Submitted:
13 September 2025
Posted:
16 September 2025
You are already at the latest version
Abstract
Background: Yellow fever (YF) persists as a major arboviral threat in South America, despite the availability of an effective vaccine. While Brazil has produced extensive clinical descriptions, data from Bolivia, Ecuador, Colombia, and Peru remain limited.
Methods: We conducted a descriptive retrospective multicenter analysis of laboratory-confirmed YF cases reported between January 2023 and August 2025 in four Andean countries. Demographic, epidemiological, clinical, and laboratory data were extracted from hospital and surveillance records.
Results: Twenty-one confirmed cases were identified: Bolivia (n = 8), Ecuador (n = 5), Colombia (n = 4), and Peru (n = 4). The median age was 25 years (IQR: 16–43), with a predominance of males (81%). Vaccination history was largely undocumented; 86% had unknown or absent records. The median delay from symptom onset to hospitalization was 5 days. Outcomes were severe, with 57% of case fatality rate (12/21), and the median time from symptom onset to death was 8 days. Early manifestations included fever (71%), arthralgia (19%), headache (19%), and myalgia (19%). During the toxic phase (severe disease), hemorrhage (86%), jaundice (62%), circulatory collapse (57%), and hepatic dysfunction (52%) predominated. Complications included intracranial hemorrhage, multiorgan dysfunction, sepsis, and renal failure. Laboratory findings revealed marked hepatic injury (AST median, 3257 U/L; ALT median, 1570 U/L), hyperbilirubinemia, metabolic acidosis, elevated lactate levels, hypoglycemia, and coagulopathy. RT-PCR for YFV was positive in 95% of tested cases.
Conclusions: This study provides one of the first systematic clinical characterizations of YF cases from Bolivia, Ecuador, Colombia, and Peru. The high fatality rate, despite the young age of patients, underscores the vulnerability of populations in resource-limited, peri-Amazonian settings. Severe hepatic dysfunction, hemorrhage, and systemic collapse were consistent hallmarks of the disease. These findings highlight the urgent need to strengthen vaccination coverage, enhance clinical recognition, and expand access to critical care in outbreak-prone areas of South America.
Keywords:
Yellow fever
; arboviral diseases
; clinical features
; South America
; hepatic dysfunction
; hemorrhagic fever
; case fatality
Introduction
Yellow fever (YF) remains one of the most significant arboviral diseases in South America, despite the availability of an effective vaccine for over eight decades [1]. Caused by the yellow fever virus (YFV), a mosquito-borne flavivirus primarily transmitted by Haemagogus species in rural areas, the disease continues to present a significant challenge to public health in endemic regions [2]. Clinical manifestations range from a mild, self-limiting febrile illness to severe disease characterized by hepatic dysfunction, hemorrhage, and multi-organ failure, with case fatality rates reaching 30–50% among severe cases [3]. While historically concentrated in the tropical regions of Africa, South America continues to experience recurrent outbreaks, often associated with sylvatic transmission cycles and spillover into human populations [4].
In the past two decades, South America has faced multiple yellow fever outbreaks with considerable epidemiological and clinical impact [5]. Large epidemics were reported in Brazil (2016–2018), spreading to previously non-endemic areas and causing international concern regarding the risk of urban transmission [6]. Meanwhile, neighboring countries such as Bolivia, Ecuador, Colombia, and Peru, although traditionally endemic, have reported fewer cases but remain highly vulnerable due to ecological, climatic, and socioeconomic factors [7,8]. In these regions, the presence of competent vectors, expanding human mobility, and uneven vaccination coverage create the conditions for sporadic but potentially severe outbreaks. Importantly, recent increases in human cases, alongside reports of epizootics in non-human primates, have highlighted the persistent circulation of YFV in the Andean-Amazonian interface [9,10].
The clinical spectrum of yellow fever in South America has been relatively well described in Brazil [11,12,13]; however, fewer systematic reports are available from Bolivia [14], Ecuador [15], Colombia [16], and Peru [17]. Most publications from these countries focus on epidemiological descriptions or outbreak notifications, while detailed clinical characterizations in adults and children remain scarce [18,19,20,21,22]. This represents a significant gap, as the clinical profile of YF cases may be influenced by host-related factors, comorbidities, co-circulating pathogens, and healthcare access [11,12,13]. Furthermore, differences in reporting practices and healthcare infrastructure across countries may contribute to under-recognition or incomplete documentation of the disease burden. Understanding the clinical presentation of yellow fever in diverse South American contexts is crucial for improving diagnostic suspicion, enhancing case management, and refining public health preparedness [23,24].
Between 2023 and 2025, yellow fever cases have been reported in Bolivia, Ecuador, Colombia, and Peru, marking one of the most recent multi-country periods of confirmed human disease in the Andean region [4,5]. These cases occurred against a backdrop of increasing arboviral activity, including dengue, chikungunya, Zika, and Oropouche, which often present with overlapping clinical features [25,26]. Distinguishing YF from other febrile syndromes is challenging, particularly in rural or resource-limited settings where access to laboratory confirmation is restricted. Thus, detailed clinical descriptions from confirmed cases are essential for both frontline clinicians and surveillance systems [25,26].
In this Brief Report, we present a retrospective analysis of yellow fever cases confirmed between January 2023 and August 2025 in four South American countries: Bolivia, Ecuador, Colombia, and Peru. Our objective is to describe the clinical features observed in these patients, highlighting both frequent and distinctive manifestations. By providing region-specific clinical insights, this study contributes to the limited body of literature on YF in these countries. It underscores the continued need for vigilant clinical recognition, timely laboratory confirmation, and preventive strategies such as vaccination.
Methods
We conducted a retrospective, multicenter study of yellow fever (YF) cases confirmed between January 2023 and August 2025 in four South American countries: Bolivia, Ecuador, Colombia, and Peru (Figure 1). Clinical, epidemiological, and laboratory data were collected from hospitals, departmental health services, and regional laboratories involved in case detection and management. Participating centers included facilities in Santa Cruz, La Paz, and Beni (Bolivia); Loja and Zamora Chinchipe (Ecuador); Putumayo (Colombia); and Amazonas (Peru). Cases were identified through local surveillance systems, medical records, and laboratory registers.
Case Definition and Inclusion Criteria
Patients were included if they had laboratory-confirmed YF infection by reverse transcription polymerase chain reaction (RT-PCR) or detection of anti-YFV IgM antibodies using ELISA, in accordance with national guidelines. Suspected cases with negative laboratory results or insufficient documentation were excluded. A total of 21 patients meeting the criteria were analyzed.
