Submitted:
08 September 2025
Posted:
09 September 2025
You are already at the latest version
Abstract
Background: Low birth weight (LBW) remains a significant contributor to neonatal morbidity and mortality worldwide. Maternal nutrition, particularly dietary diversity, plays a crucial role in fetal growth. This study aims to investigate the association between maternal dietary diversity and the occurrence of LBW in a case-control design. Methods: A total of 192 mothers were enrolled, including 64 with LBW infants and 128 with normal birth weight. Maternal dietary intake was assessed using 24-hour recalls and food frequency questionnaires to calculate dietary diversity scores (DDS). Multivariate logistic regression analyses were conducted to identify determinants of LBW, controlling for potential confounders. Findings: The results revealed that mothers of LBW infants had significantly lower dietary diversity scores (mean DDS 5.36, SD 1.19) compared to controls (mean DDS 5.77, SD 1.37; p = 0.0407). Notably, only 42.2% of mothers of LBW infants met the Minimum Dietary Diversity for Women (MDD-W) criteria in weekly assessments, compared to 71.9% of controls (p < 0.001). Multivariate analysis indicated that a maternal mid-upper arm circumference (MUAC) of less than 230 mm and lower dietary diversity were significantly associated with increased odds of LBW (adjusted OR 5.29, 95% CI 1.40–19.91; adjusted OR 0.72, 95% CI 0.54-0.95, respectively). Interpretation: This study demonstrates that inadequate maternal dietary diversity is a modifiable risk factor for low birth weight, emphasizing the urgent need for public health interventions focused on improving maternal nutrition. Addressing dietary deficiencies and promoting diverse food consumption during pregnancy could substantially reduce the incidence of LBW, with significant implications for maternal and neonatal health.
Keywords:
low birth weight
; dietary diversity
; determinants
; Binza Météo
; Kinshasa
1. Introduction
Low birth weight (LBW), defined by the World Health Organization (WHO) as a birth weight less than 2500 g, remains a major public health problem worldwide. It is estimated to affect between 15% and 20% of all live births worldwide, representing more than 20 million newborns per year. The highest burden remains concentrated in low- and middle-income countries [1,2]. Recent studies conducted worldwide, particularly in low- and middle-income countries, indicate that LBW affects 13.7% of births, with sub-Saharan Africa (SSA) accounting for approximately 9.5% [3]. Beyond its high prevalence, LBW is a major determinant of neonatal morbidity and mortality and has long-term consequences on growth, cognitive development, and susceptibility to infections [4,5]. In sub-Saharan Africa, the prevalence of LBW varies considerably, ranging from 4.8% to over 21% depending on the setting [6]. In the Democratic Republic of Congo (DRC), national surveys reported rates of 7.1% in 2014. More recent studies show fluctuations between 10% and 18%, with particularly high rates in deprived urban areas, such as informal settlements in Kinshasa [7,8]. Regional studies confirm significant disparities, with LBW ranging from 3.8% to 21.9% in the eastern provinces of the country [9]. These inequalities are strongly influenced by maternal undernutrition, infections (particularly malaria and anemia), socioeconomic insecurity, and poor access to healthcare [10,11,12].
Maternal nutrition is a key determinant of pregnancy outcomes, and maternal dietary diversity serves as a widely accepted indicator of micronutrient adequacy. The Food and Agriculture Organization of the United Nations (FAO) developed the Minimum Dietary Diversity for Women (MDD-W), which is defined as the consumption of at least five out of ten food groups in the 24 h preceding the survey, as a standardized measure of dietary quality among women of reproductive age [13]. Many studies in SSA have linked low maternal dietary diversity to these corollaries, including low birth weight, but the evidence remains conflicting. This inconsistency partly reflects methodological limitations, as many studies rely exclusively on 24 h recalls, which do not account for usual weekly dietary patterns and often do not adequately account for confounding factors such as infections, maternal height, or socioeconomic conditions [14,15,16]. In addition to nutrition, several other factors influence birth outcomes: low household income, limited education, poor living conditions, unintended pregnancies, maternal anemia, malaria, HIV infection, and short maternal height have all been associated with low birth weight [17,18,19]. Recent meta-analyses in SSA show that maternal anemia alone triples the risk of low birth weight [20]. However, the relationship between maternal dietary diversity, infections, and social vulnerability remains underexplored in urban informal settlements, despite their rapid population growth and increased nutritional and health risks [21,22].
In Kinshasa, the Binza Météo health zone and, more specifically, the Camp Luka neighborhood perfectly illustrate these vulnerabilities. Characterized by informal housing, a dense population, economic insecurity, limited access to drinking water and healthcare, and a monotonous diet poor in micronutrients, Camp Luka provides an essential setting for examining the relationship between maternal nutrition and low birth weight [23,24].
To address this gap, we designed a case–control study to investigate the role of maternal weekly dietary diversity and other maternal determinants in the development of low birth weight in an urban informal health zone of Kinshasa. The primary objective was to assess whether inadequate dietary diversity was associated with low birth weight, after adjusting for maternal infections, anthropometry, and socioeconomic factors. Two hypotheses were formulated: mothers of low-birth-weight infants had less dietary diversity during pregnancy than those with normal-birth-weight infants, and mothers of newborns were more exposed to malaria during pregnancy than those who gave birth to normal-birth-weight infants.
2. Methods
2.1. Study Setting and Participants
We conducted a facility-matched case–control study (1:2 cases–controls) from February to May 2025 in the Binza Météo health zone (HZ), located west of Kinshasa, Democratic Republic of Congo (DRC). The study included 64 cases (infants with low birth weight) and 128 controls (infants with a birth weight ≥ 2500 g), for a total analytical sample of n = 192 mother–infant pairs recruited from six health facilities (HFs): Bangu Reference Health Center; Mwinda Health and Maternity Center; Kasavubu Health and Maternity Center; Kinkenda Hospital; Asodeki Health Center; and the Lonzo Reference Health Center. The ECC/Mapasa center, the Kimia health center, the Ngolo health and maternity Center, and the Maternity of Binza were also included.
The health zone (HZ) is located in the western part of the city province of Kinshasa and operates with 11 health areas (HAs) and 70 health posts (HPs), and does not have a General Reference Hospital. Its estimated population in 2024 was 586,615 inhabitants, with an estimated area of 36 km2 [21].
The Binza Météo HZ is an urban area with a commercial focus and is marked by a significant informal sector. Due to its strategic location along a major road, the Matadi road, a variety of lucrative activities have emerged, such as retail trade, craft services (carpentry), urban transport (motorcycle and bus taxis), and informal trade. However, this dynamic is not evenly distributed across all sectors of the HZ. The Luka camp, which has nearly four of the seven health areas in the HZ, is dominated by activities related to social poverty and permanent insecurity; it has a high population density, with a predominantly young population. The majority of residents earn a modest income from various daily activities, such as local trade, domestic work, and operating motorcycle taxis. This fragile informal economy, combined with a lack of access to means of production, particularly arable land, financing, and training, severely limits households’ economic prospects and contributes to food insecurity, especially among pregnant women and young girls. Studies conducted in Kinshasa reveal that precarious areas such as Camp Luka are among the most exposed to health, nutritional, and socioeconomic risks, which may be the basis for the increase in cases of complications during pregnancy and low birth weight [21,24].
2.2. Sampling and Sample Size
We conducted two-stage probability sampling. The first stage consisted of systematic random sampling of 6 of the 11 health centers (SACs) in the Binza Météo health zone (ZS) in and around Camp Luka, including the Bangu, Bumba, Kimpe, Kinkenda, Lonzo, Lubudi, and Pigeon health centers. In the second stage, we selected 10 SACs based on 1 large SAC per center, with the exception of the Lonzo and Lubudi health centers, where two and three SACs were selected, respectively, based on the intake capacity, demographics, and delivery frequency of each maternity unit reporting data to the SZ central office. The sample size was calculated using Open Epi software (continuity Fleiss, unmatched, ratio 1:2) with the following assumptions: 95% confidence interval (CI), 80% power, case–control ratio of 1:2, the percentage of inadequate dietary diversity among controls of 62.9%, and an expected odds ratio (OR) of 2.96 [25].
