate mutational landscape, and ability to evade the immune system. Skin cancer has a complex etiology that includes both environmental and genetic factors. The most important risk factor is still ultraviolet (UV) radiation from sunshine, which can cause DNA damage, mutations in tumor suppressor genes like TP53, and the activation of oncogenes like BRAF, NRAS, and CDKN2A [4,5,6]. Tumor initiation and progression are also influenced by immunosuppression, chronic inflammation, and carcinogen exposure. Cancer cell survival, drug resistance, and immune escape are all significantly aided by the tumor microenvironment (TME), which is made up of stromal cells, immune cells, extracellular matrix (ECM), and signaling molecules. The genetic, phenotypic, and epigenetic diversity of skin cancers has been revealed by recent developments in genomics and molecular biology. Effective diagnosis and treatment are severely hampered by this complexity. Although targeted treatments (e.g., G. immune checkpoint inhibitors (e.g., BRAF and MEK inhibitors) [7,8,9]. Although anti-PD-1/PD-L1 treatments have greatly improved outcomes for patients with metastatic melanoma, many still experience resistance or relapse. Therefore, to screen for customized treatment regimens and gain a better understanding of tumor behavior, it is imperative to develop trustworthy, patient-representative preclinical models [10,11,12,13,14].
The skin is the largest and most physiologically diverse organ in the human body and is responsible for barrier protection, immune modulation, thermoregulation, and sensory recognition. Its unique, multilayered structure is directly related to these critical functions, as shown in Figure 1(A) [15]. The skin is composed of three main layers: the epidermis, which contains proliferative basal keratinocytes, melanocytes that are involved in pigmentation and UV defense, and antigen-presenting Langerhans cells, the dermis, which provides structural support and elasticity through collagen and elastin and houses blood vessels, nerve endings, and adnexal structures, and the hypodermis, which contains adipose tissue that is necessary for energy storage, insulation, and mechanical cushioning. Skin cancer is caused by the malignant transformation of these components, often caused by ultraviolet (UV) radiation. The three most common types of skin cancer are basal cell carcinoma (BCC), squamous cell carcinoma (SCC), and melanoma. The most common and least active form of BCC is basal keratinocytes, which are derived from the basal keratinocytes. SCC is more superficial and more likely to cause metastasis.
Melanoma is the most lethal form of melanocyte, and it is characterized by its aggressive metastatic behavior and immune evasion capabilities. Merkel cell carcinoma, cutaneous lymphoma, and Kaposi’s sarcoma are examples of rare but significant skin malignancies, and underscore the role of immunosuppression and viral co-infection in skin carcinogenesis. The skin microbiota and gut–skin axis are now being used to promote skin cancers, as shown in Figure 1(B) [16]. UV-induced barrier disruption alters the commensal microbial balance, causing chronic inflammation through the release of pathogen- and damage-associated molecular patterns (PAMPs and DAMPs) and microbial toxins. These factors influence immune cell behavior (CD8+ T cells, regulatory T cells, and tumor-associated macrophages) within the tumor microenvironment, promoting immune suppression, proliferation, angiogenesis, and tumor progression. Additionally, gut-derived metabolites and cytokines can enter systemic circulation and modulate skin immunity, indicating a complex interaction between internal and external environments in cancer development [16]. Figure 1(C) and Figure 1(D) indicate that indoor UVR tanning is a common risk factor for non-melanoma and melanoma skin cancers worldwide, and that indoor UVR tanning is a common risk factor for non-melanoma and melanoma skin cancers [17,18,19]. Wehner et al., A meta-analysis. The lifetime (“ever-use”) prevalence of indoor tanning ranged from 11% in Australia to 42% in Europe (Ross, 1986–2012). Past-year prevalence ranged from 2% to 21%, with adolescents using more than adults. A meta-analysis of Rodriguez-Acevedo et al. In 2009–2018, after the WHO classified indoor tanning as a Group 1 carcinogen, usage decreased, but gender disparity continued. Females were more likely than males to tan than females (16.8% vs. 8.5%), and adolescent girls were more likely than boys to tan (8.9% vs. 3.9%). These patterns, as shown in Figure 1(C) and Figure 1(D), illustrate the ongoing public health challenge of artificial UVR exposure and its significant contribution to the global skin cancer burden [17,18,19,20].
Traditional in vitro and in vivo models are essential for comprehending cancer biology, but they have major drawbacks when it comes to translational research in skin cancer. Due to their affordability and ease of use, two-dimensional (2D) monolayer cultures of cancer cell lines are now widely used [21,22,23]. The cellular heterogeneity, dynamic interactions with the TME, and three-dimensional architecture seen in vivo are not, however, replicated by them. Their inability to model tumor-stroma and tumor-immune cell crosstalk limits their ability to predict drug response. Patient-derived xenografts (PDXs) and genetically engineered mouse models (GEMMs) are two examples of animal models that can replicate some aspects of tumor progression and metastasis and provide a more complex biological context [24,25,26]. Nevertheless, their translational value is limited by interspecies immune system differences, ethical considerations, lengthy generation times, and high maintenance costs. Furthermore, these models frequently do not permit individualized evaluations of therapeutic efficacy or high-throughput screening. Furthermore, traditional organoid cultures lack the precise spatial organization and vascularization required to fully model the complexity of skin cancer, even though they are more physiologically relevant than 2D models. Active ECM embedding is a prerequisite for standard organoid protocols (e.g., 3. Heterogeneity and irregular morphology could be the outcome of spontaneous self-assembly and Matrigel. Significant obstacles to scalability, reproducibility, and integration with high-throughput drug testing platforms are presented by these limitations [27,28,29,30].
Bioprinting in three dimensions (3D) has become a revolutionary method for creating intricate, multicellular, and spatially ordered tissue models. The use of biofabrication technologies in 3D bioprinting allows for the accurate deposition of various cell types, biomaterials, and signaling factors in predetermined architectures that replicate the structure and function of native tissue. An unparalleled chance to accurately and precisely replicate the tumor microenvironment in vitro is presented by this technology. Organoids that closely mimic the layered structure of human skin, including the epidermis, dermis, and underlying vasculature, can be produced using 3D bioprinting in the context of skin cancer. To replicate the complexity of the TME, bioprinted skin cancer organoids can include immune components, fibroblasts, keratinocytes, melanocytes, endothelial cells, and cancer cells [31,32,33]. When assessing immune responses, drug resistance mechanisms, and tumor-stroma interactions in patient-specific settings, this high level of biomimicry is essential. Additionally, smaller organoid arrays that are appropriate for multiplexed drug screening can be produced quickly and reliably using high-throughput bioprinting platforms. These systems can be combined with imaging, omics-based readouts, and automated liquid handling to provide thorough information on drug toxicity, efficacy, and molecular response signatures. Crucially, patient-derived tumor cells or biopsy samples can be used to create customized tumor avatars that act as ex vivo stand-ins for clinical judgment [34,35,36,37]. From a medical standpoint, bioprinted skin cancer organoids are an effective precision oncology tool. They may be used to reduce the trial-and-error method that predominates in contemporary clinical practice by screening for the best treatment plans on an individual basis before starting therapy. By better capturing the diversity and progression of skin tumors than conventional systems, these models can also speed up the discovery of new therapeutic targets and biomarkers. Bioprinting technologies are expected to become increasingly useful in cancer research as they develop further, thanks to developments in bioinks, crosslinking chemistries, and microfluidic integration. High-throughput screening platforms, patient-derived organoid culture, and 3D bioprinting come together to usher in a new era of functional diagnostics and tailored treatment in dermatologic oncology [33,38,39].
In this review, we discuss the recent advancements in the development and application of high-throughput 3D bioprinted organoids for modeling skin cancer. A discussion of the biology of skin cancer is given first, along with a discussion of the shortcomings of traditional 2D and in vivo models. Future developments in 3D bioprinting, bioink technology, and methods for creating biomimetic skin cancer organoids are the main topics of the review. We also investigate how to incorporate these models into high-throughput platforms for molecular profiling, drug screening, and customized treatment. Lastly, we assess the field’s present difficulties, clinical translation prospects, and potential future paths in precision dermatologic oncology. In conclusion, the development of complex, patient-representative platforms is required due to the complexity of skin cancer biology and the limitations of traditional preclinical models. A promising method for accurately simulating the cellular, molecular, and structural characteristics of skin tumors is the use of high-throughput 3D bioprinted organoids. In addition to improving our knowledge of the pathophysiology of skin cancer, these biomimetic systems provide reliable platforms for immunotherapy assessment and individualized medication screening. The combination of bioprinting and clinical and molecular oncology has enormous potential to revolutionize the diagnosis and treatment of skin cancer as the field develops.
2. Advances in Skin Cancer Modeling
Skin cancer, which can be broadly classified into melanoma and non-melanoma skin cancers (NMSCs), which include squamous cell carcinoma (SCC) and basal cell carcinoma (BCC), is one of the most common cancers in the world. The majority of skin cancer-related deaths are caused by melanoma, which is derived from melanocytes and is much more aggressive than NMSCs despite being less common [3,40,41]. The most prevalent type of cancer, basal keratinocyte-derived BCC, usually grows slowly, whereas squamous keratinocyte-derived SCC has a higher potential for metastasis than BCC. Genetic mutations interact intricately to drive the development of skin cancer (e.g., A. PTCH1, CDKN2A, BRAF, TP53, and epigenetic modifications), as well as environmental elements like UV rays, persistent inflammation, and immunosuppression. To develop effective diagnostic and therapeutic strategies, it is essential to understand the multistep process of skin carcinogenesis, which encompasses normal skin epithelium, dysplasia, carcinoma in situ, and invasive carcinoma [42,43,44,45].
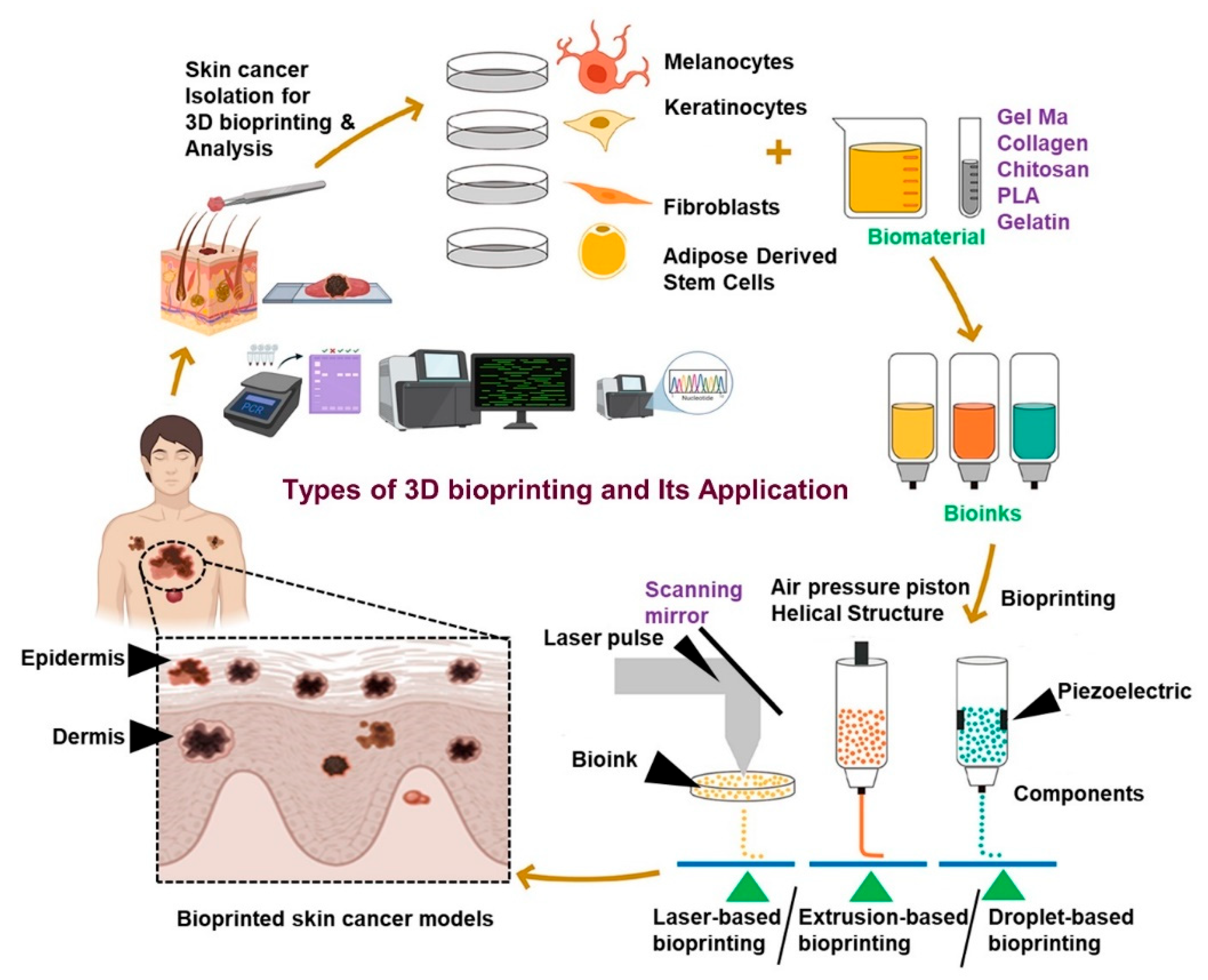
The skin bioprinting process is divided into six main steps, as shown in Figure 2. The first step is determining clinical goals, in which the researcher sets research and clinical objectives following a project design criterion based on diseases, real-world structures to imitate, and pre-existing models. To create 3D digital models and create tool paths, respectively, the second step involves using 3D computer-aided design software and computer-aided manufacturing software. Next, choosing a bioink is a crucial step in the bioprinting process. To choose the best bioink, background information on the material properties of the selected bioink, as well as the physiological and biochemical conditions of the cells, is needed. A 3D bioprinter, printheads, temperature control, and sterile conditions are necessary for the fourth step, which is the printing process. In order to achieve high resolution, this step includes an optimization sub-step that is primarily used for parameter adjustment. Functionalization is the fifth step, in which the printed model is put into a bioreactor or incubator to enable the cells to grow, stabilize, and become functional. The model’s suitability for its intended use is verified in the sixth and last step. In vitro testing, disease modeling, and in vivo implementation are common uses.
