
Submitted:
15 September 2025
Posted:
16 September 2025
You are already at the latest version
Abstract
The integration of artificial intelligence (AI) in digital pathology has shown significant promise in advancing cancer diagnostics, grading, and treatment response prediction. However, widespread development and deployment of robust AI models face critical challenges due to data silos, privacy concerns, and the need for large-scale multi-institutional datasets. Federated Learning (FL) presents a transformative approach by enabling collaborative model training across hospitals without direct data sharing. In this review, we summarize recent developments in FL as applied to digital pathology, highlight pioneering use cases, and explore the technical, regulatory, and ethical hurdles. We discuss how FL can enable scalable, privacy-preserving AI models, and outline future directions for standardizing and validating FL-based approaches in clinical workflows.
Keywords:
federated learning
; privacy-preserving AI
; digital pathology
; clinical workflows
1. Introduction
The digitization of histopathological slide, enabled by whole-slide imaging (WSI), has ushered in a new era in diagnostic pathology. By converting traditional glass slides into high-resolution digital images, digital pathology has enabled novel opportunities for computational analysis, remote consultations, and AI-driven decision support systems. At the same time, the growing application of deep learning (DL) in cancer diagnostics, prognostication, and biomarker discovery has significantly improved the accuracy and reproducibility of pathology workflows [1,2]. Despite these advances, one of the critical limitations of developing robust and generalizable AI models in digital pathology is the fragmentation of data across institutions. Medical imaging data, particularly pathology slides, are often stored locally within hospital networks due to patient privacy concerns, regulatory requirements (e.g., GDPR, HIPAA), and logistical barriers. This leads to the creation of data silos, which in turn restrict the scale and diversity of training datasets [3]. The resulting models are often biased toward institution-specific staining, scanner types, or patient populations—limiting their external validity and real-world clinical deployment [4]. Federated Learning (FL), introduced by Google in 2016 [5], offers a promising paradigm for training AI models across multiple institutions without the need to share raw data. In FL, each institution (or “client”) retains its data locally and only shares model parameters or gradients with a central aggregator. This decentralization preserves privacy while still allowing collaboration across a wide network of hospitals or laboratories [6]. In recent years, FL has gained considerable traction in healthcare, especially in radiology, oncology, and genomics, but its application to digital pathology is still in early stages [7,8]. The integration of FL into digital pathology presents a unique set of challenges and opportunities. On one hand, it enables the development of more robust and generalizable models by leveraging diverse datasets from multiple sites. On the other hand, it introduces complexities such as non-IID data distributions, differences in WSI formats and staining protocols, and system-level concerns including latency and communication costs [9,10]. This review aims to provide a comprehensive overview of the current landscape of Federated Learning in digital pathology. We examine recent advances, highlight key use cases, and discuss ongoing technical and ethical challenges. Our goal is to inform researchers, clinicians, and policy-makers about the potential of FL to transform collaborative AI in pathology while ensuring patient privacy and data sovereignty.
2. Opportunities and Challenges in Digital Pathology
Digital pathology, which involves the acquisition, management, and interpretation of pathology information in a digital environment, has gained substantial momentum in recent years due to advances in whole-slide imaging (WSI), image storage infrastructure, and artificial intelligence (AI). The ability to digitize histopathological slides allows pathologists to access, annotate, and analyze tissue samples remotely and at scale, fundamentally reshaping traditional diagnostic workflows [11,12]. The integration of computational techniques, particularly deep learning (DL), into digital pathology has enabled automated tumor detection, grading, immune cell quantification, biomarker prediction, and survival analysis [13,14,15]. These AI models can augment the diagnostic capabilities of pathologists by improving speed, reproducibility, and sensitivity, while also opening new frontiers for discovery in translational oncology and personalized medicine [16,17]. However, realizing the full potential of digital pathology faces several critical challenges: Pathology slides vary widely in staining protocols, scanner hardware, image resolution, and compression methods across institutions. Hematoxylin and eosin (H&E) staining, while standardized to a degree, is subject to differences in color intensity, section thickness, and background artifacts [18]. Additionally, discrepancies between WSI scanners (e.g., Hamamatsu, Leica, Philips) introduce variability in image contrast, brightness, and focus [19], which can significantly impact model generalizability. High-quality annotations are critical for supervised learning, but generating them is time-consuming, expensive, and subject to inter-observer variability. Unlike radiology, where labels such as lesion boundaries can often be determined programmatically, pathology annotations require meticulous outlining of regions of interest at cellular resolution by expert pathologists [20,21]. WSIs are extremely large (often exceeding 100,000 × 100,000 pixels), making them computationally expensive to store, process, and analyze. Training on such images requires special handling, such as patch extraction, multi-scale processing, and advanced data augmentation strategies [22]. Additionally, the hierarchical and spatial structure of tissue requires context-aware models that can capture patterns at both cellular and tissue levels [23]. Many current AI