
Submitted:
04 August 2025
Posted:
08 September 2025
You are already at the latest version
Abstract
Background/Objectives: Angiotensin receptor-neprilysin inhibitor (AR-NI) has a well-established advantage over angiotensin converting enzyme inhibitor or angiotensin receptor blocker (ACEI/ARB) therapy in patients (pts) with heart failure with reduced ejection fraction (HFrEF), but in pts after acute myocardial infarction (AMI) with left ventricular (LV) systolic dysfunction the advantage of ARNI has not been clearly proven. To com-pare of the efficacy of ARNI versus ACEI/ARB therapy in patients with the first AMI in terms of improvement of post-infarction LV systolic function. Methods: Overall 1473 pts (990M, median age 71 [64;77]) with AMI (the first AMI, complete coronary revascularization, no prior: coronary revas-cularization, history of HF) hospitalized in 2022-2024 were enrolled into retrospective cross-sectional analysis. The study population was catego-rized into pts receiving ARNI and ACEI/ARB. Then based on ARNI subgroup included age, sex, and LV ejection fraction (LVEF) matching was performed by using the 1:1 nearest neighbour method without returning. Finally two groups (ARNI vs ACEI/ARB) of 30 pts were obtained and an-alysed at baseline and in 6-week follow-up. The improvement of post-infarction LV systolic function was obtained as LVEF value, ΔLVEF and relative ΔLVEF (ΔLVEF / baseline LVEF). Results: The comparison of baseline characteristics revealed borderline lower initial LVEF (30 vs 36%, p=0.076) and higher frequency of of SGLT-2 inhibitors use (70% vs 36.7%, p=0.01) in the ARNI subgroup. In 6-week follow-up in both subgroups a significant improvement in the median LVEF values was achieved: from median LVEF value 30% (27.3; 38) up to 37% (30; 43; p=0.0008) in ARNI and from median LVEF value 36% (33; 39) up to 45% (42; 52; p<0.0001) in ACEI/ARB subgroup. Median ΔLVEF in the ACEI/ARB subgroup was higher [10% (6; 12)] than in the ARNI subgroup [6% (2; 10.25), p=0.018]. Similarly median relative ΔLVEF was higher in the ACEI/ARB subgroup [30% (15.4; 40)] than in the ARNI group [17.5% (7; 31.9), p=0.047]. Conclusions: Our current experience in ARNI therapy after AMI is promising, however, it is limited to a small group of patients with severe impairment of LV systolic function. Regardless of significant improvement of baseline LVEF observed in patients receiving both ACEI/ARB and ARNI in 6 week follow-up the value of absolute and relative LVEF increase were higher in subjects treated with ACEI/ARB. The clinical efficacy of early use of ARNI in the setting of AMI needs further evaluation.
Keywords:
ARNI
; AMI
; ACEI/ARB
; angiotensin receptor-neprilysin inhibitor
; acute myocardial infarction
; post-infarction left ventricular systolic dysfunction
1. Introduction
The use of angiotensin receptor neprilysin inhibitor (ARNI) in patients after acute myocardial infarction (AMI) remains an area of intense clinical research and debate. The data to date clearly support the benefits of sacubitril/valsartan in patients with heart failure with reduced ejection fraction (HFrEF), but its efficacy in the post-myocardial infraction (MI) population with left ventricular systolic dysfunction has not yet been unequivocally proven.
The landmark PARADIGM-HF trial demonstrated that ARNI was superior to enalapril in reducing the risk of cardiovascular death and hospitalization for heart failure, leading to a change in guidelines that made it the preferred therapy for patients with HFrEF [1,2,3]. This raised the question of whether even earlier administration of ARNI initiated soon after MI in patients with impaired LVEF but not yet with symptomatic heart failure could offer additional benefits in preventing remodeling and improving survival compared with conventional ACEI-based pharmacotherapy. The PARADISE-MI trial was designed to address this question, however the primary outcome showed no statistically significant difference between the two groups in the composite endpoint of death from cardiovascular causes or incident heart failure (HF), whichever occurred first [4]. The PARADISE-MI Echocardiographic Substudy also failed to demonstrate significant differences between ARNI and ramipril in terms of changes in left ventricular ejection fraction (LVEF) or left atrial volume (LAV) after 8 months of treatment [5].
In recent years, there have been many studies on the use of ARNI in MI. These studies are based on animal models, randomized clinical trials, systematic reviews, and meta-analyses. The results of these studies indicate the advantage of ARNI use over ACEI/ARB in patients with MI, or at least suggest that ARNI use is non-inferior to conventional drug therapy. Additionally, there are many studies on animal models that indicate a number of benefits resulting from the use of ARNI, such as antiarrhythmic and anti-Inflammatory effects on post-MI scar, ameliorates cardiac function and ventricular remodeling and myocardial protective effect.
In our clinical practice, we always try to make decisions based on the latest medical knowledge and with the best interests of our patients in mind. In this article, we want to present the results of study on real clinical practice using ARNI in patients with AMI, especially in patients with significantly reduced LVEF. Finally, the aim of the study was to compare of the efficacy of ARNI versus ACEI/ARB therapy in patients with the first AMI in terms of improvement of post-infarction left ventricular systolic function.
2. Materials and Methods
2.1. Data Collection and Study Design
The study was conducted as a retrospective one-centre cross-sectional analysis of 1571 consecutive hospitalizations for AMI. Into analysis, we included patients with a diagnosis of AMI using the International Classification of Diseases (ICD) billing codes (10th edition, I21.X). The analysis comprised patients hospitalized in the I Department of Cardiology, the Medical University of Silesia in Katowice from January 2022 to December 2024.
Inclusion and exclusion criteria were a key part of this study. The study included patients aged 18 years or older with a first diagnosis of myocardial infarction, who underwent percutaneous revascularization of the infarct-related coronary artery followed by complete revascularization during current hospitalization, had a LVEF of 40% or less, and were enrolled in coordinated specialist care after a MI (‘’KOS zawał” programe).
Patients were excluded if they had a history of previous MI or coronary revascularization, a history of HF or angioedema, co-occurrence of another heart disease affecting the LVEF, severe hepatic or renal dysfunction, coexisting severe diseases of the immune, hematopoietic, or respiratory systems, or systemic diseases, presence of malignant tumour, exclusion criteria also included the death of the patient during hospitalization and the lack of complete clinical data in the medical records. A summary of the inclusion and exclusion criteria is presented in Table 1.
Among all 1571 hospitalizations, 1473 individual patients were identified whose first hospitalization was analysed. The study population was divided based on ARNI or ACEI/ARB administration and analysed using the inclusion and exclusion criteria. In the first stage, after taking into account patient death, history of HF, previous MI or coronary revascularization and lack of inclusion in the coordinated care program (KOS-zawał program), 1354 patients were excluded from the study. In this way, 119 patients were selected and further analysed. In second stage, upon application of additional criteria such as incomplete revascularization during current hospitalization, incomplete clinical data in the medical records, malignant tumour in medical history, qualification for coronary artery bypass grafting (CABG), co-occurrence of another heart disease affecting the LVEF an additional 43 patients were excluded and the remaining 76 patients (30 treated with ARNI and 46 treated with ACEI/ARB) were included into detailed analysis and matching. All patients were compensated at discharge and received an optimal medical therapy of AMI and HFrEF including dual antiplatelet therapy, lipid-lowering treatment, ACEIs/ARB (quinapril, enalapril, perindopril, ramipril, zofenopril / telmisartan, valsartan) or ARNI, mineralocorticoid-receptor antagonists (MRAs), beta-blockers, and diuretics in patients with symptoms and/or signs of congestion. The data were obtained from electronic medical records.
2.2. Matching
Taking into regard differences in the sex, age, LVEF and between the ARNI and ACEI/ARB subgroups, matching was performed by 1:1 nearest neighbour (NN) method without returning. The matching resulted in two groups, each with 30 patients where the mean age, LVEF, and gender proportions were more comparable between both groups. Subgroups of 30 patients were subjected to further analysis to compare the baseline characteristics and clinical outcomes.