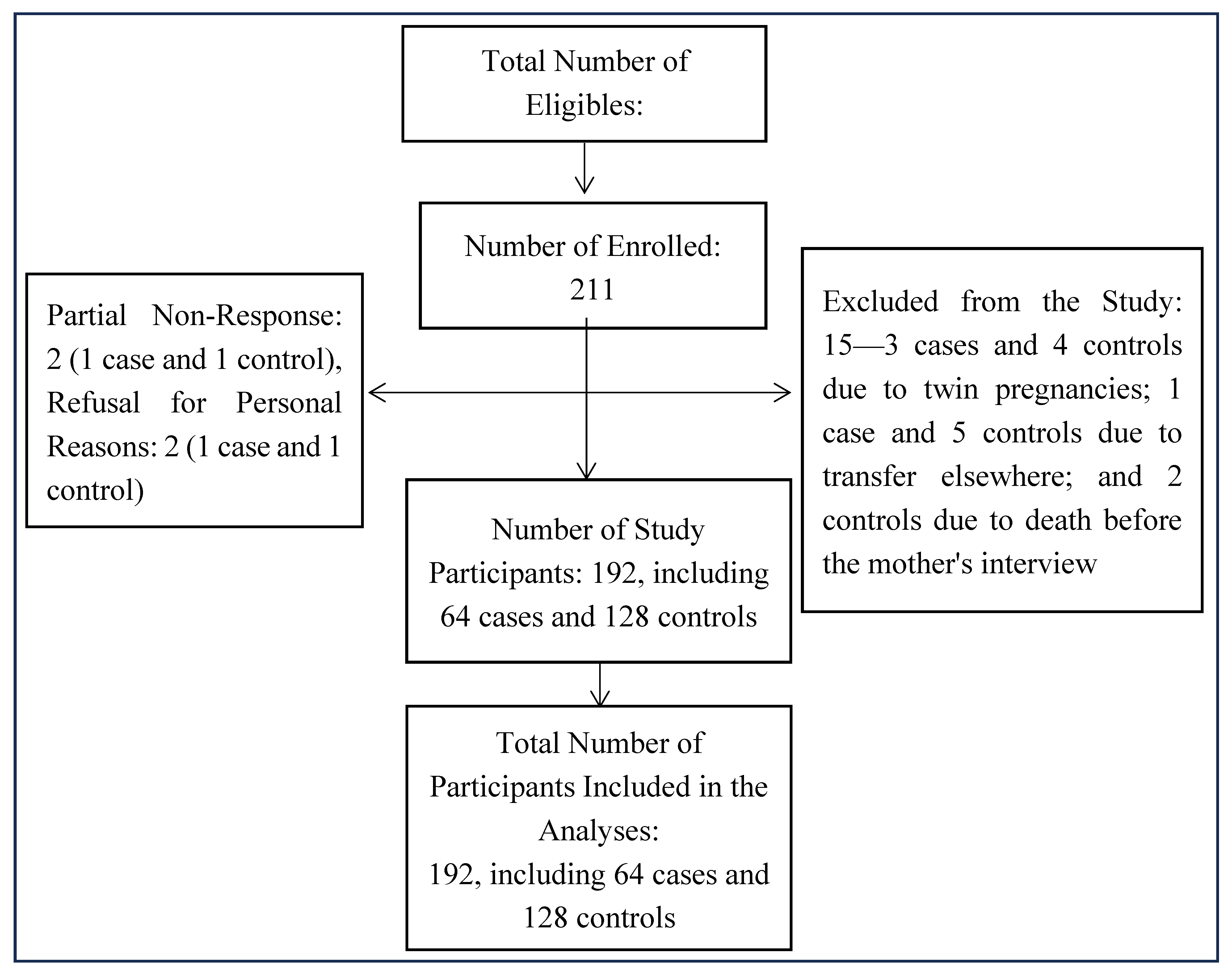
After taking into account the assumptions mentioned and considering the 10% margin for refusals and others, the required sample size was 70 cases and 141 controls, for a total of 211 participants. We did not apply any design effects, as matching by institution was taken into account, which allowed us to obtain a target sample without major deviations.
2.3. Case and Control Definitions and Eligibility Criteria
Cases were defined as newborns with a birth weight <2500 g; controls were newborns with a birth weight ≥2500 g.
- Inclusion Criteria
For cases, the study included any full-term newborn weighing less than 2500 g from a singleton pregnancy, whose delivery took place in one of the ten selected maternity units during the period from February to May 2025.
For controls, this study included any full-term newborn weighing more than 2500 g from a singleton pregnancy, whose delivery took place in one of the ten selected maternity units in the health zone during the study period.
- Exclusion criteria:
For cases, we excluded any infant born of a mother with sickle cell disease, infants born before 37 weeks of gestation (premature), infants born of a multiple pregnancy, newborns with a congenital malformation, and newborns referred from another health zone.
For controls, we excluded any infant born of a mother with sickle cell disease, newborns weighing more than 4000 g, infants born before 37 weeks of gestation, infants born of a multiple pregnancy, newborns with a congenital malformation, and newborns referred from another health zone.
2.4. Recruitment Procedure for Eligible Subjects
Eligible mothers were recruited consecutively from the selected health centers during the study period. For each case (term newborn with weight <2500 g) identified, two controls (term newborn weight ≥ 2500 g < 4000 g) were selected in the same health facility immediately after delivery. The refusal, non-response, and exclusion rates were recorded and remained below 10%.
Figure 1.
Flow chart type diagramme de flux.
2.5. Exposures and Covariates
- Main exposure: Maternal dietary diversity was measured using the Diet Quality Questionnaire (DQQ), dietary diversity score (DDS; number of distinct food groups consumed), and the minimum binary dietary diversity for women (MDD-W, DDS ≥ 5).
-
Other exposures/covariates:
- -
- Sociodemographic and economic data: maternal age (years), maternal education, marital status, maternal education level, maternal occupation, husband’s smoking status at home, and household wealth index, food security, unintended pregnancy, and facility identifier;
- -
- Maternal obstetric and health characteristics: parity, history of LBW, number of prenatal care visits (PCCs), maternal smoking status, gestational age at first PC, iron folate supplementation, hemoglobin level (mg/dL), blood pressure (mm Hg), HIV status, malaria during pregnancy;
- -
- Maternal nutritional characteristics and behavior: prior nutrition education, maternal height (cm), mid-upper arm circumference (MUAC, in mm), maternal weight in the first, second, and third trimesters of pregnancy (in kg), intermittent preventive treatment (IPT), number of IPT doses, and maternal alcohol consumption.
Missing data were addressed by a complete case analysis; no imputation was necessary due to the percentage of missing data being <5%.
2.6. Data Collection
We used structured, pre-designed, and pre-tested survey questionnaires to interview eligible mothers who gave birth during the study period. The questionnaires were administered in French and Lingala via SurveyCTO on Android devices.
Data were collected as follows:
- The mothers were interviewed to collect sociodemographic data, maternal dietary diversity, lifestyle, prenatal follow-up, maternal history, and pregnancy intention.
- Medical records (partogram and prenatal consultation form) were used to triangulate specific data collected during the interview and to collect data on the child’s birth weight, gestational age, prenatal visits, IPT for malaria, last-trimester hemoglobin (Hb) level (measured using a hemoglobinometer), and malaria, which was assessed using a thick drop test in the laboratory. Self-reports were cross-referenced with prenatal records.
- Direct measurements: Maternal anthropometry (height (cm), measured using a height chart; mid-upper arm circumference, measured using the MUAC, with a threshold of 230 mm).
-
Dietary diversity measurement: Maternal dietary diversity was measured using two complementary methods.