models are trained on single-institution datasets, often with homogeneous patient populations and uniform imaging conditions. As a result, models trained in one setting may underperform when deployed elsewhere, due to domain shift and cohort bias [24]. This lack of generalization is a major barrier to clinical adoption and regulatory approval [25]. Histopathological images, even when de-identified, may contain potentially re-identifiable information, especially when linked to rare cancers or unique tissue features. Furthermore, regulations like the General Data Protection Regulation (GDPR) and the Health Insurance Portability and Accountability Act (HIPAA) impose strict constraints on data sharing and cross-border transfers [26]. These constraints hinder the development of large, diverse, and representative datasets needed for robust model training. Digital pathology lacks universally adopted standards for WSI formats, annotations, and metadata. Although efforts like the Digital Imaging and Communications in Medicine (DICOM) for pathology exist, adoption is still limited [27]. The fragmentation across imaging platforms, software tools, and proprietary formats poses integration challenges and increases the risk of vendor lock-in [28]. Despite technological advancements, deploying AI in pathology labs requires seamless integration into existing laboratory information systems (LIS), compliance with accreditation bodies, and acceptance by clinical pathologists [29,30]. Resistance to workflow disruption, lack of trust in AI, and medicolegal liabilities remain significant hurdles.
3. Federated Learning in Healthcare
The application of artificial intelligence in medicine has been rapidly advancing, driven by large-scale datasets, powerful computational resources, and novel deep learning architectures. However, clinical data often resides in isolated silos across hospitals, laboratories, and countries. Ethical, legal, and technical barriers prevent the centralization of sensitive patient data, which limits the development of diverse and generalizable machine learning (ML) models [31,32]. Federated Learning (FL) offers a compelling solution to this problem by enabling collaborative model training without data sharing. Federated Learning is a decentralized framework for training models across edge devices [33]. In FL, each participating site (or client) trains a model locally using its own data and sends only model parameters (gradients or weights) to a central server. The server performs secure aggregation (such as FedAvg) and updates the global model, which is then redistributed to all clients [34]. This cycle continues for multiple rounds until convergence. Depending on the nature of data partitioning, FL can be classified into four groups as Horizontal FL (Clients share the same feature space but have different patients such as hospitals with WSI data of the same format), Vertical FL (Clients have different features about the same patients for instance in case of one hospital has genomic data, another has pathology), Federated Transfer Learning (Combines both, used when clients differ in both features and data points [35]). Key components of FL include, Model aggregation protocols Privacy-preserving techniques (such as differential privacy and secure multiparty computation), and System orchestration (for synchronization and determining fault tolerance) The medical imaging domain has been one of the earliest adopters of FL in healthcare, particularly in radiology and neuroimaging. Sheller et al. conducted one of the first FL studies for brain tumor segmentation across institutions in the BraTS challenge [36]. The study showed that FL-trained models could achieve performance nearly equivalent to centrally trained models. During the last years, numerous FL projects have emerged including, Federated Tumor Segmentation (FeTS) for glioma classification [37], FL for chest X-ray classification [38], FL in mammography, dermatology, and ophthalmology [39,40,41]. These studies validate the feasibility of FL in real-world healthcare settings, demonstrating its potential to overcome data silos while preserving performance and privacy. FL aligns with GDPR, HIPAA, and local data regulations by avoiding raw data transfer [42] (Data privacy compliance). Additionally, hospitals retain custody of data, avoiding centralized monopolization (Data ownership and control). FL also incorporates diverse populations, devices, and practices that leads to improving external validity (Model generalizability) [13]. It enables multi-center studies across borders and institutions that otherwise could not share data (Collaborative networks). Despite FL promise, FL in healthcare also faces major hurdles. Clinical data is heterogeneously distributed (in terms of differing demographics, and imaging protocols), which can destabilize model convergence [44]. Communication overhead is another problem. Iterative updates and synchronization across clients are computationally and network intensive. In terms of label scarcity and inconsistency, variability in annotations and labeling practices can reduce model reliability [45]. And also, still using privacy preserving techniques cause security vulnerabilities such as risks of model inversion, poisoning attacks, or reconstruction of sensitive data from updates [46]. To address these, researchers are integrating robust aggregation (FedProx, FedDyn), privacy-preserving machine learning (PPML) techniques, and heterogeneity-aware federated optimization strategies [47]. The evolution of FL toward healthcare-grade maturity involves combining it with differential privacy and homomorphic encryption, secure aggregation protocols, self-supervised and weakly-supervised learning to reduce annotation burden and, model explainability tools to enhance trust and regulatory acceptability The increasing availability of open-source FL frameworks (For instance TensorFlow Federated, PySyft, NVIDIA Clara, Flower) and FL-specific healthcare benchmarks (such as MedPerf, OpenFL, FeTS) is accelerating the field’s growth. In summary, Federated Learning is poised to transform collaborative AI development in healthcare by reconciling the demand for large-scale data with the imperatives of privacy.
