Submitted:
08 September 2025
Posted:
09 September 2025
You are already at the latest version
Abstract
The study of the gut microbiome is a relatively new, rapidly growing field of medicine. Alterations in intestinal microbial composition have been implicated in a range of cardiovascular pathologies, primarily atherosclerosis, coronary artery disease, heart failure, and hypertension. Dysbiosis disrupts the balance between commensal and pathogenic bacterial species, impairs gut barrier function, activates pro-inflammatory mechanisms, and modulates the production of microbiome-derived metabolites, such as trimethylamine-N-oxide, short chain fatty-acids, and secondary bile acids. Current data underline a bidirectional relationship between cardiovascular pharmacotherapy and gut barrier dysfunction, as well as changes in gut microbial ecosystem. Commonly used drugs in heart failure management, including statins and angiotensin-converting enzyme inhibitors, may exhibit higher efficacy and better bioavailability in the presence of specific bacterial phyla. Other agents, such as cardiac glycosides, are susceptible to microbial inactivation. Certain microbial taxa can also mitigate drug-induced gut barrier injury and help restore gut homeostasis - for instance, by ameliorating aspirin-related mucosal damage. This review explores the multifaceted relationship between cardiovascular medication and the gut microbiome, synthesizes current evidence, and highlights its potential significance for precision medicine in heart failure management.
Keywords:
gut microbiome
; heart failure
; metabolites
; cardiovascular medication
; pharmacomicrobiomics
; personalized medicine
1. Introduction to the Gut Microbiome and Cardiovascular Health
Despite tremendous advances in cardiology, heart diseases remain the leading cause of death worldwide [1]. While established risk factors contribute to the development of cardiovascular disease (CVD), new research suggests that changes in the gut microbiome community may play an additional unfavorable role in the occurrence and progression of cardiovascular pathologies, particularly heart failure [2,3]. Many drugs, used in cardiology, such as antihypertensives, cholesterol lowering substances, and antithrombotic medication have been shown to modulate gut microbial composition and diversity [4]. Some findings suggest that statins may have implication in reducing systemic inflammation by promoting the growth of various beneficial bacterial phyla, thereby improving overall cardiovascular outcomes [5]. Agents targeting the renin-angiotensin-aldosterone system may also alter the microbiome composition, potentially attenuating the risk of hypertension related complications [6,7]. On the other hand, changes in the gut microbial profile may alter drug metabolism, affecting the efficacy and safety of antithrombotic therapies [8]. This review explores the complex bidirectional interactions between cardiovascular pharmacotherapy and the gut microbiome, with a focus on implications for heart failure management and personalized medicine.
2. The Gut-Heart Axis, Dysbiosis and Systemic Inflammation
The human gut hosts an average of 1000 to 1150 microbial strain [9]. Trillions of commensal microorganisms residing in the intestinal lumen - in varying proportions – constitute a complex organ, that plays a crucial role in maintaining gut barrier integrity, metabolic homeostasis, and the inflammatory response [10]. Large-scale populational studies, including the European Metagenomics of the Human Intestinal Tract (MetaHIT) and the US-led Human Microbiome Project, managed to provide a characterization of different microbial compositions in health and disease [11,12].
Although challenges had been arisen in identifying a “healthy” gut microbiome composition due to the high inter-individual variability, it has been shown that in healthy states the gut microbial ecosystem remains relatively stable. Approximately 90% is dominated by the Firmicutes and Bacteroides species, while Proteobacteria, Actinobacteria, Cyanobacteria, Fusobacteria, and Verrucomicrobia comprise the majority of the remaining fraction [11,13]. These species are responsible for maintaining intestinal mucosal barrier, enhance digestion, supply nutrients, prevent infections, and support normal coagulation [14].
Nevertheless, in pathological conditions, an imbalance of the gut microbial milieu may arise, leading to dysbiosis [15]. This disruption, in turn leads to intestinal mucosal damage and increases the permeability of the intestinal barrier. The resulting “leaky gut” facilitates endotoxin translocation, metabolite and cytokine influx into systemic circulation. This can trigger dysbiosis-related systemic inflammation, which has been implicated in cardiovascular pathogenesis [16,17]. A self-promoting cycle can emerge in which inflammatory pathways - including the expansion of cardiac myosin specific Th17 cells, toll-like receptor signaling, and increased production of proinflammatory cytokines such as tumor necrosis factor-α (TNF-α) and interferon-γ (IFN-γ) – further compromise gut barrier function [17,18].
3. Role of the Key Gut-Derived Metabolites
Different microbiota species produce a variety of bioactive compounds, depending on the host’s individual microbiome composition and dietary habits. Emerging evidence suggests that key metabolites implicated in cardiovascular pathogenesis include trimethylamine-N-oxide (TMAO), short-chain fatty acids (SCFAs), and secondary bile acids (SBAs). These metabolites modulate vascular inflammation, lipid and glucose homeostasis, blood pressure regulation and thrombosis risk, underlining the significance of the gut-heart axis in cardiovascular disease [19].
3.1. Trimethylamine-N-oxide (TMAO)
The association between TMAO - a gut microbiome-dependent byproduct of dietary choline, phosphatidylcholine, and carnitine (found in eggs, fish and red meat) - and CVD risk was first described by Wang et al. in 2011 and has been extensively studied since [20]. Recent meta-analysis revealed a 67% risk of CVD development linked to high TMAO levels [21]. Accordingly, the relation between increased TMAO levels and the risk of major adverse cardiac events (MACE) has been demonstrated by numerous animal and human experiments [21,22,23]. By altering cholesterol metabolism - either promoting lipid deposition in the arterial walls or inhibiting reverse cholesterol transport – TMAO contributes to the development of atherosclerosis [24]. Furthermore, it aggravates vascular inflammation, induces endothelial dysfunction, enhances foam cell formation, and subsequently facilitates atherosclerotic plaque development and progression [21]. Longitudinal studies have shown that elevated plasma TMAO levels have prognostic value for arterial thrombosis, stroke and myocardial infarction [25,26]. In addition, heart failure patients exhibit higher TMAO plasma concentration than healthy individuals, and they positively correlate with B-type natriuretic peptide (BNP) levels [15]. One large-scale clinical cohort study demonstrated an impressive 2.5-fold increase in the risk of MACE for patients in the highest quartile of plasma TMAO levels compared to those in the lowest quartile [4].
3.2. Short Chain Fatty Acids (SCFAs)
SCFAs - including acetate, propionate, and butyrate – are synthesized during the fermentation of indigestible dietary fibers - are among the most well-defined, beneficial microbiome-derived metabolites [27,28]. The main gut bacteria responsible for converting complex carbohydrates into monosaccharides include Bacteroides, Bifidobacterium and Faecalibacterium spp. SCFAs have been established to contribute significantly in sustaining eubiosis, enhancing lipid and glucose metabolism, modulating immune responses, preserving intestinal mucosal integrity, and preventing bacterial translocation into systemic circulation [29,30]. Butyric acid exhibits anti-inflammatory properties and increases nitric oxide concentrations, thereby reducing atherosclerotic burden. Propionic acid supports metabolic homeostasis, while acetic acid helps regulate blood pressure and modulates lipid profiles [31,32].