- -
- Maternal dietary diversity was determined from the Diet Quality Questionnaire (DQQ), which was adapted to the DRC context, and enabled a qualitative recall of consumption over the last 24 h (MDD-W, FAO/WHO). The 10 food groups were (1) basic starchy foods; (2) legumes; (3) nuts/seeds; (4) dairy products; (5) meat products; (6) eggs; (7) dark green leafy vegetables; (8) other fruits/vegetables rich in vitamin A; (9) other vegetables; and (10) other fruits. A composite women’s dietary diversity score (SDAF) was calculated based on the number of food groups consumed by each mother, with a scale ranging from 0 (no consumption) to 10 (consumption of all groups). A score of ≥5 groups is considered to indicate adequate dietary diversity, while a score of <5 groups reflects inadequate dietary diversity [26].
- -
- Weekly recall (modified MDD-W): Using a qualitative recall of food-group consumption (MDD-W, modified FAO), the frequency of habitual consumption of food groups ≥ 3 times per week was assessed. A composite women’s dietary diversity score (SDAF) was adapted according to the country context, with a scale ranging from 0 (no consumption) to 9 (consumption of all groups). A score of ≥5 is considered to indicate adequate dietary diversity, while a score of <5 reflects inadequate dietary diversity [12].
Validation and training: The tool was pre-tested in a nearby health zone, and interviewers received three days of training on dietary assessment, survey techniques, and digital data collection. Weekly supervision ensured data quality.
2.7. Statistical Analysis
All analyses were performed in Stata version STATA 17 (Stata Corp, College Station, TX, USA); a two-sided p < 0.05 indicated statistical significance. Because this study was a case–control study, odds ratios were reported rather than risk ratios, and no inferences about population prevalence were made from case–control proportions.
For descriptive statistics, means (standard deviation) for continuous variables and numbers (percentage) for categorical variables were reported separately for cases and controls. Between-group comparisons were performed using t-tests for approximately normally distributed continuous variables and chi-square tests for categorical variables; the Wilcoxon test was used for SD where appropriate. For unadjusted associations, univariate logistic regression estimated odds ratios (ORs) and 95% confidence intervals (CIs) for the association between each exposure and case status.
For multivariate analysis, multivariate (unconditional) logistic regression adjusted a priori for parity, maternal height, MUAC < 230 mm, malaria during pregnancy, unintended pregnancy, nutrition education, and facility (included as fixed effects); robust standard errors were used. Mixed-effects logistic regression with a random intercept for facility was fitted as a sensitivity analysis to account for clustering.
The interaction term introduced did not suggest heterogeneity between MDD-W and MUAC < 230 mm. Model discrimination was assessed using the area under the receiver operating characteristic curve (AUC). Model calibration was evaluated with the Hosmer–Lemeshow goodness-of-fit test. Multicollinearity was examined using variance inflation factors (VIF). Variance-inflation factors were calculated to test for multicollinearity, with the highest found to be 1.07. Predicted probabilities were used to calculate classification metrics (sensitivity, specificity, predictive values). Model specifications were checked with the link test. Events per variable and missing data were inspected. Multiple imputation was used where necessary.
2.8. Ethical Considerations
This study was conducted in strict compliance with the ethical principles set out in the Declaration of Helsinki. The research protocol for this study was approved by the Ethics Committee of the Faculty of Medicine of the School of Public Health of Kinshasa (reference number: ESP/CE/36/2025) on 11 April 2025.
Participation was entirely voluntary. The participants were informed that they could withdraw from the study at any time without any consequences. Interviewers, who had received training in the informed consent procedure, presented the participants with a consent form written in their preferred language. For illiterate participants, verbal consent was obtained in the presence of an independent witness after the form was read aloud. The witness ensured that the participant understood the content and freely consented to participate in the study. We recorded a 99% consent rate for eligible participants enrolled.
Data collection was performed anonymously, and the survey form did not contain any elements that could personally identify the participants. Participants were informed of the possibility of refusing to participate or withdrawing from the study at any time without any prejudice. All data, whether recorded electronically (on a computer or phone) or on paper, were stored securely and protected by a password and kept in a locked location that only the principal researcher could access.
3. Results
3.1. Participant Characteristics
A total of 192 participants were included in the study, comprising 64 cases of low birth weight (LBW) infants and 128 controls with normal birth weight. The demographic analysis revealed significant differences between the two groups in maternal characteristics (Table 1). Mothers of LBW infants were younger on average (mean age 25.98 years vs. 28.35 years, p = 0.0056), had lower educational attainment, and were more likely to experience unplanned pregnancies (50% in cases vs. 17.19% in controls, p < 0.001). The study population’s mean birth weight was 2900.5 g (SD 537.9 g), with a mean maternal height of 161.3 cm (SD 7.3 cm) and mean mid-upper arm circumference (MUAC) of 255.2 mm (SD 26.7 mm).
3.2. Dietary Diversity
The analysis of dietary diversity scores (DDS) indicated that mothers of LBW infants had significantly lower dietary diversity compared to controls. The mean DDS based on 24-hour recall was 5.36 (SD 1.19) for cases and 5.77 (SD 1.37) for controls (p = 0.0407). Notably, the proportion of mothers achieving the Minimum Dietary Diversity for Women (MDD-W) was similar for both groups in the 24-hour recall (81.2% in cases vs. 83.6% in controls, p = 0.685). However, in the weekly recall assessment, only 42.2% of case mothers met the MDD-W criteria compared to 71.9% of control mothers (p < 0.001) (Table 2).
3.3. Food-Group Consumption
Food-group consumption patterns revealed that meat, fish, and poultry were the most frequently consumed, with significant discrepancies noted in the consumption of walnut seeds (21.9% in cases vs. 47.7% in controls) and vitamin A-rich vegetables (81.2% in cases vs. 64.1% in controls) (Figure 2).
3.4. Determinants of Low Birth Weight
Multivariate logistic regression analysis identified that a maternal MUAC of less than 230 mm was significantly associated with increased odds of LBW (adjusted OR 5.29; 95% CI 1.40–19.91), while greater maternal height was associated with reduced odds (adjusted OR per cm 0.85; 95% CI 0.79–0.92). Continuous modeling of dietary diversity also indicated a protective effect against LBW (adjusted OR 0.72; 95% CI 0.54-0.95). Malaria during pregnancy showed a borderline association with LBW (adjusted OR 2.06; 95% CI 0.923–4.596), corroborating existing literature on the adverse effects of maternal malnutrition and infections on birth outcomes (Table 3, Figure 3).
4. Discussion
This case-control study provides critical insights into the relationship between maternal dietary diversity and the occurrence of low birth weight (LBW). Our findings highlight the significant role that maternal nutrition plays in influencing fetal growth outcomes, underscoring the need for public health interventions aimed at improving dietary practices among pregnant women.
4.1. Key Findings and Implications
The observed association between lower dietary diversity scores and the occurrence of LBW is particularly alarming. Mothers of LBW infants exhibited significantly reduced dietary diversity, emphasizing the need for enhanced nutritional education and resources. The discrepancy in the consumption of vitamin A-rich vegetables and essential protein sources, such as meat and fish, suggests a gap in dietary intake that could be addressed through community health programs that promote diverse and nutrient-rich diets.
These findings align with previous research indicating that maternal nutrition is a key determinant of fetal growth and development [27,28,29]. The protective effect of higher maternal MUAC and height against LBW reinforces existing literature that identifies maternal anthropometric measurements as critical indicators of pregnancy outcomes. Importantly, the significant association between inadequate dietary diversity and LBW suggests that interventions aimed at improving maternal nutrition could have profound implications for public health. A systematic review in Africa indicates that inadequate dietary diversity during pregnancy doubles the likelihood of delivering a low-birth-weight infant [27]. A prospective study by Mad-zorera in Tanzania indicates that enhanced quality and diversity of foods during pregnancy mitigate the incidence of low birth weight [28]. Kheirouri et al. confirmed, via a systematic study, that inadequate dietary diversity was a significant contributor to low birth weight (LBW) [29]. Sharma et al. recently found that elevated MDD-W scores correlated with a diminished incidence of anemia, underscoring the significance of this metric for maternal health [30]. The insignificance of the binary MDD-W non our investigation suggests that the conventional threshold (≥5 groups) may lack sensitivity in certain contexts, hence endorsing the use of continuous measures of dietary variety. Moreover, forthcoming research by Geta et al. (2024) in Ethiopia demonstrated that dietary diversity assessed over a week more accurately predicts low birth weight than a 24-hour analysis, thereby underscoring the significance of our methodological selection [31].