4. Federated Learning in Digital Pathology
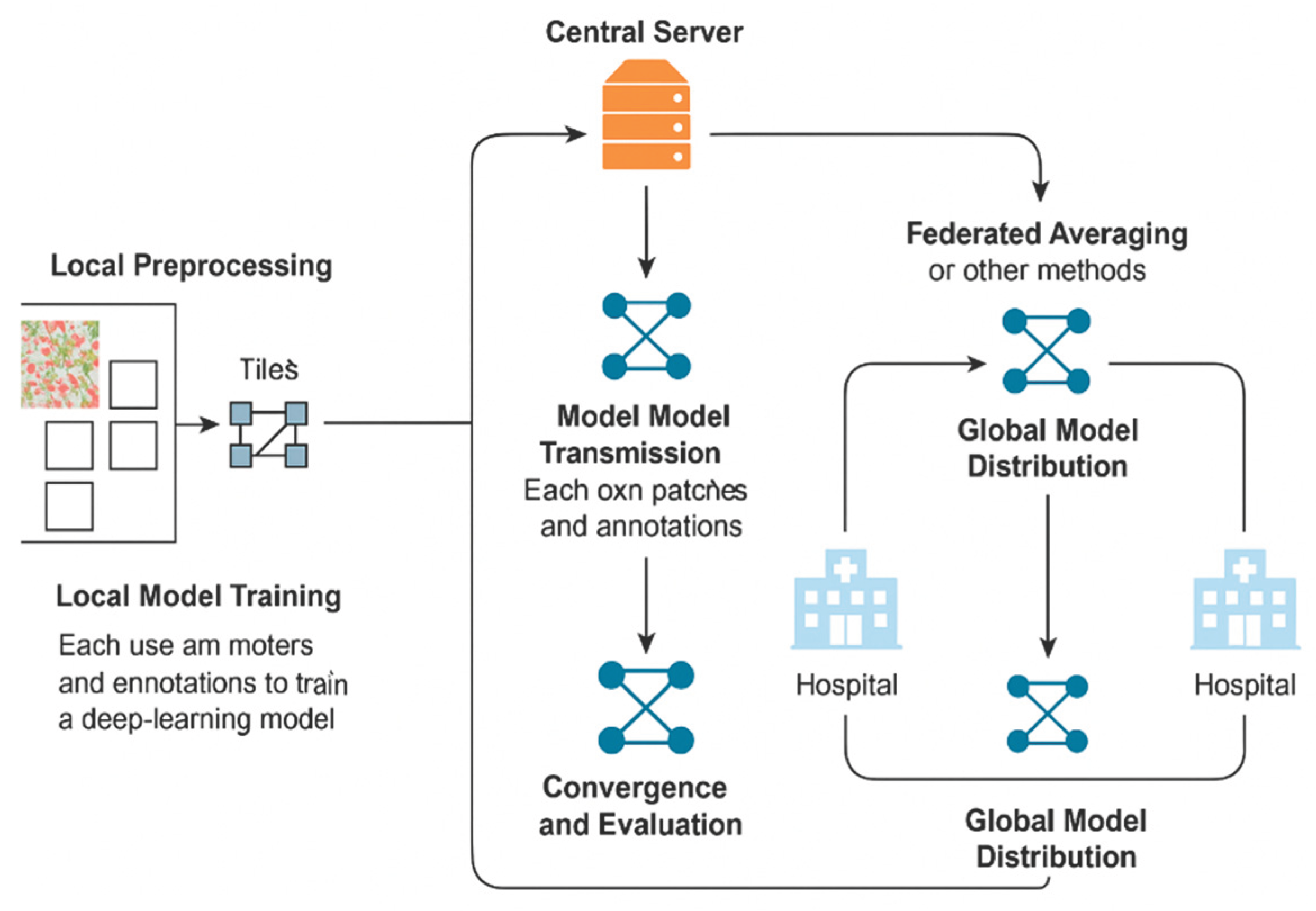
Federated Learning (FL) holds great potential for transforming digital pathology [48,49,50] by enabling collaborative training of AI models across hospitals without direct data sharing. However, applying FL to digital pathology requires adapting the generic FL paradigm to the unique characteristics of whole-slide images (WSIs), annotation styles, and computational constraints in pathology departments. This section presents the core workflow and architectural considerations for deploying FL in digital pathology, drawing on current implementations and research prototypes. WSIs are gigapixel images, often exceeding 10 GB in size, and are typically stored in vendor-specific formats (such as .svs). Their large size and high spatial resolution require preprocessing (e.g., tiling, stain normalization, tissue segmentation) before model training. In FL, this processing must happen locally at each client, increasing the need for reliable, decentralized infrastructure [51,52,53]. Annotation practices in pathology also vary widely across institutions. Labels may be at the slide level (e.g., tumor present/absent), region level (e.g., ROI annotations), or pixel level (e.g., segmentation masks). The inconsistent granularity of annotations complicates standardization across FL clients [54,55]. Moreover, domain shifts—due to staining variability, scanner models, and patient population—are more pronounced in pathology than in radiology. These non-IID (non-independent and identically distributed) data distributions are a known challenge in federated optimization and must be handled via personalization or domain adaptation strategies [56,57]. Mainly, a typical FL pipeline for digital pathology follows several steps (Figure 1). Firstly, local preprocessing is needed. Each hospital tiles WSIs into smaller patches applies stain normalization, and filters non-informative regions (mainly, whitespace or artifacts) [58]. Then, a local model training is needed. Each client uses its own patches and annotations to train a deep learning model (Such as ResNet, EfficientNet, or attention-based models). Training occurs entirely on-premise, ensuring data never leaves the hospital [59]. The next step is model update transmission. After a defined number of local training steps (epochs), each client sends its model parameters or gradients to a central server. These updates