
Submitted:
31 May 2024
Posted:
04 June 2024
You are already at the latest version
Abstract
Mpox, formerly known as Monkeypox, is a rare viral disease initially discovered in Africa in 1958. Since its first identification, several outbreaks have occurred in various African nations. Recently, the global community has witnessed a resurgence in the number of Mpox cases reported worldwide, prompting the World Health Organization (WHO) to declare the ongoing multi-country outbreak a public health emergency in July 2022. This study reports on the first cases of Mpox detected in Khartoum State, Sudan, outlining the epidemiology, preparedness, and public health response to this new challenge. A total of 55 suspected cases were identified, with two confirmed cases. The clinical manifestations observed in these cases align with the classic skin rash typical of Mpox, presenting alongside symptoms like fever, headache, and joint pain. The findings underscore the need for heightened surveillance, early detection, and timely intervention to prevent the domestic spread of Mpox and its potential impact on public health. Continued global efforts are needed to support effective screening, diagnostic, and control measures, ultimately enhancing preparedness and response in the face of this emerging disease.
Keywords:
Mpox
; Outbreak
; Pandemic Preparedness and Response
; global health emergency of international concern
; epidemiology
; Zoonoses
; One Health
; Global Health Security
1. Introduction
Mpox virus (MPXV) is a zoonotic virus that belongs to the Poxviridae family and it is similar to the Variola and Vaccinia viruses and it was first isolated in 1958 in lab monkeys [1]. There are two strains of the virus, clade I and clade II, with clade I causing more severe disease in humans [2]. In the 1970s, an outbreak occurred in the Central African Republic and the Democratic Republic of the Congo, primarily affecting people who had contact with animals. In the 1980s, the virus started spreading from human-to-human in Africa [2,3].
The first outbreak outside of Africa happened in the United States in 2003 and was traced back to infected rodents imported from Ghana [4,5]. Since then, Mpox infections have been detected in travellers coming from Nigeria to various countries including Israel, Singapore, the USA, and Italy [4,5].
The virus is believed to spread from wild animals to humans primarily, therefore, factors such as deforestation, land-use changes, and political instability contribute to increasing the risk of spillover of Mpox and other zoonotic diseases [6]. Transmission between infected animals and humans occurs through direct contact with skin, mucosae, and contaminated materials. Human-to-human transmission can occur through contact with lesions, body fluids, respiratory droplets, and potentially through sexual intercourse [6]. Investigating the recent global outbreak of Mpox revealed a high transmission rate of the virus among men having sex with men [5,6].
The clinical symptoms associated with Mpox encompass fever, headaches, muscle aches, lymphadenopathy, and distinctive skin eruptions. The progression of the rash typically transitions from macules to papules, vesicles, pustules, and eventually crusts. This skin manifestation predominantly appears on the face, extremities, and can extend to areas like mucous membranes, genitalia, and the eyes [7]. Mpox has a fatality rate spanning from Zero to 11%, with notably higher rates observed in children and individuals with underlying health conditions. Complications arising from Mpox can include secondary infections, pneumonia, sepsis, encephalitis, and even vision impairment [7]. Vigilant monitoring and timely intervention are crucial in managing these severe outcomes associated with Mpox infections.
There are currently no licensed treatments for Mpox, but vaccines against Smallpox can provide some protection [8]. The global risk of transmission has increased since Smallpox eradication and the cessation of vaccination campaigns [8]. Diagnosing Mpox infection involves using a real-time PCR (RT-PCR) testing of swab specimens, and other laboratory tests may be useful for distinguishing it from other similarly skin manifesting infections. Additional diagnostic investigations such as laboratory tests, dermoscopic observation, and biopsy may be performed to exclude other pox-like diseases [5]. Therefore, a comprehensive diagnostic approach involving a combination of tests enhances the precision of the diagnosis and facilitates appropriate management strategies for individuals affected by Mpox.
In response to the rapidly escalating situation of Mpox worldwide, on the 23rd of July 2022, the WHO declared the escalating global outbreak of Mpox a Public Health Emergency of International Concern (PHEIC) [9]. Accordingly, Human and Animal health authorities led by Ministries of Health worldwide including Sudan were urged to initiate a national Preparedness and Response strategic plan. This global spread of Mpox outbreak at an alarming rate has challenged health systems worldwide, including Sudan, before they recover from the impact of COVID-19 pandemic [10,11,12]. The main challenge was the operationalization of One Health strategy [13], including the development and implementation of pandemic preparedness, prevention, and response (PPPR) framework that prioritize preparedness and prevention [14]. This is particularly crucially urgent in countries like Sudan that are endemic with a wide range of zoonotic pandemic-prone diseases such as Chikungunya [15], Crimean-Congo haemorrhagic fever (CCHF) [16], dengue [17], Yellow fever [18], Rift Valley fever [19], Zika and other arboviruses [20], as well as hepatitis viruses [21], and several bacterial [22], fungal [23,24], and parasitic infections [25,26,27,28]. Furthermore, in Sudan, this challenge is exacerbated by additional factors including the local limited diagnostic capacity, prevalent co-infections, and unusual clinical presentation of diseases [22,29,30,31,32,33,34].
Therefore, in this communication, we describe the Preparedness and Response strategic plan, investigation, and response for Mpox outbreak in the capital of Sudan, Khartoum state, in 2022-2023.
2. Materials and Methods
In this communication, we describe the preparedness and response to the Mpox outbreak in Khartoum State, Sudan in 2022 and 2023.
- The development of pandemic preparedness and response (PPR) action plan:
Khartoum state’s Ministry of Health has engaged stakeholders of human and animal health to develop a pandemic preparedness and response (PPR) action plan. This PPR action plan focused on enhancing the coordination between human and animal health stakeholders including community engagement through tailored risk communication to support the implementation of active surveillance, case finding and management (Table 1). Also, it included strengthening the surveillance and response system and mobilizing resources to build the capacity of the national reference laboratory “National Public Health Laboratory” for a robust diagnosis and investigation of suspected cases. Additional pillars of the PPR focused on improving the case management as well as enforcing the implementation of infection prevention and control (IPC) measures in healthcare facilities and among the response teams, and healthcare providers in general (Table 1).
- Establishing an active surveillance system:
Recognizing the urgency, a federal task force has been formed in Sudan to establish active surveillance measures that can identify, isolate, and provide healthcare to suspected and confirmed cases of Mpox (Table 1). The primary aim of this task force is to assist in containing the spread of the virus and to mitigate the impact of the outbreak on the healthcare system in Khartoum State, Sudan.
- Identifying suspected cases:
In order to identify suspected cases, individuals were assessed based on their presenting symptoms and/or relevant epidemiological history, such as recent travel to countries reported the outbreak or close contact with confirmed or suspected cases.
- Samples collection:
After identifying suspected cases, samples were collected from the blister fluid using a swab. These samples were then preserved in a viral transport medium (VTM) and transported to a laboratory in compliance with WHO guidelines.
