
Submitted:
29 May 2025
Posted:
06 June 2025
You are already at the latest version
Abstract
Background/Objectives: This study aimed to assess the prevalence of low birth weight (LBW) among Roma women living in segregated settlements in Hungary and to identify key social and behavioral risk factors, with a focus on health behaviours and access to antenatal care. Methods: A cross‐sectional quantitative study was conducted using a structured 297‐item questionnaire. Data collection took place through face‐to‐face interviews in the participants’ home environment. The questionnaire explored sociodemographic, behavioural, and prenatal risk factors. In total, 231 marginalized Roma women participated. Data were analysed using SPSS 25.0, including chi‐square tests and binary logistic regression. Statistical significance was set at p < 0.05. Results: The prevalence of LBW was 13.4%. Statistically significant associations were found between LBW and smoking (p = 0.001; Cramerʹs V = 0.253), alcohol consumption (p = 0.011), lack of antenatal care (p = 0.023), and vaginal infections (p = 0.008). Smoking emerged as the strongest independent predictor, tripling the risk of LBW. No significant associations were found for vitamin intake or drug use, though both appeared as possible contributing factors. Conclusions: Roma women in segregated settlements face a significantly elevated risk of LBW due to modifiable behavioural and structural factors. These findings highlight the urgent need for culturally adapted, community‐based interventions targeting smoking cessation, increased prenatal awareness, and improved access to antenatal care among marginalized populations.
Keywords:
Roma women
; low birth weight
; health behaviour
; smoking
; alcohol consumption
; vitamin intake
; antenatal care
; social inequalities
1. Introduction
The quality of outcomes around birth is a fundamental indicator of a country's health care system and social inequalities [1]. Low birth weight prevalence is not only a medical but also a public health and social policy issue, especially for populations living in social exclusion [2]. Several international studies confirm that disadvantaged communities, especially Roma women, have higher rates of preterm birth and low birth weight [3,4,5]. Socio-economic factors such as low educational attainment, unemployment and housing poverty have a significant impact on maternal and neonatal health outcomes [6].
The Roma population, especially those living in segregated settlements, are at increased risk of factors that worsen pregnancy outcomes and the health prospects of newborns [7,8]. National and international health policy documents also clearly articulate the importance of reducing structural inequalities, highlighting the need for targeted interventions [9].
Among Roma women, there are higher rates of health behaviours - such as smoking during pregnancy, inadequate nutrition, less frequent use of antenatal care - that increase the risk of preterm birth and intrauterine growth retardation. [10,11]. In addition, socioeconomic background, low educational attainment, unemployment, and housing poverty also influence events around childbirth [8].
Roma women's limited access to the health care system is not only due to physical barriers, but also to trust and cultural barriers [2,10]. Individual or structural experiences of discrimination, low health awareness and negative attitudes towards the care system all reduce the likelihood of accessing health services [11].
Although there have been a few domestic studies on the topic, the available empirical data are scarce, especially regarding birth outcomes among Roma women living in segregated areas [12]. In recent decades, there have been minimal quantitative studies that have used statistical methods to analyse the prevalence of low birth weight and preterm birth in this population, along social and health background factors. The lack of such data is not only a problem from a scientific point of view, but also makes it difficult for public health planners to design targeted interventions.
The aim of this research is to explore what factors - in particular social status, health behaviour and participation in care - influence perinatal outcomes among Roma women living in segregated settings. The aim of our study is not only to quantify individual-level risks, but also to demonstrate that perinatal health outcomes can be interpreted along structural social factors.
2. Materials and Methods
The study was a quantitative, cross-sectional research conducted in the autumn-winter period of 2024 in three segregated Roma communities in Szabolcs-Szatmár-Bereg County. The subjects relevant for the study were selected through expert sampling, considering the aspects of spatial segregation, ethnic composition, and accessibility to the research sites. The women in the study were recruited through a personal approach using a structured questionnaire. Data was collected using a structured questionnaire, which was completed by participants during face-to-face interviews. Although the research did not follow an interview method, the personal presence resulted in an interview-like data collection situation, which allowed for clarification and refinement of questions, and responding to the questionnaire was voluntary and anonymous. The final sample size consisted of 231 respondents.
The questionnaire contained a total of 297 mostly closed questions, which were compiled considering the relevant literature and the health priorities highlighted in national and international Roma strategies. The questions covered the following main thematic areas: sociodemographic background (age, education, economic activity, housing conditions), health behaviour (smoking, alcohol consumption, vitamin intake, substance use), participation in antenatal care and health conditions during pregnancy, birth outcomes and gynaecological history.