are optionally encrypted or noise-injected for privacy [60]. Global model aggregation is the next block of the pipeline. The central server aggregates the updates using methods like Federated Averaging (FedAvg) or more robust schemes (such as FedProx, Scaffold) to update the global model [61,62]. Then, global model distribution is needed. The updated global model is then redistributed to all clients, who resume local training from this point. Finally, convergence and evaluation is required. This cycle continues until model convergence or satisfactory validation performance. Clients may also perform local testing to assess model generalization [63].
Digital pathology FL requires both hardware and software support at each participating institution. Federated orchestration frameworks include Flower: Lightweight and highly customizable FL framework [64] NVIDIA Clara Train: Optimized for healthcare imaging workloads [65] TensorFlow Federated (TFF): Research-focused framework with strong integration into TensorFlow ecosystem [66] OpenFL (Intel) and MedPerf (MLCommons): Emphasize benchmarking and reproducibility [67,68]. In digital pathology, domain shifts are inevitable and several strategies are used to mitigate their effects in FL. We can use Federated domain adaptation for the models trained to generalize across client-specific data distributions using adversarial losses or domain-invariant feature extractors [69]. We can also use local fine-tuning. In this case, each client fine-tunes the final global model on its own data, improving downstream performance. Clustered FL is another solution. Clients are grouped into similar clusters (by scanner type or staining profile), and separate models are trained per group [70]. Federated learning workflows in digital pathology require substantial adaptation to account for data scale, annotation variability, and domain heterogeneity. Despite these challenges, real-world implementations and benchmarking initiatives demonstrate that FL can enable privacy-preserving, multi-institutional collaboration in pathology without compromising model performance. As digital pathology becomes more widespread, the integration of standardized FL pipelines will be critical for democratizing access to high-quality AI models in clinical environments. Multiple studies and collaborations have demonstrated the feasibility of FL in digital pathology.
Figure 1.
A typical FL pipeline for digital pathology.