A deficiency in dietary diversity leads to insufficiencies in critical micronutrients (iron, folate, zinc, vitamins A and B12), hence undermining fetal growth. Maternal nutrition precedes newborn outcomes. Nonetheless, variables like income level, educational attainment, and access to food markets may operate as residual confounders, collectively influencing dietary diversity and the risk of low birth weight (LBW). The divergence between the 24-hour recall and the weekly technique requires meticulous consideration; the former is susceptible to daily variations and social desirability bias, whilst the latter more accurately represents actual food behaviors. The weekly recall more accurately reflects structural habits and diminishes daily fluctuation and social desirability bias associated with the 24-hour recall, hence elucidating its superior predictive accuracy [27,28,29,30,31].
4.2. Addressing Malaria and Other Determinants
While our study found a borderline association between malaria during pregnancy and LBW, further research is warranted to explore this relationship more comprehensively.
Our findings align with local data. A study conducted by Tshinzobe et al. [32]. in Kinshasa emphasized the significance of maternal factors, including weight (parity, pregnancy type), while a study by Ilunga et al. [33]. in Lubumbashi observed that maternal malnutrition and malaria markedly elevated the risk of low birth weight (LBW). The concordance of our findings with existing data, albeit certain discrepancies in determinants, emphasizes that malnutrition and infections are pivotal factors in the continued prevalence of low birth weight in the DRC [32,33]. Kapil et al. [34]. conducted a study in Africa demonstrating that a mid-upper arm circumference (MUAC) of less than 23 cm indicates a heightened risk of poor outcomes, including low birth weight. Additionally, Bilal et al. confirmed that each centimeter of MUAC is associated with a reduction in risk (AOR roughly 0.91 per cm in an African hospital) [35]. A MUAC < 230 mm signifies calorie or protein deficiency in the mother, hence limiting the availability of substrates crucial for fetal development. A woman experiencing malnutrition prior to or throughout early pregnancy has a heightened likelihood of giving birth to an infant with low birth weight. Nonetheless, residual confounding may persist, as a MUAC of less than 230 mm may potentially indicate structural poor conditions or unmeasured infectious comorbidities [34,35]. Maternal short stature has historically been linked to low birth weight; current multi-country research and meta-analyses corroborate the stature-related risk gradient, particularly in sub-Saharan Africa. Reduced maternal height, indicative of chronic malnutrition in childhood and adolescence, constitutes a structural factor influencing uterine volume and placental development. Height predates gestation and indicates previous exposure. Nonetheless, it may be challenging to differentiate this effect from enduring genetic or socioeconomic factors [36,37]. Ticona et al.’s study in Peru [38]. indicated that unexpected pregnancies, especially unwanted pregnancies, quadruple the risk of low birth weight. Additionally, van Tintelen et al. [39] established that unplanned pregnancies elevate the risk of small-for-gestational-age and preterm births in the Netherlands [39]. This information augments the research of Dibaba et al. [40] and Singh et al. [41], emphasizing that unplanned pregnancy continues to be a persistent contributor to unfavorable perinatal outcomes across diverse contexts [40,41]. An unwanted pregnancy may result in heightened stress, diminished compliance with prenatal care, and negligent behaviors, all of which can impact fetal development; hence, intentionality predicts maternal behaviors and neonatal results. Unintended pregnancies are often linked to unstable economic, educational, or psychosocial conditions, which can concurrently influence pregnancy intentions and perinatal results. The persistence of these relationships across multiple contexts (Peru, the Netherlands, and prior African research) indicates a specific role, although intervention via access to care, social aid, or mental health support remains feasible [38,39].
Given the known adverse effects of malaria on maternal and fetal health, integrating malaria prevention strategies into maternal health programs could significantly mitigate the risk of LBW and improve overall pregnancy outcomes. Malaria during pregnancy is a significant risk, during pregnancy to premature birth and low birth weight infants [42]. Malaria infection results in placental inflammation, reduced blood circulation, and maternal anemia, all of which hinder fetal growth. Exposure precedes neonatal outcomes; nonetheless, confounding factors may remain, as mothers exposed to malaria often have restricted access to preventive and therapeutic care [42]. This study presents compelling evidence that maternal nutritional and infection statuses are critical factors in decreasing low birth weight (LBW). The incorporation of more precise instruments, such as weekly dietary diversity assessments, during antenatal consultations should enhance the identification of at-risk mothers.
4.3. Recommendations for Policy and Practice
Our findings highlight the urgent need for policies that prioritize maternal nutrition and dietary diversity. Health systems should implement nutrition-sensitive interventions that focus on increasing access to a variety of food groups, particularly in low-resource settings. Community-based programs that educate pregnant women about the importance of dietary diversity and provide access to diverse food sources can play a crucial role in improving maternal and neonatal health outcomes.
4.4. Limitations and Future Research
This study, while providing important insights into the relationship between maternal dietary diversity and low birth weight (LBW), is subject to several limitations inherent to its case-control design. As a case-control study, we are limited in our ability to establish causal relationships between maternal dietary diversity and LBW. The retrospective nature of dietary assessments may not accurately reflect the nutritional status during critical periods of pregnancy. Although efforts were made to ensure appropriate matching of cases and controls, inherent selection bias may exist. Differences in socioeconomic status, access to healthcare, and cultural factors may influence both dietary practices and birth outcomes, which could confound our findings. The reliance on self-reported dietary intake through 24-hour recalls and food frequency questionnaires introduces the potential for recall bias. Participants may have difficulty accurately remembering their dietary habits, leading to misclassification of dietary diversity and nutrient intake. The sample size, while adequate for preliminary insights, may limit the generalizability of our findings to broader populations. Future studies with larger and more diverse samples are needed to confirm these associations across different demographic groups. While we controlled several key confounders, other unmeasured variables, such as maternal mental health, lifestyle factors (e.g., physical activity, smoking, alcohol consumption), and environmental influences, may impact both dietary patterns and birth outcomes. This limitation suggests that the observed associations may not fully account for all relevant factors influencing LBW. The assessment of dietary diversity was based on qualitative measures that may not fully capture the quantitative aspects of nutrient intake. Future studies should consider more comprehensive dietary assessments to provide a clearer picture of nutritional adequacy. While this case-control study provides valuable insights into the association between maternal dietary diversity and low birth weight, the limitations necessitate cautious interpretation of the results. Longitudinal studies are recommended to further explore these relationships and to identify effective interventions aimed at improving maternal nutrition.
5. Conclusions
This study highlights the critical importance of maternal dietary diversity as a modifiable risk factor for low birth weight. By prioritizing maternal nutrition in public health initiatives, we can work toward reducing the incidence of LBW and improving health outcomes for mothers and their infants. Continued research in this area is essential to develop effective interventions that address the multifaceted determinants of maternal and neonatal health.
Author Contributions
Conceptualization: D.-a.B.B., B.B.M., G.B.B. and P.A.Z.; methodology: D.-a.B.B. and P.A.Z.; software: F.K.K., D.-a.B.B. and P.A.Z.; formal analysis: D.-a.B.B., F.K.K. and P.A.Z.; investigation: D.-a.B.B.; results interpretation: D.-a.B.B., F.K.K., B.B.M. and P.A.Z.; validation: P.A.Z.; writing—original draft preparation: D.-a.B.B. and P.A.Z .; writing—review and editing: D.-a.B.B., F.K.K. and P.A.Z.; visualization: D.-a.B.B., F.K.K. and P.A.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This study did not receive external funding.
Institutional Review Board Statement
This study was approved by the ethics committee of the Kinshasa School of Public Health (ESP/CE/36/2025) on April 11,2025.
Data Availability Statement
The data used for this publication can be made available upon reasonable request to the corresponding author.
Acknowledgments
We thank the KSPH students who were involved in data collection. We also express our thanks to parents and caregivers in Mont Ngafula II HZ for sharing their experiences with us.