Data Collection
Demographic and epidemiological variables (age, sex, occupation, vaccination history, and geographic origin) were extracted from clinical charts and epidemiological reports. Clinical manifestations were categorized into initial (early) symptoms and severe findings corresponding to the toxic phase (severe disease). Complications were documented when explicitly recorded by treating physicians. Laboratory parameters included hematological, biochemical, coagulation, and virological results, with reference values used to classify abnormalities. Data were entered into standardized forms and cross-checked by local investigators to ensure accuracy.
Outcomes
Clinical outcomes were classified as survival or death. For fatal cases, the interval between symptom onset and death was calculated.
Statistical Analysis
Descriptive statistics were applied. Categorical variables were summarized as absolute numbers and percentages, while continuous variables were expressed as medians with interquartile ranges (IQR). No formal hypothesis testing was performed due to the study's limited sample size and descriptive nature.
Ethical considerations
All research was performed consistent with the ethical standards established in the 1964 Declaration of Helsinki. The study utilized secondary, anonymized data from routine surveillance and hospital records, without requiring direct patient contact. Patient confidentiality was preserved throughout the process. This study protocol was approved by the Bioethics Committee of the Universidad Nacional Autónoma de Honduras (Acta No. IRB 00003070, 2025).
Results
A total of 21 laboratory-confirmed yellow fever (YF) cases were identified between January 2023 and August 2025 across the four participating countries (Table 1). Most cases (81%, n = 17) were reported in 2025, while the remainder occurred in 2023 and 2024. Bolivia accounted for the largest share (38%, n = 8), followed by Ecuador (24%, n = 5), Colombia (19%, n = 4), and Peru (19%, n = 4). The median age of patients was 25 years (interquartile range [IQR]: 16–43), with a predominance of males (81%, n = 17). Regarding occupational background, students represented the largest group (24%), followed by agricultural (14%), construction (10%), and mining workers (5%). Nearly half of the cases were classified as “other” or “unknown” occupations. Notably, vaccination history was poorly documented: 86% (n = 18) had unknown or no vaccination against the YF virus, while only three patients (14%) were apparently vaccinated. The median interval from symptom onset to medical consultation and hospitalization was 5 days (IQR: 4–6). Clinical outcomes were severe, with 12 patients (57%) dying and 9 (43%) surviving. For fatal cases, the median time from symptom onset to death was 8 days (IQR: 6–9).
Clinical Manifestations
Initial clinical findings were generally nonspecific and compatible with other acute febrile illnesses (Table 2). Fever was the most common early symptom, present in 71% (n = 15). Other initial manifestations included arthralgia (19%, n = 4), headache (19%, n = 4), myalgia (19%, n = 4), and vomiting (5%, n = 1).
During the toxic phase (severe disease), severe features predominated. Hemorrhagic manifestations were observed in 86% of patients (n = 18), making bleeding the single most frequent severe clinical finding. Jaundice was present in 62% (n = 13), consistent with hepatic dysfunction. Circulatory collapse occurred in more than half (57%, n = 12), while overt hepatic dysfunction was documented in 52% (n = 11). Encephalopathy was noted in 38% (n = 8), renal failure in 24% (n = 5), and biochemical evidence of high transaminases in 19% (n = 4). Less frequent but notable severe findings included coagulopathy (14%, n = 3), thrombocytopenia (10%, n = 2), hyperbilirubinemia (10%, n = 2), azotemia (5%, n = 1), and coma (5%, n = 1).
Several complications were recorded (Table 2). The most frequent were severe coagulation disorders (14%, n = 3), pleural effusion (10%, n = 2), acute kidney injury (10%, n = 2), anemia (10%, n = 2), intracranial hemorrhage (10%, n = 2), and multiorgan dysfunction (10%, n = 2). Less common complications included hypokalemia, pancytopenia, pneumonia, shock, bilateral nephromegaly, cerebral anoxia, edema, and superinfections due to extended-spectrum β-lactamase (ESβL)–producing Klebsiella pneumoniae and Escherichia coli. Each of these was observed in one patient (5%).
Laboratory Findings
Laboratory data were available for a subset of patients and showed significant alterations (Table 3). Acid-base balance was frequently disrupted: 60% of tested patients had pH values below reference levels, while all tested cases exhibited reduced bicarbonate (HCO₃⁻) concentrations. Elevated anion gaps were found in 40%. Marked lactic acidosis was observed, with all measured cases (100%) showing lactate levels far above the normal range (median 13.1 mmol/L). Hypoglycemia was also prevalent, with 80% of cases showing glucose below reference values.
Renal function markers were consistently abnormal. Urea was elevated in all tested cases (100%), and creatinine was elevated in 67%, confirming renal impairment (Table 3). Hepatic markers were severely altered: total and direct bilirubin were elevated in all tested cases (100%), with indirect bilirubin elevated in 33%. Transaminases were markedly raised, with 100% of tested patients showing AST and ALT elevations, reaching median values of 3257 U/L and 1570 U/L, respectively. Gamma-glutamyl transferase (GGT) and alkaline phosphatase were also elevated in all tested cases. Protein levels were altered, with total protein and globulin decreased in all cases tested (100%), while hypoalbuminemia was observed in 75% (Table 3).
Coagulation studies revealed prolonged prothrombin times in 75% of tested patients and increased INR values in 50%. Activated partial thromboplastin times (aPTT) were prolonged in 27%. Fibrinogen levels were reduced by 75%. Hematological findings included anemia in 46%, leukopenia in 38%, and thrombocytopenia in 77% of tested patients. Elevated inflammatory and tissue injury markers were also noted: C-reactive protein was raised in 33%, lactate dehydrogenase (LDH) in 100%, and creatine phosphokinase (CPK) in 100% of tested cases (Table 3).
Molecular and serological testing confirmed the diagnosis in all cases. RT-PCR for YFV was positive in 95% (18/19) of tested cases, while IgM against YFV was positive in all tested cases (7/7) (Table 3). One case tested positive for dengue IgM, and one for dengue NS1 antigen, suggesting possible coinfections or cross-reactivity. Median RT-PCR cycle threshold (Ct) values were 23.45 (IQR: 22.6–24.6).
