
Submitted:
15 September 2025
Posted:
16 September 2025
You are already at the latest version
Abstract
Background/Objectives: Lung cancer is the leading cause of cancer death in the United States (U.S.). Virginia, South Carolina, and North Carolina are among the U.S. states with extraordinarily high rates of lung cancer mortality, particularly among Black residents. The current lung cancer screening guidelines, revised in 2021, support screening for younger, non-Medicare age-eligible individuals who smoke. However, their health insurance, if any, may not cover their screening. This lack of access could create more disparities in lung cancer mortality rates. Methods: To address this concern, the Virginia Commonwealth University Massey Comprehensive Cancer Center, the Medical University of South Carolina Hollings Cancer Center, and the University of North Carolina Chapel Hill Lineberger Comprehensive Cancer Center secured a four-year Stand Up To Cancer® (SU2C) grant with a novel aim to test the effectiveness of a multimodal, multilevel, barrier-focused patient navigation intervention to promote lung cancer screening among Black patients from federally qualified health centers. Results: A total of 170/675 Black participants have been recruited to date. The majority of participants (n=134; 78.82%) were aged 55-74 years. Most participants were unmarried (n=100; 58.82%), more than half had a high school education/GED or less (n=111; 65.29%), most currently smoked (n=142; 83.53%), and more males than females participated (n=107; 62.94% male). Their reported lung cancer screening barriers, addressed by the patient navigators, were cost concerns, insurance coverage issues, and recent medical history precluding screening. Conclusions with Relevance to Cancer Health Equity: This SU2C study includes a unique lung cancer screening cohort that is in direct contrast to the predominantly White cohort in the National Lung Screening Trial. The SU2C study has created a novel, community-engaged approach to lung cancer screening navigation that could become the gold standard in high-risk medically underserved populations.
Keywords:
lung cancer screening
; black patients
; medically underserved
; federally qualified health centers
; patient navigation
1. Introduction
Lung Cancer Mortality Rates in the United States (U.S.) and in Virginia (V.A.), South Carolina (S.C.), and North Carolina (N.C.)
Lung cancer is the leading cause of cancer death in the U.S. Lung cancer mortality rates are particularly high in southeastern U.S. states such as Virginia, South Carolina, and North Carolina [1]. In 2025, the lung cancer death rate per 100,000 population in Virginia is projected to be 58.1 for men and 41.9 for women; in South Carolina, these rates are expected to be 47.4 and 29.8, respectively; and in North Carolina the rates are anticipated to be 46.8 and 30.7[1]. These high lung cancer mortality rates, in comparison to the projected 2025 U.S. rates of 38.7 for men and 27.6 for women per 100,000 [1]., are largely attributable to the social and contextual factors experienced by the residents of each state, such as high rates of poverty and unemployment, and lower levels of education, which translate into lack of access to preventive services such as lung cancer screening.
Lung cancer death rates are significantly higher for Black men than for members of any other racial/ethnic or sex group [2]. These higher death rates appear to be due to higher levels of lung cancer risk associated with social deprivation, which has been linked to lack of access to health care and poorer health outcomes. For example, in a recent study, Jafareian et al. [3] used latent class analysis to analyze data from a sample of 729 lung cancer patients who were seen at the University of Rochester from 2016-2017 [3]. The results showed that Black patients with lung cancer experienced higher levels of social deprivation than White patients (p<0.05) and rural lung cancer patients experienced higher levels of social deprivation than urban patients (p<0.05). Social deprivation was measured using the 5-year Social Deprivation Index, which measures the level of social deprivation associated with lack of access to health care as well as health outcomes [4].
The Importance of Lung Cancer Screening in Reducing Lung Cancer Mortality Rates
In 2013, low-dose CT was recommended by the U.S. Preventive Services Task Force (USPSTF) as an evidence-based screening modality for high-risk individuals with a smoking history of 30 pack years who were 55-80 years of age [5]. In their seminal American Thoracic Society Official Statement, Rivera et al. [6] noted the precarious position in which high-risk, younger people with few financial resources would be placed if the screening age were lowered, and recommended patient navigation as a potential solution to overcoming the financial and other systemic barriers to care that face many high-risk smokers who are screening age-eligible but not eligible to have their screening costs covered by Medicare.
In March of 2021, USPSTF lowered the lower boundary of screening-eligible age to 50 years. Unfortunately, this placed a number of economically challenged individuals in a difficult position; they were age-eligible to receive lung cancer screening but they lacked the resources to successfully navigate from their places of primary care to the nearest available lung cancer screening site.
Barriers to Lung Cancer Screening
Disparities among Black patients in receipt of lung cancer screening, lung cancer surgery, and other forms of treatment are likely due to several factors, including socioeconomic status, misperceptions and biases (on the part of both patients and providers), suboptimal communication in physician-patient interactions, and/or significant financial hardship associated with receiving care [7,8].
