Submitted:
09 September 2025
Posted:
10 September 2025
You are already at the latest version
Abstract
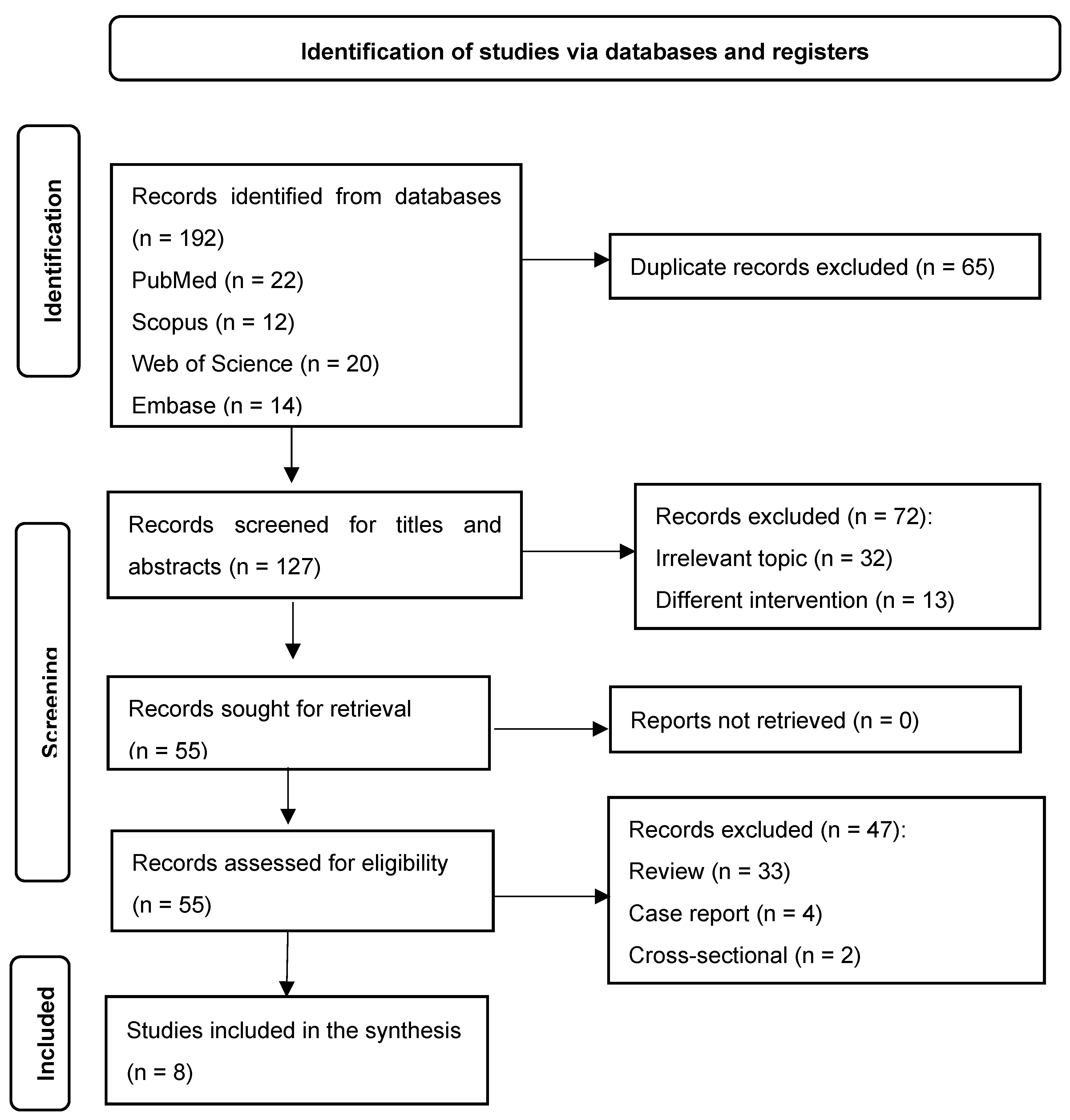
Background: Research examining the difference between the effects of deep and superficial dry needling on myofascial trigger points (MTrPs) in the upper trapezius muscle is limited. Thus, this systematic review was conducted to compare the effects of these two dry-needling techniques on pain and functional disability in adults with neck pain who demonstrated MTrPs. Methods: Randomised clinical trials (RCTs) were identified through an electronic search in PubMed, Scopus, Web of Science, Embase, Google Scholar, Dimensions and OpenAlex from inception until September 22, 2024. Only English-language studies were considered. Best-evidence synthesis was utilised to interpret the results of the included RCTs. Results: Of the 192 records obtained, eight RCTs were included (two with a low risk of bias, four with some risk-of-bias concerns and two with a high risk of bias). Overall, both deep and superficial dry needling provided short-term alleviation of pain and functional disability. No clinically meaningful differences were found between the two dry-needling techniques. Conclusion: Deep and superficial dry needling seem to have similar positive effects on pain and functional disability in patients with neck pain exhibiting MTrPs.
