
Submitted:
14 September 2025
Posted:
15 September 2025
You are already at the latest version
Abstract
Background: Chyle leakage is known to be a rare postoperative complication following liver transplantation (LT), and continuously leaked large quantities of chyle leakage can worsen prognosis. However, there is no explicit understanding of its mechanism and no existing reports showing the influence of chyle leakage after LT on blood concentration of the drug tacrolimus.
Case presentation: Despite escalating tacrolimus daily dose to 4.0 mg with CYP3A5 inhibitor, blood concentrations remained subtherapeutic (1.7–2.5 ng/mL) during active leakage. Conservative treatments failed, prompting intraperitoneal injection of erythromycin (0.75 g)-25% glucose solution (40 mL every other day). Following three treatments, chylous drainage diminished significantly, and tacrolimus concentrations abruptly increased to 14.7 ng/mL 2 days after leakage resolved. Dose adjustments subsequently stabilized levels at 4.6–6.2 ng/mL with daily dose of 2.0mg.
Conclusions: Intraperitoneal injection of erythromycin hypertonic solution may promote lymphatic fistula closure via chemical stimulation. Chyle leakage may reduce tacrolimus blood concentration through drug loss in chylous fluid. This case highlights the need for clinical attention to the association between chyle leakage and immunosuppressant concentrations, though further studies are required for validation.
Keywords:
liver transplantation
; chyle leakage
; tacrolimus
; blood concentration
; erythromycin
1. Introduction
Chylous ascites is a milky, high-triglyceride abdominal effusion caused by disruption or obstruction of the intra-abdominal lymphatic system. Common etiologies include malignant tumors, liver cirrhosis, traumatic injury, autoimmune disorders, and inflammation [1]. Surgical damage to the intestinal lymphatic pathways can cause complications such as chylous ascites or fistula, adversely affecting patient health and medication efficacy [2,3,4]. Chyle leakage is a rare but prognostically significant complication of liver transplantation, particularly in prolonged cases [5]. Standardized therapies for this complication have not yet been established, and outcomes are uncertain and fluctuate in practice [6,7,8].
Tacrolimus is a key immunosuppressant post-LT to prevent rejection, with its blood concentrations critically monitored due to risks of both subtherapeutic and toxic levels [9,10]. However, the impact of post-LT chyle leakage on tacrolimus pharmacokinetics remains unreported [9,11,12]. Here, we present a case of chyle leakage managed innovatively via intraperitoneal erythromycin hypertonic solution injection, accompanied by observed tacrolimus concentration fluctuations. Our findings aim to enhance understanding of the interplay between chyle leakage and tacrolimus pharmacodynamics, providing guidance for clinical management of this rare post-LT complication.
2. Case Presentation
The patient was a 43-year-old male weighing 60kg whose intraoperative diagnoses were primary hepatocarcinoma, decompensated cirrhosis, and massive ascites. On the fifth postoperative day after orthotopic LT, the right subphrenic drainage increased and milky white greasy fluid accumulated to 500ml in 24 hours (Figure 1). The right subhepatic drainage was identical in character but scarce in amount. The patient declared no specific discomfort. Tests results of the drainage were as follows: Rivalta test (+), specific gravity 1.028, white blood cell count 6.1X109/L, total protein 27.3g/L, glucose 7.89mmol/L, Chloride 104.8mmol/L, and negative bacteria culture. Chyle leakage was hence diagnosed. We administered albumin, diuretics, a high-protein, and low-fat diet, oral meglumine distrizoate, and hypodermic injection of octreotide as conservative treatments; however, conservative management proved ineffective. The character and amount of the drainage did not change notably and ultimately increased to approximately 2000ml/24h between the ninth and eleventh postoperative days.