- Viral DNA extraction:
Total DNA was extracted using the QIAamp Viral DNA Mini Kit (Qiagen, Düsseldorf, Germany) according to the manufacturer's guidelines.
- Laboratory investigations:
Molecular analyses were carried out at the National Public Health Laboratory (NPHL) in Khartoum, where samples from suspected cases were examined using MPXV-specific real-time PCR according to the manufacturer's instructions (LightMix Modular Monkeypox Virus, TIB Molbiol, Berlin, Germany).
3. Results
- Identification of suspected cases:
Between May 3rd and 2nd of November 2022, cases suspected of Mpox were emerging in Khartoum State. Accordingly, we initiated an active case-finding surveillance to identify these cases, associated risk factors, and collect samples for laboratory confirmation (Figure 1).
We identified 55 suspected cases across Khartoum State with 31% were scattered in the central part of Khartoum; 16.3% were in Jabal Awliya which is located in south Khartoum; 14.5% were in Omdurman and a similar per cent were in Sharg El Nile (Table 2). Demographics of the suspected cases showed that males comprised 69% whereas females comprised 31% of them representing a 2:1 female-male ratio.
- Clinical presentations of suspected cases:
All suspected cases (100%) presented with skin rash and 78% displayed fever. Headache, sore throat, lymphadenopathy, joint pain, and back pain was experienced by 47%, 45%, 45%, 13%, and 11%, respectively (Figure 2)
- Characteristics and disease outcome among confirmed cases:
Among the 55 suspected individuals of Mpox, only two cases were laboratory-confirmed positive using RT-PCR. The first case was a 34-year-old male residing in the East Nile locality who developed symptoms, including skin rash, fever, cough, headache, and joint pain, on 7 September 2022. The patient was admitted to the Dermatology Hospital in Khartoum on 17 September 2022. According to medical history, the lesions appeared on 12 September 2022.. Blood investigations showed a white blood count (WBC) of 8.7 × 109/L, haemoglobin (Hb) level of 15.4 g/dL, and platelet count of 336 × 103/L. Viral screening for human immunodeficiency virus (HIV), Hepatitis B and C (HBV, HCV) was negative. The patient had no travel history during the last 2 months nor his family members. However, the patient was a co-patient of his father who was suffering from cardiac disease at Royal Care Hospital on the 29th of August 2022. During the father’s hospitalization period, a skin rash appeared on the father but the dermatologist diagnosed it as scabies. Upon diagnosis for the father by the rapid response team, the father was negative for Mpox. Based on animal contact history, the patient had a history of animal contact in the house; goats. The human contact history of the patient was mainly with family members, and all did not develop any symptoms or signs of Mpox. During the Mpox manifestation period the patient was home-isolated and under follow-up by RRT for 21 days.
The second case was a two-year-old child suffering from autoimmune and nervous system disorder presented with fever (temperature 38°C) and skin eruption that started on 14 September 2022. The patient was admitted to Elbulk Children’s Hospital on 19 September 2022. The skin eruption consisted of two types of lesions: maculopapular pustules on an erythematous base and scattered faint erythematous macules. The child also had bilateral conjunctivitis, but no swollen lymph nodes or mucosal lesions were observed. The child's mother reported no history of travel. However, the father works as a truck driver in the Outskirt market in Omdurman where all vehicles come from the Darfur States. Also, it is worth noting that the housing conditions were not ideal, with animals, particularly cats and rodents were present within the house.
During clinical examination, the child's vital signs were normal and no signs of lymphadenopathy. The papular lesions were widespread throughout the body, with a higher concentration on the face, neck, extremities, and trunk (Figure 3). Laboratory tests were all within the normal values; complete blood count examinations reported normal total white blood cell count (WBCs) of 9.0 × 103, Hb level; 14.1 g/dL, and platelet count of 355 × 103/L. Viral screening for HIV, HBV, and HCV was negative. Consequently, Elbulk Children’s Hospital immediately notified the Ministry of Health of suspecting Mpox. RRT collected swab and skin scraping samples from the skin lesions and sent to the NPHL for molecular investigations. The patient’s family members including the mother and two brothers were screened for Mpox. One of the skin scraping samples of a maculopapular pustule from the patient's skin was positive for MPXV by RT-PCR. Herpes simplex virus (HSV-1 and HSV-2) was also investigated and was negative. Family members' samples were all negative for Mpox.
Following cases investigation and diagnosis in the NPHL, the positive samples were shipped for sequencing to confirm the circulating Mpox strain. Genomic sequencing revealed that the circulating strain of MPXV in Khartoum State belongs to clade I.

4. Discussion
This emergence of Mpox in the capital city of Sudan; Khartoum represents a serious threat to the public health in the country. This is mainly because Khartoum State hosts of nearly around 10 million individuals and it is featured with high human and animal mobility through national and international transportation and major animal markets. This high human mobility is indicated by around 2 million travellers getting and/or out of the State daily. Therefore, initiating a national Preparedness and Response strategic plan was aimed at early detection, prevention and control of the country-wide spread of the Mpox outbreak given the country's poorly structured and severely under-supported healthcare system and has not yet recovered from the COVID-19 pandemic [35]. The lack of resources and the increasing burden of other infectious diseases, including viral diseases [36,37,38,39], parasitic [33,40,41,42] and bacterial infections [43], could potentially exacerbate the situation. Despite these challenges, the prompt implementation of an integrated surveillance and response system has helped in the containment of the outbreak and prevented the further spread of Mpox highlighting the effectiveness of prompt response through quickly isolating the suspected cases and providing supportive treatment for confirmed cases [44,45].
The clinical presentations of suspected cases were consistent with the characteristic skin rash seen in Mpox [46,47,48,49] but also included other symptoms such as fever, headache, and joint pain, which suggested a broad range of clinical manifestations that may complicate diagnosis and treatment [46,47,48,49]. However, skin rash and fever are the most frequent combination of symptoms. These findings underscore the need for healthcare providers to maintain a high level of clinical suspicion and remain vigilant in their differential diagnosis and management of patients presenting to them with skin rashes and other Mpox-related symptoms [48,49]. Interestingly, in the recent MPXV global outbreak, there have been limited reports of cases in young children. This dearth of information makes it difficult to provide an accurate dermatologic description for this specific population group [50,51]. However, in our second confirmed case, Mpox rash typically manifests as papular pustules on an erythematous base and scattered faint erythematous macules resembling mosquito bites. Additionally, it is worth noting that the skin rash is generally the first visible sign of MPXV infection and is rarely reported in children [52]. Therefore, detailed descriptions of MPXV rash in children are limited, this underscores the limited attention to child care and urges improving the healthcare for children [53]. Furthermore, in this particular case, the child also exhibited bilateral conjunctivitis, which is a less common finding in MPXV but can still occur [54]. The differential diagnosis for a rash with papular pustules on an erythematous base and scattered erythematous macules in children may include insect bites; Varicella-Zoster Virus (Chickenpox); impetigo; Molluscum Contagiosum; scabies, drug eruption and contact dermatitis [55,56,57].
