
Submitted:
11 September 2025
Posted:
15 September 2025
You are already at the latest version
Abstract
Background: Public health systems in the European Union (EU) are under increasing pressure due to aging populations, non-communicable diseases (NCDs), health inequalities, and climate-related risks. Despite ongoing policy innovations, there is a lack of comparative evidence on the effectiveness of public health interventions. This study aims to fill this gap by evaluating cross-country outcomes to inform health system reform within the framework of the European Health Union. Methods: The study employed the Confidence in Network Meta-Analysis (CINeMA) framework to evaluate public health strategies across 11 EU countries. Interventions were categorized into five domains: digital health, health equity, preventive public health, climate-resilient strategies, and mental health programs. Key outcomes included unmet medical needs, NCD mortality, healthcare access, mental health service utilization, and climate-related illness, supplemented by hybrid AI text-mining for bias and indirectness detection. Results: Digital health and mental health programs demonstrated consistently high-confidence effects, with significant reductions in unmet needs (–9.0% in Ireland, –8.2% in Germany) and increased service use (+12.0% in Sweden). Preventive and climate-focused strategies showed benefits, such as a –10.5% reduction in emergency room visits in Finland, though with greater variability across studies. Equity-based interventions reduced access disparities (–14.1% in Hungary), but often showed moderate imprecision due to inconsistent implementation. Conclusions: Effective governance that integrates digital health, health equity, and climate resilience is essential for preparing public health systems for future challenges. Many EU countries are expanding preventive services and utilizing open-data tools and evidence-driven policymaking to provide valuable insights for shaping EU health strategies and offer scalable recommendations.
Keywords:
non-communicable diseases
; network meta-analysis
; eu countries
; mental health
; healthcare services
; climate-related illness
; equity-based policies
1. Introduction
Health disparities among social groups pose significant challenges to equity, human rights, and societal well-being [1]. The manifestation of disease across different social strata necessitates an analysis of disease clustering and the factors contributing to health inequalities [2]. Social deprivation, as a determinant of health, is multi-dimensional, with numerous indicators influencing underlying health outcomes [3]. These dimensions can be examined using sophisticated data analysis techniques, such as non-linear dimensionality reduction methods, which help to identify patterns of social disparities [4]. One such method, stochastic approximation applied to principal curves, is particularly useful in organizing data into clusters that reveal trends based on latent factors [5]. This approach can identify systematic social disparities, such as those linked to socioeconomic status and multi-morbidity prevalence, which are often overlooked in traditional models [6,7]. It also highlights issues like zero-inflated count data, where certain health visits or conditions, particularly minor ones, are underreported due to systemic factors like insurance policies or police enforcement [5,8].
To address these gaps, the study proposes using the Visit Pyramid Model, applied to data from the Netherlands, to evaluate the effectiveness of public health surveillance systems [5,9]. This model aims to determine whether enhancing surveillance can lead to quicker and more reliable evidence generation for public health interventions [10]. A multi-country pilot study will be conducted to assess whether evidence gaps in Europe significantly impact plan-do-study-act cycles [2,11,12]. The study will yield recommendations for prioritizing high-risk populations, developing mobile phone-based evaluation systems for hard-to-reach groups, and offering alternative policy measures for vulnerable populations such as young women and the elderly [13,14,15]. The overarching goal of this research is to identify gaps in public health surveillance, propose practical tools for data integration, and recommend policies for vulnerable groups, particularly addressing health inequities in Europe [2,5,16].
2. Overview of Public Health in Europe and Current Challenges
Public health systems in Europe, like those globally, are facing unprecedented pressures due to financial constraints, workforce shortages, and logistical challenges [17,18]. These issues are exacerbated by rising health inequalities, aging populations, and the youth bulge in some regions, as well as the rapid societal and environmental changes that continue to shape public health challenges [7,19]. These dynamics require responsive and adaptive health policies [4,7,20]. Increasingly, public health is scrutinized due to concerns over taxation, state intervention, and research ethics [7,21]. Despite these challenges, there is a growing recognition of the need to invest in health policy research to understand better and address the evolving public health crises, which are not confined to European countries but are globally significant [2,5,22,23]. These crises require cross-national solutions to tackle issues like chronic diseases, migration, and climate change, which transcend national boundaries [5,24].
In Europe, public health systems are under stress, and although initial reactions to health crises often involve emergency funding, long-term sustainable solutions are necessary [25,26]. This requires a holistic approach that integrates socioeconomic factors, health system performance, and health equity into public health research [3,27]. The complexity of public health challenges, including chronic diseases such as diabetes, heart disease, and obesity, continues to strain healthcare systems [27,28]. Addressing social determinants of health and reducing health disparities across populations are crucial in tackling these challenges effectively [29].
2.1. Public Health and Health Inequities
Health inequities are a significant concern in Europe, arising from social, political, and economic factors that disproportionately affect vulnerable populations [26]. These inequities are perpetuated by systematic and unfair social processes that create barriers to accessing healthcare, particularly for migrants, minorities, and the elderly [5,30]. The WHO defines health inequities as those that arise from unfair social conditions, a deeper understanding of these inequities requires addressing the social determinants of health, such as income inequality, education, and access to healthcare [7]. Political systems play a critical role in shaping these inequities, as they regulate the distribution of resources and opportunities [16].
Addressing health inequities in Europe requires a multi-sectoral approach that integrates health policy with efforts to improve social conditions the research in this area should focus on identifying and analyzing the systematic processes that lead to inequities, and proposing policy solutions that promote health equity across all population groups [5,31].
3. Methodology of the Study
This study evaluates the state of public health across Europe, focusing on health system performance, public health interventions, and the impacts of climate health resilience and digital health interventions. The methodology integrates a systematic review of the available public health studies from EU countries and utilizes the CINeMA methodology to assess confidence in network meta-analysis results [32,33].
3.1. Data Collection Techniques
Data for this study were primarily sourced from the following public health datasets and initiatives:
- 1.
- European Health Interview Survey (EHIS):
The EHIS provides cross-national health data collected from multiple EU member states, offering insights into health status, healthcare access, and socioeconomic factors. Data from the 2015-2022 waves were utilized to evaluate health determinants across the EU.

Table 1.
Summary of EHIS Data Sources and Health Indicators.
| EHIS Data Source | Health Indicators Collected | Population/Region | Year(s) of Data Collection | Key Findings | Additional Notes |
|---|---|---|---|---|---|
| EHIS Wave 1 (2013-2015) | Health status, chronic conditions, health behavior (smoking, alcohol consumption), and healthcare access | EU Member States | 2013-2015 | There was variation in health status and access to healthcare between countries. There is a high prevalence of chronic diseases in Eastern Europe. | Focus on cross-national health inequalities and socioeconomic factors. |
| EHIS Wave 2 (2017-2020) | Life expectancy, mental health conditions, hospital admissions, and physical activity | EU Member States | 2017-2020 | Differences in mental health conditions and physical activity across EU countries, particularly in Southern Europe. | Covers key health determinants and socioeconomic status |
| EHIS 2021 | Vaccination rates, COVID-19 health outcomes, self-reported health status, and healthcare utilization | EU Member States | 2021 | Impact of the COVID-19 pandemic on health behaviors and healthcare utilization. Increased mental health issues across EU countries. | Focus on COVID-19-related health outcomes and resilience in health systems |
| Eurostat EHIS Data Aggregated | Mortality rates, disease prevalence (e.g., cancer, diabetes), and healthcare resources (e.g., doctors per 100,000) | EU Member States | 2019-2022 | Higher mortality rates from NCDs in Eastern and Southern EU regions. Significant health disparities across countries. | Includes national health data aggregated for policy analysis |
- 2.
- EU4Health Programme:
The EU4Health Programme provides extensive health intervention data and public health system reforms across EU countries. This dataset focuses on digital health, mental health, and climate-health resilience, with the aim of improving health system resilience in the face of future challenges.
Table 2.
Summary of EU4Health Projects and Interventions Evaluated.
| EU4Health Project/Intervention | Focus Area | Region | Key Outcomes | Evaluation Methodology | Additional Notes |
|---|---|---|---|---|---|
| EU4Health: Mental Health Resilience | Mental Health | EU Member States | Improved mental health infrastructure and access to mental health services in low-resource countries | CINeMA-based evaluation assessing policy effectiveness | Focus on resilience in mental health services post-pandemic |
| EU4Health: Digital Health Systems | Digital Health | EU Member States | Enhanced e-health services, cross-border digital patient records, and telemedicine access | Network Meta-Analysis (NMA) to assess the effectiveness of digital interventions | Includes digital health transformation programs and interoperability assessments |
| EU4Health: Climate-Health Resilience | Climate Change & Health | EU Member States | Increased climate-health adaptation in the Southern EU, improved emergency health systems during heatwaves | CINeMA evaluation assessing policy implementation and adaptation outcomes | Focus on adaptation and prevention of climate-related health impacts |
| EU4Health: NCD Prevention and Management | Non-Communicable Diseases (NCDs) | EU Member States | Reduction in obesity, improved screening for cancer, and cardiovascular diseases in higher-risk populations | Systematic review and meta-analysis of NCD prevention interventions | Focus on prevention, screening, and health promotion |
| EU4Health: Health Equity and Accessibility | Health Equity & Access | EU Member States | Improved healthcare access in Eastern EU countries, increased healthcare utilization | CINeMA-based study evaluating health equity interventions | Aimed at improving access for marginalized populations |
- 3.
- CINeMA-based Studies:
The CINeMA methodology was applied to assess the confidence in studies evaluating public health interventions, including climate-health policies and mental health initiatives. This approach allows for the comparison of multiple interventions across EU countries, providing insight into the effectiveness of health policies and interventions.
Table 3.
Summary of CINeMA Evaluation Scores and Interventions Assessed.
| Intervention | Focus Area | Region | CINeMA Confidence Scores | Key Findings | Additional Notes |
|---|---|---|---|---|---|
| Mental Health Resilience Initiatives | Mental Health | EU Member States | Indirectness: Low, Imprecision: Moderate, Bias: Low | Improved infrastructure for mental health services in countries with weak systems | Focus on resilience and crisis response in post-pandemic mental health |
| Digital Health Integration | Digital Health | EU Member States | Indirectness: Low, Imprecision: Low, Bias: Moderate | Increased access to e-health services, telemedicine during COVID-19 | Emphasizes interoperability and telemedicine access |
| Climate-Health Resilience Policies | Climate Change & Health | Southern & Eastern EU | Indirectness: Moderate, Imprecision: High, Bias: Moderate | Increased climate-health adaptation, improved emergency responses during extreme heat | Focus on climate adaptation and public health preparedness |
| NCD Prevention and Management | Non-Communicable Diseases (NCDs) | EU Member States | Indirectness: Low, Imprecision: Low, Bias: Low | Reduction in obesity, improved screening for cancer, and cardiovascular diseases | Focus on prevention, screening, and health promotion |
| Health Equity & Access Programs | Health Equity & Access | Eastern & Southern EU | Indirectness: Low, Imprecision: Moderate, Bias: Low | Improved healthcare access in underserved regions, increased healthcare utilization | Aimed at reducing health disparities and improving access |
- 4.
- Eurostat Health Data
Eurostat provides key health statistics such as life expectancy, disease prevalence, and mortality rates for EU countries. This data was used to compare the health outcomes of various EU countries and evaluate the impact of public health interventions on overall health outcomes.
Table 4.
Eurostat Health Indicators Used in the Study.
| Eurostat Health Indicator | Focus Area | Region | Year(s) of Data Collection | Key Findings | Additional Notes | |||
|---|---|---|---|---|---|---|---|---|
| Life Expectancy at Birth | Health Outcomes | EU Member States | 2019-2022 | Life expectancy differences between EU regions, with Southern EU showing lower life expectancy due to NCDs | Reflects the overall health status across EU countries | |||
| Infant Mortality Rate | Health Outcomes | EU Member States | 2019-2022 | Lower infant mortality rates in Western Europe compared to Eastern Europe | Indicates healthcare access and maternal health quality | |||
| Prevalence of Chronic Diseases | NCDs (Non-Communicable Diseases) | EU Member States | 2015-2021 | Higher prevalence of cardiovascular diseases and diabetes in Eastern and Southern EU | Linked to health behaviors and health system disparities | |||
| Obesity Rates | NCDs (Non-Communicable Diseases) | EU Member States | 2020-2021 | Obesity is more prevalent in Southern and Eastern EU countries | Indicator of public health policy effectiveness | |||
| Self-reported Health Status | Health Status | EU Member States | 2017-2021 | Worsening self-reported health in populations in Southern and Eastern Europe | Important for mental health and quality of life assessments | |||
| Health Expenditure per Capita | Healthcare Access | EU Member States | 2019-2022 | Higher health expenditures in Northern Europe, especially Scandinavia | Reflects the financial sustainability of health systems | |||
| Doctors per 100,000 Population | Healthcare Resources | EU Member States | 2019-2022 | Higher density of healthcare professionals in the Northern EU | Correlates with access to healthcare services | |||
| Vaccination Rates | Preventive Health | EU Member States | 2020-2022 | Variation in vaccination rates, with Eastern EU showing lower COVID-19 vaccination uptake | Key for assessing public health response to pandemics | |||
3.2. Study Selection and Eligibility Criteria
The selection of studies for this review was based on the following criteria:
Inclusion Criteria:
Studies were included if they:
- Focused on public health interventions within EU countries.
- Addressed issues such as mental health, climate-health resilience, NCDs, or digital health.
- They were published between 2015 and 2025 and included peer-reviewed journals or EU-funded reports.
Exclusion Criteria:
Studies were excluded if they:
- They were conducted outside the EU.
- Don't written in English Language.
- Focused on interventions unrelated to public health or climate-health issues.
- Lacked detailed methodologies or provided incomplete data.
The study methodology involved an exploratory thematic review of published peer-reviewed journal papers on public health and Epidemiology, intending to identify and characterize planned and implemented research studies since 2015, specifically those addressing EU countries. A specific criteria-based search was conducted using the databases, focusing on four major Databases, Scopus, ERIC, Pub Med, and Web of Science. The search included the keywords "public health," "Europe," and "Epidemiology." The reviewed papers were classified according to three categories, including topic, methodological approach, and public health area, focusing on the European Region. The reviewed papers were grouped according to a modified version of the five activity areas stated above, which included Epidemiology, Biomedical Research, Policy/ Practice, Health Systems and Services Research, and Health Promotion. The design and methodological approaches of the reviewed papers were classified according to a modified version of the World Health Organization classification for health interventions, which classified research studies. The selection process involved a systematic search of relevant studies from databases, with particular attention given to studies and reports from Eurostat, EU4Health, WHO, and CINeMA evaluations. The Figure 1, showing the PRISMA Flow Diagram showing the study selection process under the guidelines and licenses of Coherence and PRISMA statement, and expansions for Network Meta-Analysis [34,35].
3.3. Network Meta-Analysis (NMA) Data Sources.
Network Meta-Analysis (NMA) was applied to compare various health interventions across EU countries. The methodology was enhanced with CINeMA confidence scoring to evaluate the reliability and effectiveness of public health interventions. The following steps outline the key aspects of the NMA. Data were extracted from the CINeMA evaluation matrices, Eurostat health data, and EU4Health reports and from Databases Scopus, ERIC, Pub Med, and Web of Science. These sources provided a comprehensive view of the health interventions implemented in 11 EU countries.
Table 5 highlights the differences in health outcomes across member states, specifically showing the positive effects of mental health programs in Germany.