2.3. Outcomes
Outcomes analysis consisted of LVEF data obtained in 6 weeks and 4 months follow-up (a limited number of patients) and cardiovascular outcomes (median follow-up: 695 [456; 996] days). During the 6-week follow-up period, ACEI/ARB and ARNI doses were not escalated.
The improvement of post-infarction left ventricular systolic function was obtained as direct LVEF value, ΔLVEF and relative ΔLVEF. ΔLVEF was defined as final LVEF – baseline LVEF (where final LVEF is understood as LVEF after 6 weeks or 4 months of follow-up, and baseline LVEF as LVEF at the diagnosis of MI). Relative ΔLVEF was defined as the percentage change from baseline LVEF (percentage of baseline LVEF). Relative ΔLVEF = (final LVEF – baseline LVEF)/baseline LVEF ×100%. The mathematical formulas for ΔLVEF and relative ΔLVEF are shown below.
2.4. Statistical Analysis
The study population was first dichotomized into 2 groups, receiving ARNI or ACEI/ARB. Clinical characteristics and outcomes were compared between groups. Continuous variables were presented as mean ± standard deviation or median (1–3 quartile) and categorical as absolute values and percentages. Normality was verified using the Shapiro–Wilk test. The comparisons of groups were based on student’s two-sample t-tests, nonparametric Mann–Whitney U tests or chi-squared test, as appropriate. The Wilcoxon signed-rank test or Student's t-test for related variables was used to analyse related variables. A p-value ≤ 0.05 was considered statistically significant for all tests. Matching was performed by using the 1:1 nearest neighbour (NN) method without returning – at first the logistic regression model has been trained on the study population, secondly propensity scores were calculated for each patient. At last patients from the ARNI and ACEI/ARB subgroups were matched 1:1 using nearest neighbours (NN) algorithm with propensity score difference as a distance measure. All other analyses were performed using MedCalc® software.
3. Results
3.1. Study Population, Inclusion and Exclusion Criteria
In the years 2022-2024, there were 1571 hospitalizations due to AMI, of which 1473 individual patients were identified (990 men, median age 71 [64;77]). After applying the inclusion and exclusion criteria in the first stage, 1354 (91.9%) patients were excluded from the study. In the second stage, the remaining 119 (8.1%) patients were further analysed and based on the criteria provided, an additional 43 (2.9%) patients were excluded. The remaining 76 patients (5.2%) underwent matching and detailed analysis. The details of the analysis of the inclusion and exclusion criteria are presented in Figure 1.
3.2. Matching Results
Detailed analysis included 76 patients among whom two subgroups were distinguished: ARNI subgroup (39.5%; 27 men; age 58 ± 10 years) and ACEI/ARB subgroup (60.5%; 31 men; age 65 ± 10 years). The compared values of the study population before and after matching are detailed in Table 2. Density plots and distribution of propensity scores are presented in figure 2.
3.3. Comparison of Baseline Characteristics of ARNI and ACEI/ARB Subgroups
Patients in the two subgroups did not differ clinically. In both subgroups the mean age was about 60 years, 90% of patients were men and average BMI was about 29 kg/m2. The vast majority of patients (about 80%) were diagnosed with ST-Elevation Myocardial Infarction (STEMI). Additionally, no statistically significant differences were observed in basic laboratory results.
In the ARNI subgroup, patients had lower initial LVEF (30 vs 36%, p=0.076), however the difference was not statistically relevant.
In terms of comorbidities, both groups were quite similar with no substantial burden of multimorbidity. Most of them suffered from hypertension, hyperlipidemia and had a history of nicotine addiction. No statistically significant differences were observed between the subgroups.
Patients in both subgroups were treated in a similar way. The only difference was the rate of sodium-glucose co-transporter 2 (SGLT-2) inhibitors use, which was higher in the ARNI subgroup (70% vs 36.7%, p=0.01).

Table 3.
The clinical characteristics of ARNI and ACEI/ARB subgroups.
|
Factor |
ARNI subgroup n=30 n (%) or mean ± SD or median (1-3 quartile) |
ACEI/ARB subgroup n=30 n (%) or mean ± SD or median (1-3 quartile) |
p value |
|---|---|---|---|
| Basic characteristic | |||
| Age (years) | 58 ± 10 | 62 ± 10 | 0.14 |
| Sex – men (n%) | 27 (90%) | 26 (86.7%) | 0.69 |
| BMI (kg/m2) | 29 ± 4.5 | 28.7 ± 4.2 | 0.8 |
| Type of myocardial infarction | |||
| STEMI (n%) | 24 (80%) | 23 (76.7%) | 0.756 |
| Anterior wall (n%) | 17 (56.7%) | 13 (43.3%) | - |
| Inferior wall (n%) | 4 (13.3%) | 6 (20%) | - |
| Anterior and lateral wall (n%) | 3 (10%) | 3 (10%) | - |
| Inferior and lateral wall (n%) | 0 (0%) | 1 (3.3%) | - |
| NSTEMI (n%) | 6 (20%) | 7 (23.3%) | 0.756 |
| Laboratory tests | |||
| Serum creatinine level (mg/dl) | 0.83 (0.75; 1.03) | 1.0 ± 0.25 | 0.1 |
| eGFR (ml/min/1.73) | 66.5 ± 12.8 | 67.8 ± 14.98 | 0.819 |
| eGFR <60 (ml/min/1.73) | 2 (6.7%) | 5 (16.7%) | 0.232 |
| Troponin max. level (ng/ml) | 3.46 (0.64; 5.12) | 1.03 (0.15; 3.48) | 0.085 |
| Hemoglobin level (g/dl) | 14.71 ± 1.33 | 14.86 ± 1.55 | 0.681 |
| Echocardiographic parameters | |||
| LVEF (%) | 30 (28; 38) | 36 (33; 39) | 0.076 |
| LVEDD (mm) | 52 (50; 59) | 53.18 ± 6.85 | 0.212 |
| LVESD (mm) | 40.12 ± 10.38 | 37.25 ± 7.8 | 0.257 |
| LVIVSd (mm) | 11.27 ± 1.71 | 12.1 ± 1.8 | 0.085 |
| LVPWd (mm) | 9.61 ± 1.47 | 10 (9; 11) | 0.204 |
| LAarea (cm2) | 21.86 ± 6.69 | 22.1 ± 4.57 | 0.927 |
| LAwidth (mm) | 40.72 ± 5.8 | 40 (38; 44.5) | 0.67 |
| Mitral regurgitation (II or III) (n%) | 3 (10%) | 2 (6.7%) | 1.0 |
| Tricuspid regurgitation (II or III) (n%) | 4 (13.3%) | 1 (3.3%) | 0.353 |
| Aortic regurgitation (n%) | 0 0 (%) | 2 (6.7%) | 0.492 |
| Aortic stenosis (n%) | 0 0 (%) | 1 (3.3%) | 1.0 |
| Concomitant diseases | |||
| Atrial fibrillation (n%) | 6 (20%) | 7 (23.3%) | 0.756 |
| Chronic kidney disease (n%) | 1 (3.3%) | 2 (6.7%) | 1.0 |
| Hypertension (n%) | 21 (70%) | 23 (76.7%) | 0.563 |
| Diabetes (n%) | 6 (20%) | 12 (40%) | 0.093 |
| Lipid disorders (n%) | 23 (76.7%) | 25 (83.3%) | 0.522 |
| Smoke history (n%) | 18 (60%) | 18 (60%) | 1.0 |
| History of stroke (n%) | 0 0 (%) | 1 (3.3%) | 1.0 |
| Asthma (n%) | 0 0 (%) | 2 (6.7%) | 0.492 |
| Chronic obstructive pulmonary disease (n%) | 1 (3.3%) | 3 (10%) | 0.612 |
| Medicinal treatment | |||
| ARNI (n%) |
24/26 mg – 29 (99.7%) 49/51mg – 1 (0.3%) |
- |
|
| ACEI/ARB (n%) | - | ACEI – 28 (93.3%) ARB – 2 (6.7%) |
|
| SGLT-2 inhibitor (n%) | 21 (70%) | 11 (36.7%) | 0.01 |
| Beta-blocker (n%) | 28 (93.3%) | 25 (83.3%) | 0.232 |
| Mineralocorticoid-receptor antagonist (n%) | 26 (86.7%) | 21 (70%) | 0.12 |
| Loop diuretic (n%) | 15 (50%) | 8 (26.7%) | 0.065 |
| Calcium channel blockers (n%) | 1 (3.3%) | 5 (16.7%) | 0.195 |
| Statin (n%) | 30 (100%) | 30 (100%) | 1.0 |
| Ezetimibe (n%) | 11 (36.7%) | 7 (23.3%) | 0.264 |
| Fibrate (n%) | 0 (%) | 2 (6.7%) | 0.492 |
| GLP-1 receptor agonists (n%) | 1 (3.3%) | 2 (6.7%) | 1.0 |
| Metformin (n%) | 2 (6.7%) | 8 (26.7%) | 0.08 |
| Sulfonylureas (n%) | 0 (%) | 4 (13.3%) | 0.112 |
| Insulin (n%) | 1 (3.3%) | 1 (3.3%) | 1.0 |
| Acetylsalicylic acid (n%) | 30 (100%) | 30 (100%) | 1.0 |
| P2Y12 inhibitors (n%) | 30 (100%) | 30 (100%) | 1.0 |
| NOAC (n%) | 6 (20%) | 7 (23.3%) | 0.756 |
ARNI: angiotensin receptor–neprilysin inhibitor; ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin II receptor blocker; STEMI: ST-elevation myocardial infarction; NSTEMI: non-ST-elevation myocardial infarction; BMI: body mass index; LVEF: left ventricular ejection fraction; LVEDD: left ventricular end-diastolic diameter; LVESD: left ventricular end-systolic diameter; LVIVSd: left ventricular interventricular septal diameter (at end-diastole); LVPWd: left ventricular posterior wall diameter (at end-diastole); LAarea: left atrial area; LAwidth: left atrial width; SGLT-2: sodium-glucose co-transporter 2; GLP-1: glucagon-like peptide-1; P2Y12: P2Y12 receptor (platelet ADP receptor subtype involved in platelet aggregation); NOAC: non-vitamin K antagonist oral anticoagulants.