In this study, we attempted to investigate the source of MPXV, however, this was not successful due to several limitations including limited awareness among the healthcare providers about the disease, poor diagnostic capacity, and that the country is endemic with several diseases that have similar skin manifestations [22,25]. Additionally, the lack of comprehensive monitoring of cross-border movements and poor self-reporting of travel history challenges the contact tracing system. Therefore, only 55 suspected cases were identified and tested. This highlights the need for strengthening surveillance, particularly at points of entry (POE) including Khartoum airport, ground routes, and river transportation ports [58,59]. Rigorous and extensive public health measures, such as isolating the suspected cases, contact tracing, and tracing potential infected animal hosts need to be improved to prevent other pandemics and public health emergencies. It is also crucial to educate the community about the disease, its mode of transmission, and preventive measures such as avoiding contact with infected animals or animal products and practicing good personal hygiene, and the need to seek healthcare at the onset of disease or potential exposure [60].
Countries with low social demographic index (SDI) should invest in improving sanitation, hygiene, and living conditions as a core part of the pandemic preparedness, prevention, and response [12]. This was more obvious in the second case which was categorized as having low SDI, and thus increased the risk of Mpox in children which is considered rarely occurring [52]. Therefore, the integration of community health promotion is extremely important especially in low SDI communities to educate the communities about the disease and more importantly to remove disease-related stigma [61]. Diseases such as Mpox or other sexually transmitted diseases like HIV, HSV, and Human Papilloma virus (HPV) develop a stigma in many communities since they are linked to certain groups of people [61,62,63]. Mpox’s sexual transmission poses significant challenges in containment and prevention efforts, as it thrives in environments of close human interaction. The consequences of Mpox transmission extend beyond the physical realm, impacting emotional well-being and social dynamics. Patients with Mpox develop the stigma of being socially disapproved and not accepted due to this condition, which leads them to not disclose their medical condition to avoid isolation and hospital admission, and eventually increases disease spread and difficulty in prevention and control. Therefore, the importance of education and safe practices becomes paramount in curbing its spread. [64].
Management of Mpox includes supportive care, such as maintaining hydration and treating symptoms like fever and pain. In severe cases, hospitalization may be required [65]. Although there is no specific antiviral treatment for Mpox, the smallpox vaccine (vaccinia virus) can provide immunity against the virus and reduce the severity of the disease [66]. However, disease severity depends on many associated factors including the MPXV strain and dose, and patient's immune status and existing of other co-infections such as HIV, chlamydia, gonorrhoea, and syphilis [67].
The association of MPXV strain with disease severity has been described previously. MPXV Clade I is associated with a higher mortality compared to Clade IIa and IIb. However, in the 2022 Mpox pandemic, genomic studies were able to determine that MPXV clade IIb was the strain responsible for Mpox outside the African continent [68,69,70]. In this study, genomic sequencing confirmed that the locally circulating strain of MPXV belongs to clade I. Therefore, the epidemiological implications of Mpox clade I in this outbreak are significant and warrant more prompt actions to prevent the disease progression. This also highlights the need for swift genomic investigations, strain characterization and timely reporting to support public health and healthcare providers and prioritize interventions and resource reallocation. It’s also evident that both human and animal surveillance and diagnostic capacities must be enhanced to understand the burden of the Mpox outbreak and determine local reservoirs [71]
Although climate change and conflicts are pivotal in infectious disease spread, climate change also drives for spillover of zoonotic diseases [72,73,74,75]. According to the last joint external evaluation of the International Health Regulations (IHRs-2005) core capacities conducted in Sudan in 2016, low performance in various IHRs-2005 pillars including surveillance system, preparedness, laboratory system, zoonotic diseases, workforce and risk communication, and emergency response operation [76]. Taking into consideration, the evolving situation and the ongoing conflict since the evaluation was conducted, a high number of human displacements was reported with potential emerging and re-emergence of Mpox and other infectious diseases [77,78,79,80]. Therefore, the Sudan Ministry of Health and other health partners must be vigilant in disease monitoring and detection to prevent any potential outbreaks. The need for additional resources and attention cannot be overlooked, and coordination and communication between healthcare personnel, international health organizations, and local communities are essential in addressing this situation to successfully implement a transdisciplinary One Health strategy that is based on practical and cost-effective framework for the Pandemic Preparedness, Prevention, and Response.
5. Conclusions
In summary, the findings of this study call for heightened surveillance, early detection, and timely intervention to prevent the domestic spread of Mpox and its potential impact on public health. Continued global efforts are needed to support the implementation of effective screening, diagnostic, and control measures, ultimately enhancing preparedness and response in the face of this emerging disease and other future threatening pandemics.
Author Contributions
Y.A., E.E.S. and A.A. conceived and designed the study. Y.A. and A.A. were responsible for study implementation. Y.A. and A.A. were responsible for the formal analysis and interpretation of data. Y.A., E.E.S., N.S.M., A.M., and A.A. were responsible for writing the original draft. Y.A., E.E.S., N.S.M., A.M., and A.A. were responsible for the review and editing of the article. All authors have read and agreed to the published version of the article.
Funding
None.
Institutional Review Board Statement
This study has been approved by the Federal Ministry of Health, Khartoum, Republic of Sudan Research Ethics Committee.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Acknowledgements
We would like to thank our colleagues in the Sudan Federal Ministry of Health, along with our colleagues in the WHO country office, for providing invaluable technical and logistic support, and we would like to express our gratitude towards all who helped in this work.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Giulio, D.B.D.; Eckburg, P.B. Human Monkeypox: An Emerging Zoonosis. Lancet Infect. Dis. 2004, 4, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Jezek, Z.; Szczeniowski, M.; Paluku, K.M.; Mutombo, M.; Grab, B. Human Monkeypox: Confusion with Chickenpox. Acta Trop. 1988, 45, 297–307. [Google Scholar] [PubMed]
- Proietti, I.; Santoro, P.E.; Skroza, N.; Tieghi, T.; Bernardini, N.; Tolino, E.; Dybala, A.E.; Di Guardo, A.; Rallo, A.; Di Fraia, M. A Case Report of Monkeypox in an Adult Patient from Italy: Clinical and Dermoscopic Manifestations, Diagnosis and Management. Vaccines 2022, 10, 1903. [Google Scholar] [CrossRef] [PubMed]
- Breman, J.G.; Henderson, D.A. Poxvirus Dilemmas—Monkeypox, Smallpox, and Biologic Terrorism; Mass Medical Soc, 1998; Vol. 339, pp. 556–559; ISBN 0028-4793.