3.3. Secondary Bile Acids (SBAs)
It is widely recognized that BAs are essential for cholesterol excretion. The deconjugation of primary BAs into secondary BAs - such as deoxycholic and lithocholic acids - occurs in the distal ileum through microbial enzymatic activity [33]. SBAs participate in multiple metabolic pathways. Besides aiding in the absorption of dietary fats and lipid-soluble vitamins, they modulate glucose and cholesterol metabolism via the activation of Farnesoid X receptor (FXR) and Takeda G protein-coupled receptor 5 (TGR5), and exhibit anti-inflammatory properties by inhibiting pro-inflammatory cytokines, like TNF-α [34]. Current evidence on the role of SBAs primarily stems from preclinical studies. It has been confirmed that FXR activation preserves intestinal lining integrity and permeability, alongside with controlling inflammation and fibrosis. In vitro studies have shown that higher FXR expression may reduce myocardial ischemia-reperfusion injury, whereas FXR suppression is associated with increase myocyte apoptosis and infarct size [35]. Additionally, a link has been identified between FXR activation and the upregulation of angiotensin II type 2 receptor, which was shown to prevent salt-sensitive hypertension in rat models - suggesting potential therapeutic application [36]. (Figure 1)
4. Impact of CVD Drugs on the Gut Microbiome - Pharmacomicrobiomics
Advances in genome sequencing technologies and bioinformatics have enabled detailed description of the gut microbiome’s composition, genetic diversity, and its interaction with pharmaceutical agents [37]. Large-scale human cohort studies – including the Dutch LifeLines-DEEP cohort, the Belgium Flemish Gut Flors Project, and the TwinsUK cohort - have identified associations between various medications and changes in gut microbiome composition and function [38]. Many cardiovascular drugs rank among the top microbiome-associated pharmaceuticals, including statins, angiotensin-converting enzyme inhibitors, beta-blockers, and antithrombotic agents [38,39] (Figure 2)
4.1. Statins
Statins have proven to be the most beneficial treatment for patients with hypercholesterolemia, both in primary and secondary prevention, significantly reducing cardiovascular morbidity and mortality [40]. Recent studies have shown an interplay between statin therapy and the gut microbial landscape [41]. Sun et al found that patients with extensive bacterial heterogeneity – particularly Lactobacillus, Bifidobacterium, Faecalibacterium and Eubacterium species, known for their cholesterol lowering properties - showed better response to statin treatment, successfully lowering serum low density lipoprotein (LDLc) levels below 100 mg/dL within three months [42,43]. Likewise, Liu et al identified “good responders” – patients with a significant 58.9% reduction in LDLc - among those presenting high proportions of Firmicutes phylum [44]. Species from the Oscillibacter and Akkermansia genera have also been associated with cholesterol-lowering effects [45,46,47].
Another study conducted by Khan et al, though based on a relatively small sample size, suggested that atorvastatin may selectively restore anti-inflammatory bacteria, such as Akkermansia muciniphilia and Faecalibacterium prausnitzii, which in turn promote the growth of Oscillospira species. Although the atorvastatin treated group demonstrated lower bacterial diversity compared to healthy participants, a significant reduction of pro-inflammatory taxa and enrichment of anti-inflammatory phyla were observed [48]. In contrast, Kummen et al in a randomized controlled trial found only a modest effect of rosuvastatin use on gut microbiome composition on short term follow up of two to four weeks. While the sample size limited the ability to detect subtle microbial changes, a notable increase in pro-atherogenic microbiome derived metabolites was seen among patients with poor HDL/LDL ratio improvement, suggesting a link between statin response and microbiome activity [49]. Furthermore, Kaddurah-Daouk et al. demonstrated positive correlation between plasma simvastatin concentration and increased levels of secondary BAs, which predicted the cholesterol-lowering efficacy in good responders [50,51].
4.2. Angiotensin-Converting Enzyme Inhibitors/ Angiotensin Receptor Blockers
Renin-angiotensin-aldosterone system (RAAS) blockade remains the cornerstone in heart failure management and is active throughout the gastrointestinal tract. Both angiotensin receptors - type I (AT1R) and type II (AT2R) - are expressed in epithelial villi, submucosal layers, muscular layers, the myenteric plexus and local vasculature [52]. Accordingly, angiotensin receptor blockers (ARBs) and angiotensin-converting enzyme inhibitors (ACEIs) reduce intestinal wall rigidity, enhance villi length, decrease pro-inflammatory cytokine concentration, preserve gut barrier integrity, and improve microbial diversity – as pointed out in animal experiments [53]. Recent clinical research by Dong et al. assessed the effects of ACEI/ARB treatment on gut microbiome and metabolites. Although the study used a cross-sectional design and had a small sample size, it suggested that RAAS inhibition reduces pathogenic bacteria such as Enterobacter and Klebsiella, while promoting beneficial ones like Odoribacter. Additionally, significant metabolomic shifts were observed, with higher levels of inositol in the well-controlled group [54].
Furthermore, microbiome may play a significant role in the hydrolysis of quinapril and ramipril, reducing the concentration of active drug, while others, like lisinopril is less susceptible to microbial degradation [55]. These findings were revealed by Yang et al in a research on spontaneously hypertensive rats, demonstrating that, Coprococcus comes exhibits esterase activity, capable of directly breaking down esterified ACEIs (quinapril and ramipril), a phenomenon absent with non-ester ACEIs, such as lisinopril [56].
4.3. Cardiac Glycosides
Digoxin, the most commonly used cardiac glycoside, is largely prescribed for the treatment of heart failure and atrial fibrillation. It has been widely known for its marked interindividual variability in terms of bioavailability [57]. Emerging evidence shows that digoxin can be metabolized by the gut microbiome into an inactive form, dihydrodigoxin, in around 10% of patients [57,58]. The bacteria responsible for this inactivation was identified in the early 1980s as Eubacterium lentum, a member of the Actinobacteria phyla, later renamed as Eggerthella lenta [59]. In a 2014 study, Haiser et al. used RNA-sequencing to identify a two-gene operon encoding a cytochrome in E. lenta, referring as the cardiac glycoside reductase, which was significantly upregulated in the presence of digoxin. These genes were claimed to be a predictive microbial biomarker for digoxin inactivation [60]. Moreover, they showed that the growth of E. lenta is dependent on arginine levels, which both supports its proliferation and inhibits digoxin inactivation [61]. Consequently, increasing arginine levels – whether through dietary intake or from microbial source – may offer a reasonable strategy to prevent this undesired bacterial activity [62].
4.4. Antiplatelets
Aspirin, is a widely used antiplatelet agent in the prevention and treatment of CVD, acts by inhibiting cyclooxygenase-1 enzymes and prostaglandin synthesis. According to latest findings, aspirin causes gastrointestinal damage and toxicity in up to 90% of patients. Long-term aspirin treatment leads to alterations in gut microbiome composition, impacting bacterial genera like Prevotella, Bacteroides, Barnesiella as well as Ruminococcaceae family. In contrast, studies have suggested, that dysbiosis may also influence aspirin metabolism [63,64]. For instance, Parabacteroides goldsteinii was identified by Li and Ding et al. to have beneficial effect on restoring aspirin related intestinal layer damage by suppressing bile acid receptor FXR signaling. They further established that the growth of Parabacteroides goldsteinii is inhibited by aspirin [59,65]. Clopidogrel, another platelet agent, has also been associated with distinct microbial fingerprint and enhanced diversity, as shown in metagenomic analyses from large populational studies, including the Twins UK cohort [59].