3.4. LVEF Improvement in 6 Weeks Follow-Up in ARNI and ACEI/ARB Subgroups
In ARNI and ACEI/ARB subgroup during 6-week follow-up, a significant improvement in the LVEF was achieved. In ARNI subgroup the median improvement of LVEF was from 30% (27.3; 38) up to 37% (30; 43; p=0.0008) and in ACEI/ARB subgroup the median LVEF improvement was from 36% (33; 39) up to 45% (42; 52; p<0.0001). Median ΔLVEF in the ACEI/ARB subgroup was higher [10% (6; 12)] than in the ARNI subgroup [6% (2; 10.25), p=0.018]. Similarly median relative ΔLVEF was higher in the ACEI/ARB subgroup [30% (15.4; 40)] than in the ARNI group [17.5% (7; 31.9), p=0.047]. Additionally, the direct value of LVEF after 6 weeks was statistically significantly higher in the ACEI/ARB subgroup 45% (45; 52) than in the ARNI subgroup 37% (30; 43) p=0.003.
3.5. LVEF Improvement in 4 Months Follow-Up in ARNI and ACEI/ARB Subgroups
In 4 months follow-up, statistically significant improvement in LVEF was also achieved in both subgroups - from 30.5 ± 5.9% up to 40.2% ± 7.8 (p=0.0001) in ARNI and from 34.9 ± 7.3% up to 44.6 ± 10.9% (p=0.018) in ACEI/ARB subgroup. The values of ΔLVEF and relative ΔLVEF were similar between the subgroups.
The results of the direct LVEF improvement in 6 weeks and 4 months follow-up are presented in Figure 3 and Table 4 and Table 6. Detailed comparison of the LVEF data between the ARNI and ACEI/ARB subgroups at 6 weeks and 4 months follow-up are presented in Table 5 and Table 7.
Table 4.
Comparison of baseline and 6 weeks follow-up values of LVEF in ARNI and ACEI/ARB subgroups.
Table 4.
Comparison of baseline and 6 weeks follow-up values of LVEF in ARNI and ACEI/ARB subgroups.
| Subgroup | baselineLVEF (%) median (1-3 quartile) |
LVEF (%) in 6 weeks median (1-3 quartile) |
p value |
|---|---|---|---|
| ARNI n=29 | 30 (27.3; 38) | 37 (30; 43) | 0.0008 |
| ACEI/ARB n=30 | 36 (33; 39) | 45 (42; 52) | <0.0001 |
Table 5.
Comparison of LVEF data in ARNI and ACEI/ARB subgroups in the context of 6-week follow-up.
| Factor | ARNI subgroup n=29 median (1-3 quartile) |
ACEI/ARB subgroup n=30 median (1-3 quartile) |
p value |
|---|---|---|---|
| baseline LVEF (%) | 30 (27.3; 38) | 36 (33; 39) | 0.072 |
| LVEF (%) in 6 weeks | 37 (30; 43) | 45 (42; 52) | 0.003 |
| ΔLVEF (%) | 6 (2; 10.25) | 10 (6; 12) | 0.018 |
| relative ΔLVEF (%) | 17.5 (7; 31.9) | 30 (15.4; 40) | 0.047 |
Table 6.
Comparison of baseline and 4 months follow-up values of LVEF in ARNI and ACEI/ARB subgroups.
Table 6.
Comparison of baseline and 4 months follow-up values of LVEF in ARNI and ACEI/ARB subgroups.
| Subgroup | baselineLVEF (%) n (%) or mean ± SD |
LVEF (%) in 6 weeks n (%) or mean ± SD |
p value |
|---|---|---|---|
| ARNI n=20 | 30.5 ± 5.9 | 40.2 ± 7.8 | 0.0001 |
| ACEI/ARB n=7 | 34.9 ± 7.3 | 44.6 ± 10.9 | 0.0313 |
Table 7.
Comparison of LVEF data in ARNI and ACEI/ARB subgroups in the context of 4-months follow-up.
Table 7.
Comparison of LVEF data in ARNI and ACEI/ARB subgroups in the context of 4-months follow-up.
|
Factor |
ARNI subgroup n=20 n (%) or mean ± SD |
ACEI/ARB subgroup n=7 n (%) or mean ± SD |
p value |
|---|---|---|---|
| baseline LVEF (%) | 30.5 ± 5.9 | 34.85 ± 7.27 | 0.073 |
| LVEF (%) in 4-months | 40.2 ± 7.7 | 44.6 ± 10.9 | 0.025 |
| ΔLVEF (%) | 9.65 ± 8.6 | 9.71 ± 8.01 | 0.986 |
| relative ΔLVEF (%) | 35.6 ± 34.07 | 30.11 ±27.8 | 0.705 |
3.6. Clinical Outcomes in ARNI and ACEI/ARB Subgroups
During the 1-3 years (695 [456; 996]) days follow-up, 1 patient (3.3%) in the ARNI group and 2 (6.7%) patients in the ACEI/ARB group died. In the ACEI/ARB group, 3 (10%) patients were re-hospitalized due to HF decompensation or reinfarction. The differences were statistically insignificant (Table 8).
4. Discussion
Activation of the renin-angiotensin-aldosterone system (RAAS) and increased activity of the sympathetic nervous system are important elements of the pathophysiology of heart failure after myocardial infarction. The RAAS plays a key role in the process of adverse left ventricular remodeling through pro-inflammatory, pro-fibrotic and hypertrophic effects. Inhibition of this system by ACEI or ARB is a key role in the pharmacotherapy of HF. The second important system involved in the pathophysiology of HF is the natriuretic system, regulated by neprilysin - an enzyme that breaks down natriuretic peptides with vasodilatory, antifibrotic and diuretic effects. Inhibition of neprilysin (e.g. sacubitril) leads to an increase in the concentration of these beneficial peptides, which counteracts the action of the RAA and adrenergic systems. Early initiation of adequate pharmacotherapy after AMI, especially in patients with left ventricular dysfunction, is crucial to prevent progression to chronic HFrEF and to limit adverse myocardial remodeling. Current European Society of Cardiology (ESC) guidelines recommend initiating ACEI or ARB therapy as early as possible after MI, especially in patients with reduced LVEF or signs of HF [6].