One in three Americans experiences significant financial hardship as a result of medical care, with the greatest burden in medically underserved populations, including Black and rural populations. Harmful, care-altering behavioral responses to the high cost of care, including lack of screening and delaying or foregoing medical treatment, may contribute to widely observed rural/non-rural and racial disparities in cancer mortality [9,10,11,12]. Because rural and Black individuals tend to have lower incomes, with fewer assets, higher unemployment, and higher rates of no or under-insurance than non-rural or White individuals, such out-of-pocket cost of care expenses constitute a greater share of monthly expenditures and thus create more burdensome material and psychological hardship. This hardship is most pronounced among rural communities with large minority populations [13]. Uninsured or “self-pay” individuals are generally responsible for paying the full cost of their care unless they can navigate the complex and uneven safety net of resources, including hospital charity care, entitlement programs, manufacturer assistance, and non-profit organizations’ aid, which are less available and harder to navigate in rural settings [14,15,16].
2. Materials and Methods
Institutional Review Board Approval
Virginia Commonwealth University Massey Cancer Center served as the IRB of record for the study. The IRB protocol number is MCC SU2C-WINN.
Participant Inclusion Criteria
Eligible participants were required to meet the following criteria:
- Meets current USPSTF guidelines for lung cancer screening
- Adult aged 50 to 80 years
- 20 pack-year smoking history (Note: A pack-year is a way of calculating how much a person has smoked in their lifetime. One pack-year is the equivalent of smoking an average of 20 cigarettes—1 pack—per day for a year.)
- Currently smokes or has quit smoking within the past 15 years
- Identifies as Black or African American (Note: Both Hispanic/Latino and Non-Hispanic/Latino patients are eligible as long as they also identify as Black or African American [e.g., Afro-Latino]).
- Willing to complete all navigation-related study activities
- Able to understand and the willingness to sign a written informed consent document
Federally Qualified Health Center Partnerships
As Korn et al. [7] noted, promoting cancer screening in focal population groups that face barriers related to the social drivers of health, as outlined above, benefits from establishing multi-level partnerships with providers, health care settings, and patients [7]. These partnerships can be helpful in identifying patients who are most at risk of developing lung cancer and not receiving lung cancer screening, to link these patients with patient navigators who can help to resolve screening barriers and guide the patients to lung cancer screening sites near their communities. Federally qualified health centers (FQHCs) represent an ideal partner for lung cancer screening. These community-based organizations provide comprehensive primary care services to all patients, regardless of their ability to pay or their health insurance status [27]. FQHCs tend to serve racially and ethnically diverse patient populations. Their patients typically have high smoking prevalence. Two of the cancer center sites are employing an in-person, face-to-face recruitment and eConsent strategy with their FQHC partners, while the other cancer center is relying primarily on remote contact with potential participants to describe the study and to consent them.
Virginia and Virginia Commonwealth University Massey Comprehensive Cancer Center FQHC Partner
The FQHC is a primary care, dental, and mental health center, and is the flagship clinic for a network of three FQHCs. Located in the predominantly Black East End community in Richmond, the FQHC serves approximately 12,469 patients per year, 69% of whom are Black, 61% are publicly insured, and 39% are ages 50+. As of 2018, the FQHC reported the second-lowest tobacco screening and cessation intervention (75% of eligible) among all FQHCs in the state.
North Carolina and University of North Carolina-Chapel Hill Lineberger Comprehensive Cancer Center FQHC Partners
LCCC/UNC is partnering with two FQHCs in North Carolina. The first FQHC has 25 locations, serving 16 counties in western North Carolina that are all designated as medically underserved. In 2024, the FQHC served over 100,000 patients, including 25% Black, and 81% living at or below the federal poverty level (FPL), and 92% living below 200% FPL [28,29]. About 81% of the counties served by the first FQHC had higher lung cancer incidence rates than the state average (62.10 per 100,000), with the highest at 76.9 per 100,000 (Randolph County) [29]. Adult smoking in the FQHC is also higher than the state average (19% versus 17%) [29,30]. About 95% of adults seen by the FQHC have been screened for tobacco use and received smoking cessation counseling [3]. However, only 50% of eligible smokers in the FQHC have received lung cancer screening [3].
The second FQHC in North Carolina has 7 locations, serving 5 rural counties in eastern North Carolina that are all designated as medically underserved. In 2024, the FQHC served approximately 18,000 patients, including 52% Black, 74% living at or below the FPL, and 90% living 200% below the FPL. The lung cancer incidence in the FQHC serving area ranged from 46.9 (Gates) to 65.4 (Washington) per 100,000 [29]. Adult smoking in the FQHC is higher than the state average (19% versus 17%) [5,30]. About 76% of adults seen by the FQHC have been screened for tobacco use and received smoking cessation counseling [5]. About 61% of eligible smokers in the FQHC have received lung cancer screening [5].