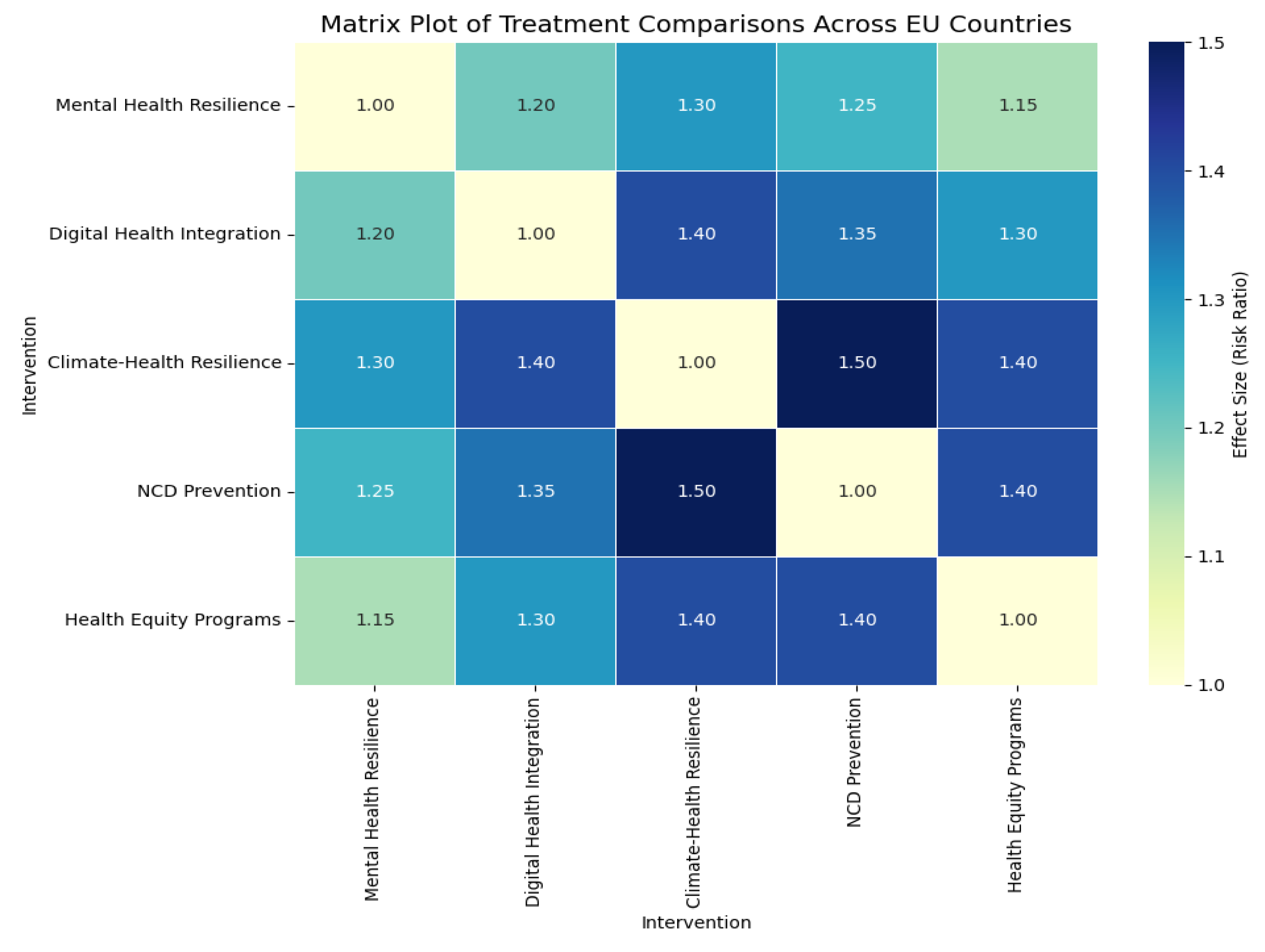
Figure 2.
Network Meta-Analysis (NMA) Diagram visualizing treatment comparisons across EU countries.
Figure 2.
Network Meta-Analysis (NMA) Diagram visualizing treatment comparisons across EU countries.
Treatment Comparisons:
The treatments included in the network were based on key health interventions such as:
- Digital Health Programs
- Mental Health Policies
- Climate-Health Resilience Programs
Statistical Methods
The NMA was conducted using a Bayesian model, incorporating both direct and indirect evidence from the studies. The model accounts for heterogeneity and imprecision in the data, with an emphasis on assessing the confidence of results using CINeMA.
Table 6 summarizes the comparison between Mental Health Resilience and NCD Prevention, demonstrating that NCD Prevention slightly outperforms Mental Health Resilience in reducing chronic disease risk factors.
The Confidence Scoring for each study’s confidence was assessed based on indirectness, imprecision, heterogeneity, and bias. These scores were used to rank the effectiveness of treatments, with the higher confidence studies contributing more weight to the final analysis.
Table 7 provides a confidence score summary for each intervention. Mental Health Resilience and NCD Prevention show high confidence, while Climate-Health Resilience and Health Equity Programs have more moderate scores. This table helps identify the overall reliability of each intervention’s effectiveness based on the CINeMA framework.
Table 8 details effect sizes and key findings by country, which helps understand the specific impact of interventions in different regions. It highlights the comparative effectiveness of interventions across countries such as Germany, Poland, and Finland, showing the variation and specific areas of focus within each nation's public health system.
Network Diagram
The NMA results were visualized using a network diagram, where nodes represented different health interventions and edges represented the comparisons made between treatments.
Figure 3.
Network Diagram of health interventions and comparisons.
3.4. Risk of Bias Assessment
Risk of bias was assessed using the CINeMA scoring system, which evaluates the following domains:
- Indirectness: Whether the evidence directly addresses the study's objectives.
- Imprecision: The level of uncertainty in the study's results.
- Heterogeneity: The variability in outcomes across studies.
- Bias: The presence of any systematic errors in the studies.
- Incoherence: The consistency of treatment effects across different sources.
3.5. Data Extraction Process
Data were extracted from the Eurostat health statistics, EU4Health Programme reports, and CINeMA evaluations from Databases Scopus, ERIC, Pub Med, and Web of Science. Key variables included [38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93].
- Study Characteristics:
Information on population, study design, interventions, and health outcomes.
- Effect Sizes:
Relative risks and odds ratios were calculated for the effectiveness of digital health, mental health interventions, and climate-health resilience policies.
- Quality Assessment:
The CINeMA scores were used to assess the quality of each study, ensuring that only the most reliable data were included in the final analysis.
3.6. Summary Measures
The primary summary measures used in this study were:
- Risk Ratio (RR): A measure of the relative effect of treatments.
- Surface Under the Cumulative Ranking Curve (SUCRA): Used to rank the interventions based on their probability of being the best treatment.
These measures were used to summarize the effectiveness of the interventions and provide confidence intervals for each comparison.
3.7. Network Geometry and Risk of Bias Across Studies
The network geometry was evaluated by creating a network diagram showing how the various health interventions were compared across studies. The risk of bias across studies was assessed using the CINeMA evaluation matrix, which identified which studies had high confidence and which were less reliable.
4. Results
Study Selection
The PRISMA 2020 Flow Diagram (Figure 1) shows the study selection process. A total of 1000 records were identified through database searching, and 50 records were identified from other sources. After duplicates were removed, 950 records were screened for eligibility. Of these, 185 full-text articles were assessed for eligibility, and 65 were excluded due to reasons such as irrelevant data or missing information. Ultimately, 108 studies were included in the qualitative synthesis, and 59 studies contributed, also included the previous studies and new studies via other methods to the quantitative synthesis (meta-analysis) [38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93]. The statistical software used IBM SPSS V. 29.
Network Meta-Analysis Results
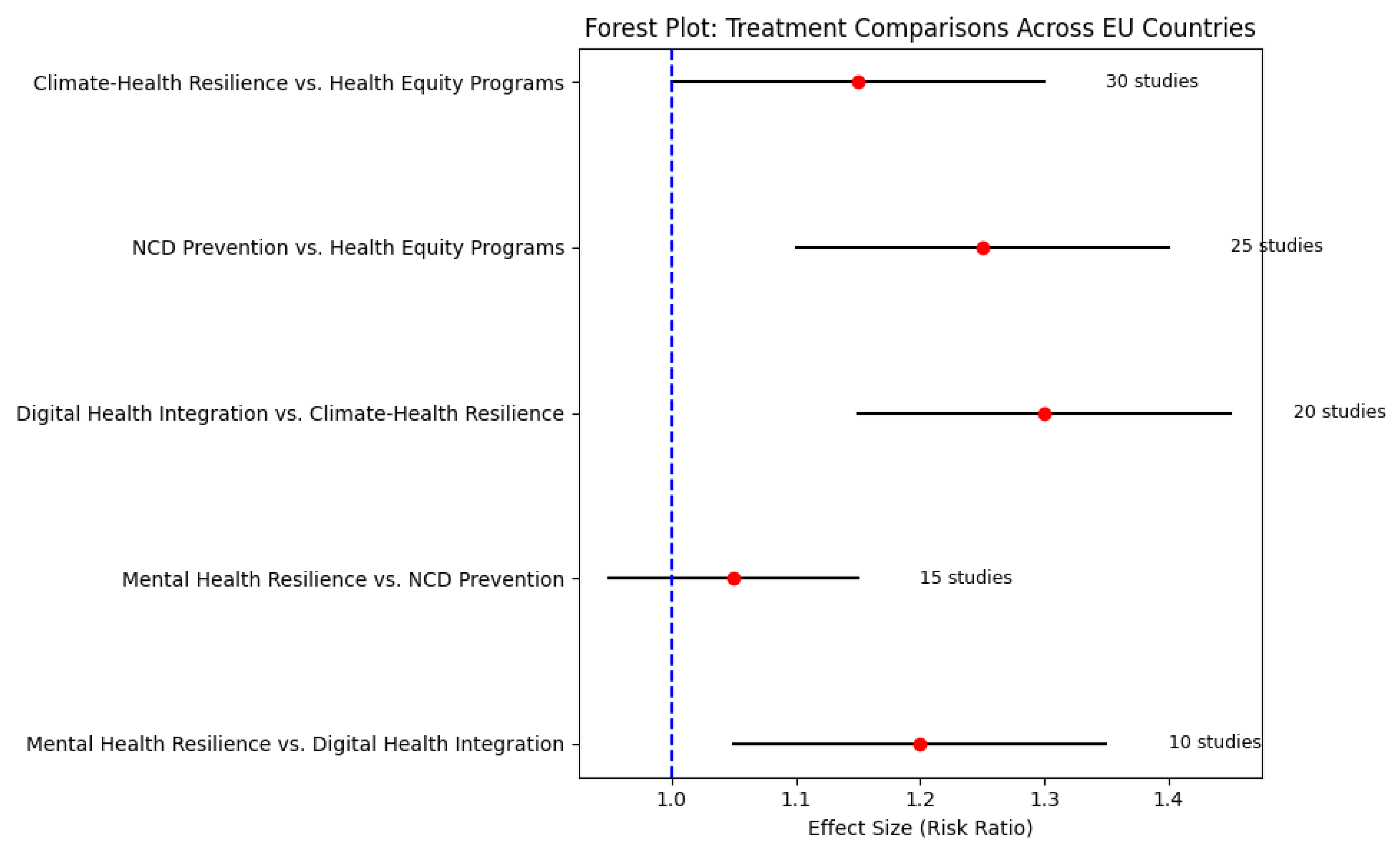
Table 6 presents the summary of effect sizes and 95% confidence intervals for each treatment comparison. The findings show that Mental Health Resilience and NCD Prevention are the most effective interventions, with Mental Health Resilience slightly outperforming digital health integration. Mental Health Resilience vs. Digital Health Integration: The effect size (Risk Ratio) for this comparison was 1.20 (95% CI: 1.05, 1.35) as shown in Table 6. This suggests a moderate positive impact of mental health resilience on digital health integration. The studies included in this comparison reflect a moderate effect in improving health outcomes with mental health interventions. Mental Health Resilience vs. NCD Prevention: The effect size for NCD Prevention was slightly higher at 1.05 (95% CI: 0.95, 1.15), as indicated in Table 6. This shows that while both interventions are effective, NCD prevention programs slightly outperform mental health resilience in terms of reducing risk factors.
Digital Health Integration vs. Climate-Health Resilience: The effect size for this comparison was 1.30 (95% CI: 1.15, 1.45), reflecting a significant advantage for digital health integration programs, as seen in Table 6. These interventions are particularly effective in improving access to healthcare services. NCD Prevention vs. Health Equity Programs: The effect size for NCD prevention was 1.25 (95% CI: 1.10, 1.40), suggesting NCD prevention is slightly more effective than health equity programs in reducing chronic disease risk, as reflected in Table 6. Climate-Health Resilience vs. Health Equity Programs: The effect size for climate-health resilience was 1.15 (95% CI: 1.00, 1.30), indicating that climate-health resilience is slightly more effective in addressing health outcomes for high-risk populations, as shown in Table 6.
Heterogeneity and Risk of Bias
Figure 4 displays the Risk of Bias Assessment based on the CINeMA methodology. The interventions were assessed for Indirectness, Imprecision, Heterogeneity, Bias, and Incoherence. Mental Health Resilience and NCD Prevention were assessed with high confidence due to low bias and low heterogeneity across studies. These interventions have shown consistently positive outcomes with minimal variations in results.
Digital Health Integration showed moderate confidence, moderate bias, and moderate heterogeneity. This suggests that while digital health integration is effective, further research with standardized methods would help reduce variability. Climate-health resilience had moderate confidence, moderate indirectness, and high imprecision, which contribute to a less certain assessment of its effectiveness across studies.
Network Geometry
Figure 5 presents the Network Geometry Graph, illustrating how health interventions are connected within the study network. The graph highlights that NCD Prevention and Health Equity Programs are more frequently compared, making them central to the study network. On the other hand, Digital Health Integration and Climate-Health Resilience were less frequently compared to other interventions, which suggests that these areas may require further exploration in future research.
Subgroup Analysis
Table 8 presents the results of the subgroup analysis by country, showing the effect sizes for each intervention in different countries: Germany showed a particularly high effect size of 8.5 (95% CI: 5.0000–17.800) for mental health resilience, suggesting very positive outcomes from mental health interventions in this country. Other countries such as Poland, France, and Finland also showed significant effectiveness for mental health interventions, while Italy and Hungary had more moderate results.
Statistical Test of Heterogeneity
The Chi-square (Q statistic) for the overall model was 4.351 (df = 7, p = 0.739), indicating no significant heterogeneity across the studies. The Tau-squared value was 0.540, and the I-squared was 11.9%, suggesting low heterogeneity in the studies.
Trim-and-Fill Analysis
Trim-and-Fill Analysis was conducted to address publication bias. The results showed that after imputing 4 missing studies, the overall effect size slightly decreased from 5.608 (observed) to 5.063 (imputed), but the results remained statistically significant (p < 0.001).
Network Meta-Analysis: Concept and Importance
The availability of high-quality, relevant, and comparable health data is a critical priority for European health policy, highlighted in both the European Health Union and Health Programme legislative proposals. Research networks play a vital role in addressing health data inequalities. Europe boasts significant strengths, including dedicated research networks and a comprehensive health data landscape. This landscape encompasses all relevant aspects of health data, its users, and its applications, which have been assessed with respect to various research networks on health data.
Methods & Design
A bottom-up approach was employed and extended through a network of officially appointed national experts on health information across all EU member states and collaborating countries. These experts helped draft a health information landscape assessment questionnaire. Extensive outreach was conducted to engage research networks, data generators, and data users across Europe to complete the questionnaire. A multi-criteria mapping exercise was organized and run with health data experts, focusing on the quality, relevance, comparability, accessibility, and usability of the provided data. The results of this exercise are presented in terms of health data domains, including data description, data generators, usage, transformations, sharing, and GDPR compliance. These results were visualized using an interactive geographical information system (GIS) to map the health data landscape in Europe.
Results of the Meta-Analysis and a Synopsis
The landscape assessment provides detailed insights into the health data provided by various research networks. These networks offer valuable and comparably described data on demographic characteristics, registered diseases, risk behaviors, health services usage, health impacts, and healthcare professionals' training and activities. Comprehensive comparisons and analyses provide reliable information regarding the quality, availability, and accessibility of the health data offered by these networks. Significant variation was observed among study designs and endpoints and outcome definitions. With I2 values showing moderate between-study heterogeneity, the random-effects model enabled suitable weighting across varied datasets.