Skin cancer is traditionally studied using xenografts, genetically engineered mouse models (GEMMs), 2D cell lines, and patient-derived xenografts (PDXs). Although 2D monolayer cultures are inexpensive and simple to manage, they lack the cellular heterogeneity, microenvironmental context, and three-dimensional architecture of in vivo tumours [46,47,48]. Their predictive ability for drug screening and comprehending disease mechanisms is thus limited. In contrast, animal models, particularly mouse models, provide systems that are more physiologically relevant by taking into account systemic effects and immune interactions. GEMMs, like those with conditional Tp53 or BrafV600E mutations, mimic some features of the onset and spread of human skin cancer [49,50,51]. Tumor fragments from patients are implanted into immunocompromised mice in PDXs, which have proven useful in assessing treatment outcomes. However, due to ethical concerns and species-specific variations, these in vivo systems are costly, time-consuming, and limited. Three-dimensional (3D) culture models, such as organoids, scaffolds, and spheroids, have become popular for bridging the gap between in vivo and in vitro research. For high-throughput drug screening and personalized medicine applications, organoids—in particular—are perfect because they can more closely resemble the cellular complexity and architecture of tumors. These models still have issues with reproducibility, standardization, and integrating various skin constituents like immune cells and vasculature [52,53,54].
Immune evasion, treatment resistance, and the advancement of skin cancer are all significantly influenced by the tumor microenvironment (TME). It is made up of a dynamic and interactive network of immune cells (e.g., CAFs), cancer-associated fibroblasts (e.g., T cells, macrophages), endothelial cells, signaling molecules, and extracellular matrix (ECM) constituents. Both innate and acquired resistance to targeted treatments, including BRAF inhibitors and immune checkpoint blockade, are greatly influenced by the TME in melanoma (e.g., A. anti-PD-1/PD-L1 treatments [55,56,57]. Heterogeneity and plasticity are two of the TME’s primary characteristics, allowing cancer cells to adjust and endure under therapeutic pressure. CAFs can secrete cytokines and remodel the extracellular matrix (e.g., A. that encourage angiogenesis, tumor growth, and drug resistance (e.g., TGF-β, IL-6). Immune checkpoint expression, myeloid-derived suppressor cells (MDSCs), and regulatory T cells (Tregs) all contribute to immune suppression in the TME, which considerably reduces the effectiveness of immunotherapies. Hypoxia in the TME also causes metabolic reprogramming and the epithelial-mesenchymal transition (EMT), both of which increase the aggressiveness of tumors. The complexity of the TME is not adequately captured by the majority of current models, despite these revelations. Improvements in organ-on-chip platforms, 3D bioprinting, and co-culture systems have made it possible to integrate TME components more effectively, increasing model fidelity and clinical relevance [58,59,60,61].
Our comprehension of tumor biology and treatment response is being revolutionized by recent developments in skin cancer modeling. The intricate spatial and cellular architecture of human tumors cannot be accurately replicated by conventional 2D cultures and animal models, despite the fact that they have yielded insightful information. New 3D models that incorporate tumor heterogeneity and microenvironmental cues are particularly promising, especially patient-derived organoids and bioengineered constructs. It is crucial to include elements of the TME in these models in order to investigate therapy resistance mechanisms and find new therapeutic targets. As these models develop further, they have the potential to significantly improve outcomes for skin cancer patients, speed up drug development, and improve personalized medicine.
3. Bioprinting Technologies for Skin Cancer Organoids
The development of biomimetic models for the study of complex diseases like skin cancer has advanced dramatically with the advent of 3D bioprinting. The complex architecture, heterogeneity, and microenvironmental dynamics of human skin tumors cannot be replicated by conventional 2D culture systems. On the other hand, skin cancer organoids that closely resemble native tissues can be created thanks to 3D bioprinting, which provides precise spatial control over a variety of cell types and extracellular matrices (ECMs). These organoids are excellent tools for researching immunological evasion, drug resistance, tumorigenesis, and creating individualized treatment plans [62,63,64]. A number of 3D bioprinting technologies have been created to create tissue-mimicking structures that are accurate, quick, and scalable. Extrusion-based bioprinting, laser-assisted bioprinting, and inkjet bioprinting are the three main bioprinting methods. Bioinks are deposited in droplet form using thermal or piezoelectric forces in inkjet bioprinting. Although the high speed and cost-effectiveness of this method are beneficial, the formation of densely populated tumor regions may be impeded by its low viscosity requirements and decreased cell density.
The most popular method for creating cancer organoids is extrusion-based bioprinting, which extrudes bioinks continuously through a nozzle using mechanical or pneumatic forces. It enables the creation of layered structures with high mechanical stability and cell viability by printing dense cell suspensions and high-viscosity materials [65,66,67]. The stratified architecture of skin, including the epidermis, dermis, and tumor mass, can be modeled with this technique. Laser-assisted bioprinting uses a concentrated laser to drive bioink droplets from a donor slide to a collector surface, providing high resolution and cell viability. Although it avoids nozzle clogging and offers precision, its cost and complexity may prevent it from being widely used. In general, the platform selection is based on the intended resolution, cell viability, biological objective, and compatibility with particular bioinks with specific types of 3D bioprinting techniques utilized for the development of skin cancer models and it’s application for detection, analysis of cancer, and the potential effects of various drugs, as shown in Figure 2.
Bioinks are essential for bioprinting skin cancer organoids because they affect tumor microenvironmental interactions, differentiation, and cell viability. The best bioinks for skin cancer modeling should support cell adhesion, permit vascularization and tumor growth, and replicate the characteristics of the natural extracellular matrix. Natural bioinks provide biological cues and biocompatibility that are vital for the growth of skin and tumor cells. Examples of these include collagen, gelatin, hyaluronic acid, alginate, and decellularized extracellular matrix (dECM). As an illustration, blends of alginate and gelatin-methacryloyl (GelMA) enable adjustable mechanical characteristics and promote the growth of melanoma and keratinocyte cells. While Pluronic F127 and polyethylene glycol (PEG) derivatives are examples of synthetic bioinks that provide fine control over mechanical and chemical properties, they frequently lack bioactivity. Hybrid bioinks that combine natural and synthetic polymers have been created to address this issue and combine their benefits. Methods of crosslinking, like ionic (e.g., heat, calcium ions for alginate gelatin), photocrosslinking (e.g., Enzymatic techniques and UV light for GelMA), are used to stabilize the printed structures. Because photo-crosslinking gels quickly and allow for spatial control, it is particularly well-liked for high-throughput applications. A comparative analysis of bioprinting methods for skin cancer models, including advantages and disadvantages, is presented in Table 1 [67,68,69].
To create skin cancer organoids that mimic the intricacy of natural tissue, several cell types must be layered in precise spatial configurations. To replicate the epidermal, dermal, and vascular compartments, a biomimetic skin cancer model usually consists of basal keratinocytes, melanocytes, fibroblasts, endothelial cells, and immune cells. Using keratinocytes and melanoma cells to create the epidermis and fibroblasts embedded in a collagen-rich matrix to create the dermis, bioprinting allows for the creation of multi-layered structures. Integrating immune cells (e.g., cancer-associated fibroblasts, or CAFs) helps address tumor heterogeneity [70,71,72]. To replicate the varied cellular and molecular environment of skin tumors using patient-derived tumor cells, macrophages, T cells, and others. Furthermore, the ability to replicate immune infiltration and nutrient diffusion depends on vascularization. Techniques like sacrificial ink removal and coaxial bioprinting enable the development of perfusable vascular channels inside the constructs. Through the introduction of fluid flow, oxygen gradients, and dynamic drug exposure conditions that replicate the in vivo tumor microenvironment, integration with microfluidic systems further improves the physiological relevance [73,74,75].
Figure 3.
Types of 3D bioprinting and their applications for the fabrication of skin cancer models for the detection and analysis of cancer and the potential effects of various drugs.
Figure 3.
Types of 3D bioprinting and their applications for the fabrication of skin cancer models for the detection and analysis of cancer and the potential effects of various drugs.
In conclusion, the development of organoids that faithfully replicate the structural and functional complexity of the tumor has been made possible by 3D bioprinting technologies, revolutionizing the field of skin cancer research. Robust and customized cancer models can be created by combining sophisticated bioprinting platforms, optimized bioinks, and engineered multicellular architectures. Advances in vascularization techniques, crosslinking chemistry, and biofabrication will improve the accuracy and translational significance of skin cancer organoids as the field develops. In the end, these developments will improve patient stratification, speed up drug discovery, and advance personalized oncology.
4. High-Throughput Strategies for Organoid Fabrication
High-throughput organoid fabrication techniques are essential for speeding up drug discovery and translational cancer research. In addition to being time-consuming and labor-intensive, traditional methods for creating cancer organoids frequently lack the scalability needed for extensive screening. These restrictions are being overcome by recent advancements in biofabrication technologies, specifically 3D bioprinting, microfluidics, and organ-on-chip systems, which make it possible to produce scalable, physiologically relevant, and reproducible skin cancer organoids. These high-throughput methods enable quick drug testing and genomic analysis, improve control over the tumor microenvironment, and provide precision in tissue architecture. With an emphasis on scalability and quality control, this section describes the creation of high-throughput organoid models via automation, multiplexed bioprinting, and the integration of microengineered systems [76,77,78].
Multiplexed and automated bioprinting platforms are transforming the production of skin cancer organoids. Clinical applications and drug discovery are limited by the high variability and low throughput of traditional manual organoid culture. Automated bioprinting systems, on the other hand, require little user intervention and can quickly deposit cells and biomaterials with spatial precision. From bioink loading to structure fabrication, these systems optimize the bioprinting process by leveraging digital control interfaces and programmable robotics. By creating several organoids with different compositions and geometries at once, multiplexed bioprinting improves throughput and experimental reproducibility. It is possible to deposit cell-rich hydrogels into multiwell formats or microarray platforms using methods like droplet-based printing and extrusion-based bioprinting. Under consistent conditions, this is especially beneficial for screening sizable drug panels or tumor cells derived from patients. Additionally, modern bioprinting systems incorporate feedback loops and real-time imaging, which enable accurate monitoring and correction throughout the printing process, lowering errors and variability in the production of organoids [79,80,81,82].
When combined with 3D bioprinted organoids, microfluidic systems, and organ-on-chip platforms offer a potent technological convergence that aims to replicate the physiology of native skin cancer. Microfluidic devices manipulate fluid flow, nutrient gradients, and chemical stimuli to provide precise control over the cellular microenvironment. By precisely delivering drug or immune effector concentrations in a time-dependent manner, these devices can be made to closely mimic in vivo pharmacodynamics. Because static cultures frequently lack dynamic conditions like shear stress, oxygen gradients, and immune infiltration, researchers can replicate these in the context of skin cancer through microfluidic integration. For example, skin cancer organoids can be used in tumor-on-a-chip platforms to mimic interactions between the tumor and the vasculature or the migration of metastatic cells across dermal barriers. Microfluidic perfusion also improves waste elimination and nutrient exchange, which prolongs culture viability and promotes the organoids’ functional maturation. Organ-on-chip technologies also make it easier to co-culture immune, stromal, and endothelial cells. This allows researchers to test immunotherapeutic approaches such as adoptive T cell therapy, immune checkpoint inhibitors, and others in a controlled microenvironment. These integrated systems enable the testing of patient-specific reactions to different therapeutic agents, making them useful tools for personalized medicine [83,84,85,86,87].
The effective use of organoid-based technologies in clinical and pharmaceutical applications depends on ensuring quality, scalability, and standardization. In high-throughput organoid fabrication, preserving consistency in size, cellular makeup, and structural integrity is one of the main obstacles. By precisely regulating printing parameters like extrusion speed, pressure, and temperature, automation helps to minimize batch-to-batch variability. To evaluate the quality of organoids in real time, sophisticated imaging techniques like live-cell imaging, optical coherence tomography, and confocal microscopy are being used. To confirm that organoids accurately replicate the phenotype and genotype of the original tumors, omics-based techniques such as transcriptomics and proteomics are employed. By using bioprinting platforms that work with common multiwell plates, scalability is accomplished (e.g., 96 or 384-well formats), allowing hundreds of organoids to be produced in parallel in a single run. Precision oncology applications and high-content drug screening depend on this. Additionally, to enhance inter-laboratory reproducibility and regulatory compliance, efforts are being made to create standardized protocols for the formulation of bioinks, the preparation of cell sources, and printing parameters [89,90,91,92].
Barros et al. (2024) and their colleagues developed a high-throughput 3D bioprinted skin/skin cancer-on-a-chip model was created by (2024) and associates to overcome the shortcomings of traditional systems in reproducing skin architecture and permitting localized drug delivery [88]. The method starts with the creation of a microfluidic skin-on-a-chip system that includes PDMS chambers and a porous membrane, as shown in Figure 4 (A-a). This allows for the application of microneedles (MNs) for transdermal drug delivery and the culture of layered skin tissue. Keratinocyte differentiation is supported by the air–liquid interface (ALI) culture as shown in Figure 4 (A-b), which encourages stratification of the epidermis. Figure 4 (B-C) illustrates layer formation and morphological integrity. Well-organized 3D dermal layers, as shown in Figure 4 (B), and the sequential development of epidermal layers on days 10, as shown in Figure 4 (C-a), and 14, as shown in Figure 4 (C-b), are seen in confocal imaging [88]. Fluorescence labeling of nuclei, actin, α-SMA, and pan-cytokeratin confirms the arrangement of cells. The dermal and epidermal layers’ time-dependent assembly and their measured thicknesses, which support full skin maturation, are further described in Figure 4(D-a-b). Marker expression and tissue identity are shown in Figure 4(E). Confocal pictures and measurements of the epidermal markers Keratin 14/19, as shown in Figure 4(E-a), Filaggrin/Keratin 10 as shown in Figure 4(E-b), and dermal markers Collagen I/Fibronectin as shown in Figure 4(E-c), validate proper stratification [88]. With cornified epidermis and layered dermis, H&E staining, as shown in Figure 4(E-d), verifies architectural resemblance to native skin.