Discussion
South American countries continue reporting confirmed cases and deaths due to yellow fever (YF). As of September 12, 2025, the 2024/2025 outbreak has resulted in 326 cases and 136 deaths (41.7%) in 6 countries (https://shiny.paho-phe.org/yellowfever/). Despite this, there is a lack of recent studies in the region that describe the clinical characteristics and profile of cases during this significant outbreak.
Our study provides one of the few systematic analyses of YF clinical characteristics across Bolivia, Ecuador, Colombia, and Peru between 2023 and 2025. Among 21 laboratory-confirmed cases, the majority were young males, often with uncertain vaccination history, and case fatality reached 57%. Hemorrhagic manifestations, jaundice, circulatory collapse, hepatic dysfunction, and encephalopathy were dominant features, frequently accompanied by multiorgan complications, including renal failure and sepsis [27]. These findings confirm that severe forms of YF remain a significant threat in the Andean-Amazonian interface, resembling the fulminant cases reported in major Brazilian outbreaks, but with particular distinctions in patient demographics, clinical spectrum, and outcomes [3,28].
The extensive retrospective study from Minas Gerais, Brazil, involving 283 hospitalized patients during the 2017–2018 epidemic, reported an in-hospital fatality rate of 24% [13]. In stark contrast, our smaller Andean cohort showed more than double that fatality (57%). Several explanations may account for this difference. First, the Brazilian study population had a median age of 46 years, considerably older than our median of 25 years. Yet despite a younger age, our cases fared worse. This suggests that factors beyond host age, including delays in care, comorbid infections, or limited critical care capacity, may have contributed to the increased lethality. Moreover, in Brazil, patients were treated in a referral center with an intensive care infrastructure. In contrast, many of our cases originated in rural or peri-Amazonian settings, where diagnostic and therapeutic resources were constrained, as has been reported in other series with high case fatality rates [16].
Risk factors linked to fatality rate in Brazil included higher age, male sex, elevated viral load, and abnormal markers such as aspartate aminotransferase (AST), international normalized ratio (INR), lactate, and leukocytosis [13]. We did not perform viral load quantification in most cases. We did not perform multivariate modeling due to sample size limitations, but severe hemorrhage, jaundice, and circulatory collapse were frequent among fatal outcomes in our series. Notably, laboratory data in our patients frequently revealed metabolic acidosis, low bicarbonate, and high lactate, consistent with the Brazilian findings [13]. These parallels suggest that despite geographical variation, markers of hepatic failure, coagulopathy, and systemic acidosis remain core prognostic indicators.
A key diagnostic challenge in yellow fever endemic areas is the co-circulation of pathogens with overlapping clinical features [25]. Arboviruses such as dengue [29], chikungunya [30], Zika [31], and Oropouche [26], as well as Leptospira spp. [32] and Plasmodium spp. [33], among others [34], may all present with fever, jaundice, renal failure, and hemorrhage, complicating differential diagnosis. Coinfections are possible and were suggested in our series by positive dengue serological markers in one patient, as well as with bacterial infections [35]. We did not find any previous report of yellow fever presenting with ESβL bacterial coinfections. This underscores the importance of comprehensive diagnostic approaches, since therapeutic needs for malaria or leptospirosis, but even bacterial infections due to resistant-organisms, differ from the supportive care required for viral hemorrhagic fevers, and unrecognized coinfections may worsen outcomes [3].
The São Paulo ICU cohort of 79 patients described by Ho and colleagues reported a strikingly high fatality of 67%, comparable to our 57% [12]. Their patients were older (median 42 years), but also mostly male and unvaccinated. Clinical parallels with our series include the predominance of hemorrhagic complications and multiorgan involvement. However, some systemic manifestations were more prominent in Brazil [12]. For instance, 73% of ICU patients required renal replacement therapy, reflecting a high burden of acute kidney injury and metabolic acidosis. In our cohort, only 24% developed renal failure, though biochemical evidence of acidosis was common. This may reflect under-recognition of renal involvement in resource-limited settings or actual epidemiological variation.
Brazilian ICU reports highlighted unexpected complications, including necrohemorrhagic pancreatitis, frequent seizures even without intracranial hypertension, and profound coagulopathy [12]. These were not observed in our cohort, though intracranial hemorrhage occurred in two patients [36]. Differences may stem from a smaller sample size in our study or underdiagnosis due to a lack of advanced imaging and laboratory support. The São Paulo group also reported the utility of preventive anticonvulsant therapy and plasma exchange as novel management strategies, underlining the importance of tertiary care interventions that remain largely inaccessible in Andean rural hospitals [12].
A study focused on ophthalmology from Minas Gerais identified YF-associated retinopathy in 20% of patients [11]. Characteristic lesions included retinal nerve fiber layer infarcts, superficial hemorrhages, and grayish outer retinal or choroidal lesions. These ocular findings correlated strongly with systemic severity; patients with elevated AST, bilirubin, creatinine, lactate, and thrombocytopenia were more likely to develop retinopathy. Notably, none of our cases included a systematic ocular examination, and no retinopathy was documented. This highlights a significant gap in Andean YF case characterization: while systemic manifestations dominate the clinical picture, ocular involvement may remain overlooked. Given that retinopathy may serve as a clinical marker of severe systemic disease, its under-recognition in our series suggests the need to integrate ophthalmologic evaluation into outbreak investigations [11].
In our cohort, vaccination history was largely undocumented; 86% had unknown or absent records. Only three patients were reportedly vaccinated, one of whom still developed severe disease. In Brazil, vaccination coverage was better documented. In the Minas Gerais study, 44% reported prior vaccination, with possible breakthrough cases when vaccination occurred within 10 days of onset [13,37]. Similarly, in São Paulo, several ICU patients developed breakthrough infections despite vaccination ≥10 days before onset [11]. These findings collectively emphasize that although vaccination remains the cornerstone of prevention, gaps in record-keeping, incomplete immunization, and rare vaccine failures complicate outbreak control [4,5].
Median time from symptom onset to hospitalization in our study was 5 days, similar to Brazil (4 days in Minas Gerais, 6 days in São Paulo) [12,13]. Nevertheless, the fatality rate was higher in our cohort. This suggests that while delays were comparable, differences in case management capacity likely influenced prognosis [3]. Intensive care resources in Brazilian referral hospitals enabled interventions such as dialysis, plasma exchange, or advanced monitoring, which were unavailable in most of our participating centers. Thus, the disparity in survival highlights the critical role of healthcare infrastructure rather than solely disease biology [12,13].