South Carolina and Medical University of South Carolina Hollings Cancer Center FQHC Partner
The FQHC partner provides comprehensive services for insured, uninsured, and underserved residents in Berkeley, Charleston, Colleton, and Dorchester Counties. The FQHC network includes 20 different sites, many located along the I-95 Corridor. The network provides care for uninsured and underinsured people in medically underserved areas. Among the 15,489 patients served by the FQHC network, 2,110 or 13.6% are tobacco users, and of those 1,289 (61%) are Black.
NCI Barrier Plan Form
The patient navigators actively asked about and addressed patients’ needs and barriers to care. To document each interaction with the participants, the navigators employed a web-based version of the NIH/NCI PN Barrier Checklist, used within the context of a Research Electronic Data Capture (REDCap) data management system. The system elicits specific barriers that could prevent patients from receiving lung cancer screening. For each identified barrier, the REDCap system then uses branching logic to link to a barrier plan that the navigator will use to address and resolve the barrier. For example, if a patient stated that their initial barrier was related to communication with medical personnel (coded as CP in Figure 1), the navigator would then ask whether the communication was related to a lack of understanding of what cancer is, not understanding what the patient is being asked to do, not understanding what the medical tests mean or how they will be used, being unaware that they needed to schedule an appointment, feeling that the medical forms are too complicated, or another reason, coded as “Other” (Figure 2). The specific actions each navigator took to address and resolve the barriers presented by their assigned participants are shown in Figure 3, which shows drop-down boxes to capture the general categories of actions taken by the navigators, which are then linked to more detailed expanded fields to allow the navigators to describe each action in greater detail, including using text fields.
3. Results
To date, 170 Black participants have been enrolled in the study. The majority of participants (n=134; 78.82%) were aged 55-74 years. Men comprised 107 (62.94%) of the participants. Only 26 (15.29%) of the participants were married or living with a partner. More than half (n= 111; 65.29%) of the participants completed high school/GED or had less than a high school education as their highest level of education. The majority of participants (n=142; 83.53%) were current smokers, and among those who quit, only 6 (3.53%) quit 10-15 years ago. The median pack years of the participants was 28 years.
As shown in Table 3, these Stand Up To Cancer® (SU2C) study data are in direct contrast to the National Lung Screening Trial (NLST) data, which showed that 73.38% of the participants were aged 55-64 years, women comprised only 40.99% of participants, Black participants comprised only 4.48% of the total sample, 66.67% of participants were married or living with a partner, only 6.14% of participants had a high school/GED degree, and none had less than a high school education. Only 16.86% of participants in the NLST were current smokers, and 19.67% had quit 10-15 years ago. The median pack years of the participants was 48.
Participants’ comments related to study recruitment are shown in Table 4. As may be seen, the most common reasons for declining study participation were related to being fearful of the word “cancer,” not being interested in the study, being wary of the injury language in the informed consent document, feeling that the study was not a good fit, feeling that they were too busy to participate, having already made a decision to receive lung cancer screening, and focusing on other health problems.
The participants’ reported barriers to completing lung cancer screening were cost concerns, insurance coverage, and recent medical history that prevented study participation. These were the focal areas that were addressed by the study navigators.
4. Discussion
The purpose of this paper was to describe the design and interim recruitment results of a four-year Stand Up To Cancer® high-impact, multimodal, and multilevel patient navigation intervention to promote lung cancer screening among rural, urban, and medically underserved Black patients from federally qualified health centers. The intervention is focused on reducing barriers to ensure timely access to screening.
The study includes a unique lung cancer screening cohort that is younger, more likely to be unmarried, has lower levels of education, and includes more current smokers than the predominantly White NLST cohort. Therefore, the study results will shed a significant amount of light on the effects of the patient navigation intervention in a population that is at high risk of developing lung cancer.
The investigators will evaluate their future navigation study findings in relation to those of similar studies. For example, Lee et al. [32] examined the effects of a telephone-based patient navigation intervention in enhancing lung cancer screening rates among patients in the context of a pragmatic randomized controlled trial in a safety-net health care system [32]. A total of 225 patients (55% of whom were Black, 15% of whom were Hispanic, and 30% of whom were White) were enrolled in the study navigation arm. Among the 225 navigation study participants, the navigators identified 559 barriers to screening during 806 telephone calls with the participants. The barriers included personal barriers (40% of the total number of barriers), followed by provider (30%) and practical barriers (17%). During the intervention, a decrease of 80% was seen in provider-related barriers (p=0.008).