The results of our work are a summary of the experiences of one center in the use of ARNI in patients with AMI and significant post-infarction left ventricular systolic dysfunction. At a time when ARNI has a well-established position in the current ESC guidelines on the treatment of HF [2,3], its use in patients with AMI (despite evidence of non-inferiority compared to conventional ACEI/ARB-based pharmacotherapy) has not been clearly defined in current guidelines [6].
Although the retrospective nature of the study, we made every effort to ensure that the impact of ARNI on the parameters we assessed was clear and not confounded by other variables. Therefore, we employed very detailed and extensive inclusion and exclusion criteria to obtain a population of patients who were free from other diseases, had no previous history of HF, and this was their first episode of coronary artery disease (CAD). We believe we met these assumptions, and the presented results support this, as as the patients had no significant underlying disease burden, except than hypertension, diabetes, hyperpilidemia, obesity, and smoking, which are themselves risk factors for CAD. A second important objective was to obtain as similar populations as possible in the ARNI and ACEI/ARB subgroups. Therefore, we employed 1:1 nearest neighbour matching – the obtained subgroups did not differ in terms of clinical characteristics, type of MI, basic laboratory test results, or pharmacotherapy. The only significant variable was a higher frequency of SLGT-2 inhibitor use (p = 0.01) and a trend toward lower LVEF (p = 0.076) in the ARNI subgroup. All these factors ultimately influenced the size of the analysed group, which consisted of 60 patients, representing only 4.1% of all patients hospitalized with a diagnosis of AMI during the study period.
Both ARNI and ACEI/ARB significantly improved post-infarction left ventricular systolic dysfunction at 6 weeks and 4 months of follow-up. In the context of the discussed results, it should be noted that the ARNI subgroup had a lower baseline LVEF (30% [28; 38]) in bordeline manner than the ACEI/ARB (36% [33; 39]). What is of importance, the ACEI/ARB subgroup demonstrated a significantly greater increase in LVEF and relative LVEF compared to ARNI subgroup in 6 week follow-up. After 4 months the differences between the subgroups were blurred, and in fact ARNI showed an advantage in improving LVEF. This may suggest that the clinical benefit of ARNI treatment becomes apparent over the longer term, which requires further observation. In the case of death and rehospitalization during (695 [456; 996]) days follow-up period, single cases were recorded in both subgroups.
Experimental studies in animal models suggest that sacubitril/valsartan may have a range of beneficial cardioprotective effects following myocardial infarction. ARNI has been shown to improve LVEF, reduce adverse cardiac remodeling, limit myocardial fibrosis, and modulate post-infarction inflammation and arrhythmogenicity. In studies conducted on animal models (pigs, rats, mice), sacubitril/valsartan significantly improves cardiac function and inhibits remodeling by modulating several molecular pathways. These include suppression of the tryptophan–kynurenine axis, reduction of pro-inflammatory cytokines, promoting macrophage polarization to the M2 phenotype, activating PI3K/Akt signaling, and inhibiting NLRP3-dependent pyroptosis via the TAK1/JNK pathway [7,8,9,10]. Antiarrhythmic effects of sacubitril/valsartan were also demonstrated in a rabbit MI model, where the drug ameliorated postinfarct heart function impairment and electrophysiologic remodeling, leading to reduced ventricular tachyarrhythmia inducibility by stabilizing the infarct scar and myocardial electrophysiology [11]. Other studies have shown that ARNI reduces collagen synthesis and myocardial fibrosis by inhibiting the synthesis pathways of TGF-β1, Smad proteins, and Wnt/β-catenin pathway-related proteins [12,13]. Reports from the rat model are reflected in the clinical trial conducted on 73 patients – the results of the research paper of Wang, L et. Al. (2024) confirm that early use of sacubitril/valsartan after AMI has a significant benefit, may have a beneficial effect on ventricular remodeling, regulate the expression levels of TGF-β1 and Smad3, inhibit the TGF-β1/Smad3 signaling pathway, improve left ventricular function and have a beneficial effect on quality of life, while maintaining a safety profile [14]. The results of these studies suggest that sacubitril/valsartan may play a multifaceted role in preventing adverse cardiac remodeling post-MI, including anti-fibrotic, anti-inflammatory, and antiarrhythmic effects, mediated through diverse signaling pathways. Although these data require further confirmation in clinical trials, they provide a strong biological basis for further testing of ARNI in patients with AMI, particularly those at high risk for left ventricular remodeling.
The benefits of using ARNI in AMI are not limited to experimental studies, but are also confirmed in everyday clinical settings, in real-world patient populations. In the study by Liu et al. (2024), it was shown that in patients with acute coronary syndrome (ACS) and concomitant reduced LVEF, sacubitril/valsartan treatment and routine treatment led to improvement in LVEF, NT-proBNP concentration and left ventricular dimensions, while in the ARNI group the assessed parameters were significantly improved than those in the routine group. An additional conclusion from the study is that patients with ACS and reduced LVEF may derive greater benefits [15]. Fan, H. et al. (2023) in a group of 78 patients with AMI undergoing PCI, treated for at least 3 months, confirmed the superiority of ARNI over irbesartan in terms of improving cardiac function, preventing ventricular remodeling and lower incidence of major adverse cardiovascular events (MACE) [16]. The randomized, single-blind, parallel-group, controlled trial performed by Yin, H. et al. (2024) on 142 patients with AMI complicated by moderate to severe mitral regurgitation (MR) treated with ARNI or benazepril showed that early use of ARNI can significantly reduce MR, improve ventricular remodeling, and decrease HF hospitalization compared to ACEI in 12 months follow-up [C17]. In the context of comparisons with ramipril, the clinical trials conducted by Rezq, A. et al. (2021) showed that sacubitril/valsartan may be a safe and effective alternative even in patients with STEMI complicated by cardiogenic shock, and that ARNI therapy led to a lower rate of hospitalization due to HF in a 6-month follow-up (18% vs. 38%) [18]. In another study, the same team showed that in patients after STEMI, ARNI additionally has a more beneficial effect on improving LVEF and LV remodeling compared to ramipril, with the same safety profile [19]. Altogether, these clinical studies confirm that in real hospital practice sacubitril/valsartan can be an effective and safe element of post-infarction therapy, bringing benefits both in terms of echocardiographic parameters and hard endpoints. Importantly, the obtained effects are consistent with previously described mechanisms of action observed in experimental models.
SGLT-2 inhibitors have been shown to reduce the risk of worsening HF and cardiovascular death in patients with HF, regardless of LVEF or diabetes status [20,21,22,23]. Although they are not yet routinely recommended after AMI, emerging evidence suggests their potential role in early post-AMI management. The EMPACT-MI and EMMY trials demonstrated that early administration of empagliflozin may improve cardiac function, accelerate NT-proBNP reduction, and support reverse remodeling, indicating a possible benefit in preventing heart failure progression in this population [24,25]. Among patients with a lower baseline LVEF, we decided to start this therapy more often, the result of which patients who received ARNI were also significantly more likely to be started on SLGT 2 inhibitors (21 vs. 11 patients, p = 0.01). In light of the latest reports, this may have some impact on the interpretation of our study, but the combination of RAAS inhibitors and SGLT-2 inhibitors in this group of patients is necessary and could not be omitted.