4.5. Beta Blockers
Known as the fundamental treatment in heart failure, beta-blockers exert their effect through modulating the sympathetic nervous system, reducing morbidity and mortality in patients with heart failure [66,67]. Until recently, little was known about their interaction with the gut microbiome. Experimental models focusing on metabolism indicate that beta-blockers are not only able to reduce intestinal microbial diversity, but their pharmacokinetics can be notably influenced by specific microbial strains. Long-term users may reveal higher abundance of harmful microbial species, such as Streptococcus and Lactobacillus genera. [25]. In 2024 a research published by Shearer et al. involving 134 participants diagnosed with cardiometabolic disease, found that beta-blocker therapy contributed to the depletion of Akkermansia muciniphila and compromised the activity of Egerthella lenta, both of which are important for energy metabolism and immune regulation [68]. However, other findings from animal models suggest that when beta-blockers used in combination with other heart failure medication, such as diuretics, ACEIs or aspirin they may enhance the abundance of butyrate-producing bacteria like Roseburia genus, contributing to additive blood pressure-lowering effects [69].
4.6. Other Classes of Heart Failure Drugs
Additional cardiovascular drugs may also modulate gut function. For example, a randomized, open-label clinical trial by Deng et al. found that patients with type 2 diabetes and several CVD risk factors treated with empagliflozin, express higher microbiome diversity. They reported a significant shift in favor of SCFAs producing bacteria, including Roseburia, Eubacterium, and Faecalibacterium [70].
Similarly, spironolactone as well facilitates the restoration of SCFAs producing bacterial species, supports Firmicutes/Bacteroidetes ratio, and reduces systemic inflammation, thus helping maintain eubiosis [36,52]. The first evidence of spironolactone’s dysbiosis reducing effect was provided by González-Correa et al. in a study on spontaneously hypertensive rats followed by a five-week treatment. As a result, administration of spironolactone lead to the restoration of acetate-producing Bacteroides and Prevotella genus on one hand and decreased the concentration of butyrate-producing bacteria on the other hand, especially Eubacteriacea family and Clostridiales order [71].
Finally, a few attempts have been made to investigate novel heart failure drugs, such as the sacubitril/valsartan combination and microbiome interactions, though these findings remain preliminary. Animal models have shown that sacubitril/valsartan treated diabetic mice exhibit reduced harmful bacterial genus like Escherichia and Shigella, and express increased proliferation of others with beneficial traits, such as Lactobacillus, Bacteroides, and Parabacteroides, potentially supporting gut barrier integrity and promoting SCFA production [72]. (Table 1)
5. Limitations and Future Directions
Due to significant development in metagenomics and next-generation sequencing, there has been an escalation in gut microbiome research over the past two decades [73]. Numerous preclinical and clinical studies have reported interrelation between changes in intestinal microbiome composition and its metabolic function. However, the underlying molecular mechanisms responsible for host-microbiome interactions remain only partially understood [74]. Although there is an undoubtful association between cardiovascular pathology and microbiome activity - highlighting the significance of the gut-heart axis - the complex, bidirectional dynamics and pathophysiological mechanisms involved in drug-microbiota interactions are far from straightforward [75]. Researches utilizing metagenomic sequencing techniques have uncovered correlations between medication consumption and gut microbial alterations. Nevertheless, the multifactorial nature of pharmacogenomic and microbiome-mediated interactions remains insufficiently elucidated [76].
Current data emphasize the detrimental impact of gut barrier dysfunction in the development and progression of CVD, particularly in relation to atherosclerosis, coronary artery disease, heart failure and hypertension. Still, these results are essentially associative, rather than casual, limiting the strength of clinical conclusions [18]. It appears that in patients with heart failure, atherosclerotic CVD, or hypertension, the altered gut microbial ecosystem influences oral drug bioavailability – a phenomenon mostly established in preclinical settings [77,78]. Hence, large randomized controlled trials and multi-omics profiling are needed, in order to shift the focus on potential causation [79,80]. Clinical translation of current findings is further impeded by the lack of precise methodological design, small sample size, short follow-up and disregard of various confounding factors - such as polypharmacy, drug-drug interactions, medication dosage and formulation, and individual variability in drug response [81,82].
Overall, cardiovascular disease management is shifting towards a more personalized care, potentially integrating genetic, epigenetic, and microbiome-based approaches. Pharmacomicrobiomics represents a promising frontier in the new era of individualized medicine [62,83]. The integration of microbiome analysis into clinical settings may enable the prediction of drug responses, minimization of adverse effects and optimization of cardiovascular therapy – ultimately supporting patient outcomes. (Table 2)
6. Conclusions
Long-term treatment of heart failure patients requires a complex and dynamic therapeutical strategy based on pharmacological interventions. Yet, in the light of recent researches, there is a need to take into consideration implications of gut microbial changes in pharmacological mechanisms, while applying the targeted, scientifically well-founded CV medication. The future outlook is the identification of specific bacterial genes and phyla in order to anticipate drug metabolism, or the development of new biomarkers aimed to lead treatment decisions. Exploring the unique microbial profile of an individual may expand medical treatments with strategies able to modify the patient’s microbiome. Including specific probiotics and prebiotics or even selected antibiotics might be beneficial to enhance drug efficacy and safety. However, due to the extensive inter-individual variability of the microbiome makeup, influenced by lifestyle, diet, environment, medical conditions and polypharmacy, major challenges arise when studying the microbiome. There is an undoubted need for well-designed studies with systematic patient selection and standardized sample collection to reduce the overload of these variables in order to optimize cardiovascular therapeutical efficacy alongside microbiome health.
Author Contributions
Conceptualization, A.R. and A.F.; writing—original draft preparation, A.R.; writing—review and editing, A.R., A.F., and A.M; figure ideation and creation, A.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CVD | Cardiovascular disease |
| MetaHIT | Metagenomics of the Human Intestinal Tract |
| TNF-α | Tumor necrosis factor alfa |
| IFN-γ | Interferon gamma |
| TMAO | Trimethylamine-N-oxide |
| SCFAs | Short-chain fatty acids |
| SBAs | Secondary bile acids |
| MACE | Major Adverse Cardiac Events |
| BNP | B-type natriuretic peptide |
| FXR | Farnesoid X receptor |
| TGR5 | Takeda G protein-coupled receptor 5 |
| LDL | Low-Density Lipoprotein |
| HDL | High-Density Lipoprotein |
| RAAS | Renin-angiotensin-aldosterone system |
| AT1R | Angiotensin 1 receptor |
| AT2R | Angiotensin 2 receptor |
| ARBs | Angiotensin receptor blockers |
| ACEIs | Angiotensin receptor inhibitors |
References
- Longoria CR, Guers JJ, Campbell SC. The Interplay between Cardiovascular Disease, Exercise, and the Gut Microbiome. Rev Cardiovasc Med. 2022;23(11):365. Published 2022 Oct 27. [CrossRef]
- Astudillo AA, Mayrovitz HN. The Gut Microbiome and Cardiovascular Disease. Cureus. 2021;13(4):e14519. Published 2021 Apr 16. [CrossRef]
- Li, X. , Ma, Y., Zhang, C., Liu, C., Shi, Y., Wang (2024). Genome-wide association analysis of gut microbiome and serum metabolomics identifies heart failure therapeutic targets.