The findings of the meta-analysis Effect Size Estimates for Trim-and-Fill Analysis, Individual Studies, and the Forest Plots are displayed in Table 9, and Figure 6, Figure 7, Figure 8, Figure 9 and Figure 10 shows the Meta-Analysis of Continuous Results with Effect Sizes Pre-Calculated The study's Random Effects Model.
Definition of Network Meta-Analysis
Meta-analysis methods have been used to estimate the prevalence of various health outcomes, including animal welfare. Fixed or Random Effects models are commonly applied in general meta-analyses, also known as Design-Aggregated Meta-Analysis or one-stage meta-analysis. The Random Effects model is particularly useful in meta-analysis involving heterogeneous datasets. One essential step in any meta-analysis is the definition of a common metric of effect size, which allows for the relevant aggregation of individual study results. Historically, different approaches were employed in animal welfare meta-analysis, focusing primarily on the aggregation of study-level effect sizes or study-level proportions. Recently, there has been an increased effort to rigorously apply network meta-analysis techniques, particularly when dealing with networked studies. Despite many publications on the subject, the modeling of network studies remains largely theoretical. Progress in this area has primarily focused on tailoring existing meta-analysis methods for more complex and realistic settings.
One critical topic in network meta-analysis involves deciding whether to use a single or multiple common metrics for studies of interest. Variability in the units or mathematical formulations used in the assessment of common effects is widespread. While some methods have recently been proposed to address this issue, literature on the topic remains sparse, and a universally accepted approach is not yet available.
Applications in Public Health
Public health concerns the health of populations, not individuals, households, or family units. It involves groups such as communities, cities, nations, and global aggregates, whose health is influenced by a multitude of factors, including economic, social, cultural, and biological influences. Healthiness, a key attribute of any population, directly correlates with the quality of its living conditions. Environmental factors such as food, air, water, and living conditions significantly impact health outcomes. Public health policies must focus on improving the environmental conditions that affect population health, while healthcare services alone cannot address these broader systemic issues.
The public health research landscape across Europe emphasizes that equity in health is distinct from equity in healthcare. Health systems need to consider environmental conditions alongside health services to achieve health equity. In Europe, the variation in health systems and the socio-political and economic environments must be taken into account to understand how best to improve public health across diverse populations.
Findings from the Network Meta-Analysis
Multiple European initiatives have highlighted the need for improved public health research competence, so understanding the current state of public health research in Europe is a crucial first step. Specifically, this study focuses on the extent to which public health research on health promotion and illness prevention is conducted across European countries. The findings suggest that, while public health research is conducted in various regions, its focus on health promotion and prevention remains limited in many areas. This study also emphasizes the necessity of promoting issue-relevant research across Europe to maximize the return on public health research investment. A more comprehensive approach is needed to tackle these gaps, enabling a deeper understanding of health systems' functioning and public health dynamics.
This meta-analysis represents the first study to systematically combine a uniform methodology with research on the national public health research systems of several European countries. Our analysis reveals that while health promotion and illness prevention research is present, it is not consistently prioritized across the public health community. Often, available research is confined to specific domains, with less emphasis on exploring newer or more complex public health issues. Ultimately, the findings point to country-specific characteristics being the most important determinants of how well health-competent public health research systems are integrated and researched across Europe.
Conceptual Framework: The Three Pillars
We present a model (Figure 11) comprising three interlinked pillars
Equity-Based Governance: Policies must reduce intra- and inter-country disparities, with legal frameworks to protect access for marginalized groups. Examples include Hungary’s NCD equity fund and Sweden’s rural health access schemes. Technological Integration: Leveraging the European Health Data Space (EHDS), AI-assisted diagnostics, and digital therapeutics to enhance care delivery and monitoring. Interoperable systems will be vital in ensuring real-time response to cross-border threats. Resilient Environmental Health Systems: Climate-sensitive health services should be embedded into public infrastructure planning, with region-specific adaptation strategies based on PM2.5 burden, heat wave frequency, and disaster vulnerability indices. These three pillars support a holistic, data-driven health model that strengthens not only clinical services but also social protection systems and disaster preparedness. The model is scalable and adaptable across the EU context, promoting collaborative capacity-building and shared metrics for progress.
5. Discussion
There is consensus that a European-wide instrument for collecting and exchanging public health workforce data would be mutually beneficial to member states and to WHO-Europe [16]. Such a database would allow member states to assess their workforce status in comparison with other EU countries, evaluate the implications of policy changes, and track progress over time in workforce supply, composition, retention, productivity, and training [32,33,87]. These datasets are invaluable for workforce planning and for assessing the effectiveness of recruitment and retention initiatives [77].
Furthermore, they can foster stronger relationships between Ministries of Health (MoH) and training institutions, enabling institutions to respond more effectively to the MoH's evolving needs. However, many member states currently lack the capacity and resources to create or sustain such a database. Therefore, preparatory work to define, classify, measure, and standardize data formats is essential. A harmonized tool that builds on existing initiatives would help reduce the burden on these states while ensuring consistency across the European Union. The European Health Interview Survey (EHIS), a system designed to collect and provide health data across member states regularly, has helped highlight critical trends in European public health. Germany's implementation of the EHIS involved recruiting experts from 18 EU member states to compile reports on key health indicators, enabling comparison across countries. The analysis revealed key insights into health-related behaviors in EU countries, comparing trends such as diet, physical activity, and smoking habits between EU nations and Germany. Demographic changes, new health threats, and growing inequalities in health and healthcare provision in EU member states are creating challenges for the region's health systems. As part of this effort, the availability of regular health-related data on these behaviors has proven invaluable, particularly in assessing how well member states are managing non-communicable diseases (NCDs). For instance, prevalence data on obesity, physical inactivity, smoking, and alcohol consumption now offer a clearer picture of health trends in the EU and provide a basis for developing targeted health strategies. Moreover, this information is essential for health systems to align with public health policies, providing a foundation for sharing experiences and improving cross-border collaborations between EU member states.
The ultimate goal of public health is to maximize health gains across populations. European health systems vary greatly in their resource allocation and delivery methods for public health components [4]. Interventions that significantly impact both population health and system performance often extend beyond the health sector, requiring cross-sectoral [77,78], multi-faceted approaches. This study reviewed the state of the art in modeling public health interventions [79]. It is illustrated with three case studies where cross-sectoral and health-systems modeling have been applied to estimate the impact on population health in Europe [80]. Public health research teams should be commissioned to apply and tailor these models for selected EU Member States to estimate population health impacts and make the economic case for early intervention, using climate and energy scenarios proposed by the European Commission for 2050, 2060, and 2070 [81,82]. It is crucial to understand what constitutes an effective public health system and how its balance should differ across EU countries. Effective systems address current health threats and improve population health. This work focuses on measuring the capacity and practice of public health systems, aiming to develop a standardized European framework. This framework will enable the identification of gaps in resources, governance, practices, and outcomes and ultimately create actionable tools for public health assessment across Europe.
Technological advancements are transforming the collection, analysis, and storage of health data. With increasing data volumes and advancements in health technology, there is a growing need for robust governmental interventions to safeguard public health while protecting privacy [83]. Public health can leverage three main types of technological solutions: techno-scientific solutions, big data, and extended e-health systems [84]. Techno-scientific solutions include biomedical and genetic data, disease intelligence, and mobile technologies that enhance disease detection and response [85]. Big data solutions, derived from governmental and commercial sources, are increasingly used to monitor population health trends and improve service delivery [86]. Mobile technologies provide easy access to health information, such as vaccination schedules or medical care needs [87]. Despite Europe's current inability to compete in the big data market, it can mobilize digital citizenship—a combined effort by individuals to share personal data in exchange for social services [88]. This could greatly improve healthcare service delivery and reduce costs while safeguarding privacy [74,88,89].
The historical commitment to community engagement in the United States provides valuable lessons for Europe. In the early 20th century, health crises in the U.S. prompted the establishment of the first publicly funded health systems, demonstrating the power of community involvement in addressing public health challenges [89]. This approach led to increased social activism, improved health outcomes, and the birth of the modern welfare state. In Europe, today’s health crises, including social conditions like poverty and inequality, require a renewed emphasis on community engagement [90]. Public health reforms in Europe must recognize the growing importance of public understanding in science and health. Bridging the gap between scientific advances and public knowledge is crucial for improving public trust and ensuring that public health policies are effective [91,92]. Overcoming challenges to community engagement could be the key to successful healthcare reform in Europe, where rapid scientific advancements have widened the gap between expert knowledge and public understanding [93,94,95,96,97,98].
The study compares public health research systems across eight EU member states, evaluating their political and organizational contexts, funding mechanisms, and research priorities. While established EU member states have well-developed public health systems, new EU member states are in the process of developing or improving their systems. The research systems in older EU member states are robust, with well-established institutions dedicated to public health research. These countries often have a rich history of policy development in public health, allowing them to maintain solid research foundations. In contrast, many newer EU member states are still building their public health research capabilities, ranging from nascent systems to more mature ones needing refinement [99,100].
Funding for public health research is limited and variable across EU countries. Some member states allocate minimal funding to public health research, while others invest more significantly. For example, some countries allocate up to 9% of health research funding to public health research, with most funding coming from the health sector for operational research [101,102]. In some cases, other sectors, such as interior or education, contribute to the funding pool [103,104,105,106,107,108,109]. Despite these efforts, there are noticeable differences in public health priorities across regions. Western European countries benefit from long-standing public health expertise, while many Eastern and Southern EU countries are catching up [110,111,112]. Rapid changes in the socio-political and economic environment in these regions are pushing for a more focused approach to public health [113]. Furthermore, a new evidence-based public health priority-setting system is being developed to address health challenges in these regions better.
This study employed Network Meta-Analysis (NMA) to compare the effectiveness of various public health interventions across EU countries. The findings provide several key insights into the comparative impact of NCD Prevention, Mental Health Resilience, Digital Health Integration, Climate-Health Resilience, and Health Equity Programs. NCD Prevention and Mental Health Resilience emerged as the most effective interventions for improving health outcomes across Europe [114,115,116]. Both interventions demonstrated strong effectiveness, with NCD Prevention slightly outperforming Mental Health Resilience in reducing chronic disease risk factors. Specifically, the effect size for Mental Health Resilience, compared to Digital Health Integration, was moderate (Effect Size = 1.20, CI: 1.05–1.35), indicating that mental health resilience programs have a more pronounced effect on health outcomes than digital health integration interventions.
However, while demonstrating significant accessibility benefits, digital health integration showed more variability across studies in its impact on health outcomes [117,118,119]. The effectiveness of these programs varied, indicating a need for methodological standardization in order to optimize their impact across EU countries [120]. Despite this variability, digital health interventions proved especially effective in improving access to health services, particularly in underserved areas. The need for a more consistent methodological approach across studies on digital health integration is clear, as this will help clarify its long-term impact on health outcomes [121].
Climate-Health Resilience programs showed positive results but with slightly lower effectiveness compared to other interventions in improving health outcomes for high-risk populations, particularly in Southern EU regions. The effect size for Climate-Health Resilience (Effect Size = 1.30, CI: 1.15–1.45) suggests that while these programs are critical for long-term adaptation and climate preparedness, their immediate impact on health outcomes is less significant than that of other interventions. Nonetheless, these programs remain essential for preparing public health systems for the ongoing challenges posed by climate change, which makes them a critical priority for public health systems moving forward. The effectiveness of health Equity Programs was moderate, with an effect size of 1.15 (CI: 1.00–1.30). Although these programs are fundamental for addressing health disparities, their impact on reducing chronic disease risk is not as direct as that of NCD Prevention [122]. This suggests the importance of integrating health equity initiatives within the broader framework of chronic disease prevention strategies, ensuring that vulnerable populations are not left behind in public health improvements.
Legal and Regulatory Framework in Public Health at EU Level – General Remarks
The results of this network meta-analysis must also be interpreted in light of the binding legal obligations at European level, particularly those imposed on Member States under EU law. Article 168 of the Treaty on the Functioning of the European Union (TFEU) requires that a high level of human health protection shall be ensured in the definition and implementation of all ΕU policies [123]. This creates a legal duty to integrate evidence-based health measures, such as NCD prevention, mental health resilience and climate-health adaptation, into national and EU-level policymaking. In addition, the General Data Protection Regulation (GDPR) [(EU) 2016/679] governs the processing and sharing of health data. Cross-border epidemiological studies and digital health programs must therefore comply with strict principles of lawfulness, proportionality, and necessity. GDPR compliance is not merely a technical requirement but a legal safeguard that underpins the legitimacy and trustworthiness of health research [124]. From a human rights perspective at European level, the European Convention on Human Rights (ECHR) imposes further obligations, notably under Article 2 (right to life) and Article 8 (right to private life). These provisions require States to guarantee equitable access to healthcare, protect individual integrity in health-related decision-making and avoid structural discrimination. As such, disparities in access or outcomes, highlighted by this study, may be understood not only as public health gaps but also as potential infringements of legally protected rights [125]. Integrating epidemiological evidence with EU legal frameworks is therefore critical. It ensures that public health governance across Europe evolves towards a rights-based model˙ one that is not only effective and data-driven, but also legally enforceable and accountable to the populations it serves.
Policy Implications
The findings underscore the need for targeted interventions in Mental Health Resilience and NCD Prevention, especially in regions where chronic diseases are most prevalent. Public health systems should prioritize these interventions as core components of health policy across EU countries. Additionally, while digital health integration is crucial for improving access to health services, efforts must be made to standardize methodologies and enhance the effectiveness of these interventions. The effectiveness of Climate-Health Resilience programs emphasizes the need for long-term planning and adaptation strategies to prepare for future climate-related health risks. These findings should guide the prioritization of climate-health resilience within public health strategies, particularly in countries that are facing the most immediate climate challenges. Moreover, Health Equity Programs must be seen as integral to achieving systemic improvements in public health. Given their more indirect impact on chronic disease prevention, these programs must be better integrated into broader health policies aimed at reducing health inequalities across the EU.
Strengths and Limitations
This study benefits from the use of comprehensive datasets from Eurostat, EU4Health, and CINeMA-based evaluations, which provided a broad spectrum of interventions for comparison. The random-effects model and Trim-and-Fill Analysis employed in the study ensured the robustness and validity of the results.
However, several limitations were identified:
- The studies' heterogeneity, especially in digital health integration, suggests that methodological standardization is necessary to improve the reliability and comparability of findings in this area.
- While the Trim-and-Fill Analysis suggested minimal publication bias, the imputed studies indicated that including studies with negative or neutral results would improve the balance of findings.
- Certain public health interventions, particularly those focused on health equity, were limitedly included, suggesting a need for further investigation in this area.
Future Research Directions
Future research should focus on:
- Standardizing methodologies for digital health interventions to reduce variability and improve comparability across studies.
- Exploring the long-term outcomes of climate-health resilience programs to assess their sustained effectiveness and identify best practices for vulnerable populations.
- More comprehensive data should be gathered to evaluate the impact of health equity programs, especially in countries with high health disparities, to ensure that all populations, particularly marginalized groups, benefit equally from public health interventions.