Keywords:
Introduction
2. Materials and Methods
Protocol Registration
Eligibility Criteria
Search Strategy
Study Selection
Risk-of-Bias Assessment
Data Extraction and Synthesis
Statistical Analysis
3. Results
3.1. Study Selection

| Measure | Value |
|---|---|
| Total number of articles screened | 127 |
| Articles included by both reviewers | 55 (43.3%) |
| Articles excluded by both reviewers | 72 (56.7%) |
| Articles with disagreements | 0 (0%) |
| Percentage of agreement | 100% |
| Cohen’s kappa (κ) | 1.00 |
| 95% confidence interval for kappa | 1.00–1.00 |
| Statistical significance (p-value) | < 0.001 |
| Domain | Percentage of agreement (%) | Cohen’s kappa (κ) | 95% Confidence interval (CI) | P-value |
|---|---|---|---|---|
| Domain 1 | 87.5% | 0.73 | 0.28–1.00 | 0.009 |
| Domain 2 | 100% | 1.00 | 1.00–1.00 | 0.005 |
| Domain 3 | 100% | 1.00 | 1.00–1.00 | 0.005 |
| Domain 4 | 100% | 1.00 | 1.00–1.00 | 0.000 |
| Domain 5 | 87.5% | 0.75 | 0.30–1.00 | 0.028 |
| Overall | 87.5% | 0.78 | 0.646–1.00 | 0.002 |
3.2. Study Characteristics
3.3. Risk of Bias
3.4. Intervention Protocol
3.5. Intervention Duration
3.6. Effect on Pain Severity
3.7. Effect on Functional Disability
3.8. Effects on Other Outcome Measures
| Authors | Sample size | Diagnostic criteria | Interventions | No. of sessions | Follow-ups | Outcome measures | Main results |
|---|---|---|---|---|---|---|---|
| Chys et al., 2023 [27] | 54 (DDN: 26, SDN: 28) | Palpable tight band, local pain on pressure and referred pain | DDN vs. SDN in the upper trapezius | 1 session | Immediately post-treatment | PPT CPM |
There were no significant differences between DDN and SDN for PPT at local or distant sites. DDN significantly improved the relative CPM efficiency. |
| Ezzati et al., 2018 [19] | 50 (DDN: 25, SDN: 25) | Palpable tight band, local pain on pressure and recognised pain | DDN vs. SDN in the upper trapezius | 3 sessions | 15 days | VAS NDI ROM |
Both groups improved, but DDN showed greater gains in ROM and NDI over follow-up. |
| Hoseininejad et al., 2023 [20] | 50 (DDN: 25, SDN: 25) | Neck/shoulder pain with at least one active trigger point in the upper trapezius persisting for 3 months | DDN vs. SDN in the upper trapezius | 1 session | 1 week | VAS NDI sEMG |
Both groups improved in VAS and NDI, but only DDN significantly increased sEMG. |
| Martín-Rodríguez et al., 2019 [28] | 34 (DDN: 17, control: 17) | Palpable tight band with local and familiar pain, and restricted ROM during full extension | Trigger point DDN vs. sham dry needling | 1 session | 1 month | CMC VAS ROM NDI |
DDN improved pain, ROM and motor control, but there were no significant differences compared to sham DDN. |
| Myburgh et al., 2012 [29] | 77 (symptomatic/ asymptomatic) | Symptomatic group: significant MTrP and self-reported pain ≥ 3 on NRS-101. Asymptomatic group: no MTrP or pain (0). | DDN vs. SDN in the upper trapezius | 1 session | 28 h post-treatment | PPT NRS-101 F-max RFD |
Both groups reduced pain, but PPT decreased across all participants. There were no significant differences in F-max or RFD. |