Binary logistic regression was used to analyse the combined effect of health behaviour and sociodemographic factors. The statistical software SPSS 25.0 was used to perform the regression analyses, and the methodological protocol followed international guidelines [13,14]. The model included maternal education, the prevalence of smoking and alcohol consumption, and attendance at care, among other factors.
Frequency distributions, means and standard deviations were calculated to describe the sample characteristics. The prevalence of small for gestational age (SGA) was examined using a chi-square test along the main sociodemographic and health behaviour variables. In addition, multivariate binary logistic regression was used to explore the risk factors underlying low birth weight. The model included maternal age, education, smoking, alcohol consumption, drug use, vitamin intake during pregnancy and antenatal care attendance as control variables. In all cases, a level of p < 0.05 was used to establish statistical significance.
The research was carried out in full compliance with the relevant data protection and research ethics regulations. Participants were fully informed, orally and in writing, about the purpose of the study, how the data would be handled, and how voluntary participation and anonymity were ensured. The study was approved by the Scientific and Research Ethics Committee of the Health Sciences Council (TUKEB). TUKEB File No: BM/2120-1/2024.
3. Results
Of the 231 women in the study, 31 (13.4%) reported having a low-birth-weight baby compared to their gestational age, of which 28 had one such outcome and 3 had more than one. The overwhelming majority of respondents, 198 (85.7%), negated that they had ever delivered a low-birth-weight baby, while 2 did not provide a meaningful response.
The prevalence of low birth weight showed a significant association with smoking and alcohol consumption during pregnancy and lack of care. These associations are consistent with findings in the national and international literature that the increased presence of these risk factors characterises marginalised communities [15,16].
11 (18.6%) admitted to regular smoking and 12 (20.3%) to occasional smoking during the pregnancy in which their low-birth-weight baby was born. 36 (61%) said they had not smoked during this period. The total number of participants who did not answer the question or provided missing data was 172, presumably due to sensitivity to the topic or distortion of memory.
Data on the frequency of alcohol consumption showed that 13 people (42%) consumed alcohol occasionally at the time of low birth weight. A similar proportion of 13 (42%) said they had not consumed alcohol during the pregnancy in question, and 5 (16%) gave an invalid response.
In terms of antenatal care habits, 9 women (29%) of women with low-birth-weight babies attended antenatal care every month, while 6 (19.4%) attended at least once a month. 14 women (45.2%) attended only a few times, while 2 women (6.5%) attended only once or not at all - the latter indicating a significantly low level of health follow-up.
In the case of the question on conscious childbearing, 46 respondents gave an evaluable answer, of whom only 9 (3.9%) said that their pregnancy resulting in a low-birth-weight newborn was a conscious decision. The majority of respondents - 37 (16%) - reported unplanned, unconscious childbearing.
These results are consistent with national and international literature showing that the prevalence of low birth weight is higher in social groups with high levels of smoking during pregnancy, alcohol consumption, low levels of childbearing awareness and unavailability or irregularity of antenatal care. The exact direction and strength of the associations were further examined using multivariate statistical modelling.
Multivariate analysis - Supplementary results
The study first analysed the possible risk and protective factors leading to the birth of low-birth-weight babies. No statistically significant association was found between intake of folic acid/foliate vitamin during pregnancy and the prevalence of low birth weight (p = 0.205), nor was the effect of drug use significant, although there were proportionally more pregnancies resulting in low-birth-weight newborns among drug users (6.9% vs. 2.4%; p = 0.199).
In contrast, a statistically validated association of moderate strength was identified between smoking and low birth weight (χ²(1) = 10.380, p = 0.001; Cramer's V = 0.253). The proportion of low-birth-weight foetuses was found to be three times higher among smoking mothers (75.9%) than among non-smoking women (24.1%). Smoking was therefore considered a significant risk factor for perinatal low birth weight.
Figure 1 illustrates the proportion of low-birth-weight babies among smoking and non-smoking pregnant women. It can be clearly seen that the prevalence of low birth weight was three times higher among smokers, which supports the significant correlation found in the statistical analysis (χ²(1) = 10.380, p = 0.001).
Also, there was a statistically significant association between alcohol consumption and low birth weight (χ²(1) = 6.431, p = 0.011; Cramer's V = 0.180). The prevalence rate was twice as high among mothers who consumed alcohol compared to non-consumers (46.4% vs. 23.5%), thus regular alcohol consumption was considered a measurable risk factor for low birth weight.
Figure 2 illustrates the proportion of low-birth-weight babies among pregnant women who drink and do not drink alcohol. It can be seen that the prevalence of low birth weight was twice as high among alcohol drinkers, supporting a statistically significant association (χ²(1) = 6.431, p = 0.011).