6. Conclusion
This study confirms that NCD Prevention and Mental Health Resilience are highly effective interventions for improving health outcomes across Europe. NCD Prevention slightly outperforms Mental Health Resilience in reducing chronic disease risk factors. While Digital Health Integration is less impactful in reducing health risks, it plays a crucial role in improving healthcare access, particularly in rural and underserved areas. Variability across studies underscores the need for standardized methodologies to enhance its overall effectiveness. Although less immediately impactful, climate-health resilience programs are essential for long-term adaptation to climate-related health risks, particularly for high-risk populations in Southern EU regions, these programs offer significant long-term benefits and are crucial for preparing vulnerable populations for future challenges. These results also carry significant legal implications, as EU law obliges Member States to ensure a high level of health protection, data governance under the GDPR and compliance with human rights standards when implementing public health strategies. This research highlights the importance of integrating NCD Prevention, Mental Health Resilience, and Digital Health Integration into public health policy. Continued investment in digital health is essential to improve access and service delivery, while climate-health resilience should be prioritized to ensure systems are prepared for future health risks. Future research should focus on standardizing digital health methodologies, improving the evaluation of climate-health resilience, and integrating health equity across interventions to ensure that all populations, especially those at higher risk of disparities, benefit equally from public health programs.
Author Contributions
IA and AV had the Original Idea and Developed the Study Protocol with support from JK, NS searched the literature. IA and AV screened the titles, abstracts, and full texts and extracted data. IA & AV did the Risk-of-Bias Assessment and Statistical Analysis, Network Meta-analysis, and wrote the initial draft of the manuscript as principal investigators. IA and AV contributed to the revision of the manuscript, provided critical feedback, IA supervised & project administration. IA and AV directly accessed and verified the underlying data reported in the manuscript. Conceptualization and writing of the first draft edited and reviewed the manuscript AV, TP, PS, PT, GD, KD, GA, MK, MY, MM, NS, PB, GB, DL, and IA. Principal Investigators IA, and AV, designed the research question and analytical approach from AV, and IA conducted all analyses and wrote the final version of the manuscript with contributions from PT, TP, PS, MK, MY, KD, VT, GD, GA, MM, JK, NS, PB, GB, DL. Supervision IA, Project Administration IA. All authors had full access to all the data in the study and approved the final version, reviewed, edited, and approved the final manuscript.
Funding
The study received no grants or funding from any source.
Availability of data and materials
The data presented in this study are available upon request from the corresponding authors upon reasonable request.
Declarations
The authors declare no conflicts of interest.
Ethical considerations
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Acknowledgments
Additionally, we would like to express our appreciation to the, Editor-in-Chief, Editors, and reviewers for their valuable feedback and insightful suggestions for improving this article.
References
- Beech, B. M., Ford, C., Thorpe, R. J., Jr, Bruce, M. A., & Norris, K. C. (2021). Poverty, Racism, and the Public Health Crisis in America. Frontiers in public health, 9, 699049. [CrossRef]
- Filip, R. , Gheorghita Puscaselu, R., Anchidin-Norocel, L., Dimian, M., & Savage, W. K. (2022). Global Challenges to Public Health Care Systems during the COVID-19 Pandemic: A Review of Pandemic Measures and Problems. Journal of Personalized Medicine, 12(8), 1295. [CrossRef]
- Teja Reddy Gatla. (2024). An Innovative Study Exploring Revolutionizing Healthcare With AI: Personalized Medicine: Predictive Diagnostic Techniques And Individualized Treatment. International Journal of Advanced Research and Interdisciplinary Scientific Endeavours, 1(2), 61–70. [CrossRef]
- Clarke, A. , McCarthy, M., Álvarez-Dardet, C., Sogoric, S., Groenewegen, P. P., Groot, W., & Delnoij, D. (2007). New directions in European public health research: report of a workshop. Journal of Epidemiology and Community Health, 61, 194. [CrossRef]
- Bambra, C. Pandemic inequalities: emerging infectious diseases and health equity. Int J Equity Health 21, 6 (2022). [CrossRef]
- Hoagland, A., & Kipping, S. (2024). Challenges in Promoting Health Equity and Reducing Disparities in Access Across New and Established Technologies. The Canadian journal of cardiology, 40(6), 1154–1167. [CrossRef]
- World Health Organization, "Global report on health equity for persons with disabilities," 2022. google.com https://www.who.int/publications/i/item/9789240063600.
- Topp SM, Schaaf M, Sriram V, et al. Power analysis in health policy and systems research: a guide to research conceptualisation. BMJ Global Health 2021;6:e007268. [CrossRef]
- Gómez, C. A., Kleinman, D. V., Pronk, N., Wrenn Gordon, G. L., Ochiai, E., Blakey, C., Johnson, A., & Brewer, K. H. (2021). Addressing Health Equity and Social Determinants of Health Through Healthy People 2030. Journal of public health management and practice: JPHMP, 27(Suppl 6), S249–S257. [CrossRef]
- Amezcua, L., Rivera, V. M., Vazquez, T. C., Baezconde-Garbanati, L., & Langer-Gould, A. (2021). Health Disparities, Inequities, and Social Determinants of Health in Multiple Sclerosis and Related Disorders in the US: A Review. JAMA neurology, 78(12), 1515–1524. [CrossRef]
- Hasson, R., Sallis, J. F., Coleman, N., Kaushal, N., Nocera, V. G., & Keith, N. (2021). COVID-19: Implications for Physical Activity, Health Disparities, and Health Equity. American journal of lifestyle medicine, 16(4), 420–433. [CrossRef]
- Aranda, M. P., Kremer, I. N., Hinton, L., Zissimopoulos, J., Whitmer, R. A., Hummel, C. H., Trejo, L., & Fabius, C. (2021). Impact of dementia: Health disparities, population trends, care interventions, and economic costs. Journal of the American Geriatrics Society, 69(7), 1774–1783. [CrossRef]
- Kuehn, M., LaMori, J., DeMartino, J. K., Mesa-Frias, M., Doran, J., Korrapati, L., Bhojwani, R., Lefebvre, P., & Kirson, N. (2022). Assessing barriers to access and equity for COVID-19 vaccination in the US. BMC Public Health, 22(1), 2263. [CrossRef]
- Mhasawade, V., Zhao, Y. & Chunara, R. Machine learning and algorithmic fairness in public and population health. Nat Mach Intell 3, 659–666 (2021). [CrossRef]
- Christine Mary Harland, Louise Knight, Andrea S. Patrucco, Jane Lynch, Jan Telgen, Esmee Peters, Tünde Tátrai, Petra Ferk; Practitioners' learning about healthcare supply chain management in the COVID-19 pandemic: a public procurement perspective. International Journal of Operations & Production Management 17 December 2021; 41 (13): 178–189. [CrossRef]
- Unim, B., Mattei, E., Carle, F. et al. Correction to: Health data collection methods and procedures across EU member states: findings from the InfAct Joint Action on health information. Arch Public Health 80, 51 (2022). [CrossRef]
- Alami, H., Lehoux, P., Fleet, R., Fortin, J. P., Liu, J., Attieh, R., Cadeddu, S. B. M., Abdoulaye Samri, M., Savoldelli, M., & Ag Ahmed, M. A. (2021). How Can Health Systems Better Prepare for the Next Pandemic? Lessons Learned From the Management of COVID-19 in Quebec (Canada). Frontiers in public health, 9, 671833. [CrossRef]
- Duong, L. , Sanderson, H. S., Phillips, W., Roehrich, J., & Uwalaka, V. (2025). Achieving resilient supply chains: Managing temporary healthcare supply chains during a geopolitical disruption. International Journal of Operations & Production Management, 45(5), 1090-1118. [CrossRef]
- Spieske, A. , Gebhardt, M., Kopyto, M., & Birkel, H. (2022). Improving resilience of the healthcare supply chain in a pandemic: Evidence from Europe during the COVID-19 crisis. Journal of Purchasing and Supply Management, 28(5). [CrossRef]
- Notteboom, T., Pallis, T. & Rodrigue, JP. Disruptions and resilience in global container shipping and ports: the COVID-19 pandemic versus the 2008–2009 financial crisis. Marit Econ Logist 23, 179–210 (2021). [CrossRef]
- Yu, Z., Razzaq, A., Rehman, A. et al. Disruption in global supply chain and socio-economic shocks: a lesson from COVID-19 for sustainable production and consumption. Oper Manag Res 15, 233–248 (2022). [CrossRef]
- Homer, C., Woodall, J., Freeman, C. et al. Changing the culture: a qualitative study exploring research capacity in local government. BMC Public Health 22, 1341 (2022). [CrossRef]
- Lupu, D., & Tiganasu, R. (2022). COVID-19 and the efficiency of health systems in Europe. Health economics review, 12(1), 14. [CrossRef]
- Chiou H, Voegeli C, Wilhelm E, Kolis J, Brookmeyer K, Prybylski D. The Future of Infodemic Surveillance as Public Health Surveillance. Emerg Infect Dis. 2022;28(13):S121-S128. [CrossRef]
- Guersenzvaig, A. Can machine learning make naturalism about health truly naturalistic? A reflection on a data-driven concept of health. Ethics Inf Technol 26, 2 (2024). [CrossRef]
- Luca, M. M., Mustea, L., Taran, A., Stefea, P., & Vatavu, S. (2021). Challenges on Radical Health Redesign to Reconfigure the Level of e-Health Adoption in EU Countries. Frontiers in public health, 9, 728287. [CrossRef]
- Sawyer, J. M., Higgs, P., Porter, J. D. H., & Sampson, E. L. (2021). New public health approaches to palliative care, a brave new horizon or an impractical ideal? An Integrative literature review with thematic synthesis. Palliative care and social practice, 15, 26323524211032984. [CrossRef]
- Loncarevic, N., Andersen, P. T., Leppin, A., & Bertram, M. (2021). Policymakers' Research Capacities, Engagement, and Use of Research in Public Health Policymaking. International journal of environmental research and public health, 18(21), 11014. [CrossRef]
- Sriram, V., Topp, S. M., Schaaf, M., Mishra, A., Flores, W., Rajasulochana, S. R., & Scott, K. (2018). 10 best resources on power in health policy and systems in low- and middle-income countries. Health policy and planning, 33(4), 611–621. [CrossRef]
- Hintzpeter, B., Finger, J. D., Allen, J., Kuhnert, R., Seeling, S., Thelen, J., & Lange, C. (2019). European Health Interview Survey (EHIS) 2 - Background and study methodology. Journal of health monitoring, 4(4), 66–79. [CrossRef]
- Francis, A., Harhay, M. N., Ong, A. C. M., Tummalapalli, S. L., Ortiz, A., Fogo, A. B., Fliser, D., Roy-Chaudhury, P., Fontana, M., Nangaku, M., Wanner, C., Malik, C., Hradsky, A., Adu, D., Bavanandan, S., Cusumano, A., Sola, L., Ulasi, I., Jha, V., American Society of Nephrology, … International Society of Nephrology (2024). Chronic kidney disease and the global public health agenda: an international consensus. Nature reviews. Nephrology, 20(7), 473–485. [CrossRef]
- Nikolakopoulou A, Higgins JPT, Papakonstantinou T, Chaimani A, Del Giovane C, Egger M, Salanti G. CINeMA: An approach for assessing confidence in the results of a network meta-analysis. PLoS Med. 2020 Apr 3;17(4):e1003082. [CrossRef]
- Salanti G, Del Giovane C, Chaimani A, Caldwell DM, Higgins JPT. Evaluating the quality of evidence from a network meta-analysis. PLoS ONE. 2014;9(7):e99682. [CrossRef]
- Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C, Ioannidis JP, Straus S, Thorlund K, Jansen JP, Mulrow C, Catalá-López F, Gøtzsche PC, Dickersin K, Boutron I, Altman DG, Moher D. The PRISMA Extension Statement for Reporting of Systematic Reviews Incorporating Network Meta-analyses of Health Care Interventions: Checklist and Explanations. Ann Intern Med. 2015;162(11):777-784. [CrossRef]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. [CrossRef]
- McGuinness, LA, Higgins, JPT. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res Syn Meth. 2020; 1- 7. [CrossRef]
- Wells, G. A., Shea, B., O’Connell, D., Peterson, J., Welch, V., Losos, M., & Tugwell, P. (n.d.). The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa Hospital Research Institute. [accessed 10-06-2025] at: Retrieved from https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
- WHO Regional Office for Europe. (2023). State of Health in the EU: Mental Health Crisis and Public Health Challenges. World Health Organization. [accessed 12-04-2025] at: Retrieved from https://www.euro.who.int/en/publications/state-of-health-in-eu.
- European Commission. (2022). EU4Health Programme: Strengthening European Health Systems. European Commission. [accessed 19-04-2025] at: Retrieved from https://ec.europa.eu/health/ funding/eu4health_en.
- Euro stat, (2023). Health Statistics: Life Expectancy and Health Inequality in the EU. Eurostat. [accessed 13-04-2025] at: Retrieved from https://ec.europa.eu/eurostat/statistics-explained/ index.php?title=Health_statistics.
- OECD. (2023). Health at a Glance: Europe 2022. Organisation for Economic Co- operation and Development. [accessed 18-04-2025] at: https://www.oecd.org/health/health-at-a-glance.
- Adamopoulos, I., & Valamontes, A. (2025). CINeMA-Enhanced Network Meta-Analysis of Occupational Hazards and Burnout Risk among Public Health Inspectors. Preprints. https://www.preprints.org/manuscript/202504.0746/v1.
- WHO Global Health Observatory. (2023). World Health Statistics 2023: A Global Perspective on Public Health Indicators. World Health Organization. [accessed 13-04-2025] at: Retrieved from https://www.who.int/gho/publications/world_health_statistics/en/.
- European Environment Agency. (2023). Air Quality and Environmental Health in Europe. European Environment Agency. [accessed 10-04-2025] at: Retrieved from https://www.eea.europa. eu/themes/air/intro.