In another similar study, Bhalla et al. [33] evaluated data from 447 patients in a randomized trial of patient navigation to lung cancer screening (n=225) or usual care (n=222) in an urban safety-net hospital in Texas. The participants included a diverse group; 69% were racial/ethnic minorities. The investigators found that an organizational barrier, the lack of clinician ordering of the lung cancer screening, was a major impediment to receipt of screening among the navigated participants.
In future analyses, we will examine potential differences in the navigation results (including the barrier types, number of barriers, and resolution of barriers) of the current study, which includes a sample comprised entirely of Black patients, in comparison with the results from the more diverse samples in previous lung cancer screening navigation studies.
5. Conclusions
The SU2C study team has developed a novel strategy for lung cancer screening navigation that could become the gold standard of care for socially vulnerable and high-risk populations. The study participants, who were first-time recipients of lung cancer screening, likely only received it because of their participation in the study. With recent cuts to publicly funded health benefits, the need for a broader application of the patient navigation approach may be greater than ever.
Abbreviations
| FQHC | Federally qualified health center |
| LCS | Lung cancer screening |
| SU2C | Stand Up 2 Cancer |
| USPSTF | U.S. Preventive Services Task Force |
| NIMHD | National Institute on Minority Health and Health Disparities Research Framework |
| NLST | National Lung Screening Trial data |
References
- American Cancer Society. Cancer Facts & Figures 2025. American Cancer Society. Accessed August 1, 2025. https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/2025-cancer-facts-figures.html.
- Barker AM, Wiener RS, Reisman J, Kearney L, Dones M, Fix GM. Black US military veterans respond favourably to a booklet using narratives to normalise shared decision-making. Public Health Pract (Oxf). Jun 2025;9:100606. [CrossRef]
- Jaferian S, Love T, Singh SK, Xie Y, Hill E, Ryan Wolf J. Racial and urban-rural disparities in lung cancer care: Insight from a Latent Class Growth Analysis. J Cancer Policy. Jun 2025;44:100585. [CrossRef]
- Butler DC, Petterson S, Phillips RL, Bazemore AW. Measures of social deprivation that predict health care access and need within a rational area of primary care service delivery. Health Serv Res. Apr 2013;48(2 Pt 1):539-59. [CrossRef]
- Moyer VA, Force USPST. Screening for lung cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. Mar 4 2014;160(5):330-8. [CrossRef]
- Rivera MP, Katki HA, Tanner NT, et al. Addressing Disparities in Lung Cancer Screening Eligibility and Healthcare Access. An Official American Thoracic Society Statement. Am J Respir Crit Care Med. Oct 1 2020;202(7):e95-e112. [CrossRef]
- Korn AR, Walsh-Bailey C, Correa-Mendez M, et al. Social determinants of health and US cancer screening interventions: A systematic review. CA Cancer J Clin. Sep-Oct 2023;73(5):461-479. [CrossRef]
- Ferguson MK, Demchuk C, Wroblewski K, et al. Does Race Influence Risk Assessment and Recommendations for Lung Resection? A Randomized Trial. Ann Thorac Surg. Oct 2018;106(4):1013-1017. [CrossRef]
- Henley SJ, Anderson RN, Thomas CC, Massetti GM, Peaker B, Richardson LC. Invasive Cancer Incidence, 2004-2013, and Deaths, 2006-2015, in Nonmetropolitan and Metropolitan Counties—United States. MMWR Surveill Summ. Jul 7 2017;66(14):1-13. [CrossRef]
- Mokdad AH, Dwyer-Lindgren L, Fitzmaurice C, et al. Trends and Patterns of Disparities in Cancer Mortality Among US Counties, 1980-2014. JAMA. Jan 24 2017;317(4):388-406. [CrossRef]
- Zafar SY, Abernethy AP. Financial toxicity, Part I: a new name for a growing problem. Oncology (Williston Park). Feb 2013;27(2):80-1, 149.
- Zafar SY, McNeil RB, Thomas CM, Lathan CS, Ayanian JZ, Provenzale D. Population-based assessment of cancer survivors’ financial burden and quality of life: a prospective cohort study. J Oncol Pract. Mar 2015;11(2):145-50. [CrossRef]
- Turrini G BD, Chen L, Conmy AB, Chappel AR, De Lew N. Access to Affordable Care in Rural America: Current Trends and Key Challenges(Research Report No. HP-2021-16). Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services Accessed August 1, 2025. https://aspe.hhs.gov/sites/default/files/documents/09e40880648376a13756c59028a56bb4/rural-health-rr.pdf.