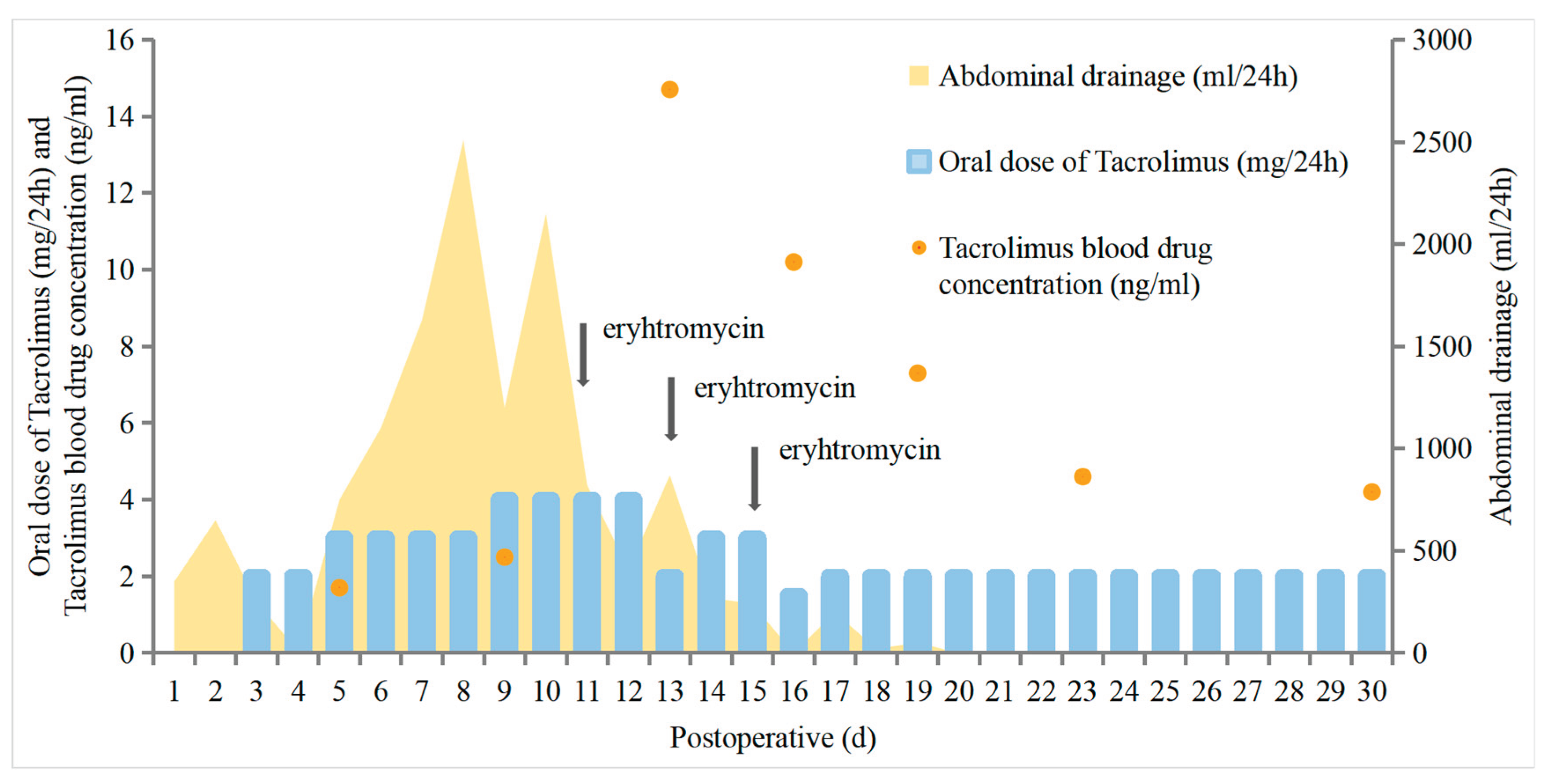
Beginning on day 11, we injected 40ml of erythromycin (0.75g) glucose (25%) hypertonic solution into the right subphrenic drainage tube every other day. Following each erythromycin injection, the drainage tube was clamped for 1 hour to facilitate local retention, after which it was unclamped to restore continuous drainage. After three rounds, the chylous drainage decreased to 800ml/24h on the 12th day, 400ml/24h on the 14th day and a little on the 16th day (Figure 2). The main complication of the manipulation was local transient pain. After a search by ultrasonic exam, the right subhepatic and subphrenic drainage tubes were extracted on the 21st and 23rd postoperative day, respectively.