The epidermis’s relative spatial expression of FLG, K14, and K10 is depicted in Figure 4(F), which shows clear localization from the stratum corneum to the basale. In Figure 4 (G-a), a metastatic layer is integrated into the dermis to simulate melanoma. Tumor invasion towards the media channel is demonstrated by live/dead staining following a 24-hour ALI culture, as shown in Figure 4(G-b). Melanoma positioning is confirmed by a 3D reconstructed image, as shown in Figure 4(G-c) [88]. After that, DOX-loaded MNs were created and described as shown in Figure 4(H). Their application in the skin cancer model with structural views (a), mechanical properties (b-c), drug release profiles (d) and schematic, analysis of confocal image as shown in Figure 4(H-a-g), all demonstrate successful and consistent penetration into tumor zones (~600 μm). The effectiveness of drug delivery is finally assessed in Figure 4 (I). A comparison of (a) perfusion, (b) DOX-free MNs, and (c) DOX-loaded MNs is shown in cross-sectional images. Melanoma cell death and drug localization attest to MN-based delivery’s superior performance. Z-stack views (d) demonstrate the targeted cytotoxicity of DOX-loaded MNs, confirming the system’s suitability for therapeutic modeling and high-throughput screening [88].
In conclusion, the advancement of high-throughput techniques for creating 3D bioprinted skin cancer organoids represents a revolutionary development in preclinical cancer research. Organoid production is significantly faster and more reproducible thanks to automation and multiplexed printing. Integration with organ-on-chip and microfluidic platforms allows for real-time drug and immune response studies as well as dynamic modeling of the tumor microenvironment. Lastly, the standardization required for clinical translation is guaranteed by strong quality control procedures and scalable systems. The implementation of bioprinted organoids in therapeutic screening and personalized diagnostics is made possible by these developments taken together.
5. 3D Bioprinted Organ-on-Chips for Skin Cancer Detection: A Converging Platform for Precision Diagnostics
An innovative method for simulating the human skin microenvironment for the early detection and research of skin cancers, especially melanoma and non-melanoma types, is provided by the combination of 3D bioprinting and organ-on-chip (OoC) technologies. The intricate structure, diversity, and dynamic microenvironmental interactions of human skin tumors are not adequately represented by conventional in vitro and in vivo models. On the other hand, 3D bioprinted organ-on-chip platforms offer miniature, physiologically relevant systems that can accurately replicate the biochemical and biomechanical characteristics of skin tissue. The first step in creating these hybrid systems is choosing biomimetic bioinks, which usually include hydrogels that resemble extracellular matrix (ECM) and skin cells that are either patient-derived or genetically modified, such as fibroblasts, tumor cells, melanocytes, keratinocytes, and melanocytes. These cellular components can be precisely spatially deposited to replicate the epidermal and dermal compartments using the layered 3D bioprinting process [93,94,95]. In order to replicate vascular flow, mechanical stress, and the interstitial transport of nutrients and medications, these constructs are subsequently incorporated into microfluidic chips that have perfusable channels. This platform’s capacity to replicate the tumor microenvironment, including immune cell infiltration, hypoxic gradients, and dynamic cytokine signaling, is one of its main advantages.
This makes it possible to track the beginning, spread, and invasion of cancer in real time. Additionally, the chip’s biosensors allow for the quantitative identification of tumor biomarkers like S100B, MIA, and LDH, which promotes early diagnosis [96,97,98,99,100]. These sensors measure electrical impedance, metabolic activity, and secreted biomarkers to monitor how cells react to stimuli like UV light or medicinal drugs. These platforms also facilitate high-throughput screening for immunotherapeutics and chemotherapeutics, providing information on patient-specific reactions. Individualized diagnostic models can be created using customized bioinks made from tumor cells derived from the patient. Additionally, the platform facilitates the co-culturing of immune cells, including macrophages and T cells, allowing for immunophenotyping and the investigation of immune evasion mechanisms in skin cancers. Notwithstanding the benefits, there are still issues to be resolved, such as preserving long-term cell viability, attaining high-resolution vascularization, and standardizing fabrication procedures. These restrictions are gradually being addressed, though, by recent developments in biocompatible materials, real-time imaging, and microfluidic control systems [14,101,102,103,104,105,106].
Three-dimensional (3D) bioprinted organ-on-chip platforms, which combine tissue engineering, microfluidics, and nanotechnology, are becoming increasingly potent instruments for skin cancer precision diagnostics. Using nanoparticle-coated microarrays, a biosensing approach based on nanotechnology allows for the high-throughput detection of cancer biomarkers, as shown in Figure 5 (A). These arrays are used to find possible markers, such as those linked to skin cancer, using a tiny blood sample taken from patients with breast cancer. Promising biomarker candidates are validated by ELISA in sizable patient cohorts after array-based screening, enabling their application in prognosis, early-stage diagnosis, disease stratification, and therapeutic monitoring. After validation, these biomarkers can be incorporated into biosensor platforms or electrochemical immunosensors for clinical use, furthering the development of accurate and non-invasive cancer diagnostics. Engineered melanoma skin models that depict the various phases of melanoma invasion and are created through bioprinting techniques are shown in Figure 5 (B) [107]. Key risk factors for the development of melanoma, including genetic predisposition and UV exposure, as shown in Figure 5 (A-a).
The disease progression is shown step-by-step, as shown in Figure 5 (A-b), starting with the presence of melanocytes at the dermal–epidermal junction and continuing through early tumor clustering, dermal infiltration, and deep tissue invasion. Skin constructs that have been tissue-engineered are used to replicate these pathological stages. Melanoma spheroids can be integrated with perfusable vascular channels using sophisticated in-bath bioprinting techniques, as shown in Figure 5 (A-c), which precisely replicates the tumor microenvironment. Additionally, modeling of tumor–vasculature interactions—which are essential for researching metastasis and immune evasion—is made possible by bioprinted stroma that incorporates both blood and lymphatic vessels as shown in Figure 5 (A-d). When combined, these systems provide a complete and expandable platform for high-throughput drug testing, biomarker validation, and disease modeling, establishing 3D bioprinted organ-on-chips as revolutionary instruments in precision oncology [107]. In conclusion, 3D bioprinted organ-on-chip systems are an effective way to improve diagnostic accuracy and model the pathophysiology of skin cancer. These platforms open the door for individualized and non-invasive skin cancer diagnostics by fusing microfluidic dynamics with cellular complexity, which eventually leads to earlier detection and better treatment approaches.
6. Applications in Diagnosis and Personalized Therapy
Three-dimensional (3D) bioprinted skin cancer organoids are a revolutionary development in personalized medicine and cancer diagnosis. These engineered constructs provide previously unheard-of possibilities for high-throughput drug screening, genomic profiling, and immunotherapeutic evaluation by simulating the intricate architecture and pathophysiological microenvironment of human tumors. The translational gap between bench research and clinical application is filled by 3D bioprinted organoids, which overcome the shortcomings of conventional 2D cultures and animal models, especially in capturing tumor heterogeneity and patient-specific responses. The use of skin cancer organoids in drug screening and sensitivity testing is among their most prominent uses. The spatial and cellular complexity of human tumors is frequently not replicated by traditional monolayer cultures, which leads to inaccurate efficacy data. However, within a biomimetic extracellular matrix, bioprinted organoids can incorporate a variety of cell types, such as immune cells, fibroblasts, endothelial cells, and tumor cells [108,109,110].
This makes it possible to summarize the kinetics of drug penetration and tumor-stroma interactions. These organoids allow hundreds of drug candidates to be tested simultaneously across a wide panel of patient-derived samples when used in high-throughput formats. For example, certain kinase inhibitors that specifically target oncogenic signaling in drug-resistant subtypes have been found using organoids from melanoma and squamous cell carcinoma. Furthermore, fluorescent or imaging-based assays can be used to track dynamic responses in real time, such as invasion suppression, proliferation inhibition, or apoptosis induction. By identifying the most effective therapeutic agents for each patient, this individualized screening method shortens the time to treatment and enhances clinical results. 3D bioprinted organoids are useful tools for genomic validation and molecular profiling in addition to pharmacological testing. The epigenetic signatures and mutational landscape of the original tumors, such as p53, NRAS, BRAF, and other oncogenic drivers frequently found in skin cancers, are preserved in patient-derived organoids [111,112,113,114].
Researchers can link genomic changes to treatment response by using high-throughput sequencing and transcriptomic analysis on organoid tissues. Finding biomarkers and predicting resistance mechanisms are improved by this combination of omics data and functional assays. To help with the logical design of combination therapies, gene expression profiling of skin cancer organoids undergoing targeted therapy, for instance, can identify compensatory pathways that mediate drug resistance. Additionally, functional interrogation of particular genes is made possible by the use of CRISPR-Cas9 genome editing within organoids, confirming their roles in drug response or tumor progression. When combined with the structural accuracy of bioprinted models, these genomic tools help to improve precision oncology by guiding clinical judgment and medication development. Immunotherapy has transformed the treatment of skin cancer, especially melanoma, but it is still very difficult to predict how a patient will react. Organoids made from bioprinted patients present a viable way to assess immunotherapy [115,116,117].
Researchers can replicate immune-tumor interactions in a controlled ex vivo setting by integrating autologous immune cells, such as peripheral blood mononuclear cells (PBMCs) or tumor-infiltrating lymphocytes (TILs), into the bioprinted constructs. This makes it possible to test adoptive cell transfer procedures, cytokine treatments, or immune checkpoint inhibitors in a customized setting. T-cell activation, cytotoxic tumor cell death, and PD-1/PD-L1 signaling can all be replicated by immune-active organoids, according to recent research. These systems also make it possible to assess the immune evasion tactics used by tumor cells, such as the release of inhibitory cytokines or the expression of immune-suppressive ligands. As a result, organoid-based immunoassays can be used as predictive instruments for patient stratification, allowing medical professionals to determine who will respond and who won’t before starting treatment [118,119,120]. In conclusion, the high-throughput 3D bioprinted skin cancer organoids offer a thorough and physiologically appropriate platform for improving therapy customization and diagnosis. Through molecular profiling, immunotherapy evaluation, and drug screening, these models aid in the creation of customized treatment plans that are less harmful and more effective. The incorporation of organoids into clinical workflows has enormous potential to revolutionize cancer treatment in the future as bioprinting technologies and biomaterials advance.
7. Future Perspectives
The creation of skin cancer organoids using high-throughput 3D bioprinting technology has created new opportunities for tumor complexity modeling, improving diagnostic precision, and allowing for individualized treatment plans. With the potential to completely transform how physicians approach treatment planning, drug sensitivity profiling, and immunotherapy response prediction, the field is moving closer to clinically meaningful applications. However, several crucial translational and regulatory issues need to be resolved to move from experimental research to standard clinical practice. Verifying that bioprinted skin cancer organoids can replicate the physiological and pathological features of native tumors, such as their cellular structure, genetic mutations, and microenvironmental interactions, is essential for clinical translation [121,122,123].
To guarantee reproducibility and comparability of results across labs, standardization of procedures across bioprinting platforms, bioink compositions, and cell sources is crucial. Furthermore, before approving these organoid models for clinical decision-making or drug screening, regulatory bodies like the FDA and EMA demand comprehensive validation studies that show their safety, effectiveness, and dependability. With informed consent, data security, and biobanking procedures in place, ethical issues of the use of patient-derived cells must also be properly handled. The widespread use of 3D bioprinted organoid technology is still constrained by many issues, despite encouraging developments. The intricacy of simulating the tumor microenvironment, which includes stromal interactions, immune cell infiltration, and vasculature—all of which are important factors in the development of cancer and resistance to treatment—is one of the main challenges. The creation of generalized models is made more difficult by the diverse nature of skin cancers, including melanoma, squamous cell carcinoma, and basal cell carcinoma. Reduced biological functionality or structural resolution is frequently the price paid for high-throughput fabrication. Furthermore, cross-study comparisons are challenging due to the absence of benchmarking tools and standardized assays among research groups [124,125,126].

Table 3.
Summary of selected 3D in vitro systems—including organoids, human planar skin constructs, and microfluidic platforms—utilized to replicate various features of skin physiology, structural organization, and the melanoma tumor microenvironment, highlighting the incorporation of immune components.
Table 3.