- Du Y, Li X, Su C, Wang L, Jiang J, Hong B. The human gut microbiome - a new and exciting avenue in cardiovascular drug discovery. Expert Opin Drug Discov. 2019;14(10):1037-1052. [CrossRef]
- Vieira-Silva S, Falony G, Belda E, et al. Statin therapy is associated with lower prevalence of gut microbiota dysbiosis. Nature. 2020;581(7808):310-315. [CrossRef]
- Mishima E, Abe T. Role of the microbiota in hypertension and antihypertensive drug metabolism. Hypertens Res. 2022;45(2):246-253. [CrossRef]
- Xiong Y, Zhu P, et al. The Role of Gut Microbiota in Hypertension Pathogenesis and the Efficacy of Antihypertensive Drugs. Curr Hypertens Rep. 2021;23(8):40. Published 2021 Sep 6. [CrossRef]
- Li W, Li C, Ren C, et al. Bidirectional effects of oral anticoagulants on gut microbiota in patients with atrial fibrillation. Front Cell Infect Microbiol. 2023;13:1038472. Published 2023 Mar 24. [CrossRef]
- Novakovic M, Rout A, Kingsley T, et al. Role of gut microbiota in cardiovascular diseases. World J Cardiol. 2020;12(4):110-122. [CrossRef]
- Zhou W, Cheng Y, Zhu P, Nasser MI, Zhang X, Zhao M. Implication of Gut Microbiota in Cardiovascular Diseases. Oxid Med Cell Longev. 2020;2020:5394096. Published 2020 Sep 26. [CrossRef]
- Battson ML, Lee DM, Weir TL, Gentile CL. The gut microbiota as a novel regulator of cardiovascular function and disease. J Nutr Biochem. 2018;56:1-15. [CrossRef]
- Morrison, Mark, Murtaza, Nida Talley, Nicholas J. Pimentel, Mark Mathur, Ruchi Barlow, Gillian M. 2023, Clinical Understanding of the Human Gut Microbiome, The Importance of the Microbiome in the Gut p 1- 11, Springer Nature Switzerland.
- Papadopoulos PD, Tsigalou C, Valsamaki PN, Konstantinidis TG, Voidarou C, Bezirtzoglou E. The Emerging Role of the Gut Microbiome in Cardiovascular Disease: Current Knowledge and Perspectives. Biomedicines. 2022;10(5):948. Published 2022 Apr 20. [CrossRef]
- Abdulrahim AO, Doddapaneni NSP, Salman N, et al. The gut-heart axis: a review of gut microbiota, dysbiosis, and cardiovascular disease development. Ann Med Surg (Lond). 2025;87(1):177-191. Published 2025 Jan 9. [CrossRef]
- Witkowski M, Weeks TL, Hazen SL. Gut Microbiota and Cardiovascular Disease. Circ Res. 2020;127(4):553-570. [CrossRef]
- Cheng CK, Huang Y. The gut-cardiovascular connection: new era for cardiovascular therapy. Med Rev (2021). 2021 Oct 21;1(1):23-46.
- Rahman MM, Islam F, -Or-Rashid MH, et al. The Gut Microbiota (Microbiome) in Cardiovascular Disease and Its Therapeutic Regulation. Front Cell Infect Microbiol. 2022;12:903570. Published 2022 Jun 20. [CrossRef]
- Lewis CV, Taylor WR. Intestinal barrier dysfunction as a therapeutic target for cardiovascular disease. Am J Physiol Heart Circ Physiol. 2020;319(6):H1227-H1233. [CrossRef]
- Duttaroy AK. Role of Gut Microbiota and Their Metabolites on Atherosclerosis, Hypertension and Human Blood Platelet Function: A Review. Nutrients. 2021;13(1):144. Published 2021 Jan 3. [CrossRef]
- Wang Z, Klipfell E, Bennett BJ, et al. Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature. 2011;472(7341):57-63. [CrossRef]
- Ahmad AF, Dwivedi G, O'Gara F, Caparros-Martin J, Ward NC. The gut microbiome and cardiovascular disease: current knowledge and clinical potential. Am J Physiol Heart Circ Physiol. 2019;317(5):H923-H938. [CrossRef]
- Tang WHW, Bäckhed F, Landmesser U, Hazen SL. Intestinal Microbiota in Cardiovascular Health and Disease: JACC State-of-the-Art Review. J Am Coll Cardiol. 2019;73(16):2089-2105. [CrossRef]
- Matter CM, Stähli BE, Scharl M. The Gut–Heart Axis: Effects of Intestinal Microbiome Modulation on Cardiovascular Disease—Ready for Therapeutic Interventions? International Journal of Molecular Sciences. 2024; 25(24):13529. [CrossRef]
- Tang WHW, Hazen SL. Unraveling the Complex Relationship Between Gut Microbiome and Cardiovascular Diseases. Circulation. 2024;149(20):1543-1545. [CrossRef]
- Dharmarathne G, Kazi S, King S, Jayasinghe TN. The Bidirectional Relationship Between Cardiovascular Medications and Oral and Gut Microbiome Health: A Comprehensive Review. Microorganisms. 2024;12(11):2246. Published 2024 Nov 6. [CrossRef]
- Jansen VL, Gerdes VE, Middeldorp S, van Mens TE. Gut microbiota and their metabolites in cardiovascular disease. Best Pract Res Clin Endocrinol Metab. 2021;35(3):101492. [CrossRef]
- Avery EG, Bartolomaeus H, Maifeld A, et al. The Gut Microbiome in Hypertension: Recent Advances and Future Perspectives. Circ Res. 2021;128(7):934-950. [CrossRef]
- BNF (British Nutrition Foundation), Sara Stanner, Sarah Coe, Keith N. Frayn, Cardiovascular Disease: Diet, Nutrition and Emerging Risk Factors, 2nd Edition, December 2018, Wiley-Blackwell, pages 276-277.