Noteworthily, the blood tacrolimus concentration was influenced substantially by the chyle leakage. From postoperative day 3, the patient was administered tacrolimus at a dose of 1.0mg BID, with a blood concentration of 1.7 ng/ml on day 5. When the dose was increased to 1.5 mg BID, Wuzhi capsules (a CYP3A5 inhibitor) were added to enhance tacrolimus concentrations [13]; however, this intervention showed minimal effect, with the blood concentration only rising to 2.5 ng/ml on day 9. From day 10, the dose was further increased to 2.0 mg BID. Following cessation of chyle leakage on day 13, the blood concentration abruptly surged to 14.7 ng/ml, prompting immediate discontinuation of Wuzhi capsules to avoid over-elevation of tacrolimus. The patient was then asked to skip the dose on the evening of the 13th day. After that, the dose was reduced to 1.5mg BID, with the concentration decreasing to 10.2 ng/ml on day 16. After another evening dose omission on day 16, the dose was reduced to 1.0 mg BID, with concentrations of 7.3 ng/ml (day 19) and 4.6 ng/ml (day 23). The patient was discharged on day 23, with a concentration of 4.2 ng/ml recorded on day 30 (Figure 2).
Follow-up
The patient underwent close monitoring of tacrolimus blood concentrations after discharge. Serial liver function tests demonstrated normal hepatic enzyme levels and synthetic function, indicating successful graft function. Notably, no signs of chyle leakage recurrence were observed during follow-up imaging (abdominal ultrasound at 1, 3, and 6 months post-discharge), and the patient reported no abdominal discomfort, weight loss, or evidence of malnutrition. As of the last follow-up on April 28, 2025, laboratory evaluations revealed stable tacrolimus levels ranging from 4.2 to 6.2 ng/mL within the therapeutic window, with no acute rejection or infectious complications; long-term follow-up also showed no evidence of hepatocellular carcinoma recurrence or metastatic disease based on abdominal and chest computed tomography scans at 12 and 18 months post-discharge, and the patient remained in good condition with consistent adherence to immunosuppressive therapy and regular clinic visits.
3. Discussion
Retrospective studies report the incidence rates of chyle leakage after adult LT to be 0.6% and 4.7%, respectively, and associate its occurrence with rare complications [2,5]. Chyle leakage after LT primarily stems from injury to abdominal lymphatic vessels during surgery or increased lymph production due to portal hypertension [5,14]. In this case, decompensated cirrhosis exacerbated lymphatic congestion, and surgical dissection near the hepatic hilum and retroperitoneal structures likely damaged lymphatic trunks. Key surgical considerations for preventing chyle leakage include: First, systematic identification and management of intraperitoneal or retroperitoneal lymphatic vessels (with focus on periportal, hepatic hilum, and para-aortic regions) and sealing suspicious lymphatic branches with clips or electrocoagulation [15,16]. Further, intraoperative lymphatic visualization using carbon nanoparticles or lipophilic contrast agents to detect injuries < 1 mm [17,18].
At present, there is no unified diagnostic criterion for chylous ascites. Matsuura et al. [19] proposed that the diagnosis can be confirmed when three or more of the following five criteria are met: (i) Milky appearance; (ii) Triglyceride (TG) > 110 mg/dL or TG-to-serum triglyceride ratio (TG-ASR) > 1.0; (iii) Cholesterol-to-serum cholesterol ratio (Cholesterol-ASR) < 1.0; (iv) Cell count > 1000/ uL with negative culture; (v) Cytology showing lymphocyte predominance. In this study, we confirmed the leaked fluid to be chyle by its character, white blood cell count, total protein, glucose, and culture results.