- Mileto, D.; Riva, A.; Cutrera, M.; Moschese, D.; Mancon, A.; Meroni, L.; Giacomelli, A.; Bestetti, G.; Rizzardini, G.; Gismondo, M.R.; et al. New Challenges in Human Monkeypox Outside Africa: A Review and Case Report from Italy. Travel Med. Infect. Dis. 2022, 49, 102386. [Google Scholar] [CrossRef]
- Antinori, A.; Mazzotta, V.; Vita, S.; Carletti, F.; Tacconi, D.; Lapini, L.E.; D’Abramo, A.; Cicalini, S.; Lapa, D.; Pittalis, S. Epidemiological, Clinical and Virological Characteristics of Four Cases of Monkeypox Support Transmission through Sexual Contact, Italy, May 2022. Eurosurveillance 2022, 27, 2200421. [Google Scholar] [CrossRef]
- Tarín-Vicente, E.J.; Alemany, A.; Agud-Dios, M.; Ubals, M.; Suñer, C.; Antón, A.; Arando, M.; Arroyo-Andrés, J.; Calderón-Lozano, L.; Casañ, C. Clinical Presentation and Virological Assessment of Confirmed Human Monkeypox Virus Cases in Spain: A Prospective Observational Cohort Study. The Lancet 2022, 400, 661–669. [Google Scholar] [CrossRef]
- Parrino, J.; Graham, B.S. Smallpox Vaccines: Past, Present, and Future. J. Allergy Clin. Immunol. 2006, 118, 1320–1326. [Google Scholar] [CrossRef] [PubMed]
- Zarocostas, J. Monkeypox PHEIC Decision Hoped to Spur the World to Act. The Lancet 2022, 400, 347. [Google Scholar] [CrossRef] [PubMed]
- El-Sadig, S.M.; Mohamed, N.S.; Ahmed, E.S.; Alayeib, M.A.; Tahir, L.H.; Edris, A.M.M.; Ali, Y.; Siddig, E.E.; Ahmed, A. Obstacles Faced by Healthcare Providers during COVID-19 Pandemic in Sudan. J. Infect. Dev. Ctries. 2021, 15, 1615–1617. [Google Scholar] [CrossRef]
- Ahmed, A.; Mohamed, N.S.; EL-Sadig, S.M.; Fahal, L.A.; Abelrahim, Z.B.; Ahmed, E.S.; Siddig, E.E. COVID-19 in Sudan. J. Infect. Dev. Ctries. 2021, 15, 204–208. [Google Scholar] [CrossRef]
- Ruppel, A.; Halim, M.I.; Kikon, R.; Mohamed, N.S.; Saebipour, M.R. Could COVID-19 Be Contained in Poor Populations by Herd Immunity Rather than by Strategies Designed for Affluent Societies or Potential Vaccine (s)? Glob. Health Action 2021, 14, 1863129. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Mahmoud, I.; Eldigail, M.; Elhassan, R.M.; Weaver, S.C. The Emergence of Rift Valley Fever in Gedaref State Urges the Need for a Cross-Border One Health Strategy and Enforcement of the International Health Regulations. Pathogens 2021, 10, 885. [Google Scholar] [CrossRef] [PubMed]
- Boyce, M.R.; Sorrell, E.M.; Standley, C.J. An Early Analysis of the World Bank’s Pandemic Fund: A New Fund for Pandemic Prevention, Preparedness and Response. BMJ Glob. Health 2023, 8, e011172. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Ali, Y.; Mohamed, N.S. Arboviral Diseases: The Emergence of a Major yet Ignored Public Health Threat in Africa. Lancet Planet. Health 2020, 4, e555. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Ali, Y.; Salim, B.; Dietrich, I.; Zinsstag, J. Epidemics of Crimean-Congo Hemorrhagic Fever (CCHF) in Sudan between 2010 and 2020. Microorganisms 2022, 10, 928. [Google Scholar] [CrossRef] [PubMed]
- Elduma, A.H.; LaBeaud, A.D.; A. Plante, J.; Plante, K.S.; Ahmed, A. High Seroprevalence of Dengue Virus Infection in Sudan: Systematic Review and Meta-Analysis. Trop. Med. Infect. Dis. 2020, 5, 120. [CrossRef] [PubMed]
- Markoff, L. Yellow Fever Outbreak in Sudan. N. Engl. J. Med. 2013, 368, 689–691. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Ali, Y.; Elduma, A.; Eldigail, M.H.; Mhmoud, R.A.; Mohamed, N.S.; Ksiazek, T.G.; Dietrich, I.; Weaver, S.C. Unique Outbreak of Rift Valley Fever in Sudan, 2019. Emerg. Infect. Dis. 2020, 26, 3030–3033. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Dietrich, I.; LaBeaud, A.D.; Lindsay, S.W.; Musa, A.; Weaver, S.C. Risks and Challenges of Arboviral Diseases in Sudan: The Urgent Need for Actions. Viruses 2020, 12. [Google Scholar] [CrossRef]
- Ahmed, A.; Ali, Y.; Mohamed, N.S.; Zinsstag, J.; Siddig, E.E.; Khairy, A. Hepatitis E Virus Outbreak among Tigray War Refugees from Ethiopia, Sudan (Response). Emerg. Infect. Dis. 2023, 29, 460–461. [Google Scholar] [CrossRef]
- Ahmed, A.; Hagelnur, A.A.; Eltigani, H.F.; Siddig, E.E. Cutaneous Tuberculosis of the Foot Clinically Mimicking Mycetoma: A Case Report. Clin. Case Rep. 2023, 11, e7295. [Google Scholar] [CrossRef] [PubMed]
- Siddig, E. Fine Needle Aspiration: Past, Current Practice and Recent Developments. Biotech. Histochem. 2014, 89, 241–244. [Google Scholar] [CrossRef] [PubMed]
- Siddig, E.E.; Ahmed, A.; Ali, Y.; Bakhiet, S.M.; Mohamed, N.S.; Ahmed, E.S.; Fahal, A.H. Eumycetoma Medical Treatment: Past, Current Practice, Latest Advances and Perspectives. Microbiol. Res. 2021, 12, 899–906. [Google Scholar] [CrossRef]
- Mohamed, N.S.; Osman, H.A.; Muneer, M.S.; Samy, A.M.; Ahmed, A.; Mohammed, A.O.; Siddig, E.E.; Abdel Hamid, M.M.; Ali, M.S.; Omer, R.A.; et al. Identifying Asymptomatic Leishmania Infections in Non-Endemic Villages in Gedaref State, Sudan. BMC Res. Notes 2019, 12, 566. [Google Scholar] [CrossRef] [PubMed]