- Lupu VV, Adam Raileanu A, Mihai CM, et al. The Implication of the Gut Microbiome in Heart Failure. Cells. 2023;12(8):1158. Published 2023 Apr 14. [CrossRef]
- Cao H, Zhu Y, Hu G, Zhang Q, Zheng L. Gut microbiome and metabolites, the future direction of diagnosis and treatment of atherosclerosis?. Pharmacol Res. 2023;187:106586. [CrossRef]
- Zaher A, Elsaygh J, Peterson SJ, Weisberg IS, Parikh MA, Frishman WH. The Interplay of Microbiome Dysbiosis and Cardiovascular Disease. Cardiol Rev. Published online April 26, 2024. [CrossRef]
- Oniszczuk A, Oniszczuk T, Gancarz M, Szymańska J. Role of Gut Microbiota, Probiotics and Prebiotics in the Cardiovascular Diseases. Molecules. 2021;26(4):1172. Published 2021 Feb 22. [CrossRef]
- Rajendiran E, Ramadass B, Ramprasath V. Understanding connections and roles of gut microbiome in cardiovascular diseases. Can J Microbiol. 2021;67(2):101-111. [CrossRef]
- Al Samarraie A, Pichette M, Rousseau G. Role of the Gut Microbiome in the Development of Atherosclerotic Cardiovascular Disease. Int J Mol Sci. 2023;24(6):5420. Published 2023 Mar 12. [CrossRef]
- Branchereau M, Burcelin R, Heymes C. The gut microbiome and heart failure: A better gut for a better heart. Rev Endocr Metab Disord. 2019;20(4):407-414. [CrossRef]
- Gao K, Wang PX, Mei X, Yang T, Yu K. Untapped potential of gut microbiome for hypertension management. Gut Microbes. 2024;16(1):2356278. [CrossRef]
- Chen HQ, Gong JY, Xing K, Liu MZ, Ren H, Luo JQ. Pharmacomicrobiomics: Exploiting the Drug-Microbiota Interactions in Antihypertensive Treatment. Front Med (Lausanne). 2022;8:742394. Published 2022 Jan 19. [CrossRef]
- Weersma RK, Zhernakova A, Fu J. Interaction between drugs and the gut microbiome. Gut. 2020;69(8):1510-1519. [CrossRef]
- Stepanov, M. S. (2024). Influence of intestinal microbiota on the metabolism of main cardiotropic drugs. Perm Medical Journal, 41(5), 54-65. [CrossRef]
- Zimmermann F, Roessler J, Schmidt D, et al. Impact of the Gut Microbiota on Atorvastatin Mediated Effects on Blood Lipids. J Clin Med. 2020;9(5):1596. Published 2020 May 25. [CrossRef]
- Wilmanski T, Kornilov SA, Diener C, et al. Heterogeneity in statin responses explained by variation in the human gut microbiome. Med. 2022;3(6):388-405.e6. [CrossRef]
- Dias AM, Cordeiro G, Estevinho MM, et al. Gut bacterial microbiome composition and statin intake-A systematic review. Pharmacol Res Perspect. 2020;8(3):e00601. [CrossRef]
- Sun B, Li L, Zhou X. Comparative analysis of the gut microbiota in distinct statin response patients in East China. J Microbiol. 2018;56(12):886-892. [CrossRef]
- Eid HM, Wright ML, Anil Kumar NV, et al. Significance of Microbiota in Obesity and Metabolic Diseases and the Modulatory Potential by Medicinal Plant and Food Ingredients. Front Pharmacol. 2017;8:387. Published 2017 Jun 30. [CrossRef]
- Shi L, Liu X, Li E, Zhang S, Zhou A. Association of lipid-lowering drugs with gut microbiota: A Mendelian randomization study. J Clin Lipidol. 2024;18(5):e797-e808. [CrossRef]
- Tian Y, Wu G, Zhao X, et al. Probiotics combined with atorvastatin administration in the treatment of hyperlipidemia: A randomized, double-blind, placebo-controlled clinical trial. Medicine (Baltimore). 2024;103(21):e37883. [CrossRef]
- Suresh, Mithil Gowda1; Mohamed, Safia2; Yukselen, Zeynep1; Hatwal, Juniali3; Venkatakrishnan, Abhinaya4; Metri, Aida5; Bhardwaj, Arshia6; Singh, Arshdeep6; Bush, Nikhil7; Batta, Akash8. Therapeutic Modulation of Gut Microbiome in Cardiovascular Disease: A Literature Review. Heart and Mind 9(1):p 68-79, Jan–Feb 2025. [CrossRef]
- Khan TJ, Ahmed YM, Zamzami MA, et al. Atorvastatin Treatment Modulates the Gut Microbiota of the Hypercholesterolemic Patients. OMICS. 2018;22(2):154-163. [CrossRef]
- Kummen M, Solberg OG, Storm-Larsen C, et al. Rosuvastatin alters the genetic composition of the human gut microbiome. Sci Rep. 2020;10(1):5397. Published 2020 Mar 25. [CrossRef]
- Kaddurah-Daouk R, Baillie RA, Zhu H, et al. Enteric microbiome metabolites correlate with response to simvastatin treatment [published correction appears in PLoS One. 2013;8(5). https://doi.org/10.1371/annotation/8e8e95ca-1ac3-4acf-abcb-223cd11ac1c1]. PLoS One. 2011;6(10):e25482. [CrossRef]
- Wang L, Wang Y, Wang H, et al. The influence of the intestinal microflora to the efficacy of Rosuvastatin. Lipids Health Dis. 2018;17(1):151. Published 2018 Jun 30. [CrossRef]
- Lucas SE, Walton SL, Mirabito Colafella KM, Mileto SJ, Lyras D, Denton KM. Antihypertensives and Antibiotics: Impact on Intestinal Dysfunction and Hypertension. Hypertension. 2023;80(7):1393-1402. [CrossRef]
- González-Correa C, Moleón J, Miñano S, et al. Differing contributions of the gut microbiota to the blood pressure lowering effects induced by first-line antihypertensive drugs. Br J Pharmacol. 2024;181(18):3420-3444. [CrossRef]
- Dong Y, Wang P, Jiao J, Yang X, Chen M, Li J. Antihypertensive Therapy by ACEI/ARB Is Associated With Intestinal Flora Alterations and Metabolomic Profiles in Hypertensive Patients. Front Cell Dev Biol. 2022;10:861829. Published 2022 Mar 23. [CrossRef]
- Kyoung J, Atluri RR, Yang T. Resistance to Antihypertensive Drugs: Is Gut Microbiota the Missing Link?. Hypertension. 2022;79(10):2138-2147. [CrossRef]
- Yang T, Mei X, Tackie-Yarboi E, et al. Identification of a Gut Commensal That Compromises the Blood Pressure-Lowering Effect of Ester Angiotensin-Converting Enzyme Inhibitors. Hypertension. 2022;79(8):1591-1601. [CrossRef]
- Zhang X, Han Y, Huang W, Jin M, Gao Z. The influence of the gut microbiota on the bioavailability of oral drugs. Acta Pharm Sin B. 2021;11(7):1789-1812. [CrossRef]
- Vázquez-Baeza Y, Callewaert C, Debelius J, et al. Impacts of the Human Gut Microbiome on Therapeutics. Annu Rev Pharmacol Toxicol. 2018;58:253-270. [CrossRef]
- Steiner HE, Gee K, Giles J, Knight H, Hurwitz BL, Karnes JH. Role of the gut microbiome in cardiovascular drug response: The potential for clinical application. Pharmacotherapy. 2022;42(2):165-176. [CrossRef]
- Haiser HJ, Seim KL, Balskus EP, Turnbaugh PJ. Mechanistic insight into digoxin inactivation by Eggerthella lenta augments our understanding of its pharmacokinetics. Gut Microbes. 2014;5(2):233-238. [CrossRef]
- Zhao Q, Chen Y, Huang W, Zhou H, Zhang W. Drug-microbiota interactions: an emerging priority for precision medicine. Signal Transduct Target Ther. 2023;8(1):386. Published 2023 Oct 9. [CrossRef]
- Curini L, Amedei A. Cardiovascular Diseases and Pharmacomicrobiomics: A Perspective on Possible Treatment Relevance. Biomedicines. 2021;9(10):1338. Published 2021 Sep 28. [CrossRef]
- Alhajri N, Khursheed R, Ali MT, et al. Cardiovascular Health and The Intestinal Microbial Ecosystem: The Impact of Cardiovascular Therapies on The Gut Microbiota. Microorganisms. 2021;9(10):2013. Published 2021 Sep 23. [CrossRef]
- Tuteja S, Ferguson JF. Gut Microbiome and Response to Cardiovascular Drugs. Circ Genom Precis Med. 2019;12(9):421-429. [CrossRef]
- Li T, Ding N, Guo H, et al. A gut microbiota-bile acid axis promotes intestinal homeostasis upon aspirin-mediated damage. Cell Host Microbe. 2024;32(2):191-208.e9. [CrossRef]
- Romano KA, Nemet I, Prasad Saha P, et al. Gut Microbiota-Generated Phenylacetylglutamine and Heart Failure. Circ Heart Fail. 2023;16(1):e009972. [CrossRef]
- Authors/Task Force Members:; McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, Burri H, Butler J, Čelutkienė J, Chioncel O, Cleland JGF, Coats AJS, Crespo-Leiro MG, Farmakis D, Gilard M, Heymans S, Hoes AW, Jaarsma T, Jankowska EA, Lainscak M, Lam CSP, Lyon AR, McMurray JJV, Mebazaa A, Mindham R, Muneretto C, Francesco Piepoli M, Price S, Rosano GMC, Ruschitzka F, Kathrine Skibelund A; ESC Scientific Document Group. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2022 Jan;24(1):4-131.