Summary of selected 3D in vitro systems—including organoids, human planar skin constructs, and microfluidic platforms—utilized to replicate various features of skin physiology, structural organization, and the melanoma tumor microenvironment, highlighting the incorporation of immune components.
| Model Type | Method | Cell Composition | Matrix Used | Purpose | Limitations | Ref. |
|---|---|---|---|---|---|---|
| Spherical Melanoma Organoids | Co-culture with fibroblasts | Human skin fibroblasts; melanoma cell lines (WM1366/1205Lu) | Bovine Collagen I | Explore stromal influence on tumor development and resistance | Limited to a single healthy cell type; lacks layered skin structure | [127] |
| Co-culture with endothelial cells | HUVECs; melanoma cell lines (A375/M21) | - | Investigate tumor angiogenesis | Absence of healthy skin cells; non-functional capillary networks | [128] | |
| Three-cell model | Fibroblasts (CCD-1137Sk), keratinocytes (HaCaT), melanoma cells (SK-MEL-28) | Endogenous Collagen IV | Model early-stage melanoma, assess chemotherapy response | No cornified epidermal layer formed | [129] | |
| Five-cell model | Primary fibroblasts, keratinocytes, melanocytes, adipocytes; melanoma cells (SK-MEL-28) | - | Tumor-stroma crosstalk in melanoma | Does not replicate melanoma penetration | Unpublished | |
| Immune-Competent Melanoma Organoids | Air-liquid interface culture | Stromal and immune cells from tumor biopsies | Type I Collagen | Personalized immunotherapy | No healthy skin or epidermal stratification | [130,131,132] |
| Combined lymph node model | Melanoma tissue; lymph node-derived immune cells | Hyaluronic acid/Collagen hydrogel | Personalized treatment screening | Few patient samples; lacks full skin context | [133] | |
| Autologous lymphocyte co-culture | Melanoma tissue; peripheral lymphocytes | Matrigel | Candidate selection for immunotherapy | Limited patient scope; lacks full skin structure | [134] | |
| Melanoma on Planar Skin Constructs | Spheroid/Cell injection | Keratinocytes, fibroblasts; melanoma cell lines (WM35, SK-MEL-28, SBCL2, etc.) | DED, Collagen I, Alvetex scaffold | Study melanoma invasion and drug responses | Missing cell types like melanocytes, vasculature | [135,136,137] |
| Vascularized melanoma model | HMVECs, keratinocytes, fibroblasts; melanoma lines | - | Drug screening in vascularized environment | Time-consuming; low throughput | [138] | |
| Immunocompetent Planar Models | Activated immune cell addition | Keratinocytes; CD4+ T cells or Langerhans cells | DED, Collagen I | Psoriasis, allergy, drug testing | Donor mismatch and limited skin cell diversity | [139,140,141,142] |
| Bioprinted with macrophages | Keratinocytes, fibroblasts, macrophages (M1/M2) | Custom bioink with nanofibrillated cellulose, fibrinogen, etc. | Chronic inflammation (e.g., atopic dermatitis) | Lacks melanocytes, vasculature | [143] | |
| Bioprinted wound models | Keratinocytes, fibroblasts, HUVECs, macrophages | Collagen I + plasma-based fibrin bioink | Wound healing and inflammation | Missing melanocytes | [144] | |
| Immune-Competent Skin Constructs with Melanoma | Co-culture with melanoma and immune cells | Keratinocytes, fibroblasts, melanocytes, melanoma cells, dendritic or T cells | Collagen I, DED | Tumor-immune interaction, progression, and immunotherapy | No vasculature; no leukocyte extravasation | [145,146,147,148] |
| Melanoma-on-a-Chip Systems | Microfluidic integration | Keratinocytes, fibroblasts, melanoma cells (WM-115) | Collagen | Cell-cell crosstalk studies | No stratified skin architecture | [149] |
| Skin-on-chip with immune components | HaCaT, U937 or HL-60 cells, HUVECs | Collagen I | Allergy and immune response modeling | Lacks full dermal/immune composition | [150,151,152] | |
| Melanoma-immune chip systems | Melanoma spheroids, immune cells from biopsy | Collagen I | Immunotherapy and drug screening | No healthy skin structure; immune cell recruitment limited | [153,154] | |
| Vascularized chip with immune cells | HUVECs, melanoma cells (BLM), whole blood | Gelatin | Inflammation modeling | No skin layers included | [155] | |
| Circulating melanoma-neutrophil interactions | Melanoma A-375/A-375 MA2, neutrophils | Fibrin | Tumor cell extravasation, metastasis | Not representative of skin architecture | [156] |
Using microfluidic systems, sometimes referred to as organ-on-chip platforms, in conjunction with bioprinted constructs to more accurately replicate physiological perfusion and dynamic nutrient exchange is one of the emerging solutions to these problems. Replicating native tissue complexity through co-culturing cancer cells with fibroblasts, endothelial cells, and immune cells in bioengineered matrices is also showing promise. More biocompatible and adjustable hydrogels that sustain long-term organoid growth while preserving cellular viability and phenotype have been developed as a result of advancements in biomaterial science [83,157,158]. Furthermore, to improve throughput and analytical accuracy, organoid-based screening platforms are integrating artificial intelligence (AI)-driven imaging and data analysis pipelines. In order to facilitate customized therapy testing, future developments in precision skin cancer modeling are probably going to concentrate on customizing organoid systems with patient-derived cells. Combining bioprinted organoid responses with genomic and transcriptomic data will aid in improving drug toxicity and efficacy prediction algorithms. To satisfy the needs of clinical labs and the pharmaceutical sector, these platforms’ scalability must also be considered. To study oncogenic drivers and therapeutic targets in a controlled environment, researchers are also investigating the use of gene-editing technologies, such as CRISPR/Cas9, to introduce or correct mutations in bioprinted organoids [159,160,161].
Collaboration between academic institutions, regulatory agencies, and biotechnology companies is crucial to ensuring broad adoption and utility. Additionally, creating centralized databases, creating open-access organoid biobanks, and investing in staff training will hasten innovation and interdisciplinary knowledge exchange. In summary, high-throughput 3D bioprinted skin cancer organoids offer a platform that connects fundamental research and clinical use, marking a revolutionary development in the field of oncology. Even though this technology has obstacles to overcome, especially in the areas of biological complexity, reproducibility, and regulation, its future looks bright. Bioprinted organoids have the potential to become a crucial part of precision medicine by overcoming present obstacles and embracing new technologies and interdisciplinary partnerships. This will allow for more efficient, individualized, and timely treatments for patients with skin cancer.
8. Conclusion
High-throughput 3D bioprinting of skin cancer organoids is an innovative development in cancer modeling, diagnosis, and personalized therapy. They allow the reconstruction of complex tumor microenvironments, including fibroblasts, keratinocytes, endothelial cells, and immune cells. Organoids are similar to traditional 2D cultures or animal models in that they closely mimic the histological architecture, genetic mutations, and immune responses of native skin tumors, including melanoma and non-melanoma. This enables drug screening, immunotherapy assessment, and treatment planning with a focus on specific drugs and immunotherapy. However, they must address a number of translational and regulatory hurdles, even though they promise. For clinical use, organoids must replicate physiological tumor features and be validated on a variety of platforms. The standardization of bioprinting techniques, cell sources, and bioink compositions is important for reproducibility and comparability of results across laboratories. Regulatory bodies like the FDA and EMA need to validate these models extensively before they can be used in clinical workflows. Replicating complete tumor microenvironment complexity, including vasculature, stromal interactions, and immune infiltration, remains challenging. Many models still lack the full spectrum of skin architecture and cell diversity. These constraints are being overcome by innovations such as organ-on-chip systems, improved biomaterials, and improved analysis pipelines with artificial intelligence. Additionally, CRISPR/Cas9 gene editing is being used to allow personalized organoid systems to predict therapeutic outcomes by patient-derived cells combined with CRISPR/Cas9 gene editing. 3D bioprinted skin cancer organoids provide a promising platform for integrating basic research and clinical applications. While there are still limitations on biological complexity, standardization, and regulatory approval, technological advances and collaboration are enabling them to be more widely implemented. As further refinements occur, bioprinted organoids could become a central part of precision oncology, allowing more accurate, individualized, and effective treatments for skin cancer patients.
Author Contributions
Conceptualization, AKS, SS, and RKM.; methodology, SS, AKS, SDD, and RKM.; writing—original draft preparation, A.K.S.; writing—review and editing, SS, AKS, SDD, and RKM.; visualization, SS, AKS, SDD, and RKM.; management, SS, AKS, and RKM. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Roky, A.H.; et al. Overview of skin cancer types and prevalence rates across continents. Cancer Pathogenesis and Therapy 2025, 3, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Hasan, N.; et al. Skin cancer: understanding the journey of transformation from conventional to advanced treatment approaches. Mol Cancer 2023, 22, 168. [Google Scholar] [CrossRef] [PubMed]
- Khayyati Kohnehshahri, M.; et al. Current status of skin cancers with a focus on immunology and immunotherapy. Cancer Cell Int 2023, 23, 174. [Google Scholar] [CrossRef] [PubMed]
- Sorino, C.; et al. Immunotherapy in melanoma: advances, pitfalls, and future perspectives. Front Mol Biosci 2024, 11, 1403021. [Google Scholar] [CrossRef] [PubMed]
- He, G.; et al. Advancements in melanoma immunotherapy: the emergence of Extracellular Vesicle Vaccines. Cell Death Discovery 2024, 10, 374. [Google Scholar] [CrossRef]
- Kolathur, K.K.; et al. Molecular Susceptibility and Treatment Challenges in Melanoma. Cells 2024, 13. [Google Scholar] [CrossRef]
- Yu, H.; et al. Tumor microenvironment: Nurturing cancer cells for immunoevasion and druggable vulnerabilities for cancer immunotherapy. Cancer Letters 2025, 611, 217385. [Google Scholar] [CrossRef]
- Khalaf, K.; et al. Aspects of the Tumor Microenvironment Involved in Immune Resistance and Drug Resistance. Front Immunol 2021, 12, 656364. [Google Scholar] [CrossRef]
- Hu, Q.; et al. Extracellular matrix dynamics in tumor immunoregulation: from tumor microenvironment to immunotherapy. Journal of Hematology & Oncology 2025, 18, 65. [Google Scholar] [CrossRef]
- Almawash, S. Revolutionary Cancer Therapy for Personalization and Improved Efficacy: Strategies to Overcome Resistance to Immune Checkpoint Inhibitor Therapy. Cancers (Basel) 2025, 17. [Google Scholar] [CrossRef]
- Zielińska, M.K.; et al. Mechanisms of Resistance to Anti-PD-1 Immunotherapy in Melanoma and Strategies to Overcome It. Biomolecules 2025, 15, 269. [Google Scholar] [CrossRef]
- Huang, A.C.; Zappasodi, R. A decade of checkpoint blockade immunotherapy in melanoma: understanding the molecular basis for immune sensitivity and resistance. Nat Immunol 2022, 23, 660–670. [Google Scholar] [CrossRef] [PubMed]
- Shukla, A.K.; Gao, G.; Kim, B.S. Applications of 3D bioprinting technology in induced pluripotent stem cells-based tissue engineering. Micromachines 2022, 13, 155. [Google Scholar] [CrossRef]
- Shukla, A.; et al. In-bath Bioprinting of Pre-vascularized Skin Patches with Different Geometrical Patterns for Effective Skin Regeneration. 한국정밀공학회 2023, 677. [Google Scholar]
- Wang, X.-Y.; et al. Organoids as Tools for Investigating Skin Aging: Mechanisms, Applications, and Insights. Biomolecules 2024, 14, 1436. [Google Scholar] [CrossRef]
- Woo, Y.R.; et al. The Human Microbiota and Skin Cancer. International Journal of Molecular Sciences 2022, 23, 1813. [Google Scholar] [CrossRef]
- Dessinioti, C.; Stratigos, A.J. An Epidemiological Update on Indoor Tanning and the Risk of Skin Cancers. Current Oncology 2022, 29, 8886–8903. [Google Scholar] [CrossRef]
- Wehner, M.R.; et al. International Prevalence of Indoor Tanning: A Systematic Review and Meta-analysis. JAMA Dermatology 2014, 150, 390–400. [Google Scholar] [CrossRef]
- Rodriguez-Acevedo, A.J.; et al. Indoor tanning prevalence after the International Agency for Research on Cancer statement on carcinogenicity of artificial tanning devices: systematic review and meta-analysis. British Journal of Dermatology 2020, 182, 849–859. [Google Scholar] [CrossRef] [PubMed]
- Ahn, M.; et al. A Study on the Effect of Bioprinted Skin Patches with Various Vascular Patterns on Wound Healing. 한국정밀공학회 2024, 140. [Google Scholar]
- Kapałczyńska, M.; et al. 2D and 3D cell cultures - a comparison of different types of cancer cell cultures. Arch Med Sci 2018, 14, 910–919. [Google Scholar] [CrossRef] [PubMed]
- Arora, S.; et al. Spheroids in cancer research: Recent advances and opportunities. Journal of Drug Delivery Science and Technology 2024, 100, 106033. [Google Scholar] [CrossRef]
- Pipiya, V.V.; et al. Comparison of primary and passaged tumor cell cultures and their application in personalized medicine. Explor Target Antitumor Ther 2024, 5, 581–599. [Google Scholar] [CrossRef]