Hemorrhagic signs were the single most frequent severe feature in our series (86%), surpassing jaundice (62%). In contrast, in São Paulo, hemorrhage was documented in 65% of ICU patients [12], while in Minas Gerais, bleeding was less commonly recorded at admission (about 10%) [13]. This suggests potential heterogeneity in clinical expression across regions or differences in documentation emphasis. Hepatic involvement was profound in both our cohort and the Brazilian ICU cases, with AST frequently above thousands of units per liter and rapid progression to hepatic encephalopathy. These consistent findings reinforce the central role of hepatic dysfunction as the hallmark of severe YF [3,12,13].
Our report adds to the growing body of literature that YF is a multisystemic infection with heterogeneous complications. We documented pleural effusion, anemia, pneumonia, superinfections with resistant bacteria, and even bilateral nephromegaly. Such findings are rarely reported in Brazilian cohorts, possibly due to a focus on hepatic, renal, and neurologic involvement. Conversely, pancreatitis and cardiac dysfunction were notable in São Paulo [12] but not in our cases. The differences may partly reflect sample size, diagnostic capacity, and reporting scope. These variations underscore that while the classic triad of jaundice, hemorrhage, and renal failure defines severe YF, additional complications should not be overlooked [1].
Taken together, the Andean and Brazilian experiences converge on several lessons. First, severe YF can present with diverse systemic involvement, requiring high clinical suspicion even in young, previously healthy individuals. Second, early laboratory abnormalities—particularly elevated AST, coagulopathy, lactate, and thrombocytopenia—serve as prognostic markers across settings. Third, ocular involvement may be an overlooked indicator of severity. Finally, fatality rate remains unacceptably high in the absence of supportive critical care. Expanding intensive care access, training healthcare providers in outbreak-prone areas, and integrating ophthalmologic screening could enhance survival and clinical recognition [38,39]. Use of evidence-based guidelines is critical, especially among patients with severe yellow fever, in order to decrease the fatality rates [3].
Limitations
Our study’s main limitation is the small sample size compared to Brazilian cohorts, which restricts statistical analysis of prognostic factors. Additionally, the lack of systematic laboratory and imaging data limited direct comparisons. Nonetheless, the high case fatality rate observed despite a younger age highlights the gravity of YF in under-resourced settings. Future multicenter collaborations across South America could harmonize data collection and allow more robust cross-country analyses.
Conclusions
This comparative analysis highlights both the commonalities and differences in the clinical expression of yellow fever (YF) between the Andean countries and Brazil. Across all studied settings, hepatic failure, hemorrhage, and systemic collapse consistently emerged as the dominant and most life-threatening features of severe disease. These manifestations confirm the classical pathophysiology of YF while highlighting the need for vigilant clinical recognition during outbreak situations.
However, the contrasts between cohorts are equally informative. Case fatality rates varied substantially, reaching alarming levels in the Andean cases despite younger patient age, whereas Brazilian referral cohorts documented a lower overall fatality rate but a broader spectrum of systemic complications, including seizures, pancreatitis, and retinopathy. Such differences illustrate the complex interplay between viral pathogenesis, host immune and metabolic responses, and the structural capacity of healthcare systems to provide timely and advanced supportive care. The underreporting of ocular involvement in Andean cases, contrasted with systematic documentation of retinopathy in Brazil, also emphasizes how diagnostic focus and available expertise can shape the clinical picture of YF.
These findings collectively reinforce that YF remains not only a biological challenge but also a challenge to the health system. Ensuring access to vaccination remains the cornerstone of prevention, but vaccination gaps, incomplete records, and occasional breakthrough infections highlight persistent vulnerabilities. Early recognition of severe disease markers, such as hypertransaminasemia, metabolic acidosis, and coagulation abnormalities, should be prioritized in outbreak protocols, particularly in rural areas where referral may be delayed. Equally, strengthening intensive care capacity, including renal replacement therapies, advanced monitoring, and multidisciplinary support, is essential to reducing the devastating impact of YF across South America.
In sum, the comparison between Andean and Brazilian experiences reveals that although the clinical core of YF is universal, its outcomes are profoundly shaped by context. Bridging these gaps through coordinated regional strategies that integrate prevention, early diagnosis, and equitable access to advanced care will be key to mitigating the high burden of YF in the region and safeguarding populations at risk.
Author Contributions
AJRM, WEVG, DKBA, ICSR: study concept and design; data collection, interpretation of data; drafting and critical revision of the manuscript; BCC, RG, OELE, JVM, CPJ, GBPB, NFDT, ICSR, CLSJ, ECCV, GEDL, CDA, OLCP, JLBA, FRAG, JEAS, MVC, SLAM, JPEA, RDMJ, CEGF, CNAG, JLAS, CMMN, HACC, NFAS, LZ, JECP, JMS: data collection, interpretation of data; critical revision of the manuscript; All authors: approved final version submitted.
Funding
The current article processing charges (publication fees) were funded by the Facultad de Ciencias Médicas (FCM) (2-03-01-01), Universidad Nacional Autonoma de Honduras (UNAH), Tegucigalpa, MDC, Honduras, Central America (granted to Zambrano).
Acknowledgements
This article has been registered in the Research Proposal Registration of the Coordination of Scientific Integrity and Surveillance of Universidad Cientifica del Sur, Lima, Peru.