- Shearer J, Shah S, Shen-Tu G, Schlicht K, Laudes M, Mu C. Microbial Features Linked to Medication Strategies in Cardiometabolic Disease Management. ACS Pharmacol Transl Sci. 2024;7(4):991-1001. Published 2024 Feb 5. [CrossRef]
- Zheng T, Marques FZ. Gut Microbiota: Friends or Foes for Blood Pressure-Lowering Drugs. Hypertension. 2022 Aug;79(8):1602-1604. [CrossRef]
- Deng X, Zhang C, Wang P, et al. Cardiovascular Benefits of Empagliflozin Are Associated With Gut Microbiota and Plasma Metabolites in Type 2 Diabetes [published correction appears in J Clin Endocrinol Metab. 2022 Nov 23;107(11):e4330. https://doi.org/10.1210/clinem/dgac506.]. J Clin Endocrinol Metab. 2022;107(7):1888-1896. [CrossRef]
- González-Correa C, Moleón J, Miñano S, et al. Mineralocorticoid receptor blockade improved gut microbiota dysbiosis by reducing gut sympathetic tone in spontaneously hypertensive rats. Biomed Pharmacother. 2023;158:114149. [CrossRef]
- Wang P, Guo R, Bai X, et al. Sacubitril/Valsartan contributes to improving the diabetic kidney disease and regulating the gut microbiota in mice. Front Endocrinol (Lausanne). 2022;13:1034818. Published 2022 Dec 16. [CrossRef]
- Cuervo L, McAlpine PL, Olano C, Fernández J, Lombó F. Low-Molecular-Weight Compounds Produced by the Intestinal Microbiota and Cardiovascular Disease. Int J Mol Sci. 2024;25(19):10397. Published 2024 Sep 27. [CrossRef]
- Schiattarella GG, Sannino A, Esposito G, Perrino C. Diagnostics and therapeutic implications of gut microbiota alterations in cardiometabolic diseases. Trends Cardiovasc Med. 2019;29(3):141-147. [CrossRef]
- Tang WHW, Li DY, Hazen SL. Dietary metabolism, the gut microbiome, and heart failure. Nat Rev Cardiol. 2019;16(3):137-154. [CrossRef]
- Vich Vila A, Collij V, Sanna S, et al. Impact of commonly used drugs on the composition and metabolic function of the gut microbiota. Nat Commun. 2020;11(1):362. Published 2020 Jan 17. [CrossRef]
- Paraskevaidis I, Briasoulis A, Tsougos E. Oral Cardiac Drug-Gut Microbiota Interaction in Chronic Heart Failure Patients: An Emerging Association. Int J Mol Sci. 2024;25(3):1716. Published 2024 Jan 31. [CrossRef]
- Mamic P, Chaikijurajai T, Tang WHW. Gut microbiome - A potential mediator of pathogenesis in heart failure and its comorbidities: State-of-the-art review. J Mol Cell Cardiol. 2021;152:105-117. [CrossRef]
- Trøseid M, Andersen GØ, Broch K, Hov JR. The gut microbiome in coronary artery disease and heart failure: Current knowledge and future directions. EBioMedicine. 2020;52:102649. [CrossRef]
- Vallianou NG, Geladari E, Kounatidis D. Microbiome and hypertension: where are we now?. J Cardiovasc Med (Hagerstown). 2020;21(2):83-88. [CrossRef]
- Muralitharan RR, Buikema JW, Marques FZ. Minimizing gut microbiome confounding factors in cardiovascular research. Cardiovasc Res. 2024;120(15):e60-e62. [CrossRef]
- Mamic P, Snyder M, Tang WHW. Gut Microbiome-Based Management of Patients With Heart Failure: JACC Review Topic of the Week. J Am Coll Cardiol. 2023;81(17):1729-1739. [CrossRef]
- Zimmermann M, Zimmermann-Kogadeeva M, Wegmann R, Goodman AL. Mapping human microbiome drug metabolism by gut bacteria and their genes. Nature. 2019;570(7762):462-467. [CrossRef]
Figure 1.
Microbiome-derived metabolite production in cardiovascular disease (created by images from Smart Servier Medical Art).
Figure 1.
Microbiome-derived metabolite production in cardiovascular disease (created by images from Smart Servier Medical Art).
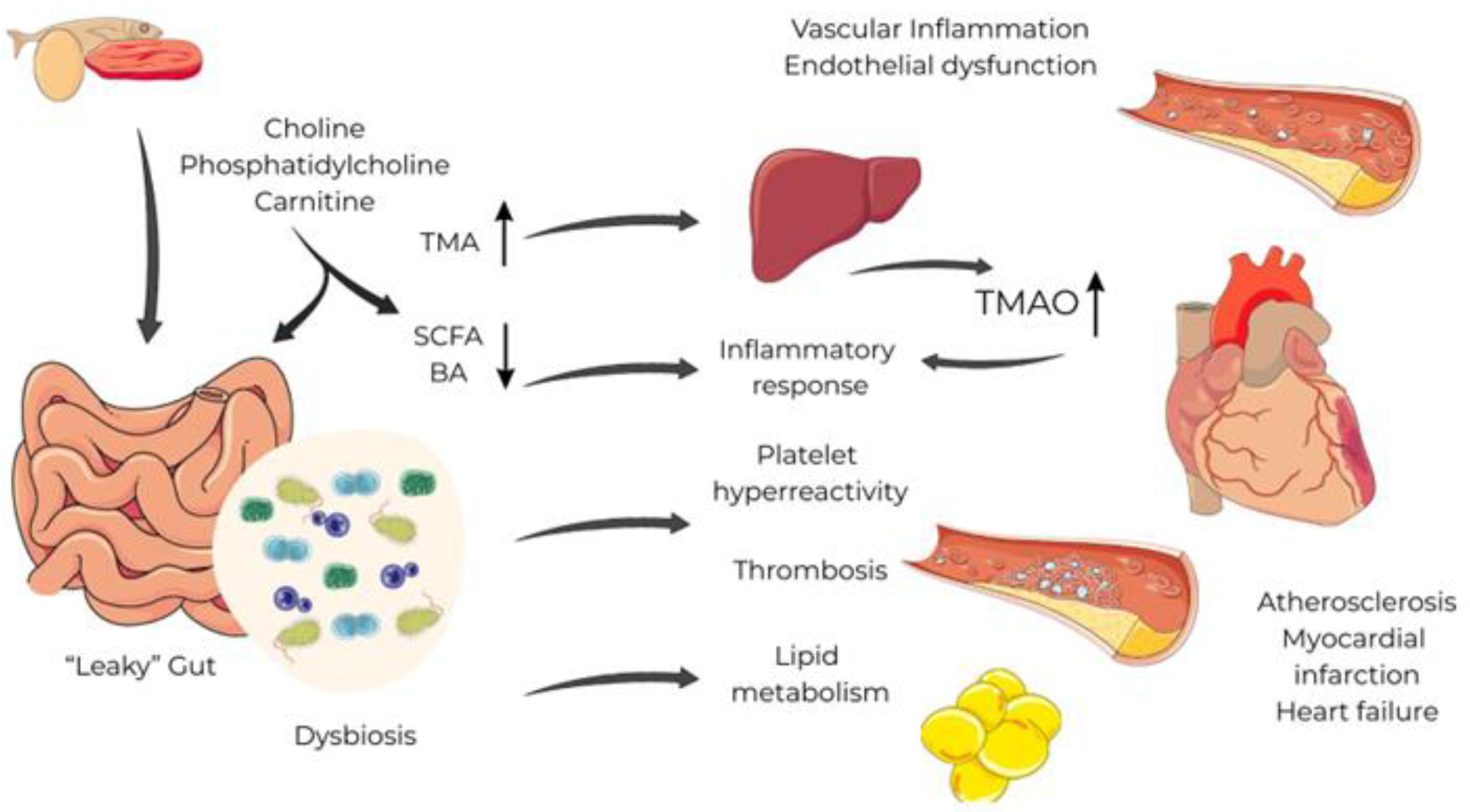
Figure 2.