| Navarro et al., 2022 [30] | 180 (DDN: 60, SDN: 60, placebo: 60) | Presence of latent MTrPs in the upper trapezius | DDN vs. SDN vs. placebo | 1 session | 1 week | PPT ACROM |
Both DDN and SDN improved PPT and ROM over time, but DDN showed better ipsilateral rotation improvement at 7 days. |
| Sarrafzadeh et al., 2018 [21] | 50 (DDN: 25, SDN: 25) | Palpable tight band, local pain on pressure and recognition of pain by the participants | DDN vs. SDN in the upper trapezius | 3 sessions | 15 days | VAS Ultrasonic evaluation |
Both DDN and SDN reduced pain and increased muscle thickness, but DDN was superior in pain reduction. |
|
Sedighi et al., 2017 [22] |
30 (DDN: 15, SDN: 15) | Unilateral neck pain spreading to the frontotemporal area, worsened by movement, restricted ROM and C1–C3 tenderness | DDN vs. SDN in the suboccipital/upper trapezius | 1 session | 1 week | HI Pain intensity TrP tenderness ROM FRI |
Both groups reduced HI and tenderness, but DDN showed superior improvements in ROM and FRI. |
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| MPS | Myofascial pain syndrome |
| MTrPs | Myofascial trigger points |
| RCTs | Randomised controlled trials |
| MCIDs | Minimal clinically important differences |
Appendix A: Search Strategy
| Database | Date of search | Search strategy | Results |
| PubMed | 22/09/2024 | (("Neck Pain"[Mesh] OR "Cervical Pain"[Mesh]) AND ("Dry Needling"[Mesh] OR "deep dry needling" OR "Superficial dry needling")) AND ("Trigger Points"[Mesh] OR "Myofascial Pain Syndromes"[Mesh]) | 22 |
| Web of Science | 22/09/2024 | TS=("Neck pain" OR "Cervical pain") AND TS=("deep dry needling" OR "Superficial dry needling") AND TS=("Trigger point*" OR "Myofascial pain syndrome") | 20 |
| Scopus | 22/09/2024 | (TITLE-ABS-KEY ("Neck pain" OR "Cervical pain")) AND (TITLE-ABS-KEY ("deep dry needling" OR "Superficial dry needling")) AND (TITLE-ABS-KEY ("Trigger point*" OR "Myofascial pain syndrome")) | 12 |
| Embase | 22/09/2024 | ('neck pain' OR 'cervical pain':ab,ti,kw) AND ('deep dry needling' OR 'superficial dry needling':ab,ti,kw) AND ('trigger point*' OR 'myofascial pain syndrome':ab,ti,kw) | 14 |
| Google Scholar | 22/09/2024 | intitle:("Neck pain" OR "Cervical pain") AND intitle:("deep dry needling" OR "Superficial dry needling") AND intitle:("Trigger point*" OR "Myofascial pain syndrome") | 51 |
| Dimensions | 22/09/2024 | ("Neck pain" OR "Cervical pain") AND ("deep dry needling" OR "Superficial dry needling") AND ("Trigger point*" OR "Myofascial pain syndrome") | 10 |
| OpenAlex | 22/09/2024 | ("Neck pain" OR "Cervical pain") AND ("deep dry needling" OR "Superficial dry needling") AND ("Trigger point*" OR "Myofascial pain syndrome") | 63 |
References
- Ailliet L, Rubinstein SM, De Vet HCW, Van Tulder MW, Terwee CB. Reliability, responsiveness and interpretability of the neck disability index-Dutch version in primary care. Eur Spine J. 2014. [CrossRef]
- Ansari NN, Komesh S, Naghdi S, Fakhari Z, Alaei P. Responsiveness of Minimal Clinically Important Change for the Persian Functional Rating Index in Patients with Chronic Low Back Pain.