It should be noted that positive ARNI effect of LV remodeling was well-documented in de novo dilated cardiomyopathy (DCM). The results of the PROVE-HF and EVALUATE-HF studies provide substantial evidence for the beneficial effect of ARNI therapy on left ventricular remodeling in patients with HFrEF. In the PROVE-HF study, 12 months of ARNI therapy were associated with a parallel decrease in NT-proBNP and significant improvements in LVEF and left ventricular volume [26]. In the EVALUATE-HF study, significant improvements in left ventricular structural and functional parameters were observed in the ARNI group compared with enalapril after just 12 weeks [27]. In patients with non-ischemic DCM, earlier ARNI administration was associated with greater LVEF improvement and more effective reverse remodeling [28]. In the case of post-AMI remodeling and scar in LV wall a potent positive ARNI effect is no so important.
In recent years, a number of meta-analyses and systematic reviews have been published assessing the efficacy and safety of early use of ARNI in AMI patients. In the meta-analysis by Liu Y. et al. (2024), including studies involving patients after percutaneous coronary angioplasty (PCI), it was shown that treatment with sacubitril/valsartan led to a significant reduction in both left ventricular end-diastolic and end-systolic dimensions and volumes, as well as with, an improvement in ejection fraction (by an average of 3.9 percentage points). Additionally, an improvement in physical capacity was noted (an increase in the 6-minute walk test [6-WMT] distance by 43m) and a decrease in NT-proBNP levels. Importantly, a reduction in the risk of MACE (by 64%), reinfarction (by 46%) and hospitalization for heart failure (by 65%) was also noted without an increase in the risk of renal failure, hyperkalemia or significant hypotension [29]. Similar results were obtained in the review by Zhou et al. (2022), which showed that ARNI use was associated with a reduction in left ventricular end-diastolic dimensions, as well as with improved exercise tolerance (increase 6-MWT distance by ~48m). The risk of cardiovascular events was reduced by 28%, and the risk of rehospitalization for HF by 27%. Although symptomatic hypotension was slightly more frequent in the analysis, cough was less frequent than in the ACEI group. Additionally, ARNI increased LVEF and decreased NT-proBNP level was better at 6 months and within 3 months of follow-up compared with the control group, but there was no significant difference at the 12-month follow-up [30]. Meta-analysis by Wang, F. et al. (2024) showed reduction in major adverse cardiovascular and cerebrovascular events (MACCE) (by 52%), rehospitalizations (by 64%) and an improvement in LVEF by an average of 2.86 percentage points. At the same time, no differences in adverse events were found between the study and control groups. [31]. In the meta-analysis by Abdullah -, et al. (2024), a significant reduction in the risk of hospitalization for HF (by 21%) and MACE (by 16%) was demonstrated, as well as a decrease in NT-proBNP levels. Although the improvement in LVEF was greater in the control group compared with ARNI, the observed differences suggest a therapeutic benefit in selected patients [32]. In the study conducted by She, J. et.al (2021) showed that patients who received ARNI had significantly lower rates of the composite cardiovascular outcome than ACEI and ARB patients. Patients who received ARNI had lower rates of cardiovascular deaths, and the subanalysis showed that the greatest benefit was experienced by patients younger than 60 years of age and with LVEF less than 40% [33].
Available systematic reviews and meta-analyses suggest that, early use of ARNI after MI can lead to significant improvements in cardiac remodeling and echocardiographic parameters, ARNI therapy can reduce the risk of cardiovascular events, including hospitalization for HF, and this drug has a favorable safety profile, with well-tolerated hypotension and a lower incidence of adverse events typical of ACEIs, such as cough. These results are consistent with the observations from our study, indicating a potential benefit of early initiation of ARNI after MI, especially in patients with reduced LVEF. Although the results are promising, further large, randomized trials with long-term follow-up are needed to clearly assess the effect of this therapy on survival and progression to HF.
Respective limitations secondary to the retrospective character of the study should be addressed when interpreting the results. First, the results may reflect local practice because the study was conducted at a single center. The small group of patients subjected to the final analysis resulted from very detailed inclusion and exclusion criteria, which we consider to be a strong point of our work, however, a low sample size may influence the nature of the cohort and limits some analysis. Certain limitations arose from the retrospective nature of the study. An important inclusion criterion was participation in the “KOS-zawał” program, which enabled follow-up of patients in the hospital outpatient clinic, however, in some patients there was missing data in the medial records, which resulted in a reduction of the 4-month follow-up group. It should be emphasized that during the 6-week follow-up period, the doses of ACEI/ARB and ARNI were not escalated, which is associated with failure to achieve the optimal therapeutic effect, especially in the ARNI group, where 99.7% of patients started treatment with the lowest dose. Moreover, different ACEI/ARB were administered. An additional confounding factor may be the effect of SGLT-2 inhibitors on adverse remodeling, which were more frequently used in the ARNI group. We believe that, despite the study limitations, our study provides important conclusions from the use of ARNI in patients with AMI in real-life experience and shows a significant trend of which patients may benefit most from ARNI use. Finally, our results confirm the findings from numerous clinical trials, meta-analyses and reviews, and the molecular basis is confirmed by experiments conducted in animal models.
5. Conclusions
Our current experience in ARNI therapy after AMI promising, however, it is limited to a small group of patients with severe impairment of LV systolic function. Regardless of significant improvement of baseline LVEF observed in AMI patients receiving both ACE/ARB and ARNI in 6 weeks and 4 months of follow-up the value of absolute and relative LVEF increase were higher in subjects treated with ACEI/ARB. Importantly, after 4 months of therapy the differences between the groups were blurred, and in fact ARNI showed an advantage in improving LVEF. There were no differences in cardiovascular outcomes between ARNI and ACEI/ARB populations.The use of ARNI and early in the setting of AMI is becoming more widespread; nevertheless, additional research is necessary.
6. Patents
Author Contributions
Conceptualization, R.N. and K.M.-S.; methodology, R.N. and K.M.-S.; software -; validation, R.N., A.P. and K.M.-S.; formal analysis, R.N. and A.P..; investigation, R.N., M.T.N., B.G., G.B., M.B, K.C.-R., M.S., A.N. and M.N.; resources, R.N., B.G., G.B., M.B, K.C.-R., M.S., A.N. and M.N; data curation, R.N.; writing—original draft preparation, R.N., M.T.N., B.G., G.B., M.B, K.C.-R., M.S., A.N. and M.N.; writing—review and editing, R.N. and K.M.-S.; visualization, R.N. and K.M.-S.; supervision, K.M.-S.; project administration, R.N. and K.M.-S.; funding acquisition, K.M.-S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Ethics Committee of the Medical University of Silesia. The Bioethics Committee of Medical University of Silesia agreed to the research using the retrospective data analysis method. .