- Xu, H.; et al. Tumor-microenvironment-on-a-chip: the construction and application. Cell Commun Signal 2024, 22, 515. [Google Scholar] [CrossRef]
- Mun, S.; Lee, H.J.; Kim, P. Rebuilding the microenvironment of primary tumors in humans: a focus on stroma. Experimental & Molecular Medicine 2024, 56, 527–548. [Google Scholar] [CrossRef] [PubMed]
- Cristini, N.; et al. Exploring bone-tumor interactions through 3D in vitro models: Implications for primary and metastatic cancers. J Bone Oncol 2025, 53, 100698. [Google Scholar] [CrossRef]
- Tan, L.; et al. Safety assessment of drugs in pregnancy: An update of pharmacological models. Placenta 2025. [Google Scholar] [CrossRef]
- Budharaju, H.; Singh, R.K.; Kim, H.-W. Bioprinting for drug screening: A path toward reducing animal testing or redefining preclinical research? Bioactive Materials 2025, 51, 993–1017. [Google Scholar] [CrossRef]
- Nikolakopoulou, P.; et al. Recent progress in translational engineered in vitro models of the central nervous system. Brain 2020, 143, 3181–3213. [Google Scholar] [CrossRef] [PubMed]
- Khalil, A.S.; Jaenisch, R.; Mooney, D.J. Engineered tissues and strategies to overcome challenges in drug development. Adv Drug Deliv Rev 2020, 158, 116–139. [Google Scholar] [CrossRef]
- Mirshafiei, M.; et al. Advancements in tissue and organ 3D bioprinting: Current techniques, applications, and future perspectives. Materials & Design 2024, 240, 112853. [Google Scholar] [CrossRef]
- Ramadan, Q.; Zourob, M. 3D Bioprinting at the Frontier of Regenerative Medicine, Pharmaceutical, and Food Industries. Front Med Technol 2020, 2, 607648. [Google Scholar] [CrossRef] [PubMed]
- Sousa, A.C.; et al. Three-Dimensional Printing/Bioprinting and Cellular Therapies for Regenerative Medicine: Current Advances. Journal of Functional Biomaterials 2025, 16, 28. [Google Scholar] [CrossRef]
- Li, W.; et al. 3D Biomimetic Models to Reconstitute Tumor Microenvironment In Vitro: Spheroids, Organoids, and Tumor-on-a-Chip. Adv Healthc Mater 2023, 12, e2202609. [Google Scholar] [CrossRef]
- Liu, L.; et al. Cancer-on-a-chip for precision cancer medicine. Lab on a Chip 2025. [Google Scholar] [CrossRef] [PubMed]
- Cristini, N.; et al. Exploring bone-tumor interactions through 3D in vitro models: Implications for primary and metastatic cancers. Journal of Bone Oncology 2025, 53, 100698. [Google Scholar] [CrossRef]
- Shukla, A.K.; et al. Vascularization strategies for human skin tissue engineering via 3D bioprinting. International Journal of Bioprinting 2024, 10, 1727. [Google Scholar] [CrossRef]
- Zhou, Z.; Cong, L.; Cong, X. Patient-Derived Organoids in Precision Medicine: Drug Screening, Organoid-on-a-Chip and Living Organoid Biobank. Front Oncol 2021, 11, 762184. [Google Scholar] [CrossRef]
- Liu, S.; Jin, P. Advances and Challenges in 3D Bioprinted Cancer Models: Opportunities for Personalized Medicine and Tissue Engineering. Polymers 2025, 17, 948. [Google Scholar] [CrossRef]
- Zambrano-Román, M.; et al. Non-Melanoma Skin Cancer: A Genetic Update and Future Perspectives. Cancers 2022, 14, 2371. [Google Scholar] [CrossRef]
- Zhou, L.; et al. Global, regional, and national trends in the burden of melanoma and non-melanoma skin cancer: insights from the global burden of disease study 1990–2021. Scientific Reports 2025, 15, 5996. [Google Scholar] [CrossRef]
- Lang, C.M.R.; et al. Wnt Signaling Pathways in Keratinocyte Carcinomas. Cancers (Basel) 2019, 11. [Google Scholar] [CrossRef]
- Riihilä, P.; Nissinen, L.; Kähäri, V.M. Matrix metalloproteinases in keratinocyte carcinomas. Exp Dermatol 2021, 30, 50–61. [Google Scholar] [CrossRef]
- Dainese-Marque, O.; et al. Contribution of Keratinocytes in Skin Cancer Initiation and Progression. International Journal of Molecular Sciences 2024, 25, 8813. [Google Scholar] [CrossRef]
- Shukla, A.K.; et al. Advancement in cancer vasculogenesis modeling through 3D Bioprinting Technology. Biomimetics 2024, 9, 306. [Google Scholar] [CrossRef]
- Manduca, N.; et al. 3D cancer models: One step closer to in vitro human studies. Front Immunol 2023, 14, 1175503. [Google Scholar] [CrossRef] [PubMed]
- Chaves, P.; et al. Preclinical models in head and neck squamous cell carcinoma. British Journal of Cancer 2023, 128, 1819–1827. [Google Scholar] [CrossRef] [PubMed]
- Ionita, I.; et al. Experimental Models for Rare Melanoma Research—The Niche That Needs to Be Addressed. Bioengineering 2023, 10, 673. [Google Scholar] [CrossRef]
- Li, Z.; et al. Application of Animal Models in Cancer Research: Recent Progress and Future Prospects. Cancer Manag Res 2021, 13, 2455–2475. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; et al. In vitro and in vivo experimental models for cancer immunotherapy study. Current Research in Biotechnology 2024, 7, 100210. [Google Scholar] [CrossRef]
- Wakefield, L.; Agarwal, S.; Tanner, K. Preclinical models for drug discovery for metastatic disease. Cell 2023, 186, 1792–1813. [Google Scholar] [CrossRef]
- Liu, Y.; et al. Patient-derived xenograft models in cancer therapy: technologies and applications. Signal Transduct Target Ther 2023, 8, 160. [Google Scholar] [CrossRef]
- Jin, J.; et al. Challenges and Prospects of Patient-Derived Xenografts for Cancer Research. Cancers (Basel) 2023, 15. [Google Scholar] [CrossRef]
- Moro, M.; et al. Patient-Derived Xenografts of Non Small Cell Lung Cancer: Resurgence of an Old Model for Investigation of Modern Concepts of Tailored Therapy and Cancer Stem Cells. BioMed Research International 2012, 2012, 568567. [Google Scholar] [CrossRef] [PubMed]
- de Visser, K.E.; Joyce, J.A. The evolving tumor microenvironment: From cancer initiation to metastatic outgrowth. Cancer Cell 2023, 41, 374–403. [Google Scholar] [CrossRef]
- Biray Avci, C.; et al. Tumor microenvironment and cancer metastasis: molecular mechanisms and therapeutic implications. Front Pharmacol 2024, 15, 1442888. [Google Scholar] [CrossRef]
- Wright, K.; et al. Cancer-Associated Fibroblasts: Master Tumor Microenvironment Modifiers. Cancers (Basel) 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Lv, K.; He, T. Cancer-associated fibroblasts: heterogeneity, tumorigenicity and therapeutic targets. Mol Biomed 2024, 5, 70. [Google Scholar] [CrossRef]
- Finger, A.-M.; et al. Tissue mechanics in tumor heterogeneity and aggression. Trends in Cancer 2025. [Google Scholar] [CrossRef]
- Fiori, M.E.; et al. Cancer-associated fibroblasts as abettors of tumor progression at the crossroads of EMT and therapy resistance. Mol Cancer 2019, 18, 70. [Google Scholar] [CrossRef] [PubMed]
- Ahn, M.; et al. 3D Bioprinting-Assisted Engineering of Stem Cell-Laden Hybrid Biopatches With Distinct Geometric Patterns Considering the Mechanical Characteristics of Regular and Irregular Connective Tissues. Advanced Healthcare Materials 2025, 2502763. [Google Scholar] [CrossRef] [PubMed]
- Augustine, R.; et al. 3D Bioprinted cancer models: Revolutionizing personalized cancer therapy. Transl Oncol 2021, 14, 101015. [Google Scholar] [CrossRef] [PubMed]
- Mazzaglia, C.; Huang, Y.Y.S.; Shields, J.D. Advancing tumor microenvironment and lymphoid tissue research through 3D bioprinting and biofabrication. Advanced Drug Delivery Reviews 2025, 217, 115485. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; et al. Advances in 3D skin bioprinting for wound healing and disease modeling. Regen Biomater 2023, 10, rbac105. [Google Scholar] [CrossRef]
- Gu, Z.; et al. Development of 3D bioprinting: From printing methods to biomedical applications. Asian Journal of Pharmaceutical Sciences 2020, 15, 529–557. [Google Scholar] [CrossRef]
- Budharaju, H.; Sundaramurthi, D.; Sethuraman, S. Embedded 3D bioprinting – An emerging strategy to fabricate biomimetic & large vascularized tissue constructs. Bioactive Materials 2024, 32, 356–384. [Google Scholar] [CrossRef]
- Gungor-Ozkerim, P.S.; et al. Bioinks for 3D bioprinting: an overview. Biomater Sci 2018, 6, 915–946. [Google Scholar] [CrossRef]
- Fernandes, S.; et al. 3D Bioprinting: An Enabling Technology to Understand Melanoma. Cancers (Basel) 2022, 14. [Google Scholar] [CrossRef]
- Parodi, I.; et al. 3D Bioprinting as a Powerful Technique for Recreating the Tumor Microenvironment. Gels 2023, 9, 482. [Google Scholar] [CrossRef]
- Lee, J.; Koehler, K.R. Skin organoids: A new human model for developmental and translational research. Exp Dermatol 2021, 30, 613–620. [Google Scholar] [CrossRef]
- Teertam, S.K.; Setaluri, V.; Ayuso, J.M. Advances in Microengineered Platforms for Skin Research. JID Innovations 2025, 5, 100315. [Google Scholar] [CrossRef] [PubMed]
- Hong, Z.X.; et al. Bioengineered skin organoids: from development to applications. Mil Med Res 2023, 10, 40. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; et al. Converging bioprinting and organoids to better recapitulate the tumor microenvironment. Trends in Biotechnology 2024, 42, 648–663. [Google Scholar] [CrossRef]
- Hwang, D.G.; Choi, Y.M.; Jang, J. 3D Bioprinting-Based Vascularized Tissue Models Mimicking Tissue-Specific Architecture and Pathophysiology for in vitro Studies. Front Bioeng Biotechnol 2021, 9, 685507. [Google Scholar] [CrossRef]
- Zhuang, P.; et al. Using Spheroids as Building Blocks Towards 3D Bioprinting of Tumor Microenvironment. Int J Bioprint 2021, 7, 444. [Google Scholar] [CrossRef]
- Zuo, J.; et al. High-throughput solutions in tumor organoids: from culture to drug screening. Stem Cells 2025, 43. [Google Scholar] [CrossRef]
- Shao, Y.; et al. Biomaterial-assisted organoid technology for disease modeling and drug screening. Materials Today Bio 2025, 30, 101438. [Google Scholar] [CrossRef]
- Lv, J.; et al. Construction of tumor organoids and their application to cancer research and therapy. Theranostics 2024, 14, 1101–1125. [Google Scholar] [CrossRef]
- Dai, R.; et al. 3D bioprinting platform development for high-throughput cancer organoid models construction and drug evaluation. Biofabrication 2024, 16. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; et al. AI-driven 3D bioprinting for regenerative medicine: From bench to bedside. Bioactive Materials 2025, 45, 201–230. [Google Scholar] [CrossRef] [PubMed]
- Tebon, P.J.; et al. Drug screening at single-organoid resolution via bioprinting and interferometry. Nature Communications 2023, 14, 3168. [Google Scholar] [CrossRef]
- Shukla, A.K.; et al. Exploring the Angiogenic Potential of Skin Patches with Endothelial Cell Patterns Fabricated via In-Bath 3D Bioprinting Using Light-Activated Bioink for Enhanced Wound Healing. Biomaterials 2025, 123575. [Google Scholar] [CrossRef]
- Morais, A.S.; et al. Organ-on-a-Chip: Ubi sumus? Fundamentals and Design Aspects. Pharmaceutics 2024, 16. [Google Scholar] [CrossRef]
- Ahmed, T. Organ-on-a-chip microengineering for bio-mimicking disease models and revolutionizing drug discovery. Biosensors and Bioelectronics X 2022, 11, 100194. [Google Scholar] [CrossRef]
- Regmi, S.; et al. Applications of Microfluidics and Organ-on-a-Chip in Cancer Research. Biosensors (Basel) 2022, 12. [Google Scholar] [CrossRef]
- Mierke, C.T. Bioprinting of Cells, Organoids and Organs-on-a-Chip Together with Hydrogels Improves Structural and Mechanical Cues. Cells 2024, 13, 1638. [Google Scholar] [CrossRef] [PubMed]
- Shukla, S.; et al. Emerging Molecular and Clinical Challenges in Managing Lung Cancer Treatment during the Covid-19 Infection. Journal of Cancer and Tumor International 2024, 14, 143–161. [Google Scholar] [CrossRef]
- Barros, N.R.; et al. A human skin-on-a-chip platform for microneedling-driven skin cancer treatment. Materials Today Bio 2025, 30, 101399. [Google Scholar] [CrossRef] [PubMed]
- Hsiung, N.; et al. Organoid-based tissue engineering for advanced tissue repair and reconstruction. Materials Today Bio 2025, 33, 102093. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; et al. Bridging the organoid translational gap: integrating standardization and micropatterning for drug screening in clinical and pharmaceutical medicine. Life Med 2024, 3, lnae016. [Google Scholar] [CrossRef]
- Roberto de Barros, N.; et al. Engineered organoids for biomedical applications. Adv Drug Deliv Rev 2023, 203, 115142. [Google Scholar] [CrossRef]
- Kim, D.; et al. Scalable production of uniform and mature organoids in a 3D geometrically-engineered permeable membrane. Nature Communications 2024, 15, 9420. [Google Scholar] [CrossRef]
- Hwangbo, H.; et al. Tumor-on-a-chip models combined with mini-tissues or organoids for engineering tumor tissues. Theranostics 2024, 14, 33–55. [Google Scholar] [CrossRef] [PubMed]
- Bosmans, C.; et al. Towards single-cell bioprinting: micropatterning tools for organ-on-chip development. Trends in Biotechnology 2024, 42, 739–759. [Google Scholar] [CrossRef] [PubMed]
- Rahmani Dabbagh, S.; et al. 3D bioprinted organ-on-chips. Aggregate 2023, 4, e197. [Google Scholar] [CrossRef]
- Gaebler, D.; Hachey, S.J.; Hughes, C.C.W. Improving tumor microenvironment assessment in chip systems through next-generation technology integration. Front Bioeng Biotechnol 2024, 12, 1462293. [Google Scholar] [CrossRef] [PubMed]
- Giannitelli, S.M.; et al. On-chip recapitulation of the tumor microenvironment: A decade of progress. Biomaterials 2024, 306, 122482. [Google Scholar] [CrossRef]
- Li, C.; et al. On-chip modeling of tumor evolution: Advances, challenges and opportunities. Materials Today Bio 2023, 21, 100724. [Google Scholar] [CrossRef]
- Thenuwara, G.; et al. Biosensor-Enhanced Organ-on-a-Chip Models for Investigating Glioblastoma Tumor Microenvironment Dynamics. Sensors 2024, 24, 2865. [Google Scholar] [CrossRef]