Possible interactions between drugs and gut microbiome (created by images from Smart Servier Medical Art).
Figure 2.
Possible interactions between drugs and gut microbiome (created by images from Smart Servier Medical Art).
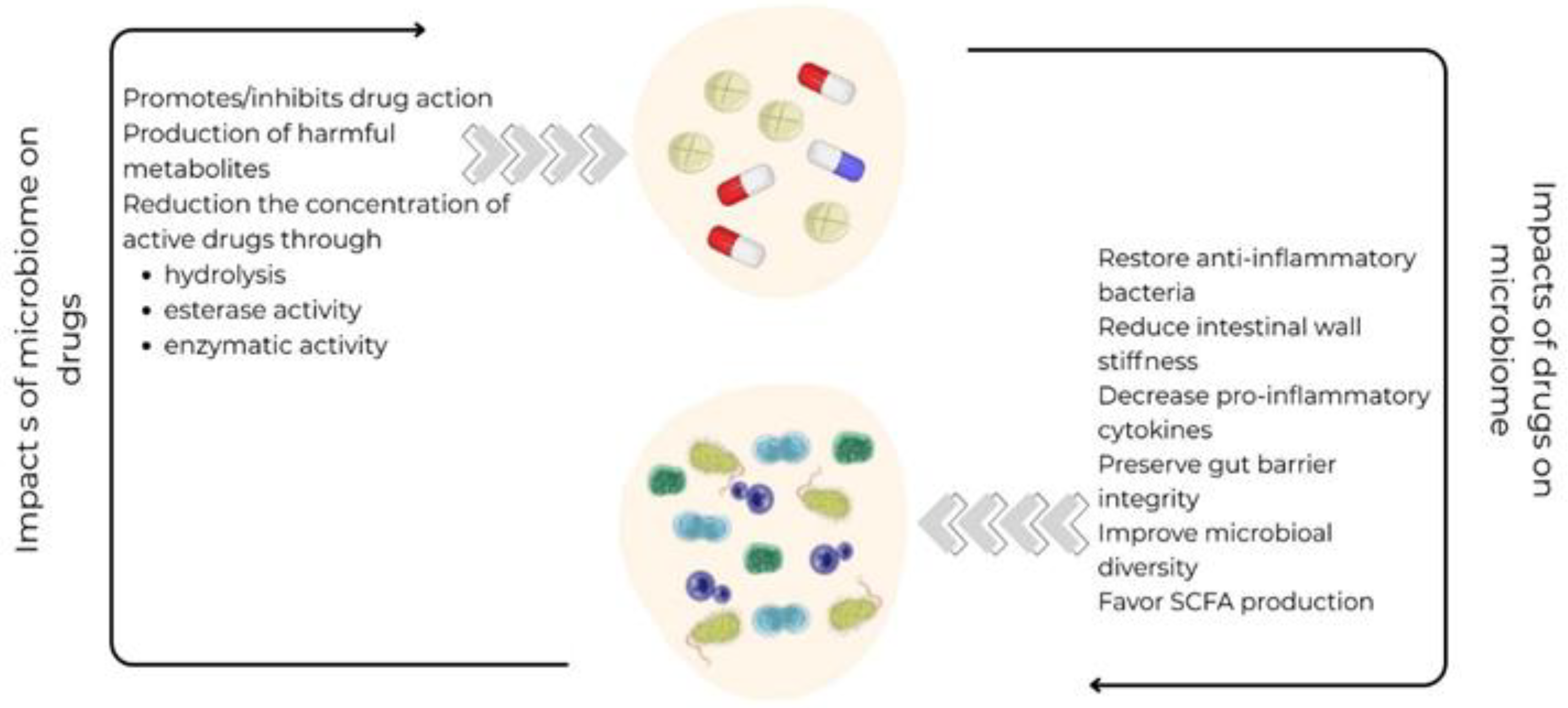

Table 1.
Microbial changes induced by heart failure medication.
| Drug effect | Microbial strain |
|---|---|
| Statins |
↑Lactobacillus ↑Bifidobacterium ↑Faecalibacterium ↑Eubacterium |
| ACEI/ARB |
↓Enterobacter ↓Klebsiella ↑Odoribacter |
| Aspirin |
↓Parabacteroides goldsteinii ↓Prevotella ↓Ruminococcaceae ↓Bacteroides ↓Barnesiella |
| Beta-blockers |
↑Streptococcus ↑Lactobacillus ↓Akkermansia muciniphila ↓Eggerthella lenta |
| Beta-blockers+aspirin/diuretics |
↑Roseburia |
| Empagliflozin |
↑Roseburia ↑Eubacterium ↑Faecalibacterium |
| Spironolactone |
↑Bacteroides ↑Prevotella ↓Eubacteriacea ↓Clostridiales |
| Sacubitril/Valsartan |
↓Escherichia ↓Shigella ↑Lactobacillus ↑Bacteroides ↑Parabacteroides |
Table 2.
Relevant articles included in this review.