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to confidentiality of the research.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations:
The following abbreviations are used in this manuscript:
| 6-WMT | 6-minute walk test |
| ACS | acute coronary syndrome |
| AMI | acute myocardial infarction |
| ARNI | angiotensin receptor–neprilysin inhibitor |
| CABG | coronary artery bypass grafting |
| CAD | coronary artery disease |
| DCM | dilated cardiomyopathy |
| ESC | European Society of Cardiology |
| HF | heart failure |
| HFrEF | heart failure with reduced ejection fraction |
| LAV | left atrial volume |
| LVEF | left ventricular ejection fraction |
| MACE | major adverse cardiovascular events |
| MACCE | major adverse cardiovascular and cerebrovascular events |
| MI | myocardial infarction |
| MR | mitral regurgitation |
| MRA | mineralocorticoid receptor antagonist |
| NN | nearest neighbour |
| RAAS | renin-angiotensin-aldosterone system |
| SGLT-2 inhibitors | sodium-glucose co-transporter 2 inhibitors |
| STEMI | ST-elevation myocardial infarction |
References
- McMurray, J.J.; Packer, M.; Desai, A.S.; et al. PARADIGM-HF Investigators and Committees. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014, 371, 993–1004. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; et al. ESC Scientific Document Group. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; et al. ESC Scientific Document Group. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart, J. 2023, 44, 3627–3639. [Google Scholar] [CrossRef]
- Pfeffer, M.A.; Claggett, B.; Lewis, E.F.; et al. PARADISE-MI Investigators and Committees. Angiotensin Receptor-Neprilysin Inhibition in Acute Myocardial Infarction. N Engl J Med. 2021, 385, 1845–1855. [Google Scholar] [CrossRef]
- Shah, A.M.; Claggett, B.; Prasad, N.; et al. Impact of Sacubitril/Valsartan Compared With Ramipril on Cardiac Structure and Function After Acute Myocardial Infarction: The PARADISE-MI Echocardiographic Substudy. Circulation. 2022, 146, 1067–1081. [Google Scholar] [CrossRef]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; et al. ESCScientific Document Group. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart, J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef]
- Martínez-Falguera, D.; Aranyó, J.; Teis, A.; et al. Antiarrhythmic and Anti-Inflammatory Effects of Sacubitril/Valsartan on Post-Myocardial Infarction Scar. Circ Arrhythm Electrophysiol. 2024, 17, e012517. [Google Scholar] [CrossRef]
- Gan, J.; Wang, Y.; Deng, Y.; et al. Sacubitril/valsartan ameliorates cardiac function and ventricular remodeling in CHF rats via the inhibition of the tryptophan/kynurenine metabolism and inflammation. Sci Rep. 2024, 14, 12377. [Google Scholar] [CrossRef]
- Jin, N.; Qiu, Y.; Zhang, K.; et al. Sacubitril/valsartan alleviates myocardial infarction-induced inflammation in mice by promoting M2 macrophage polarisation via regulation of PI3K/Akt pathway. Acta Cardiol. 2024, 79, 768–777. [Google Scholar] [CrossRef]
- Shen, J.; Fan, Z.; Sun, G.; et al. Sacubitril/valsartan (LCZ696) reduces myocardial injury following myocardial infarction by inhibiting NLRP3-induced pyroptosis via the TAK1/JNK signaling pathway. Mol Med Rep. 2021, 24, 676. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.C.; Wo, H.T.; Lee, H.L.; et al. Sacubitril/Valsartan Therapy Ameliorates Ventricular Tachyarrhythmia Inducibility in a Rabbit Myocardial Infarction Model. J Card Fail. 2020, 26, 527–537. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Guo, Y.; Wu, Y.; et al. Protective Effects of Sacubitril/Valsartan on Cardiac Fibrosis and Function in Rats With Experimental Myocardial Infarction Involves Inhibition of Collagen Synthesis by Myocardial Fibroblasts Through Downregulating TGF-β1/Smads Pathway. Front Pharmacol. 2021, 12, 696472. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zheng, X.; Zhang, C.; et al. Lcz696 Alleviates Myocardial Fibrosis After Myocardial Infarction Through the sFRP-1/Wnt/β-Catenin Signaling Pathway. Front Pharmacol. 2021, 12, 724147. [Google Scholar] [CrossRef]
- Wang, L.; Zhang, Y.; Xue, J.; et al. Early Application of Sacubitril Valsartan Sodium After Acute Myocardial Infarction and its Influence on Ventricular Remodeling and TGF-β1/Smad3 Signaling Pathway. Altern Ther Health Med. 2024, 30, 98–103. [Google Scholar]
- Liu, H.; Su, Y.; Shen, J.; et al. Improved heart function and cardiac remodelling following sacubitril/valsartan in acute coronary syndrome with HF. ESC Heart Fail. 2024, 11, 937–949. [Google Scholar] [CrossRef] [PubMed]
- Fan, H.; Wang, Y.; Wang, X.; et al. Effect of Emergency Percutaneous Coronary Intervention Combined with Sacubitril and Valsartan on the Cardiac Prognosis in Patients with Acute Myocardial Infarction. Int J Gen Med. 2023, 16, 499–505. [Google Scholar] [CrossRef]
- Yin, H.; Ma, L.; Zhou, Y.; et al. Efficacy of early administration of sacubitril/valsartan after coronary artery revascularization in patients with acute myocardial infarction complicated by moderate-to-severe mitral regurgitation: a randomized controlled trial. Heart Vessels. 2024, 39, 673–686. [Google Scholar] [CrossRef]
- Rezq, A.; Saad, M.; El Nozahi, M. Sacubitril/valsartan versus ramipril in patients with ST-segment Elevation Myocardial Infarction and cardiogenic SHOCK (SAVE-SHOCK): a pilot randomized controlled trial. Am J Cardiovasc Dis. 2021, 11, 734–742. [Google Scholar]
- Rezq, A.; Saad, M.; El Nozahi, M. Comparison of the Efficacy and Safety of Sacubitril/Valsartan versus Ramipril in Patients With ST-Segment Elevation Myocardial Infarction. Am J Cardiol. 2021, 143, 7–13. [Google Scholar] [CrossRef]
- McMurray, J.V.; Solomon, S.D.; Inzucchi, S.E.; et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef]
- Packer, M.; Anker, S.D.; Butler, J.; et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med. 2020, 383, 1414–1424. [Google Scholar] [CrossRef]
- Anker, S.D.; Butler, J.; Filippatos, G.; et al. Empagliflozin in heart failure with a preserved ejection fraction. N Engl J Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef]
- Solomon, S.D.; McMurray, J.V.; Claggett, B.; et al. Dapagliflozin in heart failure with mildly reduced or preserved ejection fraction. N Engl J Med. 2022, 387, 1089–1098. [Google Scholar] [CrossRef]
- Butler, J.; Jones, W.S.; Udell, J.A.; et al. Empagliflozin after Acute Myocardial Infarction. N Engl J Med. 2024, 390, 1455–1466. [Google Scholar] [CrossRef]
- Von Lewinski, D.; Kolesnik, E.; Tripolt, N.J.; et al. Empagliflozin in acute myocardial infarction: the EMMY trial. Eur Heart J. 2022, 43, 4421–4432. [Google Scholar] [CrossRef]
- Januzzi, J.J.; Prescott, M.F.; Butler, J.; et al. PROVE-HF Investigators Association. of Change in N-Terminal Pro-B-Type Natriuretic Peptide Following Initiation of Sacubitril-Valsartan Treatment With Cardiac Structure Function in Patients With Heart Failure With Reduced Ejection Fraction. J.A.M.A. 2019, 322, 1085–1095. [Google Scholar] [CrossRef]
- Desai, A.S.; Solomon, S.D.; Shah, A.M.; et al. EVALUATE-HF Investigators Effect of Sacubitril-Valsartan vs Enalapril on Aortic Stiffness in Patients With Heart Failure and Reduced Ejection Fraction: A Randomized Clinical Trial. J. A.M.A. 2019, 322, 1077–1084. [Google Scholar] [CrossRef]
- Kim, H.M.; Kim, K.H.; Park, J.S.; et al. Beneficial Effect of Left Ventricular Remodeling after Early Change of Sacubitril/Valsartan in Patients with Nonischemic Dilated Cardiomyopathy. Medicina (Kaunas). 2021, 57, 416. [Google Scholar] [CrossRef]
- Liu, Y.; Sun, Y.; Dai, W. Effect of sacubitril-valsartan on left ventricular remodeling in patients with acute myocardial infarction after primary percutaneous coronary intervention: a systematic review and meta-analysis. Front Pharmacol. 2024, 15, 1366035. [Google Scholar] [CrossRef]
- Zhou, X.; Zhu, H.; Zheng, Y.; et al. A systematic review and meta-analysis of sacubitril-valsartan in the treatment of ventricular remodeling in patients with heart failure after acute myocardial infarction. Front Cardiovasc Med. 2022, 9, 953948. [Google Scholar] [CrossRef]
- Wang, F.; Li, C.; Zhang, X. Sacubitril/valsartan improves the prognosis of acute myocardial infarction: a meta-analysis. Coron Artery Dis. 2024, 35, 231–238. [Google Scholar] [PubMed]
- –, A.; Rashid, M.; Soto, C.J.; et al. The Safety and Efficacy of the Early Use of Sacubitril/Valsartan After Acute Myocardial Infarction: A Meta-Analysis of Randomized Controlled Trials. Cureus. 2024, 16, e53784. [Google Scholar]
- She, J.; Lou, B.; Liu, H.; et al. ARNI versus ACEI/ARB in Reducing Cardiovascular Outcomes after Myocardial Infarction. ESC Heart Fail. 2021, 8, 4607–4616. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Detailed analysis of inclusion and exclusion criteria. ACEI: angiotensin-converting enzyme inhibitor; AMI: acute myocardial infarction; ARB: angiotensin II receptor blocker; ARNI: angiotensin receptor–neprilysin inhibitor; CABG: coronary artery bypass grafting; LVEF: left ventricular ejection fraction; PCI: percutaneous coronary intervention.