5. Case Studies and Recent Advances
As we already stated, recent years have seen a surge in efforts to apply Federated Learning (FL) within digital pathology, moving beyond theoretical frameworks to tangible implementations across academic and clinical settings. These pioneering studies illustrate both the promise and complexity of deploying FL in environments where histopathological data is inherently large, heterogeneous, and sensitive. One of the most influential case studies in medical FL, though not limited to pathology, was the Federated Tumor Segmentation (FeTS) initiative. Launched to address glioma segmentation using MRI data, FeTS laid the groundwork for applying federated principles to segmentation tasks in gigapixel whole-slide images (WSIs) [37]. It showed that a decentralized cohort of hospitals could train performant models without exchanging patient data, thus reducing legal and logistical friction while preserving data diversity. Although primarily focused on radiology, the infrastructure and protocols developed by FeTS have been adapted in pathology-oriented networks and have informed the design of similar federated trials. In order to determine whether a more privacy-preserving federated learning approach can achieve comparable diagnostic performance to a classical centralized (i.e., single-model) and ensemble learning approach for AI-based melanoma diagnostics, the study included 1025 whole-slide images of clinically melanoma-suspicious skin lesions from 923 patients, including 388 histopathologically confirmed invasive melanomas and 637 nevi [71]. Based on a clinically relevant distributed dataset, the results of this diagnostic investigation indicate that federated learning is a feasible method for the binary classification of invasive melanomas and nevi. A Convolutional Neural Network (CNN) is trained locally to categorize tissue patches that have been labeled using the local WSI dataset [72]. The Federated Averaging (FedAVG) approach is then used to aggregate the models and guarantee convergence. FL makes it possible to train deep learning models collectively on dispersed data, protecting patient privacy while gaining access to a vast and varied dataset. Using accuracy, sensitivity, specificity, and F-1 score, the authors evaluate the FL-trained model’s performance against that of a centralized model. According to the results, the simulated FL models perform as well as or better than centralized learning, with accuracy ratings ranging from 75-87% compared to 82% for centralized learning. This innovative method has the potential to transform computational pathology and aid in better medical decision-making [73,74]. This research [75] specifically looks at the performance of a YOLOv6 model trained with FedL across a number of customers. To protect data privacy, a novel homomorphic encryption and decryption technique is also suggested. A novel pruned YOLOv6 model with FedL is introduced in this study to differentiate benign and malignant tissues. The BreakHis and BUSI pathology datasets for breast cancer are used to train the model. On the BreakHis and BUSI datasets, the suggested model’s validation accuracy was 98% and 97%, respectively. An accurate instrument for early identification and successful treatment approaches against the lung cancer scourge is provided by Usharani & Selvapandian [76]. While maintaining data security and privacy, the federated learning technique makes it possible to leverage dispersed data. The suggested method was contrasted with other cutting-edge algorithms. After extensive testing, our system demonstrates impressive improvements with a 99.40% classification accuracy. To efficiently differentiate between different forms of lung cancer, the authors of [77] suggest Lung-AttNet, which combines a convolutional block with a Lightweight Global Attention Module (LGAM). With two and three clients, Lung-AttNet obtains a 92% accuracy rate in the FL environment, demonstrating its resilience and versatility for practical uses. Beyond classification and segmentation, FL has been explored for high-dimensional predictive tasks such as survival analysis and biomarker discovery. For instance, in multi-site breast cancer cohorts, federated Cox proportional hazards models have been trained on WSI-derived features to predict recurrence, while maintaining compliance with patient data privacy laws. These studies signal that FL is not limited to binary or categorical outputs but is extensible to more nuanced, clinically actionable outcomes. There is also increasing interest in combining FL with emerging learning paradigms such as self-supervised learning and multiple instance learning (MIL), which are particularly well suited to pathology. Given that WSIs are typically labeled at the slide level, MIL allows models to learn from weak labels without requiring exhaustive pixel-level annotation. Studies combining FL and MIL have shown that diagnostic performance can be preserved even when clients differ significantly in data quantity and annotation quality—a crucial consideration in federated pathology networks. Moreover, some projects are experimenting with Swarm Learning, a variant of FL in which there is no centralized aggregator. This decentralized topology—demonstrated in hematopathology and inflammatory disease histology—relies on blockchain or secure consensus protocols to coordinate model updates, thereby reducing single points of failure and increasing trust among participants. Swarm Learning approaches align closely with European values of data sovereignty and may see increased adoption in multi-national collaborations. Taken together, these case studies provide compelling evidence that Federated Learning is not only technically feasible in digital pathology but increasingly being adapted to the constraints and goals of real-world medical environments. They highlight that federated models can maintain high performance across variable cohorts, institutions, and conditions—paving the way for AI systems that are robust, generalizable, and compliant with evolving privacy frameworks..
6. Conclusions
The integration of Federated Learning (FL) into digital pathology represents a significant advancement in the pursuit of collaborative, privacy-preserving artificial intelligence in healthcare. By enabling multi-institutional model development without requiring direct data sharing, FL addresses the longstanding tension between the need for large, diverse datasets and the ethical, legal, and logistical barriers to data centralization. In pathology, where data is not only massive in size but also highly variable across institutions in terms of staining, scanner type, and annotation practices, FL offers a scalable solution for building robust and generalizable AI models. This review has outlined the technical foundations of FL, its applications in healthcare imaging, and its adaptation to the unique challenges posed by digital pathology. We have discussed emerging workflows, architectures, and real-world case studies that demonstrate the feasibility and utility of federated models in pathology-based diagnosis, prognosis, and biomarker discovery. Although challenges remain—including non-IID data, interoperability issues, and the need for trust and transparency—advances in federated optimization, privacy-enhancing technologies, and open-source frameworks are rapidly closing these gaps. As digital pathology continues its transition from research to routine clinical use, FL will play a central role in enabling equitable access to AI-driven tools across institutions, regardless of size or resources. Future efforts must focus on standardizing FL protocols, integrating clinical workflows, and ensuring rigorous validation under regulatory standards. By doing so, federated learning can serve as a cornerstone of the next generation of computational pathology—one that is not only intelligent and efficient, but also secure, inclusive, and globally connected..