- Altahir, O.; AbdElbagi, H.; Abubakr, M.; Siddig, E.E.; Ahmed, A.; Mohamed, N.S. Blood Meal Profile and Positivity Rate with Malaria Parasites among Different Malaria Vectors in Sudan. Malar. J. 2022, 21, 124. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, N.S.; Ali, Y.; Muneer, M.S.; Siddig, E.E.; Sibley, C.H.; Ahmed, A. Malaria Epidemic in Humanitarian Crisis Settings the Case of South Kordofan State, Sudan. J. Infect. Dev. Ctries. 2021, 15, 168–171. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, N.S.; Abdelbagi, H.; Osman, H.A.; Ahmed, A.E.; Yousif, A.M.; Edris, Y.B.; Osman, E.Y.; Elsadig, A.R.; Siddig, E.E.; Mustafa, M. A Snapshot of Plasmodium Falciparum Malaria Drug Resistance Markers in Sudan: A Pilot Study. BMC Res. Notes 2020, 13, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Eldigail, M.; Elduma, A.; Breima, T.; Dietrich, I.; Ali, Y.; Weaver, S.C. First Report of Epidemic Dengue Fever and Malaria Co-Infections among Internally Displaced Persons in Humanitarian Camps of North Darfur, Sudan. Int. J. Infect. Dis. 2021, 108, 513–516. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; El-Amin, R.; Musa, A.M.; Elsayed, M.A.; Fahal, L.A.; Ahmed, E.S.; Ali, Y.; Nebie, I.E.; Mohamed, N.S.; Zinsstag, J.; et al. Guillain-Barre Syndrome Associated with COVID-19 Infection: A Case Series. Clin. Case Rep. 2023, 11, e6988. [Google Scholar] [CrossRef]
- Ali, Y.; Siddig, E.E.; Mohamed, N.; Ahmed, A. Rift Valley Fever and Malaria Co-infection: A Case Report. Clin. Case Rep. 2023, 11, e7926. [Google Scholar] [CrossRef]
- Abdallah, A.T.H.; Abdelkhalig, R.E.; Hamid, E.; Ahmed, A.; Siddig, E.E. Recurrent Abdominal Wall Mass in a Hepatitis B-positive Male: An Unusual Case of Lumbar Mycetoma. Clin. Case Rep. 2023, 11, e8275. [Google Scholar] [CrossRef] [PubMed]
- Siddig, E.E.; Ahmed, A. When Parasites Stray from the Path: A Curious Case of Ectopic Cutaneous Schistosoma Haematobium. QJM Int. J. Med. 2023, 116, 794–795. [Google Scholar] [CrossRef]
- Ahmed, A.; Hemaida, M.A.; Hagelnur, A.A.; Eltigani, H.F.; Siddig, E.E. Sudden Emergence and Spread of Cutaneous Larva Migrans in Sudan: A Case Series Calls for Urgent Actions. IDCases 2023, 32, e01789. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A. Urgent Call for a Global Enforcement of the Public Sharing of Health Emergencies Data: Lesson Learned from Serious Arboviral Disease Epidemics in Sudan. Int. Health 2020, 12, 238–240. [Google Scholar] [CrossRef]
- Hamad, M.N.; Mohamed, F.I.; Osman, M.M.; Jadid, A.A.; Abdalrhman, I.K.; Yousif, A.M.; Alabid, T.; Edris, A.M.M.; Mohamed, N.S.; Siddig, E.E. Molecular Detection of Epstein-Barr Virus among Sudanese Patients Diagnosed with Hashimoto’s Thyroiditis. 2023. [CrossRef]
- Ahmed, A.; Abubakr, M.; Sami, H.; Mahdi, I.; Mohamed, N.S.; Zinsstag, J. The First Molecular Detection of Aedes Albopictus in Sudan Associates with Increased Outbreaks of Chikungunya and Dengue. Int. J. Mol. Sci. 2022, 23, 11802. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Ali, Y.; Siddig, E.E.; Hamed, J.; Mohamed, N.S.; Khairy, A.; Zinsstag, J. Hepatitis E Virus Outbreak among Tigray War Refugees from Ethiopia, Sudan. Emerg. Infect. Dis. 2022, 28, 1722–1724. [Google Scholar] [CrossRef]
- Ahmed, A.; Ali, Y.; Elmagboul, B.; Mohamed, O.; Elduma, A.; Bashab, H.; Mahamoud, A.; Khogali, H.; Elaagip, A.; Higazi, T. Dengue Fever in the Darfur Area, Western Sudan. Emerg. Infect. Dis. 2019, 25, 2126. [Google Scholar] [CrossRef]
- Elagali, A.; Ahmed, A.; Makki, N.; Ismail, H.; Ajak, M.; Alene, K.A.; Weiss, D.J.; Mohammed, A.A.; Abubakr, M.; Cameron, E.; et al. Spatiotemporal Mapping of Malaria Incidence in Sudan Using Routine Surveillance Data. Sci. Rep. 2022, 12, 14114. [Google Scholar] [CrossRef]
- Siddig, E.E.; El-Sadig, S.M.; Eltigani, H.F.; Musa, A.M.; Mohamed, N.S.; Ahmed, A. Delayed Cerebellar Ataxia Induced by Plasmodium Falciparum Malaria: A Rare Complication. Clin. Case Rep. 2023, 11. [Google Scholar] [CrossRef]
- Mohamed, N.S.; AbdElbagi, H.; Elsadig, A.R.; Ahmed, A.E.; Mohammed, Y.O.; Elssir, L.T.; Elnour, M.-A.B.; Ali, Y.; Ali, M.S.; Altahir, O. Assessment of Genetic Diversity of Plasmodium Falciparum Circumsporozoite Protein in Sudan: The RTS, S Leading Malaria Vaccine Candidate. Malar. J. 2021, 20, 1–12. [Google Scholar] [CrossRef]
- Mohamed, N.S.; Ali, Y.; Abdalrahman, S.; Ahmed, A.; Siddig, E.E. The Use of Cholera Oral Vaccine for Containment of the 2019 Disease Outbreak in Sudan. Trans. R. Soc. Trop. Med. Hyg. 2022, 116, 763–766. [Google Scholar] [CrossRef]
- Ali, Y.; Ahmed, A.; Siddig, E.E.; Mohamed, N.S. The Role of Integrated Programs in the Prevention of COVID-19 in a Humanitarian Setting. Trans. R. Soc. Trop. Med. Hyg. 2022, 116, 193–196. [Google Scholar] [CrossRef] [PubMed]
- Khairy, A.; Bashier, H.; Nuh, H.; Ahmed, N.; Ali, Y.; Izzoddeen, A.; Mohamed, S.; Osman, M.; Khader, Y. The Role of the Field Epidemiology Training Program in the Public Health Emergency Response: Sudan Armed Conflict 2023. Front. Public Health 2024, 12, 1300084. [Google Scholar] [CrossRef] [PubMed]
- US Centers for Disease Control and Prevention Mpox Cases by Age and Gender and Race and Ethnicity. Available online: https://www.cdc.gov/poxvirus/mpox/response/2022/demographics.html (accessed on 29 March 2024).