Figure 1.
Detailed analysis of inclusion and exclusion criteria. ACEI: angiotensin-converting enzyme inhibitor; AMI: acute myocardial infarction; ARB: angiotensin II receptor blocker; ARNI: angiotensin receptor–neprilysin inhibitor; CABG: coronary artery bypass grafting; LVEF: left ventricular ejection fraction; PCI: percutaneous coronary intervention.
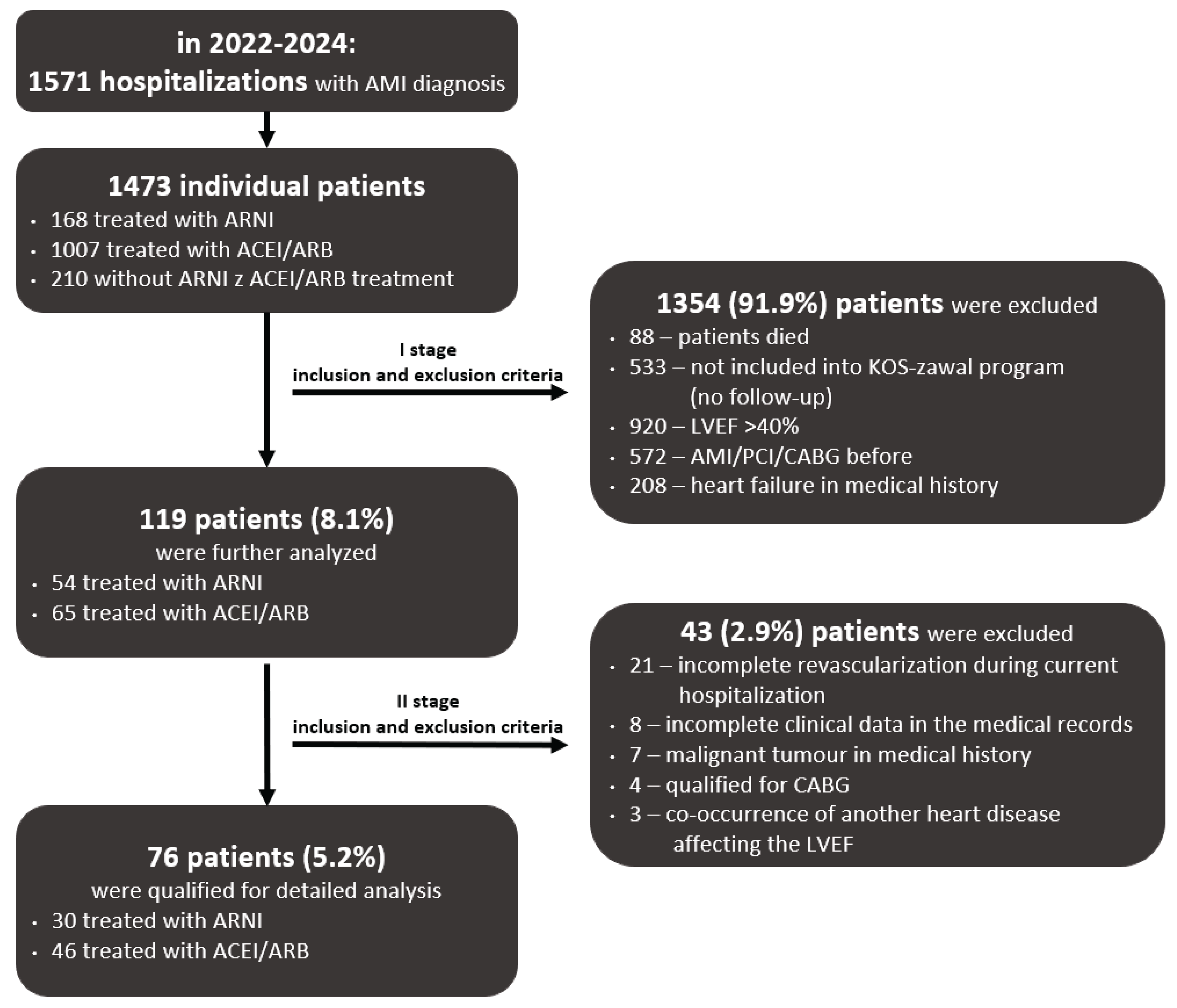
Figure 2.
Density plots and distribution of propensity scores before and after matching. ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin II receptor blocker; ARNI: angiotensin receptor–neprilysin inhibitor; LVEF: left ventricular ejection fraction.
Figure 2.
Density plots and distribution of propensity scores before and after matching. ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin II receptor blocker; ARNI: angiotensin receptor–neprilysin inhibitor; LVEF: left ventricular ejection fraction.
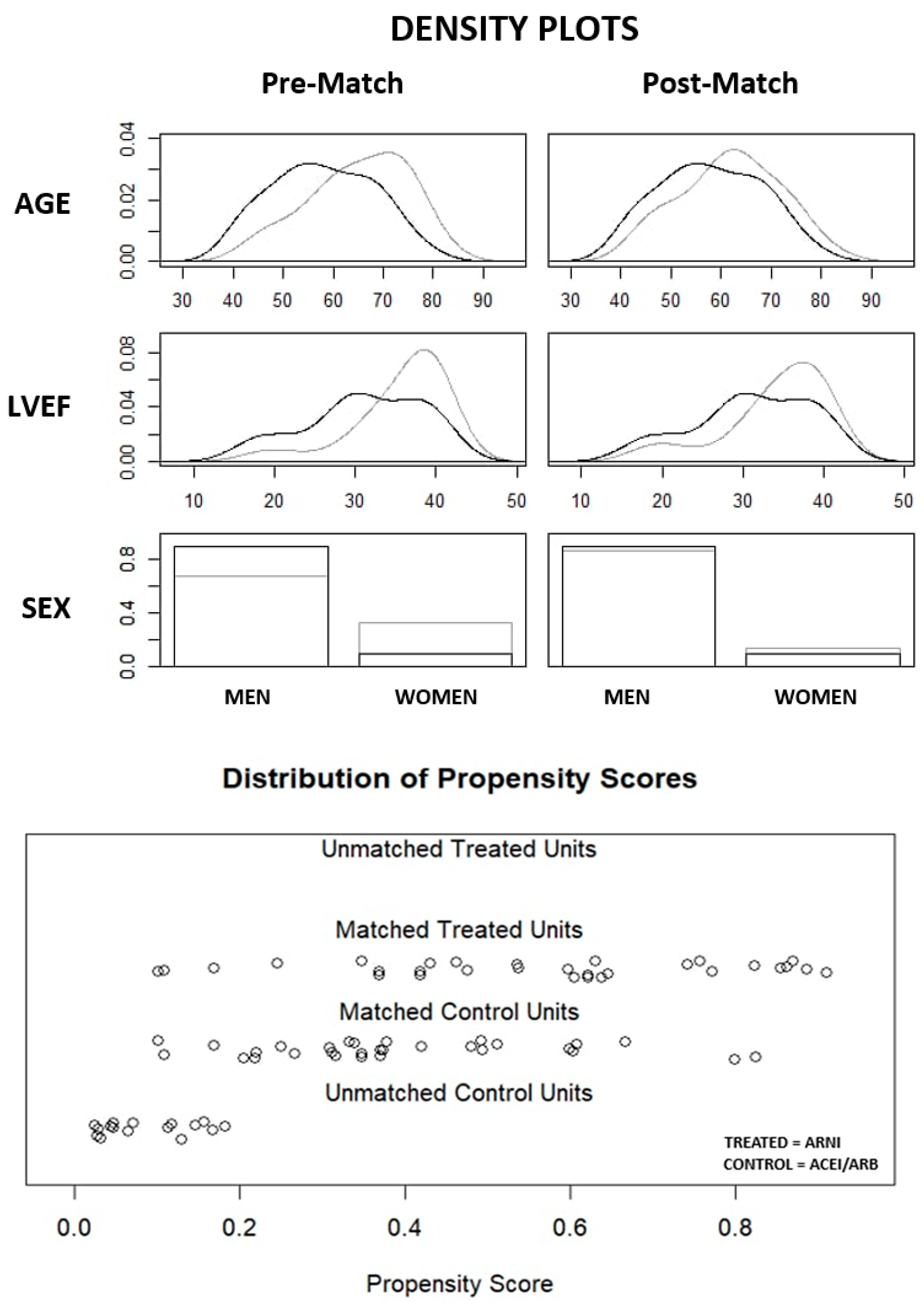
Figure 3.