- Moses, S.R.; et al. Vessel-on-a-chip models for studying microvascular physiology, transport, and function in vitro. Am J Physiol Cell Physiol 2021, 320, C92–C105. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.; et al. Revolutionizing Drug Discovery: The Impact of Distinct Designs and Biosensor Integration in Microfluidics-Based Organ-on-a-Chip Technology. Biosensors (Basel) 2024, 14. [Google Scholar] [CrossRef]
- Zhao, P.; et al. Engineering microneedles for biosensing and drug delivery. Bioactive Materials 2025, 52, 36–59. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, A.R.; et al. Organ-on-chip platforms for nanoparticle toxicity and efficacy assessment: Advancing beyond traditional in vitro and in vivo models. Materials Today Bio 2025, 33, 102053. [Google Scholar] [CrossRef]
- An, L.; Liu, Y.; Liu, Y. Organ-on-a-Chip Applications in Microfluidic Platforms. Micromachines 2025, 16, 201. [Google Scholar] [CrossRef]
- Wu, D.; et al. The blood–brain barrier: Structure, regulation and drug delivery. Signal Transduction and Targeted Therapy 2023, 8, 217. [Google Scholar] [CrossRef]
- Shukla, S.; et al. Long-lasting Response of Human Circulating T-follicular Helper Cells (cTfh) To Post SARS-CoV-2 mRNA Immunization. Asian Journal of Immunology 2024, 7, 228–246. [Google Scholar] [CrossRef]
- Ahn, M.; et al. 3D biofabrication of diseased human skin models in vitro. Biomaterials Research 2023, 27, 80. [Google Scholar] [CrossRef]
- Yao, Q.; et al. Organoids: development and applications in disease models, drug discovery, precision medicine, and regenerative medicine. MedComm (2020) 2024, 5, e735. [Google Scholar] [CrossRef]
- Heinzelmann, E.; et al. iPSC-derived and Patient-Derived Organoids: Applications and challenges in scalability and reproducibility as pre-clinical models. Current Research in Toxicology 2024, 7, 100197. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; et al. Harnessing the power of artificial intelligence for human living organoid research. Bioactive Materials 2024, 42, 140–164. [Google Scholar] [CrossRef]
- Heinrich, M.A.; et al. Translating complexity and heterogeneity of pancreatic tumor: 3D in vitro to in vivo models. Advanced Drug Delivery Reviews 2021, 174, 265–293. [Google Scholar] [CrossRef] [PubMed]
- Phan, N.; et al. A simple high-throughput approach identifies actionable drug sensitivities in patient-derived tumor organoids. Commun Biol 2019, 2, 78. [Google Scholar] [CrossRef] [PubMed]
- Skala, M.C.; Deming, D.A.; Kratz, J.D. Technologies to Assess Drug Response and Heterogeneity in Patient-Derived Cancer Organoids. Annu Rev Biomed Eng 2022, 24, 157–177. [Google Scholar] [CrossRef]
- Al-Kabani, A.; et al. Exploring Experimental Models of Colorectal Cancer: A Critical Appraisal from 2D Cell Systems to Organoids, Humanized Mouse Avatars, Organ-on-Chip, CRISPR Engineering, and AI-Driven Platforms—Challenges and Opportunities for Translational Precision Oncology. Cancers 2025, 17, 2163. [Google Scholar]
- Makesh, K.Y.; et al. A Concise Review of Organoid Tissue Engineering: Regenerative Applications and Precision Medicine. Organoids 2025, 4, 16. [Google Scholar] [CrossRef]
- Ho, D.; et al. Enabling Technologies for Personalized and Precision Medicine. Trends Biotechnol 2020, 38, 497–518. [Google Scholar] [CrossRef]
- Vitorino, R. Transforming Clinical Research: The Power of High-Throughput Omics Integration. Proteomes 2024, 12, 25. [Google Scholar] [CrossRef]
- Li, P.; et al. Novel research model for in vitro immunotherapy: co-culturing tumor organoids with peripheral blood mononuclear cells. Cancer Cell Int 2024, 24, 438. [Google Scholar] [CrossRef]
- Mackenzie, N.J.; et al. Modelling the tumor immune microenvironment for precision immunotherapy. Clinical & Translational Immunology 2022, 11, e1400. [Google Scholar] [CrossRef]
- Noorintan, S.T.; Angelius, C.; Torizal, F.G. Organoid Models in Cancer Immunotherapy: Bioengineering Approach for Personalized Treatment. Immuno 2024, 4, 312–324. [Google Scholar] [CrossRef]
- Cui, X.; et al. Advanced tumor organoid bioprinting strategy for oncology research. Materials Today Bio 2024, 28, 101198. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; et al. 3D Bioprinting in Cancer Modeling and Biomedicine: From Print Categories to Biological Applications. ACS Omega 2024, 9, 44076–44100. [Google Scholar] [CrossRef]
- Yang, Q.; et al. Flourishing tumor organoids: History, emerging technology, and application. Bioeng Transl Med 2023, 8, e10559. [Google Scholar] [CrossRef]
- Mathur, V.; et al. Innovative bioinks for 3D bioprinting: Exploring technological potential and regulatory challenges. J Tissue Eng 2025, 16, 20417314241308022. [Google Scholar] [CrossRef]
- Duarte, A.C.; et al. Animal-derived products in science and current alternatives. Biomaterials Advances 2023, 151, 213428. [Google Scholar] [CrossRef]
- Bernatoniene, J.; et al. The Future of Medicine: How 3D Printing Is Transforming Pharmaceuticals. Pharmaceutics 2025, 17, 390. [Google Scholar] [CrossRef]
- Flach, E.H.; et al. Fibroblasts contribute to melanoma tumor growth and drug resistance. Molecular pharmaceutics 2011, 8, 2039–2049. [Google Scholar] [CrossRef]
- Shoval, H.; et al. Tumor cells and their crosstalk with endothelial cells in 3D spheroids. Scientific reports 2017, 7, 10428. [Google Scholar] [CrossRef] [PubMed]
- Klicks, J.; et al. A novel spheroid-based co-culture model mimics loss of keratinocyte differentiation, melanoma cell invasion, and drug-induced selection of ABCB5-expressing cells. BMC cancer 2019, 19, 402. [Google Scholar] [CrossRef]
- Neal, J.T.; et al. Organoid modeling of the tumor immune microenvironment. Cell 2018, 175, 1972–1988. [Google Scholar] [CrossRef] [PubMed]
- Powley, I.R.; et al. Patient-derived explants (PDEs) as a powerful preclinical platform for anti-cancer drug and biomarker discovery. British journal of cancer 2020, 122, 735–744. [Google Scholar] [CrossRef]
- Yin, Q.; et al. Nanoparticle-enabled innate immune stimulation activates endogenous tumor-infiltrating T cells with broad antigen specificities. Proceedings of the National Academy of Sciences 2021, 118, e2016168118. [Google Scholar] [CrossRef] [PubMed]
- Votanopoulos, K.I.; et al. Model of patient-specific immune-enhanced organoids for immunotherapy screening: feasibility study. Annals of surgical oncology 2020, 27, 1956–1967. [Google Scholar] [CrossRef]
- Troiani, T.; et al. Alternative macrophage polarisation associated with resistance to anti-PD1 blockade is possibly supported by the splicing of FKBP51 immunophilin in melanoma patients. British Journal of Cancer 2020, 122, 1782–1790. [Google Scholar] [CrossRef]
- Haridas, P.; et al. Quantitative comparison of the spreading and invasion of radial growth phase and metastatic melanoma cells in a three-dimensional human skin equivalent model. PeerJ 2017, 5, e3754. [Google Scholar] [CrossRef]
- Vörsmann, H.; et al. Development of a human three-dimensional organotypic skin-melanoma spheroid model for in vitro drug testing. Cell death & disease 2013, 4, e719. [Google Scholar]
- Hill, D.S.; et al. A novel fully humanized 3D skin equivalent to model early melanoma invasion. Molecular cancer therapeutics 2015, 14, 2665–2673. [Google Scholar] [CrossRef] [PubMed]
- Bourland, J.; Fradette, J.; Auger, F.A. Tissue-engineered 3D melanoma model with blood and lymphatic capillaries for drug development. Scientific reports 2018, 8, 13191. [Google Scholar] [CrossRef]
- Shin, J.U.; et al. Recapitulating T cell infiltration in 3D psoriatic skin models for patient-specific drug testing. Scientific reports 2020, 10, 4123. [Google Scholar] [CrossRef]
- Wallmeyer, L.; et al. TSLP is a direct trigger for T cell migration in filaggrin-deficient skin equivalents. Scientific reports 2017, 7, 774. [Google Scholar] [CrossRef] [PubMed]
- Kosten, I.J.; et al. MUTZ-3 derived Langerhans cells in human skin equivalents show differential migration and phenotypic plasticity after allergen or irritant exposure. Toxicology and applied pharmacology 2015, 287, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Van Den Bogaard, E.H.; et al. Crosstalk between keratinocytes and T cells in a 3D microenvironment: a model to study inflammatory skin diseases. Journal of Investigative Dermatology 2014, 134, 719–727. [Google Scholar] [CrossRef]
- Lègues, M.; et al. The world’s first 3D bioprinted immune skin model suitable for screening drugs and ingredients for normal and inflamed skin. IFSCC Magazine 2020, 4, 8–12. [Google Scholar]
- Jara, C.P.; et al. Demonstration of re-epithelialization in a bioprinted human skin equivalent wound model. Bioprinting 2021, 24, e00102. [Google Scholar] [CrossRef]
- Michielon, E.; et al. Micro-environmental cross-talk in an organotypic human melanoma-in-skin model directs M2-like monocyte differentiation via IL-10. Cancer Immunology Immunotherapy 2020, 69, 2319–2331. [Google Scholar] [CrossRef]
- Michielon, E.; et al. A reconstructed human melanoma-in-skin model to study immune modulatory and angiogenic mechanisms facilitating initial melanoma growth and invasion. Cancers 2023, 15, 2849. [Google Scholar] [CrossRef] [PubMed]
- Di Blasio, S.; et al. The tumour microenvironment shapes dendritic cell plasticity in a human organotypic melanoma culture. Nature communications 2020, 11, 2749. [Google Scholar] [CrossRef]
- Kaur, A.; et al. Remodeling of the collagen matrix in aging skin promotes melanoma metastasis and affects immune cell motility. Cancer discovery 2019, 9, 64–81. [Google Scholar] [CrossRef]
- Ayuso, J.M.; et al. Microfluidic model with air-walls reveals fibroblasts and keratinocytes modulate melanoma cell phenotype, migration, and metabolism. Lab on a Chip 2021, 21, 1139–1149. [Google Scholar] [CrossRef] [PubMed]
- Ren, X.; et al. Investigations on T cell transmigration in a human skin-on-chip (SoC) model. Lab on a Chip 2021, 21, 1527–1539. [Google Scholar] [CrossRef] [PubMed]
- Ramadan, Q.; Ting, F.C.W. In vitro micro-physiological immune-competent model of the human skin. Lab on a Chip 2016, 16, 1899–1908. [Google Scholar] [CrossRef]
- Kwak, B.S.; et al. Microfluidic skin chip with vasculature for recapitulating the immune response of the skin tissue. Biotechnology and Bioengineering 2020, 117, 1853–1863. [Google Scholar] [CrossRef]
- Jenkins, R.W.; et al. Ex vivo profiling of PD-1 blockade using organotypic tumor spheroids. Cancer discovery 2018, 8, 196–215. [Google Scholar] [CrossRef]
- Sun, Y.; et al. Targeting TBK1 to overcome resistance to cancer immunotherapy. Nature 2023, 615, 158–167. [Google Scholar] [CrossRef]
- Espinoza-Sanchez, N.A.; Goette, M. Role of cell surface proteoglycans in cancer immunotherapy. in Seminars in cancer biology. 2020. Elsevier.
- Chen, M.B.; et al. Inflamed neutrophils sequestered at entrapped tumor cells via chemotactic confinement promote tumor cell extravasation. Proceedings of the National Academy of Sciences 2018, 115, 7022–7027. [Google Scholar] [CrossRef] [PubMed]
- Mendes, M.; et al. Organ-on-a-chip: Quo vademus? Applications and regulatory status. Colloids and Surfaces B: Biointerfaces 2025, 249, 114507. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; et al. Integrated applications of microfluidics, organoids, and 3D bioprinting in in vitro 3D biomimetic models. IJB 2025, 11. [Google Scholar] [CrossRef]
- Deng, S.; et al. Organ-on-a-chip meets artificial intelligence in drug evaluation. Theranostics 2023, 13, 4526–4558. [Google Scholar]
- Wang, X.; Lin, D.; Feng, N. Harnessing organoid technology in urological cancer: advances and applications in urinary system tumors. World J Surg Oncol 2025, 23, 295. [Google Scholar]
- Li, Q.; et al. Signaling pathways involved in colorectal cancer: pathogenesis and targeted therapy. Signal Transduction and Targeted Therapy 2024, 9, 266. [Google Scholar] [CrossRef]
Figure 1.
Structural and mechanistic insights into skin tissue and UV-induced skin cancer development. (A) Illustration of the anatomical structure of skin tissue, depicting its key layers and cellular components involved in maintaining skin integrity and function [15]. (B) Conceptual framework outlining how ultraviolet (UV) exposure contributes to skin cancer through disruption of the skin microbiome and skin–gut axis. UV radiation compromises the skin barrier and alters the balance of commensal skin microbes. These changes, along with the release of damage-associated molecular patterns (DAMPs), pathogen-associated molecular patterns (PAMPs), and microbial toxins, can lead to persistent inflammation and DNA damage. These pathological events promote tumor initiation and progression. Immune cells—such as cytotoxic CD8+ T cells, regulatory T cells, and tumor-associated macrophages—alongside their secreted cytokines and chemokines, play crucial roles in shaping the immunosuppressive and pro-inflammatory tumor microenvironment. Additionally, microbial metabolites, inflammatory mediators, and signaling molecules originating from the gut microbiota can circulate systemically, influencing skin tumor development and progression from a distance, highlighting the interplay between the gut and skin in cancer pathogenesis [16]. (C) Aggregated data from published meta-analyses presenting the percentage of individuals who have ever used indoor ultraviolet radiation (UVR) tanning devices, reflecting lifetime exposure trends [17]. (D) Compiled prevalence rates from meta-analyses reporting past-year usage of indoor UVR tanning, emphasizing recent behavioral patterns related to artificial UV exposure and associated cancer risks [17]. This section is adapted under the Creative Commons Attribution 4.0 (CC BY 4.0) license.