- Baldry P. Superficial versus deep dry needling. Acupunct Med. 2002;20(2-3):78-81. Available from: http://aim.bmj.com/content/20/2-3/78.full.pdf.
- Ball A, Perreault T, Fernández-De-las-Peñas C, Agnone M, Spennato J. Ultrasound Confirmation of the Multiple Loci Hypothesis of the Myofascial Trigger Point and the Diagnostic Importance of Specificity in the Elicitation of the Local Twitch Response. Diagnostics. 2022;12(2). [CrossRef]
- Ballyns JJ, Turo D, Otto P, Shah JP, Hammond J, Gebreab T, et al. Office-based elastographic technique for quantifying mechanical properties of skeletal muscle. J Ultrasound Med. 2012;31(8):1209-19. [CrossRef]
- Barbero M, Schneebeli A, Koetsier E, Maino P. Myofascial pain syndrome and trigger points: Evaluation and treatment in patients with musculoskeletal pain. Curr Opin Support Palliat Care. 2019;13(3):270-6. [CrossRef]
- Bennett R. Myofascial pain syndromes and their evaluation. Best Pract Res Clin Rheumatol. 2007;21(3):427-45. [CrossRef]
- Berger A, Dukes E, Martin S, Edelsberg J, Oster G. Characteristics and healthcare costs of patients with fibromyalgia syndrome. Int J Clin Pract. 2007;61(9):1498-508. [CrossRef]
- Bourgaize S, Newton G, Kumbhare D, Srbely J. A comparison of the clinical manifestation and pathophysiology of myofascial pain syndrome and fibromyalgia: Implications for differential diagnosis and management. J Can Chiropr Assoc. 2018;62(1):26-41.
- Ceccherelli F, Rigoni MT, Gagliardi G, Ruzzante L. Comparison of superficial and deep acupuncture in the treatment of lumbar myofascial pain: A double-blind randomized controlled study. Clin J Pain. 2002;18(3):149-53. [CrossRef]
- Chansirinukor W. Thai version of the Functional Rating Index for patients with back and neck pain: Part II responsiveness and head-to-head comparisons. Physiother Res Int. 2018 Apr;1-6. [CrossRef]
- Chys M, Bontinck J, Voogt L, Sendarrubias GMG, Cagnie B, Meeus M, De Meulemeester K. Immediate effects of dry needling on pain sensitivity and pain modulation in patients with chronic idiopathic neck pain: a single-blinded randomized clinical trial. Braz J Phys Ther. 2023;27(1):100481. [CrossRef]
- Cohen SP, Hooten WM. Advances in the diagnosis and management of neck pain. BMJ. 2017;358:j3221. [CrossRef]
- Dunning J, Butts R, Mourad F, Young I, Flannagan S, Perreault T. Dry needling: a literature review with implications for clinical practice guidelines. Phys Ther Rev. 2014;19(4):252-65. [CrossRef]
- Espejo-Antúnez L, Tejeda JFH, Albornoz-Cabello M, Rodríguez-Mansilla J, de la Cruz-Torres B, Ribeiro F, Silva AG. Dry needling in the management of myofascial trigger points: A systematic review of randomized controlled trials. Complement Ther Med. 2017;33:46-57. [CrossRef]
- Ezzati K, Sarrafzadeh J, Ebrahimi Takamjani I, Khani S. The Efficacy of Superficial and Deep Dry Needling Techniques on Functional Parameters in Subjects With Upper Trapezius Myofascial Pain Syndrome. Caspian J Neurol Sci. 2018;4(15):152-8. [CrossRef]
- Fernández-de-las-Peñas C, Dommerholt J. International consensus on diagnostic criteria and clinical considerations of myofascial trigger points: A delphi study. Pain Med. 2018;19(1):142-50. [CrossRef]
- Fernández-De-Las-Peñas C, Nijs J. Trigger point dry needling for the treatment of myofascial pain syndrome: Current perspectives within a pain neuroscience paradigm. J Pain Res. 2019;12:1899-911. [CrossRef]