- Hennessee, I. Epidemiologic and Clinical Features of Children and Adolescents Aged 18 Years with Monkeypox — United States, May 17–September 24, 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71. [Google Scholar] [CrossRef] [PubMed]
- Aguilera-Alonso, D.; Alonso-Cadenas, J.A.; Roguera-Sopena, M.; Lorusso, N.; San Miguel, L.G.; Calvo, C. Monkeypox Virus Infections in Children in Spain during the First Months of the 2022 Outbreak. Lancet Child Adolesc. Health 2022, 6, e22–e23. [Google Scholar] [CrossRef] [PubMed]
- Vaughan, A.M.; Cenciarelli, O.; Colombe, S.; de Sousa, L.A.; Fischer, N.; Gossner, C.M.; Pires, J.; Scardina, G.; Aspelund, G.; Avercenko, M. A Large Multi-Country Outbreak of Monkeypox across 41 Countries in the WHO European Region, 7 March to 23 August 2022. Eurosurveillance 2022, 27, 2200620. [Google Scholar] [CrossRef] [PubMed]
- van Furth, A.M.T.; van der Kuip, M.; van Els, A.L.; Fievez, L.C.; van Rijckevorsel, G.G.; van den Ouden, A.; Jonges, M.; Welkers, M.R. Paediatric Monkeypox Patient with Unknown Source of Infection, the Netherlands, June 2022. Eurosurveillance 2022, 27, 2200552. [Google Scholar] [CrossRef] [PubMed]
- Fuente, S.M.; de Borja Nava, F.; Valerio, M.; Veintimilla, C.; Aguilera-Alonso, D. A Call for Attention: Pediatric Monkeypox Case in a Context of Changing Epidemiology. Pediatr. Infect. Dis. J. 2022, 41, e548–e549. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Lun, W. Skin Manifestation of Human Monkeypox. J. Clin. Med. 2023, 12, 914. [Google Scholar] [CrossRef]
- Siddig, E.E.; Eltigani, H.F.; Ahmed, A. Urgent Call to Protect Children and Their Health in Sudan. BMJ 2023, 382, p1799. [Google Scholar] [CrossRef]
- Ly-Yang, F.; Miranda-Sánchez, A.; Burgos-Blasco, B.; Fernández-Vigo, J.I.; Gegúndez-Fernández, J.A.; Díaz-Valle, D. Conjunctivitis in an Individual with Monkeypox. JAMA Ophthalmol. 2022, 140, 1022–1024. [Google Scholar] [CrossRef] [PubMed]
- Long, B.; Liang, S.Y.; Carius, B.M.; Chavez, S.; Gottlieb, M.; Koyfman, A.; Brady, W.J. Mimics of Monkeypox: Considerations for the Emergency Medicine Clinician. Am. J. Emerg. Med. 2023, 65, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Siddig, E.E.; Hay, R. Laboratory-Based Diagnosis of Scabies: A Review of the Current Status. Trans. R. Soc. Trop. Med. Hyg. 2022, 116, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Del Giudice, P.; Fribourg, A.; Roudiere, L.; Gillon, J.; Decoppet, A.; Reverte, M. Familial Monkeypox Virus Infection Involving 2 Young Children. Emerg. Infect. Dis. 2023, 29, 437. [Google Scholar] [CrossRef] [PubMed]
- Cohen, N.J.; Brown, C.M.; Alvarado-Ramy, F.; Bair-Brake, H.; Benenson, G.A.; Chen, T.-H.; Demma, A.J.; Holton, N.K.; Kohl, K.S.; Lee, A.W.; et al. Travel and Border Health Measures to Prevent the International Spread of Ebola. MMWR Suppl. 2016, 65, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Venkatesan, P. Monkeypox Transmission—What We Know so Far. Lancet Respir. Med. 2022, 10, e101. [Google Scholar] [CrossRef] [PubMed]
- Craig, K.J.T.; Rizvi, R.; Willis, V.C.; Kassler, W.J.; Jackson, G.P. Effectiveness of Contact Tracing for Viral Disease Mitigation and Suppression: Evidence-Based Review. JMIR Public Health Surveill. 2021, 7, e32468. [Google Scholar] [CrossRef] [PubMed]
- Sah, R.; Mohanty, A.; Reda, A.; Padhi, B.K.; Rodriguez-Morales, A.J. Stigma during Monkeypox Outbreak. Front. Public Health 2022, 10, 1023519. [Google Scholar] [CrossRef]
- Cunningham, S.D.; Tschann, J.; Gurvey, J.E.; Fortenberry, J.D.; Ellen, J.M. Attitudes about Sexual Disclosure and Perceptions of Stigma and Shame. Sex. Transm. Infect. 2002, 78, 334–338. [Google Scholar] [CrossRef]
- Siddig, E.E.; Ahmed, A.; Ahmed, E.S.; Mohammed, M.A.; Kunna, E.; El-Sadig, S.M.; Ali, Y.; Hassan, R.A.; Ali, E.T.; Mohamed, N.S. Knowledge and Attitudes towards Cervical Cancer Prevention among Women in Khartoum State, Sudan. Womens Health 2023, 19, 17455057231166286. [Google Scholar] [CrossRef]
- Bergman, A.; McGee, K.; Farley, J.; Kwong, J.; McNabb, K.; Voss, J. Combating Stigma in the Era of Monkeypox—Is History Repeating Itself? J. Assoc. Nurses AIDS Care 2022, 33, 668–675. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.M.; Chen, S.T.; Merola, J.F.; Mostaghimi, A.; Zhou, X.A.; Fett, N.; Smith, G.P.; Saavedra, A.P.; Noe, M.H.; Rosenbach, M. Monkeypox Outbreak, Vaccination, and Treatment Implications for the Dermatologic Patient: Review and Interim Guidance from the Medical Dermatology Society. J. Am. Acad. Dermatol. 2023, 88, 623–631. [Google Scholar] [CrossRef] [PubMed]
- Siegrist, E.A.; Sassine, J. Antivirals with Activity against Mpox: A Clinically Oriented Review. Clin. Infect. Dis. 2023, 76, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Zucker, J.; Hazra, A.; Titanji, B.K. Mpox and HIV—Collision of Two Diseases. Curr. HIV/AIDS Rep. 2023, 20, 440–450. [Google Scholar] [CrossRef] [PubMed]
- Americo, J.L.; Earl, P.L.; Moss, B. Virulence Differences of Mpox (Monkeypox) Virus Clades I, IIa, and IIb. 1 in a Small Animal Model. Proc. Natl. Acad. Sci. 2023, 120, e2220415120. [Google Scholar] [CrossRef] [PubMed]
- Mauldin, M.R.; McCollum, A.M.; Nakazawa, Y.J.; Mandra, A.; Whitehouse, E.R.; Davidson, W.; Zhao, H.; Gao, J.; Li, Y.; Doty, J. Exportation of Monkeypox Virus from the African Continent. J. Infect. Dis. 2022, 225, 1367–1376. [Google Scholar] [CrossRef]
- Fleischauer, A.T.; Kile, J.C.; Davidson, M.; Fischer, M.; Karem, K.L.; Teclaw, R.; Messersmith, H.; Pontones, P.; Beard, B.A.; Braden, Z.H. Evaluation of Human-to-Human Transmission of Monkeypox from Infected Patients to Health Care Workers. Clin. Infect. Dis. 2005, 40, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Archer, B.N.; Abdelmalik, P.; Cognat, S.; Grand, P.E.; Mott, J.A.; Pavlin, B.I.; Barakat, A.; Dowell, S.F.; Elmahal, O.; Golding, J.P.; et al. Defining Collaborative Surveillance to Improve Decision Making for Public Health Emergencies and Beyond. The Lancet 2023, 401, 1831–1834. [Google Scholar] [CrossRef]
- Khatua, A.; Kar, T.K.; Nandi, S.K.; Jana, S.; Kang, Y. Impact of Human Mobility on the Transmission Dynamics of Infectious Diseases. Energy Ecol. Environ. 2020, 5, 389–406. [Google Scholar] [CrossRef]
- Williams, E.P.; Spruill-Harrell, B.M.; Taylor, M.K.; Lee, J.; Nywening, A.V.; Yang, Z.; Nichols, J.H.; Camp, J.V.; Owen, R.D.; Jonsson, C.B. Common Themes in Zoonotic Spillover and Disease Emergence: Lessons Learned from Bat- and Rodent-Borne RNA Viruses. Viruses 2021, 13, 1509. [Google Scholar] [CrossRef]
- Zinsstag, J.; Crump, L.; Schelling, E.; Hattendorf, J.; Maidane, Y.O.; Ali, K.O.; Muhummed, A.; Umer, A.A.; Aliyi, F.; Nooh, F.; et al. Climate Change and One Health. FEMS Microbiol. Lett. 2018, 365, fny085. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Mohamed, N.S.; Siddig, E.E.; Algaily, T.; Sulaiman, S.; Ali, Y. The Impacts of Climate Change on Displaced Populations: A Call for Action. J. Clim. Change Health 2021, 3, 100057. [Google Scholar] [CrossRef]
- Organization, W.H. Joint External Evaluation of IHR Core Capacities of the Republic of the Sudan: Mission Report, 9-13 October 2016. 2017.