Attendance at antenatal care was also found to be a relevant protective factor. The proportion of low-birth-weight foetuses among women who received care was 30.5%, compared with 48.3% among those who did not, representing a one-and-a-half-fold increased risk associated with lack of care (χ²(1) = 5.164, p = 0.023; Cramer's V = 0.171).
Figure 3 illustrates the proportion of low-birth-weight babies among women attending and not attending antenatal care. The prevalence of low birth weight was one and a half times higher in non-attendees, supporting a statistically significant association (χ²(1) = 5.164, p = 0.023).
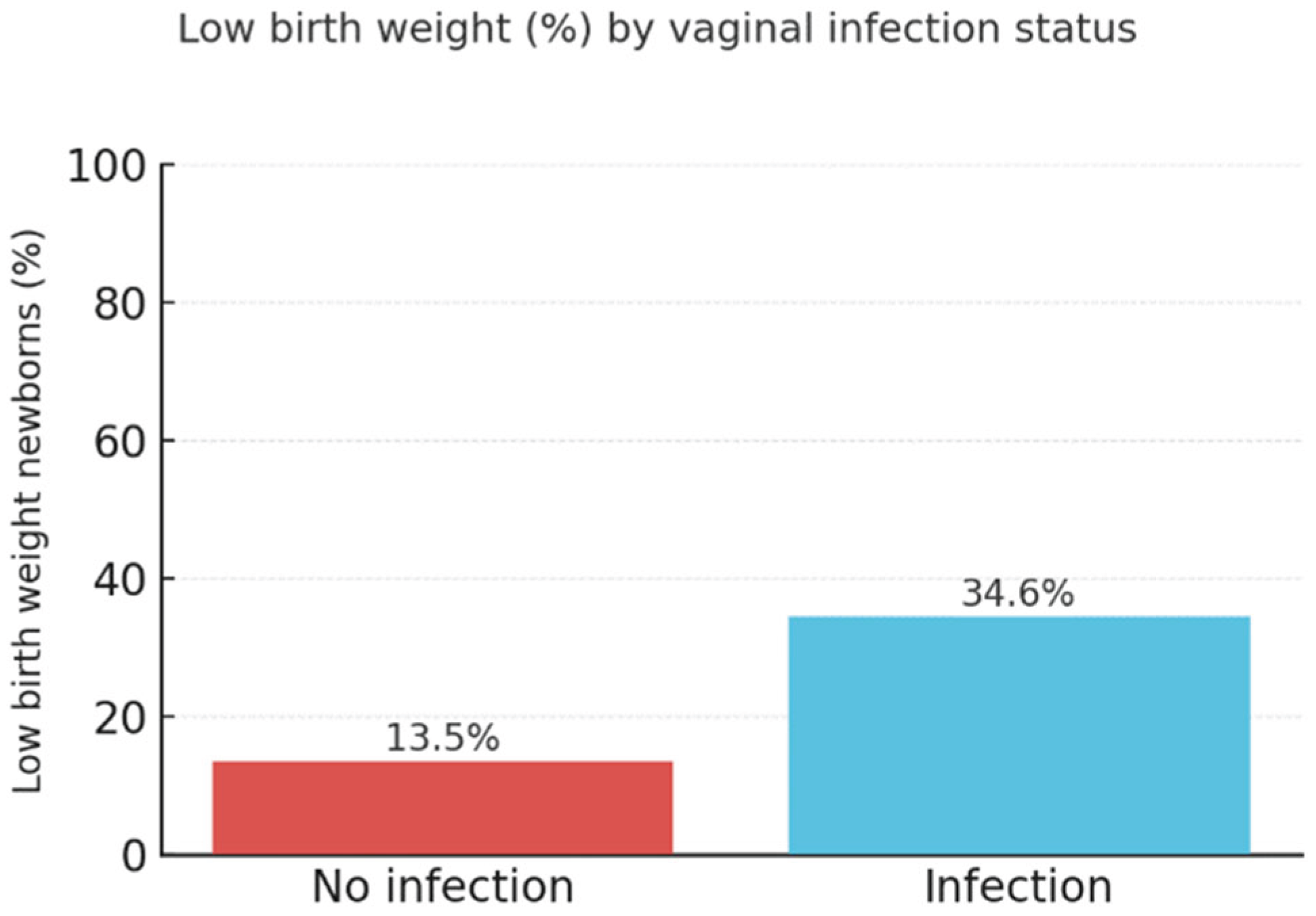
Finally, a statistically significant association was also found between vaginal infections and low birth weight (χ²(1) = 7.030, p = 0.008; Cramer's V = 0.205). The proportion of low-birth-weight babies among women without a vaginal infection during pregnancy was 13.5%, compared to 34.6% among those who experienced an infection — more than twice the prevalence.