Conflicts of interest
The authors declare that they have no conflicts of interest.
References
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10); WHO: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization; UNICEF. Estimates of Low Birthweight: Levels and Trends 2000–2015; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Mare, K.U.; Andarge, G.G.; Sabo, K.G.; Mohammed, O.A.; Mohammed, A.A.; Moloro, A.H.; Ebrahim, O.A.; Seifu, B.L.; Kase, B.F.; Demeke, H.S.; et al. Regional and Subregional Estimates of Low Birthweight and Its Determinants in 44 Low- and Middle-Income Countries: Data from Demographic and Health Surveys. BMC Pediatr. 2025, 25, 342. [Google Scholar] [CrossRef]
- Christian, P.; Lee, S.E.; Donahue Angel, M.; Adair, L.S.; Arifeen, S.E.; Ashorn, P.; Barros, F.C.; Fall, C.H.; Fawzi, W.W.; Hao, W.; et al. Risk of childhood undernutrition related to small-for-gestational age and preterm birth in low- and middle-income countries. Int. J. Epidemiol. 2013, 42, 1340–1355. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cutland, C.L.; Lackritz, E.M.; Mallett-Moore, T.; Bardají, A.; Chandrasekaran, R.; Lahariya, C.; Nisar, M.I.; Tapia, M.D.; Pathirana, J.; Kochhar, S.; et al. Low birth weight: Case definition & guidelines for data collection, analysis, and presentation of maternal immunization safety data. Vaccine 2017, 35 Pt A, 6492–6500. [Google Scholar] [CrossRef] [PubMed]
- Seid, A.; Dugassa Fufa, D.; Weldeyohannes, M.; Tadesse, Z.; Fenta, S.L.; Bitew, Z.W.; Dessie, G. Inadequate dietary diversity during pregnancy increases the risk of maternal anemia and low birth weight in Africa: A systematic review and meta-analysis. Food Sci. Nutr. 2023, 11, 3706–3717. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Planning and Monitoring the Implementation of the Revolution of Modernity (MPSMRM); Ministry of Public Health (MSP); ICF International. Demographic and Health Survey in the DRC 2013-2014; MPSMRM: Rockville, MA, USA; MSP: Rockville, MA, USA; ICF International: Rockville, MA, USA, 2014.
- Mushagalusa, F.T.; Mungo, O.M.; Kambale, A.M.; Iragi, F.M.; Baguma, M.B.; Niyukuri, A.M.; et al. Prevalence and determinants of low birth weight in Eastern Democratic Republic of Congo: A cross-sectional study. Pan Afr. Med. J. 2024, 47, 118. [Google Scholar]
- Cespedes, E.M.; Hu, F.B. Dietary patterns: From nutritional epidemiologic analysis to national guidelines. Am. J. Clin. Nutr. 2015, 101, 899–900. [Google Scholar] [CrossRef]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef] [PubMed]
- FAO; FHI 360. Minimum Dietary Diversity for Women: A Measurement Guide; FAO: Rome, Italy, 2016. [Google Scholar]
- Zerfu, T.A.; Umeta, M.; Baye, K. Dietary diversity during pregnancy is associated with reduced risk of maternal anemia, preterm delivery, and low birth weight in a prospective cohort study in rural Ethiopia. Am. J. Clin. Nutr. 2016, 103, 1482–1488. [Google Scholar] [CrossRef] [PubMed]
- Melaku, Y.A.; Gill, T.K.; Taylor, A.W.; Adams, R.; Shi, Z. Associations entre la diversité alimentaire et le syndrome métabolique et ses composantes en Australie-Méridionale. Santé Publique Nutr. 2018, 21, 2072–2080. [Google Scholar]
- Kuchenbecker, J.; Reinbott, A.; Mtimuni, B.; Krawinkel, M.B.; Jordan, I. Nutrition education improves dietary diversity of children 6-23 months at community-level: Results from a cluster randomized controlled trial in Malawi. PLoS ONE 2017, 12, e0175216. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jung AS, Yaqub N, Lattof SR, Strong J, Maliqi B. Private sector quality interventions to improve maternal and newborn health in low- and middle-income countries: a scoping review. Front Public Health. 2025;13:1332612. Published 2025 Apr 9. [CrossRef]
- Christian, P.; Stewart, C.P. Maternal micronutrient deficiency, fetal development, and the risk of chronic disease. J. Nutr. 2010, 140, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Shrimpton, R. Global policy and programme guidance on maternal nutrition: What exists, the mechanisms for providing it, and how to improve them? Paediatr. Perinat. Epidemiol. 2012, 26 (Suppl. 1), 315–325. [Google Scholar] [CrossRef] [PubMed]
- Belete, N.K.; Belete, A.G.; Assefa, D.T.; Sorrie, M.B.; Teshale, M.Y. Effects of maternal anemia on low-birth-weight in Sub-Sahara African countries: Systematic review and meta-analysis. PLoS ONE 2025, 20, e0325450. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- UrbanBirth Collective. Improving complex health systems and lived environments for maternal and perinatal well-being in urban sub-Saharan Africa: The UrbanBirth Collective. J. Glob. Health 2025, 15, 03009. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kibombi, W.I. Maternal responsibility in clandestine abortions of their underage daughters in Kinkenda at the Luka camp, DR Congo. Int. J. Soc. Sci. Sci. Stud. 2024, 3, 3482–3499. Available online: https://www.ijssass.com/index.php/ijssass/article/view/256 (accessed on 16 June 2025).
- FAO; European Union; CIRAD. Food Systems Profile–Democratic Republic of Congo. Enabling the sustainable and inclusive transformation of our food systems. Rome, Brussels, and Montpellier, France. 2022.
- Muzinga, M.S.; Leopard City Development Policy. Luka Camp in the Ngaliema Commune. 2018. Available online: https://www.scribd.com/document/797074583/TP-analyse-de-Camp-Luka (accessed on 16 June 2025).
- Review of Urbanization in the Democratic Republic of the Congo: Productive and Inclusive Cities for the Emergence of the Democratic Republic of the Congo. 2018. Available online: https://documents.banquemondiale.org/fr/publication/documents-reports/documentdetail/82983153426354100325 (accessed on 16 June 2025).
- Unicef. State of the World’s Children 2019. Children. Food and Nutrition. 2019. Available online: https://data.unicef.org/resources/state-of-the-worlds-children-2019/24 (accessed on 16 June 2025).
- Girma, S.; Fikadu, T.; Agdew, E.; Haftu, D.; Gedamu, G.; Dewana, Z.; Getachew, B. Factors associated with low birthweight among newborns delivered at public health facilities of Nekemte town. West Ethiopia: A case control study. BMC Pregnancy Childbirth 2019, 19, 220. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- DQQ Overview. Guide I. Diet Quality Questionnaire (DQQ) Indicator Guide. 2023; Volume 4, pp. 1–14. Available online: https://www.scribd.com/document/722118215/DQQ-Indicator-Guide-2023 (accessed on 16 June 2025).