Timely treatment of post-LT chyle leakage is essential, with strategies including conservative (fasting, continuous drainage, medium chain triglycerides, total parenteral nutrition, somatostatin, diuretics, etc.), interventional and surgical approaches [3]. Due to the patient’s poor condition, operative methods were avoided, and erythromycin solution was selected. As reported, erythromycin induces chemical pleurodesis via inflammatory cell recruitment and serosal fibrosis [20,21], potentially acting similarly in the peritoneum. The transient pain in our patient post-injection may have been caused by inflammation, and no additional complications were detected after symptomatic treatments. Noting limited efficacy and individual variability [22,23], erythromycin may serve as an alternative for chemical peritoneal fixation, requiring tailored clinical decisions based on drainage characteristics and etiology.
Notably, the patient exhibited persistently low tacrolimus blood concentrations from the onset of chyle leakage, despite dose escalation to 4.0 mg/d, which failed to reach recommended levels [24]. However, the tacrolimus concentration increased along with the decrease in chyle leakage. Two mechanisms might contribute to the tacrolimus loss induced by chyle leakage: first, as a lipophilic drug, tacrolimus accumulated in lipid-rich chyle, evidenced by a rat chyle leakage model administered oral tacrolimus (0.5 mg/d for 2 weeks) showing tacrolimus concentrations in chylous ascites (57.93±4.31 ng/mL) were threefold higher than those in serum (19.65±0.52 ng/mL, P=0.0003), aligning with its lipid-binding properties. Clinically, this is analogous to reports of voriconazole sequestration in chylothorax fluid, which impairs therapeutic levels in patients with chylous effusions [25]; secondly, chyle leakage exacerbated hypoalbuminemia, increasing the free fraction of tacrolimus and accelerating its metabolic clearance via CYP3A4 [26]. While prior studies have focused on tacrolimus absorption, clearance, and drug interactions [24,27], this case—combined with Yoshida et al. [28] findings that oil-formulated tacrolimus enhances lymphatic transport but reduces blood concentrations—identifies chyle leakage as a critical yet unrecognized determinant of tacrolimus concentration fluctuations, underscoring the need for close monitoring in liver transplant recipients with lymphatic complications. In contrast, a clinical study measured the concentration of tacrolimus in the ascites of post-LT patients, reporting values ranging from 0.2 to 3.0 ng/mL, which accounted for 1.19-31.87% of whole-blood tacrolimus concentrations [29]. However, they noted that the effect of ascites drainage on the blood concentration of tacrolimus could be negligible, likely due to ascites being mainly formed by the exudation of tissue fluid and has a low lipid content, while highly lipophilic tacrolimus is more likely to combine with lipid carriers (e.g., chylomicrons, lipoproteins) in chylous fluid and enter mesenteric lymph [30]. Although erythromycin may elevate tacrolimus levels via CYP3A4 inhibition [31], short retention (1-hour clamping of the drainage tube) and the drainage site in this case likely caused most intraperitoneal erythromycin to drain out, minimizing its impact on tacrolimus concentrations [32].
This case report has some limitations. First, tacrolimus concentrations in drainage and erythromycin levels in blood were untested. Secondly, as a single-case study, its findings are affected by individual uniqueness, limiting conclusion generalizability. Therefore, further large-scale clinical trials and mechanistic experiments are needed to systematically validate the relationship between tacrolimus blood concentration and chyle leakage, as well as the efficacy and safety of erythromycin in treating post-LT chyle leakage.
4. Conclusion
Chyle leakage may reduce tacrolimus bioavailability by sequestering it in chylous fluid. Intraperitoneal erythromycin successfully applied here suggests chemical pleurodesis as a viable option for refractory lymphatic leaks. These findings highlight the need for therapeutic drug monitoring and targeted fistula management in LT patients with chylous complications. Further pharmacokinetic studies are warranted to quantify drug loss and optimize immunosuppressive regimens in this context.