| Study | Year of publication | Study design | Results |
Future insights |
|---|---|---|---|---|
| Sun et al. [43] | 2018 | Clinical trial involving hypercholesterolemic patients treated with atorvastatin. It compares the composition of gut microbiota between statin sensitive and resistant groups. |
Gut microbiota composition differs significantly between statin sensitive and statin resistant patients. The statin sensitive group exhibited higher biodiversity compared to resistant group. Increased Lactobacillus, Eubacterium, Faecalibacterium, and Bifidobacterium. Decreased proportion of Clostridium. |
The impact of genetic polymorphisms on statin pharmacodynamics remains a significant area of research. Further studies could assess how different bacterial taxa influence statin efficacy and dosage adjustments. |
| Shi et al. [45] | 2024 | A Mendelian randomization two-sample design, which utilizes genetic variants to estimate the impact of lipid-lowering medication on gut microbiota diversity. |
Different genetic proxies for lipid-lowering drugs affects the abundance of gut microbiota. Some has been associated with an increase in the genus Eggerthella. Others were linked to the order Pasteurellales and the genus Haemophilus. |
Studies using individual-level data are needed for comprehensive insights on associations. Investigating the effects of lipid-lowering drugs across different patient subgroups is necessary. |
| Tian et al. [46] | 2024 | A randomized, double-blind, placebo-controlled, parallel-group trial aimed to assess the role of probiotics in treating hyperlipidemia. |
Probiotics reduced total cholesterol, triglycerides, and LDLc- levels in patients with hyperlipidemia. Probiotics increased Tenericutes and reduced Proteobacteria at the phylum level. Increased the abundance of Bifidobacterium, Lactobacillus, and Akkermansia genus, and decreased Escherichia, Eggerthella, and Sutterella. |
Future research should explore different probiotic strains and long-term effects. Larger, multi-center clinical trials are warranted to confirm findings. |
| Suresh et al. [47] | 2024 | A systematic review and meta-analysis of randomized controlled trials including clinical and observational studies, focusing on the gut microbiome and SCFAs. |
SCFAs are identified as beneficial in decreasing CVD risk factors. |
Investigating the long-term impacts of microbiome manipulation on cardiovascular health is essential. Understanding the interactions between cardiovascular medications and the gut microbiome has potentials to optimize treatment efficacy. |
| Khan et al. [48] | 2018 | A cross-sectional observational study that compares gut microbiota analyses among three groups: untreated hypercholesterolemic patients, atorvastatin-treated patients, and healthy subjects. |
Atorvastatin treatment increased anti-inflammatory bacteria, A. muciniphila and F. prausnitzii, and decreased the levels of proinflammatory taxa, such as members of Proteobacteria phylum, in hypercholesterolemic patients. |
Future studies should focus on the specific mechanisms by which gut microbiota influences lipid metabolism and inflammation. |
| Kummen et al. [49] | 2020 | A randomized controlled trial assessing the effects of rosuvastatin on gut microbiome composition. |
Rosuvastatin treatment showed no significant changes in gut microbial diversity. Reduced potential to metabolize TMAO precursors. |
Re-analyzing TMAO-related metabolites in previous statin trials could provide valuable insights. Exploring the mechanisms behind the pleiotropic effects of statins may enhance understanding of their impact on the microbiome. |
| Kaddurah-Daouk et al. [50] | 2011 | Clinical investigation aiming to elucidate variability in statin response through metabolomic profiling. |
Increased simvastatin levels correlated with higher BAs concentrations. |
Further research should focus on the interactions between genome, microbiome, and environmental factors in cardiovascular disease management. |
| Wang L et al. [51] | 2018 | An experimental investigation involving rat models to analyze the effects of intestinal microflora on lipid-reduction efficacy of rosuvastatin. |
Intestinal microflora significantly alters the lipid-reduction efficacy of rosuvastatin. Lactobacillus and Bifidobacterium populations were markedly reduced when antibiotics were associated to rosuvastatin treatment. Microbiome diversity recovered four weeks post-antibiotic treatment, restoring the efficacy of statin treatment. |
Investigating the long-term effects of antibiotic treatment on intestinal microflora diversity and lipid metabolism is essential. The role of specific probiotics in enhancing the efficacy of rosuvastatin call for further investigation. |
| Dong et al. [54] | 2022 | A cross-sectional analysis including patients with hypertension to evaluate the effects of ACEI/ARBs on gut microbiome and metabolites. |
ACEI/ARBs therapy reduces pathogenic bacteria like Enterobacter and Klebsiella while increasing beneficial ones such as Odoribacter. |
Research is needed to monitor dynamic changes in microbial and metabolic features between well-controlled hypertensive patients and healthy subjects using ACEI/ARBs. |
| Yang et al. [56] | 2022 | Preclinical research using spontaneously hypertensive rats to assess the effects of gut microbiota on antihypertensive medications. |
Gut microbiome can reduce the antihypertensive effect of quinapril in spontaneously hypertensive rats treated with antibiotics. Coprococcus comes catabolizes ester ACE inhibitors, lowering their effectiveness. |
In vivo researches are needed to investigate the impact of gut microbiota on antihypertensive medication effects. Identifying specific gut microbes could unveil new therapeutic strategies for resistant hypertension. |
| Steiner et al. [59] | 2022 | The paper discusses guidelines for reporting gut microbiome analysis in experimental hypertension. |
Various cardiovascular drugs, like captopril and aspirin, interact with gut microbiota, affecting their pharmacokinetics. |
Research should assess the impact of microbiome alterations on drug response variability across demographics and comorbidities. Advanced sequencing and computational techniques may better characterize the relationship of microbiome and cardiovascular drug therapy. |
| Haiser et al. [60] | 2014 | The research integrates gut microbiome studies into personalized medicine through various experimental approaches, involving human intervention studies and gnotobiotic mouse experiments. | The study identified a cytochrome-encoding operon in Eggerthella lenta, activated by digoxin, serving as a microbial biomarker for drug inactivation |
Investigating the predictive value of specific operon abundance on digoxin pharmacokinetics in diverse patient populations is essential. Human intervention trials are needed to explore co-therapy strategies. The application of this framework to other drugs influenced by gut microbiota is also suggested. |
| Li et al. [65] | 2024 | The study is a combination of clinical and experimental research, utilizing both human cohorts and animal models. |
Aspirin treatment significantly decreased the abundance of Parabacteroides, particularly Parabacteroides goldsteinii, in healthy individuals. Mice supplemented with Parabacteroides goldsteinii showed reduced aspirin-mediated intestinal damage. |
Future research should focus on exploring the function of specific genes found in the genomes of various microorganisms. Understanding the mechanisms by which Parabacteroides species contribute to BAs metabolism and gut health. |
| Shearer et al. [68] | 2024 | A population-based cohort study, involving 134 middle-aged adults diagnosed with cardiometabolic disease, focusing on the relationship between medication use and gut microbiota composition. |
46 associations were identified between microbial composition and single medications, including β-blockers and statins depleting Akkermansia muciniphila. Increasing medication use correlated negatively with α-diversity in gut microbiota among participants. |
Future research could utilize fecal metabolomics profiling to confirm functional changes in gut microbiota. Further exploration of the relationship between medications and gut microbiota at genus and species levels is warranted. |
| Deng et al. [70] | 2022 | Randomized, open-label, two-arm clinical trial which included treatment-naive patients with type 2 diabetes and cardiovascular risk factors. |
Significant reductions were found in glycated hemoglobin levels in both empagliflozin and metformin groups. Empagliflozin increased beneficial SCFA-producing bacteria and reduced harmful strains. |
Larger sample sizes and longer follow-up periods are needed to investigate the underlying mechanisms of empagliflozin related microbiome changes. Different SGLT2 inhibitors might have as well impact on gut microbiome composition. |
| González-Correa et al. [71] | 2023 | Experimental research on animal models, investigating the effects of spironolactone on gut microbiome and hypertension. |
Spironolactone improved gut dysbiosis in spontaneously hypertensive rats by restoring Firmicutes/Bacteroidetes proportions and acetate-producing bacteria populations to normal levels. |
Exploring the long-term effects of spironolactone treatment on gut dysbiosis and overall health in hypertensive models. |
| Wang P et al. [72] | 2022 | Preclinical investigation involving male mice, aimed to explore the effects of Sacubitril/Valsartan on diabetic kidney disease. |
Sacubitril/Valsartan treatment increased beneficial SCFAs-producing bacteria. |
Future research should verify the findings of this preliminary study in clinical experiments. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