Conflicts of Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- Reno, E.; Quan, N.G.; Franco-Paredes, C.; Chastain, D.B.; Chauhan, L.; Rodriguez-Morales, A.J.; Henao-Martínez, A.F. Prevention of yellow fever in travellers: an update. Lancet Infect Dis 2020, 20, e129–e137. [Google Scholar] [CrossRef]
- Rodriguez-Morales, A.J.; Sah, R.; Silva-Ramos, C.R.; Pava-Garzón, D.M. Challenges in Emerging and Reemerging Arboviral Diseases: The Examples of Oropouche and Yellow Fever. Pathogens 2025, 14, 621. [Google Scholar] [CrossRef] [PubMed]
- Forero-Delgadillo, A.J.; Morales-Olivera, J.A.; Celis-Guzmán, J.F.; Zapata-Díaz, O.E.; González-Varona, G.A.; Acevedo-Bedoya, C.A.; Salazar-Fernández, R.; Ordoñez, J.O.; Robayo-Amortegui, H.; Quintero-Altare, A. , et al. Colombian consensus on the care of critically ill patients with suspected or confirmed severe yellow fever. Lancet Reg Health Am 2025, 48, 101144. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Morales, A.J.; Alhazmi, A.H.; Katime, A.; Hameed, A.A.; Morales, A.; Lepetic, A.C.; Risquez, A.; Forero-Delgadillo, A.J.; Holguin, A.; Faccini-Martínez Á, A. , et al. Yellow fever in South America - A plea for action and call for prevention also in travelers from SLAMVI, ESGITM, EVASG, ALEIMC, GEPI-SEIMC, SEMEVI, and CMTZMV-ACIN. Travel Med Infect Dis 2025, 67, 102871. [Google Scholar] [CrossRef]
- Angerami, R.N.; Socorro Souza Chaves, T.D.; Rodríguez-Morales, A.J. Yellow fever outbreaks in South America: Current epidemiology, legacies of the recent past and perspectives for the near future. New Microbes New Infect 2025, 65, 101580. [Google Scholar] [CrossRef] [PubMed]
- Chaves, T.; Orduna, T.; Lepetic, A.; Macchi, A.; Verbanaz, S.; Risquez, A.; Perret, C.; Echazarreta, S.; Rodríguez-Morales, A.J.; Lloveras, S.C. Yellow fever in Brazil: Epidemiological aspects and implications for travelers. Travel Med Infect Dis 2018, 23, 1–3. [Google Scholar] [CrossRef]
- Rodríguez-Morales, A.J.; Bonilla-Aldana, D.K.; Suárez, J.A.; Franco-Paredes, C.; Forero-Peña, D.A.; Mattar, S.; Villamil-Gómez, W.E.; Ruíz-Sáenz, J.; Cardona-Ospina, J.A.; Figuera, M.E. , et al. Yellow fever reemergence in Venezuela - Implications for international travelers and Latin American countries during the COVID-19 pandemic. Travel Med Infect Dis 2021, 44, 102192. [Google Scholar] [CrossRef]
- Alvarez-Moreno, C.A.; Rodriguez-Morales, A.J. Challenges of the current yellow fever outbreak in Colombia. Lancet 2025, 405, 2273. [Google Scholar] [CrossRef]
- Bonilla-Aldana, D.K.; Bonilla-Aldana, J.L.; Castellanos, J.E.; Rodriguez-Morales, A.J. Importance of Epizootic Surveillance in the Epidemiology of Yellow Fever in South America. Current Tropical Medicine Reports 2025, 12, 16. [Google Scholar] [CrossRef]
- Sanchez-Rojas, I.C.; Bonilla-Aldana, D.K.; Solarte-Jimenez, C.L.; Bonilla-Aldana, J.L.; Belisario-Tovar, M.; Ortega-Gómez, S.; Zambrano-Quenan, V.M.; Perafan-Gomez, J.C.; Gomez-Ocampo, C.H.; Delgado-Cajigas, M.; et al. Fatal yellow fever among captive non-human primates in southern Colombia, 2025. Frontiers in Veterinary Science 2025, 12, 1655474. [Google Scholar] [CrossRef]
- Brandão-de-Resende, C.; Cunha, L.H.M.; Oliveira, S.L.; Pereira, L.S.; Oliveira, J.G.F.; Santos, T.A.; Vasconcelos-Santos, D.V. Characterization of Retinopathy Among Patients With Yellow Fever During 2 Outbreaks in Southeastern Brazil. JAMA Ophthalmol 2019, 137, 996–1002. [Google Scholar] [CrossRef]
- Ho, Y.L.; Joelsons, D.; Leite, G.F.C.; Malbouisson, L.M.S.; Song, A.T.W.; Perondi, B.; Andrade, L.C.; Pinto, L.F.; D'Albuquerque, L.A.C.; Segurado, A.A.C. Severe yellow fever in Brazil: clinical characteristics and management. J Travel Med 2019, 26. [Google Scholar] [CrossRef] [PubMed]
- McClure, M.; de Rezende, I.M.; Pereira, L.S.; Dutra, M.R.T.; Fradico, J.R.B.; Macedo, R.; Marçal, M.C.; Fonte Boa, L.S.C.; Bragato, A.M.C.; Faria, F.A.A. , et al. Risk factors associated with in-hospital mortality during yellow fever outbreak in Brazil. Front Med (Lausanne) 2025, 12, 1505005. [Google Scholar] [CrossRef] [PubMed]
- Baronti, C.; Goitia, N.J.; Cook, S.; Roca, Y.; Revollo, J.; Flores, J.V.; de Lamballerie, X. Molecular epidemiology of yellow fever in Bolivia from 1999 to 2008. Vector Borne Zoonotic Dis 2011, 11, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Garcia, E. [Yellow Fever National Service of Ecuador]. Bol Oficina Sanit Panam 1949, 28, 1099–1106. [Google Scholar] [PubMed]
- Sanchez-Rojas, I.C.; Solarte-Jimenez, C.L.; Chamorro-Velazco, E.C.; Diaz-Llerena, G.E.; Arevalo, C.D.; Cuasquer-Posos, O.L.; Bonilla-Aldana, J.L.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. Yellow fever in Putumayo, Colombia, 2024. New Microbes New Infect 2025, 64, 101572. [Google Scholar] [CrossRef]
- Smith, A. Rise and Progress of Yellow Fever in Peru. Edinb Med Surg J 1855, 82, 165–204. [Google Scholar]
- Cabezas, C. Yellow fever in Peru and the Americas and the latent risk of reurbanuzation: an avoidable threat. Rev Peru Med Exp Salud Publica 2025, 42, 113–114. [Google Scholar] [CrossRef]
- Garcia-Bereguiain, M.A.; Cisneros, S.S.; Narváez, A.; Orlando, S.A.; Rodríguez-Pazmiño Á, S. Yellow fever outbreak in Ecuador and travel vaccination policies. J Travel Med 2025. [Google Scholar] [CrossRef]