Figure 1.
Structural and mechanistic insights into skin tissue and UV-induced skin cancer development. (A) Illustration of the anatomical structure of skin tissue, depicting its key layers and cellular components involved in maintaining skin integrity and function [15]. (B) Conceptual framework outlining how ultraviolet (UV) exposure contributes to skin cancer through disruption of the skin microbiome and skin–gut axis. UV radiation compromises the skin barrier and alters the balance of commensal skin microbes. These changes, along with the release of damage-associated molecular patterns (DAMPs), pathogen-associated molecular patterns (PAMPs), and microbial toxins, can lead to persistent inflammation and DNA damage. These pathological events promote tumor initiation and progression. Immune cells—such as cytotoxic CD8+ T cells, regulatory T cells, and tumor-associated macrophages—alongside their secreted cytokines and chemokines, play crucial roles in shaping the immunosuppressive and pro-inflammatory tumor microenvironment. Additionally, microbial metabolites, inflammatory mediators, and signaling molecules originating from the gut microbiota can circulate systemically, influencing skin tumor development and progression from a distance, highlighting the interplay between the gut and skin in cancer pathogenesis [16]. (C) Aggregated data from published meta-analyses presenting the percentage of individuals who have ever used indoor ultraviolet radiation (UVR) tanning devices, reflecting lifetime exposure trends [17]. (D) Compiled prevalence rates from meta-analyses reporting past-year usage of indoor UVR tanning, emphasizing recent behavioral patterns related to artificial UV exposure and associated cancer risks [17]. This section is adapted under the Creative Commons Attribution 4.0 (CC BY 4.0) license.
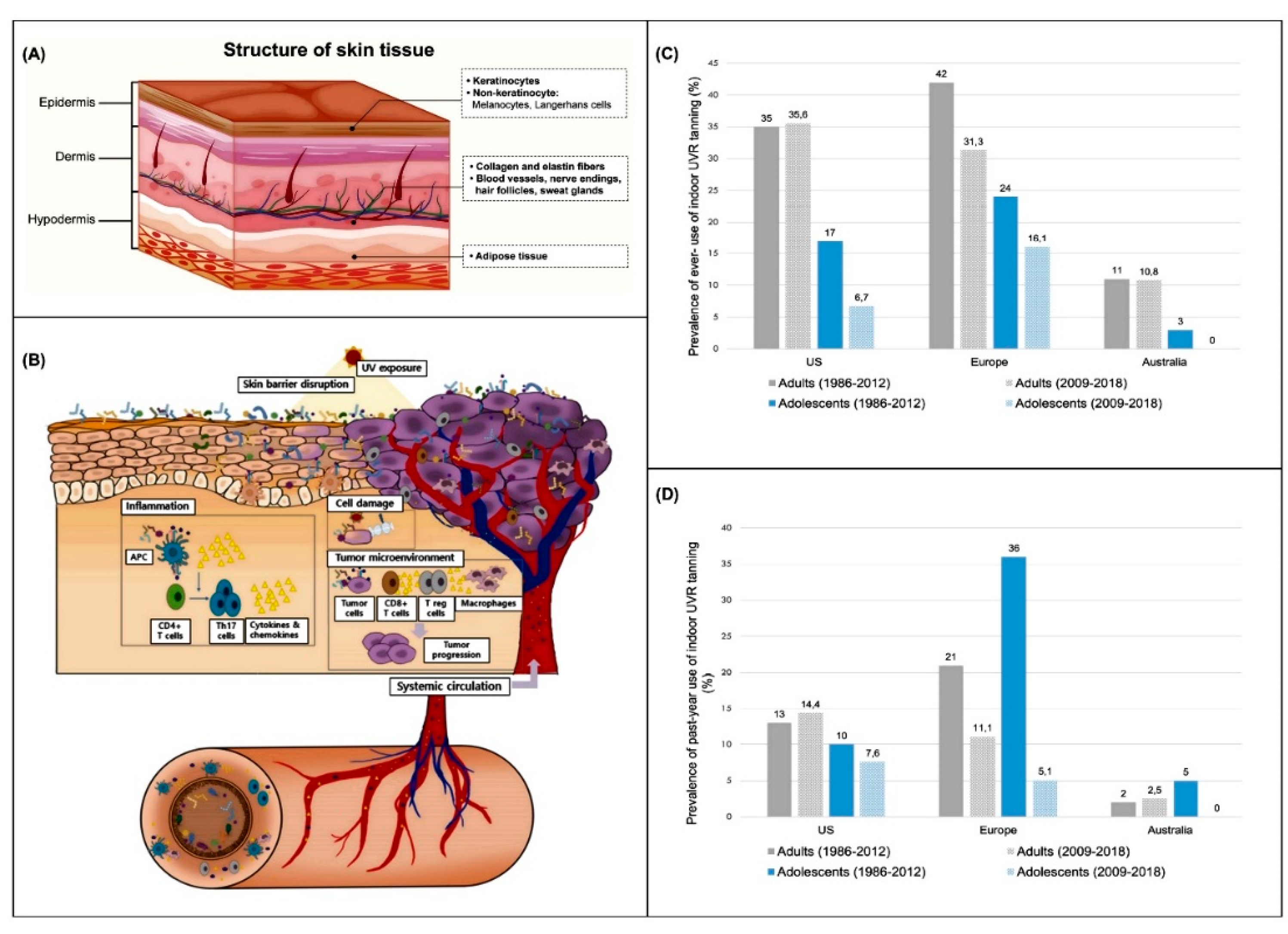
Figure 2.
The process of 3D bioprinting human-equivalent skin cancer models using organ-on-chips for skin cancer detection.
Figure 2.
The process of 3D bioprinting human-equivalent skin cancer models using organ-on-chips for skin cancer detection.
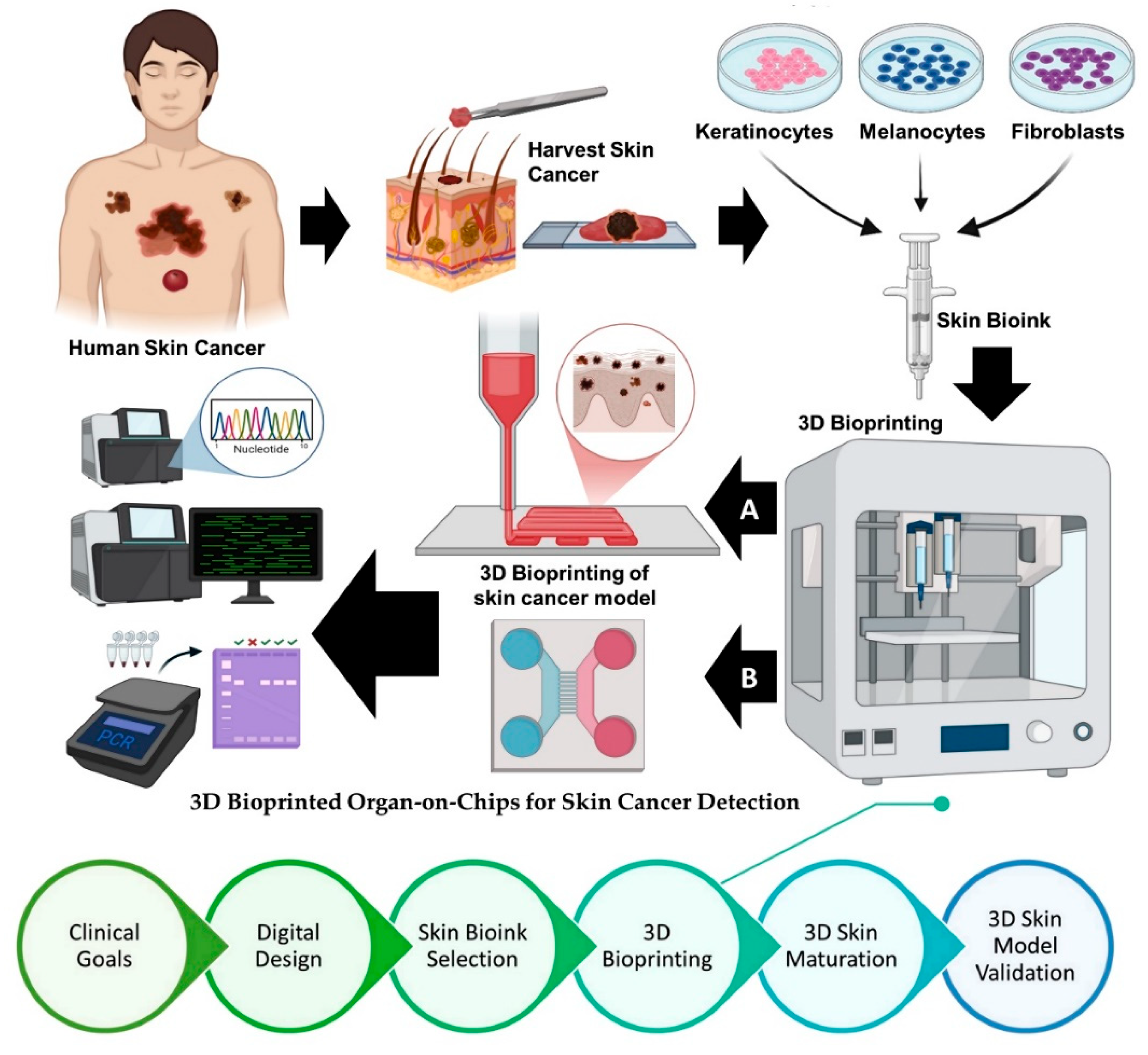
Figure 4.
Comprehensive overview of the development, characterization, and therapeutic application of a 3D skin cancer-on-a-chip platform integrated with microneedles (MNs) for the detection and delivery of drugs. (A) Skin-on-a-chip setup and application strategy. (a) Schematic illustration of the 3D skin-on-a-chip setup, showing the PDMS chip, porous membrane, and skin-media chamber interface. Cross-sectional schematic views depict the skin model architecture and microneedle (MN) application for targeted drug delivery. (b) Air-liquid interface (ALI) culture method enabling stratified epidermal formation by keratinocyte differentiation. (B) ALI-cultured epidermal layers and cellular morphology. Confocal imaging reveals the 3D dermal structure. (C) Epidermal stratification and maturation. Confocal images of epidermal layers on days 10 (a) and 14 (b), showing nuclei (blue), actin (red), α-SMA (green), and pan-cytokeratin (yellow). (D) Structural and temporal development of skin layers. (a) Timeline of layered skin-on-a-chip formation. (b) Quantification of epidermal and dermal layer thicknesses. (E) Marker expression in skin layers. Confocal images and intensity profiles of (a) Keratin 14 and Keratin 19, (b) Filaggrin and Keratin 10, (c) Collagen I and Fibronectin. (d) Comparative H&E staining of native human skin and engineered skin tissue. Scale bars: 100 μm. (F) Spatial expression profiles of epidermal/dermal markers. Distribution and intensity of FLG (stratum corneum), K14 (stratum basale), and K10 (stratum lucidum–spinosum) across skin depths. (G) Skin cancer-on-a-chip model with metastatic melanoma. (a) Schematic showing melanoma cell layer incorporation. (b) Live/dead staining confirms melanoma invasion into the media channel after 24 h ALI culture. (c) 3D confocal image of melanoma within the model. Scale bars: 200 μm. (H) Characterization and drug release from DOX-loaded MNs. (a) Confocal images of MNs (tilted, side, and 3D views). (b) Stress-strain analysis, (c) compressive modulus with varied photo-crosslinking durations, (d) cumulative DOX release at varying concentrations. (e) Schematic of DOX-loaded MN application on skin cancer-on-a-chip. Representative cross-sectional images of MN insertion: (f) single needle and (g) MN array targeting the melanoma layer. Scale bars: 200 μm. (I) Transdermal DOX delivery and therapeutic response. Confocal cross-sections showing (a) perfusion-based delivery, (b) control MNs without DOX, (c) DOX-loaded MNs insertion. Quantitative cell death profiles validate MN efficacy. (d) Z-stacked cross-sections of melanoma with (right) and without (left) DOX treatment. Scale bars: 200 μm [88]. This section is adapted under the Creative Commons Attribution 4.0 (CC BY 4.0) license.
Figure 4.