Figure 4 illustrates the proportion of low-birth-weight babies among pregnant women with and without vaginal infections. Among women with infections, the prevalence of low birth weight was almost three times higher, supporting a statistically significant association (χ²(1) = 7.030, p = 0.008).
Based on the above, smoking is the most prevalent risk factor for low-birth-weight newborns, and alcohol consumption and attendance at care also have a measurable impact.
4. Discussion
According to the latest official data available, the proportion of low-birth-weight babies in Hungary was 8.5% in 2021. This rate refers to live-born babies with a birth weight of less than 2500 grams [17].
The data from this research support the hypothesis that the prevalence of adverse perinatal outcomes, particularly low birth weight and preterm birth, among Roma women living in segregated settings is higher than the national average and are primarily rooted in social and behavioural determinants. The analyses clearly show that smoking, unconscious childbearing, and lack of vitamin intake and preventive behaviour contribute significantly to adverse outcomes. These correlations confirm previous national and international findings [2,7,11], which have emphasised the link between structural social disadvantages and health behaviour.
Logistic regression showed that smoking was a significant and strong predictor of low birth weight. Lack of conscious childbearing was also a contributing factor, although this relationship only approached statistical significance. An analysis of vitamin intake patterns showed that while intake rates increased during pregnancy, preparatory vitamin intake in the preceding months was markedly low, raising the issue of educational gaps in reproductive health [1]. Rates of drug use were found to be low; however, the presence of occasional use does not exclude background risk [10].
Although one focus of our research has been the association between vaginal infections and low birth weight, we cannot ignore the alarming increase in syphilis cases in Szabolcs-Szatmár-Bereg County. My personal experience at the obstetrics and gynaecology department confirms that the prevalence of syphilis, especially among women living in segregated settlements, has shown a marked increase in recent years.
National data: according to the National Centre for Public Health (NNK), 1,070 syphilis patients were registered in Hungary in 2022, an increase of about 40% compared to 2018. The epidemiological trend was also upward in 2023, with 151 more cases of syphilis in 2023 than in the previous year. Based on this, there were approximately 1,221 syphilis cases nationwide in 2023 (for comparison, this is ~430 more than in 2019) [18].
According to the quarterly reports of the National Centre for Public Health and Pharmacy, a total of about 63 syphilis cases were registered in Szabolcs-Szatmár-Bereg County in 2022, 19 of which occurred in the fourth quarter. In the year 2023, the number of cases in the county decreased to 45, of which 8 new cases were reported in the 4th quarter. For comparison, nationally, 1,069 cases of syphilis were recorded in 2022 and 1,220 in 2023, of which 369 cases occurred in Q4 2023 [18].
The trend is not only noteworthy from an epidemiological perspective, but also from a public health perspective - especially given the high rates of latent undetected cases and the increased risk in socially deprived communities, including the rise in sexual exploitation, prostitution and congenital syphilis. Although the present study was not specifically designed to map the epidemiology of this infection, our empirical findings on the health status of communities living in segregated settlements support the social determinants and health policy relevance of this infection.
These findings confirm that the birth of low-birth-weight babies cannot be considered a purely biological or genetic trait. Socioeconomic factors, living environment, level of education and access to care are complex determinants of the course and outcome of pregnancy [8]. Low levels of health awareness and limited participation in care among Roma women point to systemic problems that need to be addressed not only in health but also in social policy [9].
It is important to underline that self-reported data may be biased due to the sensitivity of certain questions, particularly those related to smoking, alcohol, and the use of psychoactive substances. A further limitation is the cross-sectional research design, which does not allow causal inferences to be drawn. Nevertheless, the findings fit well with international trends and confirm the direction that improving health indicators among marginalised groups requires targeted, locally based, culturally sensitive interventions [2].
The findings confirm that sociocultural and structural factors play a major role in the development of low birth weight besides biological factors. Among disadvantaged Roma women, limited access to health care, unhealthy lifestyles and social exclusion combine to influence perinatal outcomes [19] (Szabó & Boros, Socio-economic differences among low-birthweight infants in Hungary. Results of the Cohort '18 - Growing Up in Hungary birth cohort study, 2023) .
The use of longitudinal studies assessing the quality and continuity of antenatal care and the effectiveness of community-based health promotion programmes are priorities for future research. The results of the present study can serve as a basis for this while drawing attention to the importance of a preventive approach.