- Paupy, C.; Le Goff, G.; Brengues, C.; Guerra, M.; Revollo, J.; Barja Simon, Z.; Hervé, J.P.; Fontenille, D. Genetic structure and phylogeography of Aedes aegypti, the dengue and yellow-fever mosquito vector in Bolivia. Infect Genet Evol 2012, 12, 1260–1269. [Google Scholar] [CrossRef]
- Rifakis, P.M.; Benitez, J.A.; De-la-Paz-Pineda, J.; Rodriguez-Morales, A.J. Epizootics of yellow fever in Venezuela (2004-2005): an emerging zoonotic disease. Ann N Y Acad Sci 2006, 1081, 57–60. [Google Scholar] [CrossRef]
- Rodriguez-Morales, A.J.; Torres-Hernández, D.; Guevara, M.E.; Chang-Cojulun, A.; Brea-Del Castillo, J.; Rios-Blanco, R.; Mérida-Barrios, M.I.; Palmieri, M.; Avila-Agüero, M.L. Yellow fever in children and adolescents amid the South American Outbreak, 2024/2025. New Microbes and New Infections 2025, 101635. [Google Scholar] [CrossRef]
- Baba, M.M.; Ikusemoran, M. Is the absence or intermittent YF vaccination the major contributor to its persistent outbreaks in eastern Africa? Biochem Biophys Res Commun 2017, 492, 548–557. [Google Scholar] [CrossRef]
- Gianchecchi, E.; Cianchi, V.; Torelli, A.; Montomoli, E. Yellow Fever: Origin, Epidemiology, Preventive Strategies and Future Prospects. Vaccines (Basel) 2022, 10, 372. [Google Scholar] [CrossRef]
- Paniz-Mondolfi, A.E.; Rodriguez-Morales, A.J.; Blohm, G.; Marquez, M.; Villamil-Gomez, W.E. ChikDenMaZika Syndrome: the challenge of diagnosing arboviral infections in the midst of concurrent epidemics. Ann Clin Microbiol Antimicrob 2016, 15, 42. [Google Scholar] [CrossRef]
- Srivastava, S.; Sah, R.; Babu, M.R.; Sharma, D.; Sharma, D.; Kumar, S.; Sridhar, S.B.; Wadhwa, T.; Shareef, J.; Rao, G. , et al. The emergence of oropouche fever: A potential new threat? New Microbes New Infect 2025, 65, 101596. [Google Scholar] [CrossRef]
- Giugni, F.R.; Aiello, V.D.; Faria, C.S.; Pour, S.Z.; Cunha, M.D.P.; Giugni, M.V.; Pinesi, H.T.; Ledesma, F.L.; Morais, C.E.; Ho, Y.L. , et al. Understanding yellow fever-associated myocardial injury: an autopsy study. EBioMedicine 2023, 96, 104810. [Google Scholar] [CrossRef]
- Villamil-Gómez, W. Protocolo diagnóstico del síndrome febril con afectación hematológica en áreas geográficas de riesgo endémico de infecciones tropicales. Medicine - Programa de Formación Médica Continuada Acreditado 2022, 13, 3445–3454. [Google Scholar] [CrossRef]
- Carrillo-Hernández, M.Y.; Ruiz-Saenz, J.; Villamizar, L.J.; Gómez-Rangel, S.Y.; Martínez-Gutierrez, M. Co-circulation and simultaneous co-infection of dengue, chikungunya, and zika viruses in patients with febrile syndrome at the Colombian-Venezuelan border. BMC Infect Dis 2018, 18, 61. [Google Scholar] [CrossRef]
- Castellanos, J.E.; Jaimes, N.; Coronel-Ruiza, C.; Rojas, J.P.; Mejía, L.F.; Villarreal, V.H.; Maya, L.E.; Claros, L.M.; Orjuela, C.; Calvo, E. , et al. Dengue-chikungunya coinfection outbreak in children from Cali, Colombia in 2018-2019. Int J Infect Dis 2021, 102, 97–102. [Google Scholar] [CrossRef]
- Villamil-Gómez, W.E.; Rodríguez-Morales, A.J.; Uribe-García, A.M.; González-Arismendy, E.; Castellanos, J.E.; Calvo, E.P.; Álvarez-Mon, M.; Musso, D. Zika, dengue, and chikungunya co-infection in a pregnant woman from Colombia. Int J Infect Dis 2016, 51, 135–138. [Google Scholar] [CrossRef]
- Cardona-Ospina, J.A.; Jiménez-Canizales, C.E.; Vásquez-Serna, H.; Garzón-Ramírez, J.A.; Alarcón-Robayo, J.F.; Cerón-Pineda, J.A.; Rodríguez-Morales, A.J. Fatal Dengue, Chikungunya and Leptospirosis: The Importance of Assessing Co-infections in Febrile Patients in Tropical Areas. Trop Med Infect Dis 2018, 3, 123. [Google Scholar] [CrossRef]
- Rodríguez-Morales, A.J.; Paniz-Mondolfi, A.E. Venezuela's failure in malaria control. Lancet 2014, 384, 663–664. [Google Scholar] [CrossRef]
- Ortiz-Martínez, Y.; Cabeza-Ruiz, L.D.; Henao-Martínez, A.F.; Rodriguez-Morales, A.J. Clinical challenges of managing advanced AIDS in the tropics: Histoplasmosis, COVID-19, and shigellosis coinfections. New Microbes New Infect 2022, 49-50, 101015. [Google Scholar] [CrossRef]
- Bani Hani, H.; Ibrahim, S.; Esmail, M.; Waleed, S.; Gouher, S. Dengue Fever Complicated by Pneumonia in Pregnancy: A Case Report. Cureus 2024, 16, e73608. [Google Scholar] [CrossRef]
- Frassetto, F.P.; Rosemberg, S. Neuropathology of yellow fever autopsy cases. Tropical Diseases, Travel Medicine and Vaccines 2023, 9, 1. [Google Scholar] [CrossRef]
- Schnyder, J.L.; Bache, B.E.; Welkers, M.R.A.; Spijker, R.; Schaumburg, F.; Goorhuis, A.; Grobusch, M.P.; de Jong, H.K. Yellow fever breakthrough infections after yellow fever vaccination: a systematic review and meta-analysis. Lancet Microbe 2024, 5, 100937. [Google Scholar] [CrossRef]
- Wilder-Smith, A. Yellow Fever in Travelers. Curr Infect Dis Rep 2019, 21, 42. [Google Scholar] [CrossRef]
- de Ávila, R.E.; José Fernandes, H.; Barbosa, G.M.; Araújo, A.L.; Gomes, T.C.C.; Barros, T.G.; Moreira, R.L.F.; Silva, G.L.C.; de Oliveira, N.R. Clinical profiles and factors associated with mortality in adults with yellow fever admitted to an intensive care unit in Minas Gerais, Brazil. Int J Infect Dis 2020, 93, 90–97. [Google Scholar] [CrossRef]
Figure 1.