- Griswold D, Wilhelm M, Donaldson M, Learman K, Cleland J. The effectiveness of superficial versus deep dry needling or acupuncture for reducing pain and disability in individuals with spine-related painful conditions: a systematic review with meta-analysis. J Man Manip Ther. 2019;27(3):128-40. [CrossRef]
- Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. [CrossRef]
- Hoseininejad Z, Mohammadi HK, Azadeh H, Taheri N. Comparison of immediate and delayed effects of superficial and deep dry needling in patients with upper trapezius myofascial trigger points. J Bodyw Mov Ther. 2023;33:106-11. [CrossRef]
- Ja AC, Jd C, Psycho WJM. Psychometric Properties of the Neck Disability Index and Numeric Pain Rating Scale in Patients With Mechanical. Arch Phys Med Rehabil. 2008;89(January). [CrossRef]
- Kalichman L, Vulfsons S. Dry needling in the management of musculoskeletal pain. J Am Board Fam Med. 2010;23(5):640-6. [CrossRef]
- Lauche R, Langhorst J, Dobos GJ, Cramer H. Clinically meaningful differences in pain, disability and quality of life for chronic nonspecific neck pain—A reanalysis of 4 randomized controlled trials of cupping therapy. Evid Based Complement Alternat Med. 2013;2013:342-7.
- Legge D. A history of dry needling. J Musculoskelet Pain. 2014;22(3):301-7. [CrossRef]
- Lew J, Kim J. Comparison of dry needling and trigger point manual therapy in patients with neck and upper back myofascial pain syndrome: a systematic review and meta-analysis. J Man Manip Ther. 2021;29(3):136-46. [CrossRef]
- Martín-Rodríguez A, Sáez-Olmo E, Pecos-Martín D, Calvo-Lobo C. Effects of dry needling in the sternocleidomastoid muscle on cervical motor control in patients with neck pain: a randomised clinical trial. Acupunct Med. 2019;37(3):151-63. [CrossRef]
- McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J Clin Epidemiol. 2016;75:40-6. [CrossRef]
- Mi CH, Qi XY, Ding YW, Zhou J, Dao JW, Wei DX. Recent advances of medical polyhydroxyalkanoates in musculoskeletal system. Biomater Transl. 2023;4(4):234-47. [CrossRef]
- Moral OM Del. Dry needling treatments for myofascial trigger points. J Musculoskelet Pain. 2010;18(4):411-6. [CrossRef]
- Muka T, Glisic M, Milic J, Verhoog S, Bohlius J, Bramer W, Chowdhury R, Franco OH, Library M, Muka T. A 24-step guide on how to design, conduct, and successfully publish a systematic review & meta-analysis in medical research. 2019;1-25.
- Myburgh C, Hartvigsen J, Aagaard P, Holsgaard-Larsen A. Skeletal muscle contractility, self-reported pain and tissue sensitivity in females with neck/shoulder pain and upper Trapezius myofascial trigger points-a randomized intervention study. Chiropr Man Therap. 2012;20. [CrossRef]
- Näslund J, Näslund UB, Odenbring S, Lundeberg T. Sensory stimulation (acupuncture) for the treatment of idiopathic anterior knee pain. J Rehabil Med. 2002;34(5):231-8. [CrossRef]
- Navarro SM, Medina SD, Rico JMB, Ortiz MIR, Gracia MTP. Analysis and comparison of pain pressure threshold and active cervical range of motion after superficial and deep dry needling techniques of the upper trapezius muscle. Acupunct Med. 2022;40(1):13-23. [CrossRef]
- Pal U, Kumar L, Mehta G, Singh N, Singh G, Singh M, Yadav H. Trends in management of myofacial pain. Natl J Maxillofac Surg. 2014;5(2):109. [CrossRef]
- Pool JJM, Ostelo RWJG, Hoving JL. Disability Index and the Numerical Rating Scale for Patients With Neck Pain.