- Mitchell A, Muluneh B, Patel R, Basch E. Pharmaceutical assistance programs for cancer patients in the era of orally administered chemotherapeutics. J Oncol Pharm Pract. Sep 2018;24(6):424-432. [CrossRef]
- Spencer JC, Samuel CA, Rosenstein DL, et al. Oncology navigators’ perceptions of cancer-related financial burden and financial assistance resources. Support Care Cancer. Apr 2018;26(4):1315-1321. [CrossRef]
- Biddell CB, Spees LP, Petermann V, et al. Financial Assistance Processes and Mechanisms in Rural and Nonrural Oncology Care Settings. JCO Oncol Pract. Sep 2022;18(9):e1392-e1406. [CrossRef]
- Bach PB, Pham HH, Schrag D, Tate RC, Hargraves JL. Primary care physicians who treat blacks and whites. N Engl J Med. Aug 5 2004;351(6):575-84. [CrossRef]
- Wells KJ, Battaglia TA, Dudley DJ, et al. Patient navigation: state of the art or is it science? Cancer. Oct 15 2008;113(8):1999-2010. [CrossRef]
- Sherman DE. Transforming Practices Through the Oncology Care Model: Financial Toxicity and Counseling. J Oncol Pract. Aug 2017;13(8):519-522. [CrossRef]
- Reeder-Hayes KE, Biddell CB, Manning ML, et al. Knowledge, Attitudes, and Resources of Frontline Oncology Support Personnel Regarding Financial Burden in Patients With Cancer. JCO Oncol Pract. Aug 2023;19(8):654-661. [CrossRef]
- Alvidrez J, Castille D, Laude-Sharp M, Rosario A, Tabor D. The National Institute on Minority Health and Health Disparities Research Framework. Am J Public Health. Jan 2019;109(S1):S16-S20. [CrossRef]
- Freeman HP, Muth BJ, Kerner JF. Expanding access to cancer screening and clinical follow-up among the medically underserved. Cancer Pract. Jan-Feb 1995;3(1):19-30.
- Vargas RB, Ryan GW, Jackson CA, Rodriguez R, Freeman HP. Characteristics of the original patient navigation programs to reduce disparities in the diagnosis and treatment of breast cancer. Cancer. Jul 15 2008;113(2):426-33. [CrossRef]
- Swanson GM, Ward AJ. Recruiting minorities into clinical trials: toward a participant-friendly system. J Natl Cancer Inst. Dec 6 1995;87(23):1747-59. [CrossRef]
- Biddell CB, Waters AR, Angove RSM, et al. Facing financial barriers to healthcare: patient-informed adaptation of a conceptual framework for adults with a history of cancer. Front Psychol. 2023;14:1178517. [CrossRef]
- Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. Nov 2005;15(9):1277-88. [CrossRef]
- NPIdb. Federally Qualified Health Center (FQHC)—261QF0400X — South Carolina. Accessed June 7, 2025. https://npidb.org/organizations/ambulatory_health_care/federally-qualified-health-center-fqhc_261qf0400x/sc/.
- Health Resources & Services Administration. Health Center Program Uniform Data System (UDS) Data Overview. Department of Health & Human Services. August 1, 2025. https://data.hrsa.gov/tools/data-reporting/program-data?grantNum=H80CS00293.
- NCDHHS Division of Public Health. NC State Center for Health Statistics. SCHS: Cancer Incidence Data Visualization Tools. Cancer Incidence Rates by County NC Department of Health and Human Services. Accessed August 1, 2025. https://schs.dph.ncdhhs.gov/data/cancer/county_yearly_incidence.html.
- NCIOM. North Carolina Health Data. North Carolina Institute of Medicine (NCIOM). Accessed August 1, 2025. https://nciom.org/nc-health-data/.
- Crossing the Quality Chasm: A New Health System for the 21st Century. 2001.
- Lee SJC, Lee J, Zhu H, et al. Assessing Barriers and Facilitators to Lung Cancer Screening: Initial Findings from a Patient Navigation Intervention. Popul Health Manag. Jun 2023;26(3):177-184. [CrossRef]
- Bhalla S, Natchimuthu V, Lee JL, et al. Effect of Patient Navigation on Completion of Lung Cancer Screening in Vulnerable Populations. J Natl Compr Canc Netw. Mar 15 2024;22(3):151-157. [CrossRef]
Figure 1.
Examples of categories of barriers within the patient navigation intervention.