Geographical origin of the included yellow fever cases.
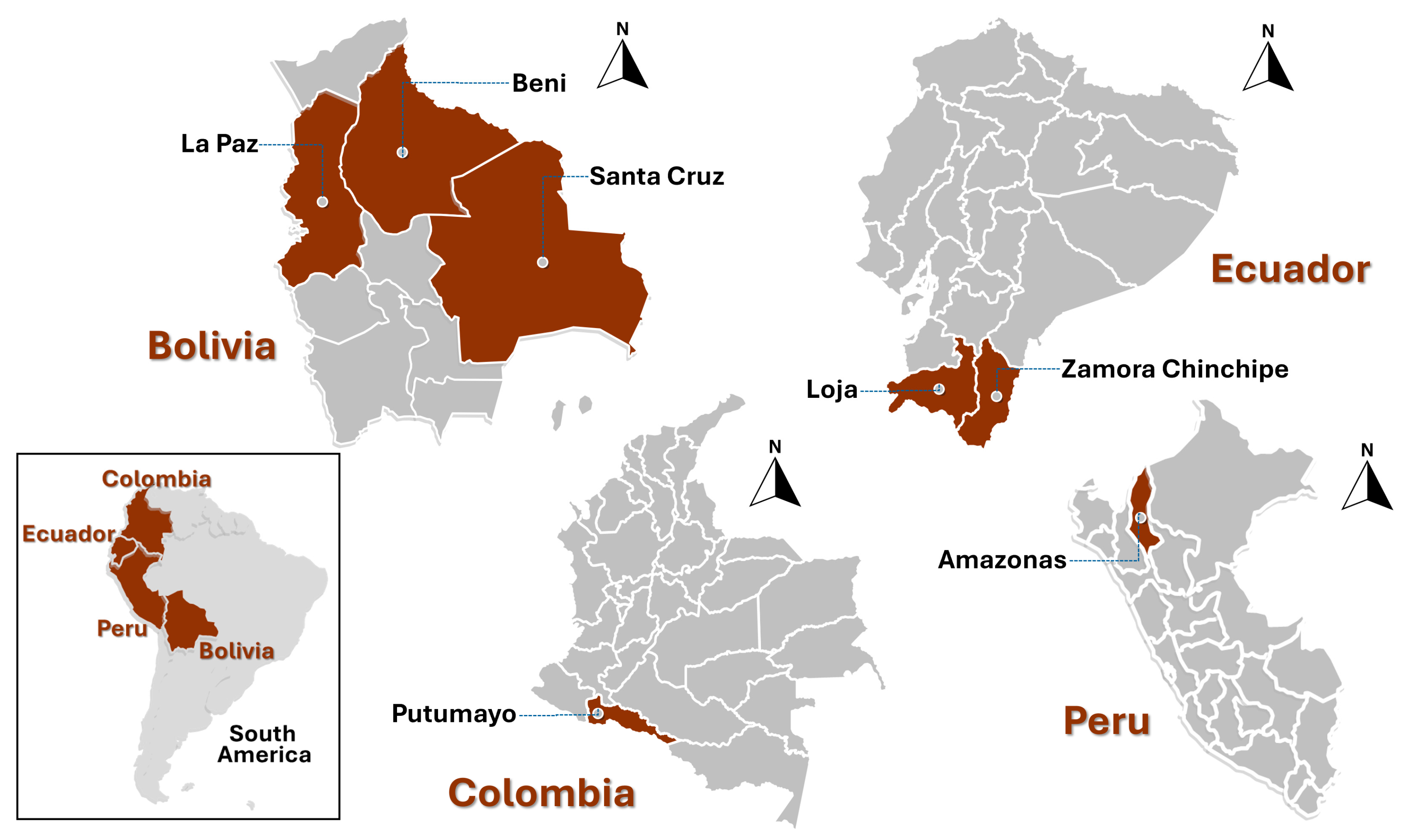

Table 1.
Epidemiological and demographic summary of variables for yellow fever cases from Colombia, Bolivia, Ecuador, and Peru (n = 21).
Table 1.
Epidemiological and demographic summary of variables for yellow fever cases from Colombia, Bolivia, Ecuador, and Peru (n = 21).
| Variable | n / Median | % / IQR |
|---|---|---|
| Year | ||
| 2025 | 17 | 81 |
| 2023/2024 | 4 | 19 |
| Country | ||
| Bolivia (Santa Cruz, La Paz, and Beni) | 8 | 38 |
| Ecuador (Loja and Zamora Chinchipe) | 5 | 24 |
| Colombia (Putumayo) | 4 | 19 |
| Peru (Amazonas) | 4 | 19 |
| Age (years) | 25 | 16-43 |
| <20 years | 6 | 29 |
| 20-59 years | 13 | 62 |
| ≥60 years | 2 | 9 |
| Sex | ||
| Male | 17 | 81 |
| Female | 4 | 19 |
| Occupation | ||
| Students | 5 | 24 |
| Agricultural worker | 3 | 14 |
| Construction worker | 2 | 10 |
| Mining worker | 1 | 5 |
| Other occupations/unknown | 10 | 48 |
| Vaccination against YFV (status) | ||
| Unknown or none | 18 | 86 |
| Apparently vaccinated | 3 | 14 |
| Days between symptom onset and consultation and hospitalization | 5 | 4-6 |
| Outcome | ||
| Died | 12 | 57 |
| Survived | 9 | 43 |
| Days from symptoms onset to death | 8 | 6-9 |
IQR, Interquartile range. YFV, yellow fever virus.
Table 2.