Comparison of LVEF improvement in 6 weeks and 4 months follow-up in ARNI and ACEI/ARB subgroups. ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin II receptor blocker; ARNI: angiotensin receptor–neprilysin inhibitor; LVEF: left ventricular ejection fraction.
Figure 3.
Comparison of LVEF improvement in 6 weeks and 4 months follow-up in ARNI and ACEI/ARB subgroups. ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin II receptor blocker; ARNI: angiotensin receptor–neprilysin inhibitor; LVEF: left ventricular ejection fraction.
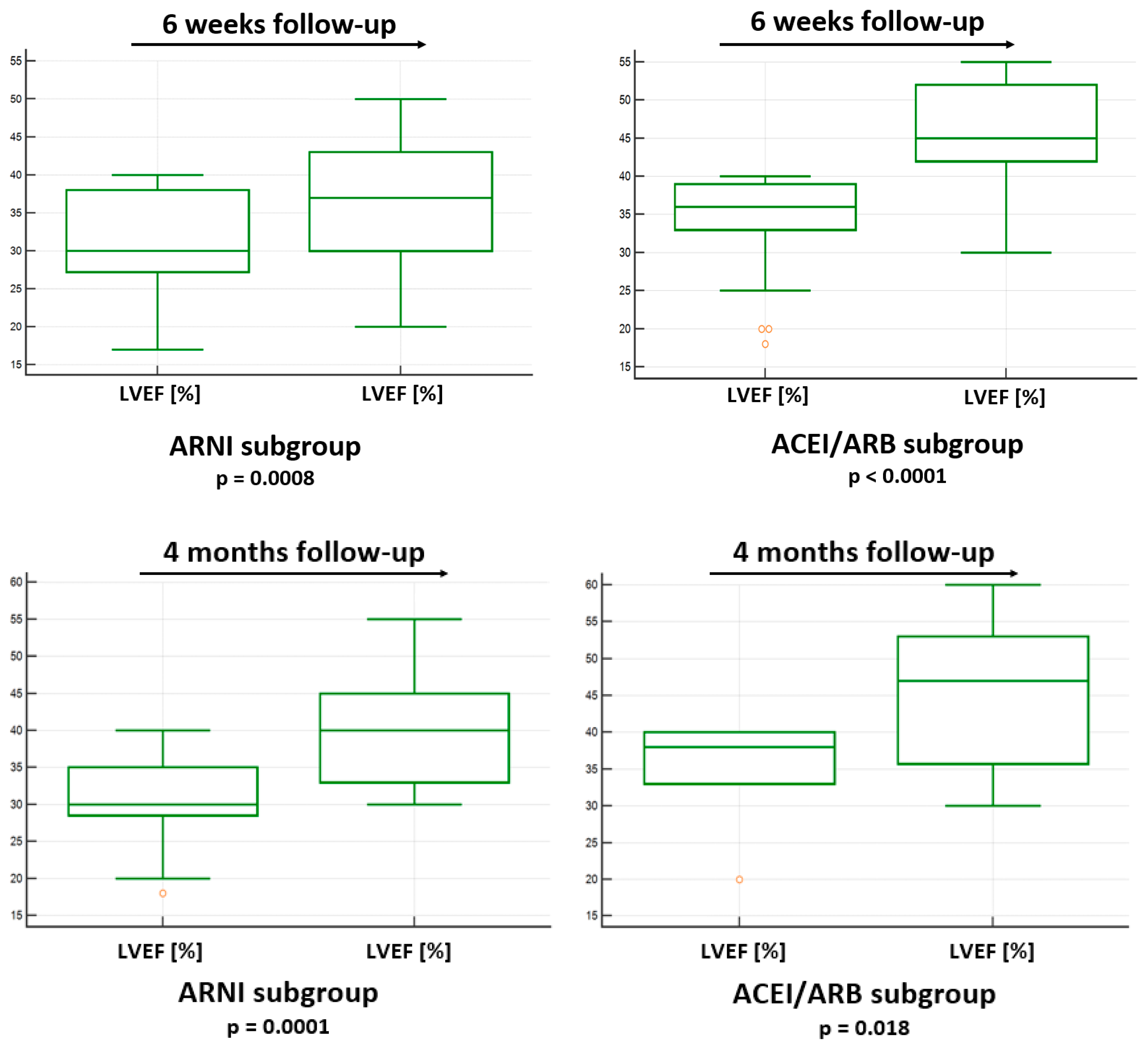
Table 1.
Inclusion and exclusion criteria.
| Inclusion criteria | Exclusion criteria |
|---|---|
| Age ≥ 18 years | 1) A history of previous myocardial infarction or coronary revascularization |
| First diagnosis of MI | 2) A history of HF or angioedema |
| Percutaneous revascularization of the infarct-related coronary artery and complete revascularization during current hospitalization | 3) Co-occurrence of another heart disease affecting the left ventricular ejection fraction |
| Post-infarction left ventricular systolic dysfunction (LVEF ≤ 40%) | 4) Severe hepatic or renal dysfunction |
| Patients enrolled into coordinated specialist care after a MI (‘’KOS zawał’’ program) | 5) Coexisting severe diseases of the immune, hematopoietic, or respiratory systems, or systemic diseases |
| Presence of a malignant tumour | |
| Death of a patient during hospitalization | |
| Incomplete clinical data in the medical records |
HF - heart failure; LVEF - left ventricular ejection fraction; MI – myocardial infarction.
Table 2.
Baseline characteristics of subgroups before and after matching.
|
Variable |
Pre-Match n (%) or mean ± SD or median (1-3 quartile) |
Post-Match n (%) or mean ± SD or median (1-3 quartile) |
||||
|---|---|---|---|---|---|---|
| ARNI subgroup n = 30 |
ACEI/ARB subgroup n = 46 |
Std. Mean Diff. |
ARNI subgroup n = 30 |
ACEI/ARB subgroup n = 30 |
Std. Mean Diff. |
|
| Age (years) | 58 ± 10 | 65 ± 10 | 0.708 | 58 ± 10 | 62 ± 10 | 0.388 |
| Men (%) | 27 (90%) | 31 (67.4%) | 0.567 | 27 (90%) | 26 (86.7%) | 0.102 |
| LVEF (%) | 30 (28;38) | 38 (33;40) | 0.704 | 30 (28;38) | 36 (33;39) | 0.451 |
ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin II receptor blocker; ARNI: angiotensin receptor–neprilysin inhibitor; LVEF: left ventricular ejection fraction, Std. Mean Diff.: standardized mean difference.
Table 8.
Comparison of clinical outcomes in ARNI and ACEI/ARB subgroups.
|
Clinical outcome |
ARNI subgroup n=30 n (%) or mean ± SD or median (1-3 quartile) |
ACEI/ARB subgroup n=30 n (%) or mean ± SD or median (1-3 quartile) |
p value |
|---|---|---|---|
| Deaths (n%) | 1 (3.3%) | 2 (6.7%) | 1.0 |
| Number of rehospitalizations (n%) | 0 | 3 (10%) | 0.24 |
ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin II receptor blocker; ARNI: angiotensin receptor–neprilysin inhibitor.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