Comprehensive overview of the development, characterization, and therapeutic application of a 3D skin cancer-on-a-chip platform integrated with microneedles (MNs) for the detection and delivery of drugs. (A) Skin-on-a-chip setup and application strategy. (a) Schematic illustration of the 3D skin-on-a-chip setup, showing the PDMS chip, porous membrane, and skin-media chamber interface. Cross-sectional schematic views depict the skin model architecture and microneedle (MN) application for targeted drug delivery. (b) Air-liquid interface (ALI) culture method enabling stratified epidermal formation by keratinocyte differentiation. (B) ALI-cultured epidermal layers and cellular morphology. Confocal imaging reveals the 3D dermal structure. (C) Epidermal stratification and maturation. Confocal images of epidermal layers on days 10 (a) and 14 (b), showing nuclei (blue), actin (red), α-SMA (green), and pan-cytokeratin (yellow). (D) Structural and temporal development of skin layers. (a) Timeline of layered skin-on-a-chip formation. (b) Quantification of epidermal and dermal layer thicknesses. (E) Marker expression in skin layers. Confocal images and intensity profiles of (a) Keratin 14 and Keratin 19, (b) Filaggrin and Keratin 10, (c) Collagen I and Fibronectin. (d) Comparative H&E staining of native human skin and engineered skin tissue. Scale bars: 100 μm. (F) Spatial expression profiles of epidermal/dermal markers. Distribution and intensity of FLG (stratum corneum), K14 (stratum basale), and K10 (stratum lucidum–spinosum) across skin depths. (G) Skin cancer-on-a-chip model with metastatic melanoma. (a) Schematic showing melanoma cell layer incorporation. (b) Live/dead staining confirms melanoma invasion into the media channel after 24 h ALI culture. (c) 3D confocal image of melanoma within the model. Scale bars: 200 μm. (H) Characterization and drug release from DOX-loaded MNs. (a) Confocal images of MNs (tilted, side, and 3D views). (b) Stress-strain analysis, (c) compressive modulus with varied photo-crosslinking durations, (d) cumulative DOX release at varying concentrations. (e) Schematic of DOX-loaded MN application on skin cancer-on-a-chip. Representative cross-sectional images of MN insertion: (f) single needle and (g) MN array targeting the melanoma layer. Scale bars: 200 μm. (I) Transdermal DOX delivery and therapeutic response. Confocal cross-sections showing (a) perfusion-based delivery, (b) control MNs without DOX, (c) DOX-loaded MNs insertion. Quantitative cell death profiles validate MN efficacy. (d) Z-stacked cross-sections of melanoma with (right) and without (left) DOX treatment. Scale bars: 200 μm [88]. This section is adapted under the Creative Commons Attribution 4.0 (CC BY 4.0) license.
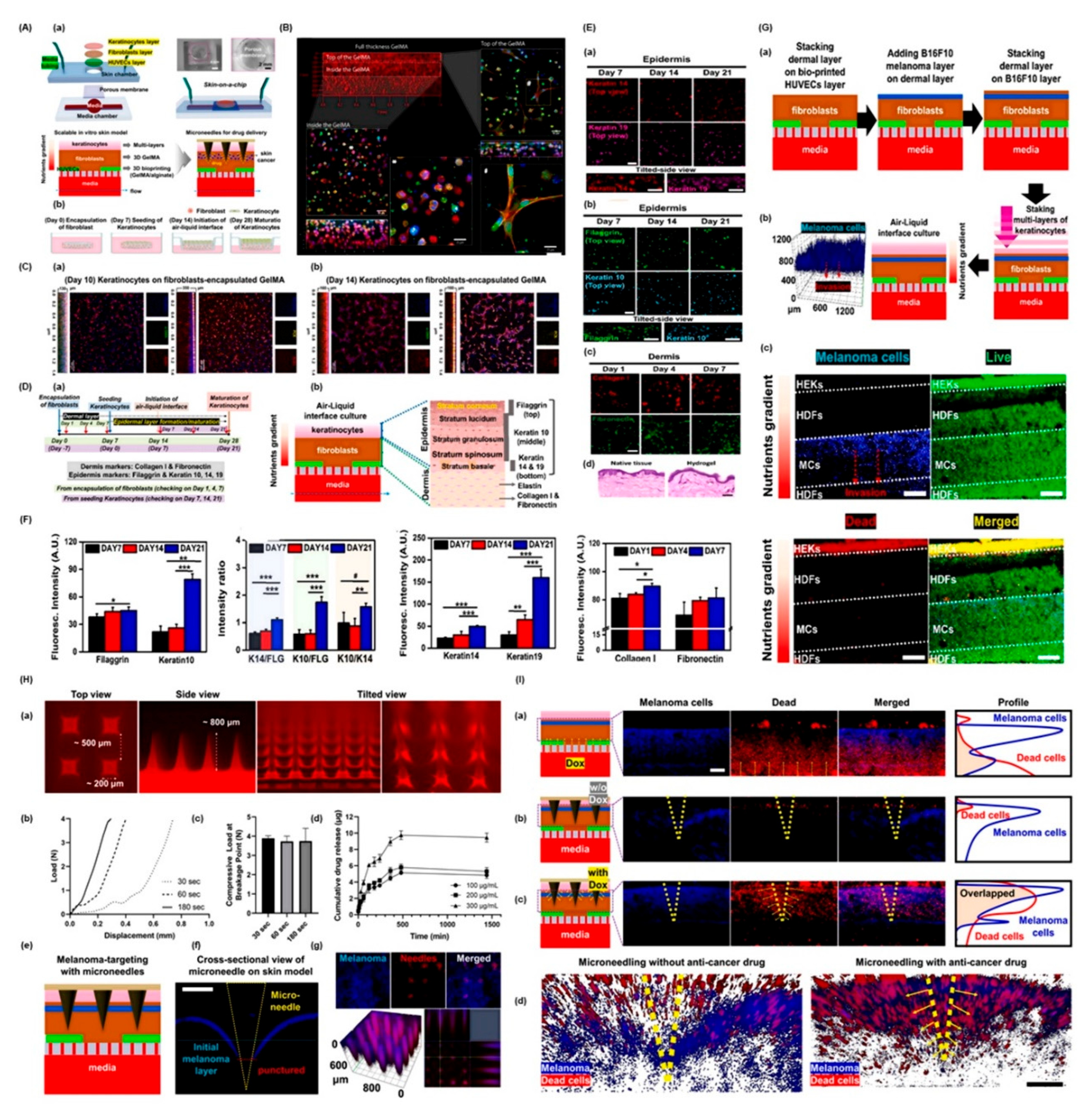
Figure 5.
Integrated biosensing and engineered melanoma models for high-throughput cancer detection and disease modeling. (A) Schematic representation of a nanotechnology-based biosensing strategy for skin and breast cancer detection. The process begins with a drop of blood obtained from breast cancer (BC) patients, which is applied to a nanoparticle-coated microarray for high-throughput screening of cancer biomarkers, including those associated with skin cancer. Candidate biomarkers identified through this screening are then validated using ELISA in a larger patient cohort. This validation enables applications in early diagnosis, disease stratification, prognosis, and monitoring of treatment responses. Based on the performance of the selected biomarker panel, ELISA-based electrochemical immunosensors or biosensors may be developed for clinical applications in breast cancer detection. (B) Representative models and fabrication strategies for melanoma-skin constructs. (a) Major risk factors contributing to melanoma development. (b) Tissue-engineered approaches for constructing in vitro melanoma models, including sequential stages of disease progression: (i) localization of melanocytes at the dermal–epidermal junction, (ii) early melanoma cell clustering at the basement membrane, (iii) invasion of melanoma cells into the dermis, and (iv) aggressive dermal invasion. (c) In-bath bioprinting of melanoma spheroids with a perfusable vascular channel to mimic the tumor microenvironment. (d) In-bath bioprinting of melanoma stroma embedded with a paired blood and lymphatic vessel system for modeling tumor–vasculature interactions [107]. This section is adapted under the Creative Commons Attribution 4.0 (CC BY 4.0) license.
Figure 5.
Integrated biosensing and engineered melanoma models for high-throughput cancer detection and disease modeling. (A) Schematic representation of a nanotechnology-based biosensing strategy for skin and breast cancer detection. The process begins with a drop of blood obtained from breast cancer (BC) patients, which is applied to a nanoparticle-coated microarray for high-throughput screening of cancer biomarkers, including those associated with skin cancer. Candidate biomarkers identified through this screening are then validated using ELISA in a larger patient cohort. This validation enables applications in early diagnosis, disease stratification, prognosis, and monitoring of treatment responses. Based on the performance of the selected biomarker panel, ELISA-based electrochemical immunosensors or biosensors may be developed for clinical applications in breast cancer detection. (B) Representative models and fabrication strategies for melanoma-skin constructs. (a) Major risk factors contributing to melanoma development. (b) Tissue-engineered approaches for constructing in vitro melanoma models, including sequential stages of disease progression: (i) localization of melanocytes at the dermal–epidermal junction, (ii) early melanoma cell clustering at the basement membrane, (iii) invasion of melanoma cells into the dermis, and (iv) aggressive dermal invasion. (c) In-bath bioprinting of melanoma spheroids with a perfusable vascular channel to mimic the tumor microenvironment. (d) In-bath bioprinting of melanoma stroma embedded with a paired blood and lymphatic vessel system for modeling tumor–vasculature interactions [107]. This section is adapted under the Creative Commons Attribution 4.0 (CC BY 4.0) license.
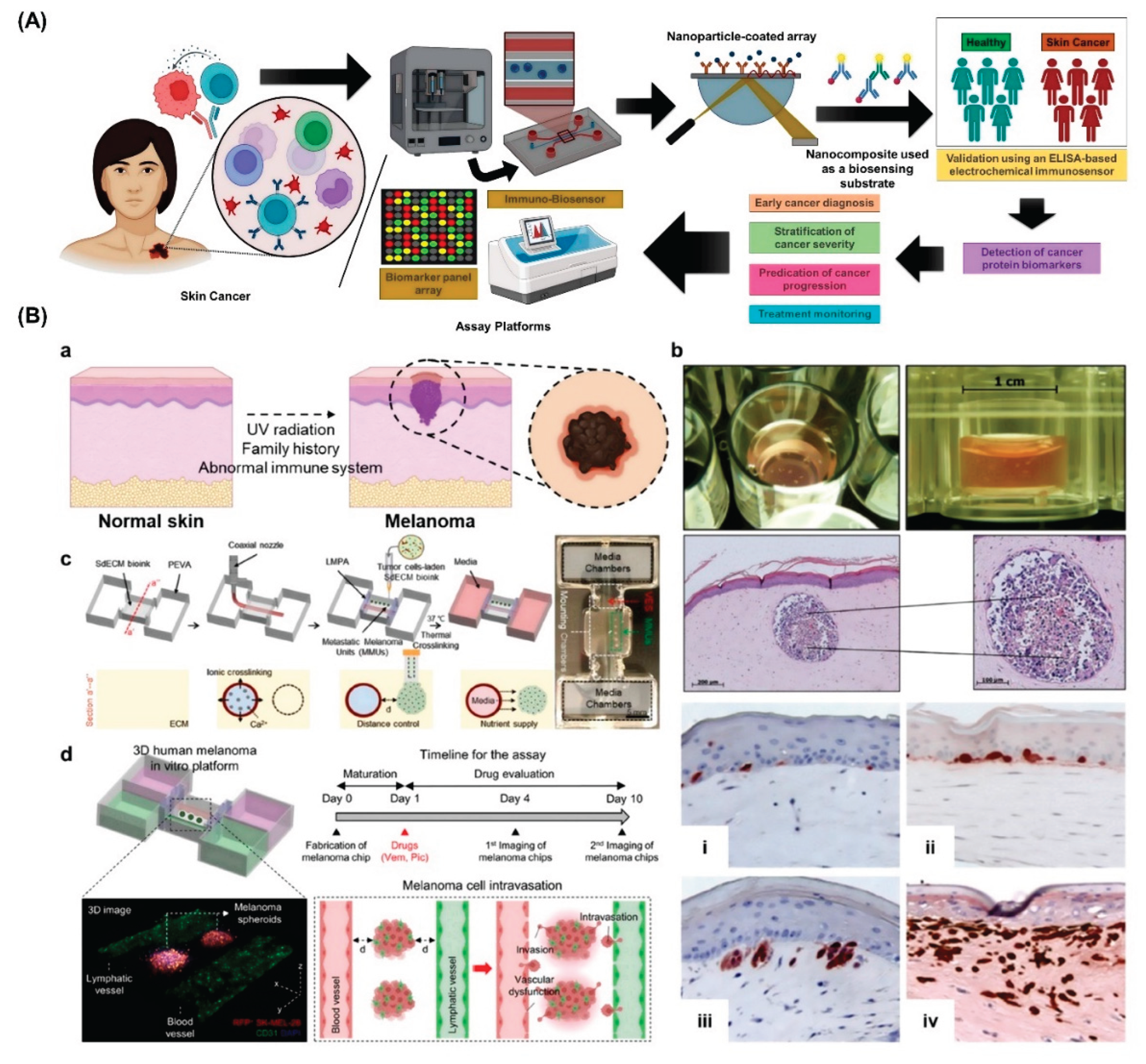
Table 1.
Comparative overview of bioprinting techniques for skin cancer models.
| Bioprinting Technique | Specific Bioinks Used | Advantages | Disadvantages |
|---|---|---|---|
| Laser-based Bioprinting (e.g., Laser-Assisted, DLW, LIFT) | - Gelatin methacrylate (GelMA) - Collagen - Cell-laden hydrogels - Photosensitive hydrogels |
- High spatial resolution (micron-scale precision) - Minimal thermal or mechanical stress on cells - Enables fabrication of complex, multicellular structures, including microvasculature - Supports multi-material patterning |
- Requires photosensitive bioinks - Low throughput for large-scale constructs - High equipment cost and operational complexity - Risk of photothermal damage - Limited bioink compatibility |
| Extrusion-based Bioprinting | - Collagen - Fibrin(ogen) - Gelatin - Hyaluronic acid - Alginate (with embedded cancer cells) - ECM-derived inks - Composite hydrogels |
- Cost-effective and technically simple - Accommodates high -viscosity and high cell -density materials - Suitable for large, tissue-scale constructs - Compatible with diverse bioinks, both natural and synthetic |
- Lower resolution (~100–200 μm) - Shear stress may affect cell viability - Soft constructs prone to collapse without support - Limited fidelity in recreating fine microarchitecture - Balance needed between printability and biofunctionality |
| Droplet-based Bioprinting (e.g., Inkjet, Microvalve, EHD Jetting) | - Collagen - Fibrin – PEG -based hydrogels - Plasma-derived matrices - Low-viscosity bioinks |
- Allows precise droplet -based patterning - High cell viability due to non-contact deposition - Well-suited for multilayered, thin constructs - High reproducibility and low material waste |
- Restricted to low-viscosity materials - Susceptible to nozzle clogging - Poor suitability for thick or volumetric structures - Lacks inherent porosity and mechanical robustness - Limited construct size and load-bearing capacity |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