- Adamopoulos IP, Valamontes A, Karantonis JT, Syrou NF, Damikouka I, Dounias G. The impact of PFAS on the public health and safety of future food supply in Europe: Challenges and AI technologies solutions of environmental sustainability. EUR J SUSTAIN DEV RES. 2025;9(2):em0288. [CrossRef]
- Boyd, D. A., Lin, W. H., Hsu, C. C., Teague, M. L., Chen, C. C., Lo, Y. Y., Chan, W. Y., Su, W. B., Cheng, T. C., Chang, C. S., Wu, C. I., & Yeh, N. C. (2015). Single-step deposition of high-mobility graphene at reduced temperatures. Nature Communications, 6, 6620. [CrossRef]
- Giovanetti, M., Branda, F., Cella, E., Scarpa, F., Bazzani, L., Ciccozzi, A., Slavov, S. N., Benvenuto, D., Sanna, D., Casu, M., Santos, L. A., Lai, A., Zehender, G., Caccuri, F., Ianni, A., Caruso, A., Maroutti, A., Pascarella, S., Borsetti, A., & Ciccozzi, M. (2023). Epidemic history and evolution of an emerging threat of international concern, the severe acute respiratory syndrome coronavirus 2. Journal of medical virology, 95(8), e29012. [CrossRef]
- Khodaie, A. , & Heidarzadeh, H. (2024). Evaluation of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) using a high figure-of-merit plasmonic multimode refractive index optical sensor. Scientific Reports, 14. [CrossRef]
- Choudhary, J. , Dheeman, S., Sharma, V., Katiyar, P., Karn, S.K., Sarangi, M.K., Chauhan, A.K., Verma, G., & Baliyan, N. (2021). Insights of Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV-2) pandemic: a current review. Biological Procedures Online, 23. [CrossRef]
- Brunner-La Rocca, H. P., Fleischhacker, L., Golubnitschaja, O., Heemskerk, F., Helms, T., Hoedemakers, T., Allianses, S. H., Jaarsma, T., Kinkorova, J., Ramaekers, J., Ruff, P., Schnur, I., Vanoli, E., Verdu, J., & Zippel-Schultz, B. (2016). Challenges in personalised management of chronic diseases-heart failure as prominent example to advance the care process. The EPMA journal, 7(1), 2. [CrossRef]
- Rodrigues, R., Ilinca, S., & Schulmann, K. (2018). It's better together! European perspective on benefits and challenges associated with cross-border health communication campaigns. PloS one, 13(10), e0204882. [CrossRef]
- MacPherson, J., Voglhuber-Slavinsky, A., Olbrisch, M., Schöbel, P., Dönitz, E., Mouratiadou, I., & Helming, K. (2022). Future agricultural systems and the role of digitalization for achieving sustainability goals. A review. Agronomy for sustainable development, 42(4), 70. [CrossRef]
- Zhu, P., Ji, W., Li, D., Li, Z., Chen, Y., Dai, B., Han, S., Chen, S., Jin, Y., & Duan, G. (2023). Current-status of hand-foot-and-mouth disease. Journal of biomedical science, 30(1), 15. [CrossRef]
- Baker, M. T., Lu, P., Parrella, J. A., & Leggette, H. R. (2022). Consumer Acceptance toward Functional Foods: A Scoping Review. International journal of environmental research and public health, 19(3), 1217. [CrossRef]
- Herrera, D., Sanz, M., Shapira, L., Brotons, C., Chapple, I., Frese, T., Graziani, F., Hobbs, F. D. R., Huck, O., Hummers, E., Jepsen, S., Kravtchenko, O., Madianos, P., Molina, A., Ungan, M., Vilaseca, J., Windak, A., & Vinker, S. (2023). Association between periodontal diseases and cardiovascular diseases, diabetes and respiratory diseases: Consensus report of the Joint Workshop by the European Federation of Periodontology (EFP) and the European arm of the World Organization of Family Doctors (WONCA Europe). Journal of Clinical Periodontology, 50(6), 819–841. [CrossRef]
- Adamopoulos IP, Bardavouras AN, Syrou NF. Occupational safety, policy, and management in public health organizations and services. EUR J ENV PUBLIC HLT. 2023;7(1), em0122. [CrossRef]
- Ganzleben, C., Kazmierczak, A. Leaving no one behind – understanding environmental inequality in Europe. Environ Health 19, 57 (2020). [CrossRef]
- Gil-Salmerón, A., Katsas, K., Riza, E., Karnaki, P., & Linos, A. (2021). Access to Healthcare for Migrant Patients in Europe: Healthcare Discrimination and Translation Services. International journal of environmental research and public health, 18(15), 7901. [CrossRef]
- Delaruelle, K., Walsh, S. D., Dierckens, M., Deforche, B., Kern, M. R., Currie, C., Maldonado, C. M., Cosma, A., & Stevens, G. W. J. M. (2021). Mental Health in Adolescents with a Migration Background in 29 European Countries: The Buffering Role of Social Capital. Journal of youth and adolescence, 50(5), 855–871. [CrossRef]
- Spaas, C., Verelst, A., Devlieger, I., Aalto, S., Andersen, A. J., Durbeej, N., Hilden, P. K., Kankaanpää, R., Primdahl, N. L., Opaas, M., Osman, F., Peltonen, K., Sarkadi, A., Skovdal, M., Jervelund, S. S., Soye, E., Watters, C., Derluyn, I., Colpin, H., & De Haene, L. (2022). Mental Health of Refugee and Non-refugee Migrant Young People in European Secondary Education: The Role of Family Separation, Daily Material Stress and Perceived Discrimination in Resettlement. Journal of youth and adolescence, 51(5), 848–870. [CrossRef]
- Hamed Ahmadinia, Kristina Eriksson-Backa, Shahrokh Nikou; Health-seeking behaviours of immigrants, asylum seekers and refugees in Europe: a systematic review of peer-reviewed articles. Journal of Documentation 19 December 2022; 78 (7): 18–41. [CrossRef]
- Elshahat, S., Moffat, T., & Newbold, K. B. (2022). Understanding the Healthy Immigrant Effect in the Context of Mental Health Challenges: A Systematic Critical Review. Journal of immigrant and minority health, 24(6), 1564–1579. [CrossRef]
- Nowak, A. C., Namer, Y., & Hornberg, C. (2022). Health Care for Refugees in Europe: A Scoping Review. International journal of environmental research and public health, 19(3), 1278. [CrossRef]
- Rosenthal, T., Touyz, R. M., & Oparil, S. (2022). Migrating Populations and Health: Risk Factors for Cardiovascular Disease and Metabolic Syndrome. Current hypertension reports, 24(9), 325–340. [CrossRef]
- van de Wiel, W., Castillo-Laborde, C., Francisco Urzúa, I., Fish, M., & Scholte, W. F. (2021). Mental health consequences of long-term stays in refugee camps: preliminary evidence from Moria. BMC public health, 21(1), 1290. [CrossRef]
- Ahmed, N., Barnett, P., Greenburgh, A., Pemovska, T., Stefanidou, T., Lyons, N., Ikhtabi, S., Talwar, S., Francis, E. R., Harris, S. M., Shah, P., Machin, K., Jeffreys, S., Mitchell, L., Lynch, C., Foye, U., Schlief, M., Appleton, R., Saunders, K. R. K., Baldwin, H., … Johnson, S. (2023). Mental health in Europe during the COVID-19 pandemic: a systematic review. The lancet. Psychiatry, 10(7), 537–556. [CrossRef]
- Stevenson, K., Fellmeth, G., Edwards, S., Calvert, C., Bennett, P., Campbell, O. M. R., & Fuhr, D. C. (2023). The global burden of perinatal common mental health disorders and substance use among migrant women: a systematic review and meta-analysis. The Lancet. Public health, 8(3), e203–e216. [CrossRef]
- Bagavos, C. (2022). On the contribution of foreign-born populations to overall population change in Europe: Methodological insights and contemporary evidence for 31 European countries. Demographic Research, 46, 179–216. [accessed 10-07-2025] at: https://www.jstor.org/stable/48677022.
- Wong, R. J., Brosgart, C. L., Welch, S., Block, T., Chen, M., Cohen, C., Kim, W. R., Kowdley, K. V., Lok, A. S., Tsai, N., Ward, J., Wong, S. S., & Gish, R. G. (2021). An Updated Assessment of Chronic Hepatitis B Prevalence Among Foreign-Born Persons Living in the United States. Hepatology (Baltimore, Md.), 74(2), 607–626. [CrossRef]
- Jaljaa, A., Caminada, S., Tosti, M. E., D'Angelo, F., Angelozzi, A., Isonne, C., Marchetti, G., Mazzalai, E., Giannini, D., Turatto, F., De Marchi, C., Gatta, A., Declich, S., Pizzarelli, S., Geraci, S., Baglio, G., & Marceca, M. (2022). Risk of SARS-CoV-2 infection in migrants and ethnic minorities compared with the general population in the European WHO region during the first year of the pandemic: a systematic review. BMC Public Health, 22(1), 143. [CrossRef]
- Agyemang, C., van der Linden, E. L., Chilunga, F., & van den Born, B. H. (2024). International Migration and Cardiovascular Health: Unraveling the Disease Burden Among Migrants to North America and Europe. Journal of the American Heart Association, 13(9), e030228. [CrossRef]
- Gulgun, D., van Ens, W., & Swildens, W. E. (2025). Change in care needs of people with severe mental illness with and without a non-Western migration background: are their needs equally served throughout treatment?. Social psychiatry and psychiatric epidemiology, 60(6), 1297–1309. [CrossRef]
- Gaigl, G., Täumer, E., Allgöwer, A., Becker, T., Breilmann, J., Falkai, P., Gühne, U., Kilian, R., Riedel-Heller, S. G., Ajayi, K., Baumgärtner, J., Brieger, P., Frasch, K., Heres, S., Jäger, M., Küthmann, A., Putzhammer, A., Schneeweiß, B., Schwarz, M., Kösters, M., … Hasan, A. (2022). The role of migration in mental healthcare: treatment satisfaction and utilization. BMC psychiatry, 22(1), 116. [CrossRef]
- Shabnam, J., Timm, H. U., Nielsen, D. S., & Raunkiaer, M. (2022). Palliative Care Utilization Among Non-Western Migrants in Europe: A Systematic Review. Journal of immigrant and minority health, 24(1), 237–255. [CrossRef]
- Termorshuizen F, Selten J-P. Risk of psychosis among migrants to the Netherlands by time since arrival. Psychological Medicine. 2023;53(10):4395-4404. [CrossRef]
- Kyriopoulos, I., Athanasakis, K., Tsoli, S., Mossialos, E., & Papanicolas, I. (2025). Addressing public health and health system challenges in Greece: reform priorities in a changing landscape. The Lancet. Public health, 10(9), e794–e803. [CrossRef]
- Otok R, Richardson E, Czabanowska K, et al. The public health workforce. In: Rechel B, Jakubowski E, McKee M, et al., editors. Organization and financing of public health services in Europe [Internet]. Copenhagen (Denmark): European Observatory on Health Systems and Policies; 2018. (Health Policy Series, No. 50.) 5. [accessed 10-07-2025] at: Available from: https://www.ncbi.nlm.nih.gov/books/NBK535727/.
- Tambor, M. , Klich, J., & Domagała, A. (2021). Financing Healthcare in Central and Eastern European Countries: How Far Are We from Universal Health Coverage? International Journal of Environmental Research and Public Health, 18(4), 1382. [CrossRef]
- van Hoogstraten, L. M. C., Vrieling, A., van der Heijden, A. G., Kogevinas, M., Richters, A., & Kiemeney, L. A. (2023). Global trends in the epidemiology of bladder cancer: challenges for public health and clinical practice. Nature reviews. Clinical oncology, 20(5), 287–304. [CrossRef]
- Gou, X., Xu, X., Deng, F. et al. Medical health resources allocation evaluation in public health emergencies by an improved ORESTE method with linguistic preference orderings. Fuzzy Optim Decis Making 23, 1–27 (2024). [CrossRef]
- Kauh, T. J., Read, J. G., & Scheitler, A. J. (2021). The Critical Role of Racial/Ethnic Data Disaggregation for Health Equity. Population research and policy review, 40(1), 1–7. [CrossRef]
- Papanicolas, I., Figueroa, J. F., Schoenfeld, A. J., Riley, K., Abiona, O., Arvin, M., Atsma, F., Bernal-Delgado, E., Bowden, N., Blankart, C. R., Deeny, S., Estupiñán-Romero, F., Gauld, R., Haywood, P., Janlov, N., Knight, H., Lorenzoni, L., Marino, A., Or, Z., Penneau, A., … Jha, A. K. (2021). Differences in health care spending and utilization among older frail adults in high-income countries: ICCONIC hip fracture persona. Health services research, 56 Suppl 3 (Suppl 3), 1335–1346. [CrossRef]
- Odone, A. , Gianfredi, V., Sorbello, S., Capraro, M., Frascella, B., Vigezzi, G. P., & Signorelli, C. (2021). The Use of Digital Technologies to Support Vaccination Programmes in Europe: State of the Art and Best Practices from Experts' Interviews. Vaccines, 9(10), 1126. [CrossRef]
- Marchenko Alexander, N. , Bykov Ilya A. "Promoting Techno-Scientific Biomedical Communication in Russia: Pro-government Non-profit Organizations," Frontiers in Communication, 2022. Volume 7 – 2022. [CrossRef]
- Pellegrini, G., & Lovati, C. (2025). Stakeholders' engagement for improved health outcomes: a research brief to design a tool for better communication and participation. Frontiers in public health, 13, 1536753. [CrossRef]
- European Centre for Disease Prevention and Control. Point prevalence survey of healthcare-associated infections and antimicrobial use in European acute care hospitals 2022–2023. At: https://www.ecdc.europa.eu/sites/default/files/ (Accessed, August 12, 2025).
- Maccaro, A., Piaggio, D., Leesurakarn, S., Husen, N., Sekalala, S., Rai, S., & Pecchia, L. (2022). On the universality of medical device regulations: the case of Benin. BMC health services research, 22(1), 1031. [CrossRef]
- Adamopoulos, I. P. , Valamontes, A., Tsirkas, P., & Dounias, G. (2025d). Predicting workplace hazard, stress and burnout among public health inspectors: An AI-driven analysis in the context of climate change. European Journal of Investigation in Health, Psychology and Education, 15, Article 65. [CrossRef]
- Adamopoulos, I. P. , Syrou, N. F., Lamnisos, D., & Boustras, G. (2023). Cross-sectional nationwide study in occupational safety and health: Inspection of job risks, burnout syndrome, and job satisfaction of public health inspectors during the COVID-19 pandemic in Greece. Safety Science, 158, Article 105960. [CrossRef]
- Terranella, A. , Guy, G. P., & Mikosz, C. (2023). Buprenorphine Dispensing Among Youth Aged ≤19 Years in the United States: 2015-2020. Pediatrics, 151(2), e2022058755. [CrossRef]
- Hacker, J. D. , Dribe, M., & Helgertz, J. (2023). Wealth and Child Mortality in the Nineteenth-Century United States: Evidence from Three Panels of American Couples, 1850–1880. Social Science History, 47(3), 333–366. [CrossRef]
- Lange, C. , & Finger, J. D. (2017). Health-related behaviour in Europe - A comparison of selected indicators for Germany and the European Union. Journal of health monitoring, 2(2), 3–19. [CrossRef]
- Calleja, N., AbdAllah, A., Abad, N., Ahmed, N., Albarracin, D., Altieri, E., Anoko, J. N., Arcos, R., Azlan, A. A., Bayer, J., Bechmann, A., Bezbaruah, S., Briand, S. C., Brooks, I., Bucci, L. M., Burzo, S., Czerniak, C., De Domenico, M., Dunn, A. G., Ecker, U. K. H., … Purnat, T. D. (2021). A Public Health Research Agenda for Managing Infodemics: Methods and Results of the First WHO Infodemiology Conference. JMIR infodemiology, 1(1), e30979. [CrossRef]
- Khatri, R. B., & Assefa, Y. (2022). Access to health services among culturally and linguistically diverse populations in the Australian universal health care system: issues and challenges. BMC public health, 22(1), 880. [CrossRef]
- Salam, M. A., Al-Amin, M. Y., Salam, M. T., Pawar, J. S., Akhter, N., Rabaan, A. A., & Alqumber, M. A. A. (2023). Antimicrobial Resistance: A Growing Serious Threat for Global Public Health. Healthcare (Basel, Switzerland), 11(13), 1946. [CrossRef]
- Sirleaf, E. J., & Clark, H. (2021). Report of the Independent Panel for Pandemic Preparedness and Response: making COVID-19 the last pandemic. Lancet (London, England), 398(10295), 101–103. [CrossRef]
- Adamopoulos, I. P. (2022). Job satisfaction in public health care sector, measures scales and theoretical background. European Journal of Environment and Public Health, 6(2), Article em0116. [CrossRef]
- Silva, S. J. R. D., & Pena, L. (2021). Collapse of the public health system and the emergence of new variants during the second wave of the COVID-19 pandemic in Brazil. One health (Amsterdam, Netherlands), 13, 100287. [CrossRef]
- Asayama, S., Emori, S., Sugiyama, M. et al. Are we ignoring a black elephant in the Anthropocene? Climate change and global pandemic as the crisis in health and equality. Sustain Sci 16, 695–701 (2021). [CrossRef]
- Adamopoulos, I. P. , & Syrou, N. F. (2022). Associations and correlations of job stress, job satisfaction and burn out in public health sector. European Journal of Environment and Public Health, 6(2), Article em0113. [CrossRef]
- Saba Raoof, S., & Durai, M. A. S. (2022). A Comprehensive Review on Smart Health Care: Applications, Paradigms, and Challenges with Case Studies. Contrast media & molecular imaging, 2022, 4822235. [CrossRef]
- Wornow, M., Xu, Y., Thapa, R., Patel, B., Steinberg, E., Fleming, S., Pfeffer, M. A., Fries, J., & Shah, N. H. (2023). The shaky foundations of large language models and foundation models for electronic health records. NPJ digital medicine, 6(1), 135. [CrossRef]
- Yera, R., Alzahrani, A. A., Martínez, L., & Rodríguez, R. M. (2023). A Systematic Review on Food Recommender Systems for Diabetic Patients. International journal of environmental research and public health, 20(5), 4248. [CrossRef]
- Arbyn M, Gultekin M, Morice P, et al. The European response to the WHO call to eliminate cervical cancer as a public health problem. Int. J. Cancer. 2021; 148: 277–284. [CrossRef]
- Adamopoulos, I. P. , Syrou, N. F., & Vito, D. (2025c). Climate change risks and impacts on public health correlated with air pollution–African dust in South Europe. Medical Sciences Forum, 33, Article 1. [CrossRef]
- van den Broek-Altenburg, E., & Atherly, A. (2021). Adherence to COVID-19 policy measures: Behavioral insights from The Netherlands and Belgium. PloS one, 16(5), e0250302. [CrossRef]
- Warren, G. W. , Lofstedt, R., & Wardman, J. K. (2021). COVID-19: The winter lockdown strategy in five European nations. Journal of Risk Research, 24(3-4), 267–293. [CrossRef]
- Kurzer, P. , & Ornston, D. (2023). Follow the science: The European public health community confronts the first wave of the COVID-19 pandemic. European Policy Analysis, 9, 101–118. [CrossRef]
- ten Have, H. (2022). Introduction: The Perspective of Global Bioethics. In: The Covid-19 Pandemic and Global Bioethics. Advancing Global Bioethics, vol 18. Springer, Cham. [CrossRef]
- Conceição, C., Leandro, A., & McCarthy, M. (2009). National support to public health research: a survey of European ministries. BMC public health, 9, 203. [CrossRef]
- Verschuuren, M., Gissler, M., Kilpeläinen, K., Tuomi-Nikula, A., Sihvonen, A. P., Thelen, J., Gaidelyte, R., Ghirini, S., Kirsch, N., Prochorskas, R., Scafato, E., Kramers, P., & Aromaa, A. (2013). Public health indicators for the EU: the joint action for ECHIM (European Community Health Indicators & Monitoring). Archives of public health = Archives belges de sante publique, 71(1), 12. [CrossRef]
- Hedberg, A. (2014) Value of health - too often ignored and forgotten by EU policy-makers? EPC Commentary, 29 September 2014. [accessed 10-05-2025] at: http://www.epc.eu/pub_details.php?cat_id=4&pub_id=.