5. Conclusions
The results of the present study confirm that the development of adverse perinatal outcomes, particularly low birth weight among Roma women living in segregated settings, is closely associated with certain health behavioural and social factors. Smoking was identified as a significant predictor of low birth weight, while the lack of conscious pregnancy planning was also associated with increased odds, albeit with marginal statistical significance.
Prenatal vitamin intake was low, particularly in the pre-pregnancy period, and although there was some increase during pregnancy, it remained below levels that support healthy foetal development. Although drug use was relatively rare, its presence in the cases concerned may have further increased perinatal risks.
The associations found clearly indicate that perinatal health among socially disadvantaged women is shaped not only by biological, but also by sociocultural and structural factors. The findings call for the development of culturally specific, community-based prevention and education interventions that effectively target health behaviours, conscious childbearing, and the promotion of participation in antenatal care.
This research may contribute to the development of social policy and public health strategies aimed at reducing health inequalities affecting Roma women and their children and at improving perinatal outcomes in this population in the long term.
Author Contributions
Kinga Pauwlik (K.P.): conceptualization, study design, questionnaire development, data collection coordination, conducting research, statistical guidance, manuscript writing and finalization. Gyöngyi Major (Gy.M.): literature consultation and professional support. Krisztina Gebréné Éles (K.G.É.): methodological advice, proofreading. Anita R. Fedor (A.R.F.): scientific supervision, final approval. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Medical Research Council – Research Ethics Committee (TUKEB) (Approval number: BM/2120-1/2024).
Informed Consent Statement
All participants received full verbal information about the aims and procedures of the study and voluntarily agreed to participate. Due to the anonymized nature of the questionnaire and the absence of sensitive personal data, written informed consent was not required according to the approval of the ethics committee.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The author gratefully acknowledges the support of the Roma Minority Self-Government in Nyíregyháza, the local Social and Child Welfare Services of Tiszavasvári and Nagyecsed, and all the Roma women who participated in the study.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| LBW | Low Birth Weight |
| SPSS | Statistical Package for the Social Sciences |
| TUKEB | Medical Research Council – Research Ethics Committee |
References
- Központi Statisztikai Hivatal. 2023. Kohorsz ’18 – magyar születési kohorszvizsgálat eredményei [in Hungarian]. Budapest, Központi Statisztikai Hivatal.
- European Union Agency for Fundamental Rights (FRA). 2014. Discrimination against and living conditions of Roma women in 11 EU Member States. Luxembourg, Publications Office of the European Union.
- Kornyicki Á, Fedor A. 2024. Inequalities and differences in health status of pre- and perinatal periods in Hungarian long-term series analysis (1997–2019). Children 11(11). [CrossRef]
- Szabó L, Veroszta Z. 2024. Discrimination against Roma women during childbirth? Unraveling the underlying effects of ethnic and socio-economic factors. Sexual & Reproductive Healthcare 41:101013. [CrossRef]
- Watson H, Downe S. 2017. Discrimination against childbearing Romani women in maternity care in Europe: a mixed-methods systematic review. Reproductive Health 14(1):1. [CrossRef]
- Szabó L, Boros J. n.d. Health inequalities at birth within the Hungarian 2018–2019 birth cohort: socioeconomic differences of low birth weight infants. Presented at the European Population Conference 2022, Groningen, The Netherlands. https://epc2022.eaps.nl/abstracts/210050.
- Kósa K, Daragó L, Ádány R. 2011. A roma nők várandósgondozásban való részvételének jellemzői Magyarországon [in Hungarian]. Orvosi Hetilap 152(50):2003–2009.
- 8.
- Belügyminisztérium. 2025. Magyar Nemzeti Társadalmi Felzárkózási Stratégia 2030 [in Hungarian]. Budapest, Kormányzati Portál. https://kormany.hu/dokumentumtar/magyar-nemzeti-tarsadalmi-felzarkozasi-strategia-2030.
- European Commission. 2021. National Roma Integration Strategies: a common European framework. Brussels, EU Publications.
- Kósa K, Daragó L, Ádány R. 2012. Roma nők egészségügyi ellátáshoz való hozzáférése Magyarországon: akadályok és lehetőségek [in Hungarian]. International Journal of Public Health 57(3):395–401.
- Szabó L, Veroszta Z. 2023. A folyosó végén: Roma nők a várandósgondozás és szülészeti ellátás rendszerében [in Hungarian]. Esély 33(3):3–24.
- Balázs P, Grenczer A, Rákóczi I, Foley K, Paulik E. 2014. A roma újszülöttek testtömege: biomedicinális és társadalmi-gazdasági tényezők Magyarországon [in Hungarian]. Orvosi Hetilap 155(24):954–962.