- Madzorera, I.; Isanaka, S.; Wang, M.; Msamanga, G.I.; Urassa, W.; Hertzmark, E.; Duggan, C.; Fawzi, W.W. Maternal dietary diversity and dietary quality scores in relation to adverse birth outcomes in Tanzanian women. Am. J. Clin. Nutr. 2020, 112, 695–706. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kheirouri, S.; Alizadeh, M. Maternal dietary diversity during pregnancy and risk of low birth weight in newborns: A systematic review. Public Health Nutr. 2021, 24, 4671–4681. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sharma, N.; Kishore, J.; Gupta, M.; Singla, H.; Dayma, R.; Sharma, J.B. The Minimum Dietary Diversity for Women (MDD-W) Score: Its Association With the Prevalence and Severity of Anemia in Pregnancy. Cureus 2024, 16, e66248. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Geta, T.G.; Gebremedhin, S.; Abdiwali, S.A.; Omigbodun, A.O. Dietary diversity and other predictors of low birth weight in Gurage Zone. Ethiopia: Prospective study. PLoS ONE 2024, 19, e0300480. [Google Scholar] [CrossRef] [PubMed]
- Ilunga, P.M.; Mukuku, O.; Mawaw, P.M.; Mutombo, A.M.; Lubala, T.K.; Shongo Ya Pongombo, M.; Kakudji Luhete, P.; Wembonyama, S.O.; Mutombo Kabamba, A.; Luboya Numbi, O. Risk factors for low birth weight in Lubumbashi, Democratic Republic of the Congo. Med. Sante Trop. 2016, 26, 386–390. (In English) [Google Scholar] [CrossRef] [PubMed]
- Tshinzobe, J.C.K.; Ngaya, D.K. Case-control study of factors associated with low birth weight at the Kingasani Hospital Center. Kinshasa (Democratic Republic of Congo). Pan Afr. Med. J. 2021, 38, 94. [Google Scholar] [PubMed]
- Kapil, S.; Ververs, M. Maternal Mid-Upper Arm Circumference: Still Relevant to Identify Adverse Birth Outcomes in Humanitarian Contexts? Volume 70, 28 September 2023. Available online: https://www.ennonline.net/fex/70/en/maternal-mid-upper-arm-circumference-still-relevant-identify-adverse-birth-outcomes (accessed on 16 June 2025).
- Bilal, J.A.; Rayis, D.A.; AlEed, A.; Al-Nafeesah, A.; Adam, I. Maternal Undernutrition and Low Birth Weight in a Tertiary Hospital in Sudan: A Cross-Sectional Study. Front. Pediatr. 2022, 10, 927518. [Google Scholar] [CrossRef]
- Kozuki, N.; Katz, J.; Lee, A.C.; Vogel, J.P.; Silveira, M.F.; Sania, A.; Stevens, G.A.; Cousens, S.; Caulfield, L.E.; Christian, P.; et al. Short Maternal Stature Increases Risk of Small-for-Gestational-Age and Preterm Births in Low- and Middle-Income Countries: Individual Participant Data Meta-Analysis and Population Attributable Fraction. J. Nutr. 2015, 145, 2542–2550. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Arendt, E.; Singh, N.S.; Campbell, O.M.R. Effect of maternal height on caesarean section and neonatal mortality rates in sub-Saharan Africa: An analysis of 34 national datasets. PLoS ONE 2018, 13, e0192167. [Google Scholar] [CrossRef]
- Ticona, D.M.; Huanco, D.; Ticona-Rendón, M.B. Impact of unplanned pregnancy on neonatal outcomes: Findings of new high-risk newborns in Peru. Int. Health 2024, 16, 52–60. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- van Tintelen, A.M.G.; Jansen, D.E.M.C.; Bolt, S.H.; Warmelink, J.C.; Verhoeven, C.J.; Henrichs, J. The Association Between Unintended Pregnancy and Perinatal Outcomes in Low-Risk Pregnancies: A Retrospective Registry Study in the Netherlands. J. Midwifery Womens Health 2024, 69, 755–766. [Google Scholar] [CrossRef] [PubMed]
- Dibaba YFantahun MHindin, M.J. The association of unwanted pregnancy and social support with depressive symptos in pregnancy: Evidence from rural Southwestern Ethiopia. BMC Pregnancy Childbirth 2013, 13, 135. [Google Scholar] [CrossRef]
- Singh, A.; Chalasani, S.; Koenig, M.A.; Mahapatra, B. The consequences of unintended births for maternal and child health in India. Popul. Stud. 2012, 66, 223–239. [Google Scholar] [CrossRef]
- Hussein, H.; Shamsipour, M.; Yunesian, M.; Hassanvand, M.S.; Agordoh, P.D.; Seidu, M.A.; Fotouhi, A. Prenatal malaria exposure and risk of adverse birth outcomes: A prospective cohort study of pregnant women in the Northern Region of Ghana. BMJ Open 2022, 12, e058343. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Satapathy, P.; Khatib, M.N.; Gaidhane, S.; Zahiruddin, Q.S.; Sharma, R.K.; Rustagi, S.; Al-Jishi, J.M.; Albayat, H.; Al Fares, M.A.; Garout, M.; et al. Adverse pregnancy outcomes in maternal malarial infection: A systematic review and meta-analysis. New Microbes New Infect. 2024, 62, 101474. [Google Scholar] [CrossRef] [PubMed]
Figure 2.
Distribution of food-group consumption based on 24-hour recall among mothers of low-birth-weight infants (LBW, <2500 g, cases, n=64) and normal birth weight infants (controls, n=128) in a case-control study in the Binza Météo health zone, Kinshasa, Democratic Republic of Congo, February–May 2025. Food groups contribute to the dietary diversity score (DDS) and Minimum Dietary Diversity for Women (MDD-W, DDS ≥ 5).
Figure 2.
Distribution of food-group consumption based on 24-hour recall among mothers of low-birth-weight infants (LBW, <2500 g, cases, n=64) and normal birth weight infants (controls, n=128) in a case-control study in the Binza Météo health zone, Kinshasa, Democratic Republic of Congo, February–May 2025. Food groups contribute to the dietary diversity score (DDS) and Minimum Dietary Diversity for Women (MDD-W, DDS ≥ 5).
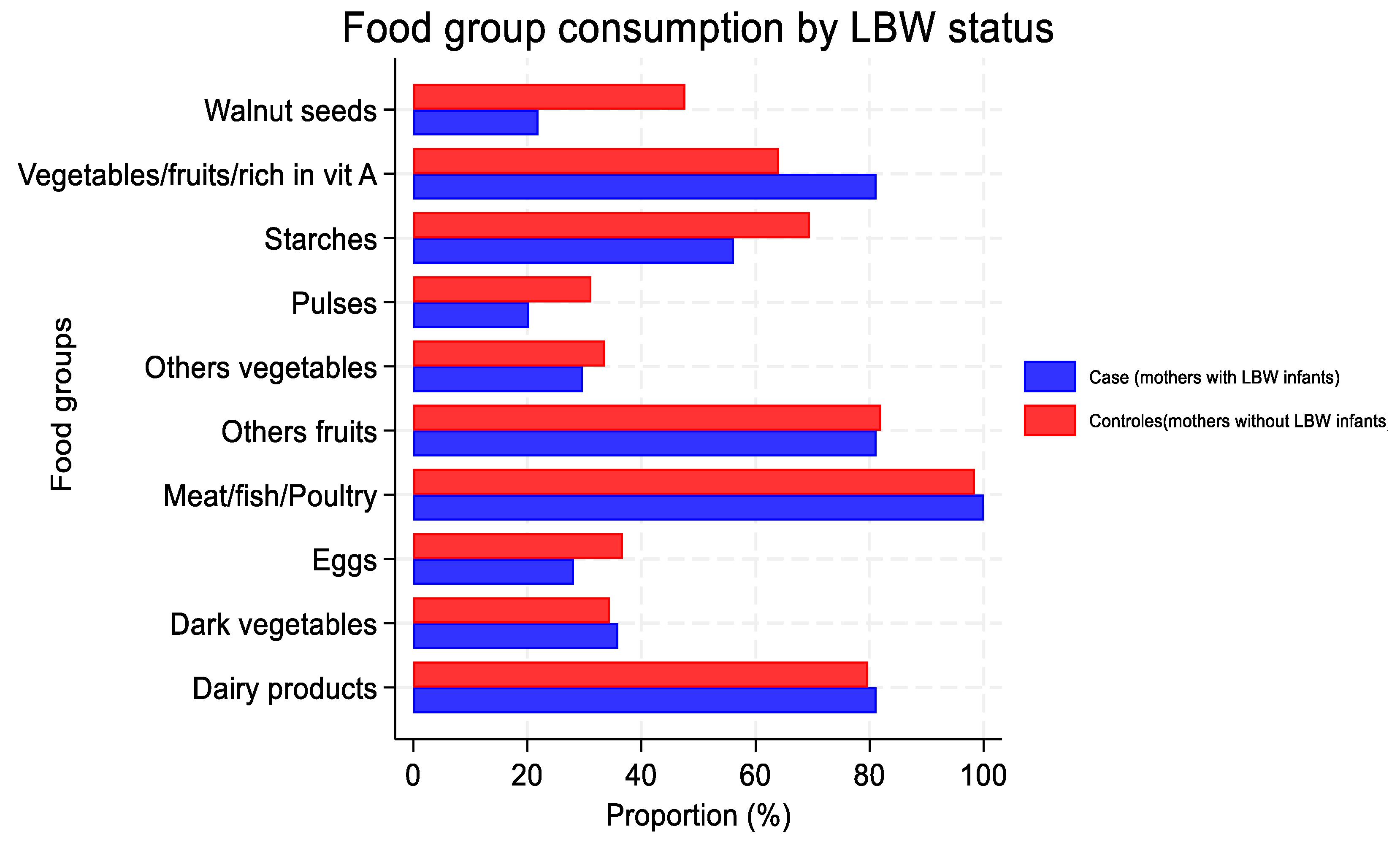
Figure 3.