Authorship contribution statement
Conceptualization, L.-S.H.; methodology, Y.-M.W. and L.-S.H.; software, Z.-Z.F.; validation, Y.-M.W., Z.-Z.F. and L.-S.H.; clinical work, B.-W., and L.-S.H.; writing—original draft preparation, Y.-M.W., Z.-Z.F. and L.-S.H.; writing—review and editing, L.-S.H.; visualization, L.-S.H; supervision, L.-S.H.
Ethics Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by Ethics Committee of The First Affifiliated Hospital of Xi’an Jiaotong University (No. XJTU1AF2023LSK-009) on 10 January 2023. Informed consent was obtained from all subjects involved in the study.
Acknowledgments
All authors have read and agreed to publish the version of this manuscript. This work was supported by National Natural Science Foundation of China (No.82070649); Shaanxi Provincial Health Commission (No.2022A001 and No.2023TD-09).
Conflicts of Interest
The authors declare no competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- Evans, J.G.; Spiess, P.E.; Kamat, A.M.; Wood, C.G.; Hernandez, M.; Pettaway, C.A.; Dinney, C.P.; Pisters, L.L. Chylous Ascites After Post-Chemotherapy Retroperitoneal Lymph Node Dissection: Review of the M. D. Anderson Experience. J. Urol. 2006, 176, 1463–1467. [Google Scholar] [CrossRef]
- Ijichi, H.; Soejima, Y.; Taketomi, A.; Yoshizumi, T.; Uchiyama, H.; Harada, N.; Yonemura, Y.; Maehara, Y. Successful management of chylous ascites after living donor liver transplantation with somatostatin. Liver Int. 2007, 28, 143–145. [Google Scholar] [CrossRef]
- Bhardwaj, R.; Vaziri, H.; Gautam, A.; Ballesteros, E.; Karimeddini, D.; Wu, G.Y. Chylous Ascites: A Review of Pathogenesis, Diagnosis and Treatment. J. Clin. Transl. Hepatol. 2018, 6, 1–9. [Google Scholar] [CrossRef]
- Lizaola, B.; Bonder, A.; Trivedi, H.D.; Tapper, E.B.; Cardenas, A. Review article: the diagnostic approach and current management of chylous ascites. Aliment. Pharmacol. Ther. 2017, 46, 816–824. [Google Scholar] [CrossRef]
- Yilmaz, M.; Akbulut, S.; Isik, B.; Ara, C.; Ozdemir, F.; Aydin, C.; Kayaalp, C.; Yilmaz, S. Chylous ascites after liver transplantation: Incidence and risk factors. Liver Transplant. 2012, 18, 1046–1052. [Google Scholar] [CrossRef]
- Adler E, Bloyd C, Wlodarczyk S. Chylous Ascites. J Gen Intern Med. 2020 May;35(5):1586–7.
- Saucedo-Crespo, H.; Roach, E.; Sakpal, S.V.; Auvenshine, C.; Steers, J. Spontaneous Chylous Ascites After Liver Transplantation Secondary to Everolimus: A Case Report. Transplant. Proc. 2020, 52, 638–640. [Google Scholar] [CrossRef] [PubMed]
- Takuwa, T.; Yoshida, J.; Ono, S.; Hishida, T.; Nishimura, M.; Aokage, K.; Nagai, K. Low-fat diet management strategy for chylothorax after pulmonary resection and lymph node dissection for primary lung cancer. J. Thorac. Cardiovasc. Surg. 2013, 146, 571–574. [Google Scholar] [CrossRef] [PubMed]
- Venkataramanan R, Swaminathan A, Prasad T, Jain A, Zuckerman S, Warty V, et al. Clinical pharmacokinetics of tacrolimus. Clin Pharmacokinet. 1995 Dec;29(6):404–30.