- Laerd Statistics. n.d. Binomial logistic regression using SPSS Statistics. https://statistics.laerd.com/spss-tutorials/binomial-logistic-regression-using-spss-statistics.php.
- UCLA Institute for Digital Research and Education. n.d. Logit regression. https://stats.oarc.ucla.edu/spss/dae/logit-regression/.
- Ohuma EO. 2023. National, regional, and global estimates of preterm birth in 2020, with trends from 2010: a systematic analysis. The Lancet 402(10409):1261–1271. [CrossRef]
- European Foundation for the Care of Newborn Infants. 2021. Disparities in the follow-up of very preterm born children in Europe.
- Központi Statisztikai Hivatal. 2017. Koraszülöttek és kis súlyú újszülöttek Magyarországon [in Hungarian]. Budapest, Központi Statisztikai Hivatal. https://www.ksh.hu/docs/hun/xftp/idoszaki/pdf/koraszul16.pdf.
- Nemzeti Népegészségügyi és Gyógyszerészeti Központ. 2024. Bejelentett szexuális úton terjedő fertőző betegségek, 2023 [in Hungarian]. Budapest, Állami Népegészségügyi és Tisztiorvosi Szolgálat. https://www.antsz.hu/data/cms110647/OSAP_STD_2023_honlapra.pdf.
- Hajdu T, Kertesi G, Kézdi G. 2019. Health differences at birth between Roma and non-Roma children in Hungary: long-run trends and decompositions. Budapest, Institute of Economics, Centre for Economic and Regional Studies, Hungarian Academy of Sciences. https://www.econstor.eu/bitstream/10419/200343/1/1025776607.pdf.
- Szabó L, Boros J. 2023. Socio-economic differences among low-birthweight infants in Hungary: results of the Cohort ‘18 – Growing Up in Hungary birth cohort study. PLOS ONE 18(9):e0291117. [CrossRef]
Figure 1.
Low birth weight (%) by maternal smoking status.
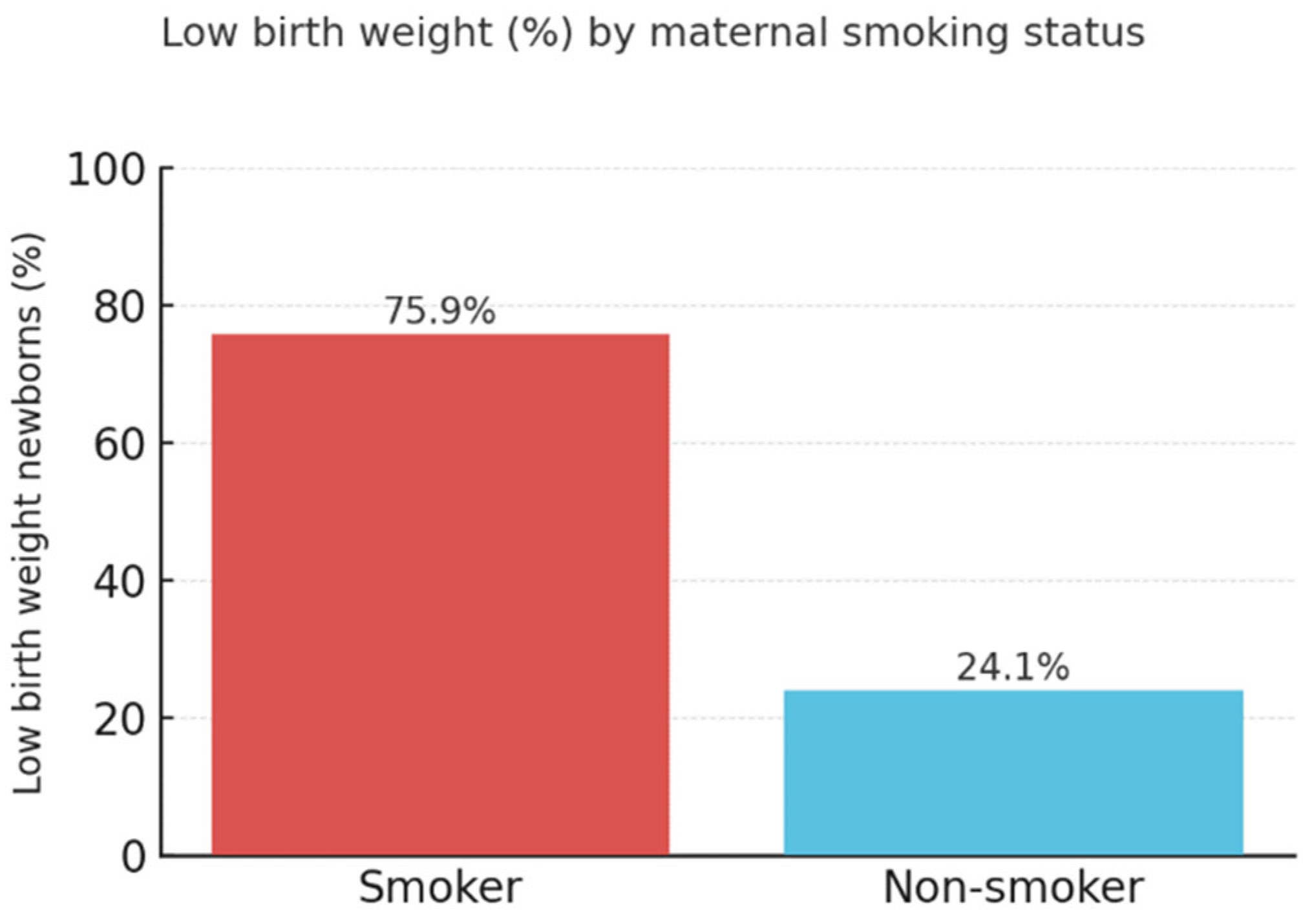
Figure 2.