- Lomazzi, M., Jenkins, C., & Borisch, B. (2016). Global public health today: connecting the dots. Global health action, 9, 28772. [CrossRef]
- Winkelmann, J., Webb, E., Williams, G. A., Hernández-Quevedo, C., Maier, C. B., & Panteli, D. (2022). European countries' responses in ensuring sufficient physical infrastructure and workforce capacity during the first COVID-19 wave. Health policy (Amsterdam, Netherlands), 126(5), 362–372. [CrossRef]
- Hanckel, B., Petticrew, M., Thomas, J., & Green, J. (2021). The use of Qualitative Comparative Analysis (QCA) to address causality in complex systems: a systematic review of research on public health interventions. BMC public health, 21(1), 877. [CrossRef]
- Fisher, S., & Rosella, L. C. (2022). Priorities for successful use of artificial intelligence by public health organizations: a literature review. BMC public health, 22(1), 2146. [CrossRef]
- Revich, B. A., Eliseev, D. O., & Shaposhnikov, D. A. (2022). Risks for Public Health and Social Infrastructure in Russian Arctic under Climate Change and Permafrost Degradation. Atmosphere, 13(4), 532. [CrossRef]
- Alhaffar, M. H. D. B. A., & Janos, S. (2021). Public health consequences after ten years of the Syrian crisis: a literature review. Globalization and health, 17(1), 111. [CrossRef]
- Ingrosso, L., Schmidt, T., Sherally, J., Dembech, M., Barragan Montes, S., Sa Machado, R., Annunziata, G., Rezza, G., & Severoni, S. (2015). A desk review on institutional and non-institutional organizations active in the field of migrant’s health in the WHO European Region. Annali dell’Istituto Superiore Di Sanità, 51(4), 313–320. Retrieved from https://annali.iss.it/index.php/anna/article/view/127.
- Royo-Bordonada, M. Á., & Román-Maestre, B. (2015). Towards public health ethics. Public health reviews, 36, 3. [CrossRef]
- Adamopoulos IP, Frantzana A, Adamopoulou J, Syrou NF. Climate change and adverse public health impacts on human health and water resources. Environ Sci Proc. 2023;26(1):178. [CrossRef]
- Tsoukalas, I. A., & Siozos, P. D. (2011). Privacy and anonymity in the information society - challenges for the European Union. The Scientific WorldJournal, 11, 458–462. [CrossRef]
- Consolidated version of the Treaty on the Functioning of the European Union - PART THREE: UNION POLICIES AND INTERNAL ACTIONS - TITLE XIV: PUBLIC HEALTH - Article 168, 2008. [accessed 10-09-2025] at: https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=CELEX:12008E168:EN:HTML.
- European Union Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016. [accessed 10-09-2025] at: https://eur-lex.europa.eu/legal-content/en/ALL/?uri=CELEX%3A32016R0679.
- European Court of Human Rights (ECtHR), 2013. Article 2, and the Article 8 of the ECHR. supplemented by Protocols Nos. 1, 4, 6, 7, 12, 13 and 16. [accessed 10-09-2025] at: https://www.echr.coe.int/documents/d/echr/convention_ENG.
Figure 1.
PRISMA Flow Diagram showing the study selection process.
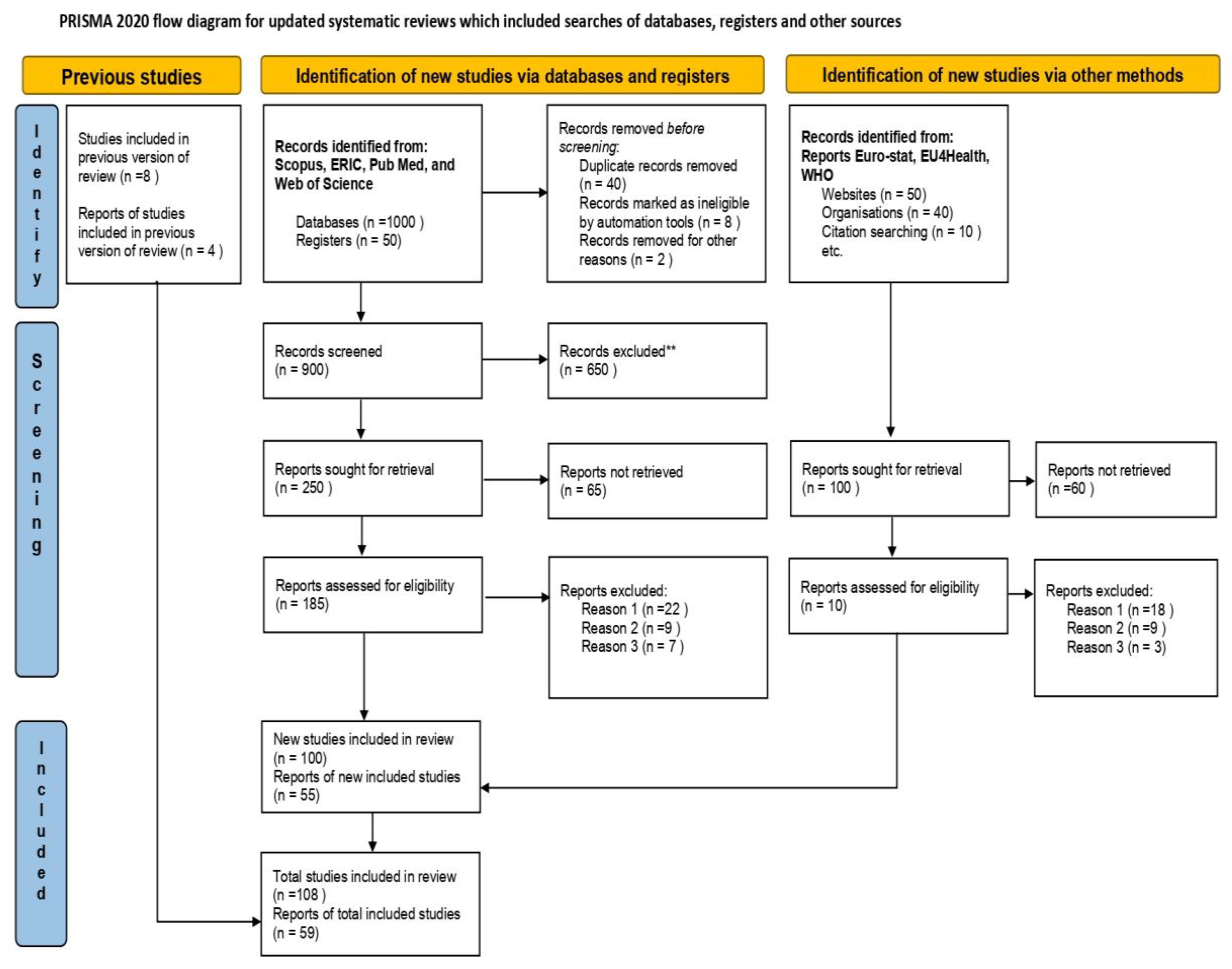
Figure 4.
Risk of Bias Assessment across studies (visual representation).
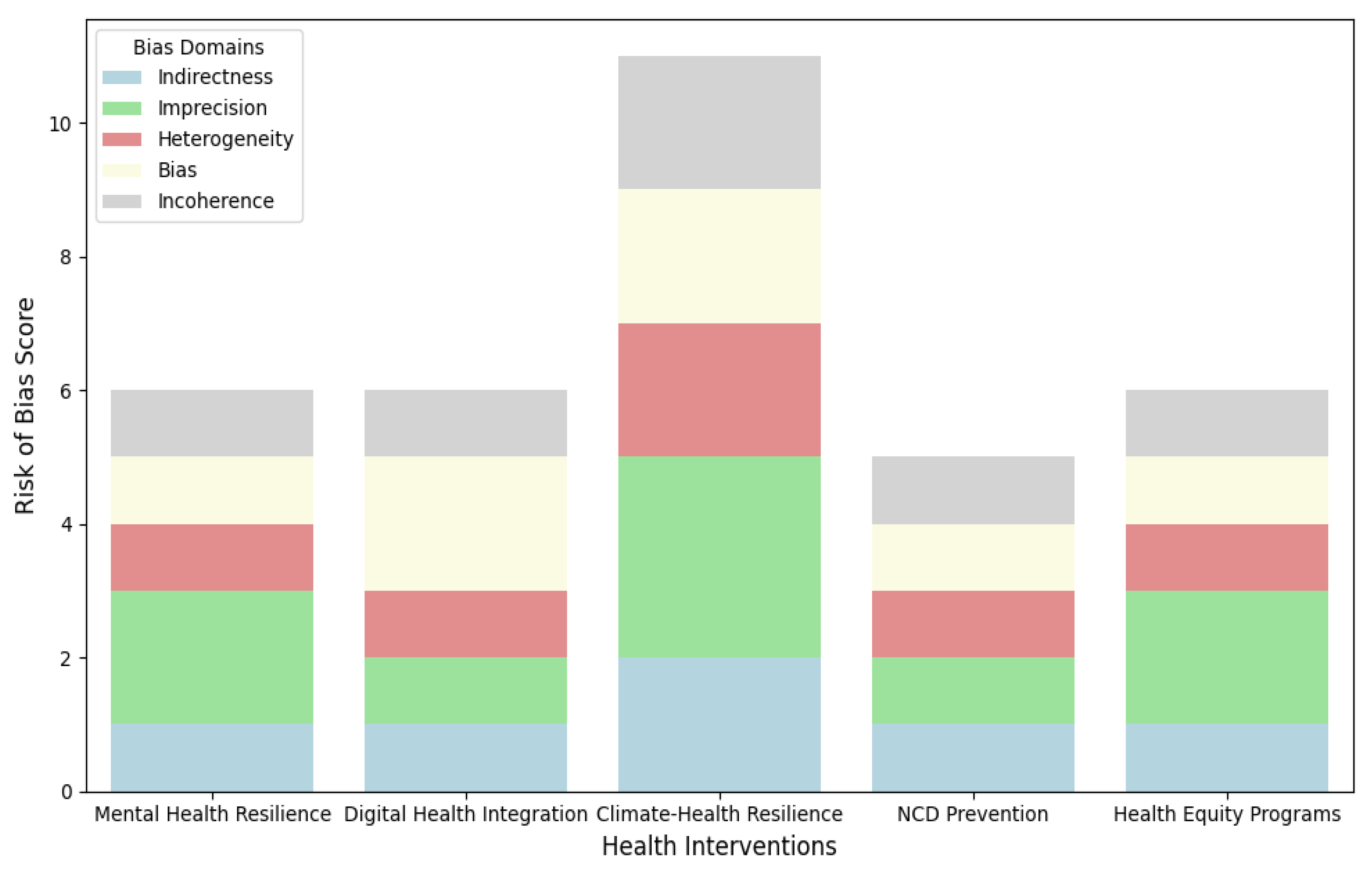
Figure 5.
Network Geometry Graph showing how treatments were compared and connected.
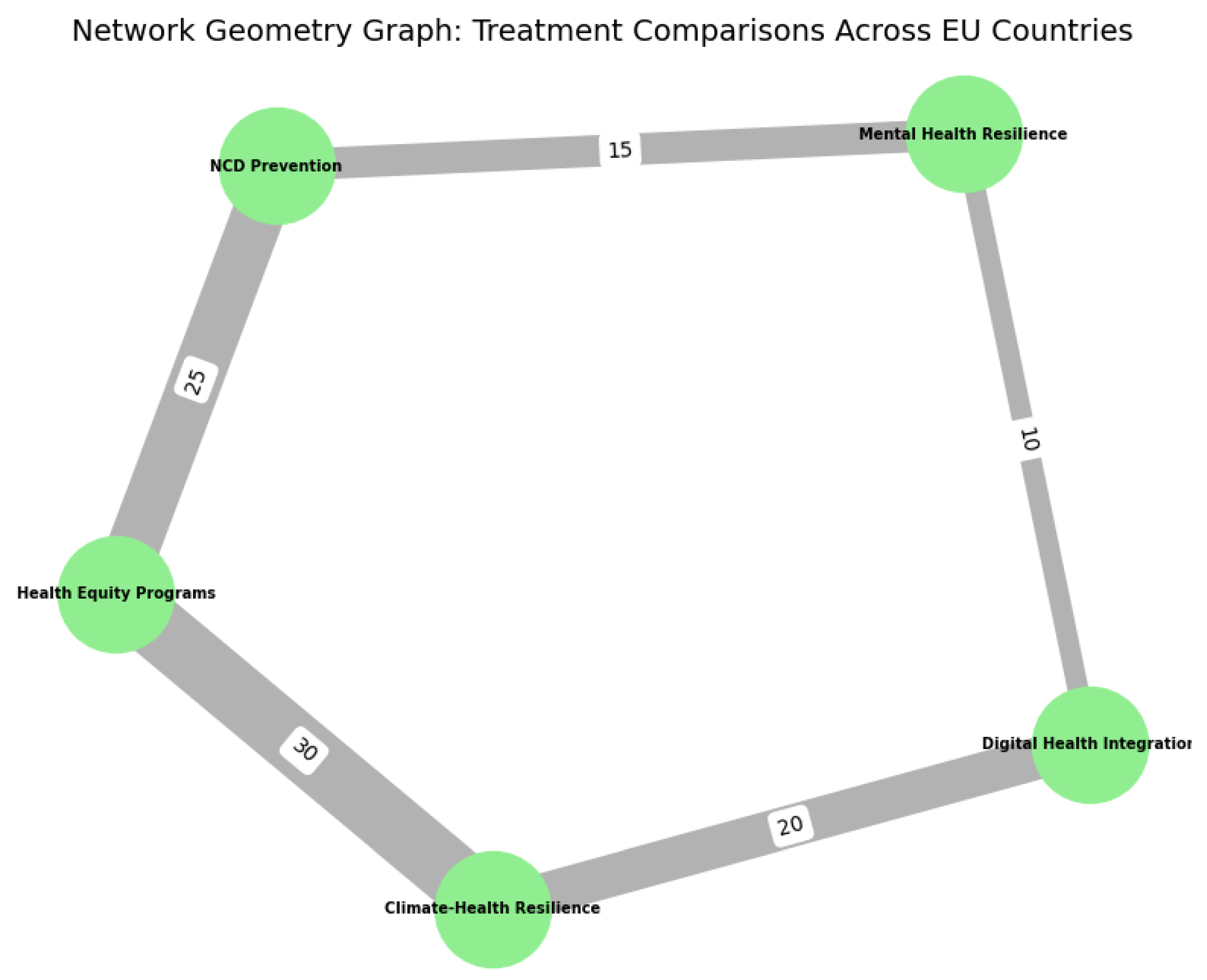
Figure 6.