- Iwasaki, K. Metabolism of Tacrolimus (FK506) and Recent Topics in Clinical Pharmacokinetics. Drug Metab. Pharmacokinet. 2007, 22, 328–335. [Google Scholar] [CrossRef]
- Suetsugu, K.; Ikesue, H.; Miyamoto, T.; Shiratsuchi, M.; Yamamoto-Taguchi, N.; Tsuchiya, Y.; Matsukawa, K.; Uchida, M.; Watanabe, H.; Akashi, K.; et al. Analysis of the variable factors influencing tacrolimus blood concentration during the switch from continuous intravenous infusion to oral administration after allogeneic hematopoietic stem cell transplantation. Int. J. Hematol. 2016, 105, 361–368. [Google Scholar] [CrossRef]
- E Staatz, C.; E Tett, S. Clinical Pharmacokinetics and Pharmacodynamics of Tacrolimus in Solid Organ Transplantation. Clin. Pharmacokinet. 2004, 43, 623–653. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Jiang, F.; Zhou, R.; Jin, W.; Li, Y.; Duan, W.; Xu, L.; Yang, H. Clinical Evaluation of the Efficacy and Safety of Co-Administration of Wuzhi Capsule and Tacrolimus in Adult Chinese Patients with Myasthenia Gravis. Neuropsychiatr. Dis. Treat. 2021, ume 17, 2281–2289. [Google Scholar] [CrossRef] [PubMed]
- Al-Busafi, S.A.; Ghali, P.; Deschênes, M.; Wong, P. Chylous Ascites: Evaluation and Management. ISRN Hepatol. 2014, 2014, 1–10. [Google Scholar] [CrossRef]
- Kanno, T.; Kobori, G.; Ito, K.; Nakagawa, H.; Takahashi, T.; Takaoka, N.; Somiya, S.; Nagahama, K.; Ito, M.; Megumi, Y.; et al. Complications and their management following retroperitoneal lymph node dissection in conjunction with retroperitoneal laparoscopic radical nephroureterectomy. Int. J. Urol. 2022, 29, 455–461. [Google Scholar] [CrossRef]
- Xing, Q.; He, L.; Cao, T.; Hu, C.; Liu, X. Managing Chyle Leakage Following Right Retroperitoneoscopic Adrenalectomy: A Case Study. Am. J. Case Rep. 2024, 26, e945469. [Google Scholar] [CrossRef]
- Su, P.; Zhang, Z. Nano Carbon Tracer in the Repairing of Congenital Abdominal Chylorus Leakage. Indian J. Pediatr. 2023, 91, 294–296. [Google Scholar] [CrossRef]
- Wang, S.; Jiang, W. Post-esophagectomy chylothorax refractory to mass ligation of thoracic duct above diaphragm: a case report. J. Cardiothorac. Surg. 2022, 17, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Matsuura, T.; Yanagi, Y.; Hayashida, M.; Takahashi, Y.; Yoshimaru, K.; Taguchi, T. The incidence of chylous ascites after liver transplantation and the proposal of a diagnostic and management protocol. J. Pediatr. Surg. 2018, 53, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Zhai, C.-C.; Lin, X.-S.; Yao, Z.-H.; Liu, Q.-H.; Zhu, L.; Lin, D.-J.; Wan, Y.-Y. Erythromycin poudrage versus erythromycin slurry in the treatment of refractory spontaneous pneumothorax. J. Thorac. Dis. 2018, 10, 757–765. [Google Scholar] [CrossRef]
- Balassoulis, G.; Sichletidis, L.; Spyratos, D.; Chloros, D.; Zarogoulidis, K.; Kontakiotis, T.; Bagalas, V.; Porpodis, K.; Manika, K.; Patakas, D. Efficacy and Safety of Erythromycin as Sclerosing Agent in Patients With Recurrent Malignant Pleural Effusion. Am. J. Clin. Oncol. 2008, 31, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.; Chen, Z.; Shen, X.; Xie, T.; Wang, X.; Liu, T.; Ma, X. Refractory thrombocytopenia could be a rare initial presentation of Noonan syndrome in newborn infants: a case report and literature review. BMC Pediatr. 2022, 22, 1–6. [Google Scholar] [CrossRef]