Low birth weight (%) by maternal alcohol consumption.
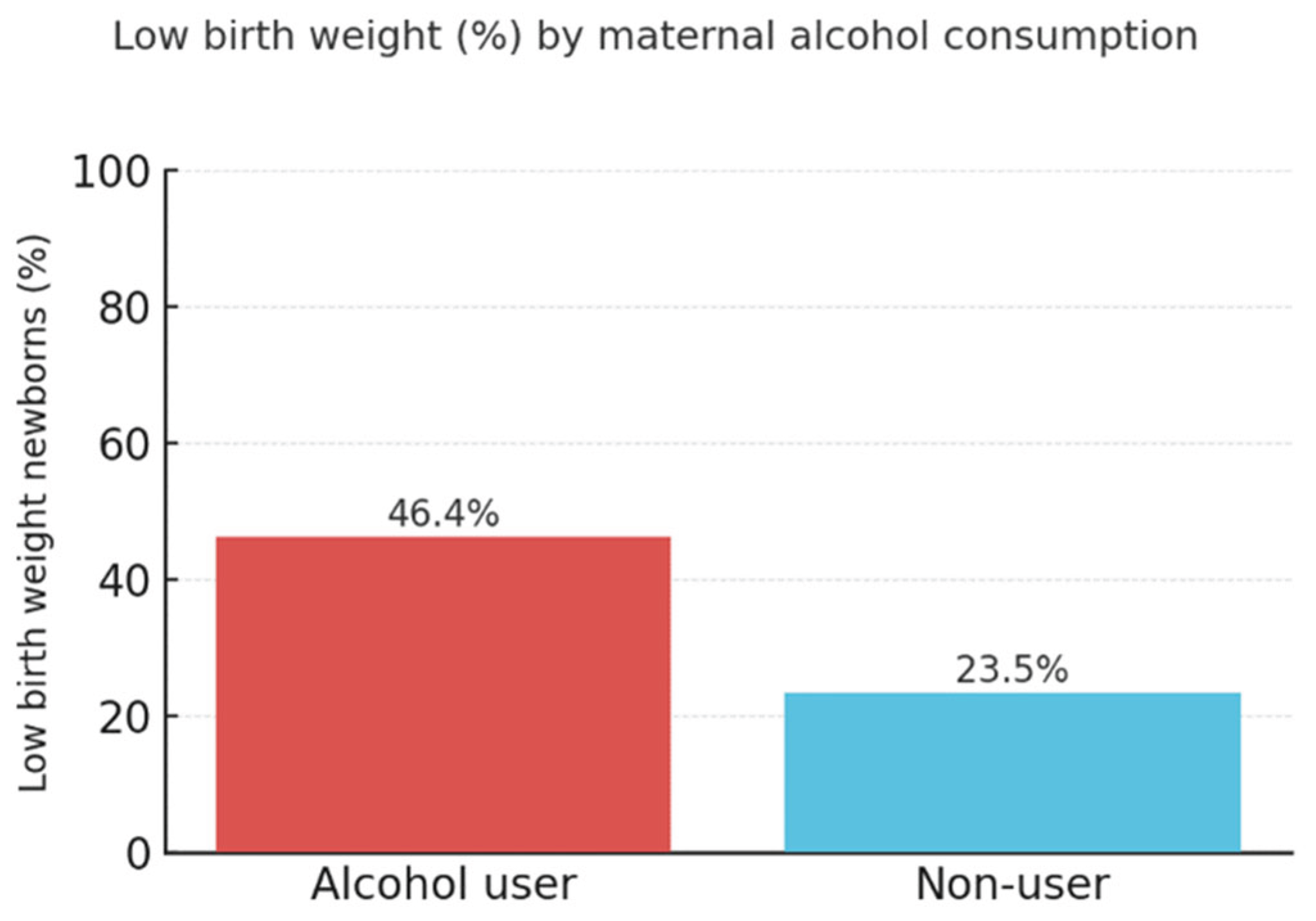
Figure 3.