- Siddig, E.E.; Eltigani, H.F.; Ahmed, A. Healing the Unseen Wounds: Sudan’s Humanitarian Crisis Traumatizing a Nation. Asian J. Psychiatry 2023, 89, 103764. [Google Scholar] [CrossRef] [PubMed]
- Siddig, E.E.; Eltigani, H.F.; Ali, E.T.; Bongomin, F.; Ahmed, A. Sustaining Hope amid Struggle: The Plight of Cancer Patients in Sudan’s Ongoing War. J. Cancer Policy 2023, 38, 100444. [Google Scholar] [CrossRef]
- Alfadul, E.S.; Alrawa, S.S.; Eltigani, H.F.; Ahmed, A.; Siddig, E.E. The Unraveling of Sudan’s Health System: Catastrophic Consequences of Ongoing Conflict. Med. Confl. Surviv. 2023, 39, 364–368. [Google Scholar] [CrossRef]
- Siddig, E.E.; Eltigani, H.F.; Ahmed, A. Urgent Call to Protect Children and Their Health in Sudan. BMJ 2023, 382. [Google Scholar] [CrossRef]
Figure 1.
Epi-curve showing of cases suspected of Mpox in Khartoum state distribution by the date of onset in 2022.
Figure 1.
Epi-curve showing of cases suspected of Mpox in Khartoum state distribution by the date of onset in 2022.
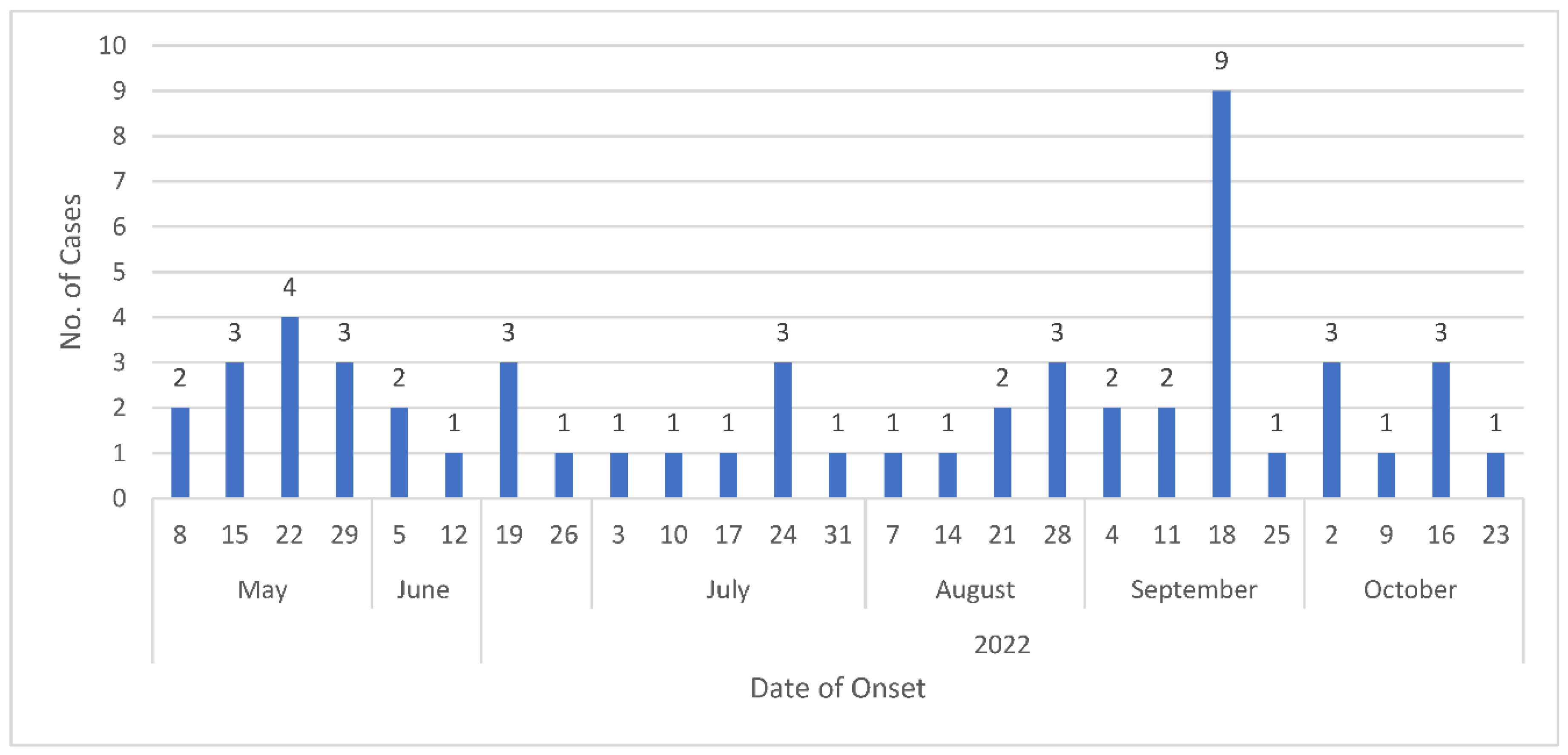
Figure 2.
The main clinical manifestations of the suspected cases.