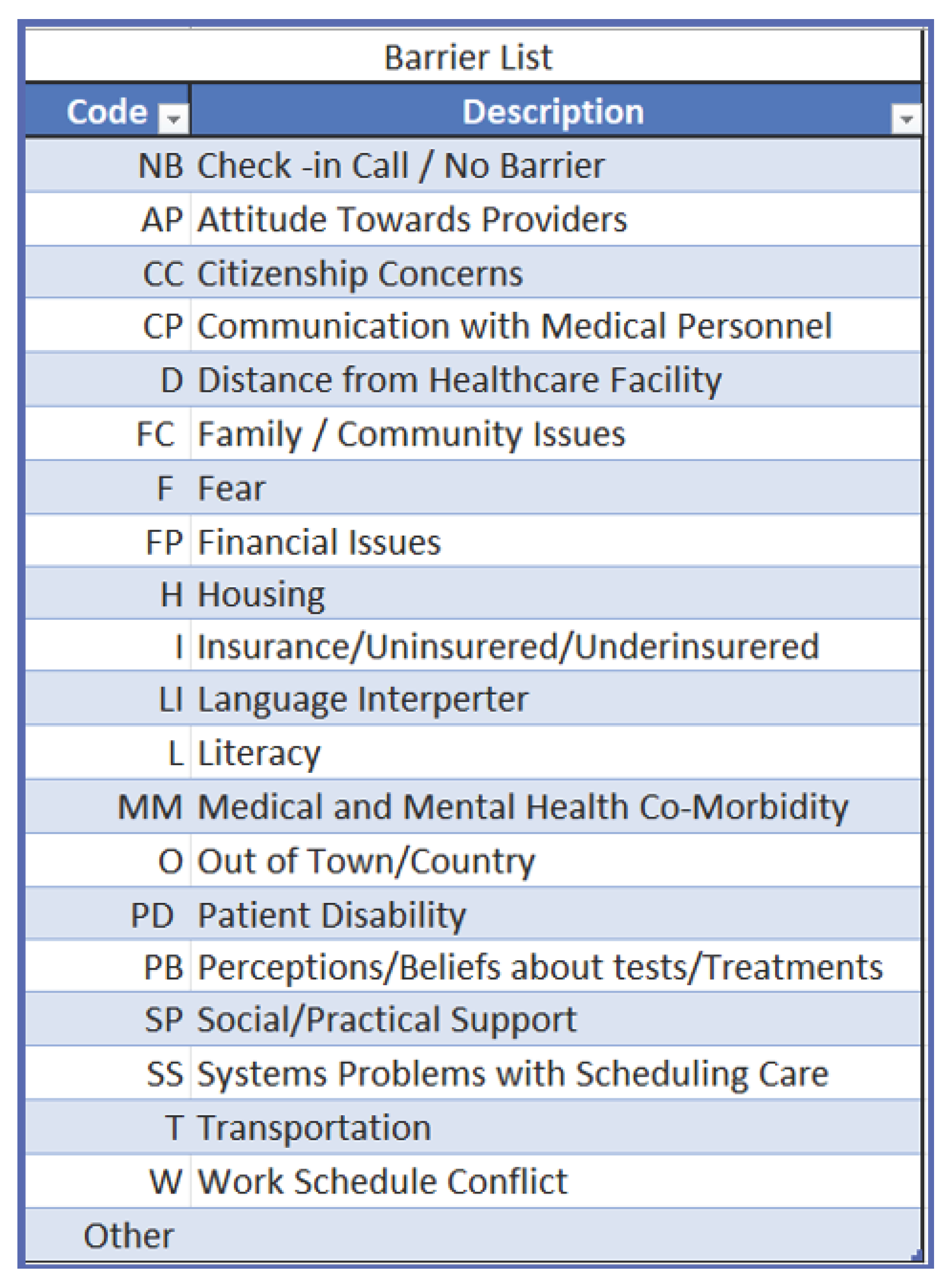
Figure 2.
Examples of expanded categories of barriers within the patient navigation intervention.
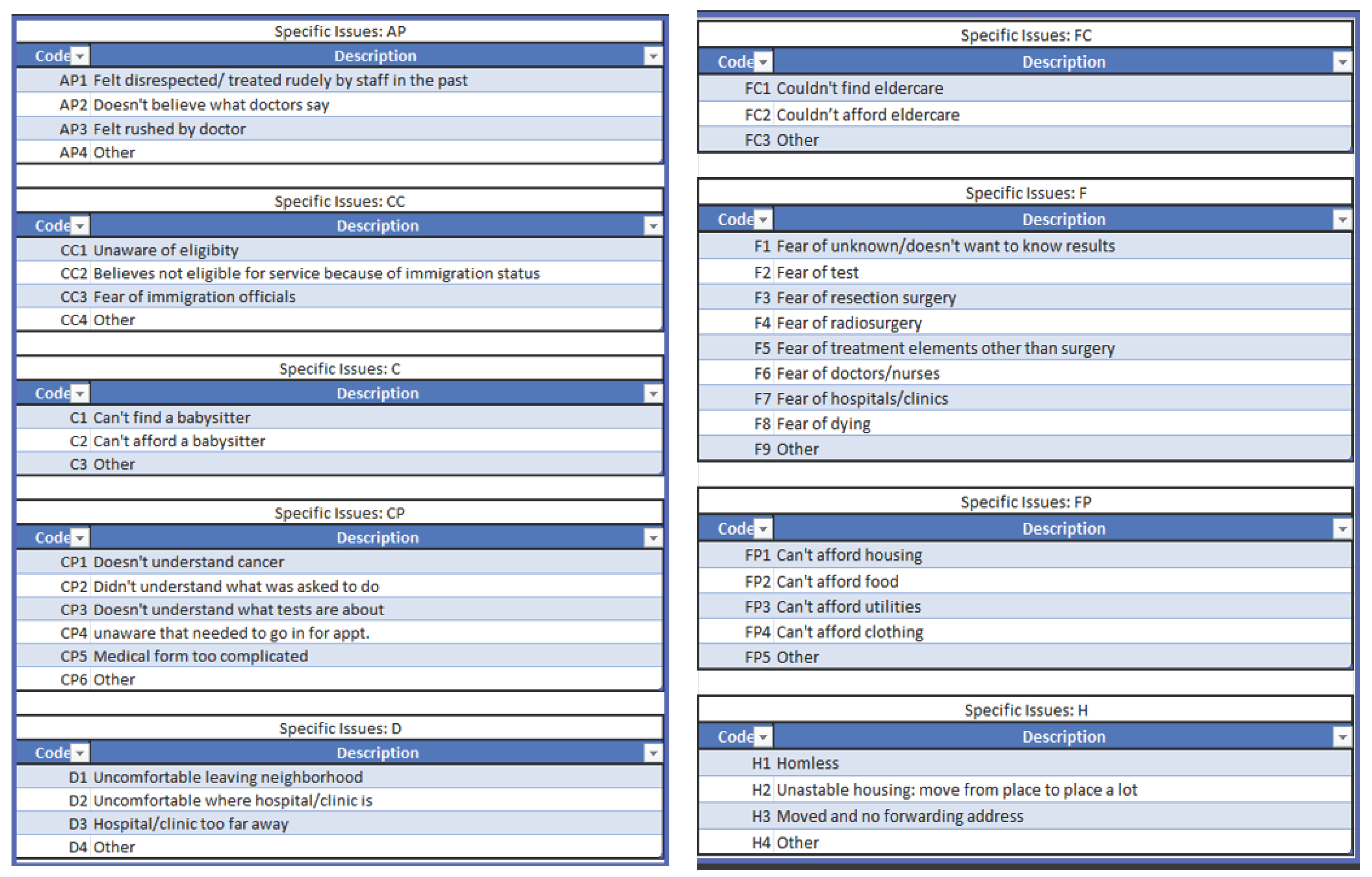
Figure 3.
The general categories of actions taken by the study’s patient navigators to address the barriers identified by each participant.
Figure 3.
The general categories of actions taken by the study’s patient navigators to address the barriers identified by each participant.
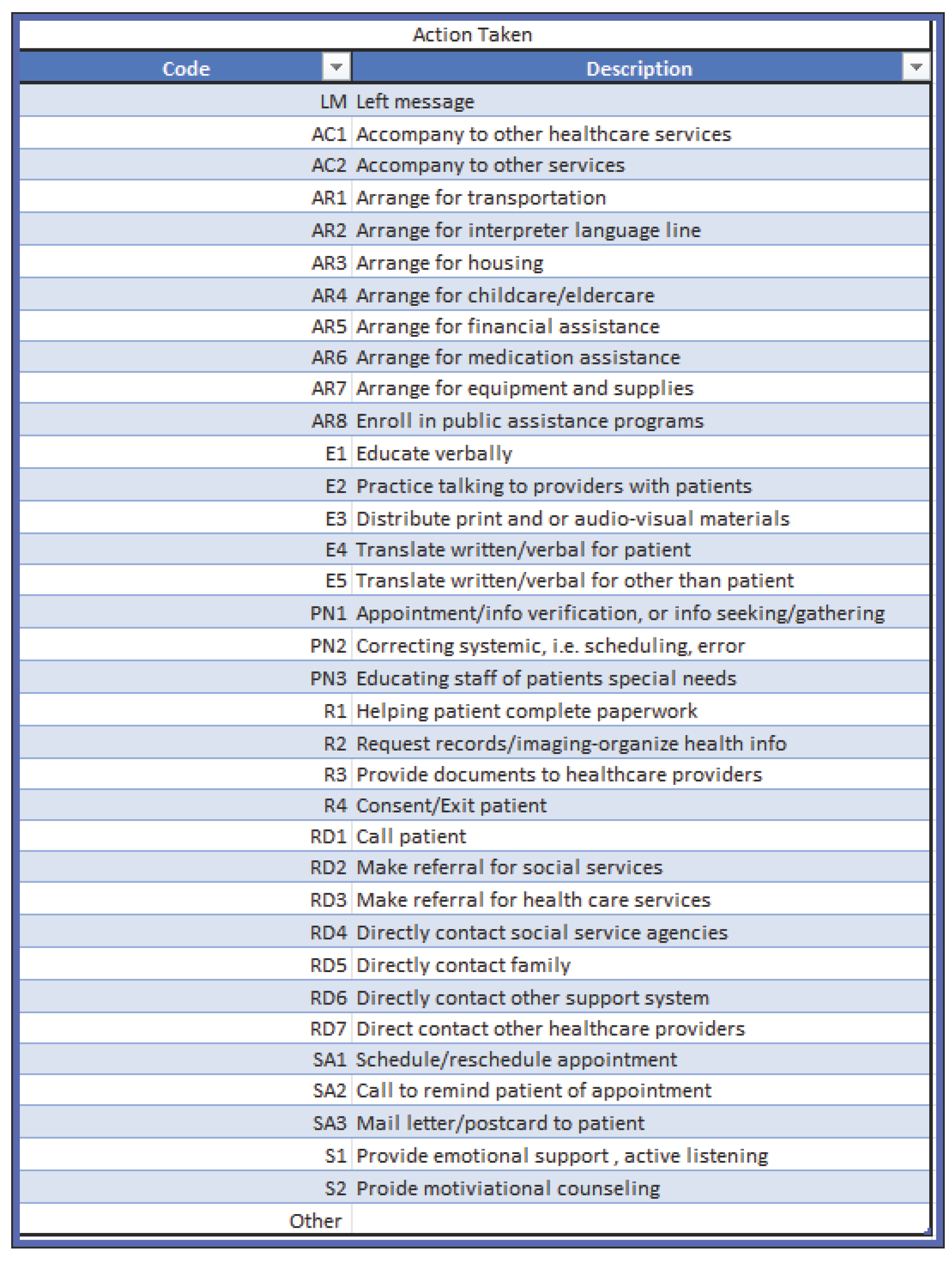

Table 1.
Stand Up To Cancer® (SU2C) Lung Cancer Screening Navigation Training Modules.
| Module 1: Research 101 | Objectives
|
| Module 1.2: Overview of Health Disparities in Lung Cancer Screening and Treatment | Objectives
|
| Module 2: Patient Navigators: Roles and Responsibilities | Objectives
|
| Module 3: Overcoming Barriers to Care | Objectives
|
| Module 4: Health Literacy | Objectives
|
| Module 5: Communication Exercise Tool | Objectives
|
| Module 5.1: Effective Communication | Objective
|