Forest plot of adjusted odds ratios (ORs) with 95% confidence intervals (CIs) for determinants of low birth weight (LBW, <2500 g) in a case-control study (cases, n=64; controls, n=128) in the Binza Météo health zone, Kinshasa, Democratic Republic of Congo, February–May 2025. Determinants include mid-upper arm circumference (MUAC), Minimum Dietary Diversity for Women (MDD-W, DDS ≥ 5), maternal height, parity, malaria during pregnancy, unintended pregnancy, and nutrition education, adjusted for parity, nutrition education, and facility effects.
Figure 3.
Forest plot of adjusted odds ratios (ORs) with 95% confidence intervals (CIs) for determinants of low birth weight (LBW, <2500 g) in a case-control study (cases, n=64; controls, n=128) in the Binza Météo health zone, Kinshasa, Democratic Republic of Congo, February–May 2025. Determinants include mid-upper arm circumference (MUAC), Minimum Dietary Diversity for Women (MDD-W, DDS ≥ 5), maternal height, parity, malaria during pregnancy, unintended pregnancy, and nutrition education, adjusted for parity, nutrition education, and facility effects.
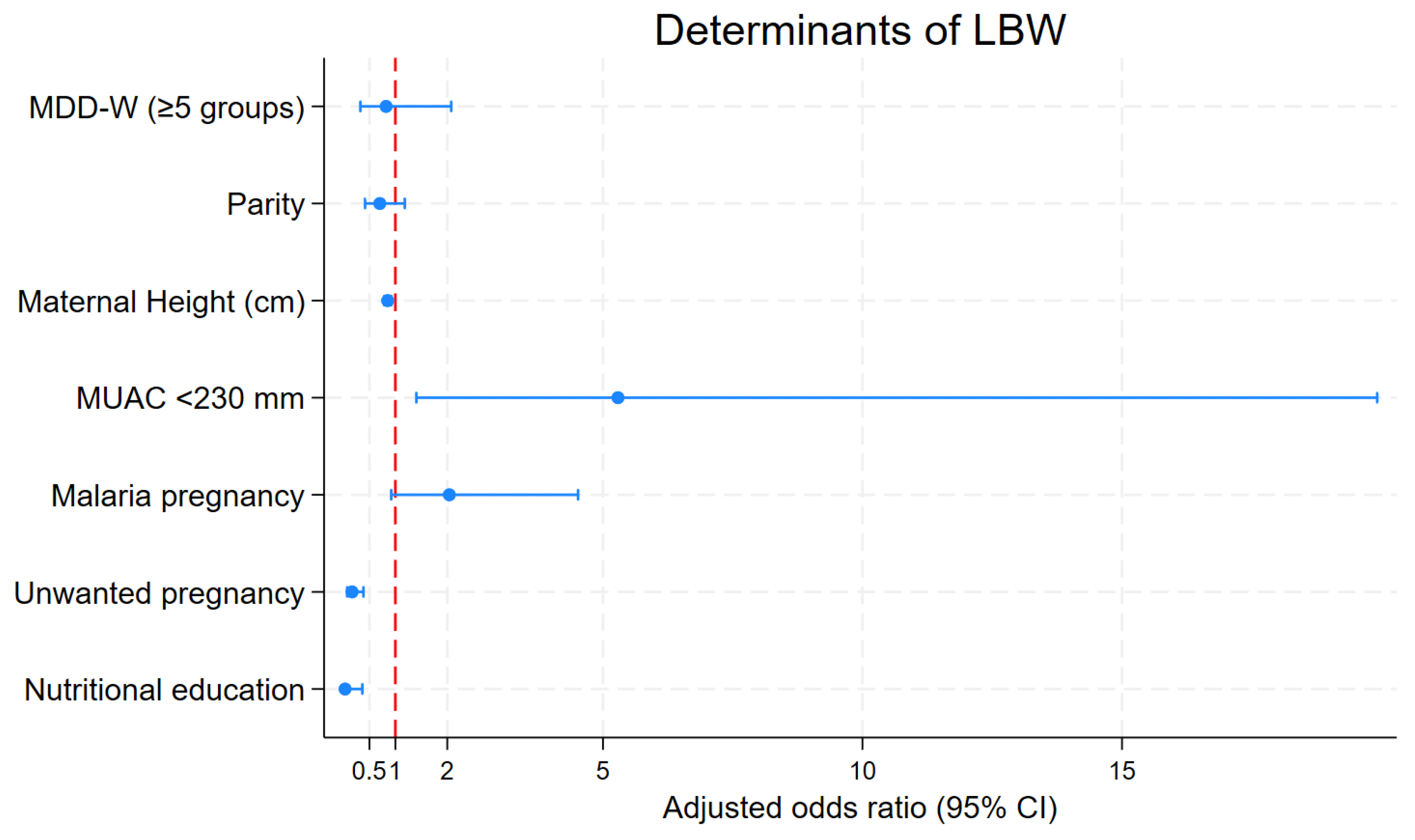

Table 1.
Sociodemographic, obstetric, and nutritional characteristics of mothers of low-birth-weight infants (LBW, <2500 g, cases, n=64) and normal birth weight infants (controls, n=128) in a case-control study in the Binza Météo health zone, Kinshasa, Democratic Republic of Congo, February–May 2025.
Table 1.
Sociodemographic, obstetric, and nutritional characteristics of mothers of low-birth-weight infants (LBW, <2500 g, cases, n=64) and normal birth weight infants (controls, n=128) in a case-control study in the Binza Météo health zone, Kinshasa, Democratic Republic of Congo, February–May 2025.