Author Contributions
“Writing—original draft preparation, M.A.; writing—review and editing, N.Z.; All authors have read and agreed to the published version of the manuscript.”
Conflicts of Interest
“The authors declare no conflicts of interest.”
References
- Madabhushi A, Lee G. Image analysis and machine learning in digital pathology: Challenges and opportunities. Med Image Anal. 2016;33:170–175. [CrossRef]
- Echle A, Rindtorff NT, Brinker TJ, et al. Deep learning in cancer pathology: a new generation of clinical biomarkers. Br J Cancer. 2021;124(4):686–696. [CrossRef]
- Kaissis GA, Makowski MR, Rückert D, Braren RF. Secure, privacy-preserving and federated machine learning in medical imaging. Nat Mach Intell. 2020;2(6):305–311. [CrossRef]
- Campanella G, Hanna MG, Geneslaw L, et al. Clinical-grade computational pathology using weakly supervised deep learning on whole slide images. Nat Med. 2019;25(8):1301–1309. [CrossRef]
- McMahan B, Moore E, Ramage D, et al. Communication-efficient learning of deep networks from decentralized data. In: Proc. AISTATS. 2017. https://arxiv.org/abs/1602.05629.
- Li T, Sahu AK, Talwalkar A, Smith V. Federated learning: Challenges, methods, and future directions. IEEE Signal Process Mag. 2020;37(3):50–60. [CrossRef]
- Sheller MJ, Edwards B, Reina GA, et al. Federated learning in medicine: facilitating multi-institutional collaborations without sharing patient data. Sci Rep. 2020;10:12598. [CrossRef]
- Lu MY, Chen TY, Williamson DF, et al. Federated learning for computational pathology on gigapixel whole slide images. Med Image Anal. 2022;76:102298. [CrossRef]
- Andreux M, du Terrail JP, Beguier C, et al. Federated survival analysis with discrete-time Cox models. In: NeurIPS 2020 Workshop on Machine Learning for Health (ML4H). https://arxiv.org/abs/2006.08997.
- Warnat-Herresthal S, Schultze H, Shastry KL, et al. Swarm Learning for decentralized and confidential clinical machine learning. Nature. 2021;594(7862):265–270. [CrossRef]
- Pantanowitz L, Sharma A, Carter AB, et al. Twenty years of digital pathology: An overview of the road traveled, what is on the horizon, and the emerging role of artificial intelligence. J Pathol Inform. 2020;11:46. [CrossRef]
- Niazi MKK, Parwani AV, Gurcan MN. Digital pathology and artificial intelligence. Lancet Oncol. 2019;20(5):e253–e261. [CrossRef]
- Coudray N, Ocampo PS, Sakellaropoulos T, et al. Classification and mutation prediction from non–small cell lung cancer histopathology images using deep learning. Nat Med. 2018;24(10):1559–1567. [CrossRef]
- Lu MY, Williamson DFK, Chen TY, et al. AI-based pathology predicts origins for cancers of unknown primary. Nature. 2021;594(7861):106–110. [CrossRef]
- Kather JN, Krisam J, Charoentong P, et al. Predicting survival from colorectal cancer histology slides using deep learning: A retrospective multicenter study. PLoS Med. 2019;16(1):e1002730. [CrossRef]
- Baxi V, Edwards R, Montalto M, Saha S. Digital pathology and artificial intelligence in translational medicine and clinical practice. Mod Pathol. 2022;35:23–32. [CrossRef]
- Aeffner F, Zarella MD, Buchbinder N, et al. Introduction to digital image analysis in whole-slide imaging: A white paper from the Digital Pathology Association. J Pathol Inform. 2019;10:9. [CrossRef]
- Stack EC, Wang C, Roman KA, Hoyt CC. Multiplexed immunohistochemistry, imaging, and quantitation: A review, with an assessment of Tyramide signal amplification, multispectral imaging and multiplex analysis. Methods. 2014;70(1):46–58. [CrossRef]
- Bandi P, Geessink O, Manson Q, et al. From detection of individual metastases to classification of lymph node status at the patient level: The CAMELYON17 challenge. IEEE Trans Med Imaging. 2019;38(2):550–560. [CrossRef]
- Litjens G, Kooi T, Bejnordi BE, et al. A survey on deep learning in medical image analysis. Med Image Anal. 2017;42:60–88. [CrossRef]
- Steiner DF, MacDonald R, Liu Y, et al. Impact of deep learning assistance on the histopathologic review of lymph nodes for metastatic breast cancer. Am J Surg Pathol. 2018;42(12):1636–1646. [CrossRef]
- Courtiol P, Maussion C, Moarii M, et al. Deep learning-based classification of mesothelioma improves prediction of patient outcome. Nat Med. 2019;25(10):1519–1525. [CrossRef]
- Chen RJ, Lu MY, Wang J, et al. Pathomic fusion: An integrated framework for fusing histopathology and genomic features for cancer diagnosis and prognosis. IEEE Trans Med Imaging. 2020;39(4):802–813. [CrossRef]
- Howard FM, Dolezal J, Kochanny S, et al. The impact of site-specific digital histology signatures on deep learning model accuracy and bias. Nat Commun. 2021;12:4423. [CrossRef]
- Stathonikos N, Veta M, Huisman A, van Diest PJ. Going fully digital: Perspective of a Dutch academic pathology lab. J Pathol Inform. 2013;4:15. [CrossRef]
- De Fauw J, Ledsam JR, Romera-Paredes B, et al. Clinically applicable deep learning for diagnosis and referral in retinal disease. Nat Med. 2018;24(9):1342–1350. [CrossRef]
- DICOM Working Group 26. Supplement 145: Whole Slide Microscopic Image IOD and SOP Classes. National Electrical Manufacturers Association (NEMA). 2010. https://www.dicomstandard.org.