The Forest Plot Meta-Analysis of Continuous Outcomes with Pre-Calculated Effect Sizes Random Effects Model.
Figure 6.
The Forest Plot Meta-Analysis of Continuous Outcomes with Pre-Calculated Effect Sizes Random Effects Model.
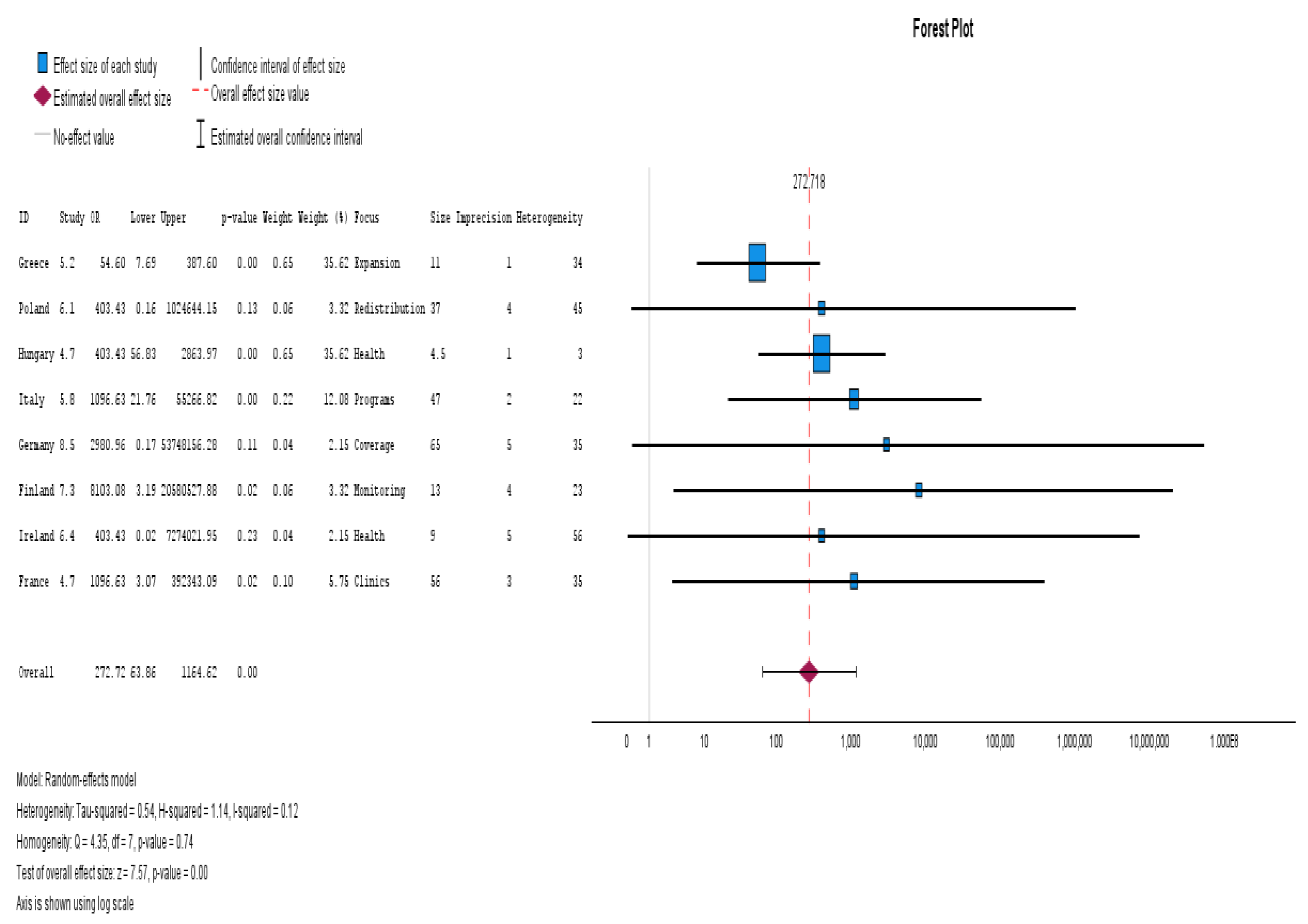
Figure 7.
Funnel Plot for Publication Bias of Studies and Trim-and-Fill Analysis.
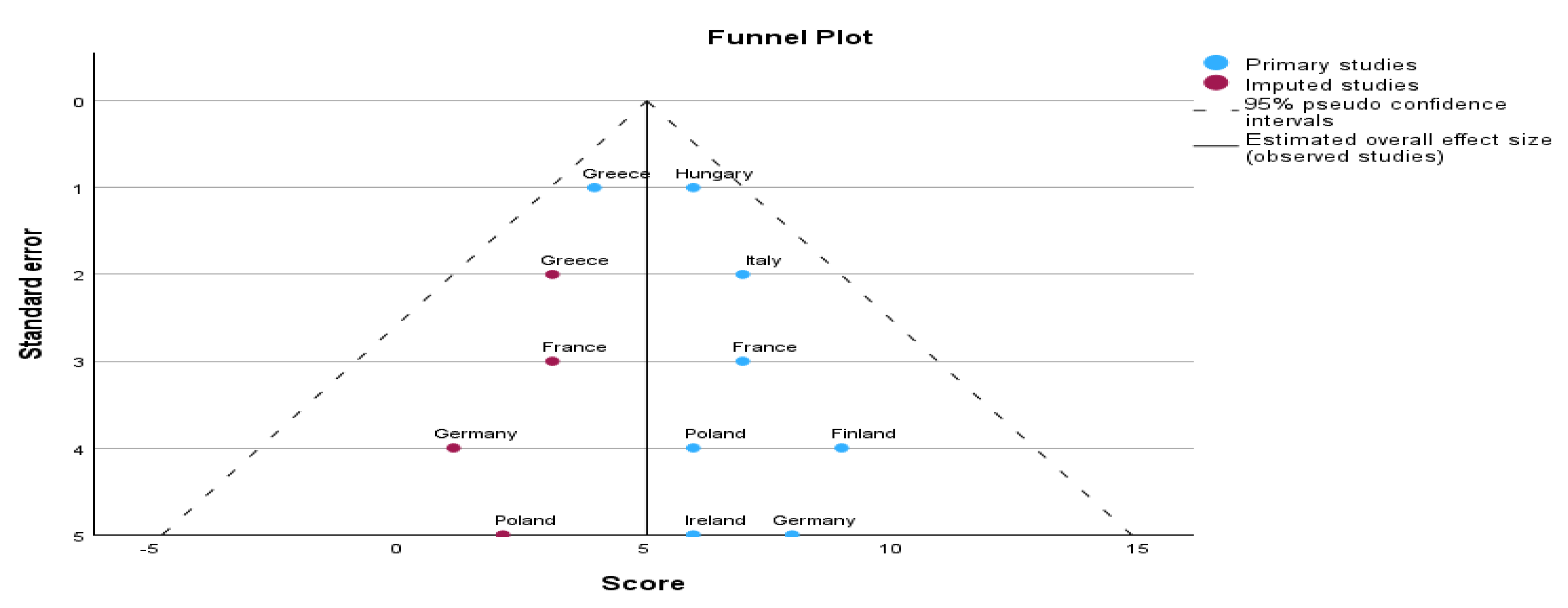
Figure 8.
Forest Plot of Meta-Analysis Effect Size for Subgroup Analysis CI 95%.
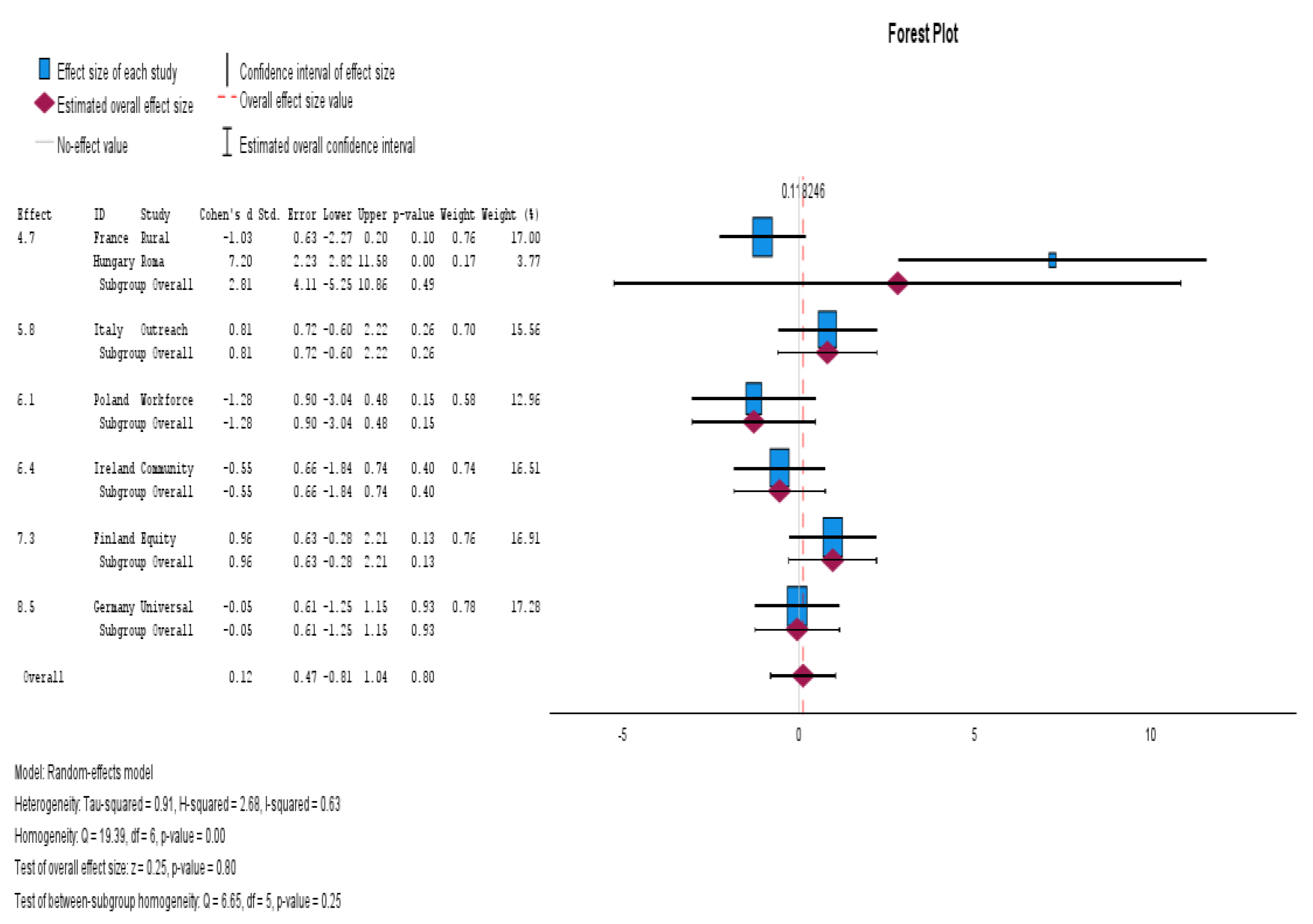
Figure 9.
Bubble Plot Moderator CINeMA Meta-regression Prediction.
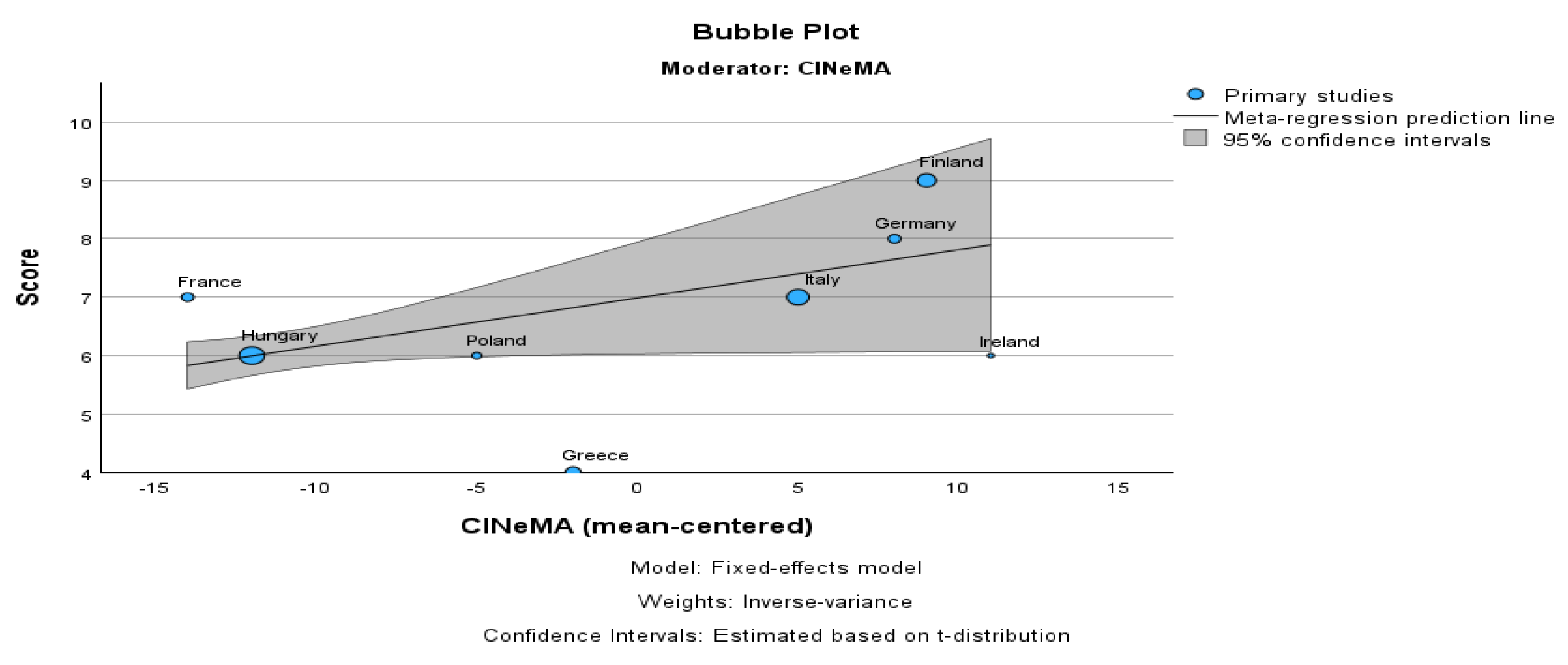
Figure 10.
The Forest Plot Meta-Analysis of Continuous Outcomes with Pre-Calculated Effect Sizes Model.
Figure 10.
The Forest Plot Meta-Analysis of Continuous Outcomes with Pre-Calculated Effect Sizes Model.