Clinical Features of Yellow Fever Cases.
| Finding | n | % |
|---|---|---|
| Main Initial Clinical Findings (Early Stage) | ||
| Fever | 15 | 71 |
| Arthralgia | 4 | 19 |
| Headache | 4 | 19 |
| Myalgia | 4 | 19 |
| Vomiting | 1 | 5 |
| Severe Findings (Toxic Phase) | ||
| Bleeding | 18 | 86 |
| Jaundice | 13 | 62 |
| Circulatory Collapse | 12 | 57 |
| Hepatic Dysfunction | 11 | 52 |
| Encephalopathy | 8 | 38 |
| Renal Failure | 5 | 24 |
| High Transaminases | 4 | 19 |
| Coagulopathy | 3 | 14 |
| Thrombocytopenia | 2 | 10 |
| Hyperbilirubinemia | 2 | 10 |
| Azotemia | 1 | 5 |
| Coma | 1 | 5 |
| Complications | ||
| Severe Coagulation Disorder | 3 | 14 |
| Pleural Effusion | 2 | 10 |
| Acute Kidney Injury | 2 | 10 |
| Anemia | 2 | 10 |
| Intracranial Hemorrhage | 2 | 10 |
| Multiorgan Dysfunction | 2 | 10 |
| Hypokalemia | 1 | 5 |
| Pancytopenia | 1 | 5 |
| Pneumonia | 1 | 5 |
| Shock | 1 | 5 |
| Bilateral Nephromegaly | 1 | 5 |
| Cerebral Anoxia | 1 | 5 |
| Edema | 1 | 5 |
| ESβL Klebsiella pneumoniae pneumonia | 1 | 5 |
| ESβL Escherichia coli sepsis | 1 | 5 |
ESβL, Extended spectrum beta lactamase.
Table 3.
Laboratory findings of the yellow fever cases.
| Laboratory Variable | n | Median | IQR | Reference Values (RV) | % <RV | % >RV | |
|---|---|---|---|---|---|---|---|
| pH | 5 | 7.3 | 7.28 | 7.41 | 7.35–7.45 | 60 | 0 |
| HCO3- (mmol/L) | 5 | 19.6 | 13.2 | 26.2 | 21–28 | 60 | 0 |
| Anion Gap (mmol/L) | 5 | 15.2 | 14.9 | 21.9 | 8–16 | 0 | 40 |
| Lactate (mmol/L) | 3 | 13.1 | 12.7 | 13.55 | 0.7–2.5 | 0 | 100 |
| Glucose (mg/dL) | 5 | 49 | 46 | 63 | 70-110 | 80 | 20 |
| Urea (mg/dL) | 3 | 124 | 106.9 | 127.85 | 15–45 | 0 | 100 |
| Creatinine (mg/dL) | 6 | 2.885 | 1.3 | 6.44 | 0.7–1.3 | 0 | 67 |
| Bilirubin total (mg/dL) | 11 | 6.68 | 5.19 | 7.85 | <1.2 | 100 | |
| Bilirubin direct (mg/dL) | 9 | 6.41 | 3.92 | 6.7 | <0.3 | 100 | |
| Bilirubin indirect (mg/dL) | 9 | 1.21 | 0.93 | 1.62 | <1.0 | 33 | |
| AST (U/L) | 11 | 3257 | 1230.5 | 11468.5 | <40 | 100 | |
| ALT (U/L) | 10 | 1570.5 | 726.25 | 4101 | <40 | 100 | |
| Alkaline phosphatase (U/L) | 3 | 154 | 150 | 227.5 | <120 | 67 | |
| GGT (U/L) | 2 | 290.5 | 254.25 | 326.75 | <60 | 100 | |
| Proteins total (g/dL) | 2 | 4.11 | 4.105 | 4.115 | 6.4–8.3 | 100 | 0 |
| Albumin (g/dL) | 4 | 2.465 | 2.1925 | 3.295 | 3.5–5.0 | 75 | 25 |
| Globulin (g/dL) | 2 | 1.95 | 1.925 | 1.975 | 2.3–3.4 | 100 | 0 |
| TP (s) | 12 | 22.8 | 15.125 | 33.45 | 11–14 | 8 | 75 |
| INR | 6 | 1.25 | 1.135 | 2.2425 | 0.9–1.2 | 0 | 50 |
| TTP/TTPA (s) | 11 | 43 | 34.65 | 63.25 | <35 | 27 | |
| Fibrinogen (mg/dL) | 4 | 142 | 119 | 203.5 | 15–20 | 75 | 0 |
| Hemoglobin (g/dL) | 13 | 13.6 | 10.4 | 14.5 | 200–400 | 46 | 8 |
| Hematocrit (%) | 13 | 36 | 25.65 | 41 | ♂13.5–17.5; ♀12–16 | 46 | 0 |
| Leukocytes (x103/µL) | 13 | 5.8 | 3.5 | 7.1 | 35–49 | 38 | 8 |
| Platelets (x103/µL) | 13 | 74 | 62 | 131 | 4–11 | 77 | 8 |
| Procalcitonin (ng/mL) | 4 | 4.96 | 1.5025 | 8.5125 | 150–400 | 25 | 0 |
| CRP (mg/L) | 3 | 5.75 | 4.065 | 50.875 | <0.5 | 33 | |
| LDH (U/L) | 2 | 2580.5 | 1439.75 | 3721.25 | <5 | 100 | |
| CPK total (U/L) | 2 | 797.25 | 694.475 | 900.025 | <250 | 100 | |
| CPK-MB (U/L) | 1 | 10 | 26–162 | ||||
| Troponin I (ng/mL) | 1 | 0.1 | 0–25 | ||||
| D-dimer (µg/mL) | 1 | 3.65 | 0.12–0.60 | ||||
| YFV RT-PCR Ct | 4 | 23.45 | 22.6 | 24.6 | <0.55 | 0 | 0 |
| n | Positive | Negative | %+ | %- | |||
| YFV RT-PCR | 19 | 18 | 1 | 95 | 5 | ||
| IgM for YFY | 7 | 7 | 0 | 100 | 0 | ||
| YFY RT-PCR/IgM | 5 | 4 | 1 | 80 | 0 | ||
| NS1 for DENV | 1 | 0 | 1 | 0 | 100 | ||
| IgM for DENV | 1 | 1 | 0 | 100 | 0 | ||
pH, potential of hydrogen. HCO3-, bicarbonate. AST, aspartate aminotransferase. ALT, alanine aminotransferase. GGT, gamma-glutamyl transferase. TP, prothrombin time. INR, international normalized ratio. TTP/TTPA, activated partial thromboplastin time. CRP, C-reactive protein. LDH, lactate dehydrogenase. CPK total, creatine phosphokinase total. CPK-MB, creatine phosphokinase MB isoenzyme. YFV RT-PCR Ct, Yellow Fever Virus reverse transcription polymerase chain reaction cycle threshold. IgM for YFY, Enzyme-Linked ImmunoSorbent Assay (ELISA) for Immunoglobulin M (IgM) against YFY. NS1 for DENV, Dengue virus non-structural protein 1 antigen test. IgM for DENV, ELISA for IgM against DENV. % <RV, proportion below reference values. % >RV, proportion above reference values.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