- Sabeh AM, Bedaiwi SA, Felemban OM, Mawardi HH. Myofascial Pain Syndrome and Its Relation to Trigger Points, Facial Form, Muscular Hypertrophy, Deflection, Joint Loading, Body Mass Index, Age and Educational Status. J Int Soc Prev Community Dent. 2020;10(6):786-93. [CrossRef]
- Sachiko F, Motohiro I, Miwa N, Megumi I. Difference between therapeutic effects of deep and superficial acupuncture needle insertion for low back pain: A randomized controlled clinical trial. J Acupunct Meridian Stud. 2011;7(1):37-45.
- Sánchez-Infante J, Navarro-Santana MJ, Bravo-Sánchez A, Jiménez-Diaz F, Abián-Vicén J. Is dry needling applied by physical therapists effective for pain in musculoskeletal conditions? a systematic review and meta-analysis. Phys Ther. 2021;101(3):1-15. [CrossRef]
- Sarrafzadeh J, Khani S, Ezzati K, Takamjani IE. Effects of Superficial and Deep Dry Needling on Pain and Muscle Thickness in Subject with Upper Trapezius Muscle Myofascial Pain Syndrome. J Pain Relief. 2018;7(03):4-9. [CrossRef]
- Sedighi A, Nakhostin Ansari N, Naghdi S. Comparison of acute effects of superficial and deep dry needling into trigger points of suboccipital and upper trapezius muscles in patients with cervicogenic headache. J Bodyw Mov Ther. 2017;21(4):810-4. [CrossRef]
- Shah JP, Danoff JV, Desai MJ, Parikh S, Nakamura LY, Phillips TM, Gerber LH. Biochemicals Associated With Pain and Inflammation are Elevated in Sites Near to and Remote From Active Myofascial Trigger Points. Arch Phys Med Rehabil. 2008;89(1):16-23. [CrossRef]
- Slavin RE. Best evidence synthesis: An intelligent alternative to meta-analysis. J Clin Epidemiol. 1995;48(1):9-18. [CrossRef]
- Tsai CT, Hsieh LF, Kuan TS, Kao MJ, Chou LW, Hong CZ. Remote effects of dry needling on the irritability of the myofascial trigger point in the upper trapezius muscle. Am J Phys Med Rehabil. 2010;89(2):133-40. [CrossRef]
- Zhang Y, Du NY, Chen C, Wang T, Wang LJ, Shi XL, Li SM, Guo CQ. Acupotomy Alleviates Energy Crisis at Rat Myofascial Trigger Points. Evid Based Complement Alternat Med. 2020;2020:5129562. [CrossRef]
- Guzmán-Pavón MJ, Cavero-Redondo I, Martínez-Vizcaíno V, Fernández-Rodríguez R, Reina-Gutierrez S, Álvarez-Bueno C. Effect of physical exercise programs on myofascial trigger points–related dysfunctions: A systematic review and meta-analysis. Pain Med. 2020;21(11):2986-96.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
- Edwards J, Knowles N. Superficial dry needling and active stretching in the treatment of myofascial pain--a randomised controlled trial. Acupunct Med. 2003 Sep;21(3):80-6. [CrossRef] [PubMed]
| Study | Bias due to the randomisation process | Bias due to deviation from the intended interventions | Bias due to missing outcome data | Bias in outcome measurement | Bias in the selection of the reported result | Overall risk of bias |
|---|---|---|---|---|---|---|
| Chys et al., 2023 [27] | Low | Low | Low | Low | Low | Low |
| Ezzati et al., 2018 [19] | High | Low | Low | High | Some concerns | High |
| Hoseininejad et al., 2023 [20] | Some concerns | Low | Low | Low | Some concerns | Some concerns |
| Myburgh et al., 2012 [29] | Some concerns | Low | Low | Low | Low | Some concerns |
| Navarro et al., 2022 [30] | Some concerns | Low | Low | Low | Low | Some concerns |
| Martín-Rodríguez et al., 2019 [28] | Low | Low | Low | Low | Low | Low |
| Sarrafzadeh et al., 2018 [21] | Some concerns | Low | Low | Low | Low | Some concerns |
| Sedighi et al., 2017 [22] | Some concerns | High | Low | Some concerns | Some concerns | High |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