- Abels E, Pantanowitz L, Aeffner F, et al. Computational pathology definitions, best practices, and recommendations for regulatory guidance: A white paper from the Digital Pathology Association. J Pathol. 2019;249(3):286–294. [CrossRef]
- Bauer TW, Slaw RJ. Validating whole-slide imaging for diagnostic purposes in pathology: Guideline from the College of American Pathologists Pathology and Laboratory Quality Center. Arch Pathol Lab Med. 2015;139(2):171–179. [CrossRef]
- Fraggetta F, L’Imperio V, Ameisen D, et al. Best practice recommendations for the implementation of a digital pathology workflow. Virchows Arch. 2021;479(4):581–590. [CrossRef]
- Rieke N, Hancox J, Li W, et al. The future of digital health with federated learning. NPJ Digit Med. 2020;3:119. [CrossRef]
- Kaissis GA, Ziller A, Passerat-Palmbach J, et al. End-to-end privacy-preserving deep learning on multi-institutional medical imaging. Nat Mach Intell. 2021;3:473–484. [CrossRef]
- McMahan HB, Moore E, Ramage D, Hampson S, y Arcas BA. Communication-efficient learning of deep networks from decentralized data. AISTATS. 2017. https://arxiv.org/abs/1602.05629.
- Kairouz P, McMahan HB, Avent B, et al. Advances and open problems in federated learning. Found Trends Mach Learn. 2021;14(1):1–210. [CrossRef]
- Yang Q, Liu Y, Chen T, Tong Y. Federated machine learning: Concept and applications. ACM TIST. 2019;10(2):12. [CrossRef]
- Sheller MJ, Reina GA, Edwards B, Martin J, Bakas S. Multi-institutional deep learning modeling without sharing patient data: A feasibility study on brain tumor segmentation. Brainlesion: Glioma, Multiple Sclerosis, Stroke and Traumatic Brain Injuries. Springer, 2019. 2019.
- Pati S, Rieke N, Bakas S, et al. Federated learning enables big data for rare cancer boundary detection. Nat Commun. 2022;13:7340. [CrossRef]
- Xu J, Glicksberg BS, Su C, et al. Federated learning for healthcare informatics. J Biomed Inform. 2021;115:103676. [CrossRef]
- Lu Y, Weng CH, Maleki S, et al. Federated learning in mammography classification: A case study. Med Phys. 2023;50(2):934–947. [CrossRef]
- Liu Y, Chen PC, Krause J, Peng L. How to read articles that use machine learning: Users’ guides to the medical literature. JAMA. 2019;322(18):1806–1816. [CrossRef]
- Lee H, Tajmir S, Lee J, et al. Fully automated deep learning system for bone age assessment. J Digit Imaging. 2017;30(4):427–441. [CrossRef]
- Brisimi TS, Chen R, Mela T, et al. Federated learning of predictive models from federated electronic health records. Int J Med Inform. 2018;112:59–67. [CrossRef]
- Huang H, Xu Y, Yu K, et al. Personalized cross-silo federated learning on non-IID data. AAAI. 2021. https://arxiv.org/abs/2007.03797.
- Zhao Y, Li M, Lai L, et al. Federated learning with non-IID data. arXiv preprint. 2018. https://arxiv.org/abs/1806.00582.