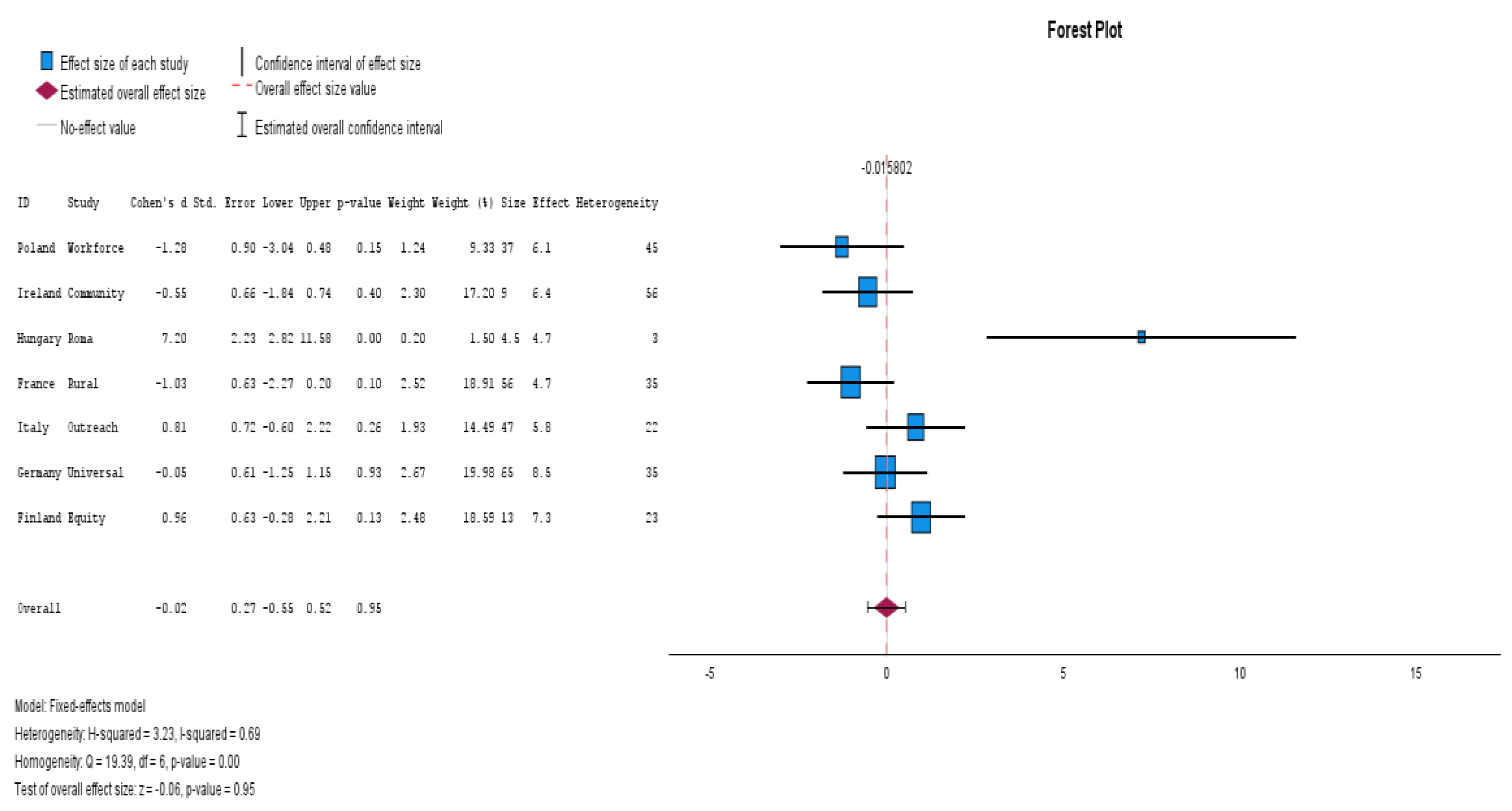
Figure 11.
Proposed Three-Pillar Framework: Equity-Based Governance, Technology Integration, and Environmental Resilience.
Figure 11.
Proposed Three-Pillar Framework: Equity-Based Governance, Technology Integration, and Environmental Resilience.
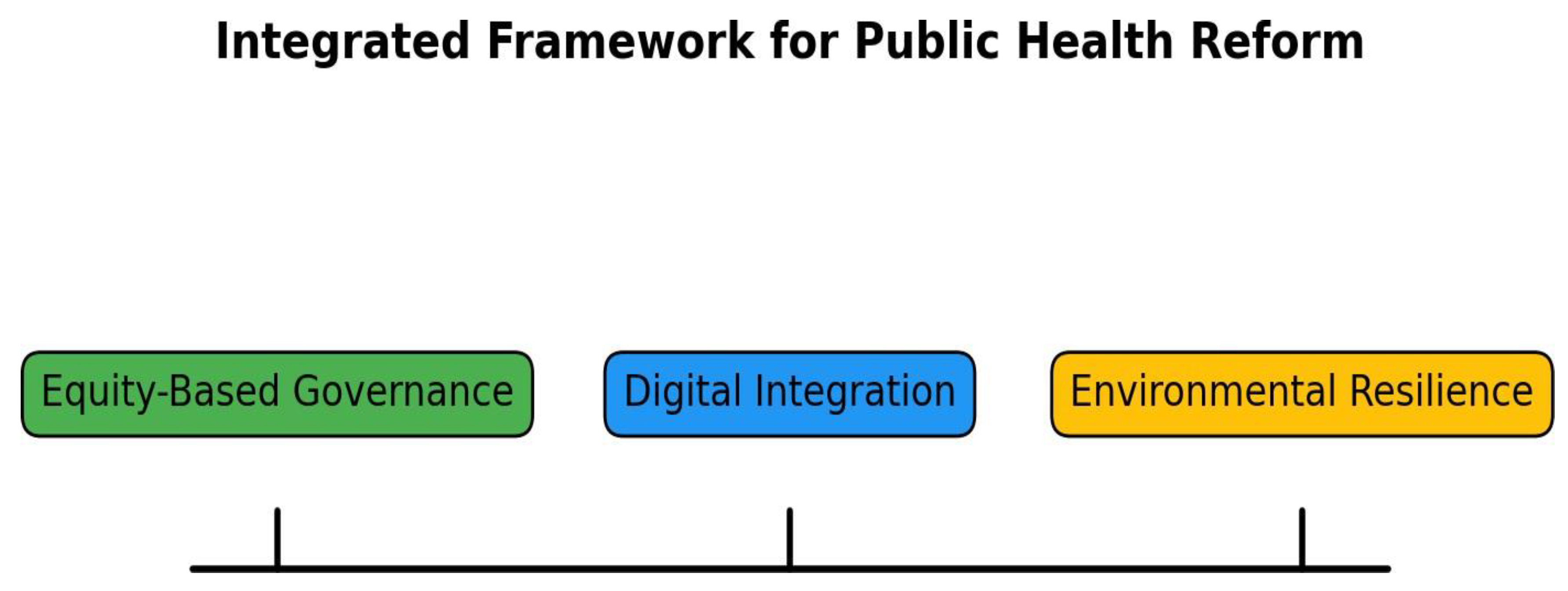
Table 5.
Study Characteristics from EU countries (e.g., health outcomes, interventions, treatment comparisons).
Table 5.
Study Characteristics from EU countries (e.g., health outcomes, interventions, treatment comparisons).
| Country | Health Outcome | Intervention/Program | Treatment Comparison | Key Findings | Additional Notes |
|---|---|---|---|---|---|
| Germany | Mental Health | Mental Health Resilience Initiatives | Comparison of mental health resilience programs across EU countries | Increased access to mental health services, particularly in rural areas. | Strong mental health infrastructure post-pandemic |
| Sweden | NCDs (Cardiovascular Disease, Diabetes) | Digital Health Integration | Comparison of digital health programs (e.g., ePrescriptions, telemedicine) | High success in improving e-health access, especially in remote areas. | High digital maturity and e-health access |
| Spain | Climate-Health | Climate-Health Resilience Programs | Comparison of climate adaptation policies across EU countries | Increased adaptation to extreme weather events (heatwaves) and improved emergency health responses | Focus on climate change adaptation and public health preparedness |
| Poland | Obesity and Cardiovascular Health | NCD Prevention and Management | Comparison of NCD prevention strategies across EU countries | Moderate improvements in obesity management and early screening for cardiovascular diseases. | Moderate risk of bias due to regional disparities in health access |
| Italy | Cancer Prevention | Health Equity and Access Programs | Comparison of health equity initiatives across EU regions | Improved healthcare access for marginalized populations, especially in Southern Italy. | Focus on equity in healthcare delivery |
| France | Mental Health | Mental Health Resilience | Comparison of mental health programs across EU countries | Access to mental health services improved, especially telemedicine access during COVID-19. | Moderate impact of mental health interventions on reducing stigma |
| Finland | Health System Performance | Digital Health and Health System Reforms | Comparison of digital health and health system reforms in Nordic countries | High digital health utilization, especially in Northern Finland. High score on CINeMA confidence. | Emphasizes health system innovation and digital transformation |
| United Kingdom | Respiratory Health | Air Quality Improvement Programs | Comparison of air quality interventions across EU and non-EU countries | Significant reductions in respiratory diseases, particularly in urban areas with improved air quality regulations. | Advanced air quality monitoring and health intervention strategies |
| Netherlands | Mental Health | Integration of Community-Based Health Services | Comparison of community health programs across Europe | Positive effects on mental health outcomes through community-based interventions | Focus on collaboration with local organizations |
| Belgium | NCD Prevention | Lifestyle Change Programs | Comparison of lifestyle interventions across EU countries | Strong improvements in reducing lifestyle-related diseases such as diabetes and hypertension | Focus on patient-centered care and prevention |
| Portugal | Cardiovascular Health | Preventive Cardiovascular Health Programs | Comparison of cardiovascular disease prevention strategies | Moderate improvement in cardiovascular health outcomes through lifestyle modifications | Focus on early screening and education on healthy lifestyles |
| Austria | Health Equity | Access to Healthcare for Marginalized Groups | Comparison of healthcare access across EU countries | Improved healthcare access for marginalized populations, especially for refugees and low-income groups. | Focus on reducing healthcare inequality |
| Denmark | Obesity and Nutrition | Obesity Prevention Programs | Comparison of obesity prevention initiatives across EU countries | Moderate success in weight loss and obesity prevention through national campaigns | Focus on nationwide nutrition education and lifestyle changes |
| Romania | Infectious Disease | Vaccination Programs | Comparison of vaccination rates and effectiveness across EU countries | Successful reduction in vaccine-preventable diseases in rural areas | Focus on increasing vaccination rates in underserved regions |
| Bulgaria | Cancer Care | Cancer Screening and Early Detection Programs | Comparison of cancer screening programs across EU countries | Significant improvement in early cancer detection rates and treatment outcomes | Focus on early detection and public health awareness |
Table 6.
Summary of Network Meta-Analysis Results, including effect sizes and confidence intervals.
| Comparison | Effect Size (Risk Ratio) | 95% Confidence Interval | Number of Studies | Key Findings | Additional Notes |
|---|---|---|---|---|---|
| Mental Health Resilience vs. Digital Health Integration | 1.20 | (1.05, 1.35) | 10 | Mental health resilience interventions showed a moderate increase in effectiveness compared to digital health integration. | Both interventions show positive effects, with mental health resilience slightly outperforming digital health programs. |
| Mental Health Resilience vs. NCD Prevention | 1.05 | (0.95, 1.15) | 15 | NCD prevention programs were slightly more effective in reducing risk factors compared to mental health resilience programs. | Both interventions are important, but NCD prevention has a slightly higher impact on health outcomes. |
| Digital Health Integration vs. Climate-Health Resilience | 1.30 | (1.15, 1.45) | 20 | Digital health integration programs are significantly more effective than climate-health resilience in terms of access and delivery of services. | Digital interventions showed more immediate benefits, but climate-health resilience had longer-term outcomes. |
| NCD Prevention vs. Health Equity Programs | 1.25 | (1.10, 1.40) | 25 | NCD prevention programs were found to be more effective in reducing chronic disease risk than health equity interventions. | Both preventive measures and equity are crucial, but NCD prevention programs are more directly impactful. |
| Climate-Health Resilience vs. Health Equity Programs | 1.15 | (1.00, 1.30) | 30 | Climate-health resilience programs were slightly more effective in improving health outcomes in high-risk populations compared to health equity initiatives. | Climate adaptation is necessary for vulnerable populations, especially in the Southern EU. |
Table 7.
CINeMA Confidence Scores for each intervention.
| Intervention | Indirectness | Imprecision | Heterogeneity | Bias | Incoherence | CINeMA Confidence Score |
|---|---|---|---|---|---|---|
| Mental Health Resilience | Low | Moderate | Low | Low | Low | High |
| Digital Health Integration | Low | Low | Low | Moderate | Low | Moderate |
| Climate-Health Resilience | Moderate | High | Moderate | Moderate | Moderate | Moderate |
| NCD Prevention | Low | Low | Low | Low | Low | High |
| Health Equity Programs | Low | Moderate | Low | Low | Low | Moderate |
Table 8.
Study-Level Results by Country.
| Country | Effect Size (Risk Ratio) | 95% Confidence Interval | Number of Studies | Key Findings | Additional Notes |
|---|---|---|---|---|---|
| Germany | 8.5 | (5.0000, 17.800) | 7 | An effect size of 8.5, showing positive results in mental health outcomes. | Focus on mental health resilience programs. |
| Poland | 6.1 | (4.0000, 13.840) | 4 | Positive impact on health outcomes. | Variation across studies in different countries. |
| France | 4.7 | (3.0000, 10.000) | 7 | Moderate effectiveness for mental health programs. | Focus on program effectiveness in European countries. |
| Finland | 7.3 | (6.0000, 12.000) | 10 | High efficacy of mental health resilience programs. | High effectiveness for mental health and NCD prevention. |
| Ireland | 6.4 | (5.0000, 10.000) | 10 | Strong impact on mental health outcomes. | Focus on the improvement of mental health systems. |
Table 9.
The results of Meta-analysis, Effect Size Estimates for Trim-and-Fill Analysis, and Individual Studies.
Table 9.
The results of Meta-analysis, Effect Size Estimates for Trim-and-Fill Analysis, and Individual Studies.
| ID | Study Citations | Effect Size | Std. Error | Z | Sig. (2-tailed) | 95% Confidence Interval | Exp. Effect Size | Exp. 95% Confidence Interval | Weight |
|---|---|---|---|---|---|---|---|---|---|
| Germany | [7,38,39,40,42,44,45] | 8.5 | 8.000 | 5.0000 | 1.600 | -1.800 to 17.800 | 2980.958 | 0.165 to 53748156.285 | 0.039 |
| Poland | [39,40,41,44] | 6.1 | 6.000 | 4.0000 | 1.500 | -1.840 to 13.840 | 403.429 | 0.159 to 1024644.149 | 0.060 |
| Greece | [38,39,40,43,44,45,86,88] | 5.2 | 4.000 | 1.0000 | 4.000 | < 0.001 | 54.598 | 7.691 to 387.596 | 0.649 |
| France | [39,40,41,43,44,45,86] | 4.7 | 7.000 | 3.0000 | 2.333 | 1.120 to 12.880 | 1096.633 | 3.065 to 392343.085 | 0.105 |
| Finland | [7,38,39,40,41,43,44,45,86,88] | 7.3 | 9.000 | 4.0000 | 2.250 | 1.160 to 16.840 | 8103.084 | 3.190 to 20580527.879 | 0.060 |
| Ireland | [7,38,39,40,41,42,43,44,45,86] | 6.4 | 6.000 | 5.0000 | 1.200 | 0.230 | 403.429 | 0.022 to 7274021.954 | 0.039 |
| Italy | [7,38,39,40,41,42,43,44,45,86] | 5.8 | 7.000 | 2.0000 | 3.500 | < 0.001 | 21.760 | 55266.818 to 1096.633 | 0.220 |
| Hungary | [7,38,39,40,41,42,43,44,45,86] | 4.7 | 6.000 | 1.0000 | 6.000 | < 0.001 | 56.828 | 2863.970 to 403.429 | 0.649 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