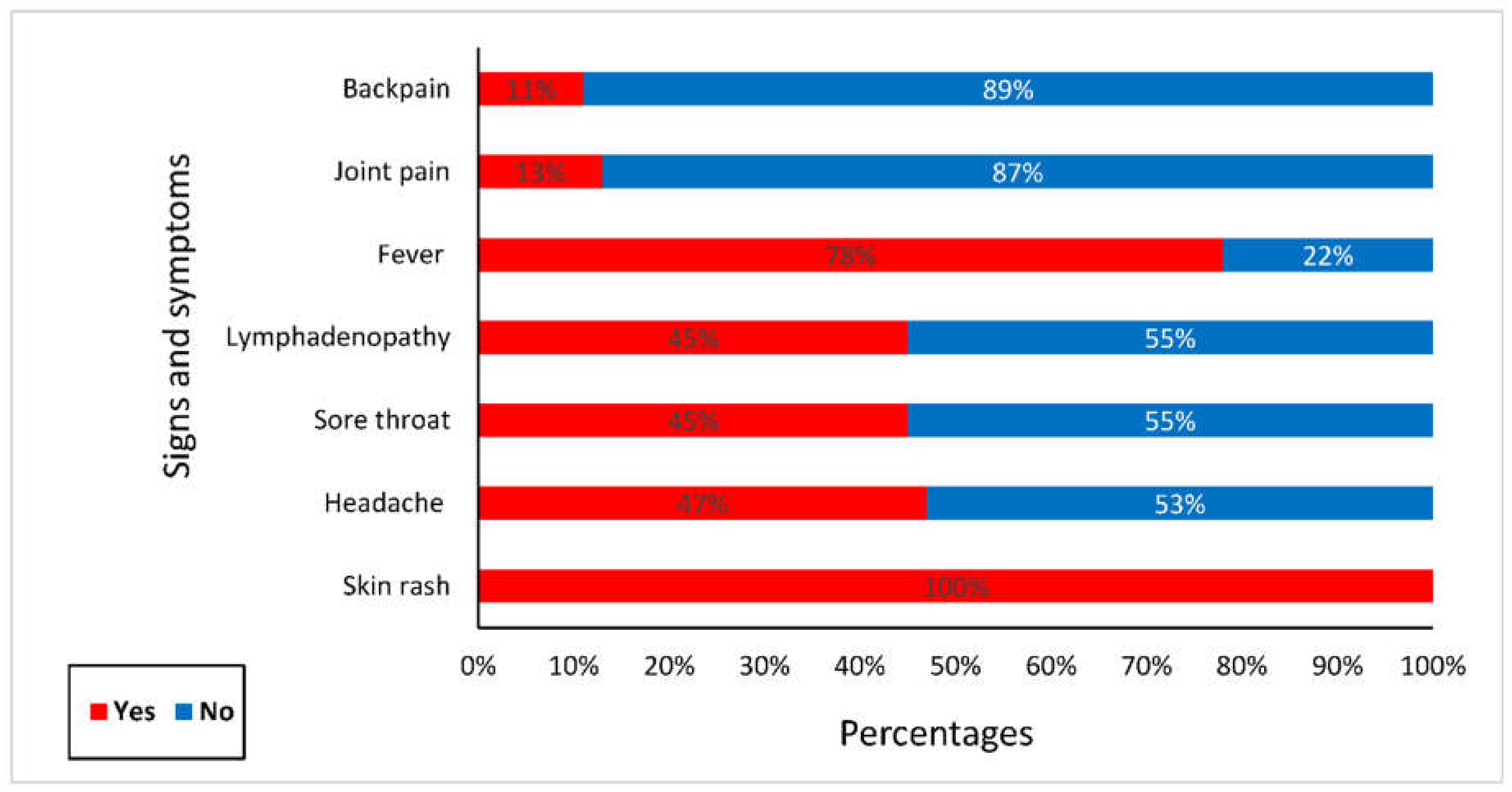
Figure 3.
Clinical manifestation of Mpox virus lesions on a 2-year old child.

Table 1.
Khartoum state’s Ministry of Health action plan of preparedness and response to Mpox in the state in 2022-2023.
Table 1.
Khartoum state’s Ministry of Health action plan of preparedness and response to Mpox in the state in 2022-2023.
| Pillars | Structure | Activities | Note |
| Coordination | Mpox taskforce committee was established at state level (Federal and state level) and seven sub-committees at each locality level (locality level). | Coordinates between the stakeholders of human, animal, and environmental health for the implementation of the preparedness, surveillance, and response at locality levels. | The committee was led by the Ministry of Health and members, including animals health authorities, United Nations (UN) agencies, and other non-governmental (NGOs) partners. |
| Disease surveillance system | Enhancement of surveillance systems among both animals and humans to facilitate early detection and response for Mpox cases. | Building capacity of integrated surveillance conducted for 596 cadres who have received training in Mpox from 298 health facilities (HFs) across seven localities, additionally 400 community volunteers were trained on community-based surveillance (CBS) for Mpox. | Case definition on Mpox distributed in all HFs and provided to CBS volunteers. |
| Laboratory | Building the diagnostic capacity and readiness to compensate serve and/or country-wide massive screening of Mpox if needed. | Three technical officers and 3 technicians were trained on the basic and advanced diagnostic tools for Mpox. Stocks of efficient diagnostic kits were mobilized, secured, and calibrated. |
Referral system was established and operated by the rapid response teams (RRTs). |
| Rapid Response Teams (RRTs) | Establishment of 7 RRTs and equipping them with necessary resources to enable early detection and response. | 7 RRTs received training on Mpox case investigation across seven localities. | The team was composed from an epidemiologist, a laboratory technician, a clinician, an infection, prevention and control (IPC) specialist, and a public health officer) |
| Case management and IPC | Training for healthcare providers on Mpox case management and IPC in isolation centres | 298 Healthcare providers received training in case management and IPC | One Isolation centre was identified (Ibrahim Malik Hospital). A referral system was established at airports and other localities. |
| Risk communication and community engagement | Social behavioural change in coordination with partners through various modalities of risk communication | Raising awareness sessions were delivered through TV, Radio and social media, mosques, mobile microphones, and health promotion theatres across seven localities. | Health promotion activities and engagements covered more than 70% of the communities. |
Table 2.
Epidemiological characteristics of Mpox suspected cases in Khartoum State in 2022.
| |
Cases | AR/10000 | CFR/100 | |
| Suspected | Confirmed | |||
| Khartoum | 17 | 0 | 0.20 | 0 |
| Jabal Awliya | 9 | 0 | 0.94 | 0 |
| Omdurman | 8 | 1 | 0.14 | 0 |
| Bahri | 4 | 0 | 0.06 | 0 |
| Sharg El Nile | 8 | 1 | 0.09 | 0 |
| Karrari | 4 | 0 | 0.05 | 0 |
| UmBada | 5 | 0 | 0.04 | 0 |
| Total | 55 | 2 | 0.11 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