| Module 5.2: Communication and Patient Navigation | Objectives
|
| Module 6: Developing Cultural Competency/ Cultural Humility in Cance Clinical Trials Research | Objectives
|
| Module 6.1: Developing Cultural Humility in Health Care | Objectives
|
Table 2.
Navigational Activities by Domain.
| Individual | Economic |
|
|
| Organizational | Sociocultural |
|
|
Table 3.
Characteristics of Current SU2C Aim 1 Cohort, as Compared to the NLST Cohort.
| Characteristic | SU2C Cohort Aim 1 (N=170) |
NLST LDCT Arm (N=26,723) |
|---|---|---|
| Age Group, years | ||
| 50-54 | 7.65% | 0.01% |
| 55-64 | 44.12% | 73.38% |
| 65-74 | 34.70% | 26.60% |
| 75-79 | 8.82% | 0.00% |
| Missing | 4.71% | 0.00% |
| Sex | ||
| Female | 37.06% | 40.99% |
| Male | 62.94% | 59.01% |
| Race | ||
| Black | 100.00% | 4.48% |
| Marital status | ||
| Married / living with partner | 15.29% | 66.67% |
| Divorced | 11.18% | 19.44% |
| Separated | 5.29% | 1.26% |
| Widowed | 11.76% | 7.43% |
| Single | 30.59% | 4.70% |
| Don’t know/unsure | 25.89 | 0.00% |
| Education | ||
| Less than high school | 40.00% | n/a |
| High school or GED | 25.29% | 6.14% |
| Some College / Associates degree | 18.82% | 23.48% |
| Bachelor degree | 5.89% | 14.10% |
| Don’t know/unsure | 10.00% | 0.00% |
| Smoking status | 23.43% | |
| Current | 83.53% | 16.86% |
| Former | 16.47% | 14.70% |
| Among those who quit, time (years) since quit smoking | ||
| Within 4 years | 6.47% | 14.76% |
| 4-9.9 years | 4.11% | 17.21% |
| 10-15 years | 3.53% | 19.67% |
| Missing | 2.35% | 0.21% |
| Median pack years | 28 | 48 |
Abbreviations: Stand Up to Cancer®=SUTC; National Lung Screening Trial = NLST; Low-Dose CT = LDCT; General Educational Development High School Equivalency Diploma = GED.
Table 4.
Participants’ Comments Related to Study Recruitment.
| Common Reasons for Declining Participation | Common Concerns/Obstacles to Engaging in Lung Cancer Screening | Satisfaction with the Multimodal Navigation Approach |
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