Low birth weight (%) by antenatal care attendance.
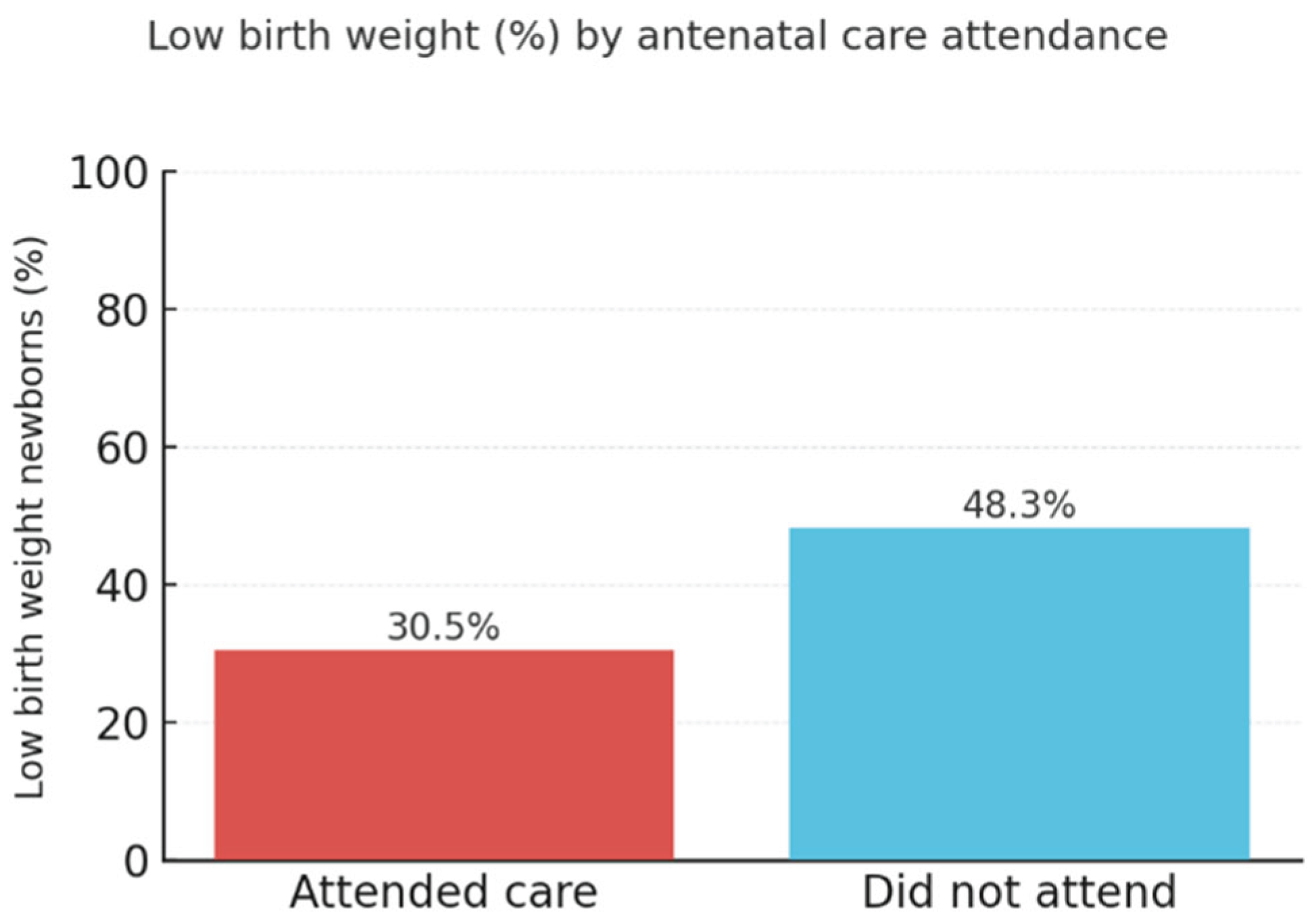
Figure 4.
Low birth weight (%) by vaginal infection status.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