- Hua, Q.-W.; Lin, Z.-Y.; Hu, X.-T.; Zhao, Q.-F. Treatment of persistent congenital chylothoraxwith intrapleural injection of sapylin in infants. Pak. J. Med Sci. 2016, 32, 1305–1308. [Google Scholar] [CrossRef]
- E Staatz, C.; E Tett, S. Clinical Pharmacokinetics and Pharmacodynamics of Tacrolimus in Solid Organ Transplantation. Clin. Pharmacokinet. 2004, 43, 623–653. [Google Scholar] [CrossRef]
- Tharanon, V.M. (.; Muangkasem, A.; Inprasit, N.M.(.; Chantharit, P.B.(. Patient With Probable Invasive Pulmonary Aspergillosis and Idiopathic Bilateral Chylothorax With Chylopericardium May Experience Unachievable Therapeutic Voriconazole Serum Levels. Ther. Drug Monit. 2025, 47, 452–456. [Google Scholar] [CrossRef]
- Chow FS, Piekoszewski W, Jusko WJ. Effect of hematocrit and albumin concentration on hepatic clearance of tacrolimus (FK506) during rabbit liver perfusion. Drug Metab Dispos. 1997 May;25(5):610–6.
- Yoshikawa, N.; Takeshima, H.; Sekine, M.; Akizuki, K.; Hidaka, T.; Shimoda, K.; Ikeda, R. Relationship between CYP3A5 Polymorphism and Tacrolimus Blood Concentration Changes in Allogeneic Hematopoietic Stem Cell Transplant Recipients during Continuous Infusion. Pharmaceuticals 2021, 14, 353. [Google Scholar] [CrossRef]
- Yoshida, T.; Nakanishi, K.; Yoshioka, T.; Tsutsui, Y.; Maeda, A.; Kondo, H.; Sako, K. Oral tacrolimus oil formulations for enhanced lymphatic delivery and efficient inhibition of T-cell’s interleukin-2 production. Eur. J. Pharm. Biopharm. 2015, 100, 58–65. [Google Scholar] [CrossRef]
- Yang, N.; Du, Y.; He, J.; Ge, J.; Wang, M.; Sun, R.; Zhu, H.; Ge, W. Distribution evaluation of tacrolimus in the ascitic fluid of liver transplant recipients with liver cirrhosis by a sensitive ultra-performance liquid chromatography-tandem mass spectrometry method. J. Sep. Sci. 2021, 45, 411–421. [Google Scholar] [CrossRef]
- Tso, P.; Bernier-Latmani, J.; Petrova, T.V.; Liu, M. Transport functions of intestinal lymphatic vessels. Nat. Rev. Gastroenterol. Hepatol. 2024, 22, 127–145. [Google Scholar] [CrossRef] [PubMed]
- Mignat, C. Clinically Significant Drug Interactions with New Immunosuppressive Agents. Drug Saf. 1997, 16, 267–278. [Google Scholar] [CrossRef] [PubMed]
- Chiang, L.-H.; Wu, T.-H.; Tsai, T.-C.; Lee, W.-C. Coadministration of Erythromycin to Increase Tacrolimus Concentrations in Liver Transplant Recipients. Transplant. Proc. 2019, 51, 1439–1441. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Milky white greasy fluid drainage from right subphrenic drainage tube.
Figure 2.
The change of abdominal drainage (ml/24h) of two tubes (right subphrenic and right subhepatic), oral dose of tacrolimus (mg/24h) and its blood drug concentration (ng/ml) from the first to the 30th day after LT. The erythromycin solution was applied on the 11th, 13th and 15th day.
Figure 2.
The change of abdominal drainage (ml/24h) of two tubes (right subphrenic and right subhepatic), oral dose of tacrolimus (mg/24h) and its blood drug concentration (ng/ml) from the first to the 30th day after LT. The erythromycin solution was applied on the 11th, 13th and 15th day.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