- Dayan I, Roth HR, Zhong A, et al. Federated learning for predicting clinical outcomes in COVID-19 patients. Nat Med. 2021;27(10):1735–1743. 1735. [CrossRef]
- Hitaj B, Ateniese G, Pérez-Cruz F. Deep models under the GAN: Information leakage from collaborative deep learning. Proc. ACM CCS. 2017. [CrossRef]
- Li X, Jiang M, Zhang X, et al. FedBN: Federated learning on non-IID features via local batch normalization. ICLR. 2021. https://arxiv.org/abs/2002.07623.
- Kisakol, Batuhan, et al. “High-resolution spatial proteomics characterizes colorectal cancer consensus molecular subtypes.” Cancer Research 85.8_Supplement_1 (2025): 161-161.
- Azimi, Mohammadreza, et al. “Spatial effects of infiltrating T cells on neighbouring cancer cells and prognosis in stage III CRC patients.” The Journal of Pathology 264.2 (2024): 148-159.
- Duggan, William P., et al. “Spatial transcriptomic analysis reveals local effects of intratumoral fusobacterial infection on DNA damage and immune signaling in rectal cancer.” Gut Microbes 16.1 (2024): 2350149.
- Aeffner F, et al. Introduction to digital image analysis in whole-slide imaging. J Pathol Inform. 2019;10:9.
- Bandi P, et al. From detection of metastases to classification: CAMELYON17. IEEE Trans Med Imaging. 2019;38(2):550–560.
- Komura D, Ishikawa S. Machine learning methods for histopathological image analysis. Comput Struct Biotechnol J. 2018;16:34–42.
- Litjens G, et al. A survey on deep learning in medical image analysis. Med Image Anal. 2017;42:60–88.
- Veta M, et al. Predicting breast cancer outcome using histopathology images: challenges and progress. Curr Opin Biomed Eng. 2021;18:100271.
- Kairouz P, et al. Advances and open problems in federated learning. Found Trends Mach Learn. 2021;14(1):1–210.
- Zhao Y, et al. Federated learning with non-IID data. arXiv. 2018. https://arxiv.org/abs/1806.00582.
- Janowczyk A, Madabhushi A. Deep learning for digital pathology image analysis: A comprehensive tutorial. Comput Med Imaging Graph. 2016;55:60–72.
- Lu MY, et al. AI-based pathology predicts origins for cancers of unknown primary. Nature. 2021;594:106–110.
- Bonawitz K, et al. Practical secure aggregation for privacy-preserving machine learning. Proc. CCS. 2017.
- Li T, et al. Federated optimization in heterogeneous networks. Proc. MLSys. 2020.
- Karim MR, et al. FedProx: A federated optimization algorithm. arXiv. 2018. https://arxiv.org/abs/1812.06127.
- Andreux M, et al. Federated survival analysis with discrete-time Cox models. arXiv. 2020. https://arxiv.org/abs/2006.08997.
- Beutel D, et al. Flower: A friendly federated learning framework. arXiv. 2020. https://arxiv.org/abs/2007.14390.
- NVIDIA Clara Train SDK. https://developer.nvidia.com/clara.
- TensorFlow Federated. https://www.tensorflow.org/federated.
- Warnat-Herresthal S, et al. Swarm learning for decentralized and confidential clinical ML. Nature. 2021;594(7862):265–270.
- MLCommons. MedPerf Benchmarking Platform. https://medperf.org.
- u Y, et al. Federated unsupervised representation learning. NeurIPS. 2020.
- Sattler F, Müller K-R, Samek W. Clustered federated learning: Model-agnostic personalization. arXiv. 2020. https://arxiv.org/abs/2008.06165.
- Haggenmüller, Sarah, et al. “Federated Learning for Decentralized Artificial Intelligence in Melanoma Diagnostics.” JAMA Dermatology 160.3 (2024): 303.
- Shukla, Shubhi, et al. “Federated learning with differential privacy for breast cancer diagnosis enabling secure data sharing and model integrity.” Scientific Reports 15.1 (2025): 13061.
- Ciobotaru, Alexandru, et al. “Deep Learning and Federated Learning in Breast Cancer Screening and Diagnosis: A Systematic Review.” IEEE Access (2025).
- Bechar, Amine, et al. “Federated and transfer learning for cancer detection based on image analysis.” Neural Computing and Applications (2025): 1-46.
- Gupta, Chhaya, et al. “Applying YOLOv6 as an ensemble federated learning framework to classify breast cancer pathology images.” Scientific Reports 15.1 (2025): 3769.
- Usharani, C., and A. Selvapandian. “FedLRes: enhancing lung cancer detection using federated learning with convolution neural network (ResNet50).” Neural Computing and Applications (2025): 1-12.
- Saha, Chamak, et al. “Lung-AttNet: An Attention Mechanism based CNN Architecture for Lung Cancer Detection with Federated Learning.” IEEE Access (2025).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