| Characteristics | Case (n = 64) n (%) |
Control (n = 128) n (%) |
Total (n = 192) n (%) |
p-Value |
|---|---|---|---|---|
| Distribution of mothers by sociodemographic characteristics | ||||
| Mother’s age (years) (mean ± SD) | 25.98 ± 5.21 | 28.35 ± 5.65 | 27.56± 5.61 | 0.0056 |
| Age group (years) | 0.127 | |||
| Less than 25 | 22 (34.38) | 33 (25.78) | 55 (28.65) | |
| 25–34 | 39 (60.94) | 78 (60.94) | 117 (60.94) | |
| 35 and above | 3 (4.69) | 17 (13.28) | 20 (10.42) | |
| Education level | 0.007 | |||
| Below secondary school | 27 (42.19) | 30 (23.44) | 57 (29.69) | |
| Secondary school and above | 37 (57.81) | 98 (76.56) | 135 (70.31) | |
| Marital status | 0.001 | |||
| Single | 17 (26.56) | 10 (7.81) | 27 (14.06) | |
| Married/in union | 46 (71.88) | 118 (92.19) | 164 (85.42) | |
| Others | 1 (1.56) | 0 (0.00) | 1 (0.52) | |
| Occupation | 0.032 | |||
| Housewife | 40 (62.50) | 76 (59.38) | 116 (60.42) | |
| Unemployed | 11 (17.19) | 9 (7.03) | 20 (10.42) | |
| Employee | 13 (20.31) | 43 (33.59) | 56 (29.17) | |
| Unwanted pregnancy | <0.001 | |||
| No | 32 (50.00) | 22 (17.19) | 54 (28.12) | |
| Yes | 32 (50.00) | 106 (82.81) | 138 (71.88) | |
| Passive smoking | 0.043 | |||
| Yes | 14 (21.88) | 14 (10.94) | 28 (14.58) | |
| No | 50 (78.12) | 114 (89.06) | 164 (85.42) | |
| Socioeconomic status | 0.092 | |||
| Poor | 28 (43.75) | 37(28.91) | 65 (33.85) | |
| Middle | 26 (40.62) | 59 (46.09) | 85 (44.27) | |
| Rich | 10 (15.62) | 32 (25.00) | 42 (21.88) | |
| Food security level | 0.123 | |||
| Food insecurity | 41(64.06) | 67 (52.34) | 108 (56.25) | |
| Food security | 23 (35.94) | 61 (47.66) | 84 (43.75) | |
| Mother’s obstetrics and health-related characteristics | ||||
| Number of ANC | 0.006 | |||
| <4 | 33 (51.56) | 40 (31.25) | 73 (38.02) | |
| ≥4 | 31 (48.44) | 88 (68.75) | 119 (61.98) | |
| Pregnancy age at 1st ANC (week) | 0.186 | |||
| Over 16 | 49 (76.56) | 108 (84.38) | 157 (81.77) | |
| Before 16 | 15 (23.44) | 20 (15.62) | 35 (18.23) | |
| History of malaria during pregnancy | 0.024 | |||
| Yes | 43 (67.19) | 64 (50.00) | 107 (55.73) | |
| No | 21 (32.81) | 64 (50.00) | 85 (44.27) | |
| Hemoglobin level (mg/dL) | 0.019 | |||
| <12 | 38 (59.38) | 53 (41.41) | 91 (47.40) | |
| ≥12 | 26 (40.62) | 75 (58.59) | 101 (52.60) | |
| Number of previous births (parity) | <0.001 | |||
| Primiparous | 35 (54.69) | 33 (25.78) | 68 (35.42) | |
| 2–3 | 24 (37.50) | 71 (55.47) | 95 (49.48) | |
| Over 3 | 5 (7.81) | 24 (18.75) | 29 (15.10) | |
| History of low birth weight | 0.504 | |||
| Yes | 8 (12.50) | 12 (9.38) | 20 (10.42) | |
| No | 56 (87.50) | 116 (90.62) | 172 (89.58) | |
| History of hypertension | 0.586 | |||
| Yes | 3 (4.69) | 4 (3.12) | 7 (3.65) | |
| No | 61 (95.31) | 124 (96.88) | 185 (96.35) | |
| Mother’s nutritional and behavioral factor characteristics | ||||
| Mother’s height (cm) | 0.200 | |||
| <150 | 3 (4.69) | 2 (1.56) | 5 (2.60) | |
| ≥150 | 61 (95.31) | 126 (98.44) | 187 (97.40) | |
| Maternal MUAC (mm) | <0.001 | |||
| <230 | 14 (21.88) | 5 (3.91) | 19 (9.90) | |
| ≥230 | 50 (78.12) | 123 (96.09) | 173 (90.10) | |
| Nutritional education | ||||
| No | 8 (12.50) | 1 (0.78) | 9 (4.69) | <0.001 |
| Yes | 56 (87.50) | 127 (99.22) | 183 (95.31) | |
| Have you ever taken IPT | 0.294 | |||
| Yes | 56 (87.50) | 118 (92.19) | 174 (90.62) | |
| No | 8 (12.50) | 10 (7.81) | 18 (9.38) | |
| How many times have you taken | 0.123 | |||
| No | 8 (12.50) | 10 (7.81) | 18 (9.38) | |
| Less than 3 | 51 (79.69) | 95 (74.22) | 146 (76.04) | |
| 3 and above | 5 (7.81) | 23 (17.97) | 28 (14.58) | |
| Have you ever drunk alcohol | 0.225 | |||
| Yes | 18 (28.12) | 26 (20.31) | 44 (22.92) | |
| No | 46 (71.88) | 102 (79.69) | 148 (77.08) | |
| Minimum Dietary Diversity for Women (MDD-W 24 h recall) | ||||
| Inadequate | 12 (18.75) | 21 (26.41) | 33 (17.19) | 0.685 |
| Adequate | 52 (81.25) | 107 (83.59) | 159 (82.81) | |
| Modified MDD-W (weekly) | <0.001 | |||
| Inadequate | 37 (57.8) | 36 (28.1) | ||
| Adequate | 27 (42.2) | 92 (71.9) |
SD: Standard Deviation; IPT: Intermittent Preventive Treatment; ANC: Antenatal Care; MUAC: Mid-Upper Arm Circumference.
Table 2.
Distribution of dietary diversity scores (DDS) and proportion achieving Minimum Dietary Diversity for Women (MDD-W, DDS ≥ 5) among mothers of low birth weight infants (LBW, <2500 g, cases, n=64) and normal birth weight infants (controls, n=128) in a case-control study in the Binza Météo health zone, Kinshasa, Democratic Republic of Congo, February–May 2025, assessed using 24-hour and weekly recall methods.
Table 2.
Distribution of dietary diversity scores (DDS) and proportion achieving Minimum Dietary Diversity for Women (MDD-W, DDS ≥ 5) among mothers of low birth weight infants (LBW, <2500 g, cases, n=64) and normal birth weight infants (controls, n=128) in a case-control study in the Binza Météo health zone, Kinshasa, Democratic Republic of Congo, February–May 2025, assessed using 24-hour and weekly recall methods.
| Dietary Diversity Indicator | Case (Low Birth Weight, n = 64) | Control (Weight > 2500 g, n = 128) | p-Value |
|---|---|---|---|
| DDS (24 h) mean ± SD | 5.36 ± 1.19 | 5.77 ± 1.37 | 0.0407 |
| Reached MDD-W (24 h) (%) | 81.2% (n = 52) | 83.6% (n = 107) | 0.685 |
| DDS (weekly) mean ± SD | 4.48 ± 1.63 | 5.21 ± 1.31 | <0.001 |
| Reached MDD-W (weekly) | 42.2% (n = 27) | 71.9% (n = 92) | <0.001 |
| Discrepancies (24 h vs. weekly) | 51.6% (n = 33) | 32.0% (n = 41) | 0.009 |
SD: Standard Deviation; DDS: Dietary Diversity Scale; MDD-W: Minimum Dietary Diversity for Women.
Table 3.
Bivariate and adjusted odds ratios (ORs) with 95% confidence intervals (CIs) for associations between maternal factors and low birth weight (LBW, <2500 g) in a case-control study (cases, n=64; controls, n=128) in the Binza Météo health zone, February–May 2025.
Table 3.
Bivariate and adjusted odds ratios (ORs) with 95% confidence intervals (CIs) for associations between maternal factors and low birth weight (LBW, <2500 g) in a case-control study (cases, n=64; controls, n=128) in the Binza Météo health zone, February–May 2025.
| Variable | Non Adjusted OR [95% CI] |
p-Value | Adjusted OR [95% CI] |
p-Value |
|---|---|---|---|---|
| MDD-W (DDS ≥ 5) | 0.85 [0.39–1.86] | 0.685 | 0.82 [0.32–2.07] | 0.678 |
| Parity | 0.67 [0.52–0.87] | 0.002 | 0.70 [0.42–1.18] | 0.182 |
| Maternal Height (cm) | 0.87 [0.82–0.92] | <0.001 | 0.85 [0.79– 0.92] | <0.001 |
| MUAC < 230 mm | 6.89 [2.36–20.14] | <0.001 | 5.29 [1.40–19.91] | 0.014 |
| Malaria during pregnancy | 2.05 [1.09–3.83] | 0.025 | 2.04 [0.92–4.52] | 0.079 |
| Unwanted pregnancy | 0.21 [0.11–0.41] | <0.001 | 0.17 [0.071–0.385] | <0.001 |
| Nutritional education | 0.055 [0.007–0.45] | 0.007 | 0.032 [0.003–0.364] | 0.006 |
MDD-W: Minimum Dietary Diversity; MUAC: Middle-Upper Arm Circumference.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



